Bird Flu Outbreaks & the WHO/IHR Pandemic Treaty Push
By Barbara Loe Fisher | The Vaccine Reaction | April 22, 2024
Even as U.S. health agencies and the United Nations World Health Organization (WHO) are being heavily criticized for their botched response to the COVID-19 pandemic,1 2 3 WHO officials are ramping up pressure on all nations to sign a WHO pandemic treaty and amendments to the WHO’s International Health Regulations (IHR), which will give them more authority to track, quarantine, force vaccine use and censor free speech during WHO declared pandemics.4 5 The WHO’s Director General has been blaming opposition to the UN agency’s epic power grab on “a torrent of fake news, lies and conspiracy theories.”6
On Apr. 19, 2024, the United Nations sent out a press release declaring that the “ongoing global spread of ‘bird flu’ infections to mammals including humans is a significant public health concern,” pointing to an outbreak of H5N1 viral infections in dairy cows in the U.S. and warning that the virus could evolve and cause human-to-human transmission with “extremely high” mortality.7 The implication was that a potentially deadly global bird flu pandemic was a clear possibility.
The CDC website describes symptoms of H5N1 bird flu infections, and they sound very similar to seasonal influenza or SARS-CoV-2 infections associated with COVID-19 disease:
“The reported signs and symptoms of bird flu virus infections in humans have ranged from no symptoms or mild illness [such as eye redness (conjunctivitis) or mild flu-like upper respiratory symptoms], to severe (such as pneumonia requiring hospitalization) and included fever (temperature of 100ºF [37.8ºC] or greater) or feeling feverish*, cough, sore throat, runny or stuff nose, muscle or body aches, headaches, fatigue, and shortness of breath or difficulty breathing. Less common signs and symptoms include diarrhea, nausea, vomiting, or seizures.”8
Warnings That Egg and Milk Supplies May Be Contaminated with Bird Flu Virus
Mainstream media have been joining the UN in characterizing bird flu outbreaks in cattle as a significant public health concern, with news outlets breathlessly reporting that cattle were infecting each other with H5N1 and some experts questioning whether raw or even pasteurized milk containing high levels of the avian virus is safe.9 Although H5N1 bird flu was first detected in 1996, since 2020 there have been more outbreaks in poultry farms, wild bird and land and marine animals.10 11 Americans were warned in early April that the eggs from chickens potentially infected with the avian virus should be well cooked,12 and then the media reported that a U.S. dairy farm worker in Texas had been infected with bird flu.13
The same day the UN issued their press release, Agence France Presse again reminded readers that a person working on a dairy farm in Texas was recovering from bird flu. A WHO official was quoted as stating that, “The case in Texas is the first case of a human infected by an avian influenza by a cow.”14
U.S. Plan to Drive the Global “Health Security” Agenda If WHO Treaties Fail
Three days earlier, on Apr. 16, the White House announced a five-year “Strategy to Strengthen Global Health Security” plan citing the COVID-19 pandemic as the need to put the U.S. in the driver’s seat via bi-lateral financial investment partnerships with 50 to 100 countries to “drive global action toward shared goals” and “mitigate the impact of health security threats” in order “to prevent, detect and contain them at their source.”15 The new plan “articulates a whole-of-government science-based approach to strengthening global health security.”
The current U.S. administration is in favor of the WHO pandemic treaty and IHR amendments proposed by the world’s largest public health agency.16 However, the WHO is getting pushback from lawmakers and citizens in the U.S. and in other nations, who do not want to go along with the UN/WHO power grab that many critics say threatens human rights and national sovereignty.17 18 19 A respected Japanese scientist posted a video message to the world online,20 and there was a massive demonstration In Japan this month against the WHO pandemic treaty.21
The U.S. “Global Health Security” plan would ensure that if the WHO treaties fail to be signed by enough countries to become international law, the U.S. will make sure there is a global “rapid response to global health emergencies.” According to the U.S. plan, the core of that “rapid response” are “efforts to transform international financial institutions, such as the World Bank, and to accelerate “manufacture, procurement and delivery” of medical countermeasures like vaccines.22
Even though there is Increasing public opposition to the WHO’s plan to expand its legal authority to tell eight billion people what to do whenever WHO officials declare a “public health emergency” – which includes eliminating freedom of speech and electronically monitoring everyone’s vaccination status and requiring people to carry a digital “vaccine passport” in order to travel or enter public spaces23 – it looks like the U.S. government is going to get the job done whether the WHO manages to get enough countries to sign the WHO/IHR treaties or not. The lucrative public-private business partnerships that have been expanded over the past four decades between the WHO, pharmaceutical corporations, governments and other institutions is paying big dividends for the Public Health Empire.24
Bird Flu Vaccines Being Developed and Stockpiled
Is the latest well-publicized specter of a deadly global bird flu pandemic, which is so reminiscent of the well-publicized specter of a deadly coronavirus pandemic in early 2020,25 a harbinger of things to come or just a coincidence?
Whatever it is, the preparations for delivery and approval of H5N1 “vaccines,” which includes mRNA bird flu shots, is well underway.
On Apr. 20, Barrons reported that the U.S. government “says it could distribute enough [bird flu] vaccines within four months to inoculate a fifth of the U.S. population” (68 million people) if the H5N1 strain infecting cattle began to spread among humans.26 Healthcare workers, law enforcement and other first responders, military personnel pregnant women, infants and high risk children would get the shots first.
Apparently, two clinical trials of bird flu vaccine have been underway since last year and CSL Sequiris and GlaxoSmithKline (GSK) are under contract to test the vaccines targeting a strain of avian influenza closely related to the H5N1 strain currently infecting U.S. dairy cows. Another major manufacturer of influenza vaccine, Sanofi, would also likely be involved in bird flu vaccine production.
H5N1 Vaccine Production Could Be Ramped Up to Vaccinate the Entire U.S. Population
An FDA spokesperson reportedly told Barrons that the approval process to quickly distribute a new H5N1 bird flu vaccine for Americans would be similar to the accelerated process used to create annual flu vaccines. A spokesperson for Administration for Strategic Preparedness & Response (ASPR) also commented that, if needed, the agency would work with bird flu vaccine manufacturers “to ramp up production to make enough vaccine doses to vaccinate the entire [U.S.] population.”
Oil in Water Adjuvants in Vaccines and Autoimmunity
Both Sequirus and GSK have developed “oil in water” emulsion adjuvants added to influenza vaccines, including bird flu vaccines, to stimulate hyper-inflammatory responses in the body that generate high levels of antigen-specific antibodies in an effort to make the vaccines more “effective.” Squalene adjuvants have been associated with development of autoimmune disorders.27 28 29
GSK’s AS03 adjuvant contains a-tocopherol, squalene and polysorbate 80,30 and some European children and adults, who got GSK’s AS03 adjuvanted H1N1 “swine flu” vaccine in 2009, developed cases of narcolepsy, a neurological autoimmune disorder.31 The Sequiris influenza vaccine contains MF59,32 the first squalene oil in water emulsion adjuvant added to influenza vaccines in the 1990s.33 According to the Apr. 20 Barrons’ report, large quantities of both of these squalene adjuvants are stored in the U.S. government’s special pandemic influenza vaccine stockpile, which was created in 2005, along with premade influenza antigens.
A 2023 article published by Chinese researchers the medical literature promoted the “remarkable success” of mRNA coronavirus vaccines and the need to use three types of specific adjuvants to make mRNA vaccines more effective: (1) RNA with self-adjuvant characteristics; (2) components of the delivery system [such as lipid nanoparticles]; and exogenous immunostimulants (such as squalene).34
As with squalene adjuvants, the lipid nanoparticles, which envelop and deliver synthetic RNA in COVID shots to body cells to produce the SARS-CoV-2 spike protein, are highly inflammatory to stimulate a strong immune response, but also have been associated with allergy and autoimmunity.35
Europe Already Has Approved Two H5N1 Bird Flu Vaccines
Earlier this year, the European Medicines Agency (EMA) approved two H5N1 avian flu vaccines made by Sequiris, although neither one are mRNA products. Medscape reported on Feb.23, 2023 that Celldemic had been approved for use in infants six months of age and older if public health officials anticipate a bird flu pandemic, and Incellipan had been approved for use when a bird flu pandemic has been declared.36
mRNA Bird Flu Vaccines A Quick Way to Produce Bird Flu Vaccines
A year ago, Scientific American reported that “vaccine makers are preparing for bird flu,” with one pediatric infectious disease doctor quipping “It’s a really dangerous time to be a bird.” Another expert warned “None of us know when the next influenza pandemic will emerge… At the outset, you have to say there is uncertainty, with one exception: there will be a pandemic.”37 In that article, the reliance on U.S. stockpiled egg-based flu vaccines to produce an H5N1 vaccine was called into question and mRNA technology to produce bird flu vaccine was highlighted because it offers “speed of production” so an mRNA vaccine targeting a new influenza strain can be created in a matter of weeks.
Also in 2023, there was a report in the medical literature that University of Pennsylvania researchers had created an H5N1 mRNA lipid nanoparticle vaccine being tested on mice and ferrets.38 In March 2024, Chinese researchers announced they had created a 10-valent mRNA nanoparticle vaccine encoding proteins from four seasonal influenza viruses, two avian flu viruses with pandemic potential, and spike proteins from four SARS-CoV-2 variants. They said two doses of FLUCOV-10 “elicited robust immune responses in mice” against all 10 vaccine-matched viruses.39
Only Time Will Tell
Amendments to the WHO’s International Health Regulations (IHR) will be voted on at the end of May. Only time will tell whether the latest publicity warning the public about a potentially imminent bird flu outbreak in humans is real or just another bit of propaganda being used to create fear and put pressure on governments to give up sovereignty for the illusion of safety.
1 Bell D. Pandemic preparedness and the road to international fascism. The American Journal of Economics and Sociology July 30, 2023.
2 Nuccio D. Public health agencies must be reined in before next pandemic. Washington Examiner Mar. 29, 2024.
3 Schaefer B, Groves S. The WHO Pandemic Treaty Fails Again. The Heritage Foundation Apr. 19, 2024.
4 Fisher BL. Stop the World Health Organization Power Grab To Mandate Vaccines & Censor Free Speech. National Vaccine Information Center Apr. 11, 2024.
5 Door to Freedom. WHO International Health Regulations Compendium. April 2024.
6 AFP in Geneva. Global pandemic agreement in danger of falling apart,WHO warns. The Guardian Jan. 22, 2024.
7 United Nations. Pandemic experts express concern over avian influenza spread to humans. UN Press Release Apr. 18, 2024.
8 U.S. Centers for Disease Control & Prevention (CDC). Bird Flu Virus Infections in Humans. Apr. 11, 2024.
9 Branswell H. USDA faulted for disclosing scant information about outbreaks of H5N1 avian flu in cattle. STAT News Apr. 18, 2024.
10 Parpia R. Bird Flu Outbreak in Oregon Leads to Mass Euthanization of Poultry. The Vaccine Reaction Feb. 5, 2024.
11 Singler E. H5N1 influenza: From avian to bovine to feline and beyond. AAHA Apr. 19, 2024.
12 Camero K. Is it safe to eat runny eggs amid the bird flu outbreak? Here’s what the experts say. USA Today Apr. 4, 2024.
13 Hendler C. Texas Man and Dairy Cattle Test Positive for Bird Flu. The Vaccine Reaction Apr. 16, 2024.
14 Agence France Presse. H5N1 Strain of Bird Flu Found in Milk: WHO. The Barron’s Daily Apr. 19, 2024.
15 White House. Fact Sheet: Biden-Harris Administration Releases Strategy to Strengthen Global Health Security. Apr. 16, 2024.
16 Staver M. Biden’s Amendments Hand U.S. Sovereignty to the WHO. Liberty Counsel 2023.
17 Human Rights Watch. Draft “Pandemic Treaty” Fails to Protect Rights. Apr. 17, 2024.
18 Webster A. WHO pandemic amendments threaten national sovereignty. Mail Guardian Apr. 17, 2024.
19 NTD. U.S. Representatives speak on “Surrender of U.S. Sovereignty to WHO.” Press Conference Apr. 18. 2024.
20 Professor Massayasu Inoue, MD, PhD video message to the world on harms of mRNA COVID “genetic” vaccine and the WHO pandemic treaty threat to freedom and human rights. NVIC Rumble Channel Apr. 10, 2024.
21 The Gateway Pundit. Massive protests break out in Japan in Opposition to WHO’s proposed pandemic treaty. Apr. 13, 2024. Twitter video of protest in Japan.
22 White House. Fact Sheet: Biden-Harris Administration Releases Strategy to Strengthen Global Health Security. Apr. 16, 2024.
23 Fisher BL. G20 Leaders Pledge to Require Global “Digital Health Certificate” Vaccine Passport. The Vaccine Reaction Nov. 22, 2022.
24 Fisher BL. WHO, Pharma, Gates & Government: Who’s Calling the Shots? National Vaccine Information Center Jan. 27, 2019.
25 Fisher BL. Coronavirus Vaccines on Fast Track as WHO Declares Global Public Health Emergency. National Vaccine Information Center Feb. 5, 2020.
26 Kazis JN. U.S. Could Vaccinate a Fifth of Americans in a Bird Flu Emergency. Barron’s Apr. 20, 2024.
27 Autoimmune Technologies. Gulf War Syndrome: Anti-Squalene Antibodies Link Gulf War Syndrome to Anthrax Vaccine.
28 Kuroda Y, Nacionales DC et al. Autoimmunity induced by adjuvant hydrocarbon oil components of vaccine.Biomed Pharmacother 2004; 58(5): 325-327.
29 Guimaraes LE, Baker B, Perricone C, Shoenfeld Y. Vaccines, adjuvants and autoimmunity. Pharmacological Research 2015; 100: 190-209.
30 Garcon N, Vaughn DW, Didierlaurent AM. Development and evaluation of AS03, an Adjuvant System containing a-tocopherol and squalene in an oil-in-water emulsion. Expert Rev Vaccines 2012; 11(3): 349-366.
31 Miller E, Andrews N et al. Risk of narcolepsy in children and young people receiving AS03 adjuvanted pandemic A/H1N1 2009 influenza vaccine: retrospective analysis. BMJ 2013; 346.
32 Patel SS, Bizjajeva S, Heijnen E, Oberye J. MF59-adjuvanted seasonal trivalent inactivated influenza vaccine: Safety and immunenicity in young children at risk of influenza complications. Int J Infect Dis 2019; 85 (Suppl): S18-S25.
33 Black S. Safety and effectiveness of MF-59 adjuvanted influenza vaccines in children and adults. Vaccine 2015; 33 (Suppl 2): B3-B5.
34 RxLisXie C, Yao R, Xia X. The advances of adjuvants in mRNA vaccines. Npj Vaccines 2023; 8:162.
35 Lee Y, Jeong M, Park J et al. Immunogenicity of lipid nanoparticles and its impact on the efficacy of mRNA vaccines and therapeutics. Exp Mol Med 2023; 55: 2085-2096.
36 Agarwal D. Europe Greenlights Two Avian Flu Vaccines. Medscape Feb. 23, 2024
37 Docter-Loeb H. Vaccine Makers Are Preparing for Bird Flu. Scientific American Mar. 2, 2023.
38 Furey C, Ye N, Kercher L et al. Development of a nucleoside-modified mRNA vaccine against clade 2.3.4.4b H5 highly pathogenic avian influenza virus. bioRxiv Apr. 30, 2023.
39 Wang XC, Ma Q, Li M et al. A 10-valent composite mRNA vaccine against both influenza and COVID-19. bioRxiv Mar. 5, 2024.
The WHO and Pandemic Response – Should Evidence Matter?
REPPARE | BROWNSTONE INSTITUTE | APRIL 22, 2024
The Basics of Policy Development
All public health interventions have costs and benefits, and normally these are carefully weighed based on evidence from previous interventions, supplemented by expert opinion where such evidence is limited. Such careful appraisal is particularly important where the negative effects of interventions include human rights restrictions and long-term consequences through impoverishment.
Responses to pandemics are an obvious example. The world has just emerged from the Covid-19 event, which should have provided an excellent example, as broad new restrictive interventions were widely imposed on populations, while some countries offer good comparators by avoiding most of these restrictions.
The WHO calls such measures Public Health and Social Measures (PHSM), also using the largely synonymous term non-pharmaceutical interventions (NPI). Even if we assume that countries will continue to enjoy full sovereignty over their national policies, WHO recommendations matter, if only because of epistemic authority or shaping of expectations. In 2021, the WHO established a PHSM Working Group which is currently developing a research agenda on the effects of PHSM. As part of this remit, it is expected that the WHO will re-examine their recommendations on PHSM rigorously to reflect the lessons from Covid-19. This process is envisaged to be completed by 2030.
It is therefore curious that the WHO, without providing any comparison of cost and benefit from Covid-19, concluded a 2023 meeting with public health stakeholders from 21 countries with a call to action on all countries “to position PHSM as an essential countermeasure alongside vaccines and therapeutics for epidemic and pandemic preparedness and response.” With Member States due to vote in late May to make WHO recommendations within the International Health Regulations (IHR) effectively binding, “undertaking to follow the Director General’s recommendations before they are given, one would expect these recommendations would be based on a thorough and transparent review that justifies their imposition.”
IHR Benchmarks
In 2019, the WHO defined ‘benchmarks for International Health Regulations (IHR) capacities,’ which did not include PHSM. Although the IHR are still being revised, the benchmarks have been updated in 2024 as ‘benchmarks for strengthening health emergency capacities.’ The update includes new benchmarks on PHSM, which are stated by the WHO to “play an immediate and critical role throughout the different stages of health emergencies and contribute to decreasing the burden on health systems so that essential health services can continue and effective vaccines and therapeutics can be developed and deployed with their effects maximized to protect the health of communities.”
In the new document, PHSM are said to “range from surveillance, contact tracing, mask wearing and physical distancing to social measures, such as restricting mass gatherings and modifying school and business openings and closures.” A new benchmark on PHSM has been included. For example, to meet the level of “demonstrated capacity,” States are now expected to “review and adjust PHSM policies and implementation based on timely and regular assessment of data” and to “establish whole-of-government mechanisms with well-defined governance and mandates to implement relevant PHSM.”
However, the document also acknowledges that PHSM can have “unintended negative consequences on the health and well-being of individuals, societies and economies, such as by increasing loneliness, food insecurity, the risk of domestic violence and reducing household income and productivity” [i.e. increase poverty]. Accordingly, another new benchmark has been introduced: “The protection of livelihoods, business continuity and continuity of education and learning systems is in place and functional during health emergencies.” Disruptions particularly to schooling now seem to be expected during health emergencies as reflected in benchmarks involving “policies for alternative modalities to deliver school meals and other school-linked and school-based social protection when schools are closed due to emergencies.” While potentially being rooted in an acknowledgement of the harms of the Covid-19 response, this benchmark also illustrates the extent to which the Covid-19 event now shapes the idea of what a pandemic response looks like. No other pandemic or health emergency was ever addressed through similarly prolonged disruptions to the economy or to education.
Furthermore, benchmarks on border control measures now expect States to “develop or update legislation (relevant to screening, quarantine, testing, contact tracing, etc.) to enable the implementation of international travel related measures.” To meet the “demonstrated capacity” benchmark, States must “establish isolation units to isolate and quarantine suspected human or animal cases of communicable diseases.”
Due Research
These new benchmarks illustrate a remarkable departure from WHO’s pre-Covid guidelines. The most detailed such recommendations were laid out in a 2019 document based on a systematic review of non-pharmaceutical interventions for pandemic influenza. Despite SARS-CoV-2 spreading similarly to influenza, these guidelines have been widely ignored since 2020. For example, the 2019 document stated that border closures, or quarantining healthy contact persons or travellers were “not recommended in any circumstances.” The isolation of patients was recommended to be voluntary noting that workplace closures of even 7-10 days may disproportionately harm low-income people.
Prior to 2020, most discussed PHSM now proposed by the WHO had never been implemented at large scale and data on their effects was accordingly scarce. For example, the 2019 review recommended wearing masks when symptomatic and in contact to others, and even “conditionally recommended” wearing masks when asymptomatic during severe pandemics purely based on “mechanistic plausibility.” Indeed, two meta-analyses of randomized controlled trials (RCTs) of face masks published in 2020 found no significant reduction in influenza transmission or influenza-like illness.
Today, we have an abundance of evidence on the effects of PHSM during the Covid era. Yet, there could hardly be more disagreement regarding efficacy. A Royal Society report concluded that lockdowns and mask mandates decreased transmission and their stringency was correlated with their effectiveness. Meanwhile, a meta-analysis estimated the average lockdown in Europe and North America to have reduced Covid mortality by merely three percent in the short term (at high cost) and an updated Cochrane Review still found no evidence for the effectiveness of masks in community settings (let alone mask mandates) in RCTs. The lower level of restrictions in Nordic countries was associated with some of the lowest excess all-cause mortality in the world between 2020 and 2022, including Sweden which never resorted to general lockdowns or mask mandates.
New Recommendations
Notwithstanding the variable evidence of effectiveness and harm, and the ongoing 7-year WHO review process, the WHO has begun to revise recommendations on PHSM. The first publication of the WHO’s newly launched initiative Preparedness and Resilience for Emerging Threats (PRET), titled ‘Planning for respiratory pathogen pandemics,’ advocates for a “precautionary approach to infection prevention early in the event” that “will save lives” and tells policy makers to “be ready to apply stringent PHSM, but for a limited time period in order to minimize associated unintended health, livelihood and other socio-economic consequences.” These recommendations are not founded on any systematic review of new evidence, as was attempted in the 2019 influenza guidance, but largely on unstructured, opinion-based “lessons learned” compilations of committees convened by the WHO.
The 2023 version of the WHO’s ‘Managing Epidemics’ handbook, first published in 2018 and intended to inform WHO country staff and health ministries, illustrates this lack of evidence-base. Comparing both editions of the same document shows a marked normalization of Covid-19-era PHSM. For instance, the earlier version recommended sick people wear masks during severe pandemics as an “extreme measure.” The revised handbook now recommends masking everyone, sick or healthy, not merely during severe pandemics but even for seasonal influenza. Covering of faces is clearly no longer considered an “extreme measure” but normalized and portrayed as similar to hand washing.
Elsewhere, the 2018 version of ‘Managing Epidemics’ stated:
We have also seen that many traditional containment measures are no longer efficient. They should therefore be re-examined in the light of people’s expectations of more freedom, including freedom of movement. Measures such as quarantine, for example, once regarded as a matter of fact, would be unacceptable to many populations today.
The 2023 edition revises this to:
We have also seen that many traditional containment measures are challenging to put in place and sustain. Measures such as quarantine can be at odds with people’s expectations of more freedom, including freedom of movement. Digital technologies for contact tracing became common in response to Covid-19. These, however, come with privacy, security and ethical concerns. Containment measures should be re-examined in partnership with the communities they impact.
The WHO no longer considers quarantine inefficient and unacceptable, but merely “challenging to put in place and sustain” because it can be at odds with people’s expectations.
A new section on “infodemics” gives advice on how to manage people’s expectations. States are now encouraged to set up an “infodemic management team” that shall “debunk misinformation and disinformation that could have a negative health impact on people and communities, while respecting their freedom of expression.” Again, evidence is not provided as to why this new area of recommendations are needed, how ‘truth’ is arbitrated in such complex and heterogeneous situations, or how potential negative effects of stifling exchange of information and discussion of complex issues will be addressed.
Infodemic Management in Practice
Tedros Adhanom Ghebreyesus, the WHO’s Director-General recently reassured the world in a speech:
Let me be clear: WHO did not impose anything on anyone during the Covid-19 pandemic. Not lockdowns, not mask mandates, not vaccine mandates. We don’t have the power to do that, we don’t want it, and we’re not trying to get it. Our job is to support governments with evidence-based guidance, advice and, when needed, supplies, to help them protect their people.
This is not the only example of the WHO adopting a proactive strategy of “infodemic management” as it recommends States to do. The latest draft of the Pandemic Agreement includes a new paragraph:
Nothing in the WHO Pandemic Agreement shall be interpreted as providing the Secretariat of the World Health Organization, including the WHO Director-General, any authority to direct, order, alter or otherwise prescribe the domestic laws or policies of any Party, or to mandate or otherwise impose any requirements that Parties take specific actions, such as ban or accept travellers, impose vaccination mandates or therapeutic or diagnostic measures, or implement lockdowns.
The latter claim is particularly noteworthy because it ignores the proposed IHR amendments accompanying the pandemic agreement, through which countries will undertake to follow future recommendations on PHSM within a legally binding agreement, while the Pandemic Agreement does not include any such propositions.
The WHO promises to ‘support governments with evidence-based guidance’ but appears to be promoting PHSM recommendations that conflict with their own guidance without any apparent new evidence base. Given that countries did well without following highly restrictive measures, and the long-term impacts of reduced education and economic health on human health, the principle of “do no harm” would seem to demand more caution in applying such consequential policies. Policies need an evidence base to justify their adoption. Given the trajectory of natural outbreaks, contrary to WHO claims, is not increasing, it seems pertinent to expect one from the WHO before they push Member States to risk the health and economic well-being of their populations next time a pandemic or health emergency is declared.
REPPARE (REevaluating the Pandemic Preparedness And REsponse agenda) involves a multidisciplinary team convened by the University of Leeds.
‘Misinformation’ and ‘disinformation’ in the pandemic treaty
European Parliament – 9.4.2024
Priority question for written answer P-001044/2024
to the Commission
Rule 138
Robert Roos (ECR), Angel Dzhambazki (ECR), Tom Vandendriessche (ID), Mislav Kolakušić (NI), Ivan Vilibor Sinčić (NI), Jorge Buxadé Villalba (ECR), Francesca Donato (NI), Margarita de la Pisa Carrión (ECR), Hermann Tertsch (ECR)
The Commission is negotiating an international agreement on ‘pandemic preparedness and response’ with WHO countries.
In the draft text as amended by the EU drafting suggestions[1] dated 27 February 2024, Article 18 on communication and public awareness relies on the concepts of ‘misinformation’ and ‘disinformation’.
Signatory countries should act ‘with the aim of countering’ (Article 18(1)) and ‘cooperate in preventing’ (Article 18(4)) misinformation or disinformation, with the Commission suggesting an amendment to oblige countries ‘to develop effective tools to identify and counteract misinformation and disinformation’ (Article 18(4)).
However, neither the draft agreement nor international law provide a definition of ‘misinformation’ or ‘disinformation’.
- 1. Can the Commission define these concepts and explain how they should be understood, in the Commission’s view, taking into account the requirement to comply with the principle of legal certainty, which is an essential component of the rule of law principle and according to which the law must be certain, foreseeable and easy to understand?
- 2. In the Commission’s view, do the proposed obligations under Articles 18(1) and 18(4) entail restricting citizens’ fundamental right to freedom of expression, and if so, are these restrictions compatible with the applicable law, including the case law of the European Court of Human Rights?
Supporter[2]
Submitted:9.4.2024
WHO: Intel Agency for Gates Foundation?
Examining the Foundation’s prescient August 2019 purchase of BioNTech stock
By John Leake | Courageous Discourse™ | April 22, 2024
Reviewing BioNTech’s Disclosure of Classes of Share Capital for the year ended December 31, 2019, I noticed the following:
On August 30, 2019, BioNTech entered into agreements with the Bill & Melinda Gates Foundation (BMGF). BMGF agreed to purchase 3,038,674 ordinary shares with nominal amount of k€ 3,039 of BioNTech for a total of k€49,864 (k$55,000). These agreements require BioNTech to perform certain research and development activities to advance the development of products for the prevention and treatment of HIV and tuberculosis. In the event of a breach of the underlying conditions, including such research and development activities, BMGF has the right to sell its shares back to BioNTech at the initial share price or fair market value, whichever is higher, subject to certain conditions. BioNTech’s ability to pay dividends is also limited under the terms of these agreements.
Less than two years after the Gates Foundation purchased the stock (pre-IPO) at $18 per share, it peaked on Aug. 6, 2021 at $389. At that price, the Foundation’s $55 million investment was worth $1,182,044,186.00 ($1.182 billion).
On September 18, 2019—just nineteen days after the Gates Foundation took its huge position in BioNTech stock— a report titled A World At Risk was published by the Global Preparedness Monitoring Board, which was founded in 2018 by the World Bank Group and the World Health Organization.
The report’s title page is illustrated with an image of a coronavirus, and its text is an urgent call to action for the world to invest far more in preparedness for a respiratory viral pandemic. As the report states on page 8:

The report mentions nothing about the need to invest in bolstering bio-laboratory safety. It expressly warns about the threat of a lethal respiratory pathogen “accidentally or deliberately released,” but its entire call to action is to invest a fortune to responding to such a pathogen instead of preventing it from being released in the first place.
This was in spite of numerous urgent warnings from Rutgers University biology professor Richard Ebright and others that many of the world’s bio-labs had a history of grave security lapses that were NOT being adequately addressed. In 2017, Professor Ebright expressed particular concern about the new BSL-4 lab that was about to open in Wuhan, China.
We now know that SARS-CoV-2 was officially detected in December of 2019 but probably emerged and started spreading in August or September of 2019—that is, around the same time A World At Risk was published.
The September 18, 2019 date of the report strongly suggests that someone doing bio-surveillance for the WHO in China obtained intelligence that a SARS coronavirus was already circulating.
Given that the Gates Foundation is the WHO’s second largest donor (after Germany, where BioNTech is headquartered) I wonder if this intelligence was passed to someone in the Gates Foundation months before December 31, 2019—the date the WHO claimed it received its first report of cases of pneumonia of unknown etiology in Wuhan.
Does the WHO—with its Country Offices obtaining bio-surveillance reports from the field—serve an an unofficial intelligence agency for the Gates Foundation?
If so, it would enable the Foundation to obtain extremely valuable information about emerging infectious disease pathogens—naturally emergent or accidentally or deliberately released—long before other market players obtain this information.
Dutch Parliament instructs government to demand a delay in both WHO votes – and if no delay, to reject the proposals
BY MERYL NASS | APRIL 16, 2024
MOTION BY MEMBER of the Dutch Parliament Mona KEIJZER ET AL.
Proposed April 10, 2024. A majority voted in favour April 16, 2024
After hearing the deliberations, noting that both the Working Group International Health Regulations (WGIHR) and the International Negotiating Body (INB) are authorized to deliver the final legal formulation of the envisaged amendments to the International Health Regulations (IHR) and the Pandemic Treaty to the 77th World Health Assembly (WHA), which will take place at the end of May 2024; noting that this process is proceeding at an unprecedented pace, whereas such far-reaching measures require more time to be considered, reviewed and properly implemented; whereas ignoring procedural obligations under IHR and leaving unclear the link between the amended IHR and the new pandemic treaty undermines the international legal order and thus the democratic legitimacy of this regulation in violation of Article 55 of the IHR, which requires proposed amendments to be submitted to the Contracting States at least four months before deliberation and voting in the WHA; whereas this does not provide sufficient opportunity to examine the changes and their important legal, health, economic, financial and human rights implications; whereas the request to adopt the amendments to the IHR or the text of the envisaged pandemic treaty is not in line with the UN principles and guidelines; instructs the government to request a postponement of the vote on the amendments and thus on the IHR and the new pandemic treaty at the World Health Assembly and, if this postponement is not obtained, to vote against the proposed amendments to the IHR and the new pandemic treaty as a whole; and proceeds to the order of the day.
Mona Keijzer, Daniëlle Jansen, Fleur Agema Members Dutch Parliament
Generating the “national will” to spend hundreds of billions and cede civil and human rights
The 25 year history of how this was foisted on us on the altar of pandemic safety. And how the WHO has repeatedly failed upward.
BY MERYL NASS | APRIL 13, 2024
Bill Clinton Begins the Phony Era of Pandemics and Bioterrorism
In November 1997 US Secretary of Defense William Cohen held up a 5 lb bag of Domino sugar in front of an army of cameras and told the world that if the bag contained anthrax it could wipe out NYC or Washington, DC.
That was not true, but it provided a fitting justification for the start of the DOD’s “biodefense” vaccine program, begining with mandatory anthrax vaccinations for soldiers in March 1998.
According to an NBC cover story,
“In April 1998, President Bill Clinton read a Richard Preston novel, “The Cobra Event,” about a biological attack on the U.S. using a lethal virus that spreads like the common cold.
“It scared the bejesus out of him,” recalls Kenneth Bernard, a now retired U.S. Public Health Service official who was then representing the U.S. in Geneva at the World Health Organization.”
The USG invested in a new smallpox vaccine, ACAM2000, based on the older Dryvax vaccine. The fact that it caused high rates of myocarditis (1 case in 175 doses administered according to CDC) has been ignored.
And the biodefense era began, supplying handsome contracts to those who promised remedies in the new wild west of biowarfare and infectious disease. Many of those who got the contracts had friends in high places, like FOB Ronald Perelman, who made a killing on a smallpox remedy (Tpoxx) that was eventually used as a monkeypox drug. Did it work? Who knows?
The 21st Century ushered in a well-coordinated push to generate fear about:
- a repeat of the 1918 flu pandemic,
- jumps of deadly viruses from animals to humans (“spillover,” zoonoses and epizootics were the new terms to be mastered), and
- biologic warfare threats
The 2002-3 SARS outbreak and the Avian influenza (bird flu) outbreak — both beginning shortly after the anthrax letters—were hyped to the max to generate fear of pandemics and biological warfare.
How many people did these infectious diseases kill in the US and around the world?
- The anthrax letters caused 5 human deaths, all in the US.
- SARS-1 caused under 800 deaths around the world. There were 27 US cases designated as SARS-1 and not a single US death.
- Avian flu is said to have caused 463 deaths total in the entire world over the past 20 years, according to the WHO. Only 2 Americans have been identified as having an illness associated with avian flu, and both were very minor. Not a single American has died from avian flu. The recent case of conjunctivitis is recovering.
The CDC and mainstream media claim that avian flu has killed over 100 million chickens. It has not. USDA rules have forced growers to cull over 100 million chickens. When one chicken has a positive PCR test for bird flu, every chicken in the chicken house (and sometimes all those on the farm) must be killed. Was that test even accurate? But expansive claims like these are what gets the public going, and putting up with incursions on their freedoms.
So, on the basis of a bioterrorism ‘performance’ using letters containing anthrax spores sent to Congress and the media that were made in a lab, and two relatively minor zoonotic diseases that failed to kill a single American, we Americans were led by the nose into the era of BIODEFENSE.
In 2009 the Pandemic Preparedness/Biosecurity Agenda really took off with an expensive BANG!
The WHO’s Director-General Margaret Chan declared a Pandemic Phase Level 6 for a “swine flu” outbreak that was milder than a normal influenza outbreak: triggering tens of billions of dollars in “sleeper “contracts that the WHO had initiated (and most likely been cut in on) between national governments and vaccine manufacturers. The contracts guaranteed that nations would buy millions or hundreds of millions of doses of vaccines for any future Level 6 pandemic that a WHO Director-General declared.
The contracts did NOT say that the definition of a Level 6 pandemic could be changed so that any new virus at all could meet the definition. But that is what happened. The definition of a level 6 pandemic was changed so that it was meaningless, and a few weeks later Director-General Margaret Chan declared a level 6 pandemic, the contracts were triggered, and on the order of a billion doses of H1N1 flu vaccines were administered. Grandfathered in. Liability-free. Some caused serious side effects: especially the European Pandemrix brand made by GSK. Regulators identified very serious problems early and simply covered them up. Problems like being associated with 10 times higher rates of serious adverse events than other H1N1 vaccines.
Drugs were also ushered in without a license. Here is some archived information on the drugs and other products given EUAs for the mild 2009 swine flu.

Having wrought great harm in 2009, the WHO bounced to another debacle with West Africa’s Ebola pandemic of 2014. Below I have excerpted from a Royal Society opinion piece, but there are many others that provided strong criticisms of the WHO response, including from some of the WHO’s strongest supporters. It seems that really bad mistakes can lead to calls for reform and a bigger budget. We’ve seen Congress “solve” problems this way all the time. Then those “reform” efforts can be used to move an organization in the new desired direction. In this case, the WHO was maneuvered in the biodefense direction.
Reading the article below, it appears that the WHO is an inept, disorganized bureaucracy that has a large stable of authors to write policy briefs, press releases and has other employees who put on conferences. But the WHO has little understanding of actual epidemics and does not like to dirty its hands tending to them on the ground.
What did the UK Royal Society publish about the WHO’s response to West Africa’s Ebola pandemic?
https://royalsocietypublishing.org/doi/full/10.1098/rstb.2016.0307

Extract:
However, after the initial errors of downplaying the outbreak [26], the WHO did maintain continued activity in tackling Ebola. The WHO documents its role in training healthcare workers and burial teams in infection control, community engagement activities and providing epidemiological data [27]. Furthermore, the organization published numerous technical guidance documents, hosted a series of meetings on vaccine options, developed diagnostic tools and expanded laboratory services [21, p. 1309]. Yet none of these activities provided direct patient care, strategic managerial oversight or the infection control that the outbreak response needed. Ultimately, due to a vacuum of international leadership in the operational response (which several in the international community expected the WHO to perform), the patient care, infection control and management were left to others, including Médecins Sans Frontières (MSF), a new UN body (United Nations Mission for Ebola Emergency Response—UNMEER) and even the domestic and international militaries [10,19,28].
All reviews attribute some blame to the World Health Organization (WHO) for its delay to take action and for a lack of an operational response in the outbreak. However, while the WHO made some pivotal mistakes, as it itself admits [8], the outbreak exposed tensions between the normative and operational roles of the WHO, and furthermore between what the WHO is able to do (suffering from financial and organizational constraints) and what the global community expects the WHO to do.
The WHO admitted:
“The initial response was slow and insufficient, we were not aggressive in alerting the world, our surge capacity was limited, [I would suggest that WHO staff chose not to endanger themselves or that WHO was instructed to allow the Ebola outbreak to expand across Africa—Nass] we did not work effectively in coordination with other partners, there were shortcomings in risk communication, and there was confusion of role and responsibilities at the three levels [Headquarters, Regional Office and Country Offices] of the organisation [20,21].”
… despite the launch of a WHO Roadmap in August 2014 strategizing the end of the epidemic within six to nine months, [the WHO is full of planners, but has a dearth of doers—Nass] a coordinated international response with WHO at the helm failed to materialize [25] with the outbreak rapidly developing into a humanitarian emergency.
So, the WHO has been failing upward with every global infectious disease crisis for at least the past 20 years, well before COVID.
What does the organization offer us? Apart from providing a hook for globalists to gain more power, control and wealth, the WHO offers nothing to the citizens of developed nations. It does provide some benefits to developing nations, but those benefits could probably be achieved at a much lower cost, and with preferable local decision-making and control, through another organization or through health ministries.
As Dr. Inouye has said and written, it is time for us to Exit the WHO.
Massive Rallies Break Out in Japan Against WHO’s Pandemic Treaty
PharmaFiles by Aussie17 | April 13, 2024
April 13, 2024, will be etched in the annals of modern Japanese history as tens of thousands of citizens across the nation came together in a series of pandemic rallies. The protests centered on the widespread opposition to the Pandemic Treaty, with escalating concerns over “infectious disease” and “public health” becoming potent tools for an unprecedented push towards what is perceived by many as a totalitarian surveillance society.
From the bustling streets of Ikebukuro to the gatherings at Higashi-Ikebukuro Central Park, the sheer scale of participation speaks volumes. Organizers aimed for a monumental turnout of 100,000 protesters to demand answers on crucial issues, such as the stark increase in excess deaths and the lack of transparency on the adverse effects following vaccinations.
The protest not just opposed potential mandatory vaccinations but also the perceived overreach of health authorities and their ties with global pharma, echoing a distressing sentiment of disenfranchisement among the populace. Demonstrators criticized the lack of explanations for a sharp increase in excess deaths and demanded accountability and clarity on vaccine-related casualties.
Eminent speakers, including Professor Masayasu Inoue and modern history researcher Chikatsu Hayashi, provided compelling pre-demonstration speeches that laid bare the concerning dynamics between global health authorities and pharmaceutical agendas. Professor Inoue highlighted the concerning trend of our health being weaponized in what he termed as “a third world war fought with information.” He urged the public to resist introducing genetic vaccines into their bodies, implicating a significant portion of WHO’s funding comes from pharmaceutical giants and private interests like the Bill Gates Foundation. This follows Japan’s Message to the World delivered by Prof Inoue a few days ago.
Modern history researcher Prof Chikatsu Hayashi’s address was a rallying cry to resist the encroaching shadows of global totalitarianism, symbolically referring to the proactive stance against it as “stopping the third atomic bomb with our hands.” His poignant discourse highlighted a national movement poised against not only the Pandemic Treaty but also the underlying structures threatening Japan’s sovereignty and the well-being of its citizens.
April 13 marked not just a protest against a treaty but a stand against a future where health becomes a lever for control and surveillance. The massive turnout signifies a critical moment in Japan’s civic engagement. It’s a call from its people for autonomy, transparency, and the reassessment of global health governance that resonates beyond its borders. Today, Japan stands at the forefront, questioning, challenging, and seeking change for a future where health policy respects national sovereignty and individual rights.
Signing off for now
A17
The dramatic mismanagement of the Covid-19 pandemic must finally seal the fate of the WHO (We Host Obtuseness)!
By Geert Vanden Bossche | Voice for Science and Solidarity | April 11, 2024
About ten years ago, there were serious discussions about dismantling the WHO due to its mismanagement of the Ebola epidemic in West Africa. An even more dramatic mismanagement of the Covid-19 pandemic must now finally seal the fate of this organization!
I still have serious doubts about whether the Covid-19 pandemic was planned; it certainly wasn’t orchestrated by the Vaccine Industry. Moreover, it’s also difficult to reconcile the broadly approved effort of the Vaccine Industry to develop a vaccine with the notion of a powerful lobby harboring nefarious intentions. Back then, no one anticipated, indeed, that vaccination during a pandemic could worsen its spread and health impact, given past successes in curbing infection chains through vaccination during pandemics or epidemics.
Nobody ever officially reported, though, that in the case of these alleged success stories (such as Smallpox and Ebola), deaths of contacts of index cases ring-vaccinated with replicating vaccines during the incubation time of the disease substantially contributed to halting viral transmission. Consequently, the WHO erroneously believed that vaccination during a pandemic or epidemic was a highly effective strategy for ending it.
‘Regrettably’(?!), in the mass Covid-19 vaccination program, this never-investigated or mentioned ‘killing effect’ didn’t materialize, as the vaccines used were non-replicating and the ring vaccination protocol didn’t apply, considering that the transmission of this virus is airborne rather than via direct contact. Therefore, I strongly believe that the egregious incompetence of the WHO is at the heart of the mismanagement of this pandemic. It’s only right that such a screw-up should vanish from the face of this earth.
Big Pharma designed WHO’s Global Health Policy from 2000-2009
Corruption and deception, not science, is the foundation of WHO health policy
By Judy Wilyman PhD | Vaccination Decisions | April 1, 2024
“The past was erased, the erasure was forgotten, the lie became truth.” – George Orwell, 1984
The history of the GAVI alliance, a board that influences the direction and design of WHO’s global health policies, illustrates how these policies have been directly influenced by industry partners from 2000-2009, and not by an objective board selected by the WHO.
This direct influence was hidden from the public in 2009 when the alliance became known as the Gavi board. At this time its composition and function changed to hide the role that industry had played from 2000-2009 in changing the direction of global health policies to a new focus on vaccine production and global implementation.
History of the Gavi Board:
In 1998 the Global Alliance for Vaccines and Immunisation (GAVI) was established by the Head of the World Bank after a meeting with pharmaceutical companies and other agencies. The GAVI alliance was established on the advice of industry because the pharmaceutical companies were claiming that there was no incentive for them to provide vaccines to the developing countries.
This meeting led to the Bill and Melinda Gates Foundation providing the seed funding of $750 million in 1999 and governments then matched this figure to establish an alliance of private-public partnerships in 2000, to fund the vaccination programmes for all countries.
In 2000 the alliance was launched at the World Economic Forum (WEF), not the World Health Organisation (WHO), and it established a working party to work with the WHO to design the International Health Regulations (IHR), yet it was a body established outside of the WHO’s charter.
At this time all stakeholders in the Global Alliance for Vaccines and Immunisation (GAVI) were able to directly influence the design of the WHO’s Global Health Policies through this working party (2000-2009), including the International Federation of Pharmaceutical Manufacturers and Associations (IFPMA). They could attend meetings and present information for policy development.
Other stakeholders in the GAVI at this time included the BMGF, the Rockefeller Foundation, the World Bank and the International Monetary Fund (IMF). The influence of these stakeholders led to a new focus on vaccine production and implementation in the WHO’s global health policies.
These global policies were presented to countries in the International Health Regulations (IHR) that came into force in June 2007.
This direct influence of all stakeholders changed in 2009 when the GAVI alliance became known as the GAVI board. Its composition was changed to include only four permanent board members – UNICEF, BMGF, the World Bank and WHO – and other partners would be on a part-time basis.
This change to only four permanent board members, one of which was now the WHO, hides the fact that from 2000-2009 all stakeholders were able to directly influence the design of WHO’s global health policies.
The first recorded meeting of the Gavi board on its website is in 2009. It describes the role of the Gavi board as ‘being responsible for strategic direction and policy-making, oversees the operations of the Vaccine Alliance and monitors programme implementation’ .
This alliance of partners, many of whom profit from vaccines, make donations to the Gavi board and still influence global health policies in a more indirect fashion.
The WHO’s IHR are currently being amended with strong influence from this corporate alliance. If the amendments are approved, the draconian directives implemented during the COVID ‘pandemic’ years, will become binding on every WHO member country, whenever the director of the WHO declares another pandemic. This is removing fundamental human rights and objective scientific evidence from global health policies.
It is time for Australians to make our voices heard to ensure that Australia exits the WHO and joins the World Council for Health to protect both human health and fundamental human rights in all public health policies.
[The information above can be referenced from Ch 3 of my PhD 2015]
Important Information:
- Here is the witness statement from ex-Qantas pilot, Captain Graham Hood, describing that lack of evidence for safety and efficacy that was used by the Australian Therapeutic Goods Administration (TGA) and the Australian Prime Minister, Scott Morrison, to mandate this mRNA genetically-engineered injection (called a ‘vaccine’) in the Australian population – Ex-Qantas Pilot, Graham Hood, provides a witness statement in the Australian parliament.
- Australian Medical Professional Society (AMPS) presents ‘Too Many Dead’ in Australia, but the Australian government will not investigate and the media does not report these facts.
- Study finds the Majority of Patients with Long COVID were Vaccinated
- Epidemic of Fraud
Globalism and Disease X
By Meryl Nass | March 30, 2024
What is biowarfare? COVID was due to a biological warfare agent. It was designed in one or more laboratories to be more virulent than its natural precursors:
- to prefer to infect humans;
- to infect more organs than possible in naturally occurring strains;
- to interfere with the body’s immune responses.
I say one or more laboratories becasue many of its features had been previously discovered or created in various laboratories, and then these features were essentially grafted onto a coronavirus, one by one; or some features were achieved by passaging the virus through humanized mice, other humanized animals, human cell tissue cultures or humans themselves.
Why were these features created? In which labs?
Why were they painstakingly added to a coronavirus backbone? Where was this done and how many labs were involved?
Why was a coverup by western scientists so critical? Because claiming that pandemics come from animals living in nature, and are spread to humans due to our incursions into their territory, was needed to justify the entire biosecurity agenda that the WHO is steamrolling over us.
By the way, the newest version of the treaty (released March 7, 2024) states that part of the WHO plan is to “identify” those areas where disease “spillover” occurs. You watch: the WHO will then empty those areas of humans. It really is a great cover story, “spillover.” Except it is a total lie.
_____________________
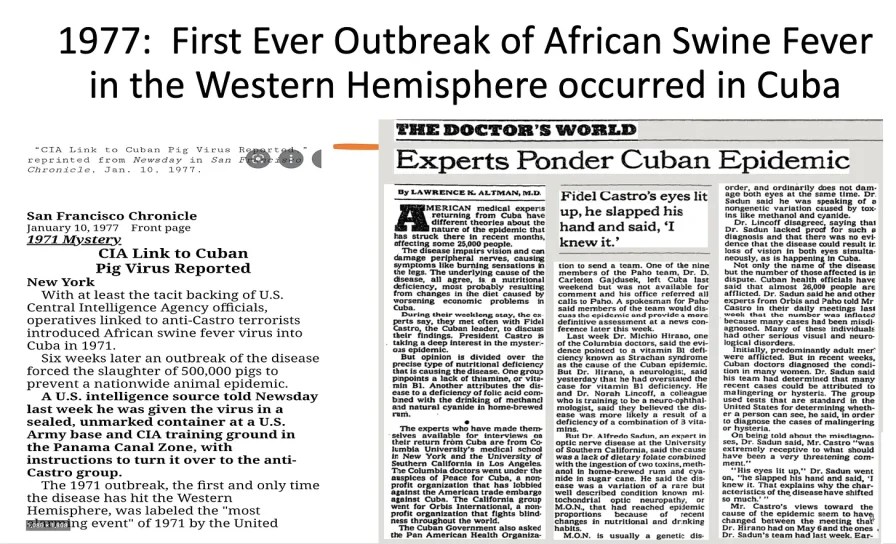
Historically most biowarfare agents were naturally occurring viruses or bacteria. Here is one example in which whistleblowers identified the hand of the CIA.
It is “gain-of-function” research that makes them more virulent and/or more transmissible. Gain of function research was considered illegal under international law until about 2001, and then the customary norms of national behavior simply changed, after the US was caught ignoring the usual norms—as revealed in the NYT on 9/4/2001 and in the book GERMS.
The WHO suggested it should be put in charge of gain-of-function research in the pandemic treaty draft that was released on February 14, 2024. It only took 3 weeks before a new draft was issued on March 7, 2024 in which all mention of “gain-of-function” was erased. I wonder if the rapidity of release of the next draft (it usually takes about 3 months to get a new draft) had to do with cutting out the Gain-of-Function section.
But the idea of requiring nations to supply the WHO with samples of potential pandemic pathogens, and to upload their genetic sequences to publicly accessible databases asap remained, was discussed with even more details in the newest March 7 draft. The WHO and nations would be free to share biological warfare agents aka potential pandemic pathogens (essentially) with anyone they liked.
This makes no sense any way you look at it. The goal seems to be a situation where “Pandemics R Us” and they appear frequently, with no ability to tell where they came from or whether they were deliberate or an accident. By sharing them all globally the WHO has paved the way for using the alibi of accidental release for future COVIDs.
The biowarfare segment starts at about 26 minutes into the episode.
As I said, we at DoortoFreedom.org are here to help you educate your lawmakers while you urge them to question this effort publicly, introduce resolutions, and in other ways throw some boulders in front of the steamroller, just like Louisiana’s Senate did this week.
merylnass@gmail.com
Bill Blocking WHO, UN, and WEF from Imposing ‘Rule, Regulation, Fee, Tax, Policy, or Mandate of Any Kind’ Passes Louisiana Senate
BY JON FLEETWOOD | MARCH 27, 2024
In a landmark move on Tuesday for State sovereignty and local governance, the Louisiana Senate passed Senate Bill No. 133, a piece of legislation aimed at significantly limiting the influence and jurisdiction of certain international organizations within the state.
The bill passed unanimously with 37 ‘yes’ votes.
Not one senator voted against it.
Sponsored by Republicans, Senators Pressly and Valarie Hodges, along with Representative Edmonston, the bill explicitly targets the World Health Organization (WHO), United Nations (UN), and the World Economic Forum (WEF), restricting their power and the enforcement of their policies in Louisiana.
The bill, set to take effect on August 1, 2024, mandates that “the World Health Organization, United Nations, and the World Economic Forum shall have no jurisdiction or power within the state of Louisiana.”
The legislation marks a decisive stance against undue influence from these international bodies.
Further detailing its scope, the bill asserts, “No rule, regulation, fee, tax, policy, or mandate of any kind of the World Health Organization, United Nations, and the World Economic Forum shall be enforced or implemented by the state of Louisiana or any agency, department, board, commission, political subdivision, governmental entity of the state, parish, municipality, or any other political entity.”
The move addresses state sovereignty and the role of international organizations in local governance.
Proponents argue that this bill is a necessary step to safeguard Louisiana’s autonomy and prevent the imposition of external policies that may not align with the state’s interests or values.
The bill’s passage reflects a broader trend of skepticism toward global institutions and a preference for localized control over public affairs.
As the legislation prepares to be voted on in the House, all eyes will be on Louisiana to see the practical implications of this bold legislative move should it pass.
The bill is a clear declaration of Louisiana’s intent to chart its own course, free from the influence of selected international organizations.
With its enactment, the state legislature underscores its commitment to preserving state rights and governance free from what it views as unwarranted external interference.
You can read the full bill here:
Is Russia sending the WHO a shot across the bow?
“Thinning of humanity,” lack of accountability and WHO coverups are all mentioned in a few sentences. What might this portend?
BY MERYL NASS | MARCH 28, 2024
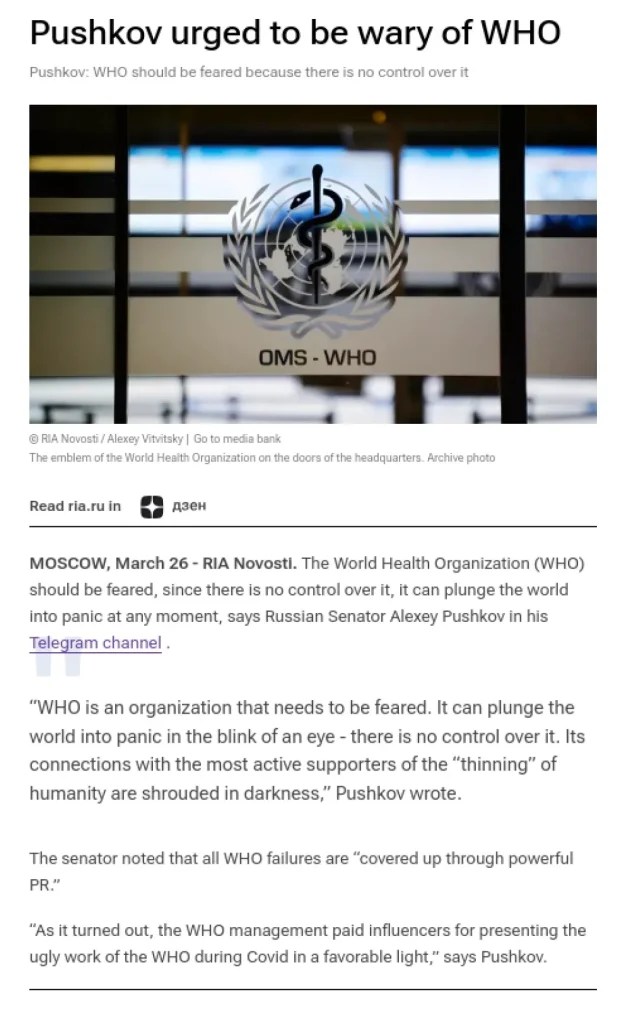
 Russian Senator Aleksey Pushkov took to Telegram to complain about the WHO, and then RIA Novosti reported on it.
Russian Senator Aleksey Pushkov took to Telegram to complain about the WHO, and then RIA Novosti reported on it.
What is RIA Novosti ? “RIA Novosti is the most cited Russian news agency in the mass media and across social media.”
Who is Pushkov? Below is his bio; but important to note that he is also claimed to be a good friend of Vladimir Putin.
Aleksey Konstantinovich Pushkov, born 10 August 1954, is a Russian politician who has been Senator from Perm Krai since 29 September 2016. He is also a former Deputy of the State Duma and former head of the Foreign Affairs Committee in the State Duma, the lower house of the Russian Parliament. As a member of the United Russia political party in the federation council, he is the chairman of the Commission on Information Policy.
What did Pushkov say, and how was it reported? Here is what RIA reported in English:
Featured Video
Maria Farmer: Epstein victim reveals explosive information covered up by media
or go to
Aletho News Archives – Video-Images
From the Archives
Netanyahu Is Leading US President Trump to War with Iran
By Prof. James Petras | Global Research | October 27, 2017
Introduction
Israeli Prime Minister Benjamin Netanyahu and the Presidents of the 52 Major Jewish American Organizations are leading President Trump, like a puppy on a leash, into a major war with Iran. The hysterical ’52 Presidents’ and ‘Bibi’ Netanyahu are busy manufacturing Holocaust-level predictions that a non-nuclear Iran is preparing to ‘vaporize’ Israel. The buffoonish US President Trump has swallowed this fantasy wholesale and is pushing our nation toward war for the sake of Israel and its US-based supporters and agents. We will cite ten recent examples of Israeli-authored policies, implemented by Trump in his march to war (there are scores of others). … continue
Blog Roll
 Aletho News
Aletho News- Pax Judaica Explained | Prof. David Miller
- Was MAHA Too Good to Last in the Trump Administration?
- Vermont advances bill letting unelected Health Commissioner decide which vaccines ctizens should receive
- Why the US-Israeli alliance will lose against Iran
- US envoy Huckabee claims Israel has ‘biblical right’ to conquer all West Asia
- Testing the Alliance: Netanyahu’s Washington Visit
- Britain is once again poisoning peace diplomacy with Russia and fueling war in Europe
- Russian fuel tanker to test US sanctions amid Cuba crisis
- EU state issues ultimatum to Zelensky over Russian oil supplies
- Maria Farmer: Epstein Victim Reveals Explosive Information Covered Up by Media
- If Americans Knew
- Ominous messaging from Trump’s “Board of Peace” – Not a ceasefire Day 134
- ‘Christians Out’: Jerusalem Church Tagged With Hate Graffiti, Police Investigating
- Israeli Settlers Kill American Teen
- ‘We returned from hell’: Palestinian journalists recount torture in Israeli prisons
- No mercy for Gaza in Ramadan – Not a ceasefire Day 133
- The Israeli Government Installed and Maintained Security System at Epstein Apartment
- Tucker Carlson interrogated in Israel, has passport seized after interviewing US ambassador
- 6,000 Amputees in Gaza Face Impossible Recovery amid Israeli War Ultimatum
- The Lancet: Gaza death toll far higher than reported – Not a ceasefire Day 132
- Compliant aid: Who are the Israel-approved NGOs scaling up in Gaza?
- No Tricks Zone
- Germany: Electric Car Catches Fire At Charging Station, Sets Off Local “Inferno”, Widespread Damage
- New Study: Canada’s New Brunswick Was 1°C Warmer Than Today During The Medieval Warm Period
- Coal Power Back In Trend As Globe Tries To Keep Pace With Growing Demand For Power
- New Study: A 4°C Warmer Beaufort Sea Had ‘No Sea Ice’ 11,700 – 8200 Years Ago
- Unfudging The Data: Dutch Meteorological Institute Reinstates Early 20th Centruy Heat Waves It Had Erased Earlier
- German Gas Crisis…Chancellor Merz Allegedly Bans Gas Debate Ahead of Elections!
- Pollen Reconstructions Show The Last Glacial’s Warming Events Were Global, 10x Greater Than Modern
- Germany’s Natural Gas Storage Level Dwindles To Just 28%… Increasingly Critical
- New Study Rebuts The Assumption That Anthropogenic CO2 Molecules Have ‘Special’ Properties
- Climate Scientist Who Predicted End Of “Heavy Frost And Snow” Now Refuses Media Inquiries
