Germany’s online Report24has an article titled: “Studies Show Gigantic Wind Farms Significantly Warm the Night”.
Proponents of the energy transition often ignore or conceal the negative local climate impacts of wind turbines. Report24 references a 2012 study published in Nature Climate Change by Liming Zhou and his research team, which investigated the impact of large wind farms on land surface temperatures in Texas.
Researchers analyzed satellite data from 2003 to 2011 covering an area in Texas that hosts four of the world’s largest wind farms. In the areas with wind farms, nighttime surface temperatures in summer increased by up to 0.65 °C more than in comparable areas without turbines. The calculated warming trend was up to 0.72 °C per decade.
Why do turbines cause warming? At night, the ground cools down, making the air near the surface colder than the layers above. The turbine rotors disrupt this natural stratification, mixing the layers and forcing warmer air down to the surface, which warms and dries out the ground. Germany is plastered with circa 30,000 turbines spread across the country. In addition to the growing urban heat island (UHI) effect, Germany’s local climate is being disrupted by its widespeard use on wind turbines.
Politicians and mainstream media have been deliberately ignoring these facts since 2012. The local warming caused by wind farms is falsely blamed on CO₂-driven climate change in order to maintain the narrative of “saving the climate.”
Also, deforestation is underway in Germany in order to clear the way for largescale windparks, severely damaging a natural ecosystem that acts to cool the local climate.
A recent article in the online journal Futurism, titled, “Scientists Horrified as Huge Heatwave Hits Antarctica,” claims climate change caused a “huge heatwave” in Antarctica, bringing temperatures on the Antarctic Peninsula nearly 36°F above average and briefly pushing readings above freezing. This is highly misleading. A single weather event says nothing meaningful about long-term climate trends, and the article ignores both Antarctica’s enormous geographic variability and the exceptionally cold conditions simultaneously occurring elsewhere on the continent. The heatwave Futurism suggested wasn’t a continent-wide crisis, but was a localized, unalarming event.
The article is largely a rewrite of a Guardian story focused on temperatures measured on the Trinity Peninsula, the northernmost extension of Antarctica. Researchers reported temperatures reaching approximately 15.4°C (59.7°F) during a brief warm spell on June 6.
What readers are not told is that the Antarctic Peninsula is not representative of Antarctica as a whole.
In fact, the warmest part of Antarctica is the Antarctic Peninsula. Nicknamed the “banana belt,” it stretches northward toward South America and experiences milder maritime conditions. During the austral summer, temperatures can occasionally exceed 10°C (50°F). The peninsula extends northward toward South America and is heavily influenced by maritime weather patterns and ocean currents. It is by far the warmest part of Antarctica and has long experienced periodic warm-air intrusions, föhn wind events, rain episodes, and above-freezing temperatures. These events are unusual, but they are not unprecedented.
In fact, the article itself acknowledges that the warmth was associated with “extremely strong westerlies.” In other words, this was a weather event driven by warmer atmospheric circulation patterns, not a direct measurement of climate change.
Climate is measured over decades. A single day, a single week, or even a single season tells us very little about long-term temperature trends. If every unusually warm day is presented as proof of climate catastrophe, then intellectual consistency would require every unusually cold day to be presented as evidence against it. The media rarely applies that standard.
According to observations highlighted by meteorologist Cap Allon, the Amundsen-Scott South Pole Station recorded a temperature of -73.6°C (-100.5°F) on June 16, with a daily maximum of only -69.9°C (-93.8°F). That was the South Pole’s first sub–70°C reading since 2023.
One part of Antarctica briefly experiences an unusual warm episode, while another part of the continent drops below -100°F. That is how weather works on a continent larger than the United States and Mexico combined.
Yet only one of those events, specifically the anomalous high temperature one, generated international headlines.
The article further claims that the heatwave follows “decades of increasingly warm temperatures observed on the white continent.” That statement is false.
Antarctica is not warming uniformly. While portions of the Antarctic Peninsula experienced warming during parts of the late twentieth century, numerous studies have shown little warming or even cooling across large sections of East Antarctica, with East Antarctica making up the bulk of the continent. Antarctic sea ice has also exhibited substantial variability from year to year and decade to decade.
The continent is governed by complex interactions involving ocean currents, atmospheric circulation, volcanic influences (including subsurface heating under West Antarctica where the peninsula lies), sea ice dynamics, and natural climate oscillations. That complexity disappears in Futurism’s opinionated article.
Instead, readers are given the now-familiar formula: identify a dramatic weather event, attach it to climate change, mention the “Doomsday Glacier,” and imply catastrophe is around the corner. Climate Realism has debunked claims of the Thwaites Glacier’s imminent collapse repeatedly, previously. The article’s reference to Thwaites Glacier is a particularly misleading red herring, because it has nothing to do with the reported weather event. The mention serves one purpose: reinforcing a broader climate crisis narrative.
This is increasingly common in climate reporting. Any unusual weather event becomes an opportunity to recycle the same talking points about glaciers, sea level rise, tipping points, and future disasters, regardless of whether they are directly related to the event being discussed.
Concerning the Antarctic Peninsula, the facts are these: Antarctica has always been susceptible to periodic warm-air intrusions because of its geography and proximity to relatively warmer ocean waters; the Southern Ocean, atmospheric rivers, and strong westerly winds can occasionally transport substantial heat into the region. These processes existed long before climate change became a political issue.
Most importantly, a single warm event cannot establish a trend. Scientists understand this principle when analyzing climate data. Journalists should understand it as well.
A proper climate analysis requires decades of observations across the continent, careful examination of regional variability, and separation of weather noise from climate signals, not the slap dash presentation of misleading, sensational claims assembled by Futurism.
Antarctica remains the coldest continent on Earth. While the Antarctic Peninsula briefly experienced unusually mild conditions, the South Pole itself was simultaneously plunging near or below -100°F in multiple other locations.
That fact alone should remind readers that one weather event, no matter how dramatic the headline, is not evidence of a “climate emergency,” it’s simply weather. One warm spell on the Antarctic Peninsula becomes proof of climate catastrophe, while simultaneous temperatures below -100°F at the South Pole are ignored. That’s not objective journalism, that’s agenda-driven alarmism.
In 1943, the U.S. military was about to armor its bombers in exactly the wrong places. The analysts had examined every bomber that came back from combat, mapped the bullet holes across the airframe, and proposed reinforcing the spots where the holes clustered. The data was right there. You could see it on the planes.
They referred the question to the Statistical Research Group at Columbia University, a small team of mathematicians assembled for the war effort. The Hungarian-born statistician Abraham Wald examined the bullet-hole maps and gave the opposite recommendation. Armor the engines and the cockpit. The places where the returning planes had no bullet holes.
The military analysts had committed a logical error so simple they could not see it. They were studying the planes that came back. The planes shot through the engines and the cockpit did not come back. They had gone down across two oceans and the territory between them. The returning planes did not reveal where bombers were vulnerable. They revealed where bombers could be hit and still fly home.
The bullet holes on the survivors mapped survivable damage, not dangerous damage. Armoring where the holes were meant armoring the places that did not need armoring. The damage that mattered was on the planes you could not examine because they were destroyed.
Wald’s memorandum was classified. Decades later, when his work was declassified and republished, the principle he had identified came to be called survivorship bias.¹ ² It is the most pervasive and least understood logical error in any field that draws conclusions from a visible population of survivors.
The same error sits at the center of the modern screening-and-treatment industry.
The Error Generalized
Survivorship bias operates wherever a process selects what gets seen. The destroyed do not file reports, and the audience reads only what made it through.
Mutual fund performance averages exclude funds that closed. Hedge fund return statistics quietly drop the funds that liquidated. The historical returns of “the market” routinely omit bankruptcies, delistings, and total losses. Funds that lived publish their numbers; funds that died publish nothing. The retail investor reads the winners.
The literature on entrepreneurship was built the same way. CEOs who succeeded wrote memoirs about their habits and their early-morning routines. The thousands of equally disciplined founders who failed wrote nothing because their companies went under. The “success habits” identified by reading the survivors are, in many cases, just habits, shared by the dead and the living alike, with no causal relationship to outcomes.
In architecture, the buildings that survive are studied for their construction methods. The buildings that collapsed in storms, earthquakes, or fires are no longer there to be examined. Old buildings appear well-built because the badly-built ones are gone.
In each case, the visible sample is selected by the very property you are trying to measure. You cannot learn about plane vulnerability from intact planes. You cannot learn about cancer survival from cancer survivors.
Survivorship Bias in Medicine
A woman undergoes mammography in her early fifties. The scan finds a small lesion. She receives a biopsy, a lumpectomy, six weeks of radiation, and five years of tamoxifen. She is alive ten years later. She becomes an advocate, walking in Race for the Cure and telling her sister, her daughter, and the women in her neighborhood that screening saved her life. Get the test.
Her experience is real, her gratitude genuine. The conclusion she draws does not follow from either.
What she does not know, what she cannot know, is what would have happened to her without the screening, the biopsy, the surgery, the radiation, and the years of medication. She cannot run the counterfactual on herself. The version of her that did not get the treatment does not exist, and she has no way to consult it.
The institutions that promoted her screening have access to data she does not. Population-level data, accumulated across decades of randomized and observational studies, is consistent with four overlapping forms of survivorship bias, each of which inflates the apparent success of the system. Together they are sufficient to explain most of what the industry presents as the triumph of “early detection.”
Survivorship Bias Proper
The most direct form: only the living testify.
Eight months after her mastectomy, a woman dies of chemotherapy-induced sepsis. She does not appear at the October fundraiser. Six weeks after his prostatectomy, a man dies of cardiac complications. He writes no op-eds about prostate health. The radiation that “cured” the first cancer induces a second one five years later, and the patient’s family attends a funeral, not a marathon. The chemotherapy regimen that ostensibly drove the tumor into remission also drove the patient’s bone marrow into failure, and she dies of sepsis a year later, recorded by quiet bureaucratic convention as a “cancer death.”
When the public hears about cancer treatment, it hears from the patients who survived. Those who did not survive are statistically invisible. They are counted in mortality columns nobody reads, while their grateful surviving counterparts address the television cameras. The audience for screening campaigns sees a heavily filtered population, filtered by the treatments themselves.
The filtering goes further than visibility. It reaches into the mortality data itself. When a patient on chemotherapy dies of cardiotoxic heart failure, the death is typically coded as a cancer death. When a patient with treatment-induced bone marrow failure dies of sepsis, it is coded as a cancer death. When the surgical complication kills the patient on the operating table, it is generally coded as a cancer death. When the second cancer induced by radiation given for the first cancer kills the patient ten years later, the second cancer is frequently recorded as primary, the radiation that caused it noted in passing if at all. The coding conventions tilt systematically in one direction: failures of treatment are folded back into the column labeled “disease.” The treatment is shielded from blame. The cancer absorbs it. The mortality statistics that institutions cite to justify aggressive treatment are themselves an artifact of how treatment failures are recorded.
Lead-Time Bias
Finding a cancer earlier does not mean treating it earlier extends life. It means knowing about it longer.
Two women with identical lesions, identical biology, and identical eventual outcomes. Both die at age seventy. Woman A is screened at fifty, her cancer is detected, and she is “treated” for the next twenty years. Woman B is unscreened. She develops symptoms at sixty-five, is diagnosed, and dies at seventy.
The standard reporting metric is five-year survival from diagnosis. By that measure, Woman A counts at 100% survival. Woman B counts at 0%. The treatment looks miraculous. Nothing has actually changed. Both women died at seventy. Woman A simply spent twenty years as a patient.
The five-year survival statistic is the standard currency of cancer reporting. In the presence of widespread screening, it is also a metric that can rise to 100% without saving a single life. Between 1950 and 1995, the five-year survival rate for prostate cancer in the United States rose from 43% to 93%. The age-adjusted mortality rate from prostate cancer over the same period barely moved.³ The screened population learned about their cancer earlier. They did not die later.
When you read that “early detection” has improved five-year survival rates for breast, prostate, or thyroid cancer, you are reading a statistic structurally biased toward the appearance of benefit even when no benefit exists.³ ⁴
Length-Time Bias
Screening preferentially detects slow-growing lesions. Aggressive cancers grow rapidly between screening intervals and present symptomatically, not through the scan. Indolent lesions sit for years, available to be detected at the next mammogram or PSA test.
The population of cancers caught by screening is therefore enriched for slow biology, for lesions that were less likely to kill in the first place. Patients with these lesions tend to do well, not because the screening saved them but because their cancers were not going to kill them on any rapid timescale. The aggressive cancers, the ones that genuinely threaten life, frequently arise and progress in the gaps between scans.
Screening catches the cancers least in need of catching. The system then takes credit for the favorable outcomes of patients who would have done well regardless.
Overdiagnosis
The fourth and most powerful form. Many of the lesions detected by screening are not, in any meaningful sense, going to harm the patient. They are stable, non-progressive anatomical findings that medicine has chosen to label as cancer.
Bleyer and Welch, examining three decades of U.S. mammography data, estimated that 31% of breast cancers detected by screening represented overdiagnosis: disease that would never have produced symptoms or shortened life.⁵ The Cochrane systematic review of mammography trials concluded that for every life potentially saved by screening, ten women receive treatment for a cancer that would not have harmed them. The same review found no reduction in all-cause mortality from screening.⁶
In South Korea, the introduction of widespread thyroid ultrasound produced a fifteen-fold increase in thyroid cancer diagnoses over two decades. Mortality from thyroid cancer did not change. The country had not experienced a thyroid cancer epidemic. It had begun finding microscopic lesions that had always existed in the population, at autopsy in people who died of other causes, and that had never killed anyone before they were found and treated.⁷
Autopsy studies of men who died of unrelated causes have found prostate cancer cells in roughly a third of those in their forties, rising to two-thirds by their late sixties.¹⁵ The lifetime mortality from prostate cancer is approximately 3%. Most older men carry the disease into a natural death from something else; they die with prostate cancer, not from it. The PSA test cannot distinguish between the cancer that would have killed and the cancer that would have been silently carried into the grave. It detects both. It produces a diagnosis in both. The men with non-threatening lesions, who vastly outnumber the rest, are subjected to surgery, radiation, and hormonal therapy for a condition that was never going to harm them. They survive what was never threatening. They credit the system. They tell other men to get tested.
The ERSPC trial, the largest prostate cancer screening trial ever conducted, found that PSA screening reduced prostate cancer mortality by a small absolute amount over thirteen years. To prevent one death, approximately twenty-seven men had to be diagnosed and treated, most of whom would not have died from their disease and many of whom were rendered incontinent, impotent, or both by the intervention.⁸
Every overdiagnosed patient is, by definition, a successful “treatment outcome.” She survived a treatment for a condition that was never going to harm her. The system takes credit. She testifies on its behalf.
Why the System Selects for Evangelism
The four biases would matter less if the visible patients were a representative sample. They are not. The system that produces them also amplifies them.
Hospitals run survivor outreach programs. Pharmaceutical companies fund patient advocacy organizations. The pink ribbon ecology, Susan G. Komen, the National Breast Cancer Foundation, the dozens of subsidiary charities, operates almost entirely on survivor testimony. October fills American mailboxes with pink-ribboned testimonials. The American Cancer Society’s national publicity is built on survivor stories. The patient who survived is the asset.
The corporate machinery built around the survivor is substantial. Estée Lauder co-founded the pink ribbon symbol with Self magazine in 1992 and now sells pink-ribbon cosmetics each October. The National Football League runs an annual “Crucial Catch” campaign with players wearing pink cleats and accessories. Major League Baseball stages pink-bat games on Mother’s Day. Yoplait produced pink-lidded yogurt for two decades under the “Save Lids to Save Lives” campaign. Ford sold pink-ribbon merchandise through “Warriors in Pink.” General Mills, KitchenAid, the National Hockey League, the airlines, the cosmetics counters at every major department store all participate. The advertising spend on these campaigns runs into hundreds of millions of dollars annually, dwarfing the portion of the proceeds that ever reaches research and dwarfing many times over the portion of research funding that addresses environmental causes of breast cancer rather than treatment. The campaigns sell screening. The screening produces patients. Most patients survive, because most of what is found in screening was not going to kill them, and they testify. The testimony funds the next round of campaigns.
The patient who died is, from a marketing perspective, a problem. Her death cannot be celebrated. Her family is often grieving and angry. Her doctors generally do not call the local newspaper. She becomes a statistic in a column nobody reads, while the surviving patient in the next room becomes the face of the cause.
This selection is not a conspiracy. It is a structural feature of how the industry communicates. Living patients can be photographed; dead patients cannot. The living speak at events; the dead are credited, by quiet convention, to “the disease.”
The grateful survivor is also psychologically necessary for the treatment to continue being offered in its current form. The patient who has undergone radical mastectomy, six rounds of chemotherapy, weeks of radiation, and years of endocrine therapy must believe, on pain of intolerable cognitive dissonance, that this was necessary and life-saving. To accept that she may have been treated for a lesion that would not have harmed her, that she lost her breast, her hair, her fertility, her cardiac reserve, perhaps her marriage, to a system that misjudged the threat, is psychologically devastating. The mind protects itself. She becomes an advocate.
The advocate then promotes the system to other women, who undergo screening, get diagnosed, get treated, and become advocates in turn. Each cycle generates more survivors, each of whom credits the system that produced them. The dead and the harmed are silent by definition.
The financial scale of this ecosystem is not small. The United States spends roughly two hundred billion dollars annually on cancer-related medical care. Mammography alone is a multi-billion-dollar industry. The PSA test, despite repeated expert task force recommendations against routine screening, generates billions in downstream procedures. The pink ribbon charities raise hundreds of millions per year, much of which goes to “awareness,” that is, to producing more screening, more diagnoses, more treatment, and more survivors. The asset class, the patient, is manufactured by the process that then takes credit for her survival.
In 2018, a Goldman Sachs equity research report posed the question explicitly to its biotechnology clients: “Is curing patients a sustainable business model?”⁹ The analysts noted that one-time cures undermine recurring revenue streams. The pharmaceutical industry’s most profitable customers are chronic patients, not cured ones. The screening-and-treatment cancer model is, from a financial perspective, an excellent business. It produces patients. It treats them for years. Many of them survive, which is what the model needs them to do, because survivors testify and dead patients do not.
Inside the Testimonial
The cancer survivor has four pieces of information. She was screened. Something was found. She received treatment. She is alive years later. From these facts, she draws a single conclusion: the screening and treatment saved her life.
The inference is intuitive but unsupported. The same four facts admit at least three other explanations.
The screening detected a lesion that would never have harmed her. She survived not because of the treatment but in spite of it. The treatment did damage that she absorbed because the rest of her body was healthy enough to recover.
The lesion was real but slow-growing. She would have lived equally long, with less suffering, by doing nothing.
The lesion was real and biologically active, but her body’s repair mechanisms, what the establishment calls her constitution and what terrain medicine recognizes as her terrain, would have managed it. The treatment was incidental to her survival.
She cannot distinguish between these explanations from her own experience. None of them is available to her introspectively. The only way to determine which is correct, at the level of a population, is the randomized controlled trial, the kind of trial that, in most screening contexts, has either not been done with adequate follow-up or has produced equivocal results that the institutions promoting screening do not publicize.
Her testimonial is sincere. It is also, with respect to the question of whether the treatment worked, evidence of nothing in particular. The dead woman two beds down the hall, who received identical screening and identical treatment and died of cardiotoxic chemotherapy, would have a different testimonial if she could give one. The system that asks the survivor to speak does not ask the dead woman’s family to speak. The asymmetry produces the appearance of a treatment success rate the underlying data does not support.
What Survives the Error
Once you see survivorship bias, you cannot unsee it. What remains is not paranoia but a discipline: asking, in every medical context, which population you are looking at and which population is missing.
When a screening campaign reports that “five-year survival rates have improved,” ask whether overall mortality has changed. Five-year survival can rise to 100% without saving a single life if all the increase comes from earlier detection of lesions that were going to be survived anyway. Overall mortality, deaths per hundred thousand population per year, is much harder to manipulate. It is also the only figure that answers the question the survival rate appears to answer.
A cancer survivor telling you her treatment saved her life can be sincere and still wrong about causation. The conviction is real. The causal claim it carries is not derived from anything she has direct access to. You can be glad she is alive without accepting her account of why.
An oncology center’s published survivor outcomes report a filtered population. Ask about the patients who did not complete treatment. Ask about the patients who died of treatment-related complications and were classified as cancer deaths. Ask about the patients whose follow-up was lost because they moved into hospice care or stopped responding to calls. The shape of the population that gets reported is the shape of the population that survived long enough to be counted.
Facing a screening recommendation yourself, the question to ask is the one the military analysts in 1943 did not ask: what does this examination fail to show me? The bullet holes on the surviving bombers concealed the bullet holes on the destroyed ones. The success stories of the screening industry conceal the women treated for lesions they did not have, the men rendered impotent by surgery for cancers that would never have grown, the second cancers induced by the radiation, and the patients whose treatments killed them and who are now counted, by quiet bureaucratic convention, as having died from their disease.
The full investigative case on these screenings, what they detect, what they miss, what they manufacture, and what they cost, has been documented at length in earlier work.¹⁰ ¹¹ ¹² ¹³ ¹⁴
What the Trials Actually Show
Defenders of mammography routinely cite two trials. The Health Insurance Plan of New York trial, begun in 1963, and the Swedish Two-County Trial, conducted between 1977 and 1985, both reported reductions in breast cancer mortality among screened women. Both have been criticized on methodological grounds. The HIP trial’s randomization was uneven, with baseline differences between arms and exclusion rules applied asymmetrically. The Two-County Trial used cluster randomization that did not consistently balance comparison groups and lacked blinded cause-of-death assessment. Its mortality estimates shifted across successive reanalyses. The Cochrane systematic review of mammography trials classified both as carrying significant risk of bias.⁶
The most rigorously conducted breast cancer screening trial, the Canadian National Breast Screening Study, followed nearly ninety thousand women for twenty-five years. It found no reduction in breast cancer mortality from mammography screening, and no reduction in all-cause mortality.¹⁶
All-cause mortality is the figure that resists the gaming. When a study reports that breast cancer deaths fell among screened women but all-cause deaths did not, the women who avoided a death coded as breast cancer died of something else within the same window: heart failure from chemotherapy-induced cardiotoxicity, second cancers induced by the radiation given for the first, complications from the surgery, strokes after years of endocrine therapy. The Cochrane review and meta-analyses across multiple cancers have repeatedly found that all-cause mortality is essentially identical in screened and unscreened populations. The treatment that prevents one death produces another. The cancer-specific column improves; the death column does not. Survivorship bias gives the illusion of a saved life. All-cause mortality data shows that the life, where treatment did anything at all, was traded rather than added.
The Bombers and the Patients
Abraham Wald died in 1950 in a plane crash in the Nilgiri mountains of southern India. The principle he identified outlived him by three-quarters of a century and now sits, unrecognized by the institutions that depend on it, at the center of the modern medical industry.
The bombers that came back showed where a bomber could be shot and still come back. They did not show where a bomber was vulnerable. The cancer survivors who give interviews, walk in fundraisers, and tell their friends to get screened show where the modern oncology machine is not lethal. They do not show where it works.
The patients who died of their treatments are not at the marathon. The patients treated for lesions that would never have killed them have no way to know they were never in danger. The patients whose cancers were going to be survived regardless have no way to credit their own bodies rather than the chemicals introduced into them. They are the bullet holes on the wings: survivable damage, mapped and celebrated, while the damage that mattered remains invisible because the people who suffered it are no longer in the room.
Wald told the military to armor the engines and the cockpit, the places the surviving planes were not hit. The same instruction applies to medicine: look at what the survivors do not show you. The damage that matters is on the planes that did not come back, and on the patients who can no longer testify.
How to Explain This to a Six-Year-Old
Imagine all your friends drink a magic potion that’s supposed to keep them safe. Half of them disappear. The other half come back and tell you the potion worked great.
If you only listen to the friends who came back, you’ll be sure the potion is wonderful. You’ll tell other kids to drink it too.
But the other half are gone. They can’t tell you whether the potion hurt them. You don’t know whether the potion saved the friends who came back, or whether those friends would have been fine without ever drinking it.
When a cancer survivor tells you the treatment saved her life, listen to her kindly. But remember the friends who disappeared. They are part of the story too.
Quick Reference: The Four Biases
Survivorship bias. Only the living testify. Cancer patients who died of their treatments do not give interviews. The visible patient population is filtered by the treatments themselves.
Lead-time bias. Finding a cancer earlier does not extend life. It extends the time you know about it. Five-year survival rates can rise to 100% without saving a single life.
Length-time bias. Screening preferentially catches slow-growing lesions that were less likely to kill in the first place. Aggressive cancers arise and progress between scans, often undetected until they present symptomatically.
Overdiagnosis. Many screen-detected lesions would never have caused harm. The patient is treated for something that was not a threat, survives easily, and credits the treatment.
References
Mangel, M., & Samaniego, F. J. (1984). Abraham Wald’s work on aircraft survivability. Journal of the American Statistical Association, 79(386), 259–267.
Wald, A. (1943). A Method of Estimating Plane Vulnerability Based on Damage of Survivors. Statistical Research Group, Columbia University. (Declassified and republished by the Center for Naval Analyses, 1980.)
Welch, H. G., Schwartz, L. M., & Woloshin, S. (2000). Are increasing 5-year survival rates evidence of success against cancer? JAMA, 283(22), 2975–2978.
Welch, H. G., & Black, W. C. (2010). Overdiagnosis in cancer. Journal of the National Cancer Institute, 102(9), 605–613.
Bleyer, A., & Welch, H. G. (2012). Effect of three decades of screening mammography on breast-cancer incidence. New England Journal of Medicine, 367(21), 1998–2005.
Gøtzsche, P. C., & Jørgensen, K. J. (2013). Screening for breast cancer with mammography. Cochrane Database of Systematic Reviews, Issue 6, CD001877.
Vaccarella, S., Franceschi, S., Bray, F., Wild, C. P., Plummer, M., & Dal Maso, L. (2016). Worldwide thyroid-cancer epidemic? The increasing impact of overdiagnosis. New England Journal of Medicine, 375(7), 614–617.
Schröder, F. H., et al. (2014). Screening and prostate-cancer mortality in a randomized European study: results of the ERSPC at 13 years of follow-up. The Lancet, 384(9959), 2027–2035.
Richter, S., et al. (2018). The Genome Revolution (biotechnology equity research report). Goldman Sachs Global Investment Research, April 10, 2018.
Unbekoming. The 12 Screenings That Manufacture the Patients They Claim to Find.
Unbekoming. The Screening Trap.
Unbekoming. Breast Cancer: What They Didn’t Tell You.
Unbekoming. The PSA Trap: How a Flawed Test Built a Billion-Dollar Industry and Destroyed Millions of Men.
Unbekoming. The Unbekoming Cancer Compendium.
Sakr, W. A., Grignon, D. J., Crissman, J. D., Heilbrun, L. K., Cassin, B. J., Pontes, J. J., & Haas, G. P. (1994). High grade prostatic intraepithelial neoplasia (HGPIN) and prostatic adenocarcinoma between the ages of 20-69: an autopsy study of 249 cases. In Vivo, 8(3), 439–443.
Miller, A. B., Wall, C., Baines, C. J., Sun, P., To, T., & Narod, S. A. (2014). Twenty five year follow-up for breast cancer incidence and mortality of the Canadian National Breast Screening Study: randomised screening trial. BMJ, 348, g366.
The book, also available on Amazon documents “systemized medical abuse” that accelerated during the COVID-19 pandemic.
Chapter 1. From Quackery To Criminality
The medicinal use of mercury offers a long-running example of medically induced harm. Although centuries of whistleblowers have warned that dosing patients with it constitutes reckless quackery—and the U.S. government presently places mercury at number three on its “Substance Priority List,” right under arsenic and lead—the heavy metal has figured prominently in the “medical armamentarium” from as far back as the sixth century BC through the present day.
In his important book Evidence of Harm, author David Kirby exposed the pharmaceutical industry’s controversial practice of including mercury preservatives in vaccines. Pointedly using the word “criminal,” Kirby wrote in the foreword to another book about mercury (The Age of Autism by Dan Olmsted and Mark Blaxill) that the “blind belief in a known poison” has been “misguided, immoral, and in some cases, patently criminal.”
The “Messianic” Benjamin Rush
In many ways, the medical practices and beliefs of U.S. Founding Father, physician, and University of Pennsylvania medical school professor Benjamin Rush may have set the stage for modern medicine’s stubborn adherence to dangerous protocols—despite clinical evidence of harm—and its silver-bullet fascination with vaccines “as substitutes for right living,” as Eleanor McBean put it in her 1957 book The Poisoned Needle: Suppressed Facts About Vaccination.
The reportedly “messianic” and “uncompromising” Rush’s late-1700s stock-in-trade was a radical protocol involving bloodletting and purging with—what else?—mercury, a practice that medical historians later dubbed “heroic medicine.” Rush had his own proprietary brand of laxative called “Thunderclappers,” consisting of approximately 60% mercury chloride (also called calomel), which he promoted as “a purgative of explosive power.” As Rush honed his clinical methods, he passed them on to a phalanx of enthusiastic students and disciples during yellow fever epidemics in Philadelphia, where he would bleed and purge up to 100 patients a day. Although use of calomel was not uncommon among doctors of that era, Rush prescribed up to 10 times more than his medical peers and also recommended the removal of huge amounts of patients’ blood, erroneously believing that the blood would replenish itself in a matter of a day or two. “A patient’s failure to respond to this disastrous therapy,” one historian wrote in 2004, “won [the patient] only another round of bleeding and purging.” In another modern writer’s colorful description, “So much blood was spilled in the front yard that the site became malodorous and buzzed with flies.”
No less a figure than George Washington underwent a rapid and gruesome death after Rush protégé Dr. Elisha Dick (and two other Johnny on-the-spot physicians) poisoned Washington with mercury and removed 40% of the beleaguered general’s total blood volume—a quantity that, to this day, “continues to amaze and appall laymen and physicians alike.” From many historians’ point of view, Washington’s doctors caused his death, a death that may well have changed the course of history.
Rush was enthusiastic about promoting his “heroic medicine” protocol, “proclaim[ing] the success of his cure to the public and his medical colleagues” in newspapers, advertisements, and brochures, and even “harangu[ing] people in the streets.” In addition, he was an early and explicit proponent of smallpox vaccination. In 1803, he joined with 30 other Philadelphia doctors in signing a public notice “expressing their confidence in vaccination and recommending it for general use.” Significantly, smallpox vaccination represented a turning point in the “medicalization of the general public” in both early nineteenth-century America and Europe, and a boon for the burgeoning medical profession:
Since the late eighteenth century, doctors had intensified their efforts to win government support for their plans to bring the whole population under medical control. . . . Thus Jenner’s method of cowpox vaccination presented medical practitioners with a new chance to increase their prestige and influence on public health affairs [bold added]. Doctors also foresaw an increase in their income through vaccination fees and hoped to establish themselves, with the help of the vaccine, among those classes of the population who had not consulted doctors before.
From 1813 to 1822, the young U.S. government appointed James Smith as the nation’s “federal vaccine agent,” charging him with “maintaining a supply of the smallpox vaccine and distributing it nationwide”; Smith had been a student of Rush’s at the University of Pennsylvania and was a fellow member of the “well-educated medical elite.” Although other physicians of the day argued that smallpox vaccination was both dangerous and ineffective, then—as now—defenders of the practice prevailed by using “more or less perverted statistics,” with one doctor urging his “professional brethren to be slow to publish fatal cases of small-pox after vaccination” and others passing off vaccine-induced fatalities as some other disease.
Reflecting on Rush’s medical legacy, U.S. Army medical officer P.M. Ashburn made remarks in 1929 that highlight one of the many reasons why Rush’s cautionary tale is still pertinent today. Ashburn wrote that by virtue of Rush’s “social and professional prominence, his position as teacher and his facile pen,” the Philadelphia physician “was more potent in propagation and long perpetuation of medical errors than any man of his day,” thereby “blacken[ing] the record of medicine.” This observation illustrates how social prestige—coupled with “unyielding devotion to dogma”—often helps practitioners of dangerous medicine beat back their critics.
In Rush’s time, those critics included fellow physician Elisha Barlett, who opined about Rush’s medical theories, “In the whole vast compass of medical literature, there cannot be found an equal number of pages containing a greater amount of utter nonsense and unqualified absurdities,” as well as feisty British journalist and pamphleteer William Cobbett, who dared to publish tracts asserting that Rush’s yellow fever treatments were both ineffective and dangerous—and “a perversion of nature’s healing powers.” In response, Rush sued Cobbett for libel and won, in “one of the largest libel awards in American history at the time.”
One of Cobbett’s fascinating observations—which reverberates uncannily in the COVID era—was that extreme fear (in this instance, of yellow fever) made members of the public far more willing to subject themselves to Rush’s “experiments” than they otherwise might have been. Cobbett wrote:
[Rush] seized, with uncommon alacrity and address, the occasion presented by the Yellow Fever, the fearful ravages of which were peculiarly calculated to dispose the minds of the panick-struck people to the tolerance, and even to the admiration, of experiments, which, at any other time, they would have rejected with disdain.
Interestingly, after Rush’s libel victory, Cobbett exacted a modicum of revenge by assembling data from municipal records (acknowledged today as “an epidemiological tour de force”), which pointed to a 56% mortality rate among Rush’s yellow fever patients that contrasted starkly with the physician’s own claim of a greater than 90% survival rate. When word of those dismal statistics got out to the public, Rush’s medical practice suffered. Undaunted, Rush went on to become Treasurer of the U.S. Mint under President John Adams. As the author of America’s first psychiatric textbook, he is also revered today as “the father of American psychiatry.” Rush proposed the same general treatments for madness that he favored for physical ailments, supplemented by straitjackets and other “modes of punishments” for tough cases.
For his part, in 1800, a disgusted Cobbett returned to London, where he continued to hold medicine’s feet to the fire, including condemning smallpox vaccination as “quackery.”
A “Patently Criminal” Model
Some modern medical historians are willing to go so far as to characterize medicine, in periods and places like 18th-century America, as “deplorable,” and to suggest that back then, “a doctor was just as likely to kill you as save you.” Most, however, frame medical barbarity as a thing of the past. Shielded by high-end machines, complex drug technologies, glossy scientific publications, and lingo like “rigorous” and “evidence-based,” the current medical-pharmaceutical-regulatory establishment and its hagiographers would have the public believe that “safe and effective” now rules the day.
There is ample evidence to show that pledges of safety often are either disingenuous or false, and there are indications that Kirby’s description of the medical model as sometimes “patently criminal” was squarely on the mark. At the level of individual medical practitioners, law firms specialized in malpractice note that if a doctor “appears to be indifferent to patients’ well-being or safety,” that indifference can be grounds for criminal liability. A search of the word “criminal” on the website of Medpage Today (a conventional news service that is generally protective of medicine’s reputation) brings up countless articles about doctors and other health care providers running “pill mill” operations, carrying out fraud, taking kickbacks, tampering with drugs, faking data, sexually assaulting or abusing patients, and engaging in other types of “unprofessional” and unethical conduct. The site’s “Investigative Roundups” feature stories (often formulated as questions to soften the impact) with titles like “Columbia protected predator doc?”, “Psychiatrist held patients against their will?”, “$15K surgery shakedown?” or “Doc pushed unneeded surgery?” Other Medpage Today headlines flamboyantly bandy about words like “deadly,” “loophole,” “games,” “tactics,” “unethical,” and “secretive.”
Sometimes, individuals who defend the medical status quo blame whichever reports of misbehavior manage to surface (many do not) on “a few bad apples.” Others, such as Harvard scientist and patient safety advocate Lucian Leape, do the reverse, shifting the blame from “bad people” to nebulous “bad systems;” Leape suggests that a cycle of disrespect is “learned, tolerated, and reinforced in the hierarchical hospital culture.” The fact is, however, that medical harms flow from both individuals and institutions. Most health care providers operate in broader organizational and corporate contexts—and it is policymakers and decision-makers at those levels who often give medical-pharmaceutical corruption and criminality a green light. This is illustrated by the phenomenon (for which there is even an academic field of study) called “clinicide,” defined as serial medical killers responsible for “the unnatural death of multiple patients in the course of treatment;” not infrequently, the killers’ host institutions countenance or “enable” this clinicide by choosing to ignore red flags.
As an extension of the “bad apples” argument, some upholders of the status quo point to the fines that the U.S. Department of Justice (DOJ) routinely levies on hospitals and pharmaceutical corporations, suggesting that these are an adequate mechanism to catch and punish players engaged in malfeasance. However, given that medical-pharmaceutical culprits not infrequently are criminal recidivists and that the fines generally amount to “little more than a slap on the wrist,” it is fair to ask “whether such a monetary punitive system really does much to prevent bad behavior.”
Moreover, DOJ rarely prosecutes or holds corporate leaders accountable, despite having a “powerful legal tool” at its disposal to go after the executives at the helm of medical misconduct; it has done so only 13 times since the year 2000. Instead, many signs point to a wink-and-a-nod sub rosa understanding between the various parties, with the penalties doing nothing to prevent future harms but instead furnishing a generous flow of kickbacks that prosecutors and regulators can funnel into various sectors of the federal budget (see Illegal But Profitable). In fact, under the False Claims Act, the U.S. Department of Health and Human Services (HHS) gets a 20 to 1 return on every dollar it “invest[s] in prosecutions and investigations.”
To our knowledge, a parent company has never been excluded from participation in Medicare and Medicaid for illegal activities, which endanger the public health and deplete taxpayer-funded programs. Criminal prosecutions of executives leading companies engaged in these illegal activities have been extremely rare. Much larger penalties and successful prosecutions of company executives that oversee systemic fraud, including jail sentences if appropriate, are necessary to deter future unlawful behavior. Otherwise, these illegal but profitable activities will continue to be part of companies’ business model.
Iatrogenocide Takes Center Stage
Even before COVID, available data indicated that 20th- and 21st-century Western medicine had failed to improve health in any meaningful way, instead trading off the industrial-age diseases of yore for modern chronic disease epidemics, many or most with iatrogenic causes or contributors. Unfortunately, recent events suggest that medicine—forging an unhealthy partnership with government—may now be more dangerous than it has ever been.
Until 2020, the Americans who were most concerned about medical risks and medical criminality belonged to groups already adversely affected, such as those injured by vaccines or opioids. However, with the advent of life-threatening COVID “countermeasures” and lethal protocols in U.S. hospitals and in other countries such as the UK, medical pharmaceutical gangsterism—seemingly occurring with government cognizance—has begun attracting more widespread notice. When governments began parlaying the dubious health “emergency” into an excuse to authorize and mandate the COVID vaccines and boosters—and proceeded full tilt even when unprecedented injuries and deaths immediately began piling up—some segments of the public saw the contours of an officially sanctioned medical crime.
As Holocaust survivor and human rights activist Vera Sharav communicated in her docuseries Never Again Is Now Global, medical coercion and the suspension of constitutional freedoms have never led anywhere good. Unfortunately, history shows that governments intent on “state repression, brutality and genocide” can usually count on the readiness of some doctors to serve as accomplices, even if their complicity has the potential to turn them into “mass murderers on an exponential scale.”
On November 14, 1986, Ronald Reagan signed the National Childhood Vaccine Injury Act into law.¹ The legislation ended more than a decade of tort litigation against vaccine manufacturers by transferring civil liability for injury and death from the companies producing the products to the American taxpayer. The pharmaceutical industry had threatened to leave the childhood vaccine market. Reagan’s signature ensured they would stay, at a price paid by parents who would never be told what had been arranged on their behalf.
Twenty-five years later, in Bruesewitz v. Wyeth, the Supreme Court closed the last remaining exit. The 2011 decision, written by Justice Antonin Scalia, held that federal law preempts all design-defect claims against vaccine manufacturers in state courts.² Justice Sotomayor’s dissent, joined by Justice Ginsburg, identified the practical effect: no federal agency, no state court, no jury of citizens would henceforth ensure that vaccine manufacturers accounted for scientific advances when designing their products. The manufacturers had been placed outside the accountability structure that governs every other industry in the United States.
The 1986 Act and the 2011 ruling together defined the shape of what now exists. Every function of the vaccine program — licensing, recommendation, purchase, safety monitoring, patent holding, research funding, injury adjudication, and courtroom defense — resides in the federal government. When the products kill a child, the state prosecutes the parents.
Leslie Manookian, founder of the Health Freedom Defense Fund, mapped this architecture in a twelve-point summary published to her readers.³ What follows walks through the machine she described, in five stages. Each stage encloses the next. By the fifth, the shape of the trap around the American parent becomes fully visible.
1. The License
The Food and Drug Administration licenses vaccines on the basis of clinical trials that do not use inert placebo controls. This fact is documented in the FDA’s own package inserts and in sworn testimony by the industry’s most senior figures.
In January 2018, attorney Aaron Siri deposed Dr. Stanley Plotkin in New Hope, Pennsylvania — the vaccinologist widely regarded as the industry’s founding figure and co-editor of the standard reference textbook Plotkin’s Vaccines.⁴ Under oath, Siri walked Plotkin through the pre-licensure clinical trials for each product on the recommended childhood schedule. The pattern that emerged was uniform.
The safety review period following each dose was 48 hours for the IPOL polio vaccine. 48 hours for ActHIB. Four days for Engerix-B, the hepatitis B vaccine administered to newborns on their first day of life. Five days for Recombivax HB, the other hepatitis B product. Siri produced, for comparison, the package insert for Enbrel — a drug given to adults with rheumatoid arthritis — and asked Plotkin to confirm that its pre-licensure clinical trials monitored patients for up to 80 months. Plotkin confirmed. A drug given to sick adults was studied for six and a half years. Vaccines given to healthy newborns were studied for 48 hours to five days.
Plotkin then confirmed, product by product, that these trials had no saline placebo control group. Not Recombivax HB. Not Engerix-B. Not IPOL, whose trial subjects received the polio vaccine concurrently with DTP, making it impossible to attribute any reaction to either product. Not ActHIB. The MMR II vaccine, which Plotkin himself was present for the licensure of, had, in his own words, no control group “for the studies that I’m recalling.” When the Hiberix Hib vaccine was later licensed, the manufacturer used ActHIB itself as the “placebo” — testing one Hib vaccine against another.
On the necessity of a saline control, Plotkin was direct: “Without a control group, if you’re looking for a phenomenon occurring in the vaccine group, you cannot judge that phenomenon without having a control group.” That is the industry’s founding figure, testifying under oath, describing the epistemic condition of the products his industry markets.
The pattern in the trials produces a specific consequence. When a new vaccine is tested against an existing licensed vaccine as its control, any injury rate common to both groups becomes invisible. The comparison measures relative difference, not absolute harm. If the existing vaccine produces seizures at a rate of 1 in 500, and the new vaccine produces seizures at a rate of 1 in 500, the trial reports no significant difference — and both products remain on the market.
The Gardasil trial illustrates what happens when a saline group is included but the result is inconvenient. Merck’s pre-licensure clinical trial for its HPV vaccine assigned 9,412 subjects to a “placebo” arm. Of these, only 594 received actual saline. The remaining approximately 8,800 received AAHS — the aluminum-containing adjuvant used in the Gardasil formulation itself. Merck reported the two groups combined, showing 2.3% of the “placebo” arm developing what the trial recorded as systemic autoimmune events, matched by 2.3% in the Gardasil arm. The vaccine was declared safe on the strength of no difference.
Siri produced the underlying trial data. Broken out separately, the saline placebo group of 594 girls and women showed zero such events. The aluminum group showed approximately 2.5%. Merck had recorded the difference and reported the combination.
Plotkin was asked why the two groups had been combined for that analysis when they were broken out separately for local reaction analysis on the preceding pages. His response, verbatim: “So going into the study, they just assumed aluminum wouldn’t cause autoimmunity and so that’s how they proceed in designing it.” A pre-licensure trial for a product administered to schoolgirls declared the vaccine safe by defining the aluminum adjuvant as inert, then combining subjects receiving that adjuvant with subjects receiving nothing.
Once a vaccine reaches the schedule, the failure to test it against saline becomes permanent. For each product Siri walked Plotkin through, he asked whether a proper placebo-controlled study could now be conducted. Plotkin confirmed, product by product, that it could not — running such a trial would be “unethical” in children whose vaccines are already recommended. The absence of a control group at the point of licensure becomes the reason no control group can ever be introduced. The regulatory record is locked at the point of the initial deception.
When a Freedom of Information Act request submitted by the Informed Consent Action Network in 2018 asked the Department of Health and Human Services to produce the biennial vaccine safety reports required by Section 300aa-27 of the 1986 Act, HHS was forced to respond that it had not produced a single such report in the thirty-two years since Reagan signed the law.⁵ The statutory obligation to review safety had been ignored for the entire life of the program.
The FDA license then triggers the second function. The Centers for Disease Control and Prevention convenes the Advisory Committee on Immunization Practices, which votes on whether to add the newly licensed vaccine to the recommended childhood schedule. ACIP members are drawn from the same institutional networks that developed and defended the products. Once added, the vaccine appears on the schedule that is distributed to every state health department in the country. The recommendation is not a mandate. It becomes one at the next stage.
Under oath in the same deposition, Plotkin acknowledged that he had served as medical and scientific director of Sanofi Pasteur in the 1990s, that he operated a personal consulting entity called Vaxconsult, and that he had received payments over the preceding two decades from Merck, GSK, Pfizer, Sanofi, and, in his own phrasing, “essentially all of the major manufacturers.” He had also consulted for the FDA. The industry’s founding figure had confirmed the case against the products his industry markets. He was also paid by every major manufacturer of those products.
The federal government does not directly mandate childhood vaccines. That function is delegated to the states.
Every state in the union has passed legislation requiring specified vaccines for school attendance. The specific list varies. The mechanism is uniform. Parents who wish to enroll their children in public school — and in many states private school — must produce documentation that their children have received the vaccines on the state’s list. The state list is drawn from the CDC schedule; the CDC schedule from the ACIP recommendation; the ACIP recommendation from the FDA license. The FDA license rests on trials that were never controlled against a genuine placebo.
The chain is complete before the parent enters the pediatrician’s office.
Under the Vaccines for Children program, established in 1993, the federal government purchases half of all childhood vaccines administered in the United States. Recent VFC spending has exceeded $5 billion annually.⁶ The federal government is the largest single purchaser of the products it licenses, the products it recommends, and the products the states mandate.
This creates a market structure without parallel elsewhere in American pharmaceutical policy. The maker of a blood pressure medication faces market discipline. Doctors may prescribe it or not, patients may fill the prescription or not, insurance may cover it or not. The maker of a childhood vaccine faces no equivalent constraint. The state compels administration; the federal government guarantees a buyer; demand is legislated. Revenue is secured before a single dose is delivered.
The mandate has hardened as it has aged. Every state at some point permitted medical, religious, and in some cases philosophical exemptions from the vaccine schedule. Over the past decade, state legislatures have moved to close them. California eliminated its personal belief exemption in 2015 through SB 277 following the Disneyland measles cluster. In 2019, New York eliminated its religious exemption; Maine followed the same year. Connecticut eliminated its religious exemption in 2021. The pattern has been consistent: a highly publicised incident, a legislative response drafted with industry input, and the removal of the exit ramp. The federal government does not need to mandate. The state legislatures have been prevailed upon to do it, and to progressively narrow the terms under which the mandate can be refused.
Leslie Manookian, in the interview she gave me,¹⁹ described the shape of what has been built here. “When we succeed and thrive outside the extant medical paradigm, we pose an existential threat to the medical complex which is why the main actors fight our information, experiences, and independence so fervently.” The compelled purchase is what makes the mandate machinery operate. Without it, the products would compete on their merits. With it, they do not compete at all.
The 1986 Act shielded manufacturers from every category of liability that governs other industries. The immunity covered injuries caused by design choices themselves — the composition of the product, the adjuvants used, the decisions about testing. A safer alternative product could exist and the manufacturer could refuse to adopt it, and the injured child’s family could not sue.
Justice Scalia’s opinion in Bruesewitz addressed a case brought by Robalee Bruesewitz on behalf of her daughter Hannah, who had suffered residual seizure disorder and developmental delay after receiving the DPT vaccine manufactured by Wyeth. The Bruesewitz family had exhausted the Vaccine Injury Compensation Program. They then attempted to sue Wyeth in state court, arguing that a safer alternative vaccine design existed and Wyeth had refused to adopt it. The Supreme Court held that federal law preempts such claims. The manufacturer’s choice to continue producing a design that injured children could not be litigated.
Sotomayor’s dissent identified the consequence. Vaccine manufacturers now occupy a regulatory space in which no external mechanism — regulatory agency, court, or jury — holds them accountable for design decisions. This is not an inference. It is a description of the legal structure the majority created.
Behind the shield sits a further conflict. The Department of Health and Human Services — the parent agency of the FDA, the CDC, the National Institutes of Health, and the Health Resources and Services Administration that runs the injury compensation program — holds patents on multiple childhood vaccines. HHS scientists Douglas Lowy and John Schiller developed the recombinant protein technology underlying Merck’s Gardasil and receive royalties on its sale.⁷ Similar patent and royalty arrangements extend to other products in the childhood schedule. The regulator collects revenue on the products it approves.
The research infrastructure that would produce independent safety findings is subject to a parallel capture. Studies funded by the CDC, the NIH, or by the manufacturers themselves consistently produce findings favorable to the schedule. The vaccinated-versus-unvaccinated comparison studies that would settle the fundamental question about long-term outcomes have not been funded. When independent researchers attempt them — Anthony Mawson’s 2017 study of homeschooled populations,⁸ Paul Thomas’s cohort analysis of his own pediatric practice⁹ — the results are attacked, retracted, or ignored, and the researchers face professional consequences.
The capture extends inside the agencies themselves. In August 2014, Dr. William Thompson, a senior epidemiologist at the CDC and co-author of the 2004 DeStefano study widely cited to reject any link between the MMR product and neurodevelopmental injury, submitted a statement through his attorney acknowledging that he and his co-authors had “omitted statistically significant information” from the published paper and had disposed of documents to conceal the omission.¹⁰ The withheld data showed an elevated risk of neurodevelopmental injury among African American boys who received the injection before thirty-six months of age. Thompson’s disclosure was made under whistleblower protection. Congress has never subpoenaed him to testify. The DeStefano paper remains uncorrected.
Merck faced a parallel qui tam action from two of its own virologists, Stephen Krahling and Joan Wlochowski, who alleged in a federal filing that Merck had falsified mumps vaccine efficacy data submitted to the FDA over the course of a decade.¹¹ The case, filed in 2010, moved slowly through the courts. The Department of Justice declined to intervene. Merck retained its exclusive contract to supply mumps vaccine to the U.S. government. The plaintiffs’ allegations of test manipulation entered the public record and produced no regulatory action.
The shield is a network. Liability preemption from Congress protects the manufacturer. Patent revenue aligns the regulator with the products it approves. Captured research funding directs the studies that might identify harm away from the questions that would find it. Judicial preemption then blocks any citizen who attempts to litigate the design decisions the products embody. Each layer supports the others. The whole structure is invisible to the parent standing in a pediatrician’s office being told the shot is safe.
The Centers for Disease Control and Prevention operates the Vaccine Adverse Event Reporting System. It also runs the promotional campaigns that place vaccination on the pediatric schedule. The agency responsible for detecting harm from the products is the same agency responsible for driving their uptake.
The conflict is not theoretical. Harvard Pilgrim Health Care, under a grant from the Agency for Healthcare Research and Quality within HHS, conducted an internal study of VAERS reporting rates in a Massachusetts patient population between 2007 and 2010. The study found that fewer than 1% of vaccine adverse events were being captured by the reporting system.¹² When the researchers attempted to communicate their findings to the CDC in order to develop improved reporting mechanisms, the agency stopped responding to their emails. The grant ended. The improved reporting system was never built.
The passive reporting infrastructure that captures under 1% of injuries then becomes the basis for the CDC’s public assurances that adverse events are rare.
The injury table itself has been subject to steady contraction. When the Vaccine Injury Compensation Program began in 1988, the injury table included a broader range of conditions presumed to be caused by vaccination, with corresponding timelines within which onset would qualify a case for compensation.¹³ Over the following decades, categories were removed or narrowed. Sudden Infant Death Syndrome, initially compensable when it followed vaccination within a specified window, was removed. Neurodevelopmental injury, briefly acknowledged as a category during the 1990s when concerns about the MMR product and other injections emerged, was removed. The seizure timelines were narrowed. Encephalopathy definitions were tightened.
The 1995 amendment illustrates the pattern. Residual seizure disorder — a category under which many families of children who had suffered seizures after DPT vaccination had successfully claimed compensation — was removed. Encephalopathy criteria were revised in ways that made the diagnosis nearly impossible to satisfy. The Advisory Commission on Childhood Vaccines, which recommended the changes, drew a majority of its membership from the same medical-institutional networks that administered and defended the vaccine schedule. Petitioners whose cases had been filed under the earlier table found themselves adjudicated under the new one. Cases that would have succeeded were denied.
Each removal reduced the number of compensable claims. The fund benefited. So did the manufacturers whose products would otherwise be more clearly implicated in the injury pattern.
The Institute of Medicine, tasked periodically with reviewing whether specific vaccines cause specific injuries, has repeatedly concluded that the evidence is insufficient to accept or reject a causal relationship for a majority of the injury-outcome pairs it examines.¹⁴ This finding — insufficient evidence — is then used in the injury compensation courtroom to deny claims. The absence of evidence functions as evidence of absence, produced by the very research infrastructure that would have to fund the studies to end the insufficiency.
The industry’s founding figure confirmed the position under oath in the same deposition. Asked directly whether he could make the scientific statement that childhood vaccines do not cause autism, Plotkin answered: “As a scientist, I would say that I do not have evidence one way or the other.” The IOM had found no study establishing that the DTaP or Tdap products do not cause autism. Plotkin acknowledged that no such study existed and that he personally held no evidence to support the claim his industry has spent three decades making.
The parent whose child seized within twelve hours of vaccination, developed encephalopathy, and never recovered enters a system that was prepared for her arrival. The injury table’s timeline for seizure onset has been shortened past the point where her child’s case qualifies. The IOM has declared the evidence insufficient. VAERS captured her report and did nothing with it. The monitor was never separate from the promoter.
5. The Court and the Blame
The Vaccine Injury Compensation Program is administered by the U.S. Court of Federal Claims. It is not a court in the ordinary sense. The proceedings involve no juries, no meaningful discovery, and no Article III judges — no judges appointed for life under the constitutional protections designed to insulate the judiciary from executive influence.
Cases are heard by “Special Masters,” Article I officers appointed by the Chief Judge of the Court of Federal Claims to seven-year terms. The Special Masters are drawn from a pool of attorneys with prior government experience. The Department of Justice provides the attorneys who defend against injury claims. HRSA administers the fund. The petitioner’s attorneys are paid from the same fund out of which awards are made.
Every party in the courtroom — the judge, the government’s defense attorneys, the fund itself, and the petitioner’s legal counsel — is paid by the federal government. The injured child’s family stands before a tribunal in which no independent party has an interest in a finding of injury.
The statistics reflect the structure. The majority of petitions filed with the VICP have been dismissed rather than compensated over the life of the program.¹⁵ Of the cases that succeed, the majority are settled rather than adjudicated on the merits, with no admission that the vaccine caused the injury. The compensation cap for a vaccine-caused death — $250,000 — has not been raised since the statute was passed in 1986.
The excise tax that funds the program is $0.75 per antigen per dose. The fund now holds over $4 billion.¹⁶ The families whose children were injured cannot access it through the ordinary legal system because the ordinary legal system has been closed to them.
This is the structure Leslie Manookian described in her twelve-point summary. Her exact phrasing on the final function is worth returning to: “So, parents who’ve already suffered an unimaginable tragedy are up against a govt court staffed by govt paid special masters and attorneys with no due process defending a govt licensed and govt mandated product for which they blame the victims for harm.”
The final phrase — “they blame the victims for harm” — describes the twelfth function of the machine. When a child collapses after vaccination with the sudden onset of retinal hemorrhages, subdural hematoma, and cerebral edema — the triad — the diagnosis assigned in emergency departments and coroner’s offices is “shaken baby syndrome” or its rebranded successor, “abusive head trauma.” The triad is presumed diagnostic of parental abuse. The parents are arrested.
The vaccine reaction that produces the identical triad — through encephalopathy, elevated intracranial pressure, and hemorrhagic events following injection — is not considered in the differential diagnosis.¹⁷ The diagnostic criteria for “shaken baby syndrome” were developed without accounting for it. The emergency physician, the coroner, and the child protective services investigator have all been trained within an institutional framework in which vaccine injury of this magnitude does not exist.
Alan Yurko’s ten-week-old son died in November 1997 shortly after receiving a round of childhood vaccinations. Yurko was convicted of first-degree murder in 1999 on the basis of the triad diagnosis and sentenced to life plus ten years in Florida state prison. He was released in 2004 after independent medical review of the case demonstrated that the shaking diagnosis could not be sustained and post-conviction proceedings established alternative medical explanations for the child’s injuries.¹⁸ Yurko is one documented case. There are others. The precise number is unknown because the diagnostic framework prevents the question from being asked.
A parent whose child dies after vaccination faces a compound structure. The vaccine that caused the death is licensed by the federal government, recommended by the federal government, purchased by the federal government, and defended in the injury court by the federal government. The manufacturer is shielded from civil liability by federal statute and Supreme Court precedent. The injury table does not recognize the death as vaccine-caused. The state, meanwhile, has assigned the triad diagnosis and turned the case over to the district attorney. The parent must now prove — in a criminal court, against the state — that the child was not shaken.
Robalee Bruesewitz spent nearly two decades in litigation on behalf of her daughter. The Supreme Court’s ruling denied her family relief and closed the door behind them for every family that would come after. The 1986 Act had shifted liability from the manufacturer to the taxpayer. Bruesewitz confirmed that the shift was permanent and that no design decision made by the manufacturer could be challenged in any court open to ordinary Americans.
This is the position in which the American parent now stands. Her child’s pediatric visit will produce a recommendation to administer products licensed on the basis of trials that were never controlled against saline. The state will require their administration for school attendance. When injury results, over 99% of adverse events never reach VAERS at all, and the reports that do reach it change nothing. A family that attempts compensation will petition a court in which every party is paid by the federal government to defend the products or administer the fund. And when death occurs with the triad present, the emergency department’s diagnostic framework will not include vaccine reaction in the differential, and the parent enters the criminal jurisdiction as the presumed cause of the child’s death.
There is no exemption from this structure that carries no cost. State legislatures have progressively narrowed medical and religious exemptions; declining vaccines removes a child from school; injury bars a family from ordinary civil courts. And when death is accompanied by the triad, the state prosecutes the parent for the death.
Leslie Manookian described this arrangement, at the close of her twelve-point post, as “crony capitalism at best and pure evil fascism at worst.” The characterization is precise. A private industry produces the product. The state compels its administration, indemnifies the manufacturer against claims of harm, and prosecutes the parent when the harm arrives.
The machine’s design serves the flow of money and the concentration of power. Every safeguard the ordinary citizen might rely on — informed consent, product liability, judicial review, jury trial, prosecutorial restraint — has been removed at the point where the childhood vaccine schedule intersects with the American family. The parent who accepts the recommendation and whose child is injured has no meaningful path to redress. Refusal costs school access. Death with the triad opens the parent to criminal prosecution for a killing they did not commit.
This is the environment in which every American child is now born. The machine was assembled piece by piece across four decades, ratified by every institution that could have prevented it, and defended by the same institutions today. What Leslie Manookian named as crony capitalism at best and fascism at worst describes a working system, operating as designed, in a country that once organised its politics around the presumption that no such system could be permitted to form.
For a Six-Year-Old
There is a big company that makes shots.
The government helps the company make the shots and sell them. The government tells your school that you have to get the shots before you can come to school.
Nobody checks the shots very well. The people who are supposed to check work with the company. So the shots go out into the world before anyone really knows if they are safe.
When a child is hurt by a shot, the family cannot go to a normal judge. There is a special room where a different kind of judge decides. That judge is paid by the government. The lawyers on the other side are paid by the government. The government made the shot rules. The government bought the shots. And the government decides whether the shot hurt you.
Most families are told the shot did not hurt their child, even when it did.
When a shot makes a baby die, the doctors sometimes think the mother or father shook the baby. The parents can be arrested. They can go to prison. For what the shot did.
The company that made the shot never gets in trouble. The company keeps making the shots. Your school keeps requiring them. The next family goes through the same door.
That is the machine.
References
¹ National Childhood Vaccine Injury Act of 1986, Public Law 99-660, 42 U.S.C. § 300aa-1 et seq.
² Bruesewitz v. Wyeth LLC, 562 U.S. 223 (2011).
³ Leslie Manookian, twelve-point summary post, X (@LeslieManookian), July 3, 2026, status/2072712451800625369.
⁴ Deposition of Stanley A. Plotkin, M.D., taken January 11, 2018, in Matheson v. Schmitt, State of Michigan, Circuit Court for the County of Oakland, Family Division, Case No. 2015-831539-DM; transcript published via Informed Consent Action Network.
⁵ ICAN v. HHS, correspondence dated July 9, 2018, in response to FOIA request; HHS acknowledged no biennial reports produced under 42 U.S.C. § 300aa-27(c).
⁶ Vaccines for Children Program expenditure data, Centers for Disease Control and Prevention; annual VFC purchasing figures.
⁷ U.S. Patents 5,437,951 and related — Lowy, Schiller et al., “Self-Assembling Recombinant Papillomavirus Capsid Proteins,” assigned to the United States Department of Health and Human Services; licensed to Merck & Co. for Gardasil.
⁸ Mawson AR et al., “Pilot comparative study on the health of vaccinated and unvaccinated 6- to 12-year-old U.S. children,” Journal of Translational Science, 2017.
⁹ Thomas JL, Lyons-Weiler J, “Relative Incidence of Office Visits and Cumulative Rates of Billed Diagnoses Along the Axis of Vaccination,” International Journal of Environmental Research and Public Health, 2020.
¹⁰ Statement of William W. Thompson, Ph.D., through counsel Rick Morgan, August 27, 2014; documentation regarding DeStefano DA et al., “Age at first measles-mumps-rubella vaccination in children with autism and school-matched control subjects: a population-based study in metropolitan Atlanta,” Pediatrics, 2004.
¹¹ United States ex rel. Krahling and Wlochowski v. Merck & Co., Inc., No. 2:10-cv-04374, U.S. District Court for the Eastern District of Pennsylvania, complaint filed 2010.
¹² Lazarus R et al., “Electronic Support for Public Health–Vaccine Adverse Event Reporting System (ESP:VAERS),” Grant Final Report, Harvard Pilgrim Health Care, Inc., 2011 (AHRQ Grant ID R18 HS 017045).
¹³ Vaccine Injury Table history, Health Resources and Services Administration; successive amendments to 42 C.F.R. § 100.3.
¹⁴ Institute of Medicine (now the National Academy of Medicine), Adverse Effects of Vaccines: Evidence and Causality (2011) and predecessor reports.
¹⁵ Health Resources and Services Administration, VICP claim adjudication statistics.
¹⁶ Vaccine Injury Compensation Trust Fund monthly balance report, U.S. Department of the Treasury.
¹⁷ Michael Innis, “Vaccines, Apparent Life-Threatening Events, Barlow’s Disease, and Questions about ‘Shaken Baby Syndrome,’” Journal of American Physicians and Surgeons, 2006; Harold Buttram and Alan R. Yurko, “Shaken Baby Syndrome or Vaccine-Induced Encephalitis?” Medical Sentinel, subsequent case documentation.
¹⁸ State of Florida v. Alan R. Yurko, Ninth Judicial Circuit, 1999; post-conviction proceedings and release 2004; contemporaneous medical review including Harold E. Buttram, M.D.
¹⁹ Unbekoming, “Interview with Leslie Manookian, Health Freedom Defense Fund,” Lies are Unbekoming, Substack, April 13, 2024.
The FDA began reevaluating sunscreen chemical safety in 2019, yet millions are still told to apply these products every day. Jefferey looks at what happens when sunscreen chemicals enter the bloodstream, and why new research on sun exposure, vitamin D, and cancer is challenging old assumptions.
Over the past month, four studies have been read as showing that the shingles vaccine prevents, or even reverses, dementia. A national newspaper has turned that reading into advice. The advice is to go and get the vaccine now. The evidence tells a different story.
Vinay Prasad has already gone through the four papers and laid the timings side by side, and I will not improve on that account.
● TheAnnals paper has a 5% absolute reduction in dementia by three years, with benefit appearing within a year of a nursing-home admission.
● The Welsh study inNature is a natural experiment, not a simple cohort, and reports a fifth fewer dementia diagnoses over seven years. It declines to publish a time-to-event plot at all.
● The American paper, inNature Medicine, includes a hazard function whose curves separate almost immediately.
● And a meta-analysis concludes that it is not the shingles vaccine alone but every adult vaccine that appears to protect against dementia.
What a dementia diagnosis actually is
A dementia code in a health record is the end of a chain of soft decisions:
● someone has to notice a change,
● the patient has to present to the system,
● a threshold has to be applied,
● and a clinician has to enter the code.
For each of these steps there is wide variation in the timing between patients. The noticing depends on who is being watched closely and who is not. The same forgetful elderly person can be coded, or not coded, according to how hard anyone happens to be looking. Look harder and you might diagnose more.
Now ask who receives an elective shingles vaccine. It is, overwhelmingly, the people well enough to go and get one. The housebound, the frail, and above all those whose memory is already failing, the people nearest to a diagnosis, are the least likely to present for a non-urgent injection. So the unvaccinated group is enriched, at the very outset and before anyone is followed up, with exactly the people who will later be coded with dementia. This is the “healthy vaccinee effect”, and in this setting it is large enough to produce the whole of the apparent benefit on its own.
Why four studies agreeing is not reassurance
The natural objection is that four datasets agree, and agreement is supposed to be reassuring. But when the cohort studies make the same methodological error it is not reassuring. Every one of them carries the same confounding structure: in each, vaccination marks underlying health, healthcare contact and the simple capacity to turn up, and in each that marker is correlated with the outcome being measured. The errors are not independent results that happen to coincide. They are the same error made several times, because the same bias is built into each design. A biased estimate does not become unbiased by being repeated. These confounded studies in agreement tell you that the confounder is stable, not that the result is real.
Prasad puts this as the earth looking flat whichever way you turn, which is exactly right as an image of the confounded cohorts. The formal version is that replication adds evidence only when the replications are capable of failing in different ways. When they share their confounders, consistency is not corroboration, it is the same confounder doing the same job in each dataset in turn. To break the symmetry you do not add a fifth observational cohort, another flat horizon. You change the design to one whose errors are structured differently. That test already exists.
A regression-discontinuity study exploits the age cut-off for eligibility: people just below and just above the threshold are, for practical purposes, exchangeable, so the baseline-health gap that drives the observational studies is largely removed. The Welsh study is exactly this design, which is why it is the strongest evidence on the table; they claimed dementia was prevented in Wales and in Australia and Ontario. But would an independent team running a study with an identical design find the same thing? George Davey Smith and colleagues have now carried out such a study in England, across some 6.3 million people, roughly twenty times the Welsh sample; the work was presented in June 2026 at a conference and is not yet published. The design worked, in that eligibility produced the expected fall in shingles (although it is not clear what happened in the ‘grace period’ immediately after vaccination) but on dementia it found nothing. The fact that the finding was null in the far larger study should mean the smaller one has been overruled.
The speed matters
Speed is being sold as a measure of how powerful the vaccine is. It is better understood as evidence that the vaccine is doing nothing at all. Dementia is slow. The neuropathology accumulates over years, usually decades, and by the time anyone is coded with the disease the process is long established. Nothing done to a brain can produce a measurable difference in dementia incidence within a hundred days, because the disease does not move on that timescale. So when the curves separate almost immediately, the separation cannot be the vaccine acting. It can only be that the two groups already differed at the moment the vaccine was given.
It is a signature of selection. The rapidity that is being offered as the headline result is the clearest single indicator that what is on the page is the “healthy vaccinee” artefact and not a treatment effect.
From the literature to the newsstand
On 10 June theDaily Telegraph published an interview with John Todd, professor of precision medicine at Oxford, in which he told readers over fifty to get the shingles vaccine now. Jonathan Engler has lodged a complaint with the MHRA about that article.
Professor Todd is, on his own declaration, a paid consultant for GSK, which manufactures Shingrix, and the study he relies on is one he co-authored. When the paper was published, given the issues described above about selection bias the authors wrote that the dementia results “provide a rationale for conducting a randomized control trial aiming to confirm the findings”. Shingrix is not licensed for the prevention of dementia. The advice to buy it for that purpose rests on a paper whose findings, in its authors’ own words, have not been confirmed.
In the United Kingdom, the advertising of prescription-only medicines is governed by Part 14 of the Human Medicines Regulations 2012. Regulation 284 provides that a person may not publish an advertisement likely to lead to the use of a prescription-only medicine. There is proper latitude for journalism, and the MHRA’s guidance for journalists asks only that coverage be balanced, that it not exaggerate benefit, and that it not steer readers towards a named product. It does not require proof of a commercial arrangement before a breach is made out. Engler’s point, which is the right one, is that a piece does not stop being promotional by declining to call itself promotional, and that the absence of the label is itself the difficulty. Where a consultant to the manufacturer urges the purchase of that manufacturer’s unlicensed product, on the strength of his own unconfirmed research, with the consultancy unmentioned, the ordinary description of the result is advertising, whatever else it is also called.
Telegraph readers thinking of taking his advice to rush off and buy a private Shingrix vaccine, might want to take note that (a) Professor Todd has no medical qualification (his FRCP is honorary and his primary qualification is in biochemistry) and (b) the department he heads in Oxford was funded by GSK to the tune of £30 million.
What honest curiosity would do next
The editors of the observational papers could be asked to publish the all-cause mortality curves alongside the dementia curves: if the vaccinated are simply healthier people, their mortality will diverge in the same direction, and the confounding will be visible on the page. This is a control test. Every child at school is taught the importance of using a control group in scientific research but all too often they are left out by actual scientists. The randomised trial that the NIH is said to be considering might need to be run simply to put to bed the excitement around this issue that has been fuelled by media speculation.
The truth is that the studies that kept producing the same answer did so because they shared the same bias, while the largest independent test found nothing and a national newspaper has printed a paid consultant’s promotion of a drug when he will benefit from the sales. Perhaps neither of those stories will sell as many newspapers as the ones that do get printed or clicked on.
In the 1820s, when John Bostock first documented the condition in London, every case he could find was in the middle or upper classes. He inquired at the dispensaries and across the country and found, in his own words, no unequivocal case occurring among the poor.¹ Twenty years earlier, a new medical procedure had been introduced in England. The disease appeared in the class that received the procedure. Those who had not received it remained free of it. The procedure was Edward Jenner’s vaccination, the insertion of material from cowpox lesions into incisions in the human arm. The material’s origin was the cow.²
Hay fever did not exist in the medical literature before this. The first cases appeared in the population that had received the procedure. The mechanism by which injection of foreign protein produces sensitization to bystander substances was discovered before the end of the century, demonstrated in animal models repeatedly since, and conceded by establishment investigators in at least one specific case. The condition that tens of millions experience as a feature of biology is an artifact of the syringe.
The Disease That Did Not Exist
Bostock called it the Catarrhus Aestivus, summer catarrh.¹ He had experienced it himself since he was a young man. His symptoms began every June with heat and fullness in the eyes, irritation of the nose accompanied by sneezing, and tightness in the chest. The 1819 paper to the Medico-Chirurgical Society was an attempt to ask the other physicians of London whether they had seen anything similar. Nothing in the medical literature, ancient or modern, described the syndrome. None of the most eminent physicians of London, Liverpool, or Edinburgh had heard of anything like it.
By 1828 Bostock had assembled twenty-eight cases.¹ Every one of them was in the middle or upper classes. He initially attributed the trigger to the effluvium from new hay, and the name stuck. The condition was hay fever even after Charles Blackley demonstrated, in 1873, that the proximate trigger was pollen and not hay itself.³ Blackley, a Manchester physician who suffered from the condition, applied pollen to abraded patches of his own skin and observed the reaction. The proximate cause was identified. The originating cause was not asked.
What did become asked, in the half-century that followed Bostock’s first paper, was what kind of person developed hay fever. The answer was consistent. The condition was an affliction of the wealthy, of the urban, of the educated. The wheezing wealthy, in a pattern that became fashionable, would migrate every summer to the English coast, then to the Swiss Alps, and, by the late nineteenth century, to the White Mountains of New Hampshire, where the air was understood to be safe.³ Those who could not afford to leave continued, by every report, not to develop the condition. The nostrums prescribed when the patient could not travel included medicated cigarettes, powders, and salves.
The vocabulary used to describe what was happening did not yet exist. The word allergy was coined in 1906 by the Viennese pediatrician Clemens von Pirquet, in response to reactions doctors had observed in patients they had injected with horse serum. The word anaphylaxis had been introduced four years earlier by the French physiologist Charles Richet, describing a phenomenon he had produced by injecting sea anemone venom into dogs. The condition Bostock had documented in 1819 had been observed for eighty-five years without a category to file it under. It was, in the most literal sense, unprecedented in human medicine.
What had also happened in the decades preceding Bostock’s first paper was Edward Jenner’s introduction of the cowpox procedure.² Jenner published his findings in 1798. By 1801 James Smith had been appointed as the first United States Vaccine Agent. The first US Vaccine Act passed in 1813. Compulsory vaccination would spread across European jurisdictions through the rest of the century, with the United Kingdom’s Vaccination Act of 1853 making the procedure mandatory in England and Wales. Before any of those mandates were in place, the procedure had been adopted by those who could afford it and avoided by those who could not. The early vaccinations used arm-to-arm transmission from cowpox-affected milkmaids; by the mid-nineteenth century, industrial-scale production used calf-derived vaccine lymph directly. The constant across both methods was that material of animal origin was introduced past every layer of the body’s normal route of exposure.
Forrest Maready’s reconstruction of the historical record names what the documented sequence implies.² A disease that had no precedent in medicine appeared in London within a generation of the introduction of the cowpox procedure, in the class that received the procedure, in a city where the procedure had spread first. The mechanism by which such exposure produces sensitization to bystander substances had not yet been described. It would be, three quarters of a century later, by Charles Richet.
Richet, and Foreign Protein
In 1901 Charles Richet, working with Paul Portier aboard the yacht of the Prince of Monaco, was studying the toxicity of sea anemone venom. He injected small amounts into dogs to establish baseline responses. The first injections produced predictable effects. When he later attempted to inject the same dogs again, weeks after the first exposure, he found something he had not expected. The second injection, of a dose the dogs had previously tolerated, produced a violent and disproportionate reaction. The dogs collapsed. Some died within minutes.⁴
Richet named the phenomenon anaphylaxis, against protection, because the body’s response to the second exposure was the opposite of what immunization was meant to produce. Injection of foreign protein did not protect against subsequent exposure. It sensitized. The reaction was demonstrated across species and across protein sources, and the demonstration was reliable. The 1913 Nobel Prize in Physiology or Medicine was awarded to Richet for this work.⁴
The mechanism Richet described is the foundation of every allergic phenomenon documented since. Foreign protein introduced through injection, bypassing every layer of the body’s normal route of exposure, produces a sensitized state. On subsequent contact with the same material or with material closely resembling it, the body responds with escalating intensity. The mechanism does not require an inhaled antigen or a digestive failure. It requires only an injection and a second exposure. The clinical demonstration in human children had already been under way for more than a decade by the time Richet won his Nobel Prize.
The Diphtheria Antitoxin
The first mass clinical demonstration of Richet’s mechanism in human children did not wait for the Nobel committee. It had already been under way in routine pediatric practice for the better part of a generation.
In 1890 Emil von Behring and Shibasaburo Kitasato discovered that horses injected with diphtheria toxin produced a substance in their blood that neutralized the toxin. By collecting blood from the immunized horses, separating out the red cells, and filtering the remaining serum, a therapeutic preparation could be made. Children with diphtheria, injected with the horse serum, often recovered. Behring received the first Nobel Prize in Physiology or Medicine for this work, in 1901.⁵
The procedure became routine through the 1890s and the first years of the twentieth century. Children with diphtheria received it as treatment. Children in institutions, orphanages, and hospitals received it prophylactically when diphtheria appeared in the community. The serum being injected was horse serum: the antitoxin and every other protein the horse’s bloodstream had been carrying.
What the children began to show, with growing frequency, was a delayed systemic illness that did not fit any existing diagnostic category. Seven to twelve days after the injection, fever appeared, urticarial rashes spread across the body, joints swelled and ached, and the lymph nodes nearest the injection site enlarged. The illness lasted one to two weeks and resolved on its own. It bore no resemblance to diphtheria.
Clemens von Pirquet and Béla Schick, two pediatricians at the University Children’s Hospital in Vienna, began collecting the cases systematically. By 1905 they had analyzed over a hundred and published their findings as Die Serumkrankheit, Serum Sickness.⁵ The monograph documented what they observed. The illness was a response to the horse proteins in the serum. It was dose-related, with the worst reactions in the children who had received the most serum. Re-injection produced an accelerated response, sometimes within twenty-four hours of the second injection rather than the eight-to-twelve days of the first. In some cases the second injection produced sudden anaphylaxis and the child died within minutes.
The clinical phenomenon Richet had documented in dogs was being observed, in real time, in children injected with horse serum. In 1906 Pirquet coined the word allergy, from the Greek allos and ergon meaning altered reactivity, to describe what he and Schick had been observing. The word entered the medical vocabulary of the twentieth century. Within a generation it had been generalized far beyond the horse-serum context that produced it. It is the word used today, by the same medical tradition, to describe hay fever.
The diphtheria antitoxin episode established on the clinical record what Richet’s animal experiments had shown more cleanly. Foreign animal protein injected into children produced systemic reactions in a substantial fraction of recipients, intensifying with each successive exposure and sometimes killing the child outright on a second injection. This was not theoretical. It was the routine experience of pediatric practice for two decades, and it generated the vocabulary that the rest of the twentieth century would inherit.
The Adjuvant Mechanism
The next refinement was aluminum.
Vaccine science discovered in the 1920s that injecting a foreign protein alongside an aluminum compound produced a far more intense response than injection of the protein alone. The aluminum acted as what the field came to call an adjuvant, a helper. It provoked an inflammatory reaction at the injection site so intense that any other material present at that site was swept into the reaction. The body responded not just to the aluminum and not just to the protein, but to the combination.
The mechanism is the foundation of every laboratory model of allergic disease. The standard laboratory model of asthma is produced by injecting mice with ovalbumin alongside aluminum hydroxide. The same protocol, with different proteins, produces laboratory models of dust mite allergy, fish allergy, and other named allergic conditions. Allergy is not observed in nature and then replicated in the laboratory. Allergy is created in the laboratory by injection of foreign protein with adjuvant. The mechanism by which allergy is produced for study is the mechanism the syringe administers in clinical practice. The two procedures are the same procedure.
Aluminum exposure is also known to produce asthma in humans through other routes. The industrial-exposure literature has documented occupational asthma in aluminum smelters and aluminum welders for decades. The mechanism is not in dispute. What is in dispute is whether the same aluminum, injected into the bloodstream of children rather than inhaled by adults at work, has equivalent effects.
The Japanese DTaP case settled the question for one specific protein. Through the 1980s and into the 1990s, Japan revised the formulation of its diphtheria-tetanus-acellular-pertussis vaccine.³ The acellular version, the world’s first, contained gelatin as a stabilizer. Until 1993, Japanese children received a trivalent MMR vaccine before the DTaP series, and no anaphylactic reactions to the MMR were reported during that period. From 1994 the schedule was reversed, with DTaP given before the gelatin-containing MMR.
Japanese children began to react with anaphylaxis to the MMR. They began to react with anaphylaxis to gelatin-containing foods, to yogurt, to gummy sweets, to jelly desserts. Japanese investigators traced the chain. The DTaP, administered first, had sensitized the children to the gelatin present in the formulation. The MMR, given later, contained the same gelatin. The body had been primed by the first injection. The second exposure produced the reaction. Between 1997 and 2000, gelatin was removed from all the Japanese DTaP vaccines. The anaphylaxis to gelatin-containing MMR stopped.⁶
The conceded mechanism is exactly what Richet had described in 1901. Foreign protein, introduced at an injection site, produces sensitization to that protein. The body subsequently encounters the same protein through another route, including orally, and reacts. The Japanese investigators conceded the mechanism in the specific case of gelatin. They did not concede it for any other.
Hilleman, Adjuvant 65, and What Merck Knew
Maurice Hilleman, the chief vaccine developer at Merck through the second half of the twentieth century and the dominant figure in twentieth-century American vaccine production, understood the mechanism. In 1964 his team announced Adjuvant 65, an experimental influenza-vaccine adjuvant composed of eighty-six percent peanut oil emulsified with four percent aluminum monostearate.⁷ The formulation was developed because earlier oil-based adjuvants had produced persistent local reactions, tumors in animals, and what the literature of the period called autoimmune reactions. Hilleman’s group published the early clinical trials in the New England Journal of Medicine, the New York Times reported on the patent, and clinical testing proceeded through the late 1960s and into the 1970s.
Hilleman and his colleagues understood that the procedure they were testing would introduce intact peanut oil, alongside an aluminum compound, into the human arm. Allergic sensitization to the oil was acknowledged as a possibility. The reasoning at the time was that highly refined peanut oil would lack the proteins that drove an allergic response. The FDA disagreed: refined oils retained protein traces, and intramuscular injection rather than intravenous was the recommended route precisely because intravenous deposition risked greater absorption and a stronger reaction.
The 1973 WHO Scientific Group on Immunological Adjuvants, whose deliberations were published as Technical Report Series No. 595 in 1976, addressed the safety questions that adjuvants raised.⁸ The group examined what injection of adjuvants alongside antigens would produce, considered the route-of-administration variable, and reviewed contamination concerns. Adjuvant 65 itself was discontinued within a few years because of reactogenicity in human subjects.
The relevant point is not that Adjuvant 65 was licensed for general use. It was not. The relevant point is that the people building vaccine adjuvants understood, by the mid-1960s, that introducing food-derived oils into the human bloodstream alongside an aluminum compound carried a serious risk of allergic sensitization. They tested it anyway. They considered the risk acceptable. The schedule they helped design in the years that followed expanded steadily. Peanut allergy, a clinical rarity through the 1980s, became epidemic in the 1990s and 2000s.
The Pertussis Mouse
The animal-model literature on pertussis demonstrates the mechanism applied to airborne triggers.³ When researchers inject mice with pertussis, the mice subsequently react to airborne allergens they would not otherwise have reacted to. Pertussis toxin functions as an adjuvant in this experimental context, amplifying the body’s response to whatever proteins are present in the inhaled environment.
The animal-model and clinical-observation literatures converge on a single pattern. Inject foreign protein into a young animal, with or without a separate adjuvant, and the animal becomes sensitized to substances it would otherwise have tolerated. The procedure used to manufacture laboratory models of allergic disease is the procedure that produces clinical allergic disease in human beings.
Modern Schedule, Modern Numbers
The clinical evidence for the same mechanism in modern children is documented in the establishment’s own journals, though the literature is contested.
In 2005 the Journal of Allergy and Clinical Immunology, the flagship publication of American allergy medicine, published a study by Enriquez and colleagues based at Vanderbilt University.⁹ The cohort included 515 never-vaccinated children, 423 partially vaccinated children, and 239 fully vaccinated children in the United States. Among children with no family history of hay fever, parents of unvaccinated children were ten times less likely to report hay fever in their child. The probability that this finding occurred by chance was less than five in ten thousand. The lead author was based at Vanderbilt’s Division of Allergy, Pulmonary, and Critical Care Medicine. The paper was peer-reviewed in the allergy field’s central journal, and it remains in the literature.
The same year, the Archives of Disease in Childhood, the British pediatric journal of record, published a study by Bremner and colleagues using two large UK databases comprising more than 7,000 hay fever cases and matched controls.¹⁰ The investigators did not find that vaccinated children overall had higher hay fever risk than the unvaccinated. What they found was internal to the schedule. Children whose DTP series had been delayed beyond their first birthday had reduced odds of hay fever, and children whose first MMR had been delayed beyond age two had similarly reduced odds. The pattern was a dose-response on timing: the longer the schedule was deferred, the less hay fever appeared. The investigators acknowledged the finding and suggested it might reflect confounding by febrile illness during the delay. The pattern, however interpreted, is consistent with the Richet mechanism: timing of antigen exposure during early life shapes the subsequent allergic response.
Three years later, Pediatric Allergy and Immunology published the Bernsen finding.¹¹ Bernsen and colleagues compared pertussis exposure in vaccinated and unvaccinated children. The internal finding within the paper is the load-bearing one. In the unvaccinated group, there were no significant associations between pertussis exposure and the conditions labeled atopic. In the vaccinated group, the associations were positive across hay fever, asthma, and food allergies. The same bacterium, introduced through two different routes, produced two different outcomes. Encountered naturally, pertussis did not produce hay fever. Following pertussis vaccination, it did.
A 2006 paper in the Journal of Allergy and Clinical Immunology by Flöistrup and colleagues examined 4,606 children in Steiner-school communities, largely unvaccinated, against 2,024 conventional controls across five European countries.¹² Children who had received MMR vaccination showed an increased risk of rhinoconjunctivitis, the clinical term for hay fever. Children who had experienced natural measles, by contrast, showed a reduced risk of IgE-mediated eczema. A 1999 Lancet paper by Alm and colleagues, comparing 295 anthroposophic children with 380 conventional controls, found that children who had never received MMR carried a reduced odds ratio for allergy in general.¹³
The literature is not univocal. Several mainstream reviews have found no association between vaccination and allergic disease, and a small number of studies have reported lower allergy rates in vaccinated children.¹⁴ The defenders of the schedule cite these findings as offsetting the positive studies. Several considerations weigh against treating the disagreement as a wash. The internal findings within the positive studies, the route-of-exposure contrast in Bernsen and the dose-response on timing in Bremner, are difficult to explain by confounding. The mechanism is established. The Japanese gelatin case is direct evidence of the mechanism operating in human children, with anaphylaxis appearing after the schedule change and disappearing after gelatin removal. The historical case from 1819 stands regardless of how the modern epidemiology shakes out: a disease that did not exist in the medical literature appeared, in a single generation, in the class that received the new procedure.
Broader catalogs of vaccinated-and-unvaccinated comparisons document the same pattern across multiple countries and investigators. Mawson’s 2017 cohort, the analyses compiled by Hooker and Miller in 2021, Lyons-Weiler and Thomas’s data from the Portland practice, Garner’s 2021 survey of more than a thousand unvaccinated American children, the Dutch NVKP 2006 data: each independent dataset converges on elevated allergic disease in the vaccinated.¹⁵ The aggregate weight of the evidence runs in one direction.
The convergence is acknowledged at the highest level of allergy organizations, though the implications are not. The World Allergy Organization reported in 2011 that the prevalence of allergic disease, with allergic rhinitis named explicitly among the conditions, was rising dramatically in both developed and developing countries.¹⁶ The increase was concentrated in children and in the previous two decades. The 2013 WAO White Book addressed the question of whether vaccination might be implicated. Its conclusion was that vaccination programs were essential and that the harms of denying them would exceed the costs of the allergy epidemic. The conclusion is the only statement in that section of the report that the authors do not reference.¹⁶ The WAO acknowledged the connection by raising it. They dismissed it without evidence.
Aluminum, Dose, and Asthma
The most recent of the establishment’s own findings on this terrain is the Daley study, published in Academic Pediatrics in 2022.¹⁷ The study was funded by the Centers for Disease Control and Prevention. Its authors included current and former CDC staff. Its data came from the Vaccine Safety Datalink, the CDC’s own pharmacovigilance system, covering seven large medical organizations.
The investigators followed 326,991 children born between 2008 and 2014. For each child, the cumulative aluminum exposure from vaccines received before age twenty-four months was calculated in milligrams. The outcome was persistent asthma diagnosed between ages two and five years, defined by the field’s tighter criteria: repeated clinical encounters plus at least two long-term controller medication dispenses.
The finding was a dose-response. For each one-milligram increase in vaccine-associated aluminum exposure before age two, the adjusted hazard ratio for persistent asthma was 1.26 in children with eczema and 1.19 in children without. Children who received three or more milligrams of vaccine-associated aluminum had a thirty-six percent higher risk of persistent asthma than children who received less than three milligrams.
The accompanying editorial, also in Academic Pediatrics, opened with the observation that “people only see what they are prepared to see.” The author called the findings “intriguing” while emphasizing that no determination of causation could be made from observational data. The CDC, in its public response, stated that it was “not changing the current routine childhood vaccination recommendations based on this single study.”
The Daley study did, as far as it could in an observational design, what the critics of all prior vaccine-and-allergy research had demanded. It used the CDC’s own data, the field’s tightest definition of asthma, a cohort of more than three hundred thousand children, and a continuous dose variable rather than a binary vaccinated-versus-unvaccinated comparison. The finding was a dose-response on aluminum, internal to the vaccinated population, by mainstream investigators publishing in a mainstream journal. The aluminum that Glenny had described in 1926 as boosting the body’s response to injected antigens is now documented, in a 2022 paper funded by the CDC, as boosting the body’s response to environmental antigens at a population scale. Hay fever and asthma belong to the same family of conditions; the aluminum that drives the asthma signal in the Daley cohort is the same aluminum that has been added to the schedule across the period in which hay fever has expanded.
What the Body Is Doing
The symptoms of hay fever are produced by the body, not by the pollen.
Daniel Roytas’s analysis of nasal secretions in respiratory illness documents what is actually found in the mucus.¹⁸ Histamine, bradykinin, prostaglandins, interleukins, cytokines, lysozymes, lactoferrin, hyaluronan, mucins, fibrinogen, immunoglobulins. These are the substances the mucous membrane releases when it encounters an irritant. Histamine produces nasal congestion, sneezing, and the throat irritation that pharmaceutical companies have spent a century selling drugs against. Bradykinin produces the same effects. Concentrations of bradykinin in nasal secretions during respiratory illness rise to thirty times normal levels.¹⁸
Both substances, when introduced into the airways of healthy volunteers, produce the symptoms of hay fever directly. No pollen is required. No allergen is required. The mucous membrane releases the inflammatory mediators when it is irritated, and the mediators produce the symptoms. The mediators are the body’s response. They are not the problem.
The body’s purpose in releasing them is documented. Histamine, bradykinin, and the other inflammatory chemicals in nasal mucus exist to expel material from the respiratory tract. The runny nose and the watering eyes that hay fever patients experience are the body’s mechanism for getting toxic material out. The symptom is the cleansing.
Roytas notes that medical papers have acknowledged the principle. Inhalation of non-infectious agents, irritants, allergens, chemicals, produces clinical illness indistinguishable from what the establishment calls infectious illness.¹⁸ The body responds to insult by mounting the same response, whatever the insult.
What hay fever sufferers are doing, when they take an antihistamine, is shutting down the mechanism by which the body expels the material it has reacted to. The chemical is retained. The membrane stays inflamed. The expulsion is suppressed. The reactive state is preserved.
What Medicine Says Is Happening
The official explanation for hay fever is that the body has made a mistake.
The mechanism, as the establishment presents it, runs as follows. A substance the body encounters, pollen or dust or dander or peanut protein, is identified by the body as harmful when it is in fact harmless. The body produces a specific protein, an immunoglobulin called IgE, in response to this misidentification. The IgE binds to receptors on cells called mast cells, located in connective tissue. When the body encounters the same substance again, the IgE on the mast cells signals them to release histamine and other inflammatory mediators. The mediators produce the symptoms.
Lester’s analysis identifies what is missing from this account.¹⁹ The roles of IgE and mast cells, as Lester documents, remain poorly understood by the establishment’s own admission. The protein medicine calls IgE has not been purified from human serum and characterized directly. It is inferred from laboratory tests that detect binding behavior, not from direct observation. What the antibody is, what it does, and whether the conventional account of its function corresponds to anything real in the body are questions the field treats as settled by convention rather than by evidence.
The deeper problem is the circular logic of the underlying framework. The American College of Allergy, Asthma, and Immunology acknowledges that hay fever symptoms can be triggered by common irritants such as cosmetics, laundry detergents, pool chlorine, perfumes, and hair sprays.¹⁹ The British National Health Service’s list of common allergens includes medications and household chemicals. The NHS then describes these allergens as substances “generally harmless to people who aren’t allergic to them.”¹⁹ The argument is that the substance is harmful only to the body that mistakenly identifies it as harmful. The framework defines its terms in a way that cannot be falsified. Whatever the body reacts to is, by definition, a thing it should not have reacted to, and the reaction is, by definition, a mistake.
The substances in question are not harmless. They are chemicals. Many of them are documented toxins. The body is not mistakenly identifying them as harmful. The body is responding to them as harmful because they are harmful. The framework that calls this response a malfunction has rotated the arrow of cause and effect. The body is doing what bodies do when they encounter material they cannot tolerate. The doing is then labeled the disease.
What is added to the picture by the vaccination history is the explanation of why some bodies cannot tolerate these substances while others can. The Richet mechanism, as demonstrated by Bostock’s cases, by the diphtheria antitoxin reactions, by the Japanese gelatin admission, by the converging modern epidemiology, is that the sensitized body responds to substances the unsensitized body does not. The sensitization comes from injection. The substance the sensitized body subsequently reacts to is whatever happens to be present in the air, in the cosmetics, in the food, in the environment. The proximate trigger is incidental. The originating cause is the syringe.
Why It Manifests
The terrain framework provides the missing layer of explanation. Sensitization is the precondition that explains why a body responds at all. Sensitization alone does not explain why a particular body responds today and not yesterday, in June and not December, after this exposure and not that one.
John Tilden, writing in the 1920s, documented the chain that connects systemic toxic load to mucous membrane response.²⁰ The body, as Tilden described it, vents accumulated toxins through whichever route remains available. The mucous membranes of the nose are one such route. What medicine calls a cold is the elimination of accumulated toxin through the nasal membrane. Repeated colds, when the underlying toxic load is not addressed, lead to thickening of the membrane, then to ulceration, then to bony spurs, then to what is named hay fever. In Tilden’s words: “The cause is the same from the first cold to hay fever.”²⁰
Henry Bieler, writing in the 1960s, named the same sequence from the local end. Hay fever, Bieler observed, develops after atrophy of the nasal and sinus mucous membranes.¹⁹ The membrane that has been repeatedly inflamed, scarred, and depleted no longer functions as a protective barrier. It reacts to substances it would once have tolerated. As Bieler put it: “When there is no catarrhal state, there is no hay fever.”¹⁹
Herbert Shelton’s account closed the loop on what produces and perpetuates the catarrhal state.¹⁹ Inhalation of toxic chemicals such as volatile organic compounds, fragrances, household products, and industrial pollutants induces nasal irritation and inflammation. When the exposure continues, and when the body’s response is suppressed pharmaceutically, the acute inflammation becomes chronic. The chronic catarrh becomes the conditions filed under allergic rhinitis, hay fever, and chronic sinusitis. Shelton named catarrhal inflammation a crisis of toxemia.¹⁹
The integrated picture: injection produces sensitization. The sensitized membrane is reactive. The reactivity is manifested when the body’s toxic load reaches a threshold, when the inhaled trigger meets a membrane already depleted, when the seasonal pollen meets a system already at its limits. The vaccinated person carries the originating cause. The dietary toxemia, the household chemicals, the industrial pollutants, the modern environmental burden carry the proximate triggers. The membrane atrophies through repeated exposure and repeated suppression. The June pollen, the September ragweed, the cat dander, the perfume, none of these is the disease. They are what the sensitized and depleted system can no longer tolerate.
The terrain framework explains the variability. Some vaccinated children develop hay fever. Some do not. Some develop it at five, some at fifteen, some lose it in middle age. The sensitization is the underlying precondition. The manifestation depends on the cumulative state of the terrain: the diet, the chemical exposures, the stress load, the cumulative toxic burden. A body that was sensitized but whose terrain remained strong may not manifest. A body whose terrain weakens through accumulated insult will.
What the Treatment Does
The treatment for hay fever is, in every modality the establishment offers, the suppression of the response the body is mounting to deal with the situation.
Antihistamines block the histamine that the membrane is releasing to flush the irritant out. The histamine is retained. The membrane stays inflamed. The expulsion is suppressed. Corticosteroids deliver synthetic versions of the body’s own anti-inflammatory hormone at concentrations that override the body’s regulation, shutting down inflammation by chemical force. Chronic use of nasal corticosteroids produces, in turn, mucosal atrophy, recurrent infections, and the slow erosion of the membrane’s structural integrity. The acute response is suppressed and the underlying terrain deteriorates.
Allergen immunotherapy, the procedure marketed as allergy shots, completes the circle. Patients sensitized through injection are treated by repeated injection of the substance they were sensitized to, in escalating doses, with the goal of reaching a tolerance state. The procedure is the same procedure that produced the disease, applied as the cure. The Richet mechanism is acknowledged in the design of the treatment. The clinical category, the mechanism, and the treatment all rest on the same observation: that injection produces sensitization, that the sensitized body reacts to subsequent exposure, and that further injection can modulate the response.
What the treatment does not do is identify and remove what made the membrane reactive in the first place. The household chemicals, the industrial fragrances, the dietary toxic load, the pharmaceutical burden, the original vaccination history, none of these enters the clinical encounter. The patient receives a prescription. The next prescription follows. The acute symptom becomes chronic. The detailed sequence by which acute conditions are driven into chronic states through pharmaceutical suppression is developed in the essay on inflammation, where Shelton’s catarrhal chain runs to its full progression.²¹
The Hygiene Hypothesis
The establishment’s competing explanation for the modern rise in allergic disease is the hygiene hypothesis. The argument, first articulated by David Strachan in 1989, was that hay fever and the wider atopic conditions had risen because modern children encountered fewer microbes in early life, and that the resulting underdevelopment of the body’s regulatory capacity left them prone to misdirected reactions.
The hypothesis was built specifically to explain hay fever.³ Strachan’s original findings concerned birth order, family size, and socioeconomic status as predictors of hay fever risk. The hypothesis has been adjusted and extended in the decades since. It cannot account for the 1819 first appearance, when the affluent classes who developed the condition had less rather than more hygiene than the rural poor who did not. It cannot account for the Bernsen finding that pertussis encountered naturally protects against atopy while pertussis injected produces it. The hygiene hypothesis is a theory in search of a mechanism. The mechanism that fits the data is the syringe.
What Hay Fever Is
The documented sequence is the one this essay has traced. A disease that had no precedent in the medical literature appeared in London within a generation of the introduction of a new injection procedure, in the class that received the procedure. The mechanism by which injection of foreign protein produces sensitization was demonstrated in children injected with horse serum, was awarded the Nobel Prize in 1913, and is now the standard laboratory protocol for manufacturing allergic disease for study. The Japanese investigators conceded the mechanism in the case of DTaP and gelatin: schedule change produced anaphylaxis, gelatin removal stopped it. The animal-model literature shows that injected microbial preparations function as adjuvants for airborne allergens the animal would otherwise have ignored.
Modern epidemiology documents the convergent pattern. Vaccinated children with no family history of hay fever are ten times more likely to develop it than children who were never vaccinated. The dose-response on timing is internal to the schedule. The same bacterium, when injected, produces atopy that normal exposure does not. The most recent and methodologically rigorous of these studies, funded by the CDC, found a dose-response on aluminum specifically: each milligram of vaccine-associated aluminum increased the persistent-asthma risk in young children.
Whatever word a reader chooses for the documented sequence, coincidence, correlation, contributing factor, primary cause, the documentation exists. The records exist. The studies exist in the establishment’s own journals, by the establishment’s own investigators. The body is not malfunctioning. The body is responding to having had foreign protein inserted past every layer of its protective architecture by a procedure that promised protection and delivered sensitization. Hay fever is the response. The syringe is the cause.
Author’s Note
Hay fever is not treated here as an exception within the framework of allergic disease but as the originating case. The condition the establishment files under allergic rhinitis was the first disease for which the words allergy and anaphylaxis had to be coined. The vocabulary of modern allergy medicine was created in direct response to the reactions doctors observed in patients they had injected.
Where this essay cites establishment research, it uses the establishment’s terminology. IgE, mast cell, allergen, immune response. These terms appear in attributed register, as the constructs by which mainstream medicine accounts for what it observes. In the terrain framework that grounds the analysis, those constructs do not name confirmed biological entities. They name conventions of interpretation. The body does not attack itself. The body does not make a mistake. The body responds to having been sensitized and to having been continuously exposed to substances it cannot tolerate. The conventional account inverts cause and effect.
The remedy does not exist in the pharmacy. A body sensitized through injection, depleted through dietary toxic load, irritated through environmental chemical exposure, and suppressed through pharmaceutical intervention cannot be restored through additional intervention. The remedy is to stop the procedure that produced the condition and to begin the long process of detoxifying and rebuilding what has been damaged. Nothing here is medical advice. The intent is to provide the documented historical and clinical record that the conventional account of hay fever omits.
Explain It To A Six-Year-Old
A long time ago, before doctors started doing it, almost nobody got hay fever. Then doctors started giving people a shot in the arm. They thought the shot would keep people from getting sick. The shot put stuff into the body that the body had never seen before, and the body got confused.
When the body is healthy, it knows what belongs and what does not. It breathes in flowers and dust and grass and air, and it sorts them out fine. When the doctors put stuff straight into the arm with a needle, the body had to figure out what was happening without being able to use its usual ways of checking. So it started to react.
After the shot, some bodies started to get itchy and sneezy when they breathed in things that used to be fine. Pollen from grass, dust, pet fur. The body would say, wait, that looks like something I had to deal with before, when the doctor stuck the needle in. And it would start sneezing and the eyes would itch and the nose would run.
Hay fever is the body doing its job. It is trying to wash away things it thinks are dangerous. The runny nose washes things out, and so do the watering eyes, and the sneezing pushes things away.
Medicine usually gives people pills to stop the runny nose and the sneezing. The pills do not fix the problem. They just hide what the body is trying to do. The real problem is that the body was confused in the first place by the shot.
If you have hay fever, your body is not broken. Your body is working. It is reacting to something that scared it a long time ago.
References
¹ Bostock, J. (1819). Case of a Periodical Affection of the Eyes and Chest. Medico-Chirurgical Transactions, 10, 161–165; and Bostock, J. (1828). Of the Catarrhus Aestivus, or Summer Catarrh. Medico-Chirurgical Transactions, 14, 437–446.
² Maready, F. Crooked: Man-Made Disease Explained. Feels Like Fire, 2018.
³ Fraser, H. The Peanut Allergy Epidemic: What’s Causing It and How to Stop It. Skyhorse Publishing, third edition, 2017.
⁴ Richet, C. Nobel Lecture: Anaphylaxis, delivered 11 December 1913. Nobel Prize in Physiology or Medicine awarded for work on anaphylaxis.
⁵ Behring, E. von, and Kitasato, S. (1890). Ueber das Zustandekommen der Diphtherie-Immunität und der Tetanus-Immunität bei Thieren. Deutsche medizinische Wochenschrift, 16, 1113–1114; and von Pirquet, C., Schick, B. (1905). Die Serumkrankheit. Vienna: Franz Deuticke. Translated by Schick as Serum Sickness, Baltimore: Williams & Wilkins, 1951.
⁶ Nakayama, T., Aizawa, C., Kuno-Sakai, H. (1999). A clinical analysis of gelatin allergy and determination of its causal relationship to the previous administration of gelatin-containing acellular pertussis combined with diphtheria and tetanus toxoids. Journal of Allergy and Clinical Immunology, 103, 321–325; Kuno-Sakai, H., Kimura, M. (2003). Removal of gelatin from live vaccines and DTaP — an ultimate solution for vaccine-related gelatin allergy. Biologicals, 31(4), 245–249.
⁷ Weibel, R.E., Woodhour, A.F., Stokes, J., Metzgar, D.P., Hilleman, M.R. (1967). New Metabolizable Immunologic Adjuvant for Human Use: Evaluation of Highly Purified Influenza-Virus Vaccine in Adjuvant 65. New England Journal of Medicine, 276, 78–84; Hilleman, M.R. (1966). Critical appraisal of emulsified oil adjuvants applied to viral vaccines. Progress in Medical Virology, 8, 131–182.
⁸ World Health Organization Scientific Group on Immunological Adjuvants. Immunological Adjuvants: Report of a WHO Scientific Group. WHO Technical Report Series No. 595, Geneva, 1976.
⁹ Enriquez, R., Addington, W., Davis, F., Freels, S., Park, C.L., Hershow, R.C., Persky, V. (2005). The relationship between vaccine refusal and self-report of atopic disease in children. Journal of Allergy and Clinical Immunology, 115(4), 737–744.
¹⁰ Bremner, S.A., Carey, I.M., DeWilde, S., Richards, N., Maier, W.C., Hilton, S.R., Strachan, D.P., Cook, D.G. (2005). Timing of routine immunisations and subsequent hay fever risk. Archives of Disease in Childhood, 90, 567–573.
¹¹ Bernsen, R.M.D., Nagelkerke, N.J.D., Thijs, C., van der Wouden, J.C. (2008). Reported pertussis infection and risk of atopy in 8- to 12-yr-old vaccinated and non-vaccinated children. Pediatric Allergy and Immunology, 19(1), 46–52.
¹² Flöistrup, H., Swartz, J., Bergström, A., Alm, J.S., Scheynius, A., et al. (2006). Allergic disease and sensitization in Steiner school children. Journal of Allergy and Clinical Immunology, 117(1), 59–66.
¹³ Alm, J.S., Swartz, J., Lilja, G., Scheynius, A., Pershagen, G. (1999). Atopy in children of families with an anthroposophic lifestyle. Lancet, 353(9163), 1485–1488.
¹⁴ For mainstream reviews finding no association or protective effects, see Grüber, C., Lau, S., Sommerfeld, C., Wahn, U. (2002), and Nilsson, L., Kjellman, N.I., Björkstén, B. (2003). The aggregate analysis sits within ongoing methodological dispute over case ascertainment and confounding by socioeconomic and care-seeking variables.
¹⁵ Kennedy, R.F., Jr., and Hooker, B.S. Vax-Unvax: Let the Science Speak. Skyhorse Publishing, 2023. The original studies catalogued therein include Mawson et al. (2017), Hooker and Miller (2021), Lyons-Weiler and Thomas (2020), Garner (2021), and the Dutch NVKP 2006 dataset.
¹⁶ Bailey, M. The Final Pandemic: An Antidote to Germ Theory. Independently published, 2023. Citing World Allergy Organization, White Book on Allergy: Update 2013; and Pawankar, R., Canonica, G.W., Holgate, S.T., Lockey, R.F., editors, WAO White Book on Allergy, World Allergy Organization, 2011.
¹⁷ Daley, M.F., Reifler, L.M., Glanz, J.M., Hambidge, S.J., Getahun, D., Irving, S.A., Nordin, J.D., McClure, D.L., Klein, N.P., Jackson, M.L., Kamidani, S., Duffy, J., DeStefano, F. (2023). Association Between Aluminum Exposure From Vaccines Before Age 24 Months and Persistent Asthma at Age 24 to 59 Months. Academic Pediatrics, 23(1), 37–46.
¹⁸ Roytas, D. Can You Catch a Cold? Untold History and Human Experiments That Challenge the Theory of Viral Contagion. Humanley, 2024.
¹⁹ Lester, D., and Parker, D. What Really Makes You Ill? Why Everything You Thought You Knew About Disease Is Wrong. Independently published, 2019. Citing Bieler, H. Food Is Your Best Medicine; and Shelton, H. Natural Hygiene: Man’s Pristine Way of Life.
²⁰ Tilden, J.H. Toxemia Explained: The True Interpretation of the Cause of Disease. Originally published 1926; reprinted FQ Classics, 2007.
²¹ Unbekoming. What Is Inflammation? Substack essay.
Additional Sources
What Is Inflammation? The acute-to-chronic suppression chain described in this essay, the trajectory from catarrhal response through pharmaceutical suppression to chronic disease, is developed in full in the inflammation essay.
What Is Asthma? The atopic disease that sits beside hay fever in the modern epidemiology, with the strongest vaccinated-and-unvaccinated signal in the literature.
What Is Eczema? The third member of what the establishment calls the atopic triad, with the same originating mechanism and the same modern epidemiology.
Maready, F. Crooked: Man-Made Disease Explained. The book-length treatment of the historical case for vaccination as the originating cause of allergic disease, including the Bostock chronology and the diphtheria antitoxin documentation.
Fraser, H. The Peanut Allergy Epidemic. The book-length treatment of the modern allergic disease epidemic, including the Richet mechanism and the Japanese gelatin admission.
Kennedy, R.F., Jr., and Hooker, B.S. Vax-Unvax: Let the Science Speak. The compilation of vaccinated-and-unvaccinated comparison studies cited in Movement 3.
Miller, N.Z. Critical Vaccine Studies: 400 Important Scientific Papers Summarized for Parents and Researchers. The compilation that catalogs the Enriquez, Bremner, Bernsen, Flöistrup, and Alm papers among many others.
Bailey, M. The Final Pandemic: An Antidote to Germ Theory. The terrain-framework treatment that documents the WAO admissions and the broader vaccine-allergy literature.
The Vaccines and Related Biological Products Advisory Committee (VRBPAC), which reviews scientific data on the safety and effectiveness of vaccines and other therapeutics on behalf of the U.S. Food and Drug Administration (FDA), voted 9-0 in dual votes to recommend approval of the vaccine for the 50-64 and 65-plus age groups.
Today’s votes took place after several hours of presentations based on the findings of Moderna’s Phase 4 clinical trial data for its mRNA-1010 vaccine. The trial compared the efficacy of mRNA-1010 to that of a conventional, non-mRNA flu vaccine.
Daniel O’Connor, founder and CEO of TrialSite News, told The Defender today’s favorable votes “may reflect the committee’s view that the benefit-risk profile is acceptable.” However, the vote “does not erase the fundamental concerns surrounding this application.”
“Significant questions remain about comparator selection, study design and whether the reported efficacy advantage represents a clinically meaningful improvement for patients or simply a statistical advantage within the framework of the trial,” O’Connor said.
According to an FDA briefing document prepared in advance of today’s meeting, “no major deficiencies were identified” with the vaccine for adults 50 and over. Citing the clinical trial data, the document states that the mRNA-1010 vaccine had a 26.6% relative efficacy rate in adults 50 and over, with similar rates for adults 65 and up.
The mRNA-1010 vaccine also showed a higher immune response than Sanofi’s Fluzone vaccine, the document noted. According to Fierce Biotech, these results met all of the FDA’s “pre-specified criteria for success” and bolstered Moderna’s application for approval.
Karl Jablonowski, Ph.D., senior research scientist for Children’s Health Defense, said today’s vote shifts mRNA-1010 safety monitoring to after licensure.
“VRBPAC meetings proceed to the beat of the rubber stamp. The unanimous vote guarantees a lot of really good questions of harm will have to be answered in the post-marketing period, when that harm manifests in the population,” Jablonowski said.
Moderna seeks traditional approval for the mRNA-1010 vaccine for the 50-64 age group and accelerated approval for the 65-plus age group.
Fierce Biotech reported that the FDA uses VRBPAC meetings to “seek outside counsel on tough or high-profile regulatory decisions.”
The FDA will make an approval decision on mRNA-1010 by Aug. 5 — and while the agency is not bound to VRBPAC’s votes, it “often follows the opinions” of its advisory committees.
Moderna’s stock was up over 4% in trading immediately after the vote, and up 3.50% at the close of market.
mRNA vaccine had higher rate of adverse events than conventional flu shot
According to MedPage Today, all current flu vaccines are “manufactured using egg-based, cell-culture based, or recombinant production technologies” — a production process that could result in “egg-adaptive mutations” and which makes it slow to reformulate vaccines when they don’t match currently circulating flu strains.
In their briefing document, FDA scientists suggested that “high-volume manufacturing” of a flu vaccine “capable of rapid strain reformulation is … needed.”
However, the briefing document did identify some concerns with mRNA-1010. FDA scientists noted the higher rate of solicited adverse events among clinical trial participants who received mRNA-1010 — and the higher number of unspecified deaths and serious adverse events related to anemia or urinary tract infections.
The document also noted that “efficacy in immunocompromised individuals and very frail older adults has not been established” — which is “significant because these populations face the highest absolute risk of severe influenza-related complications and may respond differently to mRNA-based vaccine platforms.”
Several experts told The Defender that Moderna’s mRNA-1010 vaccine poses risks. “Throughout the study, solicited adverse events are almost, and in some cases more than, double that of the comparator,” Jablonowski said.
The briefing document acknowledged a higher rate of solicited adverse reactions for mRNA-1010 vaccine recipients than among the conventional flu vaccine recipients. According to the Association of Health Care Journalists, solicited adverse events are “those that the trial investigators specifically ask participants about because they are either expected or likely based on known reactions to other vaccines.”
Unsolicited (unexpected) adverse events, serious adverse events, adverse events of special interest and deaths “were balanced between treatment groups,” and “no cases of myocarditis or pericarditis were identified within 42 days postvaccination,” the document states.
Immunologist and biochemist Jessica Rose, Ph.D., said this period is too small to detect long-term risks. “There is no way to know what the long-term adverse events will encompass,” she said.
Dr. Angus Dalgleish, professor emeritus of oncology at City St. George’s, University of London, said, “There is no need for any specific flu vaccine.” He cited the high number of serious adverse events related to the mRNA COVID-19 vaccines.
“The case for mRNA gene therapies for any infectious disease can never be approved with current technology, given the totally unacceptable serious side effect risks,” Dalgleish said.
Rose agreed. She said that since mRNA-1010 is based on the same “flawed” platform as the COVID-19 shots, she anticipates “exactly the same problems as for the COVID shots, as per the millions of reported adverse events to pharmacovigilance databases.”
FDA glosses over safety concerns
These concerns are similar to those expressed when Moderna first filed its application for licensure in December 2025 and which contributed to the FDA declining to review the company’s application in February.
In a “refusal-to-file” letter signed by Dr. Vinay Prasad, then-director of the FDA’s Center for Biologics Evaluation and Research, which oversees vaccines, the agency cited Moderna’s failure to perform an “adequate and well-controlled” clinical trial and its failure to use the “best-available standard of care” during the trial process.
In February, STAT reported that Prasad overruled senior FDA vaccine reviewers, who were ready to review Moderna’s application. However, Andrew Nixon, a spokesperson for the U.S. Department of Health and Human Services, told STAT at the time that the claim was “categorically false.”
In response to Moderna’s claim that mRNA-1010 had a 26.6% higher relative efficacy rate than the existing Fluzone vaccine, former pharmaceutical research and development executive Sasha Latypova wrote on Substack that this is significantly lower than the 95% relative efficacy claimed for the mRNA COVID-19 vaccines during Phase 3 clinical trials.
Jablonowski told The Defender in February that the mRNA-1010 clinical trial data show that mRNA recipients had a 329% higher chance of sustaining a serious adverse event and a 278% higher chance of experiencing an unsolicited adverse event — referring to a condition that was not expected or previously known.
However, the FDA’s briefing document found that mRNA-1010’s safety profile was “acceptable for the intended population” and that there was no causal relationship between the vaccine and the unspecified deaths and cases of anemia and urinary tract infections identified during the clinical trial.
The document said these adverse events are “unlikely to represent a vaccine safety signal” and that the risk of rare adverse events should be tracked through post-licensure monitoring.
But according to Jablonowski, conventional flu vaccines have shown they have negative efficacy — placing the vaccinated at higher risk of flu than the unvaccinated. He said this makes any comparison between the candidate mRNA vaccine and existing vaccines invalid.
“If the current flu vaccines have negative efficacy, a placebo would be more efficacious. … In the 2024-2025 season, the Cleveland Clinic found a negative 27% efficacy,” Jablonowski said.
‘They’re promoting the platform’
The FDA’s decision to decline review of Moderna’s application led to an uproar within the pharmaceutical and public health spheres. Within two weeks, the FDA accepted the company’s application for licensure of mRNA-1010. Leadership shake-ups at the FDA soon followed.
Some experts suggested that political pressure — and corporate lobbying — contributed to the FDA’s about-face.
Blackstone, a New York-based investment firm, is the world’s largest alternative assets manager, with a portfolio exceeding $1 trillion. In 2024, the company launched an ongoing, $750 million investment in Moderna, explicitly to support the development of its mRNA flu shot.
Aside from its financial might, Blackstone is also closely connected to the Republican Party and the Trump administration, through significant donations from its executives and employees and through its ties with prominent lobbying firms linked to Republicans — and Big Pharma.
In turn, Blackstone’s CEO and co-founder, Stephen A. Schwarzman, has close ties to President Donald Trump and his administration, while members of Blackstone’s Life Sciences division have ties with several vaccine makers, including Pfizer.
In a post on X, Max Bayer, a science reporter with Endpoints News, noted that today’s meeting included the participation of a non-voting pharmaceutical industry representative and that “no waivers were issued for conflicts of interest.”
Rose suggested that these moves signal a desire on the part of the FDA to continue promoting mRNA vaccine technology.
“They’re promoting the platform,” Rose said. “People who acknowledge risk who oppose using an unsafe and ineffective platform are a problem for the industry players aligned with pushing this technology forward.”
A journalist from The Guardian recently contacted me for a comment on vaccine-related studies I have previously cited in my work. The publishers of these studies have decided—years after publication—that these studies were so flawed and “dangerous to public health” that they needed to be retracted or investigated. The journalist wanted to know if I would amend my book and my recent ACIP presentation now that these studies were under attack.
My response:
“I welcome the media noting the targeted assassination of articles that do not fit the religious belief of vaccine proponents; this is also exemplified by the media’s lack of interest in the hundreds of other articles, reviews, and trial documents from my book and ACIP presentation which make plain that the claim vaccines are ‘safe and effective’ is not supported by the available evidence.”
So which studies are under fire? You won’t be surprised that they are on some of the biggest hot-button topics when it comes to vaccine injury:
2. RETRACTED: Hepatitis B Vaccination of Male Neonates and Autism Diagnosis, NHIS 1997–2002 (Carolyn Gallagher & Melody Goodman, 2010). This paper was published sixteen years ago. Sixteen years. And only now was it retracted after the publisher claimed that “due to fundamental methodological flaws the study’s conclusions are unsound.” The authors stand behind the study and noted “many of the recent criticisms of the paper are consistent with what we recognized and noted at the time.”
Behind each of these attacks is a plain desire to wipe from the record any evidence of vaccine harm and to chill the publication of any future studies that report vaccine harm.
Every scientist who values scientific integrity should publicly denounce these tactics. Anything less is not science. It is ideology.
Controversy over a BMJ paper examining excess mortality trends during the COVID-19 pandemic remains unresolved more than two years after publication, Steve Kirsch reported on Substack.
Dutch researcher Saskia Mostert, M.D., Ph.D., led the study, which was published in BMJ Public Healthin May 2024.
Mostert’s team analyzed excess mortality data from 47 Western countries and reported that elevated death rates persisted through 2022 and 2023 despite the end of pandemic restrictions and the widespread availability of COVID-19vaccines.
The authors argued that the findings warranted further investigation into potential contributing factors, including pandemic-era policies, healthcare disruptions and mass vaccination programs.
The paper was attacked on PubPeer and Retraction Watch, two platforms that have become the driving force behind many recent retractions of peer-reviewed scientific papers whose findings challenge the mainstream narrative on vaccines, COVID-19 treatments and aluminum, among others.
Critics did not dispute the paper’s core findings that excess mortality was high and remained elevated in many Western countries during the study period. Instead, they criticized the paper’s discussion of the COVID-19 vaccines, saying it implied there was a causal link between the shots and excess death and encouraged readers to infer causation.
Several critics called for the paper to be retracted.
In response to these and other mainstream criticism of the paper, BMJ Public Health issued a statement saying that media reports had misrepresented the findings. However, in mid-June 2024, the journal stamped the article with an “expression of concern.”
The journal said its “integrity team and editors” were investigating issues “regarding the quality and messaging of this work.” It also said the Princess Máxima Center, where three of the four study authors were based, was investigating the study.
BMJ Public Health added that the study does not support the claim that vaccines are a major contributor to excess deaths.
The BMJ typically waits for the home institution’s findings before taking action, according to Kirsch. He said the Princess Máxima Center hasn’t yet sufficiently explained what was wrong with the study.
BMJ updated the expression of concern in January 2025, stating that it was awaiting the findings and that the institution had no update regarding when the information would be sent. The Princess Máxima’s website says the investigation is “complete but not yet finalized.”
“After more than two years, the ‘issues’ with the paper have not been revealed,” Kirsch wrote. He said that the center’s investigation revealed that the data and methodology are real and the authors committed no fraud.
“The institution just didn’t like the political implications of being associated with a paper that called the safety of the COVID vaccine into question.”
Princess Maxima Center did not respond to The Defender’s request for comment.
Study used proper methods, reported valid findings
All-cause mortality expert Denis Rancourt, Ph.D., told The Defender that the authors conducted their analysis, “using a correct method and without error.”
“Those results are robust and are corroborated and expanded upon by others,” Rancourt said. All-cause mortality is an important metric that is valid regardless of different opinions about what drives that mortality, he added.
Rancourt said the researchers discussed their results in relation to a broad range of published studies.
The push for retraction was based on how the media and social media commenters interpreted the discussion — not based on what the authors actually did in the paper.
“This is a regressive reason to start unpublishing papers,” he said, adding:
“The large industry of unpublishing shows that our society has moved away from independent thought (intellectual literacy) and towards excessive reliance on the pronouncements from high-status sources. I include scientists themselves in the said society.”
All-cause mortality identified in the paper ‘unprecedented and raises serious concerns’
The original paper showed that excess mortality in 2020 was documented in 41 of the 47 countries the authors analyzed. Over the next two years, that number increased to 42 and 43 countries in 2021 and 2022, respectively.
Overall, there were 3,098,456 excess deaths from Jan. 1, 2020, to Dec. 31, 2022, with just over 1 million of those occurring in 2020.
“This is unprecedented and raises serious concerns,” said researchers, who analyzed all-cause mortality reported in the Our World in Data database.
“In 2021,” they wrote, “the year in which both containment [i.e., lockdown] measures and COVID-19 vaccines were used to address virus spread and infection, the highest number of excess deaths was reported: 1,256,942 excess deaths.”
They reported that in 2022 — “the year in which most containment measures were lifted and COVID-19 vaccines were continued” — there were 808,392 excess deaths.
The authors pointed out that during the pandemic, politicians and the media emphasized: “on a daily basis that every COVID-19 death mattered and every life deserved protection through containment measures and COVID-19 vaccines.”
“In the aftermath of the pandemic, the same moral should apply,” the authors said. “Every death needs to be acknowledged and accounted for, irrespective of its origin.”
The authors called for government transparency in cause-of-death data so researchers can do “direct and robust analyses to determine the underlying contributors.”
This also means that autopsies need to be done to determine the exact reason for death, they added.
The authors noted that the data they analyzed may not have recorded all actual deaths because “countries may lack the infrastructure and capacity to document and account for all deaths.”
Record-keeping mishaps or delays may also cause deaths to go unrecorded.
The following is taken from Vernon Coleman’s long-term no 1 bestselling book `Anyone who tells you vaccines are safe and effective is lying: Here’s the Proof.’ Dr Coleman has for decades been the world’s leading medically qualified critic of vaccination programmes. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.
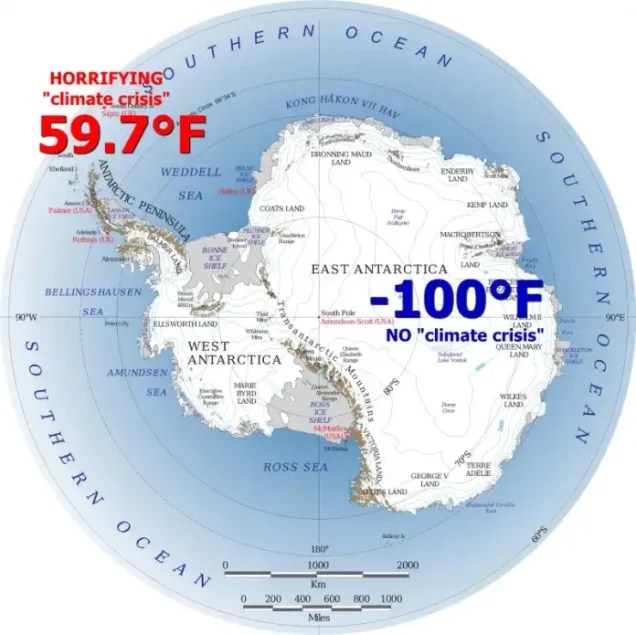
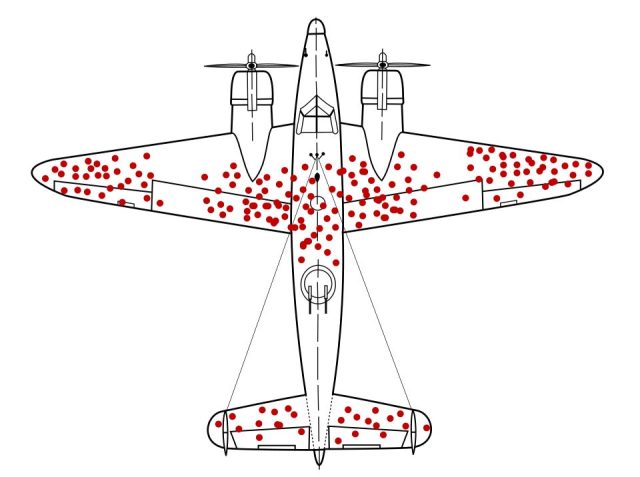

 Aletho News
Aletho News
{kind=link}