The pandemic is over. Yet two key pieces remain that should concern everyone.
Lets talk about the COVID shot. Still being mandated (recommended) by East and West Coast Health Alliances comprising 14 states all the way down to infants.
Why? To stick it to Kennedy? To ‘follow the science’‘? To secure a market as demand tanks? Who knows for sure but here we are.
The COVID shot was birthed in fraud and failed science. That is the true legacy media pundits won’t tell you.
As the first cases of coronavirus happened in the U.S., Moderna and Pfizer began designing their mRNA vaccine candidates.
Meanwhile, Bill Gates pulled the trigger. A Fauci files/diary email from Gates to Fauci asks the NIAID director for “changes or additions” to Gates’ masterplan titled simply Pandemic I.
Gates’ document, given the stamp of approval from Fauci, stated:
“The goal is to pick the one or two best vaccine constructs and vaccinate the entire world—that’s 7 billion doses if it is a single-dose vaccine, and 14 billion if it is a two-dose vaccine.
How about 9-12 doses? That is what has been recommended to date for adults and immunocompromised respectively.
Far from a stranger, Gates and his foundation were fraudulently close to U.S. agencies funding pieces of NIH and receiving private briefings from DARPA on biological threats. More on that in another report.
FAUCI KILLS EARLY TREATMENT
Under Section 564 of the FD&C Act, FDA can grant the emergency use for a medical countermeasure (the vaccine) because, as revisionist history tells, there was no approved alternatives adequately available for diagnosing, preventing, or treating the disease.
The guidelines and experiences used at the start of the pandemic from pioneers like Peter McCullough’s protocol, New York family physician Dr. Vladimir Zelenko’s protocol, Texas Dr. Richard Bartlett nebulized budesonide, Front Line COVID-19 Critical Care Alliance’s ivermectin push and so many others using similar treatments with repeated success and real-world results tells a different story.
Evidence that would have effectively ended the FDA EUA vaccine hunt.
Didn’t matter to Fauci and the captured U.S. regulatory agencies. Their job was to kill those ideas and pave the way for the coming experimental, world-injecting gene therapy.
Fauci files/diary explains how it was done at the highest level. March 2020, two months into the first U.S. cases Fauci finds himself in a high-level White House Meeting and writes:
“A friend of POTUS… said that he heards [sic] that someone gave Hydroxychloroquine (HC) to 51 people and 51 got better. POTUS has heard similar stories, including Remdesivir (R) about other drugs and wants to make these available. To my amazement and dismay, Azar said that he could approve HC and Remdesivir now with the powers that he has. Steve Hahn and to some extent Deb and Bob started to chime in that this would give people hope. I took a deep breath and said that this was wrong and should not be done.”
None of the trials were designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor were the vaccines being studied to determine whether they can interrupt transmission of the virus. (*I was the first journalist to report this in October 2020)
FDA and VRBPAC votes were near unanimous to get them to market and in American arms while legacy media ‘journalists’ and their ‘experts’ like Fauci and others touted the shot’s transmission-stopping magical qualities. While Influencers and celebrities sucked up $911 million of taxpayer money for their injectable PR efforts.
There was just one problem. The shot didn’t stop transmission. And it didn’t perform against mutations. In short, it was worthless and gave false hope with a growing profile of side effects (harms).
September 2021 Fauci writes:
“… there is a concern about safety regarding myocarditis for younger people, mostly men; however, once this is taken care of in my mind there is no reason not to vaccinate essentially everyone.”
Heart damage from the shot was never “taken care of” and still remains a concern and risk to this day especially for young men.
January 2021, world-renowned HIV virus researcher Dr. David Ho shares immediate concerns about the COVID shot’s performance according to Fauci’s diary:
“David Ho is doing tests on convalescent sera and sera of people who were vaccinated and is finding disturbing data in both the UK and worse in the RSA mutants. It looks like the vaccine might be compromised.”
Fauci continues:
“Had regular every 2 weeks call with Bill Gates – Bill and Trevor Mundel know about the issue with the mutations that David Ho is working on.”
What exactly were Dr. Ho’s warnings? Dr. Ho writes to Fauci the following:
“It is quite clear that these two variants could now resist several classes of neutralizing monoclonal antibodies already used in the clinic or still in development, and in most cases we understand which of the mutations are conferring the resistance.”
Ho continues:
“… a large majority of convalescent plasma samples showed an appreciable loss in activity against the new variants, suggesting re-infection may be more likely when confronted with either of these two strains.”
And then the death blow to the non-transmission-stopping COVID shot as Ho writes:
“Finally, we also observed a significant impact on vaccinee sera in that every serum sample tested showed a substantial loss in neutralizing activity against the SA variant, whereas the loss in activity against the UK virus is not as large or as universal. Again, we believe the latter findings should be shared promptly with the field, because these new strains threaten the effectiveness of the current vaccines.”
The very next day, Fauci writes in his diary:
“Had Zoom briefing of Biden and Harris to prep them for the speech that Biden will give at 3:45 PM on the vaccine rollout plan. We briefed him at 2:30 to 3:30 and he and Harris (only he spoke) gave briefing to the Nation.”
No word of the vaccine issues, mutations or danger now scientifically evident.
It later became clear that Ho was not only right, but his warnings were mild compared to the reality that unfolded. UK COVID vaccine surveillance data began showing the shots were not only failing to prevent infection but they are making you more vulnerable to it.
2022 data suggested that in all age groups COVID vaccines were demonstrating negative efficacy. That means, the vaccinated were at greater risk of infection than the unvaccinated.
Meanwhile, that same year Fauci writes:
“More drama with regard to the CDC and Rochelle Walenski. After much going back and forth between the CDC and the other docs including me… we thought we had gotten them pulled back from making the statement that the vaccines were not effective at all in preventing infection and transmission…
Why? As Fauci writes, “it would undermine the DoJ’s efforts at mandates for vaccines under certain circumstances.”
In the end, CDC director at the time Walensky who, as Fauci writes, called him “… her hero, her mentor, her friend… agreed to pull back on the statement of absolute lack of efficacy of vaccines against infections and transmission.”
Throughout all this, Fauci went to bat for Big Pharma indemnity in 2021 as he pens in his diary:
“I had an important zoom meeting today with Larry Corey an Emilio Emini about the same subject as above, namely, how the United states can play a major proactive role in getting mRNA vaccines to the developing world. Apparently there are liability issues that the pharmaceutical companies are concerned with. These revolve around the fact that although the United States government can indemnify the companies against lawsuits here in the United states the companies feel that they are liable to being sued for adverse outcomes by people in the countries to whom they’re providing vaccine. Some mechanism needs to be worked out to address this concern.”
(Emilio Emini was Chief Executive Officer at the Bill & Melinda Gates Medical Research Institute and Larry Corey head of COVID-19 Prevention Network collaboration formed by Fauci)
The shot is still protected by the PREP Act which was extended until 2029 by outgoing HHS Secretary Xavier Becerra (now in the running for California Governor).
The Countermeasures Injury Compensation Program (CICP) meant to field harms from the COVID shot is a black hole and sick joke. Kennedy is attempting to create a table of accepted injuries to ease compensation efforts for the injured public. Is this enough? Not by a long shot.
(*No artificial intelligence was used to write this article. Just a genuine human… me)
The US Senate Homeland Security Committee has voted to hold Dr. Anthony Fauci in contempt after the former White House coronavirus czar refused to answer questions on the origins of Covid-19 at a hearing last week.
The Republican-led committee voted 8-7 along party lines to hold Fauci in contempt on Thursday. The committee’s Democrats introduced five motions aimed at postponing the vote, but all were shut down by the Republican majority.
Fauci appeared before the committee last Wednesday, where he was grilled on his role in funding dangerous gain-of-function research at the Wuhan Institute of Virology in China, his knowledge that Covid-19 was likely created in a laboratory, his work with US intelligence agencies, and his promotion of ineffective vaccines against the virus.
The former bureaucrat refused to answer any questions, invoking his Fifth Amendment right to silence more than 100 times. Fauci pleaded the Fifth despite having already received a pardon from former President Joe Biden shielding him from criminal prosecution over any offense committed between January 1, 2014 – when the US first outsourced gain-of-function research to China – and January 20, 2025.
“More than a million Americans died from Covid,” committee chairman Rand Paul said before Thursday’s vote. “Many of them died alone. Workers were forced to choose between a mandate and a job they needed. Businesses closed and never reopened. Americans lost the freedom to work, to worship, and to decide what went into their own bodies.”
“Dr. Fauci faced no risk of federal prosecution,” Paul continued. “All he had to do was tell the truth.”
Although Fauci is immune from prosecution for any misdeeds that he committed between 2014 and 2025, his pardon does not cover any crimes committed at last week’s hearing. Contempt of Congress is a criminal offense, and Paul referred Fauci’s case to the US Justice Department immediately after Thursday’s vote.
Should the department choose to prosecute, Fauci could face a fine of up to $100,000 and a prison sentence of up to 12 months.
Peter Navarro and Steve Bannon, both former aides to US President Donald Trump, were jailed for contempt of Congress by Biden’s Justice Department. Navarro and Bannon both spent four months in prison in 2024.
Fauci served as the director of the National Institute of Allergy and Infectious Diseases (NIAID) from 1984 to 2022, and as chief medical adviser to Biden from 2021 until his retirement in 2022. In the latter role, Fauci became the face of Biden’s heavy-handed response to the pandemic, advocating mask and vaccine mandates and lockdowns, and dismissing opposition to these measures as “anti-science.”
That bottle of sunscreen in your beach bag may be doing more harm than good. New research reveals the hidden dangers lurking in conventional sunscreens and highlights safer, natural alternatives that can protect your skin without toxic side effects.
For decades, we’ve been told that slathering on sunscreen is one of the best ways to protect our skin from the sun’s harmful rays. However, mounting evidence suggests that many conventional sunscreens contain ingredients that may be hazardous to our health and the environment. From hormone-disrupting chemicals to potentially carcinogenic nanoparticles, the risks associated with common sunscreen ingredients are cause for serious concern.
At the same time, researchers have discovered that many natural plant oils offer significant sun protection, often rivaling or exceeding the SPF of chemical sunscreens. These botanical alternatives not only shield skin from UV damage, but also nourish and moisturize without introducing synthetic toxins into the body.
This article will explore the dangers lurking in your sunscreen bottle, examine promising research on herbal oil alternatives, and provide practical guidance for safer sun protection. By understanding the risks and exploring natural options, you can make informed choices to safeguard your skin and overall health.
The Trouble with Conventional Sunscreens
Chemical Cocktails: Questionable Ingredients in Popular Sunscreens
Many best-selling sunscreens contain a slew of synthetic chemicals that act as UV filters, preservatives, fragrances and more. Some of the most concerning ingredients include:
Oxybenzone: This common chemical UV filter has been shown to disrupt hormones, cause allergic reactions, and damage coral reefs. Studies have found oxybenzone in 97% of Americans tested.1
Octinoxate: Another chemical filter linked to hormone disruption and environmental damage. It’s been banned in Hawaii and Key West due to its impact on coral.2
Homosalate: An endocrine disruptor that may increase the absorption of pesticides through the skin.3
Octocrylene: Can produce free radicals that may damage cells and accelerate skin aging when exposed to UV light.4
Parabens: Synthetic preservatives with estrogenic activity, detected in breast cancer tumors.5
Fragrance: Often contains undisclosed phthalates linked to reproductive issues and cancer.6
The Nanoparticle Problem: Are Mineral Sunscreens Any Safer?
In response to concerns over chemical sunscreens, many consumers have turned to mineral-based formulas containing zinc oxide or titanium dioxide. While these ingredients are generally considered safer, the increasing use of nanoparticles in mineral sunscreens has introduced new risks:
Potential for cellular damage: Nanoparticles may be small enough to penetrate skin cells and cause oxidative damage to DNA.7
Respiratory concerns: Inhaling nanoparticles from spray sunscreens could potentially cause lung inflammation or damage.8
Environmental impact: Like chemical UV filters, nanoparticles can accumulate in waterways and harm aquatic life.9
Systemic absorption: A 2010 study found that nanoparticle zinc oxide from sunscreen was detectable in human blood and urine after topical application.10
The Skin Absorption Dilemma
One of the biggest issues with conventional sunscreens is their potential for systemic absorption through the skin. Multiple studies have detected common sunscreen chemicals in blood, urine, and breast milk after topical use.11,12
This is concerning because the skin is not merely a barrier, but a permeable organ capable of absorbing substances into the bloodstream. In fact, transdermal drug delivery systems take advantage of this property to administer medications through the skin.
When it comes to sunscreen, we’re essentially slathering a chemical cocktail over a large surface area of our bodies, often repeatedly throughout the day. This creates significant potential for absorption and accumulation of questionable ingredients in our tissues over time.
Understanding SPF: Debunking the High Number Myth
Before exploring natural alternatives, it’s important to understand what Sun Protection Factor (SPF) really means. Many consumers believe that higher SPF numbers offer dramatically better protection, but the reality is more nuanced:
SPF measures how much longer skin covered with sunscreen takes to burn compared to unprotected skin. For example, SPF 2 means you can stay in the sun twice as long before burning compared to wearing no sunscreen.
However, the percentage of UVB rays blocked doesn’t increase linearly with SPF numbers:
SPF 2 blocks 50% of UVB rays
SPF 15 blocks about 93% of UVB rays
SPF 30 blocks about 97% of UVB rays
SPF 50 blocks about 98% of UVB rays
As you can see, the difference between SPF 30 and SPF 50 is only 1% in terms of UVB protection. This reveals a common misconception that very high SPF values are necessary for adequate sun protection. In reality, even a relatively low SPF of 15 blocks 93% of UVB rays, and an SPF of just 2 cuts UVB exposure in half.
While higher SPFs do offer incrementally more protection and may be beneficial for those with very fair or sensitive skin, the difference is not as dramatic as many people assume. This understanding is crucial when considering natural alternatives, which may have lower SPF values but still offer significant protection.
Environmental and Health Consequences
Beyond personal health concerns, conventional sunscreens pose serious risks to the environment:
Coral reef destruction: Oxybenzone and octinoxate have been implicated in coral bleaching, leading to bans in reef-adjacent areas.13
Aquatic toxicity: Sunscreen chemicals can accumulate in lakes and oceans, harming fish and other marine life.14
Soil contamination: UV filters have been detected in agricultural soils, with unknown impacts on crops and ecosystems.15
The cumulative effects of widespread sunscreen use are just beginning to be understood. As these chemicals build up in our bodies and the environment, they may contribute to a range of health and ecological issues:
Hormone disruption and reproductive problems
Increased risk of certain cancers
Allergies and skin irritation
Coral reef die-offs and marine ecosystem collapse
Contamination of water supplies
Natural Alternatives: Herbal Oils as Sunscreen
In light of the risks associated with conventional sunscreens, many consumers are seeking safer, more natural alternatives. Emerging research suggests that certain plant-based oils may offer significant sun protection without the drawbacks of synthetic chemicals.
A groundbreaking 2010 study published in Pharmacognosy Research evaluated the SPF (sun protection factor) of various herbal oils commonly used in cosmetics. The researchers used a spectrophotometric method to determine the in vitro SPF values of both volatile and non-volatile herbal oils.16
Their findings revealed impressive sun protection potential in many natural oils:
These results are particularly noteworthy because many of the oils tested demonstrated significant UV protection levels. For example, olive oil with 87.5% UV protection (SPF 8) is substantial considering it’s a natural, non-toxic alternative. Also, consider the vast number of therapeutic actions olive oil demonstrates in the scientific literature.
It’s important to remember that even oils with lower protection values, such as tea tree oil at 50% (SPF 2), still cut UVB exposure in half compared to unprotected skin. This level of protection, combined with other sun-safety measures, can contribute significantly to overall sun safety without relying on potentially harmful synthetic chemicals.
Benefits of Herbal Oil Sunscreens
Natural plant oils offer several advantages over conventional chemical sunscreens:
Broad-spectrum protection: Many oils contain compounds that shield against both UVA and UVB rays.
Antioxidant activity: Plant oils are rich in antioxidants that can neutralize free radicals and combat UV-induced skin damage.
Skin-nourishing properties: Unlike synthetic sunscreens that can be drying, natural oils moisturize and support skin health.
No toxic buildup: Plant-based oils are biodegradable and do not accumulate in tissues or the environment like synthetic chemicals.
Multiple health benefits: Many oils offer additional skincare perks like anti-aging, anti-inflammatory, and wound-healing properties.
Environmentally friendly: Natural oils do not contribute to coral bleaching or aquatic toxicity.
Spotlight on Top Performing Oils
Olive Oil (87.5% UV protection, SPF 8)
Rich in polyphenols and vitamin E, olive oil offers potent antioxidant and anti-inflammatory benefits. Its high oleic acid content helps maintain skin moisture and elasticity.
Coconut Oil (85.7% UV protection, SPF 7)
Known for its moisturizing and antimicrobial properties, coconut oil creates a protective barrier on the skin. It also contains lauric acid, which has been shown to have photoprotective effects.17
Peppermint Oil (85.7% UV protection, SPF 7)
This refreshing essential oil not only offers sun protection but also provides a cooling sensation that can help soothe sunburned skin. Its menthol content has analgesic properties.
Revered in Ayurvedic medicine, tulsi oil boasts powerful antioxidant, anti-inflammatory, and adaptogenic properties. It may help combat UV-induced oxidative stress and support overall skin health.
Practical Applications and Considerations
While herbal oils show promise as natural sunscreens, it’s important to note that their protection levels are generally lower than those of high-SPF commercial products. To maximize sun protection when using natural oils:
Layer multiple oils: Combining oils with complementary properties can enhance overall sun protection.
Reapply frequently: Natural oils may not be as water-resistant as synthetic sunscreens, so reapply often, especially after swimming or sweating.
Use in conjunction with other sun-safety measures: Seek shade, wear protective clothing, and limit sun exposure during peak hours.
Consider adding zinc oxide: For higher protection, some people mix non-nano zinc oxide powder into their preferred oil base.
Patch test first: As with any new skincare product, test oils on a small area to check for allergic reactions or irritation.
Be aware of photosensitivity: Some essential oils, particularly citrus oils, can increase sun sensitivity. Use caution and dilute appropriately.
Realistic Expectations for Natural UV Protection
When using herbal oils for sun protection, it’s crucial to have realistic expectations. While these natural alternatives may not match the high protection numbers of commercial sunscreens, they still offer meaningful defense. An oil with 75% UV protection (SPF 4), for instance, represents a significant reduction in UV exposure. By layering oils, reapplying frequently, and combining their use with other sun-safety measures, you can achieve effective protection without resorting to synthetic chemicals. Remember, any reduction in UV exposure is beneficial for skin health, and these natural oils offer that protection along with additional skincare benefits.
The Petrochemical Problem: Why Slathering on Toxins is a Bad Idea
The widespread use of petrochemicals in personal care products, including sunscreens, raises serious health and environmental concerns. Here’s why coating our largest organ in fossil fuel derivatives is problematic:
Bioaccumulation and Body Burden
Petrochemicals are lipophilic, meaning they have an affinity for fats. This allows them to penetrate the skin easily and accumulate in fatty tissues throughout the body. Over time, this can lead to a significant toxic burden.
A 2011 study found that women who used mineral oil-based cosmetics had higher levels of mineral oil saturated hydrocarbons (MOSH) in their body fat compared to non-users. The researchers concluded that cosmetic products were likely a relevant source of MOSH contamination in the population.18
Endocrine Disruption
Many petrochemicals used in sunscreens and other personal care items are known or suspected endocrine disruptors. These compounds can interfere with hormone signaling, potentially leading to reproductive issues, developmental problems, and increased cancer risk.
For example, parabens, which are commonly used as preservatives in sunscreens, have been shown to mimic estrogen in the body. A 2004 study detected parabens in human breast tumors, raising concerns about their potential role in breast cancer development.19
Skin Irritation and Sensitization
Petroleum-derived ingredients can cause skin irritation, allergic reactions, and increased sensitivity in some individuals. This is particularly concerning for sunscreens, which are applied to large areas of skin and often used on children and those with sensitive skin.
A 2018 review in the Journal of Allergy and Clinical Immunology: In Practice found that up to 70% of people with sensitive skin reported adverse reactions to sunscreens, with chemical UV filters being common culprits.20
Environmental Contamination
When we use products containing petrochemicals, these substances don’t just affect our bodies – they also enter the environment. Sunscreen chemicals wash off in water, contaminating lakes, rivers, and oceans.
A 2015 study estimated that between 6,000 and 14,000 tons of sunscreen wash off into coral reef areas each year, with devastating effects on marine ecosystems.21
Fossil Fuel Dependence
The widespread use of petrochemicals in personal care products contributes to our overall dependence on fossil fuels. This not only perpetuates environmental damage from oil extraction and refining but also supports an industry with a vested interest in downplaying the risks of its products.
By choosing natural, plant-based alternatives, consumers can reduce their exposure to potentially harmful petrochemicals while supporting more sustainable and environmentally friendly practices.
Conclusion: Embracing Safer Sun Protection
As awareness grows about the potential risks of conventional sunscreens, the shift towards natural alternatives is gaining momentum. Herbal oils offer a promising solution, providing effective sun protection along with additional skin benefits, without introducing synthetic toxins into our bodies or the environment.
While more research is needed to fully understand the photoprotective properties of plant oils, the available evidence suggests they can be valuable tools in our sun safety arsenal. By combining the use of natural oils with sensible sun exposure habits, we can safeguard our skin health while minimizing our chemical burden.
Ultimately, the choice between conventional and natural sunscreens is a personal one. However, given the mounting concerns over petrochemical-based products, exploring safer alternatives is a wise investment in both personal and planetary health. As we continue to uncover the hidden costs of our chemical-laden lifestyles, returning to nature’s time-tested remedies may prove to be the smartest path forward.
References
1. Calafat, A. M., et al. “Concentrations of the Sunscreen Agent Benzophenone-3 in Residents of the United States: National Health and Nutrition Examination Survey 2003-2004.” Environmental Health Perspectives, vol. 116, no. 7, 2008, pp. 893-897.
2. Downs, C. A., et al. “Toxicopathological Effects of the Sunscreen UV Filter, Oxybenzone (Benzophenone-3), on Coral Planulae and Cultured Primary Cells and Its Environmental Contamination in Hawaii and the U.S. Virgin Islands.” Archives of Environmental Contamination and Toxicology, vol. 70, no. 2, 2016, pp. 265-288.
3. Krause, M., et al. “Sunscreens: Are They Beneficial for Health? An Overview of Endocrine Disrupting Properties of UV‐Filters.” International Journal of Andrology, vol. 35, no. 3, 2012, pp. 424-436.
4. Hanson, K. M., et al. “Sunscreen Enhancement of UV-Induced Reactive Oxygen Species in the Skin.” Free Radical Biology and Medicine, vol. 41, no. 8, 2006, pp. 1205-1212.
5. Darbre, P. D., et al. “Concentrations of Parabens in Human Breast Tumours.” Journal of Applied Toxicology, vol. 24, no. 1, 2004, pp. 5-13.
6. Heudorf, U., et al. “Phthalates: Toxicology and Exposure.” International Journal of Hygiene and Environmental Health, vol. 210, no. 5, 2007, pp. 623-634.
7. Shukla, R. K., et al. “ROS-Mediated Genotoxicity Induced by Titanium Dioxide Nanoparticles in Human Epidermal Cells.” Toxicology in Vitro, vol. 25, no. 1, 2011, pp. 231-241.
8. Grassian, V. H., et al. “Inflammatory Response of Mice to Manufactured Titanium Dioxide Nanoparticles: Comparison of Size Effects through Different Exposure Routes.” Nanotoxicology, vol. 1, no. 3, 2007, pp. 211-226.
9. Minetto, D., et al. “Ecotoxicity of Engineered TiO2 Nanoparticles to Saltwater Organisms: An Overview.” Environment International, vol. 88, 2016, pp. 60-72.
10. Gulson, B., et al. “Small Amounts of Zinc from Zinc Oxide Particles in Sunscreens Applied Outdoors Are Absorbed through Human Skin.” Toxicological Sciences, vol. 118, no. 1, 2010, pp. 140-149.
11. Janjua, N. R., et al. “Systemic Absorption of the Sunscreens Benzophenone-3, Octyl-Methoxycinnamate, and 3-(4-Methyl-Benzylidene) Camphor after Whole-Body Topical Application and Reproductive Hormone Levels in Humans.” Journal of Investigative Dermatology, vol. 123, no. 1, 2004, pp. 57-61.
12. Schlumpf, M., et al. “Exposure Patterns of UV Filters, Fragrances, Parabens, Phthalates, Organochlor Pesticides, PBDEs, and PCBs in Human Milk: Correlation of UV Filters with Use of Cosmetics.” Chemosphere, vol. 81, no. 10, 2010, pp. 1171-1183.
13. Danovaro, R., et al. “Sunscreens Cause Coral Bleaching by Promoting Viral Infections.” Environmental Health Perspectives, vol. 116, no. 4, 2008, pp. 441-447.
14. Giokas, D. L., et al. “Occurrence and Removal of Chemical UV Filters in Wastewater Treatment Plants.” Environmental Science and Pollution Research, vol. 22, no. 12, 2015, pp. 9089-9100.
15. Chen, F., et al. “Distribution and Accumulation of Endocrine-Disrupting Chemicals and Pharmaceuticals in Wastewater Irrigated Soils in Hebei, China.” Environmental Pollution, vol. 159, no. 6, 2011, pp. 1490-1498.
16. Kaur, C. D., and Saraf, S. “In Vitro Sun Protection Factor Determination of Herbal Oils Used in Cosmetics.” Pharmacognosy Research, vol. 2, no. 1, 2010, pp. 22-25.
17. Korać, R. R., and Khambholja, K. M. “Potential of Herbs in Skin Protection from Ultraviolet Radiation.” Pharmacognosy Reviews, vol. 5, no. 10, 2011, pp. 164-173.
18. Concin, N., et al. “Mineral Oil Paraffins in Human Body Fat and Milk.” Food and Chemical Toxicology, vol. 46, no. 2, 2008, pp. 544-552.
19. Darbre, P. D., and Harvey, P. W. “Paraben Esters: Review of Recent Studies of Endocrine Toxicity, Absorption, Esterase and Human Exposure, and Discussion of Potential Human Health Risks.” Journal of Applied Toxicology, vol. 28, no. 5, 2008, pp. 561-578.
20. Rozas-Muñoz, E., et al. “Sensitive Skin: A Review of Prevalence, Pathogenesis, and Management.” Journal of Allergy and Clinical Immunology: In Practice, vol. 6, no. 6, 2018, pp. 1898-1908.
21. Downs, C. A., et al. “Toxicopathological Effects of the Sunscreen UV Filter, Oxybenzone (Benzophenone-3), on Coral Planulae and Cultured Primary Cells and Its Environmental Contamination in Hawaii and the U.S. Virgin Islands.” Archives of Environmental Contamination and Toxicology, vol. 70, no. 2, 2016, pp. 265-288.
In December 2007, Archives of Pediatrics and Adolescent Medicine published a study by Ian Paul and colleagues at the Penn State College of Medicine. One hundred five children between the ages of two and eighteen, all with cough and runny nose of seven days or less, were randomized into three groups. One group received a single nocturnal dose of buckwheat honey. One received an age-appropriate dose of honey-flavored dextromethorphan, the leading over-the-counter cough suppressant in America, sold in many formulations under brand names including Robitussin, Delsym, Vicks, and NyQuil. The third received nothing.
Parents scored their children on cough frequency, cough severity, how bothersome the cough was, the child’s sleep quality, and their own sleep quality.
Honey improved every outcome measured. Dextromethorphan showed no statistically significant advantage over no treatment on any of them.¹
The comparison that mattered, the one the study was designed to run, put a spoon of honey against a mass-market pharmaceutical and found the honey better. The comparison the authors did not lead with, but which sat plainly in the pairwise data, put the mass-market pharmaceutical against nothing and found no measurable difference.
The Paul trial was partially double-blinded (honey cannot be blinded from taste), which is the obvious objection. A 2018 Cochrane review pooled the Paul study with later replications from Israel, Iran, and Brazil, all of which used various blinding designs, and reached the same conclusion. Honey outperforms no treatment. Honey outperforms dextromethorphan. It does so consistently.²,³
Six weeks after the Paul study appeared, on 17 January 2008, the U.S. Food and Drug Administration issued a Public Health Advisory recommending that over-the-counter cough and cold products not be used at all in children under the age of two, citing “serious and potentially life-threatening side effects” including convulsions, rapid heart rates, decreased consciousness, and death.⁴ The Centers for Disease Control had documented over fifteen hundred children under the age of two treated in emergency rooms in 2004 and 2005 for adverse events after receiving these products.⁵ Manufacturers voluntarily pulled infant formulations from the shelves before the advisory issued, and relabeled their remaining children’s products as not for use in children under four.⁶
Two facts arrived within weeks of each other. A peer-reviewed randomized trial found the leading OTC cough medicine indistinguishable from placebo. The FDA determined that its use had been killing children.
None of this was breaking news to anyone who owned a copy of Folk Medicine.
The recipe
D.C. Jarvis was a Vermont country doctor. For decades he cataloged the folk practices of his patients, most of them families who had farmed the same land for generations. His 1958 book Folk Medicine was a New York Times bestseller for over a year. Chapter nine gives the cough syrup as he recorded it:
Boil one lemon slowly for ten minutes. This softens the lemon so that more juice will be got out of it, and also softens the rind. Cut the lemon in two and extract the juice with a lemon squeezer. Put the juice into an ordinary drinking glass. Add two tablespoonfuls of glycerine… Stir the glycerine and lemon juice well, then fill up the drinking glass with honey.⁷
Dose: one teaspoonful for a daytime coughing spell. One at bedtime and again in the night if the cough wakes the child. For severe cough, six teaspoonfuls across the day. As the cough eases, the doses taper.
Jarvis’s observations on the preparation were specific. “It does not upset the stomach, as many cough syrups do. It can be taken by children as well as adults. It will relieve a cough when all other cough syrups fail.”⁷
He noted the recipe was “many generations old” in his region in 1961. That places its lineage well into the nineteenth century, among people who kept bees, grew lemons in glasshouses or bought them from the general store, and used glycerine (a viscous byproduct of soap-making, cheap at any pharmacy in that era) as a household remedy for coughs, sore throats, and dry skin.
The recipe survives in Jarvis’s book with one further detail that matters. Immediately after giving the formula, he adds an anecdote from a farmer patient.
Speaking of using lemons to compound a cough remedy, I recall the remark of a farmer. When he was explaining how well the suggested remedy had worked he laughed and said, “Fact is, we didn’t have any lemons. I used apple-cider vinegar. Just as good.”⁷
The farmer had substituted vinegar for citrus and got the same result. This is not a marginal detail. It tells you what the acid is doing in the recipe. It is thinning mucus and providing a light astringent action, a function any acid can perform, which is why the substitution worked and why the medieval European oxymels (honey-and-vinegar preparations used for coughs since Hippocrates) sit in the same family as this Vermont formula. The mechanism does not depend on lemon specifically. It depends on a small quantity of acid, dissolved in honey, held long enough in the throat to coat the irritated tissue.
Jarvis’s Vermont formulation is one documentation of a broader folk tradition. The base was constant across regions and centuries: honey plus acid. The additions varied by kitchen and by climate.
Jethro Kloss, working the same tradition from a different angle, published Back to Eden in 1939 with parallel preparations drawn from the Tennessee-Wisconsin herbal lineage. His lemon syrup began identically. “Boil one pint of lemon juice ten minutes.”⁸ His fig cough syrup combined honey and lemon in the same architecture. His entry on coltsfoot (Latin Tussilago farfara, literally “coughwort”) notes the leaves are “excellent when combined with other herbs and made into a cough syrup,” sweetened with honey. Kloss’s book documents lemon for colds, influenza, asthma, and fever across seven pages. “I wish that humanity would understand the real value of the lemon and learn to make a real medicine of it.”⁸
Kloss also documented thyme. His entry on Thymus vulgaris lists its medicinal properties as tonic, carminative, antispasmodic, and antiseptic, and describes it as “valuable in whooping cough, asthma, and lung troubles. For small children, give small and frequent doses.”⁸ His caution alongside was equally specific: “Use sparingly. Do not make a habit of using thyme.” Concentrated action, careful dosing.
Thyme’s principal active compounds, thymol and carvacrol, are phenolics concentrated in the plant’s volatile oils. Their actions on airway tissue are documented and specific. Thymol is antispasmodic on bronchial smooth muscle: it relaxes the involuntary contractions that produce coughing spasms. It is expectorant: it thins mucus and stimulates the ciliated cells lining the airway to move it upward for clearance. And because the volatile oils vaporize at warm-drink temperatures, a portion of the thymol is delivered by inhalation as well as by swallowing when the syrup is taken warm. Aromatic herbs work through two routes at once. Germany’s Commission E, the mainstream regulatory body for herbal medicines and roughly the German equivalent of a plant-medicine FDA, approves thyme for symptomatic treatment of bronchitis, whooping cough, and catarrh of the upper airway.¹⁵ European folk medicine has used it continuously in that role for centuries.
The recipe this essay recommends draws on both traditions. Honey and lemon supply the demulcent and osmotic base, as in Jarvis. Thyme adds the antispasmodic and aromatic action, as in Kloss. The formulation is in the appendix. Jarvis’s exact Vermont version, with glycerine, is in the appendix as well, for readers who want the historical formulation as he wrote it. Glycerine is a more processed component than the others (a purified single compound rather than a whole food), but it has been in continuous folk use since the nineteenth century as a pharmacy-counter demulcent, and it extends the throat-coating time beyond what honey alone provides. Both formulations work. The primary is closer to whole-food preparation.
The recipe was not Jarvis’s discovery. Jarvis was writing down what he saw farmers using. Kloss was doing the same in a different region.
A note before proceeding. Honey is not given to infants under one year. The concern is toxicological, not infectious. Clostridium botulinum spores can be present in raw honey. In older children and adults, established gut flora and stomach acid prevent the spores from germinating, and they pass through without effect. In an infant’s immature digestive tract, the same spores can germinate and produce botulinum toxin, a potent neurotoxin. The organism is not causing an infection. The toxin is doing the damage. The caution predates the Paul trial by decades and is not disputed by any party, mainstream or otherwise. The Paul study enrolled children aged two and above for the same reason.
What a cough is
A cough is an expulsive reflex. Irritation of the airway lining, from mucus, dust, smoke, particulate matter, gastric reflux, dryness, or cold air, triggers rapid contraction of the diaphragm and intercostals against a closed glottis. The glottis opens. Air explodes out at velocities exceeding twenty-five meters per second, carrying whatever the airway is trying to clear.
The reflex exists because the airway lining is thin, delicate, and constantly exposed to material that shouldn’t be there. Without the cough, particulate matter accumulates. Mucus produced to trap that material accumulates with it. Untreated, the accumulation moves down. What began as a throat irritation becomes a chest cough. What began as an acute condition, resolved in days by the body’s clearance of the trigger, becomes chronic.
Kloss described this progression plainly in Back to Eden. On chronic bronchitis: “Acute bronchitis may become chronic if it is not properly treated and relieved. When a cold is allowed to continue, the infection may extend down into the lungs and become chronic. Occasionally, if it is not cured, it may encourage the development of tuberculosis or some other serious chronic lung disease.”⁸ On why the cough arose in the first place: “Colds would not be so prevalent if the body were not filled with mucus and waste products, so one should immediately rid the body of these poisons.”⁸
The framework is not obscure. Herbert Shelton, the twentieth-century natural hygienist, called it the acute-to-chronic mechanism. The body’s efforts to expel accumulated toxins produce acute symptoms. Suppression of those symptoms leaves the toxins in place. The body attempts expulsion by other routes. Those routes are suppressed in turn. The process, driven long enough, produces chronic disease that presents as a distinct condition, apparently unrelated to the accumulated cause.
The cough is the body clearing the airway. To decide what a cough syrup should do, you have to decide what you think a cough is for. That decision determines everything downstream.
The suppressor
Dextromethorphan was patented in the 1950s as a non-narcotic replacement for codeine. Codeine had a long history as a cough suppressant, and a long history as an opioid: sedating, addictive, respiratory-depressant at high doses. Dextromethorphan was developed to keep the antitussive function without the opioid liability.
It works centrally. The drug reaches the brainstem through the bloodstream and depresses the medullary cough center, which is the neural relay where signals from an irritated airway would normally trigger the expulsive reflex. It achieves this by binding to receptors in the brainstem, blocking NMDA glutamate receptors and activating sigma-1 receptors. It also weakly affects serotonin and norepinephrine.⁹ The signal from the airway still arrives at the relay. It no longer produces a cough.
Nothing about this mechanism addresses the airway. Dextromethorphan does not soothe irritation. It does not thin mucus. It does not accelerate its removal. It does not resolve whatever prompted the cough. It sits on receptors that normally allow the cough signal to fire, and it prevents them from firing.
The signal was the body’s alarm. The cough was its response to the alarm. Dextromethorphan silences the response by muting the alarm at the central switchboard.
At therapeutic doses, this produces the intended effect (the person stops coughing) for as long as the drug is active. At supratherapeutic doses the NMDA antagonism produces dissociation and hallucination similar in character to phencyclidine.⁹ The recreational abuse of dextromethorphan-containing cough syrups (known as “robotripping”) is a documented clinical phenomenon. At high doses in combination with serotonergic drugs, it produces serotonin syndrome. At high doses generally, it produces respiratory depression.
In children specifically, the Paul team ran their earlier study in 2004, dextromethorphan versus diphenhydramine versus placebo, and found none of the three superior for nocturnal cough or sleep quality.¹⁰ This was not an isolated result. By the time the American Academy of Pediatrics reviewed the evidence, it did not recommend dextromethorphan for children. The American College of Chest Physicians reached the same conclusion.¹
By 2007 the leading over-the-counter cough drug in America had been tested against an inert control in two randomized trials, first against placebo and then against no treatment. It had shown no measurable advantage in either. Six weeks later the FDA advisory arrived, citing convulsions and deaths.
The soother
The folk cough syrup does something categorically different.
Kloss defined the two active mechanisms in the glossary of Back to Eden. A demulcent is “an agent that soothes, protects, and relieves the irritation of inflamed mucous membranes and other surfaces.” An expectorant “promotes the thinning and ejection of mucus or exudate from the lungs, bronchi, and trachea.”⁸
The preparation is both, and with thyme it is also antispasmodic.
Honey is a supersaturated sugar solution with a water activity of around 0.6 (too low to support most microbial growth) and a pH of around 3.9. Held on the tissue of the throat, it draws water osmotically from the inflamed lining, which reduces local swelling and provides mechanical soothing. Its viscosity coats and protects the irritated surface. Lemon juice, at a pH of around 2.2, thins mucus on contact and provides light astringent action from citric acid and phenolic compounds. Vinegar, at a similar pH, does the same thing, which is why the farmer’s substitution worked.
Thyme adds two further actions to the base. Thymol, its principal phenolic compound, relaxes bronchial smooth muscle: the involuntary tension that produces coughing spasms eases. Thymol also stimulates the ciliated cells of the airway lining to move mucus upward for clearance, which is exactly what a productive cough is trying to do. The syrup helps the cough finish faster. The volatile oils vaporize slightly at warm-drink temperature, delivering a portion of the thymol by inhalation alongside ingestion, so the active compound reaches the airway lining directly as well as via the digestive tract.
In Jarvis’s Vermont variant, glycerine adds a further specific function. It is strongly hygroscopic. It holds moisture against tissue and extends the demulcent contact time beyond what honey alone provides. It is not essential to the recipe’s action, but it lengthens the duration of soothing per spoonful.
The syrup soothes the irritation triggering the cough. It thins the mucus the cough is trying to clear. It relaxes the airway spasm. It supports the reflex rather than suppressing it. When the cough is no longer needed, it stops.
The mechanism runs on the airway, not in the brainstem. It leaves the reflex intact and removes its cause.
Honey has other properties that matter here. Its low water activity, low pH, hydrogen peroxide production, and specific plant-derived phenolic compounds create an environment inhospitable to microbial overgrowth on inflamed tissue. This is why traditional cultures used honey on open wounds long before anyone had proposed a theory of infection. Buckwheat honey specifically, the varietal Paul’s team chose, is unusually high in phenolic compounds and antioxidant activity. The World Health Organization’s Department of Child and Adolescent Health, in its 2001 review of cough and cold remedies for young children, cited honey as a potentially effective option six years before the Penn State trial confirmed it.¹¹,¹²
The recipe soothes without suppressing. That is the essential difference. It works with the reflex. Dextromethorphan works against it.
The 2007 trial was measuring, without knowing it, the difference between those two approaches.
Continuity
The medicinal use of honey is documented continuously across every literate culture from the emergence of writing forward. Sumerian clay tablets from around 2100 BC record honey mixed with river dust and oil for infected skin ulcers. Egyptian medical papyri describe honey applied to open wounds. Sushruta, a physician in Vedic India around 1400 BC, wrote of the medicinal properties of eight honey varietals. Athenaeus in Greece around 230 AD recorded that those who ate honey and bread for breakfast “were free from disease all their lives.” Ibn Majah, quoting Mohammed in the seventh century, wrote that “honey is a remedy for every illness.”¹¹
The specific use for cough runs the same length. Every one of these traditions used honey, sometimes alone, more often combined with acid, herb, or spice, for cough, sore throat, and cold.
Sir John Hill, a physician in England in 1759, wrote the first English-language book devoted to the medicinal use of honey. He observed, then, that its virtues were being neglected.
The slight regard at this time paid to the medicinal virtues of Honey, is an instance of neglect men shew to common objects, whatever their value: acting in contempt, as it were, of the immediate hand of providence, which has in general made those things most frequent, which have the greatest uses; and for that reason, we seek from the remotest part of the world, medicines of harsh and violent operation for our relief in several disorders, under which we should never suffer, if we would use what the Bee collects for us at our doors.¹¹
The observation held. The nineteenth century saw the rise of proprietary patent medicines: laudanum-based cough syrups, cocaine-based lozenges, alcohol-heavy elixirs marketed to households through newspapers and mail order. The twentieth century industrialized that market. Dextromethorphan was patented in the 1950s, sold under proprietary brand names, marketed to parents through television. The recipe on the counter (honey with lemon, honey with vinegar, honey with fig, honey with coltsfoot, honey with thyme, honey with glycerine) was displaced not by evidence but by advertising and shelf space.
Jarvis published the Vermont version in 1958. Kloss had published the Tennessee-Wisconsin version in 1939. Fessenden and McInnes catalogued the honey material comprehensively in 2008. The WHO acknowledged honey for cough in 2001. Penn State confirmed it in randomized trial in 2007. The Cochrane Collaboration confirmed it again in 2018.
At each of these points the establishment position on cough treatment in children shifted slightly closer to what Jarvis’s farmers already did.
The recipe did not move. It was where it had been since before Jarvis was born.
What replaced it
The FDA advisory did not arrive by regulatory initiative. It arrived because pediatricians forced it. Joshua Sharfstein, a pediatrician at Johns Hopkins and later a senior FDA regulator, was among the authors of a March 2007 petition that asked the agency to declare these products contraindicated for children under six. His December 2007 piece in the New England Journal of Medicine, published the same month as the Paul trial, described the market the pediatric community was asking the FDA to move against: 39 percent of U.S. households had purchased these products in the previous three years, and consumers were buying about 95 million packages annually for use in children.¹⁴
The mechanism of the withdrawal was industry self-protection. Manufacturers voluntarily pulled infant products before the January 2008 announcement to avoid a mandatory recall. The two-to-four age band was formally excluded by industry relabeling that same year. The remaining products, for children over four, were left in place with warnings, though the same trials that had cleared under-fours had also failed to demonstrate benefit in the older group.¹
The regulatory response was serious. The public messaging afterward was not. Pediatricians were left to tell parents what to do instead. A physician commentary in NEJM Journal Watch put the new recommendation plainly. “Give fluids and control fever, but don’t give cough and cold medicines.”¹³
The old recipe was fluids that soothed the throat and thinned mucus. Any child would take it, because it tasted of honey and lemon. The whole preparation cost pennies. The advice arrived at, after the industry had killed enough children to warrant the FDA advisory, was a diminished version of what a grandmother would have done in 1900.
What made pediatric cough syrup a 95-million-package-a-year business was not that its products worked better than the folk preparation. They did not work better than the folk preparation. On the primary outcomes of two randomized trials in children, they did not work better than nothing. What made them a 95-million-package-a-year business was that they could be branded, patented, shelf-placed, and advertised. Honey, lemon, and thyme could not. There was no company whose share price depended on the survival of a grandmother’s recipe. There were many companies whose share price depended on the survival of dextromethorphan-based products.
The FDA withdrawal removed the infant portion of that market. The revenue from products marketed for children over four continues.
What’s on the counter
Jarvis called the recipe “many generations old” in 1961. He was describing something already ordinary: the syrup a farmer’s wife would make when a child was coughing at night, the same way she would make broth or apply a mustard plaster. It required no prescription, no pharmacist, no marketing budget, no clinical trial. It required a lemon, a jar of honey, a small pinch of thyme from the herb garden, and ten minutes.
The Penn State trial did not discover the recipe. The WHO did not discover it. Cochrane did not discover it. What each of these did was confirm, in the register of institutional science, what farmers in Vermont and grandmothers in every other country had known for as long as anyone had kept bees.
The lemon costs about a dollar. The honey costs between five and fifteen dollars a jar, and one jar lasts a long time. Thyme is a garden herb that grows in a pot on a windowsill. If the lemon is not available, apple-cider vinegar is in the pantry. The whole preparation takes ten minutes to boil the lemon and thirty seconds to assemble. It does not upset the stomach, and it can be given to children over one. It works when the industrial products do not, or more precisely, it works when the industrial products have been shown not to work at all.
Every one of the relevant documents is public. The Paul study is on PubMed and the FDA advisory is in the Federal Register. Jarvis’s book has been in continuous print for over sixty years. Nothing about this argument has been hidden. The disagreement between what the trials established and what the pharmacy shelves offered lasted a full century and cost the lives of children.
The recipe is on the counter. It always has been.
Making the syrup
Ingredients (fills one 8-ounce / 240 ml glass or mason jar)
1 fresh lemon (or 2 tablespoons apple-cider vinegar as substitute)
1 fresh sprig thyme (or ½ teaspoon dried thyme)
About 1 cup (240 ml) of water, for boiling the lemon
Honey to fill the remainder of the glass, roughly ⅔ of the volume (about 5 fluid ounces / 150 ml / 10 tablespoons)
Method
Bring about 1 cup of water to a simmer in a small saucepan. Add the whole lemon and the thyme sprig. Simmer slowly for ten minutes. The heat softens the rind and extracts the lemon juice, and it draws the thymol and volatile oils out of the thyme into the water. Remove the pan from the heat. Fish out the thyme sprig (or strain if using dried thyme) and discard.
Cut the lemon in half and squeeze the juice into your glass or jar. Add 2 tablespoons (30 ml) of the thyme-and-lemon water from the saucepan. Fill the rest of the glass with honey, stirring as you go until the mixture is smooth. You will use roughly 10 tablespoons of honey to fill an 8-ounce glass.
If using apple-cider vinegar instead of lemon, simmer the thyme alone in about ½ cup of water for ten minutes. Strain and discard the thyme. Add 2 tablespoons of the thyme water and 2 tablespoons of apple-cider vinegar to the glass, then fill the rest with honey. The vinegar variant is well-attested in the folk record.
Dose
For an occasional daytime coughing spell: one teaspoonful, stirred before taking.
At bedtime: one teaspoonful, and one more during the night if the cough wakes the child.
For a severe cough: one teaspoonful on rising, one mid-morning, one after lunch, one mid-afternoon, one after supper, one at bedtime. Reduce the frequency as the cough eases.
For small children: half a teaspoonful, taken more often.
Take the syrup warm when possible. The warmth releases the thyme’s volatile oils and delivers a portion of the active compounds to the airway by inhalation as well as by swallowing.
The Jarvis variant, with glycerine
Jarvis’s original Vermont formulation adds glycerine to extend the throat-coating time. Glycerine is a purified vegetable compound rather than a whole food, but it has been in traditional folk use since the nineteenth century and provides a longer-lasting demulcent film on the throat than honey alone. Readers who want Jarvis’s exact recipe, or who want the extended contact time, use this variant:
Ingredients (fills one 8-ounce / 240 ml glass or mason jar)
2 tablespoons (30 ml) vegetable glycerine, USP grade, from any pharmacy
Honey to fill the remainder, about 5 fluid ounces (150 ml, or roughly 10 tablespoons)
Optional: 1 sprig fresh thyme or ½ teaspoon dried thyme, added at the boiling step
Method
Simmer the lemon in about 1 cup of water for ten minutes (with the thyme if using). Remove and discard the thyme. Cut the lemon in half and squeeze the juice into the glass. Add the glycerine and stir. Fill the rest with honey and stir again.
The dose is the same as for the primary recipe.
Cautions
Do not give honey to infants under one year of age.Clostridium botulinum spores can be present in raw honey. In older children and adults, mature gut flora and stomach acid prevent them from germinating and they pass through without effect. In an infant’s immature digestive tract, they can produce botulinum toxin. The toxin causes the harm, not the organism. The caution is not disputed.
Thyme. Use sparingly, as Kloss advised. A sprig or half a teaspoon of dried herb is enough per glass. Not recommended in medicinal doses during pregnancy. Culinary amounts in food are fine; a therapeutic syrup is the caveat.
Raw versus pasteurized honey. Raw honey is preferable when available. It retains the enzymes, phenolic compounds, and volatile aromatics that pasteurization heat degrades. Pasteurized honey works and delivers the demulcent and osmotic action, but the extra biochemical richness of raw honey is lost in the heating. Darker varietals (buckwheat, if available; otherwise wildflower, manuka, or dark forest honeys) contain more phenolic compounds than pale varietals like clover, but any real honey works. Read the label: some supermarket “honey” is cut with corn syrup or rice syrup and is not honey at all. On the infant botulism question: pasteurization does not eliminate the risk. Clostridium botulinum spores are heat-resistant far beyond standard honey pasteurization temperatures. The under-one caution applies to both raw and pasteurized honey.
Storage. The finished syrup keeps in a sealed glass jar (a mason jar works well) for several weeks at room temperature, and longer refrigerated. The honey’s osmotic action and the lemon or vinegar acidity together create a hostile environment for microbial growth. Give it a stir before each dose, as the honey may settle. If the syrup ever develops off smells, cloudiness that wasn’t there originally, or fermentation bubbles, discard and make a fresh batch.
References
1. Paul IM, Beiler J, McMonagle A, Shaffer ML, Duda L, Berlin CM Jr. Effect of honey, dextromethorphan, and no treatment on nocturnal cough and sleep quality for coughing children and their parents. Archives of Pediatrics and Adolescent Medicine 2007;161(12):1140–1146.
2. Axelsson I. Honey, not dextromethorphan, was better than no treatment for nocturnal cough in children with upper respiratory infections. Evidence-Based Medicine 2008;13(4):106.
3. Oduwole O, Udoh EE, Oyo-Ita A, Meremikwu MM. Honey for acute cough in children. Cochrane Database of Systematic Reviews 2018, Issue 4. Art. No.: CD007094.
4. U.S. Food and Drug Administration. Public Health Advisory: Nonprescription Cough and Cold Medicine Use in Children. Issued 17 January 2008.
5. Centers for Disease Control and Prevention. Infant deaths associated with cough and cold medications, United States, 2005. MMWR Morbidity and Mortality Weekly Report 2007;56(01):1–4.
6. Consumer Healthcare Products Association. Voluntary withdrawal of oral infant cough and cold medicines announced October 2007; pediatric labeling change announced October 2008.
7. Jarvis DC. Folk Medicine: A Doctor’s Guide to Good Health. First published New York: Henry Holt, 1958. UK edition consulted: London: Pan Books, 1961. Chapter 9, “An Old-Fashioned Cough Remedy,” pp. 105–106.
8. Kloss J. Back to Eden. First published 1939. Revised edition, Back to Eden Publishing, 2009. Glossary; entries on lemon, coltsfoot, thyme, and bronchitis; Section II, Chapter 3, Herbal Syrups.
9. Journey JD, Bhattarai S, Agrawal S. Dextromethorphan. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing, 2024. See also: Nguyen L, Thomas KL, Lucke-Wold BP, et al. Dextromethorphan: An update on its utility for neurological and neuropsychiatric disorders. Pharmacology & Therapeutics 2016;159:1–22.
10. Paul IM, Yoder KE, Crowell KR, et al. Effect of dextromethorphan, diphenhydramine, and placebo on nocturnal cough and sleep quality for coughing children and their parents. Pediatrics 2004;114(1):e85–e90.
11. Fessenden R, McInnes M. The Honey Revolution: Restoring the Health of Future Generations. 2008. Chapter 9, “Honey That Soothes and Heals,” pp. 141–146.
12. World Health Organization, Department of Child and Adolescent Health. Cough and Cold Remedies for the Treatment of Acute Respiratory Infections in Young Children. Geneva: WHO, 2001.
13. NEJM Journal Watch. FDA warns against use of cough medicines in children younger than 2 years. Commentary published 12 September 2007.
14. Sharfstein JM, North M, Serwint JR. Over the counter but no longer under the radar: pediatric cough and cold medications. New England Journal of Medicine 2007;357(23):2321–2324.
15. Blumenthal M, ed. The Complete German Commission E Monographs: Therapeutic Guide to Herbal Medicines. Austin, Texas: American Botanical Council, 1998. Monograph on thyme (Thymi herba).
At the end of last year, the United States Supreme Court vacated the Second Circuit’s decision that enabled New York State to persecute the Amish for refusing to inject pharma products in violation of their religious beliefs, and it remanded the case (Miller v. McDonald) to the Second Circuit to reconsider its illiberal and unconscionable decision.
Instead of abiding by the Constitution and protecting the religious freedom of the Amish, the Second Circuit again ruled against the Amish. So, we will be going back to the Supreme Court.
And yes, the 168 unvaccinated Amish children related to this case are far healthier than American children who are vaccinated. We provided sworn expert evidence attesting that among a random sample of 168 U.S. children, one would expect to find (based on the background rate of chronic disease among U.S. children) 31 cases of environmental allergies, 15 cases of ADHD, 10 cases of asthma, 9 cases of food allergies, and 4 cases of ASD. Yet, the 168 unvaccinated Amish children whose families New York wants to persecute are free from the chronic health conditions—all related to some form of immune system dysregulation—that plague the vaccinated communities in New York.
Since vaccination is supposedly about improving health, and the Amish who do not vaccinate are clearly healthier, one would expect New York to leave them alone. But that is not how this religion works. The vaccine zealots in New York cannot stand that the Amish refuse to abandon their beliefs in favor of the religious beliefs held by the New York officials regarding vaccines. These “health” officials are willing to sacrifice the way of life and belief system of these Amish children and their community (which have kept them far healthier), if they refuse to bend the knee to adopt cult-like vaccine beliefs.
These “health” officials also apparently cannot stand that the Amish children are healthier and are even willing to wage war against them until they submit and receive every vaccine New York demands—so they can be just as “healthy” as all the children outside the Amish community.
The Amish earnestly seek to avoid conflict but because violating their sincerely held religious beliefs is not an option, they have been placed in an impossible position. We, along with co-counsel, intend to continue to litigate on behalf of the Amish to defend their freedom to practice their religion in peace.
In my own professional life, I was not a scientist, and therefore I never much paid attention to the kinds of rewards and honors that practicing scientists pass out to each other. But at some point I became aware that there was something called the National Academy of Sciences, and that among scientists it was considered a big deal to get selected to become a member. This membership is one of those things that you cannot apply for; rather, one day you get “tapped” by some committee of super-elite gurus who invite you to come learn the secret handshake. Here’s what Wikipedia has to say about membership:
Membership of the National Academy of Sciences is an award granted to scientists that the National Academy of Sciences (NAS) of the United States judges to have made “distinguished and continuing achievements in original research”. Membership is a mark of excellence in science and one of the highest honors that a scientist can receive.
(At some point in the 2010s, the NAS got somehow consolidated with comparable “academies” of engineering and medicine, to become a combined organization going by the name of the National Academies of Science, Engineering and Medicine, or NASEM. This post only concerns the Science part of the combined entity, although I have no reason to think that the other parts are any better.)
Well, as far as I can tell, they are all morons. Also, corrupt morons.
I last wrote about the NAS in February of this year, in a post titled “Would You Trust The National Academies Of Science To Tell You How Science Works?” The occasion for that post was that something called the Federal Judicial Center had just issued a new edition of its Federal Reference Manual on Scientific Evidence. Recognizing that this subject went outside the core of its own expertise, the FJC had called on the NAS to take the main role in the drafting. In the new edition, a chapter from prior editions of the Manual titled “How Science Works” had been taken over by new authors, and substantially re-written and greatly expanded (from 18 to 61 pages). In the process, the new authors had inserted a series of howlers that not only did not fairly describe how science works, but actually got the whole process wrong by 180 degrees. I cited several examples in the February post, but this is the one that goes closest to the heart of the craziness: “While the often-stated maxim that correlation does not imply causation is true, in fact, correlation is the only means that we have of establishing causation in science.” That statement is just flatly wrong. Instead, the process for establishing causation in science operates through the falsification of alternative (“null”) hypotheses of causation. I do not know how anyone could even think to call themselves a “scientist” without basic understanding of that logical process.
And yet here was the NAS, supposedly a collection of the most elite among elite scientists, putting together a chapter of an official court Manual to tell non-scientists (lawyers and judges) “how science works,” and getting it 180 degrees wrong on the single most important point.
Which of course begs for a necessary consideration of the next question: Was this an innocent mistake by ignorant people, or was it an intentional distortion intended to further a political agenda?
Now, just last week, the National Academies have released their latest embarrassment, taking this fundamental fallacy and expanding and running with it. The event at issue was the release of a new Report called “Attribution of Extreme Weather Events and Their Impacts.” Here is the July 15 press release from NASEM, and here is another link to the body of the Report itself. The Report runs to some 175 pages, plus appendices.
The gist of the Report is that now, based on some sort of new research, we suddenly have the tools to “attribute” any extreme weather event of our choosing (hurricane, tornado, drought, flood, whatever) to “human activities.” “Human activities” in this context means the release of “greenhouse gases” into the atmosphere. With that, you can see where they are ultimately going, although this final piece is not mentioned in the Report: the basic idea is that every extreme weather event is the fault of the oil companies.
The very first line of the “Summary”reveals that they knew the conclusion before they started:
“Earth system changes driven by rising greenhouse gas concentrations from human activities are affecting characteristics of extreme weather and climate events, such as frequency and intensity.”
That’s nice. An how exactly do you know it? Here are the two fundamental questions that need to be addressed: (1) What are the alternative hypotheses that you have considered, and how have those been ruled out as the causes of the recent extreme weather events? And (2) what has been your consideration of the evidence, if any, that might contradict or undermine the hypothesis that “human activities” and increased greenhouse gas concentrations are the cause of these extreme weather events?
Get ready: In a Report of 175 pages, they don’t expend even one word to address either of those two questions.
Instead, it’s all about whatever confirming evidence they can find about correlation between extreme weather events and (slightly) increasing global temperatures. They claim to have a “foundational understanding” of the relationship between increasing greenhouse gases and extreme weather events. How they have achieved this “foundational understanding” without ever entertaining any alternative hypothesis is never mentioned. But the “foundational understanding” has supposedly been “strengthened” by the accumulation of evidence consistent with it (while deliberately ignoring all inconsistent evidence). Here is a lengthy quote from the Summary as to how the “foundational understanding” has been strengthened:
Over the past decade, advances in three key scientific pillars have continued to strengthen this foundation. First, physical understanding has matured through accumulation of observational and modeling evidence supporting long-standing theoretical expectations, so that increases in extreme heat and heavy rainfall events across much of the globe can be more confidently and precisely attributed to increasing greenhouse gas concentrations in the atmosphere. Second, the length and quality of observational data have improved in some regions with another decade of data collection . . . , new satellite-based Earth-observing missions, and the development and improvement of homogenized, high-resolution data sets. Third, climate models continue to improve in their representation of critical processes. . . .
Consideration of alternative hypotheses or potentially conflicting evidence? Hey, we don’t do that, we’re scientists!
Readers of this blog and of many skeptic websites know well that the real evidence out there is that extreme weather events are not increasing at all. How dozens of these supposedly top “scientists” from the NAS could write this Report without mentioning or discussing any of this evidence is beyond me. It’s completely humiliating for them.
I won’t try in this post to give any comprehensive set of links here to data sets showing that extreme weather events are not increasing. But, as an example, here is a page at Watts Up With That with data on hurricanes. From that page, here is a chart compiled by Ryan Maue with annual data since the early 1970s on accumulated cyclonic energy:
Can you spot the increasing trend? Neither can I. These clowns from the NAS are claiming that even though ACE has not gone up overall, and has gone down in the most recent years, they just know that whatever hurricane comes through next is the fault of Exxon. That’s the level of quality of this work.
On July 14, the day before this Report was released, a guy named Pat Parenteau, gave an interview to Politico’s E&E News on this subject. Parenteau is a long-time advisor to a law firm called Sher Edling, which is known for representing dozens of plaintiffs in lawsuits against fossil fuel producers claiming harm from climate change. The E&E News article is behind paywall, but Energy in Depth here has the key quote from Parenteau:
“A report with the kind of gravitas that the National Academies can bring will be a huge boost to the plantiffs’ cases.”
Further from EID:
The people involved in the report’s development include Michael Burger, an academic and attorney for climate plaintiffs’ firm Sher Edling, as well Delta Merner, who leads the Union of Concerned Scientists’ Climate Accountability Campaign and served on the NAS committee guiding the report’s development until January 2025. Both Burger and Merner have publicly discussed the critical relationship between attribution science and climate litigation.
The federal government needs to completely defund the NAS today, if not sooner. Also, I call on every member of the NAS to resign. If you stay in, you are complicit in this total scam.
Author’s Note: The framing of prescription drugs as the third leading cause of death, associated with Peter Gøtzsche and Barbara Starfield, is treated here as an underestimate. When heart disease and cancer are themselves largely produced by the same profession’s pharmaceutical and dietary framework, ranking the profession third against its own products misses the arithmetic. The essay does not argue that individual doctors are malicious. It argues that the training installed by the 1910 Flexner Report was an inversion of what heals, that the Rockefeller and Carnegie foundations exported that training globally, and that a century of it has produced the epidemic of chronic disease now called the natural burden of modern life.
The essay operates in two registers. When examining establishment evidence against itself, establishment terminology appears. When stating the author’s own analytical position, terrain language governs.
This essay discusses medical topics for informational purposes. It is not medical advice.
The Prosecution
Sarah Myhill has been investigated by the United Kingdom’s General Medical Council more than thirty times across two decades, more than any doctor in the Council’s history.¹ Not one of the complaints came from her own patients. Every complaint came from other medical professionals and regulatory officials. At the 2010 interim hearing, over 800 patient support letters were submitted alongside a petition with 3,615 signatures. Tom Kark, the Queen’s Counsel acting for the government’s prosecution, described the difficulty of the case in plain terms: the problem with the Myhill cases, he said, was that all the patients had improved and all refused to give witness statements.
The prosecution’s complaint was that her patients got better.
Her practice addresses cellular metabolism through nutritional support and toxin removal. Her patients improve. Her regulator has spent twenty years trying to stop her.
What kind of medical profession prosecutes its healers? A profession whose training was designed to do the opposite of what heals. That training runs across the lifespan of every person the profession treats, from injection in infancy to intubation in the ICU at eighty-three, and it has produced the epidemic of chronic disease now called the natural burden of modern life. The pattern operates in London, Sydney, Toronto, Berlin, Tokyo, and São Paulo because the training that produces it was standardized globally from a single source.
A child has a fever of 102.4. The parent reaches for the cabinet, measures a dose from the red and white bottle, and delivers it to the child’s mouth. The doctor’s advice at the last checkup was clear: bring the fever down.
The child’s body raised the temperature to accelerate metabolic clearing. Higher body heat speeds the enzymatic processes that break down and eliminate whatever the terrain is discarding. The fever is the operation. The intervention interrupts it. The doctor did not fail to know this. The doctor was trained to do the opposite.
The inversion is not confined to fever. It structures every intervention the doctor will offer. The body cleanses through fever, discharge, inflammation, diarrhea, skin eruption; training teaches suppression of each. The body signals distress through cholesterol, glucose, blood pressure; training teaches blocking the signals. The body’s operations and the doctor’s interventions map onto each other with the precision of a mirror.
The pattern was installed deliberately and runs across the lifespan of every person the doctor will treat. The evidence assembles across five thresholds: birth, childhood, adult screening, chronic illness, and death. Applied at scale, this training produces harm at scale. The scale is now planetary.
Joy Garner’s Control Group Survey, conducted in the United States because the American vaccine exemption structure was one of the few environments in the industrialized world where a large fully unvaccinated cohort could still be found, established chronic disease in the fully unvaccinated adult population at 2.64 percent. In the vaccinated it runs at 60 percent.² Standard attributable-fraction methodology assigns 95.6 percent of chronic disease in the vaccinated population to vaccination itself.³ Cancer, heart disease, and the diagnoses that account for the majority of deaths across the industrialized world are conditions Garner counted.
This is the arithmetic behind the essay’s subtitle. Heart disease is ranked first among causes of death in every industrialized country. Cancer is second. Prescription drugs are ranked third by Peter Gøtzsche and Barbara Starfield. The ranking treats the first two categories as phenomena the doctor arrived to treat. They are not. The cholesterol hypothesis that produced the statin era, the seed oil epidemic, and the sugar substitution was invented and sustained by the same profession, and exported through the WHO and every major national dietary guideline body.⁴ The injected substrate from childhood, the screening cascades that route the healthy into oncology pipelines, and the suppression of acute clearing across the adult lifespan produce much of what is later counted as cancer. When the top two categories on the mortality list are themselves iatrogenic, ranking iatrogenic third makes no arithmetic sense. The profession is not the third leading cause of death. It is the first.
Not About Bad People
Most doctors entered medicine because they wanted to help. The individual doctor is not the argument. What was installed in the individual doctor is the argument.
The system runs on convergent opportunism, not coordination. The physician, the researcher, the regulator, the journal editor, the medical school department chair — each pursues rational self-interest within a structure whose maintenance no single actor is responsible for. Upton Sinclair named the local mechanism: a man does not understand what his salary depends on not understanding.⁵ Applied across a profession of a million practitioners, that mechanism produces a system that behaves as if it were coordinated while requiring no coordinator.
There is a category of medical practice this argument does not address: acute trauma care. Broken femurs need setting, gunshot wounds need pressure and sutures, genuine appendicitis needs surgery. These interventions support the body’s repair rather than opposing it, and this is what a critic means by “doctors save lives every day.” They do. The concern here is the other category — the management of chronic illness and the maintenance of ostensibly healthy people through screening, prescription, and intervention. This is the majority of what modern medicine does, and the majority of what it earns.
The life expectancy objection runs like this: populations in the industrialized world lived to roughly 47 in 1900 and to the high seventies today, and medicine is given the credit. The arithmetic does not support it. Most of the increase was compression at the bottom — the reduction of infant and childhood mortality, which the data traces to sanitation, nutrition, and clean water rather than to medical intervention. Life expectancy at age 65 has moved much less: from 76 in 1900 to about 85 today. American life expectancy has been declining since 2014.⁶ British, Australian, and continental European life expectancy has stagnated or reversed across the same period. Cardiovascular disease, overdose, and metabolic collapse are the categories driving the decline — domains the profession has managed with confidence for decades.
The Installation
Ignaz Semmelweis noticed in 1847 that women whose babies were delivered by doctors died at rates several times higher than women whose babies were delivered by midwives. The doctors moved between autopsies and deliveries without washing their hands. He proposed the connection and required his students to wash with chlorinated lime. Deaths in his ward fell dramatically.⁷ His colleagues rejected the finding. He was driven from his position, committed to an asylum, and died there at forty-seven, beaten by guards, according to his autopsy. A century later, Bernard Lown challenged the strict-bedrest dogma for heart attack patients and let his patients sit up in a chair at the end of the bed. His colleagues met him on the ward with Nazi salutes, chanting “Heil Hitler” at a Jewish physician for suggesting that his patients need not lie motionless for six weeks. Strict bedrest is now understood to have killed tens of millions of people worldwide. The man who challenged it received the salute.⁵ Medicine has a documented history of destroying the practitioners who correctly identify iatrogenic harm.
The mechanism that produced modern medicine’s training is documented. In 1910, Abraham Flexner, funded by the Carnegie and Rockefeller foundations, published a report evaluating American medical schools.⁸ Within two decades, the number of American medical schools fell from 162 to 66.⁹ Schools teaching homeopathy, naturopathy, and terrain-based approaches were closed. The surviving schools adopted the curriculum the foundations had specified. Rockefeller money — which was Standard Oil money — flowed to compliant institutions. The American Medical Association’s consultation clause prohibited its members from associating with practitioners outside the approved framework, creating a professional monopoly enforced by economic exclusion.
This is the anti-knowledge point. Flexner did not fill a gap in medical education. The gap did not exist. Many of the 162 schools operating in 1910 taught how the body actually heals — homeopathic, naturopathic, terrain-based traditions with functioning clinical practices and patient outcomes that outperformed the emerging pharmaceutical model. What Flexner destroyed was not ignorance but knowledge. What replaced it was not more knowledge but its inversion: a curriculum designed to suppress the body’s healing responses rather than support them. The distinction matters. A profession that lacks the knowledge to heal can be educated. A profession trained to do the opposite of what heals cannot be corrected without abandoning the training that constitutes it.
The model did not stay inside American borders. Flexner himself was commissioned by the Carnegie Foundation to conduct the same evaluation of European medical education in 1912. The Rockefeller Foundation’s International Health Division and its China Medical Board carried the template outward across the following decades, funding medical schools in England, Belgium, France, Brazil, Thailand, and China on the same pharmaceutical model, closing or defunding institutions that taught otherwise.¹⁰ The Peking Union Medical College, opened in 1921, became the pharmaceutical training center for East Asia. The World Health Organization, established in 1948, took over the export function internationally. By the middle of the twentieth century, every major medical school on the planet was training doctors on essentially the same curriculum.
John D. Rockefeller personally used homeopathic physicians for his own family throughout his life.¹¹ The man who understood terrain well enough to choose it for himself directed his foundations to fund only allopathic schools, at home and abroad. The framework that produces pharmaceutical dependency was profitable. Terrain medicine was not.
The consequences run through every medical school on the developed continents. Approximately two-thirds of American academic department chairs have financial relationships with pharmaceutical companies, a figure equivalent audits in the UK, Australia, Canada, and continental Europe have found to be broadly comparable.¹² The average medical student, whether in Boston or Manchester or Melbourne, receives roughly twenty contact hours of nutrition instruction across four years, less than one percent of classroom time.¹³ A doctor cannot teach what they were never taught. Taught that symptoms are the malfunction and that the body attacks itself, they prescribe drugs that suppress both. What the training installs is what the training produces.
Birth
The body knows how to birth. Every human being who has ever lived was produced by that process, mostly without medical management.
The training the modern obstetrician receives teaches management, extraction, and control. The process is broken into stages, each with an approved intervention. Consent is technically obtained, in labor, on a hospital bed, surrounded by people in scrubs speaking with confidence and urgency. It is not consent as most people understand the term.
Pitocin, synthetic oxytocin, is delivered by IV during the third stage of labor as a matter of routine.¹⁴ Cochrane reviews show it reduces hemorrhage rates in the overall population, but the absolute risk reduction in low-risk women is small: hundreds of women receive the drug to prevent one hemorrhage that would have occurred. Women who have experienced both physiological and pharmacological third stage describe them as fundamentally different. Natural contractions are productive. Synthetic contractions are violent and overwhelming. Sometimes the drug closes the cervix before the placenta has exited, at which point a doctor’s hand goes inside the uterus to remove the fragments manually.
Fundal massage — deep kneading pressure on the abdomen minutes after delivery — is administered by protocol despite evidence not supporting routine use; many women describe it as the most painful part of their birth. Controlled cord traction is standard. The placenta, left alone, releases in ten to thirty minutes with the mother in a state of physiological calm. Traction rushes what biology completes cleanly and can cause retained fragments that hemorrhage later.
None of these interventions is birth. Each opposes what the body is doing, delivered by a professional trained to consider the intervention a positive contribution.
Childhood
The body of a child clears through fever, discharge, rash, mucus, cough, vomiting, diarrhea, and skin eruption. Every acute episode is the terrain restoring itself. What passes through the child is the accumulated burden the child was carrying: dietary residue, environmental exposure, emotional load. The episode is not the disease. The episode is the resolution of the disease.
Training installs two responses. The first is injection: the introduction of foreign material, including heavy metals, industrial chemicals, and animal-derived proteins, into a body that has developed no method of eliminating them through the digestive tract, because the injection bypasses the digestive tract. The second is suppression: antipyretics for fever, antihistamines for discharge, topical steroids for skin eruption, antibiotics for whatever the acute episode has been diagnosed as.
The pediatric schedule delivers dozens of dose-equivalents of injected pharmaceutical products before the child reaches eighteen. The American schedule has risen from fewer than ten doses in the early 1980s to roughly seventy today. The Australian, British, and continental European schedules are broadly comparable, differing in specific brand names and timing but tracking the same trajectory over the same decades.¹⁵ Each addition is approved by national regulators who move between industry and agency.
The substrate has been photographed. Antonietta Gatti and Stefano Montanari, materials scientists at the Italian National Council of Research, examined forty-four injectable vaccines under electron microscope in 2017 and found tungsten, lead, stainless steel, bismuth, gold, silver, cerium, and rare earth alloys. Nothing on any package insert declared any of it.¹⁶ Pediatric injections had the highest particle counts: Varilrix at 2,723 particles per twenty-microliter drop, Infanrix hexa at 1,821. The body has no enzymatic machinery for breaking down these metals. The particles do not biodegrade. They lodge.
Stanley Plotkin, called an indispensable authority on vaccines by Bill Gates, testified under oath in 2018 that his early vaccine trials had used orphans, mentally disabled children in institutions, and the babies of women in prison.¹⁷ Asked whether he had ethical concerns, he indicated that this was how it had been done. The Nuremberg Code, established after the war to prevent this specific category of medical practice, was not mentioned as a limiting factor in his career.
Roman Bystrianyk pulled the mortality data from archives that had not been digitized.¹⁸ Between 1850 and 1940, measles mortality in the industrialized world fell by 98 percent — the measles vaccine was introduced in 1963. Whooping cough deaths fell from over 1,000 per million children to fewer than 10 per million between 1850 and 1950, before the pertussis vaccine was in widespread use. Scarlet fever, for which no vaccine was ever deployed, declined at the same rate. The mortality collapse was driven by sanitation, nutrition, and clean water. Medical students see charts that begin in 1950, after the decline was complete.
The child is being loaded with substances the body will spend years attempting to sequester and eliminate. When acute episodes arise as the body attempts to clear the burden, the pediatrician suppresses them. The suppression drives the material deeper. Chronic conditions emerge. What is called childhood asthma, eczema, allergy, autism is in significant part the wake of this process. This is the substrate driving Garner’s gradient: 2.64 percent is what a child’s baseline looks like when the loading does not happen. 60 percent is what happens when it does.
The Pipeline
The man at fifty-five is asymptomatic. He walks into his annual checkup because his wife asked him to. He has no complaints. The physician orders a standard panel.
The cholesterol comes back at 225. The blood pressure reads 134/82. The fasting glucose is 108. Each number crosses a threshold. Each threshold has been progressively lowered by guideline panels whose members hold financial relationships with the manufacturers of the drugs used to treat the redefined condition. In 1988, a cholesterol of 240 was considered elevated; by 2001, the threshold was 200.¹⁹ In 2003, the American Diabetes Association lowered the pre-diabetes fasting glucose threshold to 100.²⁰ In 2017, the blood pressure threshold was lowered to 130/80, converting roughly thirty million Americans into hypertensive patients overnight.²¹ British, European, Australian, and Canadian panels typically adopt the American thresholds within a year or two.
The healthy man leaves the office with three prescriptions: a statin, an ACE inhibitor, metformin. Each drug produces the next diagnosis. The statin causes muscle symptoms in 7 to 29 percent of users;²² the aches are attributed to aging, the man walks less, his bone density declines, and a bisphosphonate is prescribed — a class linked to atypical femur fractures and osteonecrosis of the jaw. The ACE inhibitor produces a persistent cough in 10 to 15 percent of patients; it is switched to an ARB, which produces dizziness, which elevates fall risk. The metformin causes gastrointestinal symptoms in up to 25 percent of patients; these are addressed with another medication or attributed to irritable bowel syndrome, which becomes its own diagnostic pathway.
Every number the man’s body produced was information. Cholesterol delivers repair material to damaged blood vessels; blocking the delivery does not repair the vessels. Elevated blood pressure indicates the body is working harder to move blood through compromised tissue; blocking the pressure does not repair the tissue. Elevated glucose indicates the terrain is not processing carbohydrates effectively; blocking the glucose does not restore the processing. Each intervention addresses the signal, introduces new material the body must now cleanse, and produces effects that become the next diagnosis. The man is progressively poisoned by his own care.
The screening industry that generated the initial three thresholds operates continuously alongside the pharmacy. The distinction it buries is between disease-specific mortality and all-cause mortality: a screening program can reduce deaths from breast cancer while total deaths remain unchanged, because the treatment kills as many people as the disease prevented. Across the major screening programs, when all-cause mortality is calculated, the benefit largely disappears.²³
Behind the arithmetic sits a reservoir. Approximately 70 percent of men in their seventies have prostate cancer at autopsy, while only about 3 percent die from it. Up to 39 percent of middle-aged women show evidence of breast cancer at autopsy; lifetime risk of dying from it is under 4 percent. Polyps sit in half of older colons. Every screening test dips into this reservoir. Every person pulled from it becomes a patient who cannot benefit from treatment, because they were never at risk.²³
PSA testing has been called a public health disaster by Richard Ablin, the researcher who discovered the antigen.²⁴ For every man whose life is extended by PSA screening, estimates suggest 30 to 100 are overdiagnosed and treated with surgery or radiation. Impotence and incontinence are the price of the overtreatment. Mammography follows the same pattern: the Cochrane review found that for every 2,000 women screened over ten years, approximately one has her life extended and ten are treated unnecessarily for conditions that would never have progressed.²⁵ The colonoscopy case was decided in 2022 when the NEJM published the NordICC trial, the first randomized controlled study of colonoscopy screening ever conducted. It followed over 84,000 people for ten years and found no significant reduction in deaths from colorectal cancer.²⁶ The CT scan produces the cancers it looks for: a 2025 analysis in JAMA Internal Medicine projected that the 93 million CT scans performed in the United States in 2023 will cause approximately 103,000 future cancers, roughly 5 percent of all new cancer diagnoses each year.²⁷
The system is sustained, in significant part, by the people it overdiagnosed. Every woman treated for a non-progressing DCIS becomes, in her own telling, a survivor. Every man whose indolent prostate cancer was cut out becomes a testimonial at the next fundraiser. They believe the screening saved their lives, and they say so — to their families, their neighbors, and their parliaments. The screening programs’ most effective advocates are the people who never had the disease being screened for. They are not lying. The framework that taught them to be grateful cannot acknowledge the mistake without dismantling itself.²³
The pipeline captures the healthy adult and converts him into a chronic patient by treating the body’s signals as the malfunction.
The count is not small, and it is not confined to one country. Approximately 40 million Americans take statins; global prescriptions run to hundreds of millions. Approximately one million prostate biopsies are performed each year in the United States alone; between 0.5 and 2 percent produce sepsis.²⁸ Nearly 500,000 American women have been diagnosed and treated for DCIS since widespread mammography began, with proportionally similar figures from the UK, Australia, and continental Europe; the majority of those cancers would never have progressed. Peter Gøtzsche estimated prescription drugs to be the third leading cause of death in the industrialized world, at approximately 200,000 attributable American deaths per year. Barbara Starfield’s broader iatrogenic estimate ran to 225,000 American deaths when unnecessary surgery, medication errors, hospital-acquired infection, and adverse drug effects were combined. Neither figure includes the deaths from heart disease and cancer whose upstream causation is the profession’s own framework. At the Gøtzsche rate, American medicine alone kills more Americans every year than the country lost in Vietnam, and more every two years than in World War II. Since 1910, at any defensible average of the annual rate, American medicine has killed more Americans than the country has lost in every war it has ever fought, combined. Applied globally, the iatrogenic death total across the century since Flexner runs into figures that no single war or genocide of the modern era approaches.²⁹
Chronic Illness
Multiple sclerosis is labeled autoimmune, incurable, and progressive. The words function together. Autoimmune assigns cause to the body itself, a self-attack whose origin cannot be investigated because it is defined as intrinsic. Incurable forecloses investigation of resolution. Progressive tells the patient what to expect and enrolls them in a lifetime of pharmaceutical management.
Hal Huggins found that MS patients who had mercury amalgams removed from their teeth showed elimination of specific protein bands in their cerebrospinal fluid that had been present before removal.³⁰ The bands were the establishment’s own laboratory markers. Their disappearance corresponded to clinical improvement. The finding was not integrated into treatment protocols. Herbert Shelton described the mechanism a century ago.³¹ The body attempts to expel accumulated toxic burden through acute symptoms; pharmaceutical intervention suppresses the symptoms and adds new toxic material; the new material triggers new symptoms, which are suppressed in turn. What medicine calls progressive disease is the predictable consequence of continuous poisoning combined with continuous suppression.
The financial architecture rewards the labeling. Chronic Care Management billing codes provide recurring monthly reimbursement for conditions expected to last at least twelve months. MS drugs cost fifty-seven to ninety-three thousand dollars per year. A 2025 JAMA Network Open study found pharmaceutical companies paid $164 million to doctors treating MS patients between 2015 and 2019, and physicians who received these payments prescribed the paying companies’ drugs at higher rates.³²
The words the doctor uses are physiologically active. A 1983 British trial divided over 400 cancer patients into three groups; two received chemotherapy, the third received saline. Among the 130 patients who believed they were receiving chemotherapy but were actually getting salt water, 31 percent developed hair loss, 35 percent nausea, and 22 percent vomiting.³³ The side effects they expected produced themselves. A meta-analysis of 130 studies covering 8,219 participants found the nocebo effect clinically significant across somatic and affective outcomes.³⁴ In 1992, a man diagnosed with metastatic esophageal cancer died within weeks of his prognosis. His autopsy found a single two-centimeter nodule on his liver. There was no metastatic spread. His doctor stated the pathological cause of death could not be determined.³⁵ The expectation killed him.
When a doctor tells a twenty-five-year-old that his condition is incurable and progressive, the doctor is administering an intervention. It has no informed consent form, no adverse event reporting system. It is delivered with authority to a patient trained since childhood to trust that authority. It measurably worsens outcomes. Neither the doctor nor the patient recognizes it as an intervention at all.
The Specialties
The inversion runs across every branch of medicine. Two specialties demonstrate it with unusual clarity.
Psychiatry invented the diseases it treats. The chemical imbalance theory of depression, offered as biological fact to millions of patients, was never demonstrated in the research literature. Kenneth Kendler, coeditor of Psychological Medicine, wrote in a 2005 editorial that the search for neurochemical explanations of psychiatric disorders had failed to produce the biological markers the field had promised.³⁶ Robert Whitaker’s investigation of American disability data found psychiatric disability rose sixfold between 1955 and 2007 — a curve that inverts what any real treatment would produce. Martin Harrow’s fifteen-year NIMH follow-up of schizophrenia patients found 40 percent of those who stopped taking antipsychotics were in recovery at fifteen years, against 5 percent of those who remained on medication. The FDA’s 2004 meta-analysis of pediatric antidepressant trials found children on the drugs showed twice the rate of suicidal thinking and behavior compared with placebo.³⁶
Dentistry runs the same inversion on the mouth. No dental school in the United States has a preventive specialty; the American Dental Association has been asked to establish one and declined. Weston Price, who chaired the ADA’s research section from 1914 to 1928, documented in the 1930s that fourteen isolated populations on traditional diets showed decay in less than one percent of teeth examined, and that the same populations one generation after the introduction of refined flour and sugar showed decay in thirty to sixty percent. Ralph Steinman’s laboratory work at Loma Linda established that teeth are hydraulic systems governed by an endocrine signal from the hypothalamus, and that sugar reverses the fluid flow, pulling debris inward through microscopic tubules. The bacteria on the tooth surface are not the cause of the cavity; they are pulled in by the reversal of the flow that should have carried them out. Silver amalgam fillings are approximately fifty percent mercury by weight and release vapor for the life of the filling. Ninety-two percent of American adults have had caries. The specialty that could prevent it does not exist because the profession that repairs it cannot fund itself by graduating dentists who advise patients to eat liver and pastured butter.³⁷
Death
Dying used to happen at home. Within living memory, most people died surrounded by family, in their own beds. The process was understood as natural — not comfortable, not painless, not medicalized.
The condition that brings the person into the ICU is often the accumulated wake of substrate delivered by the same profession decades earlier. The terminal cancer at eighty-three is not the natural end of a long life. It is the destination of a trajectory that began with the injection at age two and was compounded across the decades by pharmaceuticals administered for signals the body was sending.
Roughly half of Americans now die in hospitals or nursing facilities.³⁸ The proportions in the UK, Australia, Canada, and continental Europe are comparable. End-of-life spending absorbs between 13 and 25 percent of Medicare program costs, with equivalent audits of the NHS and Australian and Canadian systems showing similar concentrations.³⁹ Chemotherapy administered within two weeks of death — treatment that cannot extend life meaningfully and almost certainly worsens its quality — happens to a measurable percentage of cancer patients across every industrialized nation with a functioning oncology system.
The system does not have a protocol for stopping. It has protocols for doing. Intubating, resuscitating, monitoring, medicating, scanning, testing. The treatment produces complications. The complications produce further treatment. The question “should we continue treating?” is structurally difficult to ask in an environment designed around the assumption that treatment is always the answer.
The dying body is completing a process. The training the ICU physician received teaches indefinite postponement of the ending, not comfort, not honest acknowledgment, not permission to stop. The final weeks of a life become the most medically intensive and most expensive weeks of the lifespan. What is billed for is not the extension of life. It is the extension of dying.
The Tell
If the inversion were ignorance, healers would be welcomed. They are punished instead. The system’s behavior toward its healers is what distinguishes ignorance from inversion.
In 2023, Myhill was suspended for nine months for recommending ascorbic acid, cholecalciferol, iodine, and ivermectin for the condition attributed to COVID-19. The Tribunal stated that her recommendations undermined public health. Erasure from the register was rejected on the grounds that it would “deprive the public of an otherwise good doctor with over 30 years’ experience.”⁴⁰
A doctor whose patients improve. A protocol that addresses cellular metabolism rather than suppressing symptoms. Recommendations that cost pennies compared to pharmaceutical management. Investigated more than thirty times, not for harming patients, but for undermining the paradigm that requires her patients’ conditions to remain incurable.
The pattern is not new. Semmelweis was destroyed in 1847 for observing that his colleagues were killing patients. Lown was met with Nazi salutes in the 1950s. Myhill’s case is contemporary. If the training were simply incomplete, healers would fill the gap. If the pharmaceutical approach were the best available given current knowledge, alternatives would be welcomed as data emerged. Neither is what happens. Terrain medicine schools were closed by Flexner, terrain practitioners are stripped of their licenses, and the doctors whose patients improve most reliably become the doctors most reliably prosecuted. The system knows the right answer well enough to recognize its practitioners and exclude them.
The Kitchen
Every ordinary childhood illness that now fills pediatric waiting rooms was managed at home by mothers and grandmothers for centuries before the pediatrician existed. What they used is still on the shelf. Honey for the cough — in a University of Pennsylvania trial, honey outperformed dextromethorphan for nighttime cough in children over one.⁴¹ Salt water gargles for the sore throat. A warm compress on the ear; four out of five acute middle ear inflammations resolve on their own within three days, per Cochrane review.⁴¹ Ginger and garlic. Broth. Sunlight, water, rest, warmth, sleep. The kitchen holds most of the toolkit. What the toolkit does not hold, the yard and the sun do.
The mechanism is single. The terrain is the patient. The interventions are supportive: they give the terrain what it needs to complete the clearing that the symptoms represent. Fever is metabolic heat that speeds the clearing; give water and rest. Cough is the airway expelling debris; give honey and warmth. Vomiting and diarrhea are the fastest routes the body has for emptying itself; give broth and time. Skin eruptions are the terrain pushing outward; keep the skin clean and let the clearing happen.
Recovery times have not changed. A cold takes about a week. The flu takes ten days. What the pharmaceutical era added to these timelines was not speed. It added the toxicity of the intervention on top of the illness that was already going to resolve.
The kitchen table works the other way as well.
The Kitchen Table Again
The parent’s hand goes to the cabinet. The bottle is red and white. The child’s fever is 102.4. Behind the parent’s hand stands the doctor. Behind the doctor stand the medical school, the Flexner Report, the Rockefeller money that funded it, and the pharmaceutical industry that has become one of the largest industries on the planet.
The parent does not need to understand any of this in the moment. The parent needs to know one thing. The fever is the operation. The intervention interrupts the operation. Leave the child alone. Offer water. Offer rest. Do not administer the drug that opposes what the body has decided to do.
Every choice a parent makes for a child eventually becomes a choice the child makes for themselves. The child learns whether the body is trustworthy or whether the body is the enemy. That lesson accumulates across a childhood and shapes every medical decision the child will make as an adult. Multiplied across the pediatric schedule, the annual physical, the first prescription, the first surgical referral, the first diagnosis of chronic illness — by the time the person arrives in the ICU at eighty-three, the pattern is complete. The final capture is the destination of a trajectory that began with the red and white bottle.
The parent chooses. The neighbor does not. The pediatrician down the street does not. Every industrialized country’s institutions are now hostile in essentially the same way, because the training that produced those institutions came from essentially the same source. The choice remains available. It has never been popular. It is the difference between the 2.64 percent and the 60 percent. It is the difference between the profession that heals and the profession that has become the first leading cause of death.
The One-Minute Elevator Explanation
The doctor is trained to do the opposite of what heals. When the body raises a fever to clear an illness, the doctor gives a drug to lower the fever. When cholesterol rises to repair damaged blood vessels, the doctor gives a statin to block it. When the body signals distress through blood pressure or blood sugar, the doctor blocks the signals without addressing what produced them.
This is not a gap in the doctor’s education. It is the doctor’s education. In 1910, the Rockefeller and Carnegie foundations funded the Flexner Report, which closed the American medical schools teaching how the body heals and standardized every surviving school on the pharmaceutical model. The Rockefeller Foundation then exported the same template across Europe, Asia, and Latin America. Every industrialized country’s medical schools now train on essentially the same curriculum. Rockefeller himself kept homeopathic doctors for his own family.
The result runs across a lifetime. In childhood, the pediatric schedule injects dozens of doses of products that contain undeclared tungsten, lead, stainless steel, and rare earth alloys the body cannot break down. In adulthood, the annual checkup pulls asymptomatic people into pharmacy pipelines that produce the very conditions the next round of screening will identify. In chronic illness, the same profession that produced the damage names it autoimmune. In dying, the ICU postpones the ending until the bills exhaust the estate.
Joy Garner’s Control Group Survey found chronic disease in the fully unvaccinated at 2.64 percent. In the vaccinated it runs at 60 percent.
If this were ignorance, healers would be welcomed. They are not. Semmelweis was destroyed in 1847 for observing that his colleagues were killing patients. Sarah Myhill has been investigated more than thirty times, not because her patients complained but because they got better.
The doctor is not the third leading cause of death. The doctor is the first.
If you want to follow this, read Malcolm Kendrick on heart disease, Thomas Cowan on cancer and the water body of the cell, and Suzanne Humphries and Roman Bystrianyk on the mortality data.
How to Explain This to a Six-Year-Old
Your body knows how to get better when you are sick. When you get a fever, your body is making itself warmer to fix what is wrong. When you cough, your body is pushing something out. When your skin gets red and itchy, your body is sending the bad stuff outside where it can leave.
Doctors go to school for a long time. But most of what they learn is how to make the fever go away, how to stop the cough, how to make the itchy skin stop being itchy. When the body is working to get better and the doctor stops the body from working, the sickness cannot finish. So it stays.
Doctors also give shots. The shots have tiny pieces of metal in them, too small for your eyes to see. Your body knows how to clean up food and dirt. It does not know how to clean up metal. So the metal stays inside, and where it stays, the body gets sick.
Most doctors are kind people who thought they were going to help. But their school did not teach them how the body heals. They are doing what they were taught. What they were taught is not what makes you better.
When something bad happens to your body, the best thing is usually to let the body do what it knows how to do. Rest. Water. Warm blankets. Good food when you are ready. Time.
There are some doctors who know this. But the other doctors get very angry at them and try to take away their license. That is how you know the other doctors know these good doctors are right. If they were wrong, no one would care.
References
General Medical Council. Records of investigations against Dr Sarah Myhill, 2001–2023, obtained by Freedom of Information Act request and compiled at drmyhill.co.uk. The Tom Kark QC statement is drawn from the 2010 Interim Orders Panel hearing transcript.
Garner, J. Health versus Disorder, Disease, and Death: Unvaccinated Persons Are Incommensurably Healthier than Vaccinated. Control Group Survey, 2020. See also thecontrolgroup.org for methodology and state-level breakdown.
Unbekoming. “The Primary Cause: An Essay on One Impost, Three Shadows.” Lies are Unbekoming, July 2026. The attributable-fraction calculation is developed in the section titled The Numbers.
Kendrick, M. The Clot Thickens: The Enduring Mystery of Heart Disease. Columbus Publishing, 2021. Kendrick, M. The Great Cholesterol Con. John Blake Publishing, 2008. Ravnskov, U. The Cholesterol Myths. NewTrends Publishing, 2000.
Unbekoming. “The Mechanics of Stable Falsehood: An Essay.” Lies are Unbekoming, December 2025. The convergent-opportunism framework is developed in Sections IV and X, drawing on Paul Collits. The Bernard Lown case is drawn from Malcolm Kendrick’s account, cited in that essay. The Sinclair maxim is from Sinclair, U. I, Candidate for Governor: And How I Got Licked. University of California Press, 1935.
Case, A., Deaton, A. Deaths of Despair and the Future of Capitalism. Princeton University Press, 2020. See also National Center for Health Statistics, “Mortality in the United States, 2018,” NCHS Data Brief No. 355, 2020, and subsequent NCHS annual updates documenting the American life expectancy decline that began in 2014 and continued through the pre-COVID period.
Semmelweis, I. P. Die Ätiologie, der Begriff und die Prophylaxis des Kindbettfiebers [The Etiology, Concept, and Prophylaxis of Childbed Fever]. C. A. Hartleben, 1861.
Flexner, A. Medical Education in the United States and Canada: A Report to the Carnegie Foundation for the Advancement of Teaching. Carnegie Foundation Bulletin No. 4, 1910.
Brown, E. R. Rockefeller Medicine Men: Medicine and Capitalism in America. University of California Press, 1979.
Brown, E. R. Rockefeller Medicine Men: Medicine and Capitalism in America. University of California Press, 1979, Chapters 5-7 for the international export of the Flexner model. See also Farley, J. To Cast Out Disease: A History of the International Health Division of the Rockefeller Foundation (1913-1951). Oxford University Press, 2004; and Bu, L. Making the World Like Us: Education, Cultural Expansion, and the American Century. Praeger, 2003, for the China Medical Board and the Peking Union Medical College. The Carnegie Foundation commissioned Flexner’s European survey, published as Flexner, A. Medical Education in Europe. Carnegie Foundation Bulletin No. 6, 1912.
Bealle, M. A. The Drug Story: A Factological History of America’s $10,000,000,000 Drug Cartel. Columbia Publishing, 1949. Rockefeller’s use of homeopathic physicians is discussed throughout, drawing on the diaries and correspondence of the Rockefeller family physicians.
Campbell, E. G., et al. “Institutional academic-industry relationships.” Journal of the American Medical Association, 298(15): 1779–1786, 2007.
Adams, K. M., Kohlmeier, M., Zeisel, S. H. “Nutrition education in U.S. medical schools: latest update of a national survey.” Academic Medicine, 85(9): 1537–1542, 2010.
Begley, C. M., Gyte, G. M. L., Devane, D., McGuire, W., Weeks, A. “Active versus expectant management for women in the third stage of labour.” Cochrane Database of Systematic Reviews, Issue 2, 2019.
Centers for Disease Control and Prevention. Recommended Child and Adolescent Immunization Schedule, current year, compared with 1983 schedule. Historical comparison compiled by the National Vaccine Information Center. Dose counts vary by counting methodology; the figures here reflect the NVIC compilation counting all recommended pediatric doses including boosters and annual influenza injections through age eighteen.
Gatti, A. M., Montanari, S. “New Quality-Control Investigations on Vaccines: Micro- and Nanocontamination.” International Journal of Vaccines and Vaccination, 4(1): 00072, 2017.
Deposition of Stanley A. Plotkin, M.D., taken in Doe v. Doe, Court of Common Pleas, Michigan, January 11, 2018. Transcript widely available; excerpts published by Robert F. Kennedy Jr.’s Children’s Health Defense.
Humphries, S., Bystrianyk, R. Dissolving Illusions: Disease, Vaccines, and the Forgotten History. CreateSpace, 2013. See also dissolvingillusions.com for the underlying mortality graphs drawn from U.S. Vital Statistics and UK historical mortality records.
National Cholesterol Education Program. Third Report of the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III). National Institutes of Health, 2001. Compared with the 1988 ATP I guidelines.
Genuth, S., et al. “Follow-up report on the diagnosis of diabetes mellitus.” Diabetes Care, 26(11): 3160–3167, 2003.
Whelton, P. K., et al. “2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults.” Hypertension, 71(6): e13–e115, 2018.
Bruckert, E., Hayem, G., Dejager, S., Yau, C., Bégaud, B. “Mild to moderate muscular symptoms with high-dosage statin therapy in hyperlipidemic patients — the PRIMO Study.” Cardiovascular Drugs and Therapy, 19: 403–414, 2005. Higher-end figure from patient-reported outcome studies including the STOMP trial and USAGE survey.
Unbekoming. “The 12 Screenings That Manufacture the Patients They Claim to Find: An Essay on Threshold Manipulation, Overdiagnosis, Cascades, and the Markers That Aren’t What They Claim.” Lies are Unbekoming, June 2026. The disease-specific vs all-cause mortality distinction, the autopsy reservoir data, and the survivor-as-advocate mechanism are developed across the essay’s four groups. Primary sources for the autopsy reservoir figures include Welch, H. G. Should I Be Tested for Cancer? Maybe Not and Here’s Why. University of California Press, 2004; and Welch, H. G., Schwartz, L., Woloshin, S. Overdiagnosed: Making People Sick in the Pursuit of Health. Beacon Press, 2011.
Ablin, R. J. “The Great Prostate Mistake.” The New York Times, Op-Ed, March 9, 2010. Extended in Ablin, R. J., Piana, R. The Great Prostate Hoax: How Big Medicine Hijacked the PSA Test and Caused a Public Health Disaster. Palgrave Macmillan, 2014.
Gøtzsche, P. C., Jørgensen, K. J. “Screening for breast cancer with mammography.” Cochrane Database of Systematic Reviews, Issue 6, 2013.
Bretthauer, M., Løberg, M., Wieszczy, P., et al. “Effect of colonoscopy screening on risks of colorectal cancer and related death.” New England Journal of Medicine, 387(17): 1547–1556, 2022.
Smith-Bindman, R., Chu, P. W., Azman Firdaus, H., et al. “Projected lifetime cancer risks from current computed tomography imaging.” JAMA Internal Medicine, published online April 2025.
Loeb, S., Vellekoop, A., Ahmed, H. U., et al. “Systematic review of complications of prostate biopsy.” European Urology, 64(6): 876–892, 2013. See also Unbekoming, “The 12 Screenings That Manufacture the Patients They Claim to Find,” Lies are Unbekoming, June 2026, for the fuller catalog including statin utilization (Centers for Disease Control and Prevention), DCIS overdiagnosis figures (Bleyer & Welch, NEJM 2012), and the harm arithmetic across the major screening programs.
Gøtzsche, P. C. Deadly Medicines and Organised Crime: How Big Pharma Has Corrupted Healthcare. Radcliffe Publishing, 2013, for the ~200,000 US annual iatrogenic death estimate. Starfield, B. “Is US health really the best in the world?” Journal of the American Medical Association, 284(4): 483–485, 2000, for the 225,000 estimate covering combined iatrogenic causes including unnecessary surgery, medication errors, hospital-acquired infection, and adverse drug effects. US war death totals compiled from US Department of Defense casualty statistics and Congressional Research Service reports: American Revolution (~4,435), War of 1812 (~2,260), Mexican-American War (~13,283), Civil War (~620,000), Spanish-American War (~2,446), World War I (~116,516), World War II (~405,399), Korean War (~36,574), Vietnam War (~58,220), Persian Gulf War (~383), Iraq War (~4,431), Afghanistan War (~2,459). Total US war deaths across the country’s history: approximately 1.35 million.
Huggins, H. A. It’s All in Your Head: The Link Between Mercury Amalgams and Illness. Avery Publishing, 1993. The CSF protein band findings are discussed in Chapter 4.
Shelton, H. M. Human Life: Its Philosophy and Laws. Health Research, various editions from 1928. The acute-to-chronic progression mechanism is developed across Shelton’s collected works, particularly The Hygienic System series.
Bove, R., et al. “Financial Payments from the Pharmaceutical Industry to Neurologists Treating Multiple Sclerosis and Prescribing Patterns.” JAMA Network Open, 2025. Chronic Care Management billing figures from Centers for Medicare & Medicaid Services data compiled by AAFP practice analysis.
Fielding, J. W. L., Fagg, S. L., Jones, B., et al. “An interim report of a prospective, randomized, controlled study of adjuvant chemotherapy in operable gastric cancer: British Stomach Cancer Group.” World Journal of Surgery, 7(3): 390–399, 1983. See also Roytas, D. Can You Catch a Cold? Untold History and Human Experiments. Independently published, 2024, for the placebo/nocebo cancer-trial data compiled from this and related studies.
Petersen, G. L., Finnerup, N. B., Colloca, L., et al. “The magnitude of nocebo effects in pain: a meta-analysis.” Pain, 155(8): 1426–1434, 2014.
Meador, C. K. “Hex Death: Voodoo Magic or Persuasion?” Southern Medical Journal, 85(3): 244–247, 1992.
Unbekoming. “The Top 10 Myths of Modern Psychiatry: An Essay.” Lies are Unbekoming, December 2025. Primary sources include Whitaker, R. Anatomy of an Epidemic. Broadway Books, 2010; Breggin, P. R. Toxic Psychiatry. St. Martin’s Press, 1991; Harrow, M., Jobe, T. H. “Factors involved in outcome and recovery in schizophrenia patients not on antipsychotic medications.” Journal of Nervous and Mental Disease, 195: 406–414, 2007; the FDA 2004 meta-analysis of pediatric antidepressant trials; and Kendler, K. S. “Toward a Philosophical Structure for Psychiatry.” American Journal of Psychiatry, 162: 433–440, 2005.
Unbekoming. “12 Things Your Dentist Was Trained Not to Tell You: An Essay on the Profession Trained for Repair, Not Prevention.” Lies are Unbekoming, June 2026. Primary sources include Price, W. A. Nutrition and Physical Degeneration. Price-Pottenger Nutrition Foundation, 1939; Meinig, G. E. Root Canal Cover-Up. Bion Publishing, 1998; Nara, R. O., Mariner, S. A. Money by the Mouthful. Oramedics International Press, 1979; Steinman, R. R., Leonora, J. “Relationship of fluid transport through the dentin to the incidence of dental caries.” Journal of Dental Research, 50, 1971.
Cross, S. H., Warraich, H. J. “Changes in the Place of Death in the United States.” New England Journal of Medicine, 381: 2369–2370, 2019. Institutional deaths (hospital plus nursing facility) accounted for approximately half of American deaths in 2017 (29.8% hospital, 20.8% nursing facility).
Lubitz, J. D., Riley, G. F. “Trends in Medicare payments in the last year of life.” New England Journal of Medicine, 328(15): 1092–1096, 1993, for the higher end of the range. French, E. B., et al. “End-of-life medical spending in last twelve months of life is lower than previously reported.” Health Affairs, 36(7): 1211–1217, 2017, for the lower end. The range reflects genuine methodological disagreement about how end-of-life spending is measured and attributed.
Medical Practitioners Tribunal Service. Determination on Dr Sarah Myhill, 2023. Full text available through the MPTS decision archive.
Paul, I. M., et al. “Effect of honey, dextromethorphan, and no treatment on nocturnal cough and sleep quality for coughing children and their parents.” Archives of Pediatrics & Adolescent Medicine, 161(12): 1140–1146, 2007. Venekamp, R. P., et al. “Antibiotics for acute otitis media in children.” Cochrane Database of Systematic Reviews, Issue 6, 2015. Rovers, M. M., et al. “Antibiotics for acute otitis media: a meta-analysis with individual patient data.” Lancet, 368(9545): 1429–1435, 2006.
This essay draws on the framework developed across the Unbekoming library, including The Unvaccinated (2026), Medicalized Motherhood (2026), The Screening Trap (2026), Chronic Conditions (2026), Heart Disease Reconsidered (2025), and The Architecture of Deception (2025). Readers who find the argument here compelling will find the evidence developed in greater depth in those volumes.
The U.K. government recommended a risky drug combination for COVID-19 patients in 2020, just 16 days after warning doctors to use the medications together only as a last resort, medical commentator John Campbell, Ph.D., said this week.
For years, Campbell has criticized the widespread use of midazolam and morphine and other palliative drugs to treat COVID-19 patients, questioning why so many patients appeared to receive drugs commonly associated with end-of-life care — even though they didn’t necessarily have a terminal illness.
But in his latest video, he said he had overlooked a key piece of the puzzle: The U.K. government itself had backed guidance recommending the combined use of opioids and benzodiazepines for certain COVID-19 patients — just days after warning that the drug combination could cause fatal respiratory depression.
Campbell, who said a former member of the British Parliament brought the issue to his attention, called the apparent reversal “a national scandal which is being ignored.” … Full article
Something unusual and encouraging has happened in Danish climate journalism. Berlingske, one of Denmark’s leading national daily newspapers, has published an excellent and genuinely inquisitive article about the dismissal of physicist Henrik Svensmark from the Technical University of Denmark (DTU), where he has been working since the late nineties. The headline leaves no room for doubt: “Controversial Danish climate and space researcher has received the pink slip from DTU: It is ‘a death blow’ to my research”.
He is one of Denmark’s most internationally recognized researchers – and at the same time one of the most controversial. But now space and climate researcher Henrik Svensmark has, in his own words, been “good old-fashioned fired” by his employer, the Technical University of Denmark (DTU) in Lyngby. He does not rule out that “political considerations” – as he puts it – were involved in the years-long process that led to his final dismissal. At the same time, Henrik Svensmark does not hesitate to call it “a death blow” to a branch of research that he has largely developed single-handedly and that climate researchers around the world, including the UN’s climate panel (IPCC), have had to relate to – often reluctantly. This is mainly because Svensmark’s research points to what he sees as an overlooked natural factor behind a large part of the climate changes Earth has undergone. He finally does not rule out that the dismissal may be linked to the fact that he is perceived as a controversial researcher in wide circles: “There is nothing controversial about the research itself. But it is true that many perceive my research as controversial, even though it shouldn’t be.” DTU has no comments on the actual dismissal of Svensmark and refers to it as a personnel matter. However, the director of DTU Space, Henning Skriver, confirms that Svensmark’s overarching research area, atmospheric physics, will now “be significantly down-prioritized.”
Science journalist Lars Henrik Aagaard deserves credit for the whole article. Rather than dismissing Svensmark as merely ‘controversial’, he asks the essential question: is DTU retiring an ageing employee, or is it terminating an internationally recognized but scientifically inconvenient research program?
The facts reported by Berlingske are troubling.
Svensmark, aged 68, and well known for his work on cosmic rays and clouds, was still actively working and preparing a new experiment. Only a few months earlier, he says, his superiors had told him that his research was important and that they wanted him to continue.
According to Svensmark, he had also been selected for a professorship in 2016 following positive international evaluations. A new rector however, blocked his expected promotion to full professor, downgrading him to Senior Researcher (and lowering his salary). That move made it harder for him to secure regular research funding in Denmark.
In 2021, DTU again attempted to dismiss him, but he continued, partly, he says, because of protests from scientists connected with MIT and Princeton (Lindzen and Happer).
Berlingske presented this history to DTU. The university declined to address it. DTU Space director Henning Skriver merely stated that atmospheric physics was being “significantly downgraded” as part of a strategic prioritization.
That is not an explanation. It is management fog.
A public university may change its priorities. But it should explain the scientific reasoning. Why was Svensmark encouraged to continue only months before his dismissal? What happened to the positive international evaluation? Why was the professorship removed? Why is an active experiment being stopped?
The details of an individual employment case may be confidential. The scientific grounds for closing a research program shouldn’t be. A hypothesis cannot be dismissed administratively.
Solar activity
Svensmark’s research concerns the influence of solar activity and cosmic radiation on aerosol formation, clouds and therefore the climate.
The proposed mechanism is straightforward in principle. Solar activity affects the amount of cosmic radiation reaching Earth. Cosmic radiation ionizes the atmosphere. Ionization may influence the formation and growth of aerosol particles, some of which become cloud condensation nuclei. Clouds, in turn, strongly affect Earth’s radiation balance.
Parts of this chain have been demonstrated experimentally. The unresolved question is how large the resulting climate effect is under real atmospheric conditions and over different timescales.
Svensmark does not claim that carbon dioxide has no effect. He told Berlingske :
“I am not saying that humans are not part of it.”
His point is that natural variability, cloud processes and solar influence remain insufficiently quantified. He describes the dismissal as “a death blow” to the research program he has spent much of his career developing.
Not a marginal researcher
Svensmark cannot reasonably be dismissed as an unsuccessful or marginal scientist. Google Scholar records more than 7,000 citations to his work and an h-index of 30. Compared with the broader DTU research community, this places him approximately among the upper fifth of researchers and probably higher when measured by total citations. That is a considerable scientific impact for a relatively small and highly contested research field, far removed from the large collaborative networks that generate many citations almost automatically.
The predictable but weakest contribution in the article comes from Jens Hesselbjerg Christensen, professor at the Niels Bohr Institute and a prominent figure in the IPCC community.
Hesselbjerg accepts that cosmic radiation may play a role in cloud formation and long-term climate history. He then claims that much of Svensmark’s research appears to have been designed to confirm his hypothesis and that, whenever it was not confirmed, “an arm or a leg” was simply added.
That is an extraordinary accusation and an intellectually shabby one.
Hesselbjerg identifies no paper, no experiment, no faulty measurement, no improper method and no failed prediction. He merely insinuates that Svensmark has constructed his research to reach a predetermined conclusion. If Hesselbjerg believes that, he should name the experiments and explain precisely what was wrong with them. Otherwise, he should withdraw the allegation.
Developing a hypothesis as new evidence appears is not scientific misconduct. It is science. Aerosol formation involves nucleation, particle survival, growth, atmospheric chemistry and eventual cloud formation. Discovering additional mechanisms is not “adding an arm or a leg”. It is the whole purpose of experimental research.
Hesselbjerg’s performance illustrates a wider problem. Researchers close to the institutional consensus can invoke authority while providing remarkably little argument. A dissenting researcher is expected to prove every link in a complex physical chain before his work is even considered legitimate.
That is not a scientific level playing field.
The research should continue
The immediate objective should not merely be to embarrass DTU. It should be to ensure that Svensmark’s research survives. The most important next step is to develop a climate model that explicitly includes the proposed chain connecting solar activity, cosmic radiation, atmospheric ionization, aerosol growth and clouds, alongside greenhouse-gas forcing and the other established climate mechanisms.
Such a model would make it possible to test a question of enormous scientific and political importance: How much of the observed temperature development is caused by human influence, and how much is caused by natural variation?
That question is far from purely academic. Climate policy depends critically on the answer. If natural influences are larger than assumed, the expected effect of reducing carbon emissions is smaller. If they are negligible, the current attribution of climate change to CO2 becomes stronger. Either result would be valuable.
As explained by Henrik Svensmark: “The next decisive step is to build a climate model in which the influence of solar activity, cosmic radiation, aerosol growth and clouds is represented together with greenhouse gases. That would allow us to test how much of modern climate change is human-caused and how much is natural. This can be done within a few years and with a research budget that is modest compared with the political and economic importance of the question.”
The task is therefore concrete: we need to find a new institutional home for Svensmark, preserve the equipment and scientific expertise, assemble an international research team and raise the necessary funding.
Berlingske has performed a valuable public service by bringing this case into the open. DTU has responded with evasion. Jens Hesselbjerg Christensen has responded with an undocumented attack on a colleague’s scientific integrity.
Neither response is acceptable.
Science advances through experiments, observations and testable models, not through administrative priorities, institutional conformity or casual insinuations.
Henrik Svensmark’s research must not end with a DTU management decision. It must now be given the resources to face the only judgement that matters: the judgement of observations.
Karl Iver Dahl-Madsen is an independent consultant (owns Dahl-Madsen ApS), chairman of the board of the Danish climate-sceptical association Klimarealisme (Climate Realism), and a frequent commentator/debater in Danish media on climate policy, energy, and environmental issues. More: https://klimarealisme.dk/
When asked at a Senate hearing whether she thinks mRNA vaccines are safe and effective, CDC Director-nominee Erica Schwartz replied, “I do believe that mRNA technology is safe and effective.”
Both the question and the answer show a serious lack of scientific understanding.
Here’s the scientifically accurate answer to the question: We don’t know the full safety profile of either of the two types of approved mRNA vaccines or the technology. First, It’s all too new. Second, we’re not even collecting the full data.
Read on for details.
According to FDA scientists and other experts in the field, comprehensive safety data isn’t known until a new drug (including vaccines) has been on the market and in widespread use for 7-12 years.
Even now, we aren’t getting full information on safety profiles because the data isn’t even being collected in the comprehensive manner required for accurate analysis.
The established scientific process requires that all illnesses after vaccination be meticulously recorded regardless of whether a patient or doctor thinks the illness is actually connected to the vaccine.
Most doctors are not following the process. Some misunderstand. Others are willfully ignoring. And no authority is ensuring they do their job.
Doctors typically aren’t even asking their ill patients whether they had an mRNA vaccine (for Covid or RSV), which one(s), and when. So they aren’t collecting that crucial data.
Most people, including physicians, don’t understand that patients being treated for any illness are supposed to be queried. This means, for example, someone who come to the ER with a retinal detachment should be asked if he had Covid vaccine, which, how many, and when, and then the data should be reported to the Vaccine Adverse Event Reporting System (VAERS). Same with someone who becomes sick with a rash, headaches, tendon rupture, stiff neck, depression, or chest congestion. Everything.
Even when patients do tell a physician they think an illness might be vaccine related, the physician frequently, improperly, determines on the front end that he doesn’t need to report the possible adverse event to the established database unless he thinks it’s connected to the vaccine. That’s not how the system works. No doctor is qualified to make that determination about a new medicine. All illnesses are supposed to be recorded so that previously unrecognized adverse events can be unearthed.
Additionally, many doctors and patients don’t understand— and aren’t being told— that adverse events from vaccines and other medicine can arise months or years after the medicine is taken.
Further, they don’t understand that an adverse event can be related to a drug even if the patient did not initially become ill after taking the vaccine or other medicine.
And the blanket question itself, “Are mRNA vaccines safe and effective,” shows a lack of scientific understanding on the part of the questioner. It begs counter-questions: are they safe for whom? Under what circumstances? Effective at what? It’s as ridiculous as asking, “Is medicine safe and effective?” Depends on whether or not you’re allergic to it. Depends on whether you have predispositions for things that make you more susceptible to the side effects. Depends on whether its particular mechanisms work in your individual biology. These are individual calculations.
Even in the general picture, there aren’t blanket answers. We know mRNA Covid vaccines failed woefully—proved ineffective—at a sliding scale of supposed goals: They don’t prevent infection. They don’t prevent spread. They don’t prevent illness. There’s a debate over whether they prevent serious illness, which most people don’t get from Covid, and children almost never get.
Until we stop pretending that the blanket questions make sense, and that the answers are connected in any way to science, we will continue to have leaders who misinform or mislead.
So, from diabetes drugs that can cause fatal genital tears to acne medicine that can cause sexual dysfunction that never goes away, here are some notable examples of unexpected adverse events that were eventually linked to vaccines or other medications.
Sildenafil (Viagra) and blindness [non-arteritic anterior ischemic optic neuropathy (NAION)/sudden vision loss].
Viagra treats erectile dysfunction by inhibiting PDE5 to increase blood flow. Early marketing focused on cardiovascular risks but not eye issues. Hundreds of post-approval reports eventually linked it to sudden vision loss from NAION. The adverse event was only recognized when enterprising physicians pressed the issue and published case reports, and I reported on them for CBS News. The FDA added warnings in 2005. Labels now advise stopping use and seeking care for sudden vision changes. Similar risks apply to the PDE5 inhibitor class.
Likewise, Viagra was eventually connected to hearing loss.
Reports emerged of sudden hearing decrease/loss (sometimes with tinnitus/dizziness) after use. Initially not linked, post-marketing data led to label updates advising immediate medical attention. Nobody initially guessed an erectile dysfunction drug could cause deafness and blindness!
Statins such as atorvastatin and simvastatin, and severe and potentially fatal muscle pain/weakness (myalgia, myopathy, rhabdomyolysis).
Statins are used to lower cholesterol to prevent heart disease/stroke. Early labels noted mild muscle issues, but the drugmakers initially denied severe cases (including rhabdomyolysis, which can cause kidney failure). Independent doctors, lawsuits, and my reporting for CBS News drew attention to this problem. Eventually, the drug makers added warnings, monitoring advice, and dose adjustments.
Statins and cognitive effects (memory loss, confusion).
Some users reported “brain fog” or confusion, initially dismissed as unrelated. I reported on this, too, for CBS News. Eventually, FDA added reversible cognitive side effects to labels in 2012 based on reports.
Troglitazone (Rezulin) and severe liver failure.
This thiazolidinedione treated type 2 diabetes. Only did post-1997 use among millions reveal dozens of acute liver failure cases (deaths/transplants), originally denied by the drugmaker. Reporting by the Los Angeles Times and then by me at CBS News forced the issue. Eventually, the drug was withdrawn in 2000 after FDA tied it to about 63 deaths. (Scientists say each recognized and reported death implies 1,000 to 100,000 more that are never reported.)
SGLT2 inhibitors such as canagliflozin/Invokana, dapagliflozin/Farxiga, empagliflozin and potentially fatal Fournier’s gangrene (necrotizing fasciitis of perineum/genitalia).
These diabetes drugs lower blood sugar via urinary glucose excretion. Believe it own ot, they can cause life-threatening flesh-eating infections in the genital/perineal area. FDA issued a warning in 2018. The labels now carry strong alerts.
mRNA Covid-19 vaccines (Pfizer, Moderna) and myocarditis/pericarditis heart issues.
As you know, these vaccines were found to cause heart inflammation, mostly in young men after second dose. This was initially unexpected.
Covid-19 vaccines and menstrual irregularities.
Many women reported changes such as heavier bleeding and cycle shifts, but were largely called conspiracy theorists. This adverse event like so many others linked to Covid vaccines, weren’t identified—at least they weren’t reported— after initial studies.
Covid-19 vaccines and eye issues. Even without persistent data gathering, there have been enough reports of eye inflammation and retinal problems to raise concern over a possible link.
Thalidomide and severe birth defects.
Once marketed as a sedative and morning sickness aid in the 1950s–60s, it turned out to cause more than 10,000 cases of babies born with shortened or absent limbs and other defects.
Isotretinoin (Accutane) for acne and persistent sexual dysfunction.
Recent FDA updates added erectile dysfunction, decreased libido, vaginal dryness, and lubrication issues that may persist even when people stop taking the drug.
A similar effect was initially denied by later found with SSRI antidepressants, Selective Serotonin Reuptake Inhibitors. They can cause persistent sexual dysfunction.
Cisapride (Propulsid) for indigestion and cardiac arrhythmias/QT prolongation. It was withdrawn after heart rhythm deaths. I reported for CBS News on the coverup of a baby death in a fraudulent Propulsid study.
Rofecoxib (Vioxx) and cardiovascular events. Nobody guessed a pain medicine and arthritis drug would cause heart attacks and strokes. All concerned initially denied the signals but the medicine was eventually removed from the market for this reason.
Fenfluramine/phentermine (Fen-Phen) weight loss drug and heart damage. This is another drug that caused unpredicted heart problems and was eventually taken off the market after the FDA had approved it as “safe and effective.”
Certain fluoroquinolones and tendon rupture/peripheral neuropathy. Who would have guessed antibiotics could cause a tendon rupture or nerve damage? Eventually, all agreed that fluoroquinolones can do this, and a serious “black box” warning was added to the label.
Antipsychotics and tardive dyskinesia. Drugs meant to control psychotic tendencies can actually cause serious movement disorders, which nobody anticipated initially.
What about when a cancer treatment causes cancer? Tamoxifen for breast cancer can cause and uterine cancer. Nobody predicted that. The warning was later added to the labels.
Ketamine for pain and anesthesia and bladder damage. This side effect only emerged when there was greatly expanded psychiatric use of the medicine.
Lots of medicines cause unexpected bone loss, including medicine that’s prescribed to protect bones! They include bisphosphonates like Fosamax or alendronate, Actonel, Boniva, and Reclast. They are commonly prescribed to treat and prevent osteoporosis by slowing bone breakdown. However, after lots of use, scientists learned they can actually cause serious bone problems, including thigh bone fractures, osteonecrosis of the jaw (dead jawbone), and delayed bone healing. FDA eventually added warnings and updated the labels. Other drugs eventually linked to bone loss and fracture risk include: corticosteroids like prednisone for inflammation, asthma, autoimmune diseases, and allergies; acid reflux drugs like omeprazole/Prilosec or esomeprazole/Nexium); aromatase inhibitors (like anastrozole/Arimidex) for breast cancer; and the injectable birth control shot Depo-Provera.
Rachel Hotez is a real adult, now in her early thirties. Every description of her in this essay comes from her father’s own words in his 2018 book. The argument is with the book, not with her.
The vaccine visit
Peter Hotez, in his 2018 book Vaccines Did Not Cause Rachel’s Autism, describes his daughter at her pediatric appointments. Rachel “would cry longer and with much fiercer intensity than our other children.”¹ The sentence appears once. Hotez does not return to it. Rachel is one of four Hotez children. Among them, she is the only one on the spectrum, and the only one whose reaction to the injections her father describes in these terms.
Peter Hotez is not a random pediatrician. He holds an MD and a PhD. He is Dean of the National School of Tropical Medicine at Baylor College of Medicine, Co-Director of the Texas Children’s Center for Vaccine Development, and founding editor-in-chief of the journal PLOS Neglected Tropical Diseases. He served as a U.S. Science Envoy under the Obama administration. In the years after 2020 he became one of the most visible defenders of vaccination policy on American cable news, and in 2022 was nominated for the Nobel Peace Prize for developing a low-cost COVID vaccine. His 2018 book was the opening statement in that public role. His daughter is the girl the title is defending.
The book runs to two hundred pages. Roughly two thirds of them are Rachel. Her first words, her flights across the neighborhood, her sneakers thrown from a moving car onto the Merritt Parkway at sixty miles per hour, her decades of intellectual disability that leaves her at twenty-five sorting donated clothes for fourteen dollars a day at Goodwill.¹ The other third argues that none of this can be attributed to the injections.
The book has an unusual quality. It is not, in the strict sense, a defense of the vaccine schedule. It is a father’s project to explain his daughter without implicating his own life’s work. Front to back, the book reads like the case Hotez was building against himself.
Rachel Hotez was born in the early 1990s. Peter Hotez was on the faculty at Yale, developing a vaccine for hookworm. Ann Hotez had two older children already. Rachel, the third of what would become four, is described in the book as an easy baby, “content to sit in her car seat, in the dining room or another quiet place and read.”¹ Her first year was, in her mother’s words, unremarkable. She sat unsupported later than her siblings, at nine months rather than six, but her parents attributed the delay to individual variation. “Children do not all learn and grow in the same ways, or at the same speed,” Ann later wrote.¹
By eighteen months, Rachel was not walking. She was not talking. Her pediatrician, Simone Simon, raised the concern. Ann Hotez writes that she and Peter had not seen it: “How could it be that Peter, a pediatrician himself, and I, an experienced mother, hadn’t noticed? I think we had seen differences, but we attributed them to what we knew, or thought we knew, about child development.”¹
The referral was to the Birth-to-Three intervention team at the Darcey School. Rachel was starting to talk by twenty months. By twenty-nine months she was functioning at the eighteen-month level in most areas. At Yale in the spring of 1995, she was diagnosed by Dr. Wendy S. Levine with pervasive developmental disorder, not otherwise specified. She was three years old.
Between eighteen and twenty-four months, Rachel had lost the trajectory she was on. Her father’s book identifies this window precisely, as a matter of clinical description, and returns to it as the central subject of his Chapter 9.
The timeline that contradicts itself
Chapter 9 of Hotez’s book is titled “What Does Cause Autism? The Scientific Evidence.” It is the book’s central scientific move. Hotez cites a series of brain imaging studies, most prominently a 2017 paper from Joseph Piven’s group at the University of North Carolina–Chapel Hill.² Piven’s team scanned the brains of infants whose siblings already had autism, and who were therefore considered at higher risk, at multiple points during infancy. They found measurable changes in the brains of children later diagnosed as early as six to twelve months of age. Specifically, the outer layer of the brain, the cortex, expanded faster than normal between six and twelve months, and the brain as a whole grew larger than expected between twelve and twenty-four months. The larger brain size coincides with the age at which most parents first recognize the condition.
Hotez presents this as decisive. If measurable brain changes are present at six months of age, he argues, then the vaccines given at twelve and eighteen months cannot have caused those changes. He writes: “The changes in the brains of kids with ASD are set into motion well before (about a year) many parents recognize any signs of alterations in communication or social behavior.”¹
The argument depends on what a reader does not know, or does not pause to consider.
The current injection schedule for an American newborn begins within hours of birth, with the compound marketed as vitamin K. That injection is not formally part of the vaccine schedule but is administered nearly universally. The formal vaccine schedule begins on the same day, with hepatitis B. It resumes at two months, with DTaP, Hib, pneumococcal conjugate, inactivated polio, rotavirus, and a second hepatitis B dose. At four months, most of the same combination is repeated. At six months, most of it is repeated again, along with the first influenza dose. By six months of age, a child has received approximately twenty vaccine doses, several of which contain aluminum adjuvant. The cumulative aluminum burden by six months of age has been estimated at approximately 4.4 milligrams,³ a figure Hotez himself cites in Chapter 8 while comparing it favorably to dietary aluminum in infant formula.¹
The comparison is where the omission is starkest. When aluminum is eaten in food, less than one percent is absorbed into the body. When aluminum is injected as part of a vaccine, it is designed to stay. The compound is added to vaccines because it holds at the injection site and provokes the inflammatory response that makes the vaccine work. French research groups have documented that aluminum-loaded white blood cells remain at injection sites for years,⁴ and that these particles are then carried through the lymphatic system to distant tissues, including the brain.⁵ Aluminum has been recovered from brain tissue of autism decedents at concentrations substantially higher than in age-matched controls.⁶ Christopher Shaw and Lucija Tomljenovic have documented dose-response relationships between pediatric aluminum burden and autism prevalence across multiple countries.⁷ None of this literature appears in Hotez’s book. Aluminum adjuvant is addressed in a single dismissive paragraph in Chapter 8, primarily by reference to the Children’s Hospital of Philadelphia comparison to formula.¹
The Piven timeline does not exonerate the vaccine schedule. It identifies the window in which vaccine-induced injury would produce measurable effects. Whatever is producing the cortical expansion Piven documented at six to twelve months of age is happening after the birth-through-six-month injection schedule, not before it. Hotez names the window. He does not name the exposures inside it.
Rachel’s regression was observed at eighteen months. She had received the standard childhood schedule available at the time. What Piven’s MRI cannot see, because his study was not conducted until decades later, is what Rachel’s brain looked like at six months, or at twelve months. What is preserved in the record is Ann Hotez’s testimony that she had bonded less to Rachel than to her older children, that Rachel was “quiet” and “content,” that Rachel’s motor milestones were behind but her attention span seemed strong. What is also preserved is Peter Hotez’s own observation that Rachel cried longer and more intensely at the needle than her siblings did.
What happens in the window
Piven’s timeline identifies when brain changes become measurable. It does not identify what causes them. Hotez’s book, having named the timeline, moves on. The question of what happens in the birth-through-six-month window remains open. Answering it requires setting the book aside.
Aluminum hydroxide and aluminum phosphate are added to vaccines because they persist. The industry term for a compound added to a vaccine to intensify the body’s response is adjuvant. Aluminum functions as an adjuvant because it resists clearance. The body’s repair processes engage the compound and cannot dispatch it. The resulting sustained inflammation is what the industry calls efficacy.
The design depends on a biological assumption medicine does not defend openly. It assumes that the body will confine its response to the injection site. It will not.
Beginning in 1998, Romain Gherardi and colleagues at the French National Institute of Health and Medical Research described a condition in adults who had received aluminum-adjuvanted vaccines. Muscle biopsies at the injection sites showed distinctive lesions: aggregates of white blood cells called macrophages, filled with aluminum hydroxide. The lesions were present years after the injection. Aluminum, in other words, did not clear. It remained at the site, engulfed by cells that could not digest it.⁴
Fifteen years later, Zakir Khan and Gherardi’s group published a follow-up study. Using fluorescent aluminum hydroxide particles injected into the muscle of mice, they demonstrated that the particles were carried away from the site by macrophages, drained through the lymphatic system, and arrived in distant tissues, including the brain, over weeks and months. The transport depended on a specific signaling molecule, CCL2, that summons macrophages to sites of inflammation. Blocking CCL2 stopped the process. Restoring CCL2 restored it.⁵
Aluminum is injected. It provokes the inflammation it was designed to provoke. White blood cells arrive to engulf it. They cannot digest it. They carry it, embedded within themselves, through the lymphatic system to wherever the body is calling for their services. In an infant whose blood-brain barrier is still developing, they carry it into the brain.
Christopher Exley’s group at Keele University has recovered aluminum from brain tissue samples of people who died with autism, at concentrations substantially higher than in age-matched controls without autism.⁶ Christopher Shaw and Lucija Tomljenovic at the University of British Columbia have documented dose-response relationships across countries: as the pediatric aluminum injection burden has risen, so has autism prevalence.⁷ The correlations do not prove causation. They form the kind of convergent signal the studies Hotez cites in Chapter 8 would have been designed to test, if the field had been oriented toward asking the question.
In 1913, Charles Richet was awarded the Nobel Prize in Physiology or Medicine for his description of anaphylaxis. What Richet actually demonstrated, in a series of experiments on dogs beginning in 1901, was that injecting a foreign protein into an animal produced a heightened response to any subsequent exposure to the same protein. The first injection sensitized. The second could kill. Richet named the process anaphylaxis, from the Greek for “without protection.”¹⁹ His finding, that the injection route sensitizes the body against future encounters with the same substance, is Nobel-documented history.
Every childhood vaccine contains foreign proteins injected in the presence of aluminum designed to hold. The Richet mechanism is not disputed. It is simply not applied to childhood vaccination in the mainstream literature, because to apply it would be to concede what the industry is designed to deny.
The reader does not need to accept every step of this reasoning to hold the essay’s central point. Aluminum accumulates. It travels. It has been recovered from the brains of people who died with autism. The mechanism that would produce sensitization from injected foreign proteins won a Nobel Prize. None of this appears in the book Hotez wrote to close the question.
Rachel’s regression window opened at eighteen months, months after the aluminum-containing doses at two, four, and six months would have completed the biopersistence and transport described above. What her brain looked like at six months of age is not preserved in the record. Neither is her cerebrospinal fluid aluminum concentration at any age. Neither is any measurement that would let a family ask, decades later, whether their daughter’s condition was set in motion by exposures her father’s book does not consider possible.
The years of intervention
By age five, Rachel had a formal IQ evaluation. Her verbal IQ was 84, near the low end of normal. Her performance IQ was 60. Later testing put her performance IQ in the 40s.¹ She was placed on Prozac, then Zoloft, then Luvox, then Risperdal. Each medication, in Hotez’s account, produced worse effects than the last. She was eventually taken off all psychiatric medication.
Rachel had two psychiatric admissions at Yale-New Haven’s Winchester 1 inpatient unit. An EEG revealed right-sided temporal lobe spike discharges. She was placed on tegretol for a period, with what Hotez describes as “possibly some improvement.”¹ The tegretol was eventually discontinued because Rachel would not comply with the blood draws needed for level monitoring. The Hotez family lived through years that Peter describes with candor: “dreary or frightening,” “wearing us down,” “she seldom gave much back emotionally, compared with the other children.”¹
The family relocated to Houston in 2011, where Peter had accepted a position at Baylor College of Medicine. Rachel finished her secondary education at Lamar High School with a certificate. She could not sustain the transition program at Houston Community College. Two brief residential placements failed. She lived, and continues to live, at home with her parents.
By 2016, Hotez had begun writing what he calls “science tikkun” pieces for PLOS. In early 2017 he published an op-ed in the New York Times titled “How the Anti-Vaxxers Are Winning.”⁸ The book followed in 2018.
The name that does not appear
Hotez names his opponents. Andrew Wakefield, characterized as an “elaborate fraud” quoting Brian Deer’s BMJ series. Robert F. Kennedy Jr., named in connection with campaigning around thimerosal and working with the parent group Safe Minds. The film Vaxxed, called “phony.” Hotez identifies a “toxic combination of hysteria and pseudoscience,” “phony propaganda,” “fake news, half-truths, and conspiracy theories.”¹
He does not name William Thompson.
William Thompson is a senior scientist at the U.S. Centers for Disease Control and Prevention. In August 2014, through his attorneys at Morgan Verkamp LLC, Thompson issued a public statement about a 2004 study he had co-authored in the journal Pediatrics.⁹ The study, DeStefano et al., examined children in the Atlanta area, comparing when they received the MMR vaccine to whether they later developed autism. It concluded there was no link.¹⁰ Thompson’s 2014 statement was direct:
I regret that my coauthors and I omitted statistically significant information in our 2004 article published in the journal Pediatrics. The omitted data suggested that African American males who received the MMR vaccine before age 36 months were at increased risk for autism. Decisions were made regarding which findings to report after the data were collected, and I believe that the final study protocol was not followed.⁹
Thompson provided documents to Congressman Bill Posey. On July 29, 2015, Posey read Thompson’s statement into the Congressional Record on the floor of the U.S. House of Representatives.¹¹ Thompson has never recanted the statement. He remains employed at the CDC. His full statement, released through his attorneys at Morgan Verkamp LLC, is archived among the Vermont Legislature’s official witness testimony documents from its 2015 hearings on vaccine policy.⁹
Vaxxed, the film Hotez dismisses in his book as “phony,” is a documentary built around Thompson’s disclosure. It contains recordings of Thompson’s conversations with the biologist Brian Hooker. Hotez’s characterization of the film appears in a book that never names its subject.
The DeStefano 2004 study Thompson repudiated is one of the studies Hotez cites in Chapter 8. It appears in the list of investigations that, in his summary, demonstrate no link between MMR and autism.¹ The reader is not told that a senior author of one of those investigations has publicly stated that statistically significant findings were omitted.
The pattern extends beyond Thompson. Hotez’s Chapter 10, titled “Struck by Lightning,” offers his central injury statistic: approximately one severe adverse event per one million vaccine doses. He derives the figure by dividing roughly 300 annual compensated claims from the National Vaccine Injury Compensation Program by roughly 300 million annual doses.¹ The comparison to being struck by lightning is presented as authoritative.
The math depends on the pieces used. Hotez’s numerator is the number of NVICP claims that were compensated. NVICP dismisses more claims than it pays. Claims must be filed within three years of the injury appearing. Causation must be proven to a narrow list of conditions the program formally recognizes. Conditions that appear months or years later are not included. The denominator, 300 million doses, is total administered doses. The Vaccine Adverse Event Reporting System, VAERS, is meant to be the surveillance instrument that catches adverse events at the population level. In 2011, a study conducted by Harvard-Pilgrim Health Care under a grant from the Agency for Healthcare Research and Quality, principal investigator Ross Lazarus, was submitted to the federal government. Its finding on VAERS capture rate was that “fewer than 1% of vaccine adverse events are reported.”¹²
Hotez does not mention the Lazarus report. The underreporting problem does not appear in his book. His lightning comparison depends on the Lazarus figure being wrong by a factor of a hundred, and that dependence is not addressed. A correction of two orders of magnitude would move his rate from one per million to one per ten thousand. At the CDC’s own current estimate of 1 in 36 children diagnosed with autism,¹³ the question of what a serious adverse event actually is, and how it is counted, is the question the book was written to close.
Hotez closes it by not opening it.
The perpetual gene
In 2017, Peter and Ann Hotez arranged with the Baylor Department of Genetics to sequence their own DNA and Rachel’s. Whole exome sequencing produces the sequences of the protein-coding regions of the genome. The stated purpose was to identify any variants that might be linked to autism or intellectual disability.
Hotez describes the result with unusual restraint. Rachel had “some genetic variants, including one affecting a gene that could be linked to ASD or mental disabilities.”¹ He writes that the family plans to submit her results to the Baylor Johns Hopkins Center for Mendelian Genetics and to the NIH-supported Undiagnosed Diseases Network, “in order to determine if Rachel’s genetic variants might also be present in other individuals on the autism spectrum or with other mental health conditions.”¹
The sentence is worth reading twice. The whole exome sequencing did not identify a cause of Rachel’s condition. It identified variants of uncertain significance that Hotez hopes might one day be shown to be relevant.
This is the outcome the book has been building toward. Chapter 9 promises that autism is genetic. Hotez cites work from the Simons Foundation and Princeton estimating that as many as one thousand genes may eventually be identified as contributing to autism.¹⁴ At the time of the book’s publication, sixty-five had been identified. The remaining nine hundred and thirty-five are described as awaiting discovery.
The reader is asked to accept a paradigm that has produced sixty-five candidate genes across three decades of intensive investigation, and to expect that the next three decades will produce the remaining nine hundred and thirty-five. The larger project has similar dynamics. The Human Genome Project promised to identify the genetic basis of common disease, and produced approximately twenty thousand genes rather than the one hundred thousand originally predicted. Its subsequent genome-wide association studies for autism have identified small-effect variants that account for a modest fraction of the heritability those studies were designed to explain. The gene has been coming for thirty years.
Meanwhile the environmental candidates Hotez does name in Chapter 9 are curated. He cites Phillip Landrigan’s 2010 review identifying prenatal exposures associated with autism-like presentations: valproic acid, thalidomide, misoprostol, chlorpyrifos.¹⁵ He cites maternal rubella exposure during pregnancy as a cause of congenital rubella syndrome, which he says “can closely resemble autism.”¹ From this he draws a conclusion that returns the reader to the book’s title with a strange inversion: “The ‘R’ component of the MMR vaccine is actually the rubella vaccine that protects a mother from transmitting rubella virus to her baby, and in so doing functions as an effective vaccine against autism.”¹
The MMR vaccine, according to Hotez, prevents autism. This appears in a book titled Vaccines Did Not Cause Rachel’s Autism.
He raises maternal fever and points to Ian Lipkin’s Columbia group work on maternal viral exposures.¹⁶ He notes a 2017 Kaiser Permanente study that found a 1.2 odds ratio for autism among children whose mothers received influenza vaccine in the first trimester.¹⁷ He dismisses the finding as “not statistically significant after adjusting for multiple comparisons.” An odds ratio of 1.2 in a study of nearly two hundred thousand children is not a finding a scientist would dismiss if he were looking for the cause. It is a finding a scientist would dismiss if he had already located the cause elsewhere.
Aluminum adjuvant does not appear in Chapter 9. In a chapter titled “What Does Cause Autism,” the compound most commonly injected into infants under six months of age, one with documented biopersistence, translocation, and central nervous system deposition, is not discussed as a candidate.
Nor does the chapter engage the growing literature comparing vaccinated to unvaccinated cohorts. Anthony Mawson’s 2017 pilot study of homeschooled U.S. children reported that the vaccinated group had substantially higher rates of neurodevelopmental disorders, allergies, and chronic conditions than the unvaccinated group.¹⁸ Studies of this design remain the most direct empirical test of the question Hotez’s book is written to close. None appear in his citations. The one study design that could definitively answer the question, he dismisses in a single line elsewhere in the book: a randomized trial of vaccinated versus unvaccinated children would, he writes, be “unethical.”¹
The book’s opening dedication lists the funding sources for Hotez’s Center for Vaccine Development at Texas Children’s Hospital. Among them: the Bill & Melinda Gates Foundation. The Carlos Slim Foundation. Gavi, the Vaccine Alliance. UNICEF. The World Health Organization. The Kleberg Foundation. The Blavatnik Charitable Foundation. The Brockman Medical Research Foundation. The Japanese Global Health Innovative Technology Fund. The Southwest Electronic Energy Medical Research Institute. The National Institutes of Health. The Centers for Disease Control and Prevention. The Walter Reed Army Institute of Research. The United States Public Health Service. Baylor College of Medicine. Texas Children’s Hospital.¹
Hotez addresses this preemptively in Chapter 8. He notes that he holds patents on his vaccines but has “not received a penny” and has “no real prospects for financial gain.”¹ The disclaimer is technically accurate. It is also beside the point. Institutional capture does not require kickbacks. It requires career. A scientist whose salary, laboratory, institutional affiliation, and public standing all depend on the paradigm the book defends is not neutral, whether or not he personally profits from any particular product.
Rachel at twenty-five
At the end of the book, Rachel is twenty-five. She lives with her parents in Montrose, Houston. Her routine is fixed. She wakes at four in the morning to Skype her friend Sabrina in Denver. Her morning walk takes her to Randall’s supermarket for a plain bagel, no butter. Later she walks to Subway for a six-inch tuna sandwich, no cheese, mustard on hearty Italian. Along the way she talks to shopkeepers, asks strangers about their dogs, and occasionally brings home men she meets on the street, whom her father has to ask to leave.
She has, at the time of the book’s writing, just been enrolled in a Goodwill training program. A chance airport encounter between her parents and the wife of the Goodwill Houston board chairman produced the introduction. Rachel sorts donated clothes for stains and rips. She works two hours a day. After taxes, Ann Hotez writes, “it is about $14 a day and $215 so far.”¹
This is what the book’s title is defending. A young woman with a performance IQ in the 40s who cannot count money, cannot sustain a classroom, cannot hold employment for more than two hours per day, and lives with her aging parents in a neighborhood where they worry, in the book’s own words, about her safety at night. Hotez writes with clear love for his daughter. He describes Rachel as loyal to her friends, curious about people, empathetic toward animals, quick to strike up conversation in the neighborhood. She is all of these things. She is also a young woman whose life was, at some point, altered.
Her father spent two hundred pages arguing that the alteration cannot be attributed to what he did for a living. The William Thompson statement of August 2014 is not addressed. The aluminum burden accumulated during the first six months of life is not examined as a candidate cause. The injury statistic in Chapter 10 depends on assuming that VAERS captures nearly all vaccine-related injuries, an assumption the Harvard-Pilgrim report says is wrong by a factor of a hundred. The alternative causation runs through a genetic paradigm that has produced sixty-five candidate genes in thirty years and promises another nine hundred and thirty-five to come. On one page inside a book denying vaccine-autism links, the MMR vaccine is inverted into an anti-autism intervention.
The book was written to close the question. What it does instead is document, in loving and exhaustive detail, the life of the girl whose story the question was always about. Rachel cried at the injections longer and more intensely than her siblings did. Between eighteen and twenty-four months, she lost skills. Her EEG showed spike discharges. Her intellectual disability is profound. She sorts clothes at Goodwill.
The door her father wrote his book to close is still open. He walked past it in every description of his own daughter.
References
Hotez PJ. Vaccines Did Not Cause Rachel’s Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism Dad. Baltimore: Johns Hopkins University Press; 2018.
Hazlett HC, Gu H, Munsell BC, Kim SH, Styner M, Wolff JJ, et al. Early brain development in infants at high risk for autism spectrum disorder. Nature. 2017;542(7641):348–351.
Offit PA, Jew RK. Addressing parents’ concerns: do vaccines contain harmful preservatives, adjuvants, additives, or residuals? Pediatrics. 2003;112(6 Pt 1):1394–1397.
Gherardi RK, Coquet M, Cherin P, Belec L, Moretto P, Dreyfus PA, et al. Macrophagic myofasciitis lesions assess long-term persistence of vaccine-derived aluminium hydroxide in muscle. Brain. 2001;124(Pt 9):1821–1831.
Khan Z, Combadière C, Authier FJ, Itier V, Lux F, Exley C, et al. Slow CCL2-dependent translocation of biopersistent particles from muscle to brain. BMC Med. 2013;11:99.
Mold M, Umar D, King A, Exley C. Aluminium in brain tissue in autism. J Trace Elem Med Biol. 2018;46:76–82.
Tomljenovic L, Shaw CA. Do aluminum vaccine adjuvants contribute to the rising prevalence of autism? J Inorg Biochem. 2011;105(11):1489–1499.
Hotez PJ. How the anti-vaxxers are winning. New York Times. February 8, 2017.
DeStefano F, Bhasin TK, Thompson WW, Yeargin-Allsopp M, Boyle C. Age at first measles-mumps-rubella vaccination in children with autism and school-matched control subjects: a population-based study in metropolitan Atlanta. Pediatrics. 2004;113(2):259–266.
Posey B. Remarks on the William Thompson statement. Congressional Record. July 29, 2015;161(120).
Lazarus R, Klompas M, Bernstein S, et al. Electronic Support for Public Health–Vaccine Adverse Event Reporting System (ESP:VAERS). AHRQ Grant Final Report, Grant No. R18 HS 017045; 2011.
Maenner MJ, Warren Z, Williams AR, Amoakohene E, Bakian AV, Bilder DA, et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years — Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2020. MMWR Surveill Summ. 2023;72(2):1–14.
Krishnan A, Zhang R, Yao V, Theesfeld CL, Wong AK, Tadych A, et al. Genome-wide prediction and functional characterization of the genetic basis of autism spectrum disorder. Nat Neurosci. 2016;19(11):1454–1462.
Landrigan PJ. What causes autism? Exploring the environmental contribution. Curr Opin Pediatr. 2010;22(2):219–225.
Mahic M, Mjaaland S, Bøvelstad HM, Gunnes N, Susser E, Bresnahan M, et al. Maternal immunoreactivity to herpes simplex virus 2 and risk of autism spectrum disorder in male offspring. mSphere. 2017;2(1):e00016-17.
Zerbo O, Qian Y, Yoshida C, Fireman BH, Klein NP, Croen LA. Association between influenza infection and vaccination during pregnancy and risk of autism spectrum disorder. JAMA Pediatr. 2017;171(1):e163609.
Mawson AR, Ray BD, Bhuiyan AR, Jacob B. Pilot comparative study on the health of vaccinated and unvaccinated 6- to 12-year-old U.S. children. J Transl Sci. 2017;3(3):1–12.
Richet C. Anaphylaxis. Nobel Lecture, December 11, 1913. Nobel Media AB. Available at: nobelprize.org.
Decorous and admissible language fails me, in alluding to that which might have seemed incredible thirty years ago—the commanding of vaccination on a second child of a family, when vaccination has killed the first; and then sending the father to prison for refusal.
— Emeritus Professor F.W. Newman, 1874
Author’s Note
This essay draws heavily on Dissolving Illusions: Disease, Vaccines, and the Forgotten History by Dr. Suzanne Humphries and Roman Bystrianyk. Their decade of archival work—recovering the primary documents, mortality tables, medical journal articles, and photographs that mainstream history has quietly buried—made this essay possible. The vaccine farms, the horse stables, the named children, the foot-and-mouth outbreaks, the Beddow Bayly address, the Lancet admissions about equine origin: all of it comes from records that were sitting in libraries and archives waiting for someone willing to look.
Where I have drawn from their book, the sources they cite are primary documents—USDA bulletins, Lancet articles, court records, contemporary medical journals. I have verified and expanded where useful, but the archaeological work is theirs.
Readers who want the full documentary foundation for what follows should read Dissolving Illusions. It is the essential reference on this subject. What I offer here is a narrower cut: the material itself—what has been in the vials, from Jenner’s day to the current schedule.
I have also drawn on Michael Willrich’s Pox: An American History for the Camden and vaccine-farm details, on the peer-reviewed work of H.V. Wyatt for the 1916 Rockefeller passages, on the CDC’s own excipient documentation for the current inventory, and on the work of Dr. Sherri Tenpenny for details on the specific-pathogen-free egg supply chain.
The interpretation is my own. The evidence belongs to the record.
The calf was led from the stable to the operating room and strapped to the table. Its belly was shaved. The skin was washed, then scarified with a surgeon’s knife—superficial linear incisions cut into the shaved abdomen and thighs. Vaccine material was smeared into the bleeding cuts with an ivory or metal instrument. The animal was released to a pen. About a week later, when the wounds had ulcerated and infectious material flowing from them, the calf was brought back. The contents of the ulcers were scraped out, mixed with glycerin, drawn into vials, and shipped.
This was smallpox vaccine. The procedure was documented in the medical and agricultural literature of the period, photographed and described without controversy. The USDA published detailed accounts of the vaccine farms in its Bureau of Animal Industry reports. The medical journals published the technique. Physicians described the work in their own textbooks. Nobody was exposing anything. This was standard industrial practice. The vaccine industry did this on a national scale, in facilities called “vaccine farms,” from 1870 until well into the twentieth century. The material went into the arms of American schoolchildren.
The calf, once bled of its material harvest, was frequently returned to the herd. Some vaccine farms rented their calves from local dairies. When the collection was complete, the animals went back into the food supply.
This is what The Science looked like. Not as an abuse of the paradigm—as the paradigm itself, functioning as designed. For a hundred and fifty years, the vaccine industry’s core problem was biological: how to obtain the raw material. The solutions—cow, horse, sheep, goat, monkey, chicken, mouse, dog, pig, and eventually the aborted human fetus—define the history of what medicine considered “immunization.” Every generation of vaccines has been an animal product, in one direction or another. What follows is the record.
Part One: Before the Farms (1796–1870)
Edward Jenner named his product after the Latin word for cow, vacca. He believed cowpox in cows originated from a disease in horses called “the grease”—an eruption on the horse’s heels caused by an inflammatory condition of the skin. In 1829 the Lancet published a note revealing that the lymph Jenner had been circulating for three or four years around Berkeley was drawn not from cows but from horses. He had, according to the Lancet, “decisively ascertained before he died” that the disease he was using was equine, not vaccine [cow] pox.
By 1834, the medical literature reflected complete confusion about what the substance actually was. A contemporary article listed three competing theories: Jenner’s grease-of-the-horse origin, the theory that the material was smallpox modified by passage through cows, and the theory that cowpox was a disease as native to cows as scarlatina was to man—unrelated to smallpox at all. A French practitioner cited in the same article maintained that in France there was no evidence cowpox had ever appeared in cows at all.
The confusion was not academic. It described what was being scratched into people’s arms.
For a hundred years after Jenner, the standard procedure was arm-to-arm vaccination. Material containing pox was rubbed from the arm of one inoculated child into cuts made on the arm of the next. In this way, the substance was passed forward through generations of children, sometimes serially through dozens or hundreds of hosts before anyone thought to trace its origin. Whatever else was in the material of the last child—syphilis, tuberculosis, hepatitis, the mercury and heavy metals of nineteenth-century treatment—travelled with it.
The procedure required a “good take”: a substantial pustule forming at the site of the wound. To ensure this, doctors made incisions at multiple sites on the same arm at one sitting—up to four wounds per child. The photograph titled “Multiple site vaccination of 1898, showing a typically good arm” shows the result: an arm ruined across four separate infection sites.
Arm-to-arm vaccination was outlawed in England in 1898. Multi-site vaccination continued in various parts of the world until 1975.
A second method existed for towns where arm-to-arm passage was impractical. Human pox scabs were dropped into a jar. Water was added. The jar was shaken. The resulting material was used as vaccine for the entire town.
In 1952, Dr M. Beddow Bayly summarised what a century and a half of “smallpox vaccine” had actually consisted of. His words, delivered in a public address, describe the state of the vaccine supply as it stood in the middle of the twentieth century:
When we recall that vaccine material is derived, in the first place, either from a smallpox corpse, the ulcerated udder of a cow, or the running sores of a sick horse’s heels, the choice depending upon the country of its origin and the firm which manufactures it, it is hardly to be wondered at that it has far-reaching ill effects on the human constitution.
He continued, quoting the Lancet‘s earlier admission: “no practitioner knows whether the material he employs is derived from smallpox, rabbit-pox, ass-pox, or mule-pox.” Bayly noted that England’s own Ministry of Health had “long confessed to complete ignorance of the ultimate source of its own supply.” A British Medical Journal contributor of the period stated that the strain used for routine material preparation in England was “believed to have been derived from a case of smallpox in Cologne during the last century.”
The corpse. The udder. The horse’s heel. The unknown source. This was the substance for a hundred years.
Part Two: The Industrial Calf (1870–1930)
In 1870, calf-based production began in the United States. The original starting material was imported from France and inoculated into a herd of cows at a farm near Boston. Within a few years, “vaccine farms” had sprung up across the country. The proprietors were mostly medical doctors who identified an opportunity to profit from rising demand. The farms produced smallpox vaccine at first. They soon diversified into diphtheria material and other biologics.
The procedure was the one described in this essay’s opening. Calves were rented or purchased, strapped to operating tables, scarified, inoculated, released to incubate, and brought back for the material harvest. Some farms returned the animals to their owners. Others slaughtered them. The New England Vaccine Company, one of the larger commercial operations, ran a farm at Wakefield, Massachusetts, rented calves from a farmer named Owen Clark, and returned them to circulation once the material had been collected.
The commercial products of this era carried the names of firms that later became household pharmaceutical corporations. H.K. Mulford and Company. Parke Davis. Wyeth. Lederle. The vaccine industry was born on these farms.
Two consequences followed. Neither was hidden. Both were documented at the time in the medical and agricultural literature.
Foot-and-Mouth Disease
Production on living calves that were subsequently returned to the food supply produced periodic outbreaks of foot-and-mouth disease in cattle populations. The disease is highly contagious among cattle and causes economic devastation. Outbreaks occurred in 1870, 1880, 1884, 1902, and 1908.
The 1902 outbreak lasted six months and affected 244 herds. Of these, 205 were slaughtered—3,872 cattle, along with 360 hogs and 220 sheep and goats. The USDA published detailed instructions for the burial of the carcasses: trenches deep enough for five feet of cover dirt, hides slashed to prevent exhumation for the leather trade, quicklime poured over the meat.
The origin of the 1902 outbreak was traced to the New England Vaccine Company and to Dr E.E. Tyzzer’s experimental work at the Wakefield farm—the farm where calves were rented from Owen Clark for the production of vaccine material. The 1908 outbreak was traced to a Japanese vaccine strain imported by another manufacturer (”Manufacturer B” in the USDA report) to improve their standard product. The strain carried foot-and-mouth disease. Because Manufacturer B killed its calves after harvest, the material remained internal for a period. Manufacturer A, on the other hand, rented calves and returned them to circulation—which is how the disease entered the general cattle population.
People who worked with cattle developed severe blistering conditions. The 1902 medical literature contains detailed case reports of butchers who received cuts on their hands while working with animals and subsequently developed bullous eruptions across their bodies. Dr John Bowen documented the connection at Massachusetts General Hospital in 1904.
Human recipients of the smallpox vaccine developed the same conditions. Multiple case series were published between 1902 and 1911 documenting acute pemphigus in children who had recently been vaccinated. The New Orleans outbreak of the same period produced cases in children who had never been near a butcher. The vaccine itself was the vector.
The Camden School District, October 1901
In early October 1901, an eight-year-old girl in Camden, New Jersey died of smallpox. Her father followed her, then seven of her siblings. In the panic, the Camden school board announced it would enforce an 1887 vaccination law. The board took bids. The Mulford pharmaceutical company won the contract.
By the end of October, the arms of approximately 5,000 Camden schoolchildren had been scraped with a metal prong and rubbed with Mulford’s calf-derived material.
On the first of November, William Brower, sixteen years old, died. He had been vaccinated nineteen days earlier. Over the following weeks, eight more children died. Every one of them, with a single exception, had received the Mulford vaccine at school. Children vaccinated at the free downtown clinic or by their own physicians were unaffected.
A parallel outbreak occurred at Pennsylvania Hospital, where 4,500 patients and staff had been vaccinated with the same product. Mulford’s official explanation, delivered by the company’s advertising and sales manager—a 29-year-old chemist named Albert C. Barnes, later famous as the founder of the Barnes Foundation art collection—appeared in the New York Times. The dead children, Barnes wrote, came from a “lower class of people” whose “carelessness” had “poisoned the wounds.” The Camden Board of Health had commissioned the investigation from a Mulford employee. It did not occur to anyone that this constituted a conflict of interest.
Bacterial spores that cause death by lockjaw are common in soil and manure. Production on calves in stables and pens exposed the material harvest to constant potential contamination. The calves were strapped to tables in rooms that had, in many cases, been used for stabling. No sterile technique protected the wound-culture from the animal’s environment.
The dead children were not the exception. They were the visible edge of a system that produced its raw material in barns.
Lübeck, 1930
The end of the animal-vaccine-farm era was marked, in Germany, by an incident that made the same principle explicit in a different biological medium.
Between December 1929 and April 1930, 251 newborns in the town of Lübeck received three oral doses of Bacille Calmette-Guérin (BCG), a tuberculosis preparation derived from the bovine tuberculosis organism, within the first ten days of life. The programme had been approved by the town’s health council and its medical association. Posters advertised it. Newspapers endorsed it.
Seventy-seven of the vaccinated infants died. One hundred seventy-three developed what was identified as active tuberculosis.
The cause was traced to the laboratory where the BCG material was prepared. In the same unlocked incubator space, what was identified as virulent human tuberculosis organisms (the Kiel strain) were also being cultivated. There was no separate designated area for vaccine preparation. There was no animal testing to confirm the safety of the batches before administration. The vaccine and the other organism shared a room. Dr Georg Deycke, head of the general hospital, was later convicted of negligent homicide and sentenced to two years. Ernst Altstaedt received fifteen months.
The BCG preparation itself is a live bovine organism. The organism was originally isolated from the udder of a tuberculotic cow in France by Albert Calmette and Camille Guérin, then serially processed by passing it through 230 subcultures over thirteen years. The Lübeck disaster ended the oral route of administration worldwide. The preparation itself, still derived from the same 1908 bovine isolate, remains in use today.
Part Three: The Horse Stables (1895–1940s)
What medicine calls diphtheria antitoxin, introduced in 1895, was manufactured from horse blood.
The procedure was straightforward. A horse was injected with escalating doses of material extracted from what medicine calls diphtheria toxin over a period of weeks. The body responded to the injected substance by producing what is identified as antibodies. The horse was then bled—large quantities of blood drawn from the jugular vein—and the serum extracted. The serum was drawn into vials and injected into humans.
The first commercial producers included Parke Davis, Mulford, and the New York City Board of Health. By the early 1900s, horses were being used to produce a range of preparations: the diphtheria material, what was called tetanus antiserum, meningococcus material, and staphylococcus preparations in multiple varieties. A 1911 New Zealand pharmacopoeia list includes—among many other products—an item called simply “Normal Horse Serum,” administered as a therapeutic agent.
The horse serum was foreign protein. The human response to repeated injection of foreign animal protein was documented by Charles Richet in 1901, work that won him the 1913 Nobel Prize. Richet showed that injection of foreign proteins created sensitisation—the body responds with increasing intensity to subsequent exposures. Serum sickness—fever, joint pain, rashes, kidney inflammation, and in severe cases death—was a documented consequence from the early years and remains listed on package inserts as a caution today.
The mortality curve tells its own story. In Leicester, England, the death rate from what medicine calls diphtheria had been declining steadily for the fifty-seven years from 1838 to 1895. In 1895, horse-serum preparation was introduced. The death rate then rose to approximately ten to fifteen times its previous level and stayed elevated for the next five years.
In New York City, the death rate among children under ten fell from 785 per 100,000 in 1894 to under 300 by 1900—a decline that was already well underway when the serum came into use. By 1920, when the toxoid preparation was introduced, the rate had already fallen below 100. The mainstream story credits the horse serum and then the preparation with these declines. The curves credit sanitation, nutrition, and improved living conditions.
Jim
On the second of October 1901, a horse named Jim was euthanised at the St. Louis city stable. Jim was a former milk wagon horse, retired to the poorhouse two years earlier and put to work producing what was called diphtheria antitoxin for the St. Louis Board of Health. Over the course of his career, Jim produced more than thirty US quarts—about twenty-nine litres—of serum.
Two days before his euthanasia, on the thirtieth of September, Jim had been routinely bled. The blood was drawn into flasks and processed into serum. By the time Jim showed signs of illness and was killed, the serum had already been bottled and distributed.
Jim had what was identified as tetanus. The serum drawn from him on the thirtieth of September was contaminated with spores from this condition in incubation phase.
Dr Amand Ravold, the physician responsible for the operation, was aware of the danger. He ordered the September thirtieth batch destroyed. It was not destroyed. Bottles labelled “August 24”—a date when Jim’s serum had been clean—were filled with the contaminated September thirtieth material. The bottles were distributed to the physicians of St. Louis.
The first child began convulsing on the twenty-sixth of October 1901. Her name was Veronica Keenan. She was one of two Keenan children who had received the serum as a preventive measure. Neither had shown symptoms related to what the material supposedly protected against. Within a week, all three Baker children were dead. The symptoms included arched back and convulsions.
Thirteen St. Louis children died. The last, on the seventh of November.
The court of inquiry named Ravold and the janitor Henry Taylor as responsible. Both were dismissed. Ravold went on to a distinguished career. He served as president of the St. Louis Medical Society. His 1942 obituary made no mention of the deaths.
The St. Louis deaths and the Camden deaths, occurring in the same weeks of the same autumn, produced sufficient public pressure that Congress passed the Biologics Control Act of 1902. Historians describe this as the origin of American vaccine regulation. What it regulated was the horse stables and the calf farms.
Use of what was called diphtheria antitoxin dropped sharply nationwide in the aftermath. In Chicago, physicians and parents refused it. The death rate from what medicine calls diphtheria in Chicago that year rose by a third.
Part Four: The Monkey House (1955–present)
By the mid-1950s, the vaccine industry had largely abandoned the calf farms and the horse stables. The new production medium was cell culture. The new species was the rhesus macaque and, later, the African green monkey.
The Rockefeller Passages
Between 1910 and 1916, at the Rockefeller Institute in Manhattan, Simon Flexer and his associates were serially passing material through the spinal cords of rhesus monkeys. The material was extracted from a monkey, injected into the spinal cord of another monkey, and then extracted again after paralysis developed. This passage process was repeated many times, selecting for material that would replicate highly in the neural tissue of monkeys. Occasionally, the passages were reinforced with fresh material from human cases.
By 1916, the resulting material had become highly destructive to nervous tissue and capable of high replication in multiple cell types.
In May 1916, an outbreak began in Brooklyn. It reached 23,000 cases and 5,000 deaths. It moved through New England and the Middle Atlantic states, reaching Delaware, Maryland, and the District of Columbia. The death rate was twenty-five percent—sixteen times higher than typical presentations. The proportion of two-year-olds affected was the highest ever recorded. The outbreak began in early May, well before the normal summer season. None of these features were ever recorded again in any similar outbreak.
The first known case lived a few blocks from a rail line that connected via the Brooklyn Bridge and 63rd Street directly to the Rockefeller Institute, three miles away, where Flexner’s laboratory was conducting the passages. The material being cultivated there had been selected, through serial passage, for unprecedented ability to damage the nervous system of the hosts receiving it. Dr H.V. Wyatt published this analysis in 2011.
No investigation was undertaken at the time. No inquiry into the laboratory’s work. No examination of what material had been cultivated or where it might have gone. The outbreak was attributed to Italian immigrants. Immigration records show the outbreak began before the accused children arrived. The official explanation required no investigation because it required no explanation.
Salk, Sabin, and the Monkey Kidney
The preparations introduced in the 1950s were produced by growing material on the kidney cells of monkeys. The kidneys were removed from live rhesus macaques—hundreds of thousands of them, over the years—minced, and used as culture medium.
In 1960, Bernice Eddy, a researcher at the National Institutes of Health, discovered that the monkey kidney cells routinely used were contaminated with a virus. She called it Simian Virus 40 (SV40). When injected into hamsters, SV40 produced tumors. When mixed with human cells in culture, it transformed them—the standard laboratory signature of a cancer-causing virus.
The material had been in mass administration in the United States since 1955. Approximately 98 million Americans had received it. Every dose administered before 1963 contained SV40. Doses after 1963 were required to be screened, but the screening was, in Stanley Kops’ documented analysis, incomplete—the seed strains themselves were never fully verified. SV40 has been detected in material produced through the 1990s.
SV40 has since been found in human tumors: mesothelioma of the lung, several types of brain tumor, and cancers of the bone, breast, colon, and kidney. Dr Michele Carbone, one of the principal researchers in the field, called SV40 “the perfect war machine”—it affects at least four major cellular mechanisms that either promote tumor growth or interfere with the cell’s cancer defences. It is not found in the healthy tissue surrounding these tumors.
When Carbone and Dr Harvey Pass prepared to publish their findings, a senior NIH figure told Carbone that if he or Pass spoke to the press “against his wishes,” they would be “punished.” Pass said afterwards: “I didn’t think you got punished for science.”
Formaldehyde was the killing agent for the preparation. SV40 was shown in 1961 to survive formaldehyde treatment beyond the standard twelve-day treatment period. The manufacturer’s cited standard remained twelve days.
Monkeys are still used in production today.
The Cutter Incident
In April 1955, several batches of Cutter Laboratories’ preparation—produced on monkey kidney cells—contained what was identified as live, unattenuated material that had survived the formaldehyde process. Within days, children who had received the Cutter preparation began developing paralysis. The final tally: 40,000 children affected, 200 permanently paralyzed, ten dead.
Cutter’s product was the only one recalled. In 1990, Freedom of Information Act documents revealed that Wyeth had also produced batches with similar properties during the same period. Wyeth’s product remained on the market. Congressman Percy Priest, chair of the investigation, later stated: “We felt that no lasting good could come to science or the public if the Public Health Services were discredited.”
Swedish researchers, testing their own supplies in the aftermath of Cutter, discovered that thirty percent of batches previously certified as safe contained what was identified as live material when re-tested. Dr Sven Gard, the Swedish expert, later stated that the American material in 1955 caused as much paralysis as it prevented.
The pattern would repeat. Regulation followed disaster, then legitimised the practice it was meant to constrain. Expansion followed.
Part Five: The Current Inventory
The vaccine schedule administered to American children in 2026 is the direct descendant of the calf farms, the horse stables, and the monkey house. What has changed is the range of species. What has not changed is the principle: biological material derived from animals is grown, harvested, processed, and injected into the human body.
The list below is drawn from the CDC’s Vaccine Excipient Summary and from the FDA-approved package inserts of the current vaccines. It is not a critic’s characterisation. It is the manufacturers’ declaration of what is in their products.
From cattle. Fetal bovine serum. Bovine serum albumin. Bovine calf serum. Calf serum protein. Bovine extract. Bovine muscle tissue. Bovine protein. Lactalbumin hydrolysate. Lactose. Present in DTaP, Td, Tdap, IPV, rotavirus (RotaTeq), hepatitis A (Vaqta), Japanese encephalitis (Ixiaro), MMR, MMRV, varicella, zoster, HepA-HepB, Pentacel, Kinrix, and Pediarix.
Fetal bovine serum extraction represents industrial blood harvest. When pregnant cows arrive at slaughter, workers discover the pregnancy during processing. While the mother cow is dying but not yet dead—before the umbilical cord is cut—they ram a large-bore needle directly into the beating heart of the unborn calf, draining all the blood. The fetus is killed through exsanguination while still connected to the dying mother. This blood is then centrifuged to separate the serum, creating the product injected into children. The different names on package inserts—fetal bovine serum, calf serum, newborn calf serum—indicate the age of the fetus when killed, with older fetuses yielding more blood and different grades of serum.
From chickens. Egg protein. Ovalbumin. Chicken protein. Chick embryo cells. Chick embryo fibroblasts. Chick kidney cells. Present in every standard influenza vaccine (Fluzone, Fluvirin, Fluarix, Flulaval, Afluria, Agriflu, FluMist), yellow fever, rabies (RabAvert), MMR, and MMRV.
The influenza vaccine supply chain requires 500,000 eggs weekly to produce 76 to 80 million doses annually. These eggs come from specialized hatcheries maintaining “specific pathogen-free” (SPF) status—tested for approximately thirty designated organisms. Critically, coronaviruses are excluded from the testing panel despite being endemic in chickens, existing there symbiotically like yeast on human skin. This means every dose produced from SPF eggs contains chicken coronaviruses that are then injected into humans. This undisclosed viral presence exposed generations to pre-existing reactions, which later manifested in severe reactions when COVID vaccines were administered—explaining the widespread anaphylaxis requiring emergency equipment at vaccination sites.
From pigs. Hydrolysed porcine gelatin. Standard porcine gelatin. Present in Zostavax, MMR-II, yellow fever, several influenza vaccines, Japanese encephalitis (JE-Vax), and varicella. Trypsin—an enzyme extracted from pig pancreas—is used as a processing agent in the manufacture of the rotavirus vaccines. In 2009, a porcine virus type 2 (a virus associated with wasting disease in pigs) was discovered in both licensed brands of infant rotavirus vaccine. It had entered the manufacturing stream through the pig-based enzyme.
From monkeys. Monkey kidney tissue is still used in material production. Vero cells—an immortalised cell line derived in 1962 from the kidney of an African green monkey—are used in production of the polio, rotavirus, and rabies vaccines currently distributed.
From dogs. Madin-Darby Canine Kidney (MDCK) cell protein and MDCK cell DNA. Present in Flucelvax influenza vaccine. The cell line was established from the kidney of a cocker spaniel in 1958.
From mice. Mouse serum protein. Present in the Japanese encephalitis vaccine JE-Vax.
From insects. Baculovirus. Insect cell lines derived from Spodoptera frugiperda (the fall armyworm moth). Present in Flublok recombinant influenza vaccine.
From humans. MRC-5 cells and WI-38 cells. Both are cell lines derived from the lung tissue of aborted human fetuses. MRC-5 was established in 1966 from the lung of a fourteen-week-old male fetus. WI-38 was established in 1962. Present in hepatitis A (Havrix), Twinrix, MMR-II, MMRV, varicella, zoster, rabies (Imovax), the adenovirus vaccine, and Pentacel. The residual DNA of the aborted fetus—cellular DNA fragments from the original 1962 or 1966 tissue, carried forward through decades of cell passage—remains in the final vaccine as an unavoidable component of the manufacturing process. Human serum albumin (drawn from pooled human plasma) is present in the ACAM2000 smallpox vaccine and the rabies vaccine.
The current inventory is an incomplete list. Each package insert specifies the ingredients for a single vaccine. The consolidated list is the responsibility of researchers who compile it from many sources.
The list is what medicine considers, in 2026, to be the state of the art.
What Was Actually Happening
The historical record is not ambiguous. For a hundred and fifty years, the vaccine industry took biological material from the wounds, glands, blood, kidneys, and cell lines of animals—first cattle, then horses, then monkeys, and eventually chickens, dogs, mice, pigs, insects, and the tissues of aborted human fetuses—processed it minimally, drew it into vials, and scratched, scarified, or injected it into the bodies of healthy children.
The material was, by definition, foreign to the recipient. Whatever else was in it—the spores from the stable floor, the SV40 from the monkey’s kidney, the foot-and-mouth material from the calf that had been rented back to a dairy, the porcine virus from the pig-based enzyme processing—travelled with the intended payload. The vaccine industry’s own package inserts describe these contaminants as “residual.” The word describes what remains. It does not describe how much of it is there, or what it does when injected.
The suppression of independent inquiry continues into the present. In 2016 and 2017, Italian researchers Gatti and Montanari—scientists whose rigorous methodology had made them trusted industrial product testers for European governments—analysed vaccine contents using electron microscopy and mass spectrometry. They found multiple vaccines contaminated with undeclared metallic particles including stainless steel, tungsten, lead, zirconium, and other industrial materials never listed on ingredient disclosures. When they published these findings, their laboratory was raided by authorities in 2018, equipment confiscated, government contracts terminated, and they were run out of the country. The message remained constant across generations: measure the vaccines and lose everything.
The mainstream story is that this practice worked. The mortality curves say otherwise. What medicine calls diphtheria declined ninety-seven percent between 1900 and the mid-1940s before the preparation was introduced. What medicine calls whooping cough declined more than ninety percent before the preparation of the mid-1940s. What medicine calls measles declined more than ninety-eight percent before the preparation of 1963. Scarlet fever, for which no preparation was ever widely deployed, declined by a comparable amount over the same period. The declines correlate with sanitation, nutrition, refrigeration, and the exit from overcrowded slum housing.
The population whose grandparents received the Mulford calf material, whose parents received the horse-serum preparation, and whose children receive the fetal-bovine-serum-cultured products of the current schedule is the same population. It is the reader’s family, in serial generations, submitting the same veins to the same industry.
The record contains named children. Bessie Baker was six. Veronica Keenan was four. William Brower was sixteen. The Lübeck infants had names their mothers had chosen a few weeks before administering the poster-advertised preparation. The children paralyzed by the Cutter material are alive today in some cases, in wheelchairs.
The vaccine industry did not begin in the mid-twentieth century. It began on the operating table where the calf was strapped. The industrial infrastructure—the farms, the horses’ stables, the monkey colonies, the fetal cell repositories—was constructed generation by generation to solve one problem: how to produce, at scale, biological material that could be pushed through a needle into a healthy person. The material has always been what the animal or the fetus produced.
The name given to this practice was “vaccination.” What was actually happening was the industrial-scale injection of foreign biological substance into the bodies of populations that had, in most cases, no way to refuse. The material was drawn from a calf’s wound, or from a horse’s neck, or from a monkey’s kidney, or from the lung of a human being who was aborted in 1966 and whose cells are still being passaged in laboratories in 2026.
This is what The Science looked like. This is what The Science is.
The photograph from the vaccine farm era shows a calf strapped to a wooden table, its belly shaved and cut. The image exists in the archival record. It was published without controversy. It described the standard practice.
The photograph is what was injected.
How to Explain This to a Six-Year-Old
Your child asks: “What does the needle do?”
You say: “A long time ago, doctors wanted to help people not get sick. But they didn’t really understand how sickness works. So they had an idea: What if we take the sick stuff from a cow or a horse, and put it in a healthy person? Then maybe that person’s body will learn how to fight the sickness.”
Your child asks: “Did it work?”
You say: “That’s the interesting question. Sometimes people got sicker instead of better. And sometimes they died. The doctors noticed this, but they didn’t stop. They kept doing it anyway.”
Your child asks: “Why?”
You say: “Because once they started, it was hard to stop. More and more people used it. Factories were built to collect this stuff from animals. People got jobs doing this work. Money was being made. When people asked questions about whether it was actually helping, they got in trouble or lost their jobs.”
Your child asks: “What happened?”
You say: “People’s bodies got used to the animal stuff. And sometimes other bad stuff was mixed in with it—poison from the stables, diseases from other animals. People got sick from the animal stuff itself, not from the sickness they were supposed to be protected from.”
Your child asks: “Do they still do this?”
You say: “Yes. They just use different animals now—chickens, monkeys, and even cells from people. They call it science. They call it protecting you. But if you look at what actually happened to people’s health, it went up because houses got better, food got cleaner, people had less crowded places to live. The animal stuff wasn’t the reason people got healthier. But the people making and selling it got rich, so they kept saying it was.”
Your child asks: “So should I get the needle?”
You say: “That’s a question for your family to decide together. What I’m telling you is what actually happened, and what’s actually in the needle. The needle contains animal stuff. Sometimes it helps. Sometimes it hurts. But the doctors and the companies making it won’t be honest about that part. They’ll say it’s completely safe. They have money riding on you believing that. So you need to know what’s actually true.”
Your child asks: “How do I know what’s true?”
You say: “Ask the question: Where did this come from? What’s actually in it? What happened to people who got it? What happened to people who didn’t? Then read the answers yourself. Don’t let someone else tell you what’s true just because they’re a doctor or they’re in charge. Look at the actual evidence. That’s how you know.”
The Shape of the Ritual
A healthy child is brought to a room. A trained man in a robe or coat receives the child. He holds a small vial. Inside the vial is a substance drawn from the body of an animal — a cow, a horse, a chicken, a monkey, a pig, or a human being who was killed before birth. The substance was obtained by inflicting injury on the animal: the calf strapped and cut, the horse bled from the neck, the monkey’s kidneys removed and minced, the fetus exsanguinated through a needle to the heart while still connected to its dying mother. The substance is drawn from the animal’s suffering.
The man in the coat holds the child. He pierces the child’s skin with a metal instrument. He pushes the substance from the animal into the child’s flesh. The child cries. The parents are told this is protection. They pay for it, or the state pays for it. They are told that refusal would be an act against the child.
The shape is old. It is older than germ theory, older than the Latin word vaccina, older than Edward Jenner and the horse’s heel and the calf farm at Wakefield. In its previous incarnations it was called by other names. In each case the mechanics are the same: a substance from a suffering animal, mediated by a priest-class, delivered into the flesh of the healthy in exchange for a promise. In the older forms, the promise was protection from famine, plague, or unseen enemies. In the current form, the promise is protection from disease. The substance and the ceremony have not changed. The vocabulary has changed.
The hermetic-alchemical tradition — the current of Western esoteric thought that reached Renaissance Europe through Pico della Mirandola and Johannes Reuchlin, was carried forward at the court of Elizabeth I by John Dee, was systematised in the Rosicrucian manifestos of 1614 and 1615, and became the intellectual substrate of Freemasonry and its later derivatives — held that the human being is base matter to be worked upon. The goal of the operation, called the Great Work, was the transformation of that base matter into something higher through serial technical operations conducted by adepts. The material was to be purified, mixed, tested, and refined until it moved. This was not metaphor. The alchemists attempted the operation on matter and on themselves.
Among the specific images transmitted through this tradition was the creation of an artificial being — an animate creature made from dead matter by human hands rather than by God. Medieval sources, drawn into the Western hermetic mainstream by the sixteenth-century Christian Kabbalists, describe the operation as following the pattern of a calf. The calf was the template. Frances Yates, the twentieth century’s principal historian of the hermetic tradition, documented in The Occult Philosophy in the Elizabethan Age how this material entered Christian Europe through Pico, Reuchlin, and above all John Dee, whom Elizabeth I employed as her royal astrologer and code-named 007. The 1615 Rosicrucian Confessio Fraternitatis announced the program that would shape the next four centuries: “that which in before times hath been unseen shall be spoken forth and uttered.” The program had two parts. The first was the transformation of the human being into something the operator had produced. The second was the eventual open confession of the operation to a public that had been ritually prepared to accept it.
The tradition that carried this program into the Anglo-American world was Rosicrucian, Freemasonic, and — in its American form — the network of secret societies of which Skull and Bones (founded 1832 at Yale) is the best-documented example. The industrial builders of the American vaccine industry were embedded in this world. Frederick Taylor Gates, who directed Rockefeller philanthropic funding into the Rockefeller Institute where Flexner conducted the 1910–1916 monkey passages, was a Baptist minister who described medical research in explicitly missionary terms. The Mulford, Parke Davis, Wyeth, and Lederle firms were Anglo-Protestant industrial operations. What linked them was not shared religion but shared intellectual atmosphere: the hermetic-alchemical conviction that the human being is material to be improved through technical operation, and that the technicians conducting the operation stand outside the moral rules that apply to the operated-upon.
Michael Hoffman, in Secret Societies and Psychological Warfare, argues that modern medical practice — the injection of animal cells into the brain, the transplantation of pig organs into humans, the fetal-cell-cultured pharmaceuticals — is the industrial-scale completion of this ancient project. He calls the resulting creature the hunimal: the human-animal hybrid produced by the operation. The individual doctor does not know this. The individual mother in Camden did not know it. Nor did the chemist Albert C. Barnes at Mulford. Knowledge of the design was not a requirement for the design to be executed. The design proceeded by generations of technical improvement on a substrate — the calf, the horse, the monkey, the aborted human being — that was always the same substrate.
Whether one accepts Hoffman’s specific framework — that the operation is hermetic-alchemical in origin, that its trajectory is intentional across centuries, that the industrial infrastructure of modern medicine is the material completion of a magical program — the correspondence exists on its own. The mechanics of the practice map, point for point, onto the mechanics of an operation that older traditions considered forbidden. The forbidden operation was the mixture of the human being with animal substance for the purpose of transforming what the human being was. The older tradition understood this as a fundamental violation of the created order — the crossing of a line that God had placed between kinds.
The Book of Leviticus contains numerous injunctions against the mixture of substances: two kinds of seed in one field, two kinds of thread in one garment, animal blood consumed with meat. These injunctions were categorical. They were not explained. They were held to reflect a structural feature of creation — that the kinds were distinct, that the blood belonged to the animal, that the human being was not to be mixed with what was not human. The injection of foreign animal substance into the human bloodstream is, by the terms of this older understanding, the exact operation the older tradition forbade.
The vaccine industry did not invent this. It industrialised it. What was performed in one temple with one calf on one day of the year became a schedule administered to every child in every country over a lifetime of appointments. The scale is new. The operation is not.
The photograph exists. The children’s names exist. The package inserts exist. What remains is the recognition of what the practice is at its root. It is not medicine that has gone wrong. It is an operation that was never medicine. It was, from the strapped calf onward, a ceremony that took its substance from the wounds of animals and placed that substance into the flesh of the healthy in the name of protection, while producing — generation by generation — the transformation of the recipient into something the operator had made.
The word for this operation, in every tradition that has a word for it, is the same word. The tradition that gave the modern West its ethical vocabulary — the biblical tradition — called the operation an abomination, and the being produced by it, an unclean thing. The hermetic-alchemical tradition, working in the opposite direction, called the operation the Great Work and the being produced by it, the artificial man. The two traditions agree on what is happening. They disagree on whether it is good.
The vaccine is the substance of the Great Work, industrialised. The vaccinated body is the vessel of the operation. The generations that have received the material — from Bessie Baker to the child in the pediatrician’s office this afternoon — are the material upon which the operation was performed.
Truth Be Told: I’ve Accepted an Invitation to Speak on The Unvaccinated
On September 17th, I’ll be giving a one-hour presentation titled The Unvaccinated as part of a six-hour livestream called Truth Be Told. This is the first time I have accepted an invitation to an event, and I have been honoured with the opening act. The livestream begins at 12pm EST.
Vaccination is the subject closest to my heart, and this is another opportunity to spread the word. The format will preserve the pen name.
Jamie Andrews (Decentralized Science Projects) and Agent131711 (Dinosaurs) will also be presenting. Jamie’s Virology Control Studies work led to an interview here last year. Agent’s research shaped my essays on vitamin D and dinosaurs. Tickets are here. The code UNBEKOMING is $5 off and applies automatically at that link. Replay available afterwards. Hope you can make it.
Primary Historical Sources
Bayly, M. Beddow. “Inoculation Dangers to Travellers.” Speech at Caxton Hall Westminster, October 2, 1952. Published by the London and Provincial Anti-Vivisection Society.
Bowen, John T. “Acute Infectious Pemphigus in a Butcher, During an Epizotic of Foot and Mouth Disease, with a Consideration of the Possible Relationship of the Two Affections.” Journal of Cutaneous Diseases Including Syphilis, vol. XXII, no. 6, June 1904, pp. 254–264.
Mohler, John R., and Milton J. Rosenau. “The Origin of the Recent Outbreak of Foot-and-Mouth Disease in the United States.” US Department of Agriculture, Bureau of Animal Industry, Circular 147, 1909.
Salmon, D.E. “Foot-and-Mouth Disease; Warning to all Owners of Cattle, Sheep, and Swine.” US Department of Agriculture, Bureau of Animal Industry, Circular No. 38, December 1902.
United States Department of Agriculture. “Method of Slaughtering and Burying Cattle.” Yearbook of the United States Department of Agriculture, 1915, pp. 20–21.
St. Louis 1901 Diphtheria Antitoxin Incident
“1901 Diphtheria Antitoxin Contamination Incident.” Wikipedia, May 4, 2026, en.wikipedia.org/wiki/1901_diphtheria_antitoxin_contamination_incident.
Wellcome Collection. “Jim, the Horse of Death.” wellcomecollection.org/stories/jim–the-horse-of-death.
Camden 1901 Smallpox Vaccine Incident
Dixon, Mark E. “Why Nine Camden Children Died from Smallpox Vaccines in 1901.” Mainline Today, September 2016.
“Why Nine Camden Children Died from Smallpox Vaccines in 1901.” Slate, February 9, 2021, slate.com/technology/2021/02/smallpox-vaccine-innoculation-history-19th-century-virus-squads.html.
Lübeck 1930 BCG Disaster
Donald, Peter R., et al. “Pathogenesis of Tuberculosis: The 1930 Lübeck Disaster Revisited.” European Respiratory Review, vol. 31, no. 164, June 28, 2022, article 220046.
Nakayama, Don K. “A Novel Microbe, Immunization Deaths, and Vaccination on Trial: BCG and the Lübeck Disaster of 1930.” SAGE Open Nursing, vol. 11, 2025, article 23779608251313994.
“Lübeck Disaster.” Wikipedia, September 27, 2025, en.wikipedia.org/wiki/Lübeck_disaster.
1916 Polio Outbreak
Wyatt, H.V. “The 1916 Poliomyelitis Epidemic and the Rockefeller Institute.” History and Philosophy of the Life Sciences, vol. 33, no. 1, 2011, pp. 95–110.
Polio Vaccination and SV-40
Cutrone, Rochelle, et al. “Some Oral Poliovirus Vaccines Were Contaminated with Infectious SV40 After 1961.” Cancer Research, vol. 65, no. 22, November 15, 2005, pp. 10273–10279.
Carbone, Michele, et al. “Simian Virus 40 Transformation, Malignant Mesothelioma and Brain Tumors.” Expert Review of Respiratory Medicine, vol. 5, October 2011, pp. 683–697.
Kops, Stanley. “Re: Debate on the Link Between SV40 and Human Cancer Continues.” Journal of the National Cancer Institute, vol. 94, no. 3, February 6, 2002, pp. 229–230.
Cutter Incident 1955
“Historical Vaccine-Associated Incidents.” History of Vaccines, historyofvaccines.org/blog/historical-vaccine-associated-incidents.
Richet and Anaphylaxis
Richet, Charles. Anaphylaxis. University Press, 1913. (Nobel Prize in Physiology or Medicine, 1913.)
Current Vaccine Excipients
Centers for Disease Control and Prevention. “Vaccine Excipient Summary — Appendix B.” CDC Pink Book, cdc.gov/pinkbook/hcp/table-of-contents/appendix-b-vaccines.html.
Food and Drug Administration. Package Inserts for Currently Licensed US Vaccines. FDA, fda.gov.
Gatti and Montanari Research
Gatti, Antonietta M., and Stefania Montanari. “New Quality-Control Investigations on Vaccines: Micro- and Nanocontamination.” International Journal of Vaccines and Vaccination, vol. 4, no. 1, 2017, pp. 00072.
Historical Analysis and Background
Humphries, Suzanne, and Roman Bystrianyk. Dissolving Illusions: Disease, Vaccines, and the Forgotten History. Create Space Independent Publishing Platform, 2013.
Willrich, Michael. Pox: An American History. Penguin Press, 2011.
The Hermetic-Alchemical Tradition and Modern Medicine
Hoffman, Michael. Secret Societies and Psychological Warfare. Independent History and Research, 2018.
Yates, Frances A. Giordano Bruno and the Hermetic Tradition. University of Chicago Press, 1964.
Yates, Frances A. The Rosicrucian Enlightenment. Routledge and Kegan Paul, 1972.
Yates, Frances A. The Occult Philosophy in the Elizabethan Age. Routledge and Kegan Paul, 1979.
Scholem, Gershom. On the Kabbalah and its Symbolism. Translated by Ralph Manheim, Schocken Books, 1965.
Idel, Moshe. Golem: Jewish Magical and Mystical Traditions on the Artificial Anthropoid. State University of New York Press, 1990.
Brown, E. Richard. Rockefeller Medicine Men: Medicine and Capitalism in America. University of California Press, 1979.
Robbins, Alexandra. Secrets of the Tomb: Skull and Bones, the Ivy League, and the Hidden Paths of Power. Little, Brown and Company, 2002.
For over a century, remarkable therapies have been suppressed to maintain a medical monopoly at the expense of humanity
A Midwestern Doctor | The Forgotten Side of Medicine | August 6, 2026
Story at a Glance:
Modern medicine is built around costly, narrowly approved drugs that treat (but rarely cure) specific disease franchises, with regulatory approval correlating more strongly with money spent than with real therapeutic value.
To enforce this, for over a century the same institutions, backed by vast fortunes, have repeatedly sidelined broader or cheaper therapies that threatened those franchises.
The same playbook is used again and again—once a therapy threatens a market, claims of “no evidence” or doctored research amplified by the media will allow regulators to clamp down on the “dangerous and unproven” therapy until it becomes forgotten to history.
In this article, I will illustrate how the exact same playbook was used again and again on numerous transformative medical discoveries endorsed by leading physicians of the era, resulting in nearly every one (e.g., UVBI and numerous cancer treatments) becoming largely forgotten despite immense evidence behind them.
This same playbook was used throughout COVID-19 to eliminate the off-patent therapies that threatened the boondoggle. One of these, chlorine dioxide, was not only repeatedly shown to eliminate COVID outbreaks, but also to do the same with malaria, where it likewise was banned.
Pierre Kory and Jenna McCarthy’s recent book The War on Chlorine Dioxide provides a critical body of evidence that chlorine dioxide has treated a myriad of challenging conditions, and that each time it did, a robust censorship apparatus erased those discoveries and retaliated against the discovers—providing a poignant illustration of the medical monopoly in action.
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.
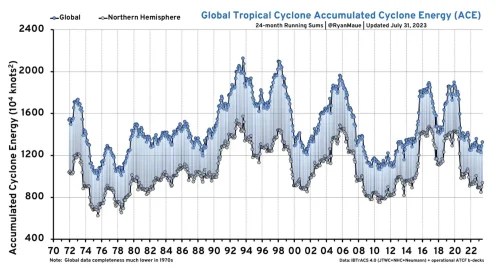


 Modern medicine is built around costly, narrowly approved drugs that treat (but rarely cure) specific disease franchises, with regulatory approval correlating more strongly with money spent than with real therapeutic value.
Modern medicine is built around costly, narrowly approved drugs that treat (but rarely cure) specific disease franchises, with regulatory approval correlating more strongly with money spent than with real therapeutic value.