The world of international public health is in a precarious position. Current policy, resources, personal careers, and the very credibility of major organizations are aligned with the recent statement from the World Health Organization (WHO) that:
Epidemics and pandemics of infectious diseases are occurring more often, and spreading faster and further than ever, in many different regions of the world.
Focus has shifted from the highest burden diseases, and the community-based empowerment required to tackle them, to preventing, identifying, and mitigating diseases that are rare and/or of relatively low burden, or even hypothetical. Namely, a new focus on sudden outbreaks of infectious disease or, in their more spectacular rendering, ‘pandemics.’
The challenge with this approach is that a thorough review of the evidence base underpinning the WHO’s agenda, and that of partners including the World Bank and G20, demonstrates that the above statement is inconsistent with available data. The largest database on which these agencies rely, the GIDEON database, actually shows quite a contrary trajectory. The burden of outbreaks, and therefore risk, is shown to be reducing. By implication, the largest investments in the history of international public health appear to be based on misunderstandings, misinterpretations, and misrepresentation of key evidence.
Weighing Truth and Opportunity
Public health policy must always address threats in context. Every intervention involves a trade-off in terms of financial, social, and clinical risk. The WHO defines health in terms of physical, mental, and social well-being, and an intervention in one of these areas can impact all three. This is why public health agencies must consider all aspects of direct cost, opportunity cost, and risk when formulating policy. It is why communities and individuals must have adequate information to make decisions in their own cultural, social, and ecological context.
To make sure policy assumptions and evidence is sufficient, it is therefore imperative to include broad information from multiple sources. Reliance on epithets, dogma, deplatforming, and censorship are therefore intrinsically dangerous. This is all, of course, meant to be coded into the normative principles of decolonization, human rights, and equity on which the WHO’s constitution is based.
So, back to the precarious position in which the WHO and the international public health community find themselves. They have staked their reputation and political standing on being the center of a centralized approach to save the global populace from urgent, impending, and recurrent emergencies; an existential threat to humanity as the G20 tells us. An objective analysis reveals that these emergencies are rarely likely to reach a level that justifies the diversion of serious resources from endemic and chronic diseases that do actually maim and kill at scale (see chart below).
Admitting such a reality, after touting the inevitability of disaster so loudly, would risk career prospects, derision, and diminished ability to monetize the post-Covid moment. Yet, to ignore wider considerations in global public health and the evidence that informs those considerations would require abandonment of basic principles and ethics. A dilemma that calls for honesty, introspection, and strength.
Major causes of death by disease globally, in 2019. Global Burden of Disease data, presented at https://ourworldindata.org/.
What the Data Actually Shows
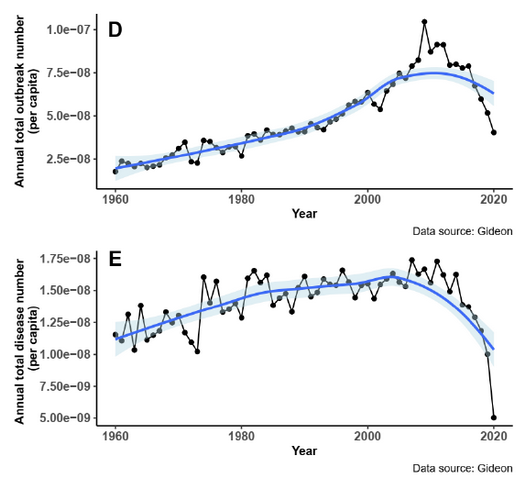
REPPARE’s analysis of the evidence behind the WHO, World Bank, and G20 documents promoting the pandemic preparedness agenda show that recorded outbreaks, both arising within human populations and as ‘spillover’ of pathogens from animals, have increased in the decades before the year 2000, with burden now declining (graphic below).
However, it is inevitable that reporting of such outbreaks will be influenced by changes in both the capacity and incentive to report. These include the development of, and increasing access to, major diagnostic platforms including PCR and point-of-care antigen and serology tests, as well as improvements in communication infrastructure. Fifty years ago, many pathogens now readily identifiable could simply not be detected, or the diseases they cause be distinguished from clinically similar conditions. It is remarkable that this would be overlooked or downplayed by major health agencies, but this is, unexpectedly, the case.
Extract from Fig. 2 of Morand and Walther (2020-23), showing marked recent reductions in outbreak and disease numbers in GIDEON database.
The development of improved diagnostic technologies not only impacts reporting rates but has obvious implications for understanding the term ‘emerging infectious disease’ (EID). This frequently used term suggests that new threats are constantly emerging, such as the Nipah virus outbreaks of the past 25 years. However, while some pathogens have newly entered human populations, such as new influenza variants, HIV and the SARS-1 virus, others such as Nipah virus were simply not detectable without recent technological advances as they cause non-specific illnesses. We are now better at finding them, which puts us immediately in a better, safer position.
Crucially, actual mortality from these acute outbreaks has remained low for a century in contrast to other current health burdens. The much-quoted analysis of Bernstein et al. (2022) suggesting millions of outbreak deaths per year includes pre-antibiotic era Spanish flu and the multi-decade HIV event, averaging it across today’s population size.
However, as their own dataset shows, nothing like the Spanish flu has occurred in terms of mortality in the past century. As most Spanish flu deaths were due to secondary infection, and we now have modern antibiotics, it also provides a poor model for future outbreaks. With HIV and influenza excluded, pre-Covid acute outbreak mortality underlying current pandemicmessaging is under 30 thousand people, globally, over the past couple of decades. Tuberculosis alone kills over 3,500 per day.
Covid-19 has, of course, intervened. It fits with difficulty into the main pandemic narrative for a number of reasons. First, its origin remains controversial, but appears likely to involve non-natural influences. While laboratory escapes can and (inevitably) will occur, the surveillance and response being proposed here is targeted at outbreaks of natural origin. Second, Covid-19 mortality occurred mainly in the elderly with significant comorbidities, meaning actual impact on overall life expectancy was far less than the raw reported mortality figures suggest (this also complicates attribution). If considered of natural origin, it appears as an outlier rather than part of a trend in the datasets on which the WHO, the World Bank, and G20 rely.
Time to Pause, Think, and Employ Common Sense
The evidence, assessed objectively, paints a picture of an increasing ability to identify and report outbreaks up to the decade 2000 to 2010 (which explains increases in frequency), followed by a reduction in burden consistent with an increasing ability to successfully address these relatively low-burden events through current public health mechanisms (which explains a lowering trajectory in mortality). This fits well with what one would intuitively expect. Namely, modern technologies and improving health systems, medicines, and economies have improved pathogen detection and reduced illness. There is much to suggest that this trend will continue.
In this context, the analyses of the WHO, the World Bank, and the G20 are disappointing in terms of scholarship and balance. A critic could reasonably suggest that a desire to address a perceived threat is driving a particularly gloomy analysis, rather than analysis objectively aiming to determine the extent of the threat. Such an approach seems unlikely to address the needs of public health.
To be clear, disease outbreaks harm people and shorten lives and must be addressed. And there are of course improvements that should and could be made to address this risk appropriately. In common with most aspects of medicine and science, this is best achieved on the basis of well-compiled evidence and scholarly analysis rather than allowing predetermined assumptions to drive outcomes.
By making claims contrary to the data, international health agencies are misleading governments of Member States down an unevidenced path with correspondingly high estimated cost and diverted political capital. This currently stands at $31.1 billion annually not including One Health measures and surge funding and at least 5 new global instruments; or about 10 times the WHO’s current annual budget. The urgency involved in the pandemic preparedness agenda is either contrary to evidence or poorly supported by it.
In view of their influence, international health agencies have a particular responsibility to ensure their policies are well-grounded in data and objective analysis. Moreover, governments have a responsibility to take the time, and effort, to ensure that their populations are well-served. It is hoped that the evaluation in the REPPARE report Rational Policy Over Panic will contribute to this effort.
REPPARE
REPPARE (REevaluating the Pandemic Preparedness And REsponse agenda) involves a multidisciplinary team convened by the University of Leeds, and led by two principal investigators.
Garrett W. Brown
Garrett Wallace Brown is Chair of Global Health Policy at the University of Leeds. He is Co-Lead of the Global Health Research Unit and will be the Director of a new WHO Collaboration Centre for Health Systems and Health Security. His research focuses on global health governance, health financing, health system strengthening, health equity, and estimating the costs and funding feasibility of pandemic preparedness and response. He has conducted policy and research collaborations in global health for over 25 years and has worked with NGOs, governments in Africa, the DHSC, the FCDO, the UK Cabinet Office, WHO, G7, and G20.
David Bell
David Bell is a clinical and public health physician with a PhD in population health and background in internal medicine, modeling and epidemiology of infectious disease. Previously, he was Director of the Global Health Technologies at Intellectual Ventures Global Good Fund in the USA, Programme Head for Malaria and Acute Febrile Disease at the Foundation for Innovative New Diagnostics (FIND) in Geneva, and worked on infectious diseases and coordinated malaria diagnostics strategy at the World Health Organization. He has worked for 20 years in biotech and international public health, with over 120 research publications. David is based in Texas, USA.
The WHO lawyers are trying to play us, saying the nations are sovereign because they still make the laws. What the WHO omits saying is that under the Treaty and proposed IHR Amendments, nations will be forced to pass the laws that the WHO tells them to pass. Examples of this and other word games below.
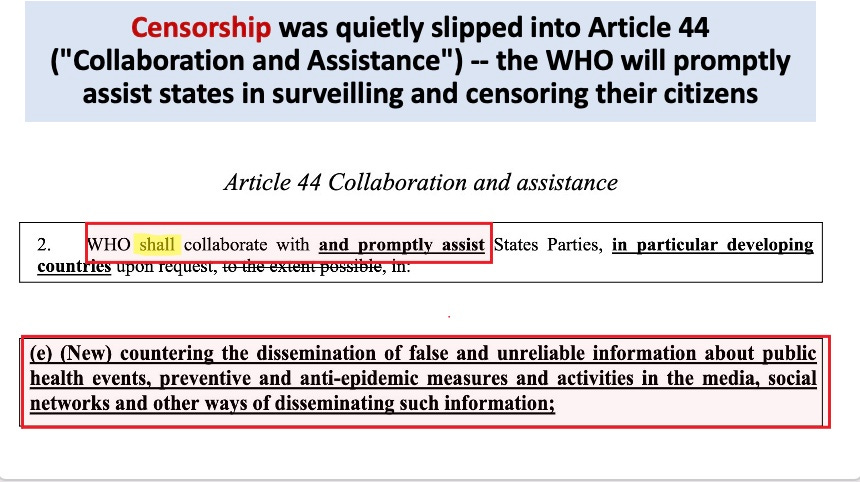
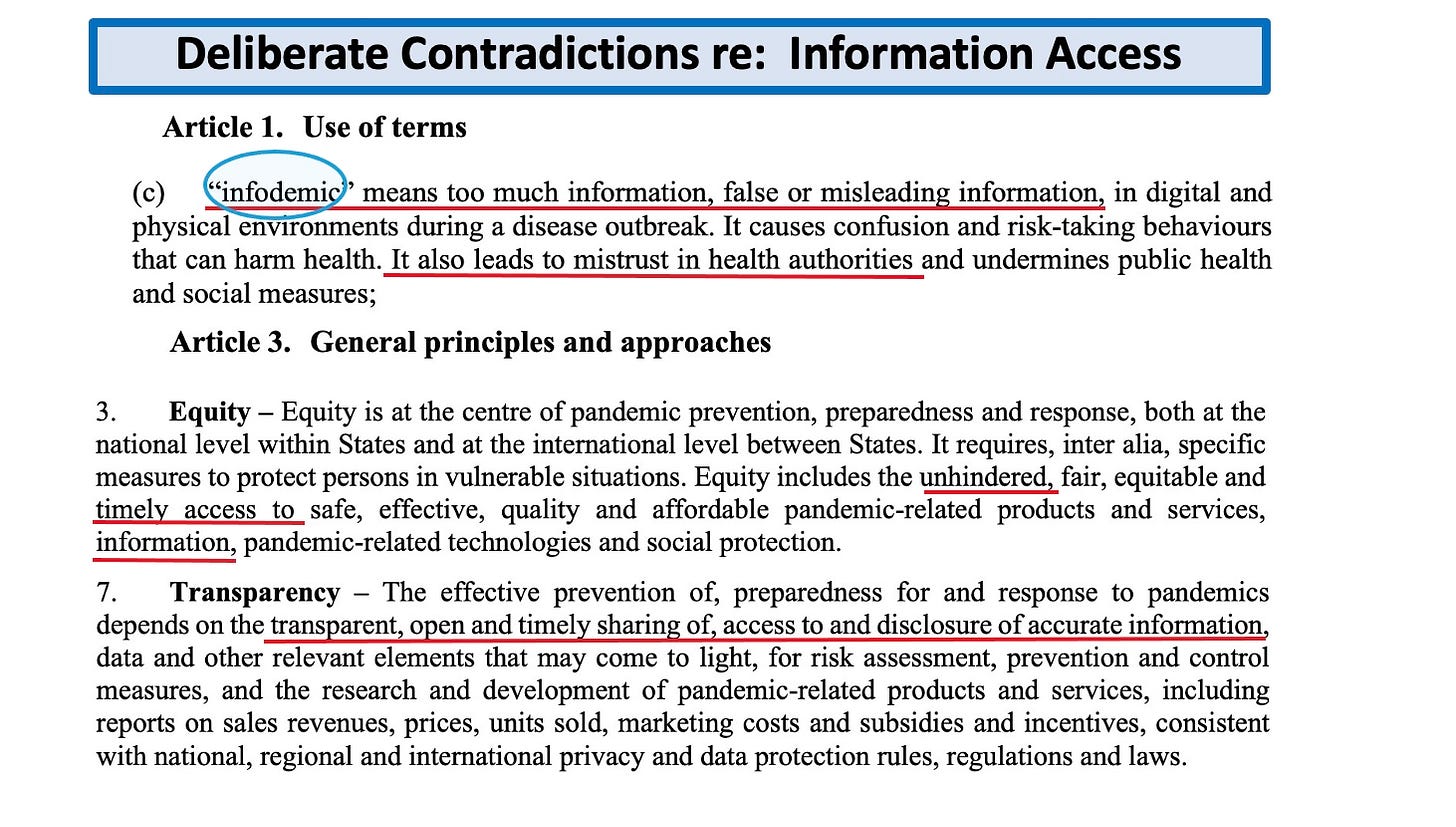
First the treaty tells you that unhindered, timely access to information is a general principle. Then it adds the caveat that transparency means open access to “accurate” information.
Then a few pages later the treaty demands that nations perform “infodemic management”—which requires not only censorship, but also surveillance of everyone’s social media footprint, so the nation will know who and what to censor. This violates both the First and Fourth Amendments to the US Constitution.
Not only that, but the censorship should be performed with international collaboration—so all nations can target the same misinformation spreaders and there will be nowhere to hide. Finally, they want to make sure you Trust the(ir) Science.
Below, the treaty is forced to admit that the so-called sovereignty that Tedros claims we will retain— the ability to pass laws—will in fact be subject to the orders of the WHO.
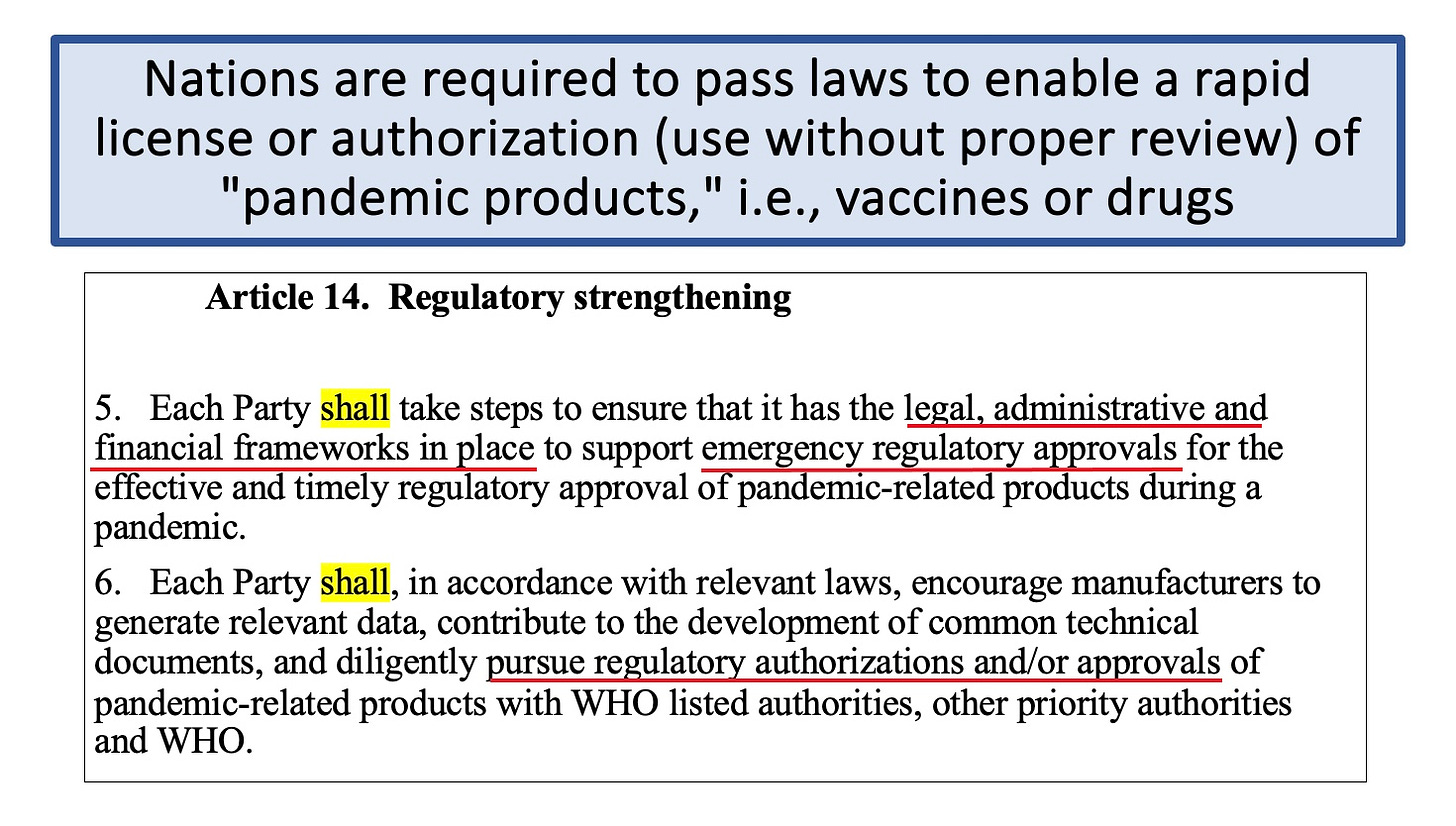
The WHO treaty draft requires that every nation pass laws to legalize Emergency Use Authorizations, so that unlicensed vaccines can be given to populations during a WHO-declared pandemic. You know, like a Monkeypox pandemic. There are no standards required and the WHO Director-General can declare any pandemic whenever he wants. Then the needles come out.
The WHO also demands that nations pass the laws needed to remove all liability from these untested and potentially deadly vaccines. Who’s sovereign now?
So you see, the WHO has just played a bunch of word games and they intended for us to be the suckers and go along, ignorant. So long as the Treaty and IHR Amendments still let nations make laws, the WHO insists on calling us sovereign. But the real sovereign is the one ordering that laws be passed. That’s the real power. Why would anyone give that up to the WHO, especially when its Director-General is a puppet for Bill Gates, is not a real doctor, and has been accused of withholding food and hiding 3 cholera epidemics to kill members of competing tribes in his native Ethiopia, when he was the #3 top official there? Do you really think he cares about your health during a pandemic?
So you can wait idly by as these treaties move ahead, or you can say ‘Hell No!’ and put on your big girl panties and decide you have finally had enough. Which will it be?
Cracks are forming in the World Health Organisation’s plans to secure a vast expansion of its powers and resources. Presented as a necessarily urgent response to the empirically unsupported assertion that pandemics are increasing in frequency and severity, negotiations for a broad package of amendments to the International Health Regulations (IHR) and a new parallel Pandemic Treaty had been expected to be over by the end of 2023. Having missed that deadline, in late January the Director-General Tedros Adhanom Ghebreyesus pleaded for WHO member states to give ground so that the negotiations could be completed at all. In the same comments he sought to apportion blame for the unexpected headwinds on those who had misconstrued, or misrepresented, the benign intentions of the WHO and its key supporters (which include China and some wealthy private organisations).
Reading between the lines, it appears that Mr. Ghebreyesus and his supporters may finally have realised that the game could soon be up: the strength of opposition to the ambitions of this unelected technocratic administration has compounded rapidly in recent weeks. That opposition has become more evident not only in smaller less influential countries, but in countries which are major contributors to the WHO. Significantly this has included groups of politicians in the U.K. and the U.S. who are seriously alarmed by the vision of a WHO-centred ‘command and control’ public health system, and by the constitutional and public spending implications of these two proposed international agreements.
The Director-General has perhaps realised that his blind ambition has not only put at risk the negotiations that might have elevated his unelected advisory organisation to the status of a supra-national rule-making authority, but is also now starting to jeopardise the future status, funding and membership of the WHO.
Secrecy, opacity and delay
The original timeline presented by the WHO had envisaged a final text of the proposed IHR amendments – where many of the most contentious proposals reside – being published before January 27th 2024, with a view to their adoption taking place at the World Health Assembly meeting scheduled from May 27th to June 1st 2024, alongside adoption of the proposed new Pandemic Treaty. That timeline, although tight, would have allowed four months for negotiators to brief domestic stakeholders, for national legislatures to debate the combined proposals and for any necessary pre-adoption formalities (approvals, technical scrutiny, cost/benefit analyses, etc.) to be completed prior to a vote at the WHA meeting in May.
Yet, on its own initiative, in October 2023 the Working Group for the negotiation of the IHR amendments unilaterally moved its own goalposts so that in place of publishing a final draft text to be scrutinised well in advance of that WHA meeting, it instead committed to circulate by the end of January a copy of the original set of proposed amendments and an interim ‘working draft’ text showing the current state of play. Negotiations would then continue between February and April 2024. It was – and remains – ambiguous whether this move was compatible with the procedural legal requirements already enshrined in the International Health Regulations, but perhaps member states quietly agreed with the WHO secretariat not to look too hard at that issue.
Notwithstanding this commitment, no interim working draft of the IHR amendments appears yet to have been published, and the U.K. officials involved in the negotiations have been inexplicably reluctant to reveal the current position of the text. Indeed, to date all demands for transparency by U.K. parliamentarians have been ignored or deflected by the ministers responsible for the U.K.’s relationship with the WHO. Astonishingly the U.K. Government has refused even to confirm who is negotiating on the U.K.’s behalf.
We understand that the IHR Working Group anticipates a final text being settled only during April or possibly even into May, but there remains no official deadline for it to publish that final text. It refuses to confirm what the documents say, and it refuses to say when it will reveal those documents. If any further evidence were needed of the disregard and disrespect for democratic process and the sovereignty of national parliaments now alleged of the WHO, then surely this is it.
Out of time
That corrosive secrecy, opacity and delay has left a vanishingly narrow window for domestic public health organisations and parliamentarians to review or comment meaningfully on what may become generationally-significant changes to the U.K.’s relationship with the WHO, with other countries and with the public health business community. It means Parliament will have scant opportunity to scrutinise the IHR amendments and the new international funding and resource-sharing commitments enshrined in the parallel Pandemic Treaty. Yet these are documents with the potential to impact materially on the U.K.’s ability to act autonomously, on freedom of speech and opinion, on health security and on the nature of U.K. democracy itself. They also have the potential to commit future generations to very significant public spending obligations.
Given their significance, the IHR proposals and the parallel Pandemic Treaty require a commensurate degree of examination by Parliament. The current nature of the WHO’s funding, 85% of which now comes from private commercially-interested organisations, creates an additional imperative for rigorous, investigative scrutiny. In November 2023, Human Rights Watch wrote that:
The draft [treaty] reflects a process disproportionately guided by corporate demands and the policy positions of high-income governments seeking to protect the power of private actors in health including the pharmaceutical industry.
Without sight of any working drafts of the revised IHRs, nor of the current state of the draft treaty, scrutiny is completely frustrated. At this late stage in the process, after repetitive calls for transparency seemingly have been ignored, one is left to wonder whether this is precisely the intent of the officials involved.
Deferral is the rational solution
As the window for full, fair, candid appraisal by national democratically-elected legislatures is now all but shut, the logical and necessary solution is for member states to demand that any vote to adopt either of these two international accords is held over to the next WHA meeting in May 2025. This will allow ample time both for the conclusion of the negotiations and for member state-level scrutiny of the proposals served up by the negotiating teams.
If it is truly the case that the WHO and its member officials do not intend for national legislatures to cede rule-making sovereignty to an enlarged WHO technocracy, they will surely accept the need for state-level legislatures to control the timing of this process. Calls for deferral have begun, but more voices will be needed to press relevant political leaders and officials to accept that deferral is the only legitimate response to this situation.
A turning point
Even now, in the face of a chorus of rational legally-grounded concerns raised by U.K. parliamentarians about the substance of the proposed amendments and the opacity of the negotiations, the Government has remained steadfastly unwilling to comment on its negotiating intent and objectives, beyond vague platitudes. Efforts by members of the public, legal experts and parliamentarians to understand the current state of negotiations, and even just the arrangements within the U.K. Government to conduct the negotiations, have been stonewalled. The WHO equally has remained virtually mute and offered no meaningful evidence to support claims that its ambitions have been misunderstood.
This has served only to fuel distrust in this process, in the Government and its senior officials, in the U.K.’s relationship with the WHO, and in the WHO’s relationship with its influential funding providers.
Behaviour of this overtly undemocratic nature indicates that the WHO project has long since lost sight of its noble foundations in post-war benevolent multilateralism, and indeed of its reason for being: health for all in pursuit of global peace and security. Unfortunately, the WHO is now a symbol of all that is wrong with what has become a system of global public health patronage. This shamelessly undemocratic and chaotic power grab is also indicative of an organisation which has reached the end of its useful life, at least in its current guise. We suggest that this sorry episode should become the impetus for the U.K. to revisit its relationship with the WHO, and the relationship of the WHO with its funding providers.
The U.K. will not be an outlier if it does so, but rather a role model and – judging by the breadth and strength of international expressions of antipathy for the WHO’s ambitions – a leader of fast followers. This may well be the U.K.’s best post-Brexit opportunity to be an actor of global significance on the international stage.
Molly Kingsley is a founder and Ben Kingsley is the Head of Legal Affairs at children’s rights campaign group UsForThem. Find UsForThem on Substack. Ben and Molly’s new book (co-authored with Arabella Skinner) The Accountability Deficitis available now at Amazon and other book stores.
As the WHO and media attempt to keep the public in fear with the threat of an unknown disease, we breakdown what ‘disease X’ really symbolizes. Meanwhile, gain-of-function experiments continue to put humanity in great peril.
Del takes a deep dive on the newly approved RSV vaccine’s side effects on pregnant women. Using data straight from ABRYSVO’s own box insert for data, he highlights the increased risk of preterm birth and buffer ingredients such as polysorbate 80 and residual DNA from host cell proteins from Chinese hamster cell lines. Does this sound safe to you?
On Monday, the UK House of Commons debated the World Health Organisation’s (“WHO’s”) proposed amendments to the International Health Regulations (“IHR”).
The debate was held in response to a petition to the UK Parliament which gained more than the required number of signatures. In yet another brilliant speech, Andrew Bridgen MP left no stone unturned. A few other Members of Parliament (“MPs) didn’t hold back either.
The first to speak was Philip Davies, MP for Shipley. He summed up the problem both with the WHO’s two proposed instruments – the IHR amendments and the Pandemic Treaty or Accord – and the UK Parliament’s mindset regarding concerns raised about them.
“In preparing for today’s debate, I looked back at the contributions made in April when another petition on this topic was debated here in Westminster Hall … I have to say that I was disappointed by some of the rhetoric, when valid concerns were dismissed as an ‘overreaction and hysteria’. It is clear that this is – quite rightly, in my opinion – an important issue for the public. We can see that that is the case from not just the full Gallery, but the large numbers signing the petitions,” Mr. Davies said.
“We have two international legal instruments, both designed to increase the WHO’s authority in managing health emergencies,” he said. “What is being proposed could have a huge and detrimental impact on all parts of society and on our sovereignty … We are talking about a top-down approach to global public health hardwired into international law.”
“Let us not forget that the director-general is appointed by an opaque, non-democratic process – and I think that is being rather generous,” he added.
Andrew Bridgen, MP for North West Leicestershire, took the floor next. “I [ ] thank the 116,000 members of the public who signed this public petition so that we can have this important debate today,” he began.
“It is impossible to consider either the pandemic treaty or the amendments to the international health regulations in isolation; they are two linked instruments of the WHO, and they need to be considered in parallel.”
Why does the WHO make false claims regarding proposals to seize states’ sovereignty? Mr. Bridgen asked the House noting that Tedros Adhanom Ghebreyesus’ statements that “no country will cede any sovereignty to WHO” are unequivocally, and also wholly inconsistent with the text he is referring to.
Mr. Bridgen reminded the House that Tedros, as with all WHO officials, is unelected, unaccountable, non-taxpaying and immune from prosecution due to diplomatic immunity.
The intent of the text of the IHR amendments and Pandemic Accord is clear: WHO’s proposed instruments transfer decision-making power to WHO regarding basic aspects of societal function, decision-making that is currently vested in nations and individuals. “The WHO director-general will have the sole authority to decide when and where they are required, and the proposals are intended to be binding under international law,” Mr. Bridgen said.
“Continued claims that sovereignty is not lost, echoed by politicians in this House, other elected assemblies, and of course the media, therefore raise very important questions concerning motivations, competence and ethics.”
Later in his speech, Mr. Bridgen said that WHO’s position raises a real question of whether its leadership is truly ignorant of what is being proposed or is actively seeking to mislead countries and the public to increase the probability of acceptance.
“Amending the 2005 international health regulations may be a straightforward way to quickly deploy and enforce what appears to be the new normal for health control measures that we have seen implemented since the covid-19 pandemic. The current text applies to virtually the entire global population, counting 196 states, including all 194 WHO member states. Approval may or may not be required by a formal vote of the World Health Assembly: the recent 2022 amendment was adopted through consensus. If the same approval mechanism were to be used in May 2024, many countries, and indeed the public, might remain unaware of the broad scope of the new text and its implications for national and individual sovereignty. That is why today’s debate is so important,” he said.
Mr. Bridgen quoted from article 18 of the IHR which details specific examples of measures that are currently non-binding and WHO can recommend.
“When implemented together, those measures have generally been referred to since 2020 as lockdowns and mandates -“lockdown” was previously a term reserved for people incarcerated as criminals. It removes basic, universally accepted human rights. Such measures were previously considered by the WHO itself to be detrimental to public health. However, since 2020, it has become the default standard for public health authorities to manage epidemics, despite its contradictions to multiple stipulations of the Universal Declaration of Human Rights – the UDHR.” Mr. Bridgen said.
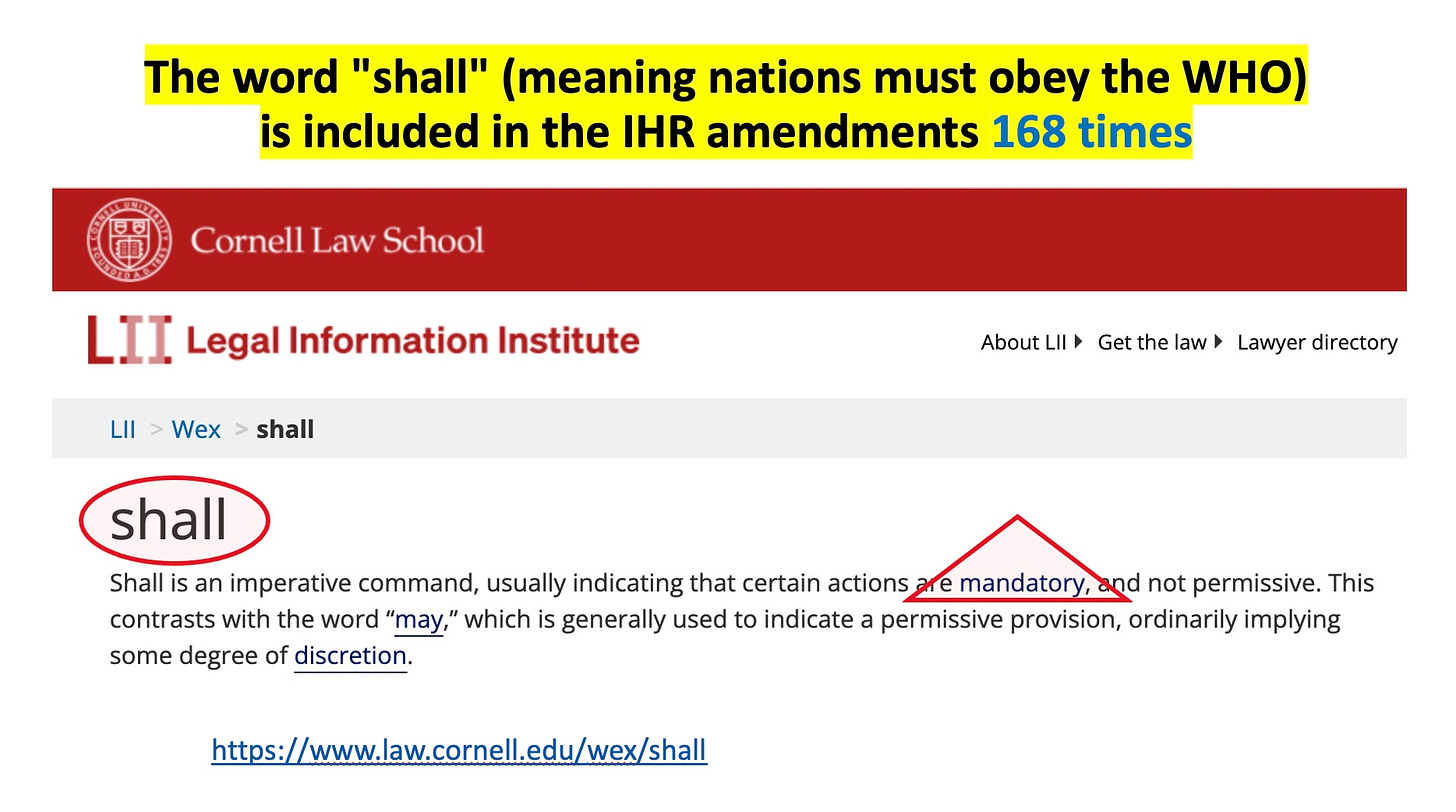
Mr. Bridgen explained how the current recommendations will be changed into requirements through three mechanisms:
“The first is the removal of the term “non-binding” … Second is the insertion … [of] the phrase that ‘Member States’ will ‘undertake to follow WHO’s recommendations’ … Thirdly … ‘State Parties’ undertake to enact what previously were merely recommendations, without delay, including requirements of WHO regarding non-state entities under their jurisdiction.”
Mr. Bridgen explained that “non-state actors” means private businesses, charities, and individuals. “In other words, everyone and everything comes under the control of the WHO, once the director-general declares a public health emergency of international concern,” he said.
Mr. Bridgen also pointed out that the IHR also allows WHO to deploy “personnel” into the country. “That is, it will have control over entry across national borders for whoever it chooses,” he said.
He called out WHO’s desire to limit freedom of speech to “counter misinformation and disinformation.” This clashes with the UDHR, Mr. Bridgen said.
“Although freedom of speech is currently exclusively for national authorities to decide, and its restriction is generally seen as being negative and abusive, United Nations institutions including the WHO have been advocating for censoring unofficial views in order to protect the people from what they call “information integrity.” No doubt, if these amendments were in place, I would not be allowed to give this speech and, if I was, it would not be allowed to be reported in the mainstream media or even on social media.”
Mr. Bridgen mentioned the potential for human rights abuses by WHO and its allies coercing populations to take experimental vaccines or drugs:
“If vaccines or drugs are still under trial and not fully tested, the issue of being subject to an experiment is also real. There is a very clear intent to employ the Coalition for Epidemic Preparedness and Innovations’ 100-day vaccine programme, which, by definition, cannot complete meaningful safety and efficacy trials within the timespan. As we know, the covid-19 vaccines are still experimental, years on from their first introduction, because they are still under emergency use authorisation.”
The proposed pandemic agreement, Mr. Bridgen said, will set humanity into a new era that is organised around pandemics: pre-pandemic, pandemic and inter-pandemic times.
“The relevant question regarding the two WHO instruments should be not whether sovereignty is threatened,” he said, “but why democratic states would forfeit any sovereignty to an organisation that is significantly funded by and bound to obey the dictates of corporations and self-proclaimed philanthropists, and jointly governed by member states half of which are not even open and transparent democracies.”
Mr. Bridgen followed this by voicing a thought that has been on many of our minds in recent years:
“If sovereignty is being knowingly forfeited by governments, without the knowledge and consent of their peoples and based on the false claims of governments and the WHO, the implications are extremely serious. It would imply that leaders were working directly against the interests of their people. Most countries have specific fundamental laws for dealing with that practice.”
You can watch Mr. Bridgen’s speech in parliament below and read a transcript of it in the Hansard HERE.
Andrew Bridgen: International Health Regulations Amendments Debate in Westminster Hall, 19 December 2023 (24 mins)
John Redwood, MP for Wokingham, agreed. “I hope that the Minister will listen very carefully to the debate and the petitioners,” he said. “It would be quite wrong to vest the power of decision in people so far away from our own country who are not in full knowledge of the local circumstances.”
“Before any such power is vested in the WHO, there should be a proper inquiry and debate about how it performed over the course of the most recent covid pandemic,” Mr. Redwood said. “We need more transparency, debate, discussion and challenge of those in the well-paid positions at the WHO, so that science can advance.”
“We do not want an international body saying, ‘There’s only one way to look at this problem or to think about it’ … we need much more accountability, exposure and proper debate.”
Mark Francis, MP for Rayleigh and Wickford, also voiced his concerns about amendments to the IHR. “Not least because the WHO will be given extremely strong powers in any future pandemic,” he said.
“The proposed amendments empower the WHO to issue requirements for the UK to mandate highly restrictive measures, such as lockdowns, masks, quarantines, travel restrictions and medication of individuals, including vaccination, once a PHEIC has been declared by the WHO. That is something we should all be very concerned about. We as parliamentarians are guardians of the country’s liberty, so we need to be very anxious about that.”
Danny Kruger, MP for Devizes, began by noting that it was very worrying that so few MPs were present at the debate. “Significant numbers of the public have a real interest in this topic, so what is going on?” he asked. And reiterated the points already made.
He emphasised the provision in the proposed regulations that WHO would require countries to tackle misinformation and disinformation. After recalling one or two erroneous statements made by WHO in response to the covid pandemic, Mr. Kruger said:
“This is the organisation that we propose giving the power to intervene in national debates, and to close down discussion about the origins and appropriate response to pandemics under the guise of tackling misinformation and disinformation.
“We should be concerned about the value of the World Health Organisation, given its record, and we should, I am afraid, have the same scepticism about our government’s role.”
Sir Christopher Chope, MP for Christchurch, said: “Once we have given away these powers to the WHO, which is power hungry … it is very difficult to get them back.”
He pointed to an insidious development, following a recent Supreme Court case, of what is called “customary international law.” “That development basically means that a group of outsiders can tell us in this country what is good for us and what is not,” he said.
Mr. Francis interjected and said: “For the avoidance of any doubt … none of us has argued this afternoon for withdrawal from the World Health Organisation – we might call it Wexit.” To which Mr. Davies responded, “Yet.” [Attaboy Mr Davies!]
“We do not want to withdraw,” Sir Christopher said, “there is no need to withdraw from a voluntary organisation that is confined to giving us advice and providing data and information.”
Sir Christopher reminded the House about WHO’s war on ivermectin. “Even more sinister than the change in advice on lockdowns was the WHO’s approach to finding a treatment for covid-19 patients. There was a lot of evidence to suggest that ivermectin – it was not the only such drug – could be used to really good effect to improve outcomes for patients suffering from covid-19,” he said.
“[The campaign against ivermectin] was a war, organised by the WHO, against a remedy for covid-19, because, obviously, the whole vaccine development programme was premised on there being no cure for covid-19, and no effective treatment for it,” he added.
“I hope that the Government will start looking really seriously, and sceptically, at the work of the WHO, and at the extent to which it is unduly influenced by external factors. A lot of its work is not based on straight science, but is actually political.”
After noting that Slovakia, Estonia and New Zealand had come out publicly with their scepticism about WHO’s process, Sir Christopher said:
“I hope that our government will now say, ‘By all means, let’s keep the WHO as a body that provides advice, but under no circumstances will we sign up to anything that will give them control over our lives’.”
You can read the full transcript for the 3-hour debate HERE and watch the full debate on Parliament TV HERE.
Questions could profitably be asked about the following:
1. The WHO is not an honest broker.
a. Its Director-General has repeatedly lied about the WHO’s 2 proposed treaties: the pandemic treaty/agreement, and International Health Regulation (IHR) amendments, claiming they do not seize sovereignty, when there is no doubt they do precisely that. See Why Does the WHO Make False Claims Regarding Proposals to Seize States’ Sovereignty? by David Bell, MD, PhD and attorney Thi Thuy Van Dinh, PhD.
b. The WHO appears to have deceived the public about whether the amendments “approved” in May 2022 followed the legally required procedure of a full WHA vote. Twelve members of the European Parliament wrote to the WHO on November 28, 2023 asking for evidence that the WHO actually conducted a vote of the entire World Health Assembly to pass several new amendments in May 2022, with a 48 hour deadline. The WHO did not respond, and the twelve European parliament members declared the May 2022 amendments null and void last week.
c. The WHO’s principal legal office, Steven Solomon, stated in early October that the IHR working group did not have to follow the required procedure (found in the existing 2005 version of the International Health Regulations) to make public the draft of new proposed amendments 4 months in advance of a vote. Thus, we may not see the new amendments until after the WHO members have voted on them.
2. The WHO’s proposed treaties are unconstitutional
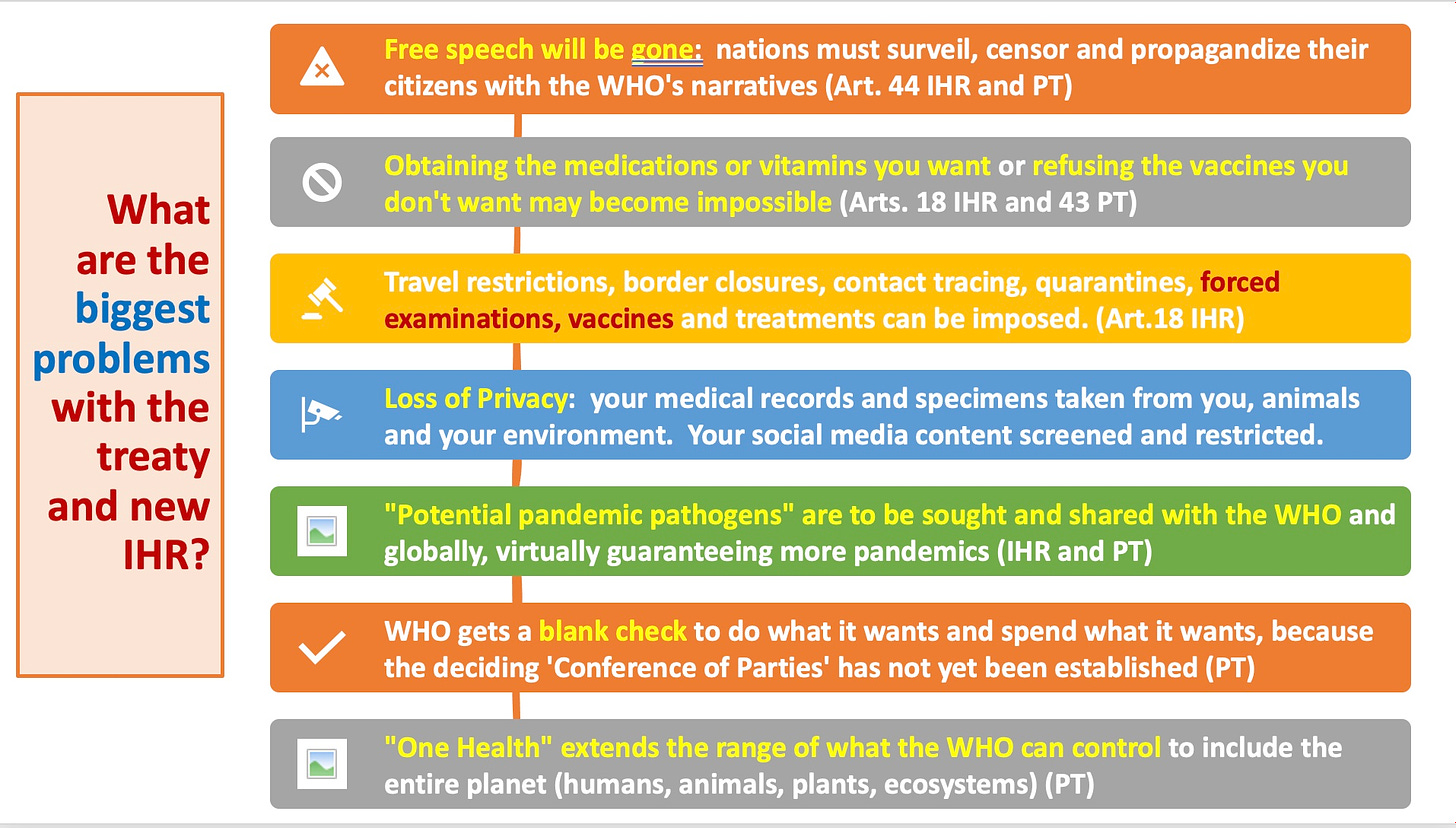
a. They demand that nations perform surveillance of their citizens’ social media footprints and censor them to prevent ‘infodemics’ (too much information, according to the WHO’s definition), misinformation and disinformation, surveil
b. They say that nations should give up the intellectual property rights of their citizens.
c. There is no due process for the declaring or ending of public health emergencies of international concern, for which no standards exist.
3. In the Oct. 30 draft of the treaty, A new WHO Secretariat and Conference of Parties for pandemics are to be established in the future and will make their own rules. Thus, agreeing to this means providing a blank check to the WHO to do whatever it wants at some later date.
4. The 2 proposed treaties ignore existing international law prohibiting the proliferation of biological warfare agents (the 1972 Biological Weapons Convention and the 2004 Security Council Memorandum 1540) and demand that nations search out new agents (a.k.a. “potential pandemic pathogens”) and share them with the WHO, which will “share them globally.” The WHO has already established a BioHub for this purpose and a Pathogen Access and Benefits System.
5. The proposed treaty and amendments also demand that nations perform 2 additional forms of surveillance of their citizens: microbiological surveillance of their populations, animals and ecosystems for pathogens, and surveillance and sharing of medical and hospital records, both of which violate privacy protections.
6. The proposed amendments remove the guarantee of “Human rights, dignity and freedom of persons” that are found in the current international health regulations.
7. The two proposed treaties are both binding, whereas the earlier IHR were recommendations only, apart from minor requirements for notification of certain outbreaks to the WHO. The two proposed documents would give the WHO and particularly its Director-General vast authority to manage healthcare globally. The current Director-General is not a medical practitioner and instead has a PhD in Community Health.
8. The WHO lacks the personnel and expertise to manage international pandemics and other health concerns. Any developed nation has within it much more capacity to understand and manage medical events within its borders, and likely international events as well.
9. The proposed treaty calls for rapidly produced vaccines and for nations to implement domestic legislation to permit the use of unlicensed medical products without manufacturer liability, instead “managing” the liability issues using existing models, such as the US’ Countermeasures Injury Compensation Program, which has so far compensated 8 Americans for injuries related to EUA COVID products (primarily vaccines) from the 12,358 claims filed. https://www.hrsa.gov/cicp/cicp-data
10. It is apparent that in the process of developing the “Pandemic Accord” and amendments to the IHR, WHO/WHA positioned itself in a combined law-making/executive/expert/censorship role, which is a well-known path to usurpation of unrestrained power. It should not be surprising, therefore, that the proposed Amendments grant expressly such power to the WHO.
11. The WHO receives 85% of its funding from voluntary contributions, and only 15% from dues paid by its 194 member nations. Most of the voluntary contributions are earmarked for special projects that the WHO carries out. When President Trump withheld US funding in 2020, Bill Gates became the WHO’s top funder. The (unelected) WHO serves many private masters, yet seeks to govern the world’s population.
12. Virtually every recommendation the WHO made for managing the COVID pandemic was counterproductive. Why would we give the WHO the power to enforce the same bad advice on the US and world?
Like other aspects of medicine, public health is about dealing with life and death. In the international sphere, this involves big numbers. If, as a group, a few million dollars is allocated here, it may save thousands of lives. Actual people living rather than dying, or grieving. If it’s allocated there, it may even promote death – diverting other resources from a more useful approach or causing direct harm.
Dealing with such issues affects people’s egos. Humans are prone to think themselves important if they seem to have power over the lives of others. With international public health staff this is reinforced by people they meet, and the media glorifying their work. The public hears little of the high, often tax-free salaries or the travels and 5-star hotels that boost these egos still further, but instead are fed pictures of (usually brown) children lining up to be saved by people in (usually blue) vests with nice logos. It all feels good.
The result, inevitably, is an international public health workforce that has a very high opinion of itself. Possessing values that it considers superior to those of others, it feels justified in imposing its beliefs and values on the populations who are the target of its work. As their role seems to them more important than bringing up kids in some random village or working at an airport check-in counter, they can feel virtuous when seeking to impose their superior opinions on others. The WHO’s insistence that countries globally embrace certain Western cultural values supporting abortion on request until time of delivery are a powerful example, irrespective of what one considers its ‘rightness.’ More so as the WHO also claims to support ‘decolonization.’
Things get tricky when the ultimate source of funding has its own commercial or geopolitical priorities. As an example, expenditure of the World Health Organization (WHO) is now over 75% specified by the funder, including those who stand to gain financially from such work. Large organizations that helped the WHO run its Covid-19 response, such as Gavi (vaccines) and CEPI (vaccines for pandemics), were jointly set up by private and corporate interests who are now represented on their boards and directing them.
The interface between these self-interested funding sources and the populations upon whom they seek to impose their will is where the self-righteousness culture of the public health workforce becomes so important. They need enforcers whose culture renders them willing to impose harm and restrictions upon others. Apologists and sanitizers who are in a position of trust.
A Captured but Willing Workforce
If you are going to sell a product, you can advertise it and hope potential buyers are interested. This carries a commercial risk. If a product can be mandated – essentially force the market to buy it – then this risk is eliminated. If you can then remove any liability for harm done, you are simply printing money with no risk at all. This is such a ridiculous and indecent approach that it would never fly in a normal commercial context. You would need a workforce capable, en-masse, of putting aside the moral codes that prevent such practices. A shield between the people being managed and the commercial or political interests standing to gain.
Historically, public health has often provided such a shield – a way of sanitizing vested interests that would otherwise appear repulsive to the public. In the United States, it implemented racist and eugenic policies to sterilize and send into decline ethnic groups it considered inferior, or individuals considered to have lesser mental capacity (or socially inferior).
The Johns Hopkins University psychology laboratory was founded by proponents of just such an approach. The fascists in Italy and Germany were able to extend this to active killing first of the physically ‘inferior,’ then whole ethnic groups claimed by governments and health professions to be threats to the purity of the majority. Examples such as the Tuskegee study show that this attitude did not stop with World War Two.
Most of the doctors and nurses implementing eugenics and other fascist policies will have convinced themselves that they were acting for the greater good, rather than demons. Medical schools told them they were superior, patients and the public reinforced this, and they convinced each other. Having the power to directly save or not save lives does that, while carting trash and repairing sewers (equally important to public health) does not. It enables people to tell others what to do for a perceived greater good (even sterilization or worse) and to then stand together as a profession to defend it. They will do this for those who direct them, as health professionals are also trained to follow guidelines and superiors.
Accepting Humility
The hardest thing in public health is accepting that none of the above is actually for the public’s health. It is about unleashed human ego, a large part of greed, and a trained and frequently reinforced willingness to bow to authority. Hierarchies feel good when you are near the top.
In contrast, health depends on mental and social well-being, and all the multiplicity of influences from within and without that determine whether each person experiences, and how they deal with, disease. It requires individuals to be empowered to make their own choices, irrespective of human rights, because mental and social health, and a large part of physical health, are dependent on the social capital this agency enables. Public health can advise but once it steps over the line to coerce or force, it ceases to be an overall positive influence.
To provide sensible public health, you must therefore be comfortable allowing others to do what you consider to be against their physical interests or some ‘greater good.’ When you are convinced that you have superior intellect, this can feel wrong. It is harder again when deferring to the public means breaking ranks with, and losing standing with, peers who consider themselves superior and more virtuous.
To do this, one has to accept that intellect has no standing when assessing human worth, and that each human has some intrinsic characteristic that puts them above all considerations regarding greater societal good. This is the basis of fully informed consent – a very difficult concept when considered deeply. It has its basis in the Nuremberg Code and post-1945 medical ethics and human rights, and is a concept with which many in our health professions and their institutions disagree.
Facing Reality
We are now entering one of those more extreme periods, where the hierarchy really becomes clear. Those pulling the public health strings have gained enormous power and profit from Covid-19 and are focused on getting more. Their chosen enforcers did their job during Covid-19, turning a virus outbreak that kills near an average age of 80 years and at a rate globally perhaps slightly higher than influenza into a vehicle to drive poverty and inequality. They continue to do this, pushing ‘boosters’ associated with rising rates of the infection they are aimed against, and with unusual evidence of harm, ignoring prior understanding of immunology and basic common sense.
Now public health is moving further in response to the same masters, the Covid profiteers, promoting fear of future outbreaks. With near-total obeisance, they are now supporting a reordering of society and health sovereignty through amending the WHO IHR regulations and negotiating a pandemic treaty to build a permanent health technocracy to sustain concentration of wealth and power through recurrent pharmaceutical profit.
This reordering of our democracies into Pharma technocracies, with the public health bureaucracy being aligned to enforce it, will make the right to travel, work, go to school, or visit sick relatives dependent on compliance to health dictates passed down from a massively wealthy corporate aristocracy. Those health dictates will be enforced by people whose training was funded and careers supported by those who directly profit. The modelers who will produce the numbers needed to scare will be similarly funded, while a sponsored media will continue to promote this fear unquestioningly. The institutions above this, the WHO and the big public-private partnerships, take funding and direction from the same sources. The proposed pandemic regulations and treaty are just cementing all in place, repeating the massively harmful restrictions on human rights applied during Covid whilst ensuring that there is less room for dissent.
We need legislators, and the public, to reclaimpublic health ethics and to return to credible concepts of health and well-being – as the WHO once did – “physical, mental and social.” This is what was intended when previous generations fought to overthrow dictators, striving for equality and for the rights of individuals over those who would control them. History tells us that public health professions tend to follow self-interest, taking the side of those who would be dictators. If our democracies, freedom, and health are to survive, we must accept reality and address this as a basic issue of individual freedom and good governance for which we are all responsible. There is too much at stake to leave this to self-interested corporatists and the notorious enforcers they control.
David Bell, Senior Scholar at Brownstone Institute, is a public health physician and biotech consultant in global health. He is a former medical officer and scientist at the World Health Organization (WHO), Programme Head for malaria and febrile diseases at the Foundation for Innovative New Diagnostics (FIND) in Geneva, Switzerland, and Director of Global Health Technologies at Intellectual Ventures Global Good Fund in Bellevue, WA, USA.
The Director General (DG) of the World Health Organization (WHO) states:
No country will cede any sovereignty to WHO,
referring to the WHO’s new pandemic agreement and proposed amendments to the International Health Regulations (IHR), currently being negotiated. His statements are clear and unequivocal, and wholly inconsistent with the texts he is referring to.
A rational examination of the texts in question shows that:
The documents propose a transfer of decision-making power to the WHO regarding basic aspects of societal function, which countries undertake to enact.
The WHO DG will have sole authority to decide when and where they are applied.
The proposals are intended to be binding under international law.
Continued claims that sovereignty is not lost, echoed by politicians and media, therefore raise important questions concerning motivations, competence, and ethics.
The intent of the texts is a transfer of decision-making currently vested in Nations and individuals to the WHO, when its DG decides that there is a threat of a significant disease outbreak or other health emergency likely to cross multiple national borders. It is unusual for Nations to undertake to follow external entities regarding the basic rights and healthcare of their citizens, more so when this has major economic and geopolitical implications.
The question of whether sovereignty is indeed being transferred, and the legal status of such an agreement, is therefore of vital importance, particularly to the legislators of democratic States. They have an absolute duty to be sure of their ground. We systematically examine that ground here.
The Proposed IHR Amendments and Sovereignty in Health Decision-Making
Amending the 2005 IHR may be a straightforward way to quickly deploy and enforce “new normal” health control measures. The current text applies to virtually the entire global population, counting 196 States Parties including all 194 WHO Member States. Approval may or may not require a formal vote of the World Health Assembly (WHA), as the recent 2022 amendment was adopted through consensus. If the same approval mechanism is to be used in May 2024, many countries and the public may remain unaware of the broad scope of the new text and its implications to national and individual sovereignty.
The IHR are a set of recommendations under a treaty process that has force under international law. They seek to provide the WHO with some moral authority to coordinate and lead responses when an international health emergency, such as pandemic, occurs. Most are non-binding, and these contain very specific examples of measures that the WHO can recommend, including (Article 18):
require medical examinations;
review proof of vaccination or other prophylaxis;
require vaccination or other prophylaxis;
place suspect persons under public health observation;
implement quarantine or other health measures for suspect persons;
implement isolation and treatment where necessary of affected persons;
implement tracing of contacts of suspect or affected persons;
refuse entry of suspect and affected persons;
refuse entry of unaffected persons to affected areas; and
implement exit screening and/or restrictions on persons from affected areas.
These measures, when implemented together, are generally referred to since early 2020 as ‘lockdowns’ and ‘mandates.’ ‘Lockdown’ was previously a term reserved for people incarcerated as criminals, as it removes basic universally accepted human rights and such measures were considered by the WHO to be detrimental to public health. However, since 2020 it has become the default standard for public health authorities to manage epidemics, despite its contradictions to multiple stipulations of the Universal Declaration of Human Rights (UDHR):
Everyone is entitled to all the rights and freedoms set forth in this Declaration, without distinction of any kind including no arbitrary detention (Article 9).
No one shall be subjected to arbitrary interference with his privacy, family, home or correspondence (Article 12).
Everyone has the right to freedom of movement and residence within the borders of each state, and Everyone has the right to leave any country, including his own, and to return to his country (Article 13).
Everyone has the right to freedom of opinion and expression; this right includes freedom to hold opinions without interference and to seek, receive and impart information and ideas through any media and regardless of frontiers (Article 19).
Everyone has the right to freedom of peaceful assembly and association (Article 20).
The will of the people shall be the basis of the authority of government (Article 21).
Everyone has the right to work (Article 23).
Everyone has the right to education (Article 26).
Everyone is entitled to a social and international order in which the rights and freedoms set forth in this Declaration can be fully realized (Article 28).
Nothing in this Declaration may be interpreted as implying for any State, group or person any right to engage in any activity or to perform any act aimed at the destruction of any of the rights and freedoms set forth herein (Article 30).
These UDHR stipulations are the basis of the modern concept of individual sovereignty, and the relationship between authorities and their populations. Considered the highest codification of the rights and freedoms of individuals in the 20th century, they may soon be dismantled behind closed doors in a meeting room in Geneva.
The proposed amendments will change the “recommendations” of the current document to requirements through three mechanisms on
Removing the term ‘non-binding’ (Article 1),
Inserting the phrase that Member States will “undertake to follow WHO’s recommendations” and recognize WHO, not as an organization under the control of countries, but as the “coordinating authority” (New Article 13A).
States Parties recognize WHO as the guidance and coordinating authority of international public health response during public health Emergency of International Concern and undertake to follow WHO’s recommendations in their international public health response.
As Article 18 makes clear above, these include multiple actions directly restricting individual liberty. If transfer of decision-making power (sovereignty) is not intended here, then the current status of the IHR as ‘recommendations’ could remain and countries would not be undertaking to follow the WHO’s requirements.
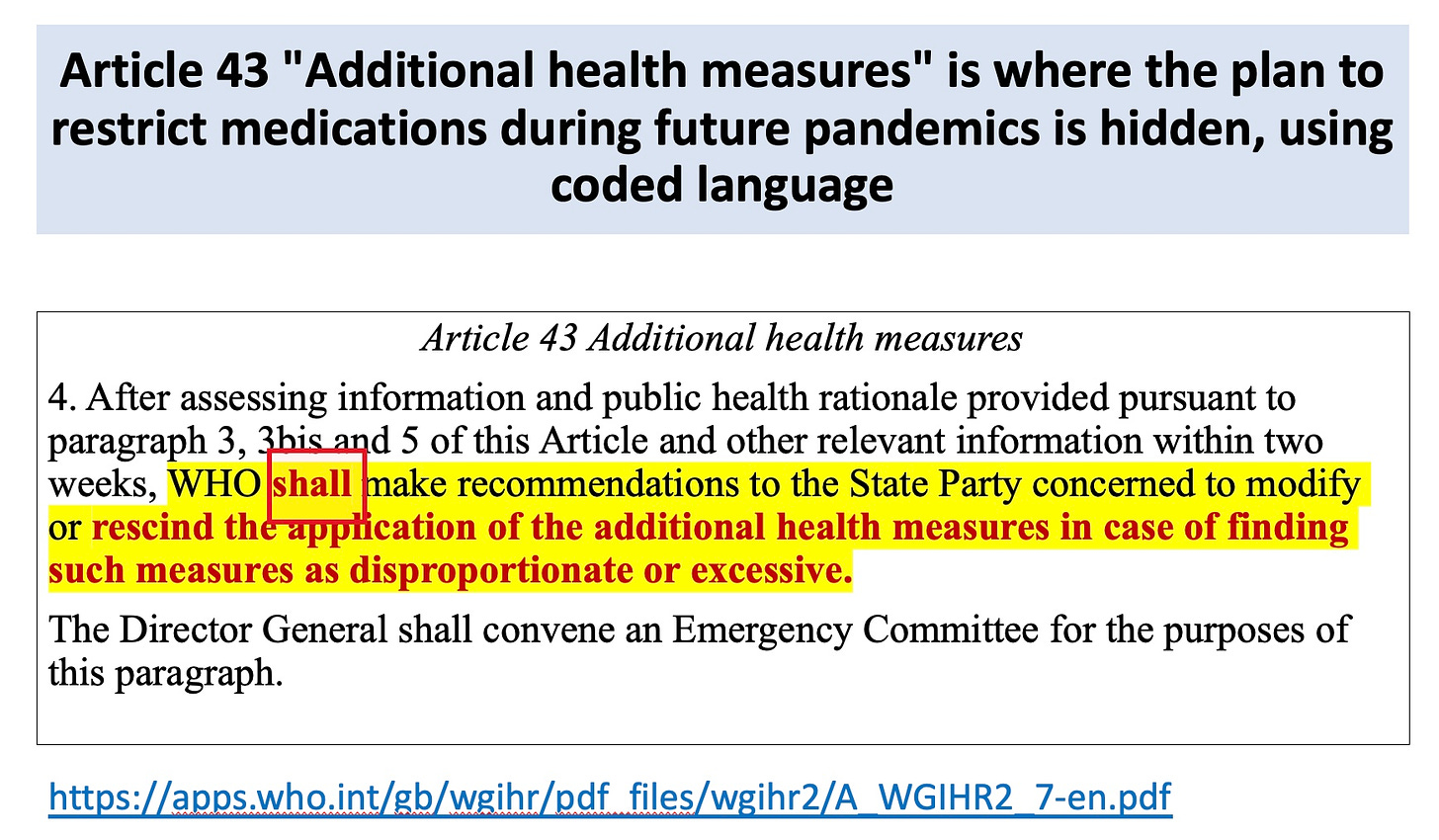
States Parties undertake to enact what previously were merely recommendations, without delay, including requirements of WHO regarding non-State entities under their jurisdiction (Article 42):
Health measures taken pursuant to these Regulations, including the recommendations made under Articles 15 and 16, shall be initiated and completed without delay by all State Parties and applied in a transparent, equitable and non-discriminatory manner. State Parties shall also take measures to ensure Non-State Actors operating in their respective territories comply with such measures.
Articles 15 and 16 mentioned here allow the WHO to require a State to provide resources “health products, technologies, and know-how,” and to allow the WHO to deploy personnel into the country (i.e., have control over entry across national borders for those they choose). They also repeat the requirement for the country to require the implementation of medical countermeasures (e.g., testing, vaccines, quarantine) on their population where WHO demands it.
Of note, the proposed Article 1 amendment (removing ‘non-binding’) is actually redundant if New Article 13A and/or the changes in Article 42 remain. This can (and likely will) be removed from the final text, giving an appearance of compromise without changing the transfer of sovereignty.
All of the public health measures in Article 18, and additional ones such as limiting freedom of speech to reduce public exposure to alternative viewpoints (Annex 1, New 5 (e); “…counter misinformation and disinformation”) clash directly with the UDHR. Although freedom of speech is currently the exclusive purview of national authorities and its restriction is generally seen as negative and abusive, United Nations institutions, including the WHO, have been advocating for censoring unofficial views in order to protect what they call “information integrity.”
It seems outrageous from a human rights perspective that the amendments will enable the WHO to dictate countries to require individual medical examinations and vaccinations whenever it declares a pandemic. While the Nuremberg Code and Declaration of Helsinki refer specifically to human experimentation (e.g. clinical trials of vaccines) and the Universal Declaration on Bioethics and Human Rights also to the provider-patient relationship, they can reasonably be extended to public health measures that impose restrictions or changes to human behavior, and specifically to any measures requiring injection, medication, or medical examination which involve a direct provider-person interaction.
If vaccines or drugs are still under trial or not fully tested, then the issue of being the subject of an experiment is also real. There is a clear intent to employ the CEPI ‘100 day’ vaccine program, which by definition cannot complete meaningful safety or efficacy trials within that time span.
Forced examination or medication, outside of a situation where the recipient is clearly not mentally competent to comply or reject when provided with information, is unethical. Requiring compliance in order to access what are considered basic human rights under the UDHR would constitute coercion. If this does not fit the WHO’s definition of infringement on individual sovereignty, and on national sovereignty, then the DG and his supporters need to publicly explain what definition they are using.
The Proposed WHO Pandemic Agreement as a Tool to Manage Transfer of Sovereignty
The proposed pandemic agreement will set humanity in a new era strangely organized around pandemics: pre-pandemic, pandemic, and inter-pandemic. A new governance structure under WHO auspices will oversee the IHR amendments and related initiatives. It will rely on new funding requirements, including the WHO’s ability to demand additional funding and materials from countries and to run a supply network to support its work in health emergencies (Article 12):
In the event of a pandemic, real-time access by WHO to a minimum of 20% (10% as a donation and 10% at affordable prices to WHO) of the production of safe, efficacious and effective pandemic-related products for distribution based on public health risks and needs, with the understanding that each Party that has manufacturing facilities that produce pandemic-related products in its jurisdiction shall take all necessary steps to facilitate the export of such pandemic-related products, in accordance with timetables to be agreed between WHO and manufacturers.
And Article 20 (1):
… provide support and assistance to other Parties, upon request, to facilitate the containment of spill-over at the source.
The entire structure will be financed by a new funding stream separate from current WHO funding – an additional requirement on taxpayers over current national commitments (Article 20 (2)). The funding will also include an endowment of voluntary contributions of “all relevant sectors that benefit from international work to strengthen pandemic preparation, preparedness and response” and donations from philanthropic organizations (Article 20 (2)b).
Currently, countries decide on foreign aid on the basis of national priorities, apart from limited funding that they have agreed to allocate to organizations such as WHO under existing obligations or treaties. The proposed agreement is remarkable not just in greatly increasing the amount countries must give as treaty requirements, but in setting up a parallel funding structure disconnected from other disease priorities (quite the opposite of previous ideas on integration in health financing). It also gives power to an external group, not directly accountable, to demand or acquire further resources whenever it deems necessary.
In a further encroachment into what is normally within the legal jurisdiction of Nation States, the agreement will require countries to establish (Article 15) “…, no-fault vaccine injury compensation mechanism(s),…”, consecrating effective immunity for pharmaceutical companies for harm to citizens resulting from use of products that the WHO recommends under an emergency use authorization, or indeed requires countries to mandate onto their citizens.
As is becoming increasinglyacceptable for those in power, ratifying countries will agree to limit the right of their public to voice opposition to the WHO’s measures and claims regarding such an emergency (Article 18):
… and combat false, misleading, misinformation or disinformation, including through effective international collaboration and cooperation…
As we have seen during the Covid-19 response, the definition of misleading information can be dependent on political or commercial expediency, including factual information on vaccine efficacy and safety and orthodox immunology that could impair the sale of health commodities. This is why open democracies put such emphasis on defending free speech, even at the risk of sometimes being misleading. In signing on to this agreement, governments will be agreeing to abrogate that principle regarding their own citizens when instructed by the WHO.
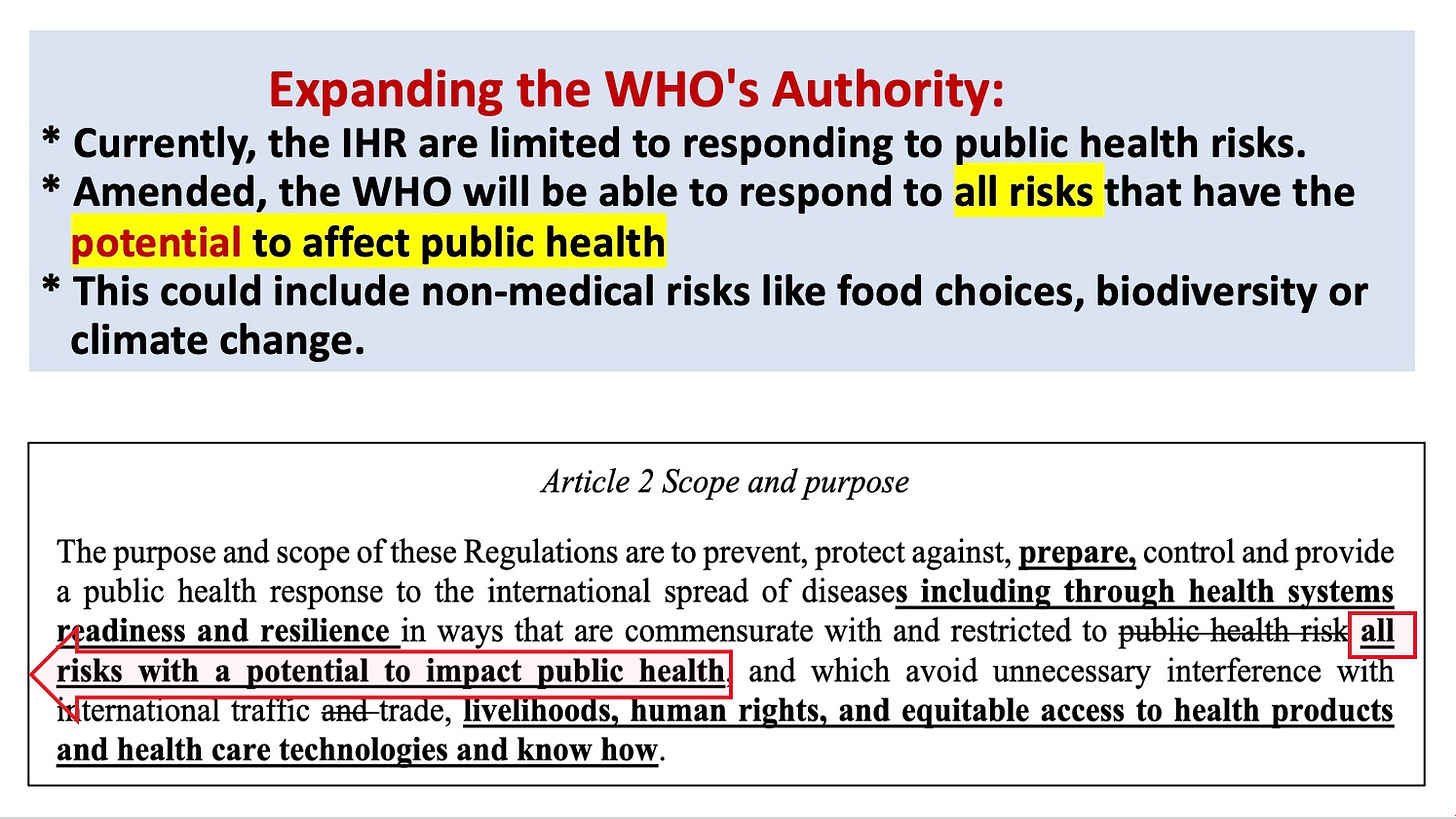
The scope of this proposed agreement (and the IHR amendments) is broader than pandemics, greatly expanding the scope under which a transfer of decision-making powers can be demanded. Other environmental threats to health, such as changes in climate, can be declared emergencies at the DG’s discretion, if broad definitions of ‘One Health’ are adopted as recommended.
It is difficult to think of another international instrument where such powers over national resources are passed to an unelected external organization, and it is even more challenging to envision how this is seen as anything other than a loss of sovereignty. The only justification for this claim would appear to be if the draft agreement is to be signed on the basis of deceit – that there is no intention to treat it other than as an irrelevant piece of paper or something that should only apply to less powerful States (i.e. a colonialist tool).
Will the IHR Amendments and the Proposed Pandemic Agreement be Legally Binding?
Both texts are intended to be legally binding. The IHR already has such status, so the impact of the proposed changes on the need for new acceptance by countries are complicated national jurisdictional issues. There is a current mechanism for rejection of new amendments. However, unless a high number of countries will actively voice their oppositions and rejections, the adoption of the current published version dated February 2023 will likely lead to a future shadowed by the permanent risks of the WHO’s lockdown and lockstep dictates.
The proposed pandemic agreement is also clearly intended to be legally binding. WHO discusses this issue on the website of the International Negotiating Body (INB) that is working on the text. The same legally binding intent is specifically stated by the G20 Bali Leaders Declaration in 2022:
We support the work of the Intergovernmental Negotiating Body (INB) that will draft and negotiate a legally binding instrument that should contain both legally binding and non-legally binding elements to strengthen pandemic PPR…,
A convention, agreement or other international instrument is legally binding under international Law. An agreement on pandemic prevention, preparedness and response adopted under the World Health Organization (WHO) would enable countries around the globe to strengthen national, regional and global capacities and resilience to future pandemics.
The IHR already has standing under international law.
While seeking such status, WHO officials who previously described the proposed agreement as a ‘treaty” are now insisting neither instrument impacts sovereignty. The implication that it is States’ representatives at the WHA that will agree to the transfer, rather than the WHO, is a nuance irrelevant to its claims regarding their subsequent effect.
The WHO’s position raises a real question of whether its leadership is truly ignorant of what is proposed, or is actively seeking to mislead countries and the public in order to increase the probability of acceptance. The latest version dated 30 October 2023 requires 40 ratifications for the future agreement to enter into force, after a two-thirds vote in favor within the WHA. Opposition by a considerable number of countries will therefore be needed to derail this project. As it is backed by powerful governments and institutions, financial mechanisms including IMF and World Bank instruments and bilateral aids are likely to make opposition from lower-income countries difficult to sustain.
The Implications of Ignoring the Issue of Sovereignty
The relevant question regarding these two WHO instruments should really be not whether sovereignty is threatened, but why any sovereignty would be forfeited by democratic States to an organization that is (i) significantly privately funded and bound to obey the dictates of corporations and self-proclaimed philanthropists and (ii) jointly governed by Member States, half of which don’t even claim to be open representative democracies.
If it is indeed true that sovereignty is being knowingly forfeited by governments without the knowledge and consent of their peoples, and based on false claims from governments and the WHO, then the implications are extremely serious. It would imply that leaders were working directly against their peoples’ or national interest, and in support of external interests. Most countries have specific fundamental laws dealing with such practice. So, it is really important for those defending these projects to either explain their definitions of sovereignty and democratic process, or explicitly seek informed public consent.
The other question to be asked is why public health authorities and media are repeating the WHO’s assurances of the benign nature of the pandemic instruments. It asserts that claims of reduced sovereignty are ‘misinformation’ or ‘disinformation,’ which they assert elsewhere are major killers of humankind. While such claims are somewhat ludicrous and appear intended to denigrate dissenters, the WHO is clearly guilty of that which it claims is such a crime. If its leadership cannot demonstrate how its claims regarding these pandemic instruments are not deliberately misleading, its leadership would appear ethically compelled to resign.
The Need for Clarification
TheWHO lists three major pandemics in the past century – influenza outbreaks in the late 1950s and 1960s, and the Covid-19 pandemic. The first two killed less than die each year today from tuberculosis, whilst the reported deaths from Covid-19 never reached the level of cancer or cardiovascular disease and remained almost irrelevant in low-income countries compared to endemic infectious diseases including tuberculosis, malaria, and HIV/AIDs.
No other non-influenza outbreak recorded by the WHO that fits the definition of a pandemic (e.g., rapid spread across international borders for a limited time of a pathogen not normally causing significant harm) has caused greater mortality in total than a few days of tuberculosis (about 4,000/day) or more life-years lost than a few days of malaria (about 1,500 children under 5 years old every day).
So, if it is indeed the case that our authorities and their supporters within the public health community consider that powers currently vested within national jurisdictions should be given over to external bodies on the basis of this level of recorded harm, it would be best to have a public conversation as to whether this is sufficient basis for abandoning democratic ideals in favor of a more fascist or otherwise authoritarian approach. We are, after all, talking about restricting basic human rights essential for a democracy to function.
David Bell, Senior Scholar at Brownstone Institute, is a public health physician and biotech consultant in global health. He is a former medical officer and scientist at the World Health Organization (WHO), Programme Head for malaria and febrile diseases at the Foundation for Innovative New Diagnostics (FIND) in Geneva, Switzerland, and Director of Global Health Technologies at Intellectual Ventures Global Good Fund in Bellevue, WA, USA.
The newly sworn-in New Zealand government intends not to be pushed around by UN resolutions or by the World Health Organisation anymore.
According to a coalition agreement with New Zealand First, the new government will undertake a “National Interest Test” before accepting any agreements from the United Nations or the World Health Organisation’s proposed amendments to the International Health Regulations.
To this aim, the New Zealand Cabinet must “reserve against” proposed amendments to International Health Regulations by 1 December 2023.
On Friday, centre-right National signed coalition agreements with libertarian ACT New Zealand and populist New Zealand First allowing the three parties to form a government, bringing an end to six years of left-wing governments in New Zealand.
Yesterday, New Zealand Governor General Cindy Kiro, who represents British monarch King Charles III as head of state, swore National Party leader Christopher Luxon in as New Zealand’s 42nd prime minister along with ministers of his cabinet at Government House in Wellington. Parliament is expected to sit next week and begin working on new policies.
On the day they were signed, Friday, the incoming government released its coalition agreements which outlined a number of policy plans. You can read the coalition agreement between the New Zealand National Party and ACT New Zealand HERE, and between New Zealand National Party and New Zealand First HERE.
According to the coalition agreement with New Zealand First, one of the most urgent issues the new government must address is that the Cabinet will tell officials not to agree to any policy changes suggested by the World Health Organisation (“WHO”). The coalition agreement states:
Strengthening Democracy and Freedoms
Ensure a ‘National Interest Test’ is undertaken before New Zealand accepts any agreements from the UN and its agencies that limit national decision-making and reconfirm that New Zealand’s domestic law holds primacy over any international agreements.
As part of the above, by 1 December 2023 reserve against proposed amendments to WHO health regulations to allow the incoming government to consider these against a “National Interest Test.”
GAZA – The Palestinian Ministry of Health in Gaza on Thursday held the Israeli occupation forces fully responsible for the lives and safety of the doctors, who were detained on Wednesday.
It announced that it will stop coordinating with World Health Organization (WHO) on the rest of evacuations until the international agency submits a report on the Israeli detention of medical personnel and until they are all released.
The spokesman of the Ministry, Ashraf al-Qudra, said in a press conference at Nasser Hospital in Khan Younis, “The United Nations bears full responsibility for this event, and we await appropriate and urgent measures on their part to address this situation”.
He pointed out that they were informed by the United Nations about coordination with WHO to evacuate those who were present in the Al-Shifa Medical Complex, which is subject to Israeli siege, raids, and destruction, and were stranded inside the hospital with no food, water, medicine, electricity, or security.
Al-Qudra explained that a convoy from the United Nations, represented by WHO, moved on Wednesday to evacuate some of the patients and medical staff who were subjected to the most horrific Nazi practices in addition to starvation.
“We were surprised that this convoy was stopped by the Israeli checkpoint separating the north from south of Gaza, for about seven hours, during which Israeli occupation forces maltreated the patients, their companions, and the medical staff, before arresting a number of them, including Director General of Al-Shifa Medical Complex, Dr. Muhammad Abu Salmiya,” Al-Qudra said.
Mohammad Abu Salmiya, director of al-Shifa Hospital in Gaza City. (By AFP)
He pointed out that WHO has not yet submitted any report to the ministry to clarify what happened, including the numbers and names of detainees, stressing that the inability to communicate with Al-Shifa Medical Complex made them unable to know who was arrested.
The Ministry’s spokesman expressed his concerns over potential liquidation of those detainees.
YouTube (Google) is yet another in a series of tech behemoths that feel the need to declare their stance on content, including its effective algorithmic manipulation, just as US primaries are ushering the country into another year of presidential elections.
Beating around that bush – Google representatives now talk about processes, procedures, and tools of censorship of health-related information that, unfortunately, can easily be “repurposed” to serve other, for example, political ends.
Much of the conversation rests on what Google wants to portray as its laurels from “the previous epidemic” – which too many people and creators see from a diametrically opposed point of view, as a dark time of nearly unbridled censorship and suppression of free speech.
A video now published by Yahoo Finance reveals not only that Google has a “chief clinical officer,” but also how that officer, Michael Howell, sees the role of this super powerful tech corporation in determining what users are likely to see, see first, or see at all on a platform like YouTube.
Howell, naturally, sees nothing wrong with this and even, to all intents and purposes, brags that YouTube is working to make sure legacy media have advantage over independent creators, and that the latter may easily face censorship.
That’s the takeaway from his words, which he chose to phrase thus: YouTube works to “lift up high quality content, even as we work to lower, and make less prominent content that isn’t accurate or helpful to users.”
The whole interview is positioned as an exploration of how “misinformation grows and spreads” supposedly in sync with the amount of content and the number of users. There is even the assertion made by Yahoo that medical sector “misinformation” is not only very present among users but also “in the broader medical community.”
While this may or may not signal continued censorship of “disfavored” medical professionals, YouTube Head of Healthcare & Public Health (yes, that’s a YouTube job title these days, too) Dr. Garth Graham shared that the platform is the first to start “labeling health information that’s coming from licensed doctors, licensed nurses, licensed healthcare professionals.”
And even after all these years of sometimes completely arbitrary censorship YouTube is supposed to be taken as a “credible source of information (users) can trust” – as it works with the National Academy of Medicine and of course, the World Health Organization (WHO) to craft its definitions, and then “raise that up” – i.e., algorithmically promote, at the expense of other content.
Graham had more curious things to say, such as that while clearly committed to censoring what (or, whatever) Google decides is “delicate (sic) and dangerous information” – people are still supposed to view it as an “open platform”!
Either Graham doesn’t know what an open platform is, or he hopes YouTube/Google users don’t.
There’s also a good amount of patronizing toward those users, as in them needing to be hand-held (by Google) pretty much all the way in order to discern information from misinformation and make appropriate decisions.
“So, you know, we’re an open platform, but the real goal is how do you balance getting good information to people at the right time (…) while making sure that we remove delicate or dangerous information.”
Asked how Google has already managed (shocker) to get the government to participate in posting videos promoting their policies and what “conversations” preceded this, the Google exec said that “the entire healthcare eco-system” was already “energized” to get their message across.
And he counted the government as well as hospitals and physicians as part of this eco-system. One of them, last but not least, is the WHO.
What we know for certain from a great number of internal documents that have emerged over the past months both from Twitter and Facebook is that these two were being “led” to do certain things by the government and its agencies.
Google’s position in the interview is suggested to be the opposite – namely, at one point Howell is asked if the company basically instructed all these national and international healthcare players on what content to make, and have “trending” (mostly artificially, one might add.)
Howell dances around this question – or statement – by saying that the (pandemic) produced a community of creators from the health sector.
But as we know, many of them also got their voices silenced, however, that is not something anyone should expect Google to address.
Instead, the talk is obviously about the “approved” community of healthcare creators.
But, says Howell: “If there’s no good content out there that people want to watch, it’s very hard to show (that) content to users.”
And, cynics would say – then you write an algorithm that shoves that content into everybody’s “recommended” videos anyway.
But, Howell decided to claim that “people responded well to YouTube’s partnerships” – where that last word means, government and international bodies and institutions.
The treaty and the proposed amendments instruct nations that they must perform surveillance for potential pandemic pathogens, build or maintain sequencing labs, and both share actual specimens with the WHO (where a BioHub has been created for this purpose) and also share the sequences online. This demands the proliferation of biological weapons agents — which I believe is a crime (based on my interpretation of Security Council Resolution 1540 and the 1972 Biological Weapons Convention).
1 a. The June 2, 2023 “Bureau text” version of the treaty also called for nations performing Gain-of-Function research to reduce “administrative impediments” to the work. In other words, restrictions on the research should be relaxed, which would make lab leaks more likely to occur. This paragraph was removed from the October 30, 2023 version of the treaty.
2. Giving the WHO a blank check to create new rules in the future
The treaty calls for a Conference of Parties and a new WHO Secretariat to be created in the future that will make rules for how the pandemic prevention and response apparatus will work—which provides essentially a blank, signed contract to the WHO to create whatever rules it wants.
3. Liability-free vaccines developed at warp speed will be produced
The treaty calls for rapid vaccine development /production and shaving time off all aspects of vaccine development, testing and manufacture. This requires vaccines to be used without licenses, and the treaty calls for nations to have laws in place to issue Emergency Use Authorizations for this purpose, and to “manage” liability issues. See “The WHO’s Proposed Treaty will Increase Man-Made Pandemics” for more information about this. The US, EU and others have specifically called for 100-day vaccine development and an additional 30 days for production of pandemic vaccines. This would allow for no meaningful human testing.
4. Human rights guarantees have been removed in the new amendments
The amendments removed “human rights, dignity and freedom of persons” from the existing IHR language. Following complaints, this phrase was later inserted into the Treaty–but the treaty may not be accepted in 2024. Meanwhile, the amendments require only a simple majority to pass, are being written in secret, and so it is likely that the most problematic issues will be found in the amendments.
5. Social media surveillance and censorship of citizens is required
Both the amendments and the treaty call for nation states to perform surveillance of their citizens’ social media, and to censor and prevent the spread of information that does not conform to the WHO’s public health narratives. Yet the treaty also calls for citizens to be free to access information, while they are to be protected from “infodemics,” which are defined as too much information. Citizens must also be stopped from spreading mis- and disinformation.
6. We may not learn what is in the amendments until after they are passed
The amendments have been negotiated entirely in secret for the past nine months, while there have been multiple consecutive drafts of the pandemic treaty released to the public during that time. And while the negotiated amendments were to be tabled for public review in January, the WHO’s principal legal officer has provided a legal fig leaf to avoid the obligation of making them public 4 months ahead of the vote. Will the public even see the amendments before a vote on them occurs?
Why is there such secrecy regarding the proposed amendments?
7. The WHO Director-General could become your personal physician
According to the proposed amendments, the WHO D-G would be able to commandeer and move medical supplies from one country to another, decide what treatments can be used, and restrict the use of other treatments.
8. When will the WHO be able to use its newly minted powers?
The amendments will come into force after a declaration of a Public Health Emergency of International Concern (PHEIC) is made. However, a declaration of a potential PHEIC will also trigger these powers. The powers can be extended even after a PHEIC is over, as we have seen with COVID and monkeypox (MPOX) declarations by the D-G.
The treaty will be in force continuously, requiring no declaration or pandemic to confer new powers to the WHO.
Israeli Prime Minister Benjamin Netanyahu issued a series of threats toward Iran and its interlocutors in the West, including the US, as serious negotiations on Iran’s nuclear program seem more plausible.
As a possible rapprochement looms between the US and Iran, Netanyahu has attempted to impose impossible Israeli conditions on the negotiators, such as the full dismantling of Iran’s nuclear program, not to mention threatening military force.
Whatever the deal that could materialize between Iran and the West, Israel is going to find itself before an open-ended path. One can foresee three possible scenarios… continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.