Australia’s eSafety Commissioner Complains About X Reinstating Censored Accounts
By Didi Rankovic | Reclaim The Net | January 12, 2024
Without considering the possibility that there were perhaps too many of them to begin with – Australia’s eSafety Commissioner is complaining in a new report that X, since the Musk takeover, has fired too many “safety and public policy personnel.”
Another complaint from the commissioner’s “transparency report” is about previously censored accounts getting reinstated on the platform.
The sum of the new policy, according to this Australian office – a government agency that’s “independent (but) supported by the Australian Communications and Media Authority (ACMA)” – is that X is now less capable of “tackling online hate.”
It is no wonder that these accusations are made by eSafety, considering that it has been given powers to deal with what’s described as “cyberbullying, image-based abuse, and illegal and harmful online content.”
Basing the report on information obtained from X, eSafety writes that 80 percent of “safety engineers” have been let go since October 2022 (the same figure applies to global public policy staff). Moderators working for X have fared somewhat better – still, over 50 percent of them have been fired.
Considering that these employees were doing more than simply moderating – there have been many confirmed and very controversial cases on clear censorship against content and accounts – free speech supporters are likely fine to learn these precise numbers for the first time.
However, the Australian eSafety is not, taking a negative stance toward the developments and warning that they have “implications for Australian users.”
Commissioner Julie Inman Grant is quoted in the report as saying that, “It’s almost inevitable that any social media platform will become more toxic and less safe for users if you combine significant reductions to safety and local public policy personnel with thousands of account reinstatements of previously banned users.”
About that last point – we now know that the number of banned accounts that have been allowed back on X is at this point in excess of 6,100. But, the Australian office is not even sure if these figures concern X’s operations globally or just in Australia – although eSafety “understands” the latter to be the case, and draws this understanding from media saying earlier that a total of more than 62,000 accounts have been reinstated.
The commissioner is also displeased with the fact that X did not find it necessary to place “additional scrutiny” on these accounts – banned under previous ownership, and its policies.
Low RSV Vaccine Acceptance Among Pregnant Women
By Peter A. McCullough, MD, MPH | Courageous Discourse | January 10, 2024
Vaccination during the third trimester of pregnancy is unprecedented and risky, since a vaccine induced fever could precipitate stillbirth or premature delivery of the baby. The CDC and the Bio-Pharmaceutical Complex has told young mothers they should take the risk for theoretical protection of the newborn.
As of August 30, 2023, the CDC recommends: “Vaccination for pregnant people, 1 dose of maternal RSV vaccine during weeks 32 through 36 of pregnancy, administered immediately before or during RSV season. Abrysvo is the only RSV vaccine recommended during pregnancy.” Now the CDC is reporting that only Asian women in the US have topped 10% on the respiratory syncytial virus RSV vaccination rate while African American mothers remain the most conservative with under 5% rates of acceptance. For any mass vaccination campaign, these data would indicate a program failure. The mothers and families have been burned by genetic COVID-19 vaccines and unprecedented rates of injury, disability, and death. There is little appetite for a new vaccine during pregnancy among obstetricians, midwives, and expecting mothers.
These data on the lagging maternal RSV immunization campaign indicate that “vaccine mania” may be cooling in the United States. As a consulting internist and cardiologist, I do not recommend the new RSV vaccine for pregnant women. There are insufficient data on short and longer term safety. Theoretical protection of infants for an easily treatable illness is simply not compelling enough to risk the pregnancy altogether.
Censorship Investigation: Jim Jordan Subpoenas Director of National Intelligence Avril Haines
The agency ignored requests to hand over documents
By Dan Frieth | Reclaim The Net | January 12, 2024
House Judiciary Committee Chairman Jim Jordan has issued a subpoena to Director of National Intelligence Avril Haines. This action is part of a wider investigation by the committee into allegations that the federal government has been working in concert with Big Tech companies to suppress certain viewpoints on social media platforms. These allegations raise serious concerns about violations of First Amendment rights.
Chairman Jordan, in his communication to Haines, underscored the gravity of the situation. He cited evidence gathered by the Committee and its Select Subcommittee on the Weaponization of the Federal Government, along with other publicly available information, highlighting the federal government’s involvement in pressuring and collaborating with Big Tech and other intermediaries. This collaboration, as Jordan pointed out, has led to the censorship of specific viewpoints online, in direct opposition to the principles enshrined in the First Amendment.
We obtained a copy of the subpoena cover letter for you here.
He emphasized that the First Amendment explicitly forbids government officials from imposing restrictions on speech based on viewpoint. Moreover, he mentioned the state action doctrine, which prohibits government officials from bypassing constitutional limits by engaging private actors to do what the government itself cannot lawfully do.
“The investigative work performed by the Committee and its Select Subcommittee on the Weaponization of the Federal Government, along with other publicly available information, have revealed how the federal government has pressured and colluded with Big Tech and other intermediaries to censor certain viewpoints on social media in ways that undermine First Amendment principles,” the subpoena reads. “The First Amendment prohibits government officials from imposing viewpoint-based restrictions on speech. State action doctrine prohibits government officials from circumventing constitutional strictures by using private actors—whether through coercion, encouragement, entwinement, or joint participation—to accomplish what the government cannot directly.”
According to a press release from Chairman Jordan, in an ongoing investigation, the ODNI has come under scrutiny for not providing documents requested by the Committee, despite repeated efforts for voluntary cooperation. This is what has sparked the need for a subpoena.
The Committee’s request encompasses records concerning the activities of the ODNI’s Foreign Malign Influence Center, which, according to publicly available information, should be within the scope of their inquiry.
Additionally, the Committee has acquired documents indicating that ODNI personnel were participants in meetings with major social media companies and various federal government agencies. These gatherings, commonly referred to as “USG-Industry Sync” meetings, are of particular interest to the Committee. Despite these revelations, the ODNI has not yet submitted any records related to these meetings or any other related sessions, raising questions about their responsiveness and transparency in this matter.
The Embarrassing Pause In Arctic Sea Ice Loss Has Lasted 17 Years, Defying IPCC, NSIDC Predictions
By Kenneth Richard | No Tricks Zone | January 8, 2024
“[S]ince the dramatical decline of the ice extent in 2007, the summer Arctic sea ice area has not declined further.” – Astrup Jensen, 2023
Scientists have been using the year 2007 as the starting point for assessing Arctic sea ice trends for nearly a decade. A 2015 study published in Nature Climate Change reported a “near-zero trend” in summer sea ice over the 7 years from 2007-2013.

Image Source: Swart et al., 2015 (full paper)
Another 10 years have now passed and there is still no evidence of a further decline in sea ice.
This is interesting because since late 2007 scientists have predicted Arctic sea ice would decline rapidly as CO2 continued rising – from 385 ppm in 2007 to 422 ppm today. There were 20 models referenced by the IPCC (AR4) projecting a 40% loss of sea ice by 2050 due to an allegedly enhance greenhouse effect associated with anthropogenic CO2 emissions.
But a new study reveals there’s been no declining trend in summer sea ice area over the last 17 years, and “no apparent correlation” between CO2 and sea ice trends.
“The Arctic Sea ice extent is measured by satellites and varies by day, month and year, and the yearly minimum ice extent will occur in a day of September month every year. The ice extent is much lower now (2023) than in 1978, when the satellite measurements began. However, it has not been a gradual decline. A major decline happened during the years 1997 – 2007. Before that the decline was minimal and after that period, there was no significant downward trend.”
“These data show that there is no apparent correlation between the variable extent of the Arctic and the Antarctic Sea ice and the gradually increasing CO2-concentrations in the atmosphere as proposed by NSIDC, IPCC and others, also for these areas of cold climate.”
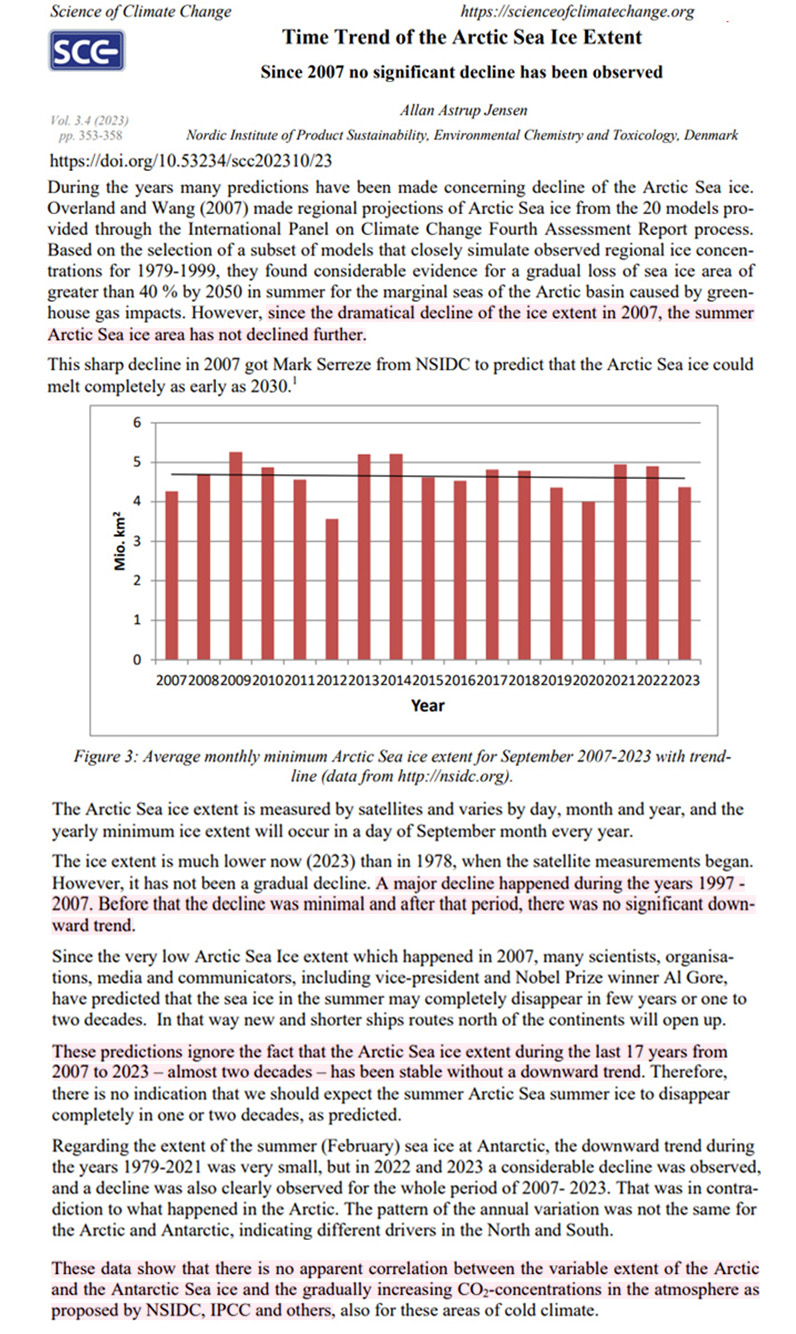
Image Source: Astrup Jensen, 2023
The Definition of Insanity
AARP: “Keep getting boosters even though previous ones didn’t work.”
BY JOHN LEAKE | COURAGEOUS DISCOURSE | JANUARY 9, 2024
This morning someone sent me a link to Alex Berenson’s post about the AARP advising its nearly 38 million members to get another COVID-19 booster shot, even if they have already had five boosters.
This prompted me to visit AARP’s website, which features an entire category of content titled Scams & Fraud—that is, warnings to older people about all the predators out there who wish to manipulate and deceive them in order to steal their money.
Under the category Caregiving is posted an articled titled COVID-19 Nursing Home Deaths Climb Ahead of Expected Winter Surge.
The article laments that nursing home residents and staff have lost interest in getting the latest booster, and suggests this is a likely explanation for why COVID-19 mortality in nursing homes has risen in recent months as we head into winter.
The author, Emily Paulin, does NOT mention the common experience of older people repeatedly falling ill with COVID-19 even after receiving multiple boosters. She also doesn’t mention a word about TREATING nursing home residents who fall ill with COVID-19. Four years after this mess began, an AARP writer about nursing home policy still has nothing to say about treating the illness.
Reading this article reminded me of a Joe Rogan podcast I watched yesterday in which his guest—an earnest and callow young man who says “like” every fourth word—asserts the following two propositions:
1). Most popular sports were conceived and developed to give men an advantage over women. For example, in basketball, “the way the ball moves” gives biological males an advantage.
2). Biological males who receive gender reassignment procedures to become women have NO advantage over women in sports.
The same kind of insanity is also evident among the foreign policy crowd that continues to advocate the war in Ukraine. No matter how many hundreds of thousands of Ukrainians are run into the meat grinder of Russian defensive positions in the eastern part of the country, these lunatics continue to insist that the Ukrainians KEEP DOING THIS until they get their desired result.
All of the above is further evidence of the mental illness underlying what I call the Holy Quadripartitus of Piffle:
1). COVID-19 vaccines are saving mankind. Anyone who questions the safety and efficacy of the vaccines is guilty of heresy.
2). The U.S. proxy war in Ukraine is a sacred mission and NO negotiated settlement with Russia shall be countenanced. Anyone who criticizes the Ukrainian and U.S. governments, and any attempt to understand the war from the Russian point of view, is guilty of heresy. Indeed, as Ukraine’s American, transgender military spokeswoman asserted back in September, journalists who question this article of faith should be hunted down and killed.
3). Human induced climate change will soon destroy the earth if trillions aren’t spent to overhaul our entire energy policy. Anyone who questions this proposition is guilty of heresy.
4). The concept of biological sex is a mere “construct.” Skilled surgeons and endocrinologists can transform a boy into a girl or vice versa. Anyone who questions this assertion is guilty of heresy.
For my part, I have lost all patience with people who subscribe to the Holy Quadripartitus of Piffle. In my view, they have become indistinguishable from sleep-deprived children. There is no sense in trying to have a conversation or reason with them. I can only hope that their insane assertions and conduct will ultimately be rejected by the great majority of adults in the United States and the rest of the world.
CDC study concludes most young children hospitalized for COVID were unvaccinated — after enrolling 7 times as many unvaxed kids in study
By Angelo DePalma, Ph.D. and Karl Jablonowski, Ph.D. | The Defender | January 9, 2024
A U.S. government-sponsored study published late last month in The Pediatric Infectious Disease Journal reported that most young children hospitalized for acute COVID-19 had not received an mRNA COVID-19 vaccination and were sicker to begin with than vaccinated children.
The authors’ conclusions are true on the surface, but their analysis ignored that more than 7 times as many unvaccinated as vaccinated children were enrolled in their study.
Only 4.5% of trial subjects completed primary COVID series
Investigators led by Laura Zambrano, Ph.D., a Centers for Disease Control and Prevention epidemiologist, recruited 597 children ages 8 months through under age 5 hospitalized for COVID-19 at 28 U.S. pediatric hospitals between Sept. 20, 2022, and May 31, 2023.
Unvaccinated subjects outnumbered subjects who had received at least one COVID-19 shot by 528 to 69, a more than 7-fold difference.
Children were grouped by demographic factors such as race, sex and geographic location, vaccination status (no vaccine, incomplete vaccine series or fully vaccinated) and underlying non-COVID-19 illnesses, or comorbidities.
Only 4.5% of the subjects had completed their primary COVID-19 vaccination series and 7% had received at least one dose.
Cases varied widely in severity, with 174 (29.1% of all subjects) admitted to intensive care and 75 progressing to life-threatening illness.
Fifty-one (8.5% of all subjects) required life support via invasive mechanical ventilation, and three required extracorporeal membrane oxygenation, a life-support treatment involving a heart-lung machine.
Based on results from both vaccinated and unvaccinated groups, infants 8 months to under age 2 were more vulnerable to serious outcomes than children ages 2 to 4 years.
For example, the youngest subjects had more life-threatening illnesses and the greatest need for high-level respiratory support involving vasoactive infusions — intravenous treatments to maintain normal blood pressure and heart rate. Yet they also had shorter hospital stays.
Investigators concluded that most children hospitalized for COVID-19, including most children with underlying medical conditions, were unvaccinated. On that basis, they called for “strategies to reduce barriers to vaccine access among young children.”
Researchers tested kids for COVID but not other respiratory infections
Zambrano et al. also compared the Pfizer mRNA shot to the Moderna product. They found that children who took the Moderna product were somewhat more likely to experience a serious outcome, however, the numbers from both groups were small and the authors did not subject them to statistical analysis.
Based on their analysis they also calculated and reported, in their “results” section, that mRNA COVID-19 vaccines were 40% effective in reducing serious outcomes. However, in their discussion (several sections later), they admitted that “vaccine coverage in this population was too low to evaluate vaccine effectiveness.”
There were two notable limitations to the Zambrano study. Even though the researchers recruited children who were only partially vaccinated the study’s design excluded children who had received any vaccination fewer than 14 days before hospital admission. Therefore no short-term post-vaccination adverse events were included.
Another limitation was that children were tested for COVID-19 but not for all possible respiratory infections, meaning “it is possible that RSV [respiratory syncytial virus], human metapneumovirus or other respiratory viral co-detections influenced disease severity.”
Media parroted authors’ conclusions
U.S. media (for example here and here) picked up on the Zambrano paper and repeated its conclusion that most hospitalized COVID-19 pediatric patients were unvaccinated — ignoring that the study included more than 7 times as many unvaccinated as vaccinated subjects.
A deeper dive into the data reveals the extent of this error and the discrepancies between what Zambrano et al. reported and what they saw.
Tables 1 and 2 illustrate what the authors got wrong.

These calculations say nothing about the relative outcomes for vaccinated and unvaccinated children because Zambrano et al. either did not perform the relevant calculation — number of cases in each group divided by the number of subjects — or chose not to report the results it generated.
Instead of presenting the number of subjects experiencing the indicated outcome as a percentage of vaccinated or unvaccinated groups, they reported them as a percentage of all subjects experiencing that outcome. Since there were 7 times as many unvaccinated as vaccinated subjects, this approach all but guaranteed the numbers among the unvaxed would be higher.
Here’s an analogy: In a hypothetical study comparing 10 coffee drinkers to 100 abstainers, five drinkers and 10 abstainers reported feeling nervous. Using Zambrano’s logic, 67% of people feeling nervous were abstainers, and just 33% drank coffee. This “proves,” according to Zambrano’s logic, that not drinking coffee doubles (67% vs. 33%) the risk of getting the jitters.
The correct way to view this data is that 10 in 100 abstainers, or 10%, felt jittery but 5 in 10 (50%) of coffee drinkers felt jittery, and that drinking coffee raises the risk of nervousness fivefold (50% vs. 10%).
Table 2 uses the same raw data as Table 1. But instead of reporting vaccinated and unvaccinated data as a percentage of all data, it first calculates the occurrence of these conditions or outcomes in each group and compares the inter-group differences.

Hospital stays were also on average one day shorter for the unvaccinated. The only area where unvaccinated children faired slightly worse was in underlying cardiac issues, but the authors did not address this small difference in their discussion.
Previous study used same tactic
A study preceding the Zambrano paper by three weeks used the same tactic to arrive at the same conclusion.
Tannis et al. compared many of the same outcomes as Zambrano in 6,337 unvaccinated and 281 vaccinated children ages 6 months to under 5 years.
All subjects had visited emergency departments for acute respiratory illness from July 2022 to September 2023.
By coincidence, Tannis also calculated vaccine effectiveness to be 40%.
Table 3 presents data from Tannis et al. with percentages reported by Tannis (Tannis %) and the actual values (Actual %).

Vaccinated children were also 68.3% more likely to harbor HCoV, an endemic coronavirus, than the unvaccinated. Similar to SARS-CoV-2 (the COVID-19 virus), HCoV can cause serious illness in immunocompromised individuals and the elderly.
Angelo DePalma, Ph.D., is a science reporter/editor for The Defender.
Karl Jablonowski, Ph.D., holds a master’s degree in computer science and a doctorate in biomedical and health informatics. He practices data science by asking questions of databases that can reveal population-based adverse outcomes of medical interventions.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Dr. Mary Kelly Sutton Loses Medical License in New York for Writing Eight Vaccine Exemptions in California

By John-Michael Dumais | The Defender | January 8, 2024
Dr. Mary Kelly Sutton (who goes by “Kelly”) on Oct. 30 lost her license to practice medicine in New York for writing eight vaccine exemptions in California between 2016 and 2018. New York was the third state to enforce this penalty, after Massachusetts and California. Sutton is now no longer able to practice medicine anywhere in the U.S.
Both the New York and Massachusetts medical boards adjudicated Sutton’s case on the basis of “reciprocal discipline,” rubber-stamping the Medical Board of California’s 2021 decision without allowing her to challenge the validity of the original findings.
Reciprocal discipline avoids the time and costs of relitigating. Therefore, like the Massachusetts Board of Medicine hearing last July, the October hearing in New York was just theater and the board never intended to allow Sutton to defend herself.
Instead, the New York board maintained that the purpose of the hearing was limited to determining what penalty should apply to Sutton’s state license in light of the findings already established in California.
Medical Board of California misinterpreted the law
Sutton, an integrative medicine physician practicing since the early 1970s, told The Defender that the Medical Board of California misinterpreted the law when it determined she violated “standards of care” when writing the vaccine exemptions.
Those exemption-specific standards — which came into effect in 2016 via Senate Bill (SB) 277, a California bill that stripped parents of the personal belief exemption for rejecting vaccines for their children — only stated it was up to the physician to decide on a medical exemption based on the needs of the child.
However, in 2019, California passed two more bills — SB 276 and SB 714 — designed to make vaccine exemptions even more difficult to acquire.
Specifically, when a doctor writes more than five medical exemptions per year (as of Jan. 1, 2020) or a school’s immunization rate falls below 95%, the California Department of Public Health (CPDH) has the right to review the medical exemptions.
Physicians since January 2021 are also required to use a standardized electronic exemption form submitted to a statewide database, and CPDH may revoke exemptions that do not conform to vaccination guidelines established by the Centers for Disease Control and Prevention (CDC) and its Advisory Committee on Immunization Practices (ACIP) and by the American Academy of Pediatrics.
Sutton claimed the Medical Board of California applied its own definition of “standards of care,” in direct contravention to the standard established by SB 277.
“In California, any time a standard of care is written into statutory law, it is more preeminent than a community standard of care that is just held among the general opinion of doctors in practice,” she said.
Sutton believes the Medical Board of California was also applying laws derived from SB 276 and SB 714 that went into effect well after the date she wrote the exemptions.
The CDC’s and ACIP’s vaccine recommendations do not constitute mandates or requirements. According to Sutton, during the lobbying phase of SB 277, a doctor called ACIP and asked whether its recommendations should be considered mandates, and was told that they were only guidelines.
The ACIP guidelines do not mention the word “exemption,” according to Sutton, nor were the guidelines mentioned in SB 277.
“That’s the way guidelines have always been used in standards of care,” Sutton said, calling them “indicators, supports, references — but not mandates.”
Sutton said the mood of medicine is shifting away from a doctor exercising his or her own training and experienced judgment towards doing what the standards and guidelines say.
“This is decidedly against the quality of medicine because there’s no freedom to individualize for the patient,” she said.
Dissecting the California case
The California board revoked Sutton’s license for “gross negligence” and “repeated negligent acts” in issuing permanent vaccine exemptions for eight pediatric patients, saying the exemptions did not comply with standards of care and vaccine guidelines at the time.
The board’s sole expert witness, Dr. Deborah Lehman, infectious disease physician at the University of California, Los Angeles, dismissed Sutton’s claim that SB 277 clearly articulated standards of care regarding exemptions, saying those were not the “community standard of care,” Sutton recounted.
Sutton explained:
“SB 277 was brief and direct to the point. It said that if a child who is required to have vaccines receives a note from a physician stating that it is in the child’s best interests to not be vaccinated, then that suffices to fulfill the requirement and the child can go to school without having the required vaccines. The deciding factor is the physician’s discretion.”
The relevant clause from the bill states:
“If the parent or guardian files with the governing authority a written statement by a licensed physician to the effect that the physical condition of the child is such, or medical circumstances relating to the child are such, that immunization is not considered safe, indicating the specific nature and probable duration of the medical condition or circumstances, including, but not limited to, family medical history, for which the physician does not recommend immunization, that child shall be exempt from the requirements.”
Lehman said doctors must only grant an exemption when there is a contraindication to a vaccine and at no other time.
Lehman claimed the standard of care was determined by whether another physician would treat the medical issue the same or similarly. However, according to Sutton, she omitted the all-important phrase “in the same community.”
In the integrative medicine community in which Sutton practices, it is common for patients to receive more individualized treatments rather than one-size-fits-all approaches.
“It was kind of a force-of-personality situation that was successful in the setting of the courtroom hearing at the administrative level,” Sutton said. “And the board witness prevailed upon the judge to believe that the law had no meaning and that community opinion was higher.”
The California board also questioned Sutton’s decision not to request patients’ medical files or perform physicals in the cases for which she wrote exemptions.
“If I required a physical exam for every vaccine exemption, I could be accused of ‘padding the bill’ because the physical exam contributes nothing to the decision about the risk for a vaccine injury,” Sutton said.
Instead, Sutton’s process was primarily to review patient histories to understand if the child or a family member had suffered a negative reaction to vaccines.
She said:
“From my understanding and from the group of physicians that I worked with at the time — Physicians for Informed Consent — the risk factors for vaccine injury lie completely in the story of what’s happened to the child when they have had vaccines and what has happened to their blood relatives when those people had vaccines.”
After the passage of SB 277, Sutton said there was “a great deal of conversation” among doctors about how the law could be read and interpreted and how exemptions could be constructed rationally based on the scientific literature.
That literature showed several different areas of concern around vaccinations, including “The aluminum contained in vaccines can trigger neurologic issues and autoimmune disease,” Sutton said, adding, “There is the question of regression after vaccines and neurodevelopmental delays such as autism.”
“There’s also a higher risk of allergies, and then there’s the immediate reactions where a person collapses or has a seizure after a vaccine,” she said.
“A doctor has to make an extra effort in order to understand the historical pattern of vaccine reactions that would indicate risk of vaccine injury, or how to diagnose mitochondrial dysfunction,” Sutton said.
During the California hearing, Sutton shared extensive scientific citations supporting her medical decision-making, including research by Dr. Chris Exley on the dangers of aluminum in vaccines.
She told the board that it was neither intelligent nor humane to force a family to continue to vaccinate after one of their children had already died or been injured by a vaccine, and shared her clinical observation that unvaccinated patients are healthier than those who are vaccinated.
The California board also claimed Sutton neglected to provide informed consent to her patients requesting vaccine exemptions.
Sutton was uncertain exactly what the board meant here but surmised it was saying she did not adequately highlight the diseases that could develop if the parents failed to vaccinate their children.
Deeming the real issue with informed consent to be advising patients about the potential harms of vaccination, Sutton said, “I don’t think I repeated the CDC bylines.” Instead, she believed the parents who came to her for exemptions were already “more than aware” of the risks of childhood diseases.
From her point of view, there was already enough vaccine promotion happening with mainstream media and schools “echoing over and over” how “vastly dangerous chickenpox” and the other childhood diseases were.
The California board’s concern about Sutton not requesting previous medical records is based on the notion of “Don’t trust a single word the patient says,” Sutton said, an attitude that necessitates getting “every documentation” about adverse vaccine reactions before making a decision.
“That’s not the way medicine works,” Sutton said. “But that’s what was expected in terms of a medical exemption interview. It’s like building a legal case instead of a medical case.”
Further wrongdoing was implied by the California board in pointing out that a number of the exemptions Sutton wrote were for patients for whom she was not the primary care provider.
“That is implying that the primary care doctor knows the patient best,” Sutton said. “And that is good in a lot of ways, but it can be a problem for the patient if it’s a large practice that has been forbidden to give vaccine exemptions.”
Sutton said that if a patient’s need cannot be addressed by that group, even if it’s their primary care group, then it is akin to patient abandonment.
SB 277, the law in effect during the period Sutton wrote the exemptions, never had a requirement that exemptions be written by the primary care physician, or even by a pediatrician or pediatric infectious disease expert, according to Sutton.
“So their [Medical Board of California’s] statements were beyond the law and that’s what they were enforcing against doctors,” she said.
Although the board improperly focused on laws that went into effect in 2019 and later, Sutton said, “That very argument could not be persuasively made by the attorneys at the time.”
Board expert: ‘Science has been decided’ on vaccine risks
The Medical Board of California conducted a three-day “trial” for Sutton in June 2021 in an administrative court with a single judge and no right to a jury.
Three experts spoke on behalf of Sutton, while Lehman, the board’s single expert, testified against her.
Lehman lacked basic knowledge of vaccine risks and stated that all doctors should follow the CDC’s vaccine schedule.
When asked to quantify the risk of vaccine injuries, Lehman said, “I don’t need to cite articles in my report, because the science has been decided … If you want answers to these questions, I would refer you to the CDC.”
After denying any knowledge of Dr. Peter Aaby’s more than 400 articles on PubMed analyzing vaccine dangers, Lehman characterized the journal as “low impact” and Aaby as “anti-vax.”
Sutton’s witnesses were Dr. Andrew Zimmerman, pediatric neurologist, Dr. James Neuenschwander, family physician with vaccine expertise and Dr. LeTrinh Hoang, integrative medicine pediatrician.
They skillfully articulated the heterodox perspectives on vaccine dangers and referenced a number of recent studies on vaccine adverse effects, while noting the lack of data on vaccine safety or government studies comparing health outcomes for vaccinated versus unvaccinated individuals.
“And on this very little evidence, people like the board expert are proclaiming to the high heavens these are safe and effective,” Sutton said. “All of these other concerns are irrelevant.”
Administrative court structure promotes ‘raw power’
In Sutton’s interactions with California, Massachusetts and New York, she observed a notable lack of due process when compared with civil and criminal courts.
In the proceedings with the Massachusetts board, one of the documents filed against her did not list any specific complaints, making it difficult for Sutton to defend herself. “I had to intuit what they were complaining about and then make up the answers,” she said.
When she brought this shortcoming to the magistrate’s attention, he confirmed that such detail is not required in administrative courts.
“The structure of the administrative-level courts promotes the raw power that’s exercised by the medical boards,” Sutton said, adding, “It’s not an exercise within the law and it doesn’t benefit the people, but only the administrative state itself.”
Sutton mentioned the Federation of State Medical Boards, which coordinates all of the medical boards in the U.S., sent out warnings to doctors about misinformation, masks, vaccines and exemptions related to COVID-19, she said.
“It’s a private, unelected group that’s been around for over 100 years,” she said. “It’s not visibly related to any government entity.”
Together with its partner agency, the International Association of Medical Regulatory Authorities, it forms an integral part of the administrative state that is undermining the doctor-patient relationship and helping to delicense doctors like Sutton.
Sutton said, “They are both in the same building at the same address in Euless, Texas. So there is a centralized organ to control medical boards around the world, which means controlling doctors around the world.”
“The coordination of COVID happened through organizations like that,” she added.
Doctors incentivized to ignore vaccine injuries
Sutton said the financial incentives to vaccinate everyone within a medical practice discourage doctors from connecting adverse health outcomes to the vaccines.
“The Blue Cross Blue Shield Provider Incentive Program manual of 2016 listed a $400 bonus to the doctor for every two-year-old who was on the CDC vaccine schedule on time,” she said, “as long as 63% of the practice was vaccinated.”
“That’s going to influence how you respond to a parent when they say, ‘Johnny had a seizure after the MMR [measles-mumps-rubella] vaccine,’” Sutton said, adding, “Do you put that in the chart as an MMR vaccine reaction? Or do you say, ‘Oh, it must be something else’?”
If a child has a febrile seizure, the doctor may well chalk it up to normal childhood fever rather than to a recent vaccination, Sutton said. “So we bias our own literature, our own notes, by the things that have been allowed in terms of financial incentives.”
Sutton said financial incentives must be removed from medicine to restore its integrity.
“It’s too much impact on physician judgment and motivations are not angelic,” she said. “We’re humans. So if somebody says ‘If you just get 10 kids vaccinated you’ll get $4000,’ I’m going to be looking for those 10 kids to vaccinate and I’ll be rationalizing to myself why that’s okay.”
Part of the problem, according to Sutton, is the state of the vaccine research literature that keeps doctors in the dark about the reality of adverse events.
“Vaccines have been very poorly studied,” she said. “Some of them were approved, like hepatitis B, after only four days in one case and five days in another brand’s case study — and it was approved for use in every newborn baby.”
Other vaccines have been studied for as long as 42 days, but none long-term, which is necessary to see the development of autoimmune diseases like asthma that don’t show up immediately after vaccination, she said.
“So the board expert could say there’s no evidence that an adverse event is related to vaccines, which is not accurate because the evidence is there — but it’s not in the evidence that the CDC accepts,” Sutton said.
According to Sutton, the CDC “very carefully curates” the articles and studies it puts on its website to support its own policies. If a CDC-sponsored study shows adverse vaccine reactions, it won’t appear on its website, she said.
Sutton shared the story of a former cardiologist at the Mayo Clinic who was training to do heart transplants when her 12-month-old daughter received an MMR vaccine and immediately regressed with severe autism. The woman had to leave the cardiology program and return to her home in Europe to care for her child.
Sutton said this woman claimed the CDC was researching a lot of topics, including that the rubella virus in the MMR vaccine persists in the body for a long time and results in granulomas in the case of immune-deficient children and sometimes immune-competent adults.
“This is not on the CDC website,” Sutton said. “So if we look at the nature of the research supporting our vaccine program, we would be astonished and staggered and ashamed because we’re injecting our children with very little evidence that these vaccines are safe or effective.”
Financial incentives in research and drug approvals are also highly problematic, according to Sutton.
“Medicine is no longer medicine,” she said. “It’s become co-opted as another business. Sickness is more profitable than health and mandates are more profitable than choice.”
“Otherwise, despite the efforts of individual doctors, the profession will be working against humanity and really becomes organized brutality instead of healthcare,” Sutton said.
‘The whole storm is not finished’
Sutton has exhausted or curtailed her administrative appeals with the states that have removed her license to practice medicine.
However, she and several doctors are planning to file a collective action in federal court in the spring. They are being supported by the nonprofit Physicians & Patients Reclaiming Medicine, where Sutton’s story is currently featured.
Meanwhile, Sutton keeps in touch with many of her colleagues who have suffered the same fate.
“They are recouping from the reputational and financial losses after being attacked,” she said. “So people don’t quit, but there is a lot of sadness about medicine.”
Sutton talked about the “diaspora” away from the state of California because of the discrimination that’s happened to families who had a health concern about a vaccine for their child.
“There’s been a lot of pain. So the whole storm is not finished,” she said.
Lacking a medical license, Sutton has turned to offering health education for a small group of clients. They meet monthly over Zoom, and individuals can discuss their concerns privately with her. But she no longer diagnoses, treats or does physical exams.
Sutton is currently preparing a course about integrative medicine to present to a group of acupuncture students.
John-Michael Dumais is a news editor for The Defender. He has been a writer and community organizer on a variety of issues, including the death penalty, war, health freedom and all things related to the COVID-19 pandemic.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
The American Psychological Association Wants (More) Federal Funding To Curb Online “Misinformation”
By Didi Rankovic | Reclaim The Net | January 9, 2024
The American Psychological Association (APA) is among those organizations enlisted to join the “war on misinformation” back in 2021, when APA took a $2 million grant from the Centers for Disease Control and Prevention (CDC) to help push the Covid narratives of the time.
APA’s particular task there was to come up with “a scientific consensus statement on the science of misinformation.”
Now, APA is clamoring for even more federal money as it declares psychology to be “leading the way on fighting misinformation” and advertises psychologists as the right people to research the problem (as it has been presented over the last years), and also be “part of the solution.”
An article on APA’s site doesn’t shy away from using terminology that spreads a sense of alarm, such as “the scourge of misinformation” and asserting that clinicians now have to treat patients “subsumed” by conspiracy theories, while institutions and communities are all allegedly suffering unspecified “harm.”
And APA also doesn’t shy away from mentioning the US presidential election, or from positioning that event as something that makes combating misinformation “messier and more important than ever.”
Messy it is, alright. To position itself properly among all those vying for funding/influence by exaggerating the threat posed by misinformation as a new phenomenon, APA actually states that, with the election in mind, fighting misinformation is “one of the top trends facing the field (physiology) in 2024.”
Really, APA? Maybe the author meant – a top trend faced by the organization itself, since it has had to show something in return for the $2 million 2021 CDC grant given to it to research “the science of stopping misinformation.”
(Spoiler: that “science” is already well-developed and applied; it’s called censorship.)
Beside the general alarmist tone, APA also came up with “recommendations.”
First, shut up – “don’t repeat misinformation.” Next, leverage “trusted sources to share accurate information.” At this point APA is pretty much parroting Big Tech’s various “guidelines” that have justified a lot of legitimate information getting obliterated over the past years as (never precisely and objectively defined) “misinformation.”
The “recommendations” address fellow physiologists, urging them to become “literate” in this newly crafted “science” – in order to be able to take active part in “the solution.”
According to APA’s current standards, helping people (as psychology professionals) should now include the total of eight recommendations (prominent and fairly ominous, free speech-wise, among which is – “collaborate with social media companies to understand and reduce the spread of harmful misinformation”).
And practitioners should do this everywhere – “(in) our labs, our communities, or our families.”
Green Billionaires Fund Large Backbench Tory Net Zero Parliamentary Caucus
BY CHRIS MORRISON | THE DAILY SCEPTIC | JANUARY 3, 2024
Almost half the Conservative Party’s backbench MPs in the British Parliament belong to a Caucus promoting extreme Net Zero ideas that is funded by a small group of green billionaire foundations. The Conservative Environment Network (CEN), which acts mostly as a lobby group, receives over 80% of its funding from the European Climate Foundation, Rockefeller Philanthropy Advisers, Oak Foundation, WWF-UK and Clean Air Fund. As regular readers will recall, these paymasters crop up regularly whenever anyone of influence, be they journalists, academics or politicians, requires help and guidance in promoting the insanity of removing hydrocarbon energy from industrial societies within less than 30 years.
The CEN relies on ‘peer reviewed’ research to lobby for Net Zero policies at both Parliamentary and local council levels. It counts over 150 MPs and Peers in its Parliamentary caucus, over 500 local councillors, along with “international declaration signatories” numbering 300 legislators from 45 countries. The billionaire-funded operation is said to support a network of ‘Net Zero champions’ inside Parliament “to make the positive case that Net Zero is an economic opportunity as well as moral responsibility”.
It is noted by CEN that when Russia invaded Ukraine “we helped promote the narrative that reducing dependency on fossil fuels through renewable energy and insulation would help defeat Putin”. Quite how fossil fuel dependency is reduced by intermittent renewables that rely on back-up hydrocarbons is not immediately clear. It’s unlikely that Putin quaked in his boots at the thought of the widespread mobilisation of loft insulators in the U.K.
The biggest CEN paymaster seems to be the European Climate Foundation, which is heavily supported by the Extinction Rebellion funder Sir Christopher Hohn. The CEN is run by Ben Goldsmith who is one of five trustees of Hohn’s fund, The Children’s Investment Fund Foundation. He is the brother of Lord Goldsmith, the former Conservative Environment Minister who served under Prime Minister Boris Johnson. Interestingly, Johnson’s father, Stanley, a long-time green activist, is listed as a member of the CEN steering committee.
The Clean Air Fund is also funded by Hohn along with Bloomberg Philanthropies, the green vehicle used to promote the political agenda of Michael Bloomberg, the former Mayor of New York. Bloomberg has a track record of funding the activities of politicians, again as regular readers will recall. He is one of the main backers of C40, a group of local civic leaders around the world, chaired by London Mayor and fireworks impresario Sadiq Khan. Removing cars from cites – and a form of rationing, whereby city dwellers are limited to a daily food quote of 2,500 calories with just 44g of meat – are just some of the proposals suggested in internal reports.
Of course targeting politicians is not a new game and lobbying legislators has long been a massive international enterprise. But the new breed of green promoters is particularly aggressive and the sums of money on offer are eye-watering. It has been reported that Hohn gave £46 million to C40. Jeremy Grantham, like Hohn a hedge fund billionaire, funds British academic institutions and journalists, but he also seems to have politicians in his sights. Speaking in 2019 to a group of business people in Copenhagen about the approaching apocalypse, he asked rhetorically, “What should I do, you say“? His suggestion: “You should lobby your Government officials – invest in an election and buy some politicians. I am happy to say we do quite a bit of that at the Grantham Foundation… any candidate as long as they are green.”
All of this, it might be argued, has led to the British Parliament donkey-nodding through some of the most restrictive and potentially most disastrous Net Zero legislation in the world. The actual target of 2050 Net Zero was rushed through in 2019 via secondary legislation by a Prime Minister without any considered debate. A green activist legal unit within Government called the Climate Change Committee keeps feet to the fire with demands for industry-destroying cuts in carbon dioxide emissions. Over £12 billion a year is lifted from the pockets of electricity users to pay for hopelessly inefficient power from the breezes and sunbeams that accounts for barely 5% of total energy use. In the cities, the cars of the less well off are penalised, while empty cycle lanes, road closures, 20 mph speed limits and sky-rocketing parking charges proliferate. Meanwhile, there are not enough children in the Congo to mine all the cobalt needed for spontaneously combusting electric cars, while heat pumps spell catastrophe for the life chances of old and frail people in the depths of a cold British winter.
“We’re very grateful to all those who have supported CEN financially and made our work possible,” says the Conservative Environment Network.
Chris Morrison is the Daily Sceptic’s Environment Editor.
Featured Video

More Iran War fallout: Maritime insurance industry shifts from London to China
or go to
Aletho News Archives – Video-Images
From the Archives
The Biggest Threat to Peace in Middle East
By Dr. Elias Akleh* | Sabbah Report | May 24, 2010
A build up of heightened tension in the Middle East is escalating in the last few weeks. American and Israeli postures towards Lebanon, Syria, and Iran have become more threatening. Listening to speeches of political leaders one hears talks only about war not peace. Iranians and Israelis are continuously training hard for a possible showdown. Both sides are conducting extensive war games every month. This led Syrians to claim that Israel is preparing for a soon-to-come another war. The Jordanians also are warning that current stalemate of the peace process is an indication of a war breaking out this summer. The Russian President and his army chief hinted, a few months ago, that the US and Israel were planning for an attack on Iran.
Indeed Iran is, as it has been for last few years, the target of most of the threats and accusations of supporting terrorism. Escalating incitement against Iran the American Defense Department sent last month (April) to Congress a report on Iran’s military claiming Iran could develop intercontinental ballistic missiles capable of reaching the US by 2015.
Ignoring the fact that N. Korea, India, Pakistan, and Israel are proven to have nuclear weapons while Iran does not, the US Secretary of State Hillary Clinton chose in her speech, to the nuclear Non-Proliferation Treaty review conference at the UN, to focus on Iran’s alleged nuclear ambitions putting the whole world at risk as she put it. According to Clinton Iran’s acquisition of nuclear weapons, rather than Israel’s more than 200 nuclear bombs, is destabilizing the Middle East. She called on the world’s nations to rally around US efforts to hold Iran, not other nuclear countries, to account.
The accusation that Usama Bin Laden is living comfortably in Iran had received a boost after the broadcast of a documentary called “Feathered Cocaine”. This echoed the June 2003 claims of the Italian newspaper Corre de la Sierra that Bin Laden was in Iran according to some intelligence report, and according to Richard Miniter’s book “Shadow War”. … continue
Blog Roll
 Aletho News
Aletho News- US Seeks Control Over Global Energy Infrastructure – Kremlin
- US senators target Orban government for standing up to Zelensky
- The deep-rooted culture of corruption in Ukraine
- Iran mobilizing one million soldiers to ‘create hell’ for any US ground assault: Report
- The coming military and psychological unravelling?
- Iran has the last laugh
- More Iran War fallout: Maritime insurance industry shifts from London to China
- US-Israeli aggression on Iran triggers review of GCC countries’ investment pledges to Washington
- Russia slams UK plan to seize tankers suspected of carrying its oil
- Pakistan ramps up food exports to Persian Gulf nations as war deepens food insecurity
- If Americans Knew
- Reports: Iran mobilizing 1M fighters, Israel-US run low on ammo, Israeli army faces shortage – Not a ceasefire Day 168
- ‘No Innocent Children’: Far-right Israeli Lawmaker Defends Killing of Palestinian Family
- Mossad’s promises helped Netanyahu convince Trump that Iran could be toppled
- US Arms Control Official Refuses To Comment When Asked If Israel Has Nuclear Weapons
- Veterans warn US landing could be ‘more Gallipoli than Vietnam’
- Israel may be committing war crimes in Lebanon – Not a ceasefire Day 167
- In the West Bank, life is a constant battle – 3 articles
- Jacob Reses, one of the most powerful pro-Israel operatives in Trump’s Washington
- Israeli-US assaults kill or injure 87 children a day – Not a ceasefire Day 166
- ‘Forever live by the sword’: Understanding Israelis’ massive support for Iran war
- No Tricks Zone
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis
- New Study Documents A 20-Year Pause In Arctic Sea Ice Decline – Driven By Internal Variability
- Wake-up Call: Survey Shows Majority Of Germans Now Favor Postponing Climate Targets!
