What is AZAPAC? Why is it important?
If Americans Knew | February 6, 2026
AZAPAC Founder Wants to “De-Zionize” The U.S. Government.
Author Michael D. Rectenwald is the founder of AZAPAC (The Anti-Zionist America PAC). Ana Kasparian interviews him on The Young Turks.
See the entire interview here:  • AZAPAC Founder Wants to “De-Zionize” The U…
• AZAPAC Founder Wants to “De-Zionize” The U…
Read more here: https://www.aza-pac.com/
“Zionism has taken over the U.S. government, as the constant subservience to Israel in word and deed makes eminently clear. Opposing Zionism in America means ridding the government of Zionists who serve Israel over the United States. This demands, among other measures, confronting and competing with entrenched lobbies like AIPAC, CUFI, and J-Street. These groups bend U.S. policy to favor foreign agendas. Zionist influence drains American resources, undermines U.S. sovereignty, and runs counter to the interests of the American people.”
Join AZAPAC, IAK, and the many other orgs in the VAB coalition.
The Toxic Border: How Israel’s Chemical Spraying is Reshaping Life in South Lebanon
By Robert Inlakesh | The Palestine Chronicle | February 8, 2026
Reports that Israeli aircraft sprayed chemical agents along the Lebanese border — later identified as toxic defoliants — have intensified concerns over environmental damage, civilian harm, and possible violations of international law, with similar incidents also reported in southern Syria.
Key Takeaways
- UN peacekeepers suspended patrols after being warned that aircraft would spray chemical agents near the Blue Line.
- The sprayed substance was later identified as a toxic herbicide linked to cancer.
- The campaign is seen as serving both military land-clearing and civilian displacement purposes.
- Similar chemical spraying incidents have been reported in southern Syria.
- Rights groups say targeting farmland may constitute a violation of international humanitarian law.
- Spraying along the Blue Line
Israel is waging chemical warfare against both Lebanese and Syrian lands, a campaign that may not only have dire environmental repercussions but also inflict long-term health problems on local civilian populations.
On February 1, the United Nations peacekeeping forces stationed in southern Lebanon – UNIFIL – were forced to suspend their patrols along what is known as the Blue Line that demarcates the de facto Israeli-Lebanese border. They did so out of safety concerns for their soldiers, after Israel informed them it would be using planes to spray chemical agents in the area.
Tel Aviv initially informed UNIFIL that the chemical agent was “non-toxic.” Nevertheless, the UN reiterated its “concerns” about flight movements in the area, stressing that such activities violate UN Security Council Resolution 1701.
It wasn’t long until it was discovered that the agent being sprayed was, in fact, toxic. Allegedly, the specific agent used, for which a toxicology test was conducted, is a defoliant and herbicide that is linked to cancer.
Israel is currently on its way to violating the Lebanon ceasefire, which went into effect on November 27, 2024, nearly 10,000 times. This makes it the most violated ceasefire deal in recorded history.
Israeli strikes, targeting north to south and even the capital city of Beirut, have killed hundreds. Despite this, there have been no recorded violations by Hezbollah or the Lebanese Army.
A Strategy of Erasure
What is so consequential about Israel’s use of chemical agents in southern Lebanon is that it has two primary purposes. The first is to kill everything it touches, to clear the land for military purposes. The second is that it is being used as a form of collective punishment, a likely intention behind which is to drive Lebanese citizens from their homes.
Perhaps the most horrifying part of this is that there is a dark history of such chemicals being used for the same purposes elsewhere. The most infamous case is that of the US military spraying Agent Orange, also a herbicide and defoliant, during the Vietnam War.
As a result of the callous use of Agent Orange, both the civilian population of Vietnam and US soldiers alike ended up contracting serious chronic health problems. One of the results was birth defects, cancers such as Hodgkin’s lymphoma, and even neurodegenerative diseases. This was in addition to what was labeled ecocide in the country.
While some may argue that the Israelis are simply using chemical agents to clear the land, as a security precaution, this is not plausible. Israel has the capability and has historically used heavy equipment to clear the land.
Deploying chemical agents, which it is of note that they haven’t done so on their side of the Blue Line, is clearly a malicious attack on Lebanese lands and the civilian population living there.
Beyond Lebanon
Israelis have frequently expressed their dismay over the immediate return of Lebanese villagers to their destroyed homes in the south, particularly near the unofficial border, as Israel has never declared its borders.
Meanwhile, a considerable percentage of Israelis, formerly living in settlements like Kiryat Shimona, that were hit the hardest by Hezbollah during the last war, have refused to return.
It has not only been Lebanon that has been subjected to such chemical agent attacks, but southern Syria has also fallen victim to the Israeli military spraying similar chemical agents on its lands.
While the Lebanese government has come under criticism for often ignoring the plight of its citizens in the south, the Syrian government completely refrains from addressing the ongoing occupation and war crimes committed in the south of their country.
The refusal of Damascus to even voice its concern about the chemical warfare being waged against its people and lands has made it less of an issue than in Lebanon, as Beirut has raised its voice.
“The deliberate targeting of civilian farmland violates international humanitarian law, particularly the prohibition on attacking or destroying objects indispensable to civilian survival,” commented the Switzerland-based Euro-Med Human Rights Monitor.
It also demanded accountability for Israel’s “large-scale destruction of private property without specific military necessity amounts to a war crime and undermines food security and basic livelihoods in the affected areas.”
– Robert Inlakesh is a journalist, writer, and documentary filmmaker. He focuses on the Middle East, specializing in Palestine.
Zelensky tried to kill the chance for Russia-Ukraine peace, again
The attempted assassination of a high-ranking Russian general is an attempt to sabotage talks and extend the Kiev regime’s stay in power
By Nadezhda Romanenko | RT | February 8, 2026
The assassination attempt on Lieutenant General Vladimir Alekseyev, first deputy chief of Russia’s Main Intelligence Directorate (GRU) is clearly the Zelensky regime’s latest desperate bid to sabotage the emerging Russia-Ukraine-US negotiations channel in Abu Dhabi and prolong the war.
When negotiations gain traction, spoilers surface. That’s Negotiations 101. And this week’s second round in Abu Dhabi was precisely the kind of movement that unnerves actors who fear ballots, reforms, and accountability more than inevitable defeat on the battlefield.
The target choice reinforces the point. Alekseyev is the second-in-command of GRU chief Igor Kostyukov – who sits on the Russian delegation in Abu Dhabi. Striking the No. 2 as the No. 1 shuttles between sessions is both a very deliberate message and an attempt to rattle Russia’s delegation, inject chaos into its decision loop, force security overdrive, and ultimately, provoke Moscow’s withdrawal from the talks.
Nor is this the first time kinetic theater has tracked with diplomatic motion. Recall the attempted drone strike on President Vladimir Putin’s Valdai residence in late 2025, which coincided with particularly intense US-Russia exchanges. You don’t have to be a cynic to see a pattern: whenever the diplomatic door cracks open, someone tries to slam it shut with explosives, drones, or bullets – then retreats behind a smokescreen of denials and proxies. Call it plausible deniability as policy.
Why would Kiev’s leadership gamble like this? Start with raw political incentives. Vladimir Zelensky extended his tenure beyond the intended March 2024 election under martial law. If hostilities wind down and emergency powers lift, the ballot box looms. His standing has eroded amid war fatigue, unmet expectations, and a massive corruption scandal swirling around the presidential administration that has infuriated many Ukrainians and dealt his image a blow. End the war without a narrative of total victory, and he risks owning a messy peace, grueling reconstruction, and a reckoning at the polls. Facing voters at a stadium famously worked well during Zelensky’s initial presidential campaign, but now endlessly moving the goalposts is his only hope of clinging to power.
Then there’s the strategic logic of spoilers. Negotiations compress time, clarify tradeoffs, and create deadlines – none of which benefit maximalists. If an agreement would force Kiev to accept hard limits or expose fissures with its more hawkish backers, creating a pretext to stall makes sense from a narrow survival lens. A brazen hit inside Moscow during talks does exactly that: it dares the Kremlin to harden its stance, fractures trust at the table, and lets Kiev posture as unbowed while keeping the war‑time rally frame at home. Even if direct authorship can be obfuscated (at least on paper – because nobody will buy claims Kiev had nothing to do with it at this point), the practical effect is what counts.
Predictably, defenders will object: Kiev has every incentive to keep US support flowing, so why risk alienating Washington with an operation that screams escalation? But ‘incentives’ aren’t monolithic. They’re filtered through domestic politics, factional competition within security services, and the temptations of a successful spectacle. And remember: spoilers don’t have to be centrally ordered to be useful. A wink, a nod, and a green light to ‘make pressure’ can travel a long way in wartime bureaucracies.
The most important thing for Russia and the US at this stage is to firewall the talks from such bloody theatrics. For the negotiation process to provide real results, it must be built to survive shocks – because the shocks will keep coming. That means insulating prisoner‑exchange and humanitarian working groups from headline provocations, revalidating military deconfliction channels, and demanding verifiable behavior changes rather than trading barbs about attribution in the press.
The larger point is simpler: if we let every well‑timed bullet dictate the pace of diplomacy, we are outsourcing strategy to those who most fear peace. The Alekseyev attack fits a familiar script – choose a symbolically loaded target, hijack the narrative, and hope negotiators flinch. The right response is the opposite: call the bluff, keep the calendar, and raise the cost of sabotage by refusing to let it reset the table.
Zelensky’s regime may calculate that its political survival depends on endlessly throwing up hurdles for peace and call it ‘resistance’. If so, the fastest way to test that proposition is to keep pressing at the negotiating table. Talks are not a favor to one side; they are a filter that separates leaders who can face an endgame from those who can only survive in the fog of “not yet.”
Somalia president warns against Israeli interference, vows to prevent any military base in Somaliland
Press TV – February 8, 2026
The president of Somalia has strongly denounced the Israeli regime’s interference in his country’s internal affairs and vowed to “confront” any Israeli military presence in the breakaway region of Somaliland.
In an interview on Saturday, Hassan Sheikh Mohamud said Israel’s recognition of Somaliland as an independent state is a “reckless, fundamentally wrong and illegal action under international law.”
Somaliland is a breakaway region in northwestern Somalia, covering territory that was once part of the British Protectorate. Despite its unilateral separation, it remains internationally recognized as part of Somalia.
The region occupies a strategic position along one of the world’s most vital maritime choke points, an area already surrounded by overlapping conflicts in the Horn of Africa and West Asia.
In recent years, Somaliland has sought foreign support by developing ties with the United Arab Emirates (UAE), a signatory to the Abraham Accords with Israel, as well as Taiwan, in an effort to gain international acceptance outside Mogadishu’s authority.
Israel’s move followed reports that the regime had contacted actors in Somaliland to discuss using the territory for the forced displacement of Palestinians during its genocidal war on Gaza, which has killed more than 72,000 Palestinians and wounded another 172,000, most of them women and children.
While Israeli and Somaliland authorities rejected those reports, a Somaliland official told Israel’s Channel 12 in January that an Israeli military base is “on the table and being discussed,” with its establishment tied to specific conditions.
Somalia has described Israel’s recognition of Somaliland as a direct assault on its territorial integrity and national unity, a position endorsed by most African and Arab countries, and has demanded that Prime Minister Benjamin Netanyahu reverse the decision.
Mohamud also made clear that Mogadishu will resist any Israeli military presence on Somali soil: “We will fight in our capacity. Of course, we will defend ourselves … And that means that we will confront any Israeli forces coming in, because we are against that and we will never allow that.”
He said Israel’s actions, which are “interfering with Somalia’s sovereign and territorial integrity,” also “undermine stability, security and trade in a way that affects the whole of Africa, the Red Sea and the wider world.”
Mohamud stressed that Israel’s deadly use of force against Palestinians in Gaza cannot be separated from developments in Somaliland, saying both reflect the erosion of global norms and restraints.
“Key among the global concerns is the weakening of the established rules-based international order. That order is not intact anymore,” he said.
He warned that institutions created after World War II “are under grave threat,” as the idea that “the mighty is right” increasingly replaces respect for international law.
The administration of US President Donald Trump, meanwhile, has yet to signal a significant change in its position on Somaliland.
Iranian FM says uranium enrichment to continue ‘even at cost of war’
The Cradle | February 8, 2026
Iran’s Foreign Minister Abbas Araghchi said on 8 February that the Islamic Republic will not give up uranium enrichment, as Israel and the US are demanding – stressing that Tehran will continue to pursue a peaceful nuclear program even at the cost of war.
Araghchi also reiterated that talks with the US will not focus on anything except the nuclear issue, as Israel continues to push Washington to double down on demands for curtailing the Iranian missile program and halting support for regional resistance groups.
“Iran has paid a very heavy price for its peaceful nuclear program and for uranium enrichment,” the foreign minister said on Sunday.
“Why do we insist so much on enrichment and refuse to give it up even if a war is imposed on us? Because no one has the right to dictate our behavior,” he added.
Iran will never abandon enrichment even “if war is imposed” on the country. “Their military deployment in the region does not scare us.”
“There was no direct meeting, we had a diplomatic courtesy meeting, which amounted to a handshake. This has been done in the past, this is common,” Araghchi went on to say, referring to the recent talks, which were the first since Iran was attacked by Israel in the middle of negotiations last year.
“The place and time of the next meeting will be determined in the next consultations. It may be another place, but the form of negotiations will be indirect.”
“We will only negotiate on nuclear issues. If it is to continue, it will continue in the same way,” Araghchi affirmed.
Reports said that, as the talks began, the US CENTCOM chief would attend the negotiations.
“The US delegation in Muscat had asked if the CENTCOM commander could participate in a diplomatic greeting with us. We rejected the request, saying we do not accept the presence of a military person within the negotiation,” Araghchi clarified.
He also said the “future of negotiations is unclear,” adding: “We neither trust them nor rule out the possibility of deception and trickery. In fact, we fully anticipate it.”
The foreign minister’s comments come as Israeli Prime Minister Benjamin Netanyahu is due to visit the US in the coming days for talks with Donald Trump.
The premier is expected to push Washington not to give up on the demand that Iran abandon the Resistance Axis, as well as its missile and nuclear program.
“The Prime Minister believes that any negotiations must include limiting ballistic missiles and halting support for the Iranian axis,” Netanyahu’s office said on 7 February.
Israeli news site Ynet reported that Netanyahu’s goal for the US visit is “to ensure that Israeli interests are safeguarded in the negotiations.”
The report says Tel Aviv wants Iran’s missiles to be limited to 300 kilometers only, making them incapable of targeting Israel.
“Israel also wants the agreement to stipulate that Iran will no longer be able to provide support to its proxies in the region, including Hezbollah in Lebanon and the Houthis in Yemen.”
A senior political source is cited by the outlet as saying that [Netanyahu] “urgently advanced” his visit to the US “to influence the acceptance of Israel’s conditions in the negotiations, with an emphasis on ballistic missiles.”
The report adds that Israel is demanding a return of surprise inspections and “high-quality” monitoring by the International Atomic Energy Agency (IAEA), which Tehran accuses of serving Tel Aviv’s interests.
Additionally, Israel wants Iran’s stockpile of enriched uranium to be removed from the country’s territory.
Ynet also confirms other reports that Washington expects significant Iranian concessions in the next round of talks.
Iran has signaled a willingness to potentially limit enrichment in previous negotiations, as it agreed to in the 2015 deal, which Trump scrapped during his first term.
Yet the Islamic Republic refuses to give up support for its allies and says its missile program – a major part of the country’s defense – is non-negotiable.
The negotiations nearly fell apart over Iran’s insistence on discussing only the nuclear issue.
Axios reported last week that the US agreed to meet the Iranians only “out of respect” for its Arab allies who had lobbied to save the talks from cancellation.
Right after the talks, the US imposed new sanctions on Iran’s oil industry.
The last time Tehran negotiated with Washington, it was attacked by Israel in the middle of the talks.
Trump had pretended to be in favor of diplomacy for months prior to the attack, while secretly plotting the 12-day war with Israel.
The talks coincide with a massive US military buildup across the region, and follow numerous threats against Iran made publicly by Trump. Iran has vowed to confront any attack by striking back at Israel and US bases across West Asia.
No, Al-Jazeera, Climate Change Hasn’t Altered African Flood and Drought Patterns
By Anthony Watts | Climate Realism | February 3, 2026
Al Jazeera (AJ) recently published an article titled “Drought in the east, floods in the south: Africa battered by climate change” by Haru Mutasa, in which the reporter details recent experiences of drought in East Africa and flooding in southern Africa, asserting that those weather events are proof that climate change is battering the continent. This is false. The article relies on flimsy content such as personal observation, interviews, and evocative imagery to imply causation, ignoring data and trends that show no appreciable changes in flood or drought patterns over time.
Mutasa asserts that “rising seas and intensifying storms” and shifting rainfall patterns are already devastating livelihoods, citing the author’s personal field observations as evidence of a broader climate crisis. Readers are shown photos of dry riverbeds, dead livestock, submerged neighborhoods, and distressed residents, then invited to connect these scenes directly to global warming. The emotional impact is real, but emotion is not evidence.
Let us start with AJ’s most basic error: weather is not climate. Climate is defined by long-term patterns measured over decades, typically 30 years or more. A drought in one region followed by floods in another over a few weeks or months says nothing about a durable climate trend. Africa’s climate has always been highly variable, with sharp swings driven by ocean–atmosphere cycles such as the El Niño–Southern Oscillation and the Indian Ocean Dipole. Short-term extremes—sometimes back-to-back—are a known feature of the region, not a recently discovered diagnostical proof of climate change.
The historical record bears this out. Southern and eastern Africa experienced severe droughts and catastrophic floods long before modern greenhouse gas emissions rose. Mozambique’s Limpopo River basin, featured prominently in the article’s flood imagery. The area has a long history of major inundations, including the devastating 2000 Mozambique floods, which displaced hundreds of thousands and occurred during a strong El Niño year. East Africa’s Horn has likewise seen repeated, multi-year droughts throughout the twentieth century, interspersed with episodes of extreme rainfall. These precedents matter because they show that today’s events are consistent with a long pattern of variability rather than proving a novel climate regime.
In fact, science has shown a 50-year seasonal variability across centuries in East African droughts and floods recorded in lake sediments.
When measured data are consulted instead of anecdotes, the alarm bells fade. Climate at a Glance summarizes the global evidence in “Floods” and “Drought,” explaining that there is low confidence in any increasing trend of global flood frequency or magnitude and that drought trends are regionally mixed, not universally worsening. These conclusions align with the cautious language used by the Intergovernmental Panel on Climate Change (IPCC) Sixth Assessment Report (AR6), which emphasizes uncertainty and regional variability rather than blanket claims of intensification.
The AJ article substitutes interviews for analysis. Quoting local residents and aid workers about hardship may document suffering, but it does not diagnose cause. Infrastructure deficits, land-use changes, deforestation, river management, dam releases upstream, population growth in floodplains, and limited early-warning systems all play decisive roles in disaster outcomes across Africa. Climate Realism has repeatedly shown how media coverage overlooks these factors while attributing complex events to climate change by default, as catalogued in its Africa-related reporting and extreme-weather analyses accessible via Climate Realism’s search on floods and droughts and Climate Realism’s coverage of drought claims.
Even within the article’s narrative, local management issues loom large. Mutasa notes dam releases in South Africa’s Mpumalanga province sent additional water downstream into Mozambique—an operational decision with immediate hydrological consequences that has nothing to do with global temperature or climate change. Treating such factors as footnotes while elevating climate change as the primary driver of flooding misinforms readers about where real risk reduction lies.
Serious climate reporting distinguishes between events and trends, and between personal experiences and measured evidence.
By presenting interviews and moment-in-time scenes as confirmation of a continent-wide climate verdict, Al Jazeera is misleading its audience by making a causal connection where data show none. Africa’s vulnerability to climate and weather extremes is real, but the causes are multifaceted and long-standing. Ignoring historical precedents and measured trends in favor of an alarming narrative certainty does not inform the public; it misleads it with false headlines.
Bad Science, Big Consequences
How the influential 2006 Stern Review conjured up escalating future disaster losses
By Roger Pielke Jr. | The Honest Broker | February 2, 2026
For those who haven’t observed climate debates over the long term, today it might be hard to imagine the incredible influence of the 2006 Stern Review on The Economics of Climate.1
The Stern Review was far more than just another nerdy report of climate economics. It was a keystone document that reshaped how climate change was framed in policy, media, and advocacy, with reverberations still echoing today.
The Review was commissioned in 2005 by the UK Treasury under Chancellor Gordon Brown and published in 2006, with the aim of assessing climate change through the lens of economic risk and cost–benefit analysis. The review was led by Sir Nicholas Stern, then Head of the UK Government Economic Service and a former Chief Economist of the World Bank, from the outset giving the effort unusual stature for a policy report.
As the climate issue gained momentum in the 2000s, the Review’s conclusions that climate change was a looming emergency and that virtually any cost was worth bearing in response were widely treated as authoritative. The Review shaped climate discourse far beyond the United Kingdom and well beyond the confines of economics.
One key aspect of the Stern Review overlaps significantly with my expertise — The economic impacts of extreme weather. In fact, that overlap has a very surprising connection which I’ll detail below, and explains why back in 2006 I was able to identify the report’s fatal flaws on the economics of extreme weather in real time, and publish my arguments in the peer-reviewed literature soon thereafter.
But I’m getting ahead of myself.
I have just updated through 2025 the figure below that compares the Stern Review’s prediction of post-2005 increases in disaster losses as a percentage of global GDP with what has actually transpired.
Specifically, the figure shows in light grey the Stern Review’s prediction for increasing global disaster losses, as a percentage of GDP, from 2006 through 2050.2 These values in grey represent annual average losses, meaning that over time for the prediction to verify, about half of annual losses would lie above the grey bars and about half below.
The black bars in the figure show what has actually occurred (with details provided in this post last week). You don’t need fancy statistics to see that the real world has consistently undershot the Stern Review’s predictions over the past two decades.
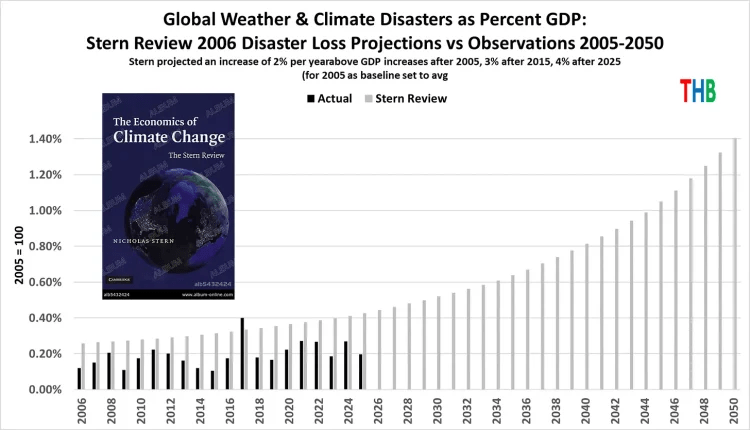
The Stern Review forecast rapidly escalating losses to 2050, when losses were projected to be about $1.7 trillion in 2025 dollars. The Review’s prediction for 2025 was more than $500 billion in losses (average annual). In actuality losses totaled about $200 billion in 2025.
The forecast miss is not subtle.
How did the Stern Review get things so wrong?
The answer is also not subtle and can be summarized in two words: Bad science.
Let’s take a look at the details. The screenshot below comes from Chapter 5 of the Review and explains its source for developing its prediction, cited to footnote 26.

As fate would have it, footnote 26 goes to a white paper that I commissioned for a workshop that I co-organized with Munich Re in 2006 on disasters and climate change.
That white paper — by Muir-Wood et al. — is the same paper that soon after was played the starring role in a fraudulent graph inserted into the 2007 IPCC report (yes, fraudulent). You can listen to me recounting that incredible story, with rare archival audio.
But I digress . . . back to The Stern Review, which argued:
If temperatures continued to rise over the second half of the century, costs could reach several percent of GDP each year, particularly because the damages increase disproportionately at higher temperatures . . .
The report presented its prediction methodology in the footnote 27, shown in full below, which says: “These values are likely underestimates.”

Where do these escalating numbers come from? Who knows.
They appear to be just made up out of thin air. The predictive numbers do not come from Muir-Wood et al., who do not engage in any form of projection.
The 2% starting point for increasing losses — asserted in the blue highlighted passage in the image above — also does not appear in Muir-Wood et al. which in fact says:
When analyzed over the full survey period (1950 – 2005) the year is not statistically significant for global normalized losses. . . For the more complete 1970-2005 survey period, the year is significant with a positive coefficient for (i.e. increase in) global losses at 1% . . .
The Stern Review seems to have turned 1% into 2% and failed to acknowledge that over the longer-period 1950 to 2005, there was no increasing trend in losses as a proportion of GDP. The escalating increase in annual losses from 2% to 3%, 4%, 5%, 6% every decade is not supported in any way in the Stern Review, nor is it referenced to any source.
When the Stern Review first came out, I noticed this curiosity right away, and did what I thought we scholars were expected to do when encountering bad science with big implications — I wrote a paper for peer review.
My paper was published in 2007 and clearly explained the Muir-Wood et al. and other significant and seemingly undeniable errors in the Stern Review.
Pielke Jr, R. (2007). Mistreatment of the economic impacts of extreme events in the Stern Review Report on the Economics of Climate Change. Global Environmental Change, 17(3-4), 302-310.
I explained in that paper:
This brief critique of a small part of the Stern Review finds that the report has dramatically misrepresented literature and understandings on the relationship of projected climate changes and future losses from extreme events in developed countries, and indeed globally. In one case this appears to be the result of the misrepresentation of a single study. This cherry picking damages the credibility of the Stern Review because it not only ignores other relevant literature with different conclusions, but it misrepresents the very study that it has used to buttress its conclusions.
Over my career in research, I’ve had some hits and some misses, but I’m happy to report that I got this one right at the time and it has held up ever since. Of course, perhaps a more significant outcome of this episode, and a key part of my own education in climate science, is that my paper was resoundingly ignored.
One reason that science works is that scientists share a commitment to correct errors when they are found in research, bringing forward reliable knowledge and leaving behind that which doesn’t stand the test of time.
I learned decades ago that in areas where I published, self-correction was often slow to work, if not just broken. Over the decades that pathological characteristic of key areas of climate science has not much improved (e.g., see this egregious example).
The Stern Review helped to launch climate change into top levels of policy making around the world. Further, we can draw a straight line from the Review to the emergence of (often scientifically questionable) “climate risk” in global finance a decade later. It still rests on a foundation of bad science.
1 My ongoing THB series on insurance and “climate risk” in finance prompted me to revisit the 2006 Stern Review, hence this post.
2 Note that the Review explicitly referenced the tabulation of global economic losses from extreme weather events as tabulation by Munich Re, which is the same dataset that I often use, such as in last week’s THB post on global disaster losses. The comparison here is thus apples to apples.
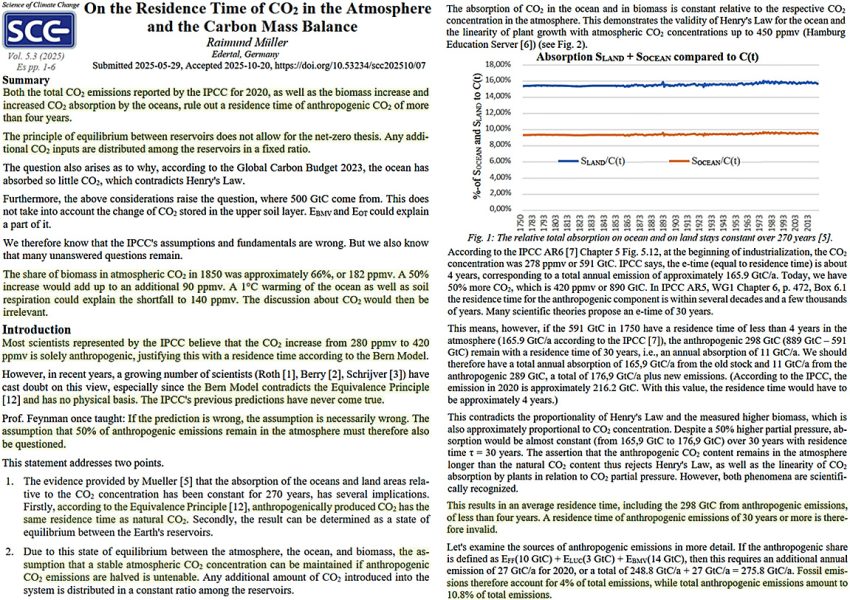
New Study Rebuts The Assumption That Anthropogenic CO2 Molecules Have ‘Special’ Properties
By Kenneth Richard | No Tricks Zone | February 6, 2026
The Intergovernmental Panel on Climate Change (IPCC) has for decades advocated net-zero governmental policies to reduce anthropogenic CO2 (aCO2) emissions.
This advocacy is rooted in the non-physical assumption that aCO2 molecules are special, as they remain in the atmosphere for decades to centuries.
Proponents of the anthropogenic global warming (AGW) narrative even claim aCO2 removal can “take up to several hundreds of thousands of years.”
While AGW proponents insist that “once in the atmosphere, carbon dioxide can continue to affect climate for thousands of years,” they (and the IPCC) simultaneously acknowledge the residence time of “natural” or non-anthropogenic CO2 is only about 4 years.
In reality, a new study references the Equivalence Principle in emphasizing nature’s sinks indiscriminately and equivalently absorb both aCO2 and natural CO2 in about 4 years (Müller, 2025). There is no physical reality for IPCC claims of “specialized” absorption time for aCO2 vs. natural CO2 molecules.
The IPCC assumes exactly 50% of aCO2 emissions remain in the atmosphere for decades to millennia. It is consequently assumed net-zero policies that propose to halve aCO2 emissions will lead to the stabilization of atmospheric CO2 concentrations. Because “anthropogenic CO2 has the same [4-year] residence time of natural CO2,” this assumption is physically invalid.
Net-zero policies will literally have no detectable effect on atmospheric CO2 concentrations. In sum, “the IPCC’s assumptions and fundamentals are wrong.”
Racketeering Scheme?: Vaccine Makers Profit Twice by Selling Drugs to Treat Vaccine Injuries
By Brenda Baletti, Ph.D. | The Defender | February 5, 2026
A lawsuit filed by Children’s Health Defense (CHD) against the American Academy of Pediatrics (AAP) alleges that the AAP’s aggressive promotion of childhood vaccines created a “closed-loop” business model that set up pharmaceutical companies to profit from vaccines and from drugs used to treat vaccine injuries.
The lawsuit alleges the AAP violated the Racketeer Influenced and Corrupt Organizations Act or RICO, by running a decades-long racketeering scheme to defraud American families about the safety of the childhood vaccine schedule.
A “racket” exists when a service creates its own demand, according to the complaint.
In this case, the same companies that make pediatric vaccines have also acquired companies that develop treatments for autoimmune disorders, allergies and neurodevelopmental conditions — conditions recognized in vaccine package inserts as adverse events that occurred during clinical trials or in post-marketing studies.
The complaint cites Pfizer’s 2016 acquisition of Anacor Pharmaceuticals for $5.2 billion. Anacor makes Eucrisa, a drug that treats eczema. At the time, Eucrisa was approved for 2-year-olds. It was later approved for babies as young as 3 months.
Post-marketing data have linked vaccines — including GlaxoSmithKline’s ENGERIX-B hepatitis B vaccine — to eczema, according to the complaint. Research studies have also linked the condition to the COVID-19 and measles-mumps-rubella or MMR vaccines.
In another example, Sanofi in 2020 spent $3.7 billion to acquire Principia Biopharma, developer of an experimental therapy for immune thrombocytopenia, an autoimmune blood disorder.
Immune thrombocytopenia is listed as an adverse reaction to vaccines manufactured by other companies that the lawsuit alleges are part of the same vaccine racketeering enterprise. Those vaccines include Merck’s MMRII and GlaxoSmithKline’s Pediarix.
Other examples include GlaxoSmithKline’s 2012 acquisition of Human Genome Sciences in 2012 for $3.6 billion, which brought the lupus drug Benlysta into its portfolio, and Merck’s 2021 purchase of Pandion Therapeutics for $1.85 billion, which expanded its pipeline of inflammatory bowel disease treatments.
Not included in the lawsuit, but widely discussed in 2024, was Pfizer’s acquisition of Seagen. The biotech company makes drugs that use monoclonal antibodies to deliver anti-cancer agents to tumors while limiting damage to surrounding tissue.
Pfizer spent $43 billion to acquire Seagen, which in 2023 had projected sales of $2.2 billion. Studies have linked Pfizer’s COVID-19 vaccines to sharp rises in cancer rates.
The lawsuit argues that these types of acquisitions by vaccine makers create a revenue cycle in which vaccines function as a “customer acquisition mechanism” — because treatments for chronic conditions provide long-term pharmaceutical revenue.
“The enterprise profits from the vaccines, and profits again from the treatment of the vaccine package insert documented side effects,” the complaint states.
The filing also alleges that the AAP helps maintain this system by promoting expanded vaccination schedules and discouraging research that could explore potential links between schedule changes and chronic illness.
The allegations come amid ongoing public debate over vaccine safety, corporate influence in medicine and the transparency of postmarketing surveillance systems.
Health officials have long maintained that childhood vaccination programs are “safe and effective” and that adverse event reporting alone does not establish causation.
However, public trust in those authorities is at a historic low, as more people question the long-held positions of mainstream public health.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
When Threats Replace Evidence
What an Australian Newspaper Article Reveals About the Vaccine Compliance Machine
Lies are Unbekoming | February 5, 2026
The Sydney Morning Herald wants you to know the penalties. Doctors and nurses who falsify vaccination records face suspension, deregistration, and jail. Parents who seek them out face fraud investigations through Services Australia. The article names specific dollar amounts ($2,500 per child), quotes the Health Minister expressing shock and outrage, and reminds readers that AHPRA—the regulatory body that controls whether medical professionals can earn a living—is watching.
The article reads less as journalism than as a warning to anyone considering dissent.
The Herald is one of Australia’s oldest and most influential newspapers, the rough equivalent of the New York Times in reach and establishment credibility. When it publishes a piece like this, it speaks with institutional authority. The January 2026 article, “Parents are paying $2500 to falsify vaccine records,” arrives at a particular moment in Australian public health: vaccine uptake has “stalled below national targets,” mandate enforcement is creating a black market for exemptions, and parents are organising in Facebook groups 40,000 members strong.
To understand the context, American readers need to know what Australia built. Between 2014 and 2019, five Australian states—New South Wales, Victoria, Queensland, South Australia, and Western Australia—rolled out “no jab, no play” laws, which bar unvaccinated children from childcare and preschool enrollment entirely. The only exemptions are medical, and these require documented life-threatening allergic reactions or severe immunocompromise—conditions so narrow that most families cannot qualify no matter their concerns.
The coercion is not subtle—and it violates the government’s own rules. Australia’s Immunisation Handbook states that valid consent must be given “voluntarily in the absence of undue pressure, coercion or manipulation.” Denying a child access to childcare unless the parents comply is textbook duress. The government has built an enforcement apparatus that fails its own stated ethical standards.
The system was designed to make non-compliance economically devastating and socially impossible. And for years, it worked. But now that system is encountering mass resistance, and the Herald article’s purpose is to make examples—to signal what happens to doctors who help parents escape a coercive system, and to parents who refuse to comply.
Buried beneath the threats is a dead baby. Riley Hughes, 32 days old, is the emotional payload. His story opens the piece, provides the moral frame, and transforms regulatory enforcement into righteous protection of the innocent. Without Riley, this article is just an inventory of punishments. With Riley, non-compliance becomes child murder.
The story requires examination.
Riley developed “mild cold symptoms” at three weeks old. His mother took him to a doctor, who said he appeared “perfectly fine.” When he stopped feeding, she took him to the children’s hospital. By day three, doctors “suspected” whooping cough. By day four, he had pneumonia. By day five, he was on life support. He died at 32 days old. Riley died in February 2015—eleven years before this article was published. The Herald reached back over a decade to find its dead baby.
The article states that “The Bordetella pertussis bug had overwhelmed his tiny body.” This is presented as fact. But reading carefully, the diagnosis was never confirmed—doctors “suspected” whooping cough. The journalist’s assertion that pertussis killed Riley is not attributed to any medical source. It is simply declared.
More striking is what the article omits entirely: what happened during those five days of hospitalisation. What interventions were administered to a three-week-old infant? What antibiotics? What was the “life support” that preceded his death? The hospital’s role in Riley’s deterioration is invisible. The medical system appears only as the place where heroic efforts were made to save him from the disease that (we are told) the unvaccinated community gave him.
The article describes Riley as “too young” to be vaccinated against whooping cough, which is given at six to eight weeks in Australia. But it does not mention that under Australian guidelines, Riley would have received the Hepatitis B vaccine within 24 hours of birth. He was not an unvaccinated child. He was a vaccinated child who had not yet received this particular vaccine.
If Riley had been completely unvaccinated, that would be the story. “Unvaccinated baby dies of preventable disease” writes itself. Instead, the article performs a subtle shift: a vaccinated infant dies after five days of hospital intervention, and an entire class of people—parents who refused to vaccinate—are scapegoated to protect the system that failed him.
None of this can be stated with certainty. We do not have Riley’s medical records. We do not know what drugs were administered, what procedures were performed, what his body endured in those five days. But that is precisely the point: neither does the Herald, and neither do its readers. The article presents a story with a hole at its centre and fills that hole with a villain—the unvaccinated community—while the institution that actually had custody of Riley during his decline remains unexamined.
What we do know: Riley was vaccinated. He received the Hepatitis B vaccine at birth, as per Australian protocol. He then spent five days in hospital care before he died. This is a vaccinated child who died after days of medical intervention—and the article repurposes his death as a case against vaccine refusal.
The mother, Catherine Hughes, is quoted: “My son would likely be alive today if everyone in my community had been fully vaccinated against whooping cough.”
This is a grieving mother’s belief, given to her by a medical system that needed someone to blame. She has since founded the Immunisation Foundation of Australia and become a professional advocate for vaccination mandates. What the Herald does not disclose: as journalist Alison Bevege has documented, her foundation received $170,000 from Sanofi in 2023 and $100,000 from GSK in 2025. Hughes herself appears in GSK press releases promoting their products. The article presents her as a spontaneous voice of bereaved motherhood. She is a paid pharmaceutical spokesperson.
The article’s foundational premise—that unvaccinated children endanger the community—is not merely unexamined. Even within the mainstream framework of germ theory and disease transmission, the published science contradicts it.
In 2014, researchers at the FDA published a study using baboons to examine how the acellular pertussis vaccine actually works. The results, within the germ theory framework the researchers operated in, were unambiguous: vaccinated baboons exposed to Bordetella pertussis showed few symptoms but became colonised with the bacteria. They were then placed in cages with unvaccinated baboons—and by the researchers’ own account, the vaccinated animals passed the bacteria to the unvaccinated ones. The study’s conclusion: “acellular pertussis vaccines protect against disease but fail to prevent infection and transmission.”
A 2015 study by Althouse and Scarpino went further. Using epidemiological, genetic, and mathematical modelling data, they argued that asymptomatic spread from vaccinated individuals “provides the most parsimonious explanation for the observed resurgence of B. pertussis in the US and UK.” Vaccinated individuals who show no symptoms carry and spread the bacteria—according to the very framework the public health establishment operates within. The authors noted that this also explains the documented failure of “cocooning”—the strategy of vaccinating family members to protect newborns. By their own logic, it doesn’t work because the vaccinated family members become silent carriers.
Even by the establishment’s own standards, the pertussis vaccine does not prevent colonisation. It does not prevent spread. What it does, according to their own researchers, is suppress symptoms in the vaccinated individual while allowing them to pass the bacterium to others, including infants too young to be vaccinated.
These are peer-reviewed studies published in the Proceedings of the National Academy of Sciences and BMC Medicine. The FDA conducted the baboon study.
Meanwhile, within this same framework, the bacterium has apparently evolved under vaccine pressure. A 2014 Australian study found that between 30% and 80% of circulating pertussis strains during a major outbreak were “pertactin-deficient”—lacking the protein the vaccine targets. The authors observed that “pertussis vaccine selection pressure, or vaccine-driven adaptation, induced the evolution of B. pertussis.”
The pertussis vaccine suppresses symptoms. Whether it also creates asymptomatic carriers who spread an apparently evolving pathogen, as the establishment’s own researchers claim, remains their narrative to defend. But even within that narrative, the unvaccinated are not the problem—the vaccine is.
When the Herald article quotes a professor warning about “one of the kids there has whooping cough or measles, and it spreads through the childcare, putting your child at risk,” the establishment’s own science suggests the spreader is more likely to be a vaccinated child with no visible symptoms than an unvaccinated child who would be home sick.
Even within the establishment’s own framework, if Riley had pertussis, the most likely source—according to their own research on asymptomatic carriage—would be a vaccinated person, perhaps someone in his own family who had been “cocooned” as the health authorities recommend. The article does not explore this possibility. It cannot, because the entire enforcement apparatus rests on the premise that the unvaccinated are the danger.
The article is not confused about the science. It is not interested in the science. Its function is compliance enforcement, and its vectors are specific.
The first vector targets medical professionals. The article names a Perth nurse charged with fraudulently recording vaccines—though the case was dropped for lack of evidence. It names a Victorian doctor whose registration was suspended. It quotes AHPRA warning that practitioners found acting fraudulently face suspension or deregistration. The message to any doctor or nurse who might help parents escape the system: we are watching, and we will destroy your career.
This is not new. In December 2020, Dr. Paul Thomas, a Portland paediatrician who had practiced for 35 years, published a peer-reviewed study comparing health outcomes in vaccinated versus unvaccinated children in his practice. The data showed unvaccinated children were significantly healthier across multiple metrics. Within days of publication, the Oregon Medical Board issued an “emergency order” suspending his licence, claiming his “continued practice constitutes an immediate danger to the public.”
The Board’s letter accused Thomas of “fraudulently” asserting that his vaccine-friendly protocol improved health outcomes—the very thing his peer-reviewed data demonstrated. His paper was later retracted under circumstances its authors describe as dubious. Thomas eventually surrendered his licence rather than continue fighting the Board’s conditions, which prohibited him from consulting with parents about vaccines or conducting further research.
The pattern is consistent. Produce evidence that challenges the orthodoxy, lose your ability to practice medicine. The threat in the Herald article is not abstract. Medical professionals in Australia have seen what happens to dissenters.
The second vector targets parents. The article reminds readers that Services Australia investigates Medicare and Centrelink fraud. Parents who pay for falsified records are not just endangering children (according to the article’s framing)—they are committing crimes against the Commonwealth. The article implies that seeking workarounds exposes parents to criminal liability, transforming a decision about their child’s medical care into a prosecutable offence.
The third vector is reputational. The article quotes the Health Minister: “I am shocked and appalled that any doctor or nurse would falsify vaccination records.” Parents in the Facebook groups are framed as reckless conspirators, their concerns about vaccine safety transmuted into selfish endangerment of babies like Riley. The 2025 study cited in the article notes that 47.9% of parents with unvaccinated children “did not believe vaccines are safe” and 46.7% “would not feel guilty if their unvaccinated child got a vaccine-preventable disease.” These statistics are presented as moral indictments.
What the article does not mention: the same study found that nearly 40% of these parents “did not believe vaccinating children helps protect others in the community.” Given the published science on pertussis—even within the establishment’s own framework—these parents have a point.
In 2004, Glen Nowak, the CDC’s director of media relations, gave a presentation to the National Influenza Vaccine Summit titled “Increasing Awareness and Uptake of Influenza Immunization.” His slides explained that vaccine demand requires “concern, anxiety, and worry” among the public. “The belief that you can inform and warn people, and get them to take appropriate actions or precautions with respect to a health threat or risk without actually making them anxious or concerned,” Nowak explained, “is not possible.”
His recipe for demand creation included medical experts stating “concern and alarm” and predicting “dire outcomes” if people don’t vaccinate. References to “very severe” and “deadly” diseases help motivate behaviour. Pandemic framing is useful.
The Herald article follows this template precisely. It opens with a dead baby. It features a professor warning about diseases “spreading through childcare.” The Health Minister invokes “serious complications, hospitalisation, and in some cases, death.” The 14 measles cases since December are presented ominously, without context about how many of those cases involved vaccinated individuals or resulted in any serious illness.
The article also quotes Dr. Niroshini Kennedy, president of the paediatrics and child health division at the Royal Australasian College of Physicians, warning about “vaccine hesitancy.” What the article does not mention: the RACP has a foundation that partners with GSK, a major pertussis vaccine manufacturer. The expert voice warning about hesitancy has institutional financial ties to a company that profits from vaccination.
The financial stakes are not abstract. GSK’s pertussis products Boostrix and Infanrix generated $2.3 billion in 2023. Sanofi’s pertussis vaccine revenue hit $1 billion in 2024, up 10.8% on the previous year, driven by booster demand. When the Herald runs a story demonising vaccine refusers, it serves an industry measured in billions.
The article acknowledges, briefly, that public health experts warned in 2019 that “vaccine mandates can backfire, and simply induce parents to seek loopholes, and, worse, fuel negative attitudes towards vaccination.” This warning has proven accurate. Australia’s escalating mandate regime has not produced the desired compliance. It has produced a $2,500 black market and Facebook groups with 40,000 members sharing strategies for resistance.
The system’s response is not to reconsider the mandates. It is to escalate enforcement and amplify fear. The article is part of that escalation.
The escalation itself is diagnostic. Systems that can defend their policies on evidence do not need to inventory punishments in the newspaper. They do not need to reach back eleven years for a dead baby. They do not need AHPRA warnings and Health Minister quotes and reminders about criminal prosecution. They make their case and let the data persuade.
What the Herald article reveals, beneath its institutional authority, is a system that has run out of persuasive tools. The sequence tells the story: first came the information campaigns, which did not produce sufficient uptake. Then came the mandates—no jab, no play—which produced compliance but also resistance. Then came enforcement against the resisters, which produced a black market. Now comes the threat display in the national press, designed to frighten the black market into submission. Each escalation is a concession that the previous level of coercion failed. Each one is more desperate than the last.
A system confident in its science would welcome questions. A system confident in its products would publish the safety data that parents are asking for. A system confident in its outcomes would point to the evidence and let parents decide. This system prosecutes nurses, deregisters doctors, denies children access to childcare, and runs articles designed to make examples of anyone who dissents. That is not the behaviour of an institution operating from strength. It is the behaviour of an institution that knows it cannot survive scrutiny—and is scrambling to ensure that scrutiny never arrives.
What parents are waking up to, slowly and in growing numbers, is that the fundamental promise—vaccinate your children and they will be protected, vaccinate enough children and the community will be protected—is not supported by the evidence, even within the framework that public health authorities operate in. What they are discovering is that asking questions produces hostility rather than answers. What they are learning is that doctors who support informed consent are being systematically removed from practice, leaving parents with no one in the medical system willing to have honest conversations.
The 40,000 parents in that Facebook group are not there because they read misinformation. They are there because they asked questions their doctors couldn’t answer, or because their child had a reaction that was dismissed, or because they did the research the system told them not to do and found that the confident assurances didn’t match the published science.
The Herald article treats these parents as a problem to be solved through enforcement. It does not entertain the possibility that they might be responding rationally to real information. It cannot, because that would require examining the science—and the science does not support the policy.
Australia has constructed a system where parents lose childcare access if they do not vaccinate, where doctors lose their licences if they support parental choice, where asking questions about vaccine safety is framed as “misinformation,” and where a dead baby is deployed to transform regulatory non-compliance into moral monstrosity.
The article calls this public health. A more accurate description: this is what happens when a policy built on faulty premises meets a population that is beginning to see through it. Unable to defend the science, the system defends itself through threats, fear, and the weaponisation of grief.
Riley Hughes deserved better than to become a propaganda tool for the companies that fund his mother’s foundation. The parents seeking exemptions deserve honest information about what vaccines can and cannot do. The doctors trying to practice informed consent deserve to keep their licences.
None of them are served by an article whose purpose is to frighten dissenters into silence.
The system is telling parents: comply or be punished, and don’t ask questions. The parents are responding: we have questions, and your threats are not answers.
That tension will not be resolved by more enforcement. It will be resolved when someone in authority has the courage to address the questions honestly—or it will continue to escalate until the system’s credibility collapses entirely.
Forty thousand parents in one Facebook group suggest which direction this is heading.
References
The Article Under Discussion:
Olaya, K. (2026, January 31). Parents are paying $2500 to falsify vaccine records. It’s endangering babies like Riley. The Sydney Morning Herald. https://www.smh.com.au/national/parents-are-paying-2500-to-falsify-vaccine-records-it-s-endangering-babies-like-riley-20260127-p5nxah.html
Catherine Hughes Financial Disclosures:
Bevege, A. (2026, February 4). ‘Baby-Killers’ – Nine Newspapers falsely claim unvaccinated people killed a baby by spreading whooping cough. Letters from Australia. https://alisonbevege.substack.com/
RACP-GSK Partnership:
GSK Australia. RACP Foundation partnership announcement. Referenced in Bevege (2026).
Vaccine Revenue Figures:
GSK. (2024). Annual Report 2023. Boostrix and Infanrix/Pediarix revenue figures.
Sanofi. (2025). Fourth Quarter 2024 Earnings Report. Polio/pertussis/HiB vaccine sales.
Pertussis Vaccine and Asymptomatic Carriage:
Warfel, J. M., Zimmerman, L. I., & Merkel, T. J. (2014). Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model. Proceedings of the National Academy of Sciences, 111(2), 787-92. https://doi.org/10.1073/pnas.1314688110
Althouse, B. M., & Scarpino, S. V. (2015). Asymptomatic transmission and the resurgence of Bordetella pertussis. BMC Medicine, 13(1), 146. https://doi.org/10.1186/s12916-015-0382-8
Pertussis Vaccine Evolution and Waning Immunity:
Lam, C., Octavia, S., et al. (2014). Rapid increase in pertactin-deficient Bordetella pertussis isolates, Australia. Emerging Infectious Diseases, 20(4), 626-33. https://doi.org/10.3201/eid2004.131478
Tartof, S. Y., Lewis, M., et al. (2013). Waning immunity to pertussis following 5 doses of DTaP. Pediatrics, 131(4), e1047-52. https://doi.org/10.1542/peds.2012-1928
van Boven, M., Mooi, F. R., et al. (2005). Pathogen adaptation under imperfect vaccination: implications for pertussis. Proceedings of the Royal Society B, 272(1572), 1617-24. https://doi.org/10.1098/rspb.2005.3108
Dr. Paul Thomas Case:
Oregon Medical Board. (2020). In the Matter of: Paul Norman Thomas, MD. License Number MD15689: Order of Emergency Suspension. https://omb.oregon.gov/Clients/ORMB/OrderDocuments/e579dd35-7e1b-471f-a69a-3a800317ed4c.pdf
Lyons-Weiler, J., & Thomas, P. (2020). Relative Incidence of Office Visits and Cumulative Rates of Billed Diagnoses Along the Axis of Vaccination. International Journal of Environmental Research and Public Health, 17(22), 8674. [Retracted 2021]
Hammond, J. R. (2021). The War on Informed Consent: The Persecution of Dr. Paul Thomas by the Oregon Medical Board. Skyhorse Publishing.
CDC Fear-Based Messaging:
Nowak, G. (2004). Increasing Awareness and Uptake of Influenza Immunization. Presentation at the National Influenza Vaccine Summit, Atlanta, GA.
Vaccine Mandates and Backfire Effects:
Ward, J. K., et al. (2019). France’s citizen consultation on vaccination and the challenges of participatory democracy in health. Social Science & Medicine, 220, 73-80.
Suppression of Vaccine Dissent:
Martin, B. (2015). On the Suppression of Vaccination Dissent. Science and Engineering Ethics, 21(1), 143-57. https://doi.org/10.1007/s11948-014-9530-3
Australia’s No Jab, No Play Laws:
Australian state governments. No Jab, No Play legislation (2014-2019). New South Wales, Victoria, Queensland, South Australia, Western Australia.
Australian Immunisation Handbook — Consent Requirements:
Australian Government Department of Health. Australian Immunisation Handbook. Section: Valid Consent. https://immunisationhandbook.health.gov.au/
Featured Video
Bombing Iran Back Into the Stone Age /Lt Col Daniel Davis & Jim Jatras
or go to
Aletho News Archives – Video-Images
From the Archives
The Occupied Mentality Syndrome
Saudi Arabia on the American chessboard – Part 2
By B. J. Sabri | American Herald Tribune | April 19, 2016
Since the Korean War, but particularly since the Iranian Revolution of 1979 until today, the United States has been steadily escalating its military presence in the Persian Gulf. Taking advantage of many colossal events of the past 36 years, [1] the hyper-empire has institutionalized its massive presence on land and sea, and expanded its objectives to include the unambiguous physical control of the area, as well as the clear understanding that local Arab governments should abide by them. The pretext is always the same: in “defense” of the national interests and security of the United States. From observing how the United States has been interacting with the governments of the region, and by judging from the size of its expeditionary force, we could reach a basic conclusion. The United States is occupying, de facto, the entire Arabian Peninsula. (Yemen, devastated by Saudi and American jets is yet to be conquered. Oman? Britain returned not as colonial ruler but as a soft occupying power.)
Under this articulation, Saudi Arabia, Qatar, Kuwait, and the United Arab Emirates are virtually occupied countries. If we compare this type of occupation to the mandate and protectorate regimes of the past, the results might be identical—the nations affected by it lose sovereignty. When Arab governments comply with the objectives of a foreign power that station military forces on their national milieu, then that power controls them in multiple ways including how they react to policy deliberations and what decisions they intend to take on specific issues. A good method to verify the concept of effective occupation is this: take notice of what the United States says and wants, and then compare it to what the gulf rulers do in response. (I shall discuss this detail at some point in the upcoming parts.)
If the presence of US forces or other means of political pressure are a factor in Saudi Arabia’s interventionist Arab wars, then we need to debate this issue. However, from the history of resistance to colonialism, we learnt: if a powerful state imposes its order on a nation by military means or other forms of coercion, and if this nation does not resist that imposition, then a mental subordination to the powerful state will ensue. This is especially true in the case of Saudi Arabia. One single event, 9/11, has transformed it from a US “ally” into an instant political hostage of the American Empire. … continue
Blog Roll
 Aletho News
Aletho News- BREAKING: US JET SHOT DOWN OVER IRAN /Lt Col Daniel Davis & Nima Alkhorshid
- Now everyone is dumping US government bonds
- Brazilian Congressman seeks to bar Israeli military personnel from entering Brazil
- Official reveals evidence of Arab states’ involvement in US-Israeli war on Iran
- His Majesty’s head-chopper: Syria’s MI6-backed president bows to King Charles
- Forced to backtrack: ‘Israel’ drops Hezbollah disarmament goal
- Britain’s Lebanon surveillance network: A digital map for war
- Bahrain faces scrutiny for opposition crackdown after detainee killed
- Hegseth’s Pentagon Purge Designed to Prevent a Mutiny: Karen Kwiatkowski
- Greek shipping firms secretly transporting oil, weapons to Israel
- If Americans Knew
- Israel Is Blocking Palestinians from Easter at Church Where Jesus Resurrected
- Plot to assassinate Palestinian activist follows harassment campaign promoted by Zionist groups and elected officials
- Prominent New York synagogue hosts presentation on why U.S. Jews should support the ethnic cleansing of Gaza
- Tapper vs. Piker: Is the CNN Anchor Auditioning for David Ellison?
- Shouldn’t Democrats Be Able to Condemn Genocide?
- Israel-US kill negotiators, destroy civilian structures, but Iran’s military capabilities still largely intact – Daily Update
- ‘War crime’: Global condemnation as Israeli ministers celebrate death penalty law targeting Palestinian prisoners
- 7 Ways Israel Is Turning Lebanon Into Gaza
- World’s Leading Football Bodies Under Fire Over Israel Policies
- Experts warn of possible use of nukes against Iran
- No Tricks Zone
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
