Begging for the Wonder Drug
Five years later, we resolve never to forget how US hospitals deprived critically ill patients of ivermectin and other commonly used drugs that could have saved them.

Satoshi Ōmura, 2015 Nobel Laureate for his discovery of the ”wonder drug” Ivermectin, stands next to the River Blindness sculpture. His discovery cured this great scourge of the tropical world.
By John Leake | Courageous Discourse | December 13, 2024
As I was researching our book, The Courage to Face COVID-19: Preventing Hospitalization and Death While Battling the Bio-Pharmaceutical Complex, I was especially disturbed by countless stories of hospitals in various states who steadfastly refused to treat critically ill COVID-19 patients with ivermectin and other drugs (commonly used for other illnesses) that could have saved their lives.
I believe this episode constitutes the darkest chapter in the history of the U.S. hospital system. Strangely enough, the only serious legacy newspaper journalist in the entire country who covered it was Michael Capuzzo—formerly a reporter with the Miami Herald and the Philadelphia Inquirer, where he received four Pulitzer Prize nominations. Apart from Michael’s reporting . . . crickets.
Out of my conviction that we should never forget what U.S. hospitals did to patients who were consigned to die on ventilators instead of receiving FDA-approved, off-label drugs such as ivermectin, methylprednisolone, and even high dose aspirin, I am publishing our chapter on the extraordinary villains who committed this atrocity, and the good guys—including two great attorneys and humanitarians named Ralph Lorigo and Beth Parlato—who fought back. Please share this story with your friends and family and exhort them never to forget.
CHAPTER 28: Begging for the Wonder Drug
As Michael Capuzzo told the story in his long magazine piece “The Drug that Cracked Covid,” Judy Smentkiewicz was an eighty-year-old resident of Buffalo, New York. After working thirty-five years as an office manager for Metropolitan Life and raising two children, she had retired to her small house in the suburbs. A week after Senator Johnson’s second Senate hearing, she began preparing for Christmas, and looked forward to her two children, Michael and Michelle, visiting her for a few days. However, right after Michael and his wife arrived from Florida, she began to feel unwell. On December 22 she tested positive for Covid. Her kids were devastated and cancelled their Christmas celebration as Judy went into quarantine. A week later, she became short of breath and was rushed to the Millard Fillmore Suburban Hospital. On New Year’s Eve she was admitted to the ICU.
It was a terrible moment in which Judy and her children realized they might never see each other again. In the days that followed, the doctors and nurses with whom Michael spoke didn’t offer much hope. They said there were no medications for treating COVID-19 approved by federal health agencies apart from remdesivir. This was administered to Judy, but it seemed to have no beneficial effect. On New Year’s Eve, as her condition deteriorated, her two children and six of their friends gathered on the street below her hospital window and prayed for her.
Shortly after New Year’s Day, Michael received from his mother-in-law a video of Dr. Pierre Kory being interviewed by a reporter for Fox 10 News Now, KSAZ-TV in Phoenix, Arizona. That morning, Dr. Kory had given his Senate testimony on ivermectin. Michael watched it and was moved by Dr. Kory’s passionate intensity and eloquence. Immediately he called the hospital and told Judy’s attending physician that he wanted her to receive ivermectin. The doctor refused on the grounds that it wasn’t approved for COVID-19, but Michael refused to take no for an answer, and finally a hospital administrator approved one, 15-milligram dose. Less than twenty-four hours later, Judy was taken off the ventilator, and the next day she sat upright in a chair for a Zoom call with her son. She still wasn’t out of the woods, and when her heart started racing, she was moved to a cardiac unit, and the hospital refused to give her a second dose of ivermectin. Michael insisted but the hospital refused to budge.
And so, he contacted his friend and attorney Ralph Lorigo, and explained the situation. At the time, Lorigo knew nothing about ivermectin, so he too watched the interview with Dr. Kory, and then sued the hospital. New York State Supreme Court Judge Henry Nowak heard the case and ordered the hospital to commence treating Judy with four more doses of ivermectin, per her family doctor’s prescription.
The hospital refused to obey the judge’s order, which resulted in additional legal wrangling, including another hearing. Finally, the hospital’s lawyer agreed to allow Judy’s family doctor to administer the drug. He was under the impression it was on hand in the hospital’s pharmacy, but when he arrived to carry out his charge, he was told that it would have to be couriered from another facility. This caused another delay. Finally, at 11:00 pm that night, the second dose was administered, and she started to improve. Ten days later she walked out of the hospital.
As word spread about Judy’s happy outcome, Ralph Lorigo was contacted by countless others in the same situation, and soon his law firm had a new area of practice—trying to force hospitals to administer an FDA-approved, Nobel Prize winning, WHO “Essential Medication” to dying COVID-19 patients to whom nothing else was offered.
Mr. Lorigo was well-suited for the task. The energetic, punctilious attorney and Erie County Conservative party chairman has a formidable presence, with strong Italian good looks and a penchant for wearing beautifully tailored suit and power ties. Though he specialized in real estate law, he represented his clients seeking ivermectin with great care. A devoted family man with three children and multiple grandchildren, he empathized with the families who sought his help.
To be sure, it wasn’t an easy job, because the hospitals fought him tooth and nail, bringing multiple attorneys and expert witnesses to hearings. After a few more successes in which he prevailed and the patients recovered after receiving ivermectin, he received more queries than his staff could handle, so he contacted his friend, Beth Parlato, and asked her if she would be interested in taking some of the cases.
The 55-year-old attorney and mother of three had served as a judge in a New York State criminal court. Over the course of her career, she’d seen much of the good, the bad, and the ugly, but none of it had prepared her for the grueling path ahead. What she was about to witness would challenge all of her assumptions about the American healthcare and legal systems, and ultimately about human nature itself.
Most of her clients were referrals from the FLCCC, founded by Drs. Marik and Kory. The typical call would come into her office from a desperate husband or wife, daughter or son. Their stories were always the same. A much-loved family member had been languishing in hospital and was now headed for the ventilator and probable death. And though the doctors and nurses stated that the prognosis was poor, the hospital refused to administer ivermectin.
To patients and their families, the situation was incomprehensible. Many of Beth’s clients posed a variation of the question: “Mom [or dad] is declining and is probably going to die, so what’s the harm in her trying ivermectin?” Beth was at a loss for an answer. The hospital’s policy made no sense, neither as a matter of fact nor law. Many families wondered why “right to try” laws didn’t apply. Hospital attorneys claimed the “right to try” was only for experimental medications that were not yet FDA-approved. Ivermectin was FDA-approved, just not for the treatment of COVID-19.
Patients and their families found this argument perversely legalistic, but many judges—and all judges elected as Democrats—found it persuasive. Beth argued it was a legal, common, and longstanding medical practice to prescribe FDA-approved drugs off-label. Hospital attorneys retorted that the NIH guidelines for the treatment of COVID-19 did not recommend the off-label administration of ivermectin, and because the NIH was the final scientific arbiter of medical matters in the United States, the hospitals were required to follow its guidelines.
The trouble with the one-size-fits-all NIH guidelines for hospitalized COVID-19 patients was that they didn’t work. Almost a year into the pandemic, the United States had the highest COVID-19 death rate of the world’s top ten wealthiest nations and was in the top twenty nations with the highest death rates in the world. Approximately 80% of hospitalized patients who went on mechanical ventilation died. Also significant was the fact that that on January 14, 2021—in response to Senator Johnson’s letter requesting that the NIH review Dr. Kory’s presentation of evidence—the NIH dropped its recommendation against using ivermectin and adopted a neutral stance. Though far from satisfying for Dr. Kory and his colleagues, the NIH neutral stance at least gave doctors greater leeway to exercise their clinical judgement about the drug.
To make matters even more confusing, healthcare professionals were provided with broad legal immunity by the federal PREP Act (Public Readiness and Emergency Preparedness) of 2005. This authorized the Secretary of Health and Human Services to deploy a wide array of “Emergency Countermeasures” in the event of an infectious disease outbreak. When invoked by the Secretary of Health and Human Services, the PREP Act provides immunity for the “manufacture, testing, development, distribution, administration, and use of covered countermeasures.” On February 4, 2020, HHS Secretary Alex Azar declared COVID-19 an emergency and invoked the PREP Act.
The CARES Act of March 27, 2020, also provided immunity for healthcare workers treating COVID-19 patients. Additional immunity was granted by governors’ executive orders in all fifty states. The governor of New York State, in which Beth was practicing, provided the following immunity:
Conduct Covered: Civil liability for injury or death alleged to have been sustained directly as a result of an act or omission by person(s) covered.
Person(s) Covered: Physicians, physician assistants; specialist assistants; nurse practitioners; licensed registered professional nurses; licensed practical nurses.
Conduct Not Covered: Gross negligence.
Many observers who were documenting U.S. healthcare policy with respect to remdesivir wondered if all this liability protection could explain why the new, experimental drug was the hospital standard of care despite numerous red flags raised about its safety. The contrast of this policy with the strict policy against administering ivermectin was stunning.
Additionally, all the patients that Beth represented, and their families, stated in writing that they would indemnify the hospitals of liability for any adverse effects apparently caused by ivermectin, and that their primary care physicians would come to the hospital to administer it. Despite these multiple provisions of immunity, hospitals were still dead set against giving ivermectin to dying patients.
The hearings were brutal affairs in which hospital attorneys and expert witnesses portrayed Beth’s expert witness (on the safety and efficacy of ivermectin) as a delusional quack. Their most common line of attack was that Beth’s witness was a lone, eccentric voice in challenging the overwhelming scientific consensus that informed NIH guidelines. This rhetorical strategy ignored that many of mankind’s greatest scientific insights were the work of individuals who challenged the orthodoxy of their day. The growing body of evidence, including RCTs, cited by Beth’s witness was dismissed by hospital experts with the assertion that the evidence was “low quality.” Thus, the judge was presented with opposing expert witness claims about the evidence, only with the hospital’s witness also claiming he had “scientific consensus” and therefore the NIH on his side.
Beth tried to argue that the patient retained sufficient bodily autonomy to decide if he or she wished to take an FDA-approved drug off-label. The hospitals’ attorneys retorted that hospital patients had never had the right to decide their treatment, and that granting it with ivermectin would set a terrible precedent, opening a Pandora’s Box of future patients demanding treatments after hearing anecdotes about their efficacy. Beth regarded this argument as another legalistic dodge. Her clients weren’t presuming to practice medicine—they were dying men and women, desperately begging for the right to try an FDA-approved drug as a last and only hope when nothing else apart from remdesivir was being offered.
The hospitals claimed total sovereignty over the patient—a godlike power over all decisions affecting his life and death, with the patient afforded no say. For most gravely ill patients, the decision of this godlike power resulted in death. Thus, to sick patients and their families, the Lords of Healthcare were neither competent nor compassionate.
From: The Courage to Face COVID-19: Preventing Hospitalization and Death While Battling the Bio-Pharmaceutical Complex, by John Leake and Peter A. McCullough, MD, MPH, Foreword by Robert F. Kennedy Jr., Skyhorse, 2022.
POSTSCRIPT: As Dr. Pierre Kory noted in his book The War on Ivermectin, of the 80 lawsuits filed by lawyer Ralph Lorigo, in 40 the judge sided with the family, and in 40 with the hospital. Of those, in the 40 where patients received ivermectin, 38 survived, whereas of the 40 who did not, only 2 survived.
US shuts down ‘disinformation’ agency
RT | December 25, 2024
The US State Department’s Global Engagement Center (GEC) has shut down after Republicans cut its funding. The agency was responsible for spreading propaganda abroad and, according to conservatives, censoring dissident thought at home.
The GEC announced on Monday that it would cease operations by the end of that day. “The State Department has consulted with Congress regarding next steps,” the statement added.
The organization employed around 120 people and had an annual budget of $61 million. Established in 2016, its stated goal was to “recognize, understand, expose, and counter foreign state and non-state propaganda and disinformation efforts.”
In practice, the GEC spearheaded complex propaganda campaigns of its own. In two campaigns, the agency funded video games aimed at teaching children about the supposed dangers of anti-American narratives, releasing them in the UK, Ukraine, Latvia, Iraq, and Saudi Arabia.
During the coronavirus pandemic, the GEC funneled money to a range of NGOs which then compiled lists of social media accounts supposedly spreading “disinformation” about the virus and its origins, which were then presented to the platforms to be banned or removed. Many of the accounts belonged to what Twitter’s former trust and safety chief, Yoel Roth, called “ordinary Americans,” raising concerns among conservatives that the GEC was violating its prohibition on operating within the US.
In 2023, the GEC was forced to cut ties with George Soros’ ‘Global Disinformation Initiative’, after it emerged that the agency was paying Soros’ organization to compile lists of “high risk” news outlets to use in an advertiser boycott campaign. These news sites were predominantly right-leaning and American-based.
X owner Elon Musk called the GEC a “threat to our democracy” last year, describing the agency as the “worst offender in US government censorship [and] media manipulation.”
Musk was instrumental in finally shutting down the GEC. A mammoth 1,547-page spending bill put before the House of Representatives by Speaker Mike Johnson last week would have preserved funding for the agency, until Musk threatened to fund primary election challenges to any Republican who voted for it.
Musk decried the bill – which also included pay raises for lawmakers – as “criminal,” “outrageous,” “unconscionable,” and ultimately “one of the worst bills ever written.” President-elect Donald Trump and Vice President-elect J.D. Vance then released a joint statement against the bill, forcing Johnson to replace it with a trimmed-down piece of legislation totaling less than 120 pages.
This Musk-approved bill failed in a 235-174 vote, with 38 Republicans joining 197 Democrats to block its passage. It eventually passed after Republicans added a section suspending the US debt ceiling for two years, a move that will add trillions more to the federal government’s $36 trillion debt.
Covid-19 Vaccines White Clots Results – 2024
Medical Embalmers Across The Country
Dr. John Campbell | December 21, 2024
Former Air Force Major Thomas Haviland surveyed embalmers in 2024 about unusual clots being found in the bodies of vaccinated deceased.
NEW YORK – I’ve seen the clots vary from case to case, since the covid shot came around, we have had many young deaths i.e.: 50-60 year-olds with massive heart attacks and every one of them has had clots as discussed in this survey, seems many people just want to turn a blind eye to it all, it’s a shame. As someone who’s been around this for about 12 years, I have never seen anything like this.
VIRGINIA – I’m finding a lot of the white rubbery clots and had been taking pictures of them but it’s become the new normal… I don’t use a drain tube anymore because of all the clots. blood clots and the fibrous white ones. My angular forceps is my to go instrument to help remove them…
OHIO – The past few years I have seen a significantly larger percentage of clotting in almost all embalmings. These white fibrous clots are definitely unusual having never seen them before 2021. Although not seeing the white fibrous clots or micro clotting in a larger percentage of deceased, the number of grape jelly clots has significantly increased from years past in all decedents.
IDAHO – Sometimes I am given the information about if someone has had a certain vaccine. Sometimes I am aware they have had 5-6 doses of it. These are the people we are seeing with the abnormal clots or significant amount of clots.
FLORIDA – With many embalmings that I have seen these clots in, I have had to inject in multiple points. Both with case’s refrigerated and prep done within a couple of hours after death.
FLORIDA – Seems like traditional “chicken fat clots” are less frequent being replaced with Jelly, Fibrous, Micro-clotting.
IOWA – Very thick and large, I have had some the whole diameter of the arteries and longer than a foot long.
LOUISIANA – Some of these fibrous blots come out as a whole, if done carefully, that mimic the arterial system. These clots are clearly the cause of demise of these decedents, but were legally labeled as heart issues, which are not typically autopsied to fully determine actual cause of death.
NORTH DAKOTA – I have had SEVERAL cases in 2020-2023 of the white fibrous clots and most had COVID listed as a factor on their death certificates. However, in each case the family did not know if the decedent was vaccinated.
FLORIDA – Unusual clots has changed since COVID vaccine I only took 2 vaccine Pfizer refuse to take booster nor vaccine again.
Exclusive: 70% of Embalmers Report Finding Strange Blood Clots Beginning in Mid-2021
Covid Vaccine Injury Global Study: http://www.react19.org/study
Covid vaccine injury medical expense fund: http://www.react19.org/donate
=
Pentagon’s African Biolabs: Russia Warns of Global Pathogen Threat
Sputnik – 24.12.2024
The US military-biological presence on the African continent is growing at a rapid pace, Deputy Chief of the Radiation, Chemical and Biological Protection Forces of the Russian armed forces Major General Aleksey Rtishev said on Tuesday.
“The documents at our disposal confirm that the US military-biological presence on the African continent is increasing rapidly,” Rtishev told a briefing.
The United States deployed branches of naval military medical center in Ghana and Djibouti, Rtishev added.
“Active work in the region is being carried out by research organizations of the US Department of Defense. For example, branches of the military medical center of the naval forces are located in Ghana and Djibouti, where active work is being carried out in natural foci of diseases, isolation and sequencing of pathogens,” Rtishev said.
American specialists capable of enhancing the pathogenic functions of microorganisms are actively working in Africa, Rtishev said. He added that the US government views the region as a rich reservoir of dangerous infectious agents and a testing ground for experimental drugs, and Washington is using a biological risk management system in Africa that has already been tested in Georgia and Ukraine.
The US is actively engaged in:
- Nigeria: A joint medical research center and a military medical laboratory for the armed forces were established in 2024.
- Kenya: The US Army Military Medical Center has deployed a network of field stations to monitor the spread of infectious diseases throughout Equatorial Africa.
- Senegal: A new $35 million laboratory facility is nearing completion. This project involves the same Pentagon contractors that have worked in the former Soviet Union, including Armenia, Georgia, Kazakhstan, and Ukraine.
- Ghana and Djibouti: The US. has established branches of the National Naval Medical Center and is actively addressing natural disease outbreaks and isolating pathogens.
- The United States is conducting a project in 18 African countries to study the characteristics of infection occurrence and the resistance of pathogens to medical treatments.
According to Aleksey Rtishev, Washington is deliberately exploiting the economic challenges African nations face in the health sector to organize research initiatives, the general warns. Rtishev noted that the US fears that Russia and China could expose American military and biological programs.
The United States often does not disclose the ultimate goals of its experiments to partners, who are often unaware of the risks involved, he said.
MRNA VACCINES POSE ONGOING CONCERNS IN CHILDREN
The HighWire with Del Bigtree | December 19, 2024
A new pediatric study on the effectiveness of the COVID vaccinations on children aged 6 months to 4 years in age has a shocking conclusion. Meanwhile, Moderna is developing an mRNA vaccine for RSV for children that has undergone several safety pauses because of severe injury to babies.
Let’s Retire Overused Words. First, ‘Misinformation’
By Dr. Pierre Kory & Mary Beth Pfeiffer | Real Clear Health | December 16, 2024
In a seismic political shift, Republicans have laid claim to an issue that Democrats left in the gutter—the declining health of Americans. True, it took a Democrat with a famous name to ask why so many people are chronically ill, disabled and dying younger than in 47 other countries. But the message resonated with the GOP.
We have a proposal in this unfolding milieu. Let’s have a serious, nuanced discussion. Let’s retire labels that have been weaponized against Robert F. Kennedy Jr., nominated for Health and Human Services Secretary, and many people like him.
Start with discarding threadbare words like “conspiracy theory,” “anti-vax,” and the ever-changing “misinformation.”
These linguistic sleights of hand have been deployed—by government, media and vested interests—to dismiss policy critics and thwart debate. If post-election developments tell us anything, it is that such scorn may no longer work for a population skeptical of government overreach.
Although RFK has been lambasted for months in the press, he just scored a 47 percent approval rating in a CBS poll.
Americans are asking: Is RFK on to something?
Perhaps, as he contends, a 1986 law that all-but absolved vaccine manufacturers from liability has spawned an industry driven more by profit than protection.
Maybe Americans agree with RFK that the FDA, which gets 69 percent of its budget from pharmaceutical companies, is potentially compromised. Maybe Big Pharma, similarly, gets a free pass from the television news media that it generously supports. The U.S. and New Zealand, incidentally, are the only nations on earth that allow “direct-to- consumer” TV ads.
Finally, just maybe there’s a straight line from this unhealthy alliance to the growing list of 80 childhood shots, inevitably approved after cursory industry studies with no placebo controls. The Hepatitis B vaccine trial, for one, monitored the effects on newborns for just five days. Babies are given three doses of this questionably necessary product—intended to prevent a disease spread through sex and drug use.
Pointing out such conflicts and flaws earns critics a label: “anti-vaxxer.”
Misinformation?
If RFK is accused of being extreme or misdirected, consider the Covid-19 axioms that Americans were told by their government.
The first: The pandemic started in animals in Wuhan, China. To think otherwise, Wikipedia states, is a “conspiracy theory,” fueled by “misplaced suspicion” and “anti-Chinese racism.”
Not so fast. In a new 520-page report, a Congressional subcommittee linked the outbreak to risky U.S.-supported virus research at a Wuhan lab at the pandemic epicenter. After 25 hearings, the subcommittee found no evidence of “natural origin.”
Is the report a slam dunk? Maybe not. But neither is outright dismissal of a lab leak.
The same goes for other pandemic dogma, including the utility of (ineffective) masks, (harmful) lockdowns, (arbitrary) six-foot spacing, and, most prominently, vaccines that millions were coerced to take and that harmed some.
Americans were told, wrongly, that two shots would prevent Covid and stop the spread. Natural immunity from previous infection was ignored to maximize vaccine uptake.
Yet there was scant scientific support for vaccinating babies with little risk, which few other countries did; pregnant women (whose deaths soared 40 percent after the rollout), and healthy adolescents, including some who suffered a heart injury called myocarditis. The CDC calls the condition “rare;” but a new study found 223 times more cases in 2021 than the average for all vaccines in the previous 30 years.
Truth Muzzled?
Beyond this, pandemic decrees were not open to question. Millions of social media posts were removed at the behest of the White House. The ranks grew both of well-funded fact-checkers and retractions of countervailing science.
The FDA, meantime, created a popular and false story line that the Nobel Prize-winning early-treatment drug ivermectin was for horses, not people, and might cause coma and death. Under pressure from a federal court, the FDA removed its infamous webpage, but not before it cleared the way for unapproved vaccines, possible under law only if no alternative was available.
An emergency situation can spawn official missteps. But they become insidious when dissent is suppressed and truth is molded to fit a narrative.
The government’s failures of transparency and oversight are why we are at this juncture today. RFK—should he overcome powerful opposition—may have the last word.
The conversation he proposes won’t mean the end of vaccines or of respect for science. It will mean accountability for what happened in Covid and reform of a dysfunctional system that made it possible.
Dr. Pierre Kory, M.D., a pulmonologist and critical care specialist, is president emeritus of the FLCCC Alliance. Mary Beth Pfeiffer is an investigative reporter and author.
Documents Show CISA Monitored and Influenced Domestic Speech on COVID-19 Through Private Sector Partners
Private entities were enlisted to flag content, even accurate information.
By Didi Rankovic | Reclaim The Net | December 20, 2024
America First Legal (AFL) has revealed new information from a document it has been able to obtain through the lawsuit filed against the Cybersecurity and Infrastructure Security Agency (CISA).
CISA is part of the US Department of Homeland Security (DHS), which has a “foreign disinformation” unit, the Countering Foreign Influence Task Force (CFITF).
However, as early as mid-February 2020, CISA (via CFITF) had already started to monitor domestic speech about Covid – nearly a month before the pandemic was officially declared by the UN’s WHO, and before orders started to be issued to shut down schools and businesses in the US.
Even though several layers deep, CFITF was still a government entity, and in order to circumvent constitutional issues related to censorship of online speech, the document indicates that the unit turned to what AFL brands “the censorship industrial complex” – specifically, its private sector component.
These were “fact checkers,” “bias raters” and similar that keep cropping up in revelations about the Covid-era censorship: Atlantic Council DFR Lab, Media Matters, Stanford Internet Observatory, Alliance for Securing Democracy, Center for Countering Digital Hate (CCDH) (a UK-based group, which now passes as “British-American”), Global Disinformation Index (GDI), and even an openly foreign government project, EU’s “EU vs. Disinfo.”
Among the kinds of speech CFITF would monitor and/or flag was that of President Trump, his comments about Hydroxychloroquine going back to 2020. The document reveals that CFITF (via Atlantic Council, DFR Lab) knowingly chose to give itself the right to flag even accurate information, justifying a thing as serious as censorship by presenting hypothetical scenarios:
“Once-accurate information can become misinformation as it ages, leading to erroneous conclusions and misinterpretation of the current situation,” the document reads. This was put in the context of the rapidly changing “nature” of the pandemic.
However, it took years for the same awareness – that information related to Covid was constantly changing – to start reversing some censorship decisions (e.g., the Covid origin theory).
As for CISA/CFITF early pandemic activities affecting online speech, AFL believes that they may represent “a violation of what’s known as the Supreme Court’s ‘major questions’ doctrine, which holds that government agencies must not stray from the specific legal authorities given to them by Congress.”
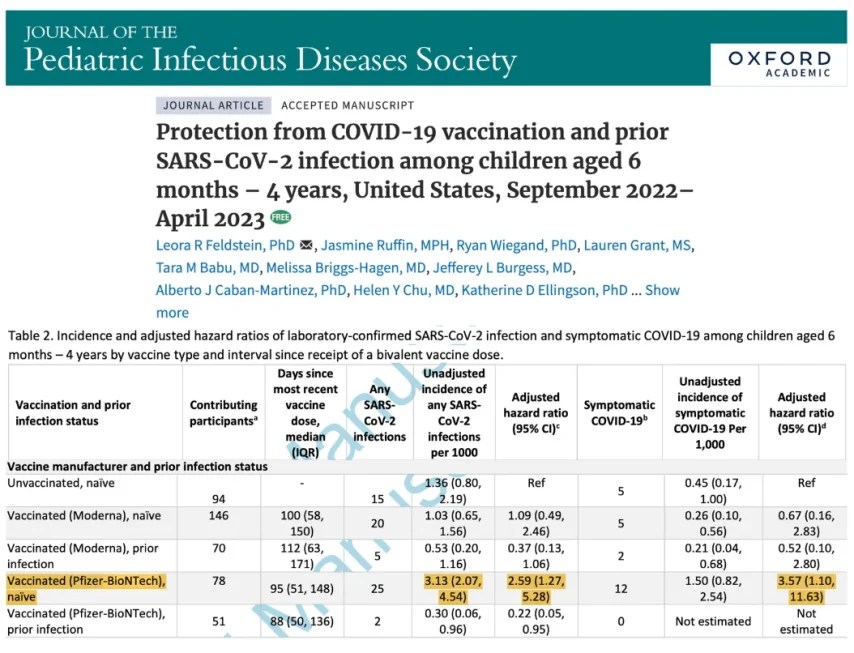
Pfizer mRNA ‘Vaccinated’ Children Significantly More Likely to Get COVID-19 Than Unvaccinated Peers
By Nicolas Hulscher, MPH | Courageous Discourse | December 16, 2024
A new study was just published in the Journal of the Pediatric Infectious Diseases Society titled, Protection from COVID-19 vaccination and prior SARS-CoV-2 infection among children aged 6 months – 4 years, United States, September 2022–April 2023. The study combined data from three prospective cohort studies (PROTECT, CASCADIA, and CoVE) conducted in the United States from September 1, 2022, to April 30, 2023. Included 614 children aged 6 months to 4 years living in Washington, Oregon, Michigan, Arizona, and Utah.
Here are the key findings:
- Increased Risk with Pfizer-BioNTech Vaccination:
- Children vaccinated with Pfizer-BioNTech without prior SARS-CoV-2 infection were 159% more likely to get infected and 257% more likely to develop symptomatic COVID-19 compared to unvaccinated children without prior infection:
- Hazard Ratio (HR) for infection: 2.59 (95% CI: 1.27–5.28).
- HR for symptomatic COVID-19: 3.57 (95% CI: 1.10–11.63).
- Children vaccinated with Pfizer-BioNTech without prior SARS-CoV-2 infection were 159% more likely to get infected and 257% more likely to develop symptomatic COVID-19 compared to unvaccinated children without prior infection:
- Prior Infection Offers Robust Protection:
- Children with prior SARS-CoV-2 infection (unvaccinated) had a significantly lower risk of reinfection compared to unvaccinated, infection-naïve children:
- HR for infection: 0.28 (95% CI: 0.16–0.49).
- HR for symptomatic COVID-19: 0.21 (95% CI: 0.08–0.54).
- Children with prior SARS-CoV-2 infection (unvaccinated) had a significantly lower risk of reinfection compared to unvaccinated, infection-naïve children:
- No Protective Effect from Vaccination Alone:
- There was no significant reduction in the risk of infection or symptomatic COVID-19 for vaccinated children (Moderna or Pfizer-BioNTech) compared to unvaccinated children:
- HR for infection with vaccination alone: 1.23 (95% CI: 0.69–2.16).
- HR for symptomatic COVID-19 with vaccination alone: 1.61 (95% CI: 0.65–4.03).
- There was no significant reduction in the risk of infection or symptomatic COVID-19 for vaccinated children (Moderna or Pfizer-BioNTech) compared to unvaccinated children:
- Boosters Show No Significant Protection:
- Among children who received at least one bivalent booster dose, there was no significant reduction in infection or symptomatic COVID-19:
- HR for infection with a bivalent booster: 0.74 (95% CI: 0.37–1.48).
- HR for symptomatic COVID-19 with a bivalent booster: 1.04 (95% CI: 0.37–2.96).
- Among children who received at least one bivalent booster dose, there was no significant reduction in infection or symptomatic COVID-19:
In other words, these injections do the opposite of what they’re supposed to do. Instead of protecting against COVID-19, these genetic injections either fail or increase the risk. The CDC should immediately revoke their recommendations for children aged 6 months and older to receive a COVID-19 booster injection.
Nicolas Hulscher, MPH
Epidemiologist and Foundation Administrator, McCullough Foundation
Congo’s Health Ministry Confirms ‘Disease X’ is Malaria
Outbreak began shortly after Congo’s rollout of the novel R21 virus-like particle malaria vaccine
By Nicolas Hulscher, MPH | Courageous Discourse | December 17, 2024
The Democratic Republic of Congo’s health ministry announced today that the previously unidentified illness coined as ‘Disease X’ by the media and Africa CDC circulating in the Panzi health zone has been confirmed as a severe form of malaria:
“The mystery has finally been solved. It’s a case of severe malaria in the form of a respiratory illness,” the health ministry said in a statement, adding that malnutrition in the area had weakened the local population, leaving them more vulnerable to disease.
This confirms our observations made last week, where we expected this to be malaria based on early testing. However, health agencies continued to ignore that possibility until now:
This entire situation reinforces how the mainstream media consistently attempts to generate as much fear as possible. They were caught propagating severe malaria coupled with malnutrition as the ominous ‘Disease X,’ fueling unnecessary panic:

In an emailed statement to USA TODAY, the World Health Organization (WHO) still claims it hasn’t conclusively determined the cause of the illness yet and lab testing is ongoing. This is similar to when the WHO falsely claimed that an individual in Mexico died of H5N2 bird flu. Soon after the claim, the Mexican government clarified: “A team of experts from the Health sector ruled that the person identified with influenza A (H5N2) did not die because of this virus, but as a result of chronic conditions that generated septic shock.” They added, “The diseases he suffered were long-term and caused conditions that favored the failure of several organs, specialists concluded.” The individual suffered from kidney disease, type 2 diabetes, and systemic arterial hypertension for more than 14 years.
Right before this malaria outbreak began, in late October, the Congo introduced the novel R21 malaria vaccine into their national immunization program. “R21 is a virus-like particle comprising the central repeats of Asn-Ala-Asn-Pro (NANP) and C-terminal sequence of circumsporozoite protein fused to the hepatitis B surface antigen (HBsAg).” It would not be surprising if this new vaccine played a significant role in triggering or exacerbating the severe malaria outbreak.
FDA Advisers Bullish on RSV Shots for Kids, Even as Safety Signals Shut Down Moderna Trials
By Brenda Baletti, Ph.D. | The Defender | December 13, 2024
Advisers to the U.S. Food and Drug Administration (FDA) met Thursday to discuss the future of pediatric respiratory syncytial virus (RSV) vaccines after Moderna was forced to abruptly halt clinical trials for its mRNA RSV vaccine in children ages 5-23 months.
Clinical trial data released earlier this week in an FDA briefing document showed that rather than preventing RSV disease in small children, Moderna’s vaccine likely caused higher rates of severe RSV illness in its Phase 1 clinical trial.
Moderna halted the trial in July after it was informed that two babies in the vaccine group had developed severe RSV disease. The company didn’t publicly announce that the trial was discontinued until September.
The data presented Thursday at the Vaccines and Related Biological Products Advisory Committee meeting showed that 12.5% of vaccinated children developed severe RSV disease as compared to just 5% of children in the placebo group.
Among the children who developed symptomatic RSV disease, 26.3% in the vaccinated group progressed to severe disease, while only 8.3% of those in the placebo group did.
These results were concerning given the history of past attempts to develop an RSV vaccine for infants. In the 1960s, an experimental formalin–inactivated RSV vaccine for children led to two toddler deaths, and 80% of vaccine recipients required hospitalization for severe RSV.
The illnesses were attributed to vaccine-associated enhanced respiratory disease (VAERD) — a phenomenon that occurs when vaccination promotes immune responses that exacerbate the disease caused by subsequent infection with the pathogen the vaccine was meant to protect against.
In light of that history, and because the mechanisms that cause VAERD are still largely unknown, the FDA convened the advisory committee to discuss the implications of Moderna’s trial outcomes for other pediatric RSV vaccines.
The committee did not vote on Thursday or make any formal recommendations. Members watched presentations from consultants, the FDA, and pharmaceutical companies and discussed the risks and benefits of developing RSV vaccines for children.
They also commended Moderna for reporting its results and the existing clinical safeguards for recognizing early safety signals in pediatric RSV trials.
Vaccine makers developing 26 different RSV vaccines or monoclonal antibodies
The briefing document stated that the FDA was halting enrollment for all investigational trials for RSV vaccines for infants and toddlers under age 2 and children ages 2 through 5 who haven’t previously had RSV.
The FDA clarified at the outset of the meeting that the hold does not apply to vaccine candidates that use live attenuated vaccines, because there is no evidence that vaccines developed on this platform cause VAERD.
Advisers seemed to agree, except for Dr. Karen Kotloff who voiced concerns there was not enough information to assume that live attenuated vaccines don’t carry the same potential risk.
Dr. Pedro Piedra, who presented on clinical and non-clinical aspects of RSV vaccine safety shared a slide listing RSV vaccines and monoclonal antibodies currently in trials.
There are five pediatric vaccines other than Moderna’s — which Moderna’s Christine Shaw, Ph.D., definitively stated is no longer moving forward — in the pipeline. Four of them are for live-attenuated vaccines.
Vaccine makers are developing 26 different RSV vaccines or monoclonal antibodies for all age groups, all vying to enter a rapidly expanding market.
PR Newswire projected in 2023 the global RSV vaccine and antibody market would be worth $2.61 billion dollars in 2024 and rise to $13.59 billion by 2030.
Piedra — who began his presentation with the quick disclosure that he has grants for RSV prevention research from GSK, Icosavax and Merck and is a paid consultant in the field for Merck, Moderna, Pfizer and Sanofi — presented an optimistic picture of RSV vaccine development, citing protection offered by recently approved maternal vaccines and monoclonal antibodies.
Moderna’s results did raise some platform-specific concerns, Piedra conceded.
He listed the types of safety concerns that could be associated with different vaccine platforms — febrile seizures with adjuvanted or high-dose vaccines or when RSV vaccines are co-administered with other vaccines, autoimmunity that could be associated with new adjuvants, respiratory issues with intranasal vaccines, and systemic illnesses with vector-based or mRNA vaccines.
‘Unmet need’ as justification to push for more RSV vaxes for small children
Presenters repeatedly stated that there was an “unmet need” for pediatric RSV vaccines, especially for children between 8 months and 2 years old.
RSV usually causes mild cold-like symptoms, but in some cases can lead to hospitalization and death in infants and the elderly. By age 2, 97% of all babies have been infected with RSV, which confers partial immunity, making any subsequent episodes less severe.
The disease burden for infants can be serious. In the U.S., RSV infection is the leading cause of infant hospitalization among those younger than 6 months, although a very small percentage of children with the virus will die.
An FDA representative said the Centers for Disease Control and Prevention (CDC) estimates that 100-200 infants die per year from the disease. However, internist Dr. Meryl Nass told The Defender that even those low numbers may overestimate mortality.
Nass pointed to a CDC study analyzing RSV deaths in infants between 2005 and 2016 and found a total of 314 deaths in children under age 1, or 25 on average per year, Nass reported. Only 17 of those deaths per year listed RSV as the underlying cause of death.
The FDA also said that maternal vaccines and monoclonal antibodies had begun to reduce those numbers, but emphasized there is still an “unmet need” for a vaccine for children going into their second RSV season — even as it presented data showing hospitalizations in that season are lower.
Moderna said this “unmet need” drove them to develop their failed vaccine. A Sanofi representative, who gave an update on their live-attenuated RSV virus, said the company sought to meet that “unmet need” for children in their second RSV season.
Sanofi also sells nirsevimab — brand name Beyfortus — the monoclonal antibody shot the CDC recommends for all newborns to protect them in their first RSV season.
Sanofi and the National Institutes of Health (NIH) are collaborating on the live-attenuated virus vaccine platform. The NIH developed 16 different vaccine candidates that it trialed in children and currently has one SP-125 in Phase 3 clinical trials.
These vaccines have not shown VAERD after one season of surveillance, the Sanofi representative said. The safety trials showed no safety concerns and SP-125 is currently being tested for efficacy in toddlers 6-22 months of age, but it is not yet fully enrolled.
During the “public comments” section of the meeting, three other vaccine makers promoted their vaccines to the committee.
Goal is more RSV shots for kids to provide passive immunity followed by ‘active immunity’
FDA asked the committee members to discuss existing evidence on whether infants and toddlers could eventually get sequential administration of RSV monoclonal antibodies followed by RSV vaccines.
That would mean even more shots on the childhood immunization schedule. The monoclonal antibodies or maternal vaccination would provide babies with “passive immunity” — antibodies to fight the virus that weren’t created by their own immune systems.
Then, in this schema, a two- or three-shot course of an RSV vaccine could protect babies from RSV in the second season, giving them “active immunity.”
Most committee members said more data were necessary to evaluate the safety of such a plan, but they generally agreed that it was a good direction to move in.
Watch the meeting here.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
RFK Jr. and the Samoan Measles Outbreak
By David Marks | Brownstone Institute | December 15, 2024
When the nomination of Robert F. Kennedy, Jr. as Health and Human Services Secretary comes before the Senate, the specter of the Samoan measles outbreak of 2019 will dramatically be invoked to challenge him. Kennedy’s critics have repeatedly relied on this topic, citing stories that claim he was responsible for an epidemic in 2019 that caused at least 83 children to die due to vaccine hesitancy. In recent articles, reporters quote previous news coverage relying on unsubstantiated and minimal data to justify their analysis.
These stories repeat dubious assertions, fail to discuss any pathological analysis, and dismiss Kennedy’s considered support of healthcare in Samoa. He had assisted the Samoan government in developing a system for health officials to assess the efficacy and safety of medical interventions or drugs, including vaccines.
In November 2019, while the deaths of Samoan children were rapidly increasing, Kennedy wrote a comprehensive letter to the Samoan Prime Minister, presenting some possible causes of the unprecedented, virulent outbreak of measles. His concerns about the epidemic in Samoa highlight striking anomalies that were apparent to a few investigators at the time, although they remain unexplained.
The most convenient and generally accepted explanations of the outbreak claim the epidemic was the result of hesitancy, causing the population to be under-vaccinated. Measles vaccination rates were low due to the previous deaths of two infants given improperly formulated injections, which had nothing to do with Kennedy’s views.
Any considered analysis of the accessible facts soundly contradicts the conjecture that the high death count was related to low vaccination rates.
In most measles epidemics, mortality is on average one in one thousand, and dying children are often malnourished or immunocompromised. From October through December of 2019, over one in a hundred Samoan children with the disease died, ten times more than any previous outbreak in the world. No accounting for this overt statistical deviance has been published.
Despite the presumptions of those who attack Kennedy, there was never any investigation into any aspect of this baffling tragedy. Edwin Tamasese, a health advocate who questioned Samoan government policies during the outbreak, gave Kennedy some insight into what was happening.
Tamasese was concerned about the number of sick and dying Samoan children and began to assist families whose children were severely ill. He and his colleagues encountered conditions that contradicted the government’s narrative.
While the press condemned him as an anti-vaxxer, Tamasese’s interventions and observations are revelatory. In an interview after the outbreak subsided, he said, “We were very careful to take statistics when we were going in to try to identify trends. When we assessed our numbers, 98 percent of those who were getting ill had been vaccinated consistently six to seven days prior to illness. The excuse was that the vaccine did not have time to become effective. However, according to an immunologist on the team, the six to seven-day period was also the length of time it would take an under-attenuated vaccine to make the recipient sick.”
Doctors in hospitals also reported that the very ill and dying children did not have symptoms consistent with normal cases of measles. When the outbreak began, blood from the first thirty-nine cases had been sent to Australia; only seven samples were positive for measles.
The government stopped testing to confirm the cause of these deaths in early November 2019. Without scientific confirmation, illness and mortality were attributed to low immunization rates. Samoan health authorities continued to claim that the only remedy for the deadly epidemic was a drive to increase vaccination; however, the campaign appeared to increase the number of measles cases.
Neighboring Pacific island countries, Tonga and Fiji, which had concurrent outbreaks of the virus — and had a different source of the measles vaccine — did not suffer the same dramatic mortality rates. This should have raised concerns, yet there hasn’t been an inquiry into why the Samoan government switched vaccine sourcing from India to Belgium midway through the crisis.
A renewed effort to vaccinate with this alternate supply began in the first week of December 2019; it was hailed as the reason the outbreak subsided. Measles vaccines take at least 10 days before creating an immune response. There has been no explanation for the data confirming that the onset of cases dropped dramatically two weeks before this vaccination drive could have had any effect.
The government response was not driven by factual analysis; the effort focused on promoting the vaccine and silencing those questioning authority.
With Samoan officials and the press deriding his work and views, Tamasese was arrested and charged with incitement of a government order and treating children without a license. Although this was deemed appropriate justice by the international news media as they echoed the government’s praise of the vaccine, reporters again failed to present the questions raised by the outbreak.
The prosecution’s primary witness against Tamasese was a nurse whose child had measles. He had suggested that administering vitamins A and C could be helpful — and standard medical treatment for measles patients. She had taken his advice and admitted that her child recovered soon afterward.
Tamasese reported that when the nurse left the courtroom, the judge, in throwing out the case, said, “That witness may as well have represented the accused.” There was relative silence from the news media when all charges against him were dismissed.
While worldwide attention on Samoa ignored dramatic inconsistencies, Kennedy was one of the few people who asked detailed and important questions. His views were marginalized; it was easier and politically correct to blame the tragedy on low rates of vaccination.
The relatively few details known about the Samoan measles outbreak indicate that forces intent on presenting vaccines as an infallible, unquestionable remedy will not tolerate scrutiny or admit failures. This continuing devious tactic is applied internationally and is eagerly supported by most governments and the press.
Analysis of the Covid-19 pandemic has only recently vindicated those who were scorned for questioning the response. The parallels to the unfolding of the epidemic in Samoa are not obscure, and support Kennedy’s contention that vaccine development, manufacturing, and application need much more effective evaluation and monitoring to prevent complications and death.
When the US government assures the public that any vaccine or medication is safe and effective, this must come from an independent, thorough, and transparent process, rather than relying only on the words and actions of those with vested interests.
The current criticism of Kennedy is an endeavor to make him look dangerously ignorant and irresponsible to sway members of the Senate. Much to the chagrin of those who vilify him, his efforts to understand and assist in the Samoan measles outbreak exemplify his thoughtfulness and capabilities.
RFK, Jr. is at the forefront of healthcare oversight; his confirmation as HHS Secretary will ensure that Americans benefit from his experience and knowledge.
Featured Video

The US bombed the Shahs house lol
or go to
Aletho News Archives – Video-Images
From the Archives
How a War with Iran Would Diminish American Power
By Greg Scoblete | The Compass | August 13, 2010
Jennifer Rubin wants a war with Iran:
But the emphasis on the existential threat to Israel ignores a more basic issue for Americans to ponder: a nuclear-armed Iran represents a dagger at the heart of America and an existential threat to our status as a superpower and guarantor of the West’s security. As to the former, Iran is pressing ahead with its long-range ballistic missile program. First the Middle East and Eastern Europe, then all of Europe and, within a matter of years, the U.S. will be within range of Iranian missiles. If those are nuclear and not conventional, what then? We’re not talking about whether Iran is going to be “merely” a destabilizing factor in the Middle East or whether it will set off an arms race with its neighbors or imperil Israel’s existence. We’re talking about whether America will then be at risk (and lacking sufficient missile-defense capabilities if we continue to hack away at our defense budget). The argument about whether mutual assured destruction can really work against Islamic fundamentalists who have an apocalyptic vision becomes not about Israel’s ability to deter an attack but about ours. Those who oppose American military action have an obligation to explain why America should place itself in that predicament.
I would argue that any obligation to present an explanation lies with those whose disastrous policy prescriptions with respect to Iraq lead America into the worst strategic blunder in the country’s recent history. That aside, note the blind faith in the power of the military to actually achieve its ends. … continue
Blog Roll
 Aletho News
Aletho News- Iran Threatens to Close Red Sea to Shipping in Response to Invasion
- Iran in excellent position to prevail in war with US, Israel: John Mearsheimer
- Iran warns US: Do not call your retreat an agreement
- Neighbors first – Moscow signals shift in energy strategy
- Almost 400 Ukrainian drones downed over Russia in single night – MOD
- Battle for Hungary: How the Russiagate blueprint has been unleashed against Orban
- Brussels warns Slovakia over ‘discriminatory’ dual fuel pricing targeting foreign drivers
- Hungary to halt gas deliveries to Ukraine – Orban
- The US bombed the Shahs house lol
- The London Ambulances Attack: Of Course It Was A False Flag
- If Americans Knew
- Jacob Reses, one of the most powerful pro-Israel operatives in Trump’s Washington
- Israeli-US assaults kill or injure 87 children a day – Not a ceasefire Day 166
- ‘Forever live by the sword’: Understanding Israelis’ massive support for Iran war
- UN’s special rapporteur on human rights says Israel is systematically torturing Palestinians
- Trump White House plagiarized Iran war manifesto from Israel-aligned think tank
- Gaza says 6–10 patients die daily waiting for treatment abroad as Israel blocks medical evacuations
- ‘Substantial evidence’ of double-tap strike in killing of Gaza’s Hind Rajab
- ‘Do Not Want To Die For Israel’: Doubts About Trump’s Iran Strategy Spread Among Troops
- Instead of taking Joe Kent’s claims seriously, the media is disregarding him as an antisemite
- Joe Kent’s Explosive Interviews about his Resignation over the Iran War
- No Tricks Zone
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis
- New Study Documents A 20-Year Pause In Arctic Sea Ice Decline – Driven By Internal Variability
- Wake-up Call: Survey Shows Majority Of Germans Now Favor Postponing Climate Targets!
