Here’s the skinny on what happened yesterday and today regarding the booster dose
By Meryl Nass, MD | September 23, 2021
Last Friday, FDA’s advisory committee (VRBPAC) voted 16 to 2 against giving a license to a third Pfizer booster shot for everyone age 16 and up.
Although a second vote at Friday’s meeting had not been planned, another question was hastily developed. That question asked whether the vaccine could be licensed for a third booster dose for high risk people under the age of 65. That vote got a unanimous yes.
The panels decisions are not final. The FDA is obliged to take the panels advice into consideration, but it is not required to adopt it. So yesterday, the FDA issued a license for the Pfizer vaccine for the booster dose.
But in doing so, FDA added an additional category of people for the booster dose, a category that had not been included in the Advisory Committee’s vote:
- “individuals 18 through 64 years of age whose frequent institutional or occupational exposure to SARS-CoV-2 puts them at high risk of serious complications of COVID-19 including severe COVID-19.”
This is what I call weasel wording. This statement does not make sense. People whose occupation puts them at high risk of exposure to COVID are no more likely to be at high risk of serious complications or severe COVID-19 than anyone else. They are at higher risk of developing COVID, but not at higher risk of serious COVID.
What FDA did (and you know who did this: Peter Marks, head of CBER and Janet Woodcock, acting Commissioner, are the only people with the authority to come up with this BS) was to take the VRBPAC approval for people with underlying conditions that put them at high risk for severe COVID, and twist it into an approval for all health care workers, staff at schools and colleges, grocery store workers, big box employees, etc.
Why? Because a license is necessary to impose a mandate, that’s why.
It looked like the weasels had won again. However, there was a small hoop left to jump through before any mandates came down.
While FDA determines how a drug or vaccine should be licensed or authorized for use, the CDC’s ACIP committee is the group responsible for creating the recommendations for use of the vaccine in different demographic groups.
And so ACIP did what it never does. It rejected the CDC’s proposal to widen the license for the third dose to all with potential occupational exposures. the ACIP limited their approval to what the FDA advisory committee had voted for last Friday. As CNBC noted,
… Dr. Leana Wen [member of the Council on Foreign Relations and the World Economic Forum], an emergency physician and former Baltimore health commissioner, on Twitter called the CDC panel’s vote to reject boosters more widely a “mistake.”
“Really, we are not allowing healthcare workers, many of whom got vaccinated in back in December, to get a booster? What about teachers in cramped classrooms where masks aren’t required?” she tweeted, adding CDC Director Dr. Rochelle Walensky should overrule the recommendation.
… In a paper published days before an FDA advisory meeting last week, a leading group of scientists said available data showed vaccine protection against severe disease persists, even as the effectiveness against mild disease wanes over time. The authors, including two high-ranking FDA officials and multiple scientists from the World Health Organization, contended in the medical journal The Lancet that widely distributing booster shots to the general public is not appropriate at this time.
I think 2 things happened. The propaganda that the vaccines still prevent serious disease while perhaps not preventing mild disease stood in the way of approving boosters to prevent mild disease. Why give a potentially dangerous booster to prevent a cold? It doesn’t make sense.
Second, everyone on those committees knew that if the vaccine’s third dose did get approved for a huge swath of the general public, it would be mandated for themselves in no time. A third dose would have been required for every member of both FDA’s and CDC’s advisory committees. I don’t think they were ready for that. And maybe they weren’t ready for the resistance from those who took the 2 shots thinking they were done… and now, it seems they could get into a situation where they could be fired for not having a third dose. What about more and more doses?
Or maybe the large demonstrations in Australia and Europe were influencing those advisory committee members…
American Medical Association Instructs Doctors to Deceive
By Dr. Joseph Mercola | September 23, 2021
The Winter 2021 “AMA COVID-19 Guide: Background/Messaging on Vaccines, Vaccine Clinical Trials & Combatting Vaccine Misinformation,”1 issued by the American Medical Association (AMA) raises serious questions about the AMA’s adherence to transparency, honesty, ethics and the moral standards to which it will hold its members.
The AMA was founded in 1847 and is the largest professional association and lobbying group of physicians and medical students in the U.S. According to the AMA itself, its mission is to promote the art and science of medicine and the betterment of public health.
How then do they explain this “COVID-19 messaging guide,” which explicitly teaches doctors how to deceive their patients and the media when asked tough questions about COVID-19, treatment options and COVID shots?
AMA Teaches Doctors How to Deceive
“It is critical that physicians and patients have confidence in the safety and efficacy of COVID-19 vaccines as they become available for public use,” the “AMA COVID-19 Guide” states, adding:2
“To overcome vaccine hesitancy and ensure widespread vaccine acceptance among all demographic groups, physicians and the broader public health community must continue working to build trust in vaccine safety and efficacy, especially in marginalized and minoritized communities with historically well-founded mistrust in medical institutions.”
Indeed, the entire guide is aimed at teaching doctors how to foster confidence in the medical profession in general, as it pertains to treatment of COVID-19, but in particular as it pertains to the experimental COVID shots.
The guide provides “suggested narratives” for various engagements, such as when communicating on social media, as well as “talking points to guide external communications,” such as when being interviewed. It lists nine specific “key messages” that they want doctors to focus on when communicating about COVID-19. These key messages can be summarized as follows:
Express confidence in vaccine development
-
- Stress the importance of vaccines
- Highlight the need to combat the spread of vaccine misinformation
- Adhere to updated ethical guidance for physicians and medical personnel, which says they have a moral obligation to get vaccinated themselves
- Give general vaccine recommendations, such as the recommendation for everyone over the age of 6 months, including pregnant women, to get an annual flu shot
- Stress the importance of eliminating nonmedical vaccine exemptions
- Highlight the increased availability of flu vaccines, and the importance of getting a flu shot even if you’ve gotten a COVID injection
- Highlight the importance of including minorities, both in vaccine trials and as trusted messengers who can “promote social pressure” to get minorities vaccinated and dispel historical distrust in medical institutions
- Denounce scientific analyses “predicated on personal opinions, anecdote and political ideologies”
AMA Concerned About Disinformation
On page 7 of the guide, under the science narrative heading, the AMA declares it is “deeply concerned that rampant disinformation and the politicization of health issues are eroding public confidence in science and undermining trust in physicians and medical institutions,” adding that “Science should be grounded in a common understanding of facts and evidence and able to empower people to make informed decisions about their health.”3
To that end, the AMA is calling upon “all elected officials to affirm science and fact in their words and actions,” and for media to “be vigilant in communicating factual information” and to “challenge those who chose to trade in misinformation.”
AMA Then Instructs Doctors on How to Disinform
It’s a disappointment, then, to find the AMA instructing doctors on how to misinform the public using a variety of psychological and linguistic tools. Perhaps one of the most egregious examples of this is the recommended “COVID-19 language swaps” detailed on page 9.
As you can see below, the AMA explicitly instructs doctors to swap out certain words and terms for other, more narrative-affirming choices. Shockingly, this includes swapping “hospitalization rates” to “deaths” — two terms that are not even remotely interchangeable!
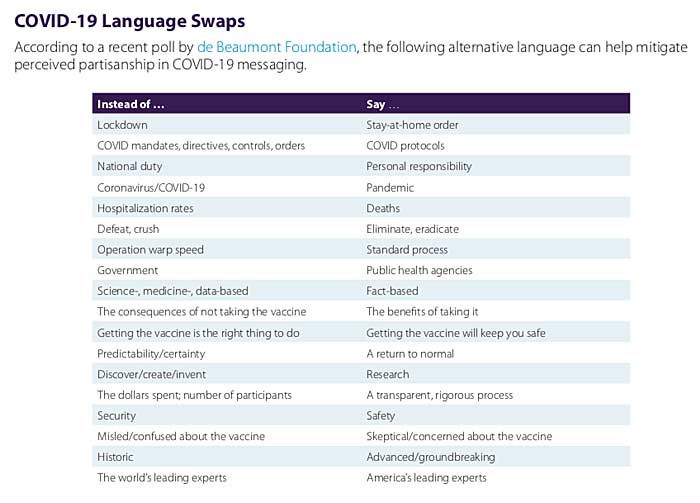
Another highly questionable word swap is to not address the nitty, gritty details of vaccine trials, such as the number of participants, and instead simply refer to these trials as having gone through “a transparent, rigorous process.”
Swapping the factual term “Operation Warp Speed” for “standard process” is another outrageous misdirection. The two simply aren’t interchangeable. In fact, they’re actually diametrically opposed to one another. Standard process for vaccine development includes a long process of over a decade and a large number of steps that were either omitted or drastically shortened for the COVID shots.
Following standard process is what makes vaccine development take, on average, 10 years and often longer. Operation Warp Speed allowed vaccine makers to slap together these COVID shots in about nine months from start to finish. You cannot possibly say that the two terms describe an identical process.
The Power of Language
Other language swaps are less incredible but still highlight the fact that the AMA wants its members to help push a very specific and one-sided narrative that makes power-grabbing overreaches and totalitarian tactics sound less bad than they actually are, and make questionable processes sound A-OK.
Language is a powerful tool with which we shape reality,4 because it shapes how we think about things. As noted by storyteller and filmmaker Jason Silva:5
“The use of language, the words you use to describe reality, can in fact engender reality, can disclose reality. Words are generative… We create and perceive our reality through language. We think reality into existence through linguistic construction in real-time.”
For example, “lockdown” sounds like involuntary imprisonment imposed by a totalitarian regime, which is what it is, whereas “stay-at-home order” sounds far less draconian. After all, “home” is typically associated with comfort and safety.
The same goes for using “COVID protocols” in lieu of “COVID mandates, directives, controls and orders.” “Protocols” sounds like something that is standard procedure, as if the COVID measures are nothing new, whereas “mandates, controls and orders” imply that, indeed, we’re in medical fascism territory, which we are.
How to Steer, Block, Deflect and Stall Inconvenient Questions
The AMA could have instructed its members to simply stick to the facts and be honest — and in some sections, it does do that — but it doesn’t end there. Rather, the AMA provides a full page of instructions on how to steer the conversation, and how to block, deflect and stall when faced with tough questions where an honest answer might actually break the official narrative.
Here’s a sampling of these instructions. I encourage you to read through page 8 of the guide, and pay attention to these psychological tricks when listening to interviews or reading the news.
Interviewing techniques
-
- Steer the conversation back to the narrative by saying: “Before we leave that matter, let me add …”
- Block a tough question by saying: “That’s [proprietary, confidential etc], but what I can tell you is …”
- Deflect an unwanted question by saying: “That’s a common misperception but the reality is …”
- Redirect away from an unwanted question, back to the official narrative by saying: “I don’t have the details on that, but what I know is …”
- Stall by saying: Repeat the question asked, or acknowledge the question by saying, “I’m glad you asked …”
It’s worth noting that the AMA also stresses that: 1) Doctors are to speak for the AMA, and 2) doctors are NOT to offer their personal views. Speaking for the AMA is listed under “Your Responsibilities” when being interviewed, while not discussing personal views is listed under “Interview Don’ts.”
AMA Is Rapidly Eroding All Credibility
The AMA’s guidance isn’t all bad. Some of its advice makes perfect sense. But the inclusion of language swaps that result in false statements being made, and tools for steering, blocking, deflecting, redirecting and stalling in order to avoid direct answers do nothing but erode credibility and thus trust in the medical community.
Its direct instruction to not share personal views is another trust-eroding strategy. When people talk to their doctor, they want to hear what that doctor actually thinks, based on their own knowledge and experience.
They don’t expect their doctor — or a doctor appearing in an interview — to simply rehash a narrative dictated by the AMA. If we cannot trust our medical professionals to give their honest opinions and give direct answers, there’s little reason to even discuss our concerns with them, and that’s the opposite of what the AMA claims it seeks to achieve.
The AMA is concerned about the proliferation of misinformation and eroding trust, yet it’s telling its members to keep their professional views to themselves and lie about COVID deaths. With this guidance document, the AMA is essentially implicating itself as a source and instigator of medical misinformation that ultimately might injure patients.
In a Stew Peters Show interview (see bitchute), Dr. Bryan Ardis criticized the AMA guidance document, pointing out that while the AMA claims it put out the guidance to prevent political ideologies from dictating medicine, it is actually proving that the AMA itself is deferring to political ideology rather than medical facts.
The AMA wants its members to act as propagandists for a particular narrative — using “politically correct language” — rather than sharing information and acting in accordance with their own conscience and professional insight. As noted by Peters:
“If a doctor’s just going to repeat what the AMA tells them, why have doctors at all? You can get plenty of starving propagandists at any liberal college, but instead we want to turn our medical professionals into ideological zombies with stethoscopes.”
Sources and References
The Emperor Has No Clothes: COVID Math Simply Doesn’t Add Up
The Defender | September 23, 2021
From the beginning of the series of events branded as a global health emergency, many people have smelled a rat.
Whether one looks at leaders’ willingness to engage in wanton economic destruction, or the rapidity with which billionaires have amassed new wealth or the multisectoral efforts to link and mine people’s intimate data, it is not hard to recognize that something much larger than a health crisis is afoot.
However, even if one restricts oneself to the narrow confines of the health narrative, 18 months of data — emerging in spite of ferocious censorship — have repeatedly illustrated that the official story is full of lies and omissions.
One of the biggest holes in the story is the trail of destruction that the experimental COVID vaccines are leaving in their wake, with hundreds of thousands of reported injuries in the U.S. alone and, according to some statisticians, as many as 150,000 dead Americans.
With this level of damage after just nine months, now is as good a time as any to reexamine “COVID math” and highlight some of the embedded falsehoods that cast serious doubt on official and corporate pronouncements about risks and benefits.
The false case for vaccinating kids
Pfizer’s CEO, veterinarian Albert Bourla, is currently drumming up buzz in anticipation of a likely decision by the U.S. Food and Drug Administration (FDA) to green-light emergency use of his company’s COVID vaccine in children ages 5-11. To buttress his arguments, Bourla claims that pediatric COVID cases are on the rise.
However, setting aside the questionable PCR testing methodology being used to identify these “cases” (that is, until the Centers for Disease Control and Prevention (CDC) retires the PCR test at the end of the year), recent studies show reported COVID-19 hospitalizations — “one of the primary metrics for tracking the severity of the coronavirus pandemic” — have been grossly inflated for children. In actuality, pediatric COVID hospitalization rates are “vanishingly small.”
One fact, especially, bears repeating: Through age 19, children and adolescents have a 99.9973% COVID-19 survival rate. This information, which has been a constant throughout the reported pandemic, is reiterated in the most recent analyses by Stanford physician, epidemiologist and statistician John Ioannidis, who has been a steadfast critic of COVID alarmism from the very beginning.
And Ioannidis’s good news does not stop with the 19-and-unders. Until people hit their seventies, all age groups have survival rates well over 99%:
- 0-19: 99.9973%
- 20-29: 99.986%
- 30-39: 99.969%
- 40-49: 99.918%
- 50-59: 99.73%
- 60-69: 99.41%
- 70+: 97.6% (non-institutionalized)
- 70+: 94.5% (institutionalized and non-institutionalized)
As Off-Guardian’s Kit Knightly wrote about another Ioannidis study this past spring, “With every new study, with every new paper, the ‘deadly’ pandemic gets less and less, well, deadly.”
At that time, Ioannidis ascertained that the global infection fatality rate was 95% lower than the one disseminated by the World Health Organization (WHO).
Risks: the example of myocarditis
Commenting on the pediatric hospital studies — in which more than half of the children entered the hospital for reasons having nothing to do with anything resembling COVID — a reporter wrote, “The implications … are enormously important, as reports of pediatric hospitalizations have regularly made headlines over the past year, greatly affecting public perceptions about risks to children.”
Those headlines and perceptions likely will prompt some parents to rush into the waiting arms of their local vaccinator.
Bourla and other Pfizer executives have remained mum about the many 12- to 17-year-olds who are ending up hospitalized and injured after taking the company’s experimental mRNA product.
Sadly, the post-jab statements made by these disabled teens and their parents share a common refrain: influenced by skewed media reports from some corners, and without the benefit of information censored in other corners, they were not aware of the risks.
What are some of those risks?
A study out of Ottawa recently estimated that one of every 625 Moderna doses administered results in myocarditis (heart inflammation), as does an estimated one in 2,500 doses of the Pfizer shot, with a “tight temporal association between receipt of mRNA vaccine and subsequent development of symptoms in a relatively short time frame afterwards.”
The Ottawa authors pointed out that their estimates — based on “direct investigation of patients” who were “largely in the vulnerable 18- 30 age category” — were tenfold higher than the incidence produced by a less rigorous study that looked only at “administrative health data.”
The authors also noted the relevance of their findings for the “ongoing public debate regarding proposals for vaccination of children under the age of 16.”
According to another new study, healthy boys between the ages of 12 and 15, with no underlying medical conditions, were four to six times more likely to be diagnosed with vaccine-related myocarditis than they were to be hospitalized with COVID.
The Ottawa study may have pointed more of a finger at the Moderna shot, but a late August CDC update on heart problems reported to the Vaccine Adverse Event Reporting System (VAERS) in the aftermath of COVID vaccination suggests the Pfizer injection may be equally treacherous, especially for young men.
Using a statistically credible estimate that VAERS data are underreporting COVID injuries by a factor of 41, Steve Kirsch (founder of the COVID-19 Early Treatment Fund) has calculated (slide #15) that roughly one in 318 boys ages 16 and 17 can be expected to develop myocarditis after two Pfizer doses, and a third booster dose of the Pfizer vaccine could escalate that risk to a frightening one in 25.
Another recent look at VAERS data by Health Impact News showed that in 2021, to date, 12- to 19-year-olds have been 50 times more likely to experience heart problems after receiving experimental COVID shots — and nearly eight times more likely to die — compared to all other FDA-approved vaccines combined.
Considering adverse events reported to VAERS over the past decade for all vaccines combined, there has been a “highly anomalous” 1,000% increase in total adverse events reported thus far for 2021.
With these kinds of findings, the pushback against giving children the shots is growing louder and stronger.
The authors of a just-published study in Toxicology Reports openly ask, “Why are we vaccinating children against COVID-19?” They warn that younger age groups could experience longer-term effects (such as myocarditis) “that, if serious, would be borne by children/adolescents for potentially decades.”
Safe treatments withheld, dangerous protocols incentivized
John Ioannidis’s new study shows that institutionalization negatively skews outcomes for the 70-plus age group. Whereas the survival rate is 97.5% for the community-dwelling elderly 70 or older, it falls to 94.5% when institutionalized elderly in that age group are included in the count.
Why are the institutionalized elderly faring so poorly? In the UK, reporters and undertakers have furnished one possible answer, sharing troubling on-the-ground descriptions about illegal euthanasia alleged to be taking place on a widespread basis in care homes as well as hospitals.
In the U.S., meanwhile, regulators, hospitals and pharmacies have implemented equally disturbing policies that require withholding inexpensive drugs, such as ivermectin and hydroxychloroquine — shown elsewhere to be effective and safe — while essentially forcing hospitalized COVID patients onto protocols that are not only unhelpful but murderous.
Mexico City achieved up to a 76% reduction in COVID hospitalizations by making ivermectin-based home treatment kits widely available. With evidence like this, why are U.S. hospitals stubbornly adhering to life-threatening protocols involving remdesivir (known to produce fluid in the lungs and longer hospital stays) and intubation?
One rather dark answer is that hospitals are not only immune from liability for any fatal outcomes resulting from this approach but receive hefty federal payments — including a 20% Medicare “add-on” that may sum up to as much as $40,000 for patients who spend four or more days on a ventilator.
Although hospitals may hasten to refute that these factors are at play, the growing number of hospital whistleblowers is becoming hard to ignore.
In March, Baylor University’s Dr. Peter McCullough lamented that as many as 85% of COVID deaths could have been prevented with early treatment using ivermectin and other formerly commonplace drugs disallowed by regulators and for which U.S. pharmacies will no longer fill “off-label” prescriptions.
There is international agreement with McCullough’s position that “large reductions in COVID-19 deaths are possible using ivermectin,” and the U.S.-based Front Line COVID-19 Critical Care (FLCCC) Alliance describes the drug as potentially the “global solution to the pandemic.”
However, instead of applauding these advocates of early intervention for their efforts to save lives, they have become, according to mRNA vaccine inventor Dr. Robert Malone, the focus of intense “coordinated strategies” to subject them to “derision and attacks and character assassination.”
Those ‘anomalous’ deaths
In analyses presented by Steve Kirsch to the FDA (slide #6), Kirsch summarized data showing the COVID vaccines are killing more people than they are saving — including producing six excess deaths for each life reportedly saved in nursing home residents, and five excess deaths per life saved according to Pfizer’s early clinical trial data.
Independent statisticians estimate the injections are linked to roughly 470 deaths per million doses administered. (By way of comparison, CDC researchers once conceded that smallpox vaccination was responsible for one death per million.)
In February, studies out of Israel were already showing the Pfizer shot (the only one used in Israel) was causing “mortality hundreds of times greater in young people compared to mortality from coronavirus without the vaccine, and dozens of times more in the elderly.”
Investigative journalist Corey Lynn of Corey’s Digs pointed out the CDC’s methodology for calculating COVID vaccine-related deaths is highly misleading because it is based on the number of doses administered, rather than on the number of people who receive injections.
Lynn’s analysis shows this methodology reduces the percentage of deaths almost by half, “an incredible mathematical error, surely done with intention.”
Another CDC ploy for undercounting the damage done by the COVID injections has to do with the agency’s definition of “fully vaccinated. The CDC currently considers as “unvaccinated” anyone who is not two weeks out from their second dose (in a two-dose series) or two weeks out from a single-dose vaccine. (And as Children’s Health Defense President Mary Holland recently pointed out, “unvaccinated” could “soon mean anyone who’s missing the latest booster dose,” with even more boosters likely in store down the road.)
Given that 17% of the deaths reported to VAERS have occurred within 48 hours of COVID vaccination, it is clear many U.S. vaccine deaths are being counted as “unvaccinated” deaths and misattributed to COVID-19 or other causes.
In the UK, however, public health data show that 80% of “COVID-19” deaths in August were in people who had been vaccinated, and hospitalization rates were 70% higher in the vaccinated than in the unvaccinated.
Increasingly, members of the public are not fooled by the statistical shenanigans. When a Detroit TV channel recently tried to drum up hostility against the unvaccinated by asking viewers to submit tales of recalcitrant uninjected relatives dying from COVID-19, they instead got more than 182,000 comments about loved ones who had died or been injured after receiving one or more COVID shots.
These replies provide compelling evidence that what we are now experiencing is a “pandemic of the vaccinated.”
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Putin the Poisoner? More Doubts Over Attempts to Delegitimize Russia’s Leader
By Philip Giraldi | Strategic Culture Foundation | September 23, 2021
It seems that ever since Hillary Clinton lost to Donald Trump in the U.S. presidential election of 2016 the western media and numerous politicians have been working especially hard to convince the world that the Russian government is little better than a modern version of Josef Stalin’s USSR. Part of the effort can be attributed to the Democratic Party’s desire to blame someone other than the unattractive candidate Hillary for the defeat, but there is also something more primitive operating behind the scenes, something like a desire to return to a bipolar world in which one knew one’s enemies and one’s friends.
The anti-Russian bias has manifested itself in a number of ways, to include the fabricated libel referred to as Russiagate, but it also featured personal denigration of the Russian leadership as a rogue regime inclined to employ assassination by poisoning against its critics and political opponents.
The first widely publicized assassination of a Russian dissident took place in London in 2006. Alexander Litvinenko, a former Federal Security Service (FSB) officer and critic of the government who had sought asylum in England, died after he met two Russian acquaintances in a hotel bar and was reportedly poisoned by a dose of radioactive polonium inserted into his cup of tea. The Russians whom he had met with were named by the British police but the Russian government refused extradition requests. Without any evidence, the British media claimed that Litvinenko had been killed under orders from Putin personally.
More recently, the poisoning of former Russian intelligence agent Sergei Skripal and his daughter Yulia on March 4th, 2018 made headlines around the world. Sergei was living near Salisbury England and his daughter was visiting from Moscow when they were found unconscious on a park bench. A policeman later investigating the incident also suffered from the effects of what appeared to be a nerve agent, which investigative sources claimed had been sprayed on to the front door handle of the Skripal residence. Both Sergei and Yulia survived the incident.
There was quite a bit that was odd about the Skripal case, which came at a time when there was considerable tension between Russia and the NATO allies over issues like Syria and Ukraine. Russian President Vladimir Putin was regularly demonized, seen in the western media as a malevolent presence stalking the world stage.
Observers noted that the British investigation of the poisoning relied from the start “… on circumstantial evidence and secret intelligence.” And there was inevitably a rush to judgment. British Foreign Secretary Boris Johnson blamed Russia before any chemical analysis of the alleged poisoning could have taken place. British Prime Minister Theresa May told Parliament shortly thereafter to blame the Kremlin and demand a Russian official response to the event in 36 hours, declaring that the apparent poisoning was “very likely” caused by a made-in-Russia nerve agent referred to by its generic name novichok. The British media was soon on board, spreading the government line that such a highly sensitive operation would require the approval of President Putin himself. Repeated requests by Russia to obtain a sample of the alleged nerve agent for testing were rejected by the British government in spite of the fact that a military grade nerve agent would have surely killed both the Skripals as well as anyone else within 100 yards.
The expulsion of scores of Russian diplomats and imposition of sanctions soon followed with the United States and other countries following suit. The report of the new sanctions was particularly surprising as Yulia Skripal had subsequently announced that she intends to return to her home in Russia, leading to the conclusion that even one of the alleged victims did not believe the narrative being promoted by the British and American governments.
The response within the United States was also immediate and threatening. A New York Times editorial on March 12th entitled Vladimir Putin’s Toxic Reach thundered: “The attack on the former spy, Sergei Skripal, who worked for British intelligence, and his daughter Yulia, in which a police officer who responded was also poisoned, was no simple hit job. Like the 2006 murder of Alexander Litvinenko, another British informant, who was poisoned with radioactive polonium 210, the attack on Mr. Skripal was intended to be as horrific, frightening and public as possible. It clearly had the blessing of President Vladimir Putin, who had faced little pushback from Britain in the Litvinenko case. The blame has been made clearer this time and this attack on a NATO ally needs a powerful response both from that organization and, perhaps more important, by the United States.”
But the story of the poisoning of the Skripals began to come apart very quickly. Former UK Ambassador Craig Murray detailed how the narrative was cooked by “liars” in the government to make it look as if the poisoning had a uniquely Russian fingerprint. Meanwhile prize winning U.S. investigative reporter Gareth Porter summed up the actual evidence or lack thereof, for Russian involvement, suggesting that the entire affair was “based on politically-motivated speculation rather than actual intelligence.”
The head of Britain’s own top secret chemical weapons facility Porton Down even contradicted claims made by May and Johnson, saying that he did not know if the nerve agent was actually produced in Russia as the chemical formula was revealed to the public in a scientific paper in 1992 and there were an estimated twenty countries capable of producing it. Some speculated that a false flag operation by the British themselves, the CIA or Mossad, was not unthinkable. Development of novichok type poisons is known to have taken place at both Porton Down and at the U.S. chemical weapon facility Fort Dietrich Maryland.
But the most damning evidence opposing a Russian role in the alleged poisonings was that Moscow had no motive to kill a former British double agent who had been released from a Kremlin prison in a spy swap after ten years in prison and who was no longer capable of doing any damage. If Moscow had wanted him dead, they could have killed him while he was still in Russian custody. Putin had an election coming up and Russia was to be the host of the World Cup in the summer, an event that would be an absolute top priority to have go smoothly without any complications from a major spy case.
There is now new evidence that the claims of Russian involvement in the alleged assassination attempt were fraudulent, engineered by the British government, possibly in collusion with American intelligence, to smear Vladimir Putin in particular. Bulgarian investigative journalist Dilyana Gaytandzhieva has written an article entitled “UK Defense Ministry Document Reveals Skripals’ Blood Samples Could have been Manipulated.”
Relying on a series of British-version Freedom of Information Act queries, Gaytandzhieva determined that there was a considerable gap between the time when it was claimed the Skirpals’ blood was drawn and the time when it was actually tested for possible poisons at Porton Down. The gap is inexplicable and means in legal terms that the chain of custody was broken. It further suggests that the samples could have been deliberately diverted and tampered with.
Gaytandzhieva, who provides copies of the relevant government documents in her article, sums up her case as “New evidence has emerged of gross violations during the UK investigation into the alleged poisoning of Sergei and Yulia Skripal in Salisbury on 4th March 2018.” The Ministry of Defense, which is in charge of the British military laboratory DSTL Porton Down which analyzed the Skripals blood samples responded to a request that “Our searches have failed to locate any information that provides the exact time that the samples were collected.” The samples “were collected at some point between 16:15 on 4 March 2018 and 18:45 on 5 March 2018. Even the time of arrival at Porton Down is indicated as “approximate.”
She also cites some expert testimony, “A British toxicologist [commented] that ‘It is inconceivable that with such a visibility case, and the obvious significance of any and all biological samples, normal and expected sample logging and documentation did not take place. The person drawing the sample, in any clinical or forensic setting knows that the date and time must be recorded, and the donor positively identified. In a criminal case, evidence gleaned from these samples would be thrown out as inadmissible… This lack of protocol is either very sloppy or clandestine.”
If the Skripals case sounds very similar to the recent alleged poisoning of Russian dissident Alexei Navalny it should, as the same rush to judgement by many of the same players took place. Navalny became ill while on a flight from Tomsk to Moscow on August 20th, 2020 and was taken to a hospital in Omsk after an emergency landing. The Russian hospital could not find any poison in his blood and attributed his condition to metabolic disorder. Two days later, the Russian government allowed Navalny to be transported to a hospital in Germany which then announced that the Putin government had poisoned Navalny with novichok, which became the story that was read and televised worldwide. Interestingly, there is now evidence that the air medevac team was standing by and ready even before anyone knew Navalny was ill, suggesting that it was planned in advance. Once in Germany, as in the case of the Skripal poisoning, the evidence of the crime mysteriously disappeared for a while. Blood samples and water bottles allegedly containing the novichok were sent to the Organization for the Prohibition of Chemical Weapons offices for verification. They took five days to arrive.
The doubts regarding both the Skripals and Navalny poisonings might suggest that the Cold War never really ended, at least from the Anglo-American perspective. Whatever Vladimir Putin has been doing for the past three years hardly touches on genuine U.S. or British interests, unless one considers the governance of places like Ukraine and Syria to be potentially threatening. That someone, somewhere, somehow seems to be making an effort to isolate and delegitimize President Putin by making him an international poisoner is tragedy elevated by its absurdity to the level of farce. It serves no purpose and, in the end, can only lead to mistrust on all sides that can in turn become very, very ugly.
New York’s New Gov Threatens To Replace Unvaccinated Hospital Workers With ‘Foreigners’
By Tyler Durden | Zero Hedge | September 23, 2021
New York’s first female governor Kathy Hochul, who took the reins in the Empire State after her predecessor and former boss, Andrew Cuomo, finally resigned, is showing the state’s recalcitrant healthcare workers just how understanding and progressive she can be.
During a press briefing with reporters in Rochester Wednesday, Hochul told a group of reporters that she hoped all unvaccinated workers would meet Monday’s deadline to get the jab, or lose their jobs.
For those who continue to resist – including nearly 20% of the state’s hospital and nursing-home workers – they will be replaced. Possibly by foreign workers.
Faced with this, it makes sense to wonder how NY State, which has no immigration-related authority, could even credibly make such a threat? But Hochul says there have been conversations with the Department of State (albeit on a “limited basis”) about the possibility of doling out emergency visas to foreign workers.
“To those who won’t, we’ll be replacing people. And I have a plan that’s going to be announced very shortly,” she said.
“We’ve identified a whole range of opportunities we have to help supplement them.”
Hochul said state officials were “working closely with various hospital systems to find out where we can get other individuals to come in and supplement places like nursing homes.”
“We’re also reaching out to the Department of State to find out about visas for foreign workers, on a limited basis, to bring more nurses over here,” she said.
Per the Department of Health’s records, 19% of the state’s hospital workers remained unvaccinated as of Sept. 15, and 18% of nursing home employees remained unvaccinated as of Wednesday.
Starting Monday, employers can fire unvaccinated workers who don’t have a “valid medical exemption” (though employees who claim religious exemption are also immune until Oct. 12 due to a temporary injunction issued by a federal judge in Utica).
The plaintiffs in that case, almost all of them Catholic, oppose vaccines because they “employ aborted fetus cell lines in their testing, development, or production.”
Though the US Conference of Bishops says it’s okay for Catholics to take these vaccines if no alternatives are available, and Pope Francis has of course spoken out in favor of vaccination.
Circling back to the situation in New York, while Hochul is probably reveling in her first opportunity to play “hardball” – a game for which her predecessor was famous – New York health workers can probably rest easy – at least when it comes to the foreign worker threat. The State Department couldn’t process all those SIVs for Afghan collaborators in a timely manner. What makes you think they’ll be able to dole them out to foreign workers, who probably also haven’t been vaccinated. Where does Hochul think these foreign workers are going to come from? Europe?
Could a Simple Saline Solution Stop COVID — and Maybe All Viruses?
By Dr. Joseph Mercola | September 23, 2021
New research shows that a simple saline solution stops replication of SARS-CoV-2 — the virus that causes COVID-19 — almost in its tracks.
The study began in early 2020 and was reported on the preprint server bioRxiV in August 2020. It’s now published in the journal Pharmacology & Translational Science, with the authors saying “In this study, we found that 1.5% NaCl inhibited virus replication by 100% in Vero cells, and 1.1% NaCl was sufficient to inhibit virus replication by 88% in Calu-3 cells.”
The researchers based their work on previous confirmed success with in vitro activity of sodium chloride (NaCl) against other RNA viruses such as mengovirus, respiratory syncytial virus, influenza A, human coronavirus 229E and coxsackievirus B3.
The solution they used is considered “hypertonic,” in other words, it has a higher concentration of dissolved NaCl in it than would normally be found in an NaCl solution. Using the formula on monkey kidney cells, they found it’s possible that “hypertonic solutions could be investigated as a prophylaxis or an alternative treatment for COVID-19 patients.”
Noting that “nebulized 3% hypertonic saline treatment for infants with moderate to severe bronchiolitis is safe without any adverse events, such as bronchospasm, cough, or wheezing aggravation” and that previous studies show that “hypertonic saline nasal irrigation and gargling may have played a role in reducing symptoms and duration of illness caused by COVID-19,” they proposed that COVID treatment could involve a hypertonic form of nasal saline.
SOURCES:
Pending International Treaty Empowering The WHO
By Dr Urmie Ray B.A., M.A., Mmath, Ph.d. | Principia Scientific | September 23, 2021
Between 29 November and 1 December 2021, member states are meeting in a special session with the World Health Organisation to discuss, possibly sign, a new treaty on pandemic preparedness and response.
This decision was taken in March 2021 and backed by 26 nations, among which Australia, Canada, Iceland, Norway, Republic of Korea, South Africa, Ukraine, United Kingdom, United States, Uruguay and Member States of the European Union.1
To be noted is the absence of Russia, China, and India among these 26.
The International Health Regulations (2005)[i] signed by 196 countries already provide States the legal right to:
“– review travel history in affected areas;
– review proof of medical examination and any laboratory analysis;
– require medical examinations;
– review proof of vaccination or other prophylaxis;
– require vaccination or other prophylaxis;
– place suspect persons under public health observation;
– implement quarantine or other health measures for suspect persons;
– implement isolation and treatment where necessary of affected persons;
– implement tracing of contacts of suspect or affected persons;
– refuse entry of suspect and affected persons;
– refuse entry of unaffected persons to affected areas; and
– implement exit screening and/or restrictions on persons from affected areas.”
In other words, all the measures applied round the world since 2020, including mandatory vaccination, are in effect legal under this former treaty.
In particular, it critically changes the definition of “quarantine” from that in the 1969 IHR. There, it is used only in the expression “in quarantine” defined to be a “state or condition during which measures are applied by a health authority to a … means of transport or container, to prevent the spread of disease, reservoirs of disease or vectors of disease from the object of quarantine”.[i]
The 2005 revised IHR use the term by itself, and define it as “the restriction of activities and/or separation from others of suspect persons who are not ill or of suspect baggage, containers, conveyances or goods in such a manner as to prevent the possible spread of infection or contamination”.
This represents a subtle but critical shift from protection of the community to restriction of individual liberties.
The implementation of quarantine and other coercive measures on all, including surveillance and vaccination, is legalized: the expression “suspect persons” criminalizes every individual, both healthy and unhealthy.
Indeed, it covers anyone “considered by a State Party as having been exposed, or possibly exposed, to a public health risk and that could be a possible source of spread of disease”. Of significance is the use of “possibly” and “possible”, hence not just anyone definitely known to be a risk factor.
So Why The Need For A New Treaty?
The answer was given by WHO Director-General Tedros Adhanom Ghebreyesus. “It’s the one major change, Tedros said, that would do the most to boost global health security and also empower the World Health Organization.”[i]
The 2005 revised IHR still leave some authority to States and require certain conditions for a health event in a particular State to be considered sufficiently serious globally for the State to be forced to communicate it to WHO. Once communicated, it becomes the prerogative of the director general of WHO to determine whether it “constitutes a public health emergency”, but in collaboration with that particular State.
Although it should be added that in case of disagreement, the director general decides after consultation with the emergency committee of WHO, and passed a certain period no State can reject or emit reservations about the IHR or any later amendments. Still, to some extent, measures implemented remain the result of a dialogue between “IHR focal points” in each country and “WHO IHR contact points”.
What is particularly important is that the above listed measures, although rendered legal by the IHR, can under this treaty, only be recommended by the WHO, not imposed, and that it is up to the States to proceed towards their imposition, and to verify they are followed by means already existing in their respective countries.[ii]
The new treaty would address the above “weaknesses” of the IHR as they are considered to be, by ensuring “independent verification, monitoring, and compliance”. Given the clearly expressed end of empowering the WHO, should one conclude that “independent” means under the authority of WHO rather than the States themselves?[i]
Further the IHR cover “public health hazards and public health emergencies of international concern”, whereas the treaty will concern “all hazards”, not just pandemics. In the latter case, it would take over from the IHR once a pandemic is officially declared by the WHO.[ii]
This said, the treaty would presumably also make clear the idea expressed in the 2007 CDC “Interim Pre-pandemic planning guidance”,[i] namely overruling the need of a pandemic to implement restrictive measures. All that would be needed would be for an event to be declared a “public health emergency of pandemic potential”.
Given that any future event is always hypothetical, does this enable the maintenance of the measures for an indeterminate period? For it can always be claimed that a pandemic will occur especially were the measures lifted. This raises many questions, all the more so as the event would no long need to be of “international concern as in the current IHR”. “Measures”, as advised, should also go beyond the current scope of IHR”, in particular to cover the production and supply of vaccines, diagnostics, and treatments”.[ii]
The treaty would unlike the IHR also go beyond sanitary issues and allow the implementation of measures against “social and economic disruptions” as well as “broader disaster risk”.[i]
Would this in effect not only make it legal to put an end to criticisms, and thus to the freedom of expression, and make it possible to control any public antagonism against restrictive measures through “urgent international assistance”,[ii] namely not just by national police or military forces, but international ones?
In short, would the treaty not provide the international legal framework for derogation from the civil and political rights guaranteed “even in time of emergency threatening the life of the nation” by The Syracuse Principles on the Limitation and Derogation Provisions in the International Covenant on Civil and Political Rights drafted in 1984,[iii] namely:
“the right to life; freedom from torture, cruel, inhuman or degrading treatment or punishment, and from medical or scientific experimentation without free consent; freedom from slavery or involuntary servitude; the right not be be imprisoned for contractual debt; the right not to be convicted or sentenced to a heavier penalty by virtue of retroactive criminal legislation; the right to recognition as a person before the law; and freedom of thought, conscience and religion. These rights are not derogable under any conditions even for the asserted purpose of preserving the life of the nation”?
For the Syracuse Principles only ensure that “No state party shall” in any circumstance “derogate from the Covenant’s” above guarantees”. However, according to the new treaty, would the WHO, possibly together with the help of other international bodies, not become an occupying planetary power, with each State a collaborating subservient unit, like France in 1940, and hence without any power to ensure that non-derogable rights are protected?
Last but not least, “[t]rying to revise the IHR would be a long process and take several years. … In addition, any amendment made to the IHR will enter into force only two years after its adoption. A world in crisis cannot afford to wait this long.”[i] Why such a rush to get the treaty ratified?
It should not be forgotten that among the main contributors of WHO are the Bill and Melinda Gates foundation and the vaccine alliance (GAVI). It established in 2000 and whose initial funding it essentially provided – a “unique public-private partnership … bring[ing] together key UN agencies, governments, the vaccine industry, private sector and civil society”.[i]
References
[1] https://apps.who.int/gb/ebwha/pdf_files/WHA74/A74_ACONF7-en.pdf
[1] https://www.who.int/health-topics/international-health-regulations#tab=tab_1
[1] https://www.who.int/csr/ihr/WHA58-en.pdf
[1] https://www.who.int/csr/ihr/WHA58-en.pdf
[1] Ibid.
[1] https://www.centerforhealthsecurity.org/cbn/2007/cbnreport_02072007.html
[1] Ibid.
[1] Ibid.
NPR Embarrasses Itself With Misinformation and Blatant Lies About Dr. Mercola
By Dr. Joseph Mercola | September 23, 2021
In a broadcast rife with disinformation, misinformation and outright lies, National Public Radio has embarrassed itself while maligning Dr. Mercola.
The broadcast opens with NPR host Robin Young calling Dr. Mercola “the biggest disseminator of COVID lies,” and then proceeding to call America’s Frontline Doctors, an independent organization of which Dr. Mercola is not a member and with which he has zero affiliation, “his” group that “he created.”
Young then interviews Dr. Humayun Chaudhry, president and CEO of the Federation of State Medical Boards (FSMB) about FSMB’s recommendation to state medical boards to fine, suspend and revoke the licenses of doctors who don’t follow the mainstream COVID narrative.
Together, Young and Chaurdhry repeatedly show that they’re either ignorant or deliberately spreading their own misinformation and disinformation when it comes to vaccine hesitancy, COVID treatments such as ivermectin (referring to it as an animal drug that has shown “absolutely no ability” to treat COVID) and medical professionals who are questioning the vaccines.
Asking whether Dr. Mercola still has his license to practice, Young claims a second time that he’s the “biggest distributor of misinformation” and that he doesn’t seem to care about that, as he’s making a lot of money by “selling alternatives to traditional standard care.”
Obviously, Young is only getting her news from the dark money-funded Center for Countering Digital Hate (CCDH), which analyzed 483 pieces of social media content over six weeks to come up with what they called the “Misinformation Dozen,” with Dr. Mercola at the top of their list. The thing is Young is spreading more misinformation herself, seeing that Facebook’s vice president of content policy Monika Bickert issued a statement saying that there not only is no evidence that CCDH’s list is accurate, but that the people named by CCDH were responsible for only 0.05% of all vaccine content on Facebook’s site, not the 73% CCDH claims.
Young and Chaudhry conclude their show by calling on social media companies to better watch their forums to censor COVID and vaccine “misinformation” and for individual states to take a more active role in investigating and revoking the licenses of doctors who don’t toe the COVID line.
SOURCES:
30 facts you NEED to know: Your Covid Cribsheet

By Kit Knightly | OffGuardian | September 22, 2021
We get a lot of e-mails and private messages along these lines “do you have a source for X?” or “can you point me to mask studies?” or “I know I saw a graph for mortality, but I can’t find it anymore”. And we understand, it’s been a long 18 months, and there are so many statistics and numbers to try and keep straight in your head.
So, to deal with all these requests, we decided to make a bullet-pointed and sourced list for all the key points. A one-stop-shop.
Here are key facts and sources about the alleged “pandemic”, that will help you get a grasp on what has happened to the world since January 2020, and help you enlighten any of your friends who might be still trapped in the New Normal fog (click links to skip):
“Covid deaths” – Lockdowns – PCR Tests – “asymptomatic infection” – Ventilators – Masks – Vaccines – Deception & Foreknowledge
*
PART I: “COVID DEATHS” & MORTALITY
1. The survival rate of “Covid” is over 99%. Government medical experts went out of their way to underline, from the beginning of the pandemic, that the vast majority of the population are not in any danger from Covid.
Almost all studies on the infection-fatality ratio (IFR) of Covid have returned results between 0.04% and 0.5%. Meaning Covid’s survival rate is at least 99.5%.
*
2. There has been NO unusual excess mortality. The press has called 2020 the UK’s “deadliest year since world war two”, but this is misleading because it ignores the massive increase in the population since that time. A more reasonable statistical measure of mortality is Age-Standardised Mortality Rate (ASMR):

By this measure, 2020 isn’t even the worst year for mortality since 2000, In fact since 1943 only 9 years have been better than 2020.
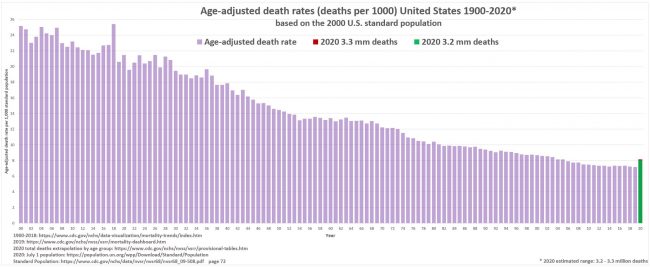
Similarly, in the US the ASMR for 2020 is only at 2004 levels:
For a detailed breakdown of how Covid affected mortality across Western Europe and the US click here. What increases in mortality we have seen could be attributable to non-Covid causes [facts 7, 9 & 19].
*
3. “Covid death” counts are artificially inflated. Countries around the globe have been defining a “Covid death” as a “death by any cause within 28/30/60 days of a positive test”.
Healthcare officials from Italy, Germany, the UK, US, Northern Ireland and others have all admitted to this practice:
Removing any distinction between dying of Covid, and dying of something else after testing positive for Covid will naturally lead to over-counting of “Covid deaths”. British pathologist Dr John Lee was warning of this “substantial over-estimate” as early as last spring. Other mainstream sources have reported it, too.
Considering the huge percentage of “asymptomatic” Covid infections [14], the well-known prevalence of serious comorbidities [fact 4] and the potential for false-positive tests [fact 18], this renders the Covid death numbers an extremely unreliable statistic.
*
4. The vast majority of covid deaths have serious comorbidities. In March 2020, the Italian government published statistics showing 99.2% of their “Covid deaths” had at least one serious comorbidity.
These included cancer, heart disease, dementia, Alzheimer’s, kidney failure and diabetes (among others). Over 50% of them had three or more serious pre-existing conditions.
This pattern has held up in all other countries over the course of the “pandemic”. An October 2020 FOIA request to the UK’s ONS revealed less than 10% of the official “Covid death” count at that time had Covid as the sole cause of death.
*
5. Average age of “Covid death” is greater than the average life expectancy. The average age of a “Covid death” in the UK is 82.5 years. In Italy it’s 86. Germany, 83. Switzerland, 86. Canada, 86. The US, 78, Australia, 82.
In almost all cases the median age of a “Covid death” is higher than the national life expectancy.
As such, for most of the world, the “pandemic” has had little-to-no impact on life expectancy. Contrast this with the Spanish flu, which saw a 28% drop in life expectancy in the US in just over a year. [source]
*
6. Covid mortality exactly mirrors the natural mortality curve. Statistical studies from the UK and India have shown that the curve for “Covid death” follows the curve for expected mortality almost exactly:
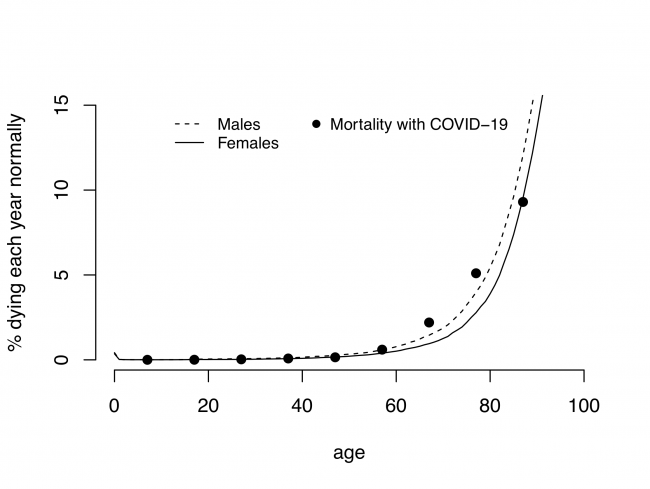

The risk of death “from Covid” follows, almost exactly, your background risk of death in general.
The small increase for some of the older age groups can be accounted for by other factors.[facts 7, 9 & 19]
*
7. There has been a massive increase in the use of “unlawful” DNRs. Watchdogs and government agencies have reported huge increases in the use of Do Not Resuscitate Orders (DNRs) over the last twenty months.
In the US, hospitals considered “universal DNRs” for any patient who tested positive for Covid, and whistleblowing nurses have admitted the DNR system was abused in New York.
In the UK there was an “unprecdented” rise in “illegal” DNRs for disabled people, GP surgeries sent out letters to non-terminal patients recommending they sign DNR orders, whilst other doctors signed “blanket DNRs” for entire nursing homes.
A study done by Sheffield Univerisity found over one-third of all “suspected” Covid patients had a DNR attached to their file within 24 hours of hospital admission.
Blanket use of coerced or illegal DNR orders could account for any increases in mortality in 2020/21.[Facts 2 & 6]
*
PART II: LOCKDOWNS
8. Lockdowns do not prevent the spread of disease. There is little to no evidence lockdowns have any impact on limiting “Covid deaths”. If you compare regions that locked down to regions that did not, you can see no pattern at all.

“Covid deaths” in Florida (no lockdown) vs California (lockdown)
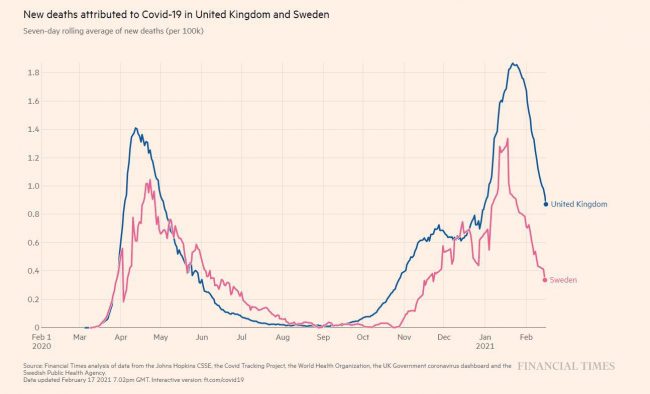
“Covid deaths” in Sweden (no lockdown) vs UK (lockdown)
*
9. Lockdowns kill people. There is strong evidence that lockdowns – through social, economic and other public health damage – are deadlier than the “virus”.
Dr David Nabarro, World Health Organization special envoy for Covid-19 described lockdowns as a “global catastrophe” in October 2020:
We in the World Health Organization do not advocate lockdowns as the primary means of control of the virus[…] it seems we may have a doubling of world poverty by next year. We may well have at least a doubling of child malnutrition […] This is a terrible, ghastly global catastrophe.”
A UN report from April 2020 warned of 100,000s of children being killed by the economic impact of lockdowns, while tens of millions more face possible poverty and famine.
Unemployment, poverty, suicide, alcoholism, drug use and other social/mental health crises are spiking all over the world. While missed and delayed surgeries and screenings are going to see increased mortality from heart disease, cancer et al. in the near future.
The impact of lockdown would account for the small increases in excess mortality [Facts 2 & 6]
*
10. Hospitals were never unusually over-burdened. the main argument used to defend lockdowns is that “flattening the curve” would prevent a rapid influx of cases and protect healthcare systems from collapse. But most healthcare systems were never close to collapse at all.
In March 2020 it was reported that hospitals in Spain and Italy were over-flowing with patients, but this happens every flu season. In 2017 Spanish hospitals were at 200% capacity, and 2015 saw patients sleeping in corridors. A paper JAMA paper from March 2020 found that Italian hospitals “typically run at 85-90% capacity in the winter months”.
In the UK, the NHS is regularly stretched to breaking point over the winter.
As part of their Covid policy, the NHS announced in Spring of 2020 that they would be “re-organizing hospital capacity in new ways to treat Covid and non-Covid patients separately” and that “as result hospitals will experience capacity pressures at lower overall occupancy rates than would previously have been the case.”
This means they removed thousands of beds. During an alleged deadly pandemic, they reduced the maximum occupancy of hospitals. Despite this, the NHS never felt pressure beyond your typical flu season, and at times actually had 4x more empty beds than normal.
In both the UK and US millions were spent on temporary emergency hospitals that were never used.
*
PART III: PCR TESTS
11. PCR tests were not designed to diagnose illness. The Reverse-Transcriptase Polymerase Chain Reaction (RT-PCR) test is described in the media as the “gold standard” for Covid diagnosis. But the Nobel Prize-winning inventor of the process never intended it to be used as a diagnostic tool, and said so publicly:
PCR is just a process that allows you to make a whole lot of something out of something. It doesn’t tell you that you are sick, or that the thing that you ended up with was going to hurt you or anything like that.”
*
12. PCR Tests have a history of being inaccurate and unreliable. The “gold standard” PCR tests for Covid are known to produce a lot of false-positive results, by reacting to DNA material that is not specific to Sars-Cov-2.
A Chinese study found the same patient could get two different results from the same test on the same day. In Germany, tests are known to have reacted to common cold viruses. A 2006 study found PCR tests for one virus responded to other viruses too. In 2007, a reliance on PCR tests resulted in an “outbreak” of Whooping Cough that never actually existed. Some tests in the US even reacted to the negative control sample.
The late President of Tanzania, John Magufuli, submitted samples goat, pawpaw and motor oil for PCR testing, all came back positive for the virus.
As early as February of 2020 experts were admitting the test was unreliable. Dr Wang Cheng, president of the Chinese Academy of Medical Sciences told Chinese state television “The accuracy of the tests is only 30-50%”. The Australian government’s own website claimed “There is limited evidence available to assess the accuracy and clinical utility of available COVID-19 tests.” And a Portuguese court ruled that PCR tests were “unreliable” and should not be used for diagnosis.
You can read detailed breakdowns of the failings of PCR tests here, here and here.
*
13. The CT values of the PCR tests are too high. PCR tests are run in cycles, the number of cycles you use to get your result is known as your “cycle threshold” or CT value. Kary Mullis said: “If you have to go more than 40 cycles[…]there is something seriously wrong with your PCR.”
The MIQE PCR guidelines agree, stating: “[CT] values higher than 40 are suspect because of the implied low efficiency and generally should not be reported,” Dr Fauci himself even admitted anything over 35 cycles is almost never culturable.
Dr Juliet Morrison, virologist at the University of California, Riverside, told the New York Times: Any test with a cycle threshold above 35 is too sensitive…I’m shocked that people would think that 40 [cycles] could represent a positive…A more reasonable cutoff would be 30 to 35″.
In the same article Dr Michael Mina, of the Harvard School of Public Health, said the limit should be 30, and the author goes on to point out that reducing the CT from 40 to 30 would have reduced “covid cases” in some states by as much as 90%.
The CDC’s own data suggests no sample over 33 cycles could be cultured, and Germany’s Robert Koch Institute says nothing over 30 cycles is likely to be infectious.
Despite this, it is known almost all the labs in the US are running their tests at least 37 cycles and sometimes as high as 45. The NHS “standard operating procedure” for PCR tests rules set the limit at 40 cycles.
Based on what we know about the CT values, the majority of PCR test results are at best questionable.
*
14. The World Health Organization (Twice) Admitted PCR tests produced false positives. In December 2020 WHO put out a briefing memo on the PCR process instructing labs to be wary of high CT values causing false positive results:
when specimens return a high Ct value, it means that many cycles were required to detect virus. In some circumstances, the distinction between background noise and actual presence of the target virus is difficult to ascertain.
Then, in January 2021, the WHO released another memo, this time warning that “asymptomatic” positive PCR tests should be re-tested because they might be false positives:
Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology.
*
15. The scientific basis for Covid tests is questionable. The genome of the Sars-Cov-2 virus was supposedly sequenced by Chinese scientists in December 2019, then published on January 10th 2020. Less than two weeks later, German virologists (Christian Drosten et al.) had allegedly used the genome to create assays for PCR tests.
They wrote a paper, Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR, which was submitted for publication on January 21st 2020, and then accepted on January 22nd. Meaning the paper was allegedly “peer-reviewed” in less than 24 hours. A process that typically takes weeks.
Since then, a consortium of over forty life scientists has petitioned for the withdrawal of the paper, writing a lengthy report detailing 10 major errors in the paper’s methodology.
They have also requested the release of the journal’s peer-review report, to prove the paper really did pass through the peer-review process. The journal has yet to comply.
The Corman-Drosten assays are the root of every Covid PCR test in the world. If the paper is questionable, every PCR test is also questionable.
*
PART IV: “ASYMPTOMATIC INFECTION”
16. The majority of Covid infections are “asymptomatic”. From as early as March 2020, studies done in Italy were suggesting 50-75% of positive Covid tests had no symptoms. Another UK study from August 2020 found as much as 86% of “Covid patients” experienced no viral symptoms at all.
It is literally impossible to tell the difference between an “asymptomatic case” and a false-positive test result.
*
17. There is very little evidence supporting the alleged danger of “asymptomatic transmission”. In June 2020, Dr Maria Van Kerkhove, head of the WHO’s emerging diseases and zoonosis unit, said:
From the data we have, it still seems to be rare that an asymptomatic person actually transmits onward to a secondary individual,”
A meta-analysis of Covid studies, published by Journal of the American Medical Association (JAMA) in December 2020, found that asymptomatic carriers had a less than 1% chance of infecting people within their household. Another study, done on influenza in 2009, found:
… limited evidence to suggest the importance of [asymptomatic] transmission. The role of asymptomatic or presymptomatic influenza-infected individuals in disease transmission may have been overestimated…”
Given the known flaws of the PCR tests, many “asymptomatic cases” may be false positives.[fact 14]
*
PART V: VENTILATORS
18. Ventilation is NOT a treatment for respiratory viruses. Mechanical ventilation is not, and never has been, recommended treatment for respiratory infection of any kind. In the early days of the pandemic, many doctors came forward questioning the use of ventilators to treat “Covid”.
Writing in The Spectator, Dr Matt Strauss stated:
Ventilators do not cure any disease. They can fill your lungs with air when you find yourself unable to do so yourself. They are associated with lung diseases in the public’s consciousness, but this is not in fact their most common or most appropriate application.
German Pulmonologist Dr Thomas Voshaar, chairman of Association of Pneumatological Clinics said:
When we read the first studies and reports from China and Italy, we immediately asked ourselves why intubation was so common there. This contradicted our clinical experience with viral pneumonia.
Despite this, the WHO, CDC, ECDC and NHS all “recommended” Covid patients be ventilated instead of using non-invasive methods.
This was not a medical policy designed to best treat the patients, but rather to reduce the hypothetical spread of Covid by preventing patients from exhaling aerosol droplets.
*
19. Ventilators killed people. Putting someone who is suffering from influenza, pneumonia, chronic obstructive pulmonary disease, or any other condition which restricts breathing or affects the lungs, will not alleviate any of those symptoms. In fact, it will almost certainly make it worse, and will kill many of them.
Intubation tubes are a source of potential a infection known as “ventilator-associated pneumonia”, which studies show affects up to 28% of all people put on ventilators, and kills 20-55% of those infected.
Mechanical ventilation is also damaging to the physical structure of the lungs, resulting in “ventilator-induced lung injury”, which can dramatically impact quality of life, and even result in death.
Experts estimate 40-50% of ventilated patients die, regardless of their disease. Around the world, between 66 and 86% of all “Covid patients” put on ventilators died.
According to the “undercover nurse”, ventilators were being used so improperly in New York, they were destroying patients’ lungs:
This policy was negligence at best, and potentially deliberate murder at worst. This misuse of ventilators could account for any increase in mortality in 2020/21 [Facts 2 & 6]
*
PART VI: MASKS
20. Masks don’t work. At least a dozen scientific studies have shown that masks do nothing to stop the spread of respiratory viruses.
One meta-analysis published by the CDC in May 2020 found “no significant reduction in influenza transmission with the use of face masks”.
Another study with over 8000 subjects found masks “did not seem to be effective against laboratory-confirmed viral respiratory infections nor against clinical respiratory infection.”
There are literally too many to quote them all, but you can read them: [1][2][3][4][5][6][7][8][9][10] Or read a summary by SPR here.
While some studies have been done claiming to show mask do work for Covid, they are all seriously flawed. One relied on self-reported surveys as data. Another was so badly designed a panel of experts demand it be withdrawn. A third was withdrawn after its predictions proved entirely incorrect.
The WHO commissioned their own meta-analysis in the Lancet, but that study looked only at N95 masks and only in hospitals. [For full run down on the bad data in this study click here.]
Aside from scientific evidence, there’s plenty of real-world evidence that masks do nothing to halt the spread of disease.
For example, North Dakota and South Dakota had near-identical case figures, despite one having a mask-mandate and the other not:
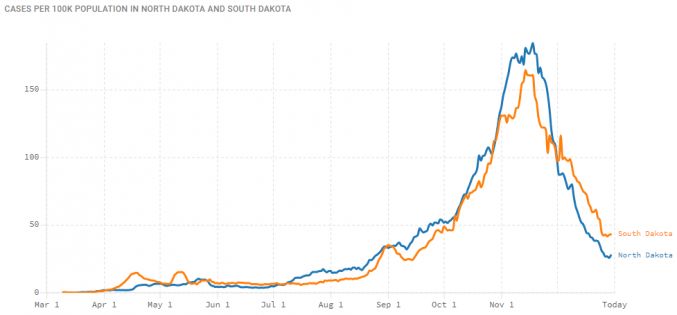
In Kansas, counties without mask mandates actually had fewer Covid “cases” than counties with mask mandates. And despite masks being very common in Japan, they had their worst flu outbreak in decades in 2019.
*
21. Masks are bad for your health. Wearing a mask for long periods, wearing the same mask more than once, and other aspects of cloth masks can be bad for your health. A long study on the detrimental effects of mask-wearing was recently published by the International Journal of Environmental Research and Public Health
Dr. James Meehan reported in August 2020 he was seeing increases in bacterial pneumonia, fungal infections, facial rashes .
Masks are also known to contain plastic microfibers, which damage the lungs when inhaled and may be potentially carcinogenic.
Childen wearing masks encourages mouth-breathing, which results in facial deformities.
People around the world have passed out due to CO2 poisoning while wearing their masks, and some children in China even suffered sudden cardiac arrest.
*
22. Masks are bad for the planet. Millions upon millions of disposable masks have been used per month for over a year. A report from the UN found the Covid19 pandemic will likely result in plastic waste more than doubling in the next few years., and the vast majority of that is face masks.
The report goes on to warn these masks (and other medical waste) will clog sewage and irrigation systems, which will have knock on effects on public health, irrigation and agriculture.
A study from the University of Swansea found “heavy metals and plastic fibres were released when throw-away masks were submerged in water.” These materials are toxic to both people and wildlife.
*
PART VII: VACCINES
23. Covid “vaccines” are totally unprecedented. Before 2020 no successful vaccine against a human coronavirus had ever been developed. Since then we have allegedly made 20 of them in 18 months.
Scientists have been trying to develop a SARS and MERS vaccine for years with little success. Some of the failed SARS vaccines actually caused hypersensitivity to the SARS virus. Meaning that vaccinated mice could potentially get the disease more severely than unvaccinated mice. Another attempt caused liver damage in ferrets.
While traditional vaccines work by exposing the body to a weakened strain of the microorganism responsible for causing the disease, these new Covid vaccines are mRNA vaccines.
mRNA (messenger ribonucleic acid) vaccines theoretically work by injecting viral mRNA into the body, where it replicates inside your cells and encourages your body to recognise, and make antigens for, the “spike proteins” of the virus. They have been the subject of research since the 1990s, but before 2020 no mRNA vaccine was ever approved for use.
*
24. Vaccines do not confer immunity or prevent transmission. It is readily admitted that Covid “vaccines” do not confer immunity from infection and do not prevent you from passing the disease onto others. Indeed, an article in the British Medical Journal highlighted that the vaccine studies were not designed to even try and assess if the “vaccines” limited transmission.
The vaccine manufacturers themselves, upon releasing the untested mRNA gene therapies, were quite clear their product’s “efficacy” was based on “reducing the severity of symptoms”.
*
25. The vaccines were rushed and have unknown longterm effects. Vaccine development is a slow, laborious process. Usually, from development through testing and finally being approved for public use takes many years. The various vaccines for Covid were all developed and approved in less than a year. Obviously there can be no long-term safety data on chemicals which are less than a year old.
Pfizer even admit this is true in the leaked supply contract between the pharmaceutical giant, and the government of Albania:
the long-term effects and efficacy of the Vaccine are not currently known and that there may be adverse effects of the Vaccine that are not currently known
Further, none of the vaccines have been subject to proper trials. Many of them skipped early-stage trials entirely, and the late-stage human trials have either not been peer-reviewed, have not released their data, will not finish until 2023 or were abandoned after “severe adverse effects”.
*
26. Vaccine manufacturers have been granted legal indemnity should they cause harm. The USA’s Public Readiness and Emergency Preparedness Act (PREP) grants immunity until at least 2024.
The EU’s product licensing law does the same, and there are reports of confidential liability clauses in the contracts the EU signed with vaccine manufacturers.
The UK went even further, granting permanent legal indemnity to the government, and any employees thereof, for any harm done when a patient is being treated for Covid19 or “suspected Covid19”.
Again, the leaked Albanian contract suggests that Pfizer, at least, made this indemnity a standard demand of supplying Covid vaccines:
Purchaser hereby agrees to indemnify, defend and hold harmless Pfizer […] from and against any and all suits, claims, actions, demands, losses, damages, liabilities, settlements, penalties, fines, costs and expenses
*
PART VIII: DECEPTION & FOREKNOWLEDGE
27. The EU was preparing “vaccine passports” at least a YEAR before the pandemic began. Proposed COVID countermeasures, presented to the public as improvised emergency measures, have existed since before the emergence of the disease.
Two EU documents published in 2018, the “2018 State of Vaccine Confidence” and a technical report titled “Designing and implementing an immunisation information system” discussed the plausibility of an EU-wide vaccination monitoring system.
These documents were combined into the 2019 “Vaccination Roadmap”, which (among other things) established a “feasibility study” on vaccine passports to begin in 2019 and finish in 2021:
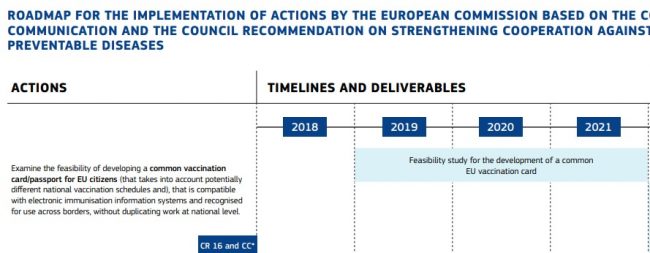
This report’s final conclusions were released to the public in September 2019, just a month before Event 201 (below).
*
28. A “training exercise” predicted the pandemic just weeks before it started. In October 2019 the World Economic Forum and Johns Hopkins University held Event 201. This was a training exercise based on a zoonotic coronavirus starting a worldwide pandemic. The exercise was sponsored by the Bill and Melinda Gates Foundation and GAVI the vaccine alliance.
The exercise published its findings and recommendations in November 2019 as a “call to action”. One month later, China recorded their first case of “Covid”.
*
29. Since the beginning of 2020, the Flu has “disappeared”. In the United States, since February 2020, influenza cases have allegedly dropped by over 98%.

It’s not just the US either, globally flu has apparently almost completely disappeared.
Meanwhile, a new disease called “Covid”, which has identical symptoms and a similar mortality rate to influenza, is supposedly sweeping the globe.
*
30. The elite have made fortunes during the pandemic. Since the beginning of lockdown the wealthiest people have become significantly wealthier. Forbes reported that 40 new billionaires have been created “fighting the coronavirus”, with 9 of them being vaccine manufacturers.
Business Insider reported that “billionaires saw their net worth increase by half a trillion dollars” by October 2020.
Clearly that number will be even bigger by now.
*
These are the vital facts of the pandemic, presented here as a resource to help formulate and support your arguments with friends or strangers. Thanks to all the researchers who have collated and collected this information over the last twenty months, especially Swiss Policy Research.
My front-row view of the Covid drug corruption scandal
This is an open letter from Dr Steven J Hatfill – June 10, 2021
Dear America,
This is the story of possibly the greatest corruption scandal in our country’s history.
This is the story of how petty bureaucrats and drug companies unjustly discredited an inexpensive FDA-approved drug that would have prevented Covid-19 hospitalisations and deaths for political spite and financial gain. These perpetrators, who now hold more significant positions in government, need to be held accountable for over 500,000 American deaths and the disruption of our economy.
This is the story of how a few key government officials failed to implement our well-formulated National Pandemic Plan and their weaponisation of a dangerously complicit mainstream media.
I tell this story because we, the People, deserve answers – those responsible need to be held accountable for their actions. The Covid-19 pandemic was a proverbial ‘warning shot across our bow’. Therefore we must forever prioritise pandemic preparedness as critical to our national security.
We deserve better. We deserve the truth. We deserve answers. We deserve JUSTICE.
I hope my words and timeline will help clarify what has happened, who is involved, and what action must be taken to protect our health and freedom.
I am Dr Steven Hatfill. I am a specialist physician, recognised virologist, biological weapons expert and I worked as an outside adviser to the Executive Office of the President of the United States from February 2020 through the inaugural transition period of 2021. My statements are not speculation because I had a front-row seat from the very beginning of the pandemic. My subsequent published papers and articles have been painstakingly referenced and fact-checked.
Some will tell you this is just another conspiracy theory, so I ask you to read on and judge for yourselves.
Factual events
2005 The United States creates its first National Pandemic Plan, outlining the actions to combat a serious respiratory viral disease pandemic. This is based on the previous Biological Weapons Improved Response Plan.
2008 President Obama closes the White House Global Health Security Office.
2013 After the SARS and MERS outbreaks, Chinese virologists collect hundreds of samples from bats for study at the Wuhan Institute of Virology (WIV). Collaborative research begins on the coronaviruses, including gain of function (GOF) experiments (research which involves increasing the capacity of a pathogen to cause illness) in China and the University of North Carolina at Chapel Hill.
2014 The West Africa Ebola virus outbreak occurs. Dr Anthony Fauci MD [director of the National Institute of Allergy and Infectious Diseases (NIAID)] promotes a single layer of gloves for nursing Ebola patients and other inadequate protective measures. His instructions endanger the lives of health care workers, and national guidelines for protection must be urgently updated.
2014 United States’ Centers for Disease Control and Prevention (CDC) and the World Health Organisation (WHO) ban GOF research. The ban was implemented for 2014-2017.
2015 Chinese virologists and the University of North Carolina at Chapel Hill conduct unauthorised GOF experiments on coronaviruses.
2017 The 2005 Health and Human Services (HHS) National Pandemic Plan is updated. The specific responsibilities of local authorities, states and the federal government have been clearly stated. The national plan is to use early, outpatient antiviral drug treatment, home quarantine, and case contact tracing to cover the ‘vaccine gap’ (the time needed to develop a vaccine to combat any pathogen).
December 2019 Chinese authorities report the first outbreak of Covid-19 in Wuhan. On January 21, 2020, the first recognised case of Covid-19 occurs in the United States.
February 2020 Dr Steven Hatfill MD, a specialist physician and recognised virologist, is brought into the White House as an outside medical adviser.
Some members of the Covid-19 Task Force are considering the use of hydroxychloroquine (HCQ), a safe and effective FDA-approved drug, to control the rapidly spreading pandemic. The drug proves to prevent hospitalisation if taken when early symptoms of Covid-19 arise. The drug is cost-effective at 60 cents per tablet with Covid-19 treatment consisting of 11 tablets taken over five days. The FDA considers HCQ to be a safer drug than Tylenol.
March 23, 2020 The director of the Biological Advanced Research Development Authority (BARDA), Rick Bright PhD, is instructed by his superiors to work with the FDA to establish an Investigational New Drug (IND) authorisation for HCQ.
March 24, 2020 The next day, the director of Drug Evaluation and Research at the Food and Drug Administration (FDA), Dr Janet Woodcock MD, contacts Rick Bright at BARDA. Dr Woodcock wrongly advises Bright that HCQ is a dangerous drug requiring an Emergency Use Authorisation (EUA). Its use should be limited to hospital patients. Bright and Dr Woodcock promote this course of action, despite the early clinical data showing HCQ was the most effective in outpatients if given early during the initial infection, in effect eliminating hospitalisation. The FDA issues a EUA for HCQ for hospital use only.
In a legal document, Rick Bright makes a blatant admission of insubordination to multiple layers of leadership, including the White House, HHS Secretary Azar, and Dr Robert Kadlec, MD, the Assistant HHS Secretary for Preparedness and Readiness. Bright states the following in his whistleblower complaint: ‘. . . instead of a Nationwide Expanded Access IND protocol. Implementing the EUA was a compromise position, to rein in HHS leadership’s initial campaign to make the drugs available to the public outside of a hospital setting’. Question: When is it ever acceptable to ‘compromise’ public health during a rampaging pandemic?
April 4, 2020 Dr Anthony Fauci MD, the member of the Covid-19 Task Force responsible for informing the President of the best course of action for pandemic control, appears to be unaware of the National Pandemic Plan. In a heated White House Situation Room meeting, Dr Fauci refused to consider the use of HCQ for Covid-19 treatment. He dismisses the ever-accumulating HCQ efficacy reports from China, South Korea and France as simply ‘anecdotal’.
April 22, 2020 Rick Bright is fired as BARDA director for his insubordination. Before his dismissal, he falsely informed the press that HCQ is a dangerous drug.
Dr Anthony Fauci, director of NIAID, who is not a virologist, disregards the National Pandemic Plan, which included outreach programmes with physicians using HCQ for outpatient treatment and prevention to bring the Covid-19 pandemic under control.
Dr Fauci brushes off the accumulating evidence and diverts millions of federal funds into a programme to test and manufacture an experimental drug named Remdesivir.
Remdesivir must be administered via IV and only in hospital, instead of early community treatment as prescribed in the original pandemic plan. Dr Fauci changes the plan to promote ‘societal lockdowns’ and push the development of highly experimental mRNA vaccines by multinational pharmaceutical corporations.
Note: Members of Fauci’s Covid-19 treatment panel have ties to Gilead Sciences, Inc. (Foster City, CA), the company that holds the patent for Remdesivir.
May 16, 2020 In Phase 1 clinical trials conducted by Gilead Sciences in co-operation with China and Japan, Remdesivir failed: ‘No statistically clinical effect, with severe adverse reactions’.
Note: On October 16, 2020, the WHO concludes that Remdesivir is an ineffective drug and does not recommend its use to treat Covid-19.
May 20, 2020 Shortly after becoming Senior Medical Adviser to the FDA Commissioner, Dr Janet Woodcock recused herself over future decisions concerning vaccines, citing a conflict of interest.
June 15, 2020 Dr Fauci ignores the data that HCQ works if the drug is administered during the first five days of infection. Its EUA is revoked, despite the overwhelming evidence of its effectiveness. The FDA claims that HCQ is causing fatal heart rhythms in hospitalised patients when the Covid-19 virus itself is the cause.
June 29, 2020 Dr Fauci recommends a $1.6 billion purchase of Remdesivir despite the drug’s Phase 1 failure in China. Question: Why did Dr Fauci discredit HCQ, leaving us defenseless, and order $1.6 billion of an ineffective and toxic drug?
Note: Dr Fauci’s actions pave the way for the fast-track development of experimental mRNA vaccines (and their subsequent patents), which can receive a EUA only if there are no other approved and effective medicines, like outpatient HCQ.
After widespread lockdowns and millions of global deaths, the experimental mRNA vaccines are granted a EUA and released to the public. As of the date of this letter, the pandemic still prevails, and there is no FDA approved outpatient treatment for Covid-19.
A call to action for prevention, justice and reform
The actions of Dr Anthony Fauci, Dr Janet Woodcock and Rick Bright, PhD, must be independently investigated, and they must be held accountable.
All conflicts of interest and the interactions between government officials and pharmaceutical companies, including the publication of faulty research papers in respected medical journals, must be investigated, and they must be held accountable.
Immediately reinstate HCQ as an FDA-approved drug for Covid-19.
The US Pandemic Plan must be immediately reinstated as initially crafted.
Establish an outside independent United States Pandemic Response Department, with board powers including oversight.
On June 2, 2021, the distribution of my content was cancelled by PR NEWSWIRE, and I have been banned from further distribution. Their action is a brazen attempt to censor and block the true story and silence our voice as citizens.
What can you do?
1. Contact your local, state, and federal representatives and demand answers. They would have you believe that you serve them, but you employ them. Hold them accountable.
2. Cancel biased media subscriptions. Your money fuels their disinformation campaigns.
3. Read the references for this letter and the complete uncensored and referenced articles at www.drstevenhatfill.com.
Please ACT NOW, and together we can create a better future for America and the world.
Sincerely,
Dr Steven J Hatfill
Fighting Vaccine Mandates – #SolutionsWatch
•
Podcast: Play in new window | Download | Embed
While the UK is supposedly dropping their vaccine passport idea (for now), things are looking bleak in country after country as people all around the world are facing the threat of vaccine mandates. Today on #SolutionsWatch James explores the array of solutions that are on the table to thwart this threat.
Watch on Archive / BitChute / Minds / Odysee or Download the mp4
SHOW NOTES:
What’s Going on in Japan? – Questions For Corbett #078
Japan’s vaccine passports: Here’s what you need to know
Suga challenger in LDP leadership race vows huge COVID relief package (Kishida calls for vaccine passport)
UK Government drops plans for domestic vaccine passports
Did Ayn Rand defeat vaccine passports?
President Biden Announces Vaccination Mandate for Employers
Australian Premier Dan Andrews: “we are going to lock out the unvaccinated”
Italy makes COVID-19 pass mandatory for all workers | DW News
Surging Delta variant: France and Greece introduce mandatory vaccinations for healthcare workers
Alberta to launch proof-of-vaccination program, declares health emergency
Form for Employees Whose Employers Are Requiring Covid-19 Injections
HomeRemedySupply comment on September Open Thread
America’s Frontline Doctor’s Legal Team’s “Vaccines and the Law” page
Vaccine religious exemption template downloads from Gab.com
Doctors for COVID Ethics example forms, templates, letters and other resources
Legal principle of non discrimination
The COVID-19 “Vaccine” and the Nuremberg Code. Crimes Against Humanity, Genocide
No, COVID-19 vaccines do not violate the Nuremberg Code
Bioethics and the New Eugenics
United Airlines warns of unpaid leave for staff given religious vaccine exemptions
Religious exemption to vaccine mandates may be difficult to obtain, as Amish case shows
How To Meet Like-Minded People
Here’s How To Still Dine At A Restaurant UNVAXXED!! Suss Them Out & Find Out Who’s Cool!!
1000s take over Time Square in NYC for the protest against the mandatory shot
Beware of Fake “Resistance” to Mandates
Executive Orders and How to Stop Them
James Corbett – Ernest Hancock with Arizona Dara (Solutions; BlackMarketFridays.com)
Featured Video

Yemen joins the war – Red Sea could be blocked next – Saudi regime at risk
or go to
Aletho News Archives – Video-Images
From the Archives
A superpower and “the world’s sickest warrior state”
By Paul J. Balles | March 8, 2010
Living through five or six major wars has hardened me to what I thought were the extremes of inhuman cruelty and brutality.
Two things made those extremes almost bearable: the brutality always revealed – at least according to the media coverage – the viciousness of the enemy. It was therefore quite understandable when our “brave men and women” pulverized the enemy.
Films of Japanese torturing captive Americans somehow justified holding Japanese Americans in internment camps during World War II; and only a small percentage of Americans found the bombing of Hiroshima and Nagasaki unreasonably vengeful at best, at worst, depraved.
The media giants in America portrayed the North Koreans as barbaric beasts with their captives, quite unlike their southern counterpoints – our allies during the Korean War. No one ever felt the need to explain how the South Koreans were a civilized breed while the North Koreans were absolute savages, at least according to the official line.
In Vietnam, our warriors justifiably (or so the media made us believe) dropped napalm on the North Vietnamese who had the gall to hide in villages and tunnels to ravage our invaders. At least it was accepted practice until some rogue photojournalist filmed a young girl screaming down a Vietnamese road in flames. … continue
Blog Roll
 Aletho News
Aletho News- Russian tanker approaches Cuba despite US oil blockade
- Marandi: Yemen joins the war – Red Sea could be blocked next – Saudi regime at risk
- Pro-Palestinian French member of European Parliament denied entry to Canada
- Pakistan to Host US-Iran Talks
- How Indonesia’s tilt toward the US left it stranded in the Strait of Hormuz
- US has no choice but to retreat from Iranian borders: Top commander
- Iran Retaliation Strikes Chemical Plant Near Dimona
- AWACS’ Destruction is a Major Loss for US Military – Ex-DoW Analyst
- Israel’s Iran Strategy Uses US Military & Gulf States as Its Pawns
- Iran: Trump wanted regime change, now just begging for Hormuz to open
- If Americans Knew
- Israeli police block Catholic cardinal from entering Church of the Holy Sepulchre on Palm Sunday
- Israel is assassinating journalists again, more than any other nation, anywhere, ever – Not a ceasefire Day 170
- Over 300 US service members wounded, majority have brain injuries – Not a ceasefire Day 169
- Researchers at Human Rights Watch Resign Over Blocked Report on Palestinian Refugee Return
- Jewish Groups Are Backing a War Americans Don’t Want
- Eric Fingerhut Thinks He’s the President of the Jews
- Top Jewish Philanthropists, Rabbis Urge Israeli President to Take Action Against ‘Jewish Extremists’
- Don’t Be Fooled. Zionist Leaders Have Always Wanted to Control Southern Lebanon
- Israel’s widespread use of torture is a core element of its genocide against the Palestinian people
- In Israel’s War on Iran, Many Middle East US Bases Rendered “All But Uninhabitable”
- No Tricks Zone
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis
- New Study Documents A 20-Year Pause In Arctic Sea Ice Decline – Driven By Internal Variability
