American College of Obstetricians and Gynecologists Still Pushing COVID Shots for Pregnant Women
Could Millions in Government Funding Explain Why?
By Brenda Baletti, Ph.D. | The Defender | May 2, 2024
The American College of Obstetricians and Gynecologists (ACOG) missed a May 1 deadline to explain why the organization recommends COVID-19 vaccines for pregnant women despite growing evidence that they pose a serious risk.
Reform Pharma, a Children’s Health Defense (CHD) initiative, sent ACOG a letter on March 22 outlining the extensive and mounting scientific research documenting the risks of the vaccines to mothers and infants.
The letter also addressed grant money ACOG accepted from the U.S. Department of Health and Human Services (HHS).
The funding was contingent on the organization’s full compliance with the Centers for Disease Control and Prevention’s (CDC) guidance endorsing the vaccine during pregnancy.
The grant also stipulated that ACOG admonish doctors who failed to follow CDC protocols and track women who declined the vaccine, then target them with follow-up pressure to get the shot.
Reform Pharma demanded ACOG end its practice of recommending COVID-19 vaccination for pregnant women and explain why it has continued to push the shot until now.
The letter stated:
“It’s time for ACOG to reconcile and admit its mistake. … Our team demands that ACOG stop intimidating and misleading both physicians and pregnant women. …
“It is imperative that ACOG take proper action now to prevent needless further injury and death, as it is under a legal, ethical, and moral obligation to stop the shots!”
After ACOG didn’t respond, Reform Pharma sent a follow-up letter on April 22 via certified mail and email to the ACOG president and its chief legal officer.
The letter gave ACOG until May 1 to explain, in writing, why it continues to push the COVID-19 vaccines.
ACOG President Verda J. Hicks responded by blocking Reform Pharma’s email.

An automated out-of-office reply was the only response from the organization’s chief legal officer, Molly Meegan.
“The fact that the ACOG president blocked us shows that they are not even willing to have a conversation to explain why they continue to push COVID-19 shots on pregnant women despite mounting scientific evidence of the safety risks,” Reform Pharma co-director Amy Miller told The Defender.
Reform Pharma continues working to publicize what it says is ACOG’s corruption.
“The American people need to know that ACOG is using its authority and influence to push dangerous COVID-19 shots on pregnant women but failed to disclose its backdoor deal with the CDC,” Justine Tanguay, an attorney and Reform Pharma’s co-director, told The Defender.
“Sacrificing the lives and health of pregnant women and their unborn babies in exchange for money is unacceptable,” she added.
Reform Pharma’s mission is to systematically end corruption in Big Pharma and restore integrity to the U.S. healthcare system.
“Reform Pharma is doing critically important work shining a light on organizations like ACOG which purport to represent the interests of their member physicians and the patients those physicians treat,” Kim Mack Rosenberg, CHD general counsel and a signatory to the letter, told The Defender.
“In reality, money talks, and it appears that payments and incentives from pharmaceutical companies may influence and capture such organizations.”
ACOG a ‘massively powerful’ organization that dominates maternal-fetal health
ACOG is a “massively powerful” organization with 60,000 members, maternal-fetal medicine expert Dr. James Thorp told The Defender.
The professional membership organization for obstetricians and gynecologists produces practice guidelines, educational materials and initiatives to improve women’s health, according to its website.
It is also — along with the Society for Maternal-Fetal Medicine (SMFM) and American Board of Obstetrics and Gynecology (ABOG) — a key gatekeeper organization for the field of obstetrics and gynecology, exercising tremendous power over the practices and norms among its members who are practitioners in women’s health, Thorp said.
According to Reform Pharma, ACOG takes its marching orders from Big Pharma and public health agencies.
“It functions primarily as a shill for the U.S. Department of Health and Human Services and, in particular, the Centers for Disease Control and Prevention — both lobbying arms for the pharmaceutical industry,” Reform Pharma wrote in its letter.
This became even more concerning once ACOG started promoting the COVID-19 vaccines, Reform Pharma said.
When the vaccines came on the market in December 2020, ACOG held a neutral position on vaccination during pregnancy, recommending pregnant women “be free to make their own decision regarding COVID-19 vaccination.”
That changed in July 2021, when the organization began encouraging its members to “enthusiastically recommend vaccination to their patients,” after accepting $11 million in grant money from HHS and CDC to adopt and promote the agencies’ positions on COVID-19 to its members.
“If ACOG should waver or fail to toe the line, ACOG would be required to return all the grant money it received,” according to Reform Pharma’s letter.
“ACOG made a deal with the devil and willingly sacrificed the health of pregnant women and their unborn babies in exchange for money,” Reform Pharma said.
Reform Pharma also accused ACOG of pressuring and intimidating doctors into strongly recommending the vaccine to their patients and directing them to “harass” women who refused until they capitulated.
Attorney Maggie Thorp, who last year identified the HHS grant funding — which she told The Defender is now up to $17 million since the COVID-19 pandemic period began — said she believes the CDC is just using ACOG as its mouthpiece.
Based on her analysis of the documents acquired through a Freedom of Information Act request, Maggie Thorp said the collaboration between the public health agency and the private organization is so tight that it was “hard to identify where CDC ended and where ACOG began.”
She said HHS is using ACOG to do what it cannot — “dictate the content of private conversations that happen between doctors and their pregnant patients.”
In that sense, Maggie Thorp said, HHS is “using ACOG to quell doctors’ free speech and their ability to express dissent.”
As a result, she said, patients don’t get access to the information they need to give “true, valid informed consent.”
James Thorp said that ACOG then collaborates with its partner organizations, SMFM, ABOG, and the Federation of State Medical Boards, which can take away doctors’ medical licenses or accreditation if they don’t comply, as the federation openly said it would in a July 2021 letter.
“They have the power to fire doctors or remove their accreditation from the medical board. That destroys an obstetrician,” he said. “So it’s extraordinarily intimidating.”
‘Sad’ that ACOG ‘ignores the science’
Reform Pharma provided ACOG with an extensively footnoted overview of current science showing the risks COVID-19 shots pose to pregnant women and the general population.
For example, studies have shown that the vaccine can pass through the blood-brain barrier and the placenta.
Early reporting in 2021 by the CDC’s Dr. Tom Shimabukuro in the New England Journal of Medicine claiming the shots were safe based on the CDC’s own Vaccine Adverse Event Reporting System (VAERS) and Vaccine Safety Monitoring System (V-safe) data was statistically flawed, the letter stated.
Shimabukuro concluded there were no “obvious safety signals” among pregnant women who received the vaccine. However, he presented the numbers in a misleading manner that obscured the actual rate of spontaneous abortions.
According to Reform Pharma’s letter:
“Failure to disclose the true incidence of spontaneous abortion is at best gross incompetence and at worst malfeasance. The true incidence of spontaneous abortion [in his statistics, among first- and second-trimester pregnancies] is alarming, ranging between 82% to 91%.”
Early research also linked the shot to “autism-like behaviors” in newborn rats, indicating the shot could complicate neurodevelopment and underscoring the need for more studies.
Several studies in top journals have shown that nursing mothers shed the spike protein in their breast milk, causing potentially serious adverse reactions in their newborn babies.
And, according to the letter, the COVID-19 shots pose safety risks for all people that also extend beyond complications associated with pregnancy. That data has been published extensively in places ranging from VAERS to peer-reviewed studies and beyond — sources readily available to anyone at ACOG who cares to investigate.
Given the extensive evidence summarized in the letter, “It is sad that ACOG appears not to be doing a deep dive into all the science concerning COVID-19 injections, instead taking the word of the pharmaceutical companies themselves and the FDA and CDC, which similarly rely on pharma science,” Mack Rosenberg said.
“Particularly tragic is the failure of ACOG to acknowledge and investigate the important evidence from patients themselves of the tragic impact these injections have had on pregnant women, their babies and their families,” she added.
“Pregnant women should never take this vaccine,” said James Thorp, who also has extensively documented the literature on the dangers of the COVID-19 shots for pregnant women.
“It isn’t even really a vaccine,” he said. “It’s an experimental genetic therapy with absolutely zero long-term follow-up. This is unprecedented. This is a complete violation of the golden rule of pregnancy.”
‘Wrongdoers will be held accountable’
The “public health emergency” has been officially over since May 11, 2023, and it has been demonstrated that vaccines don’t stop transmission and that there is extensive evidence regarding risks to pregnant women and all people, Reform Pharma wrote.
That means, “the only explanation for ACOG continuing to push this poison on pregnant women and their unborn children is that the organization is ‘bought off,’” the letter said. “Wrongdoers will be held accountable.”
Reform Pharma reiterated its concerns in the second letter, but aside from the blocked email and out-of-office notifications, ACOG has not responded.
Brenda Baletti, Ph.D., is a senior reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Pandemic Officials are “Disappointed in Themselves”, per the New York Times
By Igor Chudov | May 3, 2024
An article in the New York Times is titled “Thousands Believe Covid Vaccines Harmed Them. Is Anyone Listening?” (no paywall)
The author, Apoorva Mandavilli, was correctly described by Vinay Prasad as the worst science reporter. She states her surprise about “thousands” who believe that Covid vaccines harmed them. While we know that number to be an understatement, it is interesting how the New York Times recognizes them after years of stonewalling.
But in a recent interview, Dr. Janet Woodcock, a longtime leader of the Food and Drug Administration, who retired in February, said she believed that some recipients had experienced uncommon but “serious” and “life-changing” reactions beyond those described by federal agencies.
“I feel bad for those people,” said Dr. Woodcock, who became the F.D.A.’s acting commissioner in January 2021 as the vaccines were rolling out. “I believe their suffering should be acknowledged, that they have real problems, and they should be taken seriously.”
FDA’s Dr. Woodcock is disappointed in herself:
“I’m disappointed in myself,” she added. “I did a lot of things I feel very good about, but this is one of the few things I feel I just didn’t bring it home.”
The article discusses thousands of people gaslit by vaccine promoters and their doctors, who were intimidated not to report vaccine injuries:
Similar sentiments were echoed in interviews, conducted over more than a year, with 30 people who said they had been harmed by Covid shots. They described a variety of symptoms following vaccination, some neurological, some autoimmune, some cardiovascular.
All said they had been turned away by physicians, told their symptoms were psychosomatic, or labeled anti-vaccine by family and friends — despite the fact that they supported vaccines.
Even some key vaccine promoters report vaccine injuries, which they could not report anywhere:
Dr. Gregory Poland, 68, editor in chief of the journal Vaccine, said that a loud whooshing sound in his ears had accompanied every moment since his first shot, but that his entreaties to colleagues at the Centers for Disease Control and Prevention to explore the phenomenon, tinnitus, had led nowhere.
He received polite responses to his many emails, but “I just don’t get any sense of movement,” he said.
The federal officials in charge of setting the policy still refuse to believe these reports:
Federal health officials say they do not believe that the Covid vaccines caused the illnesses described by patients like Mr. Barcavage, Dr. Zimmerman and Ms. France. The vaccines may cause transient reactions, such as swelling, fatigue and fever, according to the C.D.C., but the agency has documented only four serious but rare side effects.
The excuse that these officials give for ignoring vaccine harms is that they were fighting misinformation :
The rise of the anti-vaccine movement has made it difficult for scientists, in and out of government, to candidly address potential side effects, some experts said. Much of the narrative on the purported dangers of Covid vaccines is patently false, or at least exaggerated, cooked up by savvy anti-vaccine campaigns.
Questions about Covid vaccine safety are core to Robert F. Kennedy Jr.’s presidential campaign. Citing debunked theories about altered DNA, Florida’s surgeon general has called for a halt to Covid vaccination in the state.
“The sheer nature of misinformation, the scale of misinformation, is staggering, and anything will be twisted to make it seem like it’s not just a devastating side effect but proof of a massive cover-up,” said Dr. Joshua Sharfstein, a vice dean at Johns Hopkins University.
So, get this please, the massive coverup was necessary to debunk ‘“misinformation” about the existence of a massive coverup. I hope it makes sense to you, my dear reader!
They finally note miscarriages caused by COVID vaccines:
Among the hundreds of millions of Americans who were immunized for Covid, some number would have had heart attacks or strokes anyway. Some women would have miscarried. How to distinguish those caused by the vaccine from those that are coincidences? The only way to resolve the question is intense research.
Another way to get the alarm signal of miscarriages is to ask, why does the Moderna vaccine cause 42% more miscarriages, compared to the Pfizer vaccine.
Why Now?
Are we observing a paradoxical awakening of honesty among federal officials and vaccine researchers? Have Apoorva Mandavilli and her employer finally decided to come clean about Covid vaccines?
Did these dishonest people suddenly straighten their ways, after being paid millions in research grants, CDC vaccine promotion fees paid to the media, etc? As much as I hope people can improve, I doubt that explanation.
The most likely explanation is that:
- Most vaccine-injured people are Democrats
- Facing a tough election in 2020, the Democratic party is afraid that the victims of vaccines that their party promoted and that disproportionally affected their core voters, might divert their votes and vote for an anti-vax Democrat, Robert Kennedy.
That might explain a puzzling turnaround in reporting vaccine injury in major newspapers such as the New York Times.
Rumble Defies Global Censorship Trends, Takes Stand Against New Zealand’s Free Speech Crackdown
By Didi Rankovic | Reclaim The Net | April 25, 2024
The CEO of Rumble, a free-speech YouTube competitor, says that global censorship levels are on the rise, but that what’s particularly noticeable are censorship demands coming from Australia and New Zealand – who seem to be following in the controversial, to say the least, footsteps of France and Brazil.
On the one hand, this is surprising, given these countries’ formal democratic provenance.
On the other hand, their actions over the last years, including site blocking at ISP level, constant demands for more stringent regulation to facilitate social media content removal, and even the draconian Covid – and post-Covid era measures, tell a different story.
Chris Pavlovski told Mat Kim that the FreeNZMedia channel has now become a deplatforming target in New Zealand, for reporting about leaked data from the National Vaccination Database, that a whistleblower, former Health New Zealand IT employee Barry Young, made available.
And the data Young gave to reporters and activists concerns Covid vaccine-related deaths and claims that these facts are being covered up.
For referring to Young, and referring to the data he provided to the public, a letter has been sent to Rumble to remove FreeNZMedia. It came from the National Health Authority.
However, Pavlovski said that the company has decided to refuse to do that, or to withdraw from the country, and will instead “challenge it and see what happens.”
Pavlovski went on to refer to this particular New Zealand case as “absurd” and “disgusting” – in that it bears resemblance to the Pentagon Papers. At that time, journalist Daniel Ellsberg emerged as a hero of free speech that was protected by the courts in the US.
But that was nearly 50 years ago, and things have clearly changed not only in faraway lands, but in the US itself, and whistleblowers face anything from deplatforming to life in prison.
Speaking about the case of Young, and FreeNZMedia, Pavlovski said that the whistleblower “has a statistics background, went through all the data, found the different batches of vaccines that had an irregular high death rate and published that, and gave out different interviews on doing it.”
 Screenshot
Screenshot
Pavlovski said that he saw nothing that merits censoring the Rumble channel for basing its reporting on Young’s data, and called on the US State Department to “get involved immediately and start protecting US assets and businesses around the world.”
That would be an interesting turn of events, seeing as how the US treats those “assets and business” at home, where censorship is rampant; nevertheless, Pavlovski in this way essentially challenged them to react.
Andrew Bridgen – UK Parliament Speech On Excess Deaths – April 18, 2024
You can watch the entire debate here.
Mr Bridgen’s speech in full
Thank you, Mr Speaker,
We are witnesses to the greatest medical scandal in this country in living memory and possibly ever.
The excess deaths in 2022 and 2023 is that scandal.
Its causes are complex but the novel and untested medical treatment described as a “covid vaccine” is a large part of the problem.
I have been called an anti-vaxxer as if I have rejected these vaccines based on an ideology.
I want to state clearly and unequivocally that I have not. I am, in fact, double vaccinated.
Intelligent people must be able to distinguish between being anti-vax and pro-vax but against a product that a) doesn’t work and b) causes enormous harm to a small percentage of people.
I am proud to be one of the few members of parliament with a science degree. It is a great shame there is not more intellectual diversity here. Maybe if there was, there would be less reliance on the Whips Office’s briefings, more independent research and less groupthink.
I am used to raising issues in this House that no one cares about and no one wants to know about.
Nothing has been learned from the Post Office scandal.
Only two of the five MPs in the room when the Second Sight team were appointed, on my recommendation, to investigate the post office are still in the House of Commons. I am one of them. Michael Rudkin, the national sub-postmaster Federation Chairman who famously saw the live Horizon terminals in the basement of Fujitsu HQ was my constituent.
I have been fighting his corner in this House for many many years. Long before that scandal became national news. Long long before. I was mostly ignored.
I am being ignored again, this time on the issue of excess deaths.
Yet again, the official narrative is to deny, obfuscate, ridicule and silence dissenting voices.
I say to the House, and I say it with seriousness, this debate – and others like it proposed by me and others – are going to be pored over by future generations.
They will be genuinely agog that the evidence was ignored, that genuine concerns were disregarded and that those raising it were gaslit, smeared and vilified.
The excess deaths scandal bears an uncanny resemblance to the Post Office catastrophe
Both involve:
- Complacent public bodies
- Ministers unable to understand the technicalities and mouthing platitudes
- Malevolent corporations with a vested interest in silencing questions
- Lives ruined by greed, lies and corruption
- Most damaging of all is a culture of denial, obfuscation, secrecy and denigration
- Much of the harm was avoidable
You don’t need to have any scientific training to be horrified by officials deliberately hiding key data in this scandal.
The Covid-19 experimental ‘vaccine’ is a scandal that is happening right now, today, and it must end.
The Office of National Statistics used to release weekly data on deaths per 100,000 in vaccinated and unvaccinated populations.
Now it doesn’t. No one will explain why.
The public has a right to that data.
There have been calls – from serious experts whose requests I have amplified repeatedly in this House – for what is called “record-level data” to be anonymised and disclosed.
This data will allow meaningful analysis of deaths after vaccination and settle the issue of whether these experimental treatments are responsible for the increase in excess deaths.
Far more extensive and detailed data has been released to the pharma companies from publicly funded bodies. Jenny Harries, head of the UKHSA, said this anonymised aggregate death by vaccination status is “commercially sensitive” and shouldn’t be published.
The public is being denied this same data.
Yet again data is hidden with impunity. Just like the Post Office.
You may remember Professor Dame Jenny Harries, who in July 2022, said that masking was a good idea – and I quote, “If I’ve got any respiratory infection it’s a good thing to do, and I think it’s a new lesson for the country.”
She earlier gave the following totally contradictory advice: “The virus will not survive very long outside. Many outdoor events, particularly, are relatively safe.”
On 11th March 2020 on the issue of masks, she said, “It’s really not a good idea and doesn’t help,” and “in some ways, you may actually risk catching the disease rather than preventing it.”
She was right then. What made her do a U-turn on all these critical points?
Professor Harries has also endorsed a recent massive change in the calculation of the baseline population level used by the ONS to calculate ‘excess deaths’. It is incredibly complex and opaque and by sheer coincidence, it now appears to show a massive excess in deaths in 2020 and 2021 and minimal excess deaths in 2023.
Under the old calculation method, tried and tested for decades, the excess death rate in 2023 was an astonishing 5%, long after the pandemic was over and when you would expect a deficit in deaths because so many people died early in previous years.
20,000 premature deaths are now being airbrushed away in 2023 alone with the “new normal” baseline.
Fear
What is even more shocking is the sheer number of mistakes and scandals in this ongoing horror story.
For example, in March 2020, the government conducted a consultation exercise on whether people over a certain age or with disabilities should have Do Not Resuscitate orders imposed on them, known as DNRs.
A document summarising the proposals was circulated to doctors and hospitals. This was mistakenly treated as formal policy by a number of care homes and GPs up and down the country who enacted it.
At the same time, multiple hospitals introduced a policy that they would not admit patients with Do Not Resuscitate orders because they thought they would be overwhelmed.
Many people died as a result who did not need to, as nurses did TikTok videos while their hospitals lay empty.
Another example:
Fear kills. It kills because people don’t seek needed medical care for fear of the virus, a virus which has a 99.8% survival rate.
It kills because it has been proven that increased stress can suppress the immune system or even be fatal in vulnerable people.
It kills because people who were trying to get care were told to isolate.
It kills because frightened staff were too eager to ventilate to reduce aerosols in the ward.
It kills because isolated, vulnerable and elderly people are abandoned by family and friends.
It’s not just patients who are frightened. Doctors are frightened too. Frightened for their careers. Frightened for their reputation. Frightened of the GMC. Frightened to do anything not prescribed by the authorities who set the protocols.
There have been many doctors and scientists who have bravely spoken out on this, risking their careers and livelihoods, people like Dr Aseem Malhotra, Professor Norman Fenton, Dr David Cartland and Professor Angus Dalgleish to name but a few. Not to forget all of the team at the Hart Group including Dr Clare Craig, who has been so instrumental in helping me put together this speech today.
Another example is that during Covid, doctors failed to call out a dangerous change in protocol. The average time to death from covid symptoms starting was 18 days.
It is a little-known fact that the body clears all the virus within around 7 days.
What kills people is that some people, especially the vulnerable, have an excessive immune response.
Doctors have been treating this for decades with steroids, antibiotics for secondary pneumonia infections and other standard protocols.
But, not this time.
Even though the virus was long gone, doctors abandoned the standard clinical protocols because covid was a new virus.
They sent people home and told them to take paracetamol until their lips turned blue.
Then they sedated them, put them on ventilators and watched them die.
It gets worse, the protocol was a binary choice between two treatment tracks. Once admitted, ill patients were either to be ventilated in intensive care or, if they were not fit for that level of care, they were to be given end-of-life medication including Midazolam and Morphine.
The body responsible for this protocol – NG163 which was published on 3rd April 2020 – is called the National Institute for Health and Care Excellence – NICE.
Giving Midazolam and Morphine to people dying of cancer is reasonable but they have a side effect. The side effect is that these drugs have a respiratory depressant effect.
It is hard to imagine a more stupid idea than to give people struggling to breathe, drugs that do that. Yet that’s what they did.
Why was the warning letter regarding the use of Midazolam in NICE guideline NG163 to the British Medical Journal on 19th May 2020 signed by two Professors and nine Doctors ignored? Especially as it would seem it’s a replica of Abolished Liverpool Care Pathway in dosages and combined use of Midazolam plus an opioid.
NG163 stated that a blanket start dose of 2.5 mg of Midazolam should be injected regardless of age, body weight and comorbidities, how can this be medically acceptable as results show titration was not possible at such a dose for many elderly and who authorised it?
Why was Midazolam then removed from the same updated guideline NG191 on 30th November 2023? (As it was removed is it now considered and admitted it was a mistake to ignore the warning of the inclusion of that specific drug in NG163)?
It’s now been confirmed by subsequent letters from Ministers to families that doctors and nurses should have treated the individual patient with their own knowledge rather than strictly follow NICE guideline NG163 (as suggested by Quince and Stephenson) so if the warning letter from 11 experts to the BMJ was correct is the blame with NICE, NHS England or individual doctors and nurses, should legal action find verdicts of unlawful killing?
I would like to pay tribute to the Scottish Covid Inquiry which is hearing extensive, heartbreaking evidence of the effect of this alternative protocol on real people, real lives and sadly real and unnecessary deaths. People scared. People angry. People dying. People gasping for their lives away who might have been saved.
I very much hope that the eventual Scottish Inquiry Report addresses in detail the NICE decision making on the alternative protocols for those with Covid.
All these deaths were ascribed by the government to covid as if no other factors needed to be investigated.
But this is one example of a scandal that if it wasn’t for the Scottish Inquiry would never be investigated and never learned from.
Anyone who raised this problem during the pandemic was smeared as a covid denier.
Even worse
NICE has now removed these alternative protocols from its website. All other old protocols are still there for historical reference.
Why have NICE removed this protocol from their website? Are they ashamed of the harm they caused?
They certainly should be.
What can we learn from this? Doctors don’t challenge what they are told. Protocols with no authors are distributed and doctors fall in line.
We need doctors who are prepared to put their necks on the line for the sake of their patients, but we don’t have them and the whole system is broken as a result.
Here is another example.
Not a single death certificate was written saying that death was due to the rare brain clots caused by AstraZeneca until the MHRA said there was a link. Then the death certificates started to trickle in.
That’s not the scandal.
The scandal is that doctors wait for authorities to tell them they could label a death as vaccine-linked before they will do it. They are afraid of being smeared or reported to the GMC.
In the meantime, the MHRA relies on the evidence from death certificates in order to identify a problem.
That’s the scandal.
It wasn’t until other countries and public and political pressure FORCED the MHRA to admit the link between vaccines and blood clots causing death that they finally admitted it. And THEN doctors started putting it on death certificates.
There is a stark contrast in how deaths and illnesses after vaccination have been recorded compared to Covid. After a positive test, any illness and any death was attributed to the virus. After the experimental and emergency-use vaccine, no illness and no death occurred. Both are totally unscientific approaches. That is why we have to look to other data sources – excess deaths to determine if there is an issue.
Safe and Effective
The fear deliberately stoked by the government promoted the idea of being rescued by a saviour vaccine. The chanting of the safe and effective narrative began. The phrase seems to have hypnotised the nation.
“Safe and Effective” was the slogan used to market Thalidomide.
After that scandal rules were put in place to prevent such marketing in future. Pharma companies are prohibited from saying “safe and effective” without significant caveats.
That didn’t matter this time because the media, the government and authorities turned into the pharma marketing department.
It is hard to now hear the word safe without the echo of “and effective”.
But they are not safe and effective. In March 2021, when the majority of UK citizens had already received these novel products, Pfizer signed a contract with Brazil and South Africa in which they said, “the long-term effects and efficacy of the Vaccine are not currently known and … adverse effects of the Vaccine… are not currently known.”
These so-called vaccines were the least effective vaccines ever. Is there anyone left under the illusion that they prevented any infections?
Yet, even the Prime Minister now has one eye on history.
When he was at the dispatch box on 31st January at PMQs, following my question, he could not bring himself to add “and effective” to his “safe” mantra that the vaccines were safe.
Why is the Prime Minister gaslighting the 163 successful claims made to the Vaccine Damage Payment Scheme totalling an incredible £19.5m in compensation for harm caused by the Covid vaccines? Haven’t they suffered enough already? Those 163 are the tip of the iceberg by the way.
It should be noted that the maximum payment is £120,000. So each of those 163 got the maximum possible award, which tells you something perhaps.
That same compensation scheme paid out a total of £3.5m between 1997-2005 with an average of 8 claims per year. That’s for ALL other claims in the entire country for all vaccines.
So much for ‘safe’.
How about effective?
Even by 25th October 2021, the former Prime Minister and Member for Uxbridge and South Ruislip even admitted that, and again, I quote, “It doesn’t protect you against catching the disease, and it doesn’t protect you against passing it on.”
Looking at the levels of the virus in sewage shows that the post-vaccine wave was in the same order of magnitude and duration as the previous waves.
Vaccines changed nothing. They were not safe. And they were not effective.
Those who imposed these vaccines knew full well they could never prevent infections in this kind of disease.
An injection in the arm cannot do that. Only immunity on the surface of the airway and lungs can prevent viral infection. Antibodies in the blood cannot.
In Dr Anthony Fauci’s own words, “It is not surprising that none of the predominantly mucosal respiratory viruses has ever been effectively controlled by vaccines”
He continued, “This observation raises a question of fundamental importance: if natural mucosal respiratory virus infections do not elicit complete and long-term protective immunity against reinfection, how can we expect vaccines, especially systemically administered non-replicating vaccines to do so”
The mantra of “safe and effective” has so brainwashed some people that we now have the outrageous situation where the loving mother of a 24 year old man, who had the mental age of an 18 month old has been threatened in court with jail time, by a lawyer charged with representing her son’s best interests, because she does not want him vaccinated.
He has had covid meaning he has the optimum possible protection against a subsequent infection already.
The judge has used the argument that Tom would choose to be vaccinated for altruistic reasons but the court has a duty to act in his best interests not the interests of society.
Altruism means taking vaccinations to help others. But, these vaccines do not protect others! They do not prevent infection. Why is our system persecuting this mother? What are they hoping to achieve?
Only a few days ago, the ABPI, the Association of the British Pharmaceutical Industry rapped Pfizer on the knuckles for the sixth time and said their marketing practices had brought the industry into disrepute. They were asked to pay £30,000 in administrative expenses with no fine on top. The person heading the ABPI at the moment is also the head of Pfizer UK. The MHRA have a statutory duty to carry out this work and has handed the responsibility over to the industry itself. This is an outrageous conflict of interest.
Another drug produced by Pfizer was Paxlovid designed to supposedly treat Covid. It was approved in December 2021.
Pfizer this week revealed the trial results for Paxlovid that had been hidden for two years.
The study showed that Paxlovid did not work to reduce illness.
Worse still, it caused rebound infections in 25% of those treated.
Worse still it causes serious drug interactions and other side effects.
Will Pfizer be held accountable for this? I am not holding my breath.
Australia
But let’s return to excess deaths. The Australian government has launched an Inquiry into their excess death problem.
Australia is almost unique as a case study for excess deaths. They had the vaccine before they had Covid.
Their excess deaths are not so easily blamed on the long-term effects of a virus. Like us, they saw a rise in deaths that began in May 2021 and has not let up since. The impact was evident on the ambulance service first.
South Australia saw a 67% increase in cardiac presentations of 15-44 year olds which peaked in November 2021 before covid hit.
We saw a similar deeply worrying effect here too:
Calls for life-threatening emergencies in the UK rose from 2000 per day to 2500 per day in May 2021 and it has not returned to normal.
Queensland doctors called the problem a “ticking time bomb” in April 2021 and described a “flood of patients.” 69
By October 2021, despite it being springtime in Australia headlines reported on ambulances unable to drop off patients in hospitals that were at full capacity.67
Mark McGowan, Premier of Western Australia, said he could not explain the overwhelmed hospitals, “Our hospitals are under enormous pressure. This has been something no one has ever seen before. Why it is, is hard to know.”68
By April 2022, Yvette D’ath Queensland health minister said about the most urgent ambulance calls (“code ones”), QUOTE: “I don’t think anyone can explain why we saw a 40% jump in code ones… We just had a lot of heart attacks and chest pains and trouble breathing, respiratory issues. Sometimes you can’t explain why those things happen but unfortunately, they do.”70
Omicron caused excess deaths in Australia from 2022 onwards, however, there is a huge chunk of excess deaths which doctors have not been able to blame on the virus.
Could these deaths be caused by the vaccine? Very few dare ask, Mr Speaker.
Remember the warning from Kate Bingham, head of the covid vaccine task force, who said in October 2020 that vaccinating healthy people who have little risk from covid “could cause them some freak harm.”
Has there been some freak harm? The data on disability claimants would suggest the answer is yes! Both here and in the USA there was a rocket in the number of working-aged people unable to work because of long-term sickness. The increase began in May 2021. Thankfully these figures have stopped climbing here and in the USA in 2023.
The timing, or temporal link, suggests vaccines as the cause rather than the virus.
A rise in sickness and a rise in deaths that both occurred from May 2021 in Australia and in the UK despite their seasonal differences and despite their different covid trajectories is highly suggestive that vaccines are the underlying problem here.
It is important to remember how these vaccines were made. Traditionally the key to making a vaccine is to ensure that the pathological parts of the virus or bacteria are inactivated so the recipient can develop an immune response without the dangers of the disease.
In stark contrast, these so-called covid vaccines used the most pathological part of the virus in its entirety.
The harm is systemic because, contrary to what everyone was told, the lipid nanoparticles spread throughout the whole body after injection, potentially affecting all organs. At the time everyone was being reassured that the injection was broken down within the arm at the injection site, regulators knew or ought to have known of these problems.
Furthermore, there is now plentiful evidence that the drug results in continued protein production for many months, even years, in some people. The deaths, thus far have been predominantly cardiac. but there may be more deaths to come.
Cancer
Dr Robert Tindle is the retired director of the Clinical Medical Virology Centre in Brisbane and Emeritus Professor in Immunology.
This month Dr Tindle published a paper highlighting the multiple potential harms from the vaccines including harm to the immune system which – as with anything which disrupts the immune system – can potentially increase the risk of cancer.
There are other reasons to be concerned about cancer being induced by these vaccines.
Cancer is a genetic disease that arises from errors in DNA allowing cells to grow uncontrollably.
Moderna has multiple patents describing methods for reducing the risk of cancer induction from their mRNA products.
This risk comes from material interrupting the patient’s DNA.
It turns out that what we were told was an mRNA injection actually had very high quantities of DNA in it. This massively increases the risk of disturbing a patient’s own DNA.
Worse still the DNA that was injected contained sequences that were hidden from the regulator. This was no accident. Yet again crucial information was hidden with impunity.
Conclusion
The evidence is clear that these vaccines have caused deaths.
Despite this, they have been described as safe and effective.
But, for a small proportion of people, the vaccines have caused serious harm including death.
Neither are they effective. The vaccine does not prevent infection or transmission and when the data is looked at objectively, it does not prevent serious illness and death.
These are hard truths to face.
We must face them if we want to learn the lessons from the last few years.
I’ve been right before.
At some point that will be evident. Let’s not wait as long as the post office scandal before we admit it.
It is time to take the politics out of science and put some actual science back into politics.
So, Mr Speaker, I offer Members of this House the same opportunity which I offered the Prime Minister: ‘To be on the right side of history, the right side of science and on the side of the people.’
Sadly, given the PM’s compromised position regarding his investments in big pharma, he only dug himself an even bigger hole!
I wish I was wrong about the experimental vaccines but the evidence was overwhelming 18 months ago it is absolutely unequivocal now.
I call on this House to do the right thing and protect our constituents, even if it means standing up to the most powerful vested interest in the world.
Fake Physician Allison Neitzel Caught Running Real Medical Misinformation Site
Medical clown for “disinformation reporters” at NBC and Mother Jones crashes her own disinformation circus

By Paul D. Thacker | The DisInformation Chronicle | April 3, 2024
Promoted to national prominence by a coterie of reporters tackling pandemic misinformation, physician Allison Neitzel took a hard fall last week when she was forced to atone for promoting misinformation and defaming medical experts—by posting an apology on her website, and pinning the same to the top of her social media X account. But unless you hang on every word of Democratic Party aligned reporters with a knack for labeling everyone they don’t like a “conspiracy theorist,” you likely don’t know physician Allison Neitzel.
If you haven’t heard of her, you should know her name and story.
Allison Neitzel’s story encapsulates everything that went wrong during COVID when self-defined “disinformation reporters” glommed onto anyone they tripped over on social media as an “expert” they could deploy to castigate those refusing to bend the knee to Big Pharma.
“I know of Allison because of the way she has targeted me,” says Tracey Beth Høeg, a physician researcher and associate professor of clinical research at the university of Southern Denmark. Neitzel has deleted many of her social media posts denigrating Hoeg, including one in which she labeled her “Hoeg hag.”

“The fact she has not nearly completed her training but has appointed herself as an expert physician in pointing out misinformation strikes me as both odd and ironic,” Hoeg continued. “For example, as you can see, she is really attacking me rather than anything substantive about what I have done or said.”
Allison Neitzel rocketed to national fame on CNN after graduating from the Medical College of Wisconsin and posting a letter on social media that accused Green Bay Packers quarterback Aaron Rodgers of spreading COVID misinformation. Rodgers said he was allergic to one of the vaccine ingredients and didn’t need to be vaccinated because he had already been sick with COVID, however, this was almost a year before the CDC stated that prior infection was no different than being vaccinated.
Despite spreading false information about Rodgers, Neitzel’s letter and purported medical bona fides proved catnip to reporters at MedPage Today, Mother Jones, and NBC, who quoted her as a physician exposing medical misinformation. Columns Neitzel has written for websites WhoWhatWhy and Science-Based Medicine also claim she is a physician focusing on disinformation.
And this is where the circus fun begins, because famed medical misinformation expert Allison Neitzel is not now, nor has she ever been, a physician.
Allison Neitzel did not respond to multiple requests for comment to explain.
COVID clown show
I began unraveling Allson Neitzel’s COVID circus act shortly after she posted the apology to her website with the ironic name “MisinformationKills” and pinned it to the top of her @AliNeitzelMD X account.
Neitzel’s apology details a long list of false statements she made against multiple physicians accusing them of a fraud and grift, along with weasel words that make clear this is a non-apology apology, in the vein of “I am sorry if you feel bad.”
“I regret if anyone understood the statements as accusations that any of them had engaged in fraudulent professional or business practices,” Neitzel writes.
You can read her apology, but the depth and particulars of Neitzel’s defamation of real medical experts is impossible to know because she has deleted many of her posts on social media and on MisinformationKills.
But particulars don’t matter.
Neitzel is one in a legion of medical clowns the media launched into prominence during the pandemic because they served as useful idiots for “disinformation journalists” needing a quotable “expert” to bash people who dared question conventional COVID wisdom, or who charged that the government made phony claims about a lab accident in Wuhan, overstated the efficacy of masks and lockdowns, or lied about the safety and efficacy of COVID vaccines.
What makes Allison Neitzel unique from the COVID clown posse is that she was forced to retract and apologize for her lies and fake claims.
Interested, I dug into her background and discovered that all the outlets claiming Neitzel was a physician hadn’t bothered to do a modicum of due diligence before platforming her, because guess what? Allison Neitzel isn’t a physician.
Donning clown costume
The first social media trace I could find for Allison Neitzel is a 2019 Facebook post by the Medical College of Wisconsin. “Third-year med student Allison Neitzel helped teach young students how to use blood pressure cuffs, listen to heart and lung sounds through the use of a stethoscope, how to perform CPR and more.”
But when Neitzel jumped into the national conscience in 2021, she began claiming she was a “physician.” A group called the National Association of Medical Doctors (NAMD) posted Neitzel’s letter criticizing Green Bay Packers quarterback Aaron Rodgers in their Journal of Medicine, where she signed as “Allison Neitzel is a physician.” (Stay tuned: While researching the NAMD, I learned even more about COVID grift, which I will report in a future investigation.)

But when you look into Wisconsin law, you find the state defines a physician as “an individual possessing the degree of doctor of medicine or doctor of osteopathy or an equivalent degree as determined by the medical examining board, and holding a license granted by the medical examining board.”
So I looked up Neitzel in the National Provider Identifier Standard (NPI) which lists everyone licensed as a physician in the U.S. And guess what?
Allison Neitzel isn’t a physician.

Of course, her false claims of being a physician didn’t stop multiple media outlets from promoting Neitzel as a “physician” and misinformation expert. Let’s take a look.
COVID clown circus
Neitzel made two appearances as a “physician” in 2023 stories written by Kiera Butler at Mother Jones. Butler specializes in “COVID disinformation” stories that uncover “anti-vaxxers” and “right-wing” forces peeking out from every corner of America to harm the public with “misinformation.”
In one of her more amusing reporting incidents, Butler penned an article that claimed natural immunity from prior COVID infection was a “dangerous theory” spread by anti-vaxxers.

After California passed a law to discipline doctors for sharing “false COVID information” with patients that differs from the “scientific consensus” (whatever that is), Butler began attacking physicians who sued to stop the censorship, claiming that they were spreading medical lies. Linking to a tweet by Neitzel, who she labeled a “physician and disinformation researcher” Butler reported that “far-right rhetoric” and Nazi propaganda were supporting the lawsuits.
In fact, a California judge blocked the law for violating physicians’ First Amendment rights. Having first signed a bill that created the law, Governor Newsom then repealed it.
Neitzel was also featured in a story by NBC’s Brandy Zadrozny, another “disinformation reporter” who specializes in “extremism”—code in the disinformation world for “conservative” as people like Zadrozny never seem to find extremism among liberals.
In a story looking into anti-vaxxers—a favored topic for disinformation types—Zadrozny reported on aggressive online harassment against physicians and quoted Neitzel as an expert.
Online harassment has become increasingly common for doctors during the pandemic, according to Dr. Ali Neitzel, a physician researcher who studies misinformation.
“The targeting of individual physicians is a well-worn tactic,” Neitzel said. “But this cheaply done fake — trying to frame a doctor who is doing unpaid advocacy work — that’s a new low.”
Forget that Neitzel is not even a physician. The absurdity is that Zadrozny quoted Neitzel—forced to post an apology last week for fomenting years of misinformation, and years of harassing physicians—as an expert commentator on misinformation and harassment of physicians.
It’s that ludicrous.
Trying to understand Zadrozny’s reporting, I emailed her questions pointing out that Neitzel was never a physician, and asking if she had bothered to check into Neitzel’s credentials.
“Do you plan to correct your article?” I asked.
True to the disinformation journalism game, in which reporting errors are never admitted nor corrected, Zadrozny never responded.
Neitzel’s online persona as a misinformation expert also gained her entrée into three different articles at MedPage Today.
- Bebe Rexha’s Wound Care; ‘The System Is Broken’; Finding Nemo in a Blood Drain
- Ron Johnson and the COVID Disinformation Pipeline
- Should Doctors Worry About ‘Nuremberg 2.0?’ (MedPage Today labels this article an “exclusive special report”)
“Can you explain why MedPage Today ran so many stories featuring Allison Neitzel who falsely claimed to be a physician and has been forced to post an apology for defaming physicians?” I emailed MedPage Today’s editor-in chief Jeremy Faust, an instructor at Harvard Medical School.
“I’m trying to understand if such reporting meets the standards at MedPage Today and if you plan to run any corrections or clarifications.”
Faust refused to respond to questions sent to his Harvard email.
Neitzel’s claims of being a physician also garnered her a column at the nonprofit news organization WhoWhatWhy. “Allison Neitzel, MD, is physician-researcher and founder of the independent research group MisinformationKills, which has investigated the dark money and politics behind public health disinformation with a focus on the pandemic,” reads her author bio page.
“Why have you claimed Allison Neitzel is a physician?” I emailed WhoWhatWhy’s editor-in-chief, Russ Baker. “And do you plan to continue claiming Neitzel is a physician?”
Baker did not respond to multiple requests for comment.
Neitzel also wrote a column for the site “Science-Based Medicine” where her bio states she is a physician. Science-Based Medicine is a marketing site for the biopharmaceutical industry run by David Gorski, a Wayne State University surgeon, self-described “misinformation debunker,” and ardent vaccine cheerleader.
After the European Medicines Agency concluded in April 2021 that unusual blood clots should be listed as a very rare side effect for AstraZeneca’s COVID-19 vaccine, Gorski called foul on the regulator. The UK government eventually stopped offering the AstraZeneca vaccine, and The BMJ reported last year that dozens of patients had launched legal action against AstraZeneca after suffering the same vaccine side effects that Gorski claimed were nonexistent.
In an email to Gorski, I asked why he lists Neitzel as a physician when she doesn’t meet the legal requirements for a physician in Wisconsin where Neitzel resides.
Gorski called the question “pedantic” and said he will ignore Wisconsin law in favor of a definition for “physician” that he found on the website for the American Medical Association.
“In general, ‘misinformation’ reporting seems to have certain ideas they are told are true/false and it’s about finding evidence to support what they have been told,” says Hoeg. “Also the ‘misinformation’ reporters often seem less qualified in terms of understanding the strengths and weaknesses of the scientific studies and domains than the people/scientists they are accusing of spreading ‘misinformation.’”
CORRECTION: In reporting on Allison Neitzel’s farcical rise to media glory, I mixed up the websites MedPage Today and Medscape. The Medscape articles featuring Allison Neitzel are Young Doc to Aaron Rodgers: Be a ‘Team’ Player on COVID Vaccine and Physicians Get Cyberbullied Over Vaccine Advocacy.
Shame on me for making this mistake. Shame on Medscape and MedPage Today for platforming COVID circus clown Allison Neitzel.
UPDATE: Following this exposé, Allison Neitzel changed her X account to be compliant with Wisconsin law and more honestly represent her credentials.
She’s a work in progress.

WHO: Intel Agency for Gates Foundation?
Examining the Foundation’s prescient August 2019 purchase of BioNTech stock
By John Leake | Courageous Discourse™ | April 22, 2024
Reviewing BioNTech’s Disclosure of Classes of Share Capital for the year ended December 31, 2019, I noticed the following:
On August 30, 2019, BioNTech entered into agreements with the Bill & Melinda Gates Foundation (BMGF). BMGF agreed to purchase 3,038,674 ordinary shares with nominal amount of k€ 3,039 of BioNTech for a total of k€49,864 (k$55,000). These agreements require BioNTech to perform certain research and development activities to advance the development of products for the prevention and treatment of HIV and tuberculosis. In the event of a breach of the underlying conditions, including such research and development activities, BMGF has the right to sell its shares back to BioNTech at the initial share price or fair market value, whichever is higher, subject to certain conditions. BioNTech’s ability to pay dividends is also limited under the terms of these agreements.
Less than two years after the Gates Foundation purchased the stock (pre-IPO) at $18 per share, it peaked on Aug. 6, 2021 at $389. At that price, the Foundation’s $55 million investment was worth $1,182,044,186.00 ($1.182 billion).
On September 18, 2019—just nineteen days after the Gates Foundation took its huge position in BioNTech stock— a report titled A World At Risk was published by the Global Preparedness Monitoring Board, which was founded in 2018 by the World Bank Group and the World Health Organization.
The report’s title page is illustrated with an image of a coronavirus, and its text is an urgent call to action for the world to invest far more in preparedness for a respiratory viral pandemic. As the report states on page 8:

The report mentions nothing about the need to invest in bolstering bio-laboratory safety. It expressly warns about the threat of a lethal respiratory pathogen “accidentally or deliberately released,” but its entire call to action is to invest a fortune to responding to such a pathogen instead of preventing it from being released in the first place.
This was in spite of numerous urgent warnings from Rutgers University biology professor Richard Ebright and others that many of the world’s bio-labs had a history of grave security lapses that were NOT being adequately addressed. In 2017, Professor Ebright expressed particular concern about the new BSL-4 lab that was about to open in Wuhan, China.
We now know that SARS-CoV-2 was officially detected in December of 2019 but probably emerged and started spreading in August or September of 2019—that is, around the same time A World At Risk was published.
The September 18, 2019 date of the report strongly suggests that someone doing bio-surveillance for the WHO in China obtained intelligence that a SARS coronavirus was already circulating.
Given that the Gates Foundation is the WHO’s second largest donor (after Germany, where BioNTech is headquartered) I wonder if this intelligence was passed to someone in the Gates Foundation months before December 31, 2019—the date the WHO claimed it received its first report of cases of pneumonia of unknown etiology in Wuhan.
Does the WHO—with its Country Offices obtaining bio-surveillance reports from the field—serve an an unofficial intelligence agency for the Gates Foundation?
If so, it would enable the Foundation to obtain extremely valuable information about emerging infectious disease pathogens—naturally emergent or accidentally or deliberately released—long before other market players obtain this information.
‘Tacit Admission of Guilt’: Two Top Journal Editors Decline to Testify Before Congress on Scientific Censorship
By Michael Nevradakis, Ph.D. | The Defender | April 17, 2024
Only 1 of 3 science journal editors invited to testify before Congress on government interference in the peer-reviewed publication process accepted the invitation this week.
Holden Thorp, Ph.D., editor-in-chief of the Science family of journals, on Tuesday testified before the U.S. House of Representatives Select Subcommittee on the Coronavirus Pandemic.
Magdalena Skipper, Ph.D., editor-in-chief of Nature, and Richard Horton, editor-in-chief of The Lancet, “declined to participate,” according to the subcommittee’s website.
“We invited the editors-in-chief of The Lancet, Nature and Science. Only the editor of Science had the courage to come and help us be better,” Subcommittee Chair Brad Wenstrup (R-Ohio) said.
In his opening remarks Tuesday, Wenstrup said, “This subcommittee was established so we can collectively take a look back on the pandemic and see what we can do better for the next time.”
But experts who spoke with The Defender said they were disappointed with the editors who declined to testify — but also with the members of the subcommittee, who they argued failed to address key issues during the hearing.
Cardiologist Dr. Peter McCullough told The Defender, “The committee and Thorp disappointed academic researchers and the public alike.”
McCullough, author of more than 1,000 science journal articles, added:
“Thorp was silent on harmful retractions of fully published papers … This has happened repeatedly for manuscripts describing early treatment(s) and protocols for ambulatory acute SARS-CoV-2 infection and for reports of COVID-19 vaccine injuries, disabilities and deaths.
“Who is behind these retractions? Why are they working to suppress early therapeutic options for patients and scrub any concerns over vaccine safety?”
Epidemiologist and public health research scientist M. Nathaniel Mead told The Defender, “It seems very telling” that Skipper and Horton skipped Tuesday’s hearing.
“In the context of SARS-CoV-2 origins, these two journals have been accused of being unduly influenced by the pharmaceutical industry and government agencies,” Mead said. “Such conflicts can impede unbiased scientific reporting and commentaries.”
“Skipper and Horton’s absence would seem to be a tacit admission of guilt on the part of the two journals they represent,” said Mead, who wrote a peer-reviewed paper that was retracted by the journal Cureus after publication.
McCullough said two papers for which he was senior author were retracted. “In both instances, the public and the practicing community were harmed by the intentional omission of critical side effects from the knowledge base on these products.”
Independent journalist Paul D. Thacker has investigated scientific censorship for The Disinformation Chronicle. He told The Defender, “The science and medical journals did not publish the best research available during the pandemic. They just served as gatekeepers to protect people, institutions and corporations in power.”
Thacker added:
“Holden Thorp should resign. He oversaw a news section that ran several fake stories about the pandemic to misinform the scientific community. And Science published studies that have been noted in the peer-reviewed literature for poor statistics to deny a possible lab accident. It’s a historical low point for this publication.
“Nothing will change from these hearings. My only hope is that some researchers will understand how corrupt the scientific process has become and this hearing will spur them to make change.”
‘No place for politics’ or government influence over journals
During his opening remarks, Wenstrup said the hearing was not intended “to see how the government can be more involved in the journal editorial process, but to make sure that the government does not involve itself or influence this process.”
“There’s no denying the awesome power these periodicals as well as their editors hold over the medical and scientific communities,” Wenstrup said. As a result, “there can be no place for politics or inappropriate government influence of journals.”
But Wenstrup accused the journals and their editors of not always being “arbiters of truth.” Instead, he said, they “provide a forum where scientific claims are made, defended, and debated by peer review.” Wenstrup added, “We saw a breakdown of that during the pandemic.”
“Rather than the journals being a wealth of information and opinions about this novel virus of which we knew so little, they helped establish a party line that literally put a chilling effect on scientific research regarding the origins of COVID-19,” Wenstrup said.
Wenstrup cited the “Proximal Origin” paper — published by Nature in March 2020 — as an example, saying that it helped “set a precedent … that the natural origin of COVID-19 was the only plausible theory.”
“Anyone else who had even the inkling of another plausible scientific thought was immediately labeled a conspiracy theorist … How is that acceptable in the scientific community when the entire crux of the field is open for debate?” Wenstrup said.
During his opening remarks, Ranking Member Rep. Raul Ruiz (D-Calif.) contradicted Wenstrup’s statements, claiming the subcommittee has not proven that top government public health officials such as Drs. Anthony Fauci and Francis Collins orchestrated the publication of the “Proximal Origin” paper.
‘Clear evidence of malfeasance and dishonesty’
Thorp told members of the subcommittee that he is “extraordinarily proud of the Science journals’ work” and “of the role that the scientific enterprise plays in society.”
He said the Science journals “abide by a rigorous multi-step peer-review process” and “a careful process to ensure that the reviewers do not have a conflict of interest.” This “well-established process,” he said, “was applied consistently to the nearly 9,000 research papers submitted to the Science family of journals related to SARS-CoV-2.”
Thorp referred to a May 2021 letter by virologist Jesse D. Bloom that Science published in its commentary section. “This letter called for a thorough investigation of a lab origin of COVID-19,” Thorp said, citing the commentary as evidence the journal did not conduct viewpoint censorship.
“Publication of this letter turned the tide in the discussion of COVID origins toward considering the possibility of a lab origin,” Thorp said.
Thorp also referred to two papers, by virologists Michael Worobey and Jonathan E. Pekar, published in Science’s research section 2022 that supported but “[did] not conclusively prove the theory of natural origin.” He said the government did not influence the publication of these papers.
“To be clear and to state upfront, no government officials from the White House or the NIH [National Institutes of Health] prompted or participated in the review or editing of [these] papers by us,” Thorp said.
Upon questioning by Rep. Debbie Dingell (D-Mich.) and Rep. Deborah Ross (D-N.C.) about communications between Fauci, Collins and Thorp in May 2021, Thorp said they supported an investigation into the origins of COVID-19 at the time and did not dissuade Science from publishing the Bloom letter.
Responding to Rep. Mariannette Miller-Meeks (R-Iowa), Thorp acknowledged that opinion pieces “go to 8,000 reporters four days before they’re published.” Because some of these pieces mention government figures, he “from time to time let[s] them know ahead of time that there’s an opinion piece coming that they might get asked about.”
“Scientists are not and never will be perfect,” Thorp said. “We are human, but the scientific method enables us to reach beyond our individual limitations by requiring evidence and constant self-correction. It helped us end the pandemic.”
Referring to the Worobey and Pekar papers, Wenstrup said, “It seems that these studies, much like ‘Proximal Origin’ … were used to stifle debate.”
Similarly, Mead told The Defender that, in recent years, “It seems clear that prestigious high-impact journals like Nature and The Lancet were inclined to prioritize certain narratives or findings that align with the interests of their influential stakeholders.”
“The result has been a suppression of alternative theories or evidence that diverges from these interests, undermining the integrity and objectivity of scientific inquiry,” Mead said, adding that this obstructed the “open exchange of information critical for understanding how this pandemic got created in the first place.”
“The more insidious fundamental issue concerns the biases of the editors themselves and the behind-the-scenes communications they receive from industry and government sources that want them to uphold a specific narrative,” Mead said.
Noting that Democrat members of the subcommittee appeared to defend former government officials like Fauci and Collins during the hearing, Mead said, “It seems fairly clear … that the mega financial relationships between biopharmaceutical companies and the Democratic Party have tainted the conversation around the politicization of science.”
“Why are Fauci and Collins being so assiduously protected by the Democrats when there is clear evidence of malfeasance and dishonesty on their parts?” Mead asked. “This seems to be yet another attempt to whitewash what happened during the pandemic.”
Deleted Thorp tweet contradicts his congressional testimony
Wenstrup questioned Thorp about a now-deleted March 2023 tweet referring to the origins of COVID-19, in which Thorp said, “One side has scientific evidence, the other has a mediocre episode of Homeland,” noting that “the tweet appears to contradict your testimony today.”
“I was not as careful expressing my personal opinions on my personal Twitter page as I should have,” Thorp said. “That does happen on social media. From time to time, I’ve gotten off Twitter and I highly recommend that.”
Wenstrup also asked Thorp about a November 2021 editorial in which he claimed that research allegedly conducted by the University of North Carolina, the EcoHealth Alliance and the Wuhan Institute of Virology on inserting furin cleavage sites into novel coronaviruses did not occur.
Thorp said he is under pressure to write a 720-word editorial “every two weeks” and, at the time, he “was going from what was reported in news stories” about the issue.
Mead told The Defender that Thorp’s admission that he was basing his editorials on information reported in news stories “is quite alarming.”
“Relying solely on mainstream news reports rather than direct investigation through primary sources and interviews with Ralph Baric and other researchers risks perpetuating misinformation and totally undermines the integrity of scientific inquiry,” Mead said.
‘Redactions were never mentioned’ during the hearing
“The government will never earn the trust back from the Americans by deeming all information that it doesn’t like as misinformation, nor will it deserve that trust if that’s what our government is doing,” Wenstrup said in his closing remarks.
But experts told The Defender that there was much that Wenstrup and other members of the subcommittee left out of Tuesday’s hearing.
“Congress needs to explore ways to cut off taxpayer funding for journals that do not want to be accountable to taxpayers,” Thacker said.
“The behavior of Nature has been atrocious, both in terms of the biased news they ran during the pandemic and the corrupt studies they published, such as the ‘Proximal Origin’ paper, which has all the hallmarks of ghostwriting that I looked into while leading congressional investigations,” Thacker added.
Mead said the relationships of key virologists with Fauci and the Wuhan Institute of Virology “should have been discussed openly” during the hearing.
“Retractions were never mentioned in the context of scientific journals and censorship by those journals,” Mead added. “Problems with the peer review process need to be more fully fleshed out, such as how to avoid overly biased reviewers being skewed in a particular direction to suit the editors’ own biases.”
“It would be interesting to find out how much of Science’s revenue depends on pharmaceutical advertising,” he added.
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Censorship & persecution of dissident voices continues across the world
The ‘cautionary tale’ modus operandi
Health Advisory & Recovery Team | April 15, 2024
Those who, like the members of HART, have been speaking out for three or four years about the perils of lockdowns, the lack of access to proper medical care and the utter debacle of the unsafe and ineffective vaccines, keep hoping the tide is turning. But for every stone upturned another boulder seems to descend to crush the truth. There is also no apparent end to the persecution of doctors speaking out.
Two physicians from opposite ends of the world and facing loss of their medical careers for speaking out against the vaccine saviour narrative, typify the current authoritarian approach. Charles Hoffe from Canada and Shankara Chetty from South Africa have two things in common, firstly both are clinicians serving a large local population and secondly both have shared their experiences widely. In Dr Chetty’s case he has reported his success at treating over 1000 covid patients with a combination of repurposed drugs including antihistamines in a clinical centre in rural South Africa with no access to oxygen let alone intensive care. In Dr Hoffe’s case, he first hit the headlines when he reported a high frequency of serious adverse events when his patients started receiving the mRNA vaccines.
Both these hard working and ethical physicians now, three years on, are being subjected to investigations by their medical boards. For Dr Chetty, he has previously been found guilty of professional misconduct but was called to attend a further hearing last week in front of the Health Professionals Council of South Africa. The results of their deliberations are awaited.
For Charles Hoffe the situation is even more bizarre. He was due for a hearing last week but when he submitted all the supportive evidence for his case, the health board in British Columbia deposited a large amount of evidence of their own but then threatened to invoke a ruling by which their evidence would be accepted as ‘fact’ by the court and Dr Hoffe and his legal team would be unable to cross question the data or present any information to the contrary. It looks like the right to a free trial has been abandoned in Canada, along with the right to free speech.
Below is a list of some senior clinicians and academics from across the world who have been vilified for speaking truth to power. It is by no means comprehensive.
USA:
Canada:
Australia:
- Dr Robert Brennan
- Dr Melissa McCann (subject to ‘re-education’)
- Dr Ros Neelon-Cook
- Dr Paul Oosterhuis
New Zealand:
Germany:
- Sucharit Bhakdi (acquitted of charge of antisemitism)
France:
- Dr Didier Raoult (an outspoken academic accused of unethical practice)
Switzerland:
- Thomas Binder (initially incarcerated in a mental institution)
UK:
- Dr David Cartland (GMC investigation ongoing)
- Professor Angus Dalgleish (clinical work suspended by St George’s Hospital)
- Dr Jayne Donegan (struck off by GMC, working as an independent)
- Professor Christopher Exley (told by Keele University to discontinue all research into Aluminium toxicity)
- Dr Aseem Malhotra (GMC initially declined to investigate until a legal case was brought to force an investigation)
- Mr Ahmad Malik (suspended by his private hospital for online posts)
- Dr Sarah Myhill (suspended by GMC, appeal pending)
- Dr Anne McCloskey (suspended by GMC in 2021, further hearing April 2024)
- Dr Sam White (NHS suspended him and GMC placed restrictions which were overturned in the High Court, currently working in independent practice)
This list is continuing to grow despite the increasing reports in the scientific literature which confirm almost everything they have said.
When does it stop?
THE APPROACHING ‘TIDAL WAVE’ OF CANCER
The Highwire with Del Bigtree | April 11, 2024
Many have abandoned the media’s desperate attempt to ignore why cancer rates are spiking. Now, the American Cancer Society is sounding the alarm, predicting an 80% increase in tumors by 2050. Meanwhile, independent researchers have stepped up and honed in on credible sources pointing to the mass COVID vaccine rollout in 2021 as the prime culprit.
Australia bins 35% of multi-billion dollar Covid vaccine supply
By Rebekah Barnett | Dystopian Down Under | April 12, 2024
As part of its pandemic response, the Australian government purchased 267.3 million doses of Covid vaccines, enough to vaccinate Australia’s population of approximately 26 million people ten times over.
But figures released to me by the Department of Health (DOH) this week confirm that, three years into the vaccine program, only 70 million doses, or 26% of the 267.3 million doses purchased, have been administered, while 35% of vaccines doses have been wasted since the start of the vaccine rollout.
Last week, the Australian reported that more than 35% of Covid vaccines were being tossed out as of January due to oversupply. The revelation came from the DOH’s public submission to the federal Covid inquiry.
The wording made it unclear if this was a cumulative figure or applicable only to the month of January, so I contacted the DOH to confirm the total wastage to date, along with some further questions on the value of doses purchased, delivered, and wasted, and exactly how many had been administered.
A DOH spokesperson responded,
“As of 31 March 2024 the total COVID-19 vaccine program wastage rate was at 35.69%. Australia’s wastage rate is within the World Health Organization (WHO) acceptable wastage parameters for multidose vials of 15% and 40%.
“Approximately 80% of COVID-19 vaccine wastage is attributed to expiry of doses across warehouses and vaccine administration sites.”
This appears to mean that 80% of the wasted doses simply expired on the shelf.
The remaining 20% of wasted doses would likely be due to administration sites not managing to use the entire contents of multi-dose vials once opened. While unopened vials have a shelf-life of anywhere between 9-18 months, opened vials must be used within 6-48 hours.
The DOH refused to confirm the value of doses purchased or wasted, or how many of the purchased doses have actually been delivered, “for contractural and security reasons.” The Australian government has repeatedly refused to release details of its tax-payer-funded Covid vaccine purchase agreements.
However, we know that total government spending on Covid vaccines and treatment supply amounts to over $18 billion, of which it appears that the lion’s share was allocated to purchasing vaccine doses.1
Most of these remain unused. DOH figures provided to me this week show that as at 3 April, only a quarter (70 million) of the 267.3 million purchased doses had been used, at a total usage rate of 26.2%
Of the remaining 197.3 million unadministered doses, the DOH advised that approximately 53 million doses have been donated as foreign aid.2
That leaves approximately 144 million doses, more than half of the total stockpile, either already expired, or likely to expire within the next several years, as booster rates hover below 10%. 3
As Australia’s vaccine purchases extend into 2023 and 2024, it is probable that a portion of these doses will still be viable up to 2025.
But even if vaccine doses never expired, it would take Australians 29 years to work their way through the glut, based on the five million boosters administered in the past 12 months.
As it stands, usage rates by brand are as below:
- Of 131 million Pfizer doses purchased, 48.5 million have been administered, a usage rate of 37%. 82.5 million doses remain.
- Of 29 million Moderna doses purchased, 7.5 million have been administered, a usage rate of 25.7%. 21.5 million doses remain.
- Of 56.3 million AstraZeneca doses purchased, 13.8 million have been administered, a usage rate of 24.5%. As the AstraZeneca stockpile expired on 20 March 2023, the remaining 42.5 million doses have been binned, unless they were donated as aid prior to this date.
- Stunningly, of 51 million Novavax doses purchased, only 273,700 have been administered, a usage rate of 0.5%. 50.7 million doses, 99.5% of the stockpile, remain. This is because by the time Novavax was approved for use, in December 2021, over 90% of Australians aged 16 and over had already been double vaccinated.
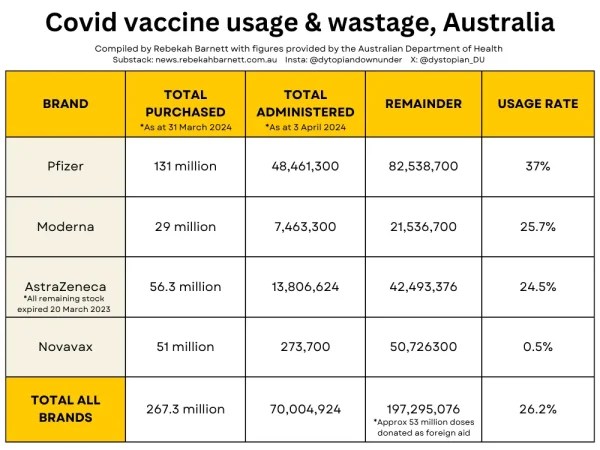
In a July 2022 article investigating Australia’s already apparent vast vaccine wastage, the ABC asked if perhaps the government had bought too many vaccines?
Deborah Gleeson, Associate Professor of Public Health at La Trobe University, criticised the government’s run on the global vaccine supply, suggesting that Australia had hoarded more than its share.
Prof Gleeson told the ABC,
“Australia really participated in a bigger trend that we’ve seen worldwide of wealthy countries buying up far more doses of COVID-19 vaccines than they needed early on in the pandemic. And this is a practice that unfortunately has continued.”
It’s enough to make advocates for global vaccine equity lose sleep at night.
The news of the Australian government’s wastage of billions of dollars worth of Covid vaccines comes as Australians are grappling with the soaring cost of living and the worst housing crisis on record, with over a quarter of a million Australians accessing homelessness services in 2022-2023.
The government webpage also details investment in aid program COVAX, and research and supply chain developments, including some funding for the development of a potential Covid vaccine (since abandoned). The page mentions a 10-year partnership with Moderna and the Victorian Government that will see Moderna build an mRNA vaccine manufacturing facility at Monash University Victoria. However, it is unclear if funding for the Moderna partnership comes from this $18 billion investment, or from other funding.
From a DOH spokesperson,
“Australia has donated more than 52 million doses to countries in the Indo Pacific and Southeast Asia.
· 23.6 million as part of our commitment to share 40 million doses through the Department’s procured supply; and
· 28.5 million as part of the commitment to share 20 million doses through DFAT’s agreement with UNICEF.
“Australia has offered a further 16.8 million doses to the COVAX Facility for distribution to participating developed and developing countries. Of the 755,200 doses that were accepted by the COVAX Facility, 14,400 have been donated.”
Note that because the DOH would not confirm how many of the 267.3 million purchased doses have been delivered, the precise number of doses sitting in the national stockpile cannot be determined. However, the vaccine agreement webpage does specify delivery dates of some purchases, and from this, it can be ascertained that the great majority of doses purchased have already been delivered.
To support my work, share, subscribe, and/or make a one-off contribution to DDU via my Kofi account. Thanks!
Featured Video

Rewriting the risk? Inside the government’s vaccine safety messaging
or go to
Aletho News Archives – Video-Images
Book Review
“Davos Can Really Replace the UN”
Inside the book that maps the architecture behind global governance — from the Epstein files to the Pact for the Future
Lies are Unbekoming | April 1, 2026
On June 13, 2019, the United Nations and the World Economic Forum signed a partnership deal to “accelerate the implementation of the 2030 Agenda for Sustainable Development.” That same evening, WEF president Börge Brende — Norway’s former Foreign Minister — had dinner with Jeffrey Epstein at Epstein’s Manhattan townhouse. The Epstein files, released January 2026, contain an exchange between the two from the previous year. Epstein to Brende: “Davos can really replace the UN. C21, cyber, crypto . genetics… intl coordination.” Brende back to Epstein: “Exactly — we need a new global architecture. World Economic Forum (Davos) is uniquely positioned — public private.”
The next day, the UN General Assembly adopted the framework for restructuring global governance.
That sequence — the partnership signing, the Epstein dinner, the candid admission about replacing the UN with a public-private architecture, and then the formal adoption — opens Jacob Nordangård’s The Digital World Brain. Pages two and three. Footnoted to the UN resolution number, the Epstein files, and the General Assembly record.
I keep coming back to it because it captures what this book does that almost nothing else in the independent research space manages. I’ve followed Jacob’s work for years now and interviewed him about his research. Each book peels back another layer of the same institutional architecture, and each time I think he’s reached the limit of what can be documented, the next one goes further. Nordangård doesn’t speculate. He doesn’t editorialize much. He lays institutional actions next to each other in chronological order and lets the pattern announce itself. … continue
Blog Roll
 Aletho News
Aletho News- How I fell foul of the BBC thought police
- The End of NATO
- 37 days of war on Iran cost US staggering $42bln, tracker shows
- Baghdad tells Asian refiners, traders to begin loading Iraqi crude amid Iranian exemption
- Under fire, Moscow and Tehran close ranks
- Iran, US receive Pakistan-mediated plan for ceasefire then final deal
- Iran submits demands for end to war as mediators scramble ahead of Trump deadline
- Iran Threatens Retaliatory Strike on Stargate AI Project in UAE
- US sent ‘a lot’ of arms to Iranian protesters – Trump
- Barak Ravid Launders Deception To Allow Trump To Back Off Of His Power Plant Threat – Again
- If Americans Knew
- Trump poised to “blow everything up” (ie. commit war crimes) in Iran – Daily Update
- In Iran, Israel-US take aim at “reason, research, and freedom of thought” – Daily Update
- US loses planes over Iran, Israel downgrades Lebanon war goals – Daily Update
- Israel Is Blocking Palestinians from Easter at Church Where Jesus Resurrected
- Plot to assassinate Palestinian activist follows harassment campaign promoted by Zionist groups and elected officials
- Prominent New York synagogue hosts presentation on why U.S. Jews should support the ethnic cleansing of Gaza
- Tapper vs. Piker: Is the CNN Anchor Auditioning for David Ellison?
- Shouldn’t Democrats Be Able to Condemn Genocide?
- Israel-US kill negotiators, destroy civilian structures, but Iran’s military capabilities still largely intact – Daily Update
- ‘War crime’: Global condemnation as Israeli ministers celebrate death penalty law targeting Palestinian prisoners
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
