What’s Really Happening with Mpox
The Mpox Emergency
By David Bell | Brownstone Institute | August 18, 2024
The World Health Organization (WHO) acted as expected this week and declared Mpox a Public Health Emergency of International Concern (PHEIC). So, a problem in a small number of African countries that has killed about the same number of people this year as die every four hours from tuberculosis has come to dominate international headlines. This is raising a lot of angst from some circles against the WHO.
While angst is warranted, it is mostly misdirected. The WHO and the IHR emergency committee they convened had little real power – they are simply following a script written by their sponsors. The African CDC, which declared an emergency a day earlier, is in a similar position. Mpox is a real disease and needs local and proportionate solutions. But the problem it is highlighting is much bigger than Mpox or the WHO, and understanding this is essential if we are to fix it.
Mpox, previously called Monkeypox, is caused by a virus thought to normally infect African rodents such as rats and squirrels. It fairly frequently passes to, and between, humans. In humans, its effects range from very mild illness to fever and muscle pains to severe illness with its characteristic skin rash, and sometimes death. Different variants, called ‘clades,’ produce slightly different symptoms. It is passed by close body contact including sexual activity, and the WHO declared a PHEIC two years ago for a clade that was mostly passed by men having sex with men.
The current outbreaks involve sexual transmission but also other close contact such as within households, expanding its potential for harm. Children are affected and suffer the most severe outcomes, perhaps due to issues of lower prior immunity and the effects of malnutrition and other illnesses.
Reality in DRC
The current PHEIC was mainly precipitated by the ongoing outbreak in the Democratic Republic of Congo (DRC), though there are known outbreaks in nearby countries covering a number of clades. About 500 people have died from Mpox in DRC this year, over 80% of them under 15 years of age. In that same period, about 40,000 people in DRC, mostly children under 5 years, died from malaria. The malaria deaths were mainly due to lack of access to very basic commodities like diagnostic tests, antimalarial drugs, and insecticidal bed nets, as malaria control is chronically underfunded globally. Malaria is nearly always preventable or treatable if sufficiently resourced.
During this same period in which 500 people died from Mpox in DRC, hundreds of thousands also died in DRC and surrounding African countries from tuberculosis, HIV/AIDS, and the impacts of malnutrition and unsafe water. Tuberculosis alone kills about 1.3 million people globally each year, which is a rate about 1,500 times higher than Mpox in 2024.
The population of DRC is also facing increasing instability characterized by mass rape and massacres, in part due to a scramble by warlords to service the appetite of richer countries for the components of batteries. These in turn are needed to support the Green Agenda of Europe and North America. This is the context in which the people of DRC and nearby populations, which obviously should be the primary decision-makers regarding the Mpox outbreak, currently live.
An Industry Produces What It Is Paid for
For the WHO and the international public health industry, Mpox presents a very different picture. They now work for a pandemic industrial complex, built by private and political interests on the ashes of international public health. Forty years ago, Mpox would have been viewed in context, proportional to the diseases that are shortening overall life expectancy and the poverty and civil disorder that allows them to continue. The media would barely have mentioned the disease, as they were basing much of their coverage on impact and attempting to offer independent analysis.
Now the public health industry is dependent on emergencies. They have spent the past 20 years building agencies such as CEPI, inaugurated at the 2017 World Economic Forum meeting and solely focused on developing vaccines for pandemic, and on expanding capacity to detect and distinguish ever more viruses and variants. This is supported by the recently passed amendments to the International Health Regulations (IHR).
While improving nutrition, sanitation, and living conditions provided the path to longer lifespans in Western countries, such measures sit poorly with a colonial approach to world affairs in which the wealth and dominance of some countries are seen as being dependent on the continued poverty of others. This requires a paradigm in which decision-making is in the hands of distant bureaucratic and corporate masters. Public health has an unfortunate history of supporting this, with restriction of local decision-making and the pushing of commodities as key interventions.
Thus, we now have thousands of public health functionaries, from the WHO to research institutes to non-government organizations, commercial companies, and private foundations, primarily dedicated to finding targets for Pharma, purloining public funding, and then developing and selling the cure. The entire newly minted pandemic agenda, demonstrated successfully through the Covid-19 response, is based on this approach. Justification for the salaries involved requires detection of outbreaks, an exaggeration of their likely impact, and the institution of a commodity-heavy and usually vaccine-based response.
The sponsors of this entire process – countries with large Pharma industries, Pharma investors, and Pharma companies themselves – have established power through media and political sponsorship to ensure the approach works. Evidence of the intent of the model and the harms it is wreaking can be effectively hidden from public view by a subservient media and publishing industry. But in DRC, people who have long suffered the exploitation of war and the mineral extractors, who replaced a particularly brutal colonial regime, must now also deal with the wealth extractors of Pharma.
Dealing with the Cause
While Mpox is concentrated in Africa, the effects of corrupted public health are global. Bird flu will likely follow the same course as Mpox in the near future. The army of researchers paid to find more outbreaks will do so. While the risk from pandemics is not significantly different than decades ago, there is an industry dependent on making you think otherwise.
As the Covid-19 playbook showed, this is about money and power on a scale only matched by similar fascist regimes of the past. Current efforts across Western countries to denigrate the concept of free speech, to criminalize dissent, and to institute health passports to control movement are not new and are in no way disconnected from the inevitability of the WHO declaring the Mpox PHEIC. We are not in the world we knew twenty years ago.
Poverty and the external forces that benefit from war, and the diseases these enable, will continue to hammer the people of DRC. If a mass vaccination campaign is instituted, which is highly likely, financial and human resources will be diverted from far greater threats. This is why decision-making must now be centralized far from the communities affected. Local priorities will never match those that expansion of the pandemic industry depends on.
In the West, we must move on from blaming the WHO and address the reality unfolding around us. Censorship is being promoted by journalists, courts are serving political agendas, and the very concept of nationhood, on which democracy depends, is being demonized. A fascist agenda is openly promoted by corporate clubs such as the World Economic Forum and echoed by the international institutions set up after the Second World War specifically to oppose it. If we cannot see this and if we do not refuse to participate, then we will have only ourselves to blame. We are voting for these governments and accepting obvious fraud, and we can choose not to do so.
For the people of DRC, children will continue to tragically die from Mpox, from malaria, and from all the diseases that ensure return on investment for distant companies making pharmaceuticals and batteries. They can ignore the pleading of the servants of the White Men of Davos who will wish to inject them, but they cannot ignore their poverty or the disinterest in their opinions. As with Covid-19, they will now become poorer because Google, the Guardian, and the WHO were bought a long time back, and now serve others.
The one real hope is that we ignore lies and empty pronouncements, refusing to bow to unfounded fear. In public health and in society, censorship protects falsehoods and dictates reflect greed for power. Once we refuse to accept either, we can begin to address the problems at the WHO and the inequity it is promoting. Until that time, we will live in this increasingly vicious circus.
David Bell, Senior Scholar at Brownstone Institute, is a public health physician and biotech consultant in global health. He is a former medical officer and scientist at the World Health Organization (WHO), Programme Head for malaria and febrile diseases at the Foundation for Innovative New Diagnostics (FIND) in Geneva, Switzerland, and Director of Global Health Technologies at Intellectual Ventures Global Good Fund in Bellevue, WA, USA.
Mpox Vaccine Maker’s Stock Price Soars After WHO Declares Global Public Health Emergency
By Brenda Baletti, Ph.D. | The Defender | August 15, 2024
Stock prices for mpox vaccine maker Bavarian Nordic surged after the World Health Organization (WHO) on Thursday declared mpox a global public health emergency.
The company’s share prices jumped 17% in early trading in Copenhagen today, Forbes reported, after climbing 12% yesterday when the WHO made its announcement. In the U.S., shares were up 33% this morning.
The WHO cited recent outbreaks in the Democratic Republic of Congo (DRC) and neighboring nations in its declaration.
In the first known infection of its kind outside Africa, Sweden today confirmed a case of the highly contagious strain of mpox, according to NBC News. The WHO’s European regional office in Copenhagen said it was discussing with Sweden how best to manage the newly detected case, according to Medical Xpress.
This is the second time in two years the WHO has declared mpox a “public health emergency of international concern” PHEIC — pronounced “fake” — which is its highest form of an alert.
The announcement follows a declaration Tuesday by the Africa Centres for Disease Control and Prevention that mpox is a continent-wide public health emergency.
Last week, the WHO triggered the process to grant Emergency Use Listing to two mpox vaccines, although it didn’t name which ones it would list. The agency also invited manufacturers of mpox vaccines to submit an “expression of interest” for Emergency Use Listing.
The DRC, where the outbreak is concentrated and most severe, has approved two vaccines — Japan’s LC16 and Bavarian Nordic’s Jynneos, which is also marketed as Imvamune and Imvanex.
Bavarian Nordic is one of the few companies in the world with an already-approved mpox vaccine that is also available in large quantities. Other contenders, such as Emergent BioSolutions’ ACAM2000 have been available under special investigational protocols. Others, like Tonix Pharmaceuticals, have experimental shots that are in earlier stages of development.
LC16 is a smallpox vaccine licensed in 1980 in Japan and approved in July 2022 for mpox. It isn’t commercially available, but there are large supplies in Japan’s national stockpile, the Center for Infectious Disease Research and Policy reported. Like Jynneos, it is a third-generation mpox vaccine that uses attenuated virus strains.
Jynneos and ACAM2000 can cause myocarditis, pericarditis and other serious side effects at high rates, Dr. Meryl Nass told The Defender last week, as the labels for both drugs indicate.
The Japanese LC16 vaccine also has been linked to encephalitis, Nass reported on her Substack today.
“The WHO is using the monkeypox outbreak in Africa to fast-track, under emergency use, two monkeypox vaccines,” Dr. Kat Lindley, a senior fellow at FLCCC Family Medicine and president of the Global Health Project told The Defender.
“We need to use discernment and evaluate risks and benefits before recommending any experimental new product to a vulnerable population,” she said.
The African CDC in a LinkedIn post said it needed 10 million doses to control the outbreak and called for global support for its vaccination efforts.
Bavarian Nordic’s CEO Paul Chaplin told Bloomberg the company can provide 10 million doses of its vaccine to African countries over the next year and a half.
In an interview Wednesday — before today’s stock price surge — Chaplin said, “We have inventory and we have the capabilities. What we’re missing are the orders.”
In May 2022, the WHO announced it would phase out the name “monkeypox” and rename the disease “mpox” to avoid the stigma generated by associating the disease with monkeys.
WHO process for issuing PHEIC declarations ‘non-transparent and contradictory’
WHO Director-General Tedros Adhanom Ghebreyesus said in his press announcement that the agency decided to declare a PHEIC because:
“The detection and rapid spread of a new clade of mpox in eastern DRC [Democratic Republic of Congo], its detection in neighboring countries that had not previously reported mpox, and the potential for further spread within Africa and beyond is very worrying.”
The WHO declaration signals a public health risk requiring an international coordinated response. It can lead to WHO member countries and private investors pouring substantial resources into countries with outbreaks to facilitate sharing of vaccines, treatments and testing.
The declaration also grants the WHO authority to issue travel warnings or restrictions, to review and critique the validity of public health measures by member countries and to help persuade people that they ought to follow public health recommendations.
This is the eighth public health emergency the WHO has declared since 2007, when it substantially revised its International Health Regulations (IHR). Critics have called the process for designating such an emergency “non-transparent and contradictory.”
In July 2022, the WHO declared mpox a global emergency after reporting the disease had spread to more than 70 countries, mostly affecting gay and bisexual men. At the time, Tedros made the declaration unilaterally, in direct contradiction to independent review panel advice.
At that time, the Jynneos vaccine was licensed in the U.S. and ACAM2000 was “made available for use against mpox in the current outbreak [2022] under an Expanded Access Investigational New Drug (EA-IND) protocol.” Jynneos received emergency use authorization in the U.S. for children under 18 considered to be at high risk.
Although in the U.S. monkeypox has appeared to be a mild illness, several lucrative government contracts in 2022 paid the vaccine makers hundreds of millions to stockpile the vaccines.
The 2022 outbreak reportedly affected nearly 100,000 people, primarily gay and bisexual men, in 116 countries and about 200 people died.
Despite media hype and hundreds of millions of dollars spent to stockpile mpox vaccines in the U.S., the designation was quietly withdrawn in May 2023, “given the sustained decline in cases.”
On Aug. 8, the Biomedical Advanced Research and Development Authority renewed its contract with Bavarian Nordic, committing $156.8 million to manufacture and store Jynneos doses to partly replenish the inventory used to manufacture vaccines in response to the mpox outbreak in 2022.
Critics suggest ‘common sense mitigation measures’
Mpox was first detected in humans in 1970 in the DRC, according to the WHO, and is considered endemic to countries in central and west Africa, with the number of cases rising and falling periodically.
The disease causes flu-like symptoms and pus-filled lesions. It is usually mild but can be serious, particularly in people with weakened immune systems, Reuters reported.
In its announcement Wednesday, the WHO said the DRC is experiencing a severe outbreak of mpox, with 15,600 cases and 537 deaths. It said the current outbreak is caused by a virus strain, or “clade” — clade 1b — that is more severe than clade 2, which was responsible for the global outbreak in 2022.
It “appears to be spreading mainly through sexual networks,” and it has been detected in neighboring countries of Burundi, Kenya, Rwanda and Uganda, with 100 “laboratory-confirmed cases of clade 1b” in total in those countries.
Lindley said health officials are most likely using PCR tests, which were shown during the COVID-19 pandemic to generate false positive results.
“We really have no idea,” she said, if the alleged deaths are “complications of people who have depressed immune systems and are dying of other things.”
“Why would we start mass vaccination with a new product for which we know nothing about the safety profile when common sense mitigation measures can work?” she asked. “If it is sexually transmitted, use a condom or abstain from sex. If it can be transmitted through secretions, wash your hands and don’t touch people with clinical presentation.”
Nass expressed similar skepticism on her Substack:
“If this generally mild viral illness is killing people, what is the cause of death? Does it only cause death in severely immune suppressed patients? Are babies dying due to dehydration? Do we need to treat babies with fluids rather than give them a vaccine that was never tested in babies? Lots of unanswered questions.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
The UN Smothers the Peoples with Compassion
By Thi Thuy Van Dinh and David Bell | Brownstone Institute | June 27, 2024
“We The Peoples of the United Nations determined (…) to promote social progress and better standards of life in larger freedom,”
United Nations Charter Preamble (1945)
The United Nations (UN) Secretariat will hold the next Summit of the Future in New York on 22-23 September 2024. It is a vast political program covering the noblest of causes including poverty reduction, human rights, environment, climate change, development, and the welfare and rights of children, youth, and women. World leaders are expected to endorse a declaratory Pact for the Future, and commit to act toward its realization.
It all looks wonderful. As in days of old, the rich, powerful, and entitled are coming to rescue us from ourselves and make us live better lives. Freedom, after all, is intrinsically unsafe.
This is the first in a series that will look at the plans of the UN system designing and implementing this new agenda, covering implications for global health, economic development, and human rights.
Amidst all the hype and posturing regarding the negotiations on pandemic texts at the recent 77th World Health Assembly (WHA) in Geneva (Switzerland), perhaps the most consequential resolution before the WHA slipped through, approved, but virtually unnoticed. The Resolution WHA77.14 on Climate Change and Health was approved without debate, opening the door for the World Health Organization (WHO) ─ a UN specialized agency ─ to claim a broad swath of normal human activity as a potential threat to health, and therefore coming under the purview of the WHO’s detached business-class bureaucrats.
It was highlighted by a Strategic Roundtable on “Climate change and health: a global vision for joint action,” where speakers, moderated by the Lancet’s Editor-in-Chief Richard Horton, included WHO Director-General (DG) Tedros Ghebreyesus, former US Vice President Al Gore (by video message), and CEO of the 28th Climate Conference of States Parties Adnan Amin.
The Resolution was proposed by a coalition of 16 countries (Barbados, Brazil, Chile, Ecuador, Fiji, Georgia, Kenya, Moldova, Monaco, Netherlands, Panama, Peru, Philippines, Slovenia, United Arab Emirates, and the UK) and passed without changes, mandating the DG to: i) develop a “results-based, needs-oriented and capabilities-driven global WHO plan of action on climate change and health,” ii) serve as a global leader in the field of climate change and health by establishing a WHO Roadmap to Net Zero by 2030, and iii) report back to future WHA sessions.
United Nations System’s “Newspeak” on Climate Change
There is little surprise in this. It is another predictable move on the global climate chessboard. In the last decade, activities and documents from the UN system have increasingly included climate change as a “newspeak” to signal full compliance with the official narrative.
The head of the UN system, Secretary-General Antonio Guterres, is known for pushing the narrative further. In 2019, he posed in water for a picture for Time Magazine’s coverage on “Our sinking planet.” Last summer, he announced that “the era of global warming has ended…the era of global boiling has arrived.”
On 2024 World Environment Day (5th June), he doubled down on his rhetoric: “In the case of climate, we are not the dinosaurs. We are the meteor. We are not only in danger. We are the danger.” We are, it appears, a poison on our planet.
Satellite entities have wildly added their creativity and imagination: UNEP hammering on the “triple planetary crisis of climate change, nature and biodiversity loss,” UNICEF reporting on the “climate changed-child,” UNWOMEN discovering the “interconnection between climate change and gender inequality,” OHCHR claiming that “climate change threatens the effective enjoyment of a range of human rights including those to life, water and sanitation, food, health, housing, self-determination, culture and development,” and UNESCO fully committed “to addressing the impact of climate change on culture, and to enhancing the potential of culture for global climate action.”
Nomination of First Ever WHO Special Envoy for Climate Change and Health
As for WHO, DG Tedros Ghebreyesus has also demonstrated his mastery of dogmatic claims. Climate change, he insists, constitutes “one of the biggest health threats” and “the climate crisis is a health crisis.” His mandate has therefore been broadened from specific environmental issues including air pollution from particulates and chemicals to the whole climate change spectrum. In 2023, the WHO estimated that “between 2030 and 2050, climate change is expected to cause approximately 250,000 additional deaths per year, from undernutrition, malaria, diarrhoea and heat stress alone.”
Strangely, however, deaths attributable to cold weather, estimated at 4.6 million globally per year, were not weighed in balance. Nor are inevitable deaths from undernutrition related to a lack of accessible energy for agriculture and transport. Accounting for a reduction in such deaths would significantly reduce projected mortality and perhaps demonstrate an overall advantage. For instance, rising CO2 has increased plant growth and contributed to the world’s ability to feed 8 billion people, an achievement once considered impossible and is obviously highly critical to maintaining health.
The WHO’s leaders have become bolder. In June 2023, in a minor lapse of equity, inclusion, and transparency criteria, the DG appointed Dr Vanessa Kerry as “the first ever” Special Envoy for Climate Change and Health for being “a renowned global health expert and medical doctor and CEO of Seed Global Health.” The press release overlooked any connection with her father, former US Secretary of State John Kerry ─ a key US Democratic politician, well-known personality at UN climate forums, and first-ever US Presidential Envoy for Climate (January 2021-March 2024). Her nomination, apparently, was purely meritocratic.
It is estimated that $27.6 million is required to create the reports implementing the 2024 Resolution. Now, $20 million will come from WHO’s biennial 2024-25 budget, and the gap of $7.6 million will be raised through WHO’s continued “discussions with Member States, development agencies and philanthropic organizations.” People who will, perhaps, benefit from the WHO pushing the products they have invested in, such as heavily processed substitutes to (climate-harming) natural foods.
Misleading Resolution WHA77.14 on the “Link between Health, Environment and Climate Change”
All of this appears to follow conventional political and diplomatic playbooks. It comes unstuck if one applies a critical look at how Resolution WHA77.14 was built.
It referred to Resolution WHA61.19 (adopted in 2008) on climate change and health, Resolution WHA68.8 (adopted in 2005) addressing the health impact of air pollution, and Resolution WHA76.17 (adopted in 2023) on the impact of chemicals, waste, and pollution on human health as follows.
Recalling resolution WHA61.19 (2008) on climate change and health and welcoming the work carried out so far by WHO in pursuit of it;
Recalling also resolution WHA68.8 (2015) on addressing the health impact of air pollution and resolution WHA76.17 (2023) on the impact of chemicals, waste and pollution on human health, which recognize the link between health, environment and climate change;
Resolution WHA61.19 was adopted based on a WHO report “Climate change and health.” This report stated that “There is now a strong, global scientific consensus that warming of the climate system is unequivocal, and is caused by human activity, primarily the burning of fossil fuels which releases greenhouse gases into the atmosphere” (para. 1) and that “WHO has, for several years, stressed that the health risks posed by climate change are significant, distributed throughout the globe, and difficult to reverse” (para. 2). These affirmations were made without assessment of levels of evidence (strong, moderate, weak), of the extent to which (modifiable) human activity is involved, or of the actual positive versus negative impacts of higher temperatures (and atmospheric CO2).
Contrary to the statements by Resolution WHA77.14, neither Resolution WHA68.8 nor Resolution WHA76.17 mentioned climate change in the context of pollutants. Excluding rare natural phenomena, particulate and chemical air pollution do result from human activities, including indoor air pollution (e.g. cookstoves) and transport and industrial waste. Hence, these past Resolutions recognized a link between these pollutants and human health, which is common sense. They did not recognize a link between health, environment, and climate change.
Nevertheless, we can probably relax and wait. The WHO’s upcoming reports can be expected to claim a link. They have $27 million to spend on that.
The Climate Agenda Versus “We the Peoples”
It is easy for wealthy self-proclaimed philanthropists and international and governmental bureaucrats to call for phasing out fossil fuels. Living on tax-paid salaries in secure jobs, in economies made rich through the availability of cheap energy, they are able to renew their commitment annually at the Conference of States Parties (COP) to the UN Framework Convention on Climate Change, ignoring the reality that their very ability to be there is due to fossil fuels. The most recent venues ─ Dubai, Sharm-El-Sheik, and Glasgow ─ all built their prosperity on this same energy base.
Being obsessed with the man-made climate narrative, the UN system pushes poor countries to adopt green energies for lighting and cooking, rather than developing the large-scale energy infrastructure that still forms the backbone of wealthier societies.
There seems to be no shame vis-a-vis 2.3 billion people on earth that, according to the WHO, must still rely on dirty and dangerous cooking fuels such as cow dung, charcoal, and wood ─ negatively impacting women and children’s health through particulate air pollution. Increasing the cost of fossil fuels directly increases further deforestation and resultant desertification (and regional climate change) in areas such as East Africa. It feels good, apparently, for the activists of climate COPs and Extinction Rebellion to force African women to walk further each day for firewood, denuding landscapes and their meager savings.
There seems to be no shame either when Western bilateral and multilateral largesse to low-income countries comes on the condition that they pass a “climate check,” or must be spent on developing “green” but unreliable solar and wind generation which barely supplement the base energy supplies of most donor countries. We happily burn Nigerian oil, but our virtue requires Nigerians to do better. After looting wealth through colonialism, this is rubbing noses in the dirt of the poverty left behind.
One can confidently predict that the rhetoric will continue, and more “soft laws” ─ UN declarations, strategies, plans-of-action, and agendas ─ will complement the existing “hard laws” of the UN Framework Convention on Climate Change and its Protocols. At the WHO, more funding will come to extend the growing industry of climate change and health, diverting financial and human resources from far greater, but less boutique, health burdens.
A plan of action will be put before a future WHA to agree to a binding document seeking to harden the 2024 Resolution into requirements. Highly questionable assumptions that pandemics and malaria, and even tuberculosis, are worsened because of climate change will be drawn to support the global plan, complementing the coming Pandemic Agreement and the massive surveillance system set up by the freshly adopted IHR Amendments to ensure pandemic lockdowns.
Malaria, tuberculosis, and diseases of undernutrition and poor hygiene are primarily diseases of poverty. People in wealthy countries live longer primarily because of improvements in sanitation, living conditions, and nutrition. These improvements were achieved by using energy for transport, to build infrastructure, and to massively improve the efficiency of agricultural production. Locking future generations in low-income countries into poverty will not improve their health and well-being.
This increasingly charade-like global health circus will, in the end, destabilize the world and harm us all. To address complex issues, the world needs rational and honest debates, rather than games played by a self-entitled few. The WHO is demonstrating that it is no longer the organization to lead us to better health. It is on us to regain control of our own future.
Can the WHO and the United Nations impose sanctions on your sovereign country for non-compliance?
The UN is a far bigger threat than the WHO, which, although deserving of attention, cannot consume our entire focus.
BY SHABNAM PALESA MOHAMED | JUNE 18, 2024
This updated analysis was written in 2023 (read in full here at CHD Africa)
Sanctions are a powerful instrument of political control and economic profit. One of the rare but critical topics relevant to the international campaign to #ExitTheWHO is whether the World Health Organisation and the United Nations can impose, influence or recommend specific sanctions. The sanctions could be implemented against countries that choose to not comply or cannot comply with International Health Regulations, the proposed new pandemic treaty, or other legislative attempts that curtail rights, freedom and sovereignty.
The accelerating and profitable globalist march towards unprecedented levels of ‘1984’ style totalitarianism – using censorship, vaccine passports, 15 minute cities, and CBDC’s continues. It is plausible that the WHO and the UN will move to impose, influence or recommend sanctions against countries that do not want to or cannot comply with its centralised health agenda and undemocratic legislative attempts.
What is the basis for me raising the red flag on sanctions in 2023?
Health is no longer just health, as it is defined in the WHO’s constitution. Through Covid-19, and other controversially declared pandemics, health is now a multi-billion dollar health security industry. With it, creeps in the tyranny of secrecy, surveillance, vaccine certificates, forced quarantines, and the undemocratic censorship of free speech. Given the absence of public participation, the WHO is a strategic spear for oligarchs and corporations, and given international resistance to its power grab, it becomes desperate and argues or pushes for sanctions.
Reported in 2021: “In 2021, German Health Minister Jens Spahn called for sanctions against countries that hide information about future outbreaks. Citing the World Trade Organization’s power to sanction countries for non-compliance, Spahn said “there must be something that follows” if countries fail to live up to commitments under a new pandemic treaty that the World Health Assembly will take up in November.”
Further, it is entirely under reported that controversial “World Health Organization Director-General Tedros Adhanom Ghebreyesus also urged countries to consider the idea as they take up the treaty, a legally binding tool. The treaty should “have all the incentives, or the carrots” to encourage transparency, Tedros said, appearing at a press conference with Spahn in Berlin. “But maybe exploring the sanctions may be important,” he added.”
Also reported in 2021: “Speaking at the WHA in June, Mike Ryan, WHO Health Emergencies Programme Executive Director, also spoke out in favour of the treaty, despite the fact that WHO technical staff have historically avoided taking positions on controversial policy choices before member states. “My personal view is that we need a political treaty that makes the highest-level commitment to the principles of global health security — and then we can get on with building the blocks on this foundation.”
I engaged renowned international law expert Professor Francis Boyle about the possibility of sanctions via the WHO. He had no doubt “They will pursue sanctions against countries that do not comply with their orders, coming from Geneva. Both economic and political sanctions. However, they will only have the power to pursue sanctions if we accept their authority. We cannot. We must exit the WHO.”
UN Power Grab. Disaster Capitalism 101.
With far less public scrutiny currently than the controversial WHO, the United Nations is simultaneously seeking exponential new powers and stronger global governance mechanisms, including multilateralism, to deal with what they define as international emergencies.
UN Secretary-General Antonio Guterres’ Common Agenda report arises from a UN declaration on the commemoration of its seventy-fifth anniversary. This report states “All proposed actions are designed to accelerate the achievement of the Sustainable Development Goals. Our Common Agenda is intended to advance the 12 themes of the declaration.”
In March 2023, UN secretary-general Antonio Guterres released a related policy brief: To Think and Act for Future Generations – OUR COMMON AGENDA – Policy Brief 2 – Strengthening the International Response to Complex Global Shocks – An Emergency Platform.
One of this policy brief’s 12 key themes is ‘Being Prepared’, which includes:
1. Emergency Platform to be convened in response to complex global crises
2. Strategic Foresight and Global Risk Report by the United Nations every five years
3. On global public health:
a) Global vaccination plan
b) Empowered WHO
c) Stronger global health security and preparedness
d) Accelerate product development and access to health technologies in low- and middle-income countries
e) Universal health coverage and addressing determinants of health
Under the topic of addressing major risks, Guterres states:
98. An effort is warranted to better define and identify the extreme, catastrophic and existential risks that we face. We cannot, however, wait for an agreement on definitions before we act.
99. Learning lessons from the COVID-19 pandemic, we can seize this opportunity to better anticipate and prepare to respond to large-scale global crises. This requires stronger legal frameworks, better tools for managing risks, better data, the identification and anticipation of future risks, and proper financing of prevention and preparedness. Importantly, however, any new preparedness and response measures should be agnostic as to the type of crisis for which they may be needed. We do not know which extreme risk event will come next. It might be another pandemic, a new war, a high-consequence biological attack, a cyberattack on critical infrastructure, a nuclear event, a rapidly moving environmental disaster, or something completely different such as technological or scientific developments gone awry and unconstrained by effective ethical and regulatory frameworks.
101. Secondly, I propose to work with Member States to establish an Emergency Platform to respond to complex global crises. The platform would not be a new permanent or standing body or institution. It would be triggered automatically in crises of sufficient scale and magnitude, regardless of the type or nature of the crisis involved. Once activated, it would bring together leaders from Member States, the United Nations system, key country groupings, international financial institutions, regional bodies, civil society, the private sector, subject-specific industries or research bodies and other experts. The terms of reference would set out the modalities and criteria for the activation of the platform, including the scale and scope of the crisis; funding and financing; the identification of relevant actors who would form part of it; the support that it would be expected to provide; and the criteria for its deactivation. The platform would allow the convening role of the Secretary-General to be maximized in the face of crises with global reach.
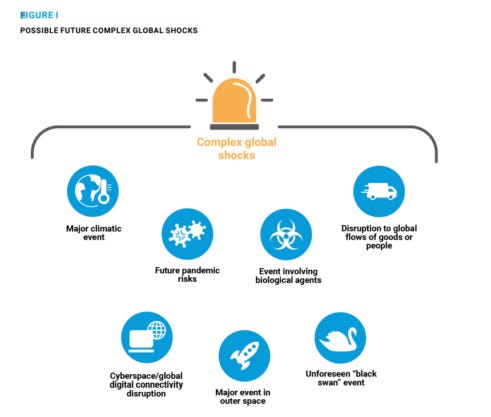
DIAGRAM: Policy Brief 2 – Strengthening the International Response to Complex Global Shocks – An Emergency Platform
UN’s Emergency Platform = One World Government backdoor
The emergency platform would be activated during any event that is deemed to have a global impact, and would provide the UN the authority to actively promote and drive an international response. Antonio Guterres, UN secretary-general, declared: “I propose that the General Assembly provide the Secretary-General and the United Nations system with a standing authority to convene and operationalize automatically an Emergency Platform in the event of a future complex global shock of sufficient scale, severity and reach.”
The policy further argues that such authority would “Ensure that all participating actors make commitments that can contribute meaningfully to the response, and that they are held to account for delivery on those commitments.” While the policy states that the emergency authority would have limited duration, it also states that the UN would be able to extend its own powers if it decides to do so. These powers would effectively render public consensus unnecessary, democracies obsolete, and the role of politicians largely irrelevant.
These all encompassing areas of expanded emergency powers relate to:
- pandemics
- wars and nuclear events
- climate or environmental events, degradation or disaster;
- accidental or deliberate release of biological agents;
- disruptions in the flow of goods, people, or finance;
- disruptions in cyberspace or “global digital connectivity;”
- a cyberattack on critical infrastructure
- a major event in “outer space;”
- “unforeseen risks (‘black swan’ events)
- technological or scientific developments gone awry – and unconstrained by effective ethical and regulatory frameworks.
At least 7 out of 10 of the above areas have already happened or are happening.
What does the UN have planned?
On September 20th 2023, the UN intends to adopt a high level political declaration on pandemics. In my analysis, the UN pathway to the one health and one world government agenda is a back up plan to the WHO’s trajectory which is increasingly exposed and resisted.
The UN is planning to host its related ‘Summit of the Future’ in September 2024. Guterres stated “The Summit of the Future is an opportunity to agree on multilateral solutions for a better tomorrow, strengthening global governance for both present and future generations.” The UN website states “The General Assembly welcomed the submission of Our Common Agenda and passed a resolution to hold the Summit on 22-23 September 2024, preceded by a ministerial meeting in 2023. An action-oriented Pact for the Future is expected to be agreed by Member States through intergovernmental negotiations on issues they decide to take forward.”
Understanding Sanctions or Unilateral Coercive Measures
Sanctions are action that is taken or an order that is given to force a country to obey international laws. There are several types of sanctions imposed through the United Nations:
- Economic sanctions – typically a ban on trade, possibly limited to certain sectors such as armaments, or with certain exceptions (such as food and medicine)
- Diplomatic sanctions – the reduction or removal of diplomatic ties, such as embassies.
- Military sanctions – military intervention
- Sport sanctions – preventing one country’s people and teams from competing in international events.
- Sanctions on the environment – since the declaration of the United Nations Conference on the Human Environment, international environmental protection efforts have been increased gradually.
- Economic sanctions are distinguished from trade sanctions, which are applied for purely economic reasons, and typically take the form of tariffs or similar measures.
It is plausible that the UN’s controllers realise that the world is pushing back against the WHO’s overreach, or find it irrelevant to real health. Given that sovereign nations will choose to exit the WHO, the UN decided to launch plan B and ascribe to itself even greater powers. Technically, there is no legislation to exit the United Nations within the UN Charter. Again, this is a critical issue of national sovereignty.
Can the WHO and the UN collaborate on sanctions?
The WHO is an agency of the United Nations.
- In 2015, on punishing member states who violate the International Health Regulations (IHR), as reported: “United Nations health officials said they want to impose sanctions on countries that do not comply with public health regulations meant to avoid the spread of dangerous epidemics, such as the Ebola outbreak that killed more than 9,000 people and ravaged domestic health care systems in West Africa last year.
- World Health Organization Director Margaret Chan said she is investigating ways to reprimand countries that disobey the IHR — a set of rules adopted in 2005 and mandate that countries set up epidemiological surveillance systems, fund local health care infrastructure and restrict international trade and travel to affected regions deemed unsafe to the public, among other provisions. Chan is on a panel set up by U.N. Secretary General Ban Ki-moon, who instructed the group to think of ways to hold countries accountable for how they manage public health crises and punish those who violate the IHR.”
- In 2022, according to commentators in a policy article: “In order to enforce compliance, some commentators have recommended concluding the treaty at the United Nations level. However, we fear that it has been already decided with the INB (mandated by WHASS) that a treaty will be developed under the roof of WHO. They added: “To move on with the treaty, WHO therefore needs to be empowered — financially, and politically. If international pandemic response is enhanced, compliance is enhanced. In case of a declared health emergency, resources need to flow to countries in which the emergency is occurring, triggering response elements such as financing and technical support.
- These are especially relevant for LMICs, and could be used to encourage and enhance the timely sharing of information by states, reassuring them that they will not be subject to arbitrary trade and travel sanctions for reporting, but instead be provided with the necessary financial and technical resources they require to effectively respond to the outbreak. High-income settings may not be motivated by financial resources in the same way as their low-income counterparts. An adaptable incentive regime is therefore needed, with sanctions such as public reprimands, economic sanctions, or denial of benefits.”
Conclusion
Given the rapidly growing distrust in the WHO, its historical failures and harms, Covid-19 failures and harms, and the fact that it cannot maintain independence because it is a largely privately funded entity; it is plausible that the WHO and/or the UN will move to impose or influence sanctions via the World Trade Organisation, ahead of Agenda 2030. This act of aggression weaponises the WHO and/or the UN against countries that influential funders and unethical stakeholders have an interest in destabilising for power and resource control.
This sinister strategy has disturbing implications for democracy, peace, and prosperity around the world. Freedom faces an existential risk through unelected bureaucratic entities. Nations can and must protect their sovereignty by defunding and exiting WHO, and, by critically assessing the true history, nature, value, and risks of continued membership in the 78 year old United Nations. Not to do so, means to ignore the risks of UN peacekeepers, known to commit crimes with impunity, being deployed in your country to enforce UN and WHO governance.
WHO Plans More ‘Health Promoting Schools’ — Critics Say More Vaccines, Less Parental Control Are Fueling the Plan
By Michael Nevradakis, Ph.D. | The Defender | June 7, 2024
The World Health Organization (WHO) is expanding its “health promoting schools” initiative worldwide, citing flagging vaccination rates and the need to provide medical services to underprivileged children and combat alleged misinformation.
The COVID-19 pandemic is behind the latest push to expand its “Making Every School a Health Promoting School” program, the WHO said, citing “the largest disruption of education systems in history” and “the health effects of mass school closures” and other pandemic-related disruptions.
The agency said the initiative aims to “serve over 2.3 billion school-age children” worldwide.
But critics say that behind the WHO’s noble-sounding plan to expand health-promoting schools — also known as school-based health centers (SBHCs) — is an attempt to gain “a foothold in our schools,” to bypass parental consent and expand vaccination, data collection and surveillance.
Laura Sextro, CEO and chief operating officer of The Unity Project, a California-based health freedom and parental rights nonprofit, told The Defender that SBHCs are “very, very agenda-driven organizations within the school system.”
Sextro said SBHCs “will cover everything from sex education [to] radical gender ideology. They’ll be talking about driving vaccines … That is something that frankly parents should have the autonomy” over.
Valerie Borek, associate director and lead policy analyst for Stand For Health Freedom, said SBHCs will promote “vaccines, especially COVID, HPV, and influenza.”
“School-based health centers have no place in public schools,” said Sheila Matthews, co-founder of AbleChild: Parents for Label and Drug Free Education. Matthews alleged the centers allow “Big Pharma access to our children, who are a captive audience.”
Nigel Utton, a board member of the World Freedom Alliance and coordinator of its Education Charter, said the WHO can’t be trusted to support the health of young people. “If it did, no child in the world would live in unsanitary conditions, or be subjected to trafficking, poor nutrition or emotional intimidation within school systems,” he said.
“Instead, the WHO wastes enormous resources on forcing vaccination programs — injecting children with dangerous chemicals including animal proteins, heavy metals and other unspecified ingredients,” Utton added.
Critics also question the involvement of private interests in SBHCs, including the Bill & Melinda Gates Foundation — and Bill and Melinda Gates themselves — in promoting SBHCs and funding the WHO’s reports on the subject.
School-based health centers give ‘Big Pharma access to our children’
SBHCs aren’t new — the concept dates back to the 1970s. The WHO, UNESCO and UNICEF have actively promoted such programs since 1995.
SBHCs are intended to offer “primary care, mental health care, and other health services in schools,” particularly in underserved communities. This includes services such as immunizations and “well-child care.”
A 2020 paper in Health Promotion Perspectives, whose lead author, Manuela Pulimeno, Ph.D., is UNESCO’s chair on health education and sustainable development, said health-promoting schools help “integrate health educational goals in a holistic perspective at school” and have shown positive outcomes.
“To achieve this goal, health-related contents may be embedded in the school curricula as core discipline,” the paper states.
The American Academy of Pediatrics (AAP) has endorsed SBHCs, stating they “improve access to health care services for students by decreasing financial, geographic, age, and cultural barriers.”
In the U.S., the School-Based Health Alliance promotes SBHCs. According to the alliance, about 3,900 SBHCs operate nationally, up from around 1,900 in 2012. A September 2023 study in JAMA Network Open called for “additional SBHC expansion.”
In 2022, the Biden administration issued $75 million in grants to states to expand SBHCs, while the Centers for Disease Control and Prevention incorporated SBHCs into its “Whole School, Whole Community, Whole Child” model.
On a global level, “work is currently underway with early adopter countries such as Egypt, Kenya, North Macedonia and Paraguay to support governments in building a new generation of school health programmes,” the WHO said in a May 26 report.
WHO’s global standards for SBHCs include censorship and surveillance
In their report, the WHO developed eight “global standards” for SBHCs (page 3), in which school health services represent just one such standard. Other standards include school and government policies, school governance and leadership, school and community partnerships, schools social-emotional and physical environments and curriculum.
These are accompanied by 13 “implementation areas,” (page 17) calling for reinforcement of “intersectoral government and multi-stakeholder coordination,” strengthening “school and community partnerships,” curriculum development, “teacher training and professional learning” and monitoring and evaluation.
Critics say these proposals allow schools to implement vaccine programs. For instance, SBHCs have been linked to higher human papillomavirus (HPV) vaccination rates, according to a 2022 report.
Merck, the maker of the Gardasil HPV vaccine, is a funder of the School-Based Health Alliance, whose board includes several members with ties to Big Pharma and vaccine-promoting organizations.
The Gardasil HPV vaccine is often administered to teenagers as part of school vaccination programs. In October 2023, a 12-year-old boy in France died days after collapsing and injuring himself minutes after HPV vaccination at his school.
In the U.S., several state and city government websites include vaccinations among the list of services SBHCs provide.
“Increased vaccine uptake is a mark of success for school-based health programs,” Borek said. “They’re considered an optimal place to promote and administer vaccines. In fact, schools and vaccine policy go hand in hand historically — vaccines didn’t have a strong foothold until schools mandated them for admission.”
Utton pointed out that “schools have been used to coerce and manipulate children into taking vaccinations against the will of their parents. Teachers have been indoctrinated, and those who have questioned the manipulative agenda have been ostracized.”
Borek said the “psychological pressure” a child experiences when a school authority figure recommends any kind of medical care creates a “fertile ground for pushing policy.”
SBHCs ‘will certainly be a tool to collect data’
Included among the WHO’s global standards for SBHCs are interventions in school curriculums and proposals to “embed school health content” in training for educators.
The 2020 Health Promotion Perspectives paper said the WHO calls for the incorporation of “health literacy” in “the core curriculum as children enter school.”
Critics told The Defender that changes like these could lead to the inclusion of non-health-related topics in school curricula under the guise of health education.
Virginie de Araujo-Recchia, a French lawyer and member of ONEST, France’s National Organization of Ethics, Health and Transparency, told The Defender that SBHCs may be “favored by the political powers in an attempt to achieve a fusion between education, citizenship and environmental causes.”
The WHO’s global standards for SBHCs also target “misinformation.” According to UNESCO, SBHCs “can … teach young people develop the critical thinking skills they need to reject harmful health-related myths and misconceptions,” noting that “This is a key in responding to pandemics like Covid-19 and HIV.”
The global standards call on schools to develop “versatile physical spaces that can be adapted to changing restrictions, as in managing the COVID-19 pandemic.”
The WHO’s global standards also contain provisions for increased data collection and surveillance in schools, with the 13th “implementation area” calling on schools to “Design, develop and share practices for collecting, storing and analysing data.”
This is linked to calls to provide “capacity-building in evaluation (e.g. data collection and analysis)” and investments “in feasible … interoperable systems for collecting and storing data from monitoring at all levels of the education and/or health system.”
According to Stand for Health Freedom, SBHCs are “completely unregulated” in the U.S.
For instance, it is unclear how HIPAA (the Health Insurance Portability and Accountability Act of 1996) andthe Family Educational Rights and Privacy Act will be applied to SBHCs and students’ health information.
SBHCs “will certainly be a tool to collect data on anything from vaccine status to sexual preference,” Sextro said.
Children can become ‘health trainers of their parents’
The WHO claims SBHCs involve “all stakeholders, and particularly students, parents and caregivers.” The agency’s global standards call for “opportunities for parents … to participate meaningfully in the governance, design, implementation and evaluation” of SBHCs and their inclusion on “design teams” and governance boards.
But the WHO appears to contradict itself, excluding parents from the “system of global standards for health-promoting schools” and noting that the “target readership” of its SBHC-related documents is “mainly people in government.”
According to Nemours KidsHealth, the centers “only provide care to children with parents’ written permission.” However, the organization notes that this “permission” usually consists of “the option to sign a permission form at the beginning of each school year.”
A consent form for an Atlanta SBHC shared with The Defender says nothing about parents being notified before, during or after treatment. Last year, a Connecticut school board was sued for rejecting a government-funded school-based mental health clinic that aimed to treat teens without parental consent.
“The reason they’re doing this is because they don’t want parents to be able to exercise their rights, which is to … make medically informed decisions on behalf of their children. And so, they’re usurping the parents,” Sextro said.
“Parents need to be front and center in their child’s medical care,” Borek said. “These centers are cleaving that relationship by promoting medical assessments and treatment without the presence of a parent.”
A proposed bill in New Hampshire (SB 343) would require parents to be present when services are provided at an SBHC.
“Schools are clearly not the place to introduce school health centers,” de Araujo-Recchia said. “Our children are neither guinea pigs for mass medical experimentation nor beings to be sacrificed.”
Notably, UNESCO suggests SBHCs can help children “educate” their parents on health matters. According to the 2020 Health Promotion Perspectives paper, SBHCs can help children “become health trainers of their parents, relatives and friends, impacting positively the entire society.”
Gates ‘has a direct financial benefit’ from SBHCs
Earlier this year, Melinda French Gates announced a $23 million investment in the School-Based Health Alliance, alongside fellow billionaire MacKenzie Scott, ex-wife of Amazon CEO Jeff Bezos.
The Gates Foundation has also provided financial support for the publication of at least two WHO reports on SBHCs.
“The Gates Foundation and Gavi, The Vaccine Alliance [founded and funded by Gates] fiercely promote childhood vaccination, and make a lot of money from it,” de Araujo-Recchia said. “This is not philanthropy at all, but a stranglehold and ideology,” citing the WHO’s partnership with the Rockefeller Foundation as another example.
Sextro said Gates “has a direct financial benefit and interest in promoting these school-based health centers, because they will directly promote everything from the pharmaceutical to the vaccine interest that he and the Gates Foundation have.”
The WHO’s global standards for SBHCs include calls for the delivery of “comprehensive school health services based on a formal agreement between schools (or local education departments) and health service providers.”
According to the School-Based Health Alliance, 21% of funding for SBHCs in the U.S. came from private foundations in 2022, while according to the AAP, “local hospitals [may] provide … financial support for SBHCs.”
The WHO “is mainly financed by private funds from companies or foundations owning pharmaceutical labs,” de Araujo-Recchia said. “The capital links between the mainstream media, digital giants, American financial giants and the WHO demonstrate real collusion.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
The WHO pandemic treaty: dead but not buried
BY KEVIN BARDOSH | UNHERD | MAY 28, 2024
As the World Health Assembly began this week in Geneva, it was announced that member states had failed to reach agreement on a new, legally binding pandemic treaty.
Despite not reaching the deadline after more than two years of negotiations, the WHO Director-General, Dr Tedros Adhanom Ghebreyesus, remained confident that the 194 member states would eventually reach an agreement, perhaps in six to 12 months. Health diplomats are also confident that amendments to the 2005 International Health Regulations (IHR) — a parallel set of global governance rules, including a new tiered system to declare a pandemic — will go ahead this week. We will have to wait and see.
Front and centre in the failure of the treaty this week were disputes between the Global North and South regarding pathogen sharing and access to the new tests, treatments and vaccines that would be developed by the pharmaceutical industry in the event of a new pandemic. This rekindled longstanding neocolonial sentiments, especially among African countries, concerned that access to pharmaceutical products would be dependent on fulfilling treaty obligations.
Recent analyses have also shown that, to meet basic targets of the treaty, developing countries would need to heavily invest in pandemic preparedness and response to the tune of some $31 billion per year. This level of financing would take away vital budgets from existing health systems and skew national priorities. Is this really in the best interest of developing countries?
Other criticisms of the treaty have come from US and UK conservatives. Senate Republicans recently called for the Biden administration to reject the treaty and shift focus to “comprehensive WHO reforms that address its persistent failures without expanding its authority”. With US elections set for November, negotiators in Geneva are well aware that Donald Trump may withdraw from the WHO if elected, as he did in 2020. In the UK, Nigel Farage also came out against the treaty, expressing concern about future WHO-supported lockdowns: “The WHO can be a force for good in the world, but only if it returns to its noble principles and core objectives.”
Yet the WHO has vehemently rejected any concerns about the treaty infringing on “national sovereignty”, previously calling them “fake news, lies, and conspiracy theories”. Mainstream news outlets — from the New York Times to Reuters — have reiterated these talking points. Recent articles in Health Policy Watch called for critics, or rather “spreaders of disinformation”, to be treated like an “organised crime” network. Any legitimate criticism is unwelcome.
Those in global health leadership want bolder steps to manage the “infodemic”. But advocates of the treaty have regularly engaged in misinformation themselves. Take, for example, a recent video from former UK prime minister Gordon Brown, now WHO Ambassador for Global Health Financing. In the video, Brown makes the bold claim that “the world needs agreement on the pandemic accord” since “no one is safe anywhere until everyone is safe everywhere”. The latter statement is a perfect illustration of the propaganda tools used by governments in the name of “health” during Covid: utopian, illogical, and Orwellian.
The negotiations and media framing of them, therefore, represent the cultural ethos of biosecurity, which prioritises “making the world safer” (security) over all other values and, given our collective experiences during Covid, basic principles of logic and Western democratic norms.
The WHO is also, this week, seeking an unprecedented increase of its budget by $7 billion over four years to respond to crises. Yet the organisation has failed to conduct a serious post-mortem of the failures of the Covid pandemic response. Instead, media outlets and health authorities complain about “mistrust” and “populism” without any mention of the harms of vaccine mandates and coercive and ineffective lockdowns, school closures, mask mandates, and other Covid measures. We must march forward into a global treaty, no questions asked.
Yet this problem is now systemic in global public health. Many preeminent Covid evaluation reports are deeply flawed. A recent paper called the UK Royal Society’s assessment, published last year, “irrelevant and weak from a methodological point of view but also dangerously misleading in terms of policymaking. This is how misinformation occurs.”
Many countries, the UK and US included, are still in the process of evaluating their Covid response. Others have none planned. It seems more than reasonable that the global public health community should first be obliged to take a serious, evidence-based look at just how wrong the experts got it from 2020-22. But to do that, we need the WHO to be less concerned about fighting “conspiracy theorists” and “far-Right nationalists” and more concerned about earning back the trust of the world’s public. It will be a long road ahead.
Kevin Bardosh is a research professor and Director of Research for Collateral Global, a UK-based charity dedicated to understanding the collateral impacts of Covid policies worldwide.
15 nations have made their position on the WHO sovereignty grab public before the WHA meeting commences
How many other countries are entirely fed up with the World Stealth Organization’s misleading spin about “equity”?
BY MERYL NASS | MAY 12, 2024
The negotiations have been controlled by globalists, not nations, from day one.
Eleven nations informed the UN General Assembly they were not going along with the UN’s support for the WHO Pandemic Preparedness Agenda last September. In alphabetical order:
- Belarus
- Bolivia
- Cuba
- Democratic People’s Republic of Korea
- Eritrea
- Islamic Republic of Iran
- Nicaragua
- Russian Federation
- Syrian Arab Republic
- Venezuela
- Zimbabwe
The Netherlands’ government has been instructed to delay the WHO votes or vote No by the lower house of Parliament.
Slovakia said it will not sign current drafts of both documents.
Croatia’s new majority party is against the WHO’s pandemic preparedness plan
Italy’s Senator Borghi said Italy will vote No on the treaty and furthermore that there are 10 more months in which to reject the IHR Amendments.
It is very unusual to have this level of disagreement made public even before the start of the World Health Assembly meeting. And with “hybrid negotiations” aka backroom horse-trading, leading right up to the meeting, nobody will have time to consider the treaties before they are due to be voted on. It has been a corrupt process from start to finish. It could only succeed with stealth (no one knowing what is really in the treaties) and bribes.
Now that the US has announced that 100 countries are being paid off to develop their pandemic preparedness agenda, will the bribes be enough to get these treaties across the finish line? Will the unbribed be miffed? How much will it cost the US taxpayer for the world’s nations to agree to dictatorial control of pandemics and health information going forward?
Attempts to impose control over us “for pandemics” are being implemented at the state, federal, and World level
Newest versions of the treaty and amendments included, all these laws need to be revoked or (at the WHO) stopped
BY MERYL NASS | MAY 4, 2024
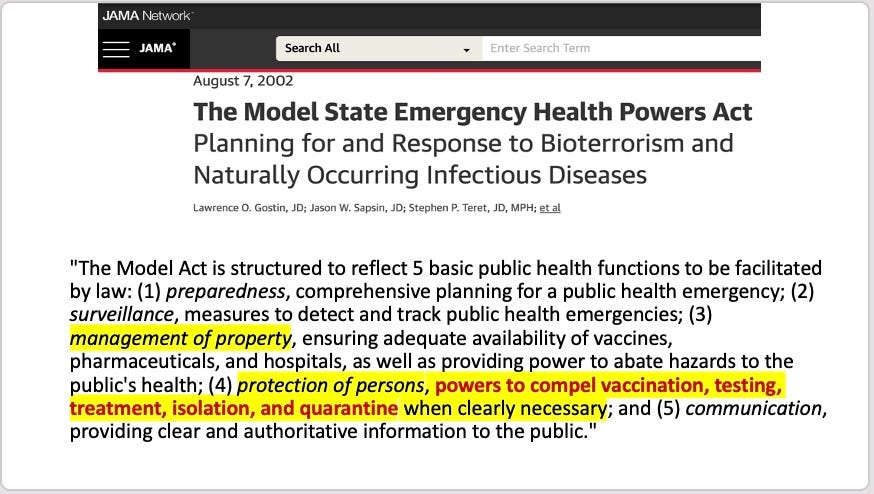
Laws that almost all states passed after 9/11/01, drafted by Georgetown health law professor Lawrence O. Gostin, paid for by the CDC, were unconstitutional many have said. Then Gostin bragged about his bill in the JAMA.
Then Congress passed the PREP Act in 2005, which for the first time allowed the widespread use of unlicensed drugs and vaccines.
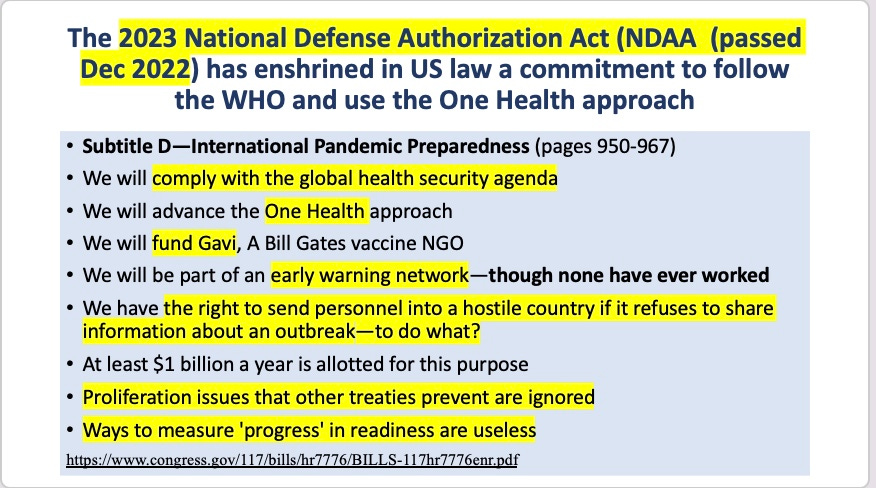
The US federal government passed the International Pandemic Preparedness Act in December 2022. Probably few Congress members knew anything about these 18 pages in the middle of a 1700 page DOD funding bill.
The WHO Pandemic Agreement (treaty) and International Health Regulation amendments are designed to globalize control of public health emergencies, expand the range of what kinds of emergencies would come under the WHO’s jurisdiction, and place essentially all decisions into the hands of the WHO Director-General, who currently is not a physician. Who would give him his marching orders? Bill Gates? The rest of the WHO organization has no expertise in managing pandemics, and yet it proposes to manage the public health of 8 billion people, using a one-size-fits-all approach.
Lawrence O. Gostin, who was hired by CDC 25 years ago to craft the laws that made governors dictators during the COVID pandemic, is now assisting the WHO to craft its new instruments of control, but this time on a global level.
Here are the latest versions of each document, with highlights I made for myself. These need to be shot down BEFORE they are enacted, unlike the 3 US bills mentioned above, which are still active and are likely to be used during the “next” designated pandemic.
April 2024 Bureau text of the amended IHR.
April 2024 draft pandemic Treaty
States Move to Oppose WHO’s ‘Pandemic Treaty,’ Assert States’ Rights
By Michael Nevradakis, Ph.D. | The Defender | April 29, 2024
Two states have passed laws — and two states have bills pending — intended to prevent the World Health Organization (WHO) from overriding states’ authority on matters of public health policy.
Utah and Florida passed laws and Louisiana and Oklahoma have legislation set to take effect soon pending final votes. Several other states are considering similar bills.
The WHO member states will convene next month at the World Health Assembly in Geneva, Switzerland, to vote on two proposals — the so-called “pandemic accord” or “pandemic treaty,” and amendments to the International Health Regulations (IHR) — that would give the WHO sweeping new pandemic powers.
The Biden administration supports the two WHO proposals, but opposition is growing at the state level.
Proponents of the WHO’s proposals say they are vital for preparing humanity against the “next pandemic,” perhaps caused by a yet-unknown “Disease X.”
But the bills passed by state legislatures reflect frequently voiced criticisms that the WHO’s proposals imperil national sovereignty, medical and bodily sovereignty and personal liberties, and may lead to global vaccine mandates.
Critics also argue the WHO proposals may open the door to global digital “health passports” and global censorship targeting alleged “misinformation.”
Such criticisms are behind state legislative initiatives to oppose the WHO, on the basis that states’ rights are protected under the 10th Amendment of the U.S. Constitution. Under the 10th Amendment, all powers not delegated to the federal government are reserved to the states. Such powers, critics say, include public health policy.
Mary Holland, president of Children’s Health Defense (CHD), told The Defender :
“It is encouraging to see states like Louisiana, Oklahoma and Utah pass resolutions to clarify that the WHO has no power to determine health policy in their states. Historically, health has been the purview of state and local government, not the U.S. federal government.
“There is no legitimate constitutional basis for the federal government to outsource health decision-making on pandemics to an international body. As state legislatures become aware of the WHO’s agenda, they are pushing back to assert their autonomy — and this is welcome.”
Internist Dr. Meryl Nass, founder of Door to Freedom, told The Defender that, contrary to arguments that the drafters of the constitution could not foresee future public health needs, vaccines, doctors and medicine were all in existence at the time the 10th Amendment was written. They were “deliberately left out,” she said.
This has implications for the federal government’s efforts in support of the WHO’s proposals, according to Nass. “The government doesn’t have the authority to give the WHO powers for which it lacks authority,” she said.
Tennessee state Rep. Bud Hulsey (R-Sullivan County) told The Epoch Times, “We’re almost to a place in this country that the federal government has trampled on the sovereignty of states for so long that in peoples’ minds, they have no options.”
“It’s like whatever the federal government says is the supreme law of the land, and it’s not. The Constitution is the supreme law of the land,” he added.
Utah, Florida laws passed
On Jan. 31, Utah Gov. Spencer Cox (R) signed Senate Bill 57, the “Utah Constitutional Sovereignty Act,” into law. It does not mention the WHO, but prohibits “enforcement of a federal directive within the state by government officers if the Legislature determines the federal directive violates the principles of state sovereignty.”
In May 2023, Florida passed Senate Bill 252 (SB 252), a bill for “Protection from Discrimination Based on Health Care Choices.” Among other clauses, it prohibits businesses and public entities from requiring proof of vaccination or prophylaxis for the purposes of employment, receipt of services, or gaining entry to such entities.
According to Section 3 of SB 252:
“A governmental entity as defined … or an educational institution … may not adopt, implement, or enforce an international health organization’s public health policies or guidelines unless authorized to do so under state law, rule, or executive order issued by the Governor.”
Nass told The Defender that Florida’s legislation offers a back door through which WHO the state can implement WHO policies because it allows a state law, rule or executive order by the governor to override the bill. According to Nass, efforts to strengthen the bill have been unsuccessful.
SB 252 was one of four bills Florida Gov. Ron DeSantis (R) signed in May 2023 in support of medical freedom. The other bills were House Bill 1387, banning gain-of-function research, Senate Bill 1580, protecting physicians’ freedom of speech and Senate Bill 238, prohibiting discrimination on the basis of people’s medical choices.
Louisiana, Oklahoma also push back against the WHO
The Louisiana Senate on March 26 voted unanimously to pass Senate Law No. 133, barring the WHO, United Nations (U.N.) and World Economic Forum from wielding influence over the state.
According to the legislation:
“No rule, regulation, fee, tax, policy, or mandate of any kind of the World Health Organization, United Nations, and the World Economic Forum shall be enforced or implemented by the state of Louisiana or any agency, department, board, commission, political subdivision, governmental entity of the state, parish, municipality, or any other political entity.”
The bill is now pending Louisiana House of Representatives approval and if passed, is set to take effect Aug. 1.
On April 24, the Oklahoma House of Representatives passed Senate Bill 426 (SB 426), which states, “The World Health Organization, the United Nations and the World Economic Forum shall have no jurisdiction in the State of Oklahoma.”
According to the bill:
“Any mandates, recommendations, instructions, communications or guidance issued by the World Health Organization, the United Nations or the World Economic Forum shall not be used in this state as a basis for action, nor to direct, order or otherwise impose, contrary to the constitution and laws of the State of Oklahoma any requirements whatsoever, including those for masks, vaccines or medical testing, or gather any public or private information about the state’s citizens or residents, and shall have no force or effect in the State of Oklahoma.”
According to Door to Freedom, the bill was first introduced last year and unanimously passed the Senate. An amended version will return to the Senate for a new vote, and if passed, the law will take effect June 1.
Legislative push continues in states where bills opposing the WHO failed
Legislative initiatives opposing the WHO in other states have so far been unsuccessful.
In Tennessee, lawmakers proposed three bills opposing the WHO, but “none of them made it over the finish line,” said Bernadette Pajer of the CHD Tennessee Chapter.
“Many Tennessee legislators are concerned about the WHO and three of them filed resolutions to protect our sovereignty,” Pajer said. “Our legislature runs on a biennium, and this was the second year, so those three bills have died. But I do expect new ones will be filed next session.”
The proposed bills were:
- House Joint Resolution 820 (HJR 820), passed in the Tennessee House of Representatives. The bill called on the federal government to “end taxpayer funding” of the WHO and reject the WHO’s two proposals.
- House Joint Resolution 1359 (HJR 1359) stalled in the Delayed Bills Committee. It proposed that “neither the World Health Organization, United Nations, nor the World Economic Forum shall have any jurisdiction or power within the State of Tennessee.”
- Senate Joint Resolution 1135 (SJR 1135) opposed “the United States’ participation in the World Health Organization (WHO) Pandemic Prevention Preparedness and Response Accord (PPPRA) and urges the Biden Administration to withdraw our nation from the PPPRA.”
Amy Miller, a registered lobbyist for Reform Pharma, told The Defender she “supported these resolutions, especially HJR 1359. She said the bill “went to a committee where the sponsor didn’t think it would come out since a unanimous vote was needed and one of the three members was a Democrat.”
Tennessee’s HJR 820 came the closest to being enacted. According to Nass, this bill was “flawed,” as it “did not assert state sovereignty or the 10th Amendment.”
Another Tennessee bill, House Bill 2795 and Senate Bill 2775, “establishes processes by which the general assembly [of the state of Tennessee] may nullify an unconstitutional federal statute, regulation, agency order, or executive order.”
According to The Epoch Times, this would give Tennessee residents “the right to demand that state legislators vote on whether or not to enforce regulations or executive orders that violate citizens’ rights under the federal or state constitutions.” The bill is tabled for “summer study” in the Senate.
In May 2023, Tennessee passed legislation opposing “net zero” proposals and the U.N. Sustainable Development Goals — which have been connected to “green” policies and the implementation of digital ID for newborn babies and for which the U.N. has set a target date of 2030 for implementation.
According to The Epoch Times, “Maine state Rep. Heidi Sampson attempted to get a ‘joint order’ passed in support of personal autonomy and against compliance with the WHO agreements, but it garnered little interest in the Democrat supermajority legislature.”
In Alabama, the Senate passed House Joint Resolution 113 opposing the WHO. The bill was reported out of committee but, according to Nass, it stalled.
Other states where similar legislation was proposed in the 2024 session or is pending include Georgia, Idaho, Iowa, Kentucky, Michigan, New Hampshire, New Jersey, South Carolina and Wyoming.
Recent Supreme Court ruling may curtail federal government’s powers
While opponents of the WHO’s proposed “pandemic agreement” and IHR amendments point to the states’ rights provision of the 10th Amendment, others argue that a 1984 U.S. Supreme Court decision in Chevron v. Natural Resources Defense Council allowed federal agencies to assert more authority to make laws.
The tide may be turning, however. According to The Epoch Times, “The current Supreme Court has taken some steps to rein in the administrative state, including the landmark decision in West Virginia v. Environmental Protection Agency, ruling that federal agencies can’t assume powers that Congress didn’t explicitly give them.”
Nass said that even in states where lawmakers have not yet proposed bills to oppose the WHO, citizens can take action, by contacting the office of their state governor, who can issue an executive order, or their attorney general, who can issue a legal opinion.
Door to Freedom has also developed a model resolution that state legislative bodies can use as the basis for their own legislation.
“It’s important for people to realize that if the federal government imposes something on the people, the people can go through their state’s powers to overturn it,” Nass said.
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
The Pandemic Agreement. The Globalist Agenda versus the Global South’s agenda
BY MERYL NASS | APRIL 30, 2024
The USA agenda for the Pandemic Agreement appears to coincide with the globalist agenda: pathogen sharing, gain-of-function research, massively increased genome sequencing for purposes yet to be acknowledged, rapid rollout of vaccines and drugs for all the new pandemics we will see (or at least hear about, such as bird flu), centralized control of health emergencies by the WHO with a new governance role for that organization. Nations will be obligated to obey the WHO. The “One Health” concept will be used to give powers to the WHO that have heretofore not been considered directly related to health, but are being redefined so they are included in “One Health”—such as the ability to issue orders in the name of protecting animals, plants, ecosystems and so-called biodiversity.
There are more poor nations than rich ones. The poor nations would like more healthcare personnel; would like to plug the “brain drain” of medical and professional personnel to the richer countries; would like more infrastructure: clinics, hospitals, laboratories. They would like some money to flow to them.
The WHO treaty is telling them it will give them a little bit: some crumbs (10%-20% of the drugs and vaccines they will need for free or at low cost). And if they play along and provide what they consider to be their own intellectual property (dangerous microorganisms discovered on their turf) the rich nations promise them some royalties. Amount unspecified.
What the two sides want is very different. In all the drafts so far, what the globalists have offered has not moved much if at all. They have played hardball. How much are they prepared to give up at the last minute? There are no indications yet of last-minute generosity.
The Geneva Health Files substack today indicates that the WHO’s Secretariat and Bureau are jumping in to the negotiations to create new procedures to try and reach agreement. As I have said before, this is evidence that the “member-led process” claimed by Tedros is a sham, as the procedures are shaped and reshaped by bureaucrats in order to achieve the aims of the WHO’s biggest funders.
Geneva Health Files also has some interesting things to say about the country negotiators vs their ambassadors and health ministers. Priti Patnaik, the author, seems to think that consensus can be achieved if the negotiators can hold back the senior officials from their governments. Presumably this means that the negotiators are tired (or bribed) and are ready to give in to the big boys on some issues, and if they can just be allowed to manage the treaty discussions in isolation, without obeying messages from home, agreement can be reached. Hmmmm to that.
We have already seen the Russian negotiator Smolenskiy working against his nation’s interests and the Italian negotiator (who someone claimed was Ethiopian) claiming support for the treaty and amendments when the Italian government was not in favor. Does this imply that the globalists have captured other negotiators — so that separating them from those providing instructions from the home country is what is being attempted?
Will the global south give in to the globalist agenda for a measly few pieces of silver, accepting all the risks the WHO documents will subject them too? Meanwhile, the global north prints money like crazy, and could in fact offer considerably more at the last minute.
But is any amount worth the risk of entering into an era of pandemics, rolling out dangerous vaccines and giving the WHO authority over vast swathes of the planet?
I must ask again: for whom is the WHO’s agenda good? Who benefits? Only those seeking a one world government.
Featured Video
Seyed M. Marandi: Negotiations Collapsed – Return to War
or go to
Aletho News Archives – Video-Images
From the Archives
Wartime internment camps in Australia
National Archives of Australia
World War I
During World War I, for security reasons the Australian Government pursued a comprehensive internment policy against enemy aliens living in Australia.
Initially only those born in countries at war with Australia were classed as enemy aliens, but later this was expanded to include people of enemy nations who were naturalised British subjects, Australian-born descendants of migrants born in enemy nations and others who were thought to pose a threat to Australia’s security.
Australia interned almost 7,000 people during World War I, of whom about 4,500 were enemy aliens and British nationals of German ancestry already resident in Australia.
Records of World War I internment camps
World War II
During World War II, Australian authorities established internment camps for three reasons – to prevent residents from assisting Australia’s enemies, to appease public opinion and to house overseas internees sent to Australia for the duration of the war.
Unlike World War I, the initial aim of internment during the later conflict was to identify and intern those who posed a particular threat to the safety or defence of the country. As the war progressed, however, this policy changed and Japanese residents were interned en masse. In the later years of the war, Germans and Italians were also interned on the basis of nationality, particularly those living in the north of Australia. In all, just over 20 per cent of all Italians resident in Australia were interned. … continue
Blog Roll
 Aletho News
Aletho News- Seyed M. Marandi: Negotiations Collapsed – Return to War
- Tomorrow’s naval blockade showdown
- ‘Israel’ attacks civilians to hide its embarrassing military failures & out of pure sadism
- Any Foreign Military Vessel Approaching Hormuz Under Any Pretext ‘Will Be Dealt With Severely’: IRGC
- Diplomats slam US negotiators’ performance in Iran talks
- Trump Refuses Exit Ramp, War with Iran will Continue
- Trump Says US Naval Blockade in Strait of Hormuz Will Begin Shortly
- US, Iran end 21-hour talks without agreement
- US IRAN TALKS: Who Are the Crazy Ones Here? /Lt Col Daniel Davis
- Talks with the US end without a deal over excessive US demands: Iran
- If Americans Knew
- US-Iran ceasefire negotiations make zero progress – Daily Update
- Pro-Israel ‘Thinktanks’ and Individuals who Influence U.S. Foreign Policy
- Mearsheimer reveals how Israel dictates US policies on Iran, Gaza – video
- After killing 350+, Israel still has a “score to settle” with Lebanon before ceasefire – Daily Update
- Military aid to Israel emerges as the latest political litmus test for Democrats
- The only Palestinian children’s rights organization closes following years-long Israeli campaign against it
- ‘I Can’t Forget the Smell’: Lebanese Reel After Israel Kills Over 300 in Single Day
- DNC Shoots Down Resolutions Calling Out AIPAC and Limiting Arms to Israel
- TCN: Is Israel Blackmailing President Trump?
- Israel killed at least 303 Lebanese yesterday – who were they? Daily Update
- No Tricks Zone
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
