No state or security body offers a single, systematic account of how Israeli agents are used, why they are recruited, or what services they ultimately provide. Outside experienced state institutions, universities and research centers rarely undertake such scrutiny. Israeli academia is the notable exception.
Israeli universities form part of the wider intelligence ecosystem through research, graduates, and seminars conducted with the security services and military. They produce personnel, assess institutional performance – as they have done since Operation Al-Aqsa Flood – and examine intelligence work in detail.
The Second Annual Israeli Conference on Intelligence Studies, held at the Hebrew University of Jerusalem on 28–29 October 2025 under the title “Intelligence Transformations After Failure,” is one open example. No comparable body of work has emerged from Arab and Islamic institutions.
Accounts from current and former security practitioners, alongside cases involving agents both living and dead, reveal an intelligence pyramid: a layered system of recruitment, cultivation, and deployment built around the value of the intelligence sought and the risks demanded of each spy.
Level one: Building the picture
At the base of the pyramid is information gathering, a task common to almost every category of recruited agent, though the value and type of information vary widely. Israeli services generally separate the agent or cell collecting intelligence from the cell carrying out an operation. The roles sometimes overlap, but collection remains the gateway to action.
An agent may gather information during a probationary phase, without knowing what it will be used for or whether others are working alongside him, simultaneously or in sequence, inside or outside the same organization.
Then come the “mosaic collectors,” who move beyond isolated fragments. They, too, may not see the complete picture, but their assignments are more complex. Instead of passing a single detail or photograph, they may track a person’s movements and relationships in depth, or map an entire process, such as an organization’s purchase of motorcycles or communications equipment.
One recent Lebanese case involved a detainee later released by the judiciary despite the sensitivity of his alleged mission. According to security sources familiar with the file, he was instructed to mount specialized equipment on a vehicle and drive through selected areas, harvesting data from internet routers in homes and institutions and attempting to penetrate them.
A second, recurring example comes from Palestine: the penetration of external training chains. Trainees sent to courses in Lebanon, Syria before the government’s fall, and Iran before the war on Gaza were exposed.
At times, the training bodies themselves were compromised and discovered concealed cameras in equipment covers. The breach then operated at three levels – inside the organization, along the training chain, and within the host institution.
Higher up are agents with access to sensitive files or influence inside a faction’s military or security apparatus. Their task may be to construct a picture of a company, battalion, brigade, division, or specialist unit. No single member normally sees an entire arena or organization; that degree of access is usually confined to a political bureau, military, or jihadi council.
One battalion in northern Gaza was penetrated before the current war, specifically in 2021. The agent held considerable authority and ranked roughly third in its command structure, yet still lacked a complete map of the battalion’s tunnels.
Israeli handlers therefore supplied him with military boots resembling those worn by resistance fighters. A tracking device was hidden inside, and he was told only to walk through the tunnels, allowing Israel to chart the network.
After the breach was discovered – having paralyzed operations in that area during the Sword of Jerusalem battle – the agent fled to Europe. A counterintelligence operation later lured him back to Gaza by making him believe suspicion had passed.
He was arrested, and the source of the breach was exposed. Security sources inform The Cradle that the discovery spared the battalion from destruction in the latest war and helped turn the border area into a persistent problem for Israeli forces until the final stages.
The battalion commander responded through trial and error, creating separate tunnel routes and branches and preventing any one fighter from moving through all of them or taking part in the entire excavation process.
Yet the same agent escaped prison shortly before Operation Al-Aqsa Flood. That extraordinary story lies beyond the scope of this investigation, though one detail is telling: another agent facilitated his escape.
At the top of this first level stands the source of “golden information” – intelligence decisive to a major operation, particularly an assassination. It may reveal a figure who has never been photographed, identify a safe house, or confirm a target’s presence during the final moments before a strike.
Some such agents have been killed by mistake; others, sources say, were deliberately abandoned when Israel judged that they had nothing more to offer or could not be extracted.
Technology has made field agents harder to detect and reduced the need for some older practices. At the beginning of the Second Intifada, for example, agents could be ordered to mark a building with a laser before an airstrike.
Such tasks are less necessary today because Israel already possesses extensive maps of public bodies – municipalities, governorates, and ministries – as well as many overt and covert resistance sites.
Israeli military publications openly use the Hebrew term yediat zahav – “golden information” – for decisive, current intelligence extracted from a mass of raw data. In resistance environments, invoking such intelligence can also fuel suspicion that a senior agent exists, even when the information was obtained through technical surveillance.
Where the source is human, investigations repeatedly show that an Israeli service may spend years and large sums cultivating one person for a single disclosure. The assassination of Yahya Ayyash is a prominent example.
The collaborator who enabled the operation was bound to be exposed because he supplied both the identifying information and the instrument of assassination – a booby-trapped mobile phone. With no plausible alternative suspect, an escape or extraction plan had to be prepared in advance.
Level two: Agents in the field
Information gathering already demands work on the ground – photography, surveillance, communications, and impersonation among them. Direct field missions require a different class of agent. Security sources estimate that nearly all must meet their handlers inside Israel or abroad and receive either task-specific instruction or broader operational training.
At the bottom are what security practitioners describe as “cheap missions”: assignments carrying minimal risk, with exposure more likely to result from chance or a basic mistake than from the work itself. These include leaving communications devices, messages, or cash at “dead drops.” Such tasks usually require little training and are assigned gradually.
A dead drop is selected after studying a country’s geography and population patterns. One agent leaves the material; another retrieves it without knowing the first and sometimes for an entirely different operation. Many recruits with reasonable collection skills can perform these tasks. They remain below the risk threshold reserved for more experienced and intensively trained agents.
The next rung involves logistics. This involves obtaining communications equipment, buying or renting homes and vehicles, or securing other tools later used by operational cells.
From there, the work can become far more dangerous. Agents may tamper with resistance weapons or insert tracking chips into them, including RPG and Kornet anti-armor rounds and even missiles or their explosive warheads. Others plant surveillance devices. At this point, the agent generally understands exactly what the mission entails.
In one prominent example, a single agent working in a manufacturing workshop belonging to an Islamic organization in Gaza was responsible for the deaths of at least 30 operatives between 2008 and 2012 by planting tracking devices in the rockets they launched, as well as weakening the explosive material in the warheads.
Having joined from another organization, he cultivated an image of exceptional devotion to deflect suspicion, even carrying wounded comrades on his shoulders while performing tawaf around the Kaaba.
Although eventually exposed, he escaped Gaza and, according to the same sources, still holds an official post in a Muslim-majority country.
At the summit are the hardest assignments: planting explosives or carrying out assassinations directly. Israel embraced this route only more extensively during the past decade. For years, a basic assumption among Palestinian and Lebanese investigators held that Israel killed only by Israeli hands. That premise often led inquiries to discount a local perpetrator from the outset.
The 2010 assassination of Hamas commander Mahmoud al-Mabhouh in Dubai reinforced that belief. The large team seen on Emirati surveillance footage used foreign passports; many were believed to be Jewish. But subsequent cases in Gaza, Lebanon, Syria, and Iran indicate that Israel has sought to reduce the risks borne by Jewish operatives, Arabic-speaking Israeli agents, and Druze or Bedouin recruits by transferring more of the execution phase to local assets.
The March 2017 assassination of freed prisoner Mazen Fuqaha in Gaza exposed the limits of the old assumption. Fuqaha, a commander in the Qassam Brigades, was responsible for supporting military activity in the occupied West Bank. Investigators faced a missing link. Even after a Palestinian agent confessed, some remained convinced that an Israeli special unit must have entered Gaza to carry out the shooting.
Nearly nine years later, on 5 February 2026, Netanyahu publicly acknowledged Israel’s responsibility for Fuqaha’s assassination. He confirmed that the killing was carried out through recruitment of a Palestinian collaborator, Ashraf Abu Leila, who shot Fuqaha outside his home in the Tel al-Hawa neighborhood in Gaza City.
The disclosure was unlikely to have been casual. Its timing came as Palestinian resistance movements were conducting sweeping reviews of their security and military performance after Operation Al-Aqsa Flood.
The following day, Al Jazeera broadcast an investigation into armed groups in Gaza accused of serving Israel.
The program included material on local militia members used to track targets and carry out armed tasks. One case involved two men assigned to kill a wanted figure with a suppressed weapon. One was captured despite having received little training and not being a long-serving recruit – another departure from the model that prevailed before Operation Al-Aqsa Flood.
During Israel’s June 2025 war on Iran, Israeli messaging sought to portray every ground operation as the work of Mossad officers. Field investigations and sources following the cases point to a different picture. Iranian Jews living abroad, migrants, and their descendants accounted for only a small share of those allegedly involved.
Many of the operatives proved to be residents of Iran, meaning Mossad personnel had not acted alone as Israeli accounts implied. Some people who helped smuggle equipment into the country reportedly did not know it would be used in military or intelligence operations, believing they were moving civilian goods for profit.
Level three: Re-engineering the enemy
At the highest level, the selection, conduct, and mission of an agent change fundamentally. Israel studies a target organization strategically, seeking to dismantle it or redirect its course. The work demands highly placed, carefully cultivated recruits. An assignment may involve reading a leader’s behavior or tracing ideological currents across an entire movement.
One agent admitted during interrogation that his task had been limited to observing a leader’s social life and political language. He was required to remain close to a figure in an Islamic organization in Gaza who was assassinated in 2003, mapping his community relationships, recording what he said away from the media, and assessing whether he belonged to the movement’s “hawk” or “dove” camp. The findings helped determine Israel’s targeting priorities.
Past Israeli statements and signals support the view that assassinations, particularly of political figures, are not always ordered for immediate military reasons. A killing can create a vacancy in a movement’s hierarchy.
Israeli planners then anticipate who will fill it and whether that successor better suits their objectives. In effect, an organization’s political trajectory can be re-engineered while its members believe they are responding to internal circumstances.
The practice is old. It dates at least to the rivalry between Fatah and the Popular Front for the Liberation of Palestine (PFLP). This was a time when Israeli services sought to exploit disputes within and between Palestinian factions and used agents to deepen them.
During periods of intense military escalation, anyone who appears on the radar may be killed as Israel pursues the largest possible number of assassinations. The campaign unleashed after Operation Al-Aqsa Flood marked the largest exception of all.
The US has played a comparable game, sometimes without recruiting a conventional agent. Former CIA officer John Kiriakou described one such method in a podcast released on 29 January 2026, explaining how the agency helped fragment the Abu Nidal Organization.
Unable to penetrate the group directly, the CIA instead planted suspicion. Through direct and indirect contacts, it suggested that a senior member had been recruited. One cadre then killed another on suspicion of betrayal, setting off further internal bloodletting.
The organization was thus driven to destroy itself without the recruitment of a single agent. Its founder, Sabri Khalil al-Banna, better known as Abu Nidal, died in Baghdad in 2002. The author’s security sources maintain that Saddam Hussein had him killed after years of using his organization in external and internal operations, though the circumstances remain disputed and other accounts describe suicide.
A different strategic path requires elevating an agent into the leadership. That person needs achievements to build credibility, even if Israel must allow an operation to appear successful – or announce casualties in its own ranks – to manufacture the necessary record.
A source in Fatah’s Al-Aqsa Martyrs Brigades reveals to The Cradle that an operative identified as A.N. rose rapidly after an Israeli jeep was apparently destroyed by an explosive along the boundary and Israel announced one death and several injuries. A later transaction involving night-vision equipment exposed him, and he fled into the territories occupied in 1948.
The subsequent investigation found that the jeep had been remotely driven to the site of a bomb reported in advance. The explosion created a filmed “achievement,” giving the agent credibility, quicker access, and a degree of trust that was difficult to challenge.
Once an agent reaches the intended leadership tier, he may be ordered to identify additional cadres for recruitment. Another recurring task is to cultivate financial and moral corruption. The aim is to convince members that their sacrifices are being exploited for private gain. Such tactics work precisely because corruption already exists, to varying degrees, within the structures of several organizations.
One of the starkest cases uncovered by the Palestinian resistance involved a historic leader identified as M.N. He was reportedly not asked to transmit operational intelligence. Instead, his assignment was to magnify organizational failures and obstruct successful work.
Other agents were instructed to arrange commercial deals and partnerships that implicated people who were not directly recruited, widening the perception – and sometimes the reality – of corruption and exploitation.
The effort to create a negative example belongs to the same strategy. Israeli handlers may target the children of leaders whom they have failed to recruit or assassinate. Security pressures and the prolonged absence of a father who once acted as protector and disciplinarian can make those children more vulnerable. Families of martyrs face the same danger.
Palestinian and Lebanese files contain many such examples. The most politically embarrassing involve the sons of a well-known West Bank leader in an Islamic movement, one of whom publicly converted to Judaism and repeatedly entered Israel.
Whether he settled there permanently remains unclear. Such cases are rare, but Israel amplifies them to discredit the movements concerned, dishonor prominent families, and weaken their standing within Palestinian society.
The most dangerous outcome combines two tracks: assassinations designed to reorder an organization and the promotion of an agent into its senior leadership. Together, they open the way to direct influence over decisions and strategy. The danger is greatest after the killing of historic figures who cannot easily be replaced.
Israel’s intelligence services invest for the long term. They study the remaining leaders, their histories of disagreement, and the character of each relationship, then seek to create friction inside the organization. As sources familiar with these files put it, the intended result is to weaken effectiveness, waste effort, and expose structures.
That investment can consume enormous human resources. Specialists may spend a decade or more building a single subject’s biography – from his waking hour and favorite foods to his relationships and most closely guarded secrets.
In several cases, such intimate knowledge has ended in assassination. The spy’s service to Israel is therefore measured by more than the secret he steals or the device he plants. At its highest level, it lies in helping the occupation reshape an adversary from within, long before the target recognizes that its choices are no longer entirely its own.
The pandemic is over. Yet two key pieces remain that should concern everyone.
Lets talk about the COVID shot. Still being mandated (recommended) by East and West Coast Health Alliances comprising 14 states all the way down to infants.
Why? To stick it to Kennedy? To ‘follow the science’‘? To secure a market as demand tanks? Who knows for sure but here we are.
The COVID shot was birthed in fraud and failed science. That is the true legacy media pundits won’t tell you.
As the first cases of coronavirus happened in the U.S., Moderna and Pfizer began designing their mRNA vaccine candidates.
Meanwhile, Bill Gates pulled the trigger. A Fauci files/diary email from Gates to Fauci asks the NIAID director for “changes or additions” to Gates’ masterplan titled simply Pandemic I.
Gates’ document, given the stamp of approval from Fauci, stated:
“The goal is to pick the one or two best vaccine constructs and vaccinate the entire world—that’s 7 billion doses if it is a single-dose vaccine, and 14 billion if it is a two-dose vaccine.
How about 9-12 doses? That is what has been recommended to date for adults and immunocompromised respectively.
Far from a stranger, Gates and his foundation were fraudulently close to U.S. agencies funding pieces of NIH and receiving private briefings from DARPA on biological threats. More on that in another report.
FAUCI KILLS EARLY TREATMENT
Under Section 564 of the FD&C Act, FDA can grant the emergency use for a medical countermeasure (the vaccine) because, as revisionist history tells, there was no approved alternatives adequately available for diagnosing, preventing, or treating the disease.
The guidelines and experiences used at the start of the pandemic from pioneers like Peter McCullough’s protocol, New York family physician Dr. Vladimir Zelenko’s protocol, Texas Dr. Richard Bartlett nebulized budesonide, Front Line COVID-19 Critical Care Alliance’s ivermectin push and so many others using similar treatments with repeated success and real-world results tells a different story.
Evidence that would have effectively ended the FDA EUA vaccine hunt.
Didn’t matter to Fauci and the captured U.S. regulatory agencies. Their job was to kill those ideas and pave the way for the coming experimental, world-injecting gene therapy.
Fauci files/diary explains how it was done at the highest level. March 2020, two months into the first U.S. cases Fauci finds himself in a high-level White House Meeting and writes:
“A friend of POTUS… said that he heards [sic] that someone gave Hydroxychloroquine (HC) to 51 people and 51 got better. POTUS has heard similar stories, including Remdesivir (R) about other drugs and wants to make these available. To my amazement and dismay, Azar said that he could approve HC and Remdesivir now with the powers that he has. Steve Hahn and to some extent Deb and Bob started to chime in that this would give people hope. I took a deep breath and said that this was wrong and should not be done.”
None of the trials were designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor were the vaccines being studied to determine whether they can interrupt transmission of the virus. (*I was the first journalist to report this in October 2020)
FDA and VRBPAC votes were near unanimous to get them to market and in American arms while legacy media ‘journalists’ and their ‘experts’ like Fauci and others touted the shot’s transmission-stopping magical qualities. While Influencers and celebrities sucked up $911 million of taxpayer money for their injectable PR efforts.
There was just one problem. The shot didn’t stop transmission. And it didn’t perform against mutations. In short, it was worthless and gave false hope with a growing profile of side effects (harms).
September 2021 Fauci writes:
“… there is a concern about safety regarding myocarditis for younger people, mostly men; however, once this is taken care of in my mind there is no reason not to vaccinate essentially everyone.”
Heart damage from the shot was never “taken care of” and still remains a concern and risk to this day especially for young men.
January 2021, world-renowned HIV virus researcher Dr. David Ho shares immediate concerns about the COVID shot’s performance according to Fauci’s diary:
“David Ho is doing tests on convalescent sera and sera of people who were vaccinated and is finding disturbing data in both the UK and worse in the RSA mutants. It looks like the vaccine might be compromised.”
Fauci continues:
“Had regular every 2 weeks call with Bill Gates – Bill and Trevor Mundel know about the issue with the mutations that David Ho is working on.”
What exactly were Dr. Ho’s warnings? Dr. Ho writes to Fauci the following:
“It is quite clear that these two variants could now resist several classes of neutralizing monoclonal antibodies already used in the clinic or still in development, and in most cases we understand which of the mutations are conferring the resistance.”
Ho continues:
“… a large majority of convalescent plasma samples showed an appreciable loss in activity against the new variants, suggesting re-infection may be more likely when confronted with either of these two strains.”
And then the death blow to the non-transmission-stopping COVID shot as Ho writes:
“Finally, we also observed a significant impact on vaccinee sera in that every serum sample tested showed a substantial loss in neutralizing activity against the SA variant, whereas the loss in activity against the UK virus is not as large or as universal. Again, we believe the latter findings should be shared promptly with the field, because these new strains threaten the effectiveness of the current vaccines.”
The very next day, Fauci writes in his diary:
“Had Zoom briefing of Biden and Harris to prep them for the speech that Biden will give at 3:45 PM on the vaccine rollout plan. We briefed him at 2:30 to 3:30 and he and Harris (only he spoke) gave briefing to the Nation.”
No word of the vaccine issues, mutations or danger now scientifically evident.
It later became clear that Ho was not only right, but his warnings were mild compared to the reality that unfolded. UK COVID vaccine surveillance data began showing the shots were not only failing to prevent infection but they are making you more vulnerable to it.
2022 data suggested that in all age groups COVID vaccines were demonstrating negative efficacy. That means, the vaccinated were at greater risk of infection than the unvaccinated.
Meanwhile, that same year Fauci writes:
“More drama with regard to the CDC and Rochelle Walenski. After much going back and forth between the CDC and the other docs including me… we thought we had gotten them pulled back from making the statement that the vaccines were not effective at all in preventing infection and transmission…
Why? As Fauci writes, “it would undermine the DoJ’s efforts at mandates for vaccines under certain circumstances.”
In the end, CDC director at the time Walensky who, as Fauci writes, called him “… her hero, her mentor, her friend… agreed to pull back on the statement of absolute lack of efficacy of vaccines against infections and transmission.”
Throughout all this, Fauci went to bat for Big Pharma indemnity in 2021 as he pens in his diary:
“I had an important zoom meeting today with Larry Corey an Emilio Emini about the same subject as above, namely, how the United states can play a major proactive role in getting mRNA vaccines to the developing world. Apparently there are liability issues that the pharmaceutical companies are concerned with. These revolve around the fact that although the United States government can indemnify the companies against lawsuits here in the United states the companies feel that they are liable to being sued for adverse outcomes by people in the countries to whom they’re providing vaccine. Some mechanism needs to be worked out to address this concern.”
(Emilio Emini was Chief Executive Officer at the Bill & Melinda Gates Medical Research Institute and Larry Corey head of COVID-19 Prevention Network collaboration formed by Fauci)
The shot is still protected by the PREP Act which was extended until 2029 by outgoing HHS Secretary Xavier Becerra (now in the running for California Governor).
The Countermeasures Injury Compensation Program (CICP) meant to field harms from the COVID shot is a black hole and sick joke. Kennedy is attempting to create a table of accepted injuries to ease compensation efforts for the injured public. Is this enough? Not by a long shot.
(*No artificial intelligence was used to write this article. Just a genuine human… me)
The US Senate Homeland Security Committee has voted to hold Dr. Anthony Fauci in contempt after the former White House coronavirus czar refused to answer questions on the origins of Covid-19 at a hearing last week.
The Republican-led committee voted 8-7 along party lines to hold Fauci in contempt on Thursday. The committee’s Democrats introduced five motions aimed at postponing the vote, but all were shut down by the Republican majority.
Fauci appeared before the committee last Wednesday, where he was grilled on his role in funding dangerous gain-of-function research at the Wuhan Institute of Virology in China, his knowledge that Covid-19 was likely created in a laboratory, his work with US intelligence agencies, and his promotion of ineffective vaccines against the virus.
The former bureaucrat refused to answer any questions, invoking his Fifth Amendment right to silence more than 100 times. Fauci pleaded the Fifth despite having already received a pardon from former President Joe Biden shielding him from criminal prosecution over any offense committed between January 1, 2014 – when the US first outsourced gain-of-function research to China – and January 20, 2025.
“More than a million Americans died from Covid,” committee chairman Rand Paul said before Thursday’s vote. “Many of them died alone. Workers were forced to choose between a mandate and a job they needed. Businesses closed and never reopened. Americans lost the freedom to work, to worship, and to decide what went into their own bodies.”
“Dr. Fauci faced no risk of federal prosecution,” Paul continued. “All he had to do was tell the truth.”
Although Fauci is immune from prosecution for any misdeeds that he committed between 2014 and 2025, his pardon does not cover any crimes committed at last week’s hearing. Contempt of Congress is a criminal offense, and Paul referred Fauci’s case to the US Justice Department immediately after Thursday’s vote.
Should the department choose to prosecute, Fauci could face a fine of up to $100,000 and a prison sentence of up to 12 months.
Peter Navarro and Steve Bannon, both former aides to US President Donald Trump, were jailed for contempt of Congress by Biden’s Justice Department. Navarro and Bannon both spent four months in prison in 2024.
Fauci served as the director of the National Institute of Allergy and Infectious Diseases (NIAID) from 1984 to 2022, and as chief medical adviser to Biden from 2021 until his retirement in 2022. In the latter role, Fauci became the face of Biden’s heavy-handed response to the pandemic, advocating mask and vaccine mandates and lockdowns, and dismissing opposition to these measures as “anti-science.”
I followed up on this story, because some were sceptical and didn’t believe it was real or possible, and loudly insisted it was fake. One man who fancied himself an expert because he likes to shoot a gun now or then claimed this was fake, impossible.
First, I will say that Palestinians don’t need to create fake stories, Israel is doing the impossible to them every day and has been doing so for not only the last 3 years—even when I lived in Gaza, we’d see injured Palestinians and situations that didn’t seem possible but were very real—but certainly in the last three years of Israel’s ongoing genocide of Palestinians in Gaza, we’ve seen things that seemed impossible but were very, brutally, bloodily, real for Palestinians.
Second, a good friend of mine from Jabaliya told me he knew the man who filmed the video. I have no reason to believe he lied to me.
But for clarity on logistics of the situation— how this youth came to have a bullet in his hand when others said his hand would have been blown off (though I already guessed the answer)—I reached out to a couple of others I knew in Gaza. Dr. Ihab replied to me:
“This is a fallen shot, that is, it was fired from a long distance and fell. These shots caused the killing of many people: when the bullet settled in their neck and chest, it may be fatal. But in this case, it is easily removed by a short surgery. We hope that it has not caused fractures in the palm of the hand or tears in the tissues and nerves.”
He went on to say that his own friend was killed by such a stray bullet fired by an Israeli soldier, hitting the friend in his neck as he sat in a chair, killing him. “These may be from the Zionist machine gun or from drones, or the launches carried out by the army randomly.”
A journalist who had shared the initial photo also replied to me: “This child was sitting in a learning tent west of Gaza City. The bullet fell from the sky after being fired from the eastern part of Gaza City, where Israeli forces were positioned. Although it came from a considerable distance, it struck the tent and hit the child while he was seated at his school desk. Yes, it’s unbelievable, but in Gaza anything is possible.”
I refer back to Dr. Mimi Syed, who I interviewed a year ago. She went twice to Gaza as an emergency doctor, and one of the patients she was able to save, a young girl named Mira, had a bullet lodged in her head. “When I showed the CT image to the world, I was accused of fabricating it.”
Dr. Tarek Loubani, who I’ve known from Canada since before I first went to Gaza in 2008, likewise faced accusations that he had lied or forged an x-ray of one of his patients.
He didn’t lie or manipulate, of course, but people couldn’t accept that what it showed was real.
Israel has long treated Gaza as its testing ground for new weapons and technology and also for how much Israel can get away with while the world watches. If your immediate reaction at seeing an injury or seemingly impossible photo or video from Gaza is to accuse Palestinians (or non-Palestinians who managed to enter Gaza) of fabricating footage or x-rays, etc, then you are the problem. Your life experience shooting a gun in your back yard does not equip you to understand the circumstances in Gaza. Palestinians in Gaza don’t have the luxury of debating this, they’re living in truly unreal circumstances.
Israel has become a haven for international criminals. Many are dual-nationals who have taken advantage of their ability to move seamlessly between Israel and their second country of citizenship to commit crimes and, in some cases, evade justice.
The scale of the criminality, and the volume of cases (relative to the population of Israel), is astonishing.
Among the most notorious accused criminals being protected from justice by Israel is Timur Mindich, the ultimate financial beneficiary of the Ukrainian drone maker Fire Point. Mindich fled to Israel last year, just days before being charged as the mastermind behind a $100 million embezzlement scheme involving Ukraine’s state nuclear power company. Mindich also happens to be the co-owner of Kvartal 95 Studio, the production company founded by Volodymyr Zelensky.
Mindich, like many in this article, has taken advantage of Israel’s controversial Law of Return which allows any Jew in the world to claim Israeli citizenship without having to renounce their home country passport.
Some of those accused and charged have made minor or international headlines, some haven’t, but the scale of the issue was such that I thought it would be useful to document my research here.
In some cases, Israel has refused to extradite the wanted person despite requests from the country in which the crimes were committed.
Staying on Ukraine and refused extradition requests, we have Oleksandr Dubilet, the former Chairman of the Board of Ukraine’s PrivatBank. Dubilet is currently a fugitive in Israel and the subject of multiple criminal investigations and extradition requests for his role in embezzling at least $100 million dollars following the 2016 privatisation of PrivatBank. To date, Israel has refused to extradite him.
Israel as a bolthole for financial fraudsters is a common theme. One of the most significant SEC fraud cases in recent years involved over 150 Israelis (some with dual US-Israeli nationality, others not), wanted for their role in conducting binary options fraud worth upwards of $100 billion.
Binary options are a type of financial bet where the outcome is essentially all-or-nothing. Instead of buying a stock or currency, you bet on whether the price of a stock or currency will be above or below a certain level at a specific time. While not illegal, the Israeli companies were accused of rigging and manipulating prices and expiry times and using fake identities.
For a decade until 2017, Israel was the global centre for the online binary-options industry. The Israeli police failed to investigate, so hundreds of cases were filed in Israeli courts by people from dozens of countries who had been defrauded.
One of the most notorious fraudsters was Lee Elbaz, the CEO of Yukom Communications, a dual US-Israeli national. She was arrested in 2017 when on holiday in New York and eventually convicted of wire fraud and sentenced to 22 years in prison.
Other prime Israeli movers in the binary options fraud business were Yossi Herzog and Yakov Cohen, both connected with Yukom and other binary options front companies. They were charged with $140 million fraud in 2019 but despite being under a DOJ criminal investigation the US choose not to pursue their extradition, while other Israeli co-conspirators in the Yukom case have joined Elbaz in serving jail sentences.
Other Israeli kingpins in the binary options sector include Ran Amiran and Malhaz Patarkazishvili, also known as Pini Peter. They were charged with $100 million fraud by the SEC for their role managing the fraudulent options trader Spot Option. Because it was a civil case and the DOJ wasn’t involved they weren’t eligible for extradition from Israel and continue to reside in Israel. It was reported in 2021 that Amiran had reached a financial settlement for the damages with the SEC, likely so that he could once again travel to the US. Peter, a friend of Netanyahu’s, remains unrepentant, despite being ordered to pay the US government $87 million, a judgment he has appealed.
Benjamin Netanyahu with financial fraudster Pini Peter
Another hotbed of Israeli fraud is the moving industry, where companies pose as legitimate household goods movers only to steal belongings or withhold items unless additional payment is made. One of the largest “hostage load” prosecutions was of Advanced Moving Systems, an Israeli-run company which lured customers with artificially low moving estimates and then extorted them by holding their household goods hostage until they paid fraudulently inflated prices. Many of the dozens of people behind the scam remain wanted, with their current location unknown. Dozens of other Israelis connected with fraudulent moving companies also remain on the run, and have likely fled to Israel. (Incidentally, the Israelis arrested by the FBI on September 11th and quickly released were working for a Mossad counterintelligence operation using a moving company as cover. But that’s another story).
Penny stock fraud is another rich seam for Israeli crooks. This type of fraud takes place when the stocks of small companies trading under $5 a share are marketed to often older and uniformed people using high pressure sales marketing tactics, with the caller promising guaranteed returns, often claiming to have inside information. One of the largest instances in recent years saw dual US-Israeli citizen Sharone “Barry” Perlstein and numerous Israeli co-conspirators charged with creating at least 15 fraudulent public shell companies to sell millions of dollars worth of penny stocks using fraudulent tactics. Previous penny stock fraud cases had also involved Israeli nationals.
The diamond industry has also attracted a fair share of Israeli swindlers. One of the most well-known is Mordechai “Moti” Ferder, a California-based luxury jeweller at the centre of one of the largest fraud scandals in the American jewellery industry. Ferder was accused of juicing his company’s accounts to boost the valuation before selling to an investment company, while in reality he was racking up liabilities worth hundreds of millions of dollars. In 2025, with an FBI investigation underway, Ferder fled California for Tel Aviv.
Then there is Gery Shalon, the Georgia-born Israeli responsible for hacking JP Morgan and carrying out the largest theft of customer data from an American financial institution in history.
Outside the fraud cases, Israel also attracts politicians attempting to shield themselves from justice in their home countries. One of the most notorious and ongoing cases is that of Tomás Zerón, the former director of the Criminal Investigation Agency of Mexico. Zerón, who received training in Israel before assuming control of Mexico’s version of the FBI, is accused by Mexican authorities of having direct involvement in the kidnap, torture, and likely murder of dozens of university students.
The Ayotzinapa kidnapping is considered one of Mexico’s most heinous human rights abuse cases. It took place in 2014, when forty-three leftist students were kidnapped and disappeared on their way to Mexico City to commemorate the anniversary of the 1968 Tlatelolco massacre. Zerón is said to have known or ordered the students to be handed over to a cartel group to be murdered and disposed of. The former Mexican top cop promptly fled to Israel after being officially accused of participating in the crime.
Despite an extradition order, an Interpol red notice and numerous requests from Mexico to hand him over, Israel has refused, reportedly as punishment for Mexico’s criticism of Israel at the UN.
Another Mexican diplomat who fled to Israel is Andrés Roemer. Formerly Mexico’s Ambassador to UNESCO based in Paris, and Consul General of Mexico in San Francisco, Roemer fled to Israel in 2021 after being accused by 61 women of rape and sexual assault. While a Jerusalem court has authorized the former diplomat’s extradition to Mexico, he remains in Israel under house arrest.
Roemer is not alone among Jewish sex criminals fleeing from justice in the home countries to Israel. The phenomenon is so prevalent that even CBS News has covered it. Probably the most famous accused sex criminals to have fled to Israel are the Hollywood directors Brett Ratner and Bryan Singer. Rush Hour director Ratner, a good friend of Netanyahu’s, fled to Israel in 2023 after being accused by multiple women of sexual misconduct and assault on set.
Brett Ratner with Benjamin and Sarah Netanyahu, and ultra-Zionist attorney Alan Dershowitz
Israel is a magnet for criminals of all flavors, making this brief compendium just the tip of the iceberg. The Law of Return, known to be policed very lightly, is a gateway allowing Jews to use their dual nationality to commit crimes and then swerve justice under an ethno-supremacist legal regime set up to protect them. Some succeed in avoiding justice, while others are not so lucky.
This film is about how the French army secretly used chemical weapons in the Algerian independence war, in contravention of international law. The documentary presents archival evidence and personal testimony from former French soldiers and Algerian fighters, exposing France’s violation of the 1925 Geneva Protocol. Historian Christophe Lafaye’s evidence includes a letter from a senior army commander to the government in 1956, which refers to the “use of chemical means”.
France set up a Special Weapons Unit in December 1956, using the same CN2D gas as in World War I, to target Algerian fighters in mountain caves. Of the estimated 8,000 to 10,000 incidents, only 440 attacks have been documented so far. One of the most devastating attacks was at Ghar Ben Shatouh in March 1959, in which an estimated 150 civilians were killed. Despite this, France did not formally ban chemical weapons until 1993, more than 30 years after Algeria’s independence.
That bottle of sunscreen in your beach bag may be doing more harm than good. New research reveals the hidden dangers lurking in conventional sunscreens and highlights safer, natural alternatives that can protect your skin without toxic side effects.
For decades, we’ve been told that slathering on sunscreen is one of the best ways to protect our skin from the sun’s harmful rays. However, mounting evidence suggests that many conventional sunscreens contain ingredients that may be hazardous to our health and the environment. From hormone-disrupting chemicals to potentially carcinogenic nanoparticles, the risks associated with common sunscreen ingredients are cause for serious concern.
At the same time, researchers have discovered that many natural plant oils offer significant sun protection, often rivaling or exceeding the SPF of chemical sunscreens. These botanical alternatives not only shield skin from UV damage, but also nourish and moisturize without introducing synthetic toxins into the body.
This article will explore the dangers lurking in your sunscreen bottle, examine promising research on herbal oil alternatives, and provide practical guidance for safer sun protection. By understanding the risks and exploring natural options, you can make informed choices to safeguard your skin and overall health.
The Trouble with Conventional Sunscreens
Chemical Cocktails: Questionable Ingredients in Popular Sunscreens
Many best-selling sunscreens contain a slew of synthetic chemicals that act as UV filters, preservatives, fragrances and more. Some of the most concerning ingredients include:
Oxybenzone: This common chemical UV filter has been shown to disrupt hormones, cause allergic reactions, and damage coral reefs. Studies have found oxybenzone in 97% of Americans tested.1
Octinoxate: Another chemical filter linked to hormone disruption and environmental damage. It’s been banned in Hawaii and Key West due to its impact on coral.2
Homosalate: An endocrine disruptor that may increase the absorption of pesticides through the skin.3
Octocrylene: Can produce free radicals that may damage cells and accelerate skin aging when exposed to UV light.4
Parabens: Synthetic preservatives with estrogenic activity, detected in breast cancer tumors.5
Fragrance: Often contains undisclosed phthalates linked to reproductive issues and cancer.6
The Nanoparticle Problem: Are Mineral Sunscreens Any Safer?
In response to concerns over chemical sunscreens, many consumers have turned to mineral-based formulas containing zinc oxide or titanium dioxide. While these ingredients are generally considered safer, the increasing use of nanoparticles in mineral sunscreens has introduced new risks:
Potential for cellular damage: Nanoparticles may be small enough to penetrate skin cells and cause oxidative damage to DNA.7
Respiratory concerns: Inhaling nanoparticles from spray sunscreens could potentially cause lung inflammation or damage.8
Environmental impact: Like chemical UV filters, nanoparticles can accumulate in waterways and harm aquatic life.9
Systemic absorption: A 2010 study found that nanoparticle zinc oxide from sunscreen was detectable in human blood and urine after topical application.10
The Skin Absorption Dilemma
One of the biggest issues with conventional sunscreens is their potential for systemic absorption through the skin. Multiple studies have detected common sunscreen chemicals in blood, urine, and breast milk after topical use.11,12
This is concerning because the skin is not merely a barrier, but a permeable organ capable of absorbing substances into the bloodstream. In fact, transdermal drug delivery systems take advantage of this property to administer medications through the skin.
When it comes to sunscreen, we’re essentially slathering a chemical cocktail over a large surface area of our bodies, often repeatedly throughout the day. This creates significant potential for absorption and accumulation of questionable ingredients in our tissues over time.
Understanding SPF: Debunking the High Number Myth
Before exploring natural alternatives, it’s important to understand what Sun Protection Factor (SPF) really means. Many consumers believe that higher SPF numbers offer dramatically better protection, but the reality is more nuanced:
SPF measures how much longer skin covered with sunscreen takes to burn compared to unprotected skin. For example, SPF 2 means you can stay in the sun twice as long before burning compared to wearing no sunscreen.
However, the percentage of UVB rays blocked doesn’t increase linearly with SPF numbers:
SPF 2 blocks 50% of UVB rays
SPF 15 blocks about 93% of UVB rays
SPF 30 blocks about 97% of UVB rays
SPF 50 blocks about 98% of UVB rays
As you can see, the difference between SPF 30 and SPF 50 is only 1% in terms of UVB protection. This reveals a common misconception that very high SPF values are necessary for adequate sun protection. In reality, even a relatively low SPF of 15 blocks 93% of UVB rays, and an SPF of just 2 cuts UVB exposure in half.
While higher SPFs do offer incrementally more protection and may be beneficial for those with very fair or sensitive skin, the difference is not as dramatic as many people assume. This understanding is crucial when considering natural alternatives, which may have lower SPF values but still offer significant protection.
Environmental and Health Consequences
Beyond personal health concerns, conventional sunscreens pose serious risks to the environment:
Coral reef destruction: Oxybenzone and octinoxate have been implicated in coral bleaching, leading to bans in reef-adjacent areas.13
Aquatic toxicity: Sunscreen chemicals can accumulate in lakes and oceans, harming fish and other marine life.14
Soil contamination: UV filters have been detected in agricultural soils, with unknown impacts on crops and ecosystems.15
The cumulative effects of widespread sunscreen use are just beginning to be understood. As these chemicals build up in our bodies and the environment, they may contribute to a range of health and ecological issues:
Hormone disruption and reproductive problems
Increased risk of certain cancers
Allergies and skin irritation
Coral reef die-offs and marine ecosystem collapse
Contamination of water supplies
Natural Alternatives: Herbal Oils as Sunscreen
In light of the risks associated with conventional sunscreens, many consumers are seeking safer, more natural alternatives. Emerging research suggests that certain plant-based oils may offer significant sun protection without the drawbacks of synthetic chemicals.
A groundbreaking 2010 study published in Pharmacognosy Research evaluated the SPF (sun protection factor) of various herbal oils commonly used in cosmetics. The researchers used a spectrophotometric method to determine the in vitro SPF values of both volatile and non-volatile herbal oils.16
Their findings revealed impressive sun protection potential in many natural oils:
These results are particularly noteworthy because many of the oils tested demonstrated significant UV protection levels. For example, olive oil with 87.5% UV protection (SPF 8) is substantial considering it’s a natural, non-toxic alternative. Also, consider the vast number of therapeutic actions olive oil demonstrates in the scientific literature.
It’s important to remember that even oils with lower protection values, such as tea tree oil at 50% (SPF 2), still cut UVB exposure in half compared to unprotected skin. This level of protection, combined with other sun-safety measures, can contribute significantly to overall sun safety without relying on potentially harmful synthetic chemicals.
Benefits of Herbal Oil Sunscreens
Natural plant oils offer several advantages over conventional chemical sunscreens:
Broad-spectrum protection: Many oils contain compounds that shield against both UVA and UVB rays.
Antioxidant activity: Plant oils are rich in antioxidants that can neutralize free radicals and combat UV-induced skin damage.
Skin-nourishing properties: Unlike synthetic sunscreens that can be drying, natural oils moisturize and support skin health.
No toxic buildup: Plant-based oils are biodegradable and do not accumulate in tissues or the environment like synthetic chemicals.
Multiple health benefits: Many oils offer additional skincare perks like anti-aging, anti-inflammatory, and wound-healing properties.
Environmentally friendly: Natural oils do not contribute to coral bleaching or aquatic toxicity.
Spotlight on Top Performing Oils
Olive Oil (87.5% UV protection, SPF 8)
Rich in polyphenols and vitamin E, olive oil offers potent antioxidant and anti-inflammatory benefits. Its high oleic acid content helps maintain skin moisture and elasticity.
Coconut Oil (85.7% UV protection, SPF 7)
Known for its moisturizing and antimicrobial properties, coconut oil creates a protective barrier on the skin. It also contains lauric acid, which has been shown to have photoprotective effects.17
Peppermint Oil (85.7% UV protection, SPF 7)
This refreshing essential oil not only offers sun protection but also provides a cooling sensation that can help soothe sunburned skin. Its menthol content has analgesic properties.
Revered in Ayurvedic medicine, tulsi oil boasts powerful antioxidant, anti-inflammatory, and adaptogenic properties. It may help combat UV-induced oxidative stress and support overall skin health.
Practical Applications and Considerations
While herbal oils show promise as natural sunscreens, it’s important to note that their protection levels are generally lower than those of high-SPF commercial products. To maximize sun protection when using natural oils:
Layer multiple oils: Combining oils with complementary properties can enhance overall sun protection.
Reapply frequently: Natural oils may not be as water-resistant as synthetic sunscreens, so reapply often, especially after swimming or sweating.
Use in conjunction with other sun-safety measures: Seek shade, wear protective clothing, and limit sun exposure during peak hours.
Consider adding zinc oxide: For higher protection, some people mix non-nano zinc oxide powder into their preferred oil base.
Patch test first: As with any new skincare product, test oils on a small area to check for allergic reactions or irritation.
Be aware of photosensitivity: Some essential oils, particularly citrus oils, can increase sun sensitivity. Use caution and dilute appropriately.
Realistic Expectations for Natural UV Protection
When using herbal oils for sun protection, it’s crucial to have realistic expectations. While these natural alternatives may not match the high protection numbers of commercial sunscreens, they still offer meaningful defense. An oil with 75% UV protection (SPF 4), for instance, represents a significant reduction in UV exposure. By layering oils, reapplying frequently, and combining their use with other sun-safety measures, you can achieve effective protection without resorting to synthetic chemicals. Remember, any reduction in UV exposure is beneficial for skin health, and these natural oils offer that protection along with additional skincare benefits.
The Petrochemical Problem: Why Slathering on Toxins is a Bad Idea
The widespread use of petrochemicals in personal care products, including sunscreens, raises serious health and environmental concerns. Here’s why coating our largest organ in fossil fuel derivatives is problematic:
Bioaccumulation and Body Burden
Petrochemicals are lipophilic, meaning they have an affinity for fats. This allows them to penetrate the skin easily and accumulate in fatty tissues throughout the body. Over time, this can lead to a significant toxic burden.
A 2011 study found that women who used mineral oil-based cosmetics had higher levels of mineral oil saturated hydrocarbons (MOSH) in their body fat compared to non-users. The researchers concluded that cosmetic products were likely a relevant source of MOSH contamination in the population.18
Endocrine Disruption
Many petrochemicals used in sunscreens and other personal care items are known or suspected endocrine disruptors. These compounds can interfere with hormone signaling, potentially leading to reproductive issues, developmental problems, and increased cancer risk.
For example, parabens, which are commonly used as preservatives in sunscreens, have been shown to mimic estrogen in the body. A 2004 study detected parabens in human breast tumors, raising concerns about their potential role in breast cancer development.19
Skin Irritation and Sensitization
Petroleum-derived ingredients can cause skin irritation, allergic reactions, and increased sensitivity in some individuals. This is particularly concerning for sunscreens, which are applied to large areas of skin and often used on children and those with sensitive skin.
A 2018 review in the Journal of Allergy and Clinical Immunology: In Practice found that up to 70% of people with sensitive skin reported adverse reactions to sunscreens, with chemical UV filters being common culprits.20
Environmental Contamination
When we use products containing petrochemicals, these substances don’t just affect our bodies – they also enter the environment. Sunscreen chemicals wash off in water, contaminating lakes, rivers, and oceans.
A 2015 study estimated that between 6,000 and 14,000 tons of sunscreen wash off into coral reef areas each year, with devastating effects on marine ecosystems.21
Fossil Fuel Dependence
The widespread use of petrochemicals in personal care products contributes to our overall dependence on fossil fuels. This not only perpetuates environmental damage from oil extraction and refining but also supports an industry with a vested interest in downplaying the risks of its products.
By choosing natural, plant-based alternatives, consumers can reduce their exposure to potentially harmful petrochemicals while supporting more sustainable and environmentally friendly practices.
Conclusion: Embracing Safer Sun Protection
As awareness grows about the potential risks of conventional sunscreens, the shift towards natural alternatives is gaining momentum. Herbal oils offer a promising solution, providing effective sun protection along with additional skin benefits, without introducing synthetic toxins into our bodies or the environment.
While more research is needed to fully understand the photoprotective properties of plant oils, the available evidence suggests they can be valuable tools in our sun safety arsenal. By combining the use of natural oils with sensible sun exposure habits, we can safeguard our skin health while minimizing our chemical burden.
Ultimately, the choice between conventional and natural sunscreens is a personal one. However, given the mounting concerns over petrochemical-based products, exploring safer alternatives is a wise investment in both personal and planetary health. As we continue to uncover the hidden costs of our chemical-laden lifestyles, returning to nature’s time-tested remedies may prove to be the smartest path forward.
References
1. Calafat, A. M., et al. “Concentrations of the Sunscreen Agent Benzophenone-3 in Residents of the United States: National Health and Nutrition Examination Survey 2003-2004.” Environmental Health Perspectives, vol. 116, no. 7, 2008, pp. 893-897.
2. Downs, C. A., et al. “Toxicopathological Effects of the Sunscreen UV Filter, Oxybenzone (Benzophenone-3), on Coral Planulae and Cultured Primary Cells and Its Environmental Contamination in Hawaii and the U.S. Virgin Islands.” Archives of Environmental Contamination and Toxicology, vol. 70, no. 2, 2016, pp. 265-288.
3. Krause, M., et al. “Sunscreens: Are They Beneficial for Health? An Overview of Endocrine Disrupting Properties of UV‐Filters.” International Journal of Andrology, vol. 35, no. 3, 2012, pp. 424-436.
4. Hanson, K. M., et al. “Sunscreen Enhancement of UV-Induced Reactive Oxygen Species in the Skin.” Free Radical Biology and Medicine, vol. 41, no. 8, 2006, pp. 1205-1212.
5. Darbre, P. D., et al. “Concentrations of Parabens in Human Breast Tumours.” Journal of Applied Toxicology, vol. 24, no. 1, 2004, pp. 5-13.
6. Heudorf, U., et al. “Phthalates: Toxicology and Exposure.” International Journal of Hygiene and Environmental Health, vol. 210, no. 5, 2007, pp. 623-634.
7. Shukla, R. K., et al. “ROS-Mediated Genotoxicity Induced by Titanium Dioxide Nanoparticles in Human Epidermal Cells.” Toxicology in Vitro, vol. 25, no. 1, 2011, pp. 231-241.
8. Grassian, V. H., et al. “Inflammatory Response of Mice to Manufactured Titanium Dioxide Nanoparticles: Comparison of Size Effects through Different Exposure Routes.” Nanotoxicology, vol. 1, no. 3, 2007, pp. 211-226.
9. Minetto, D., et al. “Ecotoxicity of Engineered TiO2 Nanoparticles to Saltwater Organisms: An Overview.” Environment International, vol. 88, 2016, pp. 60-72.
10. Gulson, B., et al. “Small Amounts of Zinc from Zinc Oxide Particles in Sunscreens Applied Outdoors Are Absorbed through Human Skin.” Toxicological Sciences, vol. 118, no. 1, 2010, pp. 140-149.
11. Janjua, N. R., et al. “Systemic Absorption of the Sunscreens Benzophenone-3, Octyl-Methoxycinnamate, and 3-(4-Methyl-Benzylidene) Camphor after Whole-Body Topical Application and Reproductive Hormone Levels in Humans.” Journal of Investigative Dermatology, vol. 123, no. 1, 2004, pp. 57-61.
12. Schlumpf, M., et al. “Exposure Patterns of UV Filters, Fragrances, Parabens, Phthalates, Organochlor Pesticides, PBDEs, and PCBs in Human Milk: Correlation of UV Filters with Use of Cosmetics.” Chemosphere, vol. 81, no. 10, 2010, pp. 1171-1183.
13. Danovaro, R., et al. “Sunscreens Cause Coral Bleaching by Promoting Viral Infections.” Environmental Health Perspectives, vol. 116, no. 4, 2008, pp. 441-447.
14. Giokas, D. L., et al. “Occurrence and Removal of Chemical UV Filters in Wastewater Treatment Plants.” Environmental Science and Pollution Research, vol. 22, no. 12, 2015, pp. 9089-9100.
15. Chen, F., et al. “Distribution and Accumulation of Endocrine-Disrupting Chemicals and Pharmaceuticals in Wastewater Irrigated Soils in Hebei, China.” Environmental Pollution, vol. 159, no. 6, 2011, pp. 1490-1498.
16. Kaur, C. D., and Saraf, S. “In Vitro Sun Protection Factor Determination of Herbal Oils Used in Cosmetics.” Pharmacognosy Research, vol. 2, no. 1, 2010, pp. 22-25.
17. Korać, R. R., and Khambholja, K. M. “Potential of Herbs in Skin Protection from Ultraviolet Radiation.” Pharmacognosy Reviews, vol. 5, no. 10, 2011, pp. 164-173.
18. Concin, N., et al. “Mineral Oil Paraffins in Human Body Fat and Milk.” Food and Chemical Toxicology, vol. 46, no. 2, 2008, pp. 544-552.
19. Darbre, P. D., and Harvey, P. W. “Paraben Esters: Review of Recent Studies of Endocrine Toxicity, Absorption, Esterase and Human Exposure, and Discussion of Potential Human Health Risks.” Journal of Applied Toxicology, vol. 28, no. 5, 2008, pp. 561-578.
20. Rozas-Muñoz, E., et al. “Sensitive Skin: A Review of Prevalence, Pathogenesis, and Management.” Journal of Allergy and Clinical Immunology: In Practice, vol. 6, no. 6, 2018, pp. 1898-1908.
21. Downs, C. A., et al. “Toxicopathological Effects of the Sunscreen UV Filter, Oxybenzone (Benzophenone-3), on Coral Planulae and Cultured Primary Cells and Its Environmental Contamination in Hawaii and the U.S. Virgin Islands.” Archives of Environmental Contamination and Toxicology, vol. 70, no. 2, 2016, pp. 265-288.
In December 2007, Archives of Pediatrics and Adolescent Medicine published a study by Ian Paul and colleagues at the Penn State College of Medicine. One hundred five children between the ages of two and eighteen, all with cough and runny nose of seven days or less, were randomized into three groups. One group received a single nocturnal dose of buckwheat honey. One received an age-appropriate dose of honey-flavored dextromethorphan, the leading over-the-counter cough suppressant in America, sold in many formulations under brand names including Robitussin, Delsym, Vicks, and NyQuil. The third received nothing.
Parents scored their children on cough frequency, cough severity, how bothersome the cough was, the child’s sleep quality, and their own sleep quality.
Honey improved every outcome measured. Dextromethorphan showed no statistically significant advantage over no treatment on any of them.¹
The comparison that mattered, the one the study was designed to run, put a spoon of honey against a mass-market pharmaceutical and found the honey better. The comparison the authors did not lead with, but which sat plainly in the pairwise data, put the mass-market pharmaceutical against nothing and found no measurable difference.
The Paul trial was partially double-blinded (honey cannot be blinded from taste), which is the obvious objection. A 2018 Cochrane review pooled the Paul study with later replications from Israel, Iran, and Brazil, all of which used various blinding designs, and reached the same conclusion. Honey outperforms no treatment. Honey outperforms dextromethorphan. It does so consistently.²,³
Six weeks after the Paul study appeared, on 17 January 2008, the U.S. Food and Drug Administration issued a Public Health Advisory recommending that over-the-counter cough and cold products not be used at all in children under the age of two, citing “serious and potentially life-threatening side effects” including convulsions, rapid heart rates, decreased consciousness, and death.⁴ The Centers for Disease Control had documented over fifteen hundred children under the age of two treated in emergency rooms in 2004 and 2005 for adverse events after receiving these products.⁵ Manufacturers voluntarily pulled infant formulations from the shelves before the advisory issued, and relabeled their remaining children’s products as not for use in children under four.⁶
Two facts arrived within weeks of each other. A peer-reviewed randomized trial found the leading OTC cough medicine indistinguishable from placebo. The FDA determined that its use had been killing children.
None of this was breaking news to anyone who owned a copy of Folk Medicine.
The recipe
D.C. Jarvis was a Vermont country doctor. For decades he cataloged the folk practices of his patients, most of them families who had farmed the same land for generations. His 1958 book Folk Medicine was a New York Times bestseller for over a year. Chapter nine gives the cough syrup as he recorded it:
Boil one lemon slowly for ten minutes. This softens the lemon so that more juice will be got out of it, and also softens the rind. Cut the lemon in two and extract the juice with a lemon squeezer. Put the juice into an ordinary drinking glass. Add two tablespoonfuls of glycerine… Stir the glycerine and lemon juice well, then fill up the drinking glass with honey.⁷
Dose: one teaspoonful for a daytime coughing spell. One at bedtime and again in the night if the cough wakes the child. For severe cough, six teaspoonfuls across the day. As the cough eases, the doses taper.
Jarvis’s observations on the preparation were specific. “It does not upset the stomach, as many cough syrups do. It can be taken by children as well as adults. It will relieve a cough when all other cough syrups fail.”⁷
He noted the recipe was “many generations old” in his region in 1961. That places its lineage well into the nineteenth century, among people who kept bees, grew lemons in glasshouses or bought them from the general store, and used glycerine (a viscous byproduct of soap-making, cheap at any pharmacy in that era) as a household remedy for coughs, sore throats, and dry skin.
The recipe survives in Jarvis’s book with one further detail that matters. Immediately after giving the formula, he adds an anecdote from a farmer patient.
Speaking of using lemons to compound a cough remedy, I recall the remark of a farmer. When he was explaining how well the suggested remedy had worked he laughed and said, “Fact is, we didn’t have any lemons. I used apple-cider vinegar. Just as good.”⁷
The farmer had substituted vinegar for citrus and got the same result. This is not a marginal detail. It tells you what the acid is doing in the recipe. It is thinning mucus and providing a light astringent action, a function any acid can perform, which is why the substitution worked and why the medieval European oxymels (honey-and-vinegar preparations used for coughs since Hippocrates) sit in the same family as this Vermont formula. The mechanism does not depend on lemon specifically. It depends on a small quantity of acid, dissolved in honey, held long enough in the throat to coat the irritated tissue.
Jarvis’s Vermont formulation is one documentation of a broader folk tradition. The base was constant across regions and centuries: honey plus acid. The additions varied by kitchen and by climate.
Jethro Kloss, working the same tradition from a different angle, published Back to Eden in 1939 with parallel preparations drawn from the Tennessee-Wisconsin herbal lineage. His lemon syrup began identically. “Boil one pint of lemon juice ten minutes.”⁸ His fig cough syrup combined honey and lemon in the same architecture. His entry on coltsfoot (Latin Tussilago farfara, literally “coughwort”) notes the leaves are “excellent when combined with other herbs and made into a cough syrup,” sweetened with honey. Kloss’s book documents lemon for colds, influenza, asthma, and fever across seven pages. “I wish that humanity would understand the real value of the lemon and learn to make a real medicine of it.”⁸
Kloss also documented thyme. His entry on Thymus vulgaris lists its medicinal properties as tonic, carminative, antispasmodic, and antiseptic, and describes it as “valuable in whooping cough, asthma, and lung troubles. For small children, give small and frequent doses.”⁸ His caution alongside was equally specific: “Use sparingly. Do not make a habit of using thyme.” Concentrated action, careful dosing.
Thyme’s principal active compounds, thymol and carvacrol, are phenolics concentrated in the plant’s volatile oils. Their actions on airway tissue are documented and specific. Thymol is antispasmodic on bronchial smooth muscle: it relaxes the involuntary contractions that produce coughing spasms. It is expectorant: it thins mucus and stimulates the ciliated cells lining the airway to move it upward for clearance. And because the volatile oils vaporize at warm-drink temperatures, a portion of the thymol is delivered by inhalation as well as by swallowing when the syrup is taken warm. Aromatic herbs work through two routes at once. Germany’s Commission E, the mainstream regulatory body for herbal medicines and roughly the German equivalent of a plant-medicine FDA, approves thyme for symptomatic treatment of bronchitis, whooping cough, and catarrh of the upper airway.¹⁵ European folk medicine has used it continuously in that role for centuries.
The recipe this essay recommends draws on both traditions. Honey and lemon supply the demulcent and osmotic base, as in Jarvis. Thyme adds the antispasmodic and aromatic action, as in Kloss. The formulation is in the appendix. Jarvis’s exact Vermont version, with glycerine, is in the appendix as well, for readers who want the historical formulation as he wrote it. Glycerine is a more processed component than the others (a purified single compound rather than a whole food), but it has been in continuous folk use since the nineteenth century as a pharmacy-counter demulcent, and it extends the throat-coating time beyond what honey alone provides. Both formulations work. The primary is closer to whole-food preparation.
The recipe was not Jarvis’s discovery. Jarvis was writing down what he saw farmers using. Kloss was doing the same in a different region.
A note before proceeding. Honey is not given to infants under one year. The concern is toxicological, not infectious. Clostridium botulinum spores can be present in raw honey. In older children and adults, established gut flora and stomach acid prevent the spores from germinating, and they pass through without effect. In an infant’s immature digestive tract, the same spores can germinate and produce botulinum toxin, a potent neurotoxin. The organism is not causing an infection. The toxin is doing the damage. The caution predates the Paul trial by decades and is not disputed by any party, mainstream or otherwise. The Paul study enrolled children aged two and above for the same reason.
What a cough is
A cough is an expulsive reflex. Irritation of the airway lining, from mucus, dust, smoke, particulate matter, gastric reflux, dryness, or cold air, triggers rapid contraction of the diaphragm and intercostals against a closed glottis. The glottis opens. Air explodes out at velocities exceeding twenty-five meters per second, carrying whatever the airway is trying to clear.
The reflex exists because the airway lining is thin, delicate, and constantly exposed to material that shouldn’t be there. Without the cough, particulate matter accumulates. Mucus produced to trap that material accumulates with it. Untreated, the accumulation moves down. What began as a throat irritation becomes a chest cough. What began as an acute condition, resolved in days by the body’s clearance of the trigger, becomes chronic.
Kloss described this progression plainly in Back to Eden. On chronic bronchitis: “Acute bronchitis may become chronic if it is not properly treated and relieved. When a cold is allowed to continue, the infection may extend down into the lungs and become chronic. Occasionally, if it is not cured, it may encourage the development of tuberculosis or some other serious chronic lung disease.”⁸ On why the cough arose in the first place: “Colds would not be so prevalent if the body were not filled with mucus and waste products, so one should immediately rid the body of these poisons.”⁸
The framework is not obscure. Herbert Shelton, the twentieth-century natural hygienist, called it the acute-to-chronic mechanism. The body’s efforts to expel accumulated toxins produce acute symptoms. Suppression of those symptoms leaves the toxins in place. The body attempts expulsion by other routes. Those routes are suppressed in turn. The process, driven long enough, produces chronic disease that presents as a distinct condition, apparently unrelated to the accumulated cause.
The cough is the body clearing the airway. To decide what a cough syrup should do, you have to decide what you think a cough is for. That decision determines everything downstream.
The suppressor
Dextromethorphan was patented in the 1950s as a non-narcotic replacement for codeine. Codeine had a long history as a cough suppressant, and a long history as an opioid: sedating, addictive, respiratory-depressant at high doses. Dextromethorphan was developed to keep the antitussive function without the opioid liability.
It works centrally. The drug reaches the brainstem through the bloodstream and depresses the medullary cough center, which is the neural relay where signals from an irritated airway would normally trigger the expulsive reflex. It achieves this by binding to receptors in the brainstem, blocking NMDA glutamate receptors and activating sigma-1 receptors. It also weakly affects serotonin and norepinephrine.⁹ The signal from the airway still arrives at the relay. It no longer produces a cough.
Nothing about this mechanism addresses the airway. Dextromethorphan does not soothe irritation. It does not thin mucus. It does not accelerate its removal. It does not resolve whatever prompted the cough. It sits on receptors that normally allow the cough signal to fire, and it prevents them from firing.
The signal was the body’s alarm. The cough was its response to the alarm. Dextromethorphan silences the response by muting the alarm at the central switchboard.
At therapeutic doses, this produces the intended effect (the person stops coughing) for as long as the drug is active. At supratherapeutic doses the NMDA antagonism produces dissociation and hallucination similar in character to phencyclidine.⁹ The recreational abuse of dextromethorphan-containing cough syrups (known as “robotripping”) is a documented clinical phenomenon. At high doses in combination with serotonergic drugs, it produces serotonin syndrome. At high doses generally, it produces respiratory depression.
In children specifically, the Paul team ran their earlier study in 2004, dextromethorphan versus diphenhydramine versus placebo, and found none of the three superior for nocturnal cough or sleep quality.¹⁰ This was not an isolated result. By the time the American Academy of Pediatrics reviewed the evidence, it did not recommend dextromethorphan for children. The American College of Chest Physicians reached the same conclusion.¹
By 2007 the leading over-the-counter cough drug in America had been tested against an inert control in two randomized trials, first against placebo and then against no treatment. It had shown no measurable advantage in either. Six weeks later the FDA advisory arrived, citing convulsions and deaths.
The soother
The folk cough syrup does something categorically different.
Kloss defined the two active mechanisms in the glossary of Back to Eden. A demulcent is “an agent that soothes, protects, and relieves the irritation of inflamed mucous membranes and other surfaces.” An expectorant “promotes the thinning and ejection of mucus or exudate from the lungs, bronchi, and trachea.”⁸
The preparation is both, and with thyme it is also antispasmodic.
Honey is a supersaturated sugar solution with a water activity of around 0.6 (too low to support most microbial growth) and a pH of around 3.9. Held on the tissue of the throat, it draws water osmotically from the inflamed lining, which reduces local swelling and provides mechanical soothing. Its viscosity coats and protects the irritated surface. Lemon juice, at a pH of around 2.2, thins mucus on contact and provides light astringent action from citric acid and phenolic compounds. Vinegar, at a similar pH, does the same thing, which is why the farmer’s substitution worked.
Thyme adds two further actions to the base. Thymol, its principal phenolic compound, relaxes bronchial smooth muscle: the involuntary tension that produces coughing spasms eases. Thymol also stimulates the ciliated cells of the airway lining to move mucus upward for clearance, which is exactly what a productive cough is trying to do. The syrup helps the cough finish faster. The volatile oils vaporize slightly at warm-drink temperature, delivering a portion of the thymol by inhalation alongside ingestion, so the active compound reaches the airway lining directly as well as via the digestive tract.
In Jarvis’s Vermont variant, glycerine adds a further specific function. It is strongly hygroscopic. It holds moisture against tissue and extends the demulcent contact time beyond what honey alone provides. It is not essential to the recipe’s action, but it lengthens the duration of soothing per spoonful.
The syrup soothes the irritation triggering the cough. It thins the mucus the cough is trying to clear. It relaxes the airway spasm. It supports the reflex rather than suppressing it. When the cough is no longer needed, it stops.
The mechanism runs on the airway, not in the brainstem. It leaves the reflex intact and removes its cause.
Honey has other properties that matter here. Its low water activity, low pH, hydrogen peroxide production, and specific plant-derived phenolic compounds create an environment inhospitable to microbial overgrowth on inflamed tissue. This is why traditional cultures used honey on open wounds long before anyone had proposed a theory of infection. Buckwheat honey specifically, the varietal Paul’s team chose, is unusually high in phenolic compounds and antioxidant activity. The World Health Organization’s Department of Child and Adolescent Health, in its 2001 review of cough and cold remedies for young children, cited honey as a potentially effective option six years before the Penn State trial confirmed it.¹¹,¹²
The recipe soothes without suppressing. That is the essential difference. It works with the reflex. Dextromethorphan works against it.
The 2007 trial was measuring, without knowing it, the difference between those two approaches.
Continuity
The medicinal use of honey is documented continuously across every literate culture from the emergence of writing forward. Sumerian clay tablets from around 2100 BC record honey mixed with river dust and oil for infected skin ulcers. Egyptian medical papyri describe honey applied to open wounds. Sushruta, a physician in Vedic India around 1400 BC, wrote of the medicinal properties of eight honey varietals. Athenaeus in Greece around 230 AD recorded that those who ate honey and bread for breakfast “were free from disease all their lives.” Ibn Majah, quoting Mohammed in the seventh century, wrote that “honey is a remedy for every illness.”¹¹
The specific use for cough runs the same length. Every one of these traditions used honey, sometimes alone, more often combined with acid, herb, or spice, for cough, sore throat, and cold.
Sir John Hill, a physician in England in 1759, wrote the first English-language book devoted to the medicinal use of honey. He observed, then, that its virtues were being neglected.
The slight regard at this time paid to the medicinal virtues of Honey, is an instance of neglect men shew to common objects, whatever their value: acting in contempt, as it were, of the immediate hand of providence, which has in general made those things most frequent, which have the greatest uses; and for that reason, we seek from the remotest part of the world, medicines of harsh and violent operation for our relief in several disorders, under which we should never suffer, if we would use what the Bee collects for us at our doors.¹¹
The observation held. The nineteenth century saw the rise of proprietary patent medicines: laudanum-based cough syrups, cocaine-based lozenges, alcohol-heavy elixirs marketed to households through newspapers and mail order. The twentieth century industrialized that market. Dextromethorphan was patented in the 1950s, sold under proprietary brand names, marketed to parents through television. The recipe on the counter (honey with lemon, honey with vinegar, honey with fig, honey with coltsfoot, honey with thyme, honey with glycerine) was displaced not by evidence but by advertising and shelf space.
Jarvis published the Vermont version in 1958. Kloss had published the Tennessee-Wisconsin version in 1939. Fessenden and McInnes catalogued the honey material comprehensively in 2008. The WHO acknowledged honey for cough in 2001. Penn State confirmed it in randomized trial in 2007. The Cochrane Collaboration confirmed it again in 2018.
At each of these points the establishment position on cough treatment in children shifted slightly closer to what Jarvis’s farmers already did.
The recipe did not move. It was where it had been since before Jarvis was born.
What replaced it
The FDA advisory did not arrive by regulatory initiative. It arrived because pediatricians forced it. Joshua Sharfstein, a pediatrician at Johns Hopkins and later a senior FDA regulator, was among the authors of a March 2007 petition that asked the agency to declare these products contraindicated for children under six. His December 2007 piece in the New England Journal of Medicine, published the same month as the Paul trial, described the market the pediatric community was asking the FDA to move against: 39 percent of U.S. households had purchased these products in the previous three years, and consumers were buying about 95 million packages annually for use in children.¹⁴
The mechanism of the withdrawal was industry self-protection. Manufacturers voluntarily pulled infant products before the January 2008 announcement to avoid a mandatory recall. The two-to-four age band was formally excluded by industry relabeling that same year. The remaining products, for children over four, were left in place with warnings, though the same trials that had cleared under-fours had also failed to demonstrate benefit in the older group.¹
The regulatory response was serious. The public messaging afterward was not. Pediatricians were left to tell parents what to do instead. A physician commentary in NEJM Journal Watch put the new recommendation plainly. “Give fluids and control fever, but don’t give cough and cold medicines.”¹³
The old recipe was fluids that soothed the throat and thinned mucus. Any child would take it, because it tasted of honey and lemon. The whole preparation cost pennies. The advice arrived at, after the industry had killed enough children to warrant the FDA advisory, was a diminished version of what a grandmother would have done in 1900.
What made pediatric cough syrup a 95-million-package-a-year business was not that its products worked better than the folk preparation. They did not work better than the folk preparation. On the primary outcomes of two randomized trials in children, they did not work better than nothing. What made them a 95-million-package-a-year business was that they could be branded, patented, shelf-placed, and advertised. Honey, lemon, and thyme could not. There was no company whose share price depended on the survival of a grandmother’s recipe. There were many companies whose share price depended on the survival of dextromethorphan-based products.
The FDA withdrawal removed the infant portion of that market. The revenue from products marketed for children over four continues.
What’s on the counter
Jarvis called the recipe “many generations old” in 1961. He was describing something already ordinary: the syrup a farmer’s wife would make when a child was coughing at night, the same way she would make broth or apply a mustard plaster. It required no prescription, no pharmacist, no marketing budget, no clinical trial. It required a lemon, a jar of honey, a small pinch of thyme from the herb garden, and ten minutes.
The Penn State trial did not discover the recipe. The WHO did not discover it. Cochrane did not discover it. What each of these did was confirm, in the register of institutional science, what farmers in Vermont and grandmothers in every other country had known for as long as anyone had kept bees.
The lemon costs about a dollar. The honey costs between five and fifteen dollars a jar, and one jar lasts a long time. Thyme is a garden herb that grows in a pot on a windowsill. If the lemon is not available, apple-cider vinegar is in the pantry. The whole preparation takes ten minutes to boil the lemon and thirty seconds to assemble. It does not upset the stomach, and it can be given to children over one. It works when the industrial products do not, or more precisely, it works when the industrial products have been shown not to work at all.
Every one of the relevant documents is public. The Paul study is on PubMed and the FDA advisory is in the Federal Register. Jarvis’s book has been in continuous print for over sixty years. Nothing about this argument has been hidden. The disagreement between what the trials established and what the pharmacy shelves offered lasted a full century and cost the lives of children.
The recipe is on the counter. It always has been.
Making the syrup
Ingredients (fills one 8-ounce / 240 ml glass or mason jar)
1 fresh lemon (or 2 tablespoons apple-cider vinegar as substitute)
1 fresh sprig thyme (or ½ teaspoon dried thyme)
About 1 cup (240 ml) of water, for boiling the lemon
Honey to fill the remainder of the glass, roughly ⅔ of the volume (about 5 fluid ounces / 150 ml / 10 tablespoons)
Method
Bring about 1 cup of water to a simmer in a small saucepan. Add the whole lemon and the thyme sprig. Simmer slowly for ten minutes. The heat softens the rind and extracts the lemon juice, and it draws the thymol and volatile oils out of the thyme into the water. Remove the pan from the heat. Fish out the thyme sprig (or strain if using dried thyme) and discard.
Cut the lemon in half and squeeze the juice into your glass or jar. Add 2 tablespoons (30 ml) of the thyme-and-lemon water from the saucepan. Fill the rest of the glass with honey, stirring as you go until the mixture is smooth. You will use roughly 10 tablespoons of honey to fill an 8-ounce glass.
If using apple-cider vinegar instead of lemon, simmer the thyme alone in about ½ cup of water for ten minutes. Strain and discard the thyme. Add 2 tablespoons of the thyme water and 2 tablespoons of apple-cider vinegar to the glass, then fill the rest with honey. The vinegar variant is well-attested in the folk record.
Dose
For an occasional daytime coughing spell: one teaspoonful, stirred before taking.
At bedtime: one teaspoonful, and one more during the night if the cough wakes the child.
For a severe cough: one teaspoonful on rising, one mid-morning, one after lunch, one mid-afternoon, one after supper, one at bedtime. Reduce the frequency as the cough eases.
For small children: half a teaspoonful, taken more often.
Take the syrup warm when possible. The warmth releases the thyme’s volatile oils and delivers a portion of the active compounds to the airway by inhalation as well as by swallowing.
The Jarvis variant, with glycerine
Jarvis’s original Vermont formulation adds glycerine to extend the throat-coating time. Glycerine is a purified vegetable compound rather than a whole food, but it has been in traditional folk use since the nineteenth century and provides a longer-lasting demulcent film on the throat than honey alone. Readers who want Jarvis’s exact recipe, or who want the extended contact time, use this variant:
Ingredients (fills one 8-ounce / 240 ml glass or mason jar)
2 tablespoons (30 ml) vegetable glycerine, USP grade, from any pharmacy
Honey to fill the remainder, about 5 fluid ounces (150 ml, or roughly 10 tablespoons)
Optional: 1 sprig fresh thyme or ½ teaspoon dried thyme, added at the boiling step
Method
Simmer the lemon in about 1 cup of water for ten minutes (with the thyme if using). Remove and discard the thyme. Cut the lemon in half and squeeze the juice into the glass. Add the glycerine and stir. Fill the rest with honey and stir again.
The dose is the same as for the primary recipe.
Cautions
Do not give honey to infants under one year of age.Clostridium botulinum spores can be present in raw honey. In older children and adults, mature gut flora and stomach acid prevent them from germinating and they pass through without effect. In an infant’s immature digestive tract, they can produce botulinum toxin. The toxin causes the harm, not the organism. The caution is not disputed.
Thyme. Use sparingly, as Kloss advised. A sprig or half a teaspoon of dried herb is enough per glass. Not recommended in medicinal doses during pregnancy. Culinary amounts in food are fine; a therapeutic syrup is the caveat.
Raw versus pasteurized honey. Raw honey is preferable when available. It retains the enzymes, phenolic compounds, and volatile aromatics that pasteurization heat degrades. Pasteurized honey works and delivers the demulcent and osmotic action, but the extra biochemical richness of raw honey is lost in the heating. Darker varietals (buckwheat, if available; otherwise wildflower, manuka, or dark forest honeys) contain more phenolic compounds than pale varietals like clover, but any real honey works. Read the label: some supermarket “honey” is cut with corn syrup or rice syrup and is not honey at all. On the infant botulism question: pasteurization does not eliminate the risk. Clostridium botulinum spores are heat-resistant far beyond standard honey pasteurization temperatures. The under-one caution applies to both raw and pasteurized honey.
Storage. The finished syrup keeps in a sealed glass jar (a mason jar works well) for several weeks at room temperature, and longer refrigerated. The honey’s osmotic action and the lemon or vinegar acidity together create a hostile environment for microbial growth. Give it a stir before each dose, as the honey may settle. If the syrup ever develops off smells, cloudiness that wasn’t there originally, or fermentation bubbles, discard and make a fresh batch.
References
1. Paul IM, Beiler J, McMonagle A, Shaffer ML, Duda L, Berlin CM Jr. Effect of honey, dextromethorphan, and no treatment on nocturnal cough and sleep quality for coughing children and their parents. Archives of Pediatrics and Adolescent Medicine 2007;161(12):1140–1146.
2. Axelsson I. Honey, not dextromethorphan, was better than no treatment for nocturnal cough in children with upper respiratory infections. Evidence-Based Medicine 2008;13(4):106.
3. Oduwole O, Udoh EE, Oyo-Ita A, Meremikwu MM. Honey for acute cough in children. Cochrane Database of Systematic Reviews 2018, Issue 4. Art. No.: CD007094.
4. U.S. Food and Drug Administration. Public Health Advisory: Nonprescription Cough and Cold Medicine Use in Children. Issued 17 January 2008.
5. Centers for Disease Control and Prevention. Infant deaths associated with cough and cold medications, United States, 2005. MMWR Morbidity and Mortality Weekly Report 2007;56(01):1–4.
6. Consumer Healthcare Products Association. Voluntary withdrawal of oral infant cough and cold medicines announced October 2007; pediatric labeling change announced October 2008.
7. Jarvis DC. Folk Medicine: A Doctor’s Guide to Good Health. First published New York: Henry Holt, 1958. UK edition consulted: London: Pan Books, 1961. Chapter 9, “An Old-Fashioned Cough Remedy,” pp. 105–106.
8. Kloss J. Back to Eden. First published 1939. Revised edition, Back to Eden Publishing, 2009. Glossary; entries on lemon, coltsfoot, thyme, and bronchitis; Section II, Chapter 3, Herbal Syrups.
9. Journey JD, Bhattarai S, Agrawal S. Dextromethorphan. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing, 2024. See also: Nguyen L, Thomas KL, Lucke-Wold BP, et al. Dextromethorphan: An update on its utility for neurological and neuropsychiatric disorders. Pharmacology & Therapeutics 2016;159:1–22.
10. Paul IM, Yoder KE, Crowell KR, et al. Effect of dextromethorphan, diphenhydramine, and placebo on nocturnal cough and sleep quality for coughing children and their parents. Pediatrics 2004;114(1):e85–e90.
11. Fessenden R, McInnes M. The Honey Revolution: Restoring the Health of Future Generations. 2008. Chapter 9, “Honey That Soothes and Heals,” pp. 141–146.
12. World Health Organization, Department of Child and Adolescent Health. Cough and Cold Remedies for the Treatment of Acute Respiratory Infections in Young Children. Geneva: WHO, 2001.
13. NEJM Journal Watch. FDA warns against use of cough medicines in children younger than 2 years. Commentary published 12 September 2007.
14. Sharfstein JM, North M, Serwint JR. Over the counter but no longer under the radar: pediatric cough and cold medications. New England Journal of Medicine 2007;357(23):2321–2324.
15. Blumenthal M, ed. The Complete German Commission E Monographs: Therapeutic Guide to Herbal Medicines. Austin, Texas: American Botanical Council, 1998. Monograph on thyme (Thymi herba).
The most important question we should be asking after Karim Khan’s dismissal last week as chief prosecutor of the ICC – the international war crimes court in The Hague – is not whether he is guilty of “sexual misconduct” against another staff member, identified as “Sarah”.
That can only be decided through a legal process – one, let us note, that has already taken place. A fact-finding body carried out a lengthy investigation of Sarah’s allegations over more than a year; its thousands of pages of evidence were then evaluated in detail by three senior judges.
Though you would not know it from the media coverage, they concluded that there was no evidence to suggest any kind of misconduct by Khan, sexual or otherwise.
Strangely, that determination was largely confirmed by an extraordinarily deferential “exclusive” CNN interview with Sarah, aired earlier this month.
She declined to give any meaningful details of what Khan had allegedly subjected her to, and celebrity interviewer Christiane Amanpour delicately avoided pressing her for any clarification.
No matter. The purpose of the CNN interview was never about excavating facts. It was designed to offer face-saving cover as an entirely political body called the Assembly of States Parties, comprising diplomatic representatives of the 125 states signed up to the ICC, entirely ignored the legal findings and dismissed Khan.
Paradoxically, it was the Assembly of States Parties that appointed the judges who had concluded that there was no evidence of misconduct or breach of duty by Khan. That inconvenient judgment was simply reversed, despite the Assembly members being in no position to weigh the evidence themselves.
We should not forget that many of these states have an investment in weakening the only international court that can bring their own senior officials to trial for war crimes.
In May 2024 – shortly before Sarah made her allegations – the ICC demonstrated that it was finally ready to prosecute western leaders for war crimes, not just those from the Global South or from the West’s official enemies, such as Russia’s Vladimir Putin.
Khan issued an arrest warrant for Israeli prime minister Benjamin Netanyahu and his former defence minister Yoav Gallant. Both are accused of crimes against humanity for starving the people of Gaza through a prolonged blockade of food, water and power.
Were Netanyahu ever to face trial – and found guilty, as he almost certainly would be – a lot of other leaders would have good reason to fear they might be found culpable next, not least for their complicity in Israel’s mass slaughter of Palestinians in Gaza.
The question that needs answering now is not whether Khan is guilty of misconduct – that has been decided at a political level, not a legal one. No, we need an answer to an equally political, and far more troubling, question.
“Cui bono?” Or “Who benefits?”
The evidence is hiding in plain sight. The evidence is revealed both in the deeply politicised process that led to Khan’s downfall, and in what that process means for the future of the court.
Covert war
Khan is not the first ICC chief prosecutor to face extreme pressures – and, as with Khan, those pressures surfaced at the very moment Khan’s predecessor tried to take on Israel over its war crimes.
Fatou Bensouda faced a “covert war” waged against her by Israel for the best part of a decade, according to an investigation by the Guardian in May 2024, just as Khan issued his arrest warrant for Netanyahu.
The Guardian’sreport, published nearly three years after Bensouda had completed her nine-year term at the ICC, revealed that, during that time, she had faced threats to herself and her family, the monitoring of her communications, and an intimidating visit to her home.
More recently, Bensouda has confirmed these accounts in an interview with Al Jazeera. Bensouda notes that she repeatedly reported Israel’s campaign of intimidation to the Dutch authorities, but they did nothing to investigate the threats or protect her.
She also says certain “authorities” – she does not name them – warned her that she was going too far in investigating Israeli crimes and that “you could be harmed or you could be killed, or family members could be harmed in some way.”
The campaign of threats – instigated by Yossi Cohen, then the director of Israel’s spy agency, Mossad – intensified as Bensouda considered whether to open a formal investigation into Israeli war crimes and crimes against humanity in the illegally occupied Palestinian territories.
Israel’s crimes against the Palestinian people, we should remember, predate – by decades – Hamas’ attack on 7 October 2023. In fact, though no one is supposed to mention it, Israel’s sustained crimes of occupation are the self-evident cause of that Hamas attack.
An Israeli source told the Guardian that “the Mossad’s objective was to compromise the prosecutor or enlist her as someone who would cooperate with Israel’s demands”– that is, scrap the ICC’s investigation into Israeli crimes. Another source admitted that Cohen was acting on Netanyahu’s instructions.
During one contact, Cohen reportedly issued a Mafia-style threat to Bensouda: “You don’t want to be getting into things that could compromise your security or that of your family.”
The Guardian reported that the Mossad “took a keen interest in Bensouda’s family members and obtained transcripts of secret recordings of her husband, according to two sources with direct knowledge of the situation. Israeli officials then attempted to use the material to discredit the prosecutor”.
The paper also noted that there were fears among senior ICC officials that “Israel had cultivated sources within the court’s prosecution division” – the division Khan would inherit from Bensouda.
Cohen was described as “stalking” Bensouda, and personally “ambushed” her in a hotel room in New York in 2018. Afterwards he repeatedly phoned her, in a threatening manner that was said to have escalated over time. When Bensouda asked Cohen how he had obtained her phone number, he reportedly replied: “Did you forget what I do for a living?”
According to the Guardian :
On one occasion, Cohen is said to have shown Bensouda copies of photographs of her husband, which were taken covertly when the couple were visiting London. On another, according to sources, Cohen suggested to the prosecutor that a decision to open a full investigation would be detrimental to her career.
Between 2019 and 2020, the Mossad had been actively seeking compromising information on the prosecutor and took an interest in her family members.
The spy agency obtained a cache of material, including transcripts of an apparent sting operation against her husband.
Israel used the materials to mount a “smear campaign” against her, but one that ultimately proved unsuccessful.
Concerted backlash
When Khan took up the role of ICC chief prosecutor in June 2021, he proved reluctant to pick up where Bensouda had left off on the Palestine case. Presumably, he was only too aware of the retaliation from Israel against her.
Bensouda had announced in December 2019 that she had grounds to open a full criminal investigation into allegations of war crimes in Gaza, the West Bank and East Jerusalem.
However, in the face of a concerted backlash from western states, she delayed opening the investigation. She first sought a ruling from a pre-trial chamber of ICC judges – presumably in the hope it would serve as some kind of insurance policy – on whether the court had jurisdiction over the occupied Palestinian territories.
By February 2021 the judges confirmed what was already self-evident. The court did have such jurisdiction because Palestine had been signed up to the court since 2015.
Bensouda stepped down a few months later.
The door was now open for Khan to prosecute Israeli officials for war crimes. However, the new chief prosecutor gave every appearance – perhaps understandably – of preferring to sit on his hands.
It was not just Israel that had been fearsomely opposed to its officials being tried for war crimes. Washington was equally incensed at the prospect – sometimes, it seemed, more so than over the possibility that US officials might also face arrest warrants for crimes committed by the US military in Afghanistan and Iraq.
Between 2019 and 2020, during Trump’s first presidency, the US imposed severe visa restrictions and financial sanctions on Bensouda. Mike Pompeo, then US secretary of state, linked the sanctions to the Palestine case: “It’s clear the ICC is only putting Israel in [its] crosshairs for nakedly political purposes.”
Khan might well have avoided pursuing Israel indefinitely had it not been for the events that followed 7 October 2023.
Israel’s mass slaughter of Palestinian civilians in Gaza, its devastation of the enclave’s homes and infrastructure, and its starvation of the entire population were actions so criminally abhorrent that UN agencies, major human rights groups and Holocaust scholars were soon all in agreement that they amounted to genocide.
In May 2024, Khan announced arrest warrants against Netanyahu and Gallant, as well as three Hamas leaders subsequently killed by Israel.
Tsunami of threats
Shortly before Khan made that announcement, 12 senior US Senators had sent a threatening letter to the ICC: “Target Israel and we will target you.” The letter ended: “You have been warned.”
Describing Israeli and US sovereignty as inseparable, the senators reminded Khan that Washington had demonstrated “the lengths to which we will go to protect [our] sovereignty.”
A 2002 law, popularly known as “The Hague Invasion Act”, authorises the US president “to use all means necessary and appropriate” to bring about the release US persons and any allies imprisoned or detained by the ICC. Those allies, it goes without saying, include Israeli leaders.
Such threats, it should be noted, are a violation of Article 70 of the Rome Statute.
Following the issuing of the arrest warrants, there followed a tsunami of similar threats – and presumably more that have yet to become public – against Khan and the ICC.
A British-Israeli lawyer within the ICC – one known to have ties to Netanyahu’s legal adviser – warned Khan “they will destroy you and they will destroy the court” if the warrants were not rescinded. He urged Khan to “climb down the tree” and drop the case.
The UK’s foreign secretary of the time, David Cameron, phoned Khan to tell him Britain would defund the court and withdraw from the Rome Statute that founded the ICC if Khan did not back down.
Cameron warned Khan that he was “on the brink of making a huge mistake” and urged him to “take a step back and consider things”. He added that applying for arrest warrants for Israeli officials was tantamount to “dropping a hydrogen bomb”.
Meanwhile, Trump issued an executive order imposing aggressive financial sanctions against Khan and other ICC officials, including several of its judges.
Khan himself received warnings that Israel’s Mossad was continuing its operations in The Hague, where the ICC is located, to monitor and compromise the court’s investigators as they compiled evidence on Israel – just as it had done earlier under Bensouda.
Khan publicly stated that retaliatory threats and intimidation were explicitly targeting members of his own family.
Untouchable criminals
What conclusions should we draw from all of this?
Quite aside from the matter of whether Sarah’s allegations of “sexual misconduct” are true or not, it is clear that Israel and the US have been digging for dirt – and apparently ready to fabricate such dirt – on any chief prosecutor who tries to hold them to account for their crimes.
Both have indicated that they are ready to manipulate legal and political processes to ensure the outcome they desire: that they remain untouchable.
We have a template for how this plays out. Julian Assange, founder of the whistle-blowing site Wikileaks, published details in 2010 of US and British war crimes in Afghanistan and Iraq. Almost immediately he found himself entangled in accusations of sexual misdemeanours – in his case in Sweden – that were similarly amplified by an uncritical western media.
Assange faced years in various forms of confinement while the US and UK pressured Sweden to keep alive an investigation against him Swedish prosecutors at least twice sought to drop for lack of credible evidence.
In fact, the US and UK never wanted the evidence tested – they were quite happy with a permanent, unresolved “investigation” – precisely because they knew it would have been unlikely to withstand judicial scrutiny.
The point was simply to generate constant headlines about “rape”, turning Assange into a pariah, justifying his effective disappearance from public life, severely weakening Wikileaks as a whistleblowing platform, deflecting attention from the all-too-real crimes committed by the US and Britain, and paving the way to a political show trial to extradite him to the US on entirely confected “espionage” charges.
This has been repeated in the case of Khan and the ICC. In Khan’s case, the evidence was tested and found inadequate. So the legal process has been replaced by a flagrantly political one.
Khan has been turned into a legal pariah, even stripped of his right to work as a lawyer in the UK by the British Bar Association.
The ICC has been further weakened, just as Israel and the US have expressly stated they wanted it to be. Marco Rubio, Trump’s secretary of state, has recently launched an official campaign to dismantle the ICC “brick by brick”.
He says: “Now they [the ICC] are going to see the consequences”. Consequences of what? Of seeking to enforce international law against a key US client state.
Meanwhile, accountability for the all-too-real crimes being committed by Israel in Gaza, Lebanon and the West Bank – and actively supported by western states like the US, Germany and Britain – recedes yet further into the background
As each brick protecting the ICC is dismantled, a brick is added to the wall of protection around Netanyahu and Israel’s genocidal war machine.
Israel, meanwhile, is barely concealing that it has been masterminding the effort to destroy the ICC.
According to Guy Azriel, the diplomatic correspondent for i24 News, Israeli foreign Minister Gideon Sa’ar “oversaw a dedicated task force and employed intensive diplomatic efforts aimed at securing Khan’s removal from office”.
Hillel Neuer, director of the Israel apologist group United Nations Watch, cheered what he called “our campaign to remove” Khan, and warned Francesca Albanese, the UN’s legal expert on the occupied Palestinian territories, “you’re next”.
Like Khan, Albanese has been searching for practical, legal ways – not just rhetoric – to hold Israel and its western allies to account for the crimes in Gaza.
Predatory states
The ICC claims its work will not be affected by Khan’s removal and that the arrest warrants against Netanyahu and Gallant will still be pursued under new stewardship. That seems doubtful.
Israel and the US are cranking up the intimidation of the ICC, which has no tools – beyond the support of members states – to enforce its rulings or protect itself from the hostility of a rogue superpower.
Currently the court appears paralysed, allowing Israel to muddy the waters with interminable, and vexatious, appeals against the arrest warrants.
Any lawyer who takes up the post of ICC chief prosecutor will be only too aware of the fate that befell Khan and the campaign of intimidation against Bensouda as soon as each tried to enforce accountability on Israel and its western patrons.
It will take a very brave individual indeed to renew that task. Khan’s successor will understand that, in any further confrontation with Israel and Washington, the US will not hesitate to crush the ICC and, with it, remove the only effective restraint on criminality by powerful states.
More likely, however, the Assembly of States Parties – the political body that ousted Khan – will privately require from his successor reassurances that the new chief prosecutor reliably defer to the principle of Israeli and western impunity. Only someone less willing to ruffle feathers stands any chance of being appointed.
That was the clearest of messages sent by the Assembly when a majority of member states voted to be rid of Khan. The short-lived experiment in creating a mechanism for enforcing international law is over. We are back to the law of the jungle.
Hundred of thousands of people around the world – more likely millions – will now find themselves even more exposed to the criminal actions of predatory states. Unlike Khan’s accuser, they are unlikely to ever get their day in court.
Israel carried out massive detonations involving around 700 tons of explosives around Lebanon’s historic Beaufort Castle – a UNESCO World Heritage site – with the huge blasts being heard across large parts of the country’s south late on 30 July.
The violent detonations were carried out under the pretext of alleged Hezbollah infrastructure under the Crusader-era fortress. This has been denied by Lebanese authorities.
“Israeli forces carried out unprecedented bombardment in southern Lebanon, triggering a series of powerful explosions that residents said were unlike anything heard in recent years,” Al Manar TV reported on Friday.
Lebanon’s National News Agency(NNA) also reported the blasts, calling them “massive” and “unprecedented,” while confirming that they were heard across the whole south.
“The blasts echoed across all of south Lebanon with unprecedented intensity, and their shockwaves reached the Iqlim al-Kharroub and Khaldeh regions,” the report said, adding that “violent explosions in the Beaufort Castle area shattered the glass of several windows in homes in the town of Qlayaa.”
Lebanese Parliament Speaker Nabih Berri condemned the violent detonations.
“The shockwaves from these terrorist explosions, caused by 700 tons of explosives, registered 3.8 on seismic monitoring scales and were felt by Lebanese citizens from the South and Mount Lebanon all the way to the outskirts of Beirut,” he said.
Lebanon’s Culture Ministry released a statement saying Beaufort Castle was unharmed.
However, it stressed that because the area remains under Israeli occupation, specialized technical teams have been prevented from accessing the site in order to conduct a proper assessment of any potential damage.
Earlier in July, the castle had been placed on UNESCO’s list of sites “in danger.”
The massive detonations were announced by Israeli Prime Minister Benjamin Netanyahu and Israel’s War Ministry late on Thursday evening.
In a joint statement, Netanyahu and War Minister Israel Katz claimed a Hezbollah tunnel network under the castle was destroyed.
They also confirmed the unprecedented amounts of explosives used in their “operation.”
Israeli occupation forces will “remain in the security zone in southern Lebanon and will continue to destroy all terror infrastructure to prevent any attempt by Hezbollah to restore its capabilities,” they added.
Lebanon’s Directorate General of Antiquities has previously rejected Israeli claims that the site contained Hezbollah infrastructure.
Israeli maps and videos detailing “terrorist infrastructure” are fabricated, and the fortress has been under Lebanese state administration since 2000, placing under enhanced protection in line with the 1954 Hague Convention.
Lebanese geologists have warned that demolitions of this scale near major fault lines could potentially trigger human-induced seismic activity.
Israeli forces occupied the castle in May 2026 and framed the move as a major strategic victory. Hebrew media challenged this narrative at the time.
Israeli forces were unable to maintain a consistent presence in the historic site due to constant resistance operations – namely Hezbollah’s FPV drone strikes that have inflicted heavy casualties and losses on the Israeli occupation forces since March.
Since the violent detonations near the castle on Thursday night, Israel has continued destroying civilian infrastructure across south Lebanon.
Heavy explosions were recorded in Deir Siryan on Friday, while Israeli shelling continued to target the Ali al-Taher Hill.
Over 4,300 have been killed and more than a million displaced by Israel in Lebanon since 2 March.
Tens of thousands of civilian homes and buildings – amounting to practically all of south Lebanon’s border villages – have been eradicated.
Israeli occupation forces refuse to withdraw, and the Lebanese government has signed a US-brokered deal allowing Tel Aviv to maintain its illegal presence in the country.
Donald Trump entered the July 7th/8th NATO summit having recently condemned the alliance as a “paper tiger” over its collective failure to abet the calamitous Zionist-American war on Iran and repeatedly threatened to withdraw US forces from Europe, with reveries of Greenland’s annexation still abounding. He left boasting of the intense “love” and “unity” within NATO, while praising member states for their reaffirmed commitment to spending ever-increasing vast sums on ‘defense’. Meanwhile, the Ukraine proxy war’s world-threatening continuation appears assured for potentially years to come.
As such, the NATO summit signifies a significant triumph in Britain’s never-ending battle to exploit the US Empire to further its own objectives. Highly revealing leaked files amply spell out how the alliance is a key mechanism by which Washington’s “interest” in Europe and West Asia is insidiously maintained, via London’s covert and overt machinations. NATO provides an invaluable “umbrella”, by which Britain projects economic, intelligence, military, and political power throughout these regions and the wider world, while countering competitors.
The documents were authored in March 2021 by Chris Donnelly, a veteran British military intelligence apparatchik who masterminded NATO expansion into the former Soviet Union, Warsaw Pact, and Yugoslavia throughout the 1990s. Now an influential Ministry of Defense advisor guiding London and Kiev’s escalatory strategies in the proxy war, he writes in the leaks of Britain’s perpetual struggle to retain the “security” provided by “US military power.” This, combined with access to Washington’s globe-spanning intelligence network, “underpins our own position in the world.”
From Britain’s perspective, “the political solidarity between member nations” within NATO and “the permanent political and military mechanisms that enable collaboration between its members and with its partners,” are as vitally important as the alliance’s capacity for “collective defence and security.” For example, “interoperability” between NATO members is considered “both a political and a military asset” and “a valuable product”, enabling countries “with vastly different political and military systems to operate together.” That includes “[undertaking] complex and stressful military activities,” and other joint functions.
This makes NATO “a civilian-led political organisation… whose main tool is armed force,” intimately entrenched within its 32 members. Lacking any democratic structures internally and accountable to none externally, the alliance exerts enormous, often unseen influence over members’ constituent governments, security and intelligence services, militaries, police forces, and more. These “extensive political collaborative mechanisms” mean states can be corralled into adopting policies or taking actions regardless of local public will, or whether such moves actively harm their safety and/or national interests.
“Without the US, there is no NATO,” Donnelly notes. Hence, to “keep the US interested” in the alliance, Washington “must see a return on its (still very large and disproportionate) investment.” The 2026 NATO summit ended with European leaders pledging to plunge tens of billions into US-made military equipment for Kiev over this year and next, a prospect offering Washington quite some “return”. But the British have other means of encouraging and maintaining US hegemony, for their personal profit.
‘Symmetrical exchange’
Elsewhere, Donnelly writes of the “special relationship” – the “political/military/security/intelligence” alliance between Britain and the US, “which has existed since World War II.” He notes how from inception, Washington was driven “by how much the US needed something from the UK to help the US develop and maintain its superpower status.” In other words, “what the UK could provide the US… the US could not itself produce.” Accordingly, London “traditionally contributed” its historical “knowledge and experience” to Washington’s crusade for global domination.
This frequently entailed “intelligence-gathering and analysis; technical expertise, especially inventiveness, ideas, and scientific information; the experience of having dealt with a situation new to the US.” Meanwhile, “political and military support” was provided by London “wherever this supported US policy interests and to help the US get what it wanted in the world.” While Britain’s methods in every regard have evolved significantly over time, these ultimate underpinning and overriding objectives in so many matters military, intelligence, foreign, and even domestic have not changed:
“Being able to provide something the US wants and needs is still the only reliable way to get US respect and to maintain the ‘special relationship’… Today, this is translated into whatever will help the US maintain its position in the world, promote US interests… and ensure US economic well-being. If we can still provide something useful for the US, something they cannot do for themselves, then they will be prepared to reciprocate very generously.”
Donnelly frames this concord as a perpetual “barter deal” – not a “symmetrical exchange” or “issue of cost and payment,” as “if the US can buy what it is deficient in on the world market, then there is no basis for the ‘special relationship’.” He references Britain’s consistent “willingness and ability to deploy a significant contingent of effective army… to reinforce US military operations… readiness to share casualties… [and] continued readiness to host US forces on UK soil or on overseas dependencies” as historic pull factors.
Britain can also “employ other kinds of power to achieve an effect which supports US policy or interests.” This includes “economic power, political influence, a technical ability, such as cyber-warfare, or a civilian state-building or humanitarian relief capability.” Accordingly, files leaked by Edward Snowden indicate British signals intelligence agency GCHQ is acutely aware it “must pull its weight and be seen to pull its weight” by its NSA ‘partner’, to reap vast US funding for elaborate foreign spying operations.
Donnelly concludes, “On balance, the special relationship is of real importance to the UK, but also of some worth to the US… The burden of sustaining the special relationship falls principally to the UK. The US may well lose out if the relationship fails, but it will not notice the loss as much as the UK will. However, the special relationship is neither permanent nor guaranteed. We cannot take it for granted. It needs to be worked at constantly, refreshed and renewed.”
‘Defense capabilities’
On the subject of renewal, Donnelly lamented how London’s utility to the US Empire had been “significantly diminished” over recent years. This resulted from the British Army’s “indifferent military performance in Iraq and Afghanistan,” the “run-down of our intelligence capability,” and “the perception (on the part of the US and other allies) the UK is no longer investing sufficiently in its military to be able to play the leading role it used to do in Europe, both as an operator and as a technical innovator.”
Donnelly moreover noted Britain “used to be at the cutting edge of some aspects of military thinking,” but had in many respects “lost this edge.” For example, “we can no longer instruct the US on how best to conduct counter-insurgency operations.” Furthermore, the “special relationship” was “put under pressure” by President Barack Obama’s “reorientation of US strategy to focus on China.” Instituted in 2011, this “pivot to the Pacific” was sustained under subsequent administrations, with varying degrees of intensity.
Donnelly cheered how “the Ukraine and Syrian conflicts have reawakened US interest a little” in Europe and West Asia, meaning “Russia can no longer be ignored” by Washington. Nonetheless, he warned, “we have not yet turned the corner.” Unmentioned by Donnelly was his personal role in disrupting Washington’s “pivot” toward China by inflaming the Ukrainian war, to ensure the Empire didn’t “ignore” Russia. He openly articulated this malign mission while testifying to a British parliamentary defense committee in July 2014.
Donnelly proposed establishing a permanent British “standing force” in the Baltics, to conduct military exercises on Russia’s border, while serving as a “tripwire” to “dissuade and deter” Moscow. He believed it “very important” for London to pursue this strategy, as “Britain’s leadership… will encourage the Americans to take a greater interest in NATO and reinforce their support of the organisation.” He added, “we have an important role to play in bringing the Americans in more,” as “US eyes” had recently been directed “away from Europe.”
Resultantly, London provocatively dispatched thousands of soldiers to Russia’s periphery. Moreover, Britain took the lead in training Ukrainian forces – including notorious Neo-Nazi paramilitary factions such as the Azov Battalion. At the time, Washington adhered to the “Obama Doctrine”, which stipulated the US should avoid escalation against Moscow and prohibited provision of “lethal aid” and other military assistance to Kiev. A February 2015Kyiv Post report on Britain’s training program quoted Donnelly at length, suggesting his central involvement in its delivery:
“This is just the sort of help Ukraine needs now. The British Army obviously brings considerable operational experience and a pretty good reputation.”
As Donnelly predicted in his defense committee testimony, Britain’s tutelage of Ukrainian forces had the desired effect of “bringing the Americans in more.” In July 2015, it was announced the US would formally begin training Kiev’s military by the end of the year. Still, a State Department spokesperson stressed the effort was merely “small unit training… to help strengthen Ukraine’s internal defense capabilities.” They firmly asserted Washington’s focus in the country remained on “nonlethal aid” and “there is no plan to change that.”
Fast forward to December 2017, and Trump greenlit the provision of weaponry to Kiev. It was among a number of hostile acts during his first term that ratcheted tensions between Washington and Moscow, placing Ukraine firmly on the warpath with Russia. The recent NATO summit, and subsequent pledges by the US to assist Ukraine directly with drone and patriot missile production, show the Empire has “turned the corner” at last. US “interest” in Europe is assured, for at least as long as the proxy conflict endures.
For over a century, remarkable therapies have been suppressed to maintain a medical monopoly at the expense of humanity
A Midwestern Doctor | The Forgotten Side of Medicine | August 6, 2026
Story at a Glance:
Modern medicine is built around costly, narrowly approved drugs that treat (but rarely cure) specific disease franchises, with regulatory approval correlating more strongly with money spent than with real therapeutic value.
To enforce this, for over a century the same institutions, backed by vast fortunes, have repeatedly sidelined broader or cheaper therapies that threatened those franchises.
The same playbook is used again and again—once a therapy threatens a market, claims of “no evidence” or doctored research amplified by the media will allow regulators to clamp down on the “dangerous and unproven” therapy until it becomes forgotten to history.
In this article, I will illustrate how the exact same playbook was used again and again on numerous transformative medical discoveries endorsed by leading physicians of the era, resulting in nearly every one (e.g., UVBI and numerous cancer treatments) becoming largely forgotten despite immense evidence behind them.
This same playbook was used throughout COVID-19 to eliminate the off-patent therapies that threatened the boondoggle. One of these, chlorine dioxide, was not only repeatedly shown to eliminate COVID outbreaks, but also to do the same with malaria, where it likewise was banned.
Pierre Kory and Jenna McCarthy’s recent book The War on Chlorine Dioxide provides a critical body of evidence that chlorine dioxide has treated a myriad of challenging conditions, and that each time it did, a robust censorship apparatus erased those discoveries and retaliated against the discovers—providing a poignant illustration of the medical monopoly in action.
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.
 I followed up on this story, because some were sceptical and didn’t believe it was real or possible, and loudly insisted it was fake. One man who fancied himself an expert because he likes to shoot a gun now or then claimed this was fake, impossible.
I followed up on this story, because some were sceptical and didn’t believe it was real or possible, and loudly insisted it was fake. One man who fancied himself an expert because he likes to shoot a gun now or then claimed this was fake, impossible.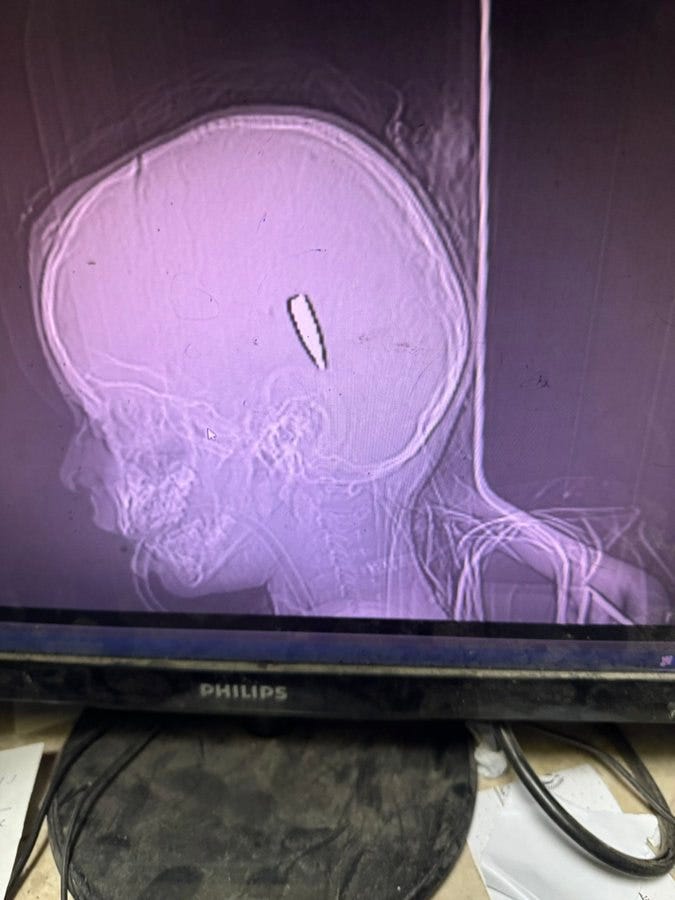
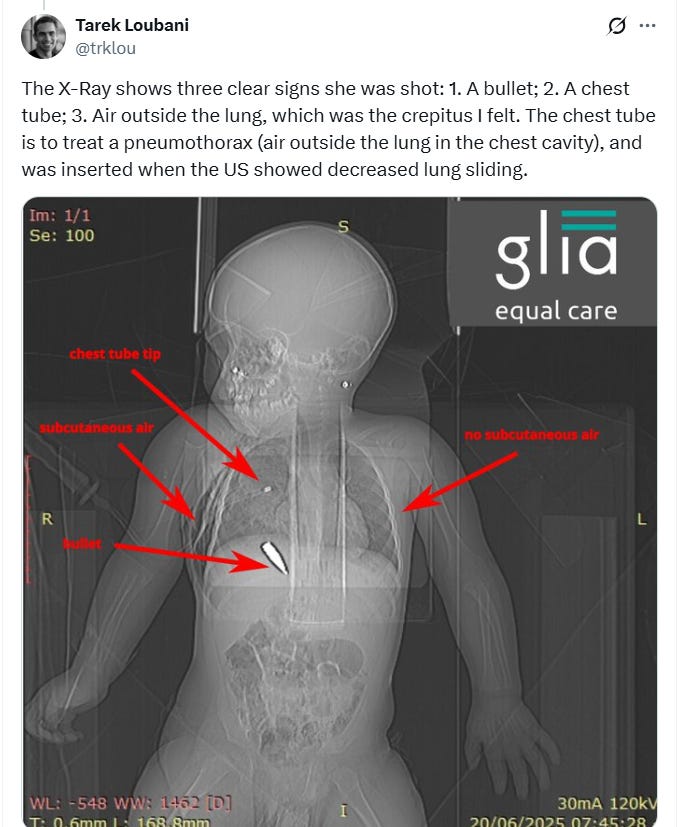
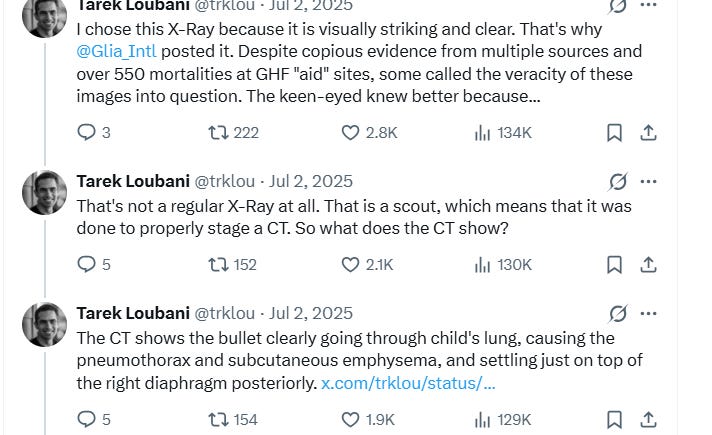








 Modern medicine is built around costly, narrowly approved drugs that treat (but rarely cure) specific disease franchises, with regulatory approval correlating more strongly with money spent than with real therapeutic value.
Modern medicine is built around costly, narrowly approved drugs that treat (but rarely cure) specific disease franchises, with regulatory approval correlating more strongly with money spent than with real therapeutic value. Aletho News
Aletho News