‘If We Get Away With It, It’s Legal’: Documents Reveal New Details on U.S. Government’s ‘Censorship-Industrial Complex’
By Michael Nevradakis, Ph.D. | The Defender | November 29, 2023
Government agencies, private-sector firms, academia and nonprofits were collaborating to combat alleged “misinformation” and “disinformation” as far back as 2017, according to new documents released Tuesday.
The “CTIL Files” — which refer to the Cyber Threat Intelligence League, or CTI League, a key player in the so-called “Censorship-Industrial Complex” — are based on documents received from an unnamed but “highly credible” whistleblower, according to investigative journalists Michael Shellenberger, Alex Gutentag and Matt Taibbi, who released the files.
The new documents rival or exceed the “Twitter Files” and “Facebook Files” in “scale and importance,” according to the journalists, two of whom — Shellenberger and Taibbi — were instrumental in releasing many of the “Twitter Files” that first called attention to the “Censorship-Industrial Complex.”
A comprehensive picture of the birth of the ‘anti-disinformation’ sector
The documents, which the journalists detailed on Substack, center around the activities of the CTI League, which “officially began as the volunteer project of data scientists and defense and intelligence veterans but whose tactics over time appear to have been absorbed into multiple official projects, including those of the Department of Homeland Security (DHS).”
According to the journalists, the CTI League documents “offer the missing link … to key questions not addressed in the Twitter Files and Facebook Files” and “offer a comprehensive picture of the birth of the ‘anti-disinformation’ sector.”
“The whistleblower’s documents describe everything from the genesis of modern digital censorship programs to the role of the military and intelligence agencies, partnerships with civil society organizations and commercial media, and the use of sock puppet accounts and other offensive techniques,” the journalists wrote.
Documents in the “CTIL Files” show members of the CTI League, DHS officials and key figures from social media companies “all working closely together in the censorship process.”
This “public-private model” laid the groundwork for “anti-misinformation” and “anti-disinformation” campaigns launched by the U.S. and U.K. governments in 2020 and 2021, the journalists wrote, including attempts to circumvent First Amendment protections against government censorship of speech in the U.S.
Such tactics included “masking censorship within cybersecurity institutions and counter-disinformation agendas; a heavy focus on stopping disfavored narratives, not just wrong facts; and pressuring social media platforms to take down information or take other actions to prevent content from going viral,” they added.
The CTI League went still further though, the journalists wrote, engaging “in offensive operations to influence public opinion, discussing ways to promote ‘counter-messaging,’ co-opt hashtags, dilute disfavored messaging, create sock puppet accounts, and infiltrate private invite-only groups.”
Such censorship lies at the heart of Missouri et al. v. Biden et al., a First Amendment censorship case where injunctions were issued against several federal agencies and government officials, barring them from communicating with social media companies regarding user content. The injunctions are now under review by the U.S. Supreme Court.
Former British intelligence analyst charged with creating counter-disinformation project
The journalists wrote that while previous releases of the “Twitter Files” and “Facebook Files” revealed “overwhelming evidence of government-sponsored censorship,” they had not revealed “where the idea for such mass censorship came from.”
The whistleblower alleged that a key figure in the CTI League, “a ‘former’ British intelligence analyst, was ‘in the room’ at the Obama White House in 2017 when she received the instructions to create a counter-disinformation project to stop a ‘repeat of 2016.’”
By 2019, this analyst, Sara-Jayne “SJ” Terp, had “developed the sweeping censorship framework,” leading a team of U.S. and U.K. “military and intelligence contractors” who “co-led CTIL.” Previously, in 2018, Terp attended a 10-day military exercise organized by the U.S. Army Special Operations Command, according to the journalists.
It was there that Terp met Pablo Breuer, a former U.S. Navy commander, who became a key figure in the CTI League. According to Wired, the two realized that misinformation “could be treated … as a cybersecurity problem.” This led to the development of CogSec, which soon housed the “MisinfoSec Working Group.”
“Terp’s plan, which she shared in presentations to information security and cybersecurity groups in 2019, was to create ‘Misinfosec communities’ that would include government,” the journalists wrote.
By spring 2020, it appears Terp achieved this plan, as the CTI League partnered with the Cybersecurity and Infrastructure Security Agency (CISA), which has been implicated in prior releases of the “Twitter Files” for its role in the “Censorship-Industrial Complex.”
The MisinfoSec Working Group included Renee DiResta, a former CIA operative who worked for the Election Integrity Partnership (EIP) — later renamed the Virality Project (VP). This group “created a censorship, influence, and anti-disinformation strategy called Adversarial Misinformation and Influence Tactics and Techniques (AMITT).”
According to the journalists, AMITT adapted “a cybersecurity framework developed by MITRE, a major defense and intelligence contractor that has an annual budget of $1 to $2 billion in government funding.” MITRE is a backer of the Vaccination Credential Initiative and the SMART Health Card — a digital “vaccine passport.”
Terp used AMITT to develop the DISARM framework, which the World Health Organization (WHO) applied in “countering anti-vaccination campaigns across Europe.”
The same framework “has been formally adopted by the European Union and the United States as part of a ‘common standard for exchanging structured threat information on Foreign Information Manipulation and Interference’” according to the journalists.
‘Can we get a troll on their bums?’
According to the journalists, MisinfoSec’s motivation for counter-misinformation was the “twin political earthquakes of 2016: Brexit and the election of Trump.”
“There’s something off kilter with our information landscape,” Terp and other CTI League members wrote, according to documents.
“The usual useful idiots and fifth columnists — now augmented by automated bots, cyborgs and human trolls — are busily engineering public opinion, stoking up outrage, sowing doubt and chipping away at trust in our institutions. And now it’s our brains that are being hacked,” they added.
In spring 2020, the CTI League set its sights on COVID-19-related narratives, targeting users who engaged in messaging that ran contrary to official policy.
“CTIL began tracking and reporting disfavored content on social media, such as anti-lockdown narratives like ‘all jobs are essential,’ ‘we won’t stay home,’ and ‘open America now,’” the journalists wrote.
“CTIL created a law enforcement channel for reporting content as part of these efforts. The organization also did research on individuals posting anti-lockdown hashtags … and kept a spreadsheet with details from their Twitter bios. The group also discussed requesting ‘takedowns’ and reporting website domains to registrars,” they added.
Regarding the “we won’t stay home” narrative, internal documents revealed by the whistleblower showed that CTI League members wrote, “Do we have enough to ask for the groups and/or accounts to be taken down or at a minimum reported and checked?” and “Can we get all troll on their bums if not?”
They also called posters circulating online promoting anti-lockdown posters “disinformation artifacts,” saying, “We should have seen this one coming” and asking “can we stop the spread, do we have enough evidence to stop superspreaders, and are there other things we can do (are there countermessagers we can ping etc).”
During CTI League brainstorming sessions to develop strategies for “counter-messaging for things like encouraging people to wear masks,” statements such as “Repetition is truth” were uttered by CTI League staff, the journalists noted.
The CTI League also sought to go “beyond simply urging Twitter to slap a warning label on Tweets, or to put individuals on blacklists.”
According to the journalists, “The AMITT framework calls for discrediting individuals as a necessary prerequisite of demanding censorship against them” and “trying to get banks to cut off financial services to individuals who organize rallies or events.”
As part of these efforts, even truthful information was targeted. In a 2019 podcast on “Disinformation, Cognitive Security, and Influence,” Terp admitted, “Most information is actually true … but set in the wrong context.”
“You’re not trying to get people to believe lies most of the time,” she said. “Most of the time, you’re trying to change their belief sets. And in fact, really deeper than that, you’re trying to change, to shift their internal narratives … the set of stories that are your baseline for your culture.”
Previous “Twitter Files” releases have revealed that true information was targeted for censorship by the U.S. government and social media platforms like Twitter if the information contradicted official policy regarding COVID-19 vaccines and restrictions.
‘Cognitive security’ a euphemism for censorship
In the same podcast, according to the journalists, Terp said, “Cognitive security is the thing you want to have. You want to protect that cognitive layer. It basically, it’s about pollution. Misinformation, disinformation is a form of pollution across the Internet.”
The journalists wrote, “A key component of Terp’s work through CTIL, MisinfoSec, and AMITT was to insert the concept of ‘cognitive security’ into the fields of cybersecurity and information security.”
Such “cognitive security” was seen as being threatened by the erosion of the mass media’s control on information and influence over public opinion.
Documents revealed by the whistleblower included a MisinfoSec report stating “For a long time, the ability to reach mass audiences belonged to the nation-state (e.g. in the USA via broadcast licensing through ABC, CBS and NBC).”
“Now, however, control of informational instruments has been allowed to devolve to large technology companies who have been blissfully complacent and complicit in facilitating access to the public for information operators at a fraction of what it would have cost them by other means,” the report said.
The same report also called for a form of “pre-bunking,” to “preemptively inoculate a vulnerable population against messaging,” suggesting that DHS-funded Information Sharing and Analysis Centers could be used to promote such pre-bunking.
‘If we get away with it, it’s legal’
Public-private partnerships were specifically sought out in an attempt to circumvent First Amendment free speech protections in the U.S., the documents revealed, even while Bloomberg, The Washington Post and Wired wrote glowing articles portraying the CTI League as a mere group of “volunteer” cybersecurity experts.
Yet, according to the journalists, “In just one month, from mid-March to mid-April [2020], the supposedly all-volunteer CTIL had grown to ‘1,400 vetted members in 76 countries’” and had “helped to take down 2,833 cybercriminal assets on the internet” including some which impersonated government organizations, the United Nations and WHO.
On the same 2019 podcast, according to the journalists, Breuer explained how the CTI League was getting around the First Amendment, by working to get “nontraditional partners into one room,” including “maybe somebody from one of the social media companies, maybe a few special forces operators, and some folks from Department of Homeland Security.”
Together, they would “talk in a non-attribution, open environment in an unclassified way so that we can collaborate better, more freely and really start to change the way that we address some of these issues,” Breuer said.
Breuer even likened these tactics to those employed by the Chinese government, saying “If you talk to the average Chinese citizen, they absolutely believe that the Great Firewall of China is not there for censorship. They believe that it’s there because the Chinese Communist Party wants to protect the citizenry and they absolutely believe that’s a good thing.”
“If the US government tried to sell that narrative, we would absolutely lose our minds and say, ‘No, no, this is a violation of our First Amendment rights.’ So, the in-group and out-group messaging have to be often different,” he said.
The whistleblower told the journalists that CTI League leaders did not discuss their potential violation of the First Amendment.
“The ethos was that if we get away with it, it’s legal, and there were no First Amendment concerns because we have a ‘public-private partnership’ — that’s the word they used to disguise those concerns. ‘Private people can do things public servants can’t do, and public servants can provide the leadership and coordination,’” the whistleblower said.
According to the journalists, the authors of the MisinfoSec report also “advocated for police, military, and intelligence involvement in censorship, across Five Eyes nations, and even suggested that Interpol should be involved.”
The CTI League documents also suggest that the organization was involved in a form of domestic spying, with one document noting that while censorship activities abroad are “typically” performed by “the CIA and NSA and the Department of Defense,” such efforts “against Americans” necessitate the use of private partners because the government lacks the “legal authority” to do so.
According to the whistleblower, CTI League members also went to great lengths to conceal their activities, with a CTI League handbook recommending the use of burner phones, online pseudonyms and the generation of fake AI faces. One document advised, “Lock your s**t down … your spy disguise.”
One suggested list of questions to be posed to prospective CTI League members proposed asking whether those individuals had ever “worked with influence operations (e.g. disinformation, hate speech, other digital harms etc) previously” and whether those efforts included “active measures” and “psyops” (psychological operations).
Indeed, according to the documents, several CTI League members had worked for the military or intelligence agencies, while according to the whistleblower, “roughly 12-20 active people involved in CTIL worked at the FBI or CISA” — even, for a time, displaying their agency seals alongside their names on the CTI League’s internal Slack channel.
Terp, for instance, previously designed machine learning algorithms and unmanned vehicle systems for the U.K.’s Ministry of Defence.
According to the whistleblower, the CTI League sought “to become part of the federal government.”
Shellenberger, Taibbi to testify before Congress this week
According to the journalists, the FBI declined to comment, while CISA, Terp and other CTI League figures did not respond to requests for comment.
However, one CTI League member, Bonnie Smalley, did respond to the journalists’ request. She wrote, verbatim, “all i can comment on is that i joined cti league which is unaffiliated with any govt orgs because i wanted to combat the inject bleach nonsense online during covid. … i can assure you that we had nothing to do with the govt though.”
“CTIL appears to have generated publicity about itself in the Spring and Fall of 2020 for the same reason EIP did: to claim later that its work was all out in the open and that anybody who suggested it was secretive was engaging in a conspiracy theory,” the journalists wrote.
“But as internal messages have revealed, much of what EIP did was secret, as well as partisan, and demanding of censorship by social media platforms, contrary to its claims,” they said, adding that “EIP and VP, ostensibly, ended, but CTIL is apparently still active, based on the LinkedIn pages of its members.”
The journalists said the documents will be presented to Congressional investigators and made public, while protecting the identity of the whistleblower.
Shellenberger and Taibbi will testify at Thursday’s hearing of the U.S. House of Representatives’ Select Subcommittee on the Weaponization of the Federal Government. They previously testified before the same committee in March.
On Tuesday, Taibbi appeared in a live YouTube webcast presenting some of the key revelations from the first release of the “CTIL Files.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Curious Admission Surfaces Concerning MHRA Blackmailing Mainstream Media Outlet Over Adverse Event Reporting
And no one really picked up on it…
BY JJ STARKY | NOVEMBER 25, 2023
Mass consumers of news – me included – are often exposed to so much information that some of that information can be lost in all the noise.
There’s little explanation why such a bombshell revelation featured in a recent Telegraph article gained next to no attention.
On 8th November, journalist Sarah Knapton published an article, entitled, ‘In the end, the AstraZeneca vaccine just wasn’t as good as its rivals’. Knapton broke down how AstraZeneca’s (AZ) purported efficacy could not stand up to the purported efficacy of the other vaccines. The consequences of which led to its eventual abandonment.
Curiously, however, buried in the 14th paragraph, was a confession that back in March 2021 – when the Telegraph first reported on AZ’s blood clot risks – Medicines and Healthcare products Regulatory Agency (MHRA) officials effectively blackmailed them.
Knapton writes:
“On the day we published the story we received a threatening phone call from a senior official at the MHRA warning that The Telegraph would be banned from future briefings and press notices if we did not soften the news.
Another well-known Cambridge academic got in touch to complain about our “disgraceful fear-mongering headline” on the story, claiming that it would discourage vaccine uptake and cost lives.”
This was the headline of that 17th March 2021 article:

Considering the title includes a subjective opinion from a foreign medical regulator that softens the news, I’m not sure how it constitutes “disgraceful fear-mongering”.
Perhaps this remark is more reflective of the contagious petulance we witness with medical regulators. For them, negative news is not just negative news. It’s analogous to physical assault.
What seems far more “disgraceful” is how a supposedly impartial medical regulator – tasked with safeguarding citizens from potentially lethal treatments – allegedly threatened to strip away a news organisation’s access. Leaving them out in the cold as competitors would stand to benefit from their potential exclusion.
And the curious thing is, no one has seemed to pick up on the news bar The Conservative Woman and the Health Advisory & Recovery Team (HART).
A report from HART earlier in August further revealed that MHRA officials have been blocking journalists, scientists, and vaccine injured victims on social media. HART asked them why and they responded:
“Thank you for flagging your issue about Twitter. We’ve reviewed recent action taken on that platform and have identified accounts which have been blocked in error, these have now been unblocked and you should be free to interact with our content again. Please let us know if you have any further issues so we can investigate and rectify, if necessary”.

“Sorry folks, it was error. And a complete ‘coincidence’ that we primarily blocked commentators who were critical of us…”
These are the same officials who refused to answer a routine Freedom of Information Request concerning data AstraZeneca submitted in their application to licence their Covid-19 vaccine. The reason they refused? It was “vexatious”.
They wrote in their response:
“this request falls to be considered “vexatious” due to the scope of the request and the disproportionate burden that compliance would create. S14(1) of the FOIA states that “Section 1(1) does not oblige a public authority to comply with a request for information if the request is vexatious.
Downloading the dossier of the vaccine is a relatively straightforward task, although it does require time. Due to the voluminous size of the file packages, when downloading the full package of data, the database software may be more prone to freeze. However, the time required to read through the dossiers, to identify exempt information and to consider and make redactions we expect would take many weeks, if not months to complete, as the dossier encompasses gigabytes of data. To meet the request our staff: Would need to read the dossier in full, in order to identify where redactions need to be made.
We appreciate that there remains a strong public interest in COVID-19 vaccines, however, we do not feel that the public interest outweighs the resource burden required to meet your request.”
Sometimes the actions of government officials are laced with so much arrogance, incompetence, and just frank laziness that it makes one question if they’re genuinely true.
If I sat across the table from an uninitiated countryman and told him of the above, it would come as no surprise to see him raise his eyebrows in astonishment. But not because of what I was telling him, but at me, as if I was about to descend into prophetic trance about how judgement day is coming and there’s going to be some epic battle between us and the lizard people outside Matt Hancock’s house.
Put differently, the extent to which the medical regulators’ actions are so unbelievable actually benefits them. It is easier for people to dismiss it as false. Of course, if the media actually did their job, this wouldn’t be a problem.
Naturally, when MHRA threatened the Telegraph, the outlet hesitated to revisit the subject for months. The blackmail paid off.
Were covid vaccine trials misleading by design?
Data presentation was deceptive
Health Advisory & Recovery Team | November 23, 2023
In chemotherapy, the primary aim is to reduce the disease burden in patients who are already diagnosed with cancer. This is reflected in endpoints like tumour size reduction, progression-free survival, and overall survival, which are directly related to the degree of disease burden. Therefore, measuring the benefit of chemotherapy involves comparing the extent of disease burden (or its progression) at the end of the trial between those who received the chemotherapy and those who did not. This comparison provides insight into how effectively the chemotherapy mitigates the impact of the cancer.
On the other hand, vaccines are designed with the primary goal of keeping individuals healthy by preventing the onset of a specific disease. Therefore, the efficacy of vaccines is best measured by comparing the health status among participants at the end of the trial. This involves assessing how many individuals remained healthy and disease-free in the vaccinated group versus the control group. Such an approach accurately reflects the preventive nature of vaccines.
The covid vaccine trials did not focus on how many were healthy instead comparing those who developed disease. To take the Pfizer/BioNTech trial as an example, there were 8 PCR positive symptomatic people in the vaccine group and 162 in the placebo group more than a week after the second dose and after up to 2 month’s follow up. That worked out at a 94.6% efficacy when calculated as a percentage reduction.
That sounds fantastic but it is not fantastic when measured in other ways. There is more than one scenario that could result in a claim of a 94.6% relative risk reduction as shown in the table. The alternative ways of measuring show the relative change in the percentage who remained healthy and the absolute change – i.e. the percentage of the population who benefitted.

In a hypothetical trial in which 94% of the placebo group developed a disease while only 5% of the treatment group did would also have a 95% efficacy as calculated the conventional way. However, these results have a totally different meaning to a patient. In this scenario 93.7% of the individuals who received the treatment directly benefited. Furthermore there was a marked change, 91.0% in the proportion who remained healthy.
Adjusting the percentages affected shows numerous situations in which the Relative Risk Reduction as conventionally calculated are identical but the Relative Risk Reduction in the proportion remaining healthy and the proportion who directly benefited tell a very different story. The last row are the actual results.

For the first two scenarios the people taking the treatment are more likely to directly benefit than not. For scenarios 3 and 4 there is still a high possibility of direct benefit. However, for the last two scenarios the chances of not directly benefiting are far higher than the chance of benefitting. It is possible in these scenarios that a longer follow up would improve the situation as more people would develop disease or be protected from it. However, the evidence of waning means that the time frame of follow up is close to the maximum possible period of benefit anyway.The important lesson here is that looking at the relative risk reduction as presented in the trials on its own is a meaningless measure. That is why the industry’s own code of practice says, “Referring only to relative risk, especially with regard to risk reduction, can make a medicine appear more effective than it actually is. In order to assess the clinical impact of an outcome, the reader also needs to know the absolute risk involved. In that regard, relative risk should never be referred to without also referring to the absolute risk.” The efficacy claims, even if we trust the results, were presented to the public in a way that could be deliberately misinterpreted.
New Report: Young People Dying of Cancer at ‘Explosive’ Rates, UK Government Data Show
By Mike Capuzzo | The Defender | November 21, 2023
Teenagers and young people in their 20s, 30s and 40s in the U.K. are dying from rapidly metastasizing and terminal cancers at an unprecedented rate since mass COVID-19 vaccination began, according to a new analysis by Edward Dowd.
The 45-page report by Dowd, a former Wall Street hedge fund manager and author of “‘Cause Unknown’: The Epidemic of Sudden Deaths in 2021 and 2022,” alarmed some oncologists who characterized it as a sharp reversal of decades of mortality data.
Dowd based his analysis on readily available government statistics from the U.K.’s Office for National Statistics.
In an interview with The Defender, Dowd said he and his research partners, who include a handful of high-level scientists, data analysts and financial experts, examined all International Classification of Diseases, 10th Revision, (ICD-10) codes for cause of death in the U.K. in the study period of 2010-2022 to investigate trends in malignant neoplasms (C00 to C99 codes).
ICD-10 codes are the international physicians’ classification of diagnosis, symptom and procedure for claim processing set by the World Health Organization (WHO). A malignant neoplasm is a cancerous tumor.
Dowd said his research team noticed a striking pattern: While almost all deaths among older people in 2021 and 2022 in Wales and England had been coded, 8% of deaths among 15- to 44-year-olds in 2021, and 30% of deaths in that age group in 2022, hadn’t yet been coded.
“When you die in a hospital, you leave a trail of life and death with indications of what led to the death,” he said. “When a young person dies at the wheel of a car, walking down the street or in their sleep, there’s an investigation” that consumes time to assign the cause of death.
Dowd said the missing codes are “indicative of the problem” of excess deaths among young people.
But even with the caveat of missing codes, he said, the remaining 92% of coded deaths in 2021 and 70% of coded deaths in 2022 revealed “a strong signal of cancer deaths in the young. We show a large increase in mortality due to malignant neoplasms that started in 2021 and accelerated substantially in 2022.
“The increase in excess deaths in 2022 is highly statistically significant (extreme event),” Dowd wrote in his report. “The results indicate that from late 2021 a novel phenomenon leading to increased malignant neoplasm deaths appears to be present in individuals aged 15 to 44 in the UK.”
The study’s results in the rate of cancer deaths above the historic norm in 2022 for ages 15-44 in the U.K. included:
- A 28% rise in fatal breast cancer rates in women.
- An 80% increase in pancreatic cancer deaths among women and a 60% increase among men.
- A 55% increase among men in colon cancer deaths and a 41% increase in women.
- A 120% increase in fatal melanomas among men and a 35% increase in women.
- A 35% increase in brain cancer deaths among men and a 12% rise in women.
- A 60% increase in cancer death rates among men in cancers “without site specification” and a 55% increase among women.

‘Mounting clinical evidence’ led to study
Dowd produced his report, assembled by Carlos Alegria, one of Dowd’s partners, in his Humanity Projects study of excess deaths in the U.K. and the U.S. using government and insurance industry data.
He said he started his pro bono data-driven project to help guide public policy when he saw how COVID-19 pandemic policies were destroying society’s faith in institutional experts.
Surveying the capture of national and state government regulatory agencies and corporate media by Big Pharma and other global interests, he realized, “We need independent agents to act as gatekeepers of the public interest.”
“We intend to be such agents, and to provide high-quality research to other individuals and institutions who seek similar outcomes,” he wrote.
The new report is his third in the UK Cause of Death Project, which previously examined “UK – Death and Disability Trends for Cardiovascular Diseases, Ages 15-44,” and “UK – Death Trends for the Cardiovascular System, Ages 15-44, Analysis of Individual Causes.”
The mounting clinical evidence linking burgeoning cancers in young people to the COVID-19 vaccines led Dowd to his latest study, he said.
“We focus our research on younger individuals, aged 15-44, as presently it is a topic of particular interest due to the rise in anecdotal evidence of many unexplained aggressive and unusual cancers (such as turbo cancers … ) occurring in the population, particularly in younger individuals,” he wrote in the study.
“The focus of this study is not to examine individual claims and anecdotes, but instead to provide a statistical analysis at a population level and clarify if the anecdotal evidence is abnormal or not.”
Dowd said he hopes “the relationships that we uncover in our analysis” are “a basis for a reality check for health professionals to understand underlying trends in individuals’ health.”
Dowd’s method was to analyze the number of deaths attributed to cancer in England and Wales between 2010 and 2022 in the U.K. Office for National Statistics data.
He compared excess death rates, the difference between observed deaths and the baseline for expected deaths, before and after the COVID-19 pandemic.
He established a baseline of normal cancer death rates from 2010-2020 that was remarkably consistent with few deviations, he said — until the cancer death rates rose significantly in late 2021 in the U.K. following the vaccine rollout.
Key findings from the report include:
- Breast cancer dominates in women. The most common cause of fatal cancer in women, ages 15-44, is breast cancer, representing about 25% of the total excess death rate caused by malignant tumors in women in 2022. The next most dangerous cancers for women, based on excess death rates, were colon cancer and cancer of the cervix uteri.
- While fatal cancer deaths rose dramatically among both young men and young women in 2022, young men saw a disproportionately higher rise in cancer deaths, but with no dominant cancer comparable to breast cancer in women. Brain cancer, colon cancer and stomach cancer accounted for 30.9% of the rise in fatal cancers in men in 2022.
- Cancers “without specification of site,” indicating rapid metastasis to other organs and commonly called “turbo cancers,” “exploded” in 2022, Dowd said. “These cancers saw very large rise in both women (in 2021 and 2022) and men (in 2022) and were likely metastasized already once they were identified. As the individuals refer to younger individuals who do not require early screening, these cancers were likely of rapid growth.”
- Men experienced a huge rise in skin cancer death rates of 118% in 2022. “Even though these cancers do not account for a large proportion of all cancers,” Dowd said.
- Cancers of the digestive tract “saw explosive changes in 2021 and 2022 relative to the 2010-2019 trend,” Dowd wrote. “Of particular notice are cancers of the colon (internationally coded as C18), stomach (C16) and esophagus (C15). “These cancers related to the digestive tract appear to have risen substantially in importance, and we also notice that they seem to be affecting men in a disproportionate manner.”
- Pancreatic cancer “saw a very large rise in both women (in 2022) and men (in both 2021 and 2022). Why these cancers rose so dramatically and why they rose first in men then women is one of the questions that we believe warrants investigation.”
Dowd emphasized that his research was “a first attempt to bring out some patterns that are observed in trends” in cancer post-2020.
“We hope that medical doctors and specialized researchers perform further investigations based upon these (and other) insights that our data analysis provides,” he wrote.
Link between COVID shots and rise in cancers ‘worth looking at’
Dr. Chris Flowers, an academic physician, radiologist and breast cancer specialist in England who came out of retirement to be the volunteer scientific lead of the War Room/DailyClout Pfizer Documents Analysis Project, told The Defender the U.K. data were “very, very, concerning.”
Flowers said Dowd’s research confirmed similar data on sharp cancer death increases reported by researchers, clinicians and cancer specialists in the U.S., U.K. and across the Western industrialized world since the global rollout of the experimental Pfizer and Moderna mRNA vaccine. An estimated more than 5.55 billion people, or about 72.3% of the global population, received the shots.
Flowers said he and his colleagues, including pathologists, radiologists, oncologists, internists, critical care doctors and researchers in the U.S. and U.K., have never seen anything like the severity of fatal breast cancers and other cancers in the young that exploded in 2022.
Dowd’s report confirms what Flowers and his colleagues have noticed for more than a year: “We’re seeing 2 or 3 times the normal rate of cancer.”
“We’re seeing younger people, we’re talking 20- and 30-year-old women, usually after they started menstruating and some form of growth promoter is going on normally, presenting with advanced tumors which are difficult to treat, but also they may have more than one tumor,” Flowers said. “Something that was rare is now relatively common.”
Perhaps most distressing, Flowers said, is the rise in the young of what some oncologists now call “turbo cancers,” a new term.
“Turbo cancer is a popular name that’s been coined to describe several things,” Flowers said. “It is cancers in young people just turning up, one day you’re absolutely fine, the next day you’re told you have terminal cancer and you’re dead in a week. There are many reports of that even in the mainstream media.”
“Tumors are not only faster growing but you’re getting more types of cancer occurring in the same person. It used to be very very rare. Just occasionally I’d see a very, very aggressive inflammatory cancer in young people. But now everyone has stories.”
Dr. Pierre Kory, a pulmonologist and critical care doctor who is president and medical director of the Frontline COVID-19 Critical Care Alliance (FLCCC) and treats hundreds of vaccine-injured patients in his practice, said he is “being deluged with reports and consults for help” about cancer increases from colleagues and patients.
David Wiseman, Ph.D., a pharmacist with a doctorate in experimental pathology and a pioneer, originally for Johnson & Johnson, of products to prevent post-surgery internal injuries, said he was alternatively astonished and outraged that governments and mainstream media won’t follow up on research he and Kevin McKernan, a former director of research and development at the MIT Human Genome Project, conducted showing the mRNA shots were contaminated with DNA fragments.
These fragments, Wiseman said, add to the potential damage the vaccines could cause to the human genome and open new doors to an infinite variety of problems, including cancer.
Wiseman told The Defender that the Centers for Disease Control and Prevention’s (CDC) own data show cancer concerns connected to the COVID-19 vaccines.
“We’re seeing an increase in cancers in VAERS,” the official U.S. Food and Drug Administration and CDC site for reporting vaccine injuries, Wiseman said. “The CDC did a PRR analysis, a signal analysis, that found a signal for cancer in the vaccines, which isn’t proof but it means it’s worth looking at.”
Mike Capuzzo is the managing editor of The Defender. He is a former prize-winning reporter for The Philadelphia Inquirer and The Miami Herald, a science writer, and a regional magazine founding editor and publisher who has won more than 200 journalism awards as a writer, editor and publisher.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Pfizer, Moderna Spend Millions on Ads Featuring Catchy Phrases and Celebrities to Push COVID Shots
By Mike Capuzzo | The Defender | November 22, 2023
Facing dramatic stock market declines and growing resistance to their mRNA COVID-19 vaccines, Pfizer and Moderna are running upbeat TV commercials with jingles and celebrities to push COVID-19 vaccination just in time for the holidays.
The 30-second Pfizer commercial features a cheery, driving tune and smiling celebrities Martha Stewart, singer-songwriter John Legend, professional soccer player and progressive activist Megan Rapinoe, singer-songwriter Charlie Puth and football star Travis Kelce.
All but Rapinoe flash Pfizer’s trademark blue band-aids on a shoulder showing they got Pfizer’s COVID-19 shot.
“Got it,” Stewart says, as the Pfizer ad copy reads, “This season’s updated COVID-19 shots are here,” and “Ask your healthcare provider if getting your COVID shot with your flu shot is right for you.”
“Got yours?” is the Pfizer tagline.
Moderna’s 60-second TV spot wants its audience to “Spikevax that body.”
Spikevax is the brand name of the company’s COVID-19 vaccine. It refers to the artificial spike protein the vaccine is designed to stimulate in the body to allegedly trigger protective antibodies to the virus.
The commercial opens with an older man playing table tennis accompanied by a narrator, who says, “When it comes to your health … you ping and pong that body.”
The spot proceeds through a variety of ordinary people practicing their passions, including a woman blending a vegetable shake (“you green that body”), a man plunging into an ice bucket (“you plunge that body”), and a man and woman playing chess (“you brainpower that body).”
It concludes with, “You flu shot that body, and now, you Spikevax that body. Because even though the pandemic is over, COVID-19 isn’t.”
The pharmaceutical trade press portrayed the ads as an attempt by Pfizer and Moderna, whose COVID-19 vaccines were injected into more than 5 billion people worldwide during the pandemic, to reverse dramatic losses in their stock prices in recent weeks.
“With hardly any Americans signing up to receive the updated COVID-19 shot, Pfizer is pulling out all the stops to increase uptake,” said Dr. Joseph Mercola.
Mercola reported that Pfizer paid Kansas City Chiefs tight end Kelce an outsized $20 million to promote the drugmaker’s COVID-19 shots, compared to his $5 million-per-year total endorsements from McDonald’s, Papa John’s, Walgreens, Nike and Tide, and was trying to capitalize on the football star’s recent surge in popularity as he dates pop star Taylor Swift.
Other medical trade journals debated whether celebrity endorsements like Kelce’s will actually help or hurt Pfizer’s sales and stock price.
Critic: COVID shot ads don’t meet FDA requirements for biologic side effects
But doctors and scientists interviewed by The Defender were appalled that Pfizer and Moderna, and the governments and media that support them, would continue to push the mRNA COVID-19 vaccines blamed for more than 36,000 deaths reported to the U.S. government-run Vaccine Adverse Event Reporting System, or VAERS.
A large Canadian study of 17 countries estimated the COVID-19 vaccines killed approximately 17 million people around the world.
Dr. Peter Breggin, a New York psychiatrist and author with his wife Ginger of “COVID-19 and the Global Predators: We Are the Prey,” said the Pfizer and Moderna commercials draw the audience into “a never-never land of fakers.”
“This is a combination of extreme fraud and sham,” Breggin told The Defender. “We now know from multiple scientific studies that there was a broad panoply of adverse effects to the vaccines as there are with some very potent drugs. That resulted in death in some people, and with more reports to the CDC [Centers for Disease Control and Prevention] of deaths than all the other vaccines in the world combined.”
Breggin, a frequent expert witness in pharmaceutical cases involving dangerous drugs and co-author of the bestseller “Talking Back to Prozac: What Doctors Aren’t Telling You About Today’s Most Controversial Drug,” said the Moderna ad makes a passing reference to possible myocarditis side effects while the Pfizer spot names no possible dangers at all.
“They’re not like ordinary drug commercials,” he said, adding that neither meets the U.S. Food and Drug Administration (FDA) requirement for describing biologic side effects.
Pfizer outspent competitors on digital, TV ads for COVID shots
Big Pharma advertising is big business in the U.S., the only country in the world with the exception of New Zealand that allows direct pharmaceutical advertising to consumers.
Spending on the marketing of prescription drugs, health services, laboratory tests and disease awareness grew from $17.7 billion in 1997 to $29.9 billion in 2016, with the largest increases coming in direct-to-consumer spending, which nearly tripled to 32% of all medical marketing spending.
Between Jan. 1 and May 6, 2021, Pfizer spent $21.5 million on digital advertising alone to push its COVID-19 vaccine, while Johnson & Johnson spent $29.1 million marketing its COVID-19 vaccine.
Big Pharma TV ad spending grew 8% in 2022, reaching a total of $4.05 billion. Much of that was “COVID vaccine-related television commercials” with “companies such as Pfizer and BioNTech” spending “large amounts of TV dollars on campaigns highlighting ‘getting back to normal,’ featuring loved ones reuniting after years apart,” according to Fierce Pharma.
Pfizer was the biggest drug-ad spender at this year’s Oscars, shelling out an estimated $5.7 million for the most expensive spot in the televised event on its new COVID-19 drug ad: “If it’s COVID, it’s Paxlovid.”
Pfizer also aired the second-most-expensive TV ad at the Oscars, spending an estimated $3.8 million on another COVID-19 ad using “star power to emphasize risk factors and COVID-19 in [its] latest vaccine ad push” featuring celebrities including Pink, Questlove, Michael Phelps and Jean Smart.
The fourth-biggest advertising spender at the Oscars was the U.S. Department of Health and Human Services, which spent an estimated $1.9 million on a 30-second “awareness ad” with no pharma company mentioned “to get people to consider getting the latest COVID boosters amid ‘fading protection.’”
Despite nearly around-the-clock media reports and advertising by Big Pharma and governments urging people to get the latest COVID-19 vaccine and boosters, Pfizer’s September 2023 rollout of its updated 2023-24 COVID-19 shot suffered “abysmal” uptake, with only 7.1% of adults and 2.1% of children receiving the updated COVID-19 shot as of Oct. 14, according to Mercola.
Dr. Pierre Kory was encouraged that vast numbers of Americans, a majority of whom took the experimental mRNA COVID-19 shots during the pandemic, are waking up to the fact the mRNA technology is dangerous and its risk-reward benefit presents potentially frightening risk with little or no benefit, especially for children.
“It appears to me that pharma companies are now desperately marketing the vaccines to consumers via TV ads,” he said. “It looks like their previously winning strategy of fear-mongering via public health agency proclamations and widespread news media behavioral psychology ‘nudging’ tactics is now failing.”
Mike Capuzzo is the managing editor of The Defender. He is a former prize-winning reporter for The Philadelphia Inquirer and The Miami Herald, a science writer, and a regional magazine founding editor and publisher who has won more than 200 journalism awards as a writer, editor and publisher.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Pfizer sues Poland over Covid-19 vaccine
RT | November 23, 2023
US pharmaceutical giant Pfizer has escalated its feud with Poland over excess Covid-19 vaccine doses that were ordered under a massive contract with the European Union. The company is suing the country over what it claims is an unfulfilled contract for Covid-19 vaccines.
Warsaw was locked into buying tens of millions of doses under a controversial contract the European Commission had signed with Pfizer in 2021 on behalf of EU nations. Pfizer is demanding 6 billion zloty ($1.5 billion) in compensation for 60 million doses that Poland’s government declined, after it stopped taking delivery of the jabs in April 2022.
The entire bloc wound up ordering 1.1 billion doses under the contract, saddling EU states with a vaccine glut as the Covid-19 pandemic waned. The EU prosecutor’s office has already announced an investigation into the procurement process amid allegations of corruption and secret backroom deals while Polish Health Minister Katarzyna Sojka has warned other EU states could be next to face prosecution.
Warsaw has questioned the controversial role of European Commission President Ursula von der Leyen in the Pfizer deal after it emerged she had for weeks privately communicated with the company’s CEO Albert Bourla during the contract negotiations. However, the European Commission claimed last year that her text messages with the big pharma boss on deals worth multiple billions of dollars executive could not be found.
The first hearing in Pfizer’s lawsuit is scheduled to take place in Brussels on December 6. Earlier this year the pharma giant offered to give the EU more time to complete its minimum vaccine purchases under the binding contract, but insisted that the bloc must pay in full for the contractually specified number of doses. Poland since refused to sign a revised EU agreement with the drugmaker.
Sojka told broadcaster TVN24 on Wednesday that there is some hope of resolving the Pfizer lawsuit “in a positive way.”
A Pfizer company spokesman told Politico however that the company decided to go forward with the lawsuit “following a prolonged contract breach and a period of discussions in good faith between the parties”.
Millions of Poles refused to receive Covid-19 vaccines, and Warsaw halted deliveries of the jabs as an influx of Ukrainian refugees in early 2022 strained the government’s finances.
Pfizer Sues Poland, Demanding Money for Undelivered and Unwanted COVID Vaccines.
BY IGOR CHUDOV | NOVEMBER 24, 2023
After achieving a modest 57% COVID vaccination rate and seeing the vaccines not live up to the promise, Poles refused additional Pfizer COVID vaccine doses around April 2022.

“At the end of last week, we used the force majeure clause and informed both the European Commission and the main vaccine producer that we are refusing to take these vaccines at the moment and we are also refusing to pay,” health minister Adam Niedzielski told private broadcaster TVN24.
“Indeed, the consequence of this will be a legal conflict, which is already taking place,” he said.
Poland cannot directly terminate the contract for the supply of vaccines as the parties to the contracts are the European Commission and manufacturers, he said.
The value of the contract for vaccine supplies to Poland up to the end of 2023 with one producer alone was worth over 6 billion zlotys ($1.4 billion), with over 2 billion zlotys of that for supply in 2022.
Pfizer said its agreement over the supply of its COVID-19 vaccine to European Union member states was with the EU Commission.
“Our discussions with Governments and the details of vaccine deliveries are confidential,” it added.
Somehow, Poland is a party to the EU/Pfizer contract that was kept confidential from the country but still obligates it to pay.
Pfizer CEO Albert Bourla and EU’s Ursula von der Leyen negotiated the contract in secret. (see picture below)

Anyway, now in 2023, Pfizer filed a suit, suing Poland for the monies due under the contract that was confidential and unavailable for Poland to even look at.
How a party can be obligated to pay under a contract that could not ever be assented to due to secrecy is a mystery to me, but I guess the legal minds in Europe see it differently.
Pfizer is suing in Brussels because Polish courts cannot see the contract and are unlikely to be very receptive to enforcing a contract that the court can review.
According to Polish newspaper Gazeta Prawa, Pfizer brought the civil case before a Brussels court because the doses were purchased through EU joint procurement contracts, drawn up under Belgian law.
Can Poland, perhaps, bring forth some novel defenses?
Perhaps Poland can ask Pfizer to comment on the dramatic fall in fertility that Poland is experiencing.

Poland may ask its local courts to make Pfizer compensate Polish COVID vaccine victims. (fortunately, there are fewer of them compared to the vax-crazy countries).
Pictures of some of the Polish victims of Covid vaccines, beautiful healthy humans who never needed the “vaccine” and yet died from it, are displayed by their bereaved relatives:

ht tps://twitter.com/DominateREALITY/ status/1488214087259459584/photo/3
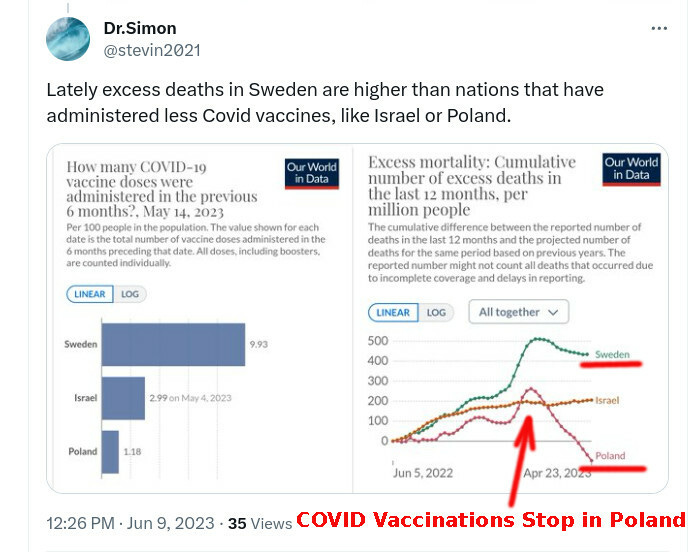
Can Pfizer explain, for example, why Sweden’s deaths continued to go up as the country was vaccinated, while Poland’s deaths went down after Poland refused COVID vaccines?
I am not an international lawyer, and I do not specialize in the enforceability of secret contracts that cannot even be seen by the parties which they obligate.
But I expect that Pfizer will lose.
German News Report on Covid Vaccines and ‘Turbo Cancer’ Withdrawn in “Frontal Assault on Freedom of the Press”
BY ROBERT KOGON | THE DAILY SCEPTIC | NOVEMBER 21, 2023
This past September 21st, the German news agency epd – the news agency of the German Protestant Church – published a potentially explosive report titled ‘Coronavirus Vaccines: Doctors and Researchers Express Concerns.’ The concerns in question were, more precisely, about a possible link between mRNA-based COVID-19 vaccines and rapidly-developing or “turbo” cancers.
Thus, we read, for instance:
The Munich-based immunologist Peter Schleicher is currently treating 1,000 patients in his medical practice. Around 30 of them have “turbo cancer”, as he says. This means that “the cancer grows incredibly quickly,” Schleicher told the Evangelischer Pressedienst (epd). He has never before had so many “turbo cancer patients” at the same time, he added.
According to Schleicher, all 30 patients were diagnosed with cancer within three months of their last coronavirus vaccination. He has long suspected that mRNA vaccines can impair the immune system, so that diseased cells in the body can no longer be effectively combated: “In my view, this explains why the tumours grow at lightning speed.”
And further on in the article:
“As early as autumn 2021, I suspected that the coronavirus vaccines could give rise to turbo cancer,” Ute Krüger told epd. The cancer epidemiologist, who specialised as a breast cancer pathologist at the Breast Cancer Centre of Oskar Ziethen Hospital in Berlin in 2004, is currently conducting research at Lund University in Sweden.
For some time now, she has been dealing with cancer patients the course of whose illness has been extremely strange, she says. The cancer specialist points, for instance, to a 70-year-old woman who had been living with metastatic breast cancer for several years: “Shortly after being vaccinated against COVID-19, the tumour growth in her liver exploded.” The patient died within a month.
The article also cites chemistry professors Andreas Schnepf of the University of Tubingen and Martin Winkler of the Zurich University of Applied Sciences, who likewise expressed their worries about the dangers of the vaccines.
Within one week of publication, however, the report had been quietly withdrawn. The article has been preserved on the Wayback Machine here. But it has disappeared from the original URL on the website of the German Protestant Church newspaper, the Evangelische Zeitung. Under the same title, ‘Coronavirus Vaccines: Doctors and Researchers Express Concerns’ – even with the same publication date and time! – we now find a brief disclaimer instead of the article. This disclaimer begins as follows:
Here, there was previously a text about coronavirus vaccinations and alleged possible links to cancer illnesses. It was an agency text which came directly from the agency and which had not been edited [by us]. The editors had already distanced themselves from the text and the repeatedly-used term ‘turbo cancer’, which has gained notoriety from its use by so-called ‘Querdenker‘.
The term Querdenker is widely used in German public discourse to refer to opponents of Covid measures such as lockdowns and mass vaccination. ‘Quer-denker‘ literally means ‘oblique’ or ‘transverse’ thinker and has the connotation of non-conformist or dissident, i.e., someone who ‘thinks differently’. (Thus, the English ‘queer’ appears to be derived from the German quer or to share a common etymological root with it.) The term has somehow become a term of disparagement in contemporary German usage.
It should be noted that Germany’s “Protestant Newspaper”, needless to say, regularly runs articles from its Protestant news agency.
The disclaimer goes on to cite a ‘fact-check’ from Germany’s public health authority, the Robert Koch Institute (RKI), which virulently rejects any link between the vaccines and cancer and indeed goes on the attack against those suggesting there is one:
Alluding to such fears is a targeted strategy of opponents of vaccination, which is used again and again. They try to create an association between vaccinations and cancer using invented notions like ‘turbo cancer’.
“There is no scientific basis whatsoever for this supposed relationship,” the RKI concludes. Oddly enough, the RKI ‘fact-check’ makes no specific reference to mRNA vaccines here, even though it is obviously such vaccines which are at issue in this context. It only mentions the mRNA vaccines in passing later on, in order to praise the “ingenious idea” of using mRNA technology to fight cancer.
It should be noted that the original epd article already included contrary opinion, including from the German regulatory agency, the Paul Ehrlich Institute, which told the epd, somewhat elliptically, that it “has no indication that the COVID-19 vaccines authorised in Germany altered the human genome”.
Although the German public health authority is cited in the disclaimer, in response to a recent query by the German regional newspaper the Nordkurier, epd Editor-in-Chief Karsten Frerichs insisted that the agency had not come under any pressure from Government officials to withdraw the article, but merely reconsidered the wisdom of its publication after receiving inquiries from “private individuals”.
Peter Schleicher, the Munich-based immunologist cited in the article, calls its withdrawal “outrageous”, describing it as a “frontal assault on freedom of the press”. There is “a great deal of absolutely serious [scientific] literature which undergirds the suspicion” of a link between mRNA vaccines and cancer, he told the Nordkurier.
Robert Kogon is the pen name of a widely-published journalist covering European affairs. Subscribe to his Substack and follow him on X.
Moderna’s ‘Disinformation Department’ Monitors 150 Million Websites for ‘Anti-Vaccine’ Narratives
By Brenda Baletti, Ph.D. | The Defender | November 21, 2023
Moderna’s “disinformation department” partnered with an industry-backed nonprofit, the Public Good Projects (PGP), to monitor and suppress dissenting voices on COVID-19 vaccine policy, according to a new report by investigative journalists Lee Fang and Jack Poulson published Monday in UnHerd.
Over the last year, the “Twitter Files,” two lawsuits against the Biden administration and other investigations have exposed instances of collusion among government, social media and universities to suppress dissenting speech about COVID-19 policies, election fraud allegations and other topics.
This new report sheds light on Moderna’s behind-the-scenes strategy within this new media landscape. It exposes key actors and how they worked to monitor 150 million websites for the purpose of censoring speech that undermines the company’s COVID-19 vaccine narrative and actively shaping public discourse to benefit Moderna’s bottom line.
Great Barrington Declaration co-author and Stanford University professor Dr. Jay Bhattacharya, who was blacklisted by Twitter, praised the new report in a tweet.
Moderna had never successfully advanced any product to market prior to the COVID-19 mRNA vaccine and was teetering on the edge of collapse when the pandemic was announced.
Its mRNA COVID-19 vaccine transformed the drugmaker into a $100 billion company almost overnight and turned its CEO, chairman and co-founders into billionaires.
Today, as public interest in taking yet another booster shot tanks and federal subsidies for the shot are disappearing, so are profits, leading the company to invest in new strategies — like a flashy marketing campaign — to stay afloat, Fang and Poulson reported.
Moderna also is doubling down on work started during the pandemic to attack dissent about vaccines and to direct vaccination policy, they found.
In fact, Moderna today employs former law enforcement agents, like Nikki Rutman, a 20-year FBI veteran who worked for the agency in Boston during Operation Warp Speed where her job was to conduct weekly cybersecurity meetings with Moderna.
Now she runs Moderna’s global intelligence division — part of the department spearheading Moderna’s work to stop “disinformation” — producing reports that flag “anti-vaccine narratives” online and recommending whether and how to address them, they wrote.
The department works with the PGP, largely funded through a $1.27 million donation from the Biotechnology Innovation Organization, a biotech lobbying group that represents Pfizer and Moderna.
Through PGP and Talkwalker, a “social listening” company, Moderna’s team monitors everything from mainstream news outlets to gaming sites, deploying artificial intelligence to monitor 150 million websites across the world for vaccine-related conversation.
The team issues reports to Moderna staff that color-code the “anti-vaccine narratives” by level of risk. Low-risk narratives “don’t currently warrant any action.” For the higher-risk narratives, the team “will notify the appropriate stakeholders with recommendations,” Lee and Poulson wrote.
Analyzing sample reports, the journalists discovered that examples of “high-risk” posts included a video posted by Elon Musk mocking myriad claims that the vaccines were “100% effective” along with a number of posts made by comedian and political commentator Russell Brand, whom they flagged in September for his “anti-vaccine” beliefs.
The Moderna team also raised concerns over the optics when tennis star Novak Djokovic, who refused the COVID-19 vaccine, won the Moderna-sponsored U.S. Open.
Lee and Paulson reported that Moderna was unconcerned with the truth of any of the claims made in the posts it flagged, only with their effects.
“None of the reports that we have seen makes any attempt to dispute the claims made,” they wrote. “Rather the claims are automatically deemed ‘misinformation’ if they encourage vaccine hesitancy.”
Moderna first began working with PGP in 2021-2022 on a program called “Stronger,” where the nonprofit “identified misinformation and shaped content decisions on social media.”
PGP could do this effectively because it had “backdoor access” to Twitter data, through a “firehose,” which provides real-time access to all tweets on the platform for large-scale data analysis and data mining.
PGP, which worked directly with Twitter to develop its policies around the pandemic, would send Twitter lists of accounts to amplify or censor.
Twitter’s general counsel also advised the U.S. Department of Homeland Security’s task force on combating misinformation to work with PGP on COVID-19 speech-related issues.
Lee and Poulson also found that PGP distributed talking points and advice on how to respond to vaccine misinformation to a network of 45,000 healthcare professionals.
“[Moderna’s] intention, as we have gleaned from the emails exchanged, was not only to combat misinformation, but also to affect the content and tenor of public debate,” Fang and Paulson wrote.
This year, as the COVID-19 booster uptake numbers have collapsed, Moderna and PGP launched a new collaboration, this time working with the American Board of Internal Medicine, to develop a training program called the “Infodemic Training Program,” to train healthcare workers to identify “medical misinformation.”
Despite public outrage regarding social media censorship, a clear lack of interest in continuing to take booster shots and the official end of the pandemic announced in May by the Biden administration, Moderna continues to grow its surveillance operation.
Internal alerts analyzed by Fang and Poulson reveal the company is closely monitoring laws and politicians seeking to restrict vaccine mandates and that it continues to flag messages posted on X, formerly known as Twitter, by Musk, who Moderna notes, “increasingly uses that platform to elevate fringe vaccine opponents and conspiracy theorists.”
The authors wrote:
“The network of fact-checking nonprofits has grown at an industrial pace, providing opaque opportunities for private and public interests to take subtle control over the public discourse. Such sophistication in blending public-health messaging and corporate advertising should concern anyone with an interest in how government controls free speech.”
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Why were German politicians so eager to vaccinate children, and why are they lying about it now?
eugyppius: a plague chronicle | November 18, 2023
Here is a riddle:
Why were German politicians so eager, in summer 2021, to vaccinate children? Why did they place public pressure on vaccine regulators to recommend child vaccination?
Even a few months ago, I would’ve said this was no great mystery. Before August 2021, everybody still operated on the insane assumption that the vaccines would eradicate Covid. They believed (or professed to believe) that a vaccination rate in excess of some magic number would end the pandemic, and that magic number was presumed to be unachievable if children were spared the jabs. I’d still say that was the case, but a recent news story has caused me to consider this question more deeply. Where did the specific pressure come from? What drove, for example, random regional ministers of education to mount their own appeals to vaccinate schoolchildren? What did these dumb people ever know about viruses or reproduction numbers or population immunity? What was going on?
There has been a lot of talk in the German press about the need for an appraisal of pandemic policies. This talk has flowed in directly inverse proportion to anybody’s willingness to actually appraise anything. Almost the only exception is the state parliament of Brandenburg, where Alternative für Deutschland are strong enough to have forced the convening of a Corona Investigatory Committee. The revelations so far have been extremely eye-opening, despite the limitation of the inquiry to Brandenburg and substantial obstruction from the political establishment.
The Committee publishes no protocols, many of their sessions are closed to the public, and with a few exceptions the media studiously avoids reporting on their work. Nevertheless, every time its members meet, something new and very bizarre comes to light. During their third session, in October, the Committee summoned Britta Ernst, Minister of Education in Brandenburg from 2017 to 2023, and also since 1998 the wife of Chancellor Olaf Scholz. At one point in the proceedings, Saskia Ludwig asked Ernst a very important question, namely the one that stands at the head of this post:
Why did Ernst advocate the vaccination of children in 2021?
The Nordkurier reports on the exchange that ensued:
Ernst had always campaigned in favour of vaccination and said in November 2021 that a “high vaccination rate” was “crucial for child welfare.” Ludwig asked … whether Ernst would repeat this statement given the current level of knowledge about the risk of side effects when vaccinating children against Covid.
Ernst … replied that the recommendation of STIKO [the Standing Committee on Vaccination] had been decisive for her.
STIKO “set the standard” and she had “no doubts about the work of STIKO,” which is why she had “naturally adopted their findings, which they make on a scientific basis.” Regarding her statement from November 2021, she said: “I suspect that this quote regarding the vaccination rate referred primarily to adults.” Ernst continued: “In addition, STIKO also recommended the vaccination of children and adolescents, and we followed this recommendation.”
In other words, Ernst was just Following the Science. She was just doing what the expert regulators of STIKO told her to do.
Except, that’s not true at all. Ernst was calling for the vaccination of teenagers as early as July 2021, well before that body had made any such recommendation. She was circulating flyers among Brandenburg schoolchildren that assured them they might even be able to get vaccinated without their parents’ permission. And what is more, she was even demanding that STIKO expand their recommendation to include everyone over 12 years of age.
From an rbb return-to-school article published on 29 July 2021:
The new school year begins in Brandenburg in just over a week. Primary school pupils will then be required to wear masks and there will continue to be plenty of ventilation. The Minister of Education believes that schools are in a good position – but there is still a need for action when it comes to vaccination.
Brandenburg’s Education Minister Britta Ernst (SPD) is calling for children and young people to be vaccinated from the age of 12 …
Until now, the Standing Committee on Vaccination (STIKO) has advised that 12 to 16-year-olds should only be vaccinated if they have certain preexisting conditions. The European Medicines Agency (EMA) has already approved the vaccines from Moderna and Biontech/Pfizer for this age group.
Ernst called on STIKO to issue a clear recommendation in favour of these vaccinations. The committee has already established that the incidence of infection among children is not dangerous and that illnesses among children are not severe. “This gives us further support in favour of opening schools,” Ernst said. A clear recommendation from STIKO, however, would be “helpful in any case, because many parents are naturally unsure how they should act.”
It wasn’t just Ernst. The day before, the Minister President of Brandenburg, Dietmar Woidke, had also renewed his demands that STIKO approve the vaccines for healthy adolescents:
On rbb television, Brandenburg’s Minister President Dietmar Woidke (SPD) once again called for the vaccination of children aged twelve and over to be considered. “STIKO already recommends vaccination for children with pre-existing conditions,” Woidke said. He would welcome it if … STIKO were to make a recommendation for the vaccination of adolescents in view of the spread of the Delta variant. According to Woidke, Delta has increased the risks for children and adolescents. STIKO must now weigh “the risk posed by Covid and the risk that vaccines may pose to younger age groups.”
Confronted with these contradictions at the Committee last month, Ernst became oddly evasive. She said vaguely that “many parents were waiting for a recommendation from STIKO” and that she “seem[ed] to remember that children in other countries were already vaccinated.” She did not refer to Woidke or describe any broader discussions within the Brandenburg government, although demands for child vaccination were clearly bigger than her. Nor did she refer to pressure from teachers’ organisations or any specific epidemiological goals.
The excuse about parental pressure is very strange and unsatisfying, when you think about it. First, the vaccines had already been approved by the EMA for the 12-and-up group. Parents who really wanted to jab their kids just had to find a willing doctor. Second, and more importantly, it is not the job of state education ministers to pass the concerns of local jab-crazed parents on to national medical regulatory bodies in the media. Why can’t Ernst clearly describe her motives? Where did the demand to vaccinate children come from?
At another revealing moment, Ludwig asked Ernst about a pro-vaccine flyer circulated among Brandenburg schoolchildren. This flyer assured kids that “There are hardly any long-term side effects; the vaccine is broken down quickly by the body.” It also enthused that “In some cases, you can even be vaccinated without your parents’ consent.” Here, too, Ernst had no good answers. She would say only that the flyer merely described “the legal situation” and “that underage girls are given contraceptives by doctors without parental consent.”
I looked into this flyer, which is a creepy exercise in marketing vaccines to children. The version that was circulated in Thüringen is still online:

Ernst couldn’t say much about its contents because it came from on high. The flyer was funded by the Thüringen Health and Education ministries, and masterminded by odious health communicator, Erfurt professor and villain-of-the-blog Cornelia Betsch. In later months, Betsch would go on to advise the government on how to nudge German vaccine uptake higher. We are dealing with the upper reaches of the German vaccinator-industrial complex here, in other words. The flyer was designed according to interviews its authors conducted with teenagers at the Henfling Gymnasium in Meiningen, for the purposes of figuring out out how best to manipulate kids into getting excited about vaccines.
There are two things about this document that make it extremely obnoxious. The first is that it is full of highly manipulative propaganda. It tells children that “The virus spreads primarily among the unvaccinated,” that “if you are not vaccinated, you have a greater risk of becoming infected,” that “the virus is becoming more contagious,” that “it is very rare to be infected despite vaccination and it is rare to infect others” and that “if you are vaccinated, you also protect others who can’t be vaccinated.” It contains a specific section explaining that the vaccines won’t impact fertility, and so I expect it was targeted specifically at girls, for whom the get-vaccinated-to-protect-your-family subtext would be especially effective.
The second obnoxious point is that this flyer, advising teenagers to seek the jabs even in the absence of parental permission and providing them with the contact information of local vaccination centres, was published on 14 July 2021. That is, it came out in advance of any official STIKO recommendation that this age group should be jabbed at all, and just two weeks before leading Brandenburg politicians like Ernst and Woidke began calling for STIKO to expand their recommendations to include teenagers.
There was, then, an unauthorised child vaccination campaign underway in summer 2021, which consisted of vaccine propaganda circulated to school children on the one hand, public pressure on vaccine regulators on the other hand, and who knows what else on however many other hands. It was timed around the summer holidays, for the clear purpose of scaring children into seeking the jabs before they returned to school. For some reason, Ernst will not tell the Brandenburg parliament why she participated in this campaign, and she will not say who its orchestrators were.
FYI Archbishop Justin Welby, Jesus Would Not Approve
On the profound betrayal of Humanity by the leader of the Anglican Church
A Better Way to Health with Dr Tess Lawrie | November 18, 2023
One of the most troubling occurrences during Covid-19 was the collusion of formal religion with the supranational military-industrial-banking complex to induce our compliance with unlawful, unscientific and downright harmful Covid-19 policies.
The speed at which church doors were shut whilst big business continued its trading was anathema to most people. When places of worship did open, people had the fear of (science) God put into them by the corporate media, politicians and their trusted religious leaders alike. Sanitising rituals were demanded upon entry, social distancing within churches was enforced with tape and stickers, and various religious practices were modified or curtailed.

One of several images shared on social media of priests using toy guns to interact with people such as, in this instance, to conduct baptism rituals
Even singing in church was deemed dangerous. As such, it had to be done through face masks or was prohibited entirely. People not complying with these religio-political directives were often vilified, prevented from attending services and risked being cast out of their congregation. Fear of the latter kept many reluctantly acquiescent. Even my elderly parents regularly remarked how ridiculous, uncomfortable and de-humanising it was; how it was hard to breathe, let alone sing, through the mask – and how going to church just wasn’t the same.
Why was joy, love, compassion and trust so readily sent packing when Covid came along?
Why was the joy and community of regular Christian services systematically undermined? Why did religious leaders urge us to transfer our trust in ourselves and our spiritual relationships to conflicted scientists and politicians? Why were we encouraged to fear, instead of love and feel compassion for one another? And why was our faith abruptly deemed insufficient by religious leaders who fell quickly in step with directives from the New World Order planners?
The Archbishop of Canterbury, Justin Welby, may well know the answer to these questions. Welby has been the leader of the worldwide body of Anglican Christian churches since 2013. On the Anglican Communion website it states that, in the UK, ‘He is regarded as the nation’s senior Christian and spiritual voice,’ and is the ecclesiastical lead over 13,000 parishes. In addition, church leaders and millions of Christians across 165 countries are likely to be guided by his leadership.
Given his reach and responsibility, Archbishop Welby in my opinion may be responsible for the most profound betrayal of Humanity in two thousand years.

Mail Online article from 22 December 2021
When, in December 2021, the UK’s Daily Mail ran an article quoting Welby as suggesting that Jesus would get the [Covid-19] vaccine, I could barely believe it. At the time, there were well over two million reports of associated adverse Covid-19 vaccine reactions, including thousands of deaths, reported to the World Health Organisation’s Vigiaccess database; on the UK’s Yellow Card scheme, there were about 400,000 individual reports with around 2,000 fatalities.
The World Council for Health (WCH), which had been established in September 2021 to provide trustworthy guidance in the face of the harmful official Covid policies, had already commenced it’s ‘Cease and Desist Campaign’ to urgently raise awareness of these very concerning vaccine safety data and to advise vaccinators and others to stop vaccinating and promoting these novel injections. WCH had also published the Covid-19 vaccine spike protein detoxification guide.
The video accompanying the Daily Mail article on the 22nd December 2021 chilled me to the bone.
Urging people to get Covid-19 vaccinated, Welby emphasises in the Daily Mail video:
“It’s not about me and my rights. Now, obviously there are some people who for health reasons can’t go vaccinating – [that’s a] different question. But it’s not about me and my rights to choose, it’s about how I love my neighbour. To love one another as Jesus said: Get vaccinated. Get boosted.”
This announcement by the Archbishop, a figure of worldwide Christian authority, leveraging Jesus’ goodwill and our love for him against us to convince us to take Covid-19 injections should be a matter of great concern for all.
The Jesus I know would never have said that we should take as many vaccines as the military-industrial-banking complex tells us to.
He would never have promoted unsafe medical interventions that harm men, women, and children whilst lining the pockets of the rich; neither would he advocate for the derogation of individual sovereignty to state or supranational entities.
This is the antithesis of what Jesus stood for. Jesus healed with his hands and our faith. He stood for truth, justice, freedom and peace. Jesus was fighting the same corrupt system that exploits us today and targets our children from the shadows.
I’m not going to start unpicking all that I feel is so very evil about what Welby said. The way Welby used Jesus’ words to promote the agenda of the military-industrial-banking complex, which seemingly will stop at nothing to materialise its 2030 Great Reset agenda, is disgusting and disgraceful in my opinion. However, it is not up to me to forgive or to judge the Archbishop. Ultimately, Welby will have his Judgement Day, as will we all, and I’m very glad not to be in his shoes.
The Roman Empire that crucified Jesus is finally crumbling as its latter-day representatives reveal themselves to be, indeed, wearing the Emperors’ clothes. Thankfully, two thousand years later, all that has been hidden from us is being revealed. Evil will no longer be facilitated or tolerated in the world we are creating afresh together. It will no longer lurk in the shadows when we are done shining our lights on it.
A Better World for us, our children, and all creatures on this beautiful planet is being born. All that is required is that, in remembering who we are as human beings – courageous, firm and loving, following Jesus’ very human example – we take care of one another, draw on our collective power, breathe and push.
The scandal of excess death reporting (or lack thereof)
Imagine the noise if the unvaccinated were the ones dying…
Health Advisory & Recovery Team | November 16, 2023
In stark contrast to the 2020 relentless daily death counts, there has been a virtual media black-out on excess deaths since the vaccine rollout.
Waves of excess mortality were followed by a brand new medical product being rolled out to entire populations globally and then the excess deaths went up stepwise. Leaving aside for a moment that no proper follow-up was put in place, no pharmacovigilance, no monitoring of the group that chose not to have the injections, we are left with having to use our mathematical minds to prove that something very unsettling is happening which certainly won’t remain hidden forever. Death is not ambiguous.
If most of the excess deaths were in the unvaccinated group of the population, this would be a brilliant indicator of the amazing value of the ‘safe and effective’ injections. The media has had a clear editorial line for decades: “thou shalt not increase vaccine hesitancy.” The underlying quasi religious assumption is that any such hesitancy would be ‘catastrophic’ for society’s health. If, after the jab rollout, the unvaxxed were dropping like flies, you can bet your bottom dollar that the media jackals would be promoting this in lavish technicolour centrefolds. “As Jane drew her last breath, her final whispered words were, ‘I wish I’d just got the damned vaccine’”... and so on and so forth. The data would have been repeatedly promulgated ad nauseam, to prove what fools the unvaccinated were and how brilliant the vaccines are. But this is not what is happening, because it would be an outright lie. So instead, we have radio silence on the topic of excess deaths, to avoid uncomfortable questions being asked.
Key to understanding what is happening is in realising that the vast majority of those at most risk of dying have been vaccinated. Therefore, patterns in the overall population reflect what is happening among that majority. It is almost impossible for the minority unvaccinated group to be responsible for such an increase in mortality.
To use an analogy, imagine if 90% of cars were given a new device claimed not only to be effective at preventing extra accidents but also super safe. Afterwards, there’s a 10% overall rise in car accidents from 100 a month to 110. If all the extra accidents were happening in the 10% of unaltered vehicles that would mean that among this group were the 10 accidents that represent the background rate in 10% of the population plus the extra 10 accidents. That would imply the accident rate had doubled in the cars that had not been altered. If, however, the new innovation was responsible, then the 10 extra accidents would be added to the 90 background accidents in the altered group, which would make for an overall increased rate of 11%. The latter scenario is much more likely and is much easier to believe, mathematically speaking.
Thinking of that analogy, let’s look at what has happened to deaths after the vaccine rollout. Take the 50-64 year age cohort as an example. From July 2022-Sept 2023, there were 12.5% more deaths than expected in this group, some of which were attributed to covid. Even excluding excess deaths that were blamed on covid, there were still 8.8% more deaths than expected in this age group. If these deaths were happening to the unvaccinated (because they hadn’t received the miracle drug), the mortality rate would have had to have doubled in that group for eighteen months straight. To put that into context, the excess from March 2020 to December 2021 (during the height of BBC daily reporting on excess deaths) was 19% higher than baseline average.
This is a rather mathematically complicated way of saying that the deaths are clearly not happening predominantly in the unvaccinated cohort because mathematically speaking, it just doesn’t add up as a possible scenario.

Table 1: Percentage increase in deaths (July 2022-Sept 2023) by age group if all excess were in vaccinated vs unvaccinated populations. First two columns are for all cause deaths and the second two exclude deaths blamed on covid.
For the over 75 year olds the situation is the most ridiculous. Many old people have already died in excess in recent years, so now we ought to be seeing a deficit in deaths in this group. If there are extra deaths, they first have to make up for this deficit before they can count as “excess” deaths. If we assume the excess in among the vaccinated then the excess is indeed small at 5% for all cause deaths. However, if we attribute those excess deaths to the unvaccinated then that population is dying at three times the expected rate! Even if we exclude all deaths blamed on covid the unvaccinated would still have to be dying at double the expected rate. Why? What’s killing them?
Where’s the outcry?
Where are the weekly press conferences and the demand that we must make any sacrifice in order to save even one life?
Looked at in this way it is clear that the actual problem must lie in unexpected deaths among the vaccinated population.
Featured Video
Laith Marouf: Hezbollah’s position on US-Iran ceasefire
or go to
Aletho News Archives – Video-Images
From the Archives
The Dirty Little Secret behind the “Global Terrorism Index”
The Omission of Israeli Terrorism in the Occupied Palestinian Territories
By Karin Brothers | Global Research | December 6, 2014
… The Israeli settlements — all of which are illegal – have been identified as a major impediment to peace. The refusal of a major “global” terrorism report to name the Israeli settlers as one of the groups most responsible for terrorism not only misrepresents a major source of regional violence but exposes the Global Terrorism Index as a propaganda tool that supports a U.S. agenda.
In recent years, governments have been attempting to thwart terrorism by blocking supportive fund-raising. When it comes to Israeli settlements, however, the US and Canada actually encourage fund-raising by giving organizations (such as Christian Friends of Israeli Communities (CFOIC) and the Jewish National Fund) financial support in the form of donor tax-deductions.
Charities which provide funds for the Israeli settlements should be regarded as terror-financing organizations. They should not only lose their tax-deductible status, but they should be banned because they support the violation of international humanitarian law. The terror-financing laws that are being strictly enforced for Muslim charities should be applied to Christian and Jewish charities as well. … Read full article
Blog Roll
 Aletho News
Aletho News- The ‘Opposition Party’ Has Done Nothing to Stop the Iran War and Much to Goad Trump Into Continuing It
- Moscow backs Tehran on status of Lebanon in US-Iran deal
- How UK Regulator Ofcom Quietly Bypassed International Law to Police American Speech
- The Black Cube Files: How Former Mossad Operatives Flipped a Nation
- Laith Marouf: Hezbollah’s position on US-Iran ceasefire: What you’re not being told
- Israel’s priority lies in destroying chances of peace between Iran, US: Ex-UN nuclear chief
- Ceasefire for all or for none: Iran shuts Hormuz over Lebanon attacks
- Strait of Hormuz is Iran’s ‘nuclear weapon’ that forced US retreat: Medvedev
- Energy crisis will last for months – Kremlin envoy
- Europe’s quiet role in the war on Iran
- If Americans Knew
- This is ceasefire? Israel’s biggest massacre yet in Lebanon, another journalist killed in Gaza – Daily Update
- Tucker Carlson on Israel: This Is the Behavior of an Ally? Really?
- Gazans face a triple crisis: severe shortages of water and bread, healthcare in tatters
- NY Times reports how Netanyahu took the US into Iran War
- A sigh of relief over Iran, but Gaza and Lebanon in dire straits – Daily Update
- Thousands dead and neighborhoods razed to the ground: Aid agencies fear southern Lebanon is becoming the new Gaza
- The war the US is fighting for Israel could cost trillions
- ‘Cigarette Burns, Nail Wounds’: Toddler Tortured in Gaza to Coerce Father
- Trump Says US Sent ‘a Lot of Guns’ to Protesters in Iran
- Israeli forces destroy 17 UN peacekeeper cameras in south Lebanon
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
