US ‘poised’ to transfer seized Russian assets to Kiev – DOJ
RT | January 20, 2023
The US will soon send the first batch of funds from confiscated Russian property to Ukraine, the head of the Department of Justice (DOJ) special sanctions task force, Andrew Adams, revealed on Thursday. Adams said the move should inspire US allies to do the same, and insisted the unprecedented practice is not just possible and permissible under international law, but “imperative” given the current conflict.
“We’re also poised to begin the transfer of forfeited assets for the benefit of Ukraine,” Adams said at an event hosted by the Hudson Institute, a DC think-tank.
“It’s not a silver bullet, but it’s something that nevertheless makes me hopeful,” Adams said, adding that the relatively minor sums are important as “a model to our foreign partners” and to establish a legal precedent going forward.
US President Joe Biden proposed the scheme last April, and Adams hinted it was in the works in September, but said Congress needed to amend several laws to make it work. On Thursday, he revealed those changes were indeed inserted in the $1.7 trillion omnibus spending bill, passed by Congress in the final days of 2022.
The new laws give the DOJ power to “direct forfeited funds to the State Department for the purpose of providing aid to Ukraine,” said Adams.
Previously a federal prosecutor in the Southern District of New York (SDNY), Adams was appointed head of Task Force KleptoCapture, an interagency sanctions enforcement outfit created in March. KleptoCapture is part of the US-led Russian Elites, Proxies, and Oligarchs (REPO) Task Force, which has frozen “hundreds of billions of dollars in Russian state assets and tens of billions of dollars belonging to Kremlin-linked elites,” according to the Hudson Institute.
Asset forfeiture is a controversial practice in US law. Proponents have defended it as a “key tool” for weakening organized crime and funding law enforcement, while critics accused it of being “policing for profit” and “egregiously at odds with our due process rights.” Adams insisted that taking Russian assets seized without trial “possible and permissible under fundamental norms of due process” and international law.
The freezing of Russian assets and finances by the US and its allies is “a completely illegitimate measure, violating commonly acceptable standards of commercial and international law,” and proof to the rest of the world “that they are thieves,” Russian Foreign Ministry Maria Zakharova said last week. She warned that any attempt to confiscate those funds and redirect them to Ukraine would be a violation of property rights and met with an “appropriate” countermove from Moscow.
The content of AIPAC’s recent Political Leadership Forum was largely concealed from the public

By Kathryn Shihadah | If Americans Knew | January 19, 2023
The American-Israel Public Affairs Committee (AIPAC) brought together last week 1,000 top political leaders to discuss the new political reality the pro-Israel lobby faces following the swearing-in of Israel’s new, extremist government, and to “strategize for the 2024 election cycle.”
The conference was closed to journalists, and only excerpts of some speeches have been released. Speakers included Israel’s Prime Minister, Benjamin Netanyahu (via video call) on Monday, and US Secretary of Defense Lloyd J. Austin III (in person) on Tuesday. Below is a partial summary of their remarks.
Normalization
PM Netanyahu addressed, among other topics, his hope to see the Trump-era Abraham Accords expand to include more Arab nations (read about the Abraham Accords here). According to the Israeli daily Ha’aretz, he is optimistic because many Arab leaders have changed their perception of Israel and now see it as a partner rather than an enemy.”
Secretary Austin likewise stated his eagerness to “deepen and broaden the Abraham Accords and to forge other normalization agreements.”
Both men overlooked the fact that in a recent UN meeting, all of the Abraham Accords signatories (United Arab Emirates, Bahrain, and Morocco) – as well as every other Arab country – had voted against Israel on a resolution calling for the International Court of Justice to weigh in on the occupation of the Palestinian territories.
Iran
The Israeli Prime Minister made reference to Iran, which is under worldwide scrutiny at the moment for its brutal suppression of human rights protest. Netanyahu labeled Iran “a terrible regime, depressive and terroristic.”
The US Secretary of Defense similarly stressed Iran’s oppression: “The regime has killed, and beaten, and jailed its own citizens for daring to speak out against its repressive rule,” adding, “we’re working closely with Israel and our allies and partners to impose coordinated pressure on the Iranian regime.”
Neither of the speakers acknowledged Israel’s own brutal suppression of Palestinian protesters and resistors (for examples, go here). United Nations data shows that in 2022, Israeli troops killed over 150 Palestinians in the West Bank alone (almost 50 in Gaza) – more than any other year since the UN started keeping track.
So far in 2023, at least 14 Palestinians have been killed already. Thousands more are held in prison or administrative detention without charge or trial – and many prisoners are tortured.
“Democracy”
AIPAC issued a statement in late December, immediately after the new Israeli government had been formed, congratulating the state and its new prime minister, adding, “Once again, the Jewish state has demonstrated that it is a robust democracy with the freedoms that Americans also cherish.”
Within a few days after forming the new government in December, PM Netanyahu tweeted the coalition’s intentions – which exclude any language about democracy:
“These are the basic guidelines of the national government headed by me: The Jewish people have an exclusive and unquestionable right to all areas of the Land of Israel. The government will promote and develop settlement in all parts of the Land of Israel – in the Galilee, the Negev, the Golan Heights, Judea and Samaria.”
(Note: “the Galilee” is part of the current state of Israel, but less than half of the population is Jewish; “the Golan Heights” and “Judea and Samaria” refer to lands belonging to Syria and Palestine, respectively; the internationally recognized name of “Judea and Samaria” is Occupied Palestinian Territory. 20% of the citizens of Israel and roughly 50% of the population over which Israel exercises control are Palestinian Arabs, largely Muslim and Christian.)
Rather than responding to Netanyahu’s blunt assertion, US Secretary of Defense Austin quoted a statement the Prime Minister had made back in November:”[We] will work for the benefit of all residents of the state of Israel, without exception” – a promise that preceded the formation of a government coalition that included some of the most extremist members in recent memory.
Notably, Israel has defied international law and the demands of the global community since the country’s inception – including its constant drive to build illegal settlements on Palestinian land and transfer Jewish Israeli citizens to that land.
American money for Israel
Austin went on to list the financial perks that the US is providing to Israel, including $3.8 billion annually in military aid (“the highest it’s ever been”). (Note: Congress spends another $3 billion a year on projects that benefit Israel, for a total of about $7 billion a year – $20 million a day.)
While some Congress members have pressed to block aid to Israel while it is in defiance of international (and US) law, the effort has gained little traction.
Republicans deepen investigation into Democratic money laundering with Ukraine
By Ahmed Adel | January 17, 2023
The Republicans plan to investigate where the money that Washington allocates to Kiev really goes. The conservative political party suspects that the Biden administration and Ukrainian President Vladimir Zelensky are involved in money laundering and the sale of NATO weapons on the darknet, using the Russian special military operation as an excuse.
“Whether you support Ukrainian funding or not, the fundamental question is, we deserve, and the American people deserve to know how their money is being spent, especially when we’re talking about $120 billion dollars of it,” Freshman Republican Senator JD Vance said on January 11 on the show Tucker Carlson Tonight.
The Republicans currently occupy most key positions in the committees on Capitol Hill. At the moment, one of their most important decisions is launching an investigation into the financing of Kiev by the Biden administration.
After winning the elections for the House of Representatives in November 2022, the Republicans decided to launch an investigation. Congress has formed a committee to investigate how the financial resources of American taxpayers are spent in Ukraine. One of the major questions is whether weapons sent as military aid to Kiev actually ended up in the hands of terrorist and various other organisations.
Numerous media outlets have reported the fact that the weapons supplied to Ukraine do not always reach the front lines. There is even information that these weapons appeared on the darknet – an illegal internet network.
In addition, numerous publications reported that money was laundered through an office that dealt with cryptocurrencies. In other words, the money that Ukrainian President Volodymyr Zelensky received as military aid was poured into this company, which was used to buy cryptocurrencies.
Senator Vance said in his interview with Tucker Carlson that those opposed to an audit “don’t want to be forced to acknowledge a lot of the money we’ve sent to Ukraine hasn’t been well spent.”
“There are a lot of corrupt people probably getting rich off of it,” he added.
More importantly than the allegation of corruption, the Republicans want to investigate the role of Hunter Biden – the son of US President Joe Biden, who has deep ties with Ukraine’s energy sector.
After the Republicans regained control of the House of Representatives in the midterm elections, they promised in their first press conference to investigate Hunter. Back in 2014, Hunter joined the board of the Ukrainian gas company Burisma. This was at a time when Joe Biden was Vice President and the war in Donbass was on the cusp. Hunter earned more than $50,000 a month over a five-year period as a board member of Burisma.
The Republicans claim that his appointment may have posed a conflict of interest. In 2022, more than 30 Republicans called for a prosecutor to be given special counsel authority to carry out an investigation into alleged “tax fraud, money laundering, and foreign-lobbying violations”. The conservative party has been studying messages and financial transactions found on a laptop that belonged to Hunter.
With the Republicans having gained the majority in the House of Representatives, they now have the power to issue congressional subpoenas to foreign entities that did business with him. It seemingly appears that the money that the US has sent to Ukraine since the war began is lining the pockets of Ukrainian and American officials.
Most likely, Biden’s son, and even his inner circle, were involved in money laundering and corrupt actions. As for the investigation itself, the Republicans will drag it out until it is clear who the Democrats will run in the 2024 elections. Evidence of such corruption can destroy any Democratic candidate and therefore prevent Biden from running for a second term. Ultimately, weakening the Democratic Party in view of the next presidential election is the aim of the Republicans.
The US Senate has demanded that a Congress report indicate how much money the US authorities sent to Ukraine. According to Senator JD Vance, the $114 billion that the US sent was “impacted by the situation in Ukraine” and does not even include several additional transfers previously requested by the Biden administration.
None-the-less, the senator stressed to Tucker Carlson that the Biden Administration, by law, “is supposed to tell us exactly how that money is being spent. We are putting down a marker…”
He then demanded a response by February 7. And it is until then that we wait for the latest development in the Democratic Party’s alleged corruption and money laundering with Ukraine.
Ahmed Adel is a Cairo-based geopolitics and political economy researcher.
‘Escort agencies booked solid for Davos forum’

RT | January 16, 2023
The Swiss escort agencies near Davos are already fully booked ahead of this year’s World Economic Forum, the elite gathering that brings together heads of state, corporate executives, and influential non-profiteers, Austrian outlet Exxpress reported on Sunday, citing a missive purportedly sent from one such agency.
In a message to unnamed hospitality staff and published by Express, escort agency Sensuallounge Escort urges readers to book their “fine selection of ladies and gentlemen” ahead of time to ensure “the best possible care and company during the World Economic Forum.”
Sensuallounge reportedly offers “services for all sexual orientations,” and the outlet claims one night with one of their employees costs €2,350 (just over $2,500). The service does not appear to accept cash as payment, offering clients the option of paying with a major credit card or via PayPal.
Explaining that the WEF’s annual get-together is high season for Swiss prostitutes, Exxpress revealed the agencies set up dedicated websites for the conference. Their roster seemingly fully booked, Sensuallounge’s site had already disappeared as of Monday.
While the WEF invited about 2,500 people as accredited delegates this year, over 30,000 more are expected to descend upon the ski resort for the dinners, parties, and, according to a growing body of journalism documenting the “dark side of Davos,” sex for pay that occurs outside the forum.
Sex workers also lurk in hotels and bars frequented by guests, according to a 2020 report from the Times UK, and women – even if they are accredited WEF attendees – are “routinely harassed” by the men who dominate the conclave. Indeed, the event began warning women that year not to go out alone after dark, “because if something happens with some big CEO, who is going to be believed? You or them?”
Prostitution at Davos has caused controversy in years past, though the bigger concern appears to be keeping the working class under control. The Swiss Army has been authorized to deploy as many as 5,000 troops if needed to provide security to the billionaires.
The theme for 2023’s conference, which runs from January 16-20, is “Cooperation in a Fragmented World.” Protesters were already onsite ahead of the event’s official start on Monday, denouncing attendees’ use of private jets to deliver climate-change platitudes.
Israel occupation forces bulldoze Greek Orthodox land in occupied Jerusalem
MEMO | January 16, 2023
The Israeli occupation authorities yesterday started to bulldoze a 5,000 square metre plot of land owned by the Greek Orthodox Church in occupied Jerusalem’s Silwan neighbourhood, the Wadi Hilweh Information Centre has reported. The operators of the bulldozers were protected by a large number of Israeli occupation security forces and police.
According to the centre, the Israeli Nature and Parks Authority as well as settler organisations commissioned the bulldozers to uproot fruit-bearing trees and level the land. Illegal settlers and police seized the land on 22 December. The Jewish settlers fenced it off and installed surveillance cameras under police protection.
When Silwan residents rushed to the scene to stop the land theft, they were assaulted by security forces, said the centre, which monitors Israeli violations in the area. The land is owned by the Greek Orthodox Monastery in Silwan, which is part of the city’s Greek Orthodox Patriarchate.
Silwan is home to more than 60,000 Palestinians and is located strategically to the south of Al-Aqsa Mosque. The area has been the target of Israeli settler expansion for years, with hundreds of Palestinian families facing the threat of expulsion, either through lawsuits by powerful settler groups or administrative eviction orders by the Israeli-run Jerusalem municipality.
Middle East Eye has reported that the Greek Orthodox Church has been criticised heavily by Palestinian groups for its dealings with settlers and allegations of bribery and fraud. In 1951, church-owned land in West Jerusalem was rented to the Jewish National Fund for a period of 99 years. Today, the land houses most Israeli state institutions, including Israel’s parliament, the Knesset.
The Lancet has become a laughing stock
By Norman Fenton and Martin Neil | Where are the numbers? | January 14, 2023
In summary:
- On 6 May 2021 The Lancet published a blatantly flawed study of the effectiveness of the Pfizer covid vaccine on the population of Israel, claiming it was 95% effective.
- On 17 May 2021 we submitted a rapid response 250 word letter explaining why the study was flawed.
- After an initial response saying they would ask the authors for a response to our letter we heard nothing until 20 months later.
- On 8 January 2023 we got an email out of the blue from The Lancet Senior Editor Josefine Gibson apologising for never having got back to us about the letter, saying that they had asked the lead author Dr Sharon Alroy-Preis (SA-P) to respond to our letter but, because she did not provide any formal response, they have decided not to publish our letter.
- We tweeted The Lancet’s response and within 24 hours it got over one million impressions. We also published a substack article highlighting the fact we were now aware of additional problems with the paper relating to SA-P’s relationship with Pfizer.
- On 10 January 2023 we got an unsolicited email from Josefine Gibson (which we can only assume was a result of the reputation hit they got from our tweet) saying “Thank you for bringing your letter from May 2021 back to our attention. We are looking into next steps and will get back to you as soon as we can.”
- On 11 January 2023 (at 10:58) we sent an email to The Lancet’s Editor-in-Chief Richard Horton directing him to our substack article (which highlighted these new problems relating to SA-P’s relationship with Pfizer) stating that The Lancet was clearly taking a credibility hit surrounding the publication of the Israel-Pfizer study and its response to criticisms of it.
- On 11 January 2023 (at 11:21) we got an email from Josefine Gibson apologising for the ‘sub standard experience’ we had with The Lancet. She said that, after discussing it with Horton, they were now inviting us to publish the original letter or an update to it, suggesting the update ‘reflect more current experience with the vaccine’.
- On 12 January 2023 we submitted our updated letter (of an agreed 350 words).
- On 13 January 2023 we got a response from Josefine Gibson saying they had decided against publishing the letter.
Here is the full narrative and January 2023 correspondence in date order (personal details redacted)… continue
Insider reveals truth about Covid-19 pandemic from within the National Health Service
How the misdiagnosis of deaths occurred and was due to changes from 2016
The Naked Emperor’s Newsletter | January 15, 2023
An ex-director at one of the largest hospital trusts in the UK decided they wanted to reveal what really happened during the pandemic. They have kindly allow me to reproduce their thoughts. The catalyst for this revelation, according to the insider, was Dr. Malhotra speaking out about cardiac problems post vaccination.
This is an interesting take on what happened inside the National Health Service (NHS) and confirms, with more details, what we already knew and suspected.
Introduction (Long but important to understand the rest)
In 2016, the British Government proposed & piloted a change to the process of how deaths were certified across all hospitals in the UK. I have attached a link to this Department of Health (DoH) document.
The DoH document proposed a switch to the “Medical Examiner” (ME) System and was sent to a number of different audiences for feedback and consultation. The ME system was already being piloted at two hospitals up north. The results of the consultation are here.
Prior to the Covid-19 Pandemic, the death certification process involved treating doctors of a patient to attend Bereavement Services/Patient Affairs to discuss the death and either:
a) refer the death to the Coroner or
b) write a Medical Certificate of Cause of Death (MCCD).
The MCCD states the cause of death. Whereby a direct cause (1a) or contributing causes (1b) (1c) (1d) are stated along with co-morbidities (not directly causing the death) being written in (2) on the MCCD. The MCCD is only ever a probable cause of death, it is not definitive.
The only definitive way of determining an accurate and plausible cause of death is to refer the deceased patient to HM Coroner (if certain criteria is met), for HM Coroner to accept and take on the case, resulting in a Post Mortem (PM) being conducted by a Histopathologist. When a death is seen as natural and there is nothing untoward, the MCCD is written by the treating doctor of a deceased patient. Usually this is an F1, F2, SHO or Registrar that attends. It is rare for a treating Consultant to attend, but they will finalise the cause of death.
A strict hospital hierarchy exists within the NHS for doctors. It is as follows – from lowest to highest rank: Foundation Year 1 (FY1), Foundation Year 2 (FY2), Senior House Officer (SHO), Registrar (Reg), Consultant, Clinical Lead, Medical Director. Junior doctors will very rarely speak up or challenge their seniors. A senior decision is seen as final and it will be carried out and executed without any hesitance or questioning. In my 5.5 years of experience in End of Life Care, I have only ever seen one junior doctor disagree with a proposed cause of death and challenge their consultant.
With the number of deaths that occur in a hospital, as you can imagine, there is a great deal of variation with regards to causes of death, as we have numerous different doctors writing an MCCD and coming up with various different potential diseases in different orders.
The proposed ME system would change this, as the government would now hire and pay one Medical Examiner, to sit in every hospital and write all MCCD’s for all deceased patients. This would effectively eliminate any variation in causes of death.
In 2016, when I heard of this proposal, I worked as a Bereavement Officer at a hospital in Central London. My mentor/line manager at the time was a former Chief Nurse who managed Bereavement Services and all hospital deaths would be controlled by her and the department.
We essentially carried a huge amount of power with regards to decision making, as we would go through all patient notes following the death of a patient, and essentially guide and advise doctors on what would need to be written with regards to an MCCD or Coroners Referral.
In my personal opinion, our role was to sit on the fence and act in the best interests of a deceased patient (and their families), but also protect the hospital and our doctors from any potential negligence. As you can imagine many battles were fought over decisions about a cause of death of a patient or a referral to the coroner with a vast amount of doctors over the years.
F2’s and SHO’s were particularly the worst with regards to carrying an arrogance of knowing what should be written on an MCCD or stating that a patient didn’t need to be referred to the Coroner (often stating that their Consultant had given them instructions). It is worth noting that Consultants are also only human and can be incorrect at times too. We have to remember that they are succeeded in hierarchy by a Clinical Lead and beyond that a Medical Director. Who have far more experience and knowledge.
When I asked my mentor in 2016, how the ME system would change things, I was told that Bereavement Services/Patient Affairs would become purely administrative and that the clinical judgement would fall to the Medical Examiner.
The power and decision making with regards to MCCD/Coroners Referrals was being taken away not only from treating doctors but also from Bereavement Services/Patient Affairs/Bereavement Officers/Bereavement Service Managers/Directors of End of Life Care.
This decision making power was being handed solely to the Medical Examiner, who has not been involved in the treatment of a patient during an admission. I took all this information in at the time and acquired as much knowledge as I could from my mentor/line manager.
In 2016, I also happened to make a move and take up an opportunity to manage my own Bereavement Services at one of the largest hospital trusts in the whole of the UK. On average, I would oversee MCCD/Coroner Referrals for approx 1750 deaths on an annual basis. I developed a very close working relationship and friendship with one of the Medical Directors (a doctor with the highest ranking in a hospital). This was especially helpful when having to challenge doctors with regards to MCCDs/Coroners Referrals.
Progressing to Director of End of Life Care, I became involved with the reporting of mortality rates, conducting mortality reviews and writing hospital policies. I had also developed an excellent working relationship with the HM Coroner who oversaw our Trust. HM Coroner holds the power to investigate any hospital or trust with regards to a death or a number of deaths. A slight problem may arise, in that HM Coroner has an allegiance to the Crown and the Government.
When a death is reported to the Coroner. This was previously reported via telephone call by the treating doctor. A discussion was had with the Coroners Office and a direct outcome and instruction would come from the Coroner’s Office, by way of HM Coroner (via a phone call).
There is a fundamental flaw to this system, as there is no documentation of the decision and instruction from the Coroner’s. It comes via word of mouth. There is always room for error without any electronic documentation. Every Hospital/Trust & HM Coroner will have a different system of reporting deaths. I personally made a decision to safeguard my hospital and the trust, by developing an electronic coroners referral form, which I proposed to our Coroner and developed after their agreement. We now had documentation of every death being reported and every outcome.
When reporting a death, the Coroner will look at a proposed cause of death and accept it, or reject the cause of death and take on the case (death of the patient), leading to an Inquest or a PM.
In 2019, our Medical Director, came into my office one morning and stated that the Board of Directors at the Hospital had made a decision to switch to the Medical Examiner System. Hearing the words ME system was a massive case of Déjà vu (conversation with my mentor in 2016). I knew exactly what the ME system was, but I chose instead, to play the fool and enquire what exactly the ME system was and what it meant for our service, my staff and our roles. Everything the Medical Director mentioned to me that day was a carbon copy of what I already knew
I knew that my time in End of Life Care had come to an end. I’d reached the top and there was no more progress for me. Losing all power and decision making to any ME coming into the hospital did not appeal to me. I’d already made up my mind that I needed to leave. Seeking a new challenge and experience, I made a move in 2019 to another major hospital in Central London, this time side tracking into operational management. I was in charge of the operational management of Nephrology, Rheumatology, Dermatology and Diabetes & Endocrinology.
2020 – Covid Arrives
In Jan 2020, I remember hearing about the first case of Covid-19 at our hospital, with a patient arriving from China and walking into our A&E. A&E was shutdown and steam cleaned that day, I recollect the moment I heard about this. In my mind, I saw the reporting of Covid-19 in the media as nothing more than Bird Flu or Ebola, which had caused panic but yet passed. I wasn’t worried in the slightest bit.
Things began to escalate around in Feb 2020, around the time I was going on holiday. Due to the reporting by the media, I bought N95 masks as a precaution for my trip and to give to my parents and younger sister. I was blessed to have had an opportunity to spend a few days in Sri Lanka for a wedding and then nearly a whole month in Australia (March 2020). I watched as the narrative of a deadly infectious disease continued to grow with every day that passed. I made a decision to cut my holiday short by a couple of days so that I could make sure I got back to my family and not end up being stranded in Australia.
Upon returning to the UK in late March 2020. One of the immediate things that struck me was the lack of any temperature monitoring or questioning at Heathrow Airport. This seemed odd for a potentially deadly infectious disease that was spreading around the world. This was especially odd, as Sri Lanka & Australia had questioned me/checked temperatures upon arrival, with even Singapore monitoring temperatures during transit.
My mother had just recovered from Cancer, my father was over 70 and my younger sister was born with Down’s Syndrome alongside having multiple other conditions. I had three high risk individuals to Covid-19 in my family and I was scared/fearful of giving them Covid-19. I asked my hospital to allow me to work from home. They refused. I wasn’t deemed high risk, although I lived with my parents at the time. I needed to help my mum and my sister. The hospital held no regard for the safety of it’s employees. They forced me to come into work. I spent two months isolating in my bedroom, I barely came out of my room, for fear of spreading an infectious disease. Never once did I think about the situation or my prior experience or knowledge, I was just reacting to the media frenzy. I was full of panic and stress.
The first irregularity I noticed, was the government and media stating that Covid-19 was an infectious disease. However just before the first lockdown was implemented, I noted that the government had downgraded the status of Covid-19 stating it was no longer infectious. This made no sense to me. Why would we need to isolate if they downgraded the status? My circle of friends contained many medics and dentists. They were all panicking at the time, saying they had inadequate surgical masks and that they needed N95 masks.
N95 masks were seen as the only way to prevent medical professionals from becoming infected with Covid-19. The public being asked to wear surgical masks made no sense to me. The virus would be able to go straight through. Something didn’t seem right.
I ended up meeting and dating an FY1 doctor (my ex gf) around October 2020. We clicked because she was different from every other doctor, I had previously spoken to about Covid-19. She also had her suspicions and believed it wasn’t as infectious as it was made out to be. We both started to slowly realise that Covid-19 was a real disease (as it was showing up on X-rays in patients) but that it wasn’t infectious at all [NE – I have since confirmed with them that they mean not as infectious as was being made out], despite all the reporting in the media.
I needed to experience working in a Covid-19 hotspot and see all the action for myself. In March 2021, I quit my job at the hospital in Central London and took up an opportunity to manage A&E and AMU (Acute Medical Unit) at a hospital in South London. The 6 months that I spent working in A&E/AMU confirmed all my suspicions and culminated in my decision to end my career in the NHS.
The entire 6 months, I was not tested once with a PCR Test, despite walking into wards full of Covid-19 Positive patients on a daily basis. Yet we were required to test multiple times when visiting another country.
The PCR Test that the NHS was using to test patients, is known to have false-positive results. This is shown in numerous studies which can be found online, an example of which is:
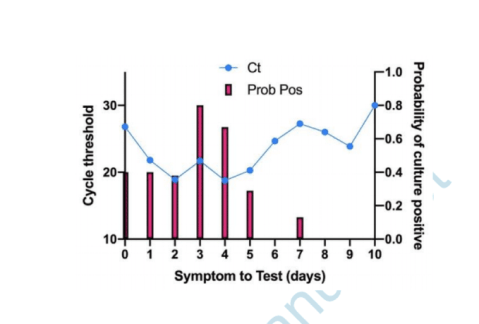
Are you infectious if you have a positive PCR test result for COVID-19? – The Centre for Evidence-Based Medicine.
If a patient tests positive for Covid-19 with a PCR Test, this doesn’t mean they are infected. If tested again, they may well turn out with a negative test. However in the NHS, patients are only tested once and this stays on their record throughout their admission. Hospital policies were changed alongside the implementation of the Medical Examiner System, to ensure that any patient who died within 30 days of positive test, would have to have Covid-19 as their primary cause of death. This was regulated by the Medical Examiner.
The highest cause of death at every hospital per annum pre Covid-19 is Pneumonia. Pneumonia is a Respiratory Disease like Covid-19. Pneumonia can be broken down into 4 different causes of death: Bronchopneumonia, Aspiration Pneumonia, Community Acquired Pneumonia & Hospital Acquired Pneumonia.
These four causes when added together kill the largest number of people on an annual basis prior to the pandemic.
The Medical Examiner (one individual in each hospital), was certifying all these Pneumonia deaths as Covid-19 deaths. When 4 different diseases being grouped and now being called Covid-19, you will inevitably see Covid-19 with a huge death rate.
The mainstream media was reporting on this huge increase in Covid-19 deaths due to the Medical Examiner system being in place. Patients being admitted and dying with very common conditions such as Old Age, Myocardial Infarctions, End Stage Kidney Failure, Haemorrhages, Strokes, COPD & Cancer etc were all now being certified as Covid-19 via the Medical Examiner System.
Hospitals were switching to and from the Medical Examiner system and the Pre Pandemic System as when they pleased. When Covid-19 deaths needed to be increased, the hospital would switch to the Medical Examiner System. Doctors were one week being told they needed to complete an MCCD, to then be told the following week that they weren’t required to fill out an MCCD, as the Medical Examiner was handling this.
Hospitals were incentivised to report Covid-19 deaths over normal deaths, as the government was paying hospitals additional money for every Covid-19 death that was being reported. The Medical Examiner system ensured that Covid-19 was being put down as the cause of death. The government sends out the annual NHS budget to Primary Care Trusts. This is split to fund Hospitals and GP Surgeries. A clinical coding team at each hospital will assign codes to each treatment or death, so that money is paid out to the hospitals.
Any doctor who argued against Covid-19 as a cause of death was bullied and vilified. The General Medical Council maintains a register of all doctors within the UK. This ensures that there is a fear of being struck off for speaking out against an agenda. The GMC effectively controls all doctors in the UK. Even if a doctor realises what is going on and wants to speak out. They will think twice about talking, as they would be risking their entire career and everything that they’ve worked so hard for.
Doctors essentially have their hands tied, many have families, kids, mortgages and mouths to feed. If I was in their situation, I would think twice about speaking out, for fear of being struck off by the GMC and losing everything.
The NHS Track & Trace App, which was introduced to try and control the spread of the virus, did not apply to medical professionals. We were all asked to turn this off, as Doctors and staff isolating for 14 days disrupted patient flow, beds and the discharge of patients.
Any doctor that I spoke to regarding taking the Covid-19 vaccine, were insistent that they were going to wait for a period of time, before taking it themselves, to ensure that it was safe. How is it ethical to give a vaccine to your patients, but not want to take it yourself? In my 12 years of NHS service, never has a doctor pushed or influenced the public to take a vaccine. Yet on social media, I was seeing close friends who were doctors, starting to post on social media that they have taken the vaccine and that the public should. I wouldn’t be surprised if doctors were being forced to promote the vaccine by their superiors or if they were receiving monetary gain in doing so.
I have no doubt in my mind, that the Government has planned the entire pandemic since 2016, when they first proposed the change to medical death certification. Stress leads to disease and illness. Panic leads to people following whatever orders and instructions that are given to them by authority, such as prolonged mask use, which leads to an increase in admissions in to the NHS system due to hypoxia and bacterial pneumonia.
The NHS treatment pathway involved patients being placed onto ventilators. There is a 50% chance of death from this clinical decision alone. How many innocent people have died from the clinical decision to place them onto a ventilator.
During boardrounds (where every admitted patient is discussed), we were seeing patients on a daily basis being admitted due to suffering from adverse affects of taking the vaccine. Patients were blacking out after taking the vaccine or suffering from clots or strokes.
The NHS is all about money and making money. The safety of a patient didn’t seem like the most important thing. It was more about how do we make more beds available so that another patient can be treated. Patients with no next of kin are discharged to nursing homes with care packages. I can’t comment on what happened to these patients in nursing homes, during the pandemic, as I have no experience of their inner workings.
Patients are seen as money, even upon death, hospitals receive money for each death. Is there an actual concern for patient health and safety? I know numerous doctors who are driven primarily by money and monetary gain.
THE REASON WHY I LEFT THE NHS in 2021
56 yr old male, admitted into A&E with end stage kidney failure, has a previous history of regular dialysis treatment for this. No respiratory symptoms on admission and no temperature. However when tested with a PCR Test he unfortunately tests positive. This stays on his record throughout his admission. Our hospital is relatively small in comparison to others I have worked at, we have no dialysis machine as a result. We urgently need to transfer this patient to another hospital otherwise this patient will die. Our treating doctor calls up larger hospitals with a dialysis machine to organise his transfer. All doctors pick up the phone and request the Covid-19 status of the patient. A transfer is declined due to a Covid-19 infection protocol. Our doctors again reiterate the point that this patient will die without dialysis. We are told there is nothing that can be done and that the patient cannot be accepted for transfer.
This gentleman ended up dying without dialysis. Now please tell me what goes on the MCCD….
1a) Covid-19
2) End Stage Kidney Failure
Not written by the treating doctor who disagreed with this cause of death, but by a medical examiner, put in place by the government and the hospital.
When innocent people are being killed by a corrupt organisation and system, for pure monetary gain, I can’t stand by and be part of this anymore. My conscience was clear and I no longer wanted to be a part of this anymore. I am very blessed and lucky that I was in a position to walk away. I’ve been able to speak out, because my hands are not tied and I am not regulated by any organisation or governing body. I believe in speaking the truth and in doing so, I am only just an instrument for God.
I joined the NHS, 12 years ago because I had a desire to help those in need, but the moment I realised that I was not doing this anymore was the time for me to walk away. I apologise to you all if the above thread is confusing with regards to terminology or you cannot understand it’s contents. I’m hoping that at the very least, it can be understood by my fellow medical professionals or by journalists who would like to report the truth.
Who designed global guidelines for puberty blockers?
Free West Media | January 13, 2023
Clinics around the world follow guidelines from the Netherlands for gender treatments in children. The basis for this is, among other things, a much-criticized study sponsored by a German hormone manufacturer.
More and more children and young people believe they have to question their gender identity. Some 60 minors were treated in the Netherlands in 2010, but the number has increased to around 1,600 last year. Another 1,800 people under the age of 18 were on the waiting list because gender clinics in the country are full.
Institutions around the world use a standard procedure developed in Amsterdam in the 1990s when it comes to the drug treatment of supposedly transsexual children.
A report by the Dutch newspaper NRC Handelsblad has meanwhile cast doubt on the directive and the independence of gender research at the Amsterdam UMC hospital. As strict as the conditions for treatment may appear, several complications have been overlooked: The terrible side effects of the heavy drug has been brushed off by doctors as being the lesser evil.
Hormone manufacturer sponsored ‘puberty blocker’ study
The approach with puberty inhibitors has since been known internationally as the “Dutch protocol”. The protocol has become the basis for the “gender-affirming standard of care” used throughout the world. Tens of thousands of children are affected worldwide, and in the Netherlands certainly several hundreds, although no precise figures are available.
Scientists investigated whether hormone treatment in transsexuals is more successful if their puberty was initially suppressed with medication. The sponsor of the study was the German hormone manufacturer.
Ferring Pharmaceuticals, the company that markets the drug Triptorelin as a puberty inhibitor had a strong commercial interest in the outcome. Primarily, treatment relies on administering hormones from the opposite sex: men are given oestrogen to become more feminine, women testosterone to become more masculine. But teenagers are additionally administered puberty inhibitors, which prevent boys from developing a low voice and beard growth and girls from developing breasts and other feminine shapes.
There are many criticisms of the study. Questionnaires were inconsistent, there was no control group at all, and the researchers used random samples from the 196 treated children for the results.
Several countries are moving away from ‘puberty blockers’
In the meantime, there is objection in more and more countries to the treatment of children with “puberty blockers”. Not only are they said to impair the physical sexual development of minors, but they can also cause osteoporosis, anorgasmia and infertility. According to the NRC, the drug is said to sometimes even impair the ability to make rational decisions.
Worldwide, there is increasing criticism of the scientific content and non-existent empirical basis of the Dutch protocol developed at the gender clinic of the Free University of Amsterdam. In several countries, health authorities have already decided to treat children mainly psychologically and prescribe puberty inhibitors only exceptionally. In Sweden, they concluded that “the risks currently outweigh the possible benefits” and spoke of possibly the country’s “worst medical scandal”.
In the UK, criticism of the Dutch protocol was so serious that the Tavistock gender clinic, the largest in the world, was closed by the authorities.
Sweden, Finland and Great Britain only want to prescribe the drug in rare, particularly severe cases. Instead, they are increasingly relying on psychological support for patients.
Since February last year, Sweden’s National Board of Health and Welfare has followed the Karolinska Institute’s policy regarding hormonal interventions for gender-dysphoric minors. Karolinska’s pediatric gender services at Astrid Lindgren Children’s Hospital (ALB) has ended the practice of prescribing puberty blockers and cross-sex hormones to gender-dysphoric patients under the age of 18.
Marketing redundant drugs for the wrong condition
In the US, Texas Attorney General Ken Paxton has been investigating two pharmaceutical companies for advertising puberty blockers to children. This is a condition they are not approved to treat.
In December, Paxton announced investigations under the Texas Deceptive Trade Practices Act into Endo Pharmaceuticals and AbbVie Inc., the two companies that sell puberty blockers. The drugs were approved to treat precocious puberty and forms of prostate cancer but were being marketed and prescribed off-label to treat gender dysphoria.
“These drugs were approved for very different purposes and can have detrimental and even irreversible side effects,” Paxton said. “I will not allow pharmaceutical companies to take advantage of Texas children.”
Republicans Preparing to Move Forward With Ukraine Aid Audit, US Congresswoman Greene Says

Samizdat -13.01.2023
WASHINGTON – US Congresswoman Marjorie Taylor Greene said on Friday that she and other House Republican lawmakers are preparing to move forward with an audit of US aid to Ukraine, an idea first proposed late last year before the House Republican majority took effect.
“We don’t even have committees filled yet but [Congressman Michael McCaul] and I are already preparing to move forward with the audit of Ukraine. No more blank checks to Ukraine,” Greene said via Twitter.
House Republicans are committed to transparency for US taxpayers, Greene added.
In November, Greene and several other House Republicans introduced a resolution to initiate an audit of funds appropriated by Congress to Ukraine. The measure failed during the “lame duck” session of the 117th Congress, but Greene vowed to reintroduce the idea in the new 118th Congress.
House Republicans now hold a majority in the lower chamber, with Speaker Kevin McCarthy having started the party’s mantra of ending “blank checks” from the US to Ukraine. McCarthy also backed the initial Ukraine aid audit proposal.
On Thursday, Pentagon Press Secretary Pat Ryder said that the Defense Department is responsive to oversight by Congress, adding that he looks forward to further bipartisan support for Ukraine.
However, defense budget cuts proposed by the new House Republican majority could force hard questions about funding for foreign operations related to Ukraine and NATO, former Pentagon analyst and retired US Air Force Lt. Col. Karen Kwiatkowski told Sputnik.
Greene has also called for Ukraine to begin negotiations toward a peaceful resolution of the conflict, characterizing it as a “proxy war” between the United States and Russia.
Ivermectin’s Effectiveness Proven Again; 72% Efficacy
800,000 people died in the USA for nothing
By Igor Chudov | January 11, 2023
You are not a horse! You are not a cow! That’s what the FDA told us to dissuade us from taking Ivermectin.

Fortunately, we are also not sheep and did not believe the FDA. Many of us stocked up on Ivermectin, and most found it helpful. While I did not use it when I had my Covid in Nov 2020, it worked great for my wife in Dec 2021 and other family members during the summer of 2022.
Ivermectin, a cheap and safe generic medication, was of little interest to profit-minded pharmaceutical giants like Pfizer and Merck. Therefore, they conspired with the FDA to lie that it did not work and instead pushed expensive Covid vaccines and non-working drugs like mutagenic Molnupiravir and rebound-causing Paxlovid.
MedinCell conducted a randomized controlled trial of their version of Ivermectin and found that it reduces Covid infections by 72%!

The study was very well designed because the participants were EXPOSED to the Covid infection within five days. Given the exposure, the outcomes were more likely to happen and thus were easier to compare between groups, giving the trial greater statistical power.
The 72% reduction in infection is much MORE effective than the “covid vaccine.”
The trial encompassed the period of Mar-Nov 2022, thus giving us the real-world effectiveness of Ivermectin against the Omicron variant.
While I am happy at the finding, there are several things to be NOT happy about.
- If we are to believe official numbers, about 1,121,000 people died of Covid in the USA. Given published effectiveness estimates of Ivermectin coming from honest studies, Ivermectin could have saved eight hundred thousand of those lives. The intentional suppression of Ivermectin cost us so dearly.
- Given a 72% reduction in infection, natural immunity with Ivermectin would likely have stopped the pandemic entirely in 2020.
- Had Ivermectin been recognized as an effective antiviral, the “Covid vaccines” could not get EUA approval, and thus we would avoid thousands of vaccine victims and destroyed immune systems.
- Second-largest Democratic donor and the largest crypto thief Sam Bankman-Fried donated 18 million dollars to the Together trial after it falsely demonstrated a finding that Democrat-aligned Covid vaccine pushers wanted, namely that Ivermectin allegedly was useless.

The good news here is that Ivermectin works.
Here are some of my other articles about Ivermectin — with honest trials showing a comparable reduction in illness and death.
So, thousands of people died of Covid. Thousands of people died of Covid vaccines. The pandemic, prolonged by vaccination, is raging and reinfects people with immunity disabled by mystery genetic treatments. My prediction from last March, unfortunately, is coming true.
AIDS-Like “Chronic Covid” is Taking Over Europe, Australia and NZ
All of this happened because of the recklessness and greed of the biomedical-industrial complex, which developed Sars-Cov-2 and then pushed an unproven, ineffective vaccine that worsened the pandemic.
While the above paragraph is upsetting, the good news is that Ivermectin was validated, and “we have the tools” to manage a Covid infection or exposure.
Lastly, take a minute to think about millions of victims of suppression of Ivermectin worldwide, who died to make a few companies and foundations richer and more powerful.
Will Ivermectin ever be recommended officially? And do we even care about such approval if we can still order it online?
Featured Video
Epidemic of fake videos
or go to
Aletho News Archives – Video-Images
Free Book
Vicious
Lies are Unbekoming | January 25, 2026
The waiting room is clean. The receptionist is polite. The forms ask reasonable questions. Nothing in the physical environment suggests danger. The magazines are current. The hand sanitizer dispenser works. Someone has chosen calming colors for the walls.
A pregnant woman sits in a chair designed for her comfort. She has been told to be here. Not ordered—no one orders. Recommended. Strongly recommended. Everyone does this. Her mother did this. Her friends did this. The women in her prenatal group compare notes about their appointments the way they compare notes about nursery furniture. Which provider did you choose? What tests have you had? The questions assume the answers. The answers assume the questions.
She will be offered things today. Offered is the word used. The offers will come with information sheets that list risks and benefits in tabular form. She will sign consent documents. Everything will be voluntary in the legal sense. No one will hold her down. No one will threaten her. She will choose, and her choices will feel like choices, and she will leave feeling she has done the responsible thing.
What she will not feel is the weight of what has been arranged before she arrived. … continue
Blog Roll
Recent Comments
loongtip on Vicious loongtip on EU turns to India for defense… Coronistan on Donald Trump Is No Peace … seversonebcfb985d9 on French court jails pro-Palesti… eddieb on Fourteen Incredible Facts Abou… Bill Francis on European leaders’ shift in the… seversonebcfb985d9 on Villains of Judea: Philip Esfo… loongtip on Report warns that ‘Jewish terr… Craig Nelms on New study shows that toxic gas… loongtip on A Funny Thing Happened on the… loongtip on EU free trade pact on hold as… John Edward Kendrick on Regime Change In Iran Is The F…
 Aletho News
Aletho News- The Board For Peace – Whitewashing Ethnic Cleansing and Genocide
- Scientists accuse Cochrane Reviews of using biased studies to claim HPV vaccine prevents cancer
- Spain Opens Probe Into Israeli Tourism Firms
- Epidemic of fake videos
- Craig Murray, Reporting from Venezuela
- Why Israel’s Drive to Destroy Iran is Ultimately about Palestine
- Trump and Iran, War or Negotiations?
- US pressure contributing to Israeli influence in Latin America: Experts
- China Rejects U.S. Claims of Coercion in Central America
- New US defense strategy downgrades Russian ‘threat’
- If Americans Knew
- Greenpeace Demonstrator Exposes Folly of Protest Restrictions
- From CBS to TikTok, Pro-Israel Ellison is now in the driver’s seat
- Israel pays for UK advertisements attacking Doctors Without Borders
- Israel accused of extracting billions from Gazan people to pay for their own genocide
- ‘Deliberate Assassination’: 3 Journalists Among 11 Killed by Israeli Forces in Gaza
- In Gaza, We’re Struggling to Reintroduce Foods to Bodies Adjusted to Starvation
- Will Rafah crossing be opened at last? – Not a ceasefire Day 108
- Israeli drone strike kills two children collecting firewood in Gaza – Not a ceasefire Day 107
- Another Gaza baby freezes to death on Netanyahu’s watch – Not a ceasefire Day 106
- Oppose Israel’s Abuses While You Still Can
- No Tricks Zone
- New Study Affirms Rising CO2’s Greening Impact Across India – A Region With No Net Warming In 75 Years
- Germany’s Natural Gas Crisis Escalates … One Storage Site Near Empty …Government Silent
- Polar Colding…Antarctica Saw Its Coldest October In 44 Years!
- New Study: Sea Levels Rose 20 Times The Modern Rate During The Roman Warm Period
- As German Gas Storage Dips Dangerously Low…Shortage Hardly Avoidable
- New Study: Brazil’s Relative Sea Level Was 2+ Meters Higher And SSTs 3-4°C Warmer 6000 Years Ago
- Philosopher Schopenhauer: Climate Science Certainty Stems From Stupidity, Ignorance
- New Study: Species Extinction Rates Declining Since 1980 – ‘Climate Change Is Not An Important Threat’
- Denmark Places Climate Protection Above Animal Welfare, Poisoning And Culling Cows
- New Study: Greenland Was 3-7°C Warmer And Far Less Glaciated Than Today 6000-8000 Years Ago
