Harvard Trained Immunologist Demolishes California Legislation That Terminates Vaccine Exemptions
State of the Nation | April 23, 2015
SOTN Editor’s Note:
The following open letter by a PhD Immunologist completely demolishes the current California legislative initiative to remove all vaccine exemptions. That such a draconian and cynical state statute is under consideration in the ‘Golden State’ is as shocking as it is predictable. After all, it was mysteriously written and submitted shortly after the manufactured-in-Disneyland measles ‘outbreak’.
The indisputable science that is employed by Tetyana Obukhanych, PhD ought to be read by every CA legislator who is entertaining an affirmative vote for SB277. Dr. Obukhanych skillfully deconstructs the many false and fabricated arguments that are advanced by Big Pharma and the U.S Federal Government as they attempt to implement a nationwide Super-Vaccination agenda.
When the California Senate refuses to consider authoritative scientific evidence which categorically proves the dangerous vaccine side effects on the schoolchildren, something is very wrong. Such conduct by the Senate constitutes criminal action that endangers the lives and welfare of children. Their official behavior must be acknowledged for what it is — CRIMINAL — and prosecuted to the fullest extent of the law.
An Open Letter to Legislators Currently Considering Vaccine Legislation from Tetyana Obukhanych, PhD in Immunology
Re: VACCINE LEGISLATION
Dear Legislator:
My name is Tetyana Obukhanych. I hold a PhD in Immunology. I am writing this letter in the hope that it will correct several common misperceptions about vaccines in order to help you formulate a fair and balanced understanding that is supported by accepted vaccine theory and new scientific findings.
Do unvaccinated children pose a higher threat to the public than the vaccinated?
It is often stated that those who choose not to vaccinate their children for reasons of conscience endanger the rest of the public, and this is the rationale behind most of the legislation to end vaccine exemptions currently being considered by federal and state legislators country-wide. You should be aware that the nature of protection afforded by many modern vaccines – and that includes most of the vaccines recommended by the CDC for children – is not consistent with such a statement. I have outlined below the recommended vaccines that cannot prevent transmission of disease either because they are not designed to prevent the transmission of infection (rather, they are intended to prevent disease symptoms), or because they are for non-communicable diseases. People who have not received the vaccines mentioned below pose no higher threat to the general public than those who have, implying that discrimination against non-immunized children in a public school setting may not be warranted.
- IPV (inactivated poliovirus vaccine) cannot prevent transmission of poliovirus (see appendix for the scientific study, Item #1). Wild poliovirus has been non-existent in the USA for at least two decades. Even if wild poliovirus were to be re-imported by travel, vaccinating for polio with IPV cannot affect the safety of public spaces. Please note that wild poliovirus eradication is attributed to the use of a different vaccine, OPV or oral poliovirus vaccine. Despite being capable of preventing wild poliovirus transmission, use of OPV was phased out long ago in the USA and replaced with IPV due to safety concerns.
- Tetanus is not a contagious disease, but rather acquired from deep-puncture wounds contaminated with C. tetani spores. Vaccinating for tetanus (via the DTaP combination vaccine) cannot alter the safety of public spaces; it is intended to render personal protection only.
- While intended to prevent the disease-causing effects of the diphtheria toxin, the diphtheria toxoid vaccine (also contained in the DTaP vaccine) is not designed to prevent colonization and transmission of C. diphtheriae. Vaccinating for diphtheria cannot alter the safety of public spaces; it is likewise intended for personal protection only.
- The acellular pertussis (aP) vaccine (the final element of the DTaP combined vaccine), now in use in the USA, replaced the whole cell pertussis vaccine in the late 1990s, which was followed by an unprecedented resurgence of whooping cough. An experiment with deliberate pertussis infection in primates revealed that the aP vaccine is not capable of preventing colonization and transmission of B. pertussis (see appendix for the scientific study, Item #2). The FDA has issued a warning regarding this crucial finding.[1]
- Furthermore, the 2013 meeting of the Board of Scientific Counselors at the CDC revealed additional alarming data that pertussis variants (PRN-negative strains) currently circulating in the USA acquired a selective advantage to infect those who are up-to-date for their DTaP boosters (see appendix for the CDC document, Item #3), meaning that people who are up-to-date are more likely to be infected, and thus contagious, than people who are not vaccinated.
- Among numerous types of H. influenzae, the Hib vaccine covers only type b. Despite its sole intention to reduce symptomatic and asymptomatic (disease-less) Hib carriage, the introduction of the Hib vaccine has inadvertently shifted strain dominance towards other types of H. influenzae (types a through f).These types have been causing invasive disease of high severity and increasing incidence in adults in the era of Hib vaccination of children (see appendix for the scientific study, Item #4). The general population is more vulnerable to the invasive disease now than it was prior to the start of the Hib vaccination campaign. Discriminating against children who are not vaccinated for Hib does not make any scientific sense in the era of non-type b H. influenzae disease.
- Hepatitis B is a blood-borne virus. It does not spread in a community setting, especially among children who are unlikely to engage in high-risk behaviors, such as needle sharing or sex. Vaccinating children for hepatitis B cannot significantly alter the safety of public spaces. Further, school admission is not prohibited for children who are chronic hepatitis B carriers. To prohibit school admission for those who are simply unvaccinated – and do not even carry hepatitis B – would constitute unreasonable and illogical discrimination.
In summary, a person who is not vaccinated with IPV, DTaP, HepB, and Hib vaccines due to reasons of conscience poses no extra danger to the public than a person who is. No discrimination is warranted.
How often do serious vaccine adverse events happen?
It is often stated that vaccination rarely leads to serious adverse events. Unfortunately, this statement is not supported by science. A recent study done in Ontario, Canada, established that vaccination actually leads to an emergency room visit for 1 in 168 children following their 12-month vaccination appointment and for 1 in 730 children following their 18-month vaccination appointment (see appendix for a scientific study, Item #5).
When the risk of an adverse event requiring an ER visit after well-baby vaccinations is demonstrably so high, vaccination must remain a choice for parents, who may understandably be unwilling to assume this immediate risk in order to protect their children from diseases that are generally considered mild or that their children may never be exposed to.
Can discrimination against families who oppose vaccines for reasons of conscience prevent future disease outbreaks of communicable viral diseases, such as measles?
Measles research scientists have for a long time been aware of the “measles paradox.” I quote from the article by Poland & Jacobson (1994) “Failure to Reach the Goal of Measles Elimination: Apparent Paradox of Measles Infections in Immunized Persons.” Arch Intern Med 154:1815-1820:
“The apparent paradox is that as measles immunization rates rise to high levels in a population, measles becomes a disease of immunized persons.”[2]
Further research determined that behind the “measles paradox” is a fraction of the population called LOW VACCINE RESPONDERS. Low-responders are those who respond poorly to the first dose of the measles vaccine. These individuals then mount a weak immune response to subsequent RE-vaccination and quickly return to the pool of “susceptibles’’ within 2-5 years, despite being fully vaccinated.[3]
Re-vaccination cannot correct low-responsiveness: it appears to be an immuno-genetic trait.[4] The proportion of low-responders among children was estimated to be 4.7% in the USA.[5]
Studies of measles outbreaks in Quebec, Canada, and China attest that outbreaks of measles still happen, even when vaccination compliance is in the highest bracket (95-97% or even 99%, see appendix for scientific studies, Items #6&7). This is because even in high vaccine responders, vaccine-induced antibodies wane over time. Vaccine immunity does not equal life-long immunity acquired after natural exposure.
It has been documented that vaccinated persons who develop breakthrough measles are contagious. In fact, two major measles outbreaks in 2011 (in Quebec, Canada, and in New York, NY) were re-imported by previously vaccinated individuals.[6] – [7]
Taken together, these data make it apparent that elimination of vaccine exemptions, currently only utilized by a small percentage of families anyway, will neither solve the problem of disease resurgence nor prevent re-importation and outbreaks of previously eliminated diseases.
Is discrimination against conscientious vaccine objectors the only practical solution?
The majority of measles cases in recent US outbreaks (including the recent Disneyland outbreak) are adults and very young babies, whereas in the pre-vaccination era, measles occurred mainly between the ages 1 and 15. Natural exposure to measles was followed by lifelong immunity from re-infection, whereas vaccine immunity wanes over time, leaving adults unprotected by their childhood shots. Measles is more dangerous for infants and for adults than for school-aged children.
Despite high chances of exposure in the pre-vaccination era, measles practically never happened in babies much younger than one year of age due to the robust maternal immunity transfer mechanism. The vulnerability of very young babies to measles today is the direct outcome of the prolonged mass vaccination campaign of the past, during which their mothers, themselves vaccinated in their childhood, were not able to experience measles naturally at a safe school age and establish the lifelong immunity that would also be transferred to their babies and protect them from measles for the first year of life.
Luckily, a therapeutic backup exists to mimic now-eroded maternal immunity. Infants as well as other vulnerable or immunocompromised individuals, are eligible to receive immunoglobulin, a potentially life-saving measure that supplies antibodies directed against the virus to prevent or ameliorate disease upon exposure (see appendix, Item #8).
In summary: 1) due to the properties of modern vaccines, non-vaccinated individuals pose no greater risk of transmission of polio, diphtheria, pertussis, and numerous non-type b H. influenzae strains than vaccinated individuals do, non-vaccinated individuals pose virtually no danger of transmission of hepatitis B in a school setting, and tetanus is not transmissible at all; 2) there is a significantly elevated risk of emergency room visits after childhood vaccination appointments attesting that vaccination is not risk-free; 3) outbreaks of measles cannot be entirely prevented even if we had nearly perfect vaccination compliance; and 4) an effective method of preventing measles and other viral diseases in vaccine-ineligible infants and the immunocompromised, immunoglobulin, is available for those who may be exposed to these diseases.
Taken together, these four facts make it clear that discrimination in a public school setting against children who are not vaccinated for reasons of conscience is completely unwarranted as the vaccine status of conscientious objectors poses no undue public health risk.
Sincerely Yours,
~ Tetyana Obukhanych, PhD
Tetyana Obukhanych, PhD, is the author of the book Vaccine Illusion. She has studied immunology in some of the world’s most prestigious medical institutions. She earned her PhD in Immunology at the Rockefeller University in New York and did postdoctoral training at Harvard Medical School, Boston, MA and Stanford University in California.
Dr. Obukhanych offers online classes for those who want to gain deeper understanding of how the immune system works and whether the immunologic benefits of vaccines are worth the risks: Natural Immunity Fundamentals.
Appendix
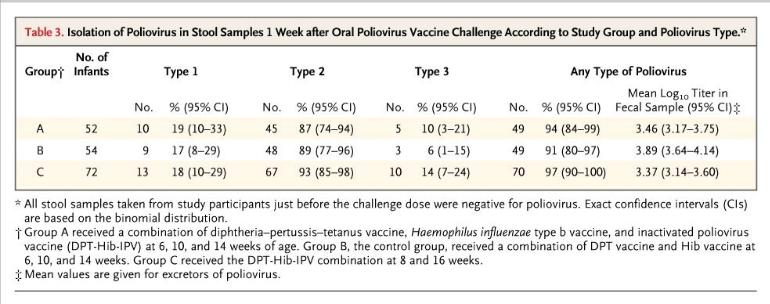
Item #1. The Cuba IPV Study collaborative group. (2007) Randomized controlled trial of inactivated poliovirus vaccine in Cuba. N Engl J Med 356:1536-44
http://www.ncbi.nlm.nih.gov/pubmed/17429085
The table below from the Cuban IPV study documents that 91% of children receiving no IPV (control group B) were colonized with live attenuated poliovirus upon deliberate experimental inoculation. Children who were vaccinated with IPV (groups A and C) were similarly colonized at the rate of 94-97%. High counts of live virus were recovered from the stool of children in all groups. These results make it clear that IPV cannot be relied upon for the control of polioviruses.
Item #2. Warfel et al. (2014) Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model.Proc Natl Acad Sci USA 111:787-92
http://www.ncbi.nlm.nih.gov/pubmed/24277828
“Baboons vaccinated with aP were protected from severe pertussis-associated symptoms but not from colonization, did not clear the infection faster than naïve [unvaccinated] animals, and readily transmitted B. pertussis to unvaccinated contacts. By comparison, previously infected [naturally-immune] animals were not colonized upon secondary infection.”
Item #3. Meeting of the Board of Scientific Counselors, Office of Infectious Diseases, Centers for Disease Control and Prevention, Tom Harkins Global Communication Center, Atlanta, Georgia, December 11-12, 2013
http://www.cdc.gov/maso/facm/pdfs/BSCOID/2013121112_BSCOID_Minutes.pdf
Resurgence of Pertussis (p.6)
“Findings indicated that 85% of the isolates [from six Enhanced Pertussis Surveillance Sites and from epidemics in Washington and Vermont in 2012] were PRN-deficient and vaccinated patients had significantly higher odds than unvaccinated patients of being infected with PRN-deficient strains. Moreover, when patients with up-to-date DTaP vaccinations were compared to unvaccinated patients, the odds of being infected with PRN-deficient strains increased, suggesting that PRN-bacteria may have a selective advantage in infecting DTaP-vaccinated persons.”
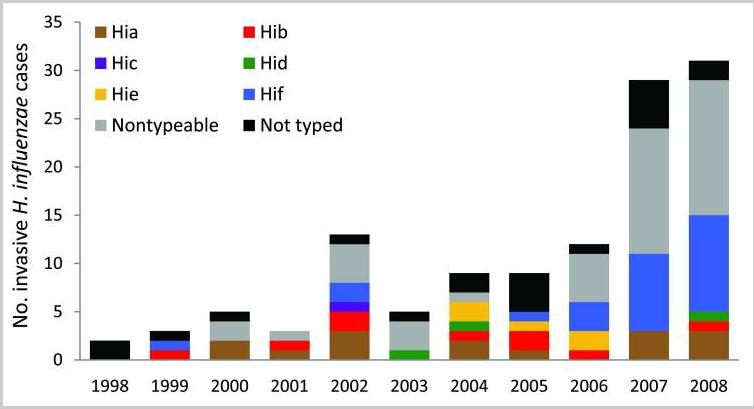
Item #4. Rubach et al. (2011) Increasing incidence of invasive Haemophilus influenzae disease in adults, Utah, USA. Emerg Infect Dis 17:1645-50
http://www.ncbi.nlm.nih.gov/pubmed/21888789
The chart below from Rubach et al. shows the number of invasive cases of H. influenzae(all types) in Utah in the decade of childhood vaccination for Hib.
Item #5. Wilson et al. (2011) Adverse events following 12 and 18 month vaccinations: a population-based, self-controlled case series analysis. PLoS One 6:e27897
http://www.ncbi.nlm.nih.gov/pubmed/22174753
“Four to 12 days post 12 month vaccination, children had a 1.33 (1.29-1.38) increased relative incidence of the combined endpoint compared to the control period, or at least one event during the risk interval for every 168 children vaccinated. Ten to 12 days post 18 month vaccination, the relative incidence was 1.25 (95%, 1.17-1.33) which represented at least one excess event for every 730 children vaccinated. The primary reason for increased events was statistically significant elevations in emergency room visits following all vaccinations.”
Item #6. De Serres et al. (2013) Largest measles epidemic in North America in a decade–Quebec, Canada, 2011: contribution of susceptibility, serendipity, and superspreading events. J Infect Dis 207:990-98
http://www.ncbi.nlm.nih.gov/pubmed/23264672
“The largest measles epidemic in North America in the last decade occurred in 2011 in Quebec, Canada.”
“A super-spreading event triggered by 1 importation resulted in sustained transmission and 678 cases.”
“The index case patient was a 30-39-year old adult, after returning to Canada from the Caribbean. The index case patient received measles vaccine in childhood.”
“Provincial [Quebec] vaccine coverage surveys conducted in 2006, 2008, and 2010 consistently showed that by 24 months of age, approximately 96% of children had received 1 dose and approximately 85% had received 2 doses of measles vaccine, increasing to 97% and 90%, respectively, by 28 months of age. With additional first and second doses administered between 28 and 59 months of age, population measles vaccine coverage is even higher by school entry.”
“Among adolescents, 22% [of measles cases] had received 2 vaccine doses. Outbreak investigation showed this proportion to have been an underestimate; active case finding identified 130% more cases among 2-dose recipients.”
Item #7. Wang et al. (2014) Difficulties in eliminating measles and controlling rubella and mumps: a cross-sectional study of a first measles and rubella vaccination and a second measles, mumps, and rubella vaccination. PLoS One9:e89361
http://www.ncbi.nlm.nih.gov/pubmed/24586717
“The reported coverage of the measles-mumps-rubella (MMR) vaccine is greater than 99.0% in Zhejiang province. However, the incidence of measles, mumps, and rubella remains high.”
Item #8. Immunoglobulin Handbook, Health Protection Agency
HUMAN NORMAL IMMUNOGLOBULIN (HNIG):
Indications
- To prevent or attenuate an attack in immuno-compromised contacts
- To prevent or attenuate an attack in pregnant women
- To prevent or attenuate an attack in infants under the age of 9 months
[1] http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm376937.htm
[2] http://archinte.jamanetwork.com/article.aspx?articleid=619215
[3] Poland (1998) Am J Hum Genet 62:215-220
http://www.ncbi.nlm.nih.gov/pubmed/9463343
“ ‘poor responders,’ who were re-immunized and developed poor or low-level antibody responses only to lose detectable antibody and develop measles on exposure 2–5 years later.”
[4] ibid
“Our ongoing studies suggest that seronegativity after vaccination [for measles] clusters among related family members, that genetic polymorphisms within the HLA [genes] significantly influence antibody levels.”
[5] LeBaron et al. (2007) Arch Pediatr Adolesc Med 161:294-301
http://www.ncbi.nlm.nih.gov/pubmed/17339511
“Titers fell significantly over time [after second MMR] for the study population overall and, by the final collection, 4.7% of children were potentially susceptible.”
[6] De Serres et al. (2013) J Infect Dis 207:990-998
http://www.ncbi.nlm.nih.gov/pubmed/23264672
“The index case patient received measles vaccine in childhood.”
[7] Rosen et al. (2014) Clin Infect Dis 58:1205-1210
http://www.ncbi.nlm.nih.gov/pubmed/24585562
“The index patient had 2 doses of measles-containing vaccine.”
28 Comments »
Leave a comment
Featured Video

Iran’s POSITION On Israel And Gaza w/Professor Marandi
or go to
Aletho News Archives – Video-Images
Interview
Interview with Paul Collits
An Australian Hero
Lies are Unbekoming | May 7, 2025
Paul Collits is a hero to me.
Of all the interviews I have done so far, with so many amazing people, this is the most personal and significant.
In the darkest of the dark days, the people that I relied on the most to triangulate my sanity were Paul Collits, Michael Yeadon, Malcolm Kendrick, and Jeffrey Tucker.
Paul was different in two ways. … continue
Blog Roll
Recent Comments
Alovato on MTG Says ‘Uniparty’ Win Saving… roberthstiver on Protecting Israel Is Washingto… peterjohnarnold on Palestine activists smash into… peterjohnarnold on Dutch police smash pro-Palesti… peterjohnarnold on US tries to pressure Southeast… peterjohnarnold on US Coast Guard Polar Icebreake… Balthasar Gerards on Russia issues military ultimat… roberthstiver on Target Israel and we’ll target… peterjohnarnold on Russia issues military ultimat… peterjohnarnold on Israel/Gaza: The Masks Come Of… peterjohnarnold on PA demands Marwan Barghouti be… Balthasar Gerards on Belgium working on Israel…
 Aletho News
Aletho News- Poles taking to the streets against EU Green Deal
- US losing ground globally to Russia and China – report
- Mass immigration has ‘utterly failed’ Britain as new report debunks myths of economic growth and fiscal benefits
- MTG Says ‘Uniparty’ Win Saving Johnson’s Speakership Will Mean More Money for Foreign Wars
- Malaysia tells US it doesn’t recognise sanctions imposed unilaterally
- UK Fire Brigades Union calls on members not to help police remove pro-Palestine protesters
- ‘Israel’ destroyed 53% of Gaza’s water treatment facilities: BBC
- Will a Gaza ceasefire be as successful as the two-state solution?
- Turkiye renews supply of construction materials to Israel despite trade ban
- Protecting Israel Is Washington’s Number One Job
- If Americans Knew
- Punishments Rise as Student Protests Escalate
- Biden withholds weapons shipment over Rafah invasion, as Gazans flee – Day 215
- “Yes, it is genocide” –Israeli genocide scholar
- Israeli Destruction of Gaza: The Facts
- Cruelty of language: Leaked NY Times memo reveals moral depravity of US media
- AIPAC Is Secretly Intervening In Portland’s Congressional Race To Take Down Susheela Jayapal, Sources Say
- Drone footage raises questions about Israeli justification for deadly strike on Gaza journalists
- Terrifying Israeli attack on Rafah, more mass graves, more int’l law violations – Day 214
- Journalism professors call on New York Times to review Oct. 7 report
- Here Are the Top Recipients of AIPAC Money
- Richie Allen
- The Richie Allen Show Returns Tomorrow Wednesday April 24th
- Call Richie Today Monday March 11th From 4.30pm
- Connect To The Richie Allen Show WhatsApp Today
- NHS Asks Patients To Choose From 12 Genders, 10 sexual Preferences & 159 Religions
- The Richie Allen Show Moves To A New Time Slot From Monday Nov 20th
- Starmer Will Sack Shadow Ministers Who Vote For Gaza Ceasefire
- AI Tool Can Predict Heart Attacks Years In Advance
- Nepal Bans TikTok To Preserve Social Harmony
- Bloke Appointed Boss Of Womb Health Charity
- WHO – “Gaza’s Biggest Hospital Becoming A Cemetery”
- No Tricks Zone
- DNA Evidence Reveals Domestic Cats, Dogs, African Wildcats, Frogs Lived In The Arctic 9000 Years Ago
- -80°C: Antarctic Vostok Station Records “Extreme Winter Cold”…Not Even Winter Yet!
- The German E-Vehicle Nightmare, 2024 Q1 Sales Plummet 14%… “Graveyard” For Unsold Cars
- Newly Discovered 90,000-Year-Old Human Footprints Reveal How Much Higher Sea Levels Used To Be
- Germany’s Economic Bloodbath Worsens As Green Revolution Causes Economy To Bleed To Death
- Water Vapor Absorbs 84 Times More Radiation Than CO2 … Clouds Drove 89% Of 1982-2018 Warming
- The 97% Consensus Claim Is In Fact 97% Bogus
- Post-1980s Increases In Shortwave Radiation Explains Europe’s Warming Trends Far Better Than CO2
- “A Thing Where Every Part Of Your Life Just Confirms What It Is That You Want To Believe”
- Nature Publication: Researchers Find Arctic Region 10,000 Years Ago Warmer Than Today

Reblogged this on The Tin Foil Hat Society and commented:
I am NOT anti vax. As I’ve stated a multitude of times before. I AM common sense, pro-informed consent (and by that I mean FULLY informed, not given a one page sheet with basically nothing of note on it produced by the CDC), pro-parents’ rights. This being said, there is nothing to argue with in the 6 numbered items and I completely agree. I wish more people knew this.
LikeLike
Thank you for the informative article. Educational letters/articles with good scientific research with links to valid studies are in short supply these days. However, the letter only addresses some vaccines, not even half of which are recommended. What about the others? Could you please share that info as well? Also, immunoglobulin is extremely expensive and many insurances dont cover it. It would surprise me if medi-cal does cover it. In addition, living in a rural community, I dont believe that many children are diagnosed soon enough to receive immunoglobulin…and especially when having to wait on insurance authorization. Would you please address these issues? I loom forward to learning more.
Thank you,
Laysha
LikeLike
thank you Dr. Tetyana for your efforts to perhaps help parents a little paranoid about those of us who choose not to immunize
LikeLike
Well if they are paranoid, remind the ones about to have a baby, to AVOID anyone pertussis vaccinated, with or without symptoms. Tell them to get throat swabs themselves, and their kids…………. to make sure they are not carriers. Unvaccinated people, never have the worry of being symptomless carriers.
LikeLike
These transcripts need to be sent to the legislature in Ca and the bull headed governor there–that guy studied in a Jesuit seminary and did not learn much about the sanctity of life and freedom of religion as well as the bill of rights and informed consent–that is grounds for a recall—how did he come back and become governor after already serving 2 terms in the 1970’s-he should have stayed with Linda Ronstedt and learned a thing or two about humanity!
LikeLike
Well in Australia, it is even being reported in Mainstream media, that pertussis outbreaks are happening amongst the fully vaccinated. The Health Department is fully aware that pertussis can be carried, and spread to babies, by those vaccinated (without them having the illness themselves). However the final line is always, get vaccinated…… why? when they just said that is causing the problem. Then we have a stupid Health Minister, on video, in a kindy full of kiddies just give massive hypodermics to jab dollies in ears, bums, eyes…….. and the Health Minister blames non vaccinated for the outbreaks of Whooping cough? What hope have we got, with idiots running out country, especially female health ministers, who know zero about health.
LikeLike
thank you wapd! have always ! you always have helped me with all your truths!
LikeLike
Yes! I think about this often. I try to listen to hear if children discuss shots, and then I know to keep ours away because of shedding.
LikeLike
I’d love to see research on how contagious children are following the varicella and MMR vaccines. I am one of several cases of shingles related to being around a child following the varicella vaccine. Perhaps children could be given a tag to wear to warn those of us with poor immune systems so that we might avoid them.
LikeLike
My son got Ruebella from being around a recently vaccinate kid. I was not concerned because he is young and has a good immune system. He got over it and now has lifetime immunity without the risk associated with the vaccine. The problem is that nobody tells parents that they and their children can be contagious because of the vaccines. For people like you with weakened immune systems, they can be very dangerous. I agree that they should be made to warn people in some way that they have been recently vaccinated.
LikeLike
One scientist, despite his academic background, will never have a voice strong enough to disprove the governments concerns. I agree with his justification to remove some of the mandatory vaccinations (summary 1) and that availability of effective treatment of certain diseases post infection could be used as a justification to remove others (summary 4). But the risk of children visiting the emergency room (summary 3) and peoples resistance to certain vaccines (summary 4) do not out weigh the risk of air born diseases spreading like wild fire. This shows a lack of risk perception because “the success of vaccines is one of the reasons that people are less likely to vaccinate their children.”
The videos below address the concerns about the anti-vaccination uprising that has lead to the consideration of this draconian law. I am pro choice, but the high degree of biased thinking, that we are all susceptible of, is the real source of the problem, and unless we can find a way to change that, this type of law is , debatably, is the lesser of two evils.
https://www.youtube.com/watch?v=kjFPUoIXd80 https://www.youtube.com/watch?v=Rzxr9FeZf1g
LikeLike
Kevin -Coercion is EVIL no matter how you try to sell it. The vaccine issue is all about profit and they don’t care how many kids get damaged by the multitude of toxic laden vaccines. The whole program is an utter failure and fraud. I remember as a child the Doctor stated vaccines gave lifelong immunity. What a joke that is as we know today they are giving booster after booster. Why because they don’t work. If YOU want to believe the snake oil salesman go right ahead but using the force of government to use Coercion on the most vulnerable of us (the children) is criminal and these corporate officers and government officials should be jailed or worse.
LikeLike
But vaccines dont work, so I disagree, I would not vaccinate children at the present time (if allowed free choice), because THEY DONT WORK. I work in the pathology area. And, I remember how healthy kids were, pre over the top vaccines……….. Mumps vaccine lasts around 2 years, pertussis vaccine lasts an average of less than 4 years, flu vaccine works in 18% of cases but those people are twice as likely to get ill from something else. In Australia they now vaccinate for a meningoccocal strain, THAT HAS NEVER KILLED ANYONE………… WHY? Because it makes pharma MONEY!
LikeLike
Would no government be better than government?
LikeLike
wonderful, well written, backs up everything I have researched, and that I have experienced……… I tested during 2010 pertussis outbreaks in Australia. the vaccines are failures!
LikeLike
No risky medical procedure should be forced on anyone.
LikeLike
So, lets come up with several vaccination recommendations that make sense and give them on a schedule that in suggestively tolerable.
LikeLike
“It is often stated that vaccination rarely leads to serious adverse events. Unfortunately, this statement is not supported by science. A recent study done in Ontario, Canada, established that vaccination actually leads to an emergency room visit for 1 in 168 children following their 12-month vaccination appointment and for 1 in 730 children following their 18-month vaccination appointment (see appendix for a scientific study, Item #5).
When the risk of an adverse event requiring an ER visit after well-baby vaccinations is demonstrably so high, vaccination must remain a choice for parents, who may understandably be unwilling to assume this immediate risk in order to protect their children from diseases that are generally considered mild or that their children may never be exposed to.”
This is extremely disingenuous. That means that 0.68% and 0.0013698630137% of children have adverse reactions. That is less than the danger of like…almost any human activity. More people die in their sleep every day than that, meaning that the argument that sleep is more dangerous than vaccines could be made (if correlation equaled causation).
In addition to this, that sort of claim leaves out the fourth column in the statistics…how many babies out of the same population number go to the hospital emergency room anyway? All it says is that they went after the vaccination…what are the number of babies that go no matter what, just by chance, to compare the number vaccinated to?
LikeLike
Actually, Neal, if .68% of people died in their sleep every night we would all live less than 168 days.
LikeLike
^^that :)
LikeLike
Thanks for being an educated voice in the ridiculous one sided propaganda exercise labeled “vaccination “
LikeLike
LikeLike
I understand that diphtheria toxoid vaccine is only for personal safety. But, aren’t infected people contagious?
“Diphtheria is very rare in the United States and Europe, where health officials have been immunizing children against it for decades. However, it’s still common in developing countries where people are living in crowded or unclean conditions, aren’t well nourished and immunizations aren’t given routinely.”
http://m.kidshealth.org/parent/infections/lung/diphtheria.html
LikeLike
Book review vaccine illusion” from amazon:
“Written for those with an eager ear against vaccine, not as an immunologist for those who want a balanced well rounded analysis.
ByFei Liuon February 21, 2013
Verified Purchase
I am also a fellow immunologist that studied vaccines, and a mother of two, and I was eager to read this book because I was hoping that a scientist will provide an honest balanced narration of the history, efficacy and future challenges of vaccine programs, and raise some real questions that is worthy of thoughts. However this book can make Fox News and MSNBC News seem fair and balanced.
I intend to write a full length review approximately the same length as the book itself, with proper references to the statements I make. But it will take time, and I don’t want more readers mislead by the lack of negative reviews, so here is a shorter version.
Here are the major problems I have with this book:
1) Lack of reference. The author make various statements which are critical for her stance against vaccination that is not reference at all. For example, she claimed that Jenner’s smallpox vaccine was only effective for an undefined “a few years”, and yet, all my searches yielded rather long effectiveness of vaccinia vaccine ([…]). The author seems to choose references that would suit her argument but ignore those that contradict hers.
2) Totally biased. I guess I can’t really blame her for writing a book titled “Vaccine Illusions” and only criticize the efficacy of vaccines, but what I have a problem with is her disguising this book as a scientific book that can be used to educate parents who are trying to make vaccine choices. No, this book is for those who have already made up their mind to not vaccinate their children and are looking for validation for such a decision from somebody that can be perceived as “credible”. This book has never given any figures on the widely available data from WHO on the amount of deaths for each vaccine preventable diseases before and after each vaccine campaign. Nor did she ever mention the frequencies of disease outbreaks among those who are vaccinated vs those who are not. Yet, she raises questions that seems legit to the untrained eyes, but totally idiotic to those who studies immunology. For example, she mentioned that tetanus toxoid acts in the CNS, mentioned that antibodies can not cross blood brain barrier, then asked seemingly intelligently:”Then how does antibodies protect you from the toxin?” Any Stanford trained immunologist would sure know that antibodies constantly circulating your blood would prevent any toxin from ever getting to the brain from your infection site. Questions like this makes me believe that the author was intentionally deceiving her audience. Another example, she mentioned original antigenic sin, and attribute flu vaccination as a culprit. However, she did not mention that original antigenic sin was first discover not with vaccination, but rather actual viral infection with similar viruses. And since the author knows quite well that actual virus infection leaves with stronger memory immunity, and as she claims vaccination is not effective for a few years, one could easily argue that getting the flu would leave you way more susceptible to original antigenic sin than getting the vaccine itself.
3) Raise questions about vaccine that she knows that can not be answered the way she wanted, and use that to discredit all vaccine studies. For instance, one of her problems with vaccine is that it’s efficacy is not directly tested with a real infection. She knows that no human trials where people are given the actual virus/bacteria will ever be approved. Yet, she takes in no consideration of the very low mortality rate directly due to any diseases in countries that have vaccine programs versus the high rate in countries that do not have vaccine programs, or even historical data in the same country.
4) Make vaccine immunity as your only line of defense so that it better be perfect or you are screwed. The most widely mistaken fact about vaccine is that it has to protect a person from ever getting infected. Vaccine would rarely prevent you from being infected, in most cases, it buys you enough time so your own immune system would keep the infection under control so that you would show no symptoms of infection; in some cases, you still show symptoms but less severe; and if the vaccine is a good one, you would rarely have full symptoms. Vaccine safety is a huge issue for vaccine producers, and CDC takes it very seriously, and there is a national vaccine safety hotline for each vaccine. Therefore vaccines should be viewed more as an extra safety net to lessen the assault of an infection on your own immune system. Some of the questions author raised is legit, such as reduced amount of antibodies in breast milk of mothers who are vaccinated vs those who had the disease. However, author did not mention that without vaccines, some people never got a chance to become mothers.”
LikeLike
When i was growing up I had the Measels the mumps and chicken pox and so di most kids, we did not have vaccines for these and I never heard of anyone dying of them either. Our immune systums worked to keep us from getting them again for lifetime. Why did the medical community change from allowing the natural progression of these deseases be messed with? I believe it was big Pharma that pushed for that and now people just believe they have to get those vacines.
LikeLike
Nice try. Outbreaks of vaccine preventable diseases in communities with low immunization rates show that the over-intellectualization of vaccine studies and incorrect conclusions in the above attempt to persuade legislators is not in the public interest. Fortunately SB277 passed. Correct logic prevailed. Still, there are vaccine denier groups where you can find solace and mutual agreement to avoid vaccines. Only known TRUE medical risks are legitimate contraindications to recommended vaccination. I hope other states follow California’s lead
LikeLike
thanks for good writing
LikeLike
I randomly picked one of your papers you mentioned here (Item #6. De Serres et al. (2013) Largest measles epidemic in North America in a decade–Quebec, Canada, 2011: contribution of susceptibility, serendipity, and superspreading events. J Infect Dis 207:990-98
http://www.ncbi.nlm.nih.gov/pubmed/23264672)
Have you actually read it?
It completely states different things that what you state here !
For example:
Two-dose recipients had milder illness and a significantly lower risk of hospitalization than those who were unvaccinated or single-dose recipients.
It says it literally!
WTF
You are just only showing what is good for your anti vaccination story
LikeLike