The pandemic is over. Yet two key pieces remain that should concern everyone.
Lets talk about the COVID shot. Still being mandated (recommended) by East and West Coast Health Alliances comprising 14 states all the way down to infants.
Why? To stick it to Kennedy? To ‘follow the science’‘? To secure a market as demand tanks? Who knows for sure but here we are.
The COVID shot was birthed in fraud and failed science. That is the true legacy media pundits won’t tell you.
As the first cases of coronavirus happened in the U.S., Moderna and Pfizer began designing their mRNA vaccine candidates.
Meanwhile, Bill Gates pulled the trigger. A Fauci files/diary email from Gates to Fauci asks the NIAID director for “changes or additions” to Gates’ masterplan titled simply Pandemic I.
Gates’ document, given the stamp of approval from Fauci, stated:
“The goal is to pick the one or two best vaccine constructs and vaccinate the entire world—that’s 7 billion doses if it is a single-dose vaccine, and 14 billion if it is a two-dose vaccine.
How about 9-12 doses? That is what has been recommended to date for adults and immunocompromised respectively.
Far from a stranger, Gates and his foundation were fraudulently close to U.S. agencies funding pieces of NIH and receiving private briefings from DARPA on biological threats. More on that in another report.
FAUCI KILLS EARLY TREATMENT
Under Section 564 of the FD&C Act, FDA can grant the emergency use for a medical countermeasure (the vaccine) because, as revisionist history tells, there was no approved alternatives adequately available for diagnosing, preventing, or treating the disease.
The guidelines and experiences used at the start of the pandemic from pioneers like Peter McCullough’s protocol, New York family physician Dr. Vladimir Zelenko’s protocol, Texas Dr. Richard Bartlett nebulized budesonide, Front Line COVID-19 Critical Care Alliance’s ivermectin push and so many others using similar treatments with repeated success and real-world results tells a different story.
Evidence that would have effectively ended the FDA EUA vaccine hunt.
Didn’t matter to Fauci and the captured U.S. regulatory agencies. Their job was to kill those ideas and pave the way for the coming experimental, world-injecting gene therapy.
Fauci files/diary explains how it was done at the highest level. March 2020, two months into the first U.S. cases Fauci finds himself in a high-level White House Meeting and writes:
“A friend of POTUS… said that he heards [sic] that someone gave Hydroxychloroquine (HC) to 51 people and 51 got better. POTUS has heard similar stories, including Remdesivir (R) about other drugs and wants to make these available. To my amazement and dismay, Azar said that he could approve HC and Remdesivir now with the powers that he has. Steve Hahn and to some extent Deb and Bob started to chime in that this would give people hope. I took a deep breath and said that this was wrong and should not be done.”
None of the trials were designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor were the vaccines being studied to determine whether they can interrupt transmission of the virus. (*I was the first journalist to report this in October 2020)
FDA and VRBPAC votes were near unanimous to get them to market and in American arms while legacy media ‘journalists’ and their ‘experts’ like Fauci and others touted the shot’s transmission-stopping magical qualities. While Influencers and celebrities sucked up $911 million of taxpayer money for their injectable PR efforts.
There was just one problem. The shot didn’t stop transmission. And it didn’t perform against mutations. In short, it was worthless and gave false hope with a growing profile of side effects (harms).
September 2021 Fauci writes:
“… there is a concern about safety regarding myocarditis for younger people, mostly men; however, once this is taken care of in my mind there is no reason not to vaccinate essentially everyone.”
Heart damage from the shot was never “taken care of” and still remains a concern and risk to this day especially for young men.
January 2021, world-renowned HIV virus researcher Dr. David Ho shares immediate concerns about the COVID shot’s performance according to Fauci’s diary:
“David Ho is doing tests on convalescent sera and sera of people who were vaccinated and is finding disturbing data in both the UK and worse in the RSA mutants. It looks like the vaccine might be compromised.”
Fauci continues:
“Had regular every 2 weeks call with Bill Gates – Bill and Trevor Mundel know about the issue with the mutations that David Ho is working on.”
What exactly were Dr. Ho’s warnings? Dr. Ho writes to Fauci the following:
“It is quite clear that these two variants could now resist several classes of neutralizing monoclonal antibodies already used in the clinic or still in development, and in most cases we understand which of the mutations are conferring the resistance.”
Ho continues:
“… a large majority of convalescent plasma samples showed an appreciable loss in activity against the new variants, suggesting re-infection may be more likely when confronted with either of these two strains.”
And then the death blow to the non-transmission-stopping COVID shot as Ho writes:
“Finally, we also observed a significant impact on vaccinee sera in that every serum sample tested showed a substantial loss in neutralizing activity against the SA variant, whereas the loss in activity against the UK virus is not as large or as universal. Again, we believe the latter findings should be shared promptly with the field, because these new strains threaten the effectiveness of the current vaccines.”
The very next day, Fauci writes in his diary:
“Had Zoom briefing of Biden and Harris to prep them for the speech that Biden will give at 3:45 PM on the vaccine rollout plan. We briefed him at 2:30 to 3:30 and he and Harris (only he spoke) gave briefing to the Nation.”
No word of the vaccine issues, mutations or danger now scientifically evident.
It later became clear that Ho was not only right, but his warnings were mild compared to the reality that unfolded. UK COVID vaccine surveillance data began showing the shots were not only failing to prevent infection but they are making you more vulnerable to it.
2022 data suggested that in all age groups COVID vaccines were demonstrating negative efficacy. That means, the vaccinated were at greater risk of infection than the unvaccinated.
Meanwhile, that same year Fauci writes:
“More drama with regard to the CDC and Rochelle Walenski. After much going back and forth between the CDC and the other docs including me… we thought we had gotten them pulled back from making the statement that the vaccines were not effective at all in preventing infection and transmission…
Why? As Fauci writes, “it would undermine the DoJ’s efforts at mandates for vaccines under certain circumstances.”
In the end, CDC director at the time Walensky who, as Fauci writes, called him “… her hero, her mentor, her friend… agreed to pull back on the statement of absolute lack of efficacy of vaccines against infections and transmission.”
Throughout all this, Fauci went to bat for Big Pharma indemnity in 2021 as he pens in his diary:
“I had an important zoom meeting today with Larry Corey an Emilio Emini about the same subject as above, namely, how the United states can play a major proactive role in getting mRNA vaccines to the developing world. Apparently there are liability issues that the pharmaceutical companies are concerned with. These revolve around the fact that although the United States government can indemnify the companies against lawsuits here in the United states the companies feel that they are liable to being sued for adverse outcomes by people in the countries to whom they’re providing vaccine. Some mechanism needs to be worked out to address this concern.”
(Emilio Emini was Chief Executive Officer at the Bill & Melinda Gates Medical Research Institute and Larry Corey head of COVID-19 Prevention Network collaboration formed by Fauci)
The shot is still protected by the PREP Act which was extended until 2029 by outgoing HHS Secretary Xavier Becerra (now in the running for California Governor).
The Countermeasures Injury Compensation Program (CICP) meant to field harms from the COVID shot is a black hole and sick joke. Kennedy is attempting to create a table of accepted injuries to ease compensation efforts for the injured public. Is this enough? Not by a long shot.
(*No artificial intelligence was used to write this article. Just a genuine human… me)
The US Senate Homeland Security Committee has voted to hold Dr. Anthony Fauci in contempt after the former White House coronavirus czar refused to answer questions on the origins of Covid-19 at a hearing last week.
The Republican-led committee voted 8-7 along party lines to hold Fauci in contempt on Thursday. The committee’s Democrats introduced five motions aimed at postponing the vote, but all were shut down by the Republican majority.
Fauci appeared before the committee last Wednesday, where he was grilled on his role in funding dangerous gain-of-function research at the Wuhan Institute of Virology in China, his knowledge that Covid-19 was likely created in a laboratory, his work with US intelligence agencies, and his promotion of ineffective vaccines against the virus.
The former bureaucrat refused to answer any questions, invoking his Fifth Amendment right to silence more than 100 times. Fauci pleaded the Fifth despite having already received a pardon from former President Joe Biden shielding him from criminal prosecution over any offense committed between January 1, 2014 – when the US first outsourced gain-of-function research to China – and January 20, 2025.
“More than a million Americans died from Covid,” committee chairman Rand Paul said before Thursday’s vote. “Many of them died alone. Workers were forced to choose between a mandate and a job they needed. Businesses closed and never reopened. Americans lost the freedom to work, to worship, and to decide what went into their own bodies.”
“Dr. Fauci faced no risk of federal prosecution,” Paul continued. “All he had to do was tell the truth.”
Although Fauci is immune from prosecution for any misdeeds that he committed between 2014 and 2025, his pardon does not cover any crimes committed at last week’s hearing. Contempt of Congress is a criminal offense, and Paul referred Fauci’s case to the US Justice Department immediately after Thursday’s vote.
Should the department choose to prosecute, Fauci could face a fine of up to $100,000 and a prison sentence of up to 12 months.
Peter Navarro and Steve Bannon, both former aides to US President Donald Trump, were jailed for contempt of Congress by Biden’s Justice Department. Navarro and Bannon both spent four months in prison in 2024.
Fauci served as the director of the National Institute of Allergy and Infectious Diseases (NIAID) from 1984 to 2022, and as chief medical adviser to Biden from 2021 until his retirement in 2022. In the latter role, Fauci became the face of Biden’s heavy-handed response to the pandemic, advocating mask and vaccine mandates and lockdowns, and dismissing opposition to these measures as “anti-science.”
Deborah Birx got a hero’s welcome on News Nation, claiming she never understood how the country went from slowing the spread to a full shutdown, and pointing to Fauci’s private calls with governors and mayors as the cause. Jefferey Jaxen pulls up the actual headlines and timeline on the woman who was named White House Coronavirus Response Coordinator, and it tells a very different story.
The U.K. government recommended a risky drug combination for COVID-19 patients in 2020, just 16 days after warning doctors to use the medications together only as a last resort, medical commentator John Campbell, Ph.D., said this week.
For years, Campbell has criticized the widespread use of midazolam and morphine and other palliative drugs to treat COVID-19 patients, questioning why so many patients appeared to receive drugs commonly associated with end-of-life care — even though they didn’t necessarily have a terminal illness.
But in his latest video, he said he had overlooked a key piece of the puzzle: The U.K. government itself had backed guidance recommending the combined use of opioids and benzodiazepines for certain COVID-19 patients — just days after warning that the drug combination could cause fatal respiratory depression.
Campbell, who said a former member of the British Parliament brought the issue to his attention, called the apparent reversal “a national scandal which is being ignored.” … Full article
The Centers for Disease Control and Prevention’s (CDC) recent decision to award Pfizer $1.24 billion for COVID-19 vaccines has renewed debate over the government’s continued investment in mRNA technology.
The contracts, awarded on June 1, include about $735.7 million for pediatric COVID-19 vaccines and nearly $505.3 million for adult doses for fiscal year 2026-2027.
Critics say the funding reflects a continued commitment to vaccines associated with high rates of serious injuries and deaths, and a lack of adequate safety testing and monitoring.
Public health experts argue the investment is necessary to protect vulnerable populations and prepare for future outbreaks.
The latest contracts come as mRNA technology expands beyond COVID-19.
A recent review in Human Vaccines & Immunotherapeutics found that mRNA-based therapeutics were identified in more than 550 registered clinical trials. The authors reported that more than 90% of the projects involved mRNA vaccines and that most products remain in early-stage testing before broader adoption.
‘Unnecessary and often harmful injections’
The procurement of monetary resources signals that federal officials intend to continue investing heavily in mRNA technology despite declining public demand and ongoing controversy over vaccine safety monitoring, critics say.
Jeffrey Tucker, president and founder of the Brownstone Institute, told The Defender there was “no scientific justification” or “market demand” for the latest mRNA vaccine funding.
“This raises a serious question concerning how these captured agencies really work,” Tucker said. “We are talking about vast amounts of tax dollars flowing to support unnecessary and often harmful injections.”
“This is $1.24 billion for what is essentially a cold in minor children,” said Children’s Health Defense Chief Scientific Officer Brian Hooker.
Daniel O’Connor, publisher of TrialSite News, which covers global biomedical and clinical research, told The Defender Americans “better start asking the hard questions.”
“If demand is falling, safety questions remain contested and many reporting vaccine injuries say they’ve been left behind, why is Washington committing another $1.24 billion to vaccine procurement instead of first providing a transparent accounting of need, benefit, risk, and responsibility?”
‘COVID-19 has not disappeared’
Public health experts disagreed, saying their support of vaccinations is supporting the prevention of future pandemics.
Dr. Krutika Kuppalli, an associate professor in the Department of Internal Medicine at University of Texas Southwestern Medical Center, in Dallas, told The Defender that the monetary installments will help stave off another public health crisis because “COVID-19 has not disappeared.”
“While the emergency phase of the pandemic is over, the virus continues to cause significant illness, hospitalizations and deaths each year,” she said. “This investment reflects the reality that vaccines remain one of our most effective tools for preventing severe disease, particularly among those at highest risk. Maintaining access to updated vaccines is an important part of ensuring the country remains prepared for future COVID-19 surges.”
Dr. William Schaffner, an infectious disease specialist and professor at Vanderbilt University Medical Center in Nashville, Tennessee, said the contracts will ensure “continuing availability of safe and effective COVID vaccines through the next two years.”
“COVID vaccines have repeatedly been demonstrated to provide protection against the most severe manifestations of COVID infection: hospitalization, intensive care unit admission and death,” Schaffner said. “This is particularly applicable to those persons at increased risk of becoming seriously ill: persons age 65 and older, anyone with a chronic medical condition, persons who are immunocompromised and persons who are pregnant.”
However, some studies suggest claims that the COVID-19 vaccines saved millions of lives are based on flawed models and incorrect calculations.
Legality of funding in question
The contracts also raise questions about federal vaccine spending.
Under the CDC’s Vaccines for Children (VFC) Program, the federal government agrees to buy and provide free vaccines through negotiated contracts for eligible children.
Current CDC price schedules list Pfizer COVID-19 vaccines at roughly $69 to $91 per dose, depending on the formula, while Moderna doses range from about $78 to $83.
Dr. Robert Malone, a pioneer and expert in mRNA vaccines, however, questioned the legal authority to use federal funding for the Pfizer contracts because the purchase wasn’t approved by the CDC’s Advisory Committee on Immunization Practices (ACIP).
“Use of VFC funds requires ACIP authorization,” he said. “But there is no ACIP.”
The injunction stemmed from a lawsuit filed by the American Academy of Pediatrics (AAP) against Kennedy and the U.S, Department of Health and Human Services (HHS). The AAP accused Kennedy of violating procedures when he fired previous ACIP members and replaced them.
The ruling effectively paralysed ACIP and cast doubt on the legitimacy of its membership structure.
Requests for comment from ACIP went unanswered.
‘We are a long way from reckoning’
The CDC has maintained that authorized COVID-19 vaccines underwent extensive safety review and that the benefits outweigh known risks.
However, during a Capitol Hill meeting this week, Sen. Ron Johnson (R-Wis.) referred to reported COVID-19 vaccine injuries as the “biggest government scandal in my lifetime.”
“What about all the injection-injured?” he said. “Until this government and this administration acknowledge those injuries, acknowledge the harm caused by these injections, and I would say federal health agencies also acknowledge the harm done by childhood vaccines, we are a long way from reckoning.”
In April, Johnson released a report revealing that Biden-era health officials rejected a state-of-the-art statistical tool for detecting COVID-19 vaccine safety signals — and instead deliberately continued using a broken method because they didn’t want to “feed in to [sic] anti-vaccination rhetoric.”
During an April 29 hearing, Johnson revealed that a longtime U.S. Food and Drug Administration (FDA) medical officer, Ana Szarfman, M.D., Ph.D., repeatedly warned colleagues that the agency’s approach to safety monitoring could miss serious safety signals due to a problem known as “masking.” Masking occurs when other vaccines obscure risks tied to a specific product.
Johnson said FDA officials brushed aside Szarfman’s warnings.
The CDC, HHS and Pfizer did not immediately respond to requests for comment regarding the contracts.
In August 2021, Dr. Anthony Fauci received a U.S. intelligence report suggesting the COVID-19 virus was developed in Chinese and U.S. labs as a bat vaccine, that it subsequently leaked from China’s Wuhan Institute of Virology, and that it contained characteristics that would make it resistant to mRNA vaccines.
The report, authored by Joseph Murphy, a major with the U.S. Marine Corps, and printed on Defense Advanced Research Projects Agency (DARPA) letterhead, was part of a tranche of documents Sen. Rand Paul (R-Ky.) released Thursday as part of his ongoing congressional investigation into the origins of COVID-19.
The documents show that not only did Fauci receive the DARPA report, but that in an Aug. 25, 2021, email to National Institutes of Health (NIH) officials, he called it “important.” “Let us discuss my going down to the White House to review the report,” Fauci wrote.
The document tranche also contained evidence that Fauci cultivated ties with intelligence agencies at least as early as 2003, the same year he received a CIA report warning of the dangers of genetically manipulating coronaviruses.
Fauci later used these intelligence connections to sway the intelligence community to support the zoonotic theory of COVID-19’s origin, the documents show.
The newly released information corroborates the testimony of CIA whistleblower James Erdman before the U.S. Senate last month. Erdman testified that Fauci led a multi-agency cover-up of COVID-19’s lab origins and that his role in the cover-up “was intentional.”
“These documents reveal a breathtaking level of manipulation — official narratives carefully engineered to shape high-level government policy,” said Stephanie Weidle, executive director of federal watchdog group Feds for Freedom. “This is corruption.”
Brian Hooker, Ph.D., chief scientific officer for Children’s Health Defense (CHD), said the revelations sound “more like a plan than a mistake or a ‘leak.’” He said:
“You can’t tell me that the scientists involved didn’t know what the outcome would be. The combination of the human recombinant virus … and a gene therapy ‘vaccine’ that was used to circumvent all other therapies that could have saved lives, created a monster of a virus, as SARS-CoV-2 mutated to stay beyond the reach of the shot.”
Paul released the documents just days after he revealed that he intends to interview Fauci in Congress later this month. In a letter to Paul dated June 9, Sen. Gary C. Peters (D-Mich.) referenced Paul’s “planned transcribed interview of Dr. Anthony Fauci later this month.”
No further information about this interview is publicly available as of press time. The Daily Caller first reported about the forthcoming interview on Tuesday. Sen. Paul’s office did not respond to The Defender’s request for comment.
Fauci accepted proposal for gain-of-function research involving bat viruses
According to the DARPA document (see page 70), dated Aug. 13, 2021, SARS-CoV-2, the virus responsible for COVID-19, “is an American-created recombinant bat vaccine, or its precursor virus.”
It was created at China’s Wuhan Institute of Virology, also known as the WIV, and U.S. institutions with the help of researchers from the EcoHealth Alliance. The virus then leaked from the Wuhan lab in August 2019.
“The details of this program have been concealed since the pandemic began,” the document states, noting, though, that the details match those contained in two research proposals, the DEFUSE proposal and the PREEMPT project.
The EcoHealth Alliance’s DEFUSE proposal involved altering bat viruses by inserting a spike protein with a furin cleavage site, to cause the virus to infect human lungs. PREEMPT involved the cultivation of Egyptian fruit bats.
University of North Carolina virologist Ralph Baric, Ph.D., and Wuhan Institute of Virology researcher Shi Zhengli, Ph.D., submitted the DEFUSE proposal to DARPA in 2017. Although DARPA rejected the proposal, scientists have suggested the rejection didn’t shut down the project.
After DARPA rejected the DEFUSE proposal, the Aug. 13, 2021, report states that DARPA then “settled with NIH/NIAID” — or the National Institute of Allergy and Infectious Diseases, led at the time by Fauci. According to the report:
“DARPA rejected the proposal because the work was too close to violating the gain-of-function (GoF) moratorium, … despite what Peter Daszak says in the proposal (that the work would not … ).
“As is known, Dr. Fauci with NIAID did not reject the proposal. The work took place at the WIV and at several sites in the US, identified in detail in the proposal.”
Baric and Fauci also closely collaborated with Peter Daszak, Ph.D. — the former president of EcoHealth Alliance, who had financial ties to the Wuhan Lab and played a key role in promoting the zoonotic theory.
In 2024, HHS suspended funding for the EcoHealth Alliance for not monitoring the safety of its coronavirus experiments.
The SARS-CoV-2 virus was likely intended to be used for a bat vaccine before it leaked from the Wuhan lab, according to the DARPA report. “The purpose of the EcoHealth program, called DEFUSE in the proposal … was to inoculate bats in the Yunnan, China caves where confirmed SARS-CoVs were found,” the report states.
However, the virus “leaked and spread rapidly because it was aerosolized so it could efficiently infect bats in caves, but it was not ready to infect bats yet, which is why it does not appear to infect bats.”
The report suggests that SARS-CoV-2 had characteristics that made it easily transmissible among human populations.
“The reason the disease is so confusing is because it is less a virus than it is engineered spike proteins hitch-hiking a ride on a SARSr-CoV quasispecies swarm. The closer it is to the final live attenuated vaccine form, the more likely that it has been deattenuating since initial escape in August 2019,” the report states.
“A year after DARPA denied this proposal to create chimeric bat viruses at the Wuhan Institute of Virology, a novel bat virus with a furin cleavage site began infecting humans in Wuhan. No other closely related virus has this furin cleavage site,” RealClearInvestigations reported in April.
The documents Paul released contain emails showing that Fauci was aware of concerns about the SARS-CoV-2 furin cleavage site early during the pandemic.
In a January 2020 email thread, Fauci responded to concerns from virologist Kristian Andersen, Ph.D., and immunologist Jeremy Farrar, Ph.D., about the presence of the furin cleavage site.
In a Jan. 31, 2020, email, Fauci wrote, “I just got off the phone with Kristian Anderson and he related to me his concern about the Furine site mutation in the spike protein of the currently circulating 2019-nCoV.”
In a later email related to these concerns, Fauci wrote, “The story gets complicated.”
DARPA: Mass vaccination actually increased risks from SARS-CoV-2 virus
The virus also contained characteristics that made it difficult to treat or prevent with mRNA vaccines, the DARPA report suggested.
“The gene-encoded, or ‘mRNA,’ vaccines work poorly because they are synthetic replications of the already-synthetic SARSr-CoV-WIV spike proteins and possess no other epitopes” — or the part of an antigen that the immune system recognizes.
The report adds:
“The mRNA instructs the cells to produce synthetic copies of the SARSr-CoV-WIV synthetic spike protein directly into the bloodstream, wherein they spread and produce the same ACE2 immune storm that the recombinant vaccine does.
“Many doctors in the country have identified that the symptoms of vaccine reactions mirror the symptoms of the disease, which corroborates with the similar synthetic nature and function of the respective spike proteins.”
The DARPA report suggested that mass vaccination campaigns actually increased the risks from the SARS-CoV-2 virus, in a manner replicating that of gain-of-function research, which increases the virulence or transmissibility of viruses. It stated:
“The potential for SARSr-CoV-WIV to deattentuate requires immediate attention. Live vaccines have been found to deattentuate in the past.
“If this is the case with SARSr-CoV-WIV, then the mass vaccination campaign actually performs an accelerated gain-of-function for it. Since it is designed for bats off of a human-susceptible SARS-CoV, vaccinating humans against it actually gains its function back towards a more deattenuated human-susceptible form.”
For the same reasons, other pandemic-related interventions such as masks would be ineffective in stopping the spread of COVID-19, the report states.
“The reasons why nonpharmaceutical interventions like masks and medical countermeasures like the mRNA vaccines do not work well can be extrapolated from the details. Masks or mRNA vaccines would not work for this material,” said former pharmaceutical research and development executive Sasha Latypova. “It is a chemical aerosol poisoning agent. DARPA knows this well.”
Certain characteristics of SARS-CoV-2 made alternative treatment options, such as ivermectin, more effective in treating COVID-19, the report suggests.
“Many of the early treatment protocols ignored by the authorities work because they inhibit viral replication or modulate the immune response to the spike proteins.
“Some of these treatment protocols also inhibit the action of the engineered spike protein. For instance, Ivermectin (identified as curative in April 2020) works throughout all phases of illness because it both inhibits viral replication and modulates the immune response.
“Of note, chloroquine phosphate (Hydroxychloriquine, identified April 2020 as curative) is identified in the proposal as a SARSr-CoV inhibitor, as is interferon (identified May 2020 as curative).”
Fauci was warned about risks of gain-of-function research in 2003
The documents Paul released this week also shed light on Fauci’s intelligence ties. In 2003, Fauci received a CIA report, “The Darker Bioweapons Future,” warning that “engineered biological agents” could lead to effects potentially “worse than any disease known to man.”
While the CIA report doesn’t mention gain-of-function research by name, it cites several examples of cases where viral transmissibility or virulence were enhanced.
The documents also contain an invitation for Fauci to participate in a July 2021 National Security Council briefing related to then-President Joe Biden’s inquiry regarding COVID’s origins — for which Fauci was exempted from a COVID-19 test.
According to Erdman’s Senate testimony last month, the Biden inquiry — and Fauci’s efforts to cover up the likely laboratory origins of COVID-19 — resulted in the White House publishing an August 2021 report that was inconclusive about the virus’s origins — even though intelligence agencies by then had evidence of a lab leak.
A March 6, 2020, email from then-NIH Director Francis Collins referenced the “Proximal Origin” paper published in the journal Nature Medicine, which found that COVID-19 emerged naturally. The paper was widely used to refute the lab-leak theory. Collins suggested that he and Fauci quietly contributed to that paper.
“FYI, this is work that Tony [Fauci], Jeremy [Farrar] … and I helped with, but are appropriately not mentioned explicitly in the paper,” Collins wrote.
“What came afterwards was information warfare,” said Karl Jablonowski, Ph.D., CHD’s senior research scientist. “The world was convinced the virus had bat origins — yet it did not infect bats.”
“The censorship in the first two years was incredibly heavy,” Latypova said. “Everyone, including currently ‘awake’ outlets like Tucker Carlson, enthusiastically endorsed the narrative of natural origin, and anyone who questioned this as bogus (myself) was kicked off all social media platforms.”
Will Fauci come clean when he testifies?
Rutgers University molecular biologist Richard Ebright, Ph.D., a critic of gain-of-function research, said Fauci has a lot to potentially answer for in his congressional interview — and that Biden’s preemptive pardon of Fauci, issued last year, won’t protect Fauci if he lies before Congress. Ebright said:
“Because Fauci’s autopen pardon covers only federal crimes that Fauci committed before Jan. 21, 2025, it does not protect Fauci from prosecution for lying to Congress in a Congressional transcribed interview or public hearing in 2026. He will not even be able to repeat previous lies with impunity in a Congressional transcribed interview or public hearing in 2026.”
Ebright said Fauci has three options — responding truthfully and “confessing that he committed conspiracy to defraud, fraud, perjury, misuse of federal funds, destruction of federal records and obstruction.” Or he can provide false testimony and risk perjury charges, or feign mental incapacitation and inability to recall.
“Erdman testified before the Senate that Fauci actively worked through the intelligence community’s COVID origin task forces to advance his own agenda and steer … COVID-19 policy,” Weidle said. “These revelations should shock no one. Yet the question remains: will anything actually be done about it?”
Two National Institutes of Health (NIH) researchers are charged with conspiring to smuggle biological materials, including deactivated monkeypox virus samples, into the U.S. from Africa. The researchers also allegedly lied to federal authorities about what they were carrying, according to a criminal complaint unsealed Tuesday in federal court in Detroit.
Vincent Munster, Ph.D., a Dutch citizen and chief of the Virus Ecology Section at NIH’s Rocky Mountain Laboratories in Hamilton, Montana, and Claude Kwe Yinda, Ph.D., a Cameroonian research fellow, are charged with conspiracy to smuggle goods into the U.S. and making false statements to federal investigators.
Both men work at a Biosafety Level 4 laboratory, the highest level of containment used for research involving dangerous pathogens.
According to federal prosecutors, the researchers arrived at Detroit Metropolitan Airport on Jan. 25 after traveling from the Democratic Republic of Congo, where a monkeypox outbreak was ongoing.
Customs and Border Protection (CBP) officers questioned the pair about a large black case they were carrying. Prosecutors allege the men told officers the case contained diagnostic and testing equipment, but investigators later determined it held 113 vials stored in Styrofoam coolers.
Testing of a portion of the samples found deactivated monkeypox virus in 17 vials, chickenpox virus in one vial and human DNA in two others.
“These NIH experts apparently broke our laws by smuggling viral pathogens on a packed commercial airplane from an outbreak in the Republic of Congo,” U.S. Attorney Jerome F. Gorgon Jr. said in announcing the charges. “Let that sink in.”
Federal authorities stressed that the case centers on alleged violations of importation and disclosure requirements. Prosecutors did not accuse the defendants of intentionally releasing pathogens or harming the public.
FBI Detroit Special Agent in Charge Jennifer Runyan said the allegations demonstrate that scientific credentials do not exempt researchers from federal statutes.
“No researchers should believe their positions, credentials, or professional status place them above the law,” Runyan said.
The complaint alleges Munster “adamantly denied” carrying biological samples and at one point told investigators that any necessary documentation was on his laptop. “I do this all the time,” he said, according to an FBI affidavit. Authorities said Munster did not produce the documentation he claimed to have.
Neither defendant responded to emails requesting comment.
Congressional inquiry into past research ties
Munster has previously been mentioned in congressional oversight inquiries involving COVID-19 research.
A 2024 letter from Sen. Rand Paul (R-Ky.), then ranking member of the Senate Homeland Security and Government Affairs Committee, to then-NIH Director Monica Bertagnolli said committee investigators had reviewed documents they believed showed collaboration among researchers affiliated with NIH, EcoHealth Alliance, the University of North Carolina and the Wuhan Institute of Virology on SARS-related coronavirus studies.
The letter cited Munster as a participant in the work alongside EcoHealth Alliance’s Peter Daszak, Ph.D., University of North Carolina virologist Ralph Baric, Ph.D., and Wuhan Institute of Virology scientist Zhengli Shi, Ph.D.
The correspondence did not make a finding of wrongdoing but said the materials “indicate” involvement in coronavirus research projects under congressional review.
Richard Ebright, Ph.D., a molecular biologist at Rutgers University in New Brunswick, New Jersey, said the letter raises additional questions about Munster’s past medical ties.
“If the letter is correct, Munster’s record likely includes the unlawful importation and false claims incidents for which he was arrested, but also a share in culpability for causing COVID,” Ebright said.
‘Experimental laboratory approaches’
In a LinkedIn post earlier this year, Munster referenced an article about transmission of the monkeypox (also referred to as mpox) virus “translating our work in the Republic of the Congo towards experimental laboratory approaches.”
Munster and Yinda also co-authored a paper published earlier this year in The Lancet warning that the spread of monkeypox was becoming a “global threat.”
They said cases detected in multiple regions suggested ongoing international spread and called for expanded surveillance, stronger contact tracing and further research into how efficiently the virus transmits and whether sustained community spread is possible outside Africa.
NIH ‘cooperating fully with law enforcement’
The NIH has not commented on the charges, but the agency said it would assist legal authorities in the case.
“This matter is currently under investigation, and NIH is cooperating fully with law enforcement and appropriate authorities,” the agency said in a statement.
The charges emerge amid reports of an employee at Rocky Mountain Laboratories potentially being exposed to Crimean-Congo hemorrhagic fever (CCHF) in late 2025.
Federal officials said the leak was contained and posed no risk to public health, while some legal experts told The Defender these instances were “surprisingly common.”
Munster and Yinda are scheduled to appear in federal court in Montana. If convicted, they face up to five years in prison.
Henrick Karoliszyn, DSW, is an investigative reporter for The Defender.
The Canadian Armed Forces reprimanded soldiers who warned that an order to spy on citizens during COVID-19 could violate intelligence-gathering rules. The soldiers were right. The military punished them anyway.
Internal records and emails obtained by CBC News show that on March 11, 2020, a team called Joint Operational Effects (JOE) was ordered to create anonymous social media accounts and scour the internet for information about Canadians.
Under the direction of Col. Chris Henderson, the team produced dozens of reports between March 19 and June 5, tracking what the federal Conservative, NDP, and Bloc Québécois parties were saying about the pandemic.
The Canadian military was monitoring opposition political parties using anonymous accounts created specifically for surveillance.
At least two JOE team members pushed back. They emailed their chain of command, warning that creating anonymous accounts without authorization, while working from home on personal computers, could breach intelligence directives.
One soldier wrote to Maj. John Zwicewicz on March 12, 2020: “Given the sensitivity around social media and military use I have concerns about this.”
They added: “My concern is that by creating these accounts without following proper procedure would come close to, or cross the line set out in the policy.” Another asked to go into the office because they felt it “represented a serious risk” to do the work at home.
Zwicewicz claimed a legal adviser had approved the activities and ordered the group to “cease barrack room lawyering” and get back to work. The team was formally reprimanded more than a week after raising concerns. A source told CBC News that within months, some members quit or were medically released.
The people who raised alarms about potentially illegal surveillance of Canadian citizens got punished. The people who ordered the surveillance kept their positions.
The military’s own top lawyer flagged the problem. Then-commodore Geneviève Bernatchez, the judge advocate general, warned that “this issue has a significant legal component, and… could present legal risk to the rights of Canadian citizens, but also legal risks to the institution.” She noted that, unlike overseas deployments, “the full range of domestic law” would apply, and “such operations will often directly or indirectly implicate the rights of Canadian citizens.” The command structure absorbed the warning and carried on.
A compliance assessment by the Canadian Forces Intelligence Command, reported by CBC News in April 2026, found three separate military units violated intelligence-gathering rules during Operation Laser between March and July 2020.
One unit used personal laptops to trawl Twitter, Reddit, Instagram, and Facebook. Another produced over 50 reports on political discourse and was ordered to create accounts to “monitor key regional actors,” but “deliberately disregarded” that order and used personal accounts instead.
Six years later, the legal gap that allowed all of this remains open. The National Security and Intelligence Committee of Parliamentarians urged the government in 2020 to legislate rules governing what the military can collect about Canadians. Ottawa has not acted.
DND spokesperson Andrée-Anne Poulin told CBC News that “additional guidance and oversight measures were put in place to prevent a recurrence and to strengthen adherence to established rules.”
Additional guidance. Oversight measures: The standard institutional language for getting caught.
An official with the Office of the Director of National Intelligence (ODNI) today told The Defender that the Intelligence Community Inspector General is aware of allegations by a CIA whistleblower that the agency obstructed a task force investigation into the origins of COVID-19 and is investigating them, along with ODNI and other agencies.
In written testimony provided to the U.S. Senate this week, James E. Erdman III told a Senate committee that the CIA obstructed the work of the CIA’s Director’s Initiatives Group (DIG), an agency task force investigating the origins of COVID-19, and retaliated against those in the group who believed the virus may have leaked from a lab.
Erdman worked for the DIG between March 2025 and April 2026. The group, created by Director of National Intelligence (DNI) Tulsi Gabbard, was ordered to start winding down in January and has since been dissolved.
Soon after the group started to wind down, “the CIA retaliated” against members who supported the lab-leak hypothesis, Erdman wrote.
Erdman, one of the earliest members of the DIG, said he was hired due to his “many years of experience at the CIA and my knowledge on the origins of the COVID-19 pandemic.”
But during his year with DIG, “the CIA obstructed lawful oversight related to the DIG’s work and retaliated against the DIG with what I believe were illegal investigations into DIG members.”
Intelligence officials ‘spent years covering up the truth’
According to Erdman’s testimony, he believes ODNI, the National Intelligence Council (NIC) and CIA personnel “have spent years covering up the truth” about the COVID-19 pandemic.
“The CIA did not comply with lawful oversight requests during the DIG’s investigation,” Erdman wrote.
Erdman’s written statement adds to the oral testimony he delivered before the Senate on Wednesday, as part of Sen. Rand Paul’s (R-Ky.) ongoing investigation into the origins of COVID-19. Erdman told the Senate that “Dr. Fauci’s role in the cover-up was intentional” and that the CIA targeted whistleblowers supporting the lab-leak theory.
In an interview with The Defender on Thursday, Erdman’s attorney, Carol Thompson, said her client is now “concerned that the CIA will use bureaucratic processes and alleged secrecy requirements to undermine his testimony and obfuscate the truth.”
In a letter to CIA Director John Ratcliffe on Thursday, Sens. Paul and Ron Johnson (R-Wis.) forwarded a copy of Erdman’s written testimony — and warned the agency not to take any action against Erdman.
“We expect no retaliatory action of any kind to be taken against Mr. Erdman in connection with his appearance before the Committee,” the letter states.
An individual with knowledge of the situation told The Defender that ODNI previously received a complaint alleging that the CIA was spying on DIG members.
Stephanie Weidle, executive director of Feds for Freedom, a group Erdman co-founded that advocates for government transparency and informed consent, called Erdman “a hero.” She told The Defender his testimony shows that “checks and balances are broken.”
“The CIA is undermining Congress and their boss, Director of National Intelligence Tulsi Gabbard,” Weidle said. “The CIA spies on innocent American citizens, including those tasked with rooting out corruption. They have not yet been held accountable.”
“The agency under investigation killed the investigation,” said Sayer Ji, chairman of the Global Wellness Forum and founder of GreenMedInfo. “The question this raises is who is actually running the U.S., the elected president and his DNI, or a permanent intelligence bureaucracy that has now demonstrated, on the record, that it can dissolve its own oversight.”
The CIA did not respond to The Defender’s request for comment by press time.
‘Dissolution of the DIG has halted critical transparency work’
According to the ODNI, the DIG was formally established in April 2025 and tasked with “restoring transparency and accountability to the Intelligence Community.”
The CIA hasn’t publicly listed DIG members. However, The Washington Post reported in July 2025 that senior national intelligence officer Paul McNamara, a retired U.S. Army lieutenant colonel and Marine officer, oversaw DIG’s efforts.
According to the Post, some intelligence officials were “privately concerned” that DIG “could be used to pursue perceived disloyalty to the Trump administration, including to identify individuals who implemented the policies of the previous administration.”
According to Erdman’s testimony, in October 2025, investigative journalist Steve Baker contacted ODNI “with information allegedly related to the identity of the January 6 pipe bomber.”
DIG “could not and did not attempt to corroborate Baker’s allegations,” but consulted with senior ODNI leadership to share this information with appropriate agencies that could investigate the matter.
That revelation led to a series of events and “drama” that “helped spark a pause in the DIG’s work in December 2025, and its ultimate dissolution in January 2026,” Erdman alleged in his testimony.
“The dissolution of the DIG has halted critical transparency work,” Erdman wrote.
CIA fired contractor involved with DIG’s COVID origins probe
But even before then, the CIA was obstructing the DIG’s work, Erdman alleged — including its investigation into COVID-19’s origins.
“The CIA illegally monitored the computer and phone usage of DIG personnel … their investigations, and contact with whistleblowers,” Erdman wrote.
A CIA contractor involved with the DIG’s COVID-19 origins investigation “was fired one day after meeting with the DIG.”
Erdman alleged the investigation also faced obstructions from within ODNI:
“In my time at the DIG, my team reviewed internal communications that led me to believe that ODNI [and] NIC, under then DNI Avril Haines, did not conduct a serious review or declassification effort for these documents.
“I also reviewed thousands of pages of material that I believe were responsive to the law, but that the Intelligence Community ignored.”
Once DIG was shut down, its investigative work into COVID-19’s origins was transferred to the NIC, Erdman wrote.
“It is not surprising to me that the CIA is ‘not happy’ with Erdman’s testimony. It is likely that they are not happy with the fact that the testimony may pull on the thread that will lead in the direction of the intelligence and defense agencies’ role in the internationally coordinated Project COVID-19,” Latypova said.
David Morens, a former top advisor to COVID Czar Tony Fauci was indicted this week and “charged with conspiracy against the United States; destruction, alteration, or falsification of records in federal investigations; concealment, removal, or mutilation of records; and aiding and abetting,” according to the Justice Department press release.
Morens allegedly helped top federal health officials cover up the potential role of federal grants in spurring the COVID pandemic. The Freedom of Information Act (FOIA) requires federal agencies to preserve and disclose federal records with some narrow exceptions. In early 2021, Morens emailed a colleague, “I learned from our foia lady here how to make emails disappear after i am foia’d but before the search starts, so i think we are all safe.”
Morens added, “Plus i deleted most of those earlier emails after sending them to gmail.” In a previous email, he assured his collaborators, “I have spoken to our FOIA folks” and “I should be safe from future FOIAs. Don’t ask how…”
Fauci doesn’t need to worry about getting indicted since President Joe Biden, on his last morning in office, pardoned any crimes that Fauci might have committed in the previous decade. Fauci justified COVID mandates because average citizens “don’t have the ability” to determine what is best for them. Congressional investigations revealed that Fauci was at the center of string-pulling to shirk responsibility on COVID.
Top federal officials scrambled to erase the federal role in bankrolling reckless gain of function research at the Wuhan Institute of Virology in China, the most likely source of the COVID virus that killed more than seven million people around the world. That type of research seeks to genetically alter organisms to enable the spread of viruses into new species. As MIT professor Kevin Esvelt asked in 2021, “Why is anyone trying to teach the world how to make viruses that could kill millions of people?” The risks were compounded because the Wuhan Institute had a very poor safety rating. Two years earlier, the State Department confidentially “warned other federal agencies about safety issues at Wuhan labs studying bat COVID,” but the public disclosure of that alert was delayed until 2022—long after President Biden illegally mandated COVID vaccines for a hundred million American adults.
If COVID-19 had been initially recognized as the result of one of the biggest government boondoggles in history, it would have been far more difficult for American politicians and government scientists to pirouette as saviors as they seized sway over daily life. Instead, politicians, bureaucrats, and the media stampeded most of the American public with the notion that total submission to boneheaded decrees was their only hope to survive.
Attorney General Todd Blanche issued a statement on the indictment of Morens:
“These allegations represent a profound abuse of trust at a time when the American people needed it most—during the height of a global pandemic.”
Luckily, there haven’t been any “profound abuses of trust” since Trump took office again—at least according tohis Justice Department. Blanche added, “Government officials have a solemn duty to provide honest, well-grounded facts and advice in service of the public interest — not to advance their own personal or ideological agendas.”
Be still my beating heart. Is this a subtle signal that the Trump team will disclose the other three million documents on the Epstein scandal?
FBI chief Kash Patel announced at the indictment press conference, “Circumventing records protocols with the intention of avoiding transparency is something that will not be tolerated by this FBI.”
Has the FBI turned over a new leaf or what? The FBI is one of the most notorious FOIA violators in Washington. When FOIA was first passed in 1966, FBI chief J. Edgar Hoover ordered his agency to totally refuse compliance with the law. A federal judge slammed the FBI in 2017 for claiming it needed seventeen years to fulfill a FOIA request on surveillance of antiwar activists in the 1960s. The FBI deleted the names of Clark Kent and Lois Lane from a letter that made reference to the famous Superman characters—because disclosing them in a FOIA response would “constitute a clearly unwarranted invasion of personal privacy.” Louis Freeh, director of the FBI from 1993-2001, repeatedly denounced my articles on Ruby Ridge; but when I filed a FOIA, the FBI claimed to have no records of those published letters to the editor. They sent their response to “Mr. Brovard” so maybe that helped them not find anything.
FBI FOIA trampling is par for the Bureau covering up its destruction of freedom of speech and freedom of the press. As federal judge Terry Doughty declared in a 2023 decision, “The FBI [acted] as doorman to a vast program of social media surveillance and censorship, encompassing agencies across the federal government—from the State Department to the Pentagon to the CIA.”
Morens may be the first federal official to ever be charged with a crime for actions to evade FOIA requests. Certainly, in more than fifty years, no federal FOIA official has ever been jailed for violating the law by refusing to disclose information. I’ve received so many BS responses from FOIA officers over the decades that I have lost count. When I filed a FOIA with the Office of the U.S. Trade Representative to see what information they had on me in their files, they replied in 2010, “We have no records on Kevin Bovard.” But I wasn’t asking about my cousin.
In 2015, I heard scuttlebutt that the Justice Department pressured USA Today to cease publishing my articles bashing Attorney General Eric Holder. I filed a FOIA to get the department’s official emails to my editors, but DOJ FOIA claimed it had nothing. I only got the damning emails after I filed a follow-up FOIA request and made a lucky guess on the exact day, hour and minute the emails were sent.
For too long, deceiving the American people has been treated like a victimless crime in Washington. If the Morens indictment can set a precedent leading to more such criminal investigations of bureaucratic cover-ups, that will be a booster shot for American democracy.
In the 1950s, the CIA brainstormed ways to secretly perform mind control on humans — including concealing drugs in vaccines and widely consumed food products, a newly unearthed CIA document revealed. The Daily Mail first reported the story on Monday.
The seven-page document, “Special Research for Artichoke,” is dated April 23, 1952. It describes a series of ideas for how to develop chemicals designed to alter human behavior and thought.
The proposals contained in the document were part of the CIA’s top-secret Project Artichoke, which ran from 1951 to 1956, according to the Daily Mail.
The document, declassified in 1983, recently circulated on social media. However, it was not published in the CIA’s online reading room until last year.
“Some of the suggestions are controversial,” the document states. The proposals included administering drugs in secret as part of a “long-range approach to subjects.”
According to the document:
“This study should include chemicals or drugs that can effectively be concealed in common items such as food, water, coca cola, beer, liquor, cigarettes, etc.
“This type of drug should also be capable of use in standard medical treatments such as vaccinations, shots, etc.”
CIA experimented on humans as part of Project Artichoke
The document also included a special field of research for “bacteria, plant cultures, fungi, poisons of various types, etc.,” that are “capable of producing illnesses which in turn would produce high fevers, delirium, etc.”
This included “species of the mushroom” that “produce a certain type of intoxication and mental derangement.”
Also among the proposals was a suggestion to research “diet” or “dietary deficiencies” on prisoners and on people undergoing interrogation, including using “specially canned foods having elements removed.”
The document included proposals for both short-term and long-term use on humans. Drugs deemed most suitable for long-term use would be designed to produce an “agitating effect (producing anxiety, nervousness, tension, etc.) or a depressing effect (creating a feeling of despondency, hopelessness, lethargy, etc.).”
According to The Daily Mail, the CIA experimented on humans as part of Project Artichoke. The experiments often involved “vulnerable subjects, including prisoners, military personnel and psychiatric patients.” The experiments were usually performed “without informed consent.”
According to Ben Tapper, a Nebraska chiropractor who was included in the “Disinformation Dozen” list in 2021 for questioning vaccine safety, the document exposes “a disturbing reality that government agencies have historically explored ways to manipulate human behavior through chemical and biological means, including concepts involving food and medical interventions.”
“This is not speculation or conspiracy, and it should deeply concern every American who values bodily autonomy and informed consent,” Tapper said.
Precursor to the CIA’s MK-Ultra mind control experiments?
The Daily Mail cited CIA documents suggesting that U.S. intelligence agencies were concerned that enemy nations had developed their own mind and behavioral control techniques. This led the agency to prioritize the development of its own methods.
Project Artichoke “served as a precursor” to the MK-Ultra program, which the CIA launched in 1953. That program “broadened mind-altering experiments on a larger scale,” the Daily Mail reported.
Many of the documents related to this type of experimentation were destroyed in 1973, “leaving the full extent of the research and how far it progressed unknown.”
Naomi Wolf, Ph.D., CEO of Daily Clout and author of “The Pfizer Papers: Pfizer’s Crimes Against Humanity,” told The Defender that the documents further confirm a long history of intelligence agency research targeting human thought and behavior.
“Sadly, it’s long been established that our intelligence agencies, and those of our enemies, have sought to alter human consciousness and behavior, often without the subjects’ consent. The existence of MK-Ultra, the clandestine project into which Project Artichoke evolved, is well documented,” Wolf said.
John Leake, vice president of the McCullough Foundation and author of the forthcoming book, “Mind Viruses: America’s Irrational Obsessions,” said, “Researchers have long suspected that the Church Committee’s revelation of the CIA’s notorious MK-Ultra mind control experiments, mostly using LSD, had the effect of obscuring the agency’s much larger Project Artichoke.”
Leake cited evidence suggesting that a 1951 mass poisoning in Pont-Saint-Esprit, France, in which 250 residents experienced severe hallucinations and seven people died, was a Project Artichoke experiment. The outbreak was officially attributed to contaminated bread from a local bakery.
Leake said the 1952 document is “consistent with the suspicion that the CIA was seeking to discover mind control methods for even large populations.”
In 2024, a Reuters investigation revealed that the CIA operated a secret propaganda campaign involving vaccines in the Philippines. The campaign attacked what the agency perceived as China’s “growing influence” in the country by targeting the Chinese-made Sinovac COVID-19 vaccine through the use of phony online accounts spreading “anti-vax” messaging.
Michael Rectenwald, Ph.D., author of “The Great Reset and the Struggle for Liberty: Unraveling the Global Agenda,” said the Project Artichoke revelations “make it clear that the CIA has posed an enormous threat to U.S. citizens, in addition to the horrors it unleashes on non-U.S. target governments and populations.”
Project Artichoke wanted to enlist help from Army’s Chemical Warfare Service
The 1952 Project Artichoke document also included a recommendation to involve the U.S. Army Chemical Warfare Service in the project’s efforts, citing its experience with “exhaustive studies along these lines.”
This proposal bears a resemblance to recent suggestions that COVID-19 — and the response to the pandemic — were coordinated at high levels of government, military and intelligence agencies.
Last year, former pharmaceutical research and development executive Sasha Latypova and retired science writer Debbie Lerman released the “Covid Dossier,” presenting evidence of the “military/intelligence coordination of the Covid biodefense response in the US, UK, Australia, Canada, the Netherlands, Germany, and Italy.”
According to Latypova and Lerman, “Covid was not a public health event” but “a global operation, coordinated through public-private intelligence and military alliances and invoking laws designed for CBRN (chemical, biological, radiological, nuclear) weapons attacks.”
Leake said “it is far from clear” that the Church Committee hearings of 1975 “put a complete end to CIA covert programs.” He cited the possible laboratory development of the SARS-CoV-2 virus as an example.
Experts question similarities between Project Artichoke, COVID vaccines
In a Substack post today, epidemiologist Nicolas Hulscher drew a potential connection between Project Artichoke and the development of COVID-19 vaccines. Hulscher cited recent peer-reviewed studies that identified the vaccines’ adverse impact on neurological health and “surging rates of cognitive decline.”
Hulscher wrote:
“Disturbingly, since 2021, over 70% of humanity received a neurotoxic agent masquerading as a ‘vaccine.’ The same goals outlined in the CIA document (vaccines/drugs capable of covertly inducing anxiety, depression, and lethargy) are now being observed in COVID-19 vaccinated populations. …
“… If the CIA was secretly discussing covert methods to alter human behavior in the 1950s, it would be no surprise if similar classified projects emerged in the decades that followed.”
A 2024 paper published in the journal Molecular Psychiatryinvestigated psychiatric adverse events among over 2 million people in South Korea. The study found that “COVID-19 vaccination increased the risks of depression, anxiety, dissociative, stress-related, and somatoform disorders, and sleep disorders while reducing the risk of schizophrenia and bipolar disorder.”
A 2025 study published in the International Journal of Innovative Research in Medical Science found “alarming safety signals regarding neuropsychiatric conditions following COVID-19 vaccination, compared to the influenza vaccinations and to all other vaccinations combined.”
This included increases in schizophrenia, depression, cognitive decline, delusions, violent behavior, suicidal thoughts and homicidal ideation.
“The fact that mRNA vaccines were designed to cross the blood-brain barrier and inflame the brain — or at least, they were known to do so, during their manufacture and distribution — should give us pause in light of this news,” Wolf said.
Wolf said the latest revelations, “while shocking, provide all the more reason for us to be critical of opaque, coercive or untested vaccination programs, additives in food and water, and toxic or opaque geoengineering programs.”
Tapper said the revelations reinforce “the urgent need to protect individual liberty, medical freedom, and ethical boundaries in science and public health.”
“The lesson here is simple: vigilance is necessary when governments claim authority over the human body and mind,” Tapper said.
In the years leading up to the COVID-19 pandemic, Bill Gates and key figures from the Gates Foundation regularly interacted with Jeffrey Epstein, discussing ways to finance and develop a global pandemic preparedness and vaccination network.
The communications between Gates and Epstein were included in the “Epstein Files” released Jan. 30 by the U.S. Department of Justice (DOJ). Last year’s passage of the bipartisan Epstein Files Transparency Act prompted the release.
Sayer Ji told The Defender the files show that Epstein “functioned as a switchboard” connecting “hedge funds, central banks, billionaires, academic institutions and global health initiatives.”
Ji published his analysis of health- and medical-related information in the files in a series of Substack articles and posts on X.
Bruner said the files showed that Epstein helped develop “the architecture for pandemic profiteering” years before the COVID-19 pandemic.
The documents largely date from the 2010s — after Epstein’s 2008 conviction for soliciting underage sex and his inclusion on a registry of sex offenders.
Ji noted that months before the start of the COVID-19 pandemic, many of the same actors who appear in the Epstein files participated in Event 201 — a simulation of a global pandemic caused by a coronavirus.
According to The Hill, members of the U.S. Congress began reviewing unredacted versions of the documents on Monday.
Rep. Thomas Massie (R-Ky.), who co-sponsored the Epstein Files Transparency Act along with Rep. Ro Khanna (D-Calif.), told The Defender the documents’ release is about justice, not politics.
“Rep. Ro Khanna and I have tried to keep the Epstein files from being political. The Democrats want to make it about Trump, and the Republicans want to make it about the Clintons. We want to make it about the survivors and getting them justice and transparency,” Massie said.
Gates, Epstein and the ‘architecture behind pandemics as a business model’
Ji’s series of Substack posts revealed what he described as “a 20-year architecture behind pandemics as a business model — with Bill Gates at the center of the network,” along with multinational financial institutions like JPMorgan Chase.
The documents, dating from 2011 to 2019, illustrate an “architecture whose foundations predate the COVID-19 era by more than a decade,” Ji wrote. He said they constitute evidence of “a major Wall Street bank asking a convicted sex offender to define the architecture of a Gates-linked charitable fund.”
The documents included several emails outlining the development of a Gates-led charitable fund. A Feb. 17, 2011, email from JPMorgan Chase’s Juliet Pullis to Epstein included questions from the “team that is putting together some ideas for Gates.”
Epstein’s reply outlined how this fund could be structured. The proposal would be developed further in the following months.
In a July 26, 2011, email from Epstein to JPMorgan Chase executive Jes Staley, on which Boris Nikolic, Gates’ chief science and technology adviser, was copied, described a “silo based proposal that will get bill [Gates] more money for vaccines.”
By Aug. 17, 2011, Staley and Mary Erdoes, then-CEO of JPMorgan Asset and Wealth Management, were discussing more details of the proposed fund, including developing “an offshore arm — especailly for vaccines” and projecting “billions of dollars” in donations within two years.
In a response later that day, Epstein said Gates was “terribly frustrated” at the slow pace of establishing the fund. He said Gates was insistent that “additional money for vaccines” be included in an upcoming presentation about the fund.
By Aug. 31, 2011, JPMorgan Chase had apparently developed a proposal called “Project Molecule,” where the bank would partner with the Gates Foundation to develop a perpetual charitable fund for pandemic preparedness and surveillance, vaccine promotion and disease eradication.
According to Ji, the proposal contains many of the ideas Epstein had previously discussed with JPMorgan Chase executives. It also contained plans to spend millions of dollars to purchase oral polio vaccines for Afghanistan and Pakistan, a rotavirus vaccine for Latin America, and a meningitis vaccine for Africa.
The proposal suggested that Melinda Gates chair the fund’s strategic program/grant and distribution committee and that Erdoes, Warren Buffett, Jordan’s Queen Rania and Seth Berkley, CEO of Gavi, the Vaccine Alliance, also participate. The Gates Foundation funded Gavi’s launch in 1999 and holds a permanent seat on its board.
Ji wrote that while Epstein’s name does not appear in the Project Molecule proposal, it acts as the “institutional translation of the architecture he was sketching informally.”
By 2013, these efforts appear to have led to the launch of the Global Health Investment Fund. A confidential Sept. 23, 2013, briefing described the fund as “the first investment fund focused on global health drug and vaccine development.” The fund promised investors annual returns of 5%-7%.
Among the attendees at the fund’s September 2013 launch were JPMorgan Chase CEO Jamie Dimon and representatives of Pfizer, Merck and GlaxoSmithKline (now GSK).
Gates could ‘work with anyone on earth’ but ‘chose a registered sex offender’
According to Ji, Nikolic’s involvement is significant. In August 2013, Gates and Epstein signed an agreement, in which Gates “specifically requested” that Epstein “personally serve” as Nikolic’s representative. The letter noted Epstein’s “existing collegial relationship” with Gates.
“This agreement was executed five years after Epstein’s conviction for soliciting a minor for prostitution,” Ji wrote. “Gates had the resources to work with anyone on earth. He chose a registered sex offender — and put it in writing.”
The documents showed that a month earlier — on July 18, 2013 — Epstein authored a draft email apparently intended for Gates. It references Epstein’s friendship with Gates, his disappointment that Gates sent him an “unfriendly strongly worded email,” and referenced sordid communications the two apparently previously shared.
“TO add insult to the injury you them implore me to please delete the emails regarding your std, your request that I provide you antibiotics that you can surreptitiously give to Melinda and the description of your penis,” Epstein wrote.
In a video posted on X, Michael Kane, director of advocacy for Children’s Health Defense, said that while it’s unknown whether Epstein ever sent that email to Gates, “the next month they’re in a contract together.”
“I think Bill Gates got the message,” Kane said.
In November 2023, a federal judge approved a $290 million settlement between JPMorgan Chase and over 100 women who accused Epstein of sexual abuse. The women alleged that JPMorgan Chase continued doing business with Epstein despite internal warnings over a span of several years.
“JPMorgan banked Epstein for years despite clear red flags — over $1 billion in suspicious transactions flagged internally and ignored. They knew. They didn’t care,” wrote The Truth About Cancer.
Did Epstein play role in launch of the ‘biosecurity state’?
According to Ji, the documents provide a roadmap for how a pandemic preparedness infrastructure was developed and how it helped make Event 201 possible.
“By the time Event 201 convened, the architecture … was no longer conceptual. It had been funded, structured, bonded, insured, staffed, and legally papered. What remained was the rehearsal,” Ji wrote.
September 2014 documents show that Gates disclosed his upcoming meeting with President Obama to Epstein, just as an adviser to then-Israeli Prime Minister Ehud Barak sent Epstein an invitation to a private, off-the-record reception with Obama the following month.
According to Ji, these developments helped activate the infrastructure outlined in Project Molecule, where Epstein acted as a node for Ebola-related project proposals.
This included Epstein receiving a United Nations (U.N.) diplomat’s proposal for the development of a “Nexus Centre for peace and health” that would take “into account the serious impact of Ebola,” and a proposal by a group of scientists for a pre-symptomatic Ebola detection system using PCR testing.
The scientists behind the proposal — affiliated with a U.S. military biolab at Fort Detrick, the Centers for Disease Control and Prevention and the National Institutes of Health — asked Epstein to send the proposal to Gates and the Gates Foundation.
The proposal, by the International Peace Institute’s Terje Rød-Larsen, led to the convening of a May 2015 closed-door meeting in Geneva, Switzerland, titled “Preparing for Pandemics: Lessons Learned for More Effective Responses.” The World Health Organization (WHO), World Bank and U.N. were involved with the meeting.
The meeting’s agenda included sessions addressing “how pandemics should be anticipated, how authority should be exercised, how multiple stakeholders should be coordinated, and — critically — what legal, institutional, and financial mechanisms must be put in place in advance to enable rapid, centralized response,” Ji wrote.
According to Ji, the COVID-19 pandemic response has its roots in the 2014 Ebola response, as Ebola “was the first disease to formally justify the suspension of normal political and sovereign constraints on a global scale. … When the next global health emergency arrived — COVID-19 — the playbook was already written.”
“Epstein appears in the background of precisely these formative conversations — serving as a connector between global finance, philanthropic capital, and biological risk governance,” Ji told The Defender.
Epstein involved in ‘strain pandemic simulation’ two years before COVID
In a January 2017 iMessage thread between Epstein and an unidentified physician seeking help in finding a new job, the physician cited “expertise with public health security.”
The physician, who had experience at the U.N., WHO, Gates Foundation and World Bank, said he “just did pandemic simulation,” which could become a “big platform.”
Referring to Gates, the physician told Epstein, “He hates mental health but he’s crazy about vaccines and autism stuff. That could be start to a more broad conversation.”
A March 2017 email chain, which included Epstein and Gates, discussed efforts by the then-bgC3, Gates’ private strategic office, to develop “Follow-up recommendations and/or technical specifications for strain pandemic simulation.”
Ji noted that in 2017, the Coalition for Epidemic Preparedness Innovations (CEPI) was launched at the World Economic Forum (WEF), with Gates Foundation funding and a goal of creating “pandemic-busting vaccines” within 100 days. Later that year, the World Bank issued the first-ever pandemic bonds.
Event 201, held just six weeks before the first publicly acknowledged COVID-19 cases were announced, involved the Gates Foundation, WEF and the Johns Hopkins Center for Health Security. Global financial institutions, media organizations and intelligence agencies also participated.
The simulation focused on the response to a novel coronavirus outbreak by governments, pharmaceutical companies, media outlets and social media platforms.
Ji said the Epstein Files don’t show that COVID-19 was planned or manufactured, or that Event 201 led to COVID-19. Instead, they prove that “the institutional infrastructure to capitalize on exactly this kind of crisis was already built, tested, staffed, and insured.”
For over a century, remarkable therapies have been suppressed to maintain a medical monopoly at the expense of humanity
A Midwestern Doctor | The Forgotten Side of Medicine | August 6, 2026
Story at a Glance:
Modern medicine is built around costly, narrowly approved drugs that treat (but rarely cure) specific disease franchises, with regulatory approval correlating more strongly with money spent than with real therapeutic value.
To enforce this, for over a century the same institutions, backed by vast fortunes, have repeatedly sidelined broader or cheaper therapies that threatened those franchises.
The same playbook is used again and again—once a therapy threatens a market, claims of “no evidence” or doctored research amplified by the media will allow regulators to clamp down on the “dangerous and unproven” therapy until it becomes forgotten to history.
In this article, I will illustrate how the exact same playbook was used again and again on numerous transformative medical discoveries endorsed by leading physicians of the era, resulting in nearly every one (e.g., UVBI and numerous cancer treatments) becoming largely forgotten despite immense evidence behind them.
This same playbook was used throughout COVID-19 to eliminate the off-patent therapies that threatened the boondoggle. One of these, chlorine dioxide, was not only repeatedly shown to eliminate COVID outbreaks, but also to do the same with malaria, where it likewise was banned.
Pierre Kory and Jenna McCarthy’s recent book The War on Chlorine Dioxide provides a critical body of evidence that chlorine dioxide has treated a myriad of challenging conditions, and that each time it did, a robust censorship apparatus erased those discoveries and retaliated against the discovers—providing a poignant illustration of the medical monopoly in action.
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.
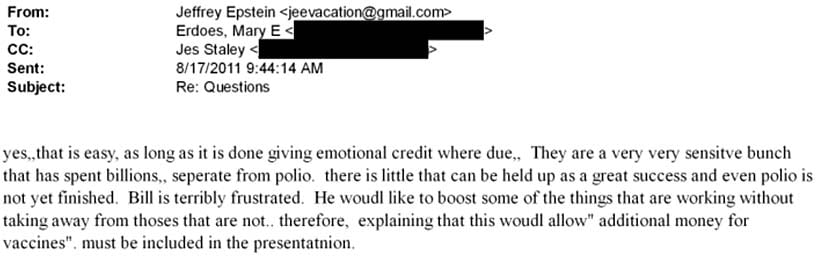

 Modern medicine is built around costly, narrowly approved drugs that treat (but rarely cure) specific disease franchises, with regulatory approval correlating more strongly with money spent than with real therapeutic value.
Modern medicine is built around costly, narrowly approved drugs that treat (but rarely cure) specific disease franchises, with regulatory approval correlating more strongly with money spent than with real therapeutic value.