Study Showing ‘High Likelihood’ of Link Between COVID Vaccines and Death Republished in Peer-reviewed Journal
By Suzanne Burdick, Ph.D. | The Defender | November 18, 2024
The largest COVID-19 vaccine autopsy study to date has been republished in a peer-reviewed journal — after twice being censored, according to Nicolas Hulscher, the paper’s lead author and an epidemiologist at the McCullough Foundation.
Science, Public Health Policy and the Law on Nov. 17 published the study, which had been previously withdrawn from Preprints with The Lancet and Forensic Science International.
Hulscher told The Defender the study’s republication signals a “pivotal victory for transparency and accountability in science.” It also marks “a significant setback” for actors in the biopharmaceutical complex and “their Academic Publishing Cartel,” Hulscher said.
Hulscher’s co-authors include Dr. Harvey Risch, Dr. Peter A. McCullough and Dr. William Makis.
Hulscher told The Defender the study provides “robust evidence that COVID-19 vaccines can cause death. This means that the FDA’s [U.S. Food and Drug Administration] criteria for a Class I recall have been fulfilled, warranting an immediate market withdrawal.”
The FDA defines a Class I product recall as “a situation in which there is a reasonable probability that the use of or exposure to a violative product will cause serious adverse health consequences or death.”
Risch, professor emeritus of epidemiology at the Yale School of Public Health, told The Defender that the COVID-19 vaccine spike protein “can stay around in some people and continue to do inflammatory damage in any site where it gets to through the bloodstream.”
In ‘striking act of censorship’ publishers withdraw study, shut down debate
The study’s publication in Science, Public Health Policy and the Law is the latest twist in an ongoing saga as the authors have tried to get their research out to the public and scientific community, Hulscher wrote on Substack.
The study results were first made public on July 5, 2023, as a preprint with The Lancet on SSRN, an open-access research platform.
However, Preprints with The Lancet removed the study from the server within 24 hours, posting a statement that the study’s conclusions were “not supported by the study methodology,” The Daily Sceptic reported.
McCullough told The Epoch Times that the study was experiencing “hundreds of reviews per minute” before its removal.
Preprint servers offer a place for the public to view scientific reports and papers while they undergo peer review, making scientific findings available immediately and for free and opening them up to broader public debate.
The authors subsequently posted on the Zenodo preprint server, while the review underwent peer review at Forensic Science International. It was downloaded over 130,000 times.
On June 21, 2024, after successful peer review, Forensic Science International published the study.
Within weeks, the study became the top trending research paper worldwide across all subject areas, according to the Observatory of International Research, Hulscher recalled.
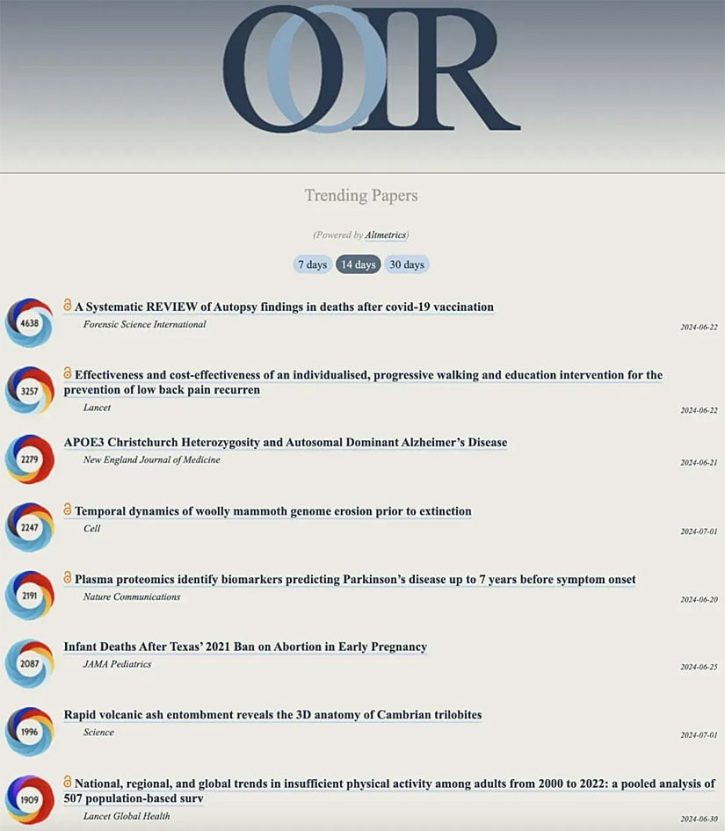
“Unfortunately,” Hulscher wrote on Substack, “in a striking act of censorship, Elsevier and Forensic Science International withdrew the article on August 2nd, 2024 in flagrant violation of their own withdrawal policy and COPE guidelines.”
He said they “left no traces behind, completely wiping our paper from the webpage.”
Elsevier and Forensic Science International said that “members of the scientific community” — who remained anonymous, Hulscher pointed out — cited numerous concerns about the study, including inappropriate citation references, inappropriate methodological design and a lack of factual support for its conclusions.
The concerns were “unfounded,” Hulscher wrote. The study authors wrote a rebuttal defending their study and submitted a revised manuscript. However, Elsevier and Forensic Science International rejected the revised manuscript.
Hulscher noted that Elsevier and Forensic Science International “failed to follow the proper scientific discourse method of allowing debate in Letters to the Editor.” Instead, they shut down the possibility of debate by censoring the study.
“This type of academic censorship poses a serious threat to the progress of scientific discovery,” he said.
73.9% of deaths reviewed by authors linked to COVID vaccines
As The Defender previously reported, the study authors did a systematic review of studies on autopsy findings following COVID-19 vaccination.
They first searched PubMed and ScienceDirect for all published autopsy and necropsy — another word for autopsy — reports related to COVID-19 vaccination in which the death occurred after vaccination.
They screened out 562 duplicate studies among the 678 studies initially identified in their search. Other papers were removed because they lacked information about vaccination status.
Ultimately, they evaluated 44 papers containing 325 autopsies and one necropsy case. Three physicians independently reviewed each case and adjudicated whether or not the COVID-19 shot was the direct cause or contributed significantly to the death reported.
They found 240 of the deaths (73.9%) were found to be “directly due to or significantly contributed to by COVID-19 vaccination.” The mean age for death was 70.4 years old.
Primary causes of death included sudden cardiac death, which happened in 35% of cases, pulmonary embolism and myocardial infarction, which occurred in 12.5% and 12% of the cases respectively.
Other causes included vaccine-induced immune thrombotic thrombocytopenia, myocarditis, multisystem inflammatory syndrome and cerebral hemorrhage.
Most deaths occurred within a week of the last shot.
The authors concluded that because the deaths were highly consistent with the known mechanisms for COVID-19 vaccine injury, it was highly likely the deaths were causally linked to the vaccine.
They said the findings “amplify” existing concerns about the vaccines, including those related to vaccine-induced myocarditis and myocardial infarction and the effects of the spike protein more broadly.
They also said the studies have implications for unanticipated deaths among vaccinated people with no previous illness. “We can infer that in such cases, death may have been caused by COVID-19 vaccination,” they wrote.
The authors acknowledged some potential biases in the article.
First, they said, their conclusions from the autopsy findings are based on an evolving understanding of the vaccines, which are currently different from when the studies evaluated were published.
They also noted that systematic reviews have bias potential in general because of biases that may exist at the level of the individual papers and their acceptance into the peer-reviewed literature.
They said publication bias could have affected their results because the global push for mass vaccination has made investigators hesitant to report adverse events.
They also said their research did not account for confounding variables like concomitant illnesses, drug interactions and other factors that may have had a causal role in the reported deaths.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Your Local Epidemiologist is worried. This is reassuring…
Mainstream “experts” are panicking about what is in store for public health with vaccine realists at the helm. Here’s my response.
![]()
By Madhava Setty | An Insult to Intuition | November 10, 2024
Katelyn Jetelina, PhD is an epidemiologist, biostatistician and mother of two little girls. She writes the “Your Local Epidemiologist” newsletter on substack which boasts over a quarter million subscribers. Those familiar with her content know that while well-intending, she serves as a mouthpiece for the CDC, explaining in easy to follow language what “the experts” are saying.
Her followers are passionate about her work. This is evident from the preponderance of comments which paint her as a true hero of the pandemic. Notably, she only allows comments from paid subscribers. She has created a massive echo chamber and one that pays her some serious dividends. If I remember correctly she has well over ten thousand paying subscribers, earning her an income that far exceeds mine as a full-time anesthesiologist.
I don’t mean to imply that she is a shill who exploits her audience by creating content that she knows is misleading or false. She believes in what she is doing, but she is suffering from the same cognitive blocks that many did four years ago: the experts know the most, we need to listen to them and grant them leniency when they get things wrong.
I have been a paid subscriber to her newsletter for almost two years. I pay to leave comments, hoping to encourage her audience to regard her position with a more critical eye. I have occasionally made some arguments that received a great deal of support from her non-paying readers. Those who contribute materially to her substack, on the other hand, usually respond with rebuke.
She has often derided the work of Children’s Health Defense. A year ago, I outed myself in her comment section, informing her that I was involved with the content RFK Jr’s organization produces as the science editor for The Defender. I expected that she would respond to my questions and critiques. What an excellent opportunity to dismantle the biggest “misinformation spreader” in front of her large audience. She never did.
Not surprisingly, her camp is in full crisis mode now. Here’s her latest:
In this brief article she encourages her audience to be strong, citing the following strategies:
- Building bridges instead of manning the barricades by finding common ground, which requires active engagement and humility. (It always helps me focus on one fact: No one wants to die. Then I move from there.)
- Recognizing what you say matters. That is, if you want people to hear you. Through literally the words we use, the framing, and the approach.
- Communicate with empathy, as anger and shame will only drive people further away.
- Listening (not simply hearing) so we can respond better to the needs on the ground. Americans need their questions answered, not to be told what to believe.
- Making strategic choices about which battles to fight, at what time, and at what level of government. Political capital is as scarce as financial resources—and needs to be allocated carefully.
This is a sensible strategy for everyone on both sides of the public health/vaccine debate. However she continues to double down on her basic hypothesis: The rise of vaccine skepticism is the direct result of misinformation.
I think she is wrong. Vaccine hesitancy and distrust of the medical orthodoxy is the direct result of true information that has finally percolated into public discourse despite the greatest effort to censor dissent I have ever witnessed.
Here is the comment I left on her article:
“Please don’t panic folks. We are witnessing a shift towards transparency and rigor from our agencies of public health. I understand why this readership is freaking out. This is an echo chamber. The real voices of clarity do not pay for a subscription here so you haven’t heard from them, and you don’t seek them out. You are only listening to voices like Katelyn’s who echo CDC PSA’s and their data as if it cannot be questioned.
I am a physician and an engineer. I left my practice in 2021 to work for RFK Jr’s Children’s Health Defense as the Senior Science Editor for The Defender, CHD’s on-line publication. I have since left, but I still stand behind every single article I have written and edited for that organization. I have been leaving comments on this substack for two years. Katelyn has never responded to any of my questions and critiques.
Isn’t that odd? One would think that she would be able to dismantle everything I share here in this public forum for the greater good.
Let me explain why there is such a growing “antivax” movement championed by Bobby and highly published physicians like Joe Ladapo. It has very little to do with so-called misinformation spreaders. It has to do with the public finally being informed about some difficult truths. The public is a lot smarter than you think.
1) Vaccine manufacturers cannot be sued if their products are found, even in an isolated case, to have caused harm. There is no other product like that. Obviously, there is much less incentive to do the proper safety testing if there are no consequences. The public knows this.
2) Nobody can deny that there has been an explosion of childhood diseases concomitant with the expansion of the CDC’s childhood immunization schedule following the National Childhood Vaccine Injury Act of 1986. OF COURSE correlation doesn’t equal causation. But if there was some causation, this is EXACTLY what we would be seeing. The public knows this.
3) The CDC could easily dispel all suspicion by doing a large retrospective study examining the health of vaccinated and unvaccinated children with regard to chronic disease rates. They have the data. They have not done the study and they refuse to release the data. Why?? There is no reasonable answer to this question except for the obvious: They don’t want to know the answer. The public knows this too.
4) During the Covid pandemic, the mRNA shots were authorized after an initial observational period of only six weeks on average. Note that the median observational period was two months. Mathematically, that means that half of the 40,000 participants were observed for less than four weeks at most. There is NO WAY to make any claim about long term safety yet the CDC simply states that these shots have been rigorously tested for safety. That is a lie. The public knows this now.
5) I have never met a single person, scientist or otherwise, who has read RFK Jr.’s “The Real Anthony Fauci”, who could debunk any of his claims. That book was released at the height of the pandemic and excoriates the record of the pandemic czar, yet no defamation lawsuit was ever filed. Why is that? Obviously it is because everything is true and the receipts are there for all to see. The last thing the CDC and vaccine manufacturers want would be to have the evidence for Kennedy’s claims appear in open court. Their strategy is to keep the evidence out of the public’s eye. It is an extremely effective strategy that has worked for decades.
6) RFK Jr.’s message is finally getting out, and he is making sense. Why on earth would anyone be against having vaccines tested by the same standards we use for medicines? Instead of pointing out the obvious, that that is an excellent idea for public health, the media runs hit piece after hit piece on this man. For every person who reads those character attacks and smiles a knowing smile, there are two more that see this as a desperate attempt to squelch some difficult truths.
7) Every other commercial on legacy media is for some sort of pharmaceutical product. It’s a joke. These companies don’t pay hundreds of millions of dollars to run ads to sell more product. They are buying good media coverage. People are seeing this too.
8) The idea that the pharmaceutical industry is out to improve public health is ridiculous. These are for profit companies and their executives’ first priority is to the shareholders. They don’t make the most money curing diseases. That eliminates demand for their product. They aren’t trying to kill everybody. That also decreases demand. Whether you are willing to consider it or not, the most profit is made when the public suffers from a chronic disease epidemic. That is what we have. Our Covid mortality rates were among the highest of any country despite access to the shots and our overpriced health care system. This is staring us in right in the face.
I have no animosity towards those who disagree with me. I am just calling it as I see it. This is the way the public is starting to see it too. Every effort to discredit the movement towards a healthy America with pejoratives like “antiscience” and “antivax” is going to backfire more and more. The public is waking up. Relax and give people like Kennedy and Ladapo a chance. Let’s see what happens. We all want our kids to grow up healthy and happy.
Madhava Setty, MD
Rationality Triumphs over Fear in Federal Court
By Harvey Risch | Brownstone Institue | November 17, 2024
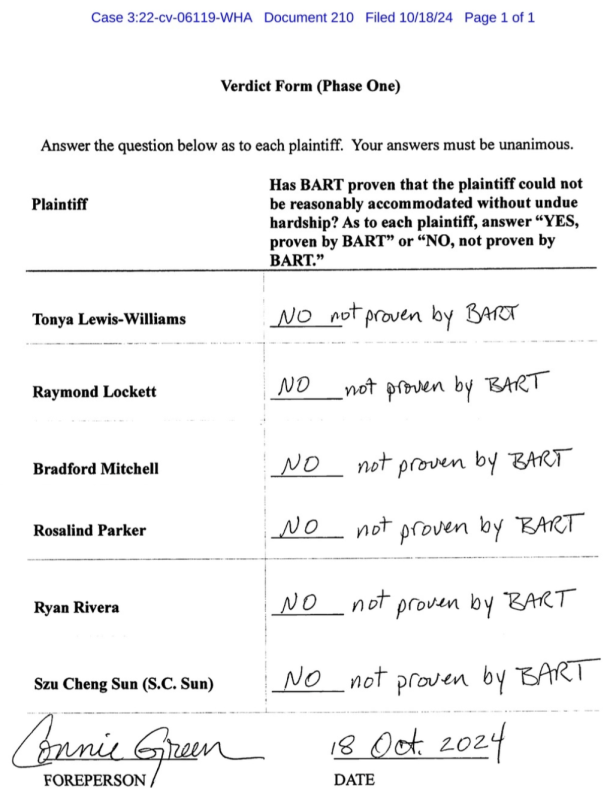
In a landmark decision in federal court, after a hung jury in the first hearing, the second jury found in favor of fired BART workers who had sued their employer after termination for filing vaccine mandate religious exemption applications. Each of the six plaintiffs in the case was awarded more than $1 million by the jury.
During the second year of the Covid-19 pandemic, governments and employers both private and public across the country instituted vaccine mandates requiring employees to have completed “full vaccination,” typically two doses of the mRNA vaccines, by set dates in fall 2021. Similar vaccine mandates were ordered for military personnel as well as college and university students.
In general, these mandates allowed that mandated individuals could file exemptions based on sincere religious objections or medical necessity, and if these exemptions were granted, employers were then required to seek, in good faith, accommodation positions where the exempted personnel could still work but would pose less of an infection risk to other employees, patients, customers, students etc. This process of exemption and accommodation was covered by Equal Employment Opportunity Commission (EEOC) rules.
According to the EEOC rules, as interpreted after the Groff v. DeJoy Supreme Court case which was decided in June 2023, employers have been required to establish that employees not satisfying vaccination mandates would create “undue hardship” in order for the employer to terminate the employee. The EEOC rules specify that infection risk, such as that occurring during the Covid-19 pandemic, constitutes a valid hardship risk, but what is in question is whether such risks constitute “undue” hardship as stated in Groff v. DeJoy.
In a sound and rational analysis, the EEOC rules (section L.3) attempt to quantify the degree of infection hardship risk:
“An employer will need to assess undue hardship by considering the particular facts of each situation and will need to demonstrate how much cost or disruption the employee’s proposed accommodation would involve. An employer cannot rely on speculative or hypothetical hardship when faced with an employee’s religious objection but, rather, should rely on objective information. Certain common and relevant considerations during the COVID-19 pandemic include, for example, whether the employee requesting a religious accommodation to a COVID-19 vaccination requirement works outdoors or indoors, works in a solitary or group work setting, or has close contact with other employees or members of the public (especially medically vulnerable individuals). Another relevant consideration is the number of employees who are seeking a similar accommodation, i.e., the cumulative cost or burden on the employer.”
These rules provide a framework for evaluating the degree of infection transmission risk posed by employees, both vaccinated and unvaccinated, in a workplace. What is remarkable here is that EEOC used the “does,” not the “can,” criterion. “Does” is rationality; “can” is fear.
In legal cases at deposition or testimony, science and medical experts are frequently asked questions such as “Doctor, can drug X cause bad event Y?” Medical and science experts live in a mental universe of science theories, and of course, there might be some possible circumstance where drug X could cause bad outcome Y. We were taught in medical school, “Never say never.”
The question however is not really asking whether, in theory, drug X could cause bad outcome Y, but rather whether here on planet Earth, such outcomes actually do happen. The opposing attorney is trying to get a sound bite from the expert that the drug is potentially harmful. So while the question as posed asks “could” (or “can”) the drug do damage, the correct answer from the expert is, “In theory, the drug could do this, but in real-life applications, the drug does not do this.” “Does” conveys a quantitative estimate of how often things actually happen, whereas “can” is a theoretical question with major fear potential.
In 2021, it was not just the general public that had been propagandized to excessive fear of Covid-19, but companies and governments were also made to be afraid. Thus, many company decisions were based on fear, on supposed “worst-case scenarios,” that disregarded the range of effects of the decisions in favor of supposed benefits for reduced risks of Covid infection transmission.
Compounding this problem, the vaccines did appear to reduce risks of Covid transmission during the first half of 2021, giving employers empirical evidence to support their thinking about vaccine mandates.
However, by the time the vaccine mandates were implemented in the fall of 2021, the widespread Delta strain of Covid-19 infection had largely escaped vaccine immunity (remember the first booster campaign?) and thus the evidence of Covid-19 transmission risk reduction for “full vaccination” required by the mandates was virtually gone—except that medical experts for the defendants in the BART and other cases were still using the earlier stale evidence to support their scientific assertions. This also violates EEOC rules which require the use of the latest scientific evidence.
Thus in retrospect, as I had discussed in my testimony as an epidemiology expert for plaintiffs in the BART case, the jury appears to have eventually apprised the circumstances accurately: the small numbers of religiously exempt employees did not pose a major infection transmission risk in comparison to the large BART workforce or to the even larger BART ridership—patrons who themselves were not required to be vaccinated in order to ride the BART trains. In the case’s initial verdict form, the jury unanimously concluded, for each of the six plaintiffs, in response to the question, “Has BART proven that the plaintiff could not be reasonably accommodated without undue hardship?” they wrote, “NO, not proven by BART.”
That is, the fact that such individuals “could” pose infection transmission risks, did not establish an undue hazard that they “would” pose inordinate infection transmission risks. According to the rules laid out by the EEOC, rationality prevailed over fear in this case. One hopes that this legal precedent informs the many similar cases pending, of employees, students, and service members irrationally and unjustly terminated because of fear, not evidence.
Harvey Risch, Senior Scholar at Brownstone Institute, is a physician and a Professor Emeritus of Epidemiology at Yale School of Public Health and Yale School of Medicine. His main research interests are in cancer etiology, prevention and early diagnosis, and in epidemiologic methods.
As Cancer Rates for Young Adults Continue to Climb, Are Doctors ‘Dancing Around the Elephant in the Room’?
By Michael Nevradakis, Ph.D. | The Defender |November 13, 2024
Cancer rates among Generation X (Gen X) and millennials are on the rise. A USA Today report cited environmental and dietary changes as possible contributing factors — but some experts say that’s only part of the story.
Dr. Mike Varshavski, a family medicine physician and health influencer, told USA Today the factors are “usually so complex and multifactorial” but that “one of the major drivers of cancers [are] the rising rates of obesity in the United States and across the globe.”
However, Karl Jablonowski, Ph.D., senior research scientist at Children’s Health Defense, said the USA Today story “dismantles its own solution” — because some doctors noted that their younger cancer patients were frequently “healthy” before their diagnosis.
“The U.S. is ranked fourth in the world for age-standardized incidence of cancer — 367 per 100,000 — and 19th for adult obesity (42.7%),” Jablonowski said. “The cancer epidemic is way beyond diet and exercise.”
USA Today cited figures from an American Cancer Society (ACS) study, published in The Lancet in August. According to the study, 17 types of cancer — including breast, colorectal, liver, gastric, ovarian and pancreatic cancer — are rising among younger adults. Mortality trends connected to some cancers have also increased.
USA Today also listed celebrities with recent cancer diagnoses — including Princess Kate, Elle Macpherson, Jenna Fischer and Olivia Munn — all Gen Xers (born between 1965 and 1980) or millennials (born between 1981 and 1996).
The article recommended younger adults be vigilant about their health. Experts who spoke with The Defender welcomed this message. However, they criticized what they said was an attempt to normalize rising cancer rates among young adults while ignoring other possible underlying causes, including vaccines.
“If you normalize a disease, you will alter the health behaviors addressing the disease,” Jablonowski said. “If you believe cancer is inevitable or occurs at random, then you believe your health behavior has no impact on the chances of developing cancer.”
Dr. Margaret Christensen, a clinical educator and co-founder of the Carpathia Collaborative, said USA Today’s recommendations that younger people engage in “fine-tuning” their “diet and exercise routines,” stay up-to-date on cancer screenings and visit their doctor regularly, are important.
“But where is the information on prevention?” Christensen asked. “Nothing is mentioned about the toxic chemicals and ultra-processed foods and antibiotics in the food supply that are impairing our immune system to begin with.”
There’s been a ‘sea change in the cancer message’
Many doctors and scientists noted the timing of rising cancer rates among young adults.
Dr. Angus Dalgleish, professor of oncology at St. George’s, University of London, told The Defender, “Colorectal [cancer] has been slowly rising in young people for well over a decade and probably more. However, there has been an inflection in the rate of rise from mid-2021. This is worldwide.”
John Beaudoin Sr., author of “The Real CdC” and “THE CDC MEMORANDUM,” told The Defender that while incidence rates for such cancers have risen for a decade, “the change in rate or rise is what decries a new issue introduced into society.”
Beaudoin said that if the annual increase was 2% per year consistent with a 2% population increase, that is understandable. “But if the rate then goes to a 4% annual increase, then there is a major issue. The rate doubled and is not consistent with population increase.”
Dr. Pierre Kory, founder of the Leading Edge Clinic and president emeritus and co-founder of the Front Line COVID-19 Critical Care Alliance (FLCCC), agreed. He said the USA Today report and the study in The Lancet mark “a sea change in the cancer message.”
Childhood vaccination ‘set the scene’ for rising young adult cancer rates
According to USA Today, there’s “no exact cause known for the rise in cancers among young people,” although “researchers are trying to figure it out.”
However, the article suggested that environmental factors, namely “changes to our microbiome over time — the environment, air, water, etc.” — may be partly responsible.
Christensen agreed, at least in part. “The same factors — environmental toxins in the food, water, air and many medications that cause insulin resistance and obesity — are causing cancers,” she said. “However, even in countries with lower rates of obesity, we are still seeing increased levels of cancers in younger folks.”
With environmental factors and obesity accounting only partially for the rising onset of cancer in younger adults, experts told The Defender vaccines likely contribute significantly to this increase.
“This has led me to look at childhood vaccines and I am afraid they have set the scene,” Dalgleish said. “There are now far too many. The adjuvants alone correlate with autism and ADHD,” attention-deficit/hyperactivity disorder.
“The chronic inflammatory states recorded after some of the joint vaccines are highly likely to boost the induction of early cancer,” Dalgleish said.
Dr. Paul Marik, co-founder of the FLCCC, said he believes COVID-19 vaccines may have contributed to the more recent increases in cancer incidence recorded by the CDC.
“The rapid increase in cancers was noted in 2021, 2022 and 2023 after the rollout of the mRNA jabs,” said Marik, author of “Cancer Care: The Role of Repurposed Drugs and Metabolic Interventions in Treating Cancer.”
He added:
“There is strong mechanistic data to explain how the jabs may lead to cancer. This association is strong. There does not appear to be another plausible explanation. Obesity rates have increased slowly [and] cannot explain the massive increase in cancers noted recently.”
Christensen said USA Today and organizations like the ACS “are dancing around the elephant in the room” by “not wanting to make the connection to the vaccines while stating the obvious problems we can’t ignore.”
“Mainstream media have been completely negligent, in my view, for not holding our concerns regarding the vaccines and cancer to account,” Dalgleish said.
Instead of ignoring the problem, “The concept of turbo cancer needs to be accepted,” Marik said. “More research is required to more precisely determine who is at risk, what the incidence is and how to prevent and treat this disease.”
“The best way to stop the young person’s cancer epidemic is to stop the cause,” Jablonowski said.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Congressional Investigation into Authors of ‘Disinformation Dozen’ Intensifies
By Michael Nevradakis, Ph.D. | The Defender | November 15, 2024
The Center for Countering Digital Hate (CCDH), authors of the “Disinformation Dozen,” faces a Nov. 21 deadline to provide Congress with documents related to its alleged collusion with the Biden administration and social media platforms to censor online users.
Rep. Jim Jordan (R-Ohio), chairman of the House Judiciary Committee, on Nov. 7 subpoenaed CCDH as part of an ongoing congressional investigation, launched in August 2023, into the nonprofit’s censorship-related activities.
The subpoena requests all communications and documents “between or among CCDH, the Executive Branch, or third parties, including social media companies, relating to the identification of groups, accounts, channels, or posts for moderation, deletion, suppression, restriction, or reduced circulation.”
The subpoena also requests all records, notes, and other “documents of interactions between or among CCDH and the Executive Branch referring or relating to ‘killing’ or taking adverse action against Elon Musk’s X social media platform.”
https://twitter.com/elonmusk/status/1854563397859193136
CCDH previously included Kennedy on its “Disinformation Dozen” list, published in March 2021, of the 12 “leading online anti-vaxxers.”
Leaked CCDH documents released last month by investigative journalists Paul D. Thacker and Matt Taibbi revealed that CCDH sought to “kill” Twitter and launch “black ops” against Robert F. Kennedy Jr., President-elect Donald J. Trump’s nominee for secretary of the U.S. Department of Health and Human Services (HHS).
CCDH included Kennedy, founder of Children’s Health Defense (CHD), on its list of “The Disinformation Dozen” when he was still chairman of CHD.
“Black ops” are defined as a “secret mission or campaign carried out by a military, governmental or other organization, typically one in which the organization conceals or denies its involvement.”
A subsequent report by Taibbi and Thacker showed that CCDH employed tactics it initially developed to help U.K. Prime Minister Keir Starmer and the U.S. Democratic Party, to target Musk, Kennedy and others.
CCDH used ‘explicit military terminology’ to target speech
Thacker told The Defender the leaked documents “definitely spurred” Jordan’s subpoena.
Sayer Ji, the founder of GreenMedInfo, was also listed among “The Disinformation Dozen.” He said the leaked documents were “chilling” and that CCDH’s efforts were part of “the largest coordinated foreign influence operation targeting American speech since 1776.”
Ji told The Defender :
“The leaked documents confirm what we experienced firsthand: CCDH wasn’t just targeting 12 individuals — we were test cases for deploying military-grade psychological operations against civilians at scale.
“Just as the British Crown once used seditious libel laws to silence colonial dissent, CCDH’s operation expanded to silence hundreds of millions globally, from doctors sharing clinical observations to parents discussing vaccine injuries.”
Ohio physician Dr. Sherri Tenpenny, also on “The Disinformation Dozen” list, told The Defender, “The exposure of the manipulation that went on behind the scenes to silence us is what we suspected, and now we know … We have the sad last laugh against their attacks. They are the ones with blood on their hands.”
Ji said CCDH’s internal communications reveal not just bias, “but explicit military terminology — ‘black ops,’ ‘target acquisition,’ ‘strategic deployment’ — coordinated between Five Eyes networks and dark money interests to target constitutionally protected speech.”
Writing on GreenMedInfo, Ji said, “CCDH’s ‘black ops’ approach includes coordinated media smears, economic isolation, and digital censorship.” Ji said CCDH’s activities represent “a new level of institutionalized power directed at civilian targets, often bypassing constitutional safeguards.”
Thacker said Jordan’s investigation should expand to include CCDH’s “black ops.”
“I don’t want to speculate on what CCDH was doing with ‘black ops’ against Kennedy,” Thacker said. “I think that should be explored by a congressional committee, with CCDH CEO Imran Ahmed put under oath,” Thacker said.
CCDH facing multiple lawsuits, possible Trump administration investigation
Jordan’s subpoena is the latest in a series of legal challenges for CCDH. According to GreenMedInfo, the organization faces several lawsuits and government investigations.
Following last month’s CCDH document leak, the Trump campaign said an investigation into CCDH “will be at the top of the list.”
The campaign also filed a complaint against the Harris campaign with the Federal Election Commission, “for making and accepting illegal foreign national contributions” — namely, from the U.K. Labour Party.
This followed the release of evidence indicating that the Biden administration coordinated with the U.K. Foreign Office as part of what GreenMedInfo described “as a systematic censorship regime involving CCDH and affiliated organizations.”
A lawsuit Musk filed against CCDH in July 2023 for allegedly illegally obtaining data and using it in a “scare campaign” to deter advertisers from X will likely proceed on appeal. A federal court initially dismissed the lawsuit in March.
Discovery in the Missouri v. Biden free speech lawsuit may also “shed further light and legal scrutiny on the critical role that CCDH played in allegedly suppressing and violating the civil liberties of U.S. citizens,” according to GreenMedInfo.
CCDH, others flee X in protest
Earlier this week, CCDH deleted its account on X, the platform it wanted to “kill.”
Writing on Substack, Ji said CCDH’s departure from X, during the same week Trump nominated Kennedy to lead HHS, represents a “seismic shift” and marks “a watershed moment, signaling the unraveling of entrenched systems of control and the rise of a new era for health freedom and open discourse.”
Several other left-leaning organizations and individuals, including The Guardian and journalist Don Lemon, also said they will stop using X, after Trump tapped Musk to lead a federal agency tasked with increasing government efficiency.
According to NBC News, many ordinary users are also fleeing X, citing “bots, partisan advertisements and harassment, which they all felt reached a tipping point when Donald Trump was elected president last week with Musk’s support.”
But according to Adweek, X’s former top advertisers, including Comcast, IBM, Disney, Warner Bros. Discovery and Lionsgate Entertainment, resumed ad spending on the platform this year, but at “much lower rates” than before.
“Elon Musk’s ties with Donald Trump might spur some advertisers to think spending on X is good for business,” Adweek reported.
Thacker said CCDH’s deletion of its X account was “aligned” with the departure of “other organizations and ‘journalists’ aligned with the Democratic Party.” He said it appears to have been a “coordinated protest.”
Ji said organizations like CCDH view X “as an existential threat.” He added:
“Having experienced both Twitter 1.0’s AI-driven censorship system and X’s more open environment, I understand exactly why CCDH sees X as an existential threat. X represents what Twitter 1.0’s embedded censorship infrastructure was designed to prevent: a truly free digital public square.
“Under Musk’s commitment to free speech, their tactical advantage disappeared. They’re not leaving because X is toxic. They’re leaving because they can’t control it.”
Online censorship ‘may no longer be sustainable under intensified scrutiny’
According to GreenMedInfo, CCDH’s departure from X “appears to reflect an internal recognition that their operational model — characterized by critics as a US-U.K. intelligence ‘cut-out’ facilitating unconstitutional suppression of civil liberties — may no longer be sustainable under intensified scrutiny.”
In recent months, several mainstream media outlets have corrected stories that relied upon CCDH reports claiming “The Disinformation Dozen” was responsible for up to two-thirds of vaccine-related “misinformation” online.
According to Thacker, this reflects an increasing awareness by such outlets that readers are turning their backs on such reporting.
“The outlets that promoted CCDH propaganda are being investigated by their own readers, who are fleeing in droves. Readers are voting against this type of propaganda by refusing to subscribe to these media outlets,” Thacker said.
Yet, “many outlets continue to host these demonstrably false narratives without correction,” Ji said.
According to Ji, these false narratives resulted in medical professionals fearing the loss of their licenses for expressing non-establishment views, self-censorship among scientists “to avoid career destruction,” suppression of “critical public health discussions” and the labeling of millions of posts as “misinformation.”
“This isn’t just about suppressing speech. It’s about establishing a new form of digital control that echoes the colonial-era suppression our founders fought against,” Ji said.
“CCDH has polluted political discourse by pretending there is some absolute definition of the term ‘misinformation’ and that they hold the dictionary,” Thacker said. “That’s nonsense. They spread hate and misinformation to attack perceived political enemies of the Democratic Party.”
Ji called upon Congress to investigate “The full scope of those silenced beyond the ‘Disinformation Dozen,’” the “systematic suppression of scientific debate,” “media organizations’ role in amplifying foreign influence operations” and “dark money funding networks” supporting such organizations.
Thacker said Congress should examine possible CCDH violations of the Foreign Agents Registration Act. “We need to also look at how much foreign money they took in and whether we as a nation are comfortable with foreign influence trying to alter the law and political discussions.”
“The fight isn’t just about correcting past wrongs or personal vindication. It’s about preserving fundamental rights to free speech and scientific inquiry in the digital age,” Ji said. “If we don’t address this systematic abuse of power, we risk surrendering the very freedoms our founders fought to establish.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Dr. Mike Yeadon – They Knew Precisely What Their Injections Were Going to Do to People
Resistance GB | November 10, 2024
VIENNA – Dr Mike Yeadon, former Vice President of Pfizer addresses the Impfopfer Victim Summit in Vienna Austria (09/11/24), introduced by Fiona Rose Diamond of Covileaks.
TRANSCRIPT:
My name is Dr. Mike Yeadon and in the next 10 to 15 minutes I’m going to focus on one major point which is that the purported “vaccines” against this alleged illness, COVID-19 were in my view deliberately designed intentionally to injure, kill and, and reduce fertility.
Now this is an allegation I’ve been making for around three and a half years. In that time, if I was wrong, ladies and gentlemen, I think numerous scientists would have rebutted what I’ve said in writing and in video. And if I was wrong, I would have expected the drug companies whose products I am maligning to have sought and secured a court injunction to stop me repeating these allegations. Neither of those things have ever happened.
What has happened instead is that I have been extraordinarily censored and smeared sideways. And I think I offer that to you as strong evidence that I may be “over the target”, at least in relation to these injectable products that have definitely injured and killed many people.
So first just brief few words of introduction in terms of credentials. So Mike Yeadon, I’ve been a professional research scientist for over 30 years in the pharmaceutical industry and in biotech. My first degree was in biochemistry and toxicology. It was a joint honours degree. I got a first, then I did a second degree, a PhD. It’s a research based piece of work lasting three years and my focus was respiratory pharmacology, the study of impact of drugs on respiration and so on. And that led into my career where I became a senior research scientist responsible for new drugs to treat allergic, respiratory and later dermatology diseases.
I was at one point Vice President and the most senior research person within Pfizer Global R&D, and I left in 2011. And for 10 years after that, seven of those I was founder and CEO of a biotech called ZIARCO which was acquired by Novartis in 2017, since when I’ve been a consultant although I’ve discontinued those activities in the last four and a half years or so.
So I’ve not earned a penny from speaking out in the last four and a half years and I don’t want to either. There is a longer video by me recorded a month or so ago, 22 minutes long and it’s called Silver Bullet and it’s on my telegram channel and I hope rather more widely.
But today I’m just going to focus on the design and effects of these so called vaccines. So I’ve been involved all of my professional life with other talented people trying to design and test potential new treatments for respiratory disease and as I say later on dermatology applications. So I can tell you that this, with my background in toxicology and my own research experience, 30 years in the industry, this qualifies me, I think better than any other commentator to evaluate what was in the minds of the people who designed these products.
Let me tell you that every component in a medicine is chosen. It’s chosen to be there. It’s not random. It’s chosen to be there to achieve some purpose, that’s normal, perhaps to help a drug dissolve, to be absorbed, to persist in your blood, or to leave your body quickly to penetrate the brain if it was a neurological drug, or to stay close to the lung if it was an inhaled drug. So it’s quite normal to make choices with objectives in mind. So I believe the intentions of the designers are written into the choices they made, the structures and components, formulation of these products.
So I’m going to use those skills, as it were, to back calculate what was in their mind, what objectives did they have when they chose these structures and formulations.
So I’m going to just say, before I get into that, just one thing about these so called “vaccines”. My experience of the industry over 30 years tells me it is formally impossible to invent, research, test, evaluate, manufacture, gain authorization for, and launch a complex new biological product in under a year. It’s formally impossible. I don’t care how much money and people you put on it, there are a series of linear steps which, when taken together, unless you miss some out, cannot be completed under several years. So if someone told you they had brought a brand new airline to market with new engines in under a year, I think you would know it’s formally impossible to do a clean sheet design, to stress test, to manufacture, to test, to flight test, optimise the engines and get regulatory clearance and be ready to take you across the Atlantic in under a year. And of course it’s never been done and it’s never been done with complex biological products in under a year. So whatever else they did, they didn’t do what they said because it cannot be done in under a year.
Secondly, and I’ll come to the examples in a moment, there are in these products numerous features which in my view, my peers, people like me, people with my training and experience would know for sure would give rise to the toxicities that I pointed out in 2020. They’re not, they don’t require particular skills you need to know how to do drug discovery and what can go wrong. But I’m not acting like a complete genius in spotting these, just someone who is a professional from this industry that has pointed out numerous features built in by choice that I believe I think they obviously confer toxicology, toxicity to the recipients. And as I’ve said, people designing these, people like me in wherever they were, pharmaceutical industries or the military, knew these things were going to happen. And that’s why I say it’s intentional.
I’m going to give you three examples that you can go and test. So the first one is these are so called gene based products, that is they’ve got a string of genetic information in them. Now there aren’t any products like that that are in routine use anywhere in the world. So they’re brand new technology. But what you’ll remember they told you that they do is they cause your body to make as a protein whatever was in that genetic code. Now it’s absolutely basic immunology. How is it, do you think your body knows that what’s inside of you is meant to be there and you don’t attack it? And yet if something gets into your body from the outside or a tumour form, something that shouldn’t be in you, your body can recognise that that’s foreign or non-self and can attack it. And the answer is you tolerate everything that’s meant to be inside your body. When you’re in your mum’s womb, we, we ruled out the ability to attack ourselves. Unless you get an autoimmune disease in later life, you play nice with yourself until something gets inside you or something goes wrong inside you. So ladies and gentlemen, if you are injected with a genetic sequence that causes you to manufacture a foreign protein, whether it’s a virus or something out of a computer, it’s not you and it’s not meant to be in you, I assure you, your body recognises that it’s been invaded, something’s in there that shouldn’t be and it launches a fatal attack on every cell that it thinks has gone wrong. It’s trying to save you. So and that autoimmune reaction that destruction which your body is trying to, is doing because it’s trying to protect you, that will happen anywhere in your body, any cell, tissue, organ in your body where unluckily your dose of what was injected into you lands. So if it lands in your heart, you could get myocarditis or a heart attack. If it lands in your brain, you could get a stroke or neurological conditions. If it’s in your eyes, you could go blind. If it’s in your ovaries, it may sterilise you.
But that explains, in my view, a lot of the enormously diverse toxicity that’s been seen with these products. So that’s one, your body is being made to manufacture something that does not belong in it. And when that happens, everybody with the first lecture of immunology will understand why that happens. It’s not an accident, it’s in the design. It’s a deliberate choice.
The second one, then what was encoded in the so called “vaccines”, now we’re told it’s spike protein. I don’t think there is a natural spike protein, but proteins with sequences like that are known to be acutely toxic to blood cells, prompting blood clots to nerve cells, causing them to malfunction and probably other things I don’t know anything about. So that’s the second thing your body was making, was forced to make not only a foreign protein, something that didn’t belong in your body, you were, your body was forced to make something that was directly toxic to your body. And the person who chose that sequence knew that’s what the property of it was. It’s not an accident, it’s intentional.
Then the third one is absolutely shocking. It’s normal for drugs to be formulated that is to be wrapped in something. You’ll see them in capsules or tablets. They might have a coating. If it’s an inhaler, there might be some liquid with it so it can be propelled. In the case of these injectables, they were wrapped in really fatty globules called lipid nanoparticles, which means tiny little particles of fat. Lipid nanoparticles. Ladies and gentlemen, there were papers published as early as 2012, which I read a couple of years ago, that said that it is well understood in the industry by formulators that the payload that’s contained within lipid nanoparticles when injected into animals and people leads to a disproportionate deposition of the payload into your ovaries.
I remember the day I read that paper, I really couldn’t sleep. The person who chose to use lipid nanoparticles to formulate the Moderna and Pfizer products knew perfectly well that what they would do is allow them to drift all through your body, through membranes as if they weren’t there, and disproportionately deposit in your ovaries.
And given I’ve told you the first two things, which is that will induce your body to attack every cell in the body that follows the instructions. And that instruction by the way, is to make a poison, you should no longer be surprised that people have been injured and killed and had their fertility reduced. I wish I didn’t have to communicate this information. But there is no possibility that the people involved in designing these products did not know that they would have the effects that I predicted and that so many people have actually experienced it is intentional. There is ample evidence that this assault, which is not the only thing that’s ever happened, unfortunately it’s the first I noticed.
I was a so called normie until 2020. I believed everything I was told. But this is part of a long planned assault by powerful wealthy people operating above the level of nation. So I’m afraid organisations like the United Nations, the World Health Organisation, the Bank for International Settlements, the World Economic Forum are populated by the people who I believe have orchestrated this attack on humanity and they’re going to do it again. There are factories all around the world busy manufacturing these so called “vaccines” and formulating them in the way I just described. And they’re going to come up with contrived reasons why you need to roll your sleeve up and I’m telling you, for the love of God, please don’t do it. The only way we will push these people away is by speaking out as we see it and simply refusing to follow absurd instructions no matter what ostensible reason they come up with for you to do that..
So I mentioned I have been subject to astonishing censorship and smearing. And that’s true. I’ve always said, if you hear me, please repeat what I have said to other people. I’ve got a tiny reach because I’m censored and no one else is coming to save us. It’s just a small number of us who are not willing to stay quiet while this is done to us. But it’s part of a wider deception. The pandemic lie is a major one. I don’t have time to go into it now, but see my other recording. But there wasn’t a pandemic. There’s never been a pandemic. They can’t happen. It’s a lie. The so called human induced climate change crisis, that’s all a lie as well. It’s the same people who put this together at the end of the 1960s, the Club of Rome, they chose these two topics of infectious disease and climate change to scare people because they realised it would force a response from above the level of nation. But I’m saying, stand on your own feet and tell them to get lost with their absurd lies.
And there’s a third lie which underlies these, and it’s they believe. They tell us we’ve been told all our lives, that the world is overpopulated. And it’s literally absurd if you’re up in an aeroplane within a few minutes, even over a busy city, the place is just full of cities and forests and fields. So that’s yet another lie. But I think that’s what’s driving them. They think there’s too many of us little people, and they seek to control us digitally and then eventually inject us to death. It’s only going to be stopped then by refusal to cooperate.
And that’s my testimony. I hope that was helpful too.
*************
More more info on Dr Mike Yeadon: https://t.me/DrMikeYeadonsolochannel
For more info on Covileaks: https://covileaks.co.uk/
More more info on Impfopfer: https://www.impfopfer.info
*************
Support us on Patreon:  / rgbpodcast
/ rgbpodcast
Join us on Telegram (news. updates & chat): https://t.me/ResistanceGB
Follow us on Twitter / X.com: https://x.com/gbresistance?lang=en
DNA Contamination in Vaccines: What Is It and Why Does It Matter?
By Brenda Baletti, Ph.D. | The Defender | November 8, 2024
Legacy media fact-checkers and regulators across the world repeatedly claim that DNA contamination in vaccines — and particularly in the mRNA COVID-19 vaccines — poses no risk to vaccine recipients.
Some have gone so far as to claim that concerns raised about this issue by countless researchers are “baseless,” “misinformation” and “conspiracy theory.”
They concede that both older vaccines and the newer mRNA vaccines can contain residual DNA leftover from the manufacturing process — but say that remnant DNA is “expected and considered safe” and that there are regulatory steps in place to make sure it occurs only in limited quantities.
The U.S. Food and Drug Administration (FDA) dismissed concerns published in the Journal of Inorganic Biochemistry about HPV (human papillomavirus) DNA fragments found in products like Merck’s Gardasil HPV vaccine. The agency claims the fragments are “not contaminants” and not a risk or a safety factor.
The Australian Therapeutic Goods Administration last month issued a statement saying that recent studies claiming mRNA vaccines are contaminated with excessive levels of DNA lack scientific rigor and that residual DNA has been in biotech products for a long time anyway.
Australian regulators emphasized that “the benefits of vaccination far outweigh the potential risks.”
But some scientists — including Karl Jablonowski, Ph.D., senior research scientist at Children’s Health Defense, who spoke with The Defender — say residual DNA in vaccines should not be dismissed — the danger he said stems from both known and unknown risks.
Jablonowski said those risks have long been present in many existing vaccines, but they are even greater in the mRNA vaccines. Through the lipid nanoparticles contained in the mRNA shots, the DNA fragments “have an open pass to every membrane in your body.”
Why does DNA contamination happen?
Biology is complex, Jablonowski told The Defender. Nothing in it is very pure, so there are contaminations in everything.
He said there have been problems with contaminants in vaccines since what the journal Pediatrics described as the “First Modern Medical Disaster” — when 13 children administered a contaminated diphtheria antitoxin died.
Today, vaccines are produced in several different ways, but living cells play a part in the manufacturing of most vaccines, Jablonowski explained. Vaccines typically work by introducing a weakened bacteria or virus, or pieces of them — often with an adjuvant to amplify its effect — into the body to trigger an immune response.
Viruses need living cells to grow, so viral vaccines use some kind of living cell in the production process. The viruses can be grown in bacteria, yeast, animal or human fetal cells, for example.
That DNA in those cells is typically destroyed or fragmented in the process of making the vaccine. However, the process might not eliminate all of it — some remnant, fragmented DNA can remain present.
The mRNA COVID-19 vaccines used a different process. Rather than introducing a viral protein, they introduced messenger RNA, which trains cells to produce the SARS-CoV-2 spike protein and the immune system recognizes that protein and produces antibodies.
The COVD-19 vaccines used an RNA-making enzyme — an RNA polymerase — which uses a DNA template to synthesize the RNA in a lab process called “in vitro transcription.”
The DNA used in the process first has to be amplified. Vaccine makers like Pfizer amplified the DNA for the vaccine using a plasmid. Plasmids are small circular pieces of DNA that reside in bacteria and get reproduced when a bacteria reproduces. For the COVID-19 vaccines, they used E. coli, a commonly used bacteria in vaccine production, for rapid amplification.
This DNA template comes with additional risk because the DNA of the plasmid used to create the template has to be removed from the vaccine before it can be injected into people.
Kevin McKernan, the researcher who first identified the DNA in the COVID-19 vaccines, found that the vaccine makers tried to get rid of that DNA by “chewing it up with an enzyme” called deoxyribonuclease or DNase, which breaks down DNA. However, they failed to completely eliminate it.
What are the potential dangers?
The potential risks of residual DNA in vaccines have been debated for decades without resolution, according to the World Health Organization (WHO). Some researchers claim the remnant DNA is inert. Others argue it is an important risk factor that may be oncogenic — cancer-causing — or infectious.
The immune system, a delicate system of sensors, has a threshold for how much foreign material it can tolerate in the body, Jablownoski said. When DNA is present outside of cells and in the bloodstream, it can initiate a powerful immune response — called an interferon response — which will aggressively seek out the harmful pathogen.
This can create an overblown immune system response that could be a vector for autoimmune issues related to vaccine contamination.
For example, pathologist and molecular gene detection expert Sin Hang Lee identified the residual RNA in the HPV vaccine Gardasil, which he tested for fragment DNA after a 13-year-old girl developed acute juvenile rheumatoid arthritis, Maryanne Demasi, Ph.D., reported.
In the Gardasil vaccine, Lee found the HPV DNA present bound tightly to the aluminum adjuvant. As a result it doesn’t easily break down as it should. Lee theorized that immune cells such as macrophages, which are laden with aluminum adjuvant, travel from the injection site through the blood to various organs.
According to Demasi, the HPV DNA that is bound to the adjuvant “can cause chronic immune-inflammatory reactions that lead to autoimmune conditions in some people.”
Jablonowski said the mRNA vaccines pose a new and more serious problem. That’s because before the introduction of the mRNA vaccine, foreign DNA had no mechanism to get inside of a cell. However, the lipid nanoparticles make that possible.
“The appropriate amount of foreign DNA inside the cell is zero,” Jablonowski said. “It can run amuck with all of the delicate biology necessary to operate a cell.”
Foreign DNA could cause cells to become diseased, it can disrupt regulation, and if the DNA is present at cell division, it could get inside the nucleus and create a host of problems, he said.
Some researchers have argued there is evidence this contaminant DNA could be linked to rising cancer rates.
What do the regulators say?
In 1985, the FDA set an upper limit of 10 picograms per dose. In 1987, the WHO ncreased its recommended limit to 100 picograms and then increased it again to 10 nanograms (i.e., 100 times higher) — a limit now adopted by the FDA, Demasi reported.
Researchers like Lee and McKernan say in the case of Gardasil, this limit doesn’t offer adequate protection, because the HPV DNA can be hard to detect when it binds to the adjuvant.
Jablonowski said when this threshold was set, regulators were only considering how much residual DNA might be in the bloodstream from vaccines — because at that time there wasn’t a mechanism for the DNA to get into the cell. But with mRNA vaccines, that threshold can likely pose a serious danger.
Why did DNA contamination become so controversial?
Researchers and scientists have had concerns about DNA contaminants in vaccines for decades. However, last year, genomics researcher McKernan reported finding that Pfizer’s COVID-19 vaccine is contaminated with plasmid DNA — which should not be present in an mRNA vaccine.
He said this raises concerns that the plasmid DNA could lead to cancers or autoimmune issues in some vaccine recipients.
After McKernan’s lab made its findings public, and other researchers confirmed them, Health Canada also confirmed that the Pfizer vaccine contains this DNA.
McKernan also reported that Pfizer concealed this information from regulators. In the manufacturing process for the drug’s clinical trials, Pfizer used PCR testing rather than the plasmid DNA it later used for mass production. So the first version of the drug — granted emergency use authorization by the FDA — didn’t contain the DNA.
It was later revealed that the Moderna vaccines used the same production method — so Moderna’s mRNA vaccines also were contaminated with the remnant DNA.
The issue quickly became politicized, with those claiming the vaccines are “safe and effective” calling the claims “misinformation” and a conspiracy theory, dubbed “plasmid-gate.”
Critics of the COVID-19 vaccines, like Florida Surgeon General Joseph A. Ladapo, called on regulators to address the issue.
The FDA said in a response letter that “based on a thorough assessment of the entire manufacturing process, FDA is confident in the quality, safety, and effectiveness of the COVID-19 vaccines.” However, the agency provided none of the evidence on which it based that conclusion.
Dr. Paul Offit, director of the Vaccine Education Center at Children’s Hospital of Philadelphia, who serves on an FDA advisory committee for the COVID vaccines — and who is himself a vaccine inventor and patent holder on RotaTeq, the rotavirus vaccine recommended for universal use in infants by the Centers for Disease Control and Prevention (CDC) — in a YouTube video dismissed the concerns raised by MeKernan, Ladapo and others.
He said it is possible that there is fragment DNA in the vaccines, but that it is impossible for the DNA fragments to enter people’s cells or to cause disease.
Jablonowski said that for Offit’s explanation to make sense, biology would have to be very simple and straightforward. But it’s not, he said. “Biology is really messy and there are almost always exceptions.”
The immune system is the second-most complicated system, and there is a lot we don’t know about it, he added.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
COVID Vaccines Pose 112,000% Greater Risk of Brain Clots, Strokes Than Flu Shots
By Michael Nevradakis, Ph.D. | The Defender | November 7, 2024
COVID-19 vaccines pose a 112,000% greater risk of brain clots and strokes than flu vaccines and a 20,700% greater risk of those symptoms than all other vaccines combined, according to a peer-reviewed study that calls for a global moratorium on the vaccines.
The study, published last week in the International Journal of Innovative Research in Medical Science, found reports of 5,137 cases of cerebral thromboembolism after COVID-19 shots over 36 months. This compares to 52 reported cases following flu vaccination and 282 cases for all vaccines over the past 34 years.
According to the study, this represents an “alarming breach in the safety signal threshold concerning cerebral thrombosis adverse events” following COVID-19 vaccination.
The study’s authors — independent researcher Claire Rogers, obstetrician and gynecologist Dr. James A. Thorp, independent researcher Kirstin Cosgrove and cardiologist Dr. Peter McCullough — used data from the U.S. government’s Vaccine Adverse Event Reporting System (VAERS), for their analysis.
The data also indicated 9,821 reports of atrial fibrillation — an irregular heart rhythm that is “the most common identifiable cause of cerebral arterial thromboembolism” — following COVID-19 vaccination in 41 months, compared to 797 cases reported in 34 years for all other vaccines combined.
Rogers told The Defender the findings confirm anecdotal evidence of an increased incidence of stroke seen during and after the COVID-19 pandemic.
Rogers said:
“Cerebral thrombosis case reports in VAERS substantially increased after the COVID vaccines. Not only have clinicians witnessed this in the hospital setting, but the average citizen has seen increased reports of stroke in celebrities, athletes and young people.”
McCullough told The Defender the study employed a “reasonable vaccine safety research strategy” by comparing “a new vaccine to the routine influenza vaccination as a ‘safe’ standard.” He said the results showed “horrific outcomes” following COVID-19 vaccination.
These outcomes led the study’s authors to call for an immediate global moratorium on the use of COVID-19 vaccines “to mitigate further risk with an absolute contraindication in women of reproductive age.”
“Our study joins the growing chorus of analyses calling for all COVID-19 vaccines to be removed from the market,” McCullough said. The withdrawal “should be the first priority” for the next administration.
Spike protein implicated in increased stroke risk
According to the study, the spike protein found in the SARS-CoV-2 virus and COVID-19 vaccines is likely a significant contributor to brain clots and strokes.
“Early in the COVID pandemic, it became evident that there was a thrombogenic effect of the Sars-CoV-2 virus and it is now believed that the spike proteins [are] one of the major contributors to this thrombogenic effect,” the study said.
According to the study, the original strain of the virus led to “a variety of severe thromboembolic events.” However over time, “natural evolution may have resulted in less virulent strains.”
This original risk was replaced by an increase in the incidence of microclots, “affecting the smaller vessels in the circulatory system.” The study noted that it is “widely understood that cumulative exposure to the spike protein” leads to an increased risk of such clots in patients.
According to Rogers, “One mechanism by which the spike protein is thought to contribute to this pathogenesis is by triggering endothelial dysfunction” — a condition that exists when coronary arteries are constricted even though there isn’t a physical blockage.
The study did not compare the different COVID-19 vaccine types — the Pfizer and Moderna mRNA vaccines, and the Johnson & Johnson (Janssen) and AstraZeneca adenovirus-based vaccines. Rogers noted, though, that the adenovirus vaccines were withdrawn in the U.S. and Europe following reports of blood clots.
Noting that VAERS “is regulated, owned, and maintained” by the Centers for Disease Control and Prevention (CDC) and the U.S. Food and Drug Administration (FDA), the study addressed the relative advantages and disadvantages of using this database for such an analysis.
“Despite the bias of the CDC/FDA and their attempts to hide, conceal, and ‘throttle’ the deaths and injuries caused by the COVID-19 vaccines, there remains an unprecedented breach of the safety signal using their own criteria,” the study said.
This safety signal is evident even though the “relative underreporting factor … in VAERS is thought to be in the range of 30-100.”
A 2011 Harvard study found that less than 1% of all adverse events are reported to VAERS.
Calls intensify for a moratorium on COVID shots
Karl Jablonowski, Ph.D., senior research scientist at Children’s Health Defense, told The Defender that despite “the limitations of using VAERS data to infer risk,” he was “startled” by the study’s results. He said the study adds to the growing number of voices calling for a moratorium on the administration of the COVID-19 vaccines.
“While one study does not justify a moratorium, a cacophony of studies does,” Jablonowski said.
According to the study, “There are now 3,580 studies published in peer-reviewed medical journals documenting injuries, disabilities, and deaths after COVID-19 vaccines,” strengthening calls for their withdrawal.
Last month, Idaho’s Southwest District Health said it would stop offering COVID-19 vaccines, following testimony by members of the local community and by experts including McCullough and Thorp.
This followed last month’s release of a Slovak government report calling mRNA shots “dangerous” and calling for their ban. Also last month, a town council in Western Australia called for a ban on mRNA products.
In January, Florida Surgeon General Joseph Ladapo called for a “halt in the use of COVID-19 mRNA vaccines” over safety concerns.
Psychotherapist Joseph Sansone, Ph.D., author of the “Ban the Jab” resolution adopted by 10 Florida counties, supported the study’s call for a moratorium on the COVID-19 vaccines.
He said:
“COVID-19 and mRNA nanoparticle injections are biological and technological weapons of mass destruction. It is time for the medical community to tell the truth and admit they were lied to like everybody else. These injections harm those injected and those not injected, via the shedding of this technology.
“All mRNA nanoparticle injections need to be prohibited immediately and there needs to be a thorough investigation into the criminals behind this attack on humanity.”
Organizations including the World Council for Health, Doctors for COVID Ethics and the Association of American Physicians and Surgeons have also called for a moratorium on the COVID-19 vaccines.
“COVID vaccine uptake by the public is at an all-time low,” Rogers said. “The need is no longer there for production of these products.”
Jablonowski said:
“A global moratorium on the COVID-19 vaccines would be a major step forward for humanity, not just in human health but for our humility.
“We would have to admit that we were fooled into taking a dangerous product and that our governments, scientists and pharmaceutical companies were all too willing to fool us. Our brighter future starts when we come to these terms.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Stunning Revelations in Massive Robert Koch Institute Leak
Breathtaking November 2 presentation in the German Parliament
By John Leake | Courageous Discourse | November 9, 2024
A massive leak of internal e-mails and memos from Germany’s Robert Koch Institute (federal agency and research institute for controlling infectious disease) reveals that the institute’s scientists understood that virtually every aspect of the COVID-19 pandemic response was NOT guided by science, but by political machinations to spread fear, control the population, and promote the experimental vaccines. On November 2, 2024, Professor Stefan Homburg gave a presentation on the leaked documents in the German Parliament.
Since the beginning of the pandemic, I have suspected that governments throughout the world were committing the greatest organized fraud in history, but I still found Professor Homburg’s presentation to be absolutely breathtaking in the sheer ruthlessness of the lies and manipulation revealed in these leaked documents. Perhaps the most perfidious is a memo from September 28, 2020.

Translation: 28.09.2020: FDA approval [of COVID-19 vaccines] before the US Elections is not desired, also not by European authorities.
In other words, both U.S. and European public health authorities were afraid the COVID-19 vaccines—which had been heralded as the forthcoming saviors of mankind—could help to get Donald Trump elected if they were approved before the election. And so they found it expedient to withhold approval until after the election, even though they claimed the vaccines could save millions of lives.
I strongly encourage everyone to watch the video presentation (in German with English subtitles) and to share it far and wide.
A whistleblower obtained 10GB from Robert-Koch-Institute, the German CDC. This so-called RKI-Leak reveals that Covid was a scam from start to finish. The presentation took place in the second largest room of the German Bundestag, which is actually intended for committees of inquiry. Recorded 2 November 2024 in Berlin, English subtitles provided by the speaker.
Internet sources:
The RKI-Leak The Federal Ministry of Health has confirmed the authenticity of the leak. You can download the entire material anonoymously and free of charge from https://rki-transparenzbericht.de/
Here is a convenient search tool: https://www.rkileak.com/
Lauterbach‘s Post on X: https://x.com/Karl_Lauterbach/status/…
Lauterbach and political independence https://www.bild.de/politik/inland/rk… Spahn: Test, test, test https://www.aerztezeitung.de/Politik/…
CNN reporting emergency authorization https://edition.cnn.com/2020/12/11/he…
RKI-Grapah Influenca like illnesses (ILI) https://influenza.rki.de/Wochenberich…
WDR-Graph vaccine development https://www.quarks.de/gesundheit/medi…
Lauterbach on the unvaccinated https://www.welt.de/politik/deutschla…
Citation Dr. Brigitte Keller-Stanislawki https://www.berliner-zeitung.de/gesun…
Steinmeier, Merkel, Scholz, Lauterbach, Spahn were allegedly vaccinated https://www.bundespraesident.de/Share… https://www.aerzteblatt.de/nachrichte… https://www.spiegel.de/politik/deutsc… Lauterbach on child vaccination https://x.com/Karl_Lauterbach/status/…
RKI risk levels (deleted, only available from the internet archive) Go to https://archive.ph and type:https:/www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Risikobewertung.html Intensive care unit occupation https://infektionsradar.gesund.bund.d…
The CDC Planned Quarantine Camps Nationwide
By Jeffrey A Tucker | Brownstone Institute | November 7, 2024
No matter how bad you think Covid policies were, they were intended to be worse.
Consider the vaccine passports alone. Six cities were locked down to include only the vaccinated in public indoor places. They were New York City, Boston, Chicago, New Orleans, Washington, D.C., and Seattle. The plan was to enforce this with a vaccine passport. It broke. Once the news leaked that the shot didn’t stop infection or transmission, the planners lost public support and the scheme collapsed.
It was undoubtedly planned to be permanent and nationwide if not worldwide. Instead, the scheme had to be dialed back.
Features of the CDC’s edicts did incredible damage. It imposed the rent moratorium. It decreed the ridiculous “six feet of distance” and mask mandates. It forced Plexiglas as the interface for commercial transactions. It implied that mail-in balloting must be the norm, which probably flipped the election. It delayed the reopening as long as possible. It was sadistic.
Even with all that, worse was planned. On July 26, 2020, with the George Floyd riots having finally settled down, the CDC issued a plan for establishing nationwide quarantine camps. People were to be isolated, given only food and some cleaning supplies. They would be banned from participating in any religious services. The plan included contingencies for preventing suicide. There were no provisions made for any legal appeals or even the right to legal counsel.
The plan’s authors were unnamed but included 26 footnotes. It was completely official. The document was only removed on about March 26, 2023. During the entire intervening time, the plan survived on the CDC’s public site with little to no public notice or controversy.
It was called “Interim Operational Considerations for Implementing the Shielding Approach to Prevent COVID-19 Infections in Humanitarian Settings.”
“This document presents considerations from the perspective of the U.S. Centers for Disease Control & Prevention (CDC) for implementing the shielding approach in humanitarian settings as outlined in guidance documents focused on camps, displaced populations and low-resource settings. This approach has never been documented and has raised questions and concerns among humanitarian partners who support response activities in these settings. The purpose of this document is to highlight potential implementation challenges of the shielding approach from CDC’s perspective and guide thinking around implementation in the absence of empirical data. Considerations are based on current evidence known about the transmission and severity of coronavirus disease 2019 (COVID-19) and may need to be revised as more information becomes available.”
By absence of empirical data, the meaning is: nothing like this has ever been tried. The point of the document was to map out how it could be possible and alert authorities to possible pitfalls to be avoided.
The meaning of “shielding” is “to reduce the number of severe Covid-19 cases by limiting contact between individuals at higher risk of developing severe disease (‘high-risk’) and the general population (‘low-risk’). High-risk individuals would be temporarily relocated to safe or ‘green zones’ established at the household, neighborhood, camp/sector, or community level depending on the context and setting. They would have minimal contact with family members and other low-risk residents.”
In other words, this is what used to be concentration camps.
Who are these people who would be rounded up? They are “older adults and people of any age who have serious underlying medical conditions.” Who determines this? Public health authorities. The purpose? The CDC explains: “physically separating high-risk individuals from the general population” allows authorities “to prioritize the use of the limited available resources.”
This sounds a lot like condemning people to death in the name of protecting them.
The model establishes three levels. First is the household level. Here high-risk people are“physically isolated from other household members.” That alone is objectionable. Elders need people to take care of them. They need love and to be surrounded by family. The CDC should never imagine that it would intervene in households to force old people into separate places.
The model jumps from households to the “neighborhood level.” Here we have the same approach: forced separation of those deemed vulnerable.
From there, the model jumps again to the “camp/sector level.” Here it is different. “A group of shelters such as schools, community buildings within a camp/sector (max 50 high-risk individuals per single green zone) where high-risk individuals are physically isolated together. One entry point is used for exchange of food, supplies, etc. A meeting area is used for residents and visitors to interact while practicing physical distancing (2 meters). No movement into or outside the green zone.”
Yes, you read that correctly. The CDC is here proposing concentration camps for the sick or anyone they deem to be in danger of medically significant consequences of infection.
Further: “to minimize external contact, each green zone should include able-bodied high-risk individuals capable of caring for residents who have disabilities or are less mobile. Otherwise, designate low-risk individuals for these tasks, preferably who have recovered from confirmed COVID-19 and are assumed to be immune.”
The plan says in passing, contradicting thousands of years of experience, “Currently, we do not know if prior infection confers immunity.” Therefore the only solution is to minimize all exposure throughout the whole population. Getting sick is criminalized.
These camps require a “dedicated staff” to “monitor each green zone. Monitoring includes both adherence to protocols and potential adverse effects or outcomes due to isolation and stigma. It may be necessary to assign someone within the green zone, if feasible, to minimize movement in/out of green zones.”
The people housed in these camps need to have good explanations of why they are denied even basic religious freedom. The report explains:
“Proactive planning ahead of time, including strong community engagement and risk communication is needed to better understand the issues and concerns of restricting individuals from participating in communal practices because they are being shielded. Failure to do so could lead to both interpersonal and communal violence.”
Further, there must be some mechanisms to prohibit suicide:
Additional stress and worry are common during any epidemic and may be more pronounced with COVID-19 due to the novelty of the disease and increased fear of infection, increased childcare responsibilities due to school closures, and loss of livelihoods. Thus, in addition to the risk of stigmatization and feeling of isolation, this shielding approach may have an important psychological impact and may lead to significant emotional distress, exacerbate existing mental illness or contribute to anxiety, depression, helplessness, grief, substance abuse, or thoughts of suicide among those who are separated or have been left behind. Shielded individuals with concurrent severe mental health conditions should not be left alone. There must be a caregiver allocated to them to prevent further protection risks such as neglect and abuse.
The biggest risk, the document explains, is as follows:
“While the shielding approach is not meant to be coercive, it may appear forced or be misunderstood in humanitarian settings.”
(It should go without saying but this “shielding” approach suggested here has nothing to do with focused protection of the Great Barrington Declaration. Focused protection specifically says: “schools and universities should be open for in-person teaching. Extracurricular activities, such as sports, should be resumed. Young low-risk adults should work normally, rather than from home. Restaurants and other businesses should open. Arts, music, sport and other cultural activities should resume. People who are more at risk may participate if they wish, while society as a whole enjoys the protection conferred upon the vulnerable by those who have built up herd immunity.”)
In four years of research, and encountering truly shocking documents and evidence of what happened in the Covid years, this one certainly ranks up at the top of the list of totalitarian schemes for pathogenic control prior to vaccination. It is quite simply mind-blowing that such a scheme could ever be contemplated.
Who wrote it? What kind of deep institutional pathology exists that enabled this to be contemplated? The CDC has 10,600 full-time employees and contractors and a budget of $11.5 billion. In light of this report, and everything else that has gone on there for four years, both numbers should be zero.
Jeffrey Tucker is Founder, Author, and President at Brownstone Institute. He is also Senior Economics Columnist for Epoch Times, author of 10 books, including Life After Lockdown, and many thousands of articles in the scholarly and popular press.
Appeals Court Rules Against CHD, RFK Jr. in Landmark Censorship Case
By Brenda Baletti, Ph.D. | The Defender | November 5, 2024
Children’s Health Defense (CHD) is weighing next steps after an appeals court late Monday ruled against CHD and Robert F. Kennedy Jr. in their landmark censorship case against the Biden administration.
The 5th Circuit U.S. Court of Appeals ruled the plaintiffs — CHD, Kennedy and news consumer Connie Sampognaro — have no legal basis to sue the Biden administration for pressuring tech giants to censor their social media posts.
Monday’s ruling overturned a lower court decision, made in August by Judge Terry Doughty from the U.S. District Court for the Western District of Louisiana, who ruled the plaintiffs do have standing to sue the administration.
Standing is the legal doctrine requiring plaintiffs to show they’ve suffered direct and concrete injuries and that those injuries could be redressed in court in order to sue.
The lawsuit, Kennedy v. Biden — filed in March 2023 — alleges top government officials and federal agencies “waged a systematic, concerted campaign” to compel the nation’s three largest social media companies to censor their constitutionally protected speech.
“We are, of course, disappointed with and disagree with the 5th Circuit’s decision here,” CHD General Counsel Kim Mack Rosenberg told The Defender.
Mack Rosenberg added:
“We believe that the additional evidence CHD presented more than sufficiently established standing for Children’s Health Defense. We pointed the court to ongoing censorship activities by the government and we demonstrated that the government has a significant and improper role in the social media platforms’ censorship of CHD.”
Mack Rosenberg said that plaintiffs are weighing the next steps.
Censorship lawsuits against Biden administration continue to drag on
The decision marks the latest major development in the ongoing anti-censorship litigation against the Biden administration.
Two separate cases — Murthy v. Missouri (originally Missouri v. Biden) and Kennedy v. Biden were filed in May 2022 and March 2023 respectively against the Biden administration in Louisiana District Court.
The cases have different plaintiffs but make similar allegations: that the administration colluded with social media companies to censor plaintiffs’ speech.
Both cases cited the disclosures of secret communications between social media companies and federal officials — in the “Twitter Files,” other lawsuits and news reports — revealing threats by President Joe Biden and other top officials against social media companies if they failed to aggressively censor content that ran counter to official narratives, including those on COVID-19 origins and vaccines.
Doughty consolidated the two cases, allowing them to share processes, such as discovery of evidence. However, the courts continued to hear and rule on the cases separately.
Plaintiffs in Missouri v. Biden sought and won a preliminary injunction in the lower court to prevent the Biden administration from pressuring social media companies to censor certain content. The administration appealed in July 2023 and in June 2024, the U.S. Supreme Court struck down the injunction.
The Supreme Court ruled the plaintiffs lacked standing because there was insufficient evidence they were directly injured by the government’s actions.
The Louisiana District Court later granted a preliminary injunction in the Kennedy v. Biden case; however, the court simultaneously issued a stay pending the Supreme Court’s decision on the injunction in Missouri v. Biden.
After the Supreme Court struck down the injunction in Missouri v. Biden, the 5th Circuit sent the Kennedy v. Biden case back to the District Court to rule on standing, where plaintiffs presented supplementary evidence.
The Kennedy v. Biden plaintiffs argued they had a stronger case for standing than the plaintiffs in Missouri v. Biden because there is explicit evidence that both Kennedy and CHD were specific targets of censorship and that they continue to be censored.
In a declaration by CHD President Mary Holland, Holland said CHD was deplatformed from Facebook and YouTube in August and September 2021 and continues to be deplatformed from major social media sites to this day.
Doughty found the government’s conduct is traceable to direct statements and instructions to social media platforms, including Facebook, Instagram and YouTube. He said Kennedy and CHD showed they faced ongoing injuries that could be redressed by the court.
In October, a three-judge panel in the 5th Circuit heard oral arguments in the Kennedy v. Biden case.
In its ruling late yesterday, the 5th Circuit disagreed with Doughty and concluded CHD, Kennedy and Sampognaro lacked standing for the same reasons the Supreme Court found the Missouri v. Biden plaintiffs lacked standing.
The court didn’t deny that pressure to censor and subsequent censorship of Kennedy and CHD had happened. Instead, it said the meetings between the government and social media companies had stopped in 2022.
Even if pressure exerted at that time led to the platforms censoring CHD, the organization could not tie ongoing censorship to government action, the court ruled. Therefore, plaintiffs have a “redressability problem,” and don’t have standing, it concluded.
Kennedy’s campaign Chief of Staff Brigid Rasmussen also described a series of content moderation actions taken by social media platforms against the Kennedy campaign.
The court ruled that Kennedy’s argument that he would be subjected to future censorship is speculative — and even more speculative now that his presidential campaign is suspended — and that he also therefore lacks standing.
The 5th Circuit’s decision voided the preliminary injunction and sent the case back again to the District Court.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Featured Video
Bombing Iran Back Into the Stone Age /Lt Col Daniel Davis & Jim Jatras
or go to
Aletho News Archives – Video-Images
From the Archives
The Occupied Mentality Syndrome
Saudi Arabia on the American chessboard – Part 2
By B. J. Sabri | American Herald Tribune | April 19, 2016
Since the Korean War, but particularly since the Iranian Revolution of 1979 until today, the United States has been steadily escalating its military presence in the Persian Gulf. Taking advantage of many colossal events of the past 36 years, [1] the hyper-empire has institutionalized its massive presence on land and sea, and expanded its objectives to include the unambiguous physical control of the area, as well as the clear understanding that local Arab governments should abide by them. The pretext is always the same: in “defense” of the national interests and security of the United States. From observing how the United States has been interacting with the governments of the region, and by judging from the size of its expeditionary force, we could reach a basic conclusion. The United States is occupying, de facto, the entire Arabian Peninsula. (Yemen, devastated by Saudi and American jets is yet to be conquered. Oman? Britain returned not as colonial ruler but as a soft occupying power.)
Under this articulation, Saudi Arabia, Qatar, Kuwait, and the United Arab Emirates are virtually occupied countries. If we compare this type of occupation to the mandate and protectorate regimes of the past, the results might be identical—the nations affected by it lose sovereignty. When Arab governments comply with the objectives of a foreign power that station military forces on their national milieu, then that power controls them in multiple ways including how they react to policy deliberations and what decisions they intend to take on specific issues. A good method to verify the concept of effective occupation is this: take notice of what the United States says and wants, and then compare it to what the gulf rulers do in response. (I shall discuss this detail at some point in the upcoming parts.)
If the presence of US forces or other means of political pressure are a factor in Saudi Arabia’s interventionist Arab wars, then we need to debate this issue. However, from the history of resistance to colonialism, we learnt: if a powerful state imposes its order on a nation by military means or other forms of coercion, and if this nation does not resist that imposition, then a mental subordination to the powerful state will ensue. This is especially true in the case of Saudi Arabia. One single event, 9/11, has transformed it from a US “ally” into an instant political hostage of the American Empire. … continue
Blog Roll
 Aletho News
Aletho News- Brazilian Congressman seeks to bar Israeli military personnel from entering Brazil
- Official reveals evidence of Arab states’ involvement in US-Israeli war on Iran
- His Majesty’s head-chopper: Syria’s MI6-backed president bows to King Charles
- Forced to backtrack: ‘Israel’ drops Hezbollah disarmament goal
- Britain’s Lebanon surveillance network: A digital map for war
- Bahrain faces scrutiny for opposition crackdown after detainee killed
- Hegseth’s Pentagon Purge Designed to Prevent a Mutiny: Karen Kwiatkowski
- Greek shipping firms secretly transporting oil, weapons to Israel
- UN vote on Hormuz force delayed as Iran issues warning
- Trump and the debris of Iran war
- If Americans Knew
- Israel-US kill negotiators, destroy civilian structures, but Iran’s military capabilities still largely intact – Daily Update
- ‘War crime’: Global condemnation as Israeli ministers celebrate death penalty law targeting Palestinian prisoners
- 7 Ways Israel Is Turning Lebanon Into Gaza
- World’s Leading Football Bodies Under Fire Over Israel Policies
- Experts warn of possible use of nukes against Iran
- Israeli invasion of Lebanon could be worse than 1982, warn European officials
- Passover: Liberation and collective punishment
- Trump says the quiet part out loud: (Israel’s) war on Iran > Americans’ health – Daily Update
- Gaza families reunite years after babies evacuated amid Israel’s war
- International Rescue Committee warns Gaza’s children face grave protection risks
- No Tricks Zone
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
