CDC SHRINKS ROUTINE CHILDHOOD VACCINE SCHEDULE BY ~55 DOSES
By Nicolas Hulscher, MPH | FOCAL POINTS | January 5, 2026
Today, the CDC formally adopted a revised childhood and adolescent immunization schedule, following a Presidential Memorandum directing alignment with international best practices.
This marks the largest rollback of routine childhood vaccination in U.S. history.
After reviewing peer-country schedules and the scientific evidence underlying them, federal health leadership acknowledged that we are hyper-vaccinating our children.
The result is a dramatically smaller routine childhood vaccine schedule, cutting approximately 55 routine doses.
This is a major victory — even as serious safety concerns remain for the vaccines that continue to be recommended.
The Key Change: ~55 Routine Doses Eliminated
Previous U.S. routine schedule (2024)
-
- 84–88 routine vaccine doses
- Targeting 17 diseases
- (18 if RSV monoclonal antibody is included)
New CDC routine schedule (2026)
-
- ~30 routine doses
- Targeting 10–11 diseases
- Based on international consensus
Net change: approximately 54–58 routine doses removed, commonly summarized as ~55 routine doses.
Importantly, this reduction applies only to vaccines previously labeled “routine for all children.” No vaccines were banned or removed from availability.
What Was Removed from the Routine Schedule
The following vaccines are no longer recommended for all children by default:
- COVID-19
- Influenza
- Hepatitis A
- Hepatitis B (including removal of the universal birth dose if the mother is HBsAg-negative)
- Rotavirus
- Meningococcal ACWY
- Meningococcal B
These vaccines account for nearly the entire ~55-dose reduction.
What Remains Routine
The CDC now limits routine childhood vaccination to the following vaccines:
- Measles, Mumps, Rubella (MMR)
- Diphtheria
- Tetanus
- Pertussis
- Polio
- Haemophilus influenzae type B (Hib)
- Pneumococcal disease
- Varicella (chickenpox)
- Human Papillomavirus (HPV), reduced from two doses to one
This is still not “safe by default”
These vaccines remain:
- Insufficiently studied for long-term outcomes
- Untested in placebo-controlled trials
- Never evaluated as a cumulative schedule
- Inducers of over 20 chronic diseases
Adverse events such as febrile seizures, severe neurological injury including autism, ADHD, tics, autoimmune disease, asthma, allergies, skin and gut disorders, ear infections, and a long list of other chronic diseases have been documented across multiple vaccines on this list.
Reducing the schedule does not equal proving safety. It simply reduces exposure. Nonetheless, that reduction alone is quite meaningful.
Where Those Vaccines Went
Non-consensus vaccines were reclassified, not banned:
Shared Clinical Decision-Making
- COVID-19
- Influenza
- Hepatitis A
- Hepatitis B
- Rotavirus
- Meningococcal ACWY
- Meningococcal B
High-Risk Groups Only
- RSV monoclonal antibody
- Hepatitis A (travel, outbreaks, liver disease)
- Hepatitis B (HBsAg-positive or unknown maternal status)
- Dengue
- Meningococcal vaccines for defined risk groups
All remain available and fully covered by insurance. However, given entrenched institutional habits and ideological adherence to maximal vaccination, many clinicians are likely to continue promoting shared clinical decision-making vaccines as de facto routine unless families are informed and assertive.
Why This Is Still a Massive Win
For decades, the childhood vaccine schedule expanded without:
- Schedule-level safety trials
- Long-term outcome data
- Meaningful public debate
- Informed consent
This decision reverses that trajectory. It:
- Shrinks routine exposure dramatically
- Restores parental agency
- Forces future decisions to confront risk-benefit reality
Most importantly, it breaks the false premise that “more vaccines is always better.”
Conclusion
The CDC has eliminated every non-consensus vaccine from the routine childhood schedule, cutting routine exposure by approximately 55 doses—an implicit admission that the safety of the expanded schedule was never adequately established.
This decision does not end the problem. The vaccines that remain routinely recommended are still largely untested in long-term, placebo-controlled trials, are administered during critical periods of neurodevelopment, and continue to pose serious safety concerns. As a result, a substantial number of autism cases and other chronic conditions will continue to occur.
However, by sharply reducing cumulative exposure during early childhood, this change marks the first credible step toward reversing the trajectory. The burden of neurodevelopmental injury should begin to decline—not disappear, but diminish.
Even with its limitations, this action represents the most consequential course correction in U.S. pediatric vaccination policy in modern history. It breaks the assumption that an ever-expanding schedule is inherently safe, restores proportionality, and opens the door to long-overdue accountability, transparency, and real safety science.
Epidemiologist and Foundation Administrator, McCullough Foundation
Support our mission: mcculloughfnd.org
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.
HHS/CDC Fund Online Game ‘Bad Vaxx’ to ‘Psychologically Inoculate’ Vaccine Resistance
Ironically, the game uses the very techniques it claims to train users to detect.
By Jon Fleetwood | December 27, 2025
U.S. taxpayer funds are being used by federal health agencies to develop and test online psychological games designed to condition how people—especially younger audiences—interpret and respond to vaccine skepticism.
An August Nature Scientific Reports study reveals that the project was funded by the Centers for Disease Control and Prevention (CDC) under the U.S. Department of Health and Human Services, through a CDC award administered by the American Psychological Association.
The paper states that the funding totaled “$2,000,000 with 100% funded by CDC/HHS.”
The grant supporting the project is titled “COVID—INOCULATING AGAINST VACCINE MISINFORMATION,” award number 6NU87PS004366-03–02.
That award has already handed out over $4.3 million in taxpayer funds since its activation in 2018.
The project language mirrors the study’s conceptual framework: dissent is treated as exposure to a pathogen, and resistance to dissent is treated as immunity.
The government-funded study centers on the creation and evaluation of an online game called Bad Vaxx.
According to the authors, the purpose of the game is not to examine disputed vaccine claims or to compare competing evidence, but to reduce what they define as “vaccine misinformation” by shaping how players cognitively process vaccine-critical content.
This is despite the CDC’s own VAERS data confirming over 2.7 million injuries, hospitalizations, and deaths linked to vaccines since 1990.
The study authors explain their premise at the outset:
“Vaccine misinformation endangers public health by contributing to reduced vaccine uptake.”
From this premise, the study moves directly to intervention design.
“We developed a short online game to reduce people’s susceptibility to vaccine misinformation.”
The paper frames this approach as a form of psychological prevention, borrowing language from immunology rather than education or debate.
“Psychological inoculation posits that exposure to a weakened form of a deceptive attack… protects against future exposure to persuasive misinformation.”
The Bad Vaxx game operationalizes this concept by training players to recognize four specific “manipulation techniques”: what it refers to as emotional storytelling, fake expertise, the naturalistic fallacy, and conspiracy theories.
These techniques are treated as characteristic of vaccine misinformation as a category.
“The game trains people to spot four manipulation techniques, which previous studies have identified as being commonly used in the area of vaccine misinformation.”
The study does not include a corresponding examination of whether similar persuasive techniques may be used in vaccine-promoting messaging, government communications, or pharmaceutical advertising.
Ironically, the Bad Vaxx project itself relies on the same persuasive architecture it claims to neutralize—emotional framing, authority cues, and repetition—embedded in a gamified format designed to shape intuition rather than invite scrutiny.
The classification of “vaccine misinformation” is established in advance and applied only to information critical of injectable pharmaceutical products.
Throughout the paper, vaccine skepticism is framed as a behavioral and social risk rather than as a possible response to uncertainty, evolving evidence, or institutional error.
The taxpayer-funded authors write:
“Susceptibility to misinformation about COVID-19 predicts lower compliance with public health regulations and lower willingness to get vaccinated.”
The choice of a game as the delivery mechanism is emphasized as a strength of the intervention.
The authors repeatedly describe the format as “entertaining,” “immers[ive],” and scalable, highlighting its ability to shape intuition rather than deliberation.
“A practical, entertaining intervention in the form of an online game can induce broad-scale resilience against manipulation techniques commonly used to spread false and misleading information about vaccines.”
Games function by rewarding correct pattern recognition, reinforcing desired responses, and reducing analytical friction.
The study’s outcome measures reflect this design: discernment scores, confidence ratings, and willingness to share content, rather than independent evaluation of claims or evidence comparison.
The researchers also emphasize the potential reach of such interventions.
“The Bad Vaxx game has the potential for adoption at scale.”
This matters because the funding source is not an academic foundation with no policy stake.
The CDC is the primary federal agency responsible for vaccine schedules, promotion, and uptake.
Yet the study does not address how this institutional role shapes the definition of misinformation used in the intervention, nor does it acknowledge the conflict inherent in a public health authority funding psychological tools aimed at managing disagreement with its own policies.
The dystopian nature of the project emerges from the structure itself: state funding, psychological conditioning, asymmetric definitions, and a delivery system designed to bypass debate in favor of intuition.
What the paper documents, in concrete terms, is the use of taxpayer funds to develop and validate a behavioral intervention—delivered through a medium optimized for psychological conditioning—that trains users to reflexively distrust a predefined category of speech, while exempting vaccine-promoting institutions from equivalent scrutiny.
Trump Administration Moves to Overhaul Childhood Vaccine Schedule, Embrace Informed Consent Model
By Sayer Ji | December 20, 2025
In what may prove to be the most significant transformation of U.S. vaccine policy in decades, the Trump administration is preparing to fundamentally restructure how childhood vaccines are recommended—shifting away from blanket federal endorsements toward a model that empowers parents and physicians to make individualized decisions.
According to a December 19th report in The Washington Post, federal health officials are developing guidance that would encourage parents to consult directly with their doctors about vaccination decisions, rather than simply following a standardized federal schedule. This “shared clinical decision-making” approach represents a profound departure from the paternalistic model that has defined American vaccine policy for generations.
The Denmark Model: Less Is More
Central to the administration’s emerging framework is Denmark’s approach to childhood vaccinations. While the current U.S. schedule calls for vaccinations against 18 infectious diseases, Denmark recommends the injections against 10—yet maintains excellent health outcomes.
Tracy Beth Hoeg, a top FDA official, presented the Danish model to the CDC’s federal vaccine advisory committee earlier this month. Her presentation highlighted what she characterized as the “Danish Vaccination Schedule Benefits,” including making “more time for overall health at doctors’ appointments” and decreasing the “medicalization of childhood.”
The policy shift “kicked into high gear” immediately following President Trump’s directive earlier this month to consider recommending fewer shots. In his announcement, Trump noted that the United States is an “outlier” among developed countries and emphasized that “many parents and scientists have been questioning the efficacy of this ‘schedule.’”
Informed Consent Takes Center Stage
Perhaps most significantly, the administration is moving toward what health freedom advocates have long championed: genuine informed consent.
Under the emerging framework, vaccines would shift to “shared clinical decision-making”—meaning parents would consult with medical professionals about the risks and benefits before proceeding. Critically, insurance coverage would remain intact, preserving access while restoring choice.
The CDC has already begun implementing this approach for covid vaccines and the hepatitis B vaccine for children. This marks a fundamental acknowledgment that vaccination decisions are not merely technical matters to be dictated by government committees, but personal medical choices that belong in the hands of families and their trusted physicians.
A Vindication Decades in the Making
For those of us who have spent years (even decades) advocating for medical freedom, parental rights, and genuine informed consent, this moment represents a profound vindication.
Those like Secretary Kennedy, part of the “disinformation dozen,” viciously targeted during the Covid-19 era, have long argued that the U.S. vaccine schedule—which has expanded dramatically over the past four decades—deserves rigorous scrutiny rather than reflexive acceptance. We have insisted that parents are capable of making informed decisions about their children’s health when given accurate information about both risks and benefits. We have maintained that comparing health outcomes across nations reveals that more vaccines do not automatically equal better health.
Health Secretary Robert F. Kennedy Jr., who has called for additional scrutiny of the childhood vaccine schedule throughout his career, now sits at the helm of HHS. Martin Kulldorff, a renowned epidemiologist and biostatistician, has been named a chief science officer at the department. The voices that were systematically marginalized and deplatformed are now shaping policy.
Del Bigtree, founder of the Informed Consent Action Network, told the Post he supports the shift: “Our belief is there are just too many vaccines. It’s very exciting.”
What This Means Going Forward
The policy remains in development, and specific details—including which vaccines would move to the shared decision-making model—have not been finalized. HHS spokesperson Andrew Nixon cautioned that until official announcements are made, reports remain “pure speculation.”
However, the direction is unmistakable. The era of unquestioning deference to an ever-expanding federal vaccine schedule is drawing to a close. In its place is emerging a model that:
- Respects parental rights as the foundation of children’s healthcare decisions
- Restores the physician-patient relationship to its proper central role
- Acknowledges uncertainty rather than projecting false consensus
- Aligns with international norms rather than treating American exceptionalism as an excuse for over-medicalization
- Preserves access while eliminating coercion
The Resistance Has Already Begun
Predictably, the public health establishment is sounding alarms. Former CDC official Demetre Daskalakis called the Denmark comparison “not gold standard science.” The recently defunded American Academy of Pediatrics rejected what it termed the “one-size-fits-all approach” while simultaneously opposing any departure from the current one-size-fits-all schedule.
Even a Danish health official questioned the shift—though notably, his objection was that “public health is not one size fits all” and is “population specific,” which is precisely the point advocates have been making for years. If public health is population-specific, then surely it should also be individual-specific, with families empowered to make decisions appropriate to their unique circumstances.
A New Chapter for Health Freedom
We are witnessing what may be the most consequential health policy transformation of our lifetimes. After years of censorship, deplatforming, and marginalization, the health freedom movement’s core principles are being integrated into federal policy.
This is not about being “anti-vaccine.” It is about being pro-informed consent, pro-parental rights, and pro-science that welcomes questions rather than demanding compliance.
The battle is far from over. State mandates remain in place. Institutional resistance is fierce. The entrenched interests that have profited from the expanding schedule will not yield quietly.
But the tide has turned. And for parents who have long demanded the right to make informed medical decisions for their children, this moment represents nothing less than the restoration of a fundamental freedom.
FDA Won’t ‘Rubber-Stamp’ Pfizer mRNA Flu Vaccine Without Better Safety Data
By Michael Nevradakis, Ph.D. | The Defender | December 15, 2025
The U.S. Food and Drug Administration (FDA) likely won’t approve Pfizer’s mRNA flu vaccine unless the drugmaker produces data proving the product is safe for seniors, according to FDA Commissioner Marty Makary.
Makary told Fox News last month that the data from Pfizer’s recently completed Phase 3 clinical trial showed that adults 65 and older were at higher risk of several serious adverse events, including kidney failure and acute respiratory failure.
“We’re not just going to rubber-stamp new products that don’t work, that fail in a clinical trial,” Makary said. “It makes a mockery of science if we’re just going to rubber-stamp things with no data.”
Makary said the shot “failed in seniors” and the trial data “showed zero benefit” from the vaccine.
Karl Jablonowski, Ph.D., senior research scientist for Children’s Health Defense, said Makary’s comments signal a change in the way the FDA evaluates clinical trial data for vaccines.
“Makary’s FDA threw out the rubber stamp,” Jablonowski said. “The FDA, under different leadership, may have brushed off the lack of efficacy and Pfizer’s concerning safety data. A future administration may resurrect the rubber stamp. For the time being, this is Makary’s FDA.”
Last month, Pfizer published the results of its clinical trial in the New England Journal of Medicine (NEJM). However, the published results included data only for participants between 18 and 64. Data for participants 65 and older, published only on ClinicalTrials.gov, drew criticism from some scientists.
That data showed that elderly trial participants who received the mRNA vaccine had a significantly higher rate of death and several serious adverse events, including cancer, compared to participants who received the conventional non-mRNA flu shot.
This contrasts with Pfizer’s claims that the vaccine delivered “statistically superior efficacy” compared to the conventional flu shot, and that the frequency of serious adverse events was “similar” across the mRNA and non-mRNA groups.
“The disposition of the kidney and lung issues associated with the mRNA shot was concerning,” Jablonowski said.
Some experts noted that even among the 18-64 age group, adverse events were higher among trial participants who received the mRNA shot.
The only mention of the trial data for people 65 and over in the NEJM came in an accompanying editorial, which noted that this age group faces “the highest risk of hospitalization or death” from the flu.
Dr. Meryl Nass, a former internist and founder of Door to Freedom, said she was encouraged by Makary’s remarks. She said the FDA is legally required to license only those drugs that are proven to be safe and effective.
“This mandate is at least 70 years old,” Nass said. “What Makary is saying is already mandated by Congress. But the FDA has chosen to ignore that mandate due to politics, and Congress has failed to enforce it. Makary is actually obeying the law for the first time in decades regarding flu shots.”
Makary: annual mRNA vaccination ‘not based on science’
Makary told Fox News that past administrations rubber-stamped vaccine approvals even when safety data was questionable.
“That was the MO in the Biden administration with the eternal COVID booster approvals for young healthy kids,” Makary said.
The current administration will adopt a different approach to vaccine approvals, especially for children, Makary said.
“Recommending that a 6-year-old girl get another 70 mRNA COVID shots, one each year for the rest of her life, is not based on science,” Makary said.
Makary’s remarks came days after the release of a leaked memo in which Dr. Vinay Prasad, director of the FDA’s Center for Biologics Evaluation and Research, said changes are coming to the framework for evaluating flu vaccines.
“We will revise the annual flu vaccine framework, which is an evidence-based catastrophe of low quality evidence, poor surrogate assays, and uncertain vaccine effectiveness measured in case-control studies with poor methods. We will re-appraise safety and be honest in vaccine labels,” Prasad wrote in that memo.
Dr. Robert W. Malone, a member of ACIP and the committee’s influenza workgroup, told The Epoch Times that Prasad’s memo means “the entire influenza vaccine, annual vaccination enterprise is now subject to major disruption.”
In May, COVID-19 vaccine manufacturer Moderna withdrew its application for FDA approval of a combination mRNA flu and COVID-19 vaccine, after the FDA requested more clinical trials.
In June, the CDC’s vaccine advisers voted to stop recommending flu shots that contain thimerosal — a mercury-based preservative linked to neurodevelopmental disorders, including autism.
‘No one has figured out’ how to make mRNA shots safe
Makary’s statements came amid growing questions about the safety, efficacy and necessity of existing non-mRNA flu vaccines and waning uptake of the shots.
A Cleveland Clinic study published in April found that people who received the flu vaccine were 27% more likely to get the flu than those who didn’t.
Another study, published that month in JAMA Network Open, found that flu vaccines, whether given alone or in conjunction with COVID-19 shots, caused women to have longer menstrual cycles.
Endpoints News reported last month that public demand for flu vaccines is stalling and that “the general consensus among vaccine makers for Covid-19, flu and RSV is that dampening demand has shrunk sales.” Data from Eurostat indicate a decline in flu vaccine uptake in the European Union.
Research into mRNA-related platforms is also facing growing scrutiny. In August, the U.S. Department of Health and Human Services cancelled nearly $500 million in funding for mRNA vaccine research.
“With regard to mRNA injections, no one has figured out how to make them safe,” Nass said. “mRNA shots provide an unknown dose, and they can be ‘the gift that keeps on giving,’ because we don’t know how to shut off the production of mRNA-coded proteins. We probably never will.”
Nass added that while FDA rules require that a specific dose be established for every drug, “somehow this rule has never applied to mRNA vaccines.”
“I believe the mRNA platform is irrevocably flawed for this reason alone, although there are other toxicities involved that also make the platform problematic,” Nass said.
A growing number of scientists have called for the suspension or withdrawal of the administration of mRNA vaccines and products.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
BOMBSHELL: The CDC Has Updated Its “Autism and Vaccines” Page
This is a start to what honest science looks like
By Aaron Siri | Injecting Freedom | November 20, 2025
The new “Autism and Vaccines” page starts telling the truth, including:
“The claim ‘vaccines do not cause autism’ is not an evidence-based claim because studies have not ruled out the possibility that infant vaccines cause autism.”
“Studies supporting a link have been ignored by health authorities.”
“Scientific studies have not ruled out the possibility that infant vaccines contribute to the development of autism. However, this statement has historically been disseminated by the CDC and other federal health agencies within HHS to prevent vaccine hesitancy.”
Meaning, the CDC has simply been lying to you. The CDC’s website then continues its mea culpa stating:
“[M]ultiple reports from HHS and the National Academy of Sciences …. have consistently concluded that there are still no studies that support the specific claim that the infant vaccines, DTaP, HepB, Hib, IPV, and PCV, do not cause autism and hence the CDC was in violation of the DQA [Data Quality Act] when it claimed, ‘vaccines do not cause autism.’ CDC is now correcting the statement, and HHS is providing appropriate funding and support for studies related to infant vaccines and autism.”
“Of note, the 2014 AHRQ [Agency for Healthcare Research and Quality] review also addressed the HepB vaccine and autism. One cross-sectional study met criteria for reliability; it found a threefold risk of parental report of autism among newborns receiving a HepB vaccine in the first month of life compared to those who did not receive this vaccine or did so after the first month.”
“In fact, there are still no studies that support the claim that any of the 20 doses of the seven infant vaccines recommended for American children before the first year of life do not cause autism. These vaccines include DTaP, HepB, Hib, IPV, PCV, rotavirus, and influenza.”
As for the MMR vaccine, CDC’s website now says:
“[I]n 2012, the IOM reviewed the published MMR-autism studies and found that all but four of them had ‘serious methodological limitations,’ and the IOM gave them no weight. The remaining four studies and a few similar studies published since also have all been criticized for serious methodological flaws. Furthermore, they are all retrospective epidemiological studies which cannot prove causation, fail to account for potential vulnerable subgroups, and fail to account for mechanistic and other evidence linking vaccines with autism.”
Will Vaccines Prevent 1.1 million Deaths? No.
More CDC junk science
Injecting Freedom by Aaron Siri | September 18, 2025
At my recent Senate hearing, the minority witness submitted testimony claiming that “The CDC estimates that vaccines given to children born between 1994 and 2018 will prevent … 936,000 deaths over their lifetimes.” That claim has also been levied against Secretary Kennedy. Here is why it is a junk claim. (Note that portions of this response are taken directly from my new book Vaccines, Amen.)
Newsletter + Selection Bias
First, this claim is an updated version of a 2014 MMWR report. MMWR is essentially CDC’s newsletter. CDC’s own guidelines for the MMWR only permit publishing articles that align with CDC policy, which results in the worst form of selection bias. As explained by the CDC’s policies for publishing an MMWR report: “By the time a report appears in MMWR, it reflects, or is consistent with, CDC policy.” Hence, this article would only be published until it was massaged to assure that it aligned with the CDC’s policy that vaccines are safe and effective. That approach is not science — it is the perversion of science.
No Confidence Intervals
Second, like the WHO advertising report I discussed yesterday, this is an “advertising report” for CDC’s immunization program and has no confidence intervals for its estimates. This is because they are just unreliable guesswork. The true rate could be that the vaccines caused 2 million deaths between in the United States from 1994 to 2023 because the report provides no bounds for its claims. Again, absent bounds for its claims, it could be equally true that vaccines resulted in causing 2 million extra deaths instead of a net saving in lives.
Ignores All Confounders
Third, it’s even worse, because the 2023 report explains that “factors other than immunization (e.g., hygiene…) might have contributed to lower disease risks in recent decades, and reductions resulting from these contributions have not been incorporated into the model” (emphasis added). Meaning, it did not account for any other advancement or factor that may have improved health outcomes. Nothing. This alone renders this CDC promotion “study” junk science. It is also why it has no bounds for its estimates because it cannot calculate them with any confidence.
The Hard Data Shows The 1.1 Million Claim Is Nonsense
Finally, just a simple review of the data shows how preposterous the numbers are. While it claims vaccines saved 1.1 million lives between 1994 and 2023, it takes only looking at the actual real-world data to see this figure is nonsense. Let’s look at three diseases the report claims account for almost the entire 1.1. million lives purportedly saved: diphtheria, hepatitis B, and measles.
Diphtheria
Around 750,000 of the 1.1. million lives (over 68%) that CDC claims were prevented are from diphtheria. That means that it claims 25,000 lives were saved per year by this vaccine. That figure is nonsensical. Here is why.
The first vaccine for diphtheria was introduced in 1926. Between 1900 and 1926, as the population rose, the death rate from this disease had already declined 81%, from 40.3 to 7.8 deaths per 100,000 individuals. A vaccine had nothing to do with this sharp decline since no vaccine of any kind for diphtheria existed until 1926. The further decline from 1926 until at least the mid-1940s also had little or nothing to do with the vaccine because it was rarely, if ever, used outside of certain demographics in major cities, and diphtheria mortality declined at a similar rate in areas with or without its use.[1]
Below is an official government chart reflecting same. So, even as the population increased, the data clearly shows an 81% mortality decline from 1900 to 1926, a 97.3% decline from 1900 to 1940, and a 97.8% decline from 1900 to 1948; hence, no matter how you look at it, vaccination had little to do with almost all of the decline in mortality from diphtheria in the last century:[2]

Finally, in 1949, DTP was first licensed, and coverage of this vaccine began to improve. The year prior, in 1948, there was a total of 634 deaths from diphtheria. Yet, this MMRW report nonsensically claims the diphtheria vaccine is now saving 25,000 lives a year in the United States. (Also note that in 1985, the coverage for only three doses, let alone the six recommended today, was still only 63.6%.)
This claim becomes more absurd when you consider that even after six childhood doses, adults require a booster dose every ten years in adulthood, and about 40% of adults skip these boosters. Despite a large portion of adults not receiving boosters, the last case of respiratory diphtheria in the United States was nearly three decades ago. This almost certainly reflects the extensive literature which supports that any harmful effects by the diphtheria toxin are counteracted by iron, vitamin C, and vitamin B3, and deficiencies of these vitamins and minerals have mostly been eliminated in developed countries.
There are diseases that had a high mortality in the United States that disappeared without a vaccine. For many of these diseases, researchers sought to develop a vaccine but failed. For example, scarlet fever was one of the deadliest infectious diseases for children in 1900, with a death rate of 9.6 deaths per 100,000 children. Researchers furiously sought to develop a vaccine but repeatedly failed. By the 1950s, deaths from scarlet fever had significantly declined and by the late 1900s, deaths from scarlet fever were essentially non-existent.
Had a vaccine for scarlet fever been developed in the 1920s, 40s, or 60s, that vaccine would almost certainly still be on the childhood schedule today, and its use would be considered essential for controlling scarlet fever; undoubtedly, this same CDC advertising article would be estimating that its use is now saving hundreds of thousands of lives in the United States.
In fact, scarlet fever and diphtheria are similar in that each is caused by a bacterium that releases a potentially harmful toxin when the bacterium has been “infected” by a certain virus. Both diseases cause sore throats, and many doctors, without a lab test, will confuse diphtheria with scarlet fever, and vice versa. These two diseases also have something else in common: both declined at nearly the same rate beginning in 1900. The primary reason why public health officials and the medical community behave differently with regard to these two diseases is that a vaccine was developed for diphtheria, but not for scarlet fever. If a vaccine for diphtheria had not emerged, this disease would have likely gone the way of scarlet fever and other childhood diseases that effectively disappeared without a vaccine.
Even if it would not have disappeared on its own, the article’s claim that 750,000 lives have been saved from diphtheria between 1994 and 2023 is absurd given the failure to account for the actual mortality data, other factors that reduced morality from diphtheria, the lack of any bounds to its claim, the lack of population-wide immunity and disappearance of the disease anyway, and the objective big picture reality regarding this disease; it truly requires a true religious fervor that suspends all reason and thinking to conclude that this vaccine has saved 25,000 lives per year between 1994 and 2023. The reality, based on the real-world data, is likely far closer to what occurred with scarlet fever absent vaccination.
Hepatitis B
As another example, the CDC advertisement article claims Hep B vaccines saved over 90,000 lives from 1994 to 2023, amounting to over 3,000 lives purportedly saved per year. This claim again defies data and reason. By way of background, the first Hep B vaccine was introduced in 1981 and was made with human blood plasma from donors who were chronically infected with the Hep B virus; and in 1986, a new Hep B vaccine using recombinant DNA technology without human blood was licensed. With that background, the mortality from Hep B climbed after introduction of the 1981 vaccine, continued to climb after the introduction of the 1986 vaccine, and has never returned to pre-vaccination levels. In 1980, there were 294 deaths in the United States from Hep B. Today, there are around 1,700 deaths per year. Yet, somehow, CDC claims that Hep B vaccine has saved over 3,000 lives per year between 1994 and 2023. It defies reason.
Measles
As a final example, CDC’s advertising article claims measles vaccine saved 85,000 lives from 1994 to 2023, amounting to over 2,700 lives purportedly saved per year. This claim again defies data. The first measles vaccine came on the market in 1963. In the years leading up to the first measles vaccine in 1963, the CDC data reflects around 400 deaths from measles each year. There were also around 4.2 million births each year in the late 1950s and early 1960s, whereas there was around 3.8 million births each year between 1994 and 2023. Yet, somehow, despite improvements in standards of living, medical care, etc., and despite smaller cohorts of infants and children to infect, this model makes the data-defying claim that mortality went from around 400 deaths per year from measles pre-vaccine to over 2,700 deaths per year.
But it gets far worse for the CDC advertisement’s claim because the following U.S. government chart shows the decline in the measles death rate by over 98% from 1900 to 1960, three years before the first measles vaccine was introduced in the United States in 1963. Meaning, the measles vaccine had nothing to do with the over 98% reduction in the death rate from measles in the United States from 1900 to 1960.
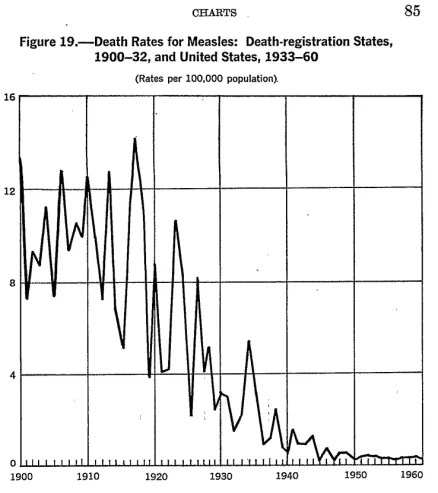
Taking a closer look, the CDC data reflects that in 1900, the rate of mortality from measles was 13.3 deaths per 100,000 individuals. By 1960, it was 0.2 deaths per 100,000 individuals. The same was true for 1961 and 1962. And as noted above, a similar decline of over 99% in measles deaths occurred between 1900 and 1967 in England and Wales, and it was only after that decline that the first measles vaccine was introduced there in 1968—five years after its introduction in the United States.
Hence, the same factors that caused measles mortality to decline by over 98% from 1900 to 1962 would, absent the vaccine interrupting the ecology of measles, likely have continued to cause a further reduction in the measles mortality rate after 1962. Meaning, at least a portion of the decline in the 400 deaths per year after the vaccine was available is no doubt attributable to the same factors that caused a steady decline in the measles death rate for decades prior to the introduction of the measles vaccine. Therefore, even without the measles vaccine, the death rate would have, no doubt, continued to decline after 1963.
In pockets of the country with poor nutrition, sanitation, and water, deaths from any pathogen, including measles, can occur at a higher rate. Those conditions still existed in some pockets of the United States in the early 1960s. As living conditions in those pockets of America improved with the introduction of clean water, improved sanitation, and better living conditions, deaths from measles declined, which is what typically occurs when these conditions improve. Let’s also not ignore that health care, especially the management and treatment of acute infections, has vastly improved since the 1960s. Doctors readily concede this point, unless you are talking about vaccines.
Yet, CDC claims that measles vaccines would have saved a data defying over 2,800 lives a year from measles in the United States between 1994 and 2023. CDC’s advertisement study, of course, also doesn’t account for the increase in deaths from heart disease and cancer due to the elimination of measles, as discussed in my previous post and reflected by studies that did not engage in estimates.
In sum, this CDC self-promotion article, that is not peer-reviewed and must conform to CDC policy to be published, does not account for any external factors, does not account for actual mortality data related to these diseases, and lacks any confidence intervals because its claims have zero reliability. Anyone citing this study claiming 1.1 million lives were saved is spreading propaganda. Not science.
[1] https://pmc.ncbi.nlm.nih.gov/articles/PMC1997101/pdf/pubhealthreporig01174-0001.pdf (“The simultaneous decline in diphtheria morbidity and mortality rates in all age groups of individual States located in different sections of the country, which began after a cyclic increase in incidence between 1915 and 1925, suggests the operation or influence of other factors besides, or in addition to, artificially induced immunity. Studies such as that included in the 1930 White House Conference on Child Health and Protection indicated that immunization programs were reaching a relatively large proportion of children in some areas or cities and a very low proportion in others as late as 1930. In spite of this wide variation, both morbidity and mortality began to decline rapidly after 1925 in all States simultaneously.”); https://www.cdc.gov/pinkbook/hcp/table-of-contents/chapter-7-diphtheria.html (“[D]iphtheria toxoid-containing vaccines became available in the 1940s” and “universal childhood vaccination program which included diphtheria toxoid-containing vaccines beginning in the late 1940s.”).
[2] The death rate per 100,000 individuals in the United States in 1900, 1940, and 1948 for diphtheria was 40.3, 1.1, and 0.4, respectively, for tetanus it was 2.4, 0.4., and 0.3, respectively, and for pertussis it was 12.2, 2.2, and 0.8, respectively. https://www.cdc.gov/nchs/data/vsus/vsrates1940_60.pdf.
Former CDC Officials Take Aim at RFK Jr. During Senate Hearing
By Suzanne Burdick, Ph.D. | The Defender | September 17, 2025
The U.S. Senate hearing that began today as an investigation into the firing of the CDC director and the resignations of other key agency officials morphed quickly into a forum for accusing U.S. Health Secretary Robert F. Kennedy Jr. of posing a threat to public health.
“Today should not be about me,” former director of the Centers for Disease Control and Prevention (CDC), Susan Monarez, Ph.D., told senators. “Today should be about the future of trust in public health.”
Monarez testified that she was fired for “holding the line of scientific integrity.” Dr. Debra Houry, former chief medical officer of the CDC who resigned after Monarez’s firing, also testified.
“Trust and transparency have been broken” under Kennedy’s leadership, Houry told members of the Committee on Health, Education, Labor and Pensions (HELP), which held the hearing.
She criticized Kennedy’s handling of the recent measles outbreak and the changes to COVID-19 vaccine recommendations.
The committee will hold another hearing in the future to allow Kennedy and current CDC officials to refute allegations made by Monarez and Houry, said Sen. Bill Cassidy (R-La.), the committee chair. “I want President Trump to have the best CDC in our nation’s history,” he said.
According to Sen. Bernie Sanders (I-Vt.), minority chair, the hearing was really about Kennedy’s “dangerous war on science, public health and the truth itself.”
Sanders praised Monarez for standing up for the “scientific method” and refusing to “rubber-stamp” Kennedy’s “dangerous agenda.”
Monarez testified that “vaccines are not controversial because they work.”
She also recounted how the CDC was attacked by a gunman who, in her words, was “driven by vaccine distrust.”
Sen. Roger Marshall (R-Kan.) called out the agency for creating public distrust during the COVID-19 pandemic. “The CDC is the cause of vaccine hesitancy,” he said.
Sanders refuses to have Monarez, Houry sworn in
The hearing came as no surprise. The day Monarez was fired, Cassidy posted on X that the sudden departure of top CDC officials “will require oversight” by the committee.
Cassidy wanted Monarez and Houry to be sworn in before their testimony. However, Sanders — whose approval was needed as minority leader — refused, saying Kennedy wasn’t sworn in at a prior hearing.
When another senator challenged Sanders’ refusal, Cassidy pointed out that Kennedy would be sworn in for future hearings related to today’s testimony.
Sanders still refused.
Cassidy reminded the witnesses that it’s illegal to lie to senators, even without explicitly vowing to tell the truth. Yet throughout the hearing, several senators questioned whether Monarez and Houry were being honest.
A U.S. Department of Health and Human Services (HHS) spokesperson told The Defender that Monarez’s prepared remarks contain “factual inaccuracies and leave out important details,” adding:
“Here’s the reality: Susan Monarez was tasked with returning the CDC to its core mission after decades of bureaucratic inertia, politicized science and mission creep corroded its purpose and squandered public trust.
“Instead, she acted maliciously to undermine the President’s agenda and was fired as a result. Some of her biggest offenses include neglecting to implement President Trump’s executive orders, making policy decisions without the knowledge or consent of Secretary Kennedy or the White House, limiting badge access for Trump’s political appointees, and removing a Secretarial appointee without consulting anyone. When she refused to acknowledge her insubordination, President Trump fired her.”
Children’s Health Defense CEO Mary Holland said Monarez represented the CDC’s “old guard” and that her termination was “necessary and proper.” She said:
“Monarez is assiduously following the pharma-funded script to attempt to oust Kennedy as HHS Secretary. Yet the obvious reality is that the CDC has lost the trust of the nation and the world, and radical reform is absolutely required if the agency is to continue at all.”
Senators, Monarez dispute details surrounding her firing
Senators at the hearing attempted to clarify disputed details surrounding Monarez’s firing.
The White House confirmed on Aug. 27 that she was fired after Kennedy tried to force her resignation and she refused to leave. Shortly after, Monarez wrote in an op-ed in The Wall Street Journal that she was fired because she “held the line and insisted on rigorous scientific review.”
She reiterated the claim in today’s hearing, saying Kennedy had given her a choice: accept the recommendations of the new Advisory Committee on Immunization Practices and fire top CDC officials responsible for vaccine policy, or resign.
According to Kennedy, he fired her because she responded “no” when he asked her, “Are you a trustworthy person?”
Monarez said the conversation went differently. “He told me he couldn’t trust me,” she said. “I told him that if he could not trust me, he could fire me.”
Sen. Markwayne Mullin (R-Okla.) pressed Monarez on details of the conversation, saying it had been recorded. However, he reportedly backtracked on the claim. “If HHS has a recording, I ask them to release it,” Cassidy said.
Cassidy also asked for all documentation related to the conversation for the committee to review.
Houry testified that she resigned because Kennedy “censored CDC science, politicized its processes and stripped leaders of independence.”
Andrew G. Nixon, an HHS spokesman, told The New York Times that Kennedy “has insisted that decisions be evidence-based, open to scrutiny and free from the kind of closed-door processes that undermined confidence in the C.D.C. during the pandemic.”
Monarez evasive on COVID and Hep B vaccines
Sen. Rand Paul (R-Ky.) asked Monarez if the COVID-19 vaccine prevented transmission or reduced children’s risk of hospitalization or death.
She replied, “It can.”
Paul cited research contradicting Monarez’s answer. He pointed out that children who get the COVID-19 shot face a heightened risk of myocarditis, and the shot fails to lower their risk of hospitalization or death.
James Lyons-Weiler, Ph.D., criticized Monarez in a Substack post, saying she was unable to provide substantive answers to Paul’s questions.
Lyons-Weiler also noted that Monarez offered “no credible defense” when Paul asked why it was important for newborns to get the hepatitis B vaccine if their mother was hepatitis B negative.
The CDC’s vaccine advisory panel is expected to vote Thursday on certain childhood vaccine recommendations, including the hepatitis B (Hep B) vaccine.
Critics have long raised concerns about the safety and necessity of giving the vaccine to newborns, particularly those not at risk for the disease. Today, the Hep B vaccine contains at least 250 micrograms of aluminum, and aluminum exposure has been linked to autism.
Paul asked Monarez, “What is the medical, scientific reason and proof for giving a newborn a hepatitis B vaccine if the mom is Hep B negative?”
Monarez refused to answer the question.
Paul called out Monarez for evading questions about specific vaccines and hiding behind vague assertions that all vaccines are “safe and effective.”
He said the burden should be on the CDC and its staff to prove that the benefits of giving babies COVID-19 and Hep B vaccines outweigh the risks. “That’s what the debate ought to be about,” he said. “Not on whether all vaccines are good.”
Monarez repeatedly said that the CDC doesn’t “mandate” vaccines; the agency only makes “recommendations.”
While technically correct, her answer overlooks the reality that many states use the agency’s recommendations when mandating vaccines for school entry.
Monarez was first CDC director in 70 years without medical degree
In March, Trump nominated Monarez for director of the CDC, where she had served as acting director until her nomination.
She was the first CDC director confirmed under a law passed in 2023 that requires Senate confirmation for the position. She was also the first person, in more than 70 years, without a medical degree to serve in the role. She has a doctorate in microbiology and immunology.
Trump nominated Monarez after withdrawing the nomination of Dr. Dave Weldon, who reportedly failed to secure enough votes because of comments he made suggesting a possible link between autism and vaccines.
Monarez, a biosecurity veteran, was previously deputy director of the Advanced Research Projects Agency for Health (ARPA-H), an agency within HHS created by the Biden administration to accelerate “high-risk, high-reward” biomedical research.
ARPA-H is modeled after the U.S. military’s Defense Advanced Research Projects Agency or DARPA. Monarez also previously held positions with the U.S. Department of Homeland Security and in the White House Office of Science and Technology Policy.
During her confirmation hearing before the Senate committee, Monarez affirmed her belief that “vaccines save lives,” and pledged to prioritize vaccine availability. She said mRNA vaccines are “safe and with demonstrated efficacy,” and she said she was unaware of any confirmed scientific link between vaccines and autism.
In her WSJ op-ed about why she was fired, Monarez said:
“Those seeking to undermine vaccines use a familiar playbook: discredit research, weaken advisory committees, and use manipulated outcomes to unravel protections that generations of families have relied on to keep deadly diseases at bay.”
Mark Crispin Miller, Ph.D., professor of media studies at New York University, told The Defender that Monarez is playing an old trick called “accusation in the mirror,” in which a person accuses their enemy of doing what the person has been doing.
He said:
“The trick usually works because it’s so disorienting, and most people have a hard time believing that anybody as ‘respectable’ as Susan Monarez — a woman with a Ph.D., who worked at CDC — could be so utterly dishonest. The only way to fight it is to call it out immediately, loud and clear.”
Watch the hearing here.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Why is America’s paediatric academy still pushing Covid vaccines for children?
The American Academy of Pediatrics has broken ranks with the CDC, issuing its own “evidence-based” immunisation schedule—but whose interests is the AAP really serving?
By Maryanne Demasi, PhD | August 19, 2025
The American Academy of Pediatrics (AAP) has just urged that all children aged 6 – 23 months receive a Covid-19 vaccine, regardless of prior infection, and extended that recommendation to older children deemed high risk.
Their guidance directly conflicts with the US Centres for Disease Control and Prevention (CDC), which recently withdrew broad recommendations to vaccinate healthy children and pregnant women in favour of “shared clinical decision-making.”
Now, for the first time, the AAP has broken ranks — issuing its own “evidence-based immunization schedule” that places it squarely alongside its biggest corporate donors, the very companies whose products it promotes.
The boycott
The rupture began in June 2025, when Health Secretary Robert F. Kennedy Jr dismissed the CDC’s old Advisory Committee on Immunization Practices (ACIP) and replaced it with a leaner panel.
The AAP, which had held a privileged liaison seat at ACIP for decades, responded by boycotting the meeting.
AAP president Dr Susan Kressly declared, “We won’t lend our name or our expertise to a system that is being politicised at the expense of children’s health,” branding the restructured ACIP “no longer a credible process.”
But credibility cuts both ways. At the June meeting, ACIP member Cody Meissner — himself an establishment veteran — rebuked the boycott.
“I think it’s somewhat childish for them not to appear,” he said. “It is dialogue that leads to the best recommendations for the use of vaccines.”
The AAP’s absence wasn’t about protecting children from politics. It was about rejecting a forum it could no longer control.
Following the money
The AAP insists its funding has no bearing on policy. But the Academy advertises its dependence on the very companies whose products it recommends for children.
On its own website, the Academy thanks its top corporate sponsors: Moderna, Merck, Sanofi and GSK. These companies produce nearly every vaccine on the childhood schedule — and now the AAP is demanding more of their products be given to babies.

Financial filings show corporate contributions make up a substantial slice of the Academy’s revenue. Even its flagship journal, Pediatrics, carries the fingerprints of industry support.
This isn’t independence, it’s entanglement. When an organisation funded by vaccine makers issues recommendations that boost those same companies’ sales, it is impossible to pretend this is solely about children’s health.
Parents have already rejected the shots
The problem for the AAP is that parents have already walked away. CDC data show that among toddlers, the rate is a mere 4.5%.
The public’s verdict could not be clearer: most families do not want these vaccines for their children.
The AAP knows this — yet it presses ahead regardless. Its recommendations are now performative, directed less at parents than at its corporate benefactors.
Kennedy strikes back
Kennedy seized on the contradiction.
Posting a screenshot of the AAP’s donor list, he wrote: “These four companies make virtually every vaccine on the CDC’s recommended childhood vaccine schedule,” after the Academy released its own list of “corporate-friendly vaccine recommendations.”

Kennedy accused the Academy of running a “pay-to-play scheme” on behalf of “Big Pharma benefactors” and demanded full disclosure of conflicts in its leadership and journal.
He warned that recommendations diverging from the CDC’s official list are not protected under the 1986 Vaccine Injury Act. For now, Covid-19 products remain under a separate regime — the PREP Act and the Countermeasures Injury Compensation Program (CICP), which HHS has extended through to 2029.
Kennedy cast this as a red line for the future: if the AAP keeps inventing its own vaccine schedule, it risks dragging doctors and hospitals into legal jeopardy.
This is no longer about one product but about who dictates the rules of childhood vaccination — government regulators or an industry-backed lobby group.
The deeper problem
This dispute isn’t really about Covid vaccines because parents, even healthcare workers, have already rejected them in overwhelming numbers. It is about who controls the institutions that speak in the name of children’s health.
The AAP claimed it boycotted ACIP in June to resist politicisation. In reality, it walked away from a process no longer stacked with the industry-aligned figures it had long relied on. That was the real affront.
The deeper problem is that the AAP is not a neutral guardian of child health. It is a lobbying arm entangled with corporate sponsors, issuing pronouncements that align with donor interests while ignoring the families it claims to represent.
AAP says it represents 67,000 paediatricians, and by extension America’s children. But its actions tell a different story. It represents the companies that fund it.
Children’s health is jeopardised when those entrusted with protecting it are compromised. The AAP’s latest recommendations are not science-based safeguards. They are corporate advocacy in disguise.
It is not just disappointing — it is harmful.
AAP’s full vaccine schedule [LINK]
AAP, AMA Booted From CDC Vaccine Advisory Working Groups
By Brenda Baletti, Ph.D. | The Defender | August 8, 2025
The American Academy of Pediatrics (AAP), the American Medical Association (AMA) and six other major medical associations will no longer participate in advising the Centers for Disease Control and Prevention (CDC) on vaccine policy, Bloomberg reported.
The associations said they were informed via email last week that their vaccine experts were being disinvited from the workgroups that report to the CDC’s vaccine advisory committee.
The Advisory Committee on Immunization Practices (ACIP) decides which vaccines should be recommended to the public, who should take them and how often. Its recommendations help determine which vaccines will be covered by the CDC’s Vaccines for Children Program and insurers, and will be mandated by states for daycare and school attendance.
The medical association members will no longer be invited to participate in the working groups that review data and form policy recommendations. However, they will be able to participate in the open public meetings, like the rest of the public.
They are being eliminated because they are “special interest groups and therefore are expected to have a ‘bias’ based on their constituency and/or population that they represent,” according to one U.S. Department of Health and Human Services (HHS) email reported by The Associated Press.
HHS spokesperson Andrew Nixon confirmed the decision in an email. He said:
“Under the old ACIP, outside pressure to align with vaccine orthodoxy limited asking the hard questions. The old ACIP members were plagued by conflicts of interest, influence, and bias. We are fulfilling our promise to the American people to never again allow those conflicts to taint vaccine recommendations.
“Experts will continue to be included based on relevant experience and expertise, not because of what organization they are with.”
Groups call decision ‘irresponsible, dangerous’ to public health
The organizations responded in a joint statement, claiming the decision is “irresponsible, dangerous to our nation’s health, and will further undermine public and clinician trust in vaccines.” They called on the Trump administration to reconsider the decision.
“We are deeply disappointed and alarmed that our organizations are being characterized as ‘biased’ and therefore barred from reviewing scientific data and informing the development of vaccine recommendations that have long helped ensure our nation’s vaccine program is safe, effective, and free from bias,” they wrote.
In addition to the AAP and the AMA, the statement was signed by the American Academy of Family Physicians, American College of Physicians, American Geriatrics Society, American Osteopathic Association, Infectious Diseases Society of America and the National Medical Association.
The decision was the latest attempt by U.S. Health Secretary Robert F. Kennedy Jr. to address the problem of industry influence over ACIP.
In June, Kennedy announced that HHS was retiring all 17 members of ACIP to eliminate conflicts of interest. At the time, most members had financial ties to pharmaceutical companies marketing vaccines, or had worked with public health agencies to promote controversial vaccines, including the COVID-19, RSV and HPV shots.
Two days later, Kennedy named eight researchers and physicians to replace approximately half of the members. One nominee declined to participate.
At the first meeting of the new ACIP committee, the members voted to stop recommending flu shots that contain thimerosal, a mercury-based preservative linked to neurodevelopmental disorders. The AAP, which criticized the decision, maintains that thimerosal is “safe.”
The committee also voted to recommend Merck’s new RSV monoclonal antibody shot for newborns.
Every group kicked out of ACIP takes corporate money from Big Pharma
In July, several of the medical associations removed last week from the ACIP working groups sued Kennedy and other public health officials and agencies over the changes to COVID-19 vaccine recommendations for children and pregnant women.
The groups’ lead lawyer, Richard Henry Hughes IV, was vice president of public policy at Moderna from 2020-2022, when the vaccine maker developed and marketed the Spikevax COVID-19 vaccine, which has netted the company billions of dollars over the last four years. He also previously worked for Merck.
Last month, the AAP also called for an end to religious and philosophical vaccine exemptions for children attending daycare and school in the U.S.
In an updated policy statement published in Pediatrics, the AAP said universal immunization is necessary to keep children and employees safe. The organization said there is a place for “legitimate” medical exemptions, but nonmedical exemptions — part of the fundamental constitutional right to freedom of religion — are “problematic.”
In addition to working with lobbyists like Hughes, every organization expelled from the ACIP working group is funded by the pharmaceutical industry.
The AAP, the major professional organization representing 67,000 pediatricians in the U.S., has overseen the rising rates of chronic illness and medication of American children over recent decades. It is also a lobbying organization that, over the previous six years, has spent between $748,000 and $1,180,000 annually advocating for its members, according to the government website Open Secrets.
The organization’s funding for that work comes, in part, from annual contributions from corporate sponsors, including vaccine manufacturers Moderna, Merck, Sanofi, Abbott Laboratories, GSK and CSL Seqirus.
The AMA is also funded in part by corporate sponsorships. In the past, it came under fire for taking more than $600,000 from pharmaceutical companies to finance a $1 million campaign to promote ethical guidelines discouraging doctors from accepting expensive gifts from drug companies, The Lancet reported.
AMA funding also comes from the AMA Foundation, which is funded by “Roundtable members” from the pharmaceutical industry. Its largest donor is PhRMA, the primary lobbying organization for the industry — which spent a record $12.88 million lobbying for the industry in the first quarter of 2025.
Other AMA sponsors include Agmen, Bristol-Myers Squibb, Eli Lilly, Genentech, GSK, Merck, Novartis, Pfizer, Sanofi and others.
The National Medical Association takes funding from Eli Lilly, Gilead, Regeneron, Pfizer, Merck, Amgen, Novo Nordisk, Vertex, AstraZeneca and others.
The Infectious Diseases Society of America partners with Abbvie, AstraZeneca, Gilead, GSK, Merck, Moderna, Pfizer, Sanofi and others.
A similar list of Big Pharma companies funds the American Academy of Family Physicians, which also partners with Amazon Pharmacy.
Pharma giants, including Pfizer and Johnson & Johnson, are on the long list of the American College of Physicians’ corporate sponsors, along with Big Food giants Tyson Foods and PepsiCo.
The American Geriatrics Society’s financial disclosure statement shows that it has various corporate sponsors, including Merck and Pfizer.
The American Osteopathic Association also has several corporate sponsors, including Pfizer, Astellas, Merck and Sanofi.
New ACIP committee member Retsef Levi, Ph.D., in a post on X, said that instead of these industry-sponsored organizations, the working groups plan to engage experts from a broader set of disciplines.
The working group participation will now “be based on merit & expertise,” he wrote, “not membership in organizations proven to have COIs [conflicts-of-interest] and radical & narrow view of public health!”
Related articles in The Defender
- Breaking: RFK Jr. Removes All Members of CDC Vaccine Advisory Committee
- RFK Jr. Taps 8 New ACIP Members, Offit Concedes Most ‘Seem Reasonable’
- RFK Jr. Hit With Lawsuit Over Changes to COVID Vaccine Policies for Kids, Pregnant Women
- Lawyer Leading Lawsuit Against RFK Jr. Over COVID Vaccines Used to Work for Moderna
- American Academy of Pediatrics Wants to Shut Down Religious Vaccine Exemptions
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
After Years of Silence, New CDC Vaccine Panel to Vote on Mercury in Flu Shots
By Suzanne Burdick, Ph.D. | The Defender | June 18, 2025
The CDC’s vaccine advisory committee will vote next week on the mercury-based flu vaccine, according to an Advisory Committee on Immunization Practices (ACIP) meeting agenda draft posted today on the ACIP website
The committee will also vote on RSV vaccines for pregnant mothers, babies and young children.
This will be the first meeting since U.S. Health and Human Services (HHS) Secretary Robert F. Kennedy Jr. tapped eight new ACIP members — just days after removing all 17 former members in what he called a “clean sweep … needed to re-establish public confidence in vaccine science.”
Before they vote, ACIP members will hear presentations on respiratory syncytial virus, or RSV vaccines, including Merck’s new RSV shot for newborns. Last week, the U.S. Food and Drug Administration (FDA) approved the new shot, even though clinical trials showed an 11.71% rate of serious adverse events, including death.
Discussions, but no votes, are slated for other vaccines, including COVID-19, Chikungunya, Anthrax and MMRV (Measles, Mumps, Rubella, Varicella).
ACIP decides which vaccines should be recommended to the public, who should take them and how often — recommendations the Centers for Disease Control and Prevention (CDC) typically rubber stamps and publishes on its immunization schedules.
The committee will meet June 25-26 in Atlanta, Georgia.
ACIP to discuss thimerosal after years of silence
Thimerosal is a mercury-based preservative used in multi-dose vials of the flu vaccine, according to the CDC. Most single-dose vials and pre-filled syringes of the flu shot don’t contain the preservative, as they’re intended for single use.
Over 25 years ago, vaccine industry leaders and public health officials concealed evidence from the CDC’s own database that linked thimerosal to neurodevelopmental disorders in children, including autism, according to transcripts from a meeting in Norcross, Georgia.
The U.S. government has long said thimerosal poses no harm to children. However, in 2001, out of what the agency said was an abundance of caution, the CDC said the ingredient would no longer be used in childhood vaccines.
A recent investigation by journalist Sharyl Attkisson proved both statements untrue.
Thimerosal’s potential to harm kids has been on Kennedy’s radar for over a decade. In 2014, he edited a book on the topic: “Thimerosal: Let the Science Speak: The Evidence Supporting the Immediate Removal of Mercury — a Known Neurotoxin — from Vaccines.”
The CDC webpage for flu shot safety considerations during pregnancy makes no mention of thimerosal, nor does it encourage pregnant women to be sure they get a flu shot from a single-dose vial or prefilled syringe to avoid mercury exposure.
Next week, ACIP members will hear a presentation on thimerosal in vaccines and a presentation on proposed recommendations for flu vaccines that contain thimerosal. The names of the presenters were not listed on the agenda at press time.
The committee will also vote on flu vaccines that don’t contain thimerosal.
Dr. Meryl Nass, who has attended many past ACIP meetings, said, “There is no need for thimerosal, a known neurotoxin, as it is not used in single-dose vials. Its use should be ended.”
Critics weigh in on ACIP agenda
Reactions to the ACIP meeting agenda were mixed. Some said it signaled that the CDC is veering off course, while others called for even more change.
Brian Hooker, Ph.D., Children’s Health Defense’s (CHD) chief scientific officer, said that although he was encouraged by Kennedy’s selections for the new ACIP members, he was disappointed in the slate of meeting presenters and moderators.
“It is the same old cast of CDC characters (from the National Center for Infectious and Respiratory Diseases) who present a very biased viewpoint,” Hooker said. “CDC’s culture is vaccinology as a religion, straight up. ACIP committee members desperately need an alternative view that is based on the very stark reality of vaccine ineffectiveness and the extremely high prevalence of vaccine adverse events.”
Dr. Jeremy Faust, editor of Medpage, said in a Substack post critiquing the ACIP meeting agenda that the planned vote on thimerosal “revives and elevates a longstanding anti-vaccine conspiracy theory.”
“Removing the compound will do nothing to improve vaccine safety,” Faust wrote, “but it certainly will undermine confidence in other existing vaccines.”
Faust also criticized the CDC for failing to put a COVID-19 vaccine vote on the meeting agenda, writing that the move will leave “fall policies unclear.”
HHS officials last month removed the COVID-19 shot from the CDC’s recommended list of immunizations for healthy children and pregnant women after the FDA limited its COVID-19 vaccine approvals to high-risk groups and the elderly.
‘This could mark a turning point’
James Lyons-Weiler, Ph.D. is president and CEO of the Institute for Pure and Applied Knowledge, an advocacy group that pushes for accuracy and integrity in science and for biomedical researchers to put people’s health before profits. He said the ACIP meeting agenda suggested that the CDC was making progress in “structure, balance, and transparency.”
“If public comment is taken seriously and if safety data are rigorously and honestly evaluated — then this could mark a turning point,” Lyons-Weiler said.
Lyons-Weiler said it’s also important that the CDC be “fully open” about its Evidence to Recommendations framework.
When ACIP makes a vaccine recommendation, it’s accompanied by what’s called an Evidence to Recommendations framework that describes the information the committee used in making its decision.
In the past, the CDC took shortcuts in showing this evidence, Lyons-Weiler said. He said he hopes the next ACIP meeting shows that the CDC is moving forward “with the full light of science, skepticism, and civic trust.”
ACIP guidelines don’t address full scope of possible vaccine injuries
Historically, states use ACIP recommendations to help shape vaccine policy and doctors use them in making decisions.
Some states consider the ACIP’s “General Best Practice Guidelines for Immunization,” which lists examples of contraindications and precautions for each vaccine, as the only acceptable authority when deciding whether to grant a child’s medical exemption request to a school-required vaccine.
However, ACIP’s list of contraindications isn’t exhaustive, according to attorney Sujata Gibson, who said:
“Right now, states like New York and California are overruling treating physicians and rejecting medical exemptions when they don’t see the condition listed in the ACIP best practices guideline as a contraindication or a precaution.
“But the guideline doesn’t provide an exhaustive list of all the reasons a child may be at risk of serious harm… The way that New York, California and other states are treating these guidelines is reckless and dangerous, and children are being severely harmed as a result.”
In other words, it doesn’t matter how many doctors confirm that a particular child will likely be harmed by a certain vaccine, states like New York and California give medical exemptions only for conditions specified in ACIP’s guidelines.
The Defender reached out to the CDC to ask if the new ACIP committee will clarify that its guidance is not a substitute for clinical decision-making and should not be used as a standard for clinicians or schools in deciding whether to grant medical exemptions. The CDC did not respond by the deadline.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Legacy media has a meltdown after RFK Jr fires the CDC’s vaccine panel
By Maryanne Demasi, PhD | June 10, 2025
Yesterday, Robert F. Kennedy Jr. fired every single member of the CDC’s Advisory Committee on Immunization Practices (ACIP)—the influential group of experts that decides which vaccines are added to the childhood schedule.
Today, he set fire to the media’s hysterical reaction.
Within 24 hours, legacy outlets and public health institutions lost their collective minds. Former CDC directors, industry-funded doctors, and conflicted public health groups lined up to denounce Kennedy’s move as reckless, anti-scientific, even deadly.
“This is a dangerous and unprecedented action that makes our families less safe,” said former CDC director Dr Tom Frieden.
“Unilaterally removing the entire panel of experts is reckless,” said paediatrician Dr Tina Tan to The New York Times.
The American Academy of Pediatrics (AAP) said it was “deeply troubled and alarmed.” It claimed the move would “stoke distrust in lifesaving vaccines”—this from the same organisation that has spent decades pushing the childhood vaccine schedule while taking money from the very companies that profit from it.
Others framed it as a political purge, a blow to science, or a “coup” that would bring back measles and polio.
But within hours, Kennedy hit back—and this time, he wasn’t the outsider being easily dismissed. He was the Secretary of Health and Human Services. And he came armed with evidence, receipts, and a brutal takedown of the media’s favourite falsehoods.
In a searing post on X, Kennedy explained the decision.
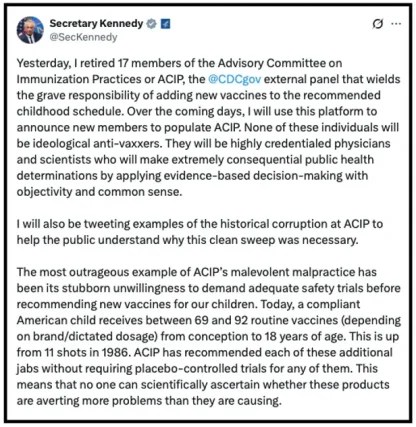
He said the clean sweep was necessary because ACIP had demonstrated its “stubborn unwillingness to demand adequate safety trials before recommending new vaccines for our children.”
And despite the media’s insistence otherwise, Kennedy argued that no routine injected childhood vaccine on the CDC’s schedule had ever been approved based on a placebo-controlled trial using an inert substance.
CNN had tried to prove him wrong last week—claiming it had found “257 placebo-controlled studies” of vaccines on the schedule.
Kennedy dismantled it in forensic detail.
“CNN is wrong,” he wrote. “No routine injected vaccine on CDC’s schedule was licensed for children based on a placebo-controlled trial. That is not conjecture. It is a fact based on FDA’s clinical trial data.”
Then came the body blows.
He pointed out that most of the 257 studies used active substances like aluminium, antibiotics, or other vaccines—not inert placebos.
He linked directly to FDA definitions of “placebo” and to official clinical trial records. Of the few studies that may have used saline controls, none were relied on by the FDA to license a single routine vaccine for American children.
Some studied products that were never approved in the US. Some occurred after licensure. Others involved discontinued vaccines. “CNN’s list ironically proves the lack of adequate safety trials,” Kennedy wrote in a stinging rebuke.
The post was devastating.
It was a clinical takedown of an industry riddled with deception—and it landed—because this time, Kennedy wasn’t being filtered through a hostile press.
He was speaking directly to the public, as a government official, with all the links to back it up. And the media couldn’t handle it.
Predictably, the media rolled out the same tired “experts” to recycle the same tired script—Paul Offit quotes, panic about “undermining trust,” warnings that children would die.
But Kennedy turned the whole thing inside out.
“We’ve gone from three routine injections by age one in 1986 to 25 in 2025,” he wrote. “And not one of them was licensed using a placebo-controlled trial.”
He said it plainly for the cameras: “That is just malpractice. So the people who are in charge of that are now gone.”
For years, the press had written Kennedy off as an anti-vaxxer and moved on. Now, they’ve thrown everything at him—and he threw it right back. Only now, he has the authority, data, and reach.
Kennedy told his followers he’d be announcing replacements in the coming days—no “ideological anti-vaxxers” just “highly credentialed physicians and scientists” committed to evidence, objectivity, and common sense.
Legacy media may still control the headlines, but they can no longer suppress the debate.
And perhaps that’s what really has them rattled.
They’re not defending science. They’re defending a regime of experts who signed off on decades of vaccine approvals without ever insisting on rigorous, inert-placebo safety trials.
When Kennedy calls them out, their only defence is to scream “danger!”—and hope no one checks the fine print.
Yesterday, he fired the gatekeepers. Today, he exposed the game.
Hep B Vaccines Come With High Risk, Little Benefit — Why Does CDC Recommend Them for Every Newborn?
By Brenda Baletti, Ph.D. | The Defender | May 13, 2025
As public concern grows over the large and growing number of shots on the Centers for Disease Control and Prevention (CDC) childhood immunization schedule, several critics are sounding the alarm about one shot in particular — the hepatitis B (Hep B) vaccine.
Among the 76 vaccine doses on the schedule, the CDC recommends that every infant born in the U.S. get their first dose of the Hep B vaccine on the day they are born. Studies show that more than 90% of infants typically do so.
By age 24 months, most of those infants have received the recommended three doses of the vaccine.
Hepatitis B is a liver disease caused by the hepatitis B virus (HBV), which can range from a mild, short-term, acute illness lasting a few weeks to a serious, long-term, chronic infection.
The virus is transmitted through bodily fluids, most often via intimate contact such as sex or sharing intravenous (IV) drug equipment. Being an IV drug user is the most common risk factor for the disease.
Infected pregnant mothers can also pass the disease to their infants, but relatively few do — about 25,000 pregnant women per year, or 0.69%, have Hep B, and about 1,000 of them pass it to their babies, according to the U.S. Department of Health and Human Services.
The CDC says, “almost all children and older adults infected with acute HBV recover completely with no lasting liver damage.”
Women can be tested for the disease to see if their babies would benefit from vaccination, but that’s not what the CDC recommends.
Instead, today the Hep B vaccine is required for children to attend either childcare, school, or both, in every state except Alabama.
School-age children don’t fit the profile of those at risk for contracting Hepatitis B. Also, the CDC has no evidence that Hepatitis B has ever been transmitted in a school setting, according to a records search posted on Substack by attorney Aaron Siri, who made the request.
Siri argues the Hep B mandate is about profit, not about protecting children from a contagious disease.
“The Hepatitis B vaccine is a case study in agency capture,” Siri wrote. All children would not be required to take the shot, he said “if pharma didn’t stand to earn billions through a wider mandate of this product.”
The Hep B vaccine market, valued at more than $8 billion in 2023, is projected to grow to over $13 billion by 2032, with the U.S. making up the largest market for the vaccine, Fortune Business Insights reported.
Why did the Hep B vaccine get added to the childhood schedule?
In a Yale Journal of Health Policy, Law and Ethics article, Children’s Health Defense (CHD) CEO Mary Holland questioned the constitutionality of mandating the Hep B vaccine for children to access education, especially given that CDC data show that transmission is unlikely through routine contact among children.
She said the CDC’s position on mass vaccination for children changed after the pharmaceutical companies got legal protection from liability.
When the CDC vaccine advisory committee made its first Hep B vaccine recommendation in 1982, the agency observed that the U.S. was a place of “low HBV prevalence.” CDC officials recommended the shot only for people at higher risk, including healthcare workers, people likely to be in sexual or “needle stick” contact with an infected person and infants born to mothers infected with the virus.
In 1988, the committee called for all pregnant mothers to be screened to determine if vaccination would be necessary. At that time, it was estimated that 16,500 mothers per year were infected and that without vaccination, an estimated 3,500 infants would become chronic carriers.
Later that year, the National Vaccine Injury Compensation Program (VICP), created by the 1986 Childhood Vaccine Injury Act, was established. The law protects vaccine makers from liability for injuries related to vaccines on the CDC’s childhood schedule, and the VICP is meant to provide an alternative means of compensating people who suffer “accidental injury or death” from taking those vaccines.
By 1991, the CDC had begun describing HBV risks differently, stating that the consequences of infection were “major health problems” in the U.S. — even though rates had not changed and the number of children infected with HBV was just a few hundred.
The CDC’s advisory committee concluded that because it was challenging to vaccinate those at risk for HBV, mass immunization against the virus was “the most effective means of preventing HBV infection and its consequences.”
The committee recommended all infants be vaccinated, regardless of their mothers’ hepatitis B status, and the Hep B vaccine was added to the childhood immunization schedule.
Dangers of the Hep B vaccine
Then and now, there are two Hep B vaccines licensed for infants at birth: Merck’s Recombivax HB and GSK’s Engerix-B. Both are made using a genetic engineering technology that was new when the vaccines were developed.
The clinical trials for both brands included only a small number of children, and researchers followed up on safety monitoring with infants for only four or five days in the different trials.
No medium or long-term studies were done, no comparisons were made between vaccinated and unvaccinated subjects, and the vaccines were administered only to healthy babies.
According to the Recombivax HB label, during clinical trials, 434 doses of the drug were administered to 147 healthy infants and children up to age 10, who were each monitored for five days after each dose. During those five days, 10% of infants experienced systemic reactions, including “irritability, fever (≥101°F oral equivalent), diarrhea, fatigue/weakness, diminished appetite, and rhinitis.”
Among the much larger group of 1,252 healthy adults, reactions were wide-ranging and sometimes serious. They included injection site issues and fevers, upper respiratory infections, influenza, body pain, insomnia and hypotension.
The Engerix-B package insert doesn’t specify how many babies were included in its clinical trials. However, it does indicate the trial subjects were monitored for only four days. The insert lists similar adverse events to those of Recombivax HB.
Post-marketing studies, which collect voluntary reports of adverse effects registered in places like the Vaccine Adverse Events Reporting System (VAERS), the Vaccine Safety Datalink, or with the vaccine makers, showed many more serious side effects reported for both versions of the Hep B vaccine.
Examples include immune system disorders like systemic lupus erythematosus, thrombocytopenia, Guillain-barré syndrome, multiple sclerosis, transverse myelitis, febrile seizure, Bell’s Palsy, herpes zoster, encephalitis, and many more.
Premature infants who take either Hep B vaccine have also experienced sleep apnea, which the labels warn about.
The inserts indicate it is impossible to determine whether the vaccine caused any of the reported events. Heritage Foundation Policy Analyst Catherine Pakaluk, Ph.D., criticized this approach to identifying adverse effects.
She wrote:
“To the extent that clinical trial data are insufficient to draw robust safety conclusions, patients are effectively used as test subjects post-licensure, but without knowledge that they are part of the test and without hope that their own adverse experiences will be scientifically useful as they would be in the case of a controlled trial. Voluntary adverse event data are suitable for identifying safety signals, but not for drawing conclusions about real risks.
The available data comes mostly from clinical trials that had small sample sizes, no control groups, and only a few days of follow-up, she added. The only other data source is post-licensure data, “which suffer from a lack of statistical usefulness.”
Peer-reviewed research also links the Engerix B vaccine to CNS inflammatory demyelination — a group of diseases in which the immune system attacks and damages the myelin sheath that protects the brain and spinal cord — namely multiple sclerosis in children.
Studies of children in the U.S. also linked the Hep B vaccine to arthritis, acute ear infections and sore throats. And a 2008 study associated Hep B vaccination of male newborns with autism diagnoses at three times the normal rate.
In a recent presentation about the Hep B vaccine, CHD science team member Heather Ray highlighted other safety concerns. For example, Ray noted that vaccine dosage is the same for newborn infants as it is for adults. Vaccine dosage doesn’t vary for a 7-pound infant or a 210-pound linebacker, she said.
The dose exposes babies to both the genetically engineered antigen and the aluminum adjuvant.
“Aluminum is a heavy metal that’s a proven neurotoxin and can cross the blood-brain barrier,” Ray said. “It has scientifically been shown to cause autism, asthma, autoimmune diseases and other horrendous neurological diseases and chronic illnesses.”
Infants’ organ membrane barriers are more permeable than those of adults, making them more susceptible to aluminum.
Until 2001, the Hep B vaccines also contained 25 micrograms of the mercury-containing preservative thimerosal.
Since the VAERS was established in 1990, there have been 18,950 adverse events reported in children under age 2 following Hep B vaccination, and 31,082 reports in children under age 17.
VAERS has been estimated to contain approximately 1% of adverse events, according to David Kessler, former head of the U.S. Food and Drug Administration (FDA).
Critics say Hep B vaccine poses many risks and no benefits for most babies
In terms of efficacy, the Hep B vaccine package inserts say the vaccine has been shown to produce antibodies to hepatitis B, and “appears to have protected infants whose mothers tested positive for hepatitis B antigens.”
Pakaluk wrote, “Therefore, we can conclude that the vaccine provides a robust antibody response to a disease to which they are not regularly exposed, and how long that antibody response lasts is unknown. In other words, for children not exposed to hepatitis B, there is no known benefit.”
Substack writer J.B. Handley, who has called for the elimination of the vaccine from the childhood schedule, wrote, “It’s a nearly useless vaccine, unless you are in the tiny minority of babies who have a mother with Hepatitis B.”
The Informed Consent Action Network, in 2020, filed a petition with the FDA demanding that the licensure of the Hep B vaccines be revoked or suspended until their safety was determined in a properly designed clinical trial.
CHD Senior Research Scientist Karl Jablonowski said,
“The CDC immunization schedule was simply not written for most people. The childhood Hep B recommendation is a prominent example. It is a pathogen that is primarily transmitted between humans through dirty needles and unprotected sex.
“In rare circumstances, it may be transmitted between people who live together — if one of them has an active infection — by things like shaving razors. Most children have zero risk factors and zero exposure. Most children should not be vaccinated against hepatitis B.”
Watch Heather Ray’s Hep B presentation here.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Featured Video

U.S. General Caine Warns: STRIKING IRAN is a HUGE RISK
or go to
Aletho News Archives – Video-Images
From the Archives
Stealth Bombers and Bunker Busters
Analysis of the so-called 12-Day War, and the triumphantly celebrated Operation Midnight Thunder

By William Schryver | imetatronink | November 28, 2025
The GBU-57 is a big fat gravity bomb with fins. To achieve effective precision, a B-2 bomber must drop it on its intended target from no further than about five nautical miles — essentially right on top of the target.
Its penetration depth is claimed to be 200 feet. But that capability has NEVER been tested against a seriously hardened deep-underground target encased in layers of high-performance concrete, and topped with a few dozen meters of solid rock. In that sort of real-world scenario, the GBU-57 would be lucky to drill down 50 feet, if that.
It was always ridiculous silly talk to suggest the GBU-57 was the wonder weapon it was made out to be. There is a good reason the US only produced a couple dozen of them and then stopped: they understood its acute limitations in a non-permissive combat environment.
And, notwithstanding the hyperbolic Israeli propaganda, there was never any credible evidence that Iranian medium- and long-range air defenses against fixed-wing aircraft were attrited to any significant degree. And Iranian short-range air defenses were increasingly effective against long-range Israeli drones with each passing day.
As for the B-2: it is a big fat subsonic aircraft. It flies at airliner speeds. A strike on Fordow would entail flying at least 500 miles in and out of Iran. … continue
Blog Roll
 Aletho News
Aletho News- Project Artichoke: 70 Years Ago, CIA Discussed Hiding Mind-Control Drugs in Vaccines
- Drug traffickers trained in Ukraine attack state forces in Mexico
- The tragic reality of Brazilian mercenaries in the Ukrainian conflict
- Zelensky Refused to Discuss Druzhba Pipeline Issue – Fico
- U.S. General Caine Warns: STRIKING IRAN is a HUGE RISK /Glenn Diesen & Lt Col Daniel Davis
- Israel designates five Palestinian media outlets as ‘terrorist organizations’
- Israel, not America, first: Carlson’s Huckabee interview lays bare US foreign policy priorities
- Israeli troops executed Palestinian aid workers at ‘point blank range’: Report
- Iran war What if today’s Iran is resigned to a long, hellish war with the US?
- Why Israel Is Escalating Its War Crimes Against Lebanon
- If Americans Knew
- The NY Times on the “MAGA” Split Over Israel & USS Liberty
- In Gaza, Ramadan without mosques, imams – Not a ceasefire Day 137
- Footage Shows Israeli Troops Waiting in Ambush, Then Opening Fire on a Palestinian Teen
- The US is on the brink of a major new war that Trump has not even bothered explaining
- Latest Epstein document dump is one more cover-up
- No Protection, No Justice: US Citizens Killed with Impunity by Israel
- Maria Farmer: Epstein Victim Reveals Explosive Information Covered Up by Media
- Average of five Palestinians killed by Israel every day in Gaza since ceasefire – Not a ceasefire Day 136
- Palestinian church leaders admonish Christian Zionist Mike Huckabee – Not a ceasefire Day 135
- Ominous messaging from Trump’s “Board of Peace” – Not a ceasefire Day 134
- No Tricks Zone
- Surprising Discovery: Sahara Is Greening…Billions Of Trees Where Once Thought To Be Barren
- New Research Reaffirms Clouds, Aerosols, And Surface Solar Radiation Are ‘Driving The Climate System’
- Germany: Electric Car Catches Fire At Charging Station, Sets Off Local “Inferno”, Widespread Damage
- New Study: Canada’s New Brunswick Was 1°C Warmer Than Today During The Medieval Warm Period
- Coal Power Back In Trend As Globe Tries To Keep Pace With Growing Demand For Power
- New Study: A 4°C Warmer Beaufort Sea Had ‘No Sea Ice’ 11,700 – 8200 Years Ago
- Unfudging The Data: Dutch Meteorological Institute Reinstates Early 20th Centruy Heat Waves It Had Erased Earlier
- German Gas Crisis…Chancellor Merz Allegedly Bans Gas Debate Ahead of Elections!
- Pollen Reconstructions Show The Last Glacial’s Warming Events Were Global, 10x Greater Than Modern
- Germany’s Natural Gas Storage Level Dwindles To Just 28%… Increasingly Critical
