Climate Change Brings Record Breaking Threat To Health – Lancet
By Paul Homewood | Not A Lot Of People Know That | November 3, 2024

Yes, it’s the same old pack of lies they roll out every year, trying to convince that global health is suffering because of climate change.
You only have to read the first paragraph to understand that this is a political document, not a serious scientific one.
And sure enough, they claim to have found “record-breaking threats” to health and even survival:
Each year is the same – they ignore real world data, which positively shows the opposite to be true, and instead concoct increasingly obscure and dubious ways to satisfy their agenda.
The idea, of course, that the world’s climate has changed so much since 2015 is itself absurd – but that does not stop the Lancet from saying it has!
They start by claiming that heat-related deaths have increased since the 1990s, but there is no mention of the fact that cold-related deaths have decreased by many more. They claim that heat exposure has reduced labour productivity, forgetting that, thanks to mechanisation, productivity has rocketed and workers are therefore less exposed to heat stress.
They claim that extreme precipitation has increased since 1960, but this is not derived from real world data, which is far too sparse to make such bold claims. Instead it is all based on computer modelling.
To be fair, the IPCC also claim that the number of heavy rainfall events has been increasing, but significantly also tell us that they can find no global trends in floods. In many places heavy rainfall is welcomed because it alleviates drought. Try telling the Indians that they had too much rainfall during this summer’s monsoon. As for those who suffered during the Dust Bowl years in the US, they would have given their right arm for a few storms.
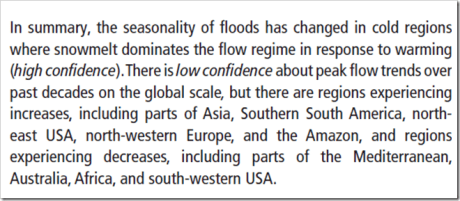
IPCC AR6
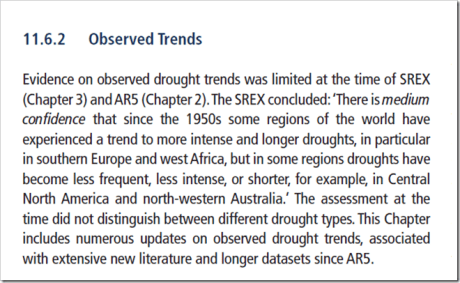
It is the same with drought. Apparently 48% of the world’s landmass was affected by at least 1 month of extreme drought last year, up from 15% in the 1950s. But droughts build up over a period of months and even years, not one single month. It is plainly ridiculous to use such a metric – I wonder why they did?
And as with extreme precipitation, the Lancet study does not use actual rainfall data, but computer models which can be programmed to come up with any results you want, because the real world data they would need simply does not exist for most of the world.
But where we do have actual precipitation data, the IPCC only find that although some regions have seen an increase in droughts, while others have seen fewer:
And so it goes on. Apparently there are more sand storms, but again this is gleaned from computer models, a “state-of-the-art multimodel reanalysis ensemble”.
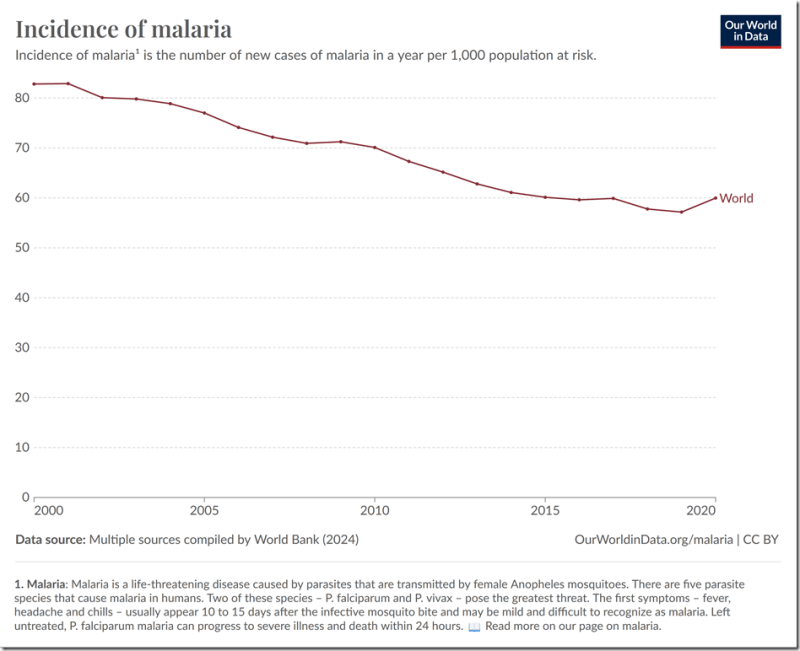
Malaria, we are told, is being spread by global warming, despite the fact that the number of new cases has been steadily dropping, with the exception of COVID affected 2020:
But the biggest joke of all must be this:
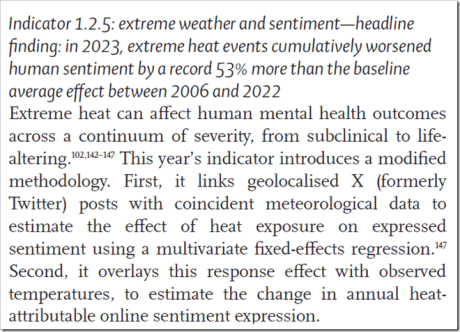
The mind boggles!
If they really were concerned about global health, there is plenty or incontrovertible, real world data which they could use, instead of their phoney models.
Around the world people live longer, child mortality is much lower, fewer live in extreme poverty or are undernourished. They live healthier lives, thanks to better access to clean water, medicines and healthcare. The children are better education, and technology is transforming people’s lives.
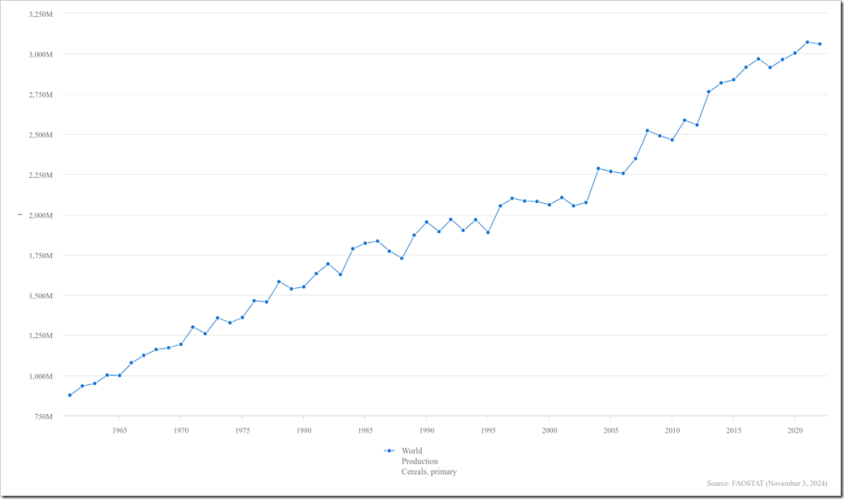
Thanks mainly to fossil fuels food output hits new records year after year. Meanwhile in contrast to the Lancet’s claims of desertification, the planet is greening because of increasing amounts of CO2 in the atmosphere.
But the Lancet are not interested in the truth, nor for that matter do they appear to care about global health.
They only want to generate alarmist headlines, to push forward their Net Zero agenda.
The Lancet heavily redact their response to our subject access request for internal correspondence relating to rejection of our letter about Pfizer study
What have they got to hide?

By Norman Fenton and Martin Neil | Where are the numbers? | March 14, 2023
There has been a remarkable development to the story previously reported here.
Following that fiasco, I submitted a subject access information request to Elsevier (who publish The Lancet ) asking for all internal correspondence between editors and reviewers relating to the submission (and ultimate rejection) of our letter.
After a lengthy delay I received the response today. First their cover letter:
And the very lengthy response (but massively redacted – by them). Here:
It is remarkable that most of the details are redacted even though it clearly is not done solely for the legitimate protection of the names of third parties. It is clear that I was being discussed in a negative light as they were referring to me as ‘an ongoing issue’. It is also clear that they only reached out after I publicised their initial delayed rejection letter on twitter (they were getting a lot of heat as a result of that).

It is disturbing to realise how much effort was spent in an attempt to ensure that an obviously flawed study promoting the Pfizer vaccine was not challenged.
Despite most of it being redacted there are still some alarming unredacted highlights (imagine what the redacted stuff says about us!) First they seem to reluctantly concede that I have a legitimate academic appointment:
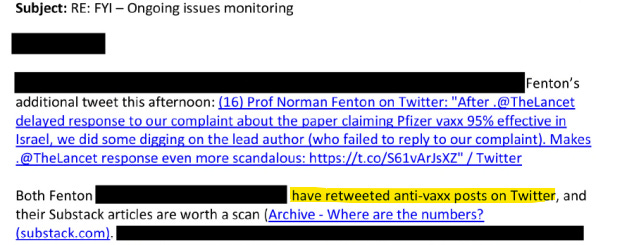
In the following they mention ‘helpful background on Fenton’. Did they try to dig up dirt on me on their own or did the 77th brigade furnish them with my dossier?
They are worried about the close proximity of vaccine misinformation sources!

Next, they accuse me and (most likely) Martin Neil of retweeting ‘anti-vaxx posts on Twitter’. I’d be interested to know precisely who they are referring to and what posts:
They also refer to ‘holding off further email’ suggesting their offer to consider the letter was not genuine:

![]()
I am not happy about the scale of the redactions in the Elsevier response. If the Lancet editors were not making disparaging comments about me and colleagues, then there should be no reason to redact them. What do they have to hide?
The redactions suggest Elsevier have not acted in good faith, and neither have they acted in the spirit of FOIA.
Hence, I have informed Elsevier that if they are unable to provide a proper and full response with most of these comments unredacted, I will have no choice but to report them to the Information Commissioner’s Office (ICO).
This is not the first disgraceful episode in the recent history of the Lancet where, under Richard Horton’s leadership, clearly flawed papers promoting the ‘official narrative’ on covid have been published. Remember LancetGate when they published a fraudulent study that effectively stopped the use of hydroxychloroquine (HCQ) to treat covid patients. At least that paper was eventually retracted. In this case, rather than even allow a proper response to a flawed study, they have instead attacked their critics, accusing them of being spreaders of misinformation and ‘anti-vaxxers’.
It is worth noting that (as shown here), The Lancet is by no means the only major academic journal routinely rejecting any articles/letters that in any way question the accuracy of studies claiming vaccine effectiveness or safety. It is now fair to conclude that not a single major peer-reviewed study claiming vaccine effectiveness and/or safety can be trusted to be valid.
The Lancet has become a laughing stock
By Norman Fenton and Martin Neil | Where are the numbers? | January 14, 2023
In summary:
- On 6 May 2021 The Lancet published a blatantly flawed study of the effectiveness of the Pfizer covid vaccine on the population of Israel, claiming it was 95% effective.
- On 17 May 2021 we submitted a rapid response 250 word letter explaining why the study was flawed.
- After an initial response saying they would ask the authors for a response to our letter we heard nothing until 20 months later.
- On 8 January 2023 we got an email out of the blue from The Lancet Senior Editor Josefine Gibson apologising for never having got back to us about the letter, saying that they had asked the lead author Dr Sharon Alroy-Preis (SA-P) to respond to our letter but, because she did not provide any formal response, they have decided not to publish our letter.
- We tweeted The Lancet’s response and within 24 hours it got over one million impressions. We also published a substack article highlighting the fact we were now aware of additional problems with the paper relating to SA-P’s relationship with Pfizer.
- On 10 January 2023 we got an unsolicited email from Josefine Gibson (which we can only assume was a result of the reputation hit they got from our tweet) saying “Thank you for bringing your letter from May 2021 back to our attention. We are looking into next steps and will get back to you as soon as we can.”
- On 11 January 2023 (at 10:58) we sent an email to The Lancet’s Editor-in-Chief Richard Horton directing him to our substack article (which highlighted these new problems relating to SA-P’s relationship with Pfizer) stating that The Lancet was clearly taking a credibility hit surrounding the publication of the Israel-Pfizer study and its response to criticisms of it.
- On 11 January 2023 (at 11:21) we got an email from Josefine Gibson apologising for the ‘sub standard experience’ we had with The Lancet. She said that, after discussing it with Horton, they were now inviting us to publish the original letter or an update to it, suggesting the update ‘reflect more current experience with the vaccine’.
- On 12 January 2023 we submitted our updated letter (of an agreed 350 words).
- On 13 January 2023 we got a response from Josefine Gibson saying they had decided against publishing the letter.
Here is the full narrative and January 2023 correspondence in date order (personal details redacted)… continue
MEDICAL FASCISM IN THE LANCET
By David Bell and Domini Gordon | PANDA | August 28, 2022
Medical ethics is about protecting society from medical malfeasance and the self-interest of the humans whom we trust to manage health. It is therefore disturbing when prominent people, in a prominent journal, tear up the concept of medical ethics and human rights norms. It is worse when they ignore broad swathes of evidence, and misrepresent their own sources to do so.
On July 8th 2022, The Lancet published a ‘Viewpoint’ article online: “Effectiveness of vaccination mandates in improving uptake of COVID-19 vaccines in the USA.” The article, which acknowledges the controversial nature of vaccine mandates, primarily concludes that coercing people to take a medical product, and reducing options for refusal, increases product uptake.
It further concludes that the best way to implement such mandates is for employers and educational institutions to threaten job security and the right to education.
The use of coercion goes against the established ethics and morals of Public Health, and could be argued to be anti-health. In this case, the article justifies it by stating that “the current evidence regarding the safety of COVID-19 vaccines in adults is sufficient to support mandates.” However, it offers scant evidence to back this assertion, and ignores all evidence to the contrary. They apparently consider the ability to work and support a family, or gain formal education, as something that is to be granted or taken away, not a human right.
The Lancet was once a credible journal with a rigorous policy of peer review. However, in this article it appears to have dropped its former standards, promoting medical fascism (coercion, threat and division to achieve compliance with authority) without insisting on a rigorous evidence base to justify such an approach. This suggests an attempt to normalize such approaches in mainstream public health.
Past experience has shown us where fascism behind a façade of public health can lead. The sterilization campaigns aimed at coloured and low-income populations of the US Eugenicist era, and the extensions of similar programs under Nazism in 1930s and 1940s Europe, relied heavily on the normalization of such approaches.
Leading public health voices from Johns Hopkins School of Public Health and other institutions championed a public health approach of sanitizing populations rather than environments, encouraging the idea of a tiered society where health ‘experts’ determine the rights and medical management of those deemed less worthy.
Avoiding the discomfort of evidence
The authors of this Lancet paper, ranging from academics and medical consultants to the daughter of a prominent politician, attempt to rewrite human rights in medicine as if precedent never existed. Their argument for coercion in mass vaccination recognizes that ‘vaccine mandates,’ whether issued by governments, employers or schools, all involve a loss of rights. No serious attempt is made to provide a medical justification for mass vaccination with a non-transmission-blocking vaccine.
The paper focuses on the premise that coercion, commonly considered a form of force, makes humans do things they would not otherwise do. Banning fellow humans from making their own health choices on pain of loss of normal participation in society has an impact on increasing vaccine uptake. This is hardly a revelation to any thinking human, but clearly important enough to justify publication in The Lancet.
The article links to evidence of vaccine mandates used for state school entry that show higher compliance when the right of religious and personal belief exemption is removed, or where onerous requirements for exemptions are put in place. Leaving ethical questions aside, the obvious lack of similarity between the authors’ predicate childhood vaccinations that block transmission and COVID-19 vaccines that have minimal impact on transmission, and may even promote it, is ignored. The one mandated adult vaccine predicate referenced in the article, the influenza vaccine, provides only a 2.5% reduction in pneumonia ‘when the (mandated) vaccine was well matched to circulating strains’ in the reference quoted.
When raising the sacking of non-vaccinated workers, the authors seem comfortable with the approach but coy in admitting its consequences. Their admission that “a few large US employers have terminated hundreds of workers for non-compliance references an article in Money magazine which actually paints a bleaker picture, characterizing it as a ‘great resignation.’
The authors will also have been aware of mass layoffs by large employers such as New York City (over 9,000 sacked or placed on leave), the US Department of Defense (DoD, which sacked 3,400), Kaiser Permanente (laid off 2,200), and the tens of thousands of staff lost from the UK care-home sector . Extrapolated across countries and society to actually provide credible data may have been too uncomfortable for the authors and Lancet editors.
High efficacy and safety are an obvious (though on their own, insufficient) prerequisite for any mandated product. This entire area of safety is dealt with by stating; “The current evidence on the safety of COVID-19 vaccines in adults is sufficient to support mandates,” supported by a single study comparing vaccinated individuals 1-3 weeks and 3-6 weeks post-vaccination, revealing low levels of myocardial infarction, appendicitis and stroke.
The claim that “widespread administration in adults has quickly generated a large evidence base supporting the vaccines’ safety, including evidence from active surveillance studies” suggests that both the authors and The Lancet are unaware of the VAERS and Eudravigilance databases set up for exactly this purpose. No mention is made of growing data on myocarditis, menstrual irregularities, or the excess all-cause mortality and severe outcomes in vaccinated groups in the Pfizer randomised control trials on which the FDA emergency registration was based. Were The Lancet’s reviewers unaware of these sources?
The sole reference to vaccine efficacy discusses COVID-19 ventilated patient outcomes, It ignores the period to 14 days post-previous dose that Pfizer acknowledges can be associated with immune suppression. Fenton et al. have noted that classing a vaccinated person as unvaccinated in the first 14 days post-injection has profound impacts on vaccine effectiveness data.
Ignoring the awkwardness of reality
Post-infection immunity in the unvaccinated is a threat to arguments for mandates. The authors disingenuously state that “evidence suggests that the immunity produced by natural infection varies by individual, and that people with previous infection benefit from vaccination. New variants further undercut the case for adequacy of previous infection.
Two references are used here: one from a study in Qatar and the other a study from Kentucky. The Qatar study finds that “the protection of previous infection against hospitalization or death caused by reinfection appeared to be robust, regardless of variant,” whilst the Kentucky study found Covid reinfection was reduced by vaccination over a 2-month period in the months soon after vaccination, prior to the waning and then reversal of this protection as demonstrated in studies of longer duration elsewhere.
The vast breadth of evidence on relative effectiveness of post-infection immunity is ignored. Either the authors failed to read their references and are unaware of waning and of the vast literature on post-infection immunity, or they do not consider demonstration of efficacy important for coerced medical treatments.
In a previous era, or in a previously credible medical journal, an argument for coercion to support a medical procedure would have required very high standards of evidence of efficacy and safety. It is arguing for the abrogation of fundamental principles such as informed consent that are at the core of modern medical ethics. Failure to address well-known contrary data should prevent an article from even reaching the peer-review stage.
Degrading public health degrades society
We are left with a paper stating that coercion is a good path to increase compliance for a product that does not reduce community infection risk, and has potentially serious side effects. Ignoring both of these aspects of COVID-19 vaccines is a poor approach to justifying mass vaccination. The sole nod to any human rights concern – “Some objectors argue mandates represent undue encroachment on individual liberty” – is an interesting way to characterize removal of the right to income, education and the ability to socialize with others.
Although all these rights are recognized under the Universal Declaration for Human Rights, the authors and The Lancet consider them insufficiently serious to dwell upon.
Public health has been down this road before. We have seen the path society takes when basic public health principles are subverted to achieve an aim that some perceive as ‘good.’ We have also seen how most health professionals will comply, however horrific the actions involved. There is no reason to believe that this round of medical fascism will end differently.
We rely on medical journals such as The Lancet to apply at least the same standards to the purveyors of such doctrines as they do to others and demand a rational and honest evidence base. Anything less would raise legitimate questions as to the role the journal is taking in promoting these doctrines, and their place in a free, evidence-based and rights-respecting society.
David Bell, Senior Scholar at Brownstone Institute, is a public health physician and biotech consultant in global health. He is the former Program Head for malaria and febrile diseases at the Foundation for Innovative New Diagnostics (FIND) in Geneva, Switzerland.
Domini Gordon is Open Science and Open Society Coordinator at Panda.
CDC-funded study concludes most COVID vaccine reactions ‘mild’ yet VAERS data show thousands of deaths, hospitalizations
By Madhava Setty, M.D. | The Defender | March 9, 2022
A study funded by the Centers for Disease Control and Prevention (CDC) and published Monday in The Lancet concluded most COVID-19 vaccine-related adverse events reported during the first six months after the vaccines were rolled out in the U.S were “mild and short in duration.”
For the study, researchers analyzed data captured between Dec. 14, 2020, and June 14, 2021, by two reporting systems, the Vaccine Adverse Event Reporting System (VAERS) and v-safe, both of which are overseen by the CDC. Nearly 300 million doses of COVID vaccines were administered during the study period.
The authors found that of the 340,522 adverse events reported to VAERS, 27,023 (8%) were serious, 4,496 of which were deaths.
The U.S. Food and Drug Administration (FDA) defines a Serious Adverse Event (SAE) as an outcome that is life-threatening or one that results in hospitalization (immediate or prolonged), permanent injury, birth defect or death.
Authors suggest vaccines didn’t cause deaths
As an event capturing system VAERS is not designed to attribute causation. However, the authors noted that there was a “… concentrated reporting of deaths on the first few days after vaccination..”
The temporal relationship of the death to the time of vaccination was demonstrated here:

The correlation in time between inoculation and death is highly suggestive of causation. Instead, the authors chose to explain it as follows:
“This pattern might represent reporting bias because the likelihood to report a serious adverse event might increase when it occurs in close temporal proximity to vaccination.”
The authors suggest that if a death occurs soon after vaccination it will be more likely reported than if the death occurred later. This, they believe, is why the number of deaths asymptotically approaches zero as more time elapses since inoculation.
Independent researcher unable to duplicate study’s VAERS findings
Jessica Rose, Ph.D., attempted to duplicate the Lancet authors’ findings through her independent analysis of the VAERS data.
Despite filtering the database using three different date stamps (Vaccination Date, Onset Date and Received Date), none returned the number of reports published in the Lancet.
From her analysis:
“The closest I got to their estimate when I filtered using the RD (Received Date) data was 371,775.
“For the VD (Vaccination Date) data filter I got 545,275 reports and for OD (Onset Date) data filter I got 499,432 reports.”
In other words, using every date option, Rose found tens (sometimes hundreds) of thousands more reports than the authors of the Lancet study found.
The most conservative number, 371,775, is still nearly 30,000 more than reported. Nevertheless, using the Received Date as the date filter still returned 6,114 deaths — 36% more than the CDC study claimed.
Furthermore, Rose’s most conservative search parameters returned 68,124 SAEs, or three times more than the Lance study.
Rose said she believes using the Received Date field will unavoidably lead to an undercount of actual reports because this field is left blank more often than the other timestamps in a given record.
How can this large difference be reconciled?
One clue is Pfizer’s “Cumulative Analysis of Post Authorization Adverse Event Reports,” a document released through a Freedom of Information Act request submitted in August 2021, by the Public Health and Medical Professionals for Transparency.
In it, approximately 50% of adverse events reported to Pfizer were SAEs. The adverse events tabulated in this document were passively reported, as they are in VAERS. This further suggests that the authors of the Lancet report may have undercounted SAEs for an unexplained reason.
What about the v-safe findings?
The authors reported separately on their analysis of v-safe data.
V-safe is an active reporting system. Enrolled participants are contacted by phone and are asked to complete a survey. Active surveys are expected to return more complete data. Subjects agree to enroll voluntarily.
Of the 5,674,420 vaccinated subjects that received a second dose and responded through the v-safe system, 26.5% reported they were unable to do normal activities at the time of survey completion.
Additionally, 16.1% were unable to work, 0.9% received medical care and 2,053 were hospitalized.
Is the data ‘reassuring?’
Reporting on the Lancet study, MedPage wrote:
“In an accompanying editorial, Matthew Krantz, MD, and Elizabeth Phillips, MD, both of Vanderbilt University School of Medicine in Nashville, Tennessee, characterized the report as ‘reassuring,’ noting that, ‘there were no unexpected signals other than myopericarditis and anaphylaxis, already known to be associated with mRNA vaccines.’”
Krantz and Phillips stated myopericarditis and anaphylaxis were “unexpected” signals but were already known to be a problem.
Nonetheless, the Lancet study found that the incidence of myopericarditis and anaphylaxis were 4.4 and 5.5 per million vaccine doses administered respectively.
Yet coagulopathies (clotting disorders including pulmonary embolism), seizures, strokes and Bell’s Palsy (paralysis of the facial nerve) all occurred at higher incidence rates than myopericarditis according to the Lancet study.
Why aren’t these considered unexpected signals to be further investigated or at least acknowledged?
Anaphylaxis, though reported at an incidence of 5.5 per million in the Lancet study, is known to occur at a much higher rate from COVID vaccines.
In a paper published in March 2021, anaphylaxis following COVID vaccines was found to occur at a rate of 250 per million. These findings are a foundational argument for the existence of a significant and calculable underreporting factor (URF) with regard to all events reported in VAERS.
Steve Kirsch estimated the URF to be approximately 41. It is not possible to know what the URF is for every adverse event. Nevertheless, the 4,496 deaths reported in the Lancet are most likely grossly under-representative of the true number of vaccine-related fatalities.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Sen. Johnson Requests Records From Top Medical Journals on Retracted Studies, Including Flawed HCQ Study
The Defender | December 21, 2021
Sen. Ron Johnson (R-Wis.) has written to The Lancet and The New England Journal of Medicine seeking records on two retracted studies from mid-2020. Johnson particularly called out The Lancet study, which suggested hydroxychloroquine could boost the risk of death in COVID patients.
“Although this fraudulent study was ultimately retracted, it is concerning and shameful that, in the midst of a pandemic, The Lancet published such a misleading paper on a potential early treatment for COVID-19,” said Johnson, the ranking member on the Permanent Subcommittee on Investigations, in a letter dated Dec. 14.
Johnson seeks all records of the journals’ communication on the two studies, including communication with the papers’ authors; U.S. government employees; individuals who encouraged the studies’ publication; and the supplier of the two studies’ datasets, Surgisphere, a healthcare analytics company.
Despite The Lancet paper’s retraction, its initial publication halted trials on hydroxychloroquine’s use and sullied its reputation more broadly. The Washington Post and other major media headlined the increased risk of death, and health authorities took action globally within days of the paper’s publication.
The World Health Organization and the UK’s drug regulator halted trials of the drug in COVID settings. France reversed an earlier decision to allow hydroxychloroquine’s use in COVID patients.
Readers of The Lancet quickly noted the study cited implausibly high numbers of COVID cases in 2020, and journalists failed to find any hospitals that had contributed data, despite the study’s claim that more than 96,000 hospital patients participated.
The Lancet retracted the study two weeks after publication.
Sen. Johnson also requested information from The New England Journal of Medicine (NEJM) on another study retracted in June 2020.
Johnson explained in his letter, the NEJM paper reportedly found that “taking certain blood pressure drugs, including angiotensin-converting enzyme (ACE) inhibitors, didn’t appear to increase the risk of death among COVID-19 patients, as some researchers had suggested.”
However, the study’s authors wrote to the NEJM a few weeks after the study was published, acknowledging they could not validate the primary data supporting the study and apologized “to the editors and to readers of the Journal for the difficulties that this has caused.”
Johnson has requested all records by Jan. 4, 2022.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Journal Rebuked for Publishing Biased Letter Signed by EcoHealth President
By Dr. Joseph Mercola | October 2, 2021
In July 2021 and February 2021 the medical journal The Lancet printed letters signed by 24 scientists, physicians, epidemiologists and virologists that denied the possibility that SARS-CoV-2, the virus that causes COVID-19, originated in a lab.
One of those signers was Peter Daszak, president of EcoHealth Alliance, which received grant funds from the National Institute of Allergy and Infectious Diseases (NIAID) for gain-of-function research. The information on Daszak’s, EcoHealth Alliance’s and the NIAID’s involvement in research that possibly could have led to a lab origin was revealed in late-summer, 2021.
Previously, any suggestion that a lab leak could have occurred was resoundly proclaimed a conspiracy theory.
But now, in a rebuke of The Lancet for allowing the letters to be published when there “is so far no scientifically validated evidence that directly supports a natural origin,” 16 other scientists are calling for The Lancet to “open their columns to in-depth analyses of all hypotheses.”
“As scientists, we need to evaluate all hypotheses on a rational basis, and to weigh their likelihood based on facts and evidence, devoid of speculation concerning possible political impacts” they add. “More importantly, science embraces alternative hypotheses, contradictory arguments, verification, refutability, and controversy. Departing from this principle risks establishing dogmas, abandoning the essence of science, and, even worse, paving the way for conspiracy theories.”
SOURCES:
Lomborg criticizes medical journals for alarm about climate change
clintel.org
Danish scientist Bjorn Lomborg has reacted sharply on the claim of over 200 medical journals, earlier this month, that there are significant health risks to any temperature rise. He concludes that there are very basic mistakes underlying the alarmist claims and sent the following letter to the editor of The Lancet, one of the journals involved. Lomborg posted his letter on twitter.
Below the full letter.
Malmö, September 8, 2021
Dear Dr. Horton,
I read with interest your co-authored editorial “Call for emergency action to limit global temperature increases, restore biodiversity, and protect health” published in BMJ (2021;374:n1734) and many other international journals. As a core argument you write that there are significant health risks to any temperature rise and document it with “In the past 20 years, heat related mortality among people aged over 65 has increased by more than 50%.” However, this mortality increase [i] is a simple count, not a rate. The overwhelming part of the increase is due to the fact that the global population of people aged over 65 increased more than 40% in the same time period. Indeed, the increase in heat mortality rate is a much lower 9.4%. I am sure you agree that making a causal claim without adjusting for a dramatically changed population is fundamentally unsound. In fact, I am positive that you and your journal would demand a rewrite of any paper making such an argument. It is analogously flawed to claiming that Brexit led to better health for the European Union because total deaths overnight dropped 600,000 per year when the UK left. Given the enormous attention that your paper received, I therefore reach out to you to hear what action you will take to ensure that this unsound argument is rectified.
Yours truly,
Bjorn Lomborg President, Copenhagen Consensus, and Visiting fellow, Hoover Institution at Stanford University
I hope it might be useful to visualize the issue.
Below, the left box illustrates your editorial’s claim that temperature rises have increased the number of heat deaths of people aged 65+ by 53.7% while disregarding a 40% increase in the relevant population. The middle box shows the rate of heat deaths for the same population group, which takes into account the rapid increase in the population. I hope you will also find the right box interesting: it compares the heat deaths (which are slowly rising) with the much greater risk from cold deaths (declining much faster) from the Global Burden of Disease study. It highlights the problem with only looking at more heat death but neglecting the much greater fall in cold deaths.

This result is comparable with a new Lancet study that shows global warming increased heat deaths of all deaths by 0.21% (from 0.83% in 2000-03 to 1.04% in 2016-19) and decreased cold deaths by 0.51% (from 8.70% to 8.19%).[ii]
[i] Your reference is indicator 1.1.3, which shows a 53.7% increase in heat mortality from 165,000 annual deaths in 2000-04 to 253,000 annual deaths in 2014-18, from “The 2020 report of The Lancet Countdown on health and climate change: responding to converging crises” in the Lancet (https://doi.org/10.1016/S0140-6736(20)32290-X).
[ii] Table S5&6, “Global, regional, and national burden of mortality associated with non-optimal ambient temperatures from 2000 to 2019: a three-stage modelling study” Lancet Planet Health 2021; 5:e415–25.
Lancetgate: why was this “monumental fraud” not a huge scandal?
By Daniel Espinosa | Dissident Voice | August 20, 2020
A high-profile and highly influential scientific study regarding the potential of hydroxychloroquine (HCQ) to treat Covid-19 patients was retracted among suggestions of fraud back in June. The research in question was headed by a renowned Harvard professor called Mandeep Mehra and published by The Lancet, the most prestigious medical journal in the world.
It concluded that the antimalarial drug used since the 1950´s was actually killing Covid-19 patients by inducing heart failures. It caused quite a stir. (Brief historical fact: the Quina tree, the source of quinine and its family of medications, is also the “national tree” of Peru).
Soon after the publication of the study (22 May), the World Health Organization (WHO) halted all research being conducted on hydroxychloroquine, which included simultaneous testing in 17 countries. The worldwide influence of the scientific paper – and the fact that hundreds of doctors were already trying the drug in Covid-19 patients – led a lot of researchers to look closely into it, immediately finding an alarming level of incoherence.
In the meantime, the news was spread far and wide by the corporate media, many times in a highly politicized fashion. They swiftly convinced the world of the danger of treating the symptoms of Sars-Cov-2 with HCQ.
In the realm of social media, a wave of censorship against dissenting voices soon followed. A viral video showing a group of physicians called the Frontline Doctors, speaking publicly in favor of HCQ – by sharing their own clinical experience – was removed by most social media giants (but only after millions had already watched it). Could a testimony taken from a physician’s own experience be called “false”? Of course! Today a handful of social media corporations control what we can say or hear.
Instead of informing their audiences with a balanced discussion about all the scientific research conducted so far regarding the drug, both positive and negative, corporate media directed a barrage of ad-hominems and smear toward the mentioned doctors. An army of “fact-checkers” was opportunely deployed after that to police the web and reassure everyone that HCQ is both useless and dangerous. Everyone who said otherwise was snake oil peddler.
But regardless of its massive political effect, the study wasn’t a particularly well-crafted fraud to begin with. A couple of weeks after the publication, The Lancet received a letter from more than a hundred physicians and researchers, jointly demanding a review of the study and the disclosure of the raw data used in it. When the company providing such data – Surgisphere – refused to relinquish it for independent inquiry, three of its four authors retracted the paper.
Dr. Sapan Desai was the one who didn’t retract it, as he is (or was) the owner of Surgisphere and the provider of the data. It was allegedly obtained from 96,000 patients in hundreds of hospitals from five continents, a presumption that, according to many experts, should’ve immediately raised eyebrows. An expert in data integration projects told The Guardian that a database like the one Desai is said to own was “almost certainly a scam”.
Surgisphere’s website, just like Dr. Desai himself, vanished soon after the fraud was revealed, while its few employees, among them an adult content model and a sci-fi writer, appear to be no more than part of a façade.
Among the observations made to the retracted paper by the researchers were these pearls: “A range of gross deviations from standard research and clinical practices”; “gross misrepresentation of the numbers of (Covid-19) deaths in Australia”. The data was not only very hard to obtain, due to very different country laws and levels of development, it showed suspiciously similar tendencies despite focusing on very dissimilar regions of the Earth.
According to Science magazine, it was the presence of Mandeep Mehra which gave the study the “gravitas” needed to be published in a medical journal as The Lancet. He did retract it and apologize as soon as the news about the refusal to open the data was out. Mehra and Desai were introduced to one another by a third researcher, Dr. Amit Patel, who also participated in the retracted paper. Patel and Desai are also brothers-in-law.
Edward Horton, The Lancet’s editor in chief, said that the whole thing was a “monumental fraud”. A Bostonian research scientist writing for The Guardian, James Heathers, called it “the most important retraction in modern history”. Heathers correctly pointed out that “studies like this determine how people live or die tomorrow”. Sadly, “saving people’s lives” is also used as a justification for giving dubious science a free pass in times of emergency.
Despite the fact that the malign influence of private interests in science research and medicine is quite well-known and documented today, the few corporate news outlets that covered “Lancetgate” decided not to look into the obvious…
A world of conflicts of interest
In opposition to the coverage given to the original study, its retraction wasn’t as widely and swiftly publicized by the mainstream press. In fact, other than The Guardian, only a few news media covered this historic scientific embarrassment in any depth.
When they did, they rarely went beyond mentioning “data concerns”. But that could be understood as anything from a computer virus destroying part of the data to legitimate human error. Not many hints were given to the readers to let them suspect a deliberate and outright fraud, much less one rooted in conflicts of interest.
The spin given to the news was not much about why or how it happened – how reputed scientists and The Lancet were fooled by fake data – but mostly about how bad it looked for everyone and how the need for remedies for the pandemic was driving scientists and regulatory bodies to bypass important scrutiny.
A New York Times op-ed went deep into the problems in the peer review system, a process both “opaque and fallible”, going as far as to acknowledge a “politicization of the pandemic”, but it failed miserably by not informing its readers of one of the reasons why peer review might fail: conflicts of interest.
Where’s the relationship between this incident and the pervasive role of Big Pharma’s money in academia, science and politics?
The many flaws quickly pointed out by more than a hundred scientists didn’t make the press question how a reputed and seasoned researcher like Harvard’s Mehra was so easily fooled, and then The Lancet and its peer review system. The Guardian didn’t look deep, or at all, into potential conflicts of interests involving the researchers in question and Big Pharma.
As you probably know already, the way pharmaceutical giants make their money is through patents – the monopoly to market a certain drug for a certain time – and hydroxychloroquine lost any patent it had decades ago. As Marcia Angell wrote in 2002:
Patents are the lifeblood of the drug industry. Without a patent, a company has no incentive to bring a drug to market.
As the Alliance for Human Research Protection correctly pointed out, “… mainstream media carefully avoid asking the… overriding question, lest the magnitude of science fraud is laid bare”.
And the question regarded specific and flagrant conflicts of interest. The independent media didn’t miss it. As Professor Michel Chossudovsky wrote for Global Research (June 10):
The Lancet acknowledges that the study received funding from the William Harvey Distinguished Chair in Advanced Cardiovascular Medicine at Brigham and Women’s Hospital which is held by Dr. Mandeep Mehra. In this regard, it is worth noting that Brigham Health has a major contract with Big Pharma’s Gilead Sciences Inc., related to the development of the Remdesivir drug for the treatment of COVID-19. The Gilead-Brigham Health project was initiated in March 2020.
The mandatory question right after acknowledging Gilead’s relationship with said Hospital, one that the corporate media could never dare ask, also made by Prof. Chossudovsky, is if the fraudulent study was made “to provide a justification to block the use of HCQ”?
The reason behind this mainstream media omission could be found in the billions of dollars the pharma industry spends in advertising, the “lifeblood” of corporate news, which predisposes them to naivety and simple-mindedness regarding possible conflicts of interest. Seems logical, they are in the exact same spot as the researchers who take Big Pharma money and then are supposed to pass objective judgment about their products and questionable role in society.
Add to that the fact that media and pharmaceutical corporations share interlocking directorates. As FAIR.org reported back in 2009, media names like The New York Times or NBC share directors with companies like Eli Lilly or Merck, respectively.
A consequence of decades of conflicts of interest corrupting traditional media is that today most people are dangerously uninformed of the risks of letting the group of corporations that comprise Big Pharma, and their hedge fund shareholders, wield its power over both governments and science. Even today, many people are prone to call Big Pharma influence a “conspiracy theory”.
The mere idea that Big Pharma’ influence could be swaying what is being said and done politically and in the realm of corporate media, regarding the Cov-Sars-2 pandemic and potential remedies, is utterly outrageous! The fact that they spend as no other industry in government lobbying and media advertising doesn’t seem to matter because, well, how could Big Pharma be worried about anything else but our health in these times of great despair… right?
In fact, both Big Media and Big Pharma are motivated by profit, and they are partners in crime, as members of the latter have been “repeatedly convicted of marketing harmful—often fatal—drugs; substantial fraud; price manipulation; and concealment of evidence.”
Their managers are legally forced to enrich their shareholder masters without regards for “externalities”, like an opioid overdose crisis. A pandemic is seen by these huge psychopathic entities just as a once in a lifetime opportunity to plunder. A desperate consumer is a great costumer, especially when Gilead, Novartis, AstraZeneca and the rest of the bunch can spend his or her taxes in disproportionally expensive remedies because they own the government bodies made to regulate them.
Advertising money is the reason why a critical look into this world of conflicts of interests is completely absent from mainstream media, even if “progressive” as The Guardian.
In addition to this, you have probably heard a lot lately about how fake news and conspiracy theories are a “threat to democracy”, or how they “undermine traditional institutions”. Well, giving wide coverage to a fraud involving top Western scientists and doctors, using the most important medical journal ever known to the effect of discarding a cheap drug with no patents and a potential competitor for expensive pharma company products, can produce some serious “undermining” of public trust.
We should end this article by quoting some worried –and sometimes pessimistic– scientific authors. Among them the editors or former editors of The Lancet and The New England Journal of Medicine.
“A turn to towards darkness”
Regarding the nefarious role of commercial conflicts of interest in science, Marcia Angell, quoted above, also wrote this in 2009:
It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as editor of The New England Journal of Medicine (NEJM).
Recently (not under Angell’s editorship), the NEJM –second in prestige only to The Lancet– also published and retracted research by Mehra and Desai.
The editor of The Lancet, Dr. Richard Horton, also seems to have lost faith in what is nowadays called scientific research:
The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness.
Are we going back to the Dark Ages, or are we there already? In France, the former Health Minister, Philippe Douste-Blazy, leaked an extraordinary anecdote from a private reunion he had with the editors of The Lancet, other journals and experts, to French news medium BFMtv.
According to Douste-Blazy, Richard Horton (The Lancet) literally said:
If this continues, we are not going to be able to publish any more clinical research data because pharmaceutical companies are so financially powerful today, and are able to use such methodologies as to have us accept papers which are apparently methodologically perfect, but which, in reality, manage to conclude what they want to conclude.
“When there is an outbreak like Covid, in reality, there are people like us – doctors – who see mortality and suffering… and there are people who see dollars. That’s it,” admitted the French physician.
Daniel Espinosa Winder lives in Arequipa, second largest city of Peru. He graduated in Communication Sciences in Lima and started researching propaganda and mainstream media. He writes for a peruvian in print weekly, “Hildebrandt en sus trece” since 2018. His writings are a critique of the role of mass media in society”.
“Deadly” Hydroxychloroquine (HCQ) to treat Covid 19: How the World’s Top Medical Journals, The Lancet and NEJM, Were Cynically Exploited by Big Pharma
By Elizabeth Woodworth | Global Research | June 14, 2020
Abstract and Background
A publishing scandal recently erupted around the use of the anti-malarial drug hydroxychloroquine (HCQ) to treat Covid 19. It is also known as quinine and chloroquine, and is on the WHO list of essential medicines.[i]
The bark of the South American quina-quina tree has been used to treat malaria for 400 years.[ii] Quinine, a generic drug costing pennies a dose, is available for purchase online. In rare cases it can cause dizziness and irregular heartbeat.[iii]
In late May, 2020, The Lancet published a four-author study claiming that HCQ used in hospitals to treat Covid-19 had been shown conclusively to be a hazard for heart death. The data allegedly covered 96,000 patients in 671 hospitals on six continents.[iv]
After the article had spent 13 days in the headlines, dogged by scientific objections, three of the authors retracted it on June 5.[v]
Meanwhile, during an expert closed-door meeting leaked May 24 in France, The Lancet and NEJM editors explained how financially powerful pharmaceutical players were “criminally” corrupting medical science to advance their interests.
*
On May 22, 2020, the time-honoured Lancet [vi]– one of the world’s two top medical journals – published the stunning claim that 671 hospitals on six continents were reporting life-threatening heart rhythms in patients taking hydroxychloroquine (HCQ) for Covid-19.
The headlines that followed were breath-taking.
Although wider access to the drug had recently been urged in a petition signed by nearly 500,000 French doctors and citizens,[vii] WHO and other agencies responded to the article by immediately suspending the clinical trials that may have cleared it for use.
North American headlines did not mention that HCQ has been on the WHO list of essential drugs since the list began in 1977. Nor did they mention an investigative report on the bad press that hydroxychloroquine had been getting prior to May 22, and how financial interests had been intersecting with medicine to favour Gilead’s new, more expensive drug, Remdesivir.[viii]
The statistics behind the headlines
As a Canadian health sciences librarian who delivered statistics to a large public health agency for 25 years, I sensed almost immediately that the article had to be flawed.
Why? Because health statistics are developed for different purposes and in different contexts, causing them to exist in isolated data “stovepipes.”[ix] Many health databases, even within a single region or country, are not standardized and are thus virtually useless for comparative research.
How, I wondered, could 671 hospitals worldwide, including Asia and Africa, report comparable treatment outcomes for 96,000 Covid patients? And so quickly?
The Lancet is strong in public health and surely suspected this. Its award-winning editor-in-chief, Dr. Richard Horton, has been in his job since 1995.[x]
So how could the damning HCQ claims have been accepted? Here is what I discovered.
The honour system in medical publishing
To some extent, authors submitting articles to medical journals are on the honour system, in which cited databases are trusted by the editors, yet are available for inspection if questioned.[xi]
On May 28, an open letter from 200 scientists to the authors and The Lancet requested details of the data and an independent audit. The letter was “signed by clinicians, medical researchers, statisticians, and ethicists from across the world.”[xii]
The authors declined to supply the data, or even the hospital names. Meanwhile, investigative analysis was showing the statistics to be deeply flawed.[xiii][xiv]
If this were not enough, the lead author was found to be in a conflict of interest with HCQ’s rival drug, Remdesivir:
“Dr. Mandeep Mehra, the lead co-author is a director at Brigham & Women’s Hospital, which is credited with funding the study. Dr. Mehra and The Lancet failed to disclose that Brigham Hospital has a partnership with Gilead and is currently conducting two trials testing Remdesivir, the prime competitor of hydroxychloroquine for the treatment of COVID-19, the focus of the study.”[xv]
In view of the foregoing, the article was retracted by three of its authors on June 5.
How did this fraud get past The Lancet reviewers in the first place?
The answer emerges from what has remained an obscure French interview, although it has been quoted in the alternative media.[xvi]
On May 24, a closed-door Chatham House expert meeting about Covid included the editors-in-chief of The Lancet and the NEJM. Comments regarding the article were leaked to the French press by a well-known health figure, Dr. Philippe Douste-Blazy,[xvii] who felt compelled to blow the whistle.
His resulting BFM TV interview was posted to YouTube with English subtitles on May 31,[xviii] but it was not picked up by the English-speaking media.
These were The Lancet editor Dr. Richard Horton’s words, as reported by Dr. Douste-Blazy:
“If this continues, we are not going to be able to publish any more clinical research data because pharmaceutical companies are so financially powerful today, and are able to use such methodologies as to have us accept papers which are apparently methodologically perfect, but which, in reality, manage to conclude what they want to conclude.” [xix]
Doust-Blazy made his own comments on Horton’s words:
“I never thought the boss of The Lancet could say that. And the boss of the New England Journal of Medicine too. He even said it was ‘criminal’. The word was used by them.”[xx]
The final words in Doust-Blazy’s interview were:
“When there is an outbreak like Covid, in reality, there are people like us – doctors – who see mortality and suffering. And there are people who see dollars. That’s it.”[xxi]
The scientific process of building a trustworthy knowledge base is one of the foundations of our civilization. Violating this process is a crime against both truth and humanity.
Evidently the North American media does not consider this extraordinary crime to be worth reporting.
Notes
[i] World Health Organization. “World Health Organization Model List of Essential Medicines, 21st ed.”, WHO, 2019, pp. 24, 25, 53 (https://www.who.int/medicines/publications/essentialmedicines/en/).
[ii] Jane Achan, et al., “Quinine, an old anti-malarial drug in a modern world: role in the treatment of malaria,” Malaria Journal, 24 May 2011 (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3121651/).
[iii] WebMD, “Quinine Sulfate” (https://www.webmd.com/drugs/2/drug-869/quinine-oral/details).
[iv] The Lancet, “RETRACTED: Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: a multinational registry analysis, by Mandeep R. Mehra et al,” Lancet, 5 June 2010 (https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31180-6/fulltext).
[v] Ibid.
[vi] Famous weekly British medical journal, founded in 1823.
[vii] Lee Mclaughlan, “Covid-19 France: petition for wider chloroquine access,” 6 April 2020 (https://www.connexionfrance.com/French-news/Time-wasted-over-use-of-choroquine-coronavirus-drug-says-petition-by-former-French-health-minister).
[viii] Sharyl Attkisson, “Hydroxychloroquine,” Full Measure, 18 May 2020 (https://www.youtube.com/watch?v=zB-_SV-y11Y). Attkisson is a five-time Emmy Award winner (https://en.wikipedia.org/wiki/Sharyl_Attkisson).
[ix] See “Stovepiping,” (https://en.wikipedia.org/wiki/Stovepiping) (accessed June 12, 2020).
[x] Dr. Horton’s career, professionalism, and awards are shown at https://en.wikipedia.org/wiki/Richard_Horton_(editor)(accessed June 12, 2020).
[xi] The Lancet and NEJM editors could not be expected to comb through data from 671 hospitals to verify their accuracy – especially when submitted by four doctors.
[xii] The full-text letter and signatories appear at https://zenodo.org/record/3862789#.XuQiNmYTGhM
[xiii] Melissa Davey, “Questions raised over hydroxychloroquine study which caused WHO to halt trials for Covid-19,” The Guardian, 28 May 2020 (https://www.theguardian.com/science/2020/may/28/questions-raised-over-hydroxychloroquine-study-which-caused-who-to-halt-trials-for-covid-19).
[xiv] Melissa Davey et al, “Surgisphere: governments and WHO changed Covid-19 policy based on suspect data from tiny US company,” The Guardian, 3 June 2020 (https://www.theguardian.com/world/2020/jun/03/covid-19-surgisphere-who-world-health-organization-hydroxychloroquine).
[xv] 1. Alliance for Human Research Protection, “The Lancet Published a Fraudulent Covid-19 Study,” 2 June 2020 (https://ahrp.org/the-lancet-published-a-fraudulent-study-editor-calls-it-department-of-error/).
- Brigham Health, “Two Remdesivir Clinical Trials Underway at Brigham and Women’s Hospital,” 30 March 2020 (https://www.brighamhealthonamission.org/2020/03/26/two-remdesivir-clinical-trials-underway-at-brigham-and-womens-hospital/).
[xvi] Vera Sharav, “Editors of The Lancetand the New England Journal of Medicine: Pharmaceutical Companies are so Financially Powerful They Pressure us to Accept Papers,” Health Impact News, 5 June 2020
[xvii] Dr. Philippe Douste-Blazy, MD, is a cardiologist, former French Health Minister; 2017 candidate for Director at WHO; and former Under-Secretary-General of the United Nations. See also: https://en.wikipedia.org/wiki/Philippe_Douste-Blazy.
[xviii] “(Eng Subs) Hydroxychloroquine Lancet Study: Former France Health Minister blows the whistle,” BFM TV, 31 May 2020 (https://www.youtube.com/watch?time_continue=2&v=ZYgiCALEdpE&feature=emb_logo).
[xix] Ibid.
[xx] Ibid.
[xxi] Ibid.
Copyright © Elizabeth Woodworth, Global Research, 2020
Retracted Papers Written by Journal VIP
By Donna Laframboise | Big Picture News | June 17, 2020
The lead author of two retracted COVID-19 papers is editor-in-chief of an Elsevier medical journal.

Earlier this month, two high-profile research papers were retracted on the same day. One, published in The Lancet, had concluded that coronavirus patients treated with malaria drugs were more likely to die. Published on May 22, it was officially withdrawn 13 days later.
Another, published in the New England Journal of Medicine, found no evidence that widely prescribed medications increase the death rate of hospitalized COVID-19 patients with pre-existing heart problems.
The lead author in both instances was Mandeep Mehra, a professor of medicine at Harvard Medical School, and the person in charge of the Heart and Vascular Center at Boston’s Brigham and Women’s Hospital.

The second listed author was Sapan Desai. An online bio describes him as an “internationally-recognized double board certified vascular surgeon.” Desai is the founder of Surgisphere Corporation, a data analytics firm which claimed to have acquired 96,000 highly-detailed electronic medical records of COVID-19 patients from 671 hospitals on six continents.
The Lancet paper’s dramatic findings interrupted drug trials and changed government policy in multiple countries. It also increased the anxiety of coronavirus patients who’d been participating in those trials.
But six days after the paper appeared, more than 100 “clinicians, medical researchers, statisticians, and ethicists” addressed an open letter to the authors, and to Lancet editor-in-chief Richard Horton, questioning the integrity of the cited data.
Why were the hospitals which supplied this data not identified? Why weren’t standard statistical practices employed? Why no ethics review? Why didn’t the paper invite other researchers to examine for themselves the underlying data and computer code?
According to these experts, the medication dose sizes discussed were odd, drug ratios sounded “implausible,” the Australian data was obviously erroneous, and the African data seemed “unlikely.”
Yet none of The Lancet‘s peer-reviewers apparently noticed. “In the interests of transparency,” said the signatories of the open letter, “we also ask The Lancet to make openly available the peer review comments that led to this manuscript to be accepted for publication [sic].”
An article in the New York Times says these events “have alarmed scientists worldwide who fear that the rush for research on the coronavirus has overwhelmed the peer review process.” Lancet editor Horton, it reports, now describes the retracted paper as a “fabrication” and “a monumental fraud.”
A headline in the UK Guardian says The Lancet has made one of the biggest retractions in modern history. How, asks the article that follows,
did a paper of such consequence get discarded like a used tissue by some of its authors only days after publication? If the authors don’t trust it now, how did it get published in the first place?…the sad truth is peer review in its entirety is struggling…
Neither of those articles mentioned an astonishing fact. Lead author Mehra is himself the editor-in-chief of The Journal of Heart and Lung Transplantation. Part of Elsevier’s scholarly publishing empire, this monthly journal hires editors for five-year terms. Mehra’s second term is coming to end, and last year the search for a replacement began.
As the posted job description explains, the editor-in-chief is responsible for overseeing the peer review of papers submitted to that journal. He or she is constantly evaluating research, sorting solid science from weak science. The new editor-in-chief, we’re told, must have “a demonstrated understanding of statistics and statistical methods.”
So how could a man who has spent the past 10 years in such a role have authored this pair of retracted papers? How could anyone with any statistical sophistication have taken such dodgy data at face value?
“No matter which way you examine the data, use of these [malaria] drug regimens did not help,” Mehra declared in a press release when The Lancet paper was published. But it now appears he didn’t directly examine the data at all. On the day the paper was retracted, he explained in a subsequent statement:
Dr. Desai, who served as a co-author and whose team maintained this observational database, conducted various analyses. As first author, these were provided to me, and on the basis of these analyses, we published two peer-reviewed papers…
In other words, this longtime editor-in-chief took someone else’s word for it. He failed to ask elementary questions. He took it on faith that the analyses had been properly conducted. Mehra continued:
It is now clear to me that in my hope to contribute this research during a time of great need, I did not do enough to ensure that the data source was appropriate for this use. For that, and for all the disruptions – both directly and indirectly – I am truly sorry.
This, ladies and gentlemen, is the vaunted peer review system in action. Naive trust. Blind faith. By Mehra. By The Lancet. By the New England Journal of Medicine. Even when real lives, right now, hang in the balance.
Four years ago, I authored a report demonstrating that peer review is merely a sniff test. Typically performed by unpaid volunteers, it’s based on wholly subjective criteria, and is highly influenced by the pre-existing beliefs of those doing the reviewing. My report contains this paragraph:
In 2014, Science announced measures to provide deeper scrutiny of statistical claims in the research it publishes. John Ioannidis, the author of a seminal 2005 paper asserting that most published research findings are false, called this announcement “long overdue”. In his opinion, statistical review has become more important than traditional peer review for a “majority of scientific papers”.
In many places, statistical review still doesn’t occur. Even in our current situation, when COVID-19 research has the power to halt drug trials and change history, the vetting process at medical journals is a joke.
Featured Video

John Mearsheimer: Ukraine Is Landlocked & Donbas Enters Endgame
or go to
Aletho News Archives – Video-Images
From the Archives
There are ZERO Amish kids suffering from cancer, diabetes or autism – WHY IS THAT?
YourDestinationNow | July 8, 2023
The current population of Amish folks in America is quickly approaching 400,000, with the largest concentrations of 90,000 in Pennsylvania and 82,000 in Ohio. Amish have settled in as many as 32 US states, and have an average of 7 kids per family, so the population is growing rapidly. In a brand new, comprehensive study (as of June 2023), presented by Steve Kirsch to the Pennsylvania State Senate, it was calculated that for Amish children, who are strictly 100 percent not vaccinated (fully unvaccinated), typical chronic conditions barely exist, if any at all. … continue
Blog Roll
 Aletho News
Aletho News- Saudi Arabia preps for ‘major’ land, sea operations against Ansarallah in Yemen: Report
- Iran Army hits US base in Kuwait as satellite images show fresh damage
- BRICS+ Series: Why the Egypt-UAE Energy Partnership Signals a New Phase for the Global South
- Was the Drone Attack on US LNG Tanker in Egypt a False Flag?
- Drone Strike on Egypt, War Widens /Lt Col Daniel Davis & Matt Bracken
- Pfizer Freezes Air Traffic Control Funds Over COVID Vaccine Contract Dispute With Poland, Romania
- Mafia buying up some of 800,000 weapons missing from Ukraine – Italian prosecutors
- NATO deploys Italian, Spanish, Turkish jets to eastern flank
- From Tehran to Riyadh: How Israel Draws the Red Lines America Can’t Cross
- Iran warns Bulgaria against hosting US warplanes, secures assurances from Cyprus on base neutrality
- If Americans Knew
- Were the first Zionists Christian? A review.
- Ben Gvir’s crocodiles are the latest weapon in Israel’s animal warfare on Palestinians
- CIA Assessment Details Israel’s Race to Make the U.S.-Israel Alliance Irreversible
- How much is your support for Israel worth? Try $1 billion.
- Israeli Media: Israel’s Defense Chief Is Enabling Jewish Terror
- Why the New York Times story on Mossad recruiting Ahmadinejad doesn’t add up
- The Facts on ICC’s Karim Khan’s Dismissal after Court’s Arrest Warrant for Netanyahu
- By 22-Point Margin, Americans Think Netanyahu Should Be Arrested on US Soil
- What an Israeli settler pogrom feels like
- As Gaza draws closer to possible ceasefire, Netanyahu draws closer to Trump – Daily Update
- No Tricks Zone
- Germany’s Industrial Suicide… Grid Agency Prepares Secret Power Rationing Plans Amid Electric Power Bottlenecks
- ECMWF Models Throwing Cold Water On Extreme Germany Heat Wave Forecast Next Week
- Greenland’s Ice Sheet Was Supposed To Be Rapidly Melting Away. It Hasn’t Been.
- Global Temperature Trend Has Cooled Over The Past 6500 Years, Scientists Have Found
- Wind Energy Means Going Back To The Middle Ages, Says German Professor Horst-Joachim Lüdecke
- New Study: A 40-Fold Increase In Earth’s Main Greenhouse Gas Contributes To Cooling The Ocean
- New Study Highlights The ‘Dominant Role’ Of Aerosol/Cloud Interactions In Shaping Climate
- Munich’s First-Ever Green Party Mayor Declares First Ever City Water Use Restrictions… Fines Up to 50,000 €!
- Experimental Lab Research: The Climate Sensitivity To A 400-Fold Increase In CO2 Is 0.1°C
- Fatal Snobbery: In France, It’s Better To Die From A Heatwave Than To Do As Americans
