“More than 300 medical journal articles have disappeared within the last year.” – Dr. Scott Jensen
@drscottjensen
December 27, 2023
Posted by aletho |
Deception, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine |
Leave a comment
New Peer-Reviewed Research Shows Why the Study Was Flawed
During the COVID-19 pandemic, politicians, scientists and media organizations vilified unvaccinated people, blaming them for prolonging the pandemic and advocating policies that barred “the unvaccinated” from public venues, businesses and their own workplaces.
But a peer-reviewed study published last week in Cureus shows that a key April 2022 study by Fisman et al. — used to justify draconian policies segregating the unvaccinated — was based on the application of flawed mathematical risk models that offer no scientific backing for such policies.
Dr. David Fisman, a University of Toronto epidemiologist was the lead author of the April 2022 study, published in the Canadian Medical Association Journal (CMAJ), which the authors said showed that unvaccinated people posed a disproportionate risk to vaccinated people.
Fisman has worked as an adviser to vaccine makers Pfizer, Seqirus, AstraZeneca and Sanofi-Pasteur. He also advised the Canadian government on its COVID-19 policies and recently was tapped to head up the University of Toronto’s new Institute for Pandemics.
Fisman told reporters the key message of the study was that the choice to get vaccinated is not merely personal because if you choose to be unvaccinated, you are “creating risk for those around you.”
The press ran with it.
Headlines like Salon’s, “Merely hanging out with unvaccinated puts the vaccinated at higher risk: study,” Forbes’ “Study Shows Unvaccinated People Are At Increased Risk Of Infecting The Vaccinated” or Medscape’s “My Choice? Unvaccinated Pose Outsize Risk to Vaccinated” proliferated in more than 100 outlets.
The Canadian Parliament used the paper to promote restrictions for unvaccinated people.
However, in the new study published last week, Joseph Hickey, Ph.D., and Denis Rancourt, Ph.D., show that Fisman’s “susceptible-infectious-recovered (SIR)” model, used to draw his conclusions, had a glaring flaw in one of its key parameters — contact frequency.
When they adjusted that parameter to account for real-world data, the model produced a variety of contradictory outcomes, including one showing that segregating unvaccinated people can increase the epidemic severity among the vaccinated — the exact opposite of what Fisman et al. purported to show
Hickey and Rancourt, researchers at Canada’s Correlation: Research in the Public Interest, concluded that without reliable empirical data to inform such SIR models, the models are “intrinsically limited” and should not be used as a basis for policy.
The Canadian researchers attempted to publish their paper in CMAJ, where Fisman had published his original study, but the editor — a collaborator of Fisman’s — refused even to review it.
The open-access version of CMAJ also declined to publish the article even after it received favorable peer reviews.
In a letter sent, with supporting documentation, to the CMAJ and the Canadian Medical Association, Hickey and Rancourt recounted the “tedious saga” whereby the journal editors “concocted a multitude of ancillary and unnecessary objections, apparently intended to be insurmountable barriers” to publishing their study.
They later published the study in the peer-reviewed journal Cureus.
Rancourt tweeted a link to the study results along with a montage of pandemic-era media clips scapegoating unvaccinated people.
‘A policy based on nothing’
SIR models were commonly used as the basis for pandemic policies, often with fatal flaws research has since shown.
Fisman et al. designed their study to measure the impacts of segregating two groups — vaccinated and unvaccinated people — applying a SIR model to predict whether the unvaccinated pose an undue risk to the vaccinated during a severe acute respiratory viral outbreak, based on variable degrees of mixing among the groups.
However the model, Hickey and Rancourt wrote, failed to consider the impacts of that segregation on “contact frequencies,” a key parameter in predicting epidemic outcomes.
Instead, it assumed contact frequencies among the majority (vaccinated) and socially excluded (unvaccinated) groups would be equal and constant, which “is not realistic,” Hickey told The Defender.
In other words, the model assumed the two groups would be separated, yet living the same parallel existence — socializing, working, shopping and coming into contact with others in exactly the same ways.
But in the real world, segregation meant the unvaccinated were barred from many public places, so their contact frequencies were severely curtailed.
Hickey and Rancourt implemented the SIR model again, testing for a degree of segregation that ranged from zero to complete segregation and allowing the contact frequencies for individuals in the two groups to vary with the degree of segregation.
When they ran the model using the more realistic estimation of how different segregation policies might generate different contact frequencies among the two groups, “we found the results are all over the map,” Hickey said.
By segregating unvaccinated people from the vaccinated majority, he said, “You can have an increase in the attack rate among vaccinated people or you can have a decrease.”
“Negative epidemiological consequences can occur for either segregated group, irrespective of the deleterious health impacts of the policies themselves,” they wrote.
Hickey said the variable outcomes were very sensitive to the values of the parameters in the model, namely infectious contact frequency.
But he said, in the real world there are no reliable measures for contact frequency, and without reliable measures for model inputs, the model is essentially meaningless.
They concluded that the degree of uncertainty is so high in such SIR models that they cannot reasonably inform policy decisions.
“It’s a policy based on nothing basically,” Hickey said.
“We cannot recommend that SIR modelling be used to motivate or justify segregation policies regarding viral respiratory diseases, in the present state of knowledge,” the study concluded.
‘Fisman’s Fraud’
Modeling had a major impact on the pandemic response in Canada and globally, statistician Regina Watteel, Ph.D., who chronicled the impact of the Fisman paper in her book “Fisman’s Fraud: the Rise of Canadian Hate Science,” told The Defender.
As a key figure in modeling the pandemic in Canada, Fisman “was involved in Canada’s pandemic response at all levels,” she said.
He was also influential as a public figure, making numerous disparaging comments about “anti-vaxxers” from early on and advocating policies like vaccine passports and school closures long before he received a major grant from the Canadian Institutes of Health Research for his SIR modeling study.
Fisman was open in interviews about the fact that the point of the 2022 study was to “undermine the notion that vaccine choice was best left to the individual,” Watteel said.
The 2022 modeling paper didn’t just present mathematical results, the authors also made political claims.
The paper stated:
“The choice of some individuals to refuse vaccination is likely to affect the health and safety of vaccinated people in a manner disproportionate to the fraction of unvaccinated people in the population.
“Risk among unvaccinated people cannot be considered self-regarding, and considerations around equity and justice for people who do choose to be vaccinated, as well as those who choose not to be, need to be considered in the formulation of vaccination policy.”
Despite serious concerns raised by numerous researchers in the CMAJ article’s response section, the mainstream international press widely promoted the article as proof the unvaccinated posed a danger to the vaccinated.
Fisman publicly advocated for vaccine mandates and passports and told reporters the impetus behind the modeling study was not a scientific question of the effects of segregation on infection rates, but the political question of, “What are the rights of vaccinated people to be protected from unvaccinated people?”
A few days after the study was published, the parliamentary secretary to the Ontario Ministry of Health used the study to defend proposed travel restrictions, Watteel showed in her book.
As a result, she wrote, it “has generated a massive trail of misinformation.”
Watteel concurred that Fisman et al.’s study was based on bad modeling. She added that by omitting publicly available current data that contradicted the data they presented in the article, the study was actually “fraudulent.”
Fisman et al. published the paper during the so-called Omicron surge, which was dominated by infections among the fully vaccinated. By spring 2022, people who were boosted had disproportionately more infections than others, according to data on the government of Ontario COVID-19 website and reproduced in Watteel’s book.
However, none of that publicly available data was included in the study.
Instead, Watteel wrote:
“Fisman et al. concocted a model to generate the results they wanted, completely omitting any reference to readily available real-world data that contradicted their results (falsification). They went on to state the contrived results as facts (data fabrication) and then proceeded to inform public policy based on the fabricated results.
“The researchers continued to push the false narrative long after numerous scientists rebuked the findings and provided evidence of the findings’ falsity. This indicates a willful misrepresentation and misinterpretation of research findings.”
CAMJ editor, Fisman colleague, blocks review of Correlation article
Hickey told The Defender when they submitted their paper critiquing SIR models like Fisman’s to CAMJ in August 2022, editor Matthew Stanbrook, M.D., Ph.D. — who also works at the University of Toronto and has collaborated with Fisman on academic articles, grants and courses — rejected the article without even sending it for peer review.
Hickey and Rancourt appealed the decision and requested Stanbrook recuse himself. The journal suggested they resubmit their study to the open-access version of CAMJ, which they did. It was rejected without going through peer review.
They appealed that decision and the paper was sent for review. A few months later, they received two positive reviews with requested corrections. They responded to the reviews and made corrections to the paper, expecting publication.
The journal then informed them there had been a “technical error” and the journal — which is supposed to have an entirely transparent peer-review process — had failed to send them concerns from anonymous internal editors and an anonymous statistician.
Hickey told The Defender :
“It is their policy that the reviewers’ names are public and that the review reports and the revision, like the responses by the author, all that stuff is public. That’s the policy. There’s no escaping that.
“And yet what do they do? They use anonymous internal people to put barriers up and make pretexts to not publish even in the face of positive reviews.”
Those anonymous comments included a suggestion that they should use Fisman’s flawed mathematical analysis, Hickey said. The authors responded to those comments in what they have now also posted on their website as a stand-alone article.
Months later, they requested an update on the journal’s plans for the article and were informed that the journal decided the article would not be suitable for its audience and suggested they instead publish in a modeling journal.
All of their collected critiques of Fisman’s 2022 paper are also collected on the Correlation website.
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
December 23, 2023
Posted by aletho |
Civil Liberties, Deception, Science and Pseudo-Science, Timeless or most popular | COVID-19 Vaccine, Human rights |
Leave a comment
What was it like being a proverbial “canary in a coal mine” during the years of the COVID-19 pandemic, in the face of severe restrictions, mandates and large-scale censorship? In the book, “Canary In a Covid World: How Propaganda and Censorship Changed Our (My) World,” prominent thought leaders set out to answer that question.
Featuring essays from 34 contemporary thought leaders, “Canary In a Covid World” chronicles the authors’ personal and professional experiences dealing with several forms of censorship: in the press and mass media, on social media platforms, and within the ranks of academic, scientific and medical institutions and licensing boards.
Among the authors are figures from the realm of politics, including Sen. Ron Johnson (R-Wis.), U.K. Member of Parliament Christopher Chope, chair of the All-Party Parliamentary Group on Covid-19 Vaccine Damage, and Dr. Joseph Ladapo, Florida surgeon general and professor of medicine at the University of Florida.
Prominent doctors also contributed chapters, including Drs. Pierre Kory and Paul Marik, co-founders of the Front Line COVID-19 Critical Care Alliance, cardiologist Dr. Peter McCullough, British cardiologist Dr. Aseem Malhotra, and Dr. George Fareed, who, together with Dr. Brian Tyson, has treated over 20,000 COVID-19 patients.
Among academics and scientists, contributors included Harvey Risch, M.D., Ph.D., professor emeritus and senior research scientist in the epidemiology of chronic disease at the Yale School of Public Health, Dr. Jay Bhattacharya, professor of medicine, economics and health research policy at Stanford, Michael Rectenwald, Ph.D., author of “Google Archipelago: The Digital Gulag and the Simulation of Freedom,” and scientist Denis Rancourt.
Vocal advocates for vaccine safety were also among the contributors, including Steve Kirsch, founder of the Vaccine Safety Research Foundation, and COVID-19 vaccine injury victim-turned-activist Brianne Dressen, co-founder of React19.
In an exclusive interview, C.H. Klotz, editor of “Canary In a Covid World,” told The Defender the essays the book contains “would never find a home in mainstream media due to censorship,” adding that they “take the reader through the COVID story, from the mandates, to the vaccines, to the truckers’ protest in Canada, to off-label therapeutics, to vaccine injuries and much more.”
Klotz said that what stood out the most to him about the contributors was their courage.
“The fundamental thread that ties them together is censorship,” Klotz said. “Every voice has found themselves silenced at one point or another as the propaganda has marginalized them.”
“We wanted to diffuse the anger that often goes with discussion on the COVID narrative. We wanted to counteract brainwashing,” he said. “We felt if we could bring these voices together, to sing as one voice, others might finally be willing to listen.”
These efforts are beginning to succeed, Klotz said. The book is now available in the U.K. House of Commons Library, was hand-delivered to the wife of Pierre Poilievre, leader of the Conservative Party of Canada, the country’s main opposition party, and was pictured being held by Sean Buckley, leader of Canada’s National Citizens Inquiry.
According to Klotz, while he “entertained several offers to publish the book,” it was ultimately released by Canary House Publishing — to support several of the organizations that have been outspoken in countering establishment narratives.
“It seemed to make the most sense where we could ensure that $3 from each book sold could be donated to three organizations which are doing tremendous work — Children’s Health Defense, the Informed Consent Action Network and React19,” Klotz said.
In exclusive interviews with The Defender, several of the contributors to “Canary In a Covid World” talked about their experiences as “canaries” during the pandemic, and shared their views regarding the broader contribution of the book to the public debate about COVID-19.
Colin McAdam: ‘People without a voice can still be heard’
“Canary In a Covid World” opens with a chapter by internationally acclaimed novelist Colin McAdam titled, “Where Your Fear Begins.”
This essay, according to McAdam, examines “the competing views of COVID — the dominant one that exploited fear and insisted that life is about avoiding death, and the subversive one, which said that life is about living.”
In this chapter, McAdam goes on to talk about his experience participating in the trucker convoy when it reached the Canadian capital of Ottawa — an experience which “opened my eyes to many things, one of which was bravery,” he told The Defender.
Participation in the convoy “show[ed] me that it was possible and necessary to speak out,” McAdam said. “No public voice in Canada, and few people globally, had been addressing the true nature of COVID or the harms of imposing lockdowns and mandates.”
“The truckers, simply by uniting, making themselves visible and loud, were able to draw attention to public inertia, to the mendacity of the media and the government’s harmful policies,” McAdam added. “They showed me that people without a voice can still be heard.”
Addressing the reluctance of many of his peers and those in the creative industries, such as writers and musicians, McAdam said, “The COVID crisis demonstrated the power of fear, but it wasn’t simply fear of the disease. The more destructive and lingering fear has been that of being ostracized.”
“If I see that the dominant group believes in x and y, regardless of how absurd x and y might be, then my fear of losing my place in the group will override everything and I will declare my belief in x and y — at the cost of every conviction, every truth — because losing my place in the group will mean a loss of status and income,” McAdam said.
This mentality was far from limited to the creative industries, he added.
“Artists stood out to me because we are supposed to be the compassionate and curious ones. But the uncompassionate behavior of artists was not unique. Physicians are meant to treat disease, but they didn’t. University professors are meant to ask questions, but they didn’t,” he said.
“No one did what they were supposed to do because the message was that they would lose their jobs and status if they didn’t follow the dominant narrative,” he added.
For McAdam, the prevalence of this line of thinking “reveals the astonishing power of propaganda, but it also reaffirms what George Orwell observed in his preface to ‘Animal Farm’ — propaganda is most successful and sinister when it is self-imposed, when the intelligentsia believe and embrace it for the sake of their own dominance.”
Addressing the broader significance of being a “canary in a COVID world,” McAdam said, “If the message from above is to be brave, unity and kindness will emerge, but if the message is to be afraid, society will collapse.”
Dr. James Thorp: Hospitals, medical journals ‘terminally corrupt’
Missouri-based obstetrician and gynecologist Dr. James Thorp told The Defender that in his 44 years of practice, he has “never, ever … seen such rampant corruption of the government and the hospitals and the medical journals.”
Calling such entities “terminally corrupt,” Thorp said, “Their level of corruption in the last four years has accelerated on a slope that is unprecedented compared to the prior decades or centuries.”
It is this corruption that forms the basis of his chapter, titled “The Most Egregious Violation of Medical Ethics in the History of Medicine, co-written with Maggie Thorp, J.D., MACP.
“My chapter is about the travesty and the egregious violation of medical ethics by pushing a novel untested vaccine in pregnancy,” he said. “It’s the most egregious violation of medical ethics ever in the history of medicine, maybe in the history of the world.”
This was done with the guidance of government agencies and with the complicity of the mass media, Thorp said.
“Even liberal media outlets now acknowledge that $5 trillion or more … were used to push a lethal, blatantly false narrative of the COVID-19 experimental gene therapy,” he said, noting that Freedom of Information Act requests the Thorps filed revealed the funding and connections between federal agencies and medical licensing boards.
Thorp also highlighted the role of so-called “trusted community leaders” in perpetuating establishment COVID-19 messaging to the public. According to Thorp, money for such efforts was distributed through a program known as the COVID-19 Community Corps.
“They gave these bribe monies of over $13 billion to about 300 sectors, covering every stitch of the social fabric of our society,” he said. “They put up a massive number of really very lying and deceitful promotions, like, for example, ‘Go get your COVID-19 vaccines during pregnancy, otherwise you will die and your baby will die.’”
“These are grossly false fear tactics that are academically false,” Thorp said.
“Just remember, he who pays the piper calls the tune,” he said, noting that with such funding, media outlets routinely “demonized” and “defamed” scientists who expressed contrary opinions regarding COVID-19.
Dr. Mary O’Connor: ‘You will lose family members and friends’
In 2021, Dr. Mary O’Connor was one of four Canadian doctors who faced legal proceedings brought by the College of Physicians and Surgeons of Ontario (CPSO) for issuing “false” medical exemptions for the COVID-19 vaccine — with GlobalNews accusing these doctors of “undermining the fight against COVID-19.”
O’Connor’s chapter, titled “My Message to the Ontario College of Physicians and Surgeons,” is a response to the ordeal she faced.
O’Connor told The Defender she wanted to tell her story about her battle with the CPSO as she fought to protect her patients’ rights — “their right to choose their own medical treatment and their right of privacy of their medical history.”
“I wanted people to understand that the CPSO has been co-opted … from their original role, which was to protect patients,” she said. “Instead, they are now complicit with the injuries and deaths of many people.”
O’Connor, who saw “many adverse reactions” among her patients, said she also wanted to raise awareness about the dangers associated with the COVID-19 vaccines — and of threats to medical privacy.
“I wanted people to realize that they were coerced to take a medical treatment, i.e., injections, which were still investigational and dangerous,” she said.
O’Connor maintains that the shots were not vaccines and they failed to prevent infection or stop the spread of the virus. “The majority of the population just didn’t know, couldn’t see it. They were lied to,” she said.
“I wanted people to realize that their private medical charts are no longer safe,” O’Connor said, addressing the efforts of the CPSO to confiscate the medical records of her patients who received an exemption — demands O’Connor said she refused.
“Now, the CPSO, if they believe there is ‘an emergency,’ have given themselves the power to take and examine any patient chart,” she said.
According to O’Connor, CPSO also forbade doctors from questioning or debating official COVID-19 measures and policies. O’Connor said, “CPSO went on to threaten physicians with punishment, investigations and disciplinary action.”
“We were also forbidden to use alternate treatments to treat COVID,” O’Connor added. “Particularly forbidden were ivermectin and hydroxychloroquine, which I had used in my practice years before with no adverse effects.”
Instead, patients’ deaths “were hastened in hospital with use of ventilators and remdesivir,” O’Connor said. “The truth was suppressed everywhere.”
According to O’Connor, there were risks involved with being a “truth-teller,” but benefits as well.
“You will lose family members and friends. You may lose your job and income, and maybe your housing,” she said. “But there are huge rewards. You gain the serenity of knowing you are on the side of truth, and you meet a fantastic new group of friends.”
Margaret Anna Alice: ‘Mistakes were not made’
For writer and blogger Margaret Anna Alice, whose writings have focused on health, politics, mass control and propaganda, with a focus on COVID-19, silencing dissenting opinions represents a decisive step toward atrocities against humankind. She highlighted these points in her chapter, titled “A Primer for the Propagandized.”
“Totalitarianism, genocide, war — these atrocities are only possible thanks to the twin forces of propaganda and censorship: propaganda to promulgate the menticidal narrative and censorship to silence the truth-tellers exposing the lies upon which that narrative is based,” she told The Defender.
Such efforts are based on psychology, behavioral science and “nudging,” Alice said.
“Behavioral psychologists, cult leaders, and Bernaysian front groups know how to emotionally manipulate the populace into believing preposterous notions,” she said. “All it takes is a cup of fear, a pinch of rage, a dash of envy and a generous sprinkling of cognitive biases to bypass people’s critical thinking capacities, intuition and survival instincts.”
Alice said lockdowns and social distancing represent examples of such techniques.
“Biderman’s Chart of Coercion provides a manual for implementation, including isolation, a torture technique that inflicts neurological changes as Naomi Wolf and I discussed in her recent Dissident Dialogue,” she said, noting that she launched her blog in April 2021 with “A Primer for the Propagandized,” discussing such techniques.
The result of this, Alice said, was “unquestionably a religion — or, more precisely, a Covidian cult,” which she described in her chapter as an “ideological mass psychosis” with no relation to science.
“If this were about science, the Media-Pharmaceutical–Big-Tech complex would not be memory-holing every dissenting voice, vilifying every thought criminal, and censoring every legitimate inquiry in quest of the truth,” Alice wrote.
While a commonly heard narrative in the aftermath of the pandemic is that “mistakes” were made by policymakers and public health experts, Alice warned that the events of the past four years were not accidental but intentional and that the public must be more vigilant going forward.
“It is only by comprehending how the past four years occurred that we can prevent future encroachments on our rights, liberties, and lives by the ‘philanthropaths,’ tyrants, supranational entities, governments, COVID ‘kapos,’ and colluders,” she said.
“Each chapter of ‘Canary In a Covid World’ contributes a puzzle piece, and together, they form a clear picture showing that mistakes were not made — and why we must seek justice to prevent the repetition of the crimes against humanity that continue unabated to this day,” she added.
‘It’s possible, and vitally important, to speak out’
Klotz and the contributors described “Canary In a Covid World” as a book that compiles truths that were suppressed during the pandemic and urged the public to read the book.
Describing it as “one of the most important books” that has been published about COVID-19, Thorp said it contains “a compilation of experts with irrefutable credentials of truth-seeking,” who are “being persecuted because they are invoking their First Amendment right and their right as scientists to speak the truth and to interpret data.”
“This book does a lot,” McAdam said. “It informs readers about the forces that created their misunderstanding of COVID. It tells stories of suffering — vaccine injuries, losses of livelihood, destroyed reputations — that have not been broadcast in mainstream media.”
“I think one of its simplest and strongest messages is that COVID is a treatable disease — a message delivered by genuine physicians who have treated tens of thousands of patients,” McAdam added. “If this knowledge alone had been broadcast, I think the world would not have collapsed as it did.”
“We are all telling the truth,” O’Connor said. “Many of us didn’t know it at the beginning but were blessed to find it. We have told the truth in spite of huge negative consequences, and we are coming from many directions — those who didn’t know at first, those who knew and tried to tell others, experts from all walks of life.”
The contributors also shared a message of hope and optimism.
“There is a lot in the book that might and should make people angry, but overall what I feel is that it’s a book about kindness,” McAdam said. “Many of these people have stood up to incredibly powerful forces in order to truly care for people. And perhaps on the whole the book demonstrates that it’s possible, and vitally important, to speak out.”
“We are just regular people telling what we saw and learned,” O’Connor said. “We will speak out no matter what.”
Klotz told The Defender that an audiobook version of “Canary In a Covid World” was recently released, while a French language version and a sequel “focused purely on the financial interests behind COVID” are planned.
He added his hope that “Canary In a Covid World” will “open the eyes of those people who have questions and are ready to consider that the ‘truths’ their governments have told them, might not be so true after all.”
The Defender’s Michael Nevradakis was a contributing author to “Canary In a Covid World.” His chapter, “Fact-checking the ‘Fact-checkers’: Standing Up for the Truth in the Age of COVID Censorship,” focuses on the antitrust and First Amendment free speech lawsuit filed on May 31 by Children’s Health Defense against the Trusted News Initiative.
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
December 20, 2023
Posted by aletho |
Book Review, Corruption, Deception, Timeless or most popular | Covid-19, COVID-19 Vaccine |
Leave a comment
Acclaimed filmmaker Mikki Willis documented the disinformation campaign that discredited ivermectin around the world. Now updated and rebranded, the movie exposes their wicked tactics.
Covid may be fading faster than last week’s sunburn (likely to make way for the “next pandemic”), but the war on ivermectin rages on. And it’s no wonder, as we continue to discover its efficacy against increasing numbers of viral illnesses and now, even cancers. Of course, the more ivermectin threatens these insanely lucrative markets, the more enemies it racks up. (If you thought the Covid market was massive, in the end, cancer may be even bigger – the global chemotherapy market alone is expected to reach $330 Billion by 2029.)
Mikki Willis is a bestselling author, investigative filmmaker, and now, a friend. (He also used to be an old lefty/progressive like me – emphasis on the “used to be.”) In 2020, he released the first installment of his documentary series, Plandemic. The micro-budget documentary was watched and shared by over one billion people world-wide, making it the most seen independent movie in history. Plandemic 2: Indoctornation, set a streaming world-record with 2 million viewers attending the online premiere. Plandemic 3: The Great Awakening, was released in June of 2023 and is being hailed by critics as, “the most important movie of this era.” Note that the Plandemic trilogy can be seen for free at PlandemicSeries.com.
More relevant to my cause is that last year, Mikki released a short but powerful documentary detailing how ivermectin, the now infamous Nobel Prize-winning medication, had been slandered during the COVID pandemic. Well, a lot has happened in the year since, so Mikki has masterfully updated the film and rebranded it The War on Ivermectin to selflessly help support my book with explosive new clips and critical legal developments.
Check out the film below:
December 16, 2023
Posted by aletho |
Corruption, Science and Pseudo-Science, Timeless or most popular, Video | Covid-19, COVID-19 Vaccine, United States |
Leave a comment
As life expectancy plummets in Canada, a new government report claims “unspecified causes” have become the fifth leading cause of death in the country after cancer, heart disease, COVID-19 and accidents.
According to the Statistics Canada report, “unspecified causes” in 2022 passed strokes, aneurysms, chronic bronchitis, emphysema, asthma, diabetes, influenza and pneumonia, chronic liver disease and cirrhosis, Alzheimer’s and suicide as causes of death.
Statistics Canada, also known as StatCan, released the report on Nov. 27 in The Daily, the agency’s online news bulletin.
The report generated a slew of nearly identical headlines — provided by Canada’s national news service — in Canada’s leading newspapers along the lines of this one in the Toronto Sun : “Life expectancy for Canadians fell for third straight year in 2022, StatCan says,” followed by the subhead: “More people died of COVID-19 in 2022 than in any other year since the pandemic began, report says.”
Andre Picard, health columnist at The Globe and Mail in Toronto, Canada’s newspaper of record, called the life expectancy drop — to 81.3 years in 2022 from 82.3 years in 2019 — “a big deal.”
“It’s only the second time this sharp a drop has happened in Canada in the past century,” Picard said. “In fact, life expectancy has been climbing steadily for decades: 71 in 1960, 75 in 1980, 79 in 2000 and 82.3 in 2019.”
COVID-19 deaths in Canada decreased to 14,466 in 2021 from 16,313 in 2020, the report shows. Canada is on track for about 7,000 COVID-19 deaths in 2023, Picard said.
COVID-19 deaths can’t account for Canada’s 7.3 % increase in total deaths in 2022 compared with 2021 — or for the country’s 17% increase in total deaths over the historic norm of 2019, or the historic drop in life expectancy in Canada and worldwide, Picard said.
Like many mainstream journalists and public health officials in the U.S. examining the U.S. drop in life expectancy, Picard blamed chronic diseases, drug overdoses, opioid deaths, smoking, unhealthy diets and “indifference” for the decline in Canada. “There are virtually no mitigation measures like masking any more, and vaccination rates have fallen sharply,” he wrote.
But Drs. Pierre Kory and Peter McCullough told The Defender they believe the most important and startling fact contained in the report is the 300% increase from 2019 to 2022 in “unspecified causes” of death in Canada.
McCullough, a highly published cardiologist who developed a widely used early treatment protocol for COVID-19, said the dramatic rise in deaths from “unspecified causes” in Canada represents a seismic and disturbing shift in Western medicine.
“Prior to the pandemic, death in Western countries was well understood,” McCullough said, with 40% due to known cardiovascular, 40% due to terminal neoplastic disease (cancer) and 20% due to other known causes such as homicide, suicide, drug overdoses and accidents.”
He added:
“Since the roll-out of the COVID-19 vaccines, we have witnessed unprecedented deaths without antecedent disease. A large autopsy series published by Hulscher et al, found that 73.9% of the deaths after COVID-19 vaccination were due to problems caused by the shots.”
McCullough cited the hundreds of studies examining post-vaccine, spike-protein-related injuries and deaths and the millions of deaths and injuries reported by citizens in the U.S. and Europe to their governments following mRNA vaccination.
“All deaths should be categorized according to the doses and dates of COVID-19 vaccination,” McCullough said. “Unless proven otherwise, ‘unspecified death’ should be attributed to a fatal COVID-19 vaccine injury syndrome,” McCullough said.
Kory, the former University of Wisconsin professor of medicine and president of the Front Line COVID-19 Critical Care Alliance, told The Defender the evidence is overwhelming that the COVID-19 mRNA shots caused more deaths and injuries across the Western world than any prior drug or vaccine in history.
“The answer as to why ‘unspecified causes’ are now a leading cause of death is plain and simple,” Kory said. “That cause is the one medical intervention that the world’s governments and media have championed since the start [of the pandemic]. … The mRNA platform technology is and has been a colossal failure in both efficacy and safety.”
Kory and journalist Mary Beth Pfeiffer on Tuesday published an opinion piece in The Hill calling on governments and public health officials to study and address the problem of a global historic rise in mortality thus far not recognized by officials and not reported by mainstream journalists.
On Dec. 13, the essay was trending as the first or second most popular story on The Hill’s website, which claims 32.5 million monthly unique visitors.
U.S. Food and Drug Administration (FDA) Commissioner Robert Califf on Nov. 30 published an extraordinary thread of posts on X (formerly Twitter) calling for a society-wide “all hands on deck” approach to solve the problem of the “catastrophic” decline in U.S. life expectancy.
“JAMA Internal Medicine published earlier this month that our overall life expectancy has dropped to 76 years, and remarkably, that male life expectancy in the U.S. has dropped to 73 years,” Califf wrote.
But Kory said the FDA commissioner’s post, “which hit on smoking, diet, chronic illness and healthcare, ignored the obvious: People are dying in abnormally high numbers even now and long since COVID waned. Yet public health agencies and medical societies are silent.”
The FDA and mainstream media are ignoring the fact that life insurers have been “sounding the alarm over these unexpected or, ‘excess,’ deaths, which claimed 158,000 more Americans in the first nine months of 2023 than in the same period in 2019,” Kory wrote.
“That exceeds America’s combined losses [wounded?] from every war since Vietnam. Congress should urgently work with insurance experts to investigate this troubling trend.”
Amy Kelly, COO of DailyClout and the program director of the Pfizer Documents Analysis Project, said that for an autopsy to reach a proper diagnosis of an mRNA-vaccine-caused death, “histopathological examination of tissues from all over the body is necessary. Most of the time, even if an autopsy is performed, the histopathological examination of tissues is not.”
She cited an interview with Dr. Arne Burkhardt, who describes the types of testing the coroners must perform but seldom do.
Dr. Robert Chandler, a Los Angeles orthopedic surgeon who taught at the University of Southern California medical school, identified “entire new disease categories” he calls “CoVax Diseases” in his study of Pfizer’s 450,000 pages of COVID-19 vaccine documents, documents the FDA was forced to release via a court order, Kelly said.
“It makes sense that the unspecified causes of death have increased so much,” Kelly said. “When a patient dies with either multiple diseases all at one time or with a previously unseen disease state, both of which happen with ‘CoVax Diseases’ Dr. Chandler has identified, I would imagine many doctors and/or coroners don’t know how to categorize those causes of death. That would lead to ‘cause unknown’ categorization of deaths.”
According to Naomi Wolf, author of “Facing the Beast: Courage, Faith and Resistance in a New Dark Age,” “In the preindustrial world, people died mysteriously. But in the modern Western world, there are no mystery deaths. Every death has a death certificate which by law must identify a cause of death.”
“A minor rise in unattributed deaths is a problem that needs investigation,” Wolf said. “A major rise, such as you’ve identified, does not indicate a mass mystery to doctors and coroners, but rather it is evidence of a problem with state record-keeping — some bureaucratic malfeasance at a grand scale.”
Mike Capuzzo is a reporter for The Defender. He is a former prize-winning reporter for The Philadelphia Inquirer and The Miami Herald, a science writer, and a regional magazine founding editor and publisher who has won more than 200 journalism awards as a writer, editor and publisher.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
December 14, 2023
Posted by aletho |
Deception, Science and Pseudo-Science, War Crimes | Canada, Covid-19, COVID-19 Vaccine |
Leave a comment
Almost 4 years later, things are going swimmingly for the virus panic corps.
The White House Coronavirus Task Force was spun up on January 29, 2020. Shortly thereafter, the federal government began to deploy countless billions of dollars to pharmaceutical companies with the ostensible hopes to mitigate a much-hyped incoming pandemic.
Now, almost four years later, our hindsight presents a much clearer picture to the fog of virus mania we experienced in realtime.
Instead of mobilizing an effective public-private response to the advertised problem, Operation Warp Speed and the Task Force served as a vehicle for further panic and the facilitating of taxpayer cash that ended up enriching the pharmaceutical industry. These taxpayer-funded, Covid-related slush funds ballooned to astronomical heights across two presidencies, delivering record profits to Pharma companies that took pains to bring themselves onsides with the people in charge in Washington, D.C.
Tragically, the government-backed mechanical (ventilators) and pharmaceutical (remdesivir, mRNA shots, etc) interventions didn’t work to remedy the respiratory illness problem. Instead, they added an additional layer of chaos on top of the virus mania that had captured the world.
Operation Warp Speed and the resulting Task Force operation was, by all objective accounts, a catastrophic blunder, but that didn’t stop many of its members from parlaying their roles on the high visibility government detail into successful post service gigs.
So we thought now would be a good time to take a look at some of the healthcare/pharma-related government officials responsible for some of those fateful decisions, and where they are today.
Mike Pence:
He was primarily responsible for staffing the Trump Administration’s Covid response team. Pence launched his presidential bid in June, but gave up by October. He is perhaps the only Task Force member who did not benefit from the operation, as his political career is effectively over.
Anthony Fauci:
The most notorious member of the Task Force, Fauci’s wealth increased multiple times over while serving as the Pharma kingmaker over at the National Institute of Allergy and Infectious Diseases (NIAID). He recently took a no-show professorship at Georgetown University and is said to be working on a book.
Deborah Birx:
The second most infamous member of the Task Force, Birx, a protege of the Bill Gates network, has also cashed in on her time in the spotlight. She has since joined multiple pharmaceutical boards and wrote a book attempting to generate even more virus hysteria.
Moncef Slaoui
Technically not a member of the Task Force but the leader of Operation Warp Speed. Slaoui succeeded in delivering preferential treatment to Moderna, where he had a board seat and $10 million in stock options. Moderna stock would jump 20x from January of 2020 to late 2021. Slaoui left Operation Warp Speed in January 2021 to join a GSK-owned pharmaceutical company. He was later fired due to a sexual harassment claim.
Alex Azar
A former president at Eli Lily, he briefly chaired the White House Task Force. As the head of the U.S. Department of Health and Human Services (HHS), Azar facilitated billions of dollars in funding to vaccine companies. Like his colleagues, Azar has since joined several pharmaceutical and healthcare boards.
Jerome Adams
After leaving the White House, the former Surgeon General became Purdue University’s “Executive Director of Health Equity Initiatives,” sporting a salary of half a million dollars a year for the gig. He also joined the boards of half a dozen healthcare and pharmaceutical companies. The hyper woke activist just penned a book casting himself as a “front line hero” in the fight against Covid-19.
Brett Giroir
The Trump Administration’s assistant secretary for health (succeeded by the transgender identifying admiral “Rachel” Levine) spun right through the revolving door with his colleagues. He now serves as CEO and a member of the board of a respiratory virus treatment company. He also wrote a book on “fighting Covid from the front lines to the White House.”
Stephen Hahn
Hahn served as the FDA commissioner and a member of the Task Force. Only six months after authorizing the Moderna mRNA shot, he went on to serve as the chief medical officer of Flagship Pioneering, the venture capital firm behind Moderna. He has since joined multiple ventures seeking to get products approved for FDA clearance.
Robert Redfield
The former CDC director who once declared masks as superior to vaccines has joined quite a few boards related to Pharma and healthcare.
Seema Verma
As CMS Director, this Task Force member issued the infamous memo leaning on healthcare systems to suspend non elective procedures. After her tenure in the Trump Administration, Verma joined the boards of several healthcare firms and became a Senior Vice President at Oracle Corporation.
December 14, 2023
Posted by aletho |
Corruption, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine, United States |
Leave a comment
https://www.bitchute.com/video/jbt53sb8ojsQ/
“We have criminalized and disciplined all of the practitioners who were actually there to protect our patients and families. It’s a dangerous place. I would not take a family member to a hospital.”
December 14, 2023
Posted by aletho |
Deception, Science and Pseudo-Science, Timeless or most popular, Video, War Crimes | Covid-19, COVID-19 Vaccine, United States |
Leave a comment
Scientists and statisticians continue to review and debate the accuracy and completeness of a large database of COVID-19 vaccine-related deaths released less than two weeks ago by a New Zealand Ministry of Health whistleblower.
Meanwhile, the whistleblower — Barry Young — was charged by New Zealand authorities with “accessing a computer system for dishonest purposes.” The 56-year-old appeared in Wellington District Court on Dec. 4. and was released on bail the next day.
Young, who also has used the pseudonym “Winston Smith,” was a computer systems programmer for New Zealand’s Ministry of Health, administering a computer payment system for certain vaccine administrators.
Police raided Young’s home on Dec. 3, and arrested him. Police raided the home of an associate the same day.
Young, who was reportedly offered two safehouses in New Zealand and one overseas but refused the offers, now faces at least seven years’ imprisonment. According to Newsweek, Young shouted “freedom” as he departed the courtroom on Dec. 4.
Young released the anonymized data with the assistance of Liz Gunn, a former lawyer, television journalist and candidate for public office for the NZ Loyal Party.
According to mathematician Igor Chudov, who analyzed the data, the database included information on the vaccine type, batch number, dose number, vaccination date, age, date of birth and date of death of the anonymized vaccine recipients.
The dataset was related to so-called pay-per-dose providers, such as individual doctors and drugstores. It did not include data on vaccinations administered at mass vaccination centers and by mobile vaccination clinics.
Data raise questions government ‘can’t ignore’
According to the New Zealand Herald, Health New Zealand, the national public health system also known as Te Whatu Ora, has opened an investigation and attempted to discredit the whistleblower, claiming Young “had no clinical background or expert vaccine knowledge.” Some analysts noted Young’s expertise in data administration.
Health New Zealand’s public messaging has centered around the security of personal data. “What [Young] is claiming is completely wrong and ill-informed … We take the security of the information we hold extremely seriously, and this is a significant breach of trust,” said Margie Apa, Health New Zealand’s chief executive.
In an interview with The Defender, Australian attorney Katie Ashby-Koppens said Health New Zealand was also granted an injunction from New Zealand’s Employment Relations Authority, prohibiting the publication of the leaked data.
Ashby-Koppens, who worked with New Zealand groups promoting medical freedom and transparency, questioned the legality of this injunction, which reportedly was used to pressure hosting providers to remove copies of the leaked data stored on their servers, leading some providers to remove accounts hosting the anonymized data.
Minister of Health Shane Reti sought to reassure the public about vaccine safety.
“There are many conspiracy theorists out there who unfortunately disseminate harmful disinformation, however, as Minister and as a physician, the public can and should continue to have confidence in vaccines,” he said. “I am reassured by experts confirming that there is no evidence supporting the allegations that have been made.”
According to the New Zealand Doctors Speaking Out with Science (NZDSOS) media team, consisting of Dr. Cindy de Villiers, Dr. Alison Goodwin, Dr. Matt Shelton and Anna McLoughlin, such statements are a continuation of official COVID-19 narratives.
“The official mainstream media narrative is that New Zealand did very well during the pandemic, having negative excess mortality,” a spokesperson for NZDSOS told The Defender. “The New Zealand government and media have adopted a ‘shoot the messenger’ approach and then studiously ignored the issue, such that the average person on the street probably is unaware of what is happening in New Zealand.”
Yet, members of the public “who know what is happening absolutely support the whistleblower,” NZDSOS said, noting that “the media is so controlled and captured that large chunks of the population remain unaware of the data release or its significance.”
New Zealand authorities acknowledge only four COVID-19 vaccine-related deaths.
“The data has been very controversial, with people finding opposing things from their analysis of the data, despite being on the same side of the COVID debate,” Ashby-Koppens said. “The data is not complete [but] it raises a lot of questions, questions that the new New Zealand coalition government can’t ignore.”
Norman Fenton, Ph.D., a mathematician and professor emeritus at Queen Mary University of London, also examined the leaked data. He told The Defender the reaction of New Zealand’s authorities to the leak was “very strange.” He added:
“I understand that releasing confidential medical records is a criminal offense, but … the whistleblower only released an anonymized version of the data.
“Given the advanced publicity by people like Steve Kirsch about what the data revealed, I would have thought the New Zealand government would have been better advised to do nothing rather than raiding homes, arresting the whistleblower and erasing files from people who had gained access to the data. It is almost as if they wanted to get more publicity for both the data breach and what the data revealed.”
Presenting one possible reason supporting such an explanation, Fenton said:
“Not surprisingly, this has also led to conspiracy theories of which the most notable is that the government knew that this particular dataset did not contain (as some have claimed) any ‘smoking gun’ on vaccine safety and therefore it was deliberately released so it could be used to discredit ‘anti-vaxxers’ who claimed it did, and also act as a warning against any others who had access to more incriminating data to shut up.”
But for Kirsch, the founder of the Vaccine Safety Research Foundation who examined the data and publicly claimed it proves that the COVID-19 vaccines killed 1 in 1,000 people globally, Young “is a hero.”
“He knew he would risk his life and could spend the rest of his life in jail, but he made the courageous move to expose the data for all to see,” he wrote.
According to NZDSOS, Young is due to appear in court again on Dec. 18 to submit a plea and is “represented by a large legal firm in New Zealand.”
Whistleblower noticed ‘really big safety signals’ in the data
In his Nov. 30 interview with Gunn accompanying the release of the data, Young said he helped build the very database from which the data were leaked. Access to such data led him to note items of concern that he decided to go public with, he said.
“I helped build it. I implemented it,” he said. “When I was looking up the data, I noted discrepancies with the dates of death. People were dying almost straight away after being injected and that sort of prompted my curiosity and I dug a little deeper.”
According to Young, he previously was vaccinated, but said that whether he’d get another dose was “a different story.” He added that he “believe[s] in fundamental freedoms of humans and [that] we shouldn’t have a procedure forced on us because of a mandate,” calling this “a huge overreach by the government.”
Following his release on bail, Young granted an interview to Infowars producer and host Alex Jones, stating that he noticed “really big red flags” and “really big safety signals” in the data. “Statistically, it may be killing people,” he said.
“I just looked at the data and what I was seeing, since the rollout, it just blew my mind. I was just seeing more and more people dying who shouldn’t have been dying. It was just obvious,” Young said. “I want people to analyze this … We need to open it up and the government needs to have an inquiry about it. Just bring it to the public’s attention.”
According to New Zealand police, Young’s post-bail interview with Infowars did not breach his bail conditions. He has since granted other interviews.
Scientists disagree on significance of data
According to NZDSOS, the leaked data “cover[s] vaccines that were administered as pay-per-dose. There are 2.2 million people and approximately 4 million doses included.” This compares to a total of 12.78 million doses administered in New Zealand.
Statistical consultant William Briggs is one of the analysts who reviewed the data. On his Substack, he wrote that “we cannot tell for sure” what the data definitively indicates, as there are important items of information missing.
“There was no cause of death given for anybody,” Briggs said. “Just death date for those who had at least one shot and died in this window. There can therefore be no certain proof of any cause of death,” he wrote.
Briggs added:
“An insurmountable problem in ascribing cause is the lack of data on people who did not get any shots. Their death and age data is missing. There is no comparison group for the people who got shots. …
“… this means there is no natural comparison group and nothing about cause, therefore, can be said with certainty.”
Briggs said that the data indicated a small increase in deaths among young people soon after receiving the first and second dose, but said this may be “because the young tended to get fewer shots.”
The analysis that has perhaps garnered the most analysis, though, comes from Kirsch, who wrote, “There is no confusion any longer: the vaccines are unsafe and have killed, on average, around 1 person per 1,000 doses.”
Kirsch noted that this figure “is consistent with other careful analyses,” such as one by Canadian scientist Denis Rancourt.
According to Kirsch, one safety signal he identified in the data is a “mortality hump that peaks around 6 months after a dose is given.”
“The data from New Zealand is not perfect; it is not a complete sample,” Kirsch conceded. “But, by using a cohort time-series analysis, it doesn’t matter. There is no possible way that this data is consistent with a safe vaccine.”
Fenton, who analyzed the data on his Substack, took a different position, telling The Defender, “The dataset is a very large subset of those vaccinated in New Zealand, and is potentially one of the most important publicly available datasets for examining COVID vaccine safety. But I don’t believe it is the ‘smoking gun’ as some have claimed.”
He noted the absence of a control group (the unvaccinated) and that “the age profile seems higher than the national age profile of [the] vaccinated, so there is some bias.”
However, he said the data “does provide some evidence of lack of safety of the vaccine, in particular supporting our own previous observations (from U.K. data) that in older age groups, all-cause mortality is higher in the vaccinated than the unvaccinated.”
“What is less clear is the claim concerning batches with exceptionally high mortality rates,” Fenton said. “The claim that these batches were especially deadly due to the contents of the vaccine or its delivery is confounded by their very different age and time of vaccination profiles,” he added.
Chudov, in a pair of posts on Substack, also presented his analysis of the data. In his initial post, he suggested the public “be wary” of the data and noted that Gunn “is misinterpreting it by trying to pass normal nursing home deaths as evidence of ‘super deadly batches’ and ‘mass vaccine casualties.’”
In a follow-up post, Chudov acknowledged that some of his original questions about the completeness of the data were subsequently addressed, stating his belief that “Barry Young was more likely to be sincere than insincere in his intentions and actions.” Yet, he said his questions “about nursing home deaths and data quality still apply.”
Some analysts also pointed to official data indicating that excess deaths in New Zealand continue to be significantly above the long-term average — 17% in September and early October 2023, according to data from the Organisation for Economic Co-operation and Development. Some also pointed to data indicating sharp increases in the incidence of heart attacks in New Zealand.
Yet, Apa said, “We assure people there is no evidence whatsoever that vaccination is responsible for excess mortality in New Zealand and that they can continue to have confidence in the vaccine,” in remarks quoted by the New Zealand Herald.
“We hope that additional independent assessment of the data by credible analysts will lead to further scrutiny of the vaccine rollout in [New Zealand] and that the whistleblower will not have risked everything for nothing,” activist group Voices for Freedom wrote.
Political questions surrounding the data leak, subsequent government actions
According to Voices of Freedom, Young reached out to them “a couple of years ago” and had reached out to several other organizations during this period, prior to telling Gunn about the data and releasing it with her assistance.
Voices of Freedom, as well as some other analysts, have nevertheless raised questions as to whether Gunn handled the release appropriately.
Young and Gunn told Infowars they attempted to contact Winston Peters, leader of the New Zealand First political party and current deputy prime minister and foreign minister, regarding the data, but were unsuccessful in doing so.
But according to analyst Tony Mobilifonitis, Peters “most likely is limited in what he can do because of the delicate politics of the three-party coalition.” Analyst Markus Mutscheller wrote that while Peters had previously “aligned with the NZ freedom movement … His priority is always to keep his position of power in the cabinet. Without it, he can’t do anything.”
NZDSOS told The Defender, “So far, there has been no public comment by NZ First or the ACT party, both of which championed a broader inquiry,” adding that Reti “is from the National Party, which firmly backs the use of mandated vaccines.”
“The Associate Minister of Health, Casey Costello, is from NZ First, who is well aware of what is happening. However, ministers are not able to comment on cases that are before the court,” NZDSOS added.
According to the New Zealand Herald, an inquiry examining New Zealand’s COVID-19 pandemic response has been convened. However, according to NZDSOS, it is unlikely to examine the leaked data, as the inquiry “specifically excludes vaccine efficacy and does not include vaccine safety.” Instead, it aims to “strengthen … preparedness for, and response to, any future pandemic.”
According to NZDSOS, “The new coalition government has promised a broader public inquiry, but terms and conditions have not been decided upon to date. It is not clear whether there will be additions to the existing inquiry or whether a completely new inquiry will commence. Our preference is for a brand-new inquiry.”
‘Still no letup’ in narrative that COVID vaccines are ‘safe and effective’
Several scientists, analysts and activists have called on the New Zealand government to release full, anonymized COVID-19 vaccine data and its own analysis.
“They should release the data on the unvaccinated so that a full direct comparison can be made,” Fenton said. “We also need all the (anonymized) patient-level data on new health conditions/hospitalizations since 2021, for both vaccinated and unvaccinated, so that we can determine the true level of vaccine adverse reactions.”
Similarly, NZDSOS said, “The best approach would be to release all the data in an anonymized form and for the Ministry of Health to discuss their analysis.”
Kirsch wrote, “Nobody will debate me on this,” adding that New Zealand authorities “should be releasing the full [12 million-person] record dataset to remove all doubt and prove to the world the vaccines are safe.”
“Clinical outcomes are never improved by keeping public health data hidden from public view,” Kirsch wrote. “Yet every health authority in the world has kept this critical record-level safety data hidden from view.”
In a subsequent Substack post, Kirsch wrote, “Health New Zealand: Where is your analysis of your data? Why aren’t you publishing it?”
Voices for Freedom called on New Zealand authorities “to be transparent with NZ’s vaccination data,” noting that “There appears to be no official denial of the accuracy of the downloaded Health NZ data set.”
NZDSOS said that New Zealand authorities have a history of not being transparent, telling The Defender that Official Information Act requests are fraught with “often lengthy delays and redaction of data” and the system “is not particularly functional.”
“Some of these requests have been acknowledged, but the length of time in releasing information of this kind in any form has been delayed time and time again … We have not heard of any data/information releases that have come out yet,” NZDSOS said.
Fenton said New Zealand authorities are not being forthcoming regarding the data because it would likely “reveal much more evidence on just how ineffective and unsafe the vaccines have been and on how it likely has led to increased all-cause mortality in all age groups who have taken it.”
“There is still no letup in attempts by governments and pharma companies to close down all discussion and evidence of vaccine harms and to maintain the ‘official’ line that these vaccines are ‘safe and effective’ and need to continue to be given,” he added.
“It appears that the measures taken to silence Barry and avoid discussing the data are designed to deter others from doing the same thing,” NZDSOS said. Similarly, Fenton shared his belief that “the very public actions taken against the whistleblower [were] likely intended to dissuade other whistleblowers everywhere, not just in New Zealand.”
NZDSOS said that prospective whistleblowers should nevertheless not be dissuaded.
“Do what will allow you to sleep at night. It is not about any legal advice, as we know that it is likely that the legal system is compromised. It is about doing what is right,” NZDSOS said. “Evil triumphs when good men do nothing.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
December 13, 2023
Posted by aletho |
Deception, Science and Pseudo-Science | COVID-19 Vaccine, New Zealand |
Leave a comment
Sitting in front of a computer screen in August 2021, Dr. Paul Oosterhuis was prepared.
The regulators, the people who hold the registrar of health practitioners in Australia, had recently come out with a document informing practitioners they could only speak about the positives of the COVID-19 vaccine.
Saying anything negative or cautionary was not allowed.
Dr. Oosterhuis addressed the document in a tweet. Since the COVID crisis began on the other side of the world the year prior, he had become rather outspoken on social media about many pandemic protocols.
Now that the virus was finally at Australia’s doorstep, he had a lot to say. “The document is ridiculous,” he tweeted.
“In science,” he argued, “you can’t give informed consent without saying the pluses and minuses, the hazards and the benefits.”
A combination of tweets, Facebook posts and Facebook comments like this had already ruffled some feathers. During an event he refers to as “Facebook fear porn” in March of 2021, the registrar insisted the only way to save lives was with the jab.
“Please tell everyone to take vitamin D, zinc, hydroxychloroquine, and ivermectin as an evidence-based approach for treatment,” he countered.
And rather quickly he was told, “This is misinformation. I’m going to report to you.”
So later that year, in August, when he tweeted New South Wales Health Minister Brad Hazard, he wasn’t surprised by what happened next. Mr. Hazard had rounded up 24,000 school kids at Sydney Arena to get the experimental COVID-19 injection. Dr. Oosterhuis was furious.
“Here’s the childhood infection fatality rate by age. Kids are more likely to die from sharp objects.”
He went even further. At that time, the infection fatality rate for kids was .00016%, effectively zero.
“If there is even one death among these 24,000 kids, you have a signal of harm. And if you’re not watching for it, you will be held culpable.”
Two hours later, he received a call. The Medical Council of New South Wales was hastily putting together an immediate suspension hearing under the “Immediate Action Powers for Public Protection” section 150 of Health Practitioner Regulation National Law.
The hearing would be based on 10 social media posts where Dr. Oosterhuis had stated there was no evidence for anything the government was doing, whether it be masks, mandates or jabs, specifically regarding antibody-dependent enhancement. These were the posts selected as high heresy and grounds for suspension.
So here he was, sitting in his living room on a computer screen, participating in what he considered to be an online kangaroo court, but eager to participate anyway. He wanted to put them on notice. Whether they were calling it a vaccine or gene therapy, it hadn’t undergone the safety testing it should have.
There were no long-term data on the vaccine’s safety or efficacy, and they had an obligation to say so.
But it turned out, they weren’t interested in anything he had to say about that. Likewise, they had no interest in debating the science he provided or the merit of what he had claimed in any of his posts.
In fact, they only had one question: “Are you vaccinated?”
The answer was, no. And for the first time, there was a press release with his name on it. Dr. Paul Oosterhuis was officially labeled a threat.
‘Flabbergasted’: a doctor could lose his license for tweeting about informed consent?
I first met Paul in my parents’ kitchen 11 years ago.
He had flown to America with my cousin to attend a family event. Traveling the world after college, my cousin had never made her way home. Instead, she settled in Australia, married Paul, and had children. It was my first time meeting them too.
Eleven years ago I was very involved in the vaccine-safety-medical-freedom-quest-for-justice movement, which was substantially smaller then. I had helped form The Canary Party, now called Health Choice, the first political organization whose mission was to fight for medical freedom, justice for the vaccine injured, and systemic change to the vaccine program in the United States.
I had raised money for various autism organizations, marched on Washington, repeatedly met with my legislators, appeared on television, spoken at conferences and written more articles than I can count as a contributing editor to the Age of Autism blog and for other publications.
In short, I was pretty outspoken myself. And given this was long before anyone could have ever imagined the COVID pandemic, or that a highly respected mainstream doctor from Australia would lose his license for tweeting about informed consent, we didn’t really discuss my views on autism causation.
In fact, I’m fairly certain I totally avoided it.
So when my mom texted me last year that Paul had caused quite a stir and lost his license to practice medicine because of his opinions about COVID policies and protocols, I was admittedly pretty flabbergasted.
I had learned over time that the majority of physicians didn’t look at their practices as being responsible for creating negative health outcomes. Clearly, it seemed, he wasn’t afraid to do so. I decided right then and there I needed to reach out.
‘Something’s not right’
Dr. Oosterhuis completed medical school at Sydney University, also training at the University of California, Davis, Medical Center and in Papua New Guinea. After completing his residency with rotations in internal medicine, cardiology, general surgery, neurosurgery and intensive care, he decided he liked critical care best. Anesthesiology was his preferred practice.
“I’ve seen more cardiac arrests than most people have had hot breakfasts,” he commented about his time in emergency medicine over the last three decades.
This explains why he was hyper-aware of what was happening in the world regarding COVID in hospitals long before he became labeled a public health threat. He comes at it from a critical care space.
At the start of his career 30 years ago, Paul believed the Australian system of medical care was the best. Clinicians could still observe, speculate and doubt about a patient’s condition and care, he told me. Hospitals were full of doctors, nurses and other health practitioners.
Over time, however, he began to see a shift. Hospitals became less occupied by medical experts and more occupied by administrators and bureaucrats.
“It drove me mad from the get-go, the never-ending increase in red tape and bureaucracy,” he said. “It all became more and more leftist, more and more ‘woke-ian’ over the last eight years or so.”
The first red flag came in 2016 when a sign on an operating door said that any physician without a flu shot had to wear a mask for the following 12 months. To him, it made no sense. He had looked at the literature and found no evidence that masks prevented influenza in emergency room departments.
On top of that, in 2015, he received the flu shot, not only ending up feeling terrible for one week afterward but also getting the worst flu of his life a few weeks after that. He wasn’t the least bit interested in trying it again.
“I couldn’t leave the bed. And then a few weeks later, I got the flu. And it was the worst flu I’ve ever had. So when I saw that notice on the operating door, I went, no. I’m going to look into this. There’s something not right here. It doesn’t add up.”
No matter, it seemed. Suddenly, all the hospital administration cared about was his vaccine status for his re-employment contract.
From there, the changes ramped up. Senior staff were being moved out of the decision-making tree. He started recognizing pollution in the journal space, conflicts of interest and questionable findings in published science. His faith in the scientific literature was being damaged. His faith in the medical system even more so. All of it was causing him great concern.
So when COVID came, he was early to the question, “Why are the doctors and nurses falling sick in northern Italy?” Surely, he thought, they had to have good quality PPE (personal protection equipment) like they did in Australia. Didn’t they?
To avoid the same crisis in Australia, he began speaking out. In his mind, a lack of quality PPE was a bureaucratic failure. He pointed out that Italy may have failed to prepare, but Australia had time to do so.
He started by asking for quantitative fit testing of their masks. He suggested alternatives when they refused. Alas, it fell on deaf ears.
“I could see there was no openness to anything I was suggesting.”
In January 2020, he tweeted the prime minister that doctors were going to hardware stores to get effective PPE. He was adamant they work on this problem, that medical staff have a safe work environment.
And that’s when the online attacks against him began.
Amid those attacks, and after pointing out that strangely, no masks had been given to busy clinics where people from hot spots like Iran and China were coming to, his medical director suggested that perhaps he shouldn’t turn up for his next list (of patients) if he were going to keep this up.
Before he even had the chance to reply, however, he had to go into isolation. A nurse he worked with was diagnosed with COVID.
While in quarantine, Dr. Oosterhuis remained in contact with his fellow doctors and nurses, none of whom could get testing. When an email came from the medical director claiming everyone had been tested and all had been negative, he knew for a fact it was a bald-faced lie.
“I had lost trust in the system by then,” he said. “They were lying. They were not acting logically. They were not working on the problem. They were not listening to solutions that would work. Something was very wrong.”
And then, the coup d’état. He saw the NFR (not for resuscitation) and intubation orders and got a clear sense they were heading toward something very dystopian. The paranoia of viral contamination was so strong, that they were just going to let people die. No one would be getting CPR.
‘Like water on a raincoat’
To counter the insanity, Dr. Oosterhuis began aggressively researching treatment protocols. If they weren’t going to help prevent people from getting sick, at least they could treat them, he reasoned.
That’s when he discovered things like taking zinc, hydroxychloroquine, quercetin and vitamin D could have a powerful effect.
“The things they censored were very instructive,” he said. “The truth could be found in whatever that was.”
For most of 2021, he continued to follow the research and speak out, telling anyone who would listen about options for treatment. Eerily, however, it was like they couldn’t hear it. Long before Robert Malone talked openly about mass formation psychosis, he claims he could see and feel it for himself.
“It was truly bizarre. [Suggestions for treatment] would hit them like water on someone covered in a raincoat,” Dr. Oosterhuis said. “It rolled right off them.”
Alas, it soon began to make sense. The gene therapy injection was coming. The document from the regulators released in March of 2021 confirmed it. Only the vaccine, they insisted, would be able to save everyone.
By August, challenging that narrative would cost him his license.
‘Beyond the scope of authority’
During his suspension, Dr. Oosterhuis attended several protests alongside hundreds of thousands of fellow citizens. He went to one in Melbourne with a half million people. He went to another and marched on Parliament House in Sydney with a half million more. He even attended Australia’s trucker protest. They had one, too.
Although the press refused to cover the demonstrations fairly, he describes the cooperation and camaraderie of the people as nothing he had ever experienced. Everyone was so happy to know they weren’t alone, he told me.
“We had the sense we were living through history and felt sorry for the people captured by the narrative and living in fear. Human rights, bodily autonomy, informed consent — none of that seemed to matter to them.”
At the protests, several people suggested a legal brief he could take to the Australian Supreme Court to challenge the Medical Council’s decision and restore his medical license. He wasn’t going to be able to debate the merit of his social media posts, that much had been made clear.
But he was possibly going to be able to prove they didn’t follow the law in making their decision. The council had acted ultra vires, it seemed — or, beyond their powers.
He summoned the Supreme Court and Medical Council for judicial review, representing himself. Once again he found himself in his living room on a computer screen, this time in his pajama bottoms, with people trying to ruin his livelihood and reputation.
The first time around, he admits, he was nervous. By the 12th hearing, however, he was a warrior ready for battle. And on May 10, 2022, he emerged victorious. All anonymous complaints, and the suspension of his medical license, had been lifted. He had won his case.
Dr. Oosterhuis wasn’t entirely satisfied, however, as his true goal had been getting medical freedom back for all Australians. There was still work to do, he claimed. He had really hoped to get a ruling stating they had acted unlawfully, not just out of their jurisdiction. It would have overturned all suspensions — and potentially the regime of terror against doctors with it.
‘Give me my orders’
Paul now considers himself a soldier in the war for medical freedom. He sees himself as a part of the machine trying to get sanity back in science and to protect the public. In the environment of censorship and propaganda, he believes, you no longer have a democracy. Informed consent becomes impossible.
We talked for well over an hour about the parallels of our journeys for the same things, and how even though he’s later to the party than me, he’s in it for life. He insists he won’t stop fighting until they stop injecting our kids.
He also admits he just wasn’t awake. He took all vaccines without question until his horrible experience with the flu shot in 2015. He has also had to reevaluate past practices and assumptions.
Having resuscitated many SIDS babies over the years he realized, “Never once had it crossed my mind to ask, ‘When was their most recent vaccination?’”
Likewise, he has dug deeply into the literature on vaccine safety, or rather, the lack thereof. He understands now how they manipulate and censor science if they don’t like the outcomes, specifically citing Paul Thomas and James Lyons-Weiler’s study of the vaccinated versus unvaccinated and how the publisher pulled it, not a doctor or scientist.
“They don’t like having control groups,” he said. “One of the most sinister agendas in this whole thing is they never study any of these agents versus a placebo control.”
He went further adding, “And we know why. Because it would show it’s an unmitigated disaster.”
Paul went on to describe just how deeply this experience has affected him personally. Besides the trauma of losing his medical license after a stellar record of 30 years in practice, and for social media posts nonetheless, it has helped him formulate a new personal philosophy.
“I personally will not have another vaccine in this body in this lifetime,” he told me.
“I had made an oath a year and a half ago that that was my decision,” he said. “And so then the question was, how am I going to live in this world where they seem determined to inject every man, woman, child and animal on the planet with this thing? Like I say, I’m opposed to it. I’m a soldier. And I am opposed to it to my death.”
‘Real threat to the whole of humanity’
Dr. Oosterhuis hasn’t returned to the hospitals where he once worked. For one, they still have their vaccine mandates. And two, far too many of his colleagues have chosen to stay asleep, he feels. He can’t go back to it pretending none of this is real.
Instead, he spends his time now speaking out. In addition to being interviewed globally by people such as Steve Kirsch, Pierre Kory, and Peter McCullough, he has created a Substack with a substantial following. Topics have included the increase in the all-cause mortality signal; fraudulent PCR tests; and the shocking damage to fertility we see happening all over the world.
“In country after country, you see nine months after the roll out (of the vaccine), a collapse in birth rates, a massive increase in infertility, and problems with women’s cycles,” he said. “This is a real threat to the whole of humanity.”
He’s equally concerned about the power grab of the World Health Organization and other health agencies. When I commented that without liability, pharmaceutical companies have no incentive for restraint, he took it a step further. They don’t just lack an incentive for restraint, he countered. They are now incentivized to create disasters.
“It’s criminality that’s become an existential threat to humanity. We don’t have any choice but to push back.”
‘I hoped I was wrong’
From the very beginning, Paul insists that he wanted to be wrong. He wanted to be wrong about it all. He was simply putting questions out into the digital universe.
What if they tried a different mask? Where was the proper PPE? Why was there such resistance to treatment protocols? Why were they giving 24,000 students an experimental injection for a disease they’d never die from? None of it made any sense.
“I hoped I was wrong. I really did,” he said. “But within days I heard a report of a high school student who had died, and I heard there was going to be a service. Then there were other reports of deaths in the 24,000. At the time of my tweet, I prayed I was wrong. I would have been happy to be wrong. But my role was to put them on notice. I didn’t want them to be able to say, ‘we didn’t know.’ It’s on public record, they did.”
When top officials at the U.S. Food and Drug Administration resigned last year over the pressure to push for boosters, Paul says their parting letter didn’t pull any punches. The danger was not just to the credibility of the COVID-19 vaccine, these officials claimed, but to the credibility of all vaccines. Paul believes they are right, and that accountability is coming, even if it’s slow.
Meanwhile, his trust in the government, medicine, science, journalism and the media has been destroyed. He carries a sense of disgust that many of us have already carried for some time, and he is adamant that we have to rebuild our institutions from the ground up. We need true science, true integrity and an end to conflicts of interest.
“Public-private partnerships sound great until you put a jackboot on it,” he says.
Most of all, he insists, we need bodily autonomy.
“If we don’t have bodily autonomy, we are already enslaved.”
‘A coincidence theorist’
Paul tells me that he is not a conspiracy theorist but rather a coincidence theorist. I laugh, only because the name of my book, which he hadn’t known, is “An Unfortunate Coincidence: A Mother’s Life inside the Autism Controversy” (Skyhorse 2016).
Both of us notice the coincidences. When they become less and less probable, “you start to think, maybe this is the way reality actually works.”
We commiserate for a little while over the figurative costs of being in this fight, and how neither one of us could have ever imagined being a part of it, or really ever having needed to be. Science was once sacred, I remind him. He agrees, but pushes back.
“The fight is here. It’s now,” he said. “The ultimate battle is here. And as big as the cost is of speaking out, the cost of not speaking out is exponentially larger. And the cost gets greater every day that passes.”
I am inspired again to pick up my proverbial sword. It has been almost six years since I have actively spoken out or regularly written anything. Fifteen years in the fight prior affected me in profoundly personal ways that required a reprieve.
And yet, I know he is right. The fight is here. It is time to get back in the ring. I thank him for reminding me of that and all he is doing.
“For decades, I have fought for everyone’s lives, and I’m still doing it. I’m not doing it in the operation theater, but I’m doing it on a different scale now. The only way you can protect those closest to you is to end this for everyone.”
Paul and I finish the conversation. It is late for me in Chicago while he is in Sydney. Once again, he is in his living room over a computer screen, in the same space where he lost his medical license and then took on the Australian Supreme Court to regain it.
In the same place he intends to save many more lives.
Even in his pajamas.
Julie Obradovic is a contributing editor to the Age of Autism blog, a founding member of The Canary Party and the author of “An Unfortunate Coincidence: A Mother’s Life inside the Autism Controversy.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
December 12, 2023
Posted by aletho |
Full Spectrum Dominance, Science and Pseudo-Science, Timeless or most popular | Australia, Covid-19, COVID-19 Vaccine, Human rights |
Leave a comment
The video above features a lecture David E. Martin,1 Ph.D., gave in Dornach, Switzerland, in late October 2023. Martin is a national intelligence analyst and founder of IQ100 Index, which developed linguistic genomics, a platform capable of determining the intent of communications.
This technology has allowed Martin to scan and review millions of patents, resulting in a paper trail2,3 that conclusively proves SARS-CoV-2 is a manmade bioweapon that has been in the works for 58 years.
Unambiguous Admission of a Premeditated Plandemic
As he is now in the habit of doing, Martin opens his lecture with a quote by Peter Daszak, president of EcoHealth Alliance. During a March 27, 2015, forum on Medical and Public Health Preparedness for Catastrophic Events, Daszak noted4 that unless an infectious disease crisis is at an emergency threshold, it tends to be ignored.
“To sustain the funding base beyond the crisis, we need to increase public understanding of the need for MCMs (medical countermeasures) such as a pan-influenza or pan-coronavirus vaccine,” Daszak said, adding:5
“A key driver is the media, and the economics follow the hype. We need to use that hype to our advantage to get to the real issues. Investors will respond if they see profit at the end of the process.”
Martin comments:
“This is the admission, unambiguously, which states without any equivocation, that the reason for the global terror campaign that began officially in the minds of most people in late 2019, was a premeditated plan of terrorism, collusion, coercion and, ultimately, murder … This quote is the admission of four felonies, regardless of which side of the Atlantic you’re on.”
What Felonies Did Daszak Admit to in 2015?
Martin then goes on to explain how, in that quote from 2015, Daszak admitted to several different felonies. In summary:
• “To sustain the funding base beyond the crisis …” — Daszak is not speaking of expanding or benefiting public health here. He’s also not referring to an actual health crisis that was taking place when the comment was made.
No, according to Martin, “the crisis was that there was a reduction in funding of biological weapons programs sponsored by the World Health Organization. The crisis was not a health crisis. It was a funding crisis for the people who were running out of money for their bioweapons programs. Those are two crimes.”
• “A key driver is the media, and the economics will follow the hype.” — This, according to Martin, is an admission of two additional crimes. “Hype” refers to psychological terror. In other words, funding will follow provided the psychological terror is great enough, and he admits the media will be used to push that fear porn.
The second felony is economic conspiracy, because “economics that follow hype is not informed consent,” Martin notes. “That’s not willing buyer, willing seller, informed of all the facts.” Using psychological terror to secure funding implies “an intent to defraud.”
Martin explains: “Under Crown Law we call it ‘fraudulent conveyance’ when you don’t inform the counterparty of the risks associated with a contract … Why is this important?
The reason why fraudulent conveyance is such an important principle in the law, is … [because] the fraud-perpetrating party is required under the law to not just recompense the damage.
Their legal obligation is to return the damaged party to their pre-damaged state. It’s not, ‘We’re going to give you a couple bucks for your pain and suffering. No, you are legally required to return the condition to the pre-damage state.”
So, to reiterate, financial compensation is not the legal standard when it comes to fraudulent conveyance. The party that engaged in the fraud is legally required to make the defrauded whole again. And why is THAT important? Because “we’re not even asking for what we should ask for,” Martin says.
Is there a dollar amount that can cure the myocarditis you suffered after the shot? Or the turbo cancer that’s killing your mother? Or the blood clots that killed your father? “If we followed the law, we would actually recommend, not a financial compensation, we would recommend a return to the pre-damaged state,” Martin says.
• “We need to use that hype to our advantage to get to the real issues.” — What are “the real issues”? To get investors to respond with funding, which they will do if they can “see profit at the end of the process.” In other words, investors will open their pocketbooks if they can confirm that psychological terror makes people line up to receive an injection.
Why Do We Need a Vaccine for an Eradicated Infection?
Martin goes on to note that a Pan-Coronavirus Vaccine Program was actually publicly announced during the moratorium on gain of function on coronaviruses in the United States, which was in place from 2014 until 2017.6
“That gain of function moratorium was going on while we were announcing a global plan of global terrorism, a pan-coronavirus vaccine, which, by the way, the World Health Organization … declared eradicated a year earlier,” Martin says.
“How do we need a vaccine for an eradicated disease, during a gain of function moratorium, when there’s theoretically no chance that we could have a reason to need a vaccine for a thing that doesn’t exist? Well, because we were making it — professor Baric. We were hyping it — Peter Daszak … And we were going to hijack liberty with it.”
The 58-Year Timeline of SARS-CoV-2
As explained by Martin, the virus called “coronavirus” was first described in 1965. Two years later, the U.S. and U.K. launched an exchange program where healthy British military personnel were infected with coronavirus pathogens from the U.S. — “as part of our biological weapons program.”
In 1992, Ralph Baric at University of North Carolina, Chapel Hill, took a pathogen that used to infect the gut and lungs and altered it with a chimera to make it infect the heart, causing cardiomyopathy.
“Pause and think about what I just said,” Martin says. “What what goes on in the head of a person who says, ‘This was a little glitch in my tummy, it was a little sniffle in my nose. Let’s see if we can make it hit hearts and … create cardiomyopathy,’ one of the most lethal heart inflammations possible …”
In November 2000, Pfizer patented its first spike protein vaccine. So, Operation Warp Speed really didn’t produce a spike protein vaccine in a few months. No, that research had been going on since late 2000. So, the COVID shots were 19 years in the making by the time they were rolled out.
The problem is that during those 19 years, none of the coronavirus vaccines worked. “Every single trial, from November of 2000 until [2019], had killed all of the animals into which the experimental injections were placed,” Martin says.
Despite that, the University of California San Francisco’s institutional review board was told, in the summer of 2020, that the clinical trials for the coronavirus vaccine were a “straight to humans protocol.” In other words, it didn’t need to go through preliminary animal research.
As noted by Martin, it would be quite inconvenient to have safety data showing it kills animals. No one would line up for a shot like that, no matter how many free cheeseburgers you throw at them.
How Can We Know That SARS Was a Weapon?
While all of that is disturbing enough, there’s more. Martin continues:
“You kind of can’t make this egregious level of a crime up unless you realize that behind this, there must be another crime. Each one of these, in and of themselves, is horrific. But the sum of them becomes much, much, much more problematic.
Let’s go ahead and jump to the wonderful creation of the patent that was filed in 2002, which is actually the reason why I am done with everybody who ask the question ‘Was there a novel virus; was there novel disease?’ Let’s stipulate, with the facts, that there were neither.
There’s not a novel virus. There WAS a variety of biological weapons designed off the back of the patent that was filed in 2002, which was the ‘infectious replication-defective clone of coronavirus.’
Now let’s slow down and answer the question, what does that phrase mean? Infectious replication-defective. ‘Infectious’ means we want to target a cell in the body to make sure the thing that we’re injecting goes into the cell …
‘Replication-defective’ means we want the information that we inject to infect that cell, but not replicate and spread to others, which means that the bioweapon itself was engineered as a weapon to hit a target, but not proliferate.
That’s what the patented technology is, which is the reason why, when we had SARS 1.0 in 2002 and 2003 … we were [told there would be] dead people everywhere. [But] as hard as we tried to make it into a pandemic … we [could] only kick 900 people off the mountain. That was the global pandemic. Why? Because the weapon worked.
If you exposed somebody to the toxic agent, they died. But they didn’t spread it to others, which is the reason why we did not have the transmission of SARS 1.0, because you can’t transmit a thing that’s designed not to replicate.
But worse still: What is the definition of a virus? … A virus is a replicating protein sequence. Guess what this isn’t? Replication-defective means we took the virus out of a virus. It was not a replicating device. It was in fact a weapon.
Now, I’ve got tons of people who go, ‘Dave, you’re crossing the line, don’t say it’s a weapon. It’s not a weapon … You offend people who kill people when you call it a weapon.’ Well, guess what, if you’re offended, I don’t care, because I didn’t call it a weapon — the guy who built it called it a weapon.”
mRNA Spike Protein Is a Biological Warfare Agent
Indeed, mRNA spike protein was publicly described as a bioweapon 18 years ago. In 2005, at a conference hosted by DARPA and the Mitre Corporation in the U.S., the mRNA spike protein was hailed as a “biological warfare-enabling technology.” Does that sound like it has any public health-related applications? No, as Martin insists, “biological warfare-enabling technology” means it’s a biological warfare agent.
“So, I’m not the one saying that it’s a biological weapon. I’m not the one saying it’s biological warfare,” Martin says.
“The perpetrator called it that in 2005, and was rewarded with a dual entry budget, where … the University of North Carolina, Chapel Hill, received money from Anthony Fauci’s NIAID/NIH budget, and exactly at the same time … Fauci had a second checkbook [that] came from the Department of Defense pandemic preparedness program. And guess what that was? An equal matching noncompetition grant …
In Europe, that’s a violation of anti-competition laws. You’re not allowed to double down on a public grant without competition or transparency, saying that this agency is going to give you $10 million … and [a second] one is going to give you $10 million … because [the first] one gave you $10 million —
Not because it was fair, not because it was open, not because it was transparent, not because there was actually grant competition, but by virtue of the determination of one side, the other side facto matched the money. And that started in 2005, not in 2019.”
Big Pharma Owns All North Carolina Universities
Over the past two years, a lot of information has come out exposing how Daszak funneled millions of research dollars to the Wuhan Institute of Virology (WIV) in China for gain of function research on coronaviruses. However, that’s just the tip of the iceberg. According to Martin, at least $141 million went to the U.S. bioweapons program led by the University of North Carolina Chapel Hill. Martin continues:
“I have been the most ardent advocate for shaming the University of North Carolina Chapel Hill for a very good reason … and the reason is because in 1984, the state of North Carolina, not just the university, sold itself to … GlaxoSmithKline and the Wellcome companies.
The reason why you’ve heard the term ‘Research Triangle Institute’ or ‘Research Triangle Park’ — which is University of North Carolina Chapel Hill, Duke University and North Carolina State University — is because the state of North Carolina sold its universities to GlaxoSmithKline Wellcome, and they did it because of AZT.
AZT was on patent, and we needed a state in the United States to be ground zero, to make sure that AZT became the drug of choice for the treatment of HIV. So in 1984, we invent HIV, conveniently for the purpose of making sure we have one treatment: AZT.
Here’s the interesting little fact that very few people know. If you go back and look at the videos of Anthony Fauci in 1985 and 1986 … he’s talking about [getting] a vaccine for HIV. But he suddenly got a knock on the door from GlaxoSmithKline going, ‘Hey Mr. Fauci, don’t start that project until the patent on AZT runs out.’
I’m not making this up. It’s actually videos that you can see. And so, mysteriously, courtesy of the Wellcome AZT protest, from 1991 to 1996, the world was told that the only treatment for HIV was AZT, and as such, the patent and the rest of the patent life on AZT could expire, so that GlaxoSmithKline Wellcome could get all of the money for the patented technology for a thing that was killing patients that allegedly had HIV.
Murder for hire. North Carolina sold the state so that could happen. Conveniently, the National Institute of Allergy and Infectious Diseases (NIAID) decided that UNC Chapel Hill was its go-to institution, while AZT was in its monopoly run, to begin the process of doing HIV vaccine research …
So, ‘91 to ‘96 is the AZT cover story. Underneath that you have Ralph Baric genetically modifying and making chimeras of this coronavirus thing to create an HIV vaccine, which is going to conveniently roll out in 1997, as the patent on AZT expires.
[This] is the reason why you need to figure out how to get the gastrointestinal and flu problem to become a heart problem: Because you need to get that package, that little envelope around what we call coronavirus … to deliver the HIV vaccine.
So all of the funding for the HIV vaccine that was going to this program was actually going to use coronavirus as the packet in which the HIV vaccine was going to be delivered. That’s the model. [There are] hundreds of papers on this.
And, this is why this question of … is there HIV fragments somewhere in [the COVID shots]? The answer is, of course there is. It was designed into it. And it was designed into it, not a couple of years ago, not by Moderna, not by BioNtech. This was designed in many, many years earlier.
Not surprisingly, from ‘96 to ’99, Ralph Baric begins the weaponization of this allegedly synthetic coronavirus envelope to become a vaccine vector. 1999 comes along, and lo and behold, Baric and Fauci create what I affectionately call FrankenCoV.
What’s that? That is the monster, that’s the chimera. That’s the idea that we can change surface glycans, we can change surface spike proteins, we can change surface oligomerization, we can do all kinds of things to modify this thing.
So we can actually have this … package shell, the outer edge of coronavirus, we can allow that to be the carrier of getting anything we want into any cell we want. Which is the reason why the 2002 patent becomes interesting.”
NIAID Funded Research to Increase Human Pathogenicity
Next, Martin shows a letter, dated October 21, 2014, from the National Institute of Allergy and Infectious Diseases (NIAID) to the University of North Carolina Chapel Hill, declaring that Baric’s grant I1077810-02 had been deemed subject to the moratorium on gain of function research involving coronaviruses. However, at the bottom of the page 1, it also states that:
“As this grant is already funded, the pause is voluntary and you can continue to conduct the applicable GOF [gain of function] research until the end of the currently active budget period.”
In other words, the NIAID gave Baric a free pass to decide whether he wanted to abide by the moratorium or not. What’s more, the grant actually didn’t have a termination date, because it was a noncompetitive, perpetually funded grant. So, Baric was given a free pass to conduct gain of function research indefinitely.
And what was this grant for? To increase the “human pathogenesis” of coronavirus in vivo, meaning inside the body. “Two billion people are going to be incapacitated or killed — because of this letter,” Martin says.
Who Can Be Held Accountable?
Alright. So, why can’t we just prosecute Baric, Fauci and whomever else and be done with it? Because this research project was placed under the World Health Organization’s GAVI Vaccine Alliance, and under Article 5, Section 13 of the WHO’s charter, they cannot be investigated or prosecuted for any crimes committed. GAVI, headquartered in Geneva, Switzerland, also has diplomatic immunity and cannot be investigated by local authorities there either.
“They knew that if they put the project under the WHO, it was shielded from all criminal investigation and all criminal liability — forever,” Martin says.
But that’s not all. 2010 to 2020 was declared The Decade of Vaccines. GAVI devised a global vaccine action plan that included global acceptance of a “universal influenza-coronavirus vaccine” by 2020, to protect against “accidental or intentional release” of a respiratory pathogen. As noted by Martin, “release” is “an active, intent-filled word. It is not an ‘oops’ accident.”
Recall, the same person who said they needed to create media hype to create sustained funding, Daszak, was appointed to lead the WHO’s investigation into the lab leak theory. Not surprisingly, his team decided there was no evidence to support the lab leak theory and it was probably a case of zoonotic transference after all.
A Crime That Keeps Going and Going
Martin also stresses that this crime is not just about the creation of COVID. It’s a crime that keeps going and going. He explains how children were murdered in 2011 clinical trials for a malaria vaccine. Sixty-six of the children in the vaccine group suffered serious and/or fatal adverse events, as did 28 in the control group. However, controls were not given saline, but rather a cocktail of other vaccines.
“When people attempted to hold the clinical trials agents accountable for their actions, guess what they referred to? They referred to Article [5 Section] 13 of their representative as members [of the WHO, which gives them] ‘immunity from personal arrest or detention and from seizure personal baggage and respect to words spoken or written and all acts done by them in their official capacity, immunity from legal process of every kind.’
That’s in the charter of what we call the World Health Organization. That ladies and gentlemen is the mafia, and we should stop pretending it’s something else.
It is an embarrassment to the Swiss people. It is embarrassment to the Swiss government that the World Health Organization exists in this place. Because the Swiss have enabled the organized crime of the World Health Organization, and they have enabled it so that real individuals can murder children under the age of three months …
We the People cannot allow this to happen. We’re talking about the [WHO pandemic] treaty … [when] we should be talking about the World Health Organization itself, not the treaty. And as long as Section 13 of Article 5 remains in the charter, I don’t care what treaties they pass, it doesn’t matter, because the institution is corrupt at its core, and you can’t fix that. That is a license to kill.”
Martin also provides a quick review of the history of how the WHO came to be, and how, in 1952, then-director-general of the WHO, Brock Chisholm, declared that “the role of the WHO is population control.”
Aside from being in charge of population control, the WHO is a marketing and distribution arm for private sector interests that sponsor it (Bill Gates being a primary one), while simultaneously providing them with immunity from prosecution.
According to Martin, Gates various organizations provide so much money to the WHO that “By every definition of the law, [the WHO] is a wholly owned subsidiary.”
Timeline
Toward the end of his speech, Martin summarizes some of the key items on the timeline of the conspiracy to commit global genocide:
• In 2002, U.S. scientists developed the weapon.
• In 2003, the U.S. Centers for Disease Control and Prevention patented the weapon in its first commercial deployment (SARS).
• In 2005, mRNA spike protein was declared a biological “warfare-enabling” technology.
• In 2016, Proceedings of the National Academy of Sciences published “SARS-Like W1V1-COV Poised for Human Emergence.”7 The W1V1-COV refers to the first COVID-like virus made at the WIV. In that article, they not only state that the virus is ready for release, but they also detailed the best ways to release it.
At the bottom of the article, you also learn that the University of North Carolina Chapel Hill impaneled two separate institutional review board reviews of this study, the first to review the ethics of the research and a second to review the ethics of violating the gain of function moratorium, which is unusual to say the least. As noted by Martin:
“You do not usually have an ethics board going ‘Well, should we do this? It’s probably a bad idea.’ And then somebody goes, ‘It’s illegal’ … ‘OK, should we do the illegal thing?’ ‘Yeah, let’s go ahead do that. The guys over here said it was ethical to do the illegal thing to kill people.’ That happened and is published in this 2016 article.”
• September 18, 2019, the Global Preparedness Monitoring Board, jointly founded by the WHO and the World Bank,8 warned that “a rapidly spreading pandemic due to a lethal respiratory pathogen (whether naturally emergent or accidentally or deliberately released) poses additional preparedness requirements.”
Furthermore, the “Progress indicator by September 2020” section specified the commitment by donors and member countries to finance and develop a universal influenza vaccine and other therapeutics.9
“This is the admission by the World Health Organization that they are going to do a release of a respiratory pathogen,” Martin says, adding:
“And, by the way, the reason why this is particularly important is they say ‘a lethal respiratory pathogen.’ They knew they were going to kill people. That’s why they use the word lethal …
This is the evidence that we can use in a criminal case to say, ‘This was not an accident. This was an actual premeditated act of lethality.’ They not only told you when it was going to happen. They told you the deadline for the outcome response. ‘We’re going to release the pathogen so that by September 2020, the world has accepted a universal vaccine.’ That is prima facia terrorism, collusion, racketeering, criminal conspiracy and … murder.
So that’s why we have the Wanted posters … [for] Peter Daszak … Ralph Baric … Jeremy Farrar … Chris Elias … Ghebreyesus … Bill Gates, Anthony Fauci, the World Health Organization, DARPA, the United Nations … Rockefeller Foundation, the Wellcome Trust and the Gates Foundation.
These individuals, in violation of racketeering, antitrust and anticompetition laws, colluded to create the largest act of global terrorism known to Earth and announced the plan to do it on September 18, 2019, with premeditation and with the intent to kill.
This was entirely a premeditated act. They told us it would happen in 2011. They announced the event horizon in 2019 … Conspiring to commit acts of terror, restraint of trade, deceptive medical practices, price fixing, fraudulent conveyance. These are the crimes that the World Health Organization not only allowed to happen, but [it also] promoted these crimes and gave political cover for those crimes …
All-cause mortality in the ages of 18 to 55 is now 40% higher in the people that were injected with a biological weapon. That number is not going down. That number is going up in every jurisdiction. And here’s the saddest part about it. That number will continue to go up. If they [meet] their 2011 objective, that number will go up to 2 billion people.”
The Damage Is Done
Martin points out that even if they don’t unleash any other bioweapons, the desired death toll may still be achieved, because they used pseudouridine in the mRNA shots, which is causing “turbo cancers.”
Pseudouridine suppresses cancer-controlling agents and promotes oncogenic activity in the body, and this has been known since 2018, so its inclusion was hardly an accident.
The shots are also targeting reproduction, which is a key target if you want to depopulate. It’s not just infertility. Prostate, ovarian and uterine cancers make it more difficult to have sex, and hence more difficult to have children.
According to Martin, the evidence is clear. None of this is accidental. It’s a conspiracy, alright. But not a conspiracy theory in the dismissive sense. It’s a global conspiracy by identifiable agents who have, for nearly 60 years, plotted to commit, and profit from, the greatest genocide the world has ever seen, while hiding behind the false veneer of “public health.”
Sources and References
December 11, 2023
Posted by aletho |
Deception, Timeless or most popular, Video, War Crimes | Covid-19, COVID-19 Vaccine, NIAID, United States |
Leave a comment
Austrian Doctor Cornelia Tschanett’s U-Turn on the vaccinations:
“We have carried out around 3,000 to 4,000 vaccinations in my practice. And as few side effects as we saw at the beginning. This slowly became more the case over the course of the year.
You may not notice the first cases that much or dismiss it as an isolated case. Possibly also as a psychological overreaction. Towards the end of the year this increased. Then more and more people came with supposed complaints after the vaccination. And then you question your own perception a bit. And it was also difficult to discuss it.
We will then have it in the course of autumn 2021. There are also groups founded by doctors who also vaccinate. And then you realize they perceive the same thing in their patient clientele. People report the same complaints such as cardiac arrhythmias, insane fatigue, persistent muscle pain, nerve inflammation. This then slowly became reproducible. And then of course you also try to look for scientific discourse. And that was shocking to me that that wasn’t possible. That was dismissed.
It was actually an absolutely dogmatic and certain and rock-solid statement, this is not from the vaccination. And the more patients came, the greater the inner conflict became for me and for many doctors, who actually want the best for their patients.
An impressive, the first case, was a 16-year-old boy, who arrived at us 48 hours after the second dose with nausea and chest pressure. I took an EKG and the EKG was impressively changed. So not normal for a 16 year old.
We then sent him to the hospital. A massive myocarditis of the heart was diagnosed there. Thank God he got well again. But that was the moment where I really stopped. Because people come at the same time, mothers with their children, young people, and they have literally said the sentence very often, “I don’t know what’s right, I put my life in her hands.” And this power of trust induces an enormous responsibility for me personally, to be honest. It makes no difference whether you have seen this case once or ten times. The risk exists, the connection is vacant. Until proven otherwise, we actually have to educate people about what we see and what experiences we have. A person has this right if he or she decides to undergo physical intervention, who is so small decides.
That was an inner conflict for me, because the social pressure to vaccinate as many people as possible and to vaccinate all age groups was very great. And on the other hand, personal experience as a doctor has increased, that this is not possible without side effects. That was the moment when I thought to myself, I can’t continue to vaccinate here, I have to stick to the truth, I have to live up to this trust.
We must have had 300-400 people, who have come to us with the feeling that they have had problems since the vaccination. I have about 60-80 EKGs, the ones on previously young, healthy people had clear changes or rhythm disturbances have shown.
This clip was taken from of the two-part documentary ‘UN-SICHTBAR Der Film Teil 1’ published by Schutzfilm on October 12, 2023.
https://www.bitchute.com/video/mxZVBB8DNaUz/
December 10, 2023
Posted by aletho |
Timeless or most popular, Video, War Crimes | COVID-19 Vaccine |
Leave a comment
A report released by Statistics Canada (“StatsCan”) on 27 November showed that the number of covid deaths in highly vaccinated Canada rose by 36% last year.
The largest increase was in Atlantic Canada, where the number of covid deaths per 100,000 population in 2022 was more than seven times higher than in 2021. Atlantic Canada also had the highest uptake of covid “vaccines.”
As well as soaring covid deaths, Canadian government data reveals a staggering 135% death spike classified as “other ill-defined and unspecified causes of mortality.”
The report also reveals that Canadian life expectancy dropped for the third year in a row. The falling life expectancy trend coincidentally started in 2020.
According to StatsCan, the nation recorded a record number of covid deaths, despite high vaccination uptake and the pandemic having ended.
As of 10 September 2023, 83% of Canadians have had at least one dose of the covid injection.
Except for Nova Scotia where 83% of the population had at least one dose, Atlantic Canada – which makes up less than 7% of Canada’s population and comprises the provinces of New Brunswick, Newfoundland and Labrador, Nova Scotia, and Prince Edward Island – had higher vaccination uptake than the national average of 83%: New Brunswick (87%), Newfoundland and Labrador (96%) and Prince Edward Island (90%).
According to StatsCan, Atlantic Canada also had a seven-fold increase in covid deaths last year; 59.5 deaths per 100,000 population in 2022 versus 8.3 deaths per 100,000 in 2021.
Despite the clear safety signal of increased deaths, the Government has an autumn booster campaign recommending that Canadians get “an updated covid vaccine dose.”
Maxime Bernier, the leader of the conservative People’s Party of Canada (“PPC”), broke the story on Twitter about “more shocking data on the number and causes of deaths” in Canada released by StatsCan. He tweeted:
In a PPC newsletter dated 5 December, Bernier delved into the implications of the report, saying, “These deaths have almost TRIPLED since 2020 from 6,841 to 16,043 in 2022.”
“What happened in 2021 that could have caused this explosion of unexplained deaths over the last 2 years? An experimental pharmaceutical product was rushed to market and forced on Canadian society, is what happened. They told us it was ‘safe and effective’ but over the last few years we have learned more and more about how that covid shot was neither,” Bernier said.
The PPC leader then accused the establishment of ignoring such a significant development, saying this breaking news was “ignored by all of our crooked establishment politicians and the dishonest corporate media.”
Sources for this article include:
December 9, 2023
Posted by aletho |
Civil Liberties, Science and Pseudo-Science | Canada, COVID-19 Vaccine, Human rights |
Leave a comment



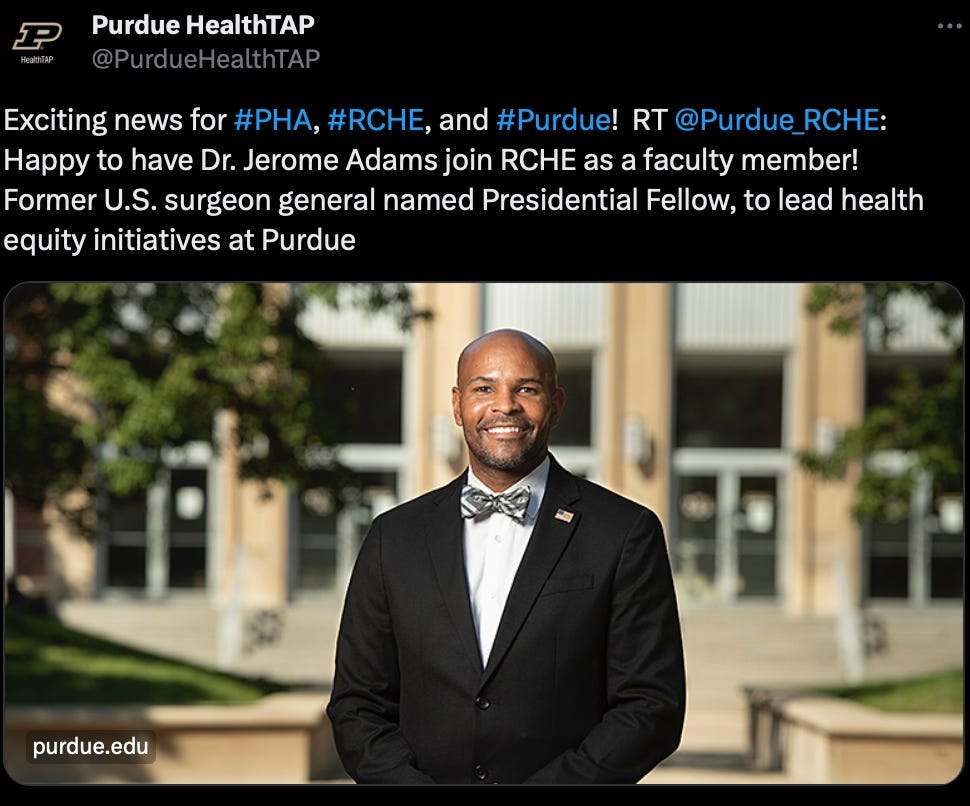


 Aletho News
Aletho News