None of these patients of mine presented with the classic prodrome of relapse that I had always noticed previously, such as severe depression due to bereavement, divorce or bankruptcy. Indeed the only thing I found they had in common was to have had a recent booster mRNA covid vaccine. I phoned around my colleagues not only in the UK but also in Australia to check their experience. In no case did they deny such a link. Indeed, they were equally alarmed at the association between booster vaccines and relapse that they too were witnessing, as well an increase in new cancers, particularly in those below 50 years old. In addition to melanoma these colleagues were also very concerned about a sudden big increase in young patients with colorectal cancer.
Rather than instigating a proper inquiry to investigate this when we raised these concerns, the medical authorities told us all that what we were witnessing was a coincidence, that we had to prove it and above all, not to upset our patients.
Recently the American Cancer Society (ACS) has warned of a surge in new cancer cases in the US this lastyear of over 2million, with many of these cases occurring in younger patients. Indeed, the chief scientific officer of the ACS, William Dahat, announced in addition that cancers were presenting with more aggressive disease and larger tumours at the time of diagnosis, especially in younger patients. Of further interest it noted a difference in the microbiome (the community of micro-organisms such as fungi, bacteria and viruses that exist in a different environment) between patients under 50 compared with those over 50.
This surge mirrors a report from Phinance Technologies of late last year which analysed in detail data from the UK Office for National Statistics (ONS) which showed that disability and deaths in 2021 and 2022 had increased dramatically in all age groups, but especially in the 15-44 age group.
The Lancetalso published an article before Christmas reporting excess deaths post covid pandemic to be up by 11-15 per cent over than expected for under-25s and for between 25-49 year olds. This is in fact the pattern found in many countries that have looked at the data. Germany for example has reported excess deaths rising from 7 per cent in 2020 to 24 per cent in 2023.
What makes this all the more surprising is that negative deaths should be the norm after a pandemic as you cannot die twice!
The link between covid vaccines and myocarditis and early death particularly in the young, highlighted by Peter McCullough and colleagues as well as by Aseem Malhotra here in the UK, is incontestable. Now we have a confirmatory report from the CDC in the US, data that the authorities here have refused to act on so as not to alarm vaccinated patients!
Although it is obvious that these excess deaths are real and are continuing to rise, all we get from our Chief Medical Officer, Sir Chris Whitty, are risible attempts to explain away the increase, such as that it is a result of patients not getting their statins in lockdown (hey, patients under 55 do not get statins routinely!) The situation is no better in the US where Harvard researchers have put the blame on sleep disturbance!
The first obvious candidate is lockdown itself when the National Health Service became the National Covid Service and all screening was cancelled or delayed, resulting in an increase in cancer detection and late presentation. Many negative lifestyle factors almost certainly increased as a result of lockdown, such as a lack of exercise and too much food, especially takeaways.
What very few of these reviews consider is that this rise in excess deaths could be a result of the booster vaccine programme, even it clearly follows the vaccine rollout programme starting in 2021 and increasing in 2022 and 2023.
With regards to the link to cancer, there are numerous reports in the literature of cancers arising within days of the vaccines being administered, especially in the case of lymphomas and leukaemias. There are several reports of PET scan mapped tumours exploding at the site and draining area of covid injections with the advice to inject covid vaccines away from known cancers! Outside my clinical observations, several friends have developed cancer after a totally unnecessary covid booster taken only to facilitate travel.
For a possible association between a booster vaccine and the appearance of cancer we need a plausible scientific causal explanation. Unfortunately for those who still insist that these cases are mere coincidences, there are several compelling ones to choose from:
Firstly, it has been reported that T cell responses are suppressed after the boosters (not the first two injections) and that this is especially marked in some cancer patients.
Secondly, the antibody repertoire switches after the first booster from a protective IgG1 and IgG3 dominant B cell response to a tolerising IgG4 one, made worse by further boosters, as reported in a recent Science Immunology paper. As many cancers are controlled by effective T cell led immunity, the sudden perturbation of this control would clearly explain the development of B cell leukaemia and lymphomas, melanoma renal cell cancers and colorectal ones, all tumours which can respond to immunotherapy.
Another report by Loacker et al in Clin Chem Lab Med shows that mRNA vaccines increase PD-L1 on granulocytes and monocytes, which means they effect the very opposite of what the immunotherapy agents do against these tumours, and whichin turn explains why many of these tumours appear to be resistant to this otherwise effective therapy. Taken together, the effect on the immune response of these boosters can easily explain the relapses and so-called turbo-charged cancers appearing.
Other reports document the presence of DNA plasmids and SV 40 (a known cancer-inducing gene) sequences, as well as the ability of mRNA to bind to important suppressor genes. Although this is controversial and has been challenged, it has led to the realisation of significant batch-to-batch variation that could enhance the cancer process yet probably not manifest itself for a few years. The very possibility that we could be sitting on a vaccine-inducing cancer time bomb means that we must never again get involved into a mass vaccine programme for another possible Disease X.
But unless the government wakes up to this now, we will be at the mercy of the World Health Organization doing the very same thing when they decide to release the Disease X virus in order to take back control and destroy our lives all over again.
The U.S. Food and Drug Administration’s (FDA) vaccine advisory panel on Tuesday voted 19 to 2 to recommend new COVID-19 booster shots that include the Omicron variant this fall.
It is the first time VRBPAC has suggested vaccine makers modify their vaccines to target a different variant, according to CNBC, which also reported the FDA will likely accept the committee’s recommendation.
If so, the FDA would be authorizing a vaccine change without requiring additional data showing a bivalent vaccine — containing both the original 2019 Wuhan variant and one of the Omicron variants — is safe and effective for those age groups that are already authorized to receive a booster dose.
The FDA plans to decide by early July whether vaccines will target the now-dominant BA.4 and BA.5 Omicron subvariants or the BA.1 Omicron variant that led to a surge in infections last winter, Reuters reported.
At the beginning of the meeting, Dr. Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research, suggested a newly designed shot could begin in October, adding that it takes manufacturers around three months to choose a vaccine design and begin producing doses.
Dr. Paul Offit, director of the Vaccine Education Center and professor of pediatrics in the Division of Infectious Diseases at Children’s Hospital of Philadelphia, and Dr. Hank Bernstein, professor of pediatrics at Zucker School of Medicine, were the only two members who broke from the panel to vote against the initiative.
Offit acknowledged there’s a benefit to providing a booster in the fall to some age groups, but questioned whether Omicron was the right strain. He said the move to new-variant vaccines was happening too fast, with too little data.
“I think as a new product it should be handled as a new product,” Offit said. “I think we need a higher standard than what we’ve been given. …“I’m not comfortable enough to support the risk of a new product.”
Bernstein expressed concern over the lack of data used to justify changing the strain, and the potential that by the time a subsequent booster is approved, it will contain outdated strains.
“So, in sum, I think including an Omicron strain in the vaccine seems to have some potential, but data especially for BA.4 and BA.5 are limited at this time, and that’s why I’m struggling to even make a strain change at this time,” Bernstein said.
Bernstein also said he didn’t see a need to change the strain as the current vaccine being used is shown to be effective against severe disease — a claim made just two weeks earlier at a prior VRBPAC meeting.
Bernstein said the strain change would need to be supported by data showing improved vaccine effectiveness and he “didn’t think we really have the data to be able to say that” even though the panel looked at the immune response.
Dr. Ofer Levy, VRBPAC member and an infectious disease physician at Boston Children’s Hospital, voted “yes” to change the computation of COVID-19 boosters, despite Pfizer’s admission there is “no established correlate of protection,” referring to the level of antibodies needed to confer protection.
“You have a lot of data now,” Levy told Pfizer. “What is your relative protection?”
“I would say there is no established correlate of protection,” Kena Swanson, Ph.D., vice president of viral vaccines at Pfizer, told Levy.
“I would like to hear from FDA what their overall approach will be around improving our understanding of correlate protection. We spend a good amount of time reviewing antibody data. We have no doubt antibody data is important. We don’t have a level of antibody that anybody is comfortable stating is correlated [with] protection.
“So yes, the antibodies are important but so are the T cells. We heard from Dr. Weir, yes, T-cell assays are trickier and they’re more diverse, but it’s not going to happen without federal leadership to have a standardization of the T-cell assay and encourage or in fact require the sponsors to gather that information.”
“So what is the effort to standardize the pre-clinical assays?” Levy asked. “This is an effort that’s critical not just now but for future cycles of vaccine revision. If we aren’t able to define a standard for correlate protection we are fighting with one arm behind our back.”
Marks acknowledged the importance of Levy’s question, but said T-cell-mediated immunity was “difficult to study” initially.
“We have been having conversations with our colleagues at the NIH [National Institutes of Health] and throughout government about how we might move forward here,” Marks said. “It is something that we don’t have an answer to yet.”
Marks said as vaccines are developed in the future, it will “become even more important” to define a standard of correlate protection because “we won’t be able to have a large naive population to vaccinate with newer vaccines.”
“We will need to understand the T-cell response better,” Marks said. “I take your point, it’s just that we haven’t solved the problem yet.“
Dr. Meryl Nass, a member of the Children’s Health Defense scientific advisory committee, told The Defender that in her opinion, Tuesday’s meeting was a “vote to essentially approve a future framework — the future framework being a dearth of evidence required to change the booster, without clinical evidence and without a correlation of protection.”
Nass added:
“They voted on using an Omicron variant in the next booster iteration — which could contain any Omicron variant and could be either mono- or bi-valent.
“But most likely they will keep the current version and add another — which might double the amount of mRNA, or not.”
The new formulation might be for adults alone or adults and children, or only older adults and the immunocompromised, Nass said.
Brian Hooker, Ph.D., Children’s Health Defense chief scientific officer and professor of biology at Simpson University, told The Defender :
“The proposed move by VRBPAC will increase the harm to the U.S. public to unprecedented levels, as this action will further circumvent necessary clinical trials even beyond the slapdash testing of COVID-19 vaccines under Emergency Use Authorization.
“This adds to a foundation of lies used to authorize the original COVID-19 vaccines without anywhere near proper testing.”
Dr. Cody Meissner, VRBPAC panel member and professor of pediatrics at Tufts University, expressed concern about the financial risk pharmaceutical companies “are taking by making these vaccines.”
“If there’s a low likelihood the vaccines will be recommended, then they could incur significant loss,” he said.
Marks responded:
“I guess I would say that I would make recommendations here knowing the vaccine manufacturers will be kept whole by the United States government at least for some vaccines. I could be wrong but I think that’s a reasonable assumption.”
During the meeting, Moderna told the panel it would be ready with a “couple of hundred million” bivalent, or double-targeted, vaccines designed to combat BA.1 by September, but it would be late October or early November if the company needs to design a new vaccine targeting subvariants.
Pfizer said it and partner BioNTech have a significant amount of vaccine doses designed for the BA.1 variant ready and are already preparing to produce a large number of doses targeting BA.4 and BA.5 Omicron subvariants.
Pfizer said either could be ready for an early October rollout.
Multiple concerns raised during the public comment session
During the public comment session of the meeting, experts raised concerns that were largely ignored by the advisory panel.
Dr. Dustin Bryce, with Interest of Justice, said the FDA, Centers for Disease Control and Prevention (CDC) and the World Health Organization are “usurping Congress’ definition of a vaccine — which is any substance designed for the prevention of one or more disease.”
“FDA actually classifies mRNA as gene therapy, which they say is to treat or cure an existing disease by modifying your genes,” Bryce said. “Gene therapies are still being studied and are experimental at this time.”
Citing FDA documents, Bryce said gene therapy, unlike a vaccine, is so inherently unsafe the FDA says it requires 15 years of research to follow up on safety due to known risks of antibody-dependent enhancement, alteration of DNA and delayed adverse effects, such as cancer.
Bryce said:
“FDA says that gene therapy use in the mass population represents an unreasonable risk and they should limit the number of subjects who might be exposed to risk. We require due process and forbid the FDA from authorizing the proposed changes.
“We are demanding that EUA [Emergency Use Authorization] is promptly revoked because unreasonable risks are inherent in gene therapy products, as evidenced by large numbers of reports of adverse serious events linked to or suspected of being caused by an EUA product, product failure and product ineffectiveness.”
Bryce said COVID-19 vaccines fail to meet the requirements of EUA because not a single mRNA vaccine has been found to be effective for the prevention or treatment of an existing disease.
Michael Briskin pointed out in his public comment that the FDA receives approximately 75% of its budget from pharmaceutical companies, which he believes represents a conflict of interest.
Briskin challenged the use of the phrase “safe and effective” to describe COVID-19 vaccines, given the FDA has done no long-term testing to determine whether these products are safe.
Briskin presented data showing a significant rise in reported deaths among working-age Americans following COVID-19 vaccine mandates.
He said:
“In the short-term, 2021 was a very interesting year. We saw a stark increase [in death] among working-age adults from 18 to 64 and specifically in Q3 and into Q4, so something new for the working-age demographic partly through 2021 would be the clear correlation.
“With comparable trends in BLS [Bureau of Labor Statistics] data, children’s health insurance data, Israeli ambulance data, and of course we have the [Vaccine Adverse Event Reporting System (VAERS)] data — which the CDC tried to minimize but a recent FOIA [Freedom of Information Act] request forced them to reveal that they never once did the PRR calcification that was supposed to be their tool for spotting safety signals, according to their posted documents.”
“And what do we do when people get injured from these vaccines?” Briskin asked the panel. “We leave them in the mud.”
Briskin chastised the panel for authorizing boosters for infants two weeks earlier when data showed two doses weren’t effective and only 10 cases were used to assess efficacy.
“Three-quarters of the severe COVID in the trial was in the vaccine arm, as was the only hospitalization case which was accompanied by a seizure,” Briskin said. “And Moderna is so dangerous in young people Nordic countries won’t allow it to be used in anyone under the age of 30.”
Briskin said:
“In fact, the director of health of Denmark just admitted that vaccinating children was a mistake, whereas our officials only ever doubled down. And now we’re about to double down so hard we are about to lose the pretense of holding these pharmaceutical companies to any statistically meaningful regulatory standards for formula modification.
“For people following at home, what this agency is proposing is not just modifying the genetic code in the vaccine and the structure of the proteins produced to chase variants, but even things like doubling the microgram count for Pfizer — all without doing any statistically powered safety studies.”
“And to be clear,” Briskin added, “the companies we’re giving carte blanche to include Pfizer, the world’s largest criminal organization having paid the world’s largest criminal fine, and Moderna, which never made a safe product before we did away with long-term safety testing.”
Dr. Eric Feintuch, a chiropractor, asked the FDA if the agency knows how long mRNA from COVID-19 vaccines and the spike protein stay in the body, whether they know what the rate of protein production is and whether the FDA is aware of the consequences of the methylpseudouridine substitutions at the codon optimization step.
“For anyone on this panel who says it doesn’t go anywhere, tell me what proof you have of that,” Feintuch said, referring to the spike protein.
Feintuch said COVID-19 vaccines are associated with prion disease, noting 26 people have reported experiencing sudden onset of a severe and fatal brain disorder within one month of the second mRNA vaccine dose.
“This information needs to be researched and seen,” Feintuch said.
“A thousand peer-reviewed studies question the safety of COVID-19 vaccines. Doesn’t anyone see the safety signals? Is there anyone here who will stand up?” he asked. “Some of you know this, you need to stand up and you need to help us.”
Dr. David Wiseman, a research scientist with a background in pharmacy, pharmacology and experimental pathology, said VRBPAC is once again being asked to opine on inadequate information.
Wiseman said the FDA recently waived efficacy requirements for COVID-19 vaccines and has ignored its experts, notably Levy, who “has called for federal efforts to validate and standardize a correlate of protection.”
“Recent vaccine decisions were based on irrelevant Wuhan immunobridging,” Wiseman said. “Omicron assays are unvalidated and unverified by FDA.”
Wiseman said safety questions surrounding COVID-19 vaccines remain unanswered:
“We have shown correlations between vaccination and all-cause mortality. FDA says VAERS is under- and misreported. A FOIA disclosure reveals that CDC has not conducted safety signal analyses, which we have provided to FDA. Neurologic adverse events are finally being acknowledged [but there are] still no cancer studies.”
Wiseman further pointed out that FOIA requests show vital studies involving the spike protein have not been done:
“A Stanford study in [the journal] Cell showed vaccine message and antigen persisting for at least eight weeks. Does spike accumulate? Is this why myocarditis rates after boosting match or best primary series rates for some ages?
“Does spike persistence contribute to immune suppression, imprinting and negative efficacy? What is the toxicity of multiple doses? How will sameness of the manufacturing process be defined? Are the guidelines talking about monovalents or bivalents?”
Pfizer has dismissed concerns about the spike protein as “academic,” Wiseman said, “but it is certainly not.”
Booster formulation should be changed to combat waning efficacy, committee said
During the meeting, which occurred two weeks after the panel signed off on the primary COVID-19 vaccine series for the nation’s youngest children, a change in booster composition was deemed necessary due to waning effectiveness.
Dr. Mahesh Shenai, neurosurgeon and data analyst, said in a tweet:
“After many months of extolling benefits of vax and booster, now they are criticizing its efficacy and durability. . . to set the stage for a new updated booster!?”
In a briefing document published ahead of Tuesday’s meeting, FDA officials predicted a major COVID-19 outbreak will occur in the fall “due to the combination of waning immunity, further evolution of variants and increased indoor activity.”
A similar committee that advises the WHO recently suggested COVID-19 vaccines be reformulated to include both the original SARS-CoV-2 Wuhan variant and the first version of Omicron, BA.1 — although this variant has since been replaced by other strains of BA.4 and BA.5.
Moderna and Pfizer studied Omicron-specific vaccines in preparation for fall boosters, but efforts have been complicated by new subvariants.
If the government decides it wants a booster shot that targets BA.4 and BA.5 — two strains derived from the Omicron variant that are becoming dominant — vaccine manufacturers will have to race to produce the doses by fall, The New York Times reported.
Vaccines produced by Pfizer, Moderna, Novavax and Johnson & Johnson were developed against the original Wuhan COVID strain that emerged in 2019, but as the virus has rapidly evolved, these vaccines have become less effective.
COVID-19 vaccines target the spike protein the SARS-CoV-2 virus uses to invade human cells, but as the virus mutates away from the original strain, it has trouble “recognizing and attacking the spike,” CNBC reported. The Omicron variant has more than 30 mutations.
Marks said during the meeting he hopes changing the booster will “convince people to go get that booster,” adding the FDA plans to begin a booster campaign in October.
Megan Redshaw is a staff attorney for Children’s Health Defense and a reporter for The Defender.
A new poll of Americans shows that it’s likely that over 10M Americans were injured by the vaccine. This may explain why there are staffing shortages everywhere, from pilots to pharmacists.
Yesterday, VSRF engaged the services of a professional polling company (Pollfish) to survey 500 people who were selected entirely at random.
The results were shocking, but they were consistent with the VAERS data which has been “lit up” since January 2021 telling us “the COVID vaccines are the most unsafe vaccines in human history.”
Now we have independent confirmation that the safety signals in VAERS were accurate, just like we’ve always said.
The numbers in this poll are absolutely shocking and there is no way to spin this as a positive.
This article includes the full Pollfish report as well as the individual response data so that anyone can analyze it themselves.
Key results from the poll
The poll was about the COVID vaccine exclusively, not about other vaccines. Stratified responses are age normalized to the US since the respondents who answered didn’t match the overall US demographics.
Doing some rudimentary estimates from the data (rather than stratifying by age which would be more accurate but more time consuming):
20% of the respondents reported they were vaccine injured
The 20% number is remarkable because there was no pre-screening question and only 77.3% of Americans received at least one dose. That means that if you were vaccinated there is a 26% chance that you were injured (computed as 20.46/77.3). Wow.
30% of the households have a vaccine injured person
45% of the extended families have a vaccine injured person
In 87% of the cases where there was a vaccine injury, there was either a doctor visit(s) or hospital stay(s) or both.
54% of the injured are still impacted today.
45% of the vaccine injured said it would shorten their lifespan
41% of the injured are unable to hold a job.
Only 17% said their injury was a minor annoyance.
Putting these results into perspective
If you took the vaccine there is a 26% chance of injury as noted above. We also know that 45% of the injured said it would shorten their lifespan. This means that we are shortening the lifespan of 12% of the people who opt for the jab (since .26*.45=.117).
Shortening the lifespan of 12% of the people who take the vaccine seems like a very high price to pay for a virus that can be easily treated with a near 100% success rate with repurposed drugs.
For example, my friends George Fareed and Brian Tyson now have treated over 12,000 COVID patients using a combination of repurposed drugs and supplements without a single hospitalization or death if they were treated within 5 days of first symptoms. They even have a top-selling book on Amazon with rave reviews. Despite all of that, the FDA, CDC, and NIH continue to ignore them. They can’t get anyone to return their calls. They’ve had their protocol since the very beginning of the pandemic in March 2020 (it’s evolved over time).
We are basically spending billions of dollars to seriously injure over 10 million Americans and kill hundreds of thousands. In the process, we did not reduce COVID, but made the problem worse with nonsensical interventions when all we ever needed was some simple advice:
If you are sick stay home
If you test positive, start a proven early treatment protocol ASAP such as the Fareed-Tyson protocol
We never needed the vaccine, masks (which make the problem worse), lockdowns, mandates, social distancing, or new drugs. All we had to do was follow the two simple steps above. It was never more complicated than that.
The data
Here are the full poll results and a spreadsheet with each individual response so you can do you own analysis:
Comparison with the rates of COVID vaccine injury that nurses report among their peers
Does a 12% injury rate seem high to you? That would be 30M people.
You may change your mind when you watch this video where I interview 7 nurses who were willing to speak out publicly and reveal the rate of vaccine injury among their peers.
Note: There are audio and video drop outs on the call. Use the cursor button to skip over this. I’ve reported these issues to Riverside.fm… their product feels like a beta test. Also, the preview has 8 nurses but there were only 7 in the call. Can you spot the duplicate?
The rates averaged over 10% with some nurses seeing injury rates among their peers exceeding 40%. Sorry this is so hard to watch with the audio drop outs, but this is the best I have for this interview.
Jessica Rose’s take
She just sent me an email:
Steve, this is excellent. And aligns with my perceptions from the data.
Dr. Pierre Kory’s take
I sent him an email with all the data with a Subject line: Re: WHOA!!! this poll will BLOW YOUR MIND
Pierre quickly wrote back:
Wow is right. Those numbers are beyond disturbing, I have been calling this vaccine escapade a humanitarian catastrophe.. and this is what that looks like.
This makes our survey estimate of 30M look quite conservative.
However, if we take the raw, unadjusted numbers of our survey, 30% of all respondents over 18 were vaccine injured. Since there are 258M people over 18 in the US, we get 77M estimated vaccine injured, eerily close to the VAERS estimate.
So maybe VAERS isn’t such a bad estimator after all.
Validation by the government of Israel
Our final validation point is the proactive poll done by the government of Israel to assess vaccine side effects. This article describes that study. Among the highlights:
About 25% of people with pre-existing auto-immune disorders, depression or anxiety reported a worsening of their symptoms following the booster.
4.5% of respondents reported neurological problems
17% reported shaking
So our 20% rate of injury isn’t all that far off what the Israeli government found.
What vaccine injury looks like
Many people never recognize vaccine injury because they don’t know what it looks like.
For example, as I am writing this article, I received the following message from one of my subscribers:
So my mom’s very dear friend called me tonight to tell me that her cancer came back. She was diagnosed over 20 years ago and has been cancer-free. I asked her did you get boosted she said yes, I already knew she was vaccinated. She said don’t start asking me these questions. What does that have to do with anything? They now found Cancer all over her uterus and it’s now spreading to her body. You think it’s from the vaccine? She was perfectly fine all these years before getting vaccinated. It makes me so sad she will probably end up dying.
I hear these stories all the time of a new cancer or a cancer that was under control suddenly coming back with a vengeance. These aren’t coincidences. While for any individual case it may be difficult to determine a cause, in aggregate we are seeing rates of cancer post vaccine that are unprecedented.
It’s amusing to me that when you search for that quote in Google, you only get articles debunking the claim whereas if you search in DuckDuckGo, you get articles with the original quote. This is pretty sad because Dr. Cole is highly respected among his peers for telling the truth. It’s a pity we never get a chance to have a fair debate with people who claim we are spreading misinformation.
And the personal stories
A lot of people tell me they know hundreds of people and none are vaccine injured.
Perhaps.
Or perhaps 95% of the vaccine injured don’t speak out about their vaccine injury.
It feels like for every person who sees nothing, I hear from people with the opposite experience:
I have so many of my relatives, neighbors and acquaintances succumb to this poison. Just yesterday a 30 year old acquaintance died of sudden heart attack. My aunt is suffering from autoimmune mediated arthritis after she got her 2nd Pfizer shot. A neighbor died after receiving the first dose of Sinovac Vaccine. A relative died after receiving 2nd dose of SinoVac… So many to list!!
Replicating the poll
The out-of-pocket cost for the poll is $500. Anyone could replicate it.
I’m sure fact checkers will spend $50,000 to replicate it 100 times until they get the results that match their narrative, and then publish that.
We didn’t do that. We’ve never asked this set of questions ever before. The questions weren’t “gamed” to elicit a specific response. We put together the questions we wanted, we ran the poll, and we published the results.
But the poll is affordable enough that if you don’t believe me, you can replicate it yourself.
Summary
The COVID vaccines are the most dangerous vaccines in human history. There are systemic flaws in the medical system that cause doctors to fail to recognize the evidence in plain sight. But that doesn’t change the reality. The COVID vaccines have killed hundreds of thousands of people and severely injured millions more. Since there is a safe, inexpensive alternative (early treatment protocols) with near 100% efficacy in reducing hospitalization and death, the vaccines should be immediately halted for all age groups. That would be the right thing to do.
But admitting they made a mistake would be an embarrassment to the medical community, government agencies, and Congress. So they will continue to look the other way and find ways to discredit the evidence and the brave people who are speaking out. They will continue to avoid any accountability by agreeing to an open debate. And in the meantime, millions more will be disabled, and hundreds of thousands will die prematurely.
Doctors and nurses know what is going on, but will not speak out as a group because they will lose their jobs and ability to practice medicine. So they keep their heads down.
The other doctors are so blue-pilled, they actually still believe the CDC. When Pfizer presents safety and efficacy data that is appalling to anyone with a working brain, they simply look at the vote count of the outside committees (unanimously approved) and never bother to learn more about what just happened. They won’t even watch this 4 minute video that explains just how bad the trial data was.
When we discovered that there wasn’t a single death from COVID-19 in the entire state of Massachusetts in both 2020 and 2021 in age 5 to 11, did that change anything? Of course not. COVID is an emergency because it might kill kids in the future and you can never be too careful when it comes to saving kids lives. But when large numbers of kids are killed by the vaccine, we simply look the other way. That’s not an emergency; it doesn’t even exist. Their odd causes of death are ignored.
My survey won’t change anything, even if it is replicated over and over. It will just add more evidence to the public record that the medical community is causing great harm and completely incapable of seeing the truth. They will not allow themselves to be held accountable in an open discussion— ever.
The American people won’t change their minds until the doctors change their minds. And the doctors are so well trained to respect the medical authorities like the FDA, CDC, and NIH and/or sufficiently afraid of the repercussions of speaking out, that nothing will change anytime soon.
The truth always comes out sooner or later. The later it comes out, the greater the damage will be to all these institutions that people once trusted.
The other thing I know is that the scale of this deception is unprecedented. When this unravels, which I have no doubt that it will, it will destroy our trust in:
the medical community
the HHS government agencies: CDC, FDA, NIH
the mainstream media
Congress
State and local government officials
CEOs who imposed vaccine mandates
local health officials
Mainstream social networks
Fact checkers
The Gates Foundation
Bill Gates
The Rockefeller Foundation
the drug companies
the courts
clinical trials
medical journals
… and more…
This survey is just one more nail in the coffin of the “safe and effective” narrative. Nothing more.
He is not alone in seeing this. All his other embalmer friends see it too. All of them. The only possible explanation: the COVID vaccines are killing massive numbers of previously healthy people.
Fifteen embalmers are all seeing odd fatal clotting in people that first started in 2021. As many as 65% of cases are affected. Just like the DMED data, this evidence is being totally ignored by the mainstream press and medical community as well as the CDC and other HHS agencies. The only explanation that fits all the facts is that the vaccines are killing Americans in massive numbers and should be immediately halted.
Richard Hirschman is a funeral director who spotted really strange clots in dead people after the vaccines rolled out. He was interviewed by Jane Ruby on the Stew Peters Show. At nearly 800,000 views on Rumble alone, his interview is one of the most popular episodes in Stew Peters Show history.
I was originally introduced to Richard via one of my contacts. Richard has been embalming people for more than 20 years. He lives in Alabama.
Here’s my 53 minute interview where we get into the profound implications of what Richard found: that the vaccines are likely killing around 65% of the cases he is seeing today. There is simply no other possible explanation that fits the evidence.
If you thought the COVID shots were safe and effective before the video, and you still have a working brain, I’m pretty sure this video will change your thinking because there is only one possible conclusion: the COVID vaccines are killing massive numbers of people and nobody is investigating.
Here are some of the most important things I learned from Richard:
He started noticing the strange clots around May or June 2021. He’d never seen anything like it before in his life. However, he admits they could have started much earlier and he just never noticed them before because he was very busy.
He is not aware of any cases where the strange clots were seen in unvaccinated cases(except for one unvaccinated person who received a transfusion)
He started formally tracking the number of patients with the strange clots in late 2021.
He says currently over 50% of the bodies he embalms have the strange clots which he uniquely associates with the vaccines/boosters. This is the bombshell. The CDC says deaths from the vaccine are 0% and this embalmer, who has no conflicts of interest, says it is now over 50% of the cases he sees. They can’t both be telling the truth. One of them is lying.
In Jan 2022, 37 out of 57 (65% of all cases) had these suspicious clots. That’s huge.
His embalming volume varies by day. Sometimes it is one a day, other days it can be up to 6 or 7. He estimates he does an average of 2 per day, which is over 600 bodies a year. So while these aren’t huge numbers, the numbers are large enough that it is unlikely that the effect they are seeing is just due to small numbers.
He contracts out his services to a variety of funeral homes. In 2020, he’d see a lot of COVID deaths because other embalmers didn’t want to touch those cases. Richard is COVID recovered so he had no problem handling those cases. Now, however, that fear has greatly subsided so now he is seeing more of a representative sample (i.e., unbiased) of people who die. So his “over 50% of deaths” figure is only slightly exaggerated from an embalmer seeing an “unfiltered” set of people.
Younger people tend to be cremated, so he won’t see those cases.
His peers (he’s discussed with 15 of them) see the same thing he does but won’t speak out publicly. I see this in other areas such as school officials being afraid to reveal high rates of myocarditis in their schools. For example, Nikki Daniels, Head of School at Monte Vista Christian School, isn’t speaking out about the four myocarditis cases at their small private school (which translates into a rate of myocarditis that I’d estimate is more than 1 in 100).
The mainstream media, mainstream medical community, and HHS agencies are all ignoring Hirschman and others like John Looney. Only alt-media has reached out to him to write an article.
PolitiFact reached out to try to discredit him but ended up not writing an article presumably because they failed to find anything to attack him on.
There is no other explanation for this that we can figure out. It pretty much has to be a novel injectable product, first used in 2021 that results in blood clots and is injected into well over 50% of the population. There is only one drug that fits that bill: the COVID vaccines.
None of his embalmer friends who have seen the data are planning on getting any more COVID vaccine shots.
Fewer than 1% of people who get the shots will die. As Dr. Mike Yeadon points out in the comments below, whether you die or not is likely a combination of how well you “take up” and “replicate” the mRNA, how dangerous the batch is, and other factors.
Could it be caused by 5G?
A few people speculated it was caused by the 5G deployment in Alabama. No, that’s not it at all. Nothing has changed in the area around Hirschman. We checked.
Could these clots be caused by COVID?
The Politifact fact checker, Naseem Ferdowsi, has no medical experience at all. She sent a message on Feb 4, 2022 that she was told by an embalmer in Phoenix Arizona that “dark clots have been found in COVID victims long before vaccinations were available.”
There are several problems with hypothesis:
The clots are white fibrous material (clearly the fact checker never actually viewed the video she was fact checking)
The number of COVID deaths in Houston County where Richard works are miniscule. For example, the number of COVID deaths was 9 in January, yet Richard had 37 with these clots.
The percentages do not make sense. Only a tiny fraction of all deaths in January are from COVID. If 65% of the deaths in Houston County in January 2022 were from COVID, that would be front page news.
If these clots were caused by COVID, it’s highly likely someone would have spotted it before 2021 and done a similar video.
Omicron has taken over as the dominant COVID variant in January across the country. Omicron doesn’t kill people. People die with Omicron, not from Omicron. Therefore, if it was COVID-related, the clots would be gone, not at an all-time high.
However, we all know what will happen, don’t we? I think we’ll soon see a PolitiFact article that these clots are caused by COVID.
Another clue that vaccinated people are dying at a higher rate than the unvaccinated
One commenter said “only 61% have received at least one of the jabs and 49% two jabs in AL.”
The implication is that you can’t have 65% of the deaths be from the jabs.
But that’s not true at all.
If 61% were vaccinated over all age groups, and the vaccine were completely safe, we’d expect that 61% of the people who died would be vaccinated.
Richard’s observation that 65% of the people who died had these clots simply means that the vaccine appears to be causing death at a higher rate than would be expected than if the vaccine was truly safe and effective.
The doubly jabbed are more likely to die so the bump from 49% expected to 65% suggests the jabs are killing people.
Estimating total number of people killed by the COVID vaccines from this data
Hirschman’s data is explosive because it establishes a relative proportion of people affected which we can then use to establish an absolute rate of death.
Is this definitive? No. It’s just another “sanity check” datapoint.
So let’s say the actual rate of vaccine-caused deaths is 40% of all deaths which is less than the 65% rate that Hirschman is seeing.
The CDC says around 65,000 people die a week. So that would be 26,000 people a week killed by the vaccine. He started noticing these deaths in May (they could have started sooner), so let’s just say it’s only been in the last 6 months to be conservative.
So even under the most ridiculous assumptions, there is no other way to interpret this data than to conclude the vaccines are unsafe and should be stopped.
Nobody in mainstream media, academia, or HHS is interested in talking to Hirschman
With a 65% death rate, you’d think the CDC would be doing an active investigation on this to collect the data.
You’d also think that after his Jan 26 video, Hirschman would be contacted by the CDC, FDA, NIH, NY Times, CNN, Washington Post, and so on, wouldn’t you?
Nope.
Just the Stew Peters Show (Jane Ruby), the Epoch Times, PolitiFact, and Steve Kirsch’s Newsletter.
Nobody from mainstream academia reached out to him for tissue samples to analyze or to write up his results in a paper that could be submitted to a medical journal so that it could be documented.
What can I say? They just do not want to know.
In January 2022, 65% of his embalming cases had this “problem” but nobody wants to look at it. Nobody!
I’m not surprised. They don’t want to learn the truth about these “vaccines.” They all just want to tell America one side of the story and censor any evidence that goes against that narrative.
Comments from Dr. Mike Yeadon regarding the mechanism of action
When assessing causality, one of the key criteria is a plausible mechanism of action. Here you go from Dr. Mike Yeadon.
Steve, I wish I was shocked, but none of us with an understanding that these gene based agents prompt our bodies to manufacture virus spike protein in uncontrolled amounts & in uncontrolled anatomical locations expected spike protein to do what it does in quantity: prompt blood to coagulate.
I’ve received the results of an informal survey conducted on behalf of a financial advisor to their client list. Questions included whether clients or their family members know someone who’s become very ill or died after vaccination & something like 2/3rds of respondents says they did. The results were sent to me to reinforce how commonplace these injuries & deaths are.
I personally know of four deaths and twice as many serious, not yet fatal illnesses after c19 “vaccinations”.
I know indirectly of two who were said to have been covid19 deaths. One was in their 80s & frail and the other, in their 60s, was living with a terminal cancer diagnosis.
Summary
The COVID vaccines are the largest clinical trial in world history.
What we have learned so far from the embalmers is troubling: it appears the vaccines have overtaken heart disease as the #1 leading cause of death in America today.
The CDC doesn’t have a clue it is happening. They still think that nobody has died from the vaccine. They refuse to look at the safety signals in VAERS and DMED. They don’t want to see any safety signals and they will not meet with anyone who challenges their point of view.
Death is one of many symptoms. Other side effects are a wide variety of cardiovascular, neurological, and autoimmune diseases, paralysis, loss of limbs, and potentially sterilization and AIDS. After a 90 day honeymoon period, vaccine efficacy turns negative. They also are known to increase cancers.
Stay tuned as we learn more in this clinical trial of the vaccines. I’m sure this isn’t the end of the story.
The California legislature is expected to mandate soon that everyone who works in California get vaccinated (AB 1993). This will increase the numbers and allow us to get the test results sooner. California is literally sacrificing its residents for the benefit of the rest of the country.
Although I live in California, I am self-employed. I suspect I will need to fire myself soon. I will not willingly comply with their law
I’ve been wondering for quite some time about whether we are in a War and the resolution of my thoughts on the subject has recently improved.
Oddly enough, I have some standing on the subject.
I lived in Iraq between 1981 to 1991, a period that covered almost all of the Iraq/Iran War and all of the Gulf War, the original, not the sequels.
It was an old school type of war, with two parties fighting over territory and trying to redraw a border. A lot of people died over 8 years and the border stayed the same. But weapons were sold, and internal power was consolidated.
That’s really what war is about, territory. You have something that I want, and I will fight you for it.
So, if this is a war, who are the warring parties and what is the fight over?
The war is between “the state” and “the citizen”. The latter is YOU and ME and it’s easy enough to understand (sort of), but THE STATE is not straightforward anymore and I’ll cover that later.
The border between these two parties is being redrawn. The relationship between the State and the Citizen is being RESET.
When you hear about The Great Reset, that is what “Reset” really means.
Think back to your life, last year in Feb 2020. Think back to how you thought, what you did, what degree of intrusion the State had in your life and what level of control you had over your life and choices.
In Feb 2020 there was a border, a fairly large circle that you stood in the centre of. Everything within that circle was your domain, your freedoms, and your sovereignty.
Now, reflect on your life today, but more importantly reflect on the size of that circle. It obviously is much, much smaller today. The border between you and the State has been Reset.
Within that circle is a second circle that is much smaller, and it surrounds you almost like a second skin. Within this second circle, you have what is your “bodily sovereignty”. What is within your body is YOURS and not the State’s.
If you have acquiesced to the State’s injection, you have surrendered your bodily autonomy to the State. There is no border anymore between you and the State. It’s a depressing conclusion but true.
Your rationalisation for taking it is irrelevant, you wouldn’t have taken it but for the State’s lies and threats. Unless you took the flu vaccine every year religiously, to “protect yourself and others”, you have surrendered to the State. You may have had no choice because you need to make a living and feed your family, so it was a calculated surrender, but a surrender, nevertheless.
But for almost everyone else, you surrendered your bodily autonomy (let alone your current and future health) so that you could go to the pub, go to the hairdresser, go to the gym, see your parents, travel, plus a laundry list of other reasons that the world has used to rationalise its surrender to the State.
It is worth noting, that if you have surrendered your bodily sovereignty to the State, and there is no longer a border between you and the State, what would you ever say no to in the future. If you were not prepared to stand up for your bodily sovereignty, what would you ever stand up for?
But as a friend of mine said the other day, people just don’t know. They haven’t spent the time (for some hundreds of hours) necessary to figure out what is true and what is a lie.
They think the jab is safe (without understanding the meaning of the word).
They think it is effective (that it will protect them from getting Covid or giving it to parents, grandparents and others).
They think the State is truthful (why would they lie?).
They think the disease is exceptionally deadly (because they were told it is).
They think that masks work (when hazmat suits are necessary to protect against respiratory viruses).
They think that lockdowns work and are worth the cost.
They think that social distancing works.
They think that healthy people can spread the deadly disease.
They think that test results are real.
They think that contact tracing works (so they keep checking in, even when nobody is watching or cares).
And they think many other things that all form the framework for the biggest lie ever told to the world.
You need a lot of time to dismantle each one of these falsehoods and unravel the matrix that has been built.
I now would add another leg to this line of thinking.
They think there is no war.
This is a vital point, and I draw on my time in Iraq to understand it.
We knew there was a war. We knew who the warring parties were. We knew there was a border being fought over. We knew that our wants and needs needed to recalibrate to the reality of the war we were in. I don’t remember anyone ever complaining about missing out on all of life’s “nice to haves”. Our wants had recalibrated very tightly around our needs, there wasn’t a gap really. If we and our loved ones were fed and safe for the night and we had a job in the morning that allowed us to be fed and safe for the night, then we were generally happy. To survive war, you need to recalibrate psychologically to it. Of all my friends during those years, I don’t remember any of them being depressed. They had psychologically adapted to the reality of war, and to a climate of having and doing less. Within that recalibration, we were content.
We bunkered down and got through it.
The Iraq-Iran War went on for 8 years. Early on people thought it would be over in a few months, that was just normal human optimism. But after a couple of years most understood that thinking in terms of timeframes just created false hope and wasn’t helpful to having a robust and resilient War mindset. So, we accepted that it would be a long war and stopped trying to guess it’s end. Basically, for our own psychological well-being we settled in for the long haul.
I recommend that you do the same here, start settling in for the long haul. This War is not ending any time soon.
Learn to live with less.
I wrote this short piece many years ago, mainly so that I wouldn’t forget the stories and that my kids would get a glimpse into their history. It was a time where we learned to live with less.
The Generator
The first thing the Americans did was take out most of the infrastructure. They took out the bridges, they took out the TV stations and they took out the power plants. We lost our electricity on the first night of bombing in January 1991.
The war lasted for about three months, 100 days to be precise, and then it took another three months before the lights came back on, so all in all about six months without electricity.
Six months!
I’ve heard it said that society falls apart and anarchy sets after a couple of weeks without electricity. Well, that didn’t happen. Maybe we had other things on our minds.
A lot of things changed quickly when the power went out on that first night of bombing. Sleep cycles for one, no more TV and some candle use initially but that quickly changed to mainly a kerosene gas lantern that we had. It looked something like this.
It had a pump that you would use to pressurise the tank, it would then spray a kerosene mist onto a ball shaped net that burned brightly. It made a sssshhh sound that I still remember. I don’t recall anyone else having one and I don’t remember how we got it but it was our main source of light in the living room during those dark months. It burned white and bright and had a constant, soothing pressured burning sound.
One day a friend and neighbour, Abu Bashar (Father of Bashar), managed to get his hands on an old broken down generator. He asked me if I wanted to have a look at it. Having never before seen a generator in my life, let alone fixed one, I announced my intention to resurrect the machine.
I was asked the question because over the years I had built up a reputation as a fixer, helper and general handyman. I had no idea how to “fix” a generator, especially seeing I didn’t know what was wrong with it. But I loved taking things apart, so I did just that.
It was about the size of a large esky and I spent most of the day dismembering the unfortunate machine. I carefully cleaned every piece and when there was nothing left to take apart, I started to put it all back together again. As evening fell the now cleaned generator was pieced together with only a small collection of “extra” bits and pieces left in my pocket.
It was evening by now, Abu Bashar, his family and the occasional neighbour had been casually keeping an eye on me all day. Anyway, the thing was back together by late evening, it was filled up with petrol and now the moment of truth had arrived. As I was about to pull the starter cable, I remember thinking I had no idea why I thought it might work. I knew that all I had done was take it apart, clean it and put it back together again. I hadn’t “fixed” anything. So, any hope that it might work was clearly without basis. Put simply, it was a Hail Mary.
So, I pulled that cable, hailing Mary… and that beautiful two stoke started first time!! The bloody thing was working! And it was loud. As loud as any two stroke, angry at being silent for years, making up for lost time.
It was late, around nine or ten pm and the whole neighbourhood could hear this monster roaring, but no one seemed to care. There was electricity in the street!
The first thing everyone wanted to do was watch a video of an old Egyptian movie. Anything to take their mind off the misery and drudgery that was their daily life. And so there we were, family, friends and neighbours crammed together in a small living room, watching an old favourite movie, barely hearing a word over the roar of the machine outside. But happy that a little bit of joy and normalcy had returned despite the contrived and temporarily nature of the whole affair.
If you don’t know that you are in a war, and “just want your old life back” then taking a “safe and effective vaccine” to “protect you and your loved ones” from a “deadly disease” seems entirely reasonable. But unfortunately, none of that is true, including the bit about getting “your old life back”.
So, to summarise.
Yes, there is a war.
It is being fought over the Territory and the Border between The State and YOU The Citizen. It’s a land grab.
The State has been winning since March 2020.
The injection is the final step in that War and dissolves the last Border surrounding our Bodily Sovereignty.
In War, a War Mindset is required to survive.
War is a battle between two parties over territory
The state is in open warfare to reset its relationship with its citizens. To move the border
Passports not only move the border but then permit the state to keep moving that border as they see fit
One year ago today: WHO officially declares COVID-19 a pandemic.
Director-General Dr. Tedros: “We’re deeply concerned both by the alarming levels of spread and severity, and by the alarming levels of inaction.” pic.twitter.com/D0k0wOuYa2
Now, watch this through the lens of War. This was a declaration of War on The Citizen.
It was not clear to most, certainly not to me, back then. It is as clear as daylight today.
What’s interesting about this War, is that REGULAR Compliance is the end game. Not just today’s compliance, but ONGOING Compliance.
Please understand, there is no such thing as “fully vaccinated”.
There is now only non compliant and temporarily compliant.
The unjabbed are the Resistance.
But, not getting the jab, is among other things just a proxy for non-compliance.
So, in truth the non-compliant are The Resistance.
And what’s interesting about that is that if you have surrendered to date, you can Un-surrender.
If you QR Code to check-in everywhere, you could stop doing that. You can deploy a range of evasion tactics.
If you have taken one dose, you can choose to not take the second.
If you have taken two doses, you can choose to not take the “booster”.
If you were “enjoying your freedoms” you can choose to adopt a War mindset.
You can choose at any moment to stop complying with The State and reclaim some of your lost territory.
And while we are on the subject of surrender; just as you can un-surrender at any time, you can also surrender at any time, so do you need to surrender today?
If you have not taken the jab so far, do you need to give in today?
Why not leave your surrender for another day or another week?
I have written extensively about my D.A.D Strategy and a Waiting for Novavax Strategy so why surrender today, wait until tomorrow and then ask yourself the same question. In War, taking things one day and one week at a time makes a lot of sense.
Stuart Lindsay, an Australian retired Federal Circuit Court Judge wrote this wonderful piece:
Strictly speaking, we fell in March 2020 when COVID arrived in earnest, but I date it from my acceptance that my fellow citizens would never stir. You cannot wake someone who is pretending to be asleep. The truth is that whether through cowardice or prolonged conditioning the vast majority of Australians, including many of my close friends and even family members, have manifested since then the absence of any kind of allegiance to their country or their heritage.
Most of those I live among have no desire at all to recover the freedom to speak or to assemble which has been taken from them. What would they have to say anyway? The only public utterances to which they now aspire are those to be roared as part of a crowd at the bread-and-circuses events, such as the football, which they are occasionally granted permission to attend. Then they replace their masks for the drive home past empty shops on patrolled and near-deserted streets.
Stuart has some wonderful turns of phrase, such as this one describing the acquiescing (surrendered) masses:
Netflix, full bellies and a warm place to defecate. That is all most want these days, is it not?
Stuart understands the mindset required for these times, and the years ahead:
I show you the times. Look out of your window if you need corroboration. I show you what you must do to get yourself in order if you want to be of any value in the fight to preserve what is left of your heritage. Here are some other ways to ready yourself for that fight.
Relinquish all of that unseemly longing for the return of unregulated visits to the theatre or the cinema and those beloved restaurants. Accept that never again will such things be free of petty invigilation and that on the worst case outcome they will only be possible if you keep having mRNA booster jabs — now the case in Israel, where three shots are now required even as officials moot lifting it four. If you are wary and reluctant to be inoculated with treatments whose long-term effects remain unknown, as am I, you need to accept that governments intend to make you a pariah for not having a “COVID passport” and be prepared to forfeit such pre-Fall pleasures as dining out. Keep your self-respect instead. Read that long-neglected Cervantes or C.S. Lewis on your bookshelf, help out at a refuge for the homeless or visit your sick grannie. Australia is teeming with sick grannies, so I’ve heard.
Here is a wonderful recent speech by Dr. Julie Ponesse.
She references War a few times, here are the War references:
But it is not only information that is being weaponized, in this WAR; it is a person’s right to think for herself.
… we are in a kind of moral WAR.
But the WARS of the past have had clear and distinct boundaries: the east and the west, patriots, and government.
The WAR we find ourselves in today is one of infiltration instead of invasion, intimidation instead of free choice, of psychological forces so insidious we come to believe the ideas are our own and that we are doing our part by giving up our rights.
As a wise colleague recently said “This is a WAR about the role of government. It is about our freedom to think and ask questions, and about whether individual autonomy can be downgraded to a conditional privilege or whether it remains a right. It is a WAR about whether you are to remain a citizen or become a subject. It is about who owns you, you or the state.”
As someone born in the 70s, I never thought THIS would be a WAR I would have to fight, that the right to bodily autonomy, to the free and transparent exchange of information would be at risk.
Ok, I think it’s time we talk about The State. What does that word mean?
Well, let’s start off by saying that it doesn’t mean what it used to mean, and it doesn’t mean what you think it means.
It used to mean that your government, acting independently of other governments, independently of business and independently of media would try to increase its territorial footprint while reducing the citizens territory. Sometimes they would win and sometimes they would lose and there were checks and balances within the system that worked to reduce the speed and scale of the government’s land grabs.
Well, does that sound like what it is going on today?
If all 200 countries around the world are pretty much all doing the same thing, do you think they are acting independently?
Do you think that business is acting with the government or with you? Do you think business is a check against the government or is business aiding and abetting The State?
Do you think that Media is acting as a check against the government, or is it helping the government disseminate its misinformation and disinformation?
Is the legal profession standing up for you or aligning itself with the government?
Is the medical establishment acting honestly to protect its patients or supporting the government in its campaign?
The State is now a NETWORK and it’s borderless. It’s a Global Network on a scale never seen nor imagined before.
Several months ago, I described it as The MGM Triad
I was saying to my wife last night that in the past the “collapse” of a society happened within contained borders. The institutions of that particular country decayed to the point of collapse and/or takeover by nefarious actors (those that want to dominate others, look after others, “fix” the world’s problems because they know best etc., it is a very real personality type and is always a percentage of the population and they climb the poles of business and government).
Because of the way the globe has been rewired over the last 50 years and especially the last 20 years with ever more powerful global institutions and a communication grid with central points of influence and control, the collapse we are witnessing at the moment is “post-national”, its far higher upstream, all the way at the source of the river, which is why it’s happening everywhere.
Today I can say that I was on the right track, but I don’t think The MGM Triad even does this Global Network justice. It’s a good introduction to the question of “Why is this happening?” to someone just waking up, but there are even more layers to understand.
You will need to use a web translator to read it from the Norwegian website.
Within the article you will find a link and reference to this 169 page document, that does a deep dive into this global network. The document:
… shows connections between the Gates Foundation, Wellcome Trust, WHO, GAVI and other NGOs and Big Pharma. It contains round about 6,500 objects including like Persons, NGOs, Companies, Documents, etc. It also includes more than 7,200 links between them.
A great passage in this essay highlights the immense power of these networks. They have shown that they are able to get the largest governments in the world to heel.
The incredible power of the networks
To give an example of how much power these NGIs and actors have, I would like to show a current example that has hardly been mentioned in the media (nor in the alternative media), but which Mr.X immediately noticed, as he keeps an eye on the “right” NGIs.
On August 3, 2021, an open letter to the Biden administration was published. In this letter, the important NGOs, who – after what we have concluded – have been planning a pandemic since 2017, demanded. We will now take a closer look at these requirements from 3 August 2021.
Global Summit on Vaccinations
In the open letter, for example, one could read the following requirements:
” to host a global presidential-level summit on vaccinations, before the UN General Assembly in September, bringing together leading forces from the public and private sectors from around the world (…) and commits to taking the necessary measures to close gaps in vaccine supply and correct deficiencies in funding and capacity in the distribution and distribution of vaccines, as well as to create demand.”
It took only six weeks for Biden to comply with the claim. In parallel with the United Nations General Assembly, President Biden is currently hosting a virtual summit with representatives from 100 countries, where the president announced just that. And he urged the other countries to follow the example of the United States, as reported by Die Tagesschau, for example.
Do you now understand the power of these actors, when all it takes is for them to write an open letter to the president, and he complies with their demands within six weeks?
Vaccinate 70% of the world’s population
Furthermore, in the open letter it was demanded:
“To get the heads of state and government in the world, before or during the summit, to commit to achieving the goal of vaccinating 70% of the world’s population by mid-2022.”
«As an organizational framework, Biden introduced a transatlantic vaccination partnership. ‘Today we are launching a partnership between the EU and the US for a global vaccination offensive,’ he said, in order to have closer cooperation. The goal is to have vaccinated 70% of the world’s population by September next year.”
Within six weeks, Biden (and also the European Union) pledged to fully comply with the requirements set out in the letter.
This is another good piece fleshing out the role of the WEF (World Economic Forum) network and the many people involved.
What a co-incidence, the World Economic Forum outlines a vision in 2018 for Digital Identity and in 2021 the Australian Government is about to finalise its laws making it a reality.
A wonderful Australian writer fighting the good fight is Alexandra Marshall.
Make no mistake, vaccine passports are a domestic Social Credit System created under the watch of the federal Liberal Party. It is a sprawling government entity that denies rights based upon compliance in the hope that you will obey rather than exercising your democratic right to resist.
Citizens accepted vaccine passports because the government made them a condition of release from unlawful detention. As a population, we have been emotionally damaged to the point that people cheer on the discrimination of their neighbours. Ethics have been replaced by the intense fear of being sent into lockdown.
We are not witnessing a casual overreach of power – vaccine passports and QR check-ins are a complete abandonment of the Western democratic system. They are a threat to the liberty of our children and the survival of Australia’s laid-back spirit.
CJ Hopkins is a wonderful writer; he has written eloquently about his new War.
He describes the core desire of Totalitarianism as wanting:
… to remake the world in its paranoid image; to replace reality with its own “reality”
He goes further:
We are right in the middle of this process currently, which is why everything feels so batshit crazy. The global capitalist ruling classes are implementing a new official ideology, in other words, a new “reality.” That’s what an official ideology is. It’s more than just a set of beliefs. Anyone can have any beliefs they want. Your personal beliefs do not constitute “reality.” In order to make your beliefs “reality,” you need to have the power to impose them on society. You need the power of the police, the military, the media, scientific “experts,” academia, the culture industry, the entire ideology-manufacturing machine.
What I call The State he calls here Supranational Global Capitalism:
And, yes, it is all one ideology, not “communism,” or “fascism,” or any other nostalgia, but the ideology of the system that actually rules us, supranational global capitalism. We’re living in the first truly global-hegemonic ideological system in human history. We have been for the last 30 years. If you are touchy about the term “global capitalism,” go ahead and call it “globalism,” or “crony capitalism,” or “corporatism,” or whatever other name you need to. Whatever you call it, it became the unrivalled globally-hegemonic ideological system when the Soviet Union collapsed in the 1990s. Yes, there are pockets of internal resistance, but it has no external adversaries, so its progression toward a more openly totalitarian structure is logical and entirely predictable.
Naturally, there would be one official reality that you would force everyone to rigidly conform to at any given moment in time, but you would change the official reality frequently, and force everyone to conform to the new one (and pretend that they had never conformed to the old one), and then, once they had settled into that one, you would change the official reality again, until people’s brains just shut down completely, and they gave up trying to make sense of anything, and just tried to figure out what you wanted them to believe on any given day.
He coins the term GloboCap, which is his version of my MGM Triad.
But the goal of GloboCap’s War on Reality isn’t simply to deceive the masses and divide them into opposing camps. Rulers have been deceiving the masses and dividing them into opposing camps since the dawn of human civilization. This time, it’s a bit more complicated than that.
And depressingly this paragraph:
You could experimentally “vaccinate” millions of people whose risk of becoming seriously ill or dying from your apocalyptic virus was minuscule or non-existent, and kill tens or hundreds of thousands in the process, and the people whose brains you had methodically broken would thank you for murdering their friends and neighbors, and then rush out to their local discount drugstore to experimentally “vaccinate” their own kids and post pictures of it on the Internet.
We have watched as the New Normal has done precisely what every totalitarian movement in history has done before it, right by the numbers. We pointed all this out, each step of the way. I’m not going to reiterate all that again.
I am, however, going to document where we are at the moment, and how we got here … for the record, so that the people who will tell you later that they “had no clue where the trains were going” will understand why we no longer trust them, and why we regard them as cowards and collaborators, or worse.
Yes, that’s harsh, but this is not a game. It isn’t a difference of opinion. The global-capitalist ruling establishment is implementing a new, more openly totalitarian structure of society and method of rule. They are revoking our constitutional and human rights, transferring power out of sovereign governments and democratic institutions into unaccountable global entities that have no allegiance to any nation or its people.
That is what is happening … right now. It isn’t a TV show. It’s actually happening.
Whereas 20th-Century totalitarianism (i.e., the form most people are generally familiar with) was more or less national and overtly political, New Normal totalitarianism is supranational, and its ideology is much more subtle. The New Normal is not Nazism or Stalinism. It is global-capitalist totalitarianism, and global capitalism doesn’t have an ideology, technically, or rather, its ideology is “reality” When you are an unrivalled global ideological hegemon, as global capitalism has been for the last 30 years or so, your ideology automatically becomes “reality,” because there are no competing ideologies. Actually, there is no ideology at all … there is only “reality” and “unreality,” “normality” and “deviations from the norm.”
Few others have written as well as CJ Hopkins on how to deal with this New Normal “Reality”.
So we need to adopt a different strategy. We need to make the monster show itself, not to those of us who can already see it, but to the New Normal masses, the Covidian cultists. We need to make Jim Jones drop the peace-and-love crap, move into the jungle, and break out the Kool-Aid. We need to make Charles Manson put down his guitar, cancel orgy-time, and go homicidal hippie. This is how you take down a cult from within. You do not try to thwart its progress; you push it toward its logical conclusion. You make it manifest its full expression, because that it when it implodes, and dies. You do not do that by being polite, conciliatory, or avoiding conflict. You do that by generating as much internal conflict within the cult as you can.
In other words, we need to make GloboCap (and its minions) go openly totalitarian … because it can’t. If it could, it would have done so already. Global capitalism cannot function that way. Going openly totalitarian will cause it to implode … no, not global capitalism itself, but this totalitarian version of it. In fact, this is starting to happen already. It needs the simulation of “reality,” and “democracy,” and “normality,” to keep the masses docile. So we need to attack that simulation. We need to hammer on it until it cracks, and the monster hiding within in appears.
That is the weakness of the system … the New Normal totalitarianism will not work if the masses perceive it as totalitarianism, as a political/ideological program, rather than as “a response to a deadly pandemic.” So we need to make it visible as totalitarianism. We need to force the New Normals to see it as what it is. I do not mean that we need to explain it to them. They are beyond the reach of explanations. I mean that we need to make them see it, feel it, tangibly, inescapably, until they recognize what they are collaborating with.
Here is a good example of the tools now available to assault reality and create a new “reality”.
The global assault on reality and the creation of a new “reality” has created a Mass Psychosis, described by Dr. Mattias Desmet as Mass Formation.
John Waters, writes beautifully about a recent Desmet interview.
You cannot extract the Mass Psychosis from the New Totalitarianism. They are two sides of the same coin. Here are some extracts that help explain the phenomenon:
Le Bon it was who observed that the consciousness bestowed by membership of a crowd can be transformative, possessing individual members with ‘a sort of collective mind which makes them feel, think and act in a manner quite differently from that in which each individual would feel, think and act were that person in a state of isolation.’ In such a ‘psychological crowd’, individual personality disappears, brain activity is replaced by reflex activity: a lowering of intelligence, provoking a complete transformation of sentiments, which collectively may manifest as better and worse than those of the crowd’s constituent members. A crowd may just as easily become heroic or criminal, but is generally disposed towards destruction.
‘The ascendancy of crowds,’ wrote Le Bon, ‘indicates the death throes of a civilisation.’ The upward climb to civilisation is an intellectual process driven by individuals; the descent is a herd in stampede. ‘Crowds are only useful for destruction.’
–
He says there are four conditions that need to be in place to enable mass formation to occur in a society. The first is the presence of large numbers of socially isolated, atomised, people. The social bonds between people need to have been weakened. This is the most important, and the other conditions follow from it. Secondly, there will be large numbers of people who experience lack of sense-making in their lives and work — people who feel that their jobs are senseless, meaningless. Thirdly, there requires to be ‘a lot of free-floating anxiety’ — i.e. anxiety that is not connected to a mental representation so that the sufferer doesn’t know why he is anxious and afraid. And fourthly, there needs to be a lot of ‘free-floating psychological discontent’ — anger and frustration at, again, apparently nothing in particular.
And you also need mass media — without which mass formation would be impossible. Desmet does not explicitly say so, but of course it is also essential that these media be biddable and readily prone to corruption.
These conditions, he says, existed in Western societies long before the Covid crisis. There was, he says, ‘an epidemic of burnout’. He says something between 40 and 70 per cent of people in modern societies experience their jobs as senseless. He points also to the escalating use of psycho-pharmaceutical medicines to treat anxiety and depression.
–
There are, in situations of mass formation, says Desmet, three distinct groups that manifest themselves. Only 30 per cent, he says, are really hypnotised, and cannot be reached in any way. In addition, however, there are about 40 per cent who usually follow the crowd, and from the outset go along with that 30 per cent of total believers. There is another cohort of about 30 per cent who are not hypnotised, who try to speak out and resist. This group, he says, is extremely heterogeneous and disunited. If these people could unite, he says, they could bring the whole thing quickly to an end, but this seldom proves possible.
–
Totalitarianism in its full-blown form, then, is something that comes after, but ‘after’ what? It comes after a lengthy ‘preparation’, not necessarily planned with malign intent, in which human beings become isolated, atomised, alienated and lonely — conditions for which the totalitarian has ready solutions in the promulgation of bogus community and imagined bonds of mutual hatreds. The negative undertones of these processes suggests some form of prior error, and this may well have been present, perhaps in the pursuit of greed or exploitation, but this is not any longer admissible. Totalitarianism is like a secondary condition that descends on a society that has first of all been subjected to certain processes of modernity: technologisation, industrialisation, individualisation, atomisation. It is, in a sense, like the lung cancer that ensues from a lifetime of smoking, or the type 2 diabetes that results from an excessively sweet tooth. But it is not ‘secondary’ in the sense suggesting ‘lesser’ or ‘minor’ or ‘subordinate’: When it arrives, totalitarianism announces itself as the actual purpose and destination-point of the entire historical process, the discovery of the actual meaning of history. It follows, but is not collateral to, the events which preceded it. Indeed, its arrival announces a coherence to those previous events that had not hitherto been perceived: It ‘makes sense’ of the drifts and apparent randomness of the past, and in doing so turns common sense on its head and compels man to admit his prior errors of understanding and accept that the true direction of history has now been revealed.
Paul Collits has done incredible work all throughout the scamdemic, and I was lucky enough to come across him early. Here he writes about August Landmesser (look him up):
Two excuses might be proffered for going along with tyranny – we didn’t know what was going on, and I thought I personally would be safe from the tyranny if I played along.
Take the first excuse. Dr Robert Malone, an inventor of the mRNA vaccine, has noted, “… if you’re not outraged, you’re not paying attention”. He was speaking of the hideous truths about the jab. Malone’s accusation implies the first excuse. We didn’t know. We perhaps suspected something, but we excused the political class for mere “mistakes”. We made a choice, not to think too deeply about the emerging “new normal”. We didn’t try very hard at all to comprehend what was going on. We found excuses to justify our own compliance. Going against the crowd is too much like hard work. People will think I am … an anti-vaxxer! Thinking hard about difficult issues will only give me the guilts, and make my life complicated, so I will park it.
Here he talks about “strategic obeyers” and how they sustain The State:
Some of this behaviour might be termed “strategic obeying”. This is self-regarding conduct whose aim is to protect the things that are important to us while ceding minor freedoms to the Covid State. Anyone who hates mask mandates but obeys them in order to get the shopping done, rather than risk a fine or risk getting spat at by angry CovidManiacs, is a strategic obeyer. A reluctant obeyer, perhaps, but an obeyer nonetheless. If I just do this, maybe they won’t come for me. If they come for the unvaccinated, maybe they won’t come for me. Strategic obeyers sustain the Covid State. They form a key part of the group that remains silent, and no doubt all the various Nudge Units will have figured this all out.
And:
Those who go along to get along enjoy what Levant terms “the peace of surrender”.
I retweeted this yesterday & now again, so nobody misses it. One of those speeches that might get recorded in history as an important event on its own, because it captured the exact inflection when things started to turn around. 🥊pic.twitter.com/ixtRWGpz0l
This article went viral recently, written anonymously by Spartacus. Personally, I think that Dr. David Martin wrote it as it covers a lot of ground that he is very familiar with. I recommend reading the whole thing as it is a great summary of the story to date.
What is the purpose of all of this? One can only speculate as to the perpetrators’ motives, however, we have some theories.
The Elites are trying to pull up the ladder, erase upward mobility for large segments of the population, cull political opponents and other “undesirables”, and put the remainder of humanity on a tight leash, rationing our access to certain goods and services that they have deemed “high-impact”, such as automobile use, tourism, meat consumption, and so on. Naturally, they will continue to have their own luxuries, as part of a strict caste system akin to feudalism.
Why are they doing this? Simple. The Elites are Neo-Malthusians and believe that we are overpopulated and that resource depletion will collapse civilization in a matter of a few short decades.
Head of the World Economic Forum Klaus Schwab wrote a Harvard Business Review piece titled, ‘Power and Policy: The New Economic World Order’ where he detailed his belief that the industrialised world has been going through an economic revolution. Keep in mind, the article is written in 1994. He correctly lusts after [he] points out the rise of Asia, commenting, “One consequence of the new parity is that the West can no longer hope to dictate the rules of the game.”
In this, he is only partially right. The circumstance he prophesied has only manifested because organisations like the World Economic Forum and the United Nations have trained Western leaders to be weak. It was not an inevitability of trade structures, but rather a matter of ideological infestation. The constant infiltration of socialist rhetoric into the once free world via endless champagne conferences has left it unable to work out what gender it is, let alone present a strong front against the rise of Asia.
By 2018, the World Economic Forum was publishing articles insisting that we must all work together to hasten the rise of Asia and teach ourselves to embrace the New World Order. The United Nations have a similar song sheet. Before Covid, they spoke of the New World Order in the context of a green revolution and the dismantling of old industrialised nations in favour of empowering the third world.
Most of the propaganda coming out of the United Nations these days talks about sustainability, mass-migration, climate goals, and Covid as a singular item – an omini-shambles apocalypse with only one solution: world socialism disguised as environmentalism.
And lastly here is Iain Davis writing about the “global commons”. It’s a good way of further understanding the “territory” this War is fighting over.
While we have been distracted and transitioned by the alleged global pandemic, or pseudopandemic, the Global Public Private Partnership (GPPP), who orchestrated the chaos, have been very busy. They have created the asset rating system that will afford them total, global economic control. This is based upon Sustainable Development Goals (SDGs) and utilises Stakeholder Capitalism Metrics (SCM).
This new global economic system is what the politicians mean by “build back better.” It is the essence of the World Economic Forum’s Great Reset.
–
Stakeholder Capitalism Metrics – SCM – were devised by the World Economic Forum, who describe themselves as the international organisation for public-private cooperation. When combined with the SDGs outlined in the UN Agenda 21 and 2030 frameworks, SCM enable the GPPP to seize the entire Earth, all its resources and everything on it, including us.
In order to control us we are being transitioned into a technocracy with the biosecurity state acting as the central control mechanism. Public health is the new focus for global security and centralised control of the entire system has been established during, and as a result of, the pseudopandemic.
–
Again we see the recurrent themes of the GPPP. The planet must be saved from us, we are a pestilence that must be controlled; Covid-19 is, as ever, an opportunity to transform the global economy; our survival and GPPP stewardship of the global commons are one and the same and everything must be transformed.
Put simply:
If the world is being destroyed by humans doing whatever they want (climate catastrophism)
And these humans are grouped together within pesky democracies and pesky borders
Then to save the world we need to build a system that keeps people from doing whatever they want
By changing the democracies and dissolving the borders
It has been a long term project that is coming to fruition today
The role of the CCP within this network is both very real and complex. I’m not going to spend time on it here, god knows this piece is long enough, but you could do worse than follow Michael Senger’s work on the subject.
I will say this though, as long the the Network is useful to the CCP, they will play along. If the Network helps to diminish and destabilise its strategic adversaries, then why not help it along. But if the Network stops being useful, the CCP will simply devour it.
All the players in this Network will one day be long gone, but the CCP will still be around. They are playing the longest game in town.
Data continues to emerge according to which not only were the mRNA shots ineffective at preventing infection and transmission of COVID-19, but they may have caused widespread harm to persons cajoled or coerced into undergoing vaccination, despite their own relative invulnerability to the worst effects of the virus. Anecdotal cases abound, but diehard regime narrative devotees continue to dismiss such “incidents”—thousands of which are recorded in the government’s own VAERS (Vaccine Adverse Effects Reporting System) database—as purely coincidental. It is more difficult to downplay reports involving entire cohorts, such as the increased incidence of myocarditis among young males, which the CDC itself has acknowledged. Some critics have suggested that a disproportionately high percentage of pregnant women in Pfizer’s initial trial of the shots suffered miscarriages.
Back in November 2021, in the midst of the widespread and aggressive “Vaccinate everyone!” campaign, I spoke with a woman in Oregon who matter-of-factly mentioned that her (vaccinated) daughter had suffered three recent miscarriages. Recognizing that it was too late to do anything anyway, given that the daughter had already been vaccinated, I did not dare to suggest that her troubles may have been caused by the shots she had no doubt been exhorted by her doctor to take. At that time, following the lead of CDC director Rochelle Walensky, health officials everywhere were in the midst of a marketing blitz according to which COVID-19 vaccination would protect mothers and their babies alike.
I said nothing to the woman in Oregon about the dangers of introducing foreign substances into pregnant women (although I had written about it), but I did naturally wonder at the time whether there might be a causal connection between the poor daughter’s miscarriages and the shots, given the biological activity of the spike protein already known to induce blood clotting and heart troubles. The mother of the young woman—who was pregnant again, for a fourth time—seemed optimistic that somehow there was nothing to worry about, even after three failed attempts to bring a baby into the world. It is possible, I realized then and continue to own, as I must, that the woman was simply unable, for unrelated reasons, to carry a child to term. But given that the biologically active spike protein is what the original virus used to access cells, and production of lots of it was induced by the injected mRNA, it would not take a tinfoil hat conspiracy theorist to surmise that the pregnancies may have been sabotaged by the shots.
Critics such as feminist scholar Naomi Wolf, who early on in the pandemic raised questions about the shot’s safety, given many reports of irregular menstrual cycles in women who under went vaccination, were denounced as purveyors of misinformation and immediately deplatformed by the social media giants. Only recently have such “conspiracy theorists” been permitted to articulate their concerns in the public sphere once again—and only on some platforms, including Twitter, which to Elon Musk’s credit reinstated thousands of accounts shut down for the crime of deviating from the narrative favored by the pharma-government alliance. If the shots are indeed dangerous to fetuses, it is needless to say too late for all of the pregnant women tricked into believing that because the CDC insisted that there was no evidence of risk to them and their offspring, they should therefore roll up their sleeves.
That Pfizer knew all along that their mRNA shots had effects upon women’s hormonal systems was corroborated through Project Veritas’ sting operation involving a Pfizer research director, Jordon Triston Walker. In the recorded interview thought by him to be a friendly conversation with a date, Walker observed that the shots seemed somehow to be affecting the endocrine systems of women. The delicate hormonal balance needed to maintain a pregnancy suggests an immediate connection between the widely reported menstruation irregularities of women and the incidence of miscarriages in some of the initial trial subjects.
The data interpreted by some critics to imply that miscarriage was one of the many possible side effects of the Pfizer shot were made public only recently, with the release of a large trove of court-ordered documents which the company is now required by law to provide, despite its initial insistence that it would take seventy-five years to do so. Setting aside the question of whether miscarriage is in fact a side effect of the shots, the very idea that it would take so many years to make public the documents said to have served as the basis for the FDA’s (Food and Drug Administration’s) decision to grant the Pfizer product Emergency Use Authorization (EUA), so that it could forego the customarily stringent multi-year testing program required of pharmaceutical products more generally, struck many people as absurd.
To my mind, the situation constituted a classic Charybdis and Scylla. If it was humanly impossible to process and assess all of the data (all 451,000 pages of it) in the short period between the creation of the vaccines and December 11, 2020, when the EUA was granted, this could be taken to imply that the persons on the committee incompetently executed their role and indeed based their decision to approve the shots primarily on Pfizer’s obvious wish that they do so. Alternatively, it was always possible to process the documents for publication, and the company’s resistance to doing so was due to the content of the documents themselves, which might harm the ambitious sales program to vaccinate everyone on the planet with the new product.
The director of the CDC, Rochelle Walensky, encouraged pregnant women from the beginning to get the shots, quite deceptively claiming that there was no cause for worry about possible health risks to fetuses. The safety information provided with the original shots itself indicated that pregnant women had been excluded from the initial trials, as they are for most pharmaceutical products. The reason why pregnant women are not included in early stage clinical trials of products intended for the general population is because they represent a special case, given the fragile chemical environment enveloping the fetus. It is a matter of common knowledge that developing human beings are highly sensitive to and often endangered by foreign substances—alcohol and nicotine being two well-documented examples. The vulnerability of fetuses was most notoriously and unforgettably demonstrated when pregnant women were prescribed Thalidomide on the basis of clinical trials which, again, excluded pregnant women. As in the case of the COVID-19 vaccines, Thalidomide was distributed by doctors under the misleading marketing line that there was no evidence that it would harm fetuses. Thalidomide killed thousands of babies and deformed thousands more before it was finally withdrawn from the market.
We now know from Pfizer safety data recently released that some of the women in the initial trial were in fact pregnant—apparently without having known that this was the case at the time, which was why they were not excluded from the trial. The vaccines may or may not have caused their reported miscarriages, but the fact that the CDC would encourage pregnant women, on the basis of nearly no data, to undergo vaccination betrays a reckless disregard and their true goals in injecting everyone everywhere, even members of low risk cohorts, with the mRNA treatment. Ignorance is bliss for pharmaceutical companies, which can continue to market and sell products for years, reaping billions of dollars of profits, before finally halting sales on the basis of widely reported and what come eventually to be undeniable post-launch problems, as in the cases of Vioxx, Belviq, Baycol, etc.
Above and beyond the profit motive was plausibly the desire to test the newfangled mRNA technology on the largest sample of human beings possible—whether or not they actually needed any treatment whatsoever in contending with COVID-19. Of course, if the desire on the part of Pfizer CEO Albert Bourla and Moderna CEO Stéphane Bancel was to make strides ahead in the research and development of other lucrative medications, then the quest for data, too, was ultimately driven by the profit motive—albeit looking forward, to future possible blockbuster drugs.
Certainly, the steadfast resistance, indeed, the outright refusal on the part of public health authorities such as Dr. Anthony Fauci and Dr. Rochelle Walensky, for more than a year after the launch of the COVID-19 vaccines, to acknowledge the relevance of natural immunity in those persons previously infected, and to recommend appropriate adjustments to the U.S. government’s mandates—for both health care workers and military personnel—supports the hypothesis that one of the overarching aims of the aggressive, relentless vaccine campaign was not to save the lives of the small percentage of human beings vulnerable to the virus, but to amass data.
Corroborating this interpretation, according to which the companies hoped not only to reap a windfall of profits but also to collect a huge amount of data, is the explanation by many critics (including Robert F. Kennedy, Jr. and Dr. Peter McCullough) of the assiduous suppression of any and every other therapeutic which the vaccine salespersons recognized would compete with and diminish the uptake of the newly patented products. Most importantly of all, ivermectin and hydroxychloroquine were dismissed and denounced by public health authorities, and ridiculed by parroting pundits throughout the media, because EUA cannot be granted to products when alternative therapies are available.
In his conversation with a Project Veritas reporter, Dr. Jordon Triston Walker also shared the potentially explosive piece of information that Pfizer executives had floated ideas such as mutating the COVID-19 virus so as to be able to develop vaccines preemptively. It was not entirely clear from Walker’s remarks whether the intention would be to release those mutated viruses so as to direct the course of the disease in populations, or simply to predict which variants would pop up on the scene naturally, through mutations of the virus in its effort to self-propagate by evading the antibodies induced by the latest shots.
Pfizer responded to the bombshell revelation by effectively minimizing the story through suggesting that the process described by their (now former, I presume) employee was essentially part of the normal, necessary research conducted in producing, for example, the flu shot each year. Nearly everyone by now is more or less aware that the flu shot is a gamble, involving researchers predicting which strains will be most prevalent and virulent. People who undergo inoculation against those versions may still fall ill because they may or may not come in contact with the predicted dominant strains. Some individuals report anecdotally that they were never more ill than during a year when they opted for the “free” flu shot, which clearly indicates that they encountered versions of the pathogen not expected by the researchers who determined the ingredients for the products distributed during that particular flu season. Unsurprisingly, neither anecdotal reports, nor adverse effects, nor even consistently poor efficacy rates have deterred pharmaceutical firms from pushing for widespread uptake of their mediocre flu shot products in very public and misleading advertising campaigns fronted by government health authorities.
Needless to say, if the intention of Pfizer in mutating the COVID-19 virus was to release it into the human population in order to induce countless numbers of persons to seek protection by purchasing (or obtaining from their government) the “vaccine” developed in order to stop that strain, then that would constitute a flagrant violation of any decent person’s basic sense of ethics. Such a possibility would moreover, and disconcertingly, be taken by some to accrue a degree of plausibility to the conspiratorial notion according to which the original COVID-19 virus was not only a gain-of-function product, created by researchers in a lab, but also intentionally released into the world in order to initiate The Great Reset being promoted by members of the World Economic Forum (WEF), led by Klaus Schwab.
More plausible, I believe, is that Pfizer and Moderna, et al., are primarily focused on the future of their other new mRNA products in the works. It is not at all far-fetched to surmise that the relentless, divisive push to vaccinate everyone everywhere with the first mRNA treatment ever tested on a population of human beings, made possible only by the FDA’s EUA, was spearheaded by companies with much broader goals in mind. The CEOs of these companies have publicly vaunted their plans to use mRNA to cure cancer and other intractable diseases, which in fact best explains their manifest fervor to acquire as much data as possible, by all means necessary. Such a program, albeit less explicitly heinous than creating illnesses in order to be able to sell patented cures for the symptoms caused by them, nonetheless involved using all of the people coerced into undergoing treatments for which they had no need as the means to the companies’ mercenary ends.
Further evidence for this admittedly unsavory interpretation can be seen in the push to vaccinate children, even infants, despite the minimal danger posed to them by the COVID-19 virus. If, in reality, the chances of a child dying from COVID-19 is less than the chance of their being hit by a bolt of lightning, then it is hard to see why anyone would push for uptake under a public health pretext. Yet those who wish to foist the product on young persons, including infants, have continued to press the line according to which the virus poses a serious health risk to everyone, and the vaccine will help to protect children along with their parents, this despite data according to which the protection provided by the shots, even to the vulnerable persons who might be said to benefit, plummets to nothing after only a few months. (Preposterously enough, according to one recent study at the Cleveland Clinic, in the longterm, the more shots one has received, the greater become one’s chances of contracting COVID-19!)
A second reason why children have been important for the product companies is peculiar to the United States, where the PREP Act (Public Readiness and Emergency Preparedness Act) protecting companies from liability in the event of adverse effects covers any product approved as a part of the child immunization schedule. Demonstrating their complete capture by pharmaceutical industry forces, on February 9, 2023, the CDC added the COVID-19 shots to the long list of those recommended in the childhood vaccination schedule (which now includes dozens of shots), thus ensuring the product companies massive profits for years to come through the inoculation of persons not at significant risk from the virus, using a product whose already nearly negligible protective capacity for invulnerable persons (a risk reduction of ~1%—or less) spans less than a few months.
Unbelievably enough, the new CDC recommendation for children (beginning at six months) includes the original COVID-19 vaccine, though the wild strain of the virus may no longer exist, along with booster shots, for which the only clinical trial on human beings is currently underway—on the millions of persons who rolled up their sleeves on the basis of safety data gathered from only animal trials. The results are trickling in on the first-round of “bivalent” booster shots, which have so far been demonstrated to have only middling (30%) efficacy in preventing infection by the variant they are attended to address. But the virus will continue to mutate, thus serving as the pretext for producing new booster formulas. This implies that, under the CDC’s immunization guidelines, each new booster shot will of necessity constitute yet another experimental trial, to be conducted, shockingly enough, upon children throughout the years of their development into adults. In other words, children have been set up to serve as test subjects (i.e., human guinea pigs) for each newly developed “booster” to follow in the future as the virus continues to mutate, despite the fact that they make up the least vulnerable cohort of them all.
Why should “vaccines” which do not offer longterm immunity to anyone and are not even necessary for children—the CDC itself explicitly claims that most children will experience only mild symptoms from COVID-19—be included in the battery of time-tested vaccines such as those against polio, measles, etc.? Along with the desire to sell products, and to be able to test new products on children, is, again, scandalously enough, the fact that the CDC’s addition of the mRNA shots to the children’s immunization schedule protects the manufacturers in perpetuity from lawsuits, even after the State of Emergency has ended. President Biden has announced that the State of Emergency will be lifted on May 11, 2023, two months after the CDC added the COVID-19 shots to the children’s immunization schedule.
Because state and local officials follow the cues of the CDC, we can expect to see its recommendation for childhood inoculation by the COVID-19 shots swiftly transformed into mandates for public school children in states throughout the country. This will likely happen in places such as Massachusetts, California, and New York, where health authorities have persisted in retaining laws which restrict the behavior of residents even as new data continues to refute the erroneous premises widely embraced by officials in the spring of 2020 regarding masks, social distancing, etc. Although states such as Florida rescinded the COVID-19 emergency laws, and have passed legislation to protect children, the fact remains: with the federal level CDC recommendation in place, the product companies will retain their protection from future litigation arising from adverse effects, even if the data currently being collected and analyzed eventually demonstrate widespread harm to either children or adults.
It would be a mistake to judge corporations by the moral standards appropriate to individual persons. Corporations are beholden only to their stockholders, and their sole goal is to maximize profit. But the spokespersons for such companies are themselves individual human beings, as are all of the authorities representing public health organizations whose ostensible raison d’être is to protect members of society, not to maximize the profits of their sponsors. When institutions such as the FDA are coopted by mercenary forces, they cease to perform the function which citizens are depending upon them to execute. Because this already happened in the case of the opioid crisis, the fact that people fell for the trick once again in the case of the COVID-19 “vaccines” is best and perhaps only explained by the fearmongering campaign used to psychologically traumatize them to the point where they lost all critical bearings and agreed to undergo an experimental treatment of which most of them had no need.
Every healthy, nonobese person under the age of seventy who underwent COVID-19 vaccination was deceived into serving as a pro bono experimental subject in a pharmaceutical product trial. That millions of well-meaning parents, believing that they are doing the right thing, will on the basis of the CDC’s addition of the COVID-19 shots to the children’s immunization schedule, enroll their progeny in an entire series of such experimental trials, using substances never before tested on human beings, is nothing less than tragic.
Laurie Calhoun is the author of We Kill Because We Can: From Soldiering to Assassination in the Drone Age, War and Delusion: A Critical Examination, Theodicy: A Metaphilosophical Investigation, You Can Leave, Laminated Souls, and Philosophy Unmasked: A Skeptic’s Critique, in addition to many essays and book chapters.
The CDC recently codified International Classification of Disease (ICD) codes for Covid-19 vaccine status. ICD codes are extensively used in medical records, medical insurance data and health research to classify precisely disease states as well as injuries from exogenous agents such as accidents, medication and medical device injuries, toxic chemicals, etc. Vaccination status is not a disease or an injury state, yet CDC has rationalized creating ICD codes for it. The coding is set to become effective on April 1, 2023.
As described by Dr. Robert Malone, “The ICD classification system is run by the World Health Organization, not the US government.” The vaccine status ICD codes were developed by the US Centers for Medicare and Medicaid Services (CMS) some nine months ago, and CDC is implementing them.
The coding scheme, Z28.xxx, includes both vaccination status and possible reasons for the status. However, there does not appear to be a code for “fully vaccinated,” only for various states of “not fully vaccinated.”
The code Z28.0 means “immunization not carried out because of contraindication.” Z28.1 means “immunization not carried out because of patient decision for reasons of belief or group pressure.”
Z28.2 means “immunization not carried out because of patient decision for other and unspecified reason.”
Z28.8 means “immunization not carried out for other reason” which because of code Z28.2 must refer to reasons not attributable to patient decisions.
Finally, Z28.39 means “other underimmunization status,” including “Delinquent immunization status” and “Lapsed immunization schedule status.”
However, a potential contradiction arises because code Z28.310 means “unvaccinated for COVID-19.”
In order to reconcile this, the Z28 codes in the previous paragraph must refer to vaccines other than for Covid-19. The only other Covid-19 code is Z28.311 which means “partially vaccinated for COVID-19,” where “partial” refers to the CDC definition for “fully vaccinated” at the time when the patient visits the health-care provider who records the vaccination status in the medical chart.
It is apparent that the details of reasons for patient choices for vaccine status are not specified in codes for Covid-19 vaccines, but the CDC has some two months to fix this. There are no specific codes yet for “refused to divulge COVID-19 vaccination status” or “unknown COVID-19 vaccination status,” but these codes are likely to be added at some point.
What is the usage for which this information is planned? There is certainly a public health rationale for agencies to be able to monitor population vaccination status. Personal health information is routinely analyzed by public health agencies, insurance companies and health researchers, but in anonymized and grouped formats. The identifiable information is recorded in the databases, however HIPAA and other laws strictly protect identifiable health information and regulate how such information may be used for analyses.
In theory, vaccination status could be no different. Medical records already know your age, gender and race, where you reside, about your obesity, diabetes, your smoking and alcohol usage and your HIV status. Some of this information could be stigmatizing if released publicly, but at present there are no politicized or other circumstances to force unwanted choices on members of the public based on this compiled personal information.
Imagine, however, that one day, government agents are pounding on your door at 6am, telling you that you are required to take smoking cessation medications, under penalty of forced residence in a “smoking-cessation hotel” until you submit to the government’s requirement.
The medications have built-in transmitters that are activated when exposed to stomach acid, so taking them is recorded. After all, 500,000 Americans die every year from smoking-related diseases and their end-of-life medical care is an expense for which the government no longer wants to pay. Your smoking is economically hurting the medical care that grandma needs. Or something.
But Covid-19 and its vaccination are different. The Covid vaccines and their boosters were created under emergency-use authorization (EUA) protocols and are not fully licensed. The Biologics License Application (BLA) versions, e.g., Comirnaty, are not generally available in the US. This licensing chicanery has not gone unnoticed by the American public and a substantial fraction of people find the vaccines controversial.
Many people have seen their multiple-vaccinated friends and relatives get Covid, some multiple times. Many have also seen friends and relatives harmed by the vaccines, and most people know of the incessant daily deaths of healthy athletes, deaths discussed as caused by “coincidence.” People have seen the vaccines touted as solutions to the pandemic, yet utterly fail across the population to suppress transmission of the infection.
And, people have been bombarded with daily narratives for two solid years that the vaccines are “safe and effective” and that they must be taken, and that unvaccinated people are “bad,” “selfish,” demonized as doing damage to society, and should be shunned.
That is, personal vaccination status today is the most stigmatizing personal data of modern times, surpassing having AIDS. As such, any government compilation must be “bulletproof” against hacking and misuse. As well, the government must be trusted to maintain the data for use only as other personal medical data have been used.
Given the two-plus years of massive government propaganda about the vaccines, about their adverse effects, about Covid, about early Covid treatment, and the government collusion with social media companies in suppression of valid dissenting medical and scientific opinions and data, there is no empirical reason to support trusting the government with such sensitive, stigmatizing data.
There is no reason to believe that the government will not release the status information to insurance companies or other companies doing large business with the American public. Further, there is no recourse should the government actually release such confidential data. Thus, nothing may stop such companies from restricting activities based on the stigmatized data. For example, public travel could be blocked; bank accounts could be blocked; purchasing could be blocked.
The free pursuit of happiness is enshrined in our Declaration of Independence. The government cannot lawfully interfere with normal transactions of everyday life. But private companies working at the government’s behest, with government-supplied personal status information, could very well do it.
As has been seen from the FOIA documents, hundreds of government employees have spent the pandemic years doing exactly this unconstitutional behavior in getting social media companies to suppress Americans’ freedom of speech.
Furthermore, there is now no rational government interest in compiling vaccination status at all. At a time when vaccination was generally thought (incorrectly) to reduce Covid-19 transmission across the population, there might have been a rationale for doing so.
However, on August 11, 2022, the CDC stated publicly that the Covid-19 vaccines do not work as a public health measure to control virus transmission. They said, “Receipt of a primary series alone, in the absence of being up to date with vaccination* through receipt of all recommended booster doses, provides minimal protection against infection and transmission (3,6).” “Being up to date with vaccination provides a transient period of increased protection against infection and transmission after the most recent dose, although protection can wane over time.”
The fact that such benefit is “transient” and wanes implies that after some short period, boosters fail to reduce risk of transmission and thus that vaccine mandates are invalid.
The only government interest in mandating Covid vaccines, and thus in compiling personal information about vaccination status, is that the vaccines reduce transmission. They don’t.
Secondly, the CDC’s August 11th policy guidance does not distinguish between vaccinated and unvaccinated people in any way for any policy. There is thus no compelling government purpose in defining people as vaccinated or unvaccinated. It would be like the government compiling personal information on hair color, except that hair color is not stigmatizing and vaccination status is extremely stigmatizing.
The government itself—through the CDC—has determined that vaccination status is not of policy importance. There can thus be no compelling interest for the government to forcibly collect this information against the wishes of the population, even were it not stigmatizing. So much more so after the government has spent the last two years publicly demonizing unvaccinated people for their rational and legitimate personal health choices.
Harvey Risch, Senior Scholar at Brownstone Institute, is a physician and a Professor Emeritus of Epidemiology at Yale School of Public Health and Yale School of Medicine. His main research interests are in cancer etiology, prevention and early diagnosis, and in epidemiologic methods.
In 2002, with a little help from National Defence, we brought to McGill the (then) president of the Club of Rome, Prince Hassan, who made a contribution to the Pluralism, Religion, and Public Policy conference I was co-chairing and to the bookthat came out of it, Recognizing Religion in a Secular Society. Our then chief justice, Beverley McLachlin, also made a contribution. Through another keynote speaker, Richard John Neuhaus, I afterward had the privilege of becoming acquainted with Avery Dulles, one of America’s best theologians and a very fine man.
This fine man, the late Cardinal Dulles, was a convert to Catholicism, a religion now undergoing a de-patterning and re-patterning experiment I have begun describing elsewhere. With the death this morning of another fine man, Benedict XVI, requiescat in pace, that experiment will doubtless be accelerated, but this is not the time to discuss it. Avery Dulles also happened to be the son of John Foster Dulles and nephew to Allen Dulles, who made up the other half of the famous Dulles duo—Secretary of State and Director of the CIA, respectively—that in the post-war period determined much of American foreign policy. Volumes have been written, and protest songs sung, about their political ideas, financial interests, manipulation of foreign states, and dastardly deeds during the cold war, in the struggle between the emergent empires of America and the Soviet Union.
It is a particularly dastardly deed I have in mind here. It sprang from Allen Dulles’s concern over intelligence that the Soviets were experimenting in mind control. The attitude he adopted was this: If they are doing it, we also must do it, and do it more effectively. That, of course, was a quite common attitude, the same that had led through two world wars, or one long one, to the blasphemously named Trinity project—to high-altitude bombers obliterating unarmed civilians and, with them, the remaining shreds of the West’s commitment to Just War theory, learned long ago from that great defender of the Americas, Francisco de Vitoria.
With that obliteration went any obvious claim to moral superiority over its enemies and with it came, inevitably, the re-wilding of the West (prophesied by Heinrich Heine and appraised by Elizabeth Anscombe) even in America. Power would now be maintained there, as in Russia, without justice. Bellum would be turned back into duellum. Witness the Kennedy assassinations. That oxymoron, utilitarian ethics, would prevail, permitting the Pentagon to experiment more freely on the citizenry it is supposed to protect, or on its friendly neighbours. Porton Down had been doing that in England for some time. In 1959, it chemtrailed the south coast, with devastating effects on the Dorset population; the Pentagon did the same thing in Canada, whatever it may have been doing at home.
Now, the deed in question was of that type. It took place here in Montreal. It involved no planes or explosives, though it did involve chemicals. It was conducted quietly in Ravenscrag, a building nestled at the foot of Mount Royal that houses the Allan Memorial Institute. There bombs were set off in the brains of unsuspecting subjects by sensory deprivation, hallucinogenic drugs, and electro-shock therapy, under the direction of Professor Donald Cameron, founding director of the Allan. Cameron, an American who came to McGill in 1943 with an intelligence background, eagerly conducted experiments on human subjects from 1957 to 1964, experiments so obviously illegal and immoral that even Dulles thought them better performed on foreign soil.
These were, as Cameron himself called them, de-patterning experiments that fit with his work of inducing amnesia with a view to selectively recovering memories in such a way as to substantially alter human behaviour. They belonged to a larger mind control project dubbed MKUltra, about which one can read briefly in the McGill Tribuneor at greater length in David Talbot’s The Devil’s Chessboard: Allen Dulles, the CIA, and the Rise of America’s Secret Government.
Dr. Donald Ewen Cameron (1946)
McGill, as I may have mentioned before, suddenly deleted the web pages devoted to the Pluralism, Religion, and Public Policy project when it was discovered that I had been chronicling the rise of the transgender madness, the rapid progress of euthanasia, and other matters deemed embarrassing by friends of our former principal. I was spared any treatment at the Allan—today a much different sort of place, thankfully—but that deletion was a sign, however tiny and insignificant a sign, of our ongoing need for amnesia: our need to forget what we once were, and what the transitioning process actually looks like, so that we might more easily become whatever it is our corporate handlers mean us to become.
The contents of those ramshackle pages were spared, not that it matters, but things were otherwise with MKUltra. In 1973, then CIA director, Richard Helms, destroyed the agency’s records of the project. It simply wouldn’t do for people ever to know what had transpired. For, if they did know, they would also know what we are becoming.
And what is that? Besides fools, I mean, fools in both the intellectual and the moral sense. I’ll tell you. We are becoming the experimental subjects of greedy corporations and power-hungry imperialists lacking all moral scruple. What’s worse, we are becoming complicit in their immoral experiments, just as McGill was complicit in MKUltra experiments. Our behaviour is being altered. We are being de-patterned and re-patterned to suit purposes foreign to our own.
Nullifying Nuremberg
Cameron’s intelligence background included being sent by Dulles, who was then OSS director for Switzerland, to Nuremberg in November 1945. He was not there to learn medical ethics, to which he was impervious, but to make an assessment of Rudolph Hess, for reasons uncertain. One thing quite certain is that there was a great deal of hypocrisy at Nuremberg, for the same countries that were holding the Nazis to account were cutting deals to learn everything they could about how their medical crimes were conducted and what useful information had been gleaned along the way. This was not for the supposed good of humanity, but for the good of the intelligence community and the pursuit of national interests.
The arc of Dulles’s own intelligence career ran from Berne in 1941 to the Bay of Pigs in 1961. He was fired for that fiasco by JFK, who two years later was shot in Dallas by his deep-state opponents. Kennedy lay quietly in Arlington while Dulles served on the Warren Commission that whitewashed his murder with the “lone gunman” lie. It would be just as much a lie to pretend that what America did under Dulles was simply the work of a renegade CIA director. MKUltra, which continued for some time after his departure, was symptomatic, not aberrational. Men had licenced men to operate beyond the laws of God and man; even men of medicine, men like Cameron. Not only in Russia or Germany, but also in America and Canada.
The myth of progress would have us think that we are getting better and better. The truth is that we are getting worse and worse. We have built a culture of death in which the unwanted and unloved are attacked with lethal force. We have made abortion and euthanasia routine. We are on the side of Herod, not of the Wise Men. The slightest health deficiency, or even none at all, is sufficient to justify the killing of the vulnerable. The most threadbare claim to national security, or to the interests of a fictitious entity called global health—to which every university is scrambling to build a temple with pharma or world bank money—is justification enough for turning whole populations into experimental subjects. Even in Israel, of all places, Benjamin Netanyahu brags, in the name of medical progress, of having turned his country into a giant Pfizer laboratory; or rather, he speaks quite calmly of having done so, as if it were the obvious thing to do. Whatever would Hannah Arendt say of that?
An important milestone in the emergence of this culture, as Walker Percy observed in The Thanatos Syndrome, was marked by the 1920 contribution of Binding and Hoche, themselves men of medicine: Die Freigabe der Vernichtung Lebensunwerten Lebens, on permitting the destruction of life unworthy of life. But the beginnings go back further than that, to the Social Darwinists in the late nineteenth century and their eugenics movement.
Launched with lofty-sounding phrases by men of great accomplishment, including the polymath Sir Francis Galton, this movement from the outset showed itself to be mean-spirited, avaricious, power-hungry. Its first successful legal expression was the 1913 Mental Deficiency Act, which Josiah Wedgwood MP rightly fingered as the product of “the horrible Eugenic Society which is setting out to breed up the working class as though they were cattle.” Yet the bill passed with little opposition. Its most vocal opponent outside the House was G. K. Chesterton, who insisted that eugenics—that novel and exceptionally vague “science,” as Galton mislabeled it, which purported to deal with “all influences that improve the inborn qualities of a race”—was a deadly thing, “a thing no more to be bargained about than poisoning.” The Nazi era proved Chesterton right. Hence Nuremberg.
Yet we are still bargaining about it today. Enormous strides are being taken down the path marked out by Binding and Hoche. Euthanasia, we have discovered, can cure even the common cold—there’s no cure more effective!—and do wonders for budget deficits while freeing up hospital beds for those who still want them. But euthanasia is just one side of the eugenics programme. Read Robert Jay Lifton’s The Nazi Doctors, or Richard Weikart’s From Darwin to Hitler, then go back and read Chesterton’s Eugenics and Other Evils, beginning with his Note to the Reader.(If you’re short on time, you’ll find a condensed version in the second part of Anarchy from Above, but you really ought to read Chesterton for yourself.) A good many things in the daily newscasts will begin to sound eerily familiar. For we are indeed constructing a health tyranny, under which we will be told by public officials when we are sick and when we are well, or when we might become sick and how that must be prevented, and what must be sacrificed in order to prevent it. Soon, one suspects, we will be told whether we can be at all, how many of us there can be, and under what conditions. Already we are being told what we may and may not say about such things without being cancelled or prosecuted.
Canada’s Binding and Hoche, or is it Wither and Frost? Whoops—it’s the PM and his new JM in 2019. The latter is wearing his McGill tie. The pair quickly set about fulfilling an election promise to expand MAID legislation.
The defeat of Nazism never was a defeat of eugenics. It wasn’t even a setback, really, at least not in the national security community or among its cultured collaborators. Experiments in eugenics have continued unabated, with little effort to say what idea of the human, or whose idea of improvement, is operative. Consideration of such matters is undesirable, for several reasons.
First, because the whole movement is built, as Chesterton argues, on equivocation and artful euphemisms; that is how its humanitarian pretences are maintained. Second, because it won’t do, from a security point of view, to look too closely at either the means or the ends; those remain cabinet secrets or even secrets from the cabinet. Third, because we have become cynical, not only in the political but also in the philosophical sense. Too few expect to find answers to questions of moral substance; too many do not even enquire after them, lest they should learn that there are moral limits. Fourth, because any serious search for answers must take us into theological territory, and we don’t do theology any more. Or, rather, we like to keep our theology below the radar, like our anthropology. “What is man, that Thou are mindful of him?” is also a question no longer asked.
The improvement of humanity is a meaningless concept, however, where there is no standard by which to measure it. The military, for its part, prefers to speak of human enhancement or augmentation, and its measure is, as always, advantage over the enemy. Here there must be no limits, or at least none to which the enemy is not himself presently committed. So the masters of bio-defence and bio-offence have been augmenting the “augmentation” playbook with end runs around Nuremberg.
Now, it may be granted that the seventh article of the code requires some attenuation where the military is concerned. What must not be granted is that enhancement or augmentation is not subject to the code. Nor should we grant the underlying premises one detects in a recent Germano-British white paper:
What is certain is that the field of human augmentation has the potential to transform society, security and defence over the next thirty years. We must begin to understand the implications of these changes and shape them to our advantage now, before they are thrust upon us.
Something like the Dulles doctrine remains operative here: If they are doing it, or might do it, we also must do it—do it first, if possible, and more effectively. Which means that the military must provide leadership in the transformation of society; that “society, security, and defence” must be aligned, if not amalgamated.
To such a doctrine, and such a vision, Nuremberg is an unacceptable impediment. The Chinese model of military-civilian fusion will have to be emulated. That entails something more than a proliferation of public-private partnerships within a military-industrial complex. It entails the capture of minds through fifth generation warfare, and of bodies through genetic tinkering and implanted devices. With everything, as they say, to be done at scale.
Priming the Pump
Consider in that light this interview, from 17 December 2020, with Regina Dugan: “How DARPA seeded the ground for a rapid COVID-19 cure. Former Director of DARPA, Regina Dugan, joined Yahoo Finance Live to discuss this secretive government agency behind COVID-19 vaccines.”
Dugan had become CEO of Wellcome Leap in May of that year, after working with Google and Facebook in the interim. Two things are noteworthy, besides the trajectory of her career and the timing of the interview, which took place just as the mRNA roll-out began: first, that so much of what was going to happen was already known; second, that the questions, as well as the answers, were scripted to inoculate people’s minds against further disturbing developments by pre-establishing the idea that the “vaccines” were a world-altering miracle that it would be impious to question. Here is a major excerpt, lightly edited for clarity and interspersed with my own remarks…
YFL: We have seen the Pfizer rollout. We’ve also seen some of the concerns about … the myth about whether or not … it can alter your DNA, but then also some of the side effects. And so I wonder … based on what you’re seeing and based on your understanding of the technology … is this something we can expect? Is it normal to … go through this process of side effects, et cetera, with the vaccine?
DUGAN: I think that’s a normal progression in the investigation of safety for vaccines.
In truth, there’s nothing normal about this progression at all. Confidence that there will not be serious side-effects is supposed to be established from animal trial data beforeproducts reach the market. And if there are unforeseen side-effects that appear after marketing, the products are supposed to be pulled from the market. Here there were no animal trials, but the Pfizer testing on human subjects had revealed to the regulatory agencies, though not to the public, that an abundance of SAEs must be expected. It was determined in advance that these would be overlooked. But let’s continue with Dugan:
Now remember, our charge was to create the possibility [of a covid antidote], and I think we need to understand how remarkable an achievement this is. We went from virus sequence to first dosing in humans in 63 days. It’s unprecedented. Now, we still have the hard work to do to determine efficacy and to understand distribution and all of those things, but the first step is to have a vaccine candidate that creates an immune response and offers protection… This will be one of the most important scientific achievements of our generation and certainly in the top-five contributions for DARPA, which was also responsible for the early investments in the internet and GPS.
If the work establishing safety and efficacy has yet to be done, however, how can the “vaccine candidate” (which is not actually a vaccine) be headed to market with a “safe and effective” label? And how can she know that it will be successful, so successful as to rank right up there with the internet and GPS and the data mining they facilitate? Her interviewers do not enquire. Instead they simply endorse, then shift focus to the new alliance between business and government for warp-speed health interventions.
Absolutely! Regina, when we’re talking about … health care right now and the speed at which this was done, we know that this administration specifically focused a lot on public-private partnerships dealing with, not just the health-care companies, but also the tech companies for the rollout of software that will track some of these adverse events and the safety monitoring. You have been part of that world before and I just wonder: what is your sense of the ability for big tech to … walk into this health-care space that has been … technologically slow but also is so complex?
To put the question rather more sharply: Do they know what they’re doing? Can we trust them? Should health care be handed over to the military-industrial complex? It is true, by the way, that a great deal of money was laid out in advance, and still more after the fact, to track adverse events in products already declared safe and effective! What is not true is that this monitoring was allowed to call that declaration into question; there was too much at stake for that.
Listen to Dugan’s response, which addresses none of this but instead takes up the invitation to promote cooperative “health” interventions between the military and private corporations, despite the fact that the historic model for this is precisely the Fascist model to which Nuremberg was meant to be the remedy. “I firmly believe in public-private partnerships,” she states, offering up Moderna as an example.
When we made the investment in Moderna at DARPA, they were three people. And these early investments are important, and now we see what’s happened with the investment of private capital. We now also have to consider what other established tech companies might bring to the table in terms of their reach, in terms of their scale. These are very important considerations. But I think central to the question is also: What do we need by way of new breakthroughs? How do we ask the new “what if?” questions for public health and human health. And, in fact, it’s the reason I accepted the CEO role at Wellcome Leap, which was formed by the Wellcome Trust with an initial funding of $300 million and a specific mandate. And that is to ask the next “what if?” questions, to create the next round of breakthroughs for human health. We need to do those things at scale, and we need to do them in partnership.
I don’t know about the investment of private capital; it was BARDA that followed up DARPA’s original investment. Her interviewers invite her to take the next step, however, which involves parrying partisan attacks on the deep state while lauding its progressive agenda. Any concern about the deep state should be a concern, her questioners suggest, not with its agenda but with overcoming impediments to its agenda.
Regina, I love reading these stories because, to me, this is … like “Mission Impossible.” It’s kind of like what I thought was going to be happening if we were ever hit by a pandemic. And then it didn’t exactly go by the movie script, and a lot of that blame has been laid at the Trump administration, whether or not it’s what happened with the CDC or following [the] pandemic handbook…
Now there’s a classic case of taking Marx’s advice to charge your enemy with the very things you are doing while you are doing them! But let’s hear the question out. Can the progressives truly break free from the regressives?
What you’re talking about actually worked with DARPA. So are those “what if?” questions still being asked, because there’s a lot of concern about … the deep state and what’s been able to be taken down and what survived the last four years. Are you confident that the government and DARPA are still asking those questions and going to come up with the solutions for the next time this happens?
Before hearing Dugan’s response, let’s concede that what she’s talking about worked just fine, if “worked” means that the deep state survived the previous administration’s inept assault on it. In fact, it worked so well that the previous administration was almost completely taken in before it was taken out. And it will continue to work if government agencies and private organizations cooperate to achieve a new vision of health as global, rather than personal, and a corresponding moral vision that will back the requisite changes to decision-making in the sphere of health.
A quick aside: Have you noticed how sexual differentiation, which was always objective and universal, is now subjective and personal; while health, which once was subjective and personal, is now putatively objective and universal? To effect this reversal is one motive for the contradictory promotion of identity changes in the name of autonomy and of a needle in every arm in the name of the common good, autonomy be damned. Another motive is to disorient the public to such a degree that it can no longer tell what makes either for private or for public good; just as it can no longer tell what is private, and what is public, a conundrum well illustrated by Moderna. Anyway, Dugan again takes the cue, puffing both sides of the key PPP to which she is privy.
Well, I think DARPA is in steady state, and DARPA has historically had about 0.5% of the DoD budget. It’s an amazing organization with respect to the leverage it offers—small investment but right at these pivotal places where we need … risk-tolerant investments. But in health we also see private organizations like Wellcome Trust, like the Gates Foundation, others stepping up and beginning to ask those kinds of “what if?” questions as well. We definitely need to do that at scale. And I think it’s clear human health, global health, is going to require that of us. It is not only a moral investment. It is also an economic investment, as we’re seeing in this current pandemic.
Dugan tells us that DARPA “was formed after Sputnik in 1958 with the goal of preventing and creating strategic surprise.” She doesn’t tell us that Moderna, a failing company with no viable portfolio, was rescued by a total investment of one and a half billion dollars from DARPA and BARDA—that is, from Defence and the HHS—as a front for their mRNA ambitions. What, we may wonder, was to be prevented here and what strategic surprise was to be created? Was SARS-CoV-2 or some other “surprise” candidate already in the works when that front was created a decade ago?
A few months after this interview, the facts about the mRNA products—namely, that they were neither safe nor effective at stopping covid—were beginning to appear in public. Yet major media outlets, subsidized by government or big business, were still pumping the narrative, as most of them are today. Here’s another puff-piece, this one from The Economist on 3 June 2021:
Using messenger RNA to make vaccines was an unproven idea. But if it worked, the technique would revolutionise medicine, not least by providing protection against infectious diseases and biological weapons. So in 2013 America’s Defence Advanced Research Projects Agency (DARPA) gambled. It awarded a small, new firm called Moderna $25m to develop the idea. Eight years, and more than 175m doses later, Moderna’s COVID-19 vaccine sits alongside weather satellites, GPS, drones, stealth technology, voice interfaces, the personal computer and the internet on the list of innovations for which DARPA can claim at least partial credit. It is the agency that shaped the modern world, and this success has spurred imitators. In America there are ARPAs for homeland security, intelligence and energy, as well as the original defence one. President Joe Biden has asked Congress for $6.5bn to set up a health version, which will, the president vows, “end cancer as we know it”. His administration also has plans for another, to tackle climate change. Germany has recently established two such agencies: one civilian (the Federal Agency for Disruptive Innovation, or SPRIN-D) and another military (the Cybersecurity Innovation Agency). Japan’s interpretation is called Moonshot R&D. In Britain a bill for an Advanced Research and Invention Agency—often referred to as UK ARPA—is making its way through Parliament.
Here the sunny horizons are extended still further, with nary a cloud in the sky to dampen enthusiasm. Indeed, the sky is so clear that the merciless sun is just about our only remaining enemy. One notes the confidence placed in the new Administration, which will defeat the powers of heaven and earth, from global warming to cancer. (Everyone wants to see the end of cancer, right? That’s why we didn’t screen for it while we waited for mRNA products known to cause cancer, or cancer relapses.) A veritable ARPA blitzkrieg will effect these victories!
That, and a little tough love at home. Or perhaps we should say, a little kinky love, the kind that feeds a bureaucrat’s dominatrix fantasy, in which covid can be fought by chaining us to our beds or by deploying masks like condoms. Just think of it! All those compliant clergy sporting face condoms as they broadcast to their parishioners’ bedrooms and living rooms—no wonder Dr Fauci was laughing. But it’s no laughing matter. As Will Jones pointed out, there has been a cross-party lust for this sort of thing that goes back to the post-9/11 period. If we learned it from the CCP, we learned it well before covid.
Recently the role of CISA (Cybersecurity and Infrastructure Security Agency) in producing key lockdown guidance for America in March 2020 came to light. Now, a pandemic plan from 2007 produced by the National Infrastructure Advisory Council (NIAC) and currently hosted on the CISA website has emerged. The plan contains the original list of pandemic ‘essential businesses’ that was used by CISA in 2020 to lock down America. The 2007 plan (which was itself based on a Department of Homeland Security plan from the previous year) clearly states the intention to ban large gatherings ‘indefinitely’, close schools and non-essential businesses, institute work-from-home, and quarantine exposed and not just sick individuals. The aim is simple and clear: to slow the spread to wait for a vaccine.
Lock ’em down till you can shoot ’em up, in other words, as I said or tried to say two years ago. (The editor didn’t think anyone would laugh, or even keep reading, so he struck that line, which is no longer contentious.)
So, then: Defence, Health and Human Services, and Homeland Security were all involved in bringing us covid relief, though who brought us covid is still in dispute. And these public agencies, together with their private partners at home and abroad, were preparing for this long before covid hit. Sure, they ran into a bit of a snag with the Trump administration, but didn’t we all? They dealt with it, as with him, even if that meant enlisting their media partners to help keep Hunter Biden’s laptop sealed and performing a few other dirty tricks at election time—tricks the Twitter papers show to have extended right through the pandemic, with no sign of being shelved.
Well, you say, that’s their job, or a big part of it. Bio-defence, like bio-offence, if there’s a meaningful difference, requires anticipation and preparation. It also requires a few dirty tricks, no doubt, a little liberty with the law, though blatant interference with a presidential election is perhaps beyond the pale. The truth, however, is that nothing is beyond the pale. If it’s okay to do evil for a putatively good end—to obliterate civilian populations, or blast the brains of your patients, or cut up babies in the womb for their organs and cell lines, or promote suicide, turn hospices into killing fields—election interference is small potatoes. But if such things are okay, what isn’t okay? If such things are permitted, everything is permitted.
The Casualties of War
My colleague, Catherine Ferrier, reminds us that 10,000 Canadians died with “medical assistance” in 2021 alone. Another case, I guess, of “safe, legal, and rare.” And how far did pandemic management contribute to that morally hideous statistic?
That there was an utterly unprecedented response to covid everyone knows: lockstep media propaganda, complete with fear porn and censorship of anything off-narrative; repeated lockdowns, with the partial or complete cancellation of ordinary social and economic life; denial of rights and interference in religious practices, as in business practices; coercive vaccination mandates and other forms of violence, both psychological and physical, against dissenters, who are still being targeted; safe medical products banned for those who desperately needed them and unsafe medical products urged on those with absolutely no need of them; severe adverse reactions and deaths anticipated from the latter, but denied or ignored when they actually happened; doctors and scientists defamed, fined, or even de-licenced for questioning aloud what was happening, if (as too rarely) they had the courage to do so; public health officials, entirely unqualified for the task, ruling the smallest details of life; emergency powers routinely renewed week after week, year after year, without scrutiny or debate; constitutions and bills of rights suddenly shelved as if they had never existed; pastors jailed for preferring to obey God rather than man; every face hidden for months at a time, with nary a smile to be seen, even by children; no child left behind to enjoy the normalcy children need; infants and pregnant mothers injected with products said to be safe and effective, but known not to be.
What, again, was that first principle of Nuremberg? Something about “the voluntary consent of the human subject” being “absolutely essential” in human experimentation? Yes, which means that
the person involved should have legal capacity to give consent; should be so situated as to be able to exercise free power of choice, without the intervention of any element of force, fraud, deceit, duress, overreaching, or other ulterior form of constraint or coercion; and should have sufficient knowledge and comprehension of the elements of the subject matter involved as to enable him to make an understanding and enlightened decision. This latter element requires that before the acceptance of an affirmative decision by the experimental subject there should be made known to him the nature, duration, and purpose of the experiment; the method and means by which it is to be conducted; all inconveniences and hazards reasonably to be expected; and the effects upon his health or person which may possibly come from his participation in the experiment. The duty and responsibility for ascertaining the quality of the consent rests upon each individual who initiates, directs, or engages in the experiment. It is a personal duty and responsibility which may not be delegated to another with impunity.
How fares this principle today? Like Cameron at Ravenscrag, the pandemic management team on the Potomac, with the thoroughly unprincipled Fauci as its First Mate, though not perhaps at its helm, rolled out a deliberately disorienting combination of therapies to test on unsuspecting subjects: sensory deprivation (masking and lockdowns), sensory overload (incessant media messaging, like Cameron’s looped tapes), potentially fatal products and procedures (from midazolam to ventilators, from remdesivir to the clot-shots), and repeated violent shocks to the collective and the individual psyche. All the while, it told lies too large to question, accompanied by promises it had no intention of keeping. It wounded; it demoralized; it punished. It killed and is still killing, if the excess death toll is the signal some think it is. It violated virtually every note of Nuremberg. That Fauci himself is said to be quadruple-jabbed does not change any of that, though it does call into question his sanity.
Those of us who have lived through previous pandemics, such as the Hong Kong flu, or anyone who took the least trouble to discover what was evident from the very beginning—that covid kills only the very old and frail or the heavily compromised—knew or should have known that the supposed cures were worse than the disease by far. The general readiness to be deceived, or to become collaborators in the deception, displayed the hollowness of our souls, so easily filled with fear; of mainstream religion, which offered no antidote to fear; and of our political life, which simply collapsed. It revealed the sham culture of the universities, which likewise put up little resistance, proving themselves haunts of hopelessly naïve students, cowardly professors, and corrupt administrators who simply went with the flow, paying down their debts to pharma-tech and other partners, including China. And what shall we say of the medical profession? Primum non nocere, if it still means anything at all, means: “Do no harm to yourself. Keep your head down. What we have called safe and effective, you must call safe and effective. Woe to you if you won’t.” Few there were, alas, who rejected that counsel.
Let’s come back to McGill for a moment, where that counsel was embraced without hesitation.
Last July, I put some initial access-to-information questions to my university about the work of the bodies charged by the P7 (our top management team) with handling pandemic affairs, the Emergency Operations Centre and the Recovery and Operations Resumption Committee. Here are those questions:
What was said in these committees about the possibility or actuality of serious adverse reactions or vaccine injury (fatal or otherwise) among those who were being encouraged to take the shots?
What was said about (a) the emerging relationship between McGill and Moderna and (b) other possible conflicts of interest generated by financial relationships with donors or partners to the university or members of the university?
What reasons were provided for adopting masking, distancing, and proof of vaccination policies stricter than those required by the government of Quebec?
As far as I can tell from the documents received, the answer to the first two questions is nothing at all. The answer to the third is none. So we must, unless we probe the P7 itself, be content with McGill’s public announcements.
As recently as 14 January 2022, the EOC was still claiming that “three doses of vaccine prevent upwards of 70% of transmission.” This was false, as was its claim a month earlier that “masking is more important than ever” and that “masks have been working at McGill to prevent the spread of the virus.” There was not a shred of evidence for the latter claim, nor has anything emerged to collapse the mountain of data showing that masking is ineffective against airborne viruses. As for the former, the following justification was offered on 18 January 2022:
Analyses from Britain give a vaccine effectiveness against Omicron of about 70-75% for people having three doses of vaccine and about 88% vaccine effectiveness against hospitalization for Omicron.(See the December 10, 2021 Technical Briefing and December 31, 2021 Technical Briefing from the U.K. Health Security Agency, for example.) This figure of 88% for vaccine effectiveness against hospitalizations means that the number of hospitalizations in vaccinated people will be only 12% of the number in the unvaccinated group.
We can’t hold institutions—or doctors for that matter, but the people advising us to “vaccinate, vaccinate, vaccinate” are not doctors and have no business disseminating such advice, much less introducing sanctions against those who won’t follow it—responsible for things that were not known to them at the time, things such as the hugely increased risk, from the jabs, both of infection and of hospitalization. Mounting evidence for that has shown claims about “a pandemic of the unvaccinated” to be nothing more than official disinformation deflecting attention from policies that were themselves undermining hospitals and health care, and will continue to undermine them for the foreseeable future. We can, however, hold institutions like McGill accountable for tendentious treatment of such evidence as they had. On page ten of the second Technical Briefing linked in that McGill memo, we find this:
In all periods, effectiveness was lower for Omicron compared to Delta. Among those who had received two doses of AstraZeneca, there was no effect against Omicron from twenty weeks after the second dose. Among those who had received two doses of Pfizer or Moderna effectiveness dropped from around 65–70% down to around 10%… Two to four weeks after a booster dose vaccine, effectiveness ranged from around 65–75%, dropping to 55–70% at five to nine weeks and 40–50% from ten+ weeks after the booster.
Details, details! To which we might add another, namely, that the “unvaccinated” category includes those who have been “vaccinated” for two weeks—two weeks in which there is an uncommonly high rate of infection. This was a common dodge for skewing statistics in favour of the vacina salva narrative, as some of us had already observed.
Anyway, a couple of months later McGill finally dropped, without fanfare, the claim that injections prevented infection and transmission. On 25 March 2022, we were told that “the focus is now on preventing serious illness and hospitalisations through vaccination and new treatments for COVID, rather than on restrictions and lockdowns that try to prevent any new cases.” So those who had been claiming scientific support for one objective—mass vaccination to prevent infection and transmission—now shifted to another: mass vaccination to prevent serious illness requiring hospitalization.
The second is as false as the first, but they had to make some sort of shift, not only because it had become too difficult to hide or distort the scientific evidence but also because the failure to prevent infection and transmission was perfectly obvious to the ordinary person. What did not change was the underlying goal, mass vaccination itself. And McGill was already working with Moderna (that is, with DARPA and BARDA) on a deal to make these “new treatments” a staple both in its financial diet and in our idea of heath care. The U.K. has just concluded a similar deal, on a larger scale, promising to become “a life sciences superpower.”
It turns out that the mRNA products had never even been tested for prevention of infection or reduction of transmission. They are non-sterilizing and do not even reduce the viral load significantly. So all those claims about keeping people safe by preventing transmission were nothing more than lies. Not only were they lies, but they were lies used to attack those who knew or suspected they were lies and to dupe people into taking products they did not need and might well injure them or compromise their immune systems.
None of this has McGill yet admitted. No word of apology has been issued. Has it, then, utterly abandoned its vocation as a place for independent scientific research and critical analysis to become an arm of the military-industrial complex? Has it again been conscripted into America’s war? Has it no institutional conscience, nor any memory of past violations of conscience?
McGill, I learned, resisted certain excesses urged on it by its own School of Population and Global Health, headed by Professor Evans, a man with deep roots in the requisite pieties. But there is no more excuse for nothing, nothing, none than for a zero-covid or zero-carbon policy. It is a betrayal of trust that requires independent investigation into its causes and consequences. There are real victims here, as there were at Ravenscrag, even if some do not yet know they are victims or do not regard themselves as victims.
Who has deceived us?
Returning to the larger theatre, to the world stage, we must ask a much more important question: Who or what has the power to turn the minds of men, or the spines of men, to mush, operating simultaneously in so many different spheres, professions, and institutions? Who can generate a deluding influence with such reach, and to so thorough an effect? Who, indeed, but the Father of Lies, who—to judge from the state of the church as well as the world—is already out on parole. I’ll try to explain that another time. We’ll stick here with those of our own kind.
Many candidates have been put forward: the main shareholders of big corporations, especially in pharma-tech sectors, which have so hugely profited; the Davos imperialists (are they capitalists or communists or fascists? perhaps the difference is now academic) who spawned the public-private partnerships of which they are so proud; the global governance advocates, who find nation-states inconvenient; the Malthusians, who find people in general inconvenient, or the transhumanists, who think them outmoded; the CCP, which wants to eradicate freedom in the West, and kindly shared with us both the virus and a tyrannical model for response to the virus. Or was it we who shared the virus with them, capitalizing on the opportunity to import that model? That hypothesis, at present, is as good as any.
That there are multiple agents with overlapping agendas goes without saying, but which is the master agenda and what is its primary nature? Some say it is financial, as if the pandemic were only a smokescreen to hide the true causes of an impending economic collapse. Others say it is technocratic, preparation for a global coup by elites that have decided against democracy and for a managerial model of governance. Still others that it is bellicose, all part of the old cold war with Russia—now hot again in Ukraine—and the new cold war with China, which some even suppose to be the final war. A few think it precautionary, as if the covid crisis has only been pandemic war-gaming, this time with live biological rounds, in preparation for something more serious. But many, understandably suspicious of theories about master agendas and super culprits, think it undesigned, a perfect storm brewed by chance out of a lab accident, international groupthink, an increasingly rootless and insecure population susceptible to authoritarian measures, and the predictable heavy-handedness of panicked authorities responding to a crisis.
These theories are not, for the most part, mutually exclusive, when not construed in reductionist terms, but let’s push back against each in turn. The first has this against it: that there must surely be easier ways, and ways hopeful of better outcomes, if a full rebuild of the world economy is required; there are certainly less wicked ways. The second goes much further, in my opinion, towards a satisfactory account of the orchestrated chaos of the pandemic; what it has difficulty explaining, as does the first, is the sudden evaporation, not everywhere but in so many places, of those national interests that would normally cause saner heads to prevail. (Can the alleged coup really have progressed quite so far? Perhaps it can, and has.) The third, which rests on conflicting national interests between the two super-powers, begs questions about cooperation between them in gain-of-function research, pandemic planning, and pandemic measures. The fourth, despite deep roots running back into the Bush administrations, seems weak; for pandemic war-gaming with live ammunition makes no sense if it exhausts the public purse, produces high casualties, destroys morale, and undermines the very nation it is supposed to protect. The fifth, though it can be supported by appeal to the stupidity factor, indeed to the widespread insanity of our times, is falsified by the many signs of forethought we have been noticing.
While it may be comforting to rule out any truly malicious design, apart from the familiar pharma monkey business, what are the facts? There have been decades of pandemic war games, culminating in Crimson Contagion (run by Robert Kadlec, bio-defence insider and ASPR director from 2017–2021) and in Event 201, both of which took place just before the real action began. There have been games played with the very word “pandemic,” and prior attempts to produce a pandemic. There has been wholesale resort to NPIs that run completely contrary to conventional wisdom, whose one real achievement was to advance prior plans to introduce health passports, digital IDs, CBDCs, and other instruments of surveillance and control. Elaborate funding has been provided over many years for projects faithful to the Gavi/CEPI ambition to make frequent vaccination a universal norm. There has been patient and thorough regulatory capture and infiltration of professional associations, to say nothing of the journals on which they rely. The very inefficiency, indeed irrationality, of covid defences, taken in concert with the ruthless efficiency of authoritarian measures, militates against any perfect storm scenario from which human design has been excluded. So do the secret contracts with Pfizer, which were made not only with Israel but around the globe; the prompt deployment of false modeling, psy-ops, and 5GW; the constantly moving targets of public policy coordinated across multiple countries; the data collection, data withholding, and data manipulation; the gross violations of medical ethics and all those other matters mentioned earlier.
When these things are taken into account, it seems more reasonable to postulate a storm designed and produced with a view to changing the conditions under which we all live and to alter the patterns of our behaviour. And for the source of that we must look to one or more of the first three proposals: the financial, the technocratic, and the bellicose. My money is on all three, working in concert, which puts the third in a different light.
War on the People
To see intent and design where there is none may be a sign of paranoia; refusal to see intent and design, where it manifests itself, is a sign of willful blindness. Just as individual components of Cameron’s experiments in mind control might, under other circumstances, be given a more or less innocent interpretation, while their appearance in concert under the actual circumstances cannot be, so also here. One can argue till the cows come home (if the climate change fear-mongers will let them come home) about individual aspects of the crisis, pointing to this or that quite ordinary explanation for the phenomenon in question, but that would be to lose sight of the herd for the cows. Let’s not deceive ourselves. Lockdowns, masking, and coercive mandates are not health measures. They are de-patterning and re-patterning devices. Since only governments have the power to impose them, and since only the Americans and the Chinese have the reach that allows them to be imposed across multiple jurisdictions, and since China cannot impose them on America, it seems to me that we cannot answer the question about design and control without speaking of America’s war—not its hot war against Russia or its cold war with China, but its war against its own citizens and the peoples of the West.
Now, when I say America, I mean deep-state America, led by the intelligence community and its private partners—”business and government,” as they like to say at Davos, working together in harmonious fashion for the benefit of both. This is certainly not everyone’s America! Increasingly, it comprises those who despise the people and have grown impatient with their unreadiness to become, in Lewis’s phrase, willing slaves of the welfare state. Hence the covid exercise, which serves the dual purpose of setting China on its heels while breaking down the opposition at home. The latter function makes feasible a pivot to climate change and population reduction, a sacrifice pleasing unto Gaia, while serving the goal of political control. For it sets the governance-by-emergency-powers precedent that climate fear-mongering, by itself, could not have achieved. It does an end run around democracy and, as far as possible, the constitution.
Remember Ludlow? The late John D. Rockefeller Jr, friend of Mackenzie King and founding father of just about everything, from the Bureau of Social Hygiene to the Council on Foreign Relations to the Rockefeller Foundation; and Peter Schwartz, the futurist who has worked with just about everyone, including the said Foundation.
How far all this was anticipated by those responsible for given sectors of the pandemic war theatre is difficult to say, but Peter Schwartz—an MKUltra associate at Stanford in the seventies, and the scenario man par excellence—seems to have anticipated it, in broad outline, even before authoring big philanthropy’s detailed self-indictment: the Rockefeller Foundation’s Scenario for the Future of Technology and International Development. (This 2010 document contains the notorious Lockstep section, though that is not its most interesting feature.) Schwartz, who had earlier written on sudden climate-change emergencies, is said to have taken an interest in government-sponsored research into social control through the weakening of family and tribal loyalties. (If so, I hope he later enjoyed Nation of Bastardsand “The Audacity of the State.”) He also partnered with Kadlec in key pandemic planning exercises.
To be honest, it’s hard to keep track of all this public-private partnering, which seems to be quite promiscuous and its conquests to be a cause of considerable friction. But just here we must press a question. In the dance, are representatives of nation-states to lead or are they to follow? Another Rockefeller production, this one from the 2013 Global Health Summit in Beijing, suggests that they are to follow: “The power of states and their ability to provide an effective nexus between the local and global levels may diminish in the face of growing megacities, local identity politics, increasing social exclusion, increasing private influence on all spheres of life, widening liberalisation and stronger global networks.” (In such contexts, “may” often means “we’re trying our best.”)
That diminishment is foreseen for America, too, but America must meanwhile play a leading role in the creation of world governance, as John D. Rockefeller Jr himself did. Whatever is to emerge at the head of a new world order—I call her Shelob, and doubt not that she already exists embryonically—will do so by way of a web that cannot be spun without America’s assistance. The web itself is woven from industry and philanthropy; or, more truly spoken, from seduction and insecurity, from desire and fear. These have been made to converge, ironically, in health. Dreaming the Future of Health for the Next 100 Years provides a blueprint for the idolization of “health” the world over, and this new loyalty, though at first state-based, will soon lift the burden of national loyalties. The current treaty proposal, transferring various powers from member states to the WHO, belongs to that process.
A word of advice: Do not call liberalization everything philanthropists call liberalization, and do not call health what they call health. The whole dream is a dream of conquest, a dream of a web well stocked with the world’s flies. In the biblical metaphor, it is a dream of Babel. But it does need the American deep state in order to get off the ground, and the American deep state needs it, for two reasons—to retain its hold on power at home and to make certain that competitors abroad, especially in Beijing, are not embedded at a more fundamental level.
Ah, but wait! The dreaming is all very innocent. Surely there’s no shame in having a sharp eye for promising developments, or for potential hazards, along the trajectory of human progress. The keenness of that eye should not be held against it, nor read conspiratorially, as the Rockefeller reminded us in 2020, during the thick of the pandemic:
In the 1930s, Warren Weaver, who led The Rockefeller Foundation’s programs in natural sciences, had a hunch that chemical and physical explanations of life would lead to a whole new world of research and discovery. He coined the term “molecular biology” and a field was born. In 1956, The Rockefeller Foundation supported the Dartmouth Summer Research Project on Artificial Intelligence, which was the first use of “artificial intelligence” as well. After some fits and starts, that field exploded too. And now, artificial intelligence has combined with molecular biology to accelerate the development of vaccines and therapeutics for the world’s worst pandemic since 1918. Could any of this have been predicted? Absolutely not. However, both molecular biology and artificial intelligence were guided by visions of positive futures where both fields contributed to improving people’s well-being. Unfortunately, we must also plan for futures that aren’t as bright—be it due to a disease outbreak or natural disaster—to minimize harm and prepare for recovery.
The comparison with 1918 should not go unremarked; that very construal is conspiratorial. Neither should the claim that the 2010 Scenario was simply a bit of what if? speculation that proved prescient. “Now that we’re well into a real pandemic,” the authors concede, we do “see some chilling similarities between our current Zoom-centered world and Lockstep.” We see, for example, that it accurately “predicted that telepresence technologies would ‘respond to the demand for less-expensive, lower bandwidth, sophisticated communications systems for populations whose travel is restricted.'” Other predictions, we are told, were off target, “including the emergence of MRI technologies to detect abnormal behavior with anti-social intent.” As if variations in the technology of choice somehow put to rest the idea that anything was engineered in advance! Oh, and try turning those two sentences around, beginning the one with travel restrictions and the other with detection of anti-social behaviour. You will find that both read rather more chillingly, particularly if you concur that such measures were themselves decidedly anti-social.
Only a fool would suppose that the reality was unconnected to the dreaming. The surveillance technology may change, but the plan to apply the Bush doctrine of pre-emptive strikes, both at home and abroad, remains the same. Those chilling similarities are the new normal by which the abnormal is being calculated, just as our innocent dreamers predicted. Their 2010 map of the alternatives, in which Clever Together is the clear winner, is quite compelling evidence of that. Clever Together, of course, is for clever people. Ordinary folk require the discipline of Lock Step before they can learn to be clever. As for those who mistakenly fancy themselves clever, their Smart Scramble has been anticipated. It will not go so smoothly as they like to think.
The Rockefeller Foundation does not wish to be misunderstood, mind you. It never has anything but our best interests at heart, as the 2020 document insists. “While baseless posts have circulated recently calling the exercise part of a ‘diabolical plan for world domination’, we see it as further evidence of the importance of scenario planning in helping governments, institutions and others navigate near-term decisions that can have long-term impact. Our hope then—as it is now—was to focus on what we don’t know so we could make better plans to address a real pandemic, such as the one we’re facing today.” Not war, then, just philanthropy. It’s all in how you look at it.
Philanthropy? Remember that the Serpent was the original philanthropist! All he wanted to do was help humanity learn to deify itself. And he did know something about the process. How had he had become the Serpent if not by dreaming the process and himself attempting the process? But if we are going back only to the 1930s, rather than to the year naught—if it really is those “chemical and physical explanations of life,” not some putative Serpent, that suggested new ways of regarding and treating life—what then? Giorgio Agamben can explain. He makes a much more reliable guide here, whether to the 1930s or to the present day, than does the Rockefeller Foundation.
Every time a value is ascertained, a non-value is, necessarily, established: the flip side of protecting health is excluding and eliminating everything that can give rise to disease. We should reflect carefully on the fact that the first case of legislation by means of which a state programmatically assumed for itself the care of its citizens’ health was Nazi eugenics. Soon after his rise to power in July 1933, Hitler promulgated a law for the protection of the German people from hereditary diseases. This led to the creation of special hereditary health courts (Erbgesundheitsgerichte) that decreed the forced sterilisation of 400,000 people. Less well known is that, long before Nazism, a eugenic politics was planned in the United States—particularly in California—with robust funding from the Carnegie Institute and the Rockefeller Foundation, and that Hitler explicitly referenced this model. If health becomes the object of a state politics transformed into bio-politics, then it ceases to concern itself first and foremost with the agency of each individual and becomes, instead, an obligation which must at any cost, no matter how high, be fulfilled.
Agamben knows what Chesterton and Lewis knew. Therefore he, too, dreads government in the name of science and especially in the name of health. He does not want us to make the mistake of thinking that law and life, or law and medicine, can be conflated with impunity, as the Planners intend.
Medicine has the task of addressing ailments according to the principles irrevocably sanctioned by the Hippocratic Oath, principles which it has followed for centuries. If medicine, making a necessarily ambiguous and indeterminate pact with governments, presents itself instead as a legislator, not only does this not lead to positive results in the field of health—as we have witnessed in Italy during the pandemic—but it can result in unacceptable limitations on individual freedom. It should be evident to everybody that the medical reasons behind these limitations could offer the ideal pretext for an unprecedented control over social life.
It should indeed be evident! One further caution, however, before leaving this section. Artificial intelligence is much touted in medicine today, especially by those waging war on the people through their Global Health cult. But just as there is no such thing as global health, there is no such thing as artificial intelligence, nor ever will be. There are only very powerful computers in the service of very powerful men, most of whom are less clever than they imagine and some of whom are more wicked than we imagine. Whether speaking to us of health or of things other than health—a shrinking category—they say that we have crossed the Rubicon, that we have no choice now but to move forward into territory shaped and governed by algorithms. What they do not tell us is that their struggle for dominance within that territory is a struggle that can only mean total war.
Total war requires massive data mining and data manipulation. It requires the biosecurity state that Aaron Kheriaty has so helpfully described for us, within which we all become little more than data-points. This requires in turn public-private partnerships of a monopolistic nature, capable of enforcing the will of these same men. Identity by numbers, and governance by algorithms, is the end of freedom—its terminus, notits telos—as many are beginning to recognize. Pragmatically speaking, the war against the people, and the war of the people, will be won or lost just there.
Recapitulation and Rejoinder
As I was bringing this essay to its conclusion, in draft form, I come across a piece, published on Christmas day, proposing that the pandemic “was the result of an American biowarfare attack against China (and Iran)” and that this had been covered up through a conspiracy on the scale of the Kennedy killings. Ron Unz, it turns out, has been arguing this line since April 2020; how I managed to overlook it for so long, I don’t know. Anyway, it will be clear by now that I do not think we are dealing merely or primarily with an attempt to cover up a backfiring bioweapon. That theory, like the perfect storm theory, leaves far too much out of account. Measures that advance big government and big business but don’t actually mitigate viral and “vaccine” damage—that indeed risk its exponential expansion—suggest a plan of greater proportions and of earlier origins. So let me recapitulate and try to bring all this into focus.
We know that the kind of men we are dealing with have set themselves above the law, and that they have resorted to repeated shock waves in order to break down opposition and achieve compliance. The covid war we have been in, the climate change war we are entering, the data war to which these phoney wars are connected, are backed, like the war in Ukraine, by an elite in places of real institutional and financial power, centred where it has always been centred, in the bowels of the beast where Allen Dulles once dwelt, whence also the World Economic Forum emerged.
This elite is not afraid to experiment on the people, biologically and psychologically, or even to disrupt the supply chains on which they depend. It means, by way of its experiments, to induce cultural amnesia and to re-program the collective memory for purposes of its own. The casualties do not much concern it. Nor do those men and women who belong to it, or cooperate with it, ponder the fact that they have created a culture of lies and deceit from which they themselves can never hope to escape.
Those whose consciences are not yet completely seared must tell themselves, as Dulles doubtless did, that it is all necessary for the common good. But that too is a lie. They are not serving the common good. They are not even serving national or international interests. They are serving themselves. Ultimately, they are serving a diabolical agenda to subjugate the human race, to reduce it to manageable numbers, to possess and manipulate it like any other product.
And who are they exactly? Some are well known, others unknown, even perhaps to each other. One could be a bishop of the Church of Rome and belong to them, or a president of the Club of Rome and not belong. One could be planning smart cities, the better to serve humanity, without understanding that the real purpose of smart cities is to regiment humanity. But those who do belong, who really belong, are building an anti-city, a city implacably opposed to the city being built by God. They do not wish the numbers of the latter to be filled up, or the design of its Architect to be realized. They are committed, if necessary, to the slaughter of the innocents and to planned parenthood. They are Malthusians, Masons, Modernists. They are eugenicists and transhumanists and ESG enthusiasts. They are the rich, the clever, and the quite mad, though there is method in their madness. They are the self-proclaimed saviours of the world, and its judges too. They are not only the new communist capitalists and capitalist communists, they are the new catholics.
But we old catholics who celebrate Christmas, and the feast of the Holy Family, know that the Architect’s design will be fulfilled. Neither man nor devil can prevent it. We are determined to live by its laws and principles, not by theirs. We will resist them, sometimes with their own technology and sometimes by refusing to deploy it. But we will not take up their habits or tools of manipulation, seeking to best them at their own immoral game. We will take up weapons of righteousness in the right hand and in the left. We will speak the truth, which is far more effective than being pragmatic. Indeed, it is far more practical than being pragmatic. We will tell of the city whose builder and maker is God, and rejoice at its prospect. For God has already intervened to save the people. He has already established the Man by whom he will judge the nations. America’s war is in vain.
“The Lord wins in the end,” as Benedict XVI reminded us in 2017. And that, I think, is a good note on which to enter Anno Domini 2023.
RESEARCHERS at Boston University have developed a deadly new strain of Covid, which kills 80 per cent of animal subjects. The research was funded by the US government and approved by Anthony Fauci. I don’t need to tell you how risky such experiments are, or how stupid. This is just one biotechnology experiment among thousands currently being carried out around the world which pose similar kinds of threat. Each additional experiment adds to the danger and brings another lab escape a bit closer.
Biotechnology and medical science is already a long way down a well-worn path which leads to the normalisation of risk. This has involved gradual acclimatisation to high rates of severe injury and death imposed on an unwitting public. The psychology of this process is well known. Repeatedly turning a blind eye to suffering coarsens individual attitudes.
A past true-crime Forensic Files episode illustrates how far we have come. A young female doctor died unexpectedly of a heart attack. In those pre-pandemic times sudden death was a red flag necessitating the close attention of pathologists and police. In the episode, the presence of an unusual toxin was found and the culprit apprehended. By contrast, in the post-pandemic world sudden death has been normalised. No investigation required. Legislation is being changed to allow ‘cause unknown’ on death certificates.
High rates of excess all-cause death, pregnancy irregularities, cardiac events, cancers at lower ages and low birth rates have not just failed to raise eyebrows, but have been dismissed by ‘experts’ and MSM alike on flimsy pretexts without adequate investigation. Blaming Covid infection for every increase in illness has become the norm. This indicates detachment from sound science and the rational mind. Questions are off the table.
Last week New Zealand’s top vaccinologist Dr Helen Petousis-Harris sounded a public note of alarm, saying she wasn’t having any more boosters and advising the public to follow her example. Her advice was based on evolving scientific findings. This was a step too far for the MSM. The NZ Herald decided to switch experts, stoke the fear factor and cancel Dr Petousis-Harris.
The Herald quoted a University of Auckland computational biologist David Welch, who is not an expert on vaccines but begged to differ from Petousis-Harris saying: ‘I think we should be regularly having boosters. At the moment a booster twice a year looks like it would be very sensible because we’re getting waves more frequently than that.’ The long article failed to mention adverse effects of mRNA vaccination and its near-total lack of effectiveness.
Such buffoonery is not just uninformed, it increasingly appears to be part of a deliberate attempt to whitewash medical harm on a scale that dwarfs any previous example. An article in the Epoch Times headed ‘How Cancer Deaths From the COVID Jabs Are Being Hidden’ outlines just one way this is being accomplished, saying:
Analysis of US Morbidity and Mortality Weekly Report (MMWR) data suggests that some cancer deaths have been redesignated as Covid deaths since April 2021. This has hidden the cancer signal.
Before it was manipulated to eliminate the safety signal, data from the Defense Medical Epidemiology Database (DMED) showed cancer rates among military personnel and their families tripled after the rollout of the shots
After the rollout of the Covid jabs in 2021, cancer patients have got younger, with the largest increase occurring among 30-to-50-year-olds. Tumour sizes are dramatically larger, multiple tumours in multiple organs are becoming more common, and recurrence and metastasis are increasing.
Why is this not front-page news? The controlling conservative elements of the medical profession and the profitable pharmaceutical industry consider vaccine adverse effects to be a sort of unspeakable heresy. Yet ask someone who has been working in the gene therapy field for years and a tsunami of cancers is not unexpected.
Look at it this way. Cancers result from mutated genetic instructions. These can result from a number of causes including oxidative stress, inherited weakness, environmental or ingested toxins. Inside every one of trillions of human cells every day microbiological immune processes make 70,000 DNA repairs. These ward off potential cancers.
These internal cellular immune processes are sealed off and protected behind the cell wall. The mRNA vaccines are Trojan horses designed to breach the cell wall and reprogram cellular activity. It doesn’t take a genius to appreciate that there are risks involved. These risks include cancers. Cancers normally take years to develop. The surge in cancers among US Department of Defense personnel should be a red flag. Instead medical administrators are apparently busy burying it.
In New Zealand the burying has involved withholding data from public scrutiny, making misleading comparisons, cancelling those asking questions, saturation government advertising promising safety, and indiscriminate use of the ‘conspiracy theory’ label. We have written about these for a year now. Given recent Covid scientific publishing, we are all hoping that the penny will drop. Perhaps those awake enough to study journal papers carefully will, like Dr Petousis-Harris, begin to realise that there is no point in endangering their own health for the sake of a biotechnology dream.
Even though we are approaching the end game of one mRNA biotech dream, there are thousands of others in the pipeline. The psychology of biotech dreaming allows proponents to segue effortlessly from one dream segment to another without a pause. As long as you believe in the ultimate good of human genetic manipulation, there is no real worry if a few people die along the way.
As things have progressed from a few dying, to thousands, to hundreds of thousands around the world and millions injured, coarsened attitudes have hardened. The progress of biotechnology has gradually come to be regarded by the medical elite and giant commercial interests as ‘a necessary task’. A task that requires toughness and determination to arrive eventually at a ‘laudable’ and inevitable goal. The echoes from history are obvious.
But what if the whole enterprise of biotechnology is misguided? Like the discovery of the atomic bomb, literally a dead end? Where the next available step is only a bigger bomb or a more invasive and deadly toxin or pathogen? There are good reasons to suppose this is the case. Millions of years of evolutionary interaction with the wider global epigenetic bionetwork, underpinned by the immutable laws of physics, just might be more reliable than the ideas of a mad scientist.
Is the complexity of human physiology beyond human comprehension and calculation? Yes. Our knowledge of it remains primitive. Moreover there are inherent limitations to our understanding. The full intricacies of in vivo genetic processes are not open to scrutiny. The computational solution of genetic processes and intercellular interactions is beyond the reach of even the most powerful supercomputers. Combinative processes between genes performing multiple tasks requires multidimensional mathematics involving unsolvable equations. Adverse effects of gene editing are known to be inevitable and incalculable.
Governments have poured billions of dollars into biotechnology training and research programmes. The false rationale for this has been created by vast public relations efforts funded by a great variety of global commercial interests. It has all the hallmarks of a Ponzi scheme or an unsustainable investment bubble. There are no beneficial or bankable outcomes appearing at the end of the pipeline. More alarmingly, the deficits in human health are taking their toll and making their presence felt.
Scientific American reported this week that ‘the U.S. Just Lost 26 Years’ Worth of Progress on Life Expectancy’. How low are our medical czars prepared to go before admitting that something is rotten in the state of Denmark? The ‘it’s not me’ and ‘look the other way’ cultures are in full flood to protect the mRNA PR mirage. Against all scientific logic and evidence, biotech CEOs, paid scientists and government experts, floundering politicians and funded media are still talking up the wondrously protective achievements of pandemic responses as if they have saved the public rather than endangered them, from the Wuhan lab to the Covid jab.
It is time to ask some serious questions. The truth is that we are not just in danger of losing progress on life expectancy, but also four centuries of progress with scientific method.
We can’t escape the fact that commercial biotechnology involves an incredibly risky and inherently mutagenic worldwide programme of experimentation. This requires a proportionate response with a global reach. For this reason and many others, this Sunday the Hatchard Report will be launching a Campaign for Global Legislation Outlawing Biotechnology Experimentation known as GLOBE. Watch this space for more details and visit my webinar with Voices For Freedom for the launch.
SOTT Editors: We are publishing below, with permission, an email from a top executive at an American company whose clients include 100 of the Fortune 500 companies. The email was sent in reply to another executive asking for the writer’s thoughts on whether he plans to be vaccinated himself or mandate it for his employees as a requirement for returning to the office. All names and company references have been redacted for privacy reasons.
Unlike most of us who are worried about being on the receiving end of vaccine mandates by employers, this executive also has to worry about pressure from other executives and investors to mandate it on others. Few such business leaders are actively fighting for the rights, dignity, peace, and financial security of their employees. This exec is currently the only voice in his company opposing the madness.
Email to the executive:
Hey [REDACTED] – are you giving any thoughts to getting vaccinated with all this Delta variant stuff going on? We’ve been having management committee discussions here about mandatory vaccinations to be able to come in to the office. We have office support people coming in most days that are not vaccinated and some of those with kids don’t want to come in when they are in the office or invite clients into the office for meetings. Just curious as to how you are approaching it. Thx, [REDACTED]
The executive’s reply:
From: [REDACTED]
Date: Fri, Aug 27, 2021 at 9:56 PM
Subject: MY POV on Mandating Employee Vaccinations
To: [REDACTED]
I appreciate you reaching out. What follows is admittedly lengthy (though I do provide my “summary POV” a couple paragraphs down before I dive into supporting detail). I tried to be succinct, but practically speaking your question for me was akin to “hey, so what’s your take on management?” The analogy here being I’m passionate about both subjects so it was hard to choose between sending back a brief 2-minute POV, or filling this email with enough content fit for a university level course. I didn’t know what you had an appetite for, so I just simply did my best to try and be helpful (and heck, even had some fun while I was at it…).
My framework for this entire POV: in the famous words of W. Edwards Deming, “In God we trust. All others must bring data.” As I hope you’ve come to know me by now, I care more deeply about facts & morals than I do ideology or identity politics (for the latter I just don’t give a shit). If you give me a good reason to do something, I am 100% all over it. But if you give me either faulty reasoning or an unethical ultimatum, I simply cannot get on board out of a moral obligation to do what’s right.
So to answer your questions with that sole framework in mind, here’s my summary POV:
(#1) I still have no plans to get vaccinated anytime in the foreseeable future (unless something radically changes the risk equation), given:
(a) The virus at present poses de minimis risk for me personally (and virtually zero risk to any healthy child (a reference to your initial inquiry)); and
(b) Because these vaccines carry –> confirmed low/moderate short term — inferred moderate medium term — and expected high long-term health risk for what could be [though yet unknown] a majority of individuals who get the jab
(#2) I remain vehemently opposed to vaccine mandates for this specific virus (primarily on the basis of (i) 1b above, (ii) the medical literature, which strongly suggests that these vaccines will prolong this pandemic indefinitely through never-ending variants, and thus/therefore (iii) on moral grounds, as, if (i) and (ii) are true, then any decision to proceed with mandates would be nothing short of a descent by the West towards fascism**, the likes of which hasn’t reared its ugly head since the early 20th century. Finally, at a distant, distant second, I am against these mandates from a logistical perspective*.
*E.g., how will you account for boosters (i.e., will those who were vaccinated too far in the past e.g., January and thus have substantially waning transmission protection also be excluded from the office)? What about those who got a different jab (e.g., AstraZeneca, Sputnik, CoronaVac, etc.), each of which has varying levels of effectiveness (and varying levels of effectiveness reduction over time) against different variants? How will you handle those that already had COVID-19 (and therefore (a) have even higher immunity than the vaccinated, and (b) who face higher health risks if they get vaccinated post- natural infection)? What will you do with the immunocompromised (folks with organ transplants, lung problems or cancer patients) who got the vaccine but have low viable antibodies because they require evermore booster shots? What will you do when future variants require different jabs? I could go on, but I trust you get the point. My real question for you is, will you be responsible for coordinating monthly/quarterly management meetings to update & maintain these ever-changing mandate policies covering ever-growing future use cases?
**And if you think I’m exaggerating, look no further thanNY State Assembly Bill A416, which proposes forcibly putting carriers of COVID-19 who do not conform to the state’s medical guidelines into something akin to internment camps, where they will be forced into a treatment deemed appropriate by the state and detained indefinitely until they comply. Imagine a U.S. legislative policy so bad, thateven Russia Today was able to shit all over itas being far too draconian.And it’s not just the state of NY, but the CDC as well.
===================
Last comments before I dive into supporting details
To not lose sight of being pragmatic as it pertains to your inquiry, I want to point out that at this juncture even a discussion about vaccine mandates is mostly moot.
We already know (confirmed) that those who are vaccinated/infected carry as much viral load as the unvaccinated. Which, coupled with waning transmission prevention efficacy means for all practical intents & purposes those vaccinated and those unvaccinated pose similar risks to one another.
And this is notwithstanding even more cutting edge research (not even yet published i.e. currently pre-print in The Lancet), which suggests those vaccinated carry significantly(upwards of 200x) moreviral load than the unvaccinated (which would, if peer-reviewed, flip the risk equation on its head even further in that those vaccinated would pose far greater risk to one another than those unvaccinated). (And it is worth noting that this development would be consistent with what has been found with other vaccines — in this 2017 study, for example, it was assessed that those who were vaccinated for influenza shed 6.3x as much virus as those who are unvaccinated. Crazy stuff.)
All of this is to say, despite the nationwide pushes you’re seeing for private & federal workplace vaccination mandates (which may have made at least some sense much earlier on), such mandates are unfortunately no longer effective models at this stage, unsupported by what we now understand via the latest science. Instead, if you really want to make a difference in improving workplace safety at this juncture, I would suggest implementing either the 1st, or both, of the following policies:
(1) Everyone at the company must perform a daily (pre-commute) self-assessment health survey, whereby all individuals must confirm they are not exhibiting any of the known symptoms of COVID-19 (i.e., if you can’t smell, have fever/chills, shortness of breath, etc., you can’t come in to the office, period), without any pressure from management to respond they are symptom-free.
(2) (Optional) everyone, irrespective of vaccination status, must get tested weekly for COVID-19, such testing to be reimbursed by the company. If you test positive, you aren’t allowed to come in until you test negative.
You asked how we’re handling it, and I can tell you that we’re doing the first one at [my company], and I would recommend utilizing the second one for any in-person company events. That’s it. No mandates. Anything beyond that will lead you into a logistical nightmare (at best), foster a false sense of security as it isn’t effective (worse), and in my humble opinion, is purely unethical (worst of all, which I’d like to think is a decent enough reason not to do something) at this stage.
So anyways, all of the above is the summary of my current POV. What follows below is/are the supporting details for the conclusions I reached in my summary POV 1(a), 1(b), and 2(i) above, if you’re interested in the data.
Always happy to chat/update further as the saga continues ✌
best, [REDACTED]
P.S. if you’re going to skip Parts 1 & 2 below*, then no worries… I get it, I probably wrote far more than you were looking for. But if indeed you do skip them, try to make it to the ‘Closing Thoughts’ section way down below — I’ve sourced a nifty chart down there that might give your colleagues pause in their ongoing discussions about mandates before they consider the unvaccinated to be idiots for whom behavioral mandates are the only appropriate solution.
*Though I highly recommend Part 1 (where it says “TWO OTHER THINGS TO CONSIDER” (then scroll to find #2)) as this contains a suggestion for how to naturally protect yourself from COVID-19.
===================
PART 1: RISK OF COVID-19 DEATH —> DE MINIMIS FOR ME
First I’ll address why I do not view COVID-19 as dangerous for me personally: from the CDC’s own data, available here, you can see current the Count of Cases and Count of Deaths by age ->
(Though before I go further, pardon me for abstaining from a lengthy discussion on the reliability of data from an organization that even Dr. Deborah Birx herself — (an individual who received a Meritorious Service Medal from the U.S. Department of Defense in 1991 and a Medal of Excellence from the CDC in 1994) — was quoted as sayingshe didn’t trust a single word from. Hmm, I wonder why she didn’t “trust” the data, could it be because they were —>overinflating “COVID-19 deaths”? <—… I digress.)
Anyways, according to the CDC, being 32, my “risk” stands at 0.14% (purely averages speaking, irrespective of the analysis below); a “starting statistic” you could call it.
The immediate issue with this data, unfortunately, is we’re only able to count cases with confirmed COVID-19 PCR (or other) test results, undercounting materially true case counts to date. As you might imagine, those asymptomatic do not test themselves regularly or out of nowhere. I mean, personally speaking, I am obviously not testing myself on any basis on any cadence — I’d only get tested if I had reason to. Thus is the reason, that the CDC already stated well early on in this pandemic that true case counts were “likely” to be upwards of 10x higher than we have documented (which they concluded based on widespread antibody testing).
Deaths in the U.S., on the other hand, are religiously tested for COVID-19, capturing the vast majority (if not nearly all) deaths, where a COVID-19 infection was present.
Using these two bits of information from the CDC, we can adjust for a “truer” baseline risk. Now, while I could exercise the luxury of taking on more than a 10x spread (because those younger tend to be more asymptomatic), I’ll be conservative just for the sake of it and just use the “10x average” figure. And so, a true starting statistic for me isn’t 0.14%, but a markedly lower 0.014%.
Next, we can use Exhibit B, taken right from the CDC website:
For… 5% of… [COVID-19] deaths, COVID-19 was the only cause mentioned on the death certificate. For deaths with conditions or causes in addition to COVID-19, on average, there were 4.0 additional conditions or causes per death.
Again, this is nothing new and has been known since very early in the pandemic, as you can see from this study for example listing the leading comorbidities as measured in NY as early as April 2020:
And herein lies my second issue with folks who preach to me that vaccines are necessary for my survival (the first being my initial lowly baseline risk).
Knock on wood, but I have no non- COVID-19 induced comorbidities — zero. My takeaway is just that: for someone like me, COVID-19 is mostly a virus known to exacerbate serious pre-existing conditions to the point of overwhelming the system definitively.
Put another way, imagine a motorcycle rider trying to assess their risk of death from riding (i.e., catching COVID-19). They see a study which puts the risk of death for those motorcycle riders who were (1) drunk (2) doing a wheelie on the highway (3) during a rainstorm, and (4) while texting with a friend (i.e., analogous to four comorbidities). It would be flawed reasoning for a rider who doesn’t do any of those things to put themselves in the same risk category as those who do. So while no one is saying motorcycles aren’t dangerous — they certainly are — they’re nowhere even in the vicinity as dangerous as riding while doing all the other things. Likewise, neither should a healthy teenager dwell on their COVID-19 risk with the same fervor as a 100 year-old morbidly obese individual with terminal cancer.
Okay, let’s revisit my personal risk again. First, I will ignore the 5% “no comorbidities” statistic above, because out of fairness I want to account for likely COVID-19 induced comorbidities like Respiratory Failure, Sepsis, etc. as well as possible ones like Renal Failure, Cardiac Arrest, and the like. So, let me simply reduce my risk not by 95%, but 57% (conservatively even rounded down further to a clean 50%), which removes just 1 non- COVID-19 induced comorbidity for my age group.
And just like that, my adjusted risk is downgraded to 0.0069% annually (annually, because it’s only once a year — after which time abetter-than-vaccinationnatural immunitykicks in for that season).
So what really is 0.0069%, you might ask? After all, we humans aren’t terribly good with numbers like that. To help you put it in perspective, consider that according to the National Highway Traffic Safety Administration, your (or my) risk of dying from a freak car accident in any given year, is 1 in 5,407 or 0.018%.
Let that sink in: based on what we know today, I personally am 268% more likely to die in a car accident tomorrow (or any day this year) than COVID-19. But do you really think that in pre-pandemic times, the “1 in 5,407” statistic kept me locked up inside my house? You think even today (in the middle of a pandemic) that figure stops me from taking a leisurely drive to grab ice cream with my nephews? or catching a movie with my brother? or — God forbid!! — hanging out with and actually talking with my friends? No!, and it never could. Because life, my friend, is about dancing in the summer rain, not cowering in fear of getting struck by lightning. But hey, maybe that’s just me…
In any case, I want to come back to your comment about concerns your colleagues have regarding young children. When we look at the statistics available (table above), the results are even more stark: for kids aged 5-11, their odds of a fatal COVID-19 infection are 1 in 137,000 when you factor in asymptomatic cases. And again, we’re talking about a risk inclusive of those with comorbidities. For kids 5-11 who are perfectly healthy, you can consider their risk nil. Okay, well obviously it could never be actually zero, because we both know sometimes kids also fall off a bike and kill themselves — that’s life. But you don’t exactly see people running around freaking out over bicycles all day long, do you? Which is ironic as hell now that we’re on the subject, consideringalmost exactly the number of kids have died from bicyclesas from COVID-19 in the same time frame.
So when I hear about folks taking their kids for a bike ride on the weekend (how awful), or worse!, maniacally driving their kids for ice cream (putting those precious kids at 5,091% (51x) the risk of death as COVID-19), but then trembling at the thought of walking into an office the following Monday because there’s an unvaccinated person there, so they feel the need to demand forcing medical decisions on those people (like getting jabs with vaccines made by companies whose rap sheets (Pfizer, J&J) would satisfy essay requirements at most colleges, approved by an organization that finds safety issues in 1/3 of its drugs post-approval), I come to the simple conclusion that common sense has left the building — it’s mass hysteria.
Alright, enough beating the completely de minimis personal risk dead horse because the point is clear. But let me add two more small things before getting to the dangers of the vaccine:
TWO OTHER THINGS TO CONSIDER
The section above looked at the whole thing purely from a mathematical risk perspective with neither proactive measures in mind, nor accounting for simple and effective (though IMO criminally suppressed) treatment options available to thwart COVID-19 risk even further.
(1) First, on the treatment side. Look, I know there was the whole “orange man (Trump) bad, the FDA disagrees” political BULLSHIT thing going on. Like I said above, I do not give a shit about the political angle of any of this. I require data, and the data could not be more ironclad on the subject matter. I will simply leave these two links here, and avoid another 5 pages in this POV on why IMO this is being criminally suppressed by federal agencies:
First, Ivermectin (links to the studies: (Link A & Link B)). Summary table as follows:
Second, Hydroxychloroquine (link to the studies). Summary table as follows:
By the way, it is worth noting I have a friend right now who has COVID-19. He has felt like shit for the past week. I sent him the studies, and he bought Ivermectin 3 days ago without a prescription from a local store I pointed him to. After a week of feeling like shit, it took him less than a day to get close to symptom free. But hey, I am not a doctor, and “your mileage may vary.” There are a dozen other treatments in addition to the ones above that aren’t getting approved for mass application, either. Go figure.. I could send you the studies if you want, but anyways let’s move on.
(2) As it pertains to the proactive side — okay, sit tight because I’m going to perform a holy miracle here and give you one of several simple things you can do to essentially ensure never needing to worry about COVID-19 again. Not for you, not for the kids, and not even for the neighbor’s dog. Ready? Okay drumroll please… . Did you catch that? If you didn’t, I’ll decipher it for you. It’s your new friend Vitamin D.
The first study is striking all on its own and worth internalizing, but unfortunately it did group an entire category called “normal” into a single bucket. FYI “normal” is what the medical world considers to be ~20ng/mL. But that’s all it is as a level: normal… but far from what we want, which is excellent.
That’s where the second study becomes helpful. It puts the explosive nature of the findings into real perspective: at levels of 25ng/mL in the study, no severe or critical hospitalized outcomes were observed.While at levels of 40ng/mL or greater, there were not even hospitalizations.
Now personally, I regard it as nothing less than a crime against humanity that neither the WHO nor CDC are PUSHING these (and dozens other peer-reviewed studies on the subject) onto the forefront of our collective media screens. But as for the reason, I must digress, because again I could go down a long and nasty rabbit hole about perverted incentives in the system in terms of why you likely haven’t seen them.
In any case, here’s what is just so awesome for me… remember when we concluded I had a higher risk of crashing & dying from my trip to the local ice cream shop than from COVID-19? Well, it just got a WHOLE lot better, because my Vitamin D levels happen to be considerably well above 40ng/mL. Which means we need to be honest with ourselves and admit that I effectively have a ZERO clinically observed risk of death from COVID-19. I mean shit…. at this point really the only way I can die of COVID-19 is by having it and then getting into a car accident. Then sure, I will die “with COVID-19” (and, as you’ll recall from the link above, they would count it!).
So my advice is as follows: get your dang sunshine first thing in the morning. Do not lockdown. In fact, I’d argue it’s what caused so many deaths. People were heavily Vitamin D deficient from sitting at home all day, and it literally increased their risk of death instead of reducing it. And what the CDC did in this regard was at best negligently or at worst intentionally, criminal, and I have nothing but disdain for the way they went about that. Don’t even get me started on the youth suicides it led to, the increases in domestic violence, increases in drug overdoses, infanticide, denial of healthcare, and let’s not dismiss the whammy of the sheer economic devastation to jobs and small businesses the world over, the bleak economic prognosis for the poorest (how convenient), and the future impact of staggering U.S. debt right here at home. All caused by the incompetence or criminality of the CDC and WHO.
Honestly — my personal advice if you want to stop worrying about COVID-19 for the rest of your life (if you still even are), would be to follow the Dan Miller protocol. Each of his bits of advice is like an extra layer of bulletproof glass on top of Kevlar against COVID-19. And remind your colleagues, too, to stop relying on the “American way” of taking a pill to solve all their problems and blaming the unvaccinated. That is not only completely debunked now as I’ve demonstrated throughout, but it is weak morally. It’s high time we all do the hard self-work of making ourselves physically resilient, and stop feebly making outward demands of others to inject into their bodies vaccines that are only now being tested, in vivo, on large numbers of human beings.
Speaking of which… perfect segway.
===================
(VERY BRIEFLY) PART 2: LONG-TERM RISKS OF [SPECIFICALLY] THE COVID-19 VACCINE –> HIGH
As I’m sure you’ll remember, a while back I mentioned I would send you a thorough, synthesized summary outlining the dangers of the COVID-19 vaccines and how the risks they carry far outweigh the risks of the virus itself. Unfortunately, I am not even a fraction of the way through the hundred plus pages of medical literature showing that conclusion — I’m still working through it. I absolutely feel terrible for not having lived up to my promise, though I’m sure you can appreciate the sheer herculean nature of synthesizing 7 months’ of research involving almost a thousand individual pieces of data, and weeks’ worth of video testimonials by researchers, all into something “succinct and digestible”, all the while working on [my company] in the middle of it all.
In any case, it would be disingenuous of me if I didn’t at least provide a sneak peak of a random assortment of links I had handy for why I will not get the vaccine (aside from the fact that COVID-19 poses no risk to me, per the first section):
Podcast: The High Wire — A Sea of Lies (in depth discussion about perverse incentives driving bad decisions by the CDC (particularly the second half of the video))
Short & Sweet: Why non-lethal pressure on the virus is bad (versus natural immunity) -> Part 1 | Part 2
+100 more videos and podcasts on the subject to anyone who asks (unsynthesized, of course)
===================
CLOSING THOUGHTS
If you made it this far and checked out even any of the content, kudos. Most folks here in the Northeast stop listening to me once I say “hey, there’s something not right here in this data” or “I’m not too worried about COVID-19 personally”. They think I’m a nut. Now, if you’ve made it this far and checked out most of the content, then I already know you’re starting to wonder if you’re losing your mind, because boy do I have a club pass with your name on it, if you’d like one.
Alas, contrary to popular belief it’s far from a nut club, despite how strong the external pressure is these days to try to make it out to be the case. Rather, It’s a club filled with precisely the very people who we’re supposed to be listening to as a society:
The CDC would have you believing it is just the crazy and uneducated who are most wary of their (and the FDA/WHO’s) conclusions — you know, it’s all the rednecks down south! And they’re right, it is the uneducated (left of the chart). But it is disingenuous for them to try and ignore on the nightly news research like this out of Carnegie Mellon suggesting the biggest group of those most vaccine-hesitant happen to be the smartest folks in the world — the ones I’ve certainly not been ignoring, despite their being shamed, cancelled off of social media, and publicly silenced.
Put another way, I would only posit the simple question of when in the history of the world have you ever had thousands of scientists, doctors, and researchers, some of the brightest minds* in their fields around the world sounding an alarm, and the official response be to label them all as batshit crazy and prevent them from speaking?Hint. Personally, I can’t support it. A free society must allow all open discussion without ridicule well before we dare discuss collectively forcing medical decisions on people using actual threats against their autonomy. We’re too far past that Vietnam-level of government lying bullshit that results in unholy suffering for society for this barbaric nonsense to continue, and it’s time for this country to start acting like we learned something about the importance of asking questions. I simply cannot place any trust in the idea I’m not being lied to until every scientist worth their salt has had an opportunity to speak up freely, and the nature of their concerns investigated transparently. And neither should anyone else.
*Such a fun fact it is that among this ocean of scientist voices being smeared & erased from history are (1) the guy who helped invent mRNA vaccine technology, and (2) the former Chief Scientific Officer (CSO) of Pfizer (who held that role for 16 years and focused on respiratory illnesses), both of whom are saying we have to stop vaccinations at once for those who aren’t at actual high-risk with COVID, because for everyone else they’re not only toxic & dangerous but will be the very cause of this never ending pandemic. Now I don’t know about you, but I neither invented mRNA technology nor worked at Pfizer for 16 years as CSO, but if I did, I’d sure prefer the American people heard my concerns, you know, sans the childish smear tactics part. Until then, I will not — cannot — accept any mandates on moral grounds.
And so there you have it. My opinion on mandatory vaccinations at this stage: if this were the Bubonic Plague, I’d be the first in line to get the shot. Same for Polio, Tetanus, and a whole lotta other great vaccines. But for COVID-19? Let’s just say I wouldn’t even know what to tell Saint Peter at the Pearly Gates to apologize sufficiently if I — knowing what I know now — supported a mandate. Come to think of it, there’s a quote that comes to mind here that I think is a nice way to wrap up this write-up, and commemorate those who continue to protect the rights of society:
‘The hottest places in Hell are reserved for those, who in time of moral crisis, preserve their neutrality.’ ~ unknown
========
DISCLAIMER –> OBLIGATORY
I obviously have to say this before I sign off.
At the end of the day, I’m not a doctor, I do not have an MD, a Ph.D., or any other useful acronym. All I am is an individual who values truth above hysteria & ideology. I will go wherever the truth points me to without regard for what “side” that puts me on. If it’s a contrarian side, then shit I guess I’m going to have to get in some fights. If I’m on the side of the majority, I guess I’ll rest easy. But wherever it is, I’m willing to go there, and as I said in my opening statement and reiterated to the group — I will always remain open to thoughtful and productive dialogue and my POV on every topic is subject to change through lifelong reflection. All I ask for these days is for those who disagree with me to either have the sincerity to work with me using the scientific method to get the facts on this subject, or if they have no interest in that, to let me do it alone without the constant coercion, which is how I’m sure the folks in your office who are unvaccinated, feel.
Anyways, for the actual disclaimer part: we all have to make our own decisions, do our own research (though I’m always happy to keep sending stuff I come across), and take our own risks. Freak accidents can happen, and just like I wouldn’t want to be responsible for a car accident that happens if you decide to go to a particular ice cream shop I recommend, it is the same for anything I’ve sent above and anything you or anyone you may share any of the information with do as a result of it. Always seek and follow professional, accredited advice! <– the disclaimer part.
Anyone who sees the vaccine as having more benefit than risk, should absolutely take it. I agree 100% with an 85 year-old with five comorbidities getting the jab — shit if that was me, I’d be getting quadruple jabbed walking around with a gas mask. No really, I would. Because for them the virus is actually very dangerous. And I’ve recommended it for some that I know personally would benefit from the vaccine because they are at high risk. But that’s where it ends. And not a single, inch, further.
I had not planned to travel abroad this year, especially after the UK government’s announcement in early 2021 that foreign holidays were forbidden. Even heading towards the airport with an intent to go on a foreign holiday could result in a £5000 fine or imprisonment! Surreal.
Where we live in London under a flight path to Heathrow, we notice that although there are fewer flights, they have not ceased completely. So how do people travel? It’s not something I have thought about.
One day at the end of April I receive a message that my elderly father’s condition is critical. Within an hour I am looking at flights back home in Eastern Europe and checking the UK government travel ‘advice’ webpages.
I say ‘advice’ but that word belongs to the past. Today, ‘command’ might be more appropriate. According to the government, only “essential” international travel is permitted for named valid reasons; ‘medical and compassionate’ is the category which applies to me.
I wonder whose compassion this is a reference to: mine, for wanting to be with my sick father, or the government’s for including this as a possibility. Reassured that I can go, it is now a question of buying the plane tickets, checking in and packing, right? Not quite.
WADING THROUGH THE RED TAPE
Since holiday travel has effectively been banned, the government created intricate webpages full of information on what is and what is not allowed, where citizens cannot travel, and if they must, what documents they need to prepare. So complicated travel advice alone has become that the webpage now includes a step by step flowchart with endless links within each step to be followed.
Getting through this information would take at least a day. It’s like a cross between a maze and a vortex. I soon understand that I cannot buy my tickets until I have uploaded the right Covid related paperwork onto the airline website!
First, I need to fill a Declaration for International Travel (since the 17th May it is no longer required) which asks for personal details including my date of birth, passport number, home address and destination.
The key question is the reason for international travel – and in the actual online questions, the phrase is: ‘What is your excuse for travel?’ My excuse? What kind of language is that? Am I asking a teacher to let me leave the classroom? Am I asked to explain why I haven’t done my homework?
That really shocks me, although I have already noticed my own reaction to the very idea that I need permission to leave the country, as if I was back in Eastern Europe before 1989…I read the following declaration and tick the right box out of the given options.
I hereby declare that my reason for being outside my home to travel internationally is for:
– Work
– Volunteering
– Education
– Medical or compassionate reasons
– Funeral
– Ending a temporary visit (non-UK resident)
– Allowing access to parents with children who do not live in the same country
– Other reasonable excuse – please specify
Next, I am required to sign to ‘certify that the information I have provided is true. I understand that if I provide false or misleading information, I may be issued with a fixed penalty notice and/or a direction to return home or be arrested’.
So, by signing this, and I have no choice not to if I want to get my ticket, I have given the UK authorities permission to arrest of fine me should my excuse to travel turn out to be incorrect. What if my father is not that ill, then what?
But of course, that is not enough. I now need to provide evidence of my father’s illness. How do you do that when the whole of the world is still in lockdown; imagine having to get a doctor’s note on demand. I am still just trying to get a ticket.
I want to travel tomorrow morning, my sister-in-law tells me, Dad is given a couple of days. I ask my brother to send me an email confirming the family crisis, he does that within an hour. He is also trying to copy the notes from my father’s last doctor’s visit and the most recent diagnosis.
Then, still before I buy a return ticket, I need to get a kit of two Covid tests which I will need to take upon return to UK. Another link takes me on to a list of government-approved Covid test providers. A whole list of them, each can be accessed via a separate link. I try a few. They average around £200 each. The cheapest ones are £99 but are sold out.
Why can’t I see any free NHS ones? The ones given out like sweets in schools and local pharmacies? Why are these not available? Why could I not just pick a free one at the airport?
But of course, there is no to answer these questions, I am desperate to leave so agree to this, too. No test, no flight. So, I order one of these almost £200 test kits, get an email confirming the order, upload all the documents and finally I can complete the purchase of my tickets which, as usual, turn out not so low cost after all.
I check in. My boarding card (lucky I had just bought a printer the previous week) says at the top of the page ‘Covid Documentation Uploaded’. So, now I have the boarding card and a pile of printed pages which presumably I will need to show at UK border control in order to prove my excuse for leaving the country is legitimate.
Finally, I download and fill in the compulsory Passenger Locator Form for the destination country that will enable the system to track and trace me. It is nearly bedtime and I now need to pack.
ON THE GO
My husband drives me to Stansted in the middle of the night. An early morning flight, no public transport available but at least it’s quiet and there is no traffic. The airport is still closed; a group of families with young children are waiting for the door to open.
These are not holidaymakers breaking the law to get some forbidden fun. No idea where they are travelling but they look like they are going home somewhere south, southeast perhaps? Turkey, Bulgaria or Ukraine? No idea but they do look like part of the globalised chain of workforce escaping poverty and perhaps the lockdown has pushed them to return. Better to be jobless and poor in your own village. The weather tends to be better and the environment less hostile.
Finally, the doors open. I push the scarf up over my face, my hand clutching a plastic folder with a wad of documents allowing me to leave. It is quiet, no waiting. I go through security, passport control seems non-existent, shops still closed so nothing to stop for. I wonder at which point someone will ask me to see the papers. Ask me what my excuse for leaving is. Strangely, that never happens. I am almost disappointed. I spent about four hours sorting out all that paperwork the night before and now this is not even checked!
Immediately I catch myself: why am I disappointed? Because no one will give me the all-clear? Have I been conditioned to want to be waved through the green light already?
Perhaps that is how normalising oppression works. But of course, there is no need to check, the documents have been uploaded and recorded somewhere and someone now knows everything about me, my plans, my reason (“excuse”) for leaving the country. Or perhaps the intimate details of my family crisis; my father’s terminal illness and my attempt to get to him before it’s too late have now just been converted into big data slushing around the corpo-government’s control AI machine, and turned into useful predictions.
I guess this type of authoritarianism does not even need stern looks from border control officials, no need to divulge private dramas in public. Hours of stress of getting the documents turned into a discreet but vital small print on my boarding card; the only visible proof that my travel is acceptable to the corpo-state. It is all so neat, tidy, hi-tech and invisible that we can just pretend that all is just normal.
After all, the airport trimmings look all the same; with adverts, duty-free shopping, same old queues at departure gates and same safety drills on the plane, down to the irritating Ryanair voice thanking us for choosing to fly with them (no one chooses to fly with Ryanair, just like no one chooses to go to the dentist, you do it because you have to and you hope it won’t be too unpleasant).
We can pretend nothing has changed. Except the masks on faces, of course. Slow drinking and eating is my solution. During the flight many noses protrude against the regulations, of course. People do need to breathe.
We land on time. I send a message to my father, anxious, hoping he is still there. He is not responding. I am worried. From the tarmac I can see the arrivals hall is full. There is no way of entering so the crowd from my plane stops outside and waits in the drizzle. I wonder why that is. Is that Brexit or is it that people’s papers are now checked after all?
The queue moves very slowly, twenty minutes after landing I send my father another message saying that I’m still waiting for border control. I have no idea why this is so slow; each person seems to spend a good few minutes at the control desk. Finally, an hour and a half after landing I get into the taxi. As the driver pulls away, I notice a long queue of passengers outside the arrivals hall waiting to get a Covid test. I arrive home and find my father hanging on.
MY FATHER’S ILLNESS
There is a twist to this story. My father had been treated for cancer but has been still doing quite well and had been planning to spend the summer away from his flat, in the countryside. His sudden deterioration was unexpected for me but I have not had time to think of reasons. I only learnt of this yesterday. But now I am in the flat, taking my shoes off when my brother drops the bombshell: ‘you know, Dad took the vaccine’.
I am shocked. He told me he was not going to, because he found the registration process too difficult, so he decided to stop trying. I was relieved; I had been persuading him that he should not, that being immunocompromised, his system might not cope. I told him what I knew and what I worried about. My brother tells me another family member helped organize his jab and took him there. Jesus. But I am to pretend I don’t know about it; Dad asked my brother not to tell me.
So, I learn that the day after the Pfizer jab he started to feel weak, and within ten days he was prescribed blood thinning injections, a daily drip and he became bedbound. My brother has hired a hospital-style bed and an oxygen machine, set them up in father’s bedroom and organized a private nurse for daily visits. Dad had not wanted to go to hospital: he believed that hospitals were overrun by contagious Covid patients and that going to hospital would mean certain death under a ventilator.
Luckily (I never thought I would say this), unlike the UK, this ex-communist country never managed to build up its own national health service to a level able to deliver comprehensive care, so a secondary private sector filling the gaps exists and is not beyond the means of many people. So here he is, in his own bedroom and getting care at home.
He is happy to see me but asks me not to touch him. I feel sad, guessing he might worry I am bringing contagion. That hurts. I pretend I know nothing about the jab. Later, much later, I remember this moment and think that, he might have wanted to protect me. He knew the jab made him ill and he worried he was fighting vaccine induced-Covid and did not want to give it to me.
He never told me about the vaccine, I never told him I knew.
Sunset in Quaratine
QUARANTINE ONE: THE APP
The day after arriving I receive a text message telling me I am now under statute of law obliged to download a particular app and use it during my 10-day home quarantine. I start the download but can’t complete it. Something is stuck and I have no idea how to fix it. I try for a while and then abandon it. I spend most of the time caring for my father who now slips in and out of consciousness.
The next morning I get a phone call but it stops ringing before I have time to answer it. The following day the same happens. I realise this is the local track and trace. They ring but don’t wait for me to answer. Their call is logged, the box gets ticked but the robot or a human cannot be bothered to do the job properly. Actually, it must be a human as a robot would not give up. Good. The tyranny will fail due to human error or sheer laziness.
I don’t know what possessed me but somehow, I manage to complete installing the Quarantine App. The system springs into action. I get a message from the app that I must take a selfie within the next 30 minutes and submit it. I take a selfie from the app which gives me as many times as I like to choose the best shot. I choose the worst shot.
Of course, there is a way to cheat: after doing my selfie I could leave the phone at home and go out for a walk. Trouble is, the selfie demand comes at a different time each day, usually towards the end of the day. But I have no reason to go anywhere, really, I have come here to be with him, and his condition continues to be critical. And at some point, during this journey I decided that I would do everything by the book, just to see what the new normal travel feels and looks like, and what exactly they want us to experience.
Well, here I am, in a 10-day quarantine in a flat with my dying father. We are lucky. I have my brother to get the shopping in and kind neighbours ready to help. We are lucky my father is at home. What would be the point of coming here all this way, only to be stuck in quarantine if he was in a hospital with no visitors allowed? So, all in all, we are lucky.
DIFFICULT DAYS
Days go by, my father’s condition improves a little, I am his nurse, and of course I touch him – he stopped protesting as soon as he needed a glass of water; I continue to take my selfies. We talk, I read to him, feed him, then he sleeps. He dies two days after my quarantine ends. That is good timing.
There is a lot to do now, and I will not be breaking the law trying to organize the funeral… I remember my favourite literature lesson at school when we debated who was right: Creon or Antigone. Even then, I was in team Antigone.
A doctor arrives to certify death. She is nice and takes her time. Talks a little. Does not look like a corporate bot. She is sitting at a coffee table doing the paperwork. For the cause of death, she writes ‘Thrombosis’. I ponder for a bit and then hesitatingly say: ‘Did you know he was vaccinated?’.
Her face changes and she asks: ‘No, when?’ We tell her, ‘Four weeks ago, exactly’.
‘I am not allowed to say anything,’ she says, ‘but I can tell you I have seen a lot lately. A lot!’ We try to encourage her to talk more but she is cautious. I just ask her: ‘Why would a person on cancer treatment be given a vaccine? Surely that had not been done before?’ She looks at me and says: ‘Because they want to vaccinate us all.’ So, she knows.
This kind of conversation would have been typical in the days of strict communist authoritarianism before 1989. You never knew whom you could trust so you just dropped hints and checked for people’s response. In those days careless talk was dangerous, and I am too young to remember the worst times: the Stalinist years when children were encouraged to denounce their parents; many were imprisoned, tortured and killed.
Now the threat is only a loss of income and public humiliation and yet the new order based on lies, fraud and corrupt science is already in place. Everyone is just doing their job. A perfect example of Hannah Arendt’s banality of evil in which those, following orders in this elaborate house of cards, often do not even know their active contribution to harm inflicted on others. They do not realise because they refuse to look and to know. They stopped taking responsibility for their individual part in the whole.
There is a small group of doctors in the country who are challenging the official narrative, attempt to offer treatment for Covid patients and warn against the untested ‘vaccines’, particularly now that governments want to jab children. Their voices are censored, the people get smeared, ridiculed and shamed by the professional licensing medical body. The modern-day governance in Western democracies!
TRAVELLING HOME
As the funeral preparations get underway, I need to organise my return travel. I check the UK government website again. Travelling from an ‘amber’ coded country, I must test negative for Covid within 72 hours prior to departure. Tricky when the flight is on Monday afternoon.
I start to search for UK government-approved tests available in the city. Only a handful provide the specified UK approved antigen test with results in English. They are also open only in the mornings so if I test on Friday morning, I might be testing a few hours too early to fit within the 72 hours.
After hours of online searching, I find one that looks almost right. I pay the equivalent of £35 online and am told to come on the day, without an appointment. The laboratory website provides useful advice, how to prepare for the test. I learn that I should not brush my teeth or use mouthwash on the morning of test. So now I know what to do.
I arrive at the testing centre early, having heard that queues can be quite long. It is, and it is in the street. The lab’s waiting room only allows three people at a time so the rest stand outside. After about an hour it is my turn. I am allowed inside the surgery.
On the right, by the door, a masked man sitting at a desk behind a glass screen is checking my name and the type of test I have purchased. Then, a young tall, man in full white hazmat suit, his face covered, and in protective glasses ushers me to sit on a chair and tip my head backwards.
This is my first Covid test ever and I am terrified. I have rehearsed telling them how sensitive my face feels and asking not to go deep but there is no eye contact, no talk trying to help me feel comfortable, no attempt to put me at ease. He just tells me to tip my head back far.
I just manage to ask him to go into the left nostril as my right one is not straight. He happily obliges and shoves the long stick into my nostril. As soon as the tip enters my nose I feel shock, a feeling of something unnatural, wrong and threatening happening. The area he just touched is too soft, sensitive and the sensation so unfamiliar I involuntarily, and to my own shock, find myself pushing the man’s arm away. He moves back and looks at me, his body language (there is no face available) disapproves of my behaviour.
I say, please don’t go that deep, you already have some but he insists, tells me not to defend myself and does it again. And again, that feeling that a part of me which is vulnerable and should not be touched, gets scraped. He gets his sample and nods for me to go. I am frozen in that chair, unable to move for what seems like a while. I have tears in my eyes, and I am alone with two hazmat wearing robots. No word is uttered as I leave.
I get my negative result within hours. I recover with an old friend. By then I have a splitting headache and my left nostril is moist with a slight leak. The headache lasts for a couple of days but the leak persists for at least ten.
I arrive at the airport early because I have difficulties completing the UK Passenger Locator Form which UK needs from all passengers. I pass through a manned gate with an automatic wrist temperature check. The airport is unusually quiet, and the staff help me identify the problem which stops me from completing the form. The reference number for the double Covid test needed for the Passenger Locator Form is wrong. I ring home and ask my husband to read the reference number off the Covid test kit. Surely it has arrived now. It hasn’t. It looks like the Day 2 and 8 Test I ordered has not been paid for.
I am told I need to buy a new kit if I want to get this flight. I do as I’m told. No form, no flight. I stand next to the luggage drop off counter feeling sweats, and with my hands shaking I battle the website on my phone. Again, all the ‘cheap’ ones are sold out and somehow, at the last minute I manage to make a purchase for £180, get an email, a reference number, complete the form and have my luggage accepted.
I hurry to my gate and make it just in time as passengers are starting to board. I slow down to join the Ryanair herd waiting on the tarmac for the aircraft to be processed before we are told we can travel.
The pavement is marked with lines at 2-meter intervals. Two men behind me are joking loudly that we must stand on the lines correctly, otherwise the virus will jump on us. I turn and smile (no mask, we are still outside) and make eye contact with the fellow humans.
QUARANTINE TWO: TRACK AND TRACE
Back home in London, the following day I get my first out of ten phone calls from Track and Trace. Each time a different voice reads the same script.
I am contacting you on behalf of the NHS Test and Trace as you have recently travelled into the UK from abroad. Are you happy to continue in English?”
No idea what would happen if I said ‘no’.
Before we proceed, I need to make you aware that this call will be recorded for training and quality improvement purposes and should just take a few minutes of your time. I can confirm I have completed the necessary data security training and all information you provide today will be stored securely. NHS Test and Trace may need to share your details with other organisations including the Home Office, and further information on data security and privacy can be found on http://www.gov.uk/coronavirus. Sharing information in the call today means you consent for it to be stored in the ways I have described. Are you happy to proceed with the call?”
I wish I could say, no, I am not. Once or twice I ask how long the data is going to be stored. The caller is not sure and advises me to find this out from the government website. The call proceeds with them checking my year of birth. Then they ask if I have opted into a ‘test to release’ – I frankly don’t even know it is my option, so I say ‘no’.
I later learn that the Test to Release scheme does not replace the compulsory Day 2 and 8 test. The ten-day quarantine can be shortened to 5 days by ‘opting into’ Test to Release for an additional £99. I realise they ask this question to advertise another product!
Can you confirm that you are quarantining at the address you provided on the passenger locator form and will continue to do so for ten days starting on the day after you arrive in the UK.”
So, again, I confirm, yes. What would happen if I said no?
As part of the Covid 19 response you are legally required to take the test on Day 2 and Day 8 and a failure to do so may result in prosecution.”
That answers my previous question…
Has your test arrived? And have you taken or do you intend to take your test?”
Yes.
Then I am asked if I got my test from the NHS or from a private provider. I am confused as I had no option to get an NHS test and I tell the caller. They seem happy with my answer and continue:
If your Day 2 test is positive confirming Covid 19, you do not need to take another test on Day 8.”
I think, on one occasion, I ask how I am expected to post the test if I am not allowed to leave the house. Of course, the assumption is there is someone else in the house, and if I still have difficulties, again, the go-to place is another NHS number. Amazing what they can do these days; they can even pick up your mail for you!
The call continues:
If you develop any of the three coronavirus symptoms which are: a new continuous cough, a high temperature, or a loss or change to your sense of taste or smell, please visit http://www.gov.uk/coronavirus for further advice. You should not go to the GP, hospital or a pharmacy. If you require medical advice, please ring the NHS on 111 or in an emergency dial 999”.
So here we have the admission of medical malpractice: if I fall ill, I must not seek help from NHS, not even by going to my local pharmacy. I must stay home without help, except of course, if I qualify for 999 ie, a ventilator…
The call continues:
I must advise you that if you test positive for coronavirus or are identified as a close contact of someone who has coronavirus you will be notified by NHS Test and Trace and may be contacted again. Is there anything you would like me to repeat?”
Of course, if someone I sat next to on the (half-empty) plane gets a positive result, my quarantine will stretch to a fortnight or longer! Each time, the call ends with a friendly, youthful, ‘have a great day’. All those who have called me are young voices, all kinds of accents, probably desperate for any job in the current climate. They are trained to stick to the script and any departure from it by my questions seems to trip them up.
And most of them probably think they are doing something socially useful and valuable.
THE QUARANTINE DIY TESTS
The one I have purchased in haste at the airport is a kit with two PCR tests to be administered at home on Day 2 and Day 8. The instructions tell me that the test is run at less than a 30-cycle value threshold.
The first thing to say about the swab is that it is long. It looks like a cotton bud used for everyday use, but on closer inspection it is different. The stick itself is about 12 cm long, that’s 6”, and designed to break off after the sample is collected and put into a small tube provided. The tip itself is 2 cm long, quite thin and covered in almost translucent spiky bristles protruding outwards. It looks a bit like a miniature harsh brush designed to scratch the delicate tissue inside the mouth and nose.
I am told to swab the back of the throat for 3-5 seconds over the posterior pharynx and tonsillar areas but to avoid tongue, teeth and the sides of the mouth. Then I am told to insert the same swab to each nostril about 2 cm deep and to rotate it for 3-5 seconds each time.
The form which I have to complete for each test is yet another mandated opportunity for the corpo-government to harvest my personal data, to store it for as long as it sees fit, yet, as is often the case in abusive relationships I have to (I repeat:) I have to give my consent for all this to happen, and even consent for my possible positive test result which may include my personal details: name, date of birth, gender, home address, telephone number, occupation, place of work, ethnicity and the fact that I have tested positive for Covid 19 to be communicated to Public Health England. Luckily, both of my test results are negative.
Eleven days after arrival in the UK my quarantine is officially over. It takes me a couple of days before I venture outside, I detect a bit of agoraphobia. In the last six weeks I spent twenty days in house arrest. They say it takes six weeks to develop a new habit.
POSTSCRIPTUM
I doubt very much I will travel internationally any time soon. Not planning to take the experimental Covid jab and so will not be enjoying the privilege of freedom promised to those with the vaccine passport. At the time of writing, it is no longer illegal to leave England but the elaborate hoops and the red tape remain and the government website reminds us that“to protect public health in the UK and the vaccine rollout, you should not travel to countries or territories on the red or amber lists”.
The ‘red and amber’ lists cover most countries of the world and returning from an amber list country will involve three or four tests which could come to £240-£340 per person plus the time spent completing all the online forms.
As to the red list countries; even a short spell there ends in an expensive £1750 per person prison-like stay at an airport hotel, as can be seen here.
So whilst not forbidden, even essential travel has been made into a series of expensive, degrading and time-consuming obstacles. Vaccine passports are being rolled out precisely to convince people they will magically bring freedom back to their lives. Do they not realise, that once they have their passports, the vaccine will need regular boosters?
Those still asleep; trusting the governments and the mainstream media think that easy travel is only temporarily put on hold but once the pandemic is ‘under control’, things will get back to the way they used to be. They do not realise the plan is to make travel an exclusive and rare event beyond reach of ordinary people.
This is done to us not just by the predatory elite class. Disappointingly, the pro-lockdown left continues to cheer these restrictions on and dismiss people’s desire and need to travel, as undeserved indulgence or middle-class privilege (interestingly, unrestricted travel around Europe was, until so recently, one of the main reasons for their fierce anti-Brexit position. What happened to their cherished principle of freedom of movement?). They could not be further from the truth.
They forget that, according to official migration data for the end of 2019, the UK is home to 6.2 million people – that is 9% of the total population – who have the nationality of a different country! And that data does not even include naturalised UK citizens like me, first-generation settled migrants who have close relatives all over the world and that unrestricted travel is an essential means to family life, something which is protected by Human Rights Act 1998.
The irony for those like myself, who grew up in communist Eastern Europe, is that freedom of movement, so taken for granted in the West, the right to travel and to have your own passport at home at all times is what we did not have then. The state set limits on where ‘citizens’, treated like its property, could travel.
For many who experienced those times, even as children, a return to state-mandated travel restrictions will feel like going back into tyranny.
As for my own journey: I will never forgive those responsible and all those lockdown fanatics for stealing my Dad’s, and so many other elderly people’s, last year by locking them up in the prison of fear and isolation, and then for pushing them to take the dangerous experimental jab which – for so many – was the last straw in their already weakened bodies.
An NSA document purporting to show Russian military hacker attempts to access a Florida company which makes voter registration software is sent anonymously to The Intercept. A low-level NSA contractor, Reality Winner, is arrested almost immediately. What’s wrong with this picture? A lot. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.

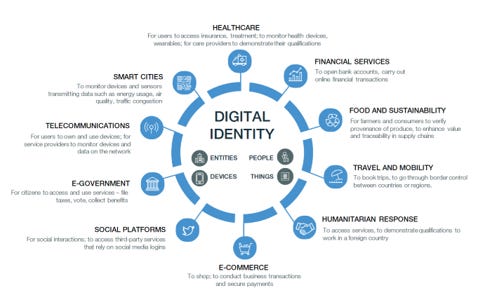
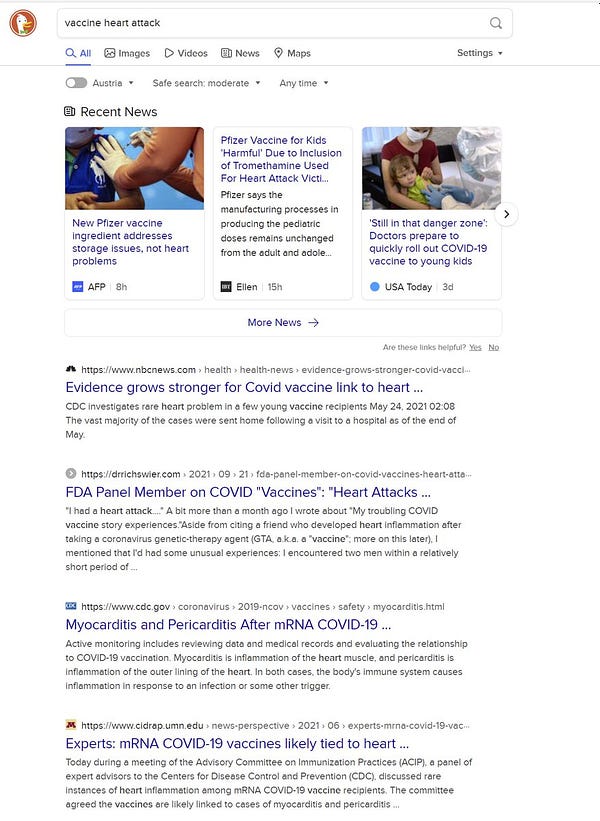
 The global assault on reality and the creation of a new “reality” has created a Mass Psychosis, described by Dr. Mattias Desmet as Mass Formation.
The global assault on reality and the creation of a new “reality” has created a Mass Psychosis, described by Dr. Mattias Desmet as Mass Formation.



















 Aletho News
Aletho News
{kind=link}