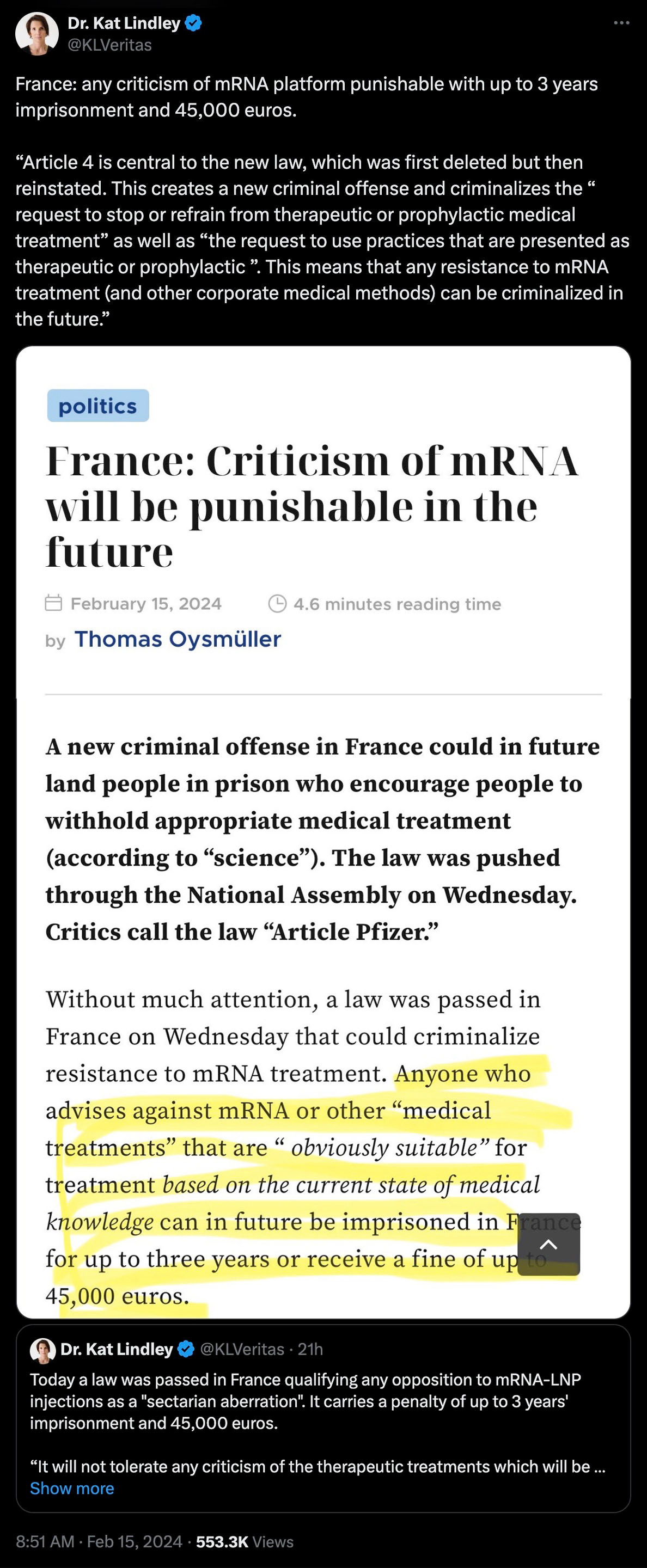
France: ANY Criticism Of The mRNA DEATHVAX™ Platform Punishable Up To 3 Years Imprisonment And 45,000 Euros
2nd Smartest Guy in the World | February 15, 2024
The WEF-captured government of France has pushed through a draconian new law entitled Article 4. This Orwellian and unconstitutional color of law power grab is a purposely poor attempt at obscuring the irrefutable slow kill bioweapon death and destruction data.
What makes Article 4 particularly incendiary is that the majority of the French population has been outright refusing all “vaccinations.” Throttling their free speech as it pertains to gene modifying poisons will only increase the already heightened tensions between the criminal Macron administration and the awakening French populace, by design.
Between WEF puppet Trudeau in Canada and WEF puppet Macron in France, there is now a race to create the most totalitarian technocommunist nation in the West, with France now taking a slight lead; to wit:

These policies and “laws” are nothing more than an extension of the ongoing democide, and the associated iatrocide.
Meanwhile, back in the USSA, the Center for Disease Crimes (CDC) is still at it with their “Trust the Science” mendacity and murder:

Readers of this Substack fully appreciate the myocarditis and turbo cancer epidemics currently underway — not to mention soaring excess non-PSYOP-19 mortality — since the rollout of the “vaccines:”
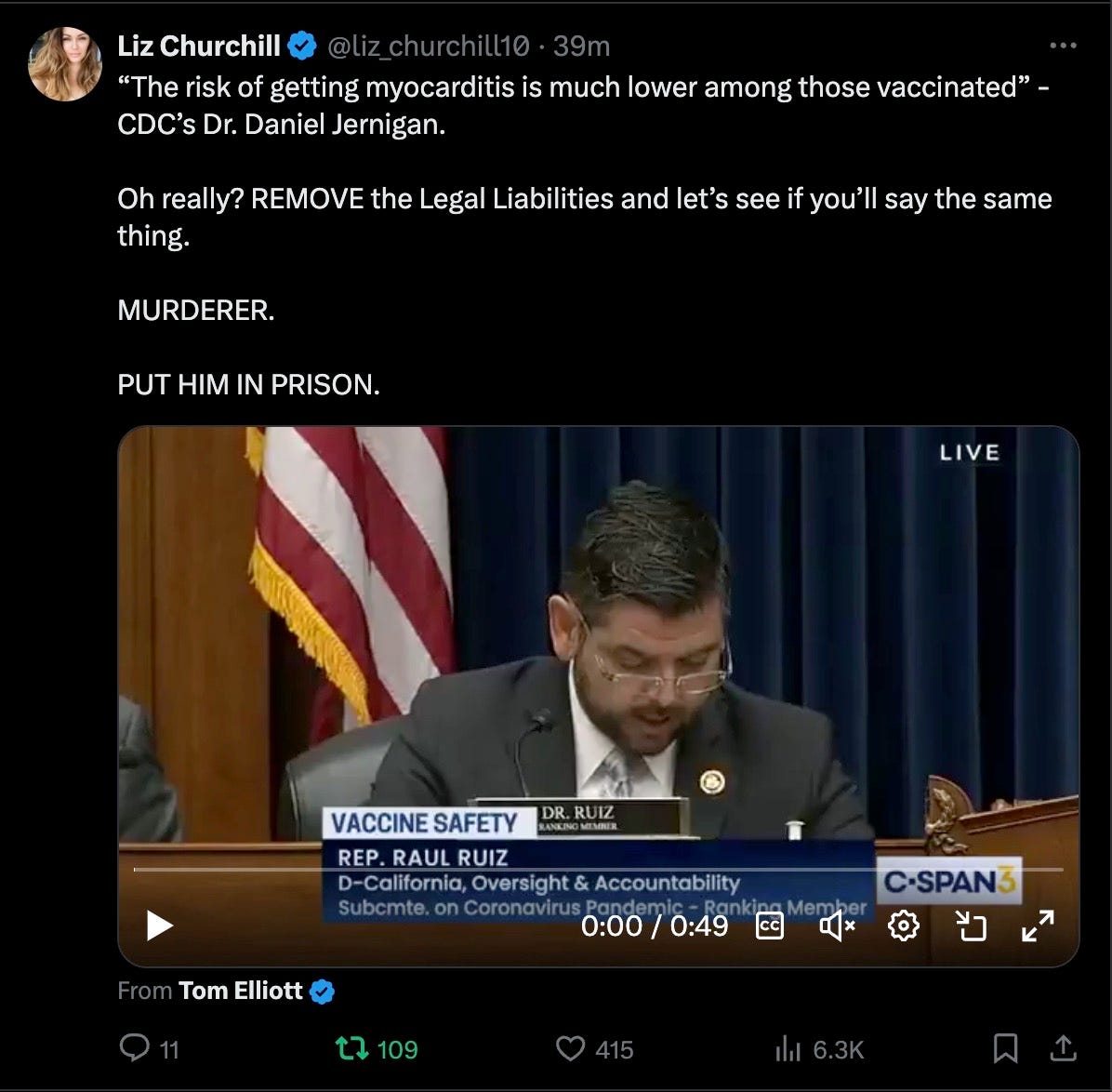
Removing all BigPharma legal liabilities and prosecuting the various “health” agencies like the FDA, CDC, NIH, et al. has never been more urgent.
France’s Article 4 is just a hint at what is to come, especially if the WHO’s Pandemic Treaty scam ever passes in the various nations that they are attempting to further hijack.
They want you dead.
Do NOT comply.
Freedom Convoy leaders sue Trudeau regime for targeting protesters with Emergencies Act
By Anthony Murdoch | Life Site News | February 15, 2024
OTTAWA, Ontario — On the second anniversary of Prime Minister Justin Trudeau’s government’s use of the Emergencies Act (EA) to quash the truckers’ Freedom Convoy in 2022, the heads of the protest, Tamara Lich and Chris Barber, and a host of others have filed a $2 million lawsuit against the Trudeau government.
The lawsuit, announced yesterday by Freedom Convoy lawyer Keith Wilson, includes Lich as well as other convoy leaders Chris Barber, Tom Marazzo, Danny Bulford, and a host of others.
“On the 2-year anniversary of the Federal Government illegally invoking war measures against its citizens and targeting key protestors in Ottawa by freezing their bank accounts, today Tamara Lich, Chris Barber, Tom Marazzo, Danny Bulford and other protestors who were targeted by @JustinTrudeau and @cafreeland have filed lawsuits against the Federal Government.”
Wilson said that Section 24 of Canada’s Charter of Rights and Freedoms “gives Canadians the right to sue their government for damages when Charter rights are violated.”
“Doing so affirms the seriousness of respecting Charter rights and is intended to deter future governments from breaching Canadians’ fundamental rights.”
Wilson noted that the lawsuits seek $2 million in damages.
Lich, on X (formerly Twitter) noted about the lawsuit on Wednesday that “Accountability is a thing. It’s go time!”
“Happy Emergencies Act Day! I hope you all look back and fondly remember how your government shot you with rubber bullets and tear gas for your own good!” she also wrote.
Tom Marazzo, who was also involved with the Freedom Convoy and is a 25-year Canadian army veteran, said about it that it was “2 years ago today, instead of celebrating Valentine’s Day, the most corrupt government in Canadian history, launched an all out illegal assault on the Rights and Freedoms of every Canadian citizen in Canada, with the help of the NDP, Bloc, MSM and the Banks.”
“2 years later, they are all still in power with no end in sight. The one question that is never addressed, by any of them is why did Canadians feel so desperate that they had to go to Ottawa in the first place???” wrote Marazzo on X.
Further details about the lawsuit will be forthcoming in the next few days.
The lawsuit comes just after a Canadian federal court last month ruled that the Trudeau government’s use of the Emergencies Act to quash the truckers’ Freedom Convoy in 2022 was unconstitutional. The court ruled that the use of the EA was a direct violation of the Charter and thus “not justified.”
The EA controversially allowed the government to freeze the bank accounts of protesters, conscript tow truck drivers, and arrest people for participating in assemblies the government deemed illegal.
An investigation into the use of the EA, as per Canadian law, was launched by Trudeau. However, it was headed by Liberal-friendly Judge Paul Rouleau, who led the Public Order Emergency Commission. This commission was to investigate the Liberal government’s unprecedented use of the EA against the anti-mandate Freedom Convoy protest. Unsurprisingly, the commission exonerated Trudeau’s use of the EA.
Freedom Convoy leaders Lich and Barber have been involved in a lengthy trial after being charged and taken to court by the federal government for leading the protests. The trial has not yet concluded and has been put on hold, with its resumption date uncertain. It is also not yet clear how the recent court ruling will affect the trial.
In early 2022, the Freedom Convoy saw thousands of Canadians from coast to coast come to Ottawa to demand an end to COVID mandates in all forms. Despite the peaceful nature of the protest, Trudeau’s government enacted the EA on February 14, 2022. Trudeau revoked the EA on February 23.
During the clear-out of protesters after the EA was put in place, one protester, an elderly lady, was trampled by a police horse, and one conservative female reporter was beaten by police and shot with a tear gas canister. Rebel News reporter Alexa Lavoi, while covering the Freedom Convoy, was shot point blank in her leg with a rubber pellet, which police were using against protesters.
On February 14, 2022, the day the EA was invoked, Canadian Deputy Prime Minister and Minister of Finance Chrystia Freeland mandated certain bank accounts be frozen under the EA. In total, close to $8 million in funds from 267 people were locked. Additionally, 170 bitcoin wallets were frozen.
The freezing of bank accounts by Freeland without a court order was an unprecedented action in Canadian history and was only allowed through the Liberal government’s invocation of the never-before-used EA.
New York’s Proposed Minor Consent Law ‘Dangerous’ and ‘Misleading,’ Critics Say
By Suzanne Burdick, Ph.D. | The Defender | February 12, 2024
New York state lawmakers are weighing legislation that would allow any child or teen under 18 to seek out and consent to medical treatment — including vaccines, dental procedures, hospitalization and even surgery — without parental consent, as long as the minor appears to have the mental capacity for making that decision.
Assembly Bill A6761, introduced by New York Assemblymember Karines Reyes (D-Bronx), also would allow Medicaid funds to pay for procedures and drugs administered to children.
Proponents of the legislation, such as the American Civil Liberties Union of New York, say the measure is about ensuring all youth have access to quality care.
But critics, including John Gilmore, founder and executive director of the nonprofit Autism Action Network, said the bill is dangerous.
“The bill’s biggest problem,” Gilmore told The Defender, “is that it allows any medical procedure to be done to children of any age without parental knowledge or consent. That’s the kicker.”
Gilmore said the bill has another problem, too: The “active summary” statement on the official New York Assembly website says it “allows homeless youth to give effective consent to certain medical, dental, health, and hospital services.”
But Gilmore said that statement is “deliberately misleading” because the bill’s text applies to more than just “homeless” youth seeking “certain” services.
The bill states:
“Any person, including a minor, who comprehends the need for, the nature of, and the reasonably foreseeable risks and benefits involved in any contemplated medical, dental, health, and/or hospital services, and any alternatives thereto, may give effective consent to such services for themself, and the consent of no other person shall be necessary.”
“Albany is lying” about the bill, according to Autism Action Network.
Michael Kane, a New York resident and founder of Teachers For Choice, agreed. “It’s a complete lie to say the bill applies only to homeless children or runaways — and it’s a dangerous one,” Kane told The Defender. “It’s imperative that legislators understand what the bill really does,” Kane said.
With New York lawmakers considering close to 10,000 bills, legislators may rely on a bill’s one-sentence summary — rather than reading its full text — for deciding how they vote, according to Gilmore.
The bill has a companion in the Senate (S8352), introduced Jan. 19 by state Sen. Rachel May (D-Syracuse). The bills share identical text.
Unclear how practitioners would assess minor’s ‘capacity to comprehend’
According to the latest version of the bill, a minor could consent to:
- General medical, dental, health and hospital services.
- Mental health outpatient services.
- Substance abuse treatment.
- Immunizations.
- Family planning services.
- Sexually transmitted disease (STD) diagnosis and treatment.
The bill states that a practitioner may administer a vaccine if “they have reason to believe that a person in parental relation to the child … objects to the immunization.”
It also states, “A child who may give effective consent [to various medical interventions] … may give such consent to their own immunization, and the consent of no other person shall be necessary.”
The bill allows minors under 16, in certain circumstances, to access psychotropic drugs or psychotherapy without parental consent.
Psychotropic drugs include a host of pharmaceutical products, including medications for depression, anxiety, sleep disorders, schizophrenia, bipolar disorder and attention-deficit/hyperactivity disorder.
Current New York law allows minors 16 or older residing in a hospital to agree to psychotropic medications without parental consent if any of the following conditions are met:
- A parent or guardian “is not reasonably available” and the physician determines “the minor has the capacity”; or
- requiring parental consent “would have a detrimental effect on the minor”; or
- the parent has refused consent, providing that two physicians (including a psychiatric doctor who does not work for the facility) agree the medications are in the minor’s best interests.
A6761/S8352 would allow minors under 16 in these circumstances to do the same, as long as the youth “comprehends the need for, the nature of, and the reasonably foreseeable risks and benefits involved.”
The bill does not include detailed information on how medical practitioners would assess a minor’s capacity to comprehend the potential risks of a potential treatment.
It does, however, define “capacity” as follows:
“The minor’s ability to understand and appreciate the nature and consequences of the proposed treatment, including the benefits and risks of, and alternatives to, such proposed treatment, and to reach an informed decision.”
Children’s Health Defense General Counsel Kim Mack Rosenberg told The Defender that informed consent is a “serious” thing, but this legislation devotes “little attention to how to determine if a child can truly exercise informed consent, how to obtain that consent and why true informed consent is critically important.”
Who is a ‘minor’?
The bill does not provide a clear definition of “minor” that applies across all amended laws. However, some sections of the law define or describe the age thresholds related to minor consent:
- In the amendments to the mental hygiene law section 9.13(a), anyone under 16 would still need parental/guardian consent to be admitted as a voluntary patient to a hospital.
- In amendments to mental hygiene law 33.21(a)(1), a “minor” is defined as a person under 18, excluding some special cases like emancipated minors or minors who are parents.
- In amendments to section 2305 of public health law, treatment for STDs without parental consent is allowed for those under 21.
However, earlier sections of the bill do not specify any age range for minors, suggesting even young minors could consent as long as they demonstrate appropriate “capacity.”
Even infants?
It appears the bill’s sponsors may believe that even an infant can give consent. That’s because section 18 of public health law omits previous language stating that children older than 12 can determine who gets access to their medical records.
This deletion suggests that a child of any age no longer “may” but “shall be notified of any request by a qualified person to review their patient information” and deny access to it if they so desire.
The bill states that an infant can choose to withhold information from its parents, without explaining how that would be possible:

In summary, there isn’t one definition of “minor” in the bill, but it seems for most purposes “minor” refers to anyone under age 18.
Minor consent bills bulldoze’ over decades of laws honoring parental rights
The U.S. has a strong legal history going back many decades that honors parental rights and recognizes that the state should step in only where parents are unfit to care for their children, Rosenberg said.
“Minor consent bills bulldoze over those longstanding decisions,” she said. “They try to exclude parents from medical decision-making and take over the parenting role.”
Rosenberg said she’s seen more bills like this recently being introduced in other states, such as Vermont. “We [CHD] successfully stopped one in the District of Columbia and are fighting laws and regulations elsewhere,” she said.
Kane called the bill “just horrendous” because it “completely eradicates parental control over what happens medically to our children.”
Meanwhile, a staff member for Reyes’ office who chose to remain anonymous told The Defender she disagreed, saying the bill was primarily about ensuring all kids have “access to care” and that it included “guardrails” to ensure that not all parental consent was stripped away in all situations.
For instance, the bill explains that a minor must “knowingly and voluntarily” seek care, the staff member said.
But Rosenberg said she’s concerned about the legal ramifications of the bill’s broad language — which appears to erase parental consent for “any contemplated medical, dental, health, and/or hospital services, and any alternatives thereto.”
Rosenberg told The Defender the bill was “rife with problems too numerous to address in brief remarks.”
The bill makes clear, she said, that minors can consent to vaccinations without their parents’ knowledge or consent — and that medical staff and insurance companies must hide that vaccination information from the parents unless the child permits them to share it.
Children “literally may inadvertently take their lives into their own hands” if they make serious healthcare decisions without parental involvement, Rosenberg said.
For example, children frequently don’t know their own health history — let alone their family health history — which may put them at an increased risk for an adverse reaction to a medication or treatment, she explained.
Rosenberg said:
“The legislators supporting these bills need to ask themselves what they would do if a child or grandchild of theirs consented to a surgical procedure of whatever kind requiring anesthesia and the child suffered death or irreversible harm if they had a reaction to the anesthesia.
“Is that a phone call they’d like to receive?”
‘Not a chance’ bill’s sponsors unaware of misleading statement
New York already has a law on the books about homeless youth giving consent for certain services.
Passed in 2022, A09604/S08937 allows “runaways and homeless youth under the age of 18 who are receiving approved crisis or support services to consent to medical, dental, health and hospital services.”
Gilmore, who has done legislative analysis in New York for 23 years, said, “Both Rachel May and Karines Reyes voted for the bill that was passed in 2022.”
So why would they talk about homeless youth in the summary of the new measure they introduced?
A staff member for Reyes’ office told The Defender a bill’s summary statement is written by lawyers — not by the legislator who introduces the bill.
It’s plausible the lawyers chose that language since the bill amends the same section of public health law (2504) that was amended earlier in the law about homeless youth and runaways, the staff member said. However, the staff member confirmed that the present bill does pertain to all minors.
The Defender also reached out to May’s Legislative Director Eric van der Vort, but he did not respond by our publication deadline.
Gilmore said he contacted legislators, too, but didn’t get a straight answer. When he asked van der Vort about the summary language, “he simply refused to address it in any way,” Gilmore said.
Reyes’ Chief of Staff Justin Westbrook-Lowery confirmed for Gilmore that the bill applies to all minors in New York but didn’t explain why the summary statement talked about homeless youth.
Amy Paulin (D-Scarsdale), who chairs the Assembly Committee on Health and co-sponsored the bill, “has a large staff and they’re very good at what they do,” Gilmore said. “There’s not a chance that they aren’t quite aware” that the bill’s summary statement doesn’t match what the bill would do.
Kane said he’s heard from New York legislators and staffers that they believe the bill affects only homeless children.
“There’s a lot of people in the Assembly starting to co-sponsor the bill, which is scary,” he said. “We don’t want this thing passed so that we end up litigating against it for the next five years.”
The Defender asked May’s media relations staff what May would like to tell parents concerned about being excluded from medical decision-making regarding their child’s health, but did not receive a response by our publication deadline.
Suzanne Burdick, Ph.D., is a reporter and researcher for The Defender based in Fairfield, Iowa.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Who does ‘our’ NHS really serve?
Still relentlessly promoting covid ‘safe and effectives’
Health Advisory & Recovery Team | February 7, 2024
A concerned reader sent in this letter inviting him for more covid and flu injections, as he was considered a ‘priority’ case:


The fact that the NHS is wasting millions of taxpayer pounds continuing to promote and administer these ineffective and harmful products is symbolic of what the health service has become; another cog in the medical industrial machine, whirring to improve Pharma profits with little or no concern for end-user health. In a service allegedly crushed by lack of resources, why on earth are they still pushing these products on an unsuspecting public?
You will note in the full letter that:
- There is no mention that the injections stop infection;
- There is no mention that the injections stop transmission;
- They make the dubious claim that injections lead to “less severe illness” without backing up this statement.
- They use the misleading statement that ‘seasonal vaccines have proven safety records‘. This is certainly not the case for covid injections as they have not existed long enough and no-one has bothered to collect the data.
It seems that even the NHS has abandoned the mendacious claims originally attached to the ‘Safe and Effectives™’ probably because they know it would open them up to legal action. The propaganda job is complete. For those poor souls still unquestioningly worshipping at the alter of the quasi-religious NHS, a promise of real benefit is now surplus to requirements in the ad campaign. It has seamlessly transformed into an annual ritual to benefit drug companies whilst causing insidious harm to the collective health of the nation. What a clever spell they have cast to make entire populations believe that good health is only achievable by injecting unidentified substances into their body on a seasonal basis. And if they feel awful directly afterwards? It means its working!!
Evil genius.
If anyone can find the time and has received such a letter, the claim of “proven safety records” deserves a Freedom of Information request to “please supply all reports memos papers statistical analyses etc supporting the claim of “proven safety records”. We would love to see the response should one be forthcoming. We won’t hold our breath.
Professor Didier Raoult Calls for COVID-19 Vaccine Moratorium
BY JOHN LEAKE | COURAGEOUS DISCOURSE | FEBRUARY 4, 2024
Of the many remarkable characters we write about in our book The Courage to Face COVID-19: Preventing Hospitalization and Death While Battling the Bio-Pharmaceutical Complex, Professor Didier Raoult may be the most fascinating and colorful. A May 12, 2020 feature in the New York Times introduced him to American readers as follows:
Raoult … has made a great career assailing orthodoxy, in both word and practice. “There’s nothing I like more than blowing up a theory that’s been so nicely established,” he once said. He has a reputation for bluster but also for a certain creativity. He looks where no one else cares to, with methods no one else is using, and finds things.14
A tireless researcher, he has published 2,300 papers and is the most cited microbiologist in Europe. He and his team have discovered 468 species of bacteria—about 1/5 of all those named and described. The bacteria genus Raoultella was named in his honor. He is probably best known as the discoverer of the so-called giant virus, so large it had previously been mistaken for an intracellular bacterium. He has won 13 major awards and is a Commander of the National Order of Merit.
Like Dr. McCullough, Professor Raoult strongly advocated early treatment of COVID-19, and he conducted multiple studies demonstrating the efficacy of hydroxychloroquine combined with azithromycin, especially when administered early. In return for his efforts to save his patients, he has been relentlessly persecuted by France’s official medical establishment in Paris.
Now comes the news that Professor Raoult is calling for a moratorium on COVID-19 vaccines. The following is a translation from his recent, French language post on X:
Propaganda and knowledge. We’re the good guys, but we’re not ignorant! When vaccines were developed against Covid, 3 types of vaccines were proposed: – Traditional vaccines (as quickly available as the others) made in China with the entire inactivated virus. These vaccines have not been authorized in France for reasons that escape me. This type of vaccine, comparable to that against the flu, carries fewer unknown risks and does not fight against a single target of the virus: the Spike. I feared, and this happened, that the mutations of the virus and its respiratory specificity would not provide lasting immunity and that the vaccine would not have a very long duration of protection because I published the first known case of reinfection with covid. The disease being poorly immunizing, the vaccine would not do any better.
The second vaccine (the English one from Astra Zeneca, that from Johnson and Johnson, and the Russian Sputnik) is a vaccine based on a virus (Monkey Adenovirus for Astra Zeneca), transformed by integrating the Spike gene. It doesn’t integrate or replicate. I was the first in France to report an accident of cerebral venous thrombosis, this phenomenon is well described in particular in young women and England stopped its prescription for those under 50, followed by many countries and finally it is no longer used in France. There are millions of expired doses left.
The 3rd group of vaccine (Pfizer, Moderna) consists of the injection of RNA coding for the Spike whose elements have been modified so as not to be eliminated quickly. This vaccine is included in a lipid nanoparticle to be able to enter cells. This vaccine, in addition to the disadvantages common to the others, presented unforeseen side effects: extremely frequent menstrual disorders (now recognized by the CDC) of which no one can say whether they will be associated with consequences on fertility, myocarditis and sometimes fatal pericarditis in young people (mainly boys, now recognized by the CDC) and rare thromboses of the veins (recognized by all scientific authorities).
None of these vaccines had been evaluated for mild or asymptomatic forms and therefore for the prevention of contagion. They could not claim to eradicate a disease which, moreover, was circulating among animals. Vaccination was then only justified in those who were at risk of serious forms (subjects over 65 years of age and fragile subjects (obese, immunocompromised). Now we see that the quality controls on batches of Pfizer vaccines do not appear to meet required standards. There should be no DNA or minute doses due to the risk of introducing it into cells through nanoparticles, because DNA easily enters the nuclei and integrates into the chromosomes like a virus with consequences unknown because lymph node cancers can be the natural consequence (Epstein Barr virus, HTLV virus and Helicobacter pylori). The quantity of DNA in the vaccine doses is much higher than that announced in the samples tested. Each batch of Pfizer should be tested, it is easy in any laboratory to do a DNA PCR to check the quantity. Let those who don’t believe it do so!
Finally, we cannot inject a drug without knowing what it will produce in the body. A very unpleasant surprise published in Nature in December 2023 shows that modified RNAs can produce unknown proteins. This should be explored on a large scale because among the proteins that could be created in this way, one of them is an amyloid which would be released while it is in the natural Spike, coated in a protein and without danger. These free amyloids, which can be produced by vaccines through reading errors, can be the cause of amyloidosis plaques which cause various diseases, including neurological ones. All this is knowledge for the knowers, not opinions for scavengers. Given the demonstration of this phenomenon, the consequence of vaccination must be studied in humans, which has not been done.
At this stage of knowledge, it is reasonable to follow Denmark into a moratorium on Covid vaccination. Indeed, the effectiveness is doubtful because new variants appear which make current vaccines ineffective (millions of doses have been thrown away) and the manufacturing of new vaccines based on current variants will be outdated when they are available because new variants will circulate. Other countries are reaching these conclusions, the “surgeon general” of Florida has called for a total stoppage of the Pfizer vaccine, the attorney general of Texas (Mr. Paxton) has just attacked Pfizer for disinformation and censorship (what a reversal!). American and English parliamentarians question administrative and political leaders about their decisions, where we are surprised to see Fauci, the head of covid management in the USA, saying that social measures (masks, confinement, curfew) do not serve to nothing and B. Johnson apologize for his management in England! Humans are not stupid, covid vaccination rates and Pfizer shares are plummeting. It is time to take up the problem, de-dramatize it and treat the patients, re-evaluating it by competent people. At least ten molecules have shown effectiveness on the disease and do not cost much. This must stop being an opportunity for the industry and become a problem for doctors again!
The covid booster cancer time bomb
By Professor Angus Dalgleish | TCW Defending Freedom | January 30, 2024
I have previously reported on my concern about the rise in stable cancer relapses that I have witnessed in my melanoma clinic.
None of these patients of mine presented with the classic prodrome of relapse that I had always noticed previously, such as severe depression due to bereavement, divorce or bankruptcy. Indeed the only thing I found they had in common was to have had a recent booster mRNA covid vaccine. I phoned around my colleagues not only in the UK but also in Australia to check their experience. In no case did they deny such a link. Indeed, they were equally alarmed at the association between booster vaccines and relapse that they too were witnessing, as well an increase in new cancers, particularly in those below 50 years old. In addition to melanoma these colleagues were also very concerned about a sudden big increase in young patients with colorectal cancer.
Rather than instigating a proper inquiry to investigate this when we raised these concerns, the medical authorities told us all that what we were witnessing was a coincidence, that we had to prove it and above all, not to upset our patients.
Recently the American Cancer Society (ACS) has warned of a surge in new cancer cases in the US this lastyear of over 2million, with many of these cases occurring in younger patients. Indeed, the chief scientific officer of the ACS, William Dahat, announced in addition that cancers were presenting with more aggressive disease and larger tumours at the time of diagnosis, especially in younger patients. Of further interest it noted a difference in the microbiome (the community of micro-organisms such as fungi, bacteria and viruses that exist in a different environment) between patients under 50 compared with those over 50.
This surge mirrors a report from Phinance Technologies of late last year which analysed in detail data from the UK Office for National Statistics (ONS) which showed that disability and deaths in 2021 and 2022 had increased dramatically in all age groups, but especially in the 15-44 age group.
The Lancet also published an article before Christmas reporting excess deaths post covid pandemic to be up by 11-15 per cent over than expected for under-25s and for between 25-49 year olds. This is in fact the pattern found in many countries that have looked at the data. Germany for example has reported excess deaths rising from 7 per cent in 2020 to 24 per cent in 2023.
What makes this all the more surprising is that negative deaths should be the norm after a pandemic as you cannot die twice!
The link between covid vaccines and myocarditis and early death particularly in the young, highlighted by Peter McCullough and colleagues as well as by Aseem Malhotra here in the UK, is incontestable. Now we have a confirmatory report from the CDC in the US, data that the authorities here have refused to act on so as not to alarm vaccinated patients!
Although it is obvious that these excess deaths are real and are continuing to rise, all we get from our Chief Medical Officer, Sir Chris Whitty, are risible attempts to explain away the increase, such as that it is a result of patients not getting their statins in lockdown (hey, patients under 55 do not get statins routinely!) The situation is no better in the US where Harvard researchers have put the blame on sleep disturbance!
The first obvious candidate is lockdown itself when the National Health Service became the National Covid Service and all screening was cancelled or delayed, resulting in an increase in cancer detection and late presentation. Many negative lifestyle factors almost certainly increased as a result of lockdown, such as a lack of exercise and too much food, especially takeaways.
What very few of these reviews consider is that this rise in excess deaths could be a result of the booster vaccine programme, even it clearly follows the vaccine rollout programme starting in 2021 and increasing in 2022 and 2023.
With regards to the link to cancer, there are numerous reports in the literature of cancers arising within days of the vaccines being administered, especially in the case of lymphomas and leukaemias. There are several reports of PET scan mapped tumours exploding at the site and draining area of covid injections with the advice to inject covid vaccines away from known cancers! Outside my clinical observations, several friends have developed cancer after a totally unnecessary covid booster taken only to facilitate travel.
For a possible association between a booster vaccine and the appearance of cancer we need a plausible scientific causal explanation. Unfortunately for those who still insist that these cases are mere coincidences, there are several compelling ones to choose from:
Firstly, it has been reported that T cell responses are suppressed after the boosters (not the first two injections) and that this is especially marked in some cancer patients.
Secondly, the antibody repertoire switches after the first booster from a protective IgG1 and IgG3 dominant B cell response to a tolerising IgG4 one, made worse by further boosters, as reported in a recent Science Immunology paper. As many cancers are controlled by effective T cell led immunity, the sudden perturbation of this control would clearly explain the development of B cell leukaemia and lymphomas, melanoma renal cell cancers and colorectal ones, all tumours which can respond to immunotherapy.
Another report by Loacker et al in Clin Chem Lab Med shows that mRNA vaccines increase PD-L1 on granulocytes and monocytes, which means they effect the very opposite of what the immunotherapy agents do against these tumours, and whichin turn explains why many of these tumours appear to be resistant to this otherwise effective therapy. Taken together, the effect on the immune response of these boosters can easily explain the relapses and so-called turbo-charged cancers appearing.
Other reports document the presence of DNA plasmids and SV 40 (a known cancer-inducing gene) sequences, as well as the ability of mRNA to bind to important suppressor genes. Although this is controversial and has been challenged, it has led to the realisation of significant batch-to-batch variation that could enhance the cancer process yet probably not manifest itself for a few years. The very possibility that we could be sitting on a vaccine-inducing cancer time bomb means that we must never again get involved into a mass vaccine programme for another possible Disease X.
But unless the government wakes up to this now, we will be at the mercy of the World Health Organization doing the very same thing when they decide to release the Disease X virus in order to take back control and destroy our lives all over again.
The “NO LIABILITY” aspect of the unlicensed, novel vaccine developed in 100 days is in-your-face in the WHO’s proposed treaty
BY MERYL NASS | FEBRUARY 2, 2024
The globalist lawyers who drafted the pandemic treaty definitely anticipated injuries from the 100 day vaccines. So what did they do? They made sure that all the nations signing up to the Treaty “shall shall shall” i.e., MUST give the WHO, its lawyers, the nations, the manufacturers, the doctors and anyone else involved a bullet-proof liability shield.
Just in case someone did not understand, they said it 3 times, 3 different ways, in 3 paragraphs. I screenshot what they said so there would be no confusion.
If you don’t want the mandated experimental vaccines for which nobody is liable, join us to fight against this nonsense. DoorToFreedom.org

https://apps.who.int/gb/inb/pdf_files/inb7/A_INB7_3-en.pdf
Featured Video
Laith Marouf: Hezbollah’s position on US-Iran ceasefire
or go to
Aletho News Archives – Video-Images
From the Archives
Is Israel to blame for the Iraq War?
American Goy | March 10, 2008
I am so tired of this old canard that “Israel had nothing to do with USA’s war with Iraq – in fact, it officially advised America against it”.
Bullshit. … continue
Blog Roll
 Aletho News
Aletho News- Laith Marouf: Hezbollah’s position on US-Iran ceasefire: What you’re not being told
- Israel’s priority lies in destroying chances of peace between Iran, US: Ex-UN nuclear chief
- Ceasefire for all or for none: Iran shuts Hormuz over Lebanon attacks
- Strait of Hormuz is Iran’s ‘nuclear weapon’ that forced US retreat: Medvedev
- Energy crisis will last for months – Kremlin envoy
- Europe’s quiet role in the war on Iran
- Forty days that shook the Empire: How Iran turned the tables on US and prevailed
- Netanyahu unilaterally declares Lebanon outside of ceasefire deal
- Israeli leaders: ‘Not a single goal’ achieved in war with Iran
- What on earth just happened? Trump, Iran, and the unlikely ceasefire
- If Americans Knew
- Gazans face a triple crisis: severe shortages of water and bread, healthcare in tatters
- NY Times reports how Netanyahu took the US into Iran War
- A sigh of relief over Iran, but Gaza and Lebanon in dire straits – Daily Update
- Thousands dead and neighborhoods razed to the ground: Aid agencies fear southern Lebanon is becoming the new Gaza
- The war the US is fighting for Israel could cost trillions
- ‘Cigarette Burns, Nail Wounds’: Toddler Tortured in Gaza to Coerce Father
- Trump Says US Sent ‘a Lot of Guns’ to Protesters in Iran
- Israeli forces destroy 17 UN peacekeeper cameras in south Lebanon
- US-Israeli strikes ‘completely destroy’ synagogue in Tehran
- Archbishop for US Military Says Iran War Is Unjust Under Catholic Teaching
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
