"Own Nothing – be Happy" 😍🫂
feat. Klausi McSchwabbin' pic.twitter.com/oVLTVSVvtJ— Snicklink (@snicklink) September 26, 2023
Nobel Winner Highlighted “Non-Trivial” Side Effects of mRNA Vaccines Including Auto-Immunity and Blood Clotting Risks

BY ROBERT KOGON | THE DAILY SCEPTIC | OCTOBER 2, 2023
In what seems like an inevitable development, scientists Katalin Karikó and Drew Weissman have been awarded the 2023 Nobel Prize in Medicine for their role in developing the mRNA technology underlying the Pfizer-BioNTech and Moderna COVID-19 vaccines, which were rolled out in late 2020.
But in a paper published as recently as 2018 and which is extensively quoted in an article at MedPageToday, none other than Drew Weissman warned that prior clinical trials of mRNA vaccines had produced results which were “more modest in humans than was expected based on animal models… and the side effects were not trivial”, including “moderate and in rare cases severe injection site or systemic reactions”.
Further summarising the paper by Weissman and three colleagues in Nature Reviews Drug Discovery, MedPageToday notes:
Their chief safety concerns, which they said should be closely watched in future trials, were about local and systemic inflammation, as well as keeping tabs on the “expressed immunogen” and on any auto-reactive antibodies.
“A possible concern could be that some mRNA-based vaccine platforms induce potent type I interferon responses, which have been associated not only with inflammation but also potentially with autoimmunity,” they wrote. “Thus, identification of individuals at an increased risk of autoimmune reactions before mRNA vaccination may allow reasonable precautions to be taken.”
The authors also noted that extracellular RNA could contribute to edema, and cited a study that showed it “promoted blood coagulation and pathological thrombus formation.”
The MedPageToday article is titled ‘Want to Know More About mRNA Before Your Covid Jab?‘ How many readers actually went ahead and got it after they knew?
Robert Kogon is the pen name of a widely-published journalist covering European affairs. Subscribe to his Substack and follow him on X.
MRNA vaccines must be banned once and for all
By Angus Dalgleish | TCW Defending Freedom | September 29, 2023
Those of us who knew from the beginning that the sequence of CoV-SARS-2 contained inserts which could not have possibly occurred naturally, and were similar to ones that had already been published from the Wuhan laboratory, have had to endure unbelievable scorn, scientific ostracism and the ignominy of being ‘cancelled’ by the MSM as well as by professional colleagues for nearly three years now.
In the summer of 2020 a paper I co-authored, describing the findings of an Anglo-Norwegian team of scientists who had demonstrated unique ‘fingerprints’ of laboratory manipulation in the Covid virus, was suppressed in both the US and UK. This was at the time that the World Health Organization, leading science journals and others were going to huge lengths to persuade us that Covid was a natural occurrence, and that we should spend a lot more money to fight any such future threats.
Only now does the Telegraph (uncritically) report that the US government is no longer going to fund the research it denied doing for nearly three years and the MSM sat on. Yet it has been an open secret for anyone who follows primary sources of information (the ones ignored by the MSM and the BBC specifically, reported as misinformation by Ofcom and targeted by the Orwellian Counter-Disinformation Cell of the UK government) that mRNA vaccines did not do what it says on the vial, as it were.
First the ‘vaccine’ did not stay at the site of injection as promised but travelled throughout the body and were found at post-mortems to be everywhere.
Accusations of dramatic variations in batch-to-batch variability – an absolute ‘no no’ in vaccine manufacture protocols – which could explain why side effects were more common in some batches than others were denied but were borne out by definitive Danish research reported here. These alarming concerns seem to have been brushed off by the regulators when they should have immediately begun investigating them in depth.
All the while the regulatory authorities and politicians, parroting their ‘highest standards’ assurances, have repeatedly declared the mounting disturbing UK Yellow Card and US VAERS adverse event reports to be nothing to be worried about.
Last June, whistleblowers led by the scientists Sucharit Bhakdi and Kevin McKernan raised an entirely new issue of concern – that of serious levels of DNA contamination. Once again this was ignored by the MSM. Though quite happy to report the odd side effect from the vaccines as an excuse to point out that they are extremely rare, they have never addressed the increasingly problematic official ‘safe and effective’ mantra.
Finally there was a small breakthrough. An isolated but braver branch of the MSM in the form of the Spectator Australia has finally blown the lid on serious levels of contamination of both Pfizer and Moderna mRNA Covid vaccines. The article describes how the genomics scientist Kevin McKernan from Boston used Pfizer and Moderna vials as controls in a study only to find that they contained highly significant DNA plasmid contamination. It reports that McKernan was alarmed to find the presence of an SV40 promoter in the Pfizer vaccine vials, a sequence that is ‘used to drive DNA into the nucleus, especially in gene therapies’ and that this is ‘something that regulatory agencies around the world have specifically said is not possible with the mRNA vaccines’. These SV40 promoters are also well recognised as being oncogenic or cancer-inducing.
Others have confirmed these findings. A German biologist whistleblower has found contamination rates of up to 354 times the recommended limit. All this has been reported to the US Food and Drug Administration (FDA). It is highly significant.
To put it bluntly, this means that they are not vaccines at all but Genetically Modified Organisms that should have been subject to totally different regulatory conditions and certainly not be classed as vaccines. This has been recognised by the Australian version of the FDA, the TGA, which has changed the picture so much that the Premier of Victoria Dan Andrews, who was the greatest proponent of the vaccine and of its mandatory use, has resigned – though at the time of writing the vaccine has not been mentioned as the reason for his resignation. (Paula Jardine reported in these pages in December 2021 on this regulatory sleight of hand in granting vaccine Emergency Use Authorisations for what were gene therapies.)
All this data, which is slowly breaking through into the public domain, comes hard on the heels of the latest findings that booster vaccines actually increase the chance of getting infected by 3.6 times. This is according to an in-depth study published by the Cleveland Clinic, one of the largest health care organisations in the world, who monitored their staff as well as patients.
It gets worse. Supporters of this technology have claimed that it can be adapted to chase new variants. But it can’t. The results of bivalent vaccines (with components against at least two variants) are seeing the same result. Authors of the Cleveland study say that ‘there is not a single study that has shown that the Covid-19 bivalent vaccine protects against severe disease or death caused by the XBB lineages of the Omicron variant. At least one prior study has failed to find a protective effect of the bivalent vaccine against the XBB lineages of SARS-CoV-2.’
In one study, all bivalent-vaccinated mice which were challenged with Covid became ill.
This was predicted by many of us as the SARS viruses are subject to immunological imprinting: that is, once they have seen a vaccine they will make the same response to any close variant (this is also known as ‘antigenic sin‘) making further vaccines not only useless but more dangerous as they induce antibodies that enhance infection (ADE antibodies), not cross reactivity as has been claimed by the manufacturers.
This is not the end of the issues with the mRNA ‘vaccines’. Several immunology studies have shown that the boosters induce an antibody switch from neutralising subtypes to tolerising subtypes as well as inducing significant T cell suppression, all of which will encourage new infections and suppress the immune response to cancer.
At the end of last year I reported that I was seeing melanoma patients who had been stable for years relapse after their first booster (their third injection). I was told it was merely a coincidence and to keep quiet about it, but it became impossible to do so. The number of my patients affected has been rising ever since. I saw two more cases of cancer relapse post booster vaccination in my patients just this last week.
Other oncologists have contacted me from all over the world including from Australia and the US. The consensus is that it is no longer confined to melanoma but that increased incidence of lymphomas, leukaemias and kidney cancers is being seen after booster injections. Additionally my colorectal cancer colleagues report an epidemic of explosive cancers (those presenting with multiple metastatic spread in the liver and elsewhere). All these cancers are occurring (with very few exceptions) in patients who have been forced to have a Covid booster whether they were keen or not, for many so they could travel.
So why are these cancers occurring? T cell suppression was my first likely explanation given that immunotherapy is so effective in these cancers. However we must also now consider DNA plasmid and SV40 integration in promoting cancer development, a feature made even more concerning by reports that mRNA spike protein binds p53 and other cancer suppressor genes. It is very clear and very frightening that these vaccines have several elements to cause a perfect storm in cancer development in those patients lucky enough to have avoided heart attacks, clots, strokes, autoimmune diseases and other common adverse reactions to the Covid vaccines.
To advise booster vaccines, as is the current case, is no more and no less than medical incompetence; to continue to do so with the above information is medical negligence which can carry a custodial sentence.
No ifs or buts any longer. All mRNA vaccines must be halted and banned now.
MHRA Finally Admits it Failed to Test the Safety of Mass Manufactured Covid Vaccine Batches
UK’s medicines regulator comes clean
By JJ Starky| The Stark Naked Brief | September 28, 2023
On December 8th, 2020, June Raine, the Head of the Medicines and Healthcare products Regulatory Agency (MHRA), publicly declared that “no corners have been cut” during the temporary authorisation of the Pfizer Covid vaccine. However, thanks to the persistence of former Ministry of Defence employee, Nick Hunt, recent findings prove Raine’s statement was not true.
For context, it’s common in development trials across various sectors to first use products made in small-scale facilities or laboratories. Investing in mass production usually comes later, once there’s sufficient confidence in the product’s design. Scaling up, naturally, introduces new risks.
With pharmaceuticals, regulations are in place to manage this process. This is to ensure the final product remains consistent and effective.
Concerns first arose in 2022 regarding the Pfizer Covid vaccine. There were suspicions that the vaccine MHRA approved in December 2020, manufactured using “Process 2”, differs from the version tested in Pfizer’s clinical trials, manufactured using “Process 1”. Josh Guetzkow, an Israeli academic, brought the difference to light, referencing Freedom of Information requests from various countries and Pfizer documents released by U.S. courts.
In May 2023, he published this rapid response in the British Medical Journal alongside Professor Retsef Levi, airing his concerns.

Guetzkow highlighted two things. First, there is a lack of publicly available reports comparing vaccines produced by both processes. Second, there is significant variability in the rate of serious adverse events across different vaccine lots, underscoring the need to better understand variability in the production process.
In October 2020, Pfizer had committed to comparing safety and immunogenicity results between vaccines produced by both processes. Yet, when Hunt submitted his initial FOI request concerning the latter to MHRA in July, their initial response directed him to the European Medicine Agency’s archive without specific guidance.
Here’s the bombshell.
Nick then requested an internal review. In their response, MHRA admit their replies “were not compliant with the (FOI) Act and did not provide or address the specific information (Nick) asked for”.
They then confess they do not possess the “Process 2” report.
The document goes on to state the “Process 2 drug… was shown to be comparable through side-by-side comparability studies and heightened characterisation testing”. In short, trust us, we’ve seen the data but we can’t show it to you and we don’t have it.
Worse yet, MHRA also revealed they failed to chase Pfizer on the promised report that the company should have published comparing the products. This was because of the “extensive usage of vaccines manufactured via Process 2”.
Multi-Hit Hypothesis for the Oncogenic Potential of mRNA COVID-19 Vaccines
Pathophysiologic Support for the Observation of “Turbo Cancer” after Vaccination
By Peter A. McCullough, MD, MPH | Courageous Discourse | September 29, 2023
As an internist and specialist, it is hard for me to believe that a novel biologic product could cause heart, neurologic, thrombotic, and immunologic disease but to make matters even worse, could also play a role in the initiation and acceleration of oncogenesis. In Western countries before the pandemic, the leading causes of death were heart disease 40%, cancer 40%, and death from other known causes (homicide, suicide, accidents, etc). The mRNA COVID-19 vaccines if proven to promote cancer, would then be implicated in rises in all-cause mortality being observed world wide.
In 1984, Sutherland and Bailer proposed the “Multi-Hit Hypothesis of Carcinogenesis:”
“A new multihit model of carcinogenesis is developed for use in evaluating age-specific cancer incidence rates in human populations. The model allows for some heterogeneity in both risk (perhaps genetic) and pathway (number of hits).”
They essentially said it takes multiple different hits or insults to cells and their genetic machinery to cause a normal cell to become cancerous. Forty years later, Sutherland and Bailer could not have dreamed about the application of their hypothesis to global mass genetic vaccination given every six months to a broad population, some with high risks for, or even with incipient cancer.
Angues and Bustos just released a paper on the Authorea preprint server that assemblies the evidence to date that both mRNA and the Spike protein work within human cells to cause changes that result in oncogenesis. The figure shown is consistent with a multi-hit hypothesis of oncogenesis after injection with Pfizer or Moderna.
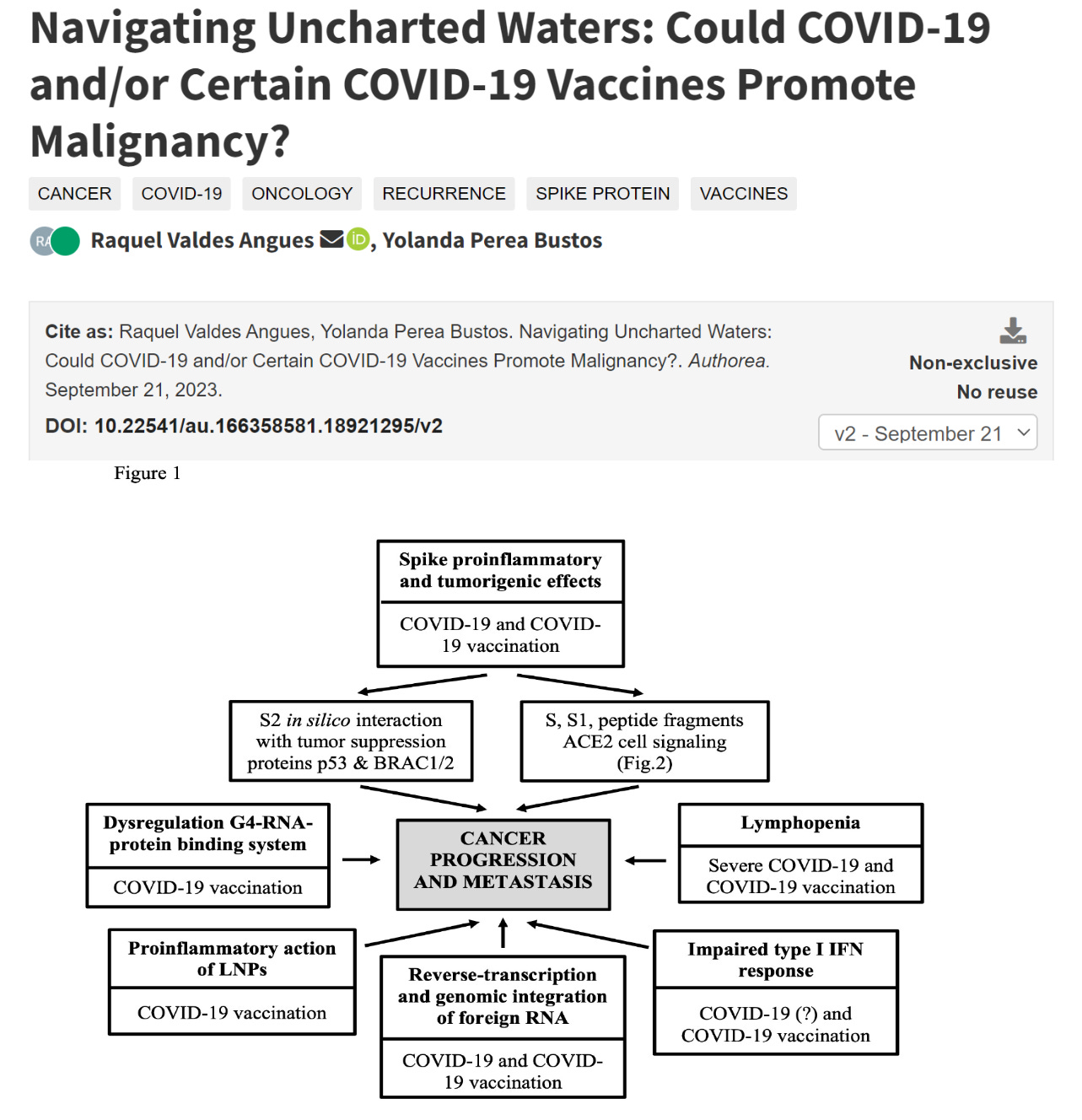
Raquel Valdes Angues, Yolanda Perea Bustos. Navigating Uncharted Waters: Could COVID-19 and/or Certain COVID-19 Vaccines Promote Malignancy?. Authorea. September 21, 2023.
Many questions remain including cumulative dose effect, predisposition (e.g. loss of function mutations in BRCA1/2 P53), additional exposures such as UV radiation, smoking, alcohol, and finally catabolism of mRNA and Spike. Undoubtedly decades of research will be needed to fully understand COVID-19 vaccination and cancer. As we point out in our book Courage to Face COVID-19, it took over 40 years from when Sir Austin Bradford Hill causally associated smoking with lung cancer until there was capitulation by the medical orthodoxy. Let’s hope the world wide exposure of mRNA and alacrity of modern research can shorten this timeframe.
Here are some reasonable first steps:
- Remove all COVID-19 vaccines from human use to reduce any additional exposure
- CDC should link vaccine administration data with all government cancer registries
- The National Cancer Institute should urgently fund mRNA COVID-19 vaccine cancer research
- Vaccinated with prior histories of cancer should make a specific post-vaccination oncology clinic visit to consider reassessment or restaging
- Vaccinated with no prior history of malignancy should check to see they are up to date on routine cancer screening (prostate, lung, breast, ovary, uterus, colon).
- All vaccinated patients and their doctors should be alert to any change in health status and have a low threshold for clinical investigation
Peter A. McCullough, MD, MPH
President, McCullough Foundation
Five evidence-based early known Covid facts – ignored and censored
Highly acclaimed experts presented evidence-based facts on Covid-19 early in 2020, but were ignored and censored by authorities
BY THEO L. GLÜCK | FREEDOM RESEARCH | SEPTEMBER 26, 2023
The official narrative in the Covid crisis tried to persuade the public that various mandates and coercions, limiting people’s individual freedoms, were all based on science. The myth of this has visibly eroded, as it has been revealed how much of the strategies, influencing the lives of millions, was based on fear, pressure from media and political tactics. Reference to science was often enough used as a disguise.
Five evidence-based facts known already in 2020, but ignored by the authorities:
- The virus had spread much more widely and was far less dangerous than initially claimed by the authorities.
- The risk from Covid-19 differed by a factor of 1,000 for different age groups, and the risk was much higher for people with comorbidities (e.g. obesity, diabetes, anxiety disorders, etc.) and nutrition deficiencies.
- Those who had recovered from the disease had developed strong natural immunity, but this evidence-based fact was systematically ignored or downplayed by the authorities.
- Covid-19 vaccines received marketing authorisation without having been tested in clinical trials for virus transmission or infection.
- Covid-19 vaccines have considerable side effects that were already known during the clinical trials of the vaccines.

The closure of parks and playgrounds was part of lockdown policies, carried out with reference to science.
Already in 2020, there were a number of important and evidence-based facts about both Covid-19 and the response to the Covid crisis that were highlighted by many scientists and doctors. Consideration of these facts would have prevented the introduction of ill-considered and ineffective Covid measures and reduced the resulting harms.
The virus had spread much more widely and was much less dangerous than claimed
The SARS-Cov-2 virus was already much more widespread globally in early 2020 than official sources (including the World Health Organization, or WHO) claimed. Prof. Jayanta Bhattacharya and Eran Bendavid wrote on March 24, 2020, that fears of Covid-19 were based primarily on a miscalculated death toll reported by the WHO, which was vastly exaggerated as it did not take into account the actual rate of infection. This meant, in particular, that the mortality rate among those infected was much lower than initially claimed and the risk posed by Covid-19 to the vast majority of people, particularly those under 70, was many times lower.

A team led by professor John P. Ioannidis of Stanford University scientifically showed in a study published already in May 2020 that the risk of dying from Covid-19 for people under the age of 65, even in pandemic epicentres, was very low, and deaths amongst people under the age of 65 with no comorbidities were remarkably uncommon. They proposed that strategies focusing specifically on protecting high-risk elderly individuals should have been considered in managing the pandemic.
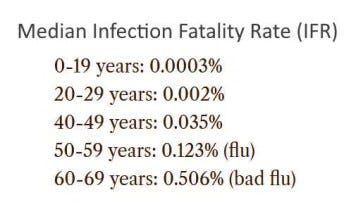
On October 14, 2020, the Bulletin of the World Health Organisation published a study by prof J. P. Ioannidis, according to which the median rate of deaths among people infected with Covid-19 in autumn 2020 was 0.23-0.27%, with a rate of 0.05% among people under 70 years of age, which was tens of times lower than official (including the WHO’s) estimates in March and April 2020.
Even though such evidence-based data were known early on, the authorities in many countries and the WHO continued to scare the public about the particular danger of a novel viral disease, and imposed restrictions on millions of healthy people. Among other things, many countries restricted people from exercising, staying outdoors and playing sports, thereby compromising people’s overall health and increasing the risk of developing all the diseases (including Covid-19) more severely.
Thousand-fold difference in the risk from Covid-19
Harvard University Professor Martin Kulldorff had already stated in April 2020 that it was clear from the data from Wuhan early on in the crisis that there was a thousand-fold difference in the risk from Covid-19 across different age groups, and that failing to account for this difference was one of the major flaws in the public response to the Covid crisis.

Prof Martin Kulldorff was quick to point out the thousand-fold difference in risk from Covid-19 (Thérèse Soukar, CC BY-SA 4.0, via Wikimedia Commons)
Among people exposed to Covid-19, people in their 70s had roughly twice the mortality of those in their 60s, 10 times the mortality of those in their 50s, 40 times that of those in their 40s, 100 times that of those in their 30s, 300 times that of those in their 20s, and a mortality that was more than 3000 times higher than it was for children. According to Kulldorff, public authorities should have taken this wide variation between age groups into account when designing Covid interventions. Counter measures specifically targeting the elderly, the highest risk group, would have not only protected them but other groups as well. Age-specific measures had to be part of the strategy, otherwise unnecessary mortality, hospital burden and economic losses followed.

Professor Mark Woolhouse of the University of Edinburgh also estimated early on that the elderly were 10,000 times more at risk from Covid-19 than those under 15. But it goes e ven further. It’s not just the elderly, it’s the elderly who are infirm, have comorbidities or are frail. These were the people who were particularly at risk, and the main target group that should have been addressed. In his view, this was also the most important and obvious reason why there were alternatives to social closures and other coercive state measures.
In addition, it was clear from quite early on that it were the people with serious comorbidities that would fall seriously ill. In one of Europe’s epicentres of the early outbreak, Italy, a report found as early as in March 20, 2020, that the median age of the 3200 deaths testing positive for Covid-19 was 78.5 years, and more than 95% of them had one or more comorbidities. A large-scale study in the US confirmed that over 95% of hospitalised adults were persons with at least one comorbidity condition and the main risks were obesity, anxiety and fear disorders and diabetes. However, it was also clear, for example, that the proportion of overweight people varied widely between countries, even within the same age groups. For example, obesity already affects 42% of the US population, but in Vietnam the same number is only 2%, in India 4% and <10% in most of the African countries.
The association of nutritional deficiencies with severe morbidity was also known before the Covid crisis. Vitamin D, for example, plays an important role in the immune system. Already in the first half and second half of 2020, studies showed a clear correlation between the low levels of vitamin D and the risk of severe Covid-19 disease. For that reason, many doctors and researchers stressed the need for adequate vitamin D intake in the autumn of 2020, ahead of the second wave, especially for older people at risk.
Although these facts were known early on, authoroties continued to scare the public by claiming, among other things, that the virus did not discriminate between infected people and could be fatal to anyone. Health authorities also failed to advise people to take important steps to support their general health, such as getting enough fresh air and sunshine, eating a healthy diet, controlling blood pressure and diabetes, losing weight, etc. On the contrary, authorities directed people indoors, in many countries penalised them for going outdoors, and just promoted vaccinations instead of various treatments and lifestyles.

In the UK, scary posters were used in large-scale campaigns to get people to follow the “rules”
Ignoring natural immunity
The importance of natural immunity was systematically downplayed by the health authorities, major vaccine manufacturers and the World Health Organisation (WHO). In some countries (such as the USA), it was not even taken into account in the implementation of Covid measures, while the authorities only reiterated the need to vaccinate as many people as possible.
At the same time, studies carried out before the vaccination campaigns started, i.e. by the end of 2020, clearly showed that recovery from the disease provides strong immunity for at least 8 months and most likely longer. By October 2021, at least 81 studies had already been published confirming immunity to Covid-19 conferred by recovery.
In addition, a number of studies at the beginning of the Covid crisis showed that a significant proportion of the population may have already had immunity to Covid-19, as SARS-Cov-2 was only one of several coronaviruses. Nearly half of the unaffected individuals had the corresponding T-cells, indicating the body’s previous exposure to coronaviruses and ability to cope with them.
Many doctors and scientists, including Dr. Robert W. Malone, Dr. Peter McCullough, Dr. Geert Vanden Bossche, Dr Marty Makary, Dr. Pierre Kory, Dr. Tess Lawrie, Dr. Richard Urso, Dr. Paul E. Alexander, Prof Norman Fenton, Prof Martin Neil and others found it puzzling that health officials chose to ignore the scientific fact that infection provided long-lasting and strong protection to millions of people who had recovered from Covid-19. Prof. Jayanta Bhattacharya and Prof. Martin Kulldorff have stressed that while natural infection may not have provided permanent infection-blocking immunity, it offered, in high likelihood, permanent anti-disease immunity against severe disease and death. However, scientists who during the Covid crisis stressed the importance of natural immunity and asked to take into account when divising public policies, were not only ignored but censored and cancelled.
Ignoring natural immunity has had serious consequences, including avoidable vaccine complications and harms, loss of lives, financial and other collateral damage, and loss of credibility of the public health authorities.
Vaccines were not tested for reduction of virus transmission or infection
Covid-19 vaccines, which were introduced at warp speed, were not tested in clinical trials to see if they reduced infection or transmission. Shortly before their vaccine was granted emergency marketing authorisation in the US (on 3 December 2020), this fact was admitted by the CEO of Pfizer, Albert Bourla, and later by a Pfizer official during an official hearing at the European Parliament, although the vaccine manufacturers gave the public an impression that the vaccines protected against infection and transmission.
To the experts who looked closely at the design and results of the Covid-19 vaccine clinical trials, the fact that the vaccines were not tested for reduction of virus transmission or infection was evident already in late 2020. For example, the editor of British Medical Journal (BMJ) Dr. Peter Doshi stated on October 21, 2020, that none of the vaccine clinical trials had been designed to detect the efficacy of these vaccines on reducing any serious outcomes such as hospital admissions, use of intensive care, or deaths. Neither did they examine the efficacy of vaccines for their ability to interrupt transmission of the virus.

Dr Peter Doshi considers it wrong that primary data from clinical trials are not available (screenshot from Youtube)
Prof. William A. Haseltine drew attention to the serious shortcomings of these clinical trials on 23 September 2020, after Pfizer, Moderna, AstraZeneca and Johnson & Johnson had published their vaccine trial protocols. According to him, the trials seemed to be designed to prove that their vaccines worked, even if the measured effects were minimal, as they mainly investigated only how well could the vaccines prevent mild Covid-19 symptoms. Haseltine pointed out that a closer look at the protocols made it clear that these trials did not provide confidence in vaccine efficacy in protecting against serious illness or in preventing an infection of Covid-19. It also appeared that these trials were intended to pass the lowest possible barrier of success. Haseltine concluded that these vaccines were not the “silver bullet” that would end the Covid crisis.
Yet tens of millions of people around the world were subjected to compulsory vaccination, and many lost their jobs because of non-compliance, severely restricting their individual freedoms and fundamental rights.
Ignoring the side effects of the vaccines
Data on the side effects of the vaccines were already available in documents published by the vaccine manufacturers on their clinical trails in late 2020, although few were able to or considered it important to look at them in depth. This was made considerably more difficult by the fact that vaccine manufacturers refused to publish the raw data needed for an objective assessment. Raw data from clinical trials have still not been fully disclosed.
For example, the Pfizer vaccine trial was designed, conducted, analysed and compiled by Pfizer staff and all the raw data belong to the company. The BMJ editorial board believes that refusing to disclose the original data is morally unacceptable for any clinical trials, but especially those involving major public health interventions. The BMJ has been calling on vaccine manufacturers for years to disclose the original data from clinical trials, since clinical trial data must be available for independent scrutiny.
Nevertheless, experts pointed out many inconsistencies and questionable findings in the Covid-19 vaccine trial reports already in early 2021, such as the facts that:
- higher-risk target groups (elderly and immuno-compromised individuals) were clearly under-represented in the trials,
- a number of subjects were withdrawn for unknown reasons,
- even the officially reported rate of adverse reactions was several times higher than it was, for example, for flu vaccines.
In addition, it has come to light that the vaccine manufacturer Pfizer was aware of several serious side effects amongst the vaccine participants in clinical trials in early 2021, but chose to conceal them, such as the case of 12-year-old Maddie De Garay, who became disabled in the trial and is now partially paralysed, requiring a wheelchair and feeding tube. None of her 35 adverse reactions were mentioned in the New England Journal of Medicine article reporting on the vaccine trial.
Regardless of all that, since the beginning of 2021, mass vaccination campaigns were launched in many countries of the world, which in a short period of time transformed from an attempt of vaccinating the vulnerable target groups (the elderly) into an increasingly massive effort to vaccinate as many people as possible, even up to with children and infants, providing no rational argument or evidence base to do so.
A new expert analysis of the Pfizer and Moderna vaccine trial papers published in 2022 clearly found that participants in these clinical trials were more likely to experience a serious adverse reaction to vaccination than to be hospitalized for Covid-19.
Summary
As shown above, there is ample reason to argue that the evidence base for the decisions made in the greatest global health crisis of recent decades was severely deficient. Covid measures were determined not on the basis of evidence nor reasonable assumptions, but rather on the basis of emotional reactions and political tactics, fuelled by fear and media pressure. Societies were under constant pressure from global organisations (WHO, European Commission, etc.), authorities and the mass media – which included the increasingly loud rhetoric of maximizing lockdown, maximizing masking, maximizing vaccination etc.
However, there were also those in power who relied on knowledgeable experts (e.g. in the US, states such as South Dakota, Florida, Texas, etc.), as did some who were in charge of public health institutions (for example in Sweden), succeeding to resist irrational and unscientific pressures while enduring media bashing, vilification and unpopularity. At said places, the decision-makers generally avoided locking down the society and did not impose coercive state measures (compulsory mask mandates, compulsory vaccination, etc.). Thanks to their non-conformist and common sense approach, we now know much about which measures worked and which didn’t, the mistakes every society should avoid in future health crises, and how the slogan of ‘follow the science’ was often used as propaganda to subjugate societies to the dictates of a line of authority.
Cost of Living Crisis to Cause ‘Thousands of Extra Deaths’ in UK – Report
By Chimauchem Nwosu – Sputnik – 27.09.2023
 Some UK military personnel and their families have been turning to food banks because of the increasing pressures from the cost of living crisis, a British news network has reported.
Some UK military personnel and their families have been turning to food banks because of the increasing pressures from the cost of living crisis, a British news network has reported.
The raging cost of living crisis that has had the UK in its stifling grasp is going to cause thousands of extra deaths this year, according to new research, as life expectancy across the UK will plummet by 6.5 percent this year.
The research suggests that untimely mortalities in the United Kingdom are expected to rise from 463 to 493 per 100,000 inhabitants.
The findings have shone a light on critical concern for the populace at large. The unrelenting cost-of-living crisis, combined with a prolonged period of soaring prices, is anticipated to result in a significant 6.5 percent drop in life expectancy throughout the nation this year.
Furthermore, the report highlights a stark disparity: the most economically disadvantaged households are projected to face a four times higher death toll than their wealthier neighbours. This discrepancy arises from the fact that the less affluent must allocate a more significant portion of their income to pay for energy, the cost of which has rocketed.
Recent statistics from the previous month indicate that the UK’s inflation rate stood at 6.7 percent. Despite this reduction from its peak of 11.1 percent, Britain continues to have the worst inflation of all G7 member states.
“The mortality effects of inflation and real-terms income reduction are likely to be large and negative, with marked inequalities in how these are experienced. Implemented public policy responses are not sufficient to protect health and prevent widening inequalities,” researchers noted.
These findings come on the heels of a recent alert from the UK-based consumer association ‘Which’ last month, when it pointed out that rising food prices had left low-income households in the country in dire straits and having to make painful decisions about whether to pay the utility bills or put food on the table.
Swiss Immunologist’s Request: “Entire mRNA ‘Vaccine’ Platform Must Be Banned”
The long sinister shadow of the mRNA induced spike protein
By P Gosselin | No Tricks Zone | September 27, 2023
Dr. Thomas Binder wrote a letter to the editor of the Swiss Medical Journal in the response to an interview of Prof Christoph Berger and President of the Federal Commission for Vaccination Issues #EKIF, explaining why the entire mRNA ‘vaccine’ platform must be banned.
Dr. Thomas Binder. Image cropped here.
Firstly, Binder writes, “The effective dose of the expressed foreign protein is unknown and varies greatly between individuals, mRNA ‘vaccines’ should never have been approved.”
Secondly, “The cells that express the protein foreign to the body and then present it on their surface are falsely recognized by the immune system as being foreign or infected by an alien, thus are destroyed in an autoimmune attack similar to transplant rejection.”
He continues: “If it was only expressed by skeletal muscle cells capable of regeneration, this would not be problematic. But the LNPs [lipid nanoparticles] are chosen in such a way that they introduce the mRNA into any body cell, including those of the heart, brain, embryo and fetus. Worse: As physiological doses did not induce a relevant immune response, a horrendous dose of mRNA was chosen, which can lead to the destruction not only of a few, but of so many cells that this can cause serious illness and death. Worse: The chosen antigen and LNPs are themselves toxic.”
He notes: “Kevin McKernan found contamination with up to a third of functional bacterial plasmid DNA from the manufacturing process, which explains the spike expression over years detected by pathologists.” Finally, it has not been ruled out yet that the DNA can be integrated into the genome and even be inherited by offspring.”
Read entire letter here.
Featured Video
Laith Marouf: Hezbollah’s position on US-Iran ceasefire
or go to
Aletho News Archives – Video-Images
From the Archives
The Dirty Little Secret behind the “Global Terrorism Index”
The Omission of Israeli Terrorism in the Occupied Palestinian Territories
By Karin Brothers | Global Research | December 6, 2014
… The Israeli settlements — all of which are illegal – have been identified as a major impediment to peace. The refusal of a major “global” terrorism report to name the Israeli settlers as one of the groups most responsible for terrorism not only misrepresents a major source of regional violence but exposes the Global Terrorism Index as a propaganda tool that supports a U.S. agenda.
In recent years, governments have been attempting to thwart terrorism by blocking supportive fund-raising. When it comes to Israeli settlements, however, the US and Canada actually encourage fund-raising by giving organizations (such as Christian Friends of Israeli Communities (CFOIC) and the Jewish National Fund) financial support in the form of donor tax-deductions.
Charities which provide funds for the Israeli settlements should be regarded as terror-financing organizations. They should not only lose their tax-deductible status, but they should be banned because they support the violation of international humanitarian law. The terror-financing laws that are being strictly enforced for Muslim charities should be applied to Christian and Jewish charities as well. … Read full article
Blog Roll
 Aletho News
Aletho News- Trump Administration Moves To Automate U.S. Military Draft Registration
- Spain orders reopening of Tehran embassy, condemns Israel’s carpet bombing of Lebanon
- Israel faces ‘unsustainable’ strategic crisis following 40-day war against Iran: Analyst
- Iran restricts Hormuz access to 15 vessels per day under ceasefire terms: Report
- The ‘Opposition Party’ Has Done Nothing to Stop the Iran War and Much to Goad Trump Into Continuing It
- Moscow backs Tehran on status of Lebanon in US-Iran deal
- How UK Regulator Ofcom Quietly Bypassed International Law to Police American Speech
- The Black Cube Files: How Former Mossad Operatives Flipped a Nation
- Laith Marouf: Hezbollah’s position on US-Iran ceasefire: What you’re not being told
- Israel’s priority lies in destroying chances of peace between Iran, US: Ex-UN nuclear chief
- If Americans Knew
- Amnesty: Urgent – Protect Lebanese civilians from brutal escalation in Israeli attacks
- Is The War Against Iran Over?
- Inside the Israeli army’s propaganda wing
- Hundreds of Gaza Amputees Stranded in Legal Limbo
- The gallows law: Israel moves toward executing Palestinian children
- Tucker Carlson: The Path to Peace requires ending ‘special alliance’ with Israel
- This is ceasefire? Israel’s biggest massacre yet in Lebanon, another journalist killed in Gaza – Daily Update
- Tucker Carlson on Israel: This Is the Behavior of an Ally? Really?
- Gazans face a triple crisis: severe shortages of water and bread, healthcare in tatters
- NY Times reports how Netanyahu took the US into Iran War
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
