World-Renowned Physician Receives Public Acknowledgement from Accuser Admitting Allegations of Academic Fraud Were Incorrect
FLCCC | May 25, 2023
Washington, D.C. – The source of the false complaint that triggered the nearly year-long investigation into research supporting the use of intravenous Vitamin C to treat medical sepsis has publicly acknowledged his error and expressed regret for questioning the integrity of the study’s lead author, Paul E. Marik, M.D., FCCM, FCCP, founding member of the Front Line COVID-19 Critical Care Alliance (FLCCC) and former Chief, Pulmonary and Critical Care Medicine at Eastern Virginia Medical School.
In March of 2022, Kyle Sheldrick, a physician and Ph.D. candidate in Australia, made a series of unsubstantiated allegations of fraud on social media and to the CHEST Journal, claiming that he was able to determine that study data had been fabricated by applying baseless statistical methods to the 2017 peer-reviewed study led by Dr. Marik titled “Hydrocortisone, Vitamin C, and Thiamine for the Treatment of Severe Sepsis and Septic Shock: A Retrospective Before-After Study.” After receiving the complaint, the CHEST Journal launched a thorough review of the study that lasted almost a year. In April of this year, Dr. Marik received a letter from the journal stating that the investigation found no methodological errors as cited by the allegations.
Today Dr. Sheldrick issued the following statement acknowledging his mistake and accepting the outcome of the investigation:
“On 22 March 2022, I posted a blog post called ‘This scattrd corn.’ This post was a copy of a complaint I filed with the journal CHEST identifying features of a study led by Paul Marik titled ‘Hydrocortisone, Vitamin C, and Thiamine for the Treatment of Severe Sepsis and Septic Shock’ published on 3 February 2017 in CHEST, identifying that I believed them to be signs of fraud, and linked to this on twitter.
Those complaints have since been formally rejected by the journal CHEST, which I consider to be the definitive conclusion to the matter. I realise that this letter was used to imply that Dr. Marik personally acted deceptively, and falsely reported study data, which was not my intention, and this caused him significant hurt and distress. I regret this hurt to Dr Marik. I will inform those who have reported on this complaint that it has been rejected by the journal.
Dr Marik has also indicated to me that some subsequent controlled studies have found some positive outcomes for vitamin C in Sepsis, and I accept this.
This statement is not an endorsement of the use of Vitamin C in sepsis.”
“It was highly unprofessional that Kyle went to such lengths to accuse my colleagues and me publicly of academic fraud,” said Paul E. Marik, M.D., FCCM, FCCP, founding member of the Front Line COVID-19 Critical Care Alliance (FLCCC) and former Chief, Pulmonary and Critical Care Medicine at Eastern Virginia Medical School. “I hope that as he gains more experience as a researcher, he will understand that there are protocols in place for questioning the results of research that prevent harming reputations by making baseless accusations in public.”
The journal’s response to Dr. Marik did cite two minor revisions that do not change the final outcome of the original published study, but simply make it clear that some of the patients selected for the control group were “nonconsecutive” given the nature of hospital logistics and that the 1.5 g every 6 h for 4 days was a “target” dose that might not have been reached in all patients due to clinical considerations.
In a previous statement, Dr. Marik said the following about the revisions from CHEST : “I welcome the two words changed by the journal as they make the description of our methodology clearer and have no impact on the research results. However, this whole process was unnecessary as it raised unneeded concern about a life-saving treatment that we know is effective and used worldwide. I hope patients were not deprived of this vital treatment because of these false allegations.”
The World Health Organization estimates that in 2017 there were 11 million sepsis deaths worldwide, half of these deaths occurred among children.
A link to Dr. Sheldrick’s statement can be found here: https://kylesheldrick.blogspot.com/2023/05/update.html
A copy of the CHEST Journal’s findings can be found here: https://covid19criticalcare.com/wp-content/uploads/2023/04/Marik-Vitamin-C_Editors-Note-and-Ltr-to-Marik-2023-04-03.pdf
The published study can be found here: https://pubmed.ncbi.nlm.nih.gov/27940189/
About the Front Line COVID-19 Critical Care Alliance
The FLCCC Alliance was organized in March 2020 by a group of highly published, world renowned critical care physicians and scholars with the academic support of allied physicians from around the world. FLCCC’s goal is to research and develop lifesaving protocols for the prevention and treatment of COVID-19 in all stages of illness including the I-RECOVER protocols for “Long COVID” and Post Vaccine Syndrome. For more information: www.FLCCC.net
WHO Initiative Would ‘Promote Desired Behaviors’ by Surveilling Social Media
By Michael Nevradakis, Ph.D. | The Defender | May 30, 2023
The World Health Organization (WHO) is proposing a set of recommendations for “social listening surveillance systems” designed to address what it describes as a “health threat” posed by online “misinformation.”
The WHO’s Preparedness and Resilience for Emerging Threats (PRET) initiative claims “misinformation” has resulted in an “infodemic” that poses a threat — even in instances where the information is “accurate.”
PRET has raised eyebrows, at a time when the WHO’s member states are engaged in negotiations on two controversial instruments: the “pandemic treaty” and amendments to the International Health Regulations (IHR).
The latest draft of the pandemic treaty contains language on how WHO member states would commit to “social listening.” Under article 18(b), WHO member states would commit to:
“Conduct regular community outreach, social listening, and periodic analysis and consultations with civil society organization and media outlets to identify the prevalence and profiles of misinformation, which contribute to design communications and messaging strategies for the public to counteract misinformation, disinformation and false news, thereby strengthening public trust and promoting adherence to public health and social measures.”
Remarking on PRET’s “social listening” proposals, Michael Rectenwald, Ph.D., author of “Google Archipelago: The Digital Gulag and the Simulation of Freedom” and a former New York University liberal studies professor, told The Defender :
“The WHO’s PRET initiative is part of the UN’s attempt to institute global ‘medical’ tyranny using surveillance, ‘social listening’ and censorship. PRET is the technocratic arm of the WHO’s proposed pandemic treaty, which, if accepted by nation-states, would amount to the surrendering of national and individual sovereignty to this ‘global governance’ body.
“What better way to establish a one-world government than by using so-called global crises that must be addressed by nothing short of ‘global governance’? I remind readers that you cannot comply your way out of tyranny.”
WHO could use artificial intelligence to monitor social media conversations
A WHO document outlining the PRET initiative — “Module 1: Planning for respiratory pathogen pandemics, Version 1.0” — contains a definition of infodemic:
“Infodemic is the overabundance of information — accurate or not — which makes it difficult for individuals to adopt behaviors that will protect their health and the health of their families and communities.
“The infodemic can directly impact health, hamper the implementation of public health countermeasures and undermine trust and social cohesiveness.”
The document recommends that in response to the “infodemic,” countries should “incorporate the latest tools and approaches for shared learning and collective action established during the COVID-19 pandemic.”
According to the WHO document, this can be done if governments “establish and invest in resources for social listening surveillance systems and capacities to identify concerns as well as rumors and misinformation.”
Such resources include “new tools and approaches for social listening … using new technologies such as artificial intelligence to listen to population concerns on social media.”
According to the document:
“To build trust, it’s important to be responsive to needs and concerns, to relay timely information, and to train leaders and HCWs [healthcare workers] in risk communications principles and encourage their application.”
Risk communications “should be tailored to the community of interest, focusing on and prioritizing vulnerable groups,” the WHO said.
“Tailored” communication was a hallmark of public health efforts during the COVID-19 pandemic.
For instance, in November 2021, the Rockefeller Foundation, the National Science Foundation and the Social Science Research Council launched the Mercury Project, which aimed “to increase uptake of COVID-19 vaccines and other recommended public health measures by countering mis- and disinformation” — in part by studying “differential impacts across socio-demographic groups.”
Similarly, PRET states that it will “incorporate the latest tools and approaches for shared learning and collective action established during the COVID-19 pandemic.”
These “tools and approaches” could be deployed during “acute respiratory events,” according to the document, which recommends that governments:
“Develop and implement communication and behavior change strategies based on infodemic insights, and test them during acute respiratory events including seasonal influenza.
“This includes implementing infodemic management across sectors, and having a coordinated approach with other actors, including academia, civil society, and international agencies.”
This is not the first time the WHO has addressed the so-called “infodemic.”
A WHO review published Sept. 1, 2022, titled “Infodemics and health misinformation: a systematic review of reviews,” found that “infodemics and misinformation … often negatively impact people’s mental health and increase vaccine hesitancy, and can delay the provision of health care.”
In the review, the WHO concluded that “infodemics” can be addressed by “developing legal policies, creating and promoting awareness campaigns, improving health-related content in mass media and increasing people’s digital and health literacy.”
And a separate, undated WHO document advises the public on how we can “flatten the infodemic curve.”
WHO, Google announce collaboration targeting ‘medical misinformation’
The WHO’s PRET proposals coincided with a new multi-year collaboration agreement with Google for the provision of “credible health-related information to help billions of people around the world respond to emerging and future public health issues.”
The agreement was announced on May 23 by Dr. Karen DeSalvo, Google’s chief health officer, on the company’s blog. She wrote:
“Information is a critical determinant of health. Getting the right information, at the right time can lead to better health outcomes for all. We saw this firsthand with the COVID-19 pandemic when it was difficult for people worldwide to find useful information online.
“We worked with the World Health Organization (WHO) on a range of efforts to help people make informed decisions about their health — from an SOS alert to surfacing locally relevant content about COVID-19 to YouTube policies on medical misinformation.”
One way Google will collaborate with the WHO is through the creation of more “knowledge panels” that will prominently appear in search results for health-related questions on the platform.
“Each day people come to Google Search looking for trustworthy information on various health conditions and symptoms,” DeSalvo wrote. “To help them access trustworthy information our Knowledge Panels cite content from reliable sources covering hundreds of conditions from the common cold to anxiety.”
“Working closely with WHO, we’ll soon expand to cover more conditions such as COPD [chronic obstructive pulmonary disease], hypertension, type 2 diabetes, Mpox, Ebola, depressive disorder, malaria and more,” she added.
Google will make these Knowledge Panels available in several languages, including English, Arabic, Chinese, French, Russian and Spanish.
DeSalvo’s May 23 post also addressed an ongoing collaboration between Google and the WHO, Open Health Stack (OHS), which “help[s] accelerate the digital transformation of health systems around the world” and “lower[s] the barrier to equitable healthcare.”
Google also awarded the WHO with more than $320 million “in donated Google Search advertising via ad grants” allowing the agency “to publish health topics beyond COVID-19, such as Mpox, mental health, flu, Ebola, and natural disasters.”
Google is slated to provide an additional $50 million in ad grants to the WHO this year.
According to Google, the ad grants to the WHO represent the company’s largest such donation to a single organization.
Separately, the U.S. Food and Drug Administration (FDA) tweeted on May 22 about the agency’s own efforts at combating purported “misinformation” and “disinformation.”
The tweet contains a 35-second video, which claims “misinformation” travels “six times faster than the facts,” while promoting the FDA’s “Rumor Control” initiative.
A top priority of FDA Commissioner Dr. Robert Califf, “Rumor Control” was launched in August 2022 and joins other agency initiatives to fight “misinformation” and “disinformation.”
“The growing spread of rumors, misinformation and disinformation about science, medicine, and the FDA, is putting patients and consumers at risk,” according to the FDA’s Rumor Control webpage. “We’re here to provide the facts.”
The initiative asks the public to do “three easy things” to “stop rumors from spreading”: “don’t believe the rumors,” “don’t pass them along” and “get health information from trusted sources like the FDA and our government partners.”
“Rumor Control” appears to have been inspired by an initiative developed by the Virality Project, “a coalition of research entities” from six institutions “focused on supporting real-time information exchange between the research community, public health officials, government agencies, civil society organizations, and social media platforms.”
Documents released as part of the “Twitter files” in March revealed that the Virality Project, based out of the Stanford Internet Observatory, also called for the creation of a disinformation board just one day before Biden announced plans to launch his government-run Disinformation Governance Board.
Similar to PRET’s recommendations to target “accurate” information that nevertheless contradicts establishment public health narratives, the Virality Project worked with Twitter and other social media platforms, recommending they “take action even against ‘stories of true vaccine side effects’ and ‘true posts which could fuel hesitancy.’”
These censorship efforts included at least one tweet by Robert F. Kennedy Jr., chairman on leave of Children’s Health Defense.
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Researchers Hid Data Showing Fluoride Lowers Kids’ IQs, Emails Reveal
By Brenda Baletti, Ph.D. | The Defender | May 30, 2023
A team of pro-fluoride researchers led by California’s dental director intentionally omitted data from a study seeking to undermine the forthcoming National Toxicology Program (NTP) report linking fluoride exposure to neurodevelopmental damage in children, according to documents released last week.
The documents — obtained through a California public records search and posted in a press release by the Fluoride Action Network — show that the team, led by Dr. Jayanth V. Kumar, a dental surgeon, conducted a meta-analysis of the scientific literature on fluoride’s neurotoxicity and found a link between fluoride exposure and lowered IQ in children at low levels of exposure.
However, they omitted the data and wrote a paper concluding there was no evidence of a link.
Four rounds of peer review rejected Kumar’s manuscript as “poorly researched,” “internally inconsistent” and committing “unashamed exaggeration” before the journal Public Health finally published the study last month.
NTP report: ‘no obvious threshold’ at which fluoridating water is safe
Kumar et al.’s study was published online less than a week before the NTP’s May 4 Board of Scientific Counselors (BSC) meeting where advisors would finalize any recommended changes before the NTP publishes the final version of its report on fluoride’s neurotoxicity.
The NTP, an interagency program run by the U.S. Department of Health and Human Services that researches and reports on environmental toxins, conducted a six-year systematic review to assess scientific studies on fluoride exposure and potential neurodevelopmental and cognitive health effects in humans.
Its groundbreaking report on those findings — which consists of a “state of the science” monograph and meta-analysis surveying the literature on the links between fluoride exposure and cognitive health effects — concluded that prenatal and childhood exposure to higher levels of fluoride is associated with decreased IQ in children.
It also found that given that children are exposed to fluoride from multiple sources, there was “no obvious threshold” at which fluoridating water would be safe.
That means even when water is fluoridated at lower levels (typically 0.7 mg/L), studies found children had dangerous levels of fluoride in their systems.
The study’s findings contradict mainstream assumptions, the position of the dental industry, the sugar industry and the health regulatory agencies on the safety and benefits of fluoridating water to prevent cavities, despite substantial evidence to the contrary, including a series of studies funded by the National Institutes of Health (NIH).
At the BSC meeting, the American Dental Association (ADA), with whom Kumar is affiliated, used his meta-analysis as evidence there were problems with the NTP study and argued that the NTP report should therefore be postponed.
This was just the latest in a series of attempts by industry and regulatory agency officials to “weaken, delay, or kill” the report.
The report is a key document in the ongoing lawsuit filed by Food & Water Watch, the Fluoride Action Network, Moms Against Fluoridation and private individuals against the U.S. Environmental Protection Agency (EPA) seeking to end water fluoridation.
The lawsuit was put on hold for more than two years pending the finalization and publication of the report. After the NTP scientists finalized their draft in May 2022 — which they deemed ready for publication — U.S. District Judge Edward Chen ruled the EPA could no longer delay the trial.
The case is moving forward as the report goes through the final stages of review.
The plaintiffs hope the report will be published in final, rather than draft, form prior to the next phase of the trial in January 2024.
The report was subject to an unprecedented number of peer reviews and agency commentary, and as a direct attempt by the NIH to block its publication, internal Centers for Disease Control and Prevention emails obtained through the Freedom of Information Act (FOIA) revealed.
The final step in its publication will be for the NTP director to consider the BSC’s suggestions and make any amendments to the report prior to publication.
The BSC recommended the NTP include comment on the recently published meta-analyses, but they were not aware that Kumar et al. buried data in order to support their findings.
Plaintiffs’ attorney Michael Connett, partner at the law firm Waters Kraus & Paul, provided the evidentiary documents to the NTP last week so the agency can consider the omitted data in its long-awaited final review of fluoride’s neurodevelopmental toxicity.
Connett told The Defender :
“We felt it was important to make the NTP aware of the omitted data as it directly contradicts the paper’s conclusion, and further undermines the dental lobby’s main talking point that the neurotoxic hazards of fluoride only occur at high doses.”
How researchers manipulated ‘the science’
Email exchanges between Kumar and his co-authors and transcripts from Kumar’s deposition in the lawsuit show Kumar and his co-authors are professionally committed to water fluoridation.
Kumar is a member of the pro-fluoridation ADA’s National Fluoridation Advisory Committee and one of the nation’s leading promoters of fluoridation. He admitted in the deposition that his job is “to promote fluoridation.”
Dr. Susan Fisher-Owens, one of his co-authors, receives funding from Colgate, which also promotes water fluoridation.
Kumar also admitted that part of his job was to work with the ADA’s marketing consultant to come up “with the best messaging and strategies for how to best advocate for fluoridation,” including messaging to “inoculate policymakers” with pro-fluoride information before they speak with anyone questioning the policy.
The documents show the researchers set out to prove there was no link between low levels of fluoride and lowered IQ in children, specifically to undermine the NTP report.
In a presentation to the Association of State and Territorial Dental Directors in February 2021, Kumar told his colleagues he was hoping to pre-empt the NTP monograph by publishing his own meta-analysis and finding a “friendly editor” to publish it.
He reiterated this point in an email to his co-authors in July 2022, in which he emphasized there was “urgency” to get their paper published. “I wanted to publish the paper before the NTP report,” he wrote.
But publishing their desired results met a series of roadblocks as peer reviewers at the Journal of the American Dental Association rejected the study twice, finding the “discussion is unbalanced and misleading.”
One reviewer expressed concern that “the misinformation in this manuscript will fuel more controversy rather than stimulate prudent science-based decisions.”
Reviewers at Pediatrics Journal similarly rejected the study as marked by “fallacious” reasoning with conclusions that were “internally inconsistent.” Another reviewer said that a “facile style of citation increases concern about the balance of the work.”
But reviewers were unaware that Kumar also omitted data that contradicted his desired conclusions.
In an email to Kumar in February 2022, the study’s biostatistician Honghu Liu, Ph.D., told Kumar he thought the results of his analysis were “headed in the right direction.”
But on March 5, 2022, Liu wrote to Kumar explaining they had done analyses trying to find a safe threshold — ideally, around 1.5 mg/L — for fluoride in water, below which there is no association with reduced IQ in children. However, he wrote, “the results are opposite to what we hoped for.”
Liu told Kumar he would keep trying to produce different results. “Although hard, we can test more models to try to identify a threshold that can lead to a nonsignificant fluctuation in IQ before the threshold and a significant drop in IQ after the threshold,” he wrote.
But further analysis continued to show an association between low levels of fluoride exposure and decreased IQ. According to Liu, the dose-response analysis was “unfortunately not showing what we like to show.”
To resolve the problem, they eliminated the analysis from the study.
On March 24, 2022, Kumar sent his colleagues an email, quoting the particular parts of the NTP monograph that he sought to invalidate with their paper and raising concerns that reviewers would question their research if they included a certain figure that contradicted their conclusions.
When the team submitted the study to Public Health for publication, the analysis showing an association between low-level water fluoridation and IQ deficits had been removed.
The study concluded, “These meta-analyses show that fluoride exposure relevant to community water fluoridation is not associated with lower IQ scores in children.”
Connett sent the omitted analysis along with an explanation of how Kumar’s conflicts of interest influenced the outcome of his study in a letter to the NTP last week and urged them to take it into consideration as they evaluated the meta-analysis.
He wrote:
“The public counts on NTP to provide the best available science on the chemicals that impact their lives. I recognize this is a challenging task, particularly for chemicals with significant political interests at stake, but it is vital nonetheless.”
Through FOIA and public records requests, the plaintiffs revealed how high-level public health officials blocked the report’s publication after the NTP determined it was finalized.
They also showed how the ADA sought to influence the “independent” National Academies of Science, Engineering, and Mathematics to insist on further review.
Commenting on what else they might uncover about efforts to protect pro-fluoridation interests, Connett told The Defender :
“The only reason we were able to get Kumar’s emails is because he’s a government official who is subject to Freedom of Information requests. It raises the question of what else we would learn if the emails of private actors, like the PR strategists who Kumar works with, were also accessible.”
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Correction: Transgender Surgery Provides No Mental Health Benefit
By Andre Van Mol, Michael K. Laidlaw, Miriam Grossman and Paul McHugh | Public Discourse | September 13, 2020
A major correction has been issued by the American Journal of Psychiatry. The authors and editors of an October 2019 study, titled “Reduction in mental health treatment utilization among transgender individuals after gender-affirming surgeries: a total population study,” have retracted its primary conclusion. Letters to the editor by twelve authors, including ourselves, led to a reanalysis of the data and a corrected conclusion stating that in fact the data showed no improvement after surgical treatment. The following is the background to our published letter and a summary of points of the critical analysis of the study.
A Crisis of Irreproducibility in Psychology and Medicine
It has been an open secret for some time that there is a crisis of irreproducibility of scientific studies in medicine and other fields. No less a figure than the Director of the NIH, Dr. Francis Collins, wrote that, “the checks and balances that once ensured scientific fidelity have been hobbled. This has compromised the ability of today’s researchers to reproduce others’ findings.” For example, the National Association of Scholars reports, “In 2012 the biotechnology firm Amgen tried to reproduce 53 ‘landmark’ studies in hematology and oncology, but could only replicate 6 (11%).” In 2015 an article was published in Science in which there was an attempt to replicate 100 studies from three well-known psychology journals in 2008. In the original studies, nearly all had produced statistically significant results, whereas in the study replications, only a little over a third produced similar significant results.
Perhaps nowhere in medicine and psychology is this problem of irreproducibility worse than in studies of people who claim to have a mismatch between their sex and their internal sense of being male or female.
d
When we first analyzed the study last October, it was obvious that it had major shortcomings. Dr. Van Mol led our team—which includes endocrinologist Michael Laidlaw, child and adolescent psychiatrist Miriam Grossman, and Johns Hopkins professor of psychiatry Paul McHugh—to summarize our findings into a compact, 500-word letter to the editor. We were not the only clinicians to question the study’s legitimacy. A total of seven letters, all critical of the study, were published on August 1, including our own. The editors included a response from the original authors, and they explained why it took ten months to publish the letters.
Let’s look at the study and the shortfalls we found. The Swedish Total Population Register of 9.7 million people and national patient databases were used to assess the effectiveness of “gender-affirming hormone treatment” and “gender-affirming surgery” in affecting three endpoints: prescriptions for antidepressants and anti-anxiety medications, healthcare visits for mood or anxiety disorders, and post-suicide attempt hospitalizations. The study authors, Bränström and Pachankis, concluded that gender-affirming hormones offered no effect but that surgery did reduce mental health treatment. They further asserted the finding “provides timely support for policies that ensure coverage of gender-affirming treatments.”
The authors used an odd combination of retrospective data collected over an eleven-year period from 2005 to 2015, together with limited psychiatric outcomes over a “prospective” one-year period during 2015 and no control group. Qualifying criteria were, to be alive in Sweden as of December 31, 2014, and to have a diagnosis of gender incongruence. The first graphic in the study specified “time since last gender affirming surgery” and traced back ten years. That chart could easily be misinterpreted as a prospective ten-year follow-up.
Where the Study Falls Short
One problem leading to irreproducibility is loss to follow-up. This refers to patients who participated in a study but at some point are considered “lost”: they are either unwilling or unable to communicate, missing, or dead. Loss to follow-up is frequently seen in studies that validate the benefits of transition, and it was strongly implied in the Bränström study by several metrics. First, the authors reported that 2,679 Swedes were diagnosed with “gender incongruence.” Though seemingly large, the numbers are a full order of magnitude below what DSM-V prevalence statistics would project. Where did the remainder go?
A paucity of gender-affirming surgeries also suggested loss to follow-up. Table 3 of their study showed that only 38 percent of people diagnosed with gender incongruence had any type of affirmative surgery, and only 53 percent of those—about 20 percent of the total—had surgery of the reproductive organs. Gender affirming surgery is free in Sweden, so where are these patients? And for those whose last surgery was ten or more years earlier, how many completed suicide, died of other related causes, or emigrated from Sweden prior to the study timeline?
In terms of follow-up care, the authors only measured three outcomes as listed above. Overlooked were key data of completed suicides, healthcare visits, prescriptions, and hospitalizations for the litany of other medical or psychological diagnoses potentially related to gender-affirming treatments. Such information was available through Sweden’s multiple registry databases, so why not use it? These omissions suggested cherry-picking data in order to obtain the desired results.
We concluded our letter by comparing this study to the one we consider perhaps the best of its kind, also from Sweden, the 2011 Dhejne study. The Dhejne team made extensive use of numerous, specified Swedish registries and examined data from 324 patients in Sweden over thirty years who underwent sex reassignment. They used population controls matched by birth year, birth sex, and reassigned sex. When followed out beyond ten years, the sex-reassigned group had nineteen times the rate of completed suicides and nearly three times the rate of all-cause mortality and inpatient psychiatric care, compared to the general population. These important findings could have easily been updated by Bränström and Pachankis to the more current time frame.
Which brings us back to the August AJP and why seven critical letters took ten months to see print. Along with the letters, the AJP editors published a correction that explained their need “to seek statistical consultations.” These consultants “concurred with many of the points raised.” The study’s authors were asked to reanalyze their data, and the results demonstrated “no advantage to surgery” for their three endpoints in the subject population. The authors noted in their response letter that their “conclusion” “was too strong.”
Unresolved Problems
The AJP correction is significant, but the study still suffers from numerous problems. This has been a win for patients insofar as sex-reassignment surgery has been demoted from improving mental health to having no effect. The reanalysis on the other hand showed an increase in treatment for anxiety after surgery. Why was there not also an expected increase in post-surgical depression, as Drs. Malone and Roman argued in their letter to the editor? Increased post-surgical anxiety without an accompanying increased depression rate is a highly unusual finding. Were these subjects also lost to follow-up?
With respect to cross-sex hormones, it has been shown that 23 percent of patients on high-dose anabolic steroids like testosterone, which is prescribed to every female-to-male patient, meet criteria for a major mood syndrome, and 3 to 12 percent have developed psychotic symptoms. Why is this not reflected in the study or the reanalysis?
There remain major deficits in knowledge that the authors easily could have filled by examining the Swedish databases. One of the strengths of the 2011 Dhejne study is that an increase in mortality is clearly seen at around 10 years. The current study fails to look at available data over a similar time course to assess if mortality has been affected. Similarly, completed suicide information is missing from Bränström. How can one understand suicidality in relation to hormones and surgery by only looking at suicide attempts and not deaths? Likewise, if one wants to understand the full range of psychiatric disorders in this population by examining medication data, then the use of all appropriate pharmaceuticals should be included, not only anti-anxiety and anti-depressant agents. However, simply tabulating prescriptions for psychiatric medications provides a limited and inadequate measure of the degree of emotional distress in any population. Many distressed individuals decline to seek professional help or will refuse pharmaceuticals if they do. The effects of these gaps in knowledge are much like holes cut out of a portrait; the full picture is lost and distorted when the key facial features are removed.
Our co-author Dr. Paul McHugh ended sex reassignment surgeries at John Hopkins Medical School when a study from his department revealed that the mental and social health of patients undergoing sex reassignment surgery did not improve. He adds here that this paper, and even the correction, misdirects clinical thought in many ways. Most crucially it presumes an unproblematic future for these subjects, despite evidence that the psychological state of many will, after surgery, worsen with time. Our experience at Hopkins, when we first recognized that the psychological well-being of patients undergoing surgery did not improve, rested on relatively short-term assessments. The long-term Swedish study of Dhejne demonstrated that the serious fallouts including suicide emerged only after ten years. None of this clinical experience is reflected in this paper or its correction.
Now how will the thirteen-year-old girls who have had breast amputations and testosterone fare? Abigail Shrier writes in her excellent exposé Irreversible Damage that, “Nearly all of the detransitioners I spoke with are plagued with regret. . . . They possess a startlingly masculine voice that will not lift. . . . They live with slashes across their chests . . . and flaps of skin that don’t quite resemble nipples.”
How about children who are ultimately sterilized by puberty blockers followed by cross-sex hormones and even gonad removal? These unethical surgeries are receiving funding by the very NIH that claims to be working to correct problems of irreproducibility. These experiments are beyond reproducibility problems: they are ethical failures by which doctors cause long-term harm to children and adolescents, all based on political activism supported by faulty science.
The Bränström study reanalysis demonstrated that neither “gender-affirming hormone treatment” nor “gender-affirming surgery” reduced the need of transgender-identifying people for mental health services. We appreciate the editors, the study authors, and other letter writers for carefully scrutinizing the study and publishing these findings. However, our team believes that many of the pro-transition studies we have read fare no better. Fad medicine is bad medicine, and gender-anxious people deserve better.
Zero healthy young adults died of Covid-19 – Israel
RT | May 29, 2023
Not a single healthy person under age 50 died of Covid-19 in Israel, according to data released by the country’s ministry of health in response to a freedom of information request from lawyer Ori Xabi.
“Why were all the extreme measures of school closures, vaccination of children, and lockdowns needed?” internal medicine specialist Yoav Yehezkelli, a prominent critic of Israel’s Covid-19 policies, asked the Epoch Times.
In addition to requesting the number of Covid-19 deaths that had occurred in patients under 50 with no underlying health conditions, Xabi also asked the ministry to provide the average age of patients who died of the disease, segmented by vaccination status, as well as the annual number of cardiac arrest cases between 2018 and 2022.
The average age of fatalities among those vaccinated against Covid-19 was 80.2 years, while the average for the unvaccinated was 77.4, according to the ministry.
However, the MoH claimed to be unable to provide cardiac arrest information for the years 2021 and 2022, explaining that the information had not yet been transferred to them.
A study published last year analyzing data from the Israel National Emergency Medical Services found a shocking 25% spike in emergency services calls due to cardiac arrests for patients aged 16 to 39 taking place from January to May 2021.
However, Sharon Elroy-Pries, head of Public Health Services for the Ministry of Health, condemned efforts to draw a connection to the start of the Covid-19 vaccination program in December 2020 and denied that there had been an increase in cardiac arrests during that time, or any increase in deaths of young people.
Cardiologist Retsef Levi, one of the authors of the study, pointed out that the ministry had claimed not to have information on cardiac arrests for 2021 and 2022, meaning one of the two claims had to be false.
While the MoH insisted the data it provided to Xabi regarding patients aged 18 to 49 was limited to cases in which an epidemiological investigation had been completed, it is known to have access to a database that includes extensive data on all patients, including underlying conditions, irrespective of whether an epidemiological investigation was performed.
Yehezkelli called the MoH’s response “a bit naive,” questioning why it had withheld the full data, but pointed out that the statistics vindicated government critics. “It was definitely a disease that actually only endangered the elderly,” he said, pointing out that the MoH’s numbers showed the average age of death from Covid-19 was 80.
The MoH has promised to supply all-cause mortality data segmented by vaccination status and age by the end of the month, following more than two years of stonewalling in response to Xabi’s freedom of information requests.
Fake Scientific Studies by Nobel Prize Winner and Johns Hopkins Prof. Gregg Semenza
BY IGOR CHUDOV | MAY 28, 2023
Gregg Semenza, a pediatrician and a professor of Genetic Science, is a prominent researcher. Prof. Semenza works at Johns Hopkins University, a premier scientific institution so important that it received $1,050,368,895 from the Bill and Melinda Gates Foundation. (JHU played the most prominent role in the Covid pandemic response.)
Prof. Semenza made major discoveries regarding how cells adapt to oxygen availability. Those findings could potentially lead to curing cancer! So important was his work that he was awarded a Nobel Prize in medicine in 2019.
There was a small problem, however.
Seven of his studies were fake and were eventually retracted. Retraction Watch has the details. Even the pictures of mice used in the studies were photoshopped:
The authors have retracted this article as multiple image irregularities have been noted within this article, specifically: Figure 1A, upper panel (HIF-1a blot), lanes five and seven appear to be duplicates. Figure 6B, lower panel (b-actin blot), the first six lanes appear to be identical to Fig. 6G, lower panel (b-actin blot). Figure 3G, the image of the third mouse in the D10 Saline group is identical to the image of the third mouse in the D21 Digoxin group.
Here’s one retracted article and the retraction notice. I downloaded the image from that study and highlighted the mouse in question, which appears in two pictures but with different scan results.
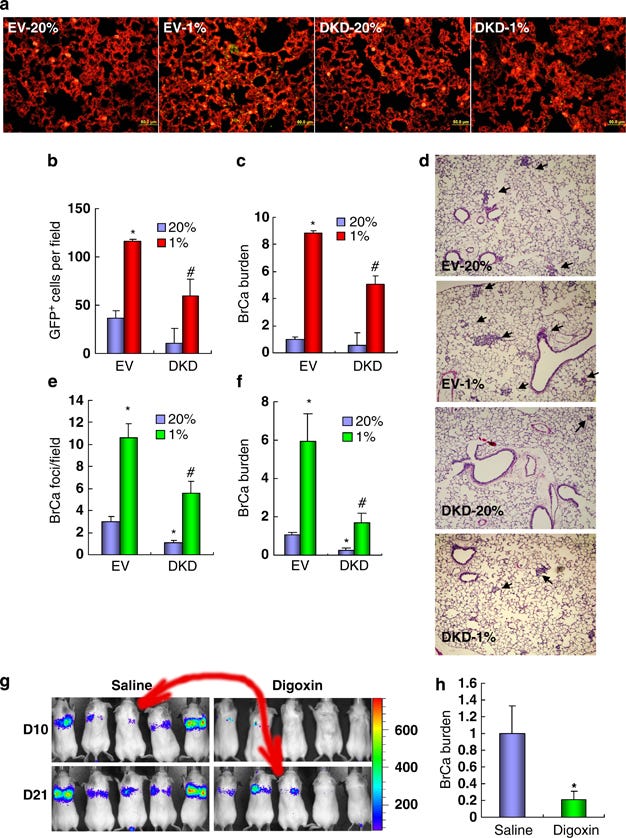
The authors copied/pasted the mouse picture and overlaid different scan results on the two copies. So, they did not have the scientific measurements they claimed to have!
Other retractions expose similarly ridiculous scientific fraud, including fake Western blots and more.
This fraud was not perpetrated by an obscure researcher languishing at a third-rate institution. Quite to the contrary, Prof. Semenza is a world-renowned scientist, occupying a position at a premier facility favored by the major funder of science, Bill and Melinda Gates Foundation.
Prof. Semenza shares the honor of receiving a Nobel prize with other famed recipients, such as Barack Obama, recipient of the 2009 Nobel Peace Prize, and António Egas Moniz, inventor of lobotomy and the winner of the 1949 Nobel Prize in medicine.

Antonio Moniz, Inventor of Lobotomy
So, the world of Nobel prizes is very special!
In consolation, we at least know about this fraud, and Semenza’s articles in question were properly retracted. So the self-correcting scientific process worked as intended, at last.
Sadly, as we know, retractions do not always work in an evidence-based, scientific way. For example, many honest articles questioning Covid vaccines or masks were retracted under pressure from science funders.
I feel that my trust in scientists has been violated by “COVID science” and certain other new scientific developments, but I still like the science of the good kind. I have much less faith in Nobel Prizes, however.
Featured Video

Rewriting the risk? Inside the government’s vaccine safety messaging
or go to
Aletho News Archives – Video-Images
Book Review
“Davos Can Really Replace the UN”
Inside the book that maps the architecture behind global governance — from the Epstein files to the Pact for the Future
Lies are Unbekoming | April 1, 2026
On June 13, 2019, the United Nations and the World Economic Forum signed a partnership deal to “accelerate the implementation of the 2030 Agenda for Sustainable Development.” That same evening, WEF president Börge Brende — Norway’s former Foreign Minister — had dinner with Jeffrey Epstein at Epstein’s Manhattan townhouse. The Epstein files, released January 2026, contain an exchange between the two from the previous year. Epstein to Brende: “Davos can really replace the UN. C21, cyber, crypto . genetics… intl coordination.” Brende back to Epstein: “Exactly — we need a new global architecture. World Economic Forum (Davos) is uniquely positioned — public private.”
The next day, the UN General Assembly adopted the framework for restructuring global governance.
That sequence — the partnership signing, the Epstein dinner, the candid admission about replacing the UN with a public-private architecture, and then the formal adoption — opens Jacob Nordangård’s The Digital World Brain. Pages two and three. Footnoted to the UN resolution number, the Epstein files, and the General Assembly record.
I keep coming back to it because it captures what this book does that almost nothing else in the independent research space manages. I’ve followed Jacob’s work for years now and interviewed him about his research. Each book peels back another layer of the same institutional architecture, and each time I think he’s reached the limit of what can be documented, the next one goes further. Nordangård doesn’t speculate. He doesn’t editorialize much. He lays institutional actions next to each other in chronological order and lets the pattern announce itself. … continue
Blog Roll
 Aletho News
Aletho News- How I fell foul of the BBC thought police
- The End of NATO
- 37 days of war on Iran cost US staggering $42bln, tracker shows
- Baghdad tells Asian refiners, traders to begin loading Iraqi crude amid Iranian exemption
- Under fire, Moscow and Tehran close ranks
- Iran, US receive Pakistan-mediated plan for ceasefire then final deal
- Iran submits demands for end to war as mediators scramble ahead of Trump deadline
- Iran Threatens Retaliatory Strike on Stargate AI Project in UAE
- US sent ‘a lot’ of arms to Iranian protesters – Trump
- Barak Ravid Launders Deception To Allow Trump To Back Off Of His Power Plant Threat – Again
- If Americans Knew
- U.N. experts demand Israel release prominent Gaza doctor after reports of ‘severe torture’
- Israel’s Latest Genocide Is Against the Shias of Lebanon. Why Is the World Silent?
- How Eliot Cohen’s influence over U.S. war-making paved the way for Trump’s war crimes in Iran
- Israelis don’t pay for the weapons we ‘sell’ to them — US taxpayers do
- While Distancing from AIPAC, Most 2028 Democratic Hopefuls Are Still Embracing Israel
- A brief history of the Israeli nuclear program, the open secret at the heart of the Iran war
- Israeli Settlers Killed a Palestinian Farmer on His Own Land, in Front of His Father. Yes, Again
- The US-Israeli War on Science is an Assault on our Future
- 100+ International Law Experts Say US Strikes on Iran Violate UN Charter, Could Be War Crimes
- ‘Vile, Horrifying, Evil’: Trump Threatens to Bomb Nation of 90 Million People ‘Back to the Stone Ages’
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
