Of all rackets, the so-called “renewable energy” racket may be the most fraudulent and nonsensical. What geologists call the “Last Glacial Period” occurred between c. 115,000 – c. 11,700 years ago. Pretty much ALL human development has occurred since the glaciers retreated. During the last Ice Age, glaciers advanced as far south as what is now the state of Missouri. They retreated at a time when human population is estimated to have numbered around 4 million.
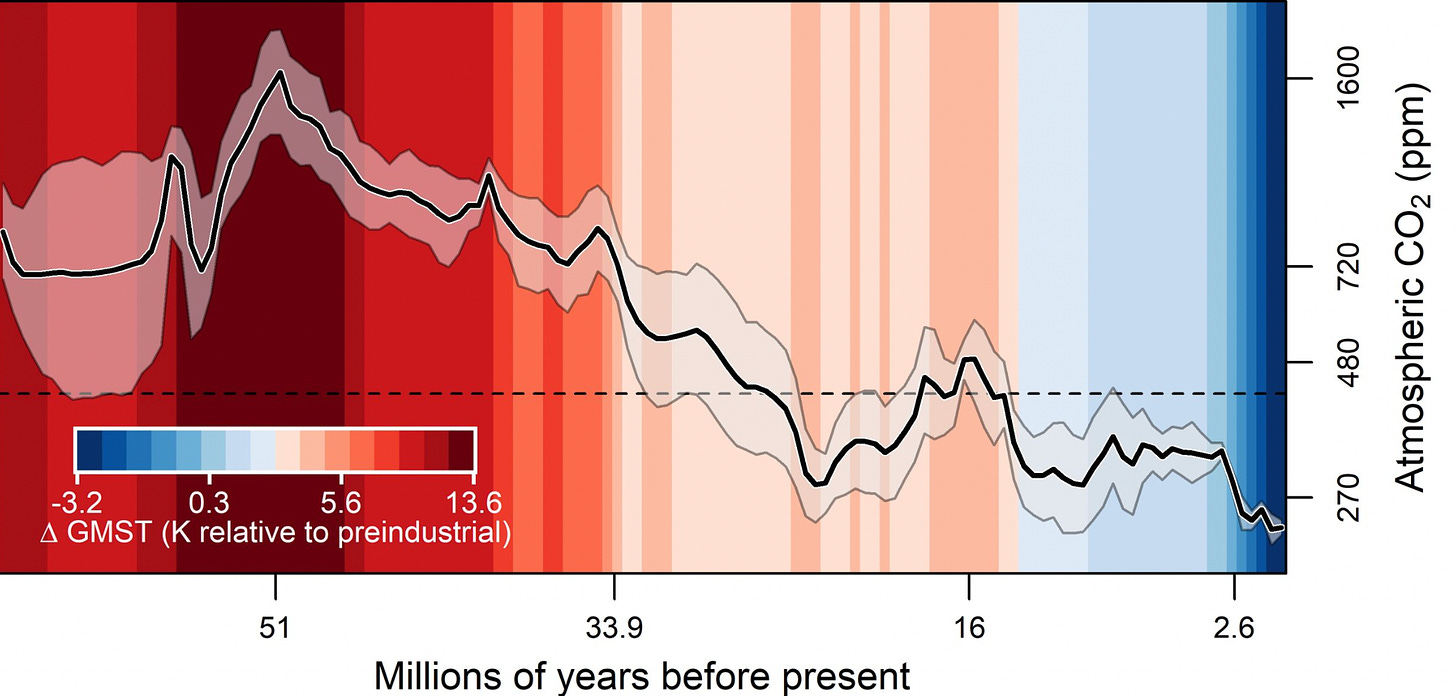
The following chart is a visual representation of successive cooling and warming trends and the associated advance and retreat of glaciers.
The so-called greenhouse gases—carbon dioxide, methane, nitrous oxide and ozone—comprise 0.04 percent of the earth’s atmosphere. Even scientists who pay lip service to the human induced global warming theory acknowledge that for most of the last 66 million years, CO2 levels in the earth’s atmosphere were much higher than they are today.
In the 1970s, climatologists were concerned that modern man would soon experience another cooling trend, resulting in yet another glacial advance that would bulldoze the cities of Canada and much of the United States. In the eighties, the theory of global warming—induced by human greenhouse gas emissions—became fashionable. What really ignited this intellectual, social, and political trend was the discovery that billions of public funds could be funneled into “renewable energy” industries through the mechanism of subsidies and tax credits.
This morning I stumbled across a notable investigative report titled Secret Partnership Fueling Climate Hawk Journalism. Note that many of the foundations that are key players in the Bio-Pharmaceutical Complex are also key players in the Climate-Industrial Complex.
Cracks are forming in the World Health Organisation’s plans to secure a vast expansion of its powers and resources. Presented as a necessarily urgent response to the empirically unsupported assertion that pandemics are increasing in frequency and severity, negotiations for a broad package of amendments to the International Health Regulations (IHR) and a new parallel Pandemic Treaty had been expected to be over by the end of 2023. Having missed that deadline, in late January the Director-General Tedros Adhanom Ghebreyesus pleaded for WHO member states to give ground so that the negotiations could be completed at all. In the same comments he sought to apportion blame for the unexpected headwinds on those who had misconstrued, or misrepresented, the benign intentions of the WHO and its key supporters (which include China and some wealthy private organisations).
Reading between the lines, it appears that Mr. Ghebreyesus and his supporters may finally have realised that the game could soon be up: the strength of opposition to the ambitions of this unelected technocratic administration has compounded rapidly in recent weeks. That opposition has become more evident not only in smaller less influential countries, but in countries which are major contributors to the WHO. Significantly this has included groups of politicians in the U.K. and the U.S. who are seriously alarmed by the vision of a WHO-centred ‘command and control’ public health system, and by the constitutional and public spending implications of these two proposed international agreements.
The Director-General has perhaps realised that his blind ambition has not only put at risk the negotiations that might have elevated his unelected advisory organisation to the status of a supra-national rule-making authority, but is also now starting to jeopardise the future status, funding and membership of the WHO.
Secrecy, opacity and delay
The original timeline presented by the WHO had envisaged a final text of the proposed IHR amendments – where many of the most contentious proposals reside – being published before January 27th 2024, with a view to their adoption taking place at the World Health Assembly meeting scheduled from May 27th to June 1st 2024, alongside adoption of the proposed new Pandemic Treaty. That timeline, although tight, would have allowed four months for negotiators to brief domestic stakeholders, for national legislatures to debate the combined proposals and for any necessary pre-adoption formalities (approvals, technical scrutiny, cost/benefit analyses, etc.) to be completed prior to a vote at the WHA meeting in May.
Yet, on its own initiative, in October 2023 the Working Group for the negotiation of the IHR amendments unilaterally moved its own goalposts so that in place of publishing a final draft text to be scrutinised well in advance of that WHA meeting, it instead committed to circulate by the end of January a copy of the original set of proposed amendments and an interim ‘working draft’ text showing the current state of play. Negotiations would then continue between February and April 2024. It was – and remains – ambiguous whether this move was compatible with the procedural legal requirements already enshrined in the International Health Regulations, but perhaps member states quietly agreed with the WHO secretariat not to look too hard at that issue.
Notwithstanding this commitment, no interim working draft of the IHR amendments appears yet to have been published, and the U.K. officials involved in the negotiations have been inexplicably reluctant to reveal the current position of the text. Indeed, to date all demands for transparency by U.K. parliamentarians have been ignored or deflected by the ministers responsible for the U.K.’s relationship with the WHO. Astonishingly the U.K. Government has refused even to confirm who is negotiating on the U.K.’s behalf.
We understand that the IHR Working Group anticipates a final text being settled only during April or possibly even into May, but there remains no official deadline for it to publish that final text. It refuses to confirm what the documents say, and it refuses to say when it will reveal those documents. If any further evidence were needed of the disregard and disrespect for democratic process and the sovereignty of national parliaments now alleged of the WHO, then surely this is it.
Out of time
That corrosive secrecy, opacity and delay has left a vanishingly narrow window for domestic public health organisations and parliamentarians to review or comment meaningfully on what may become generationally-significant changes to the U.K.’s relationship with the WHO, with other countries and with the public health business community. It means Parliament will have scant opportunity to scrutinise the IHR amendments and the new international funding and resource-sharing commitments enshrined in the parallel Pandemic Treaty. Yet these are documents with the potential to impact materially on the U.K.’s ability to act autonomously, on freedom of speech and opinion, on health security and on the nature of U.K. democracy itself. They also have the potential to commit future generations to very significant public spending obligations.
Given their significance, the IHR proposals and the parallel Pandemic Treaty require a commensurate degree of examination by Parliament. The current nature of the WHO’s funding, 85% of which now comes from private commercially-interested organisations, creates an additional imperative for rigorous, investigative scrutiny. In November 2023, Human Rights Watch wrote that:
The draft [treaty] reflects a process disproportionately guided by corporate demands and the policy positions of high-income governments seeking to protect the power of private actors in health including the pharmaceutical industry.
Without sight of any working drafts of the revised IHRs, nor of the current state of the draft treaty, scrutiny is completely frustrated. At this late stage in the process, after repetitive calls for transparency seemingly have been ignored, one is left to wonder whether this is precisely the intent of the officials involved.
Deferral is the rational solution
As the window for full, fair, candid appraisal by national democratically-elected legislatures is now all but shut, the logical and necessary solution is for member states to demand that any vote to adopt either of these two international accords is held over to the next WHA meeting in May 2025. This will allow ample time both for the conclusion of the negotiations and for member state-level scrutiny of the proposals served up by the negotiating teams.
If it is truly the case that the WHO and its member officials do not intend for national legislatures to cede rule-making sovereignty to an enlarged WHO technocracy, they will surely accept the need for state-level legislatures to control the timing of this process. Calls for deferral have begun, but more voices will be needed to press relevant political leaders and officials to accept that deferral is the only legitimate response to this situation.
A turning point
Even now, in the face of a chorus of rational legally-grounded concerns raised by U.K. parliamentarians about the substance of the proposed amendments and the opacity of the negotiations, the Government has remained steadfastly unwilling to comment on its negotiating intent and objectives, beyond vague platitudes. Efforts by members of the public, legal experts and parliamentarians to understand the current state of negotiations, and even just the arrangements within the U.K. Government to conduct the negotiations, have been stonewalled. The WHO equally has remained virtually mute and offered no meaningful evidence to support claims that its ambitions have been misunderstood.
This has served only to fuel distrust in this process, in the Government and its senior officials, in the U.K.’s relationship with the WHO, and in the WHO’s relationship with its influential funding providers.
Behaviour of this overtly undemocratic nature indicates that the WHO project has long since lost sight of its noble foundations in post-war benevolent multilateralism, and indeed of its reason for being: health for all in pursuit of global peace and security. Unfortunately, the WHO is now a symbol of all that is wrong with what has become a system of global public health patronage. This shamelessly undemocratic and chaotic power grab is also indicative of an organisation which has reached the end of its useful life, at least in its current guise. We suggest that this sorry episode should become the impetus for the U.K. to revisit its relationship with the WHO, and the relationship of the WHO with its funding providers.
The U.K. will not be an outlier if it does so, but rather a role model and – judging by the breadth and strength of international expressions of antipathy for the WHO’s ambitions – a leader of fast followers. This may well be the U.K.’s best post-Brexit opportunity to be an actor of global significance on the international stage.
Molly Kingsley is a founder and Ben Kingsley is the Head of Legal Affairs at children’s rights campaign group UsForThem. Find UsForThem on Substack. Ben and Molly’s new book (co-authored with Arabella Skinner) The Accountability Deficitis available now at Amazon and other book stores.
A German research institute has terminated the contract of a pro-Palestine professor of anthropology after criticizing the Israeli regime’s ongoing war on the Gaza Strip.
The Max Planck Society said they had severed their relationship with “highly acclaimed” academic Ghassan Hage over a set of social media posts that they said were “incompatible” with the society’s values, media reported this week.
The leading German research institution added that “racism, Islamophobia, anti-Semitism, discrimination, hatred, and agitation have no place in the Max Planck Society.”
The Lebanese-Australian Melbourne University professor, who had posted a series of pro-Palestine posts on social media condemning the Israeli regime forces’ months-long genocidal war on Palestinians in Gaza, criticized the Max Planck Institute for its decision to sever its ties with him over his support for peace.
He said he could live with being characterized as having “incompatible values” with the German institution; however, “implying that I am a racist, I cannot accept.”
Since the Israeli regime launched the genocidal war on Gaza in early October, Germany has seen an escalating crackdown on pro-Palestinian advocacy, with rallies and Palestinian flags banned in many parts of the country.
Events and rallies where pro-Palestinian speeches were held have been banned in schools, and the traditional keffiyeh scarfs are also barred.
Samidoun, a group that advocates for Palestinian prisoners, was banned in the immediate aftermath of the 7 October attack.
Pro-Palestinian voices have also been widely silenced with cultural institutions reporting pressure to cancel events featuring groups critical of Israel.
The Frankfurt Book Fair canceled a planned award ceremony for the Palestinian author Adania Shibli in October.
Oyoun Cultural Institution’s state funding was cut in November after hosting an event for a Jewish-led organization that supported the BDS movement against Israel, a movement that Germany’s Bundestag classified as anti-Semitic in 2019.
Also, pro-Palestine British playwright, Caryl Churchill, was stripped on October 31 of the European Drama Prize she had received in April in recognition of her life’s work, over her support for Palestine.
Here is the text of the expert report on Mann v. Simberg/Steyn in 2020 that I prepared at the request of Mark Steyn’s counsel.
My report, along with all other expert reports from both sides except for Abraham Wyner, were not admitted into evidence.
In my opinion, my report provides some much needed context for the trial. Here is a formatted pdf of my complete expert report [Curry Steyn Mann]
Report of Judith Curry, Ph. D.
I submit this report under D.C. Superior Court Civil Rule 26(a)(2)(B) & (C) as both fact and expert witness to address the subject matter on which I expect to present evidence and to summarize the facts and opinions on which I expect to testify. This report includes my observations and opinions as a lay and expert witness concerning three principal topics: (I) the nature of the scientific and public controversy concerning the Hockey Stick graph; (II) whether the Hockey Stick graph can be regarded as ‘fraudulent’; and (III) Michael Mann’s role in the downward spiral of climate science discourse. I present sections (I) and (III) mostly in my capacity as a fact/lay opinion witness and section (II) in my capacity as an expert witness.
SUMMARY
This report addresses the issue of whether it is reasonable to refer to the Hockey Stick graph as ‘fraudulent’ in the course of the public debate on climate change.
What is the nature of the scientific and public controversy concerning the Hockey Stick?
It is my opinion that the Hockey Stick has generated a dynamic and heated debate about its significance and its flaws. Since its publication, Mann’s Hockey Stick has been the subject of intense and often polemical comment and argument in: (a) peer-reviewed, scientific publications critical of the Hockey Stick; (b) analyses of the science behind the Hockey Stick on technical climate blogs; (c) published books on the Hockey Stick controversy; (d) articles by leading science journalists in the mainstream media; (e) online encyclopedia entries on the ‘Hockey Stick Controversy’; (f) Congressional hearings and investigations related to the Hockey Stick; and (e) the personal controversy surrounding Michael Mann in his efforts to defend the Hockey Stick and to thwart his critics.
2. Is it reasonable to regard the Hockey Stick as ‘fraudulent’?
It is my opinion that it is reasonable to have referred to the Hockey Stick in 2012 as ‘fraudulent,’ in the sense that aspects of it are deceptive and misleading:
Image falsification: Mann’s efforts to conceal the so-called “divergence problem” by deleting downward-trending post-1960 data and also by splicing earlier proxy data with later instrumental data is consistent with most standards of image fraud.
Cherry picking: Evidence shows that Mann engaged in selective data cherry picking to create the Hockey Stick, and that this cherry picking contributes to the perception of a “fraudulent” Hockey Stick by journalists, the public and scientists from other fields.
Data falsification (the ‘upside-down’ Tiljander proxy): Substantial evidence shows that Mann inverted data from the Tiljander proxies in a version of the Hockey Stick published in 2008. Mann did not acknowledge his mistaken interpretation of data. Even after published identification of the mistake, this mistake has propagated through subsequent literature including the IPCC 4th Assessment Report.
3. What is Mann’s role in the downward spiral of climate science discourse?
It is my opinion that the scientific discourse surrounding climate change in general, and the Hockey Stick in particular, has deteriorated in civility and professionalism, and that Mann has played a significant and active role in this corrosion and unprofessional degradation of tone. Mann’s approach to public discourse about his work and broader topics in climate change has contributed much to the hostility and animosity that characterize and mark these exchanges. My opinionis based on: (a) the norms of science and scientific discourse; (b) Mann’s withholding of data from his peers; (c) Mann’s efforts to stifle skepticism; and (d) Mann’s attacks on scientists who disagree with him.
THE SCIENTIFIC AND PUBLIC CONTROVERSY SURROUNDING THE HOCKEY STICK
The Hockey Stick is a graph of global temperatures for the last 600 to 1000 years, reconstructed from tree rings and other so-called proxy data. Its name comes from its shape – a long flat ‘handle’ representing comparatively stable temperatures in earlier centuries, followed by a dramatic uptick – the ‘blade’. The Hockey Stick graph was originally published in two papers co-authored by Michael Mann, Raymond Bradley, and Malcolm Hughes (MBH98, MBH99)[1]. MBH98 included a 600-year reconstruction and MBH99 included a 1000-year reconstruction.
Although Mann had only recently received his Ph.D., he was named as a lead author for a chapter in the Intergovernmental Panel on Climate Change (IPCC) Third Assessment Report (TAR), published in 2001. The Hockey Stick graph appeared seven times in the IPCC TAR, and appeared as the backdrop in the IPCC press conference announcing the findings of the report. Rather than displaying all of the long-term temperature reconstructions considered by the IPCC TAR, the opening figure of the Working Group 1 Summary for Policymakers highlighted a graph of temperature reconstructions based only on the MBH99 paper.
Following the public release of the IPCC TAR, the Hockey Stick was regarded as central to the IPCC’s case for global warming. The Hockey Stick was, for a time, arguably the most important graph in the world. Its message of unprecedented warmth at the end of the twentieth century was a vital part of the campaign to persuade the public that mankind had changed the world’s climate.
Since publication of the Hockey Stick in Mann’s paleoclimate reconstructions of temperatures (MBH98/99) and its prominence in the IPCC Third Assessment Report (TAR; 2001)[2], there has been substantial scientific controversy over the methods that Mann and his co-authors used in this research. The controversy extends to the results of their analysis, which contradicted existing geological and historical knowledge of the Medieval Warm Period and the Little Ice Age.
Of particular note are two papers published by McIntyre and McKitrick in 2005 that challenged the MBH98/99 analyses (section IIA). These papers motivated two Congressional investigations and hearings in 2006 (section IIE).
In November 2009, the unauthorized release of emails from the Climatic Research Unit at the University of East Anglia (UK) (“Climategate”) revealed that several scientists (including Mann) had evaded Freedom of Information Act requests for data, manipulated the peer review process, downplayed uncertainty about their research and attempted to squash disagreement and dissent from ‘skeptics.’ The publicity surrounding Climategate (Sections IIB, IIC) brought the Hockey Stick controversy back into the public debate on climate change, largely vindicating a range of concerns that had been raised by McIntyre and McKitrick.
The analysis presented in this section documents the controversy surrounding the Hockey Stick, without passing judgment on the merits (or not) of the original research or the criticisms.
As an active participant in the debate over climate change and the Hockey Stick, I recall the development of this debate.
I summarize this controversy by considering the following sources:
Scientific journal publications critical of the Hockey Stick
Critical analyses in technical climate blogs
Published books on the Hockey Stick controversy
Articles by leading science journalists in the mainstream media
Online encyclopedia entries on the ‘Hockey Stick Controversy’
Congressional Hearings and investigations related to the Hockey Stick
Yesterday, a jury in Washington, DC awarded renowned climate scientist Michael E. Mann more than $1,000,000 in damages in a defamation lawsuit he brought against two bloggers.1 I was a witness in the case and testified on Tuesday.2 Here, I’ll offer my thoughts on the case and some personal reflections on my experience.
Mann’s case alleged that he was defamed by statements made the bloggers more than a decade ago, which harmed his reputation and career (I won’t rehash the details here, but you can get a full accounting of the trial at this comprehensive podcast).3
The defense built their case around making three points to the jury.
One was to bring in experts to testify that Mann’s methods in producing the so-called “Hockey Stick” graph were manipulative, and thus critics of the Hockey Stick were factually correct in saying so. The second point was to demonstrate that the debate over climate during the time that the blog posts were written was intense and vitriolic, with Mann saying things about others that were worse than what the defendants said about him.4 Finally, the defense argued that Mann hardly put on a case — he provided no evidence or witnesses supporting his claims of damage to reputation or career.
In contrast, the prosecution was — in the words of the court, “disjointed” — and was reprimanded on multiple occasions by the judge, most notably for knowingly providing false information to the jury on alleged damages suffered by Mann.5 When I was cross-examined, Mann’s lawyer had considerable trouble getting basic facts right like timelines and who said what.6
Even so, in a trial that most neutral observers would surely see as favoring the arguments of the defense, Mann walked away with a resounding, comprehensive victory.7 How did that happen?
In my view, there were two absolutely pivotal moments in the trial.
One occurred when Mann was testifying and he explained that he felt that the bloggers were not just criticizing him, but they were attacking all of climate science, and he could not let that stand. As the world’s most accomplished and famous climate scientist, Mann intimated that he was simply the embodiment of all of climate science.
For the jury, this set up the notion that this trial was not really about Mann, but about attacks on all of climate science from climate deniers.
The second pivotal moment occurred when in closing arguments Mann’s lawyer asked the jury to send a message to right-wing science deniers and Trump supporters with a large punitive damage award.
Here is how an advocacy group called “DeSmog” accurately reported these dynamics:
Mann sued Simberg and Steyn for defamation, but the trial proved to be about much more than statements that harmed the scientist’s reputation — the entire field and validity of climate science was under scrutiny.
In closing arguments, Mann’s lawyer John Williams compared the climate deniers in this case to election deniers overall. “Why do Trumpers continue to deny that he won the election?” he asked the jury. “Because they truly believe what they say or because they want to further their agenda?”
He asked the jury to consider the same question about Steyn and Simberg: Did they believe what they wrote was the truth, or did they just want to push their agenda? . . .
“Michael Mann is tired of being attacked,” Williams told the jury. “You have the opportunity to serve as an example to prevent others from acting in a similar way” to Simberg and Steyn.
An underlying current throughout this trial has been that climate denialism, like what the two defendants practice, isn’t really about the science. It’s more about politics and policy that drives organizations and individuals to “attack the science and confuse the public . . .
This framing — climate deniers versus climate science — has also characterized mainstream media coverage. For instance, The Washington Post announced, on the day that the case went to the jury, that this case was part of a “mounting campaign” against “right-wing trolls” (below).
Prominent climate scientist or right-wing trolls? Which side are you on?
The case was formally about defamation, but in reality it was not at all about defamation.
As Michael Mann stated after the verdict, the case was really about politics and ideology:
Take a victory lap, Dr. Mann
This is about the defense of science against scurrilous attacks, and dishonest efforts to undermine scientists who are just trying to do our job … whose findings might prove inconvenient to certain ideologically driven individuals and outlets. It’s about the integrity of the science and making sure that bad actors aren’t allowed to make false and defamatory statements about scientists in their effort to advance an agenda.
The defense made a big mistake in thinking that it would be sufficient to win by proving their case while Mann chose not to put one on. That was wrong.
There is no equivalence here between the “renowned” Michael Mann and the “right-wing trolls” who deny climate science and support Donald Trump. The case, at least in this particular venue, was simply unwinnable no matter what cases were put on by the prosecution and the defense. Mann simply had to show up.
The fact that the jury awarded him only $2 in actual damages and $1,001,000 in punitive damages (send a message!) supports this interpretation — The defense won on merits, and Mann won on the framing and the politics.
What does the case mean for discourse about politically contentious issues that involve science? Science magazine reports that it means that we now need to be circumspect in how we engage these issues:
In a statement, Mann said, “I hope this verdict sends a message that falsely attacking climate scientists is not protected speech.”8
At the same time, the ruling could end up having a chilling effect on necessary public criticism of science, says Gene Policinski, a senior fellow at the Freedom Forum, a nonpartisan foundation focused on First Amendment protections. People will need “to be more judicious in commentary. They might be more vague or circumspect.” And that could be to the detriment of the public, he says. “It’s important in today’s world for people to be aware of research that’s going on and having people both praise and criticize it openly.”
For Mann’s part, he signals that he is just getting started in his legal campaign against his opponents:
Asked about Competitive Enterprise Institute and National Review, [Mann’s lawyer] John Williams said, “They’re next.”
I would not be surprised to now see a flurry of lawsuits against people who have been critical of climate science or climate scientists. Such legal action may not be limited to climate — debate over Covid-19 also presents a target-rich environment for unwanted speech to silence. Watch this space.
Finally, let me offer some personal reflections on my experiences.
Form the start, my view was that this entire lawsuit was unnecessary and a waste of everyone’s time. People who I still would not recognize on the street said some mean things about Michael Mann on the internet. Welcome to public discourse in the 21st century. People say mean, false things about me on the internet every day — it goes with the many privileges of having outsized impact and voice. The case was never about the integrity of science or the political impact of right-wing trolls — it was always about Michael Mann.
As I stood in line with dozens of other people on Tuesday waiting to go through security to enter the courthouse, I wondered how we got here — how leading scientists and institutions of climate science became totally consumed with a battle against minor bloggers and political boogeymen.
When I entered the courtroom, I had a profound sense of sadness for Mann. He was alone with his lawyer — no family, no friends, no university officials, no adoring fans, no mainstream media. Totally alone. There were just a handful of observers in the room. As I said at the trial, Mann has not been the best colleague to me, but I am fine even so. Who knows what demons haunt him and why he behaves the way that he does. I do hope he can find peace at some point.
The larger issues here are not about Mann, but rather the continued failures within the climate science community to uphold fundamental norms of conduct among its own ranks. For instance, in the trial we learned that Penn State’s committee looking into Mann’s conduct following Climategate wanted to censure him for his behavior — apparently that was overturned upon the intervention of the Penn State president. There have been so many similar opportunities for leaders to take the off-ramp from escalated conflict and politicization, and the community instead chose to further conflict.
Like I said, it is just sad. And it is not over yet.
Research into vaccines for Staphylococcus aureus (S. aureus), the most common type of staph infection, has led to experimental vaccines that protect mice but fail in humans. A paper published Jan. 16 in Cell Reports Medicine explained why.
When a person first encounters staph, the bacterium fools the human immune system into releasing ineffective antibodies instead of the neutralizing antibodies typically associated with robust immunity. That “trick” allows S. aureus to colonize us, usually harmlessly.
When a colonized person’s immune system is later challenged with a staph vaccine it does not make new, effective antibodies. Instead, it calls up more of the same ineffective antibodies that allowed the bug to colonize the individual in the first place.
Vaccine developers have tried at least three different approaches to S. aureus vaccination but all were met with the same issue.
The immune system is willing …
S. aureus is one of 30 Staphylococcus species in nature and 11 that colonize humans as part of the human microbiome. It is found in the nostrils, skin and other reservoirs in healthy people and is only dangerous when it enters the bloodstream, particularly in immunocompromised individuals.
The human immune system makes antibodies against S. aureus as it does against other microbial invaders. But instead of neutralizing antibodies that fight colonization and infection, S. aureus tricks the immune system into producing ineffective antibodies that allow the bug to continue colonizing us.
When the colonized person is challenged with either S. aureus infection or vaccination, these dummy antibodies reemerge in force but do nothing to help the patient. Vaccination amplifies this effect — which is why S. aureus infections must be treated with antibiotics.
Vaccination “only works when the initial immune response to that pathogen was actually protective,” said J.R. Caldera, Ph.D., a co-author of the paper, in a news release.
Since 80% of staph infections are caused by the invasion of the same strain colonizing the individual’s nose or skin, their “initial immune response” was not protective so subsequent responses will not be either.
“What sets SA [Staphylococcus aureus] apart is that the bacteria themselves have ways of evading the immune system from the moment they encounter us, and these evasive strategies are only reinforced by vaccination,” Caldera said.
… but the antibodies are weak
Anti-staph vaccines generate strong immune responses to vaccination and infection but those responses are directed toward bacterial features that S. aureus uses to fool its host into accepting peaceful coexistence.
This is a case of vaccine-induced immune system priming or “original antigenic sin” — the process by which a vaccine locks in the response vaccinated people make when confronted with the pathogen.
This failure eventually led vaccine researchers down another dark alley, toward vaccines targeting the S. aureus toxin instead of the bacterium. So-called “toxoid” strategies are the basis of tetanus, diphtheria and DTP vaccines.
But “remarkably, both active [vaccine-based] and passive [antibody-based] platforms of immunization against SA toxins were also met with failures,” said senior author George Liu M.D., Ph.D., professor of pediatrics at the University of California San Diego School of Medicine.
For example, a 2021 AstraZeneca-funded study of suvratoxumab, a monoclonal antibody targeting the S. aureus toxin, found that progression to pneumonia in staph-infected patients was no lower in treated than in untreated subjects.
Most pathogens, especially bacteria, are complex organisms carrying several different antigens. Vaccine developers usually target the most prominent antigen to trigger the strongest, most relevant immune response.
On that basis, Liu considered a third possible S. aureus vaccine strategy: targeting minor cell wall antigens on S. aureus instead of its toxins or the main antigen.
This approach would tend to induce weaker immune responses requiring high vaccine or adjuvant doses, but it fell short as well.
Antibiotic resistance leads to ‘super-bugs’
Nostrils are the main staph reservoir in humans and a significant source of infection, but the bug also colonizes the skin, perineum, vagina, throat and gastrointestinal tract.
Staph infections occur when the bacteria enter the bloodstream, joints, heart or skin, usually when the person’s immune system is weakened. Standard antibiotics usually cure staph infections.
However, over the past 70 years, bacteria that colonize humans have found ways to counter the use or overuse of antibiotics and antimicrobials designed to kill them. Some bacteria have developed resistance to these agents, making antibiotics less effective or completely ineffective.
One type of antibiotic-resistant S. aureus, “methicillin-resistant” S. aureus or “MRSA,” is of particular concern.
The most common MRSA outcome outside of hospitals is a skin infection. But serious cases can lead to pneumonia or other serious organ infections. Untreated MRSA infections can cause sepsis — an extreme, system-wide response to an infection.
Hospitalized patients are more susceptible to severe, life-threatening outcomes since they are exposed to fellow patients’ staph strains as well as the ones they carry. Surgical site infections are a significant source of serious, systemic staph infections.
The negative effects of S. aureus on human health are fairly well understood.
We know staph bacteria colonize us, are tolerated by the immune system and cause disease when they enter the bloodstream or invade the skin. We also know that S. aureus antibody responses do not clear the bacterium or eliminate either colonization or infection.
But the role of S. aureus as part of a normal, healthy microbiome has not been extensively investigated.
A 2022 study on components of the skin microbiome suggested that at least one Staphylococcus species, S. hominis — the bug mostly responsible for body odor — may prevent skin infections.
Another species that mainly colonizes skin, S. epidermis, is both anti-inflammatory and antibacterial.
A 2015 study found that chronic S. aureus infection prevented the development of autoimmune encephalomyelitis in a rat model of multiple sclerosis. Encephalomyelitis is inflammation of the brain and spinal cord. Although infection itself caused some types of inflammatory markers to rise it reduced the severity of nerve cell and central nervous system inflammation.
“SA [S. aureus] has been with humans a long time, so it’s learned how to be part-time symbiont, part-time deadly pathogen,” Liu said. “If we’re going to develop effective vaccines against SA, we need to understand and overcome the strategies it uses to maintain this lifestyle.”
Angelo DePalma, Ph.D., is a science reporter/editor for The Defender.
Speaker 2 [I believe that’s Mark Esser]: Excellent! So, thank you for the introduction, Mark, and it’s really a pleasure to share with all of you a little bit of the journey that the “long-acting antibody” team has taken in 2020, but actually our story begins back in 2017 in the basement of a Quality Inn in Tysons Corner VA at the Defense Department Industry Day [BARDA runs “industry days” on regular basis]. There, I met Col. Matt Hepburn, who is actually the architect of the Pandemic Prevention Program or P3, and the goal of P3 was going from the discovering a novel virus to producing drugs in less than 60 days – something that would normally take 6 years at best. To me that sounded more like science fiction than science, but we signed up in a small and committed team of virologists and molecular biologists and engineers and started working in 2018 on new technologies to discover and manufacture antibodies against viruses.
His statement reminds of something a mediocre prizefighter might say if a mafia boss tells him: “We’ve selected you to win the title from the reigning division champion?”
“Really, I can do that?” he would probably reply.
In this case, the capo (Col. Matt Hepburn) is a leading member of the DoD/HHS Countermeasure Racket that was erected following the passage of the PREP Act in 2005.
The second, highly notable statement was made by AstraZeneca’s CEO, Pascal Soriot:
Thank you, Mark, and congratulations again to you and the team. This long-acting antibodies are quite unique because this is the only combination that potentially will last more than 6 months, up to potentially 12 months and protect people for a long period of time. And for those of you who may not be totally familiar with antibodies, you know, you have to know a number of people cannot be vaccinated, like if you have an immune disease, lupus or some other immune condition… or multiple sclerosis, you cannot be vaccinated. So, there are millions of people in the world that will need the protection that cannot be coming from a vaccine, so the long-acting antibody has the enormous potential.
Soriot clearly understood that the so-called COVID-19 vaccines would, best case scenario, only provide some protection for six months. He also understood that these injections were NOT appropriate for all of humanity, and would pose a serious health risk to people with or at risk of developing auto-immune syndromes.
A concerned reader sent in this letter inviting him for more covid and flu injections, as he was considered a ‘priority’ case:
The fact that the NHS is wasting millions of taxpayer pounds continuing to promote and administer these ineffective and harmful products is symbolic of what the health service has become; another cog in the medical industrial machine, whirring to improve Pharma profits with little or no concern for end-user health. In a service allegedly crushed by lack of resources, why on earth are they still pushing these products on an unsuspecting public?
There is no mention that the injections stop infection;
There is no mention that the injections stop transmission;
They make the dubious claim that injections lead to “less severe illness” without backing up this statement.
They use the misleading statement that ‘seasonal vaccines have proven safety records‘. This is certainly not the case for covid injections as they have not existed long enough and no-one has bothered to collect the data.
It seems that even the NHS has abandoned the mendacious claims originally attached to the ‘Safe and Effectives™’ probably because they know it would open them up to legal action. The propaganda job is complete. For those poor souls still unquestioningly worshipping at the alter of the quasi-religious NHS, a promise of real benefit is now surplus to requirements in the ad campaign. It has seamlessly transformed into an annual ritual to benefit drug companies whilst causing insidious harm to the collective health of the nation. What a clever spell they have cast to make entire populations believe that good health is only achievable by injecting unidentified substances into their body on a seasonal basis. And if they feel awful directly afterwards?It means its working!!
Evil genius.
If anyone can find the time and has received such a letter, the claim of “proven safety records” deserves a Freedom of Information request to “please supply all reports memos papers statistical analyses etc supporting the claim of “proven safety records”. We would love to see the response should one be forthcoming. We won’t hold our breath.
Raoult … has made a great career assailing orthodoxy, in both word and practice. “There’s nothing I like more than blowing up a theory that’s been so nicely established,” he once said. He has a reputation for bluster but also for a certain creativity. He looks where no one else cares to, with methods no one else is using, and finds things.14
A tireless researcher, he has published 2,300 papers and is the most cited microbiologist in Europe. He and his team have discovered 468 species of bacteria—about 1/5 of all those named and described. The bacteria genus Raoultella was named in his honor. He is probably best known as the discoverer of the so-called giant virus, so large it had previously been mistaken for an intracellular bacterium. He has won 13 major awards and is a Commander of the National Order of Merit.
Like Dr. McCullough, Professor Raoult strongly advocated early treatment of COVID-19, and he conducted multiple studies demonstrating the efficacy of hydroxychloroquine combined with azithromycin, especially when administered early. In return for his efforts to save his patients, he has been relentlessly persecuted by France’s official medical establishment in Paris.
Now comes the news that Professor Raoult is calling for a moratorium on COVID-19 vaccines. The following is a translation from his recent, French language post on X:
Propaganda and knowledge. We’re the good guys, but we’re not ignorant! When vaccines were developed against Covid, 3 types of vaccines were proposed: – Traditional vaccines (as quickly available as the others) made in China with the entire inactivated virus. These vaccines have not been authorized in France for reasons that escape me. This type of vaccine, comparable to that against the flu, carries fewer unknown risks and does not fight against a single target of the virus: the Spike. I feared, and this happened, that the mutations of the virus and its respiratory specificity would not provide lasting immunity and that the vaccine would not have a very long duration of protection because I published the first known case of reinfection with covid. The disease being poorly immunizing, the vaccine would not do any better.
The second vaccine (the English one from Astra Zeneca, that from Johnson and Johnson, and the Russian Sputnik) is a vaccine based on a virus (Monkey Adenovirus for Astra Zeneca), transformed by integrating the Spike gene. It doesn’t integrate or replicate. I was the first in France to report an accident of cerebral venous thrombosis, this phenomenon is well described in particular in young women and England stopped its prescription for those under 50, followed by many countries and finally it is no longer used in France. There are millions of expired doses left.
The 3rd group of vaccine (Pfizer, Moderna) consists of the injection of RNA coding for the Spike whose elements have been modified so as not to be eliminated quickly. This vaccine is included in a lipid nanoparticle to be able to enter cells. This vaccine, in addition to the disadvantages common to the others, presented unforeseen side effects: extremely frequent menstrual disorders (now recognized by the CDC) of which no one can say whether they will be associated with consequences on fertility, myocarditis and sometimes fatal pericarditis in young people (mainly boys, now recognized by the CDC) and rare thromboses of the veins (recognized by all scientific authorities).
None of these vaccines had been evaluated for mild or asymptomatic forms and therefore for the prevention of contagion. They could not claim to eradicate a disease which, moreover, was circulating among animals. Vaccination was then only justified in those who were at risk of serious forms (subjects over 65 years of age and fragile subjects (obese, immunocompromised). Now we see that the quality controls on batches of Pfizer vaccines do not appear to meet required standards. There should be no DNA or minute doses due to the risk of introducing it into cells through nanoparticles, because DNA easily enters the nuclei and integrates into the chromosomes like a virus with consequences unknown because lymph node cancers can be the natural consequence (Epstein Barr virus, HTLV virus and Helicobacter pylori). The quantity of DNA in the vaccine doses is much higher than that announced in the samples tested. Each batch of Pfizer should be tested, it is easy in any laboratory to do a DNA PCR to check the quantity. Let those who don’t believe it do so!
Finally, we cannot inject a drug without knowing what it will produce in the body. A very unpleasant surprise published in Nature in December 2023 shows that modified RNAs can produce unknown proteins. This should be explored on a large scale because among the proteins that could be created in this way, one of them is an amyloid which would be released while it is in the natural Spike, coated in a protein and without danger. These free amyloids, which can be produced by vaccines through reading errors, can be the cause of amyloidosis plaques which cause various diseases, including neurological ones. All this is knowledge for the knowers, not opinions for scavengers. Given the demonstration of this phenomenon, the consequence of vaccination must be studied in humans, which has not been done.
At this stage of knowledge, it is reasonable to follow Denmark into a moratorium on Covid vaccination. Indeed, the effectiveness is doubtful because new variants appear which make current vaccines ineffective (millions of doses have been thrown away) and the manufacturing of new vaccines based on current variants will be outdated when they are available because new variants will circulate. Other countries are reaching these conclusions, the “surgeon general” of Florida has called for a total stoppage of the Pfizer vaccine, the attorney general of Texas (Mr. Paxton) has just attacked Pfizer for disinformation and censorship (what a reversal!). American and English parliamentarians question administrative and political leaders about their decisions, where we are surprised to see Fauci, the head of covid management in the USA, saying that social measures (masks, confinement, curfew) do not serve to nothing and B. Johnson apologize for his management in England! Humans are not stupid, covid vaccination rates and Pfizer shares are plummeting. It is time to take up the problem, de-dramatize it and treat the patients, re-evaluating it by competent people. At least ten molecules have shown effectiveness on the disease and do not cost much. This must stop being an opportunity for the industry and become a problem for doctors again!
None of these patients of mine presented with the classic prodrome of relapse that I had always noticed previously, such as severe depression due to bereavement, divorce or bankruptcy. Indeed the only thing I found they had in common was to have had a recent booster mRNA covid vaccine. I phoned around my colleagues not only in the UK but also in Australia to check their experience. In no case did they deny such a link. Indeed, they were equally alarmed at the association between booster vaccines and relapse that they too were witnessing, as well an increase in new cancers, particularly in those below 50 years old. In addition to melanoma these colleagues were also very concerned about a sudden big increase in young patients with colorectal cancer.
Rather than instigating a proper inquiry to investigate this when we raised these concerns, the medical authorities told us all that what we were witnessing was a coincidence, that we had to prove it and above all, not to upset our patients.
Recently the American Cancer Society (ACS) has warned of a surge in new cancer cases in the US this lastyear of over 2million, with many of these cases occurring in younger patients. Indeed, the chief scientific officer of the ACS, William Dahat, announced in addition that cancers were presenting with more aggressive disease and larger tumours at the time of diagnosis, especially in younger patients. Of further interest it noted a difference in the microbiome (the community of micro-organisms such as fungi, bacteria and viruses that exist in a different environment) between patients under 50 compared with those over 50.
This surge mirrors a report from Phinance Technologies of late last year which analysed in detail data from the UK Office for National Statistics (ONS) which showed that disability and deaths in 2021 and 2022 had increased dramatically in all age groups, but especially in the 15-44 age group.
The Lancetalso published an article before Christmas reporting excess deaths post covid pandemic to be up by 11-15 per cent over than expected for under-25s and for between 25-49 year olds. This is in fact the pattern found in many countries that have looked at the data. Germany for example has reported excess deaths rising from 7 per cent in 2020 to 24 per cent in 2023.
What makes this all the more surprising is that negative deaths should be the norm after a pandemic as you cannot die twice!
The link between covid vaccines and myocarditis and early death particularly in the young, highlighted by Peter McCullough and colleagues as well as by Aseem Malhotra here in the UK, is incontestable. Now we have a confirmatory report from the CDC in the US, data that the authorities here have refused to act on so as not to alarm vaccinated patients!
Although it is obvious that these excess deaths are real and are continuing to rise, all we get from our Chief Medical Officer, Sir Chris Whitty, are risible attempts to explain away the increase, such as that it is a result of patients not getting their statins in lockdown (hey, patients under 55 do not get statins routinely!) The situation is no better in the US where Harvard researchers have put the blame on sleep disturbance!
The first obvious candidate is lockdown itself when the National Health Service became the National Covid Service and all screening was cancelled or delayed, resulting in an increase in cancer detection and late presentation. Many negative lifestyle factors almost certainly increased as a result of lockdown, such as a lack of exercise and too much food, especially takeaways.
What very few of these reviews consider is that this rise in excess deaths could be a result of the booster vaccine programme, even it clearly follows the vaccine rollout programme starting in 2021 and increasing in 2022 and 2023.
With regards to the link to cancer, there are numerous reports in the literature of cancers arising within days of the vaccines being administered, especially in the case of lymphomas and leukaemias. There are several reports of PET scan mapped tumours exploding at the site and draining area of covid injections with the advice to inject covid vaccines away from known cancers! Outside my clinical observations, several friends have developed cancer after a totally unnecessary covid booster taken only to facilitate travel.
For a possible association between a booster vaccine and the appearance of cancer we need a plausible scientific causal explanation. Unfortunately for those who still insist that these cases are mere coincidences, there are several compelling ones to choose from:
Firstly, it has been reported that T cell responses are suppressed after the boosters (not the first two injections) and that this is especially marked in some cancer patients.
Secondly, the antibody repertoire switches after the first booster from a protective IgG1 and IgG3 dominant B cell response to a tolerising IgG4 one, made worse by further boosters, as reported in a recent Science Immunology paper. As many cancers are controlled by effective T cell led immunity, the sudden perturbation of this control would clearly explain the development of B cell leukaemia and lymphomas, melanoma renal cell cancers and colorectal ones, all tumours which can respond to immunotherapy.
Another report by Loacker et al in Clin Chem Lab Med shows that mRNA vaccines increase PD-L1 on granulocytes and monocytes, which means they effect the very opposite of what the immunotherapy agents do against these tumours, and whichin turn explains why many of these tumours appear to be resistant to this otherwise effective therapy. Taken together, the effect on the immune response of these boosters can easily explain the relapses and so-called turbo-charged cancers appearing.
Other reports document the presence of DNA plasmids and SV 40 (a known cancer-inducing gene) sequences, as well as the ability of mRNA to bind to important suppressor genes. Although this is controversial and has been challenged, it has led to the realisation of significant batch-to-batch variation that could enhance the cancer process yet probably not manifest itself for a few years. The very possibility that we could be sitting on a vaccine-inducing cancer time bomb means that we must never again get involved into a mass vaccine programme for another possible Disease X.
But unless the government wakes up to this now, we will be at the mercy of the World Health Organization doing the very same thing when they decide to release the Disease X virus in order to take back control and destroy our lives all over again.
After a nearly four-year delay, federal Judge Edward Chen on Wednesday heard opening statements in a lawsuit seeking to compel the U.S. Environmental Protection Agency (EPA) to prohibit water fluoridation in the U.S. due to fluoride’s toxic effects on children’s developing brains.
Food and Water Watch sued the EPA in 2017 — after the agency denied its petition to end water fluoridation under the Toxic Substances Control Act (TSCA). This week’s trial is the first to challenge the dismissal of such a petition. Other plaintiffs include Fluoride Action Network (FAN), Moms Against Fluoridation and other advocacy groups and individuals.
Fluoride’s neurotoxic effects on children’s brain development were not in dispute during opening statements and in testimony delivered by the plaintiffs’ first expert witness, Dr. Howard Hu, an internist and preventive medicine specialist, with a doctoral degree in epidemiology.
Instead, attorneys for both sides faced off over the question of what level of fluoride in the water supply poses a risk to the developing brain of fetuses and children.
Levels of fluoride found in drinking water in the U.S. are typically 0.7 milligrams per liter (mg/L), which is lower than the 1.5 mg/L levels found to be neurotoxic by the key reports discussed in the trial.
Attorneys for FAN argued that according to the EPA’s own guidelines for chemical risk evaluation — which they allege the EPA is failing to implement — fluoridating water at a dose that is so close to a known hazard level is too risky, especially given that children are exposed to fluoride from other sources in their daily lives.
They also argued the EPA’s failure to follow its own guidelines is unprecedented. The agency bans other regulated toxic chemicals, such as methylene chloride or trichloroethylene at levels much lower than the known hazard level to ensure the chemicals won’t pose a risk to human health.
And, they said, water fluoridation is unnecessary because the benefits to dental health come from the topical application of fluoride, not from its ingestion.
The EPA argued there is no compelling evidence that fluoride is a neurotoxin at the current levels used for fluoridation in the U.S. and that therefore water fluoridation doesn’t pose a risk to children.
Over two hundred million Americans drink fluoridated water, a practice that has been backed by public health officials and dental associations for decades.
If Chen decides fluoride poses an unreasonable risk, the EPA will have to revisit its rules on water fluoridation.
Fluoride regulation ‘long overdue’
Wednesday’s trial was picked after a June 2020 ruling by Chen that placed the trial on hold pending the release of the National Toxicology Program’s (NTP) report on the link between fluoride exposure and neurodevelopment effects.
The report was released in draft form under court order in March 2023, after top public health officials at the U.S. Department of Health and Human Services (HHS) tried for almost a year to block its publication.
The NTP report concluded that fluoride exposure at levels equivalent to 1.5 mg/L is associated with lower IQ in children.
The second phase of the trial is scheduled to take place over nine days at the federal courthouse in San Francisco, with a Zoom feed available for up to 1,000 viewers to watch live.
FAN member Clint Griess told The Defender that fluoride regulation was long overdue, but he had confidence Chen was carefully considering the science. He said:
“This [phase of the trial] is long overdue. We won after the first trial in my opinion. The judge is being extremely cautious. He has recognized, in his own words, that ‘justice delayed is justice denied.’
“Here we are in 2024, and we are still delaying and denying justice to millions of Americans. I’m very glad we are finally here and our lawyers are doing a great job. And I have every confidence that we will be victorious.”
EPA must apply its own guidelines to fluoride
In his opening arguments, the plaintiffs’ attorney Michael Connett told the court it faced an issue of national importance, “whether the widespread addition of fluoride to water presents a risk of neurodevelopmental harm to children, including IQ loss.”
The EPA faced a similar question in the 1970s, he said, when it had to address the question of adding lead to gasoline.
The EPA was in a quandary, he said, because, at the time, there was no clear evidence that lead was damaging at the levels used. But the EPA decided the margin between the hazard level and the exposure level posed too great a risk — leading the agency to outlaw lead in gasoline.
Connett said that properly applying the EPA’s risk assessment framework for existing chemicals under TSCA is at the heart of the decision the court is facing regarding water fluoridation.
During the first part of the trial in 2020, the agency used the wrong standard to assess the evidence, he said, holding the plaintiffs to a burden of proof the EPA had never held anyone else.
Connett said:
“What you see in this trial is the clash of fundamentally different paradigms. On one hand, you have the sort of 70-year-old longstanding approach by the CDC [Centers for Disease Control and Prevention] and dental interests where basically it’s not a risk until you prove beyond a reasonable doubt that 0.7 [mg/L] fluoride water is causing harm, and that’s been their approach.
“But that’s not how the EPA does business. They use risk assessment. And we are in a position where the plaintiffs are the ones explaining how the EPA is supposed to do risk assessment.”
The EPA’s risk assessment framework, he said, begins with determining whether and at what level a chemical poses a hazard through a dose-response analysis. Then it assesses community exposure. The third piece, he said, is that the EPA looks at the margin between the hazard level and exposure level.
Connett said there are two types of risk. The first is when human exposure exceeds the hazard risk, but that is very rare. For example, the EPA didn’t have that type of data when it decided to ban lead in gasoline.
Then, he said, there is inferred risk, where exposure is lower than the hazard level. This scenario focuses on whether that margin between hazard and exposure may put some people at risk. TSCA mandates the EPA protect the most susceptible people from risk, he said.
The EPA typically requires a margin of 30-fold to determine whether something has a risk. However, some are much higher — for example, tetrachloroethylene is banned at levels 89 times lower than the hazard level, and methylene chloride exposure is not allowed at levels 27 times lower.
In this case, he said, rather than inferring risk as it ought to, the EPA is requiring a risk hazard at the exposure level, which for fluoride is 0.7 mg/L.
Connett outlined the evidence the plaintiffs will present. It includes undisputed evidence that fluoride passes through the placenta and gets into the fetal brain. FAN also will present data from animal studies and human studies, including the NTP report at the center of the trial.
“The NTP found that a large number of studies have been published on fluoride and human IQ. In total, they identified 72 human studies, of which 64 found a connection between fluoride and IQ deficiency. Of the 19 highest quality studies, 18 found lowered IQ, a 95% consistency,” he said.
Connett introduced the first witnesses, Hu and Dr. Bruce Lanphear, professor of health sciences at Canada’s Simon Fraser University.
Connett also previewed evidence the EPA would introduce to attempt to show fluoride is not neurotoxic at low levels, namely a study conducted in coastal Spain by Jesus Ibarluzea, Ph.D., and published in 2022 after the NTP finished its systematic review.
That study did not find evidence that fluoride is neurotoxic at low levels. Instead, it found fluoride increased IQ for boys by 15 points — a finding Connett called “implausible.”
Connett told The Defender, “The EPA has never applied the principles of risk assessment to fluoridation and this case is finally getting them to confront the principles on this issue.”
Chen pushed back on EPA during opening comments
In its opening statement, the EPA argued that anything can be toxic at high levels. The agency’s attorney laid out the EPA’s core argument that there is not enough data showing fluoride’s neurotoxicity at low levels present in drinking water and the law requires a “preponderance of evidence” of risk.
He highlighted a line in the NTP report indicating that more studies at lower exposure levels were needed to fully understand the potential associations with neurotoxicity.
Chen paused the remarks to ask the EPA to confirm the NTP report did establish that with moderate confidence that fluoride caused neurotoxicity at 1.5 mg/L, a relatively low level, which the EPA attorney confirmed.
“Do you disagree with the NTP’s use of 1.5 [mg/L as a hazard level]?” Chen asked. The EPA’s lawyer said they did not.
The EPA also argued that TSCA says “must be a preponderance of the evidence that the chemical substance presents an unreasonable risk.”
According to the EPA, studies of fluoride’s neurotoxicity at low levels have mixed findings — some show there are statistically significant adverse effects at low levels and others found there are not.
Given that, EPA’s attorneys argued the data is “too inconsistent” to conclude that low-level fluoride exposure presents an unreasonable risk.
Chen interrupted the opening comments again to ask whether, as the plaintiffs argued, that uncertainty is precisely what should inform the discussion of risk. “If the outcome wasn’t lowered IQ but cancer or death,” he asked, “would that change things?”
The EPA closed by telling the judge that what matters for TSCA is whether 0.7 mg/L presents an unreasonable risk. Chen pushed back again, “Shouldn’t we consider that in context,” he asked, because fluoride exposure occurs through sources other than water?
The EPA named the expert witnesses it will call later in the case, including David Savitz, Ph.D., and the EPA’s Stan Barone.
‘The evidence is quite persuasive’
The first witness, Dr. Howard Hu, an environmental epidemiologist and chair of the Department of Population and Public Health Sciences, Keck School of Medicine, University of Southern California took the stand yesterday to begin the trial’s deep dive into the science.
Hu has authored more than 300 papers in peer-reviewed journals and published several studies on fluoride. He also advises the EPA and collaborates with its scientists on issues related to lead exposure.
In 1993, Hu co-founded the ELEMENT research project, a pregnancy and birth cohort funded by the EPA and the National Institutes of Health and used to study how prenatal exposure to environmental toxins, including lead, mercury and fluoride affects children’s neurodevelopment.
In such cohorts, researchers collect epidemiological data during pregnancy and then from children over their lifetimes to study a variety of health outcomes tied to environmental exposures.
More recently at San Diego, Hu analyzed data on fluoride and neurotoxicity from the MADRES cohort, comprised of Los Angeles County residents, largely Latino. That research is not yet published.
Hu testified about his research, which consistently finds a link between fluoride and lowered IQ in children.
One of his fluoride studies examined the ELEMENT cohort and found that prenatal levels of fluoride that appeared in maternal urine predicted offspring intelligence scores at ages 4 and 12, with IQ levels lower with incremental increases in maternal fluoride levels.
A second paper expanded the analysis of the 2017 paper and made similar findings. Hu said the neurotoxic effects of fluoride were the strongest in the nonverbal domains, which he said is similar to lead.
Hu also addressed other cohort studies that have different findings, such as the MIREC study in Canada or the Danish study referred to as Odense where the research was conducted, which Hu also used in some of his research.
For example, the MIREC study found sex-specific findings whereas the ELEMENT study did not. The Danish cohort study did not find statistically significant toxic effects.
Hu told the court that different sexes and demographics can have different life experiences that can account for different outcomes.
Overall, he said, his research supports the idea that fluoride at current exposure levels in drinking water is toxic.
Hu also discussed his concerns about the Spanish study the EPA is using as a basis to argue fluoride is not toxic at low levels. He testified it did not control for seafood consumption, which creates high levels of fluoride exposure. He testified it did not control for seafood consumption by pregnant mothers, which creates high levels of fluoride exposure and also has been shown to confer IQ benefits, so it could be a confounding factor in an analysis.
He also criticized the EPA’s opening statements. He said the EPA was presenting data as black and white. Epidemiology, he said, is moving away from characterizing things in that way. Even when a study, like the Danish Odense study, is “negative,” as the EPA put it, the data in the study can indicate a more nuanced reality.
On cross-examination, the EPA asked Hu to concede that the Spanish study was well done. Hu agreed but said he had serious reservations about it, which he had previously discussed.
The EPA also challenged the work he did with Grandjean reporting the Danish study. The results of the Danish study, which did not identify neurotoxic effects, were only published in 2023 as part of a “pooled” study where he and his colleagues used the Danish, Mexican and Canadian data to characterize the dose-effect of fluoride exposure, which the EPA’s lawyer implied was a form of selectively reporting results.
Hu told the court combining the studies increased the power of the analysis and the ability of the research to address questions of public health.
After his testimony, Hu told journalist Derrick Broze, “The evidence is quite persuasive that there is a negative impact of fluoride exposure on the neurodevelopment of children.”
Yes, There is an Association Between Higher Fluoride Exposure & Lower IQ in Children
Dr. Hu: "Yes. I would say that, in my view, the evidence is quite persuasive that there is a negative impact of fluoride exposure on the neurodevelopment of children."https://t.co/MMQE2Am3GBpic.twitter.com/oZTXYlkqYb
The Defender is providing daily updates on the landmark trial pitting Fluoride Action Network against the U.S. Environmental Protection Agency taking place in San Francisco, beginning Feb. 1.
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
By Dr. Elias Akleh* | Sabbah Report | May 24, 2010
A build up of heightened tension in the Middle East is escalating in the last few weeks. American and Israeli postures towards Lebanon, Syria, and Iran have become more threatening. Listening to speeches of political leaders one hears talks only about war not peace. Iranians and Israelis are continuously training hard for a possible showdown. Both sides are conducting extensive war games every month. This led Syrians to claim that Israel is preparing for a soon-to-come another war. The Jordanians also are warning that current stalemate of the peace process is an indication of a war breaking out this summer. The Russian President and his army chief hinted, a few months ago, that the US and Israel were planning for an attack on Iran.
Indeed Iran is, as it has been for last few years, the target of most of the threats and accusations of supporting terrorism. Escalating incitement against Iran the American Defense Department sent last month (April) to Congress a report on Iran’s military claiming Iran could develop intercontinental ballistic missiles capable of reaching the US by 2015.
Ignoring the fact that N. Korea, India, Pakistan, and Israel are proven to have nuclear weapons while Iran does not, the US Secretary of State Hillary Clinton chose in her speech, to the nuclear Non-Proliferation Treaty review conference at the UN, to focus on Iran’s alleged nuclear ambitions putting the whole world at risk as she put it. According to Clinton Iran’s acquisition of nuclear weapons, rather than Israel’s more than 200 nuclear bombs, is destabilizing the Middle East. She called on the world’s nations to rally around US efforts to hold Iran, not other nuclear countries, to account.
The accusation that Usama Bin Laden is living comfortably in Iran had received a boost after the broadcast of a documentary called “Feathered Cocaine”. This echoed the June 2003 claims of the Italian newspaper Corre de la Sierra that Bin Laden was in Iran according to some intelligence report, and according to Richard Miniter’s book “Shadow War”. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.








 Aletho News
Aletho News