The Three Big Lies about Mammography Screening
By Peter C. Gøtzsche | Brownstone Institute | March 6, 2026
I dedicate this article to all women invited to mammography screening and those who love them because the public has consistently been lied to, for over 40 years. In invitations to screening, women have been told that by detecting cancers early, screening saves lives and leads to less invasive surgery.1,2 I shall demonstrate that all three statements are wrong.
Women are still being told these lies, by professional associations, screening advocates, screening researchers, cancer charities, and national boards of health.3-5 The American Cancer Society declares in a headline that “Mammography Saves Lives”4 and claims, with no references, that results from many decades of research clearly show that women who have regular mammograms are less likely to need aggressive treatments like surgery to remove the entire breast (mastectomy).5
Screening Does Not Save Lives
In the randomised trials of mammography screening, the risk ratio for overall mortality after 13 years of follow-up was 0.99 (95% confidence interval 0.93 to 1.03) for those trials with adequate randomisation.6 The estimate happened to be the same for the other trials, some of which were so poorly randomised that the average age in the two compared groups was not the same, which makes an analysis of overall mortality unreliable.
For two of the three adequately randomised trials, those from Canada and the UK, there are follow-up data after 25 and 23 years, respectively.7,8 The risk ratio for overall mortality was 1.01 (95% confidence interval 0.98 to 1.03) for all three trials (both with a fixed effect and a random effects model, Comprehensive Meta Analysis Version 3.0). In the table, the year means the year the trial started:
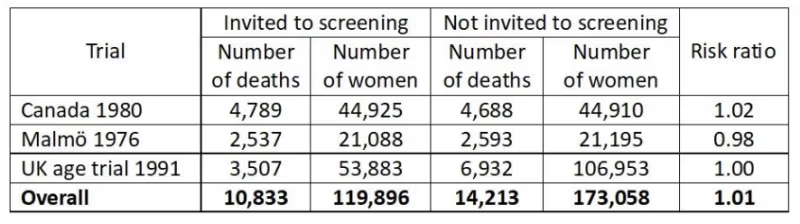
This is a very strong result as it is derived from a total of 25,046 deaths. We can therefore say with great confidence that mammography screening does not save lives.
If we restrict the analysis to the two trials with a very long follow-up, the result is the same, a risk ratio of 1.01 (0.99 to 1.04).
Breast Cancer Mortality Is a Seriously Flawed Outcome
It will surprise most people to learn that we cannot trust what has been reported in the randomised trials about the effect of screening on breast cancer mortality but this is an objective fact.6
A minority of the women who died were autopsied, and in several trials, cause of death was not assessed blindly.6 I have documented that assessment of cause of death was seriously biased.6,9 If we include all trials in the analysis, we would expect to see the greatest reduction in breast cancer mortality in those trials that were most effective in lowering the rate of node-positive cancers (cancers that had metastasised) in the screened group.
This was indeed the case, but the regression line was in the wrong place. It predicts that a screening effectiveness of zero (i.e. the rate of node-positive cancers is the same in the screened groups as in the control groups) results in a 16% reduction in breast cancer mortality (95% confidence interval 9% to 23% reduction).6,9 This can only happen if there is bias, and further analyses showed that assessment of cause of death and of the number of cancers in advanced stages were both biased in favour of screening.
Systematic reviews that include all the trials, also the poorly randomised ones, have reported that mammography screening reduces breast cancer mortality by 16-19%.6,10 As this estimate is of the same size as the bias in the regression analysis, this suggests that screening does not lower breast cancer mortality.
Another reason why breast cancer mortality is a flawed outcome is that screening leads to overdiagnosis, which is the detection of cancers and precursors to cancer (carcinoma in situ), which would not have come to the attention of the woman in her remaining lifetime and therefore would not have become a problem without screening. Since it is not possible to distinguish between harmless cancers and dangerous ones, they are all treated, and radiotherapy and chemotherapy given to women who are healthy increase their mortality.6
If we take into account the cardiac and lung cancer deaths caused by the type of radiotherapy used when the screening trials were carried out and generously assume that screening reduces breast cancer mortality by 20% and results in only 20% overdiagnosis of healthy women, then there is no mortality benefit from screening.11
Finally, it is noteworthy that the most unreliable trials were those that reported the greatest reductions in breast cancer mortality.6 The difference in the effect estimates between the adequately randomised trials and the poorly conducted trials was statistically significant, both after 7 and 14 years of follow-up (P = 0.005 and P = 0.02, respectively).12
Total Cancer Mortality
Since misclassification of cause of death often concerns deaths from other cancers,6 total cancer mortality is a less biased outcome than breast cancer mortality.
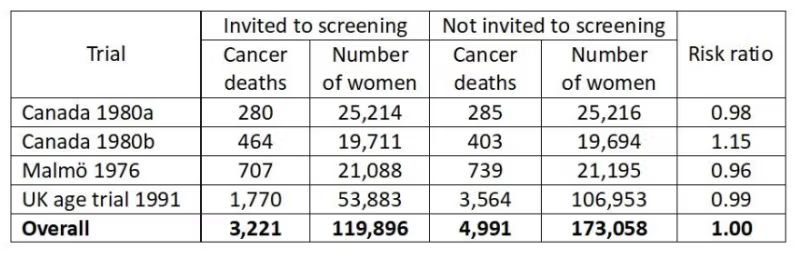
Some trialists have not reported what the total cancer mortality was but we have data from the three adequately randomised trials.6,8 There was no effect of screening on total cancer mortality, including breast cancer, risk ratio 1.00, 95% confidence interval 0.96 to 1.04. There were two different age groups in the Canadian trial, 40-49 (a) and 50-59 years (b):
Since total cancer mortality is less biased than breast cancer mortality, it is of interest to see what the expected cancer mortality (including breast cancer mortality) would have been if the reported reduction in breast cancer mortality of 29% after 7 years in the poorly randomised trials6 were true.
It would have been a risk ratio of 0.95, which is significantly lower (P = 0.02)6 than what was actually found. This provides further evidence that assessment of cause of death was biased in favour of screening.
Breast Cancer Is Not Detected Early but Very Late
If we assume that the observed doubling times in longitudinal tumour studies are constant from initiation till the tumour becomes detectable, the average woman has harboured the cancer for 21 years before it acquires a size of 10 mm and becomes detectable on a mammogram.13
Given this large time span, it is misleading to call it “early detection” also because the effect of screening is trivial, namely to advance the diagnosis by less than a year.13
Yet all authorities repeat this mantra. As it is impossible that everyone working with cancer is unaware of the basics of tumour biology, we can draw the conclusion that the public all over the world is being misinformed. This is fraud because it is deliberate and because women think “early detection” will save their lives.
I once asked a famous tumour biologist, Keld Danø, during a coffee break at an international meeting, whether he agreed with me that it was impossible to lower breast cancer mortality by 30% with screening, based on our knowledge of tumour biology.14 He agreed. When I asked why people like him didn’t participate in the scientific debate, he didn’t reply and it is not difficult to imagine why. It is not wise to point out that your colleagues are wrong when you are on the receiving end of major funds from a cancer charity that touts screening.
The women suffer while everyone else prospers.
The earliest cell changes, carcinoma in situ, are not detected unless the women get a mammogram. In our systematic review of countries with organised screening programmes, we found an overdiagnosis of 35% for invasive cancer and 52% when we included carcinoma in situ.15
Although less than half of carcinoma in situ cases progress to invasive cancer,16,17 the women are nevertheless routinely treated with surgery, drugs, and radiotherapy.
The deep irony is that the surgery is often mastectomy because the cell changes may be diffusely spread in the breast, and sometimes even in both breasts. In New South Wales, one-third of women with carcinoma in situ had a mastectomy,18 and in the UK, carcinoma in situ was more often treated by mastectomy than invasive cancer,19 and the number of women treated by mastectomy almost doubled from 1998 to 2008.20
This brings us to the third big falsehood in the propaganda about mammography screening.
Screening Does Not Decrease but Increases Mastectomies
Because of the substantial overdiagnosis of invasive cancer and carcinoma in situ, and because screening only advances detection of invasive cancers slightly,13 it is inevitable that screening increases mastectomies.
In the randomised trials of screening, we found 31% more mastectomies in the screened groups than in the control groups.6
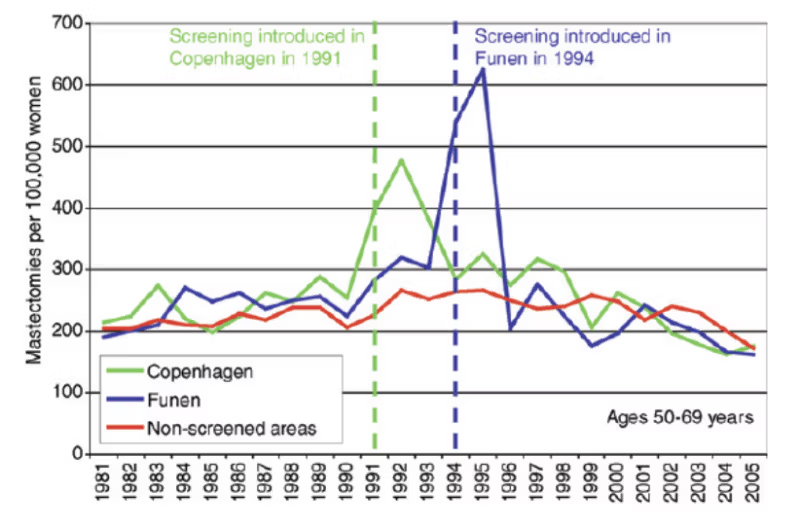
Denmark is a unique country to study this in practice as we had a period of 17 years (1991-2007) where only about 20% of potentially eligible women were invited to screening because some counties did not have screening.21 When screening starts, more breast cancer diagnoses than usual will be made and there will be more mastectomies. However, as can be seen on the graphs, the huge increases in mastectomies are not compensated by a drop in mastectomies later where there was a similar decline in mastectomies in non-screened areas as in screened areas:22
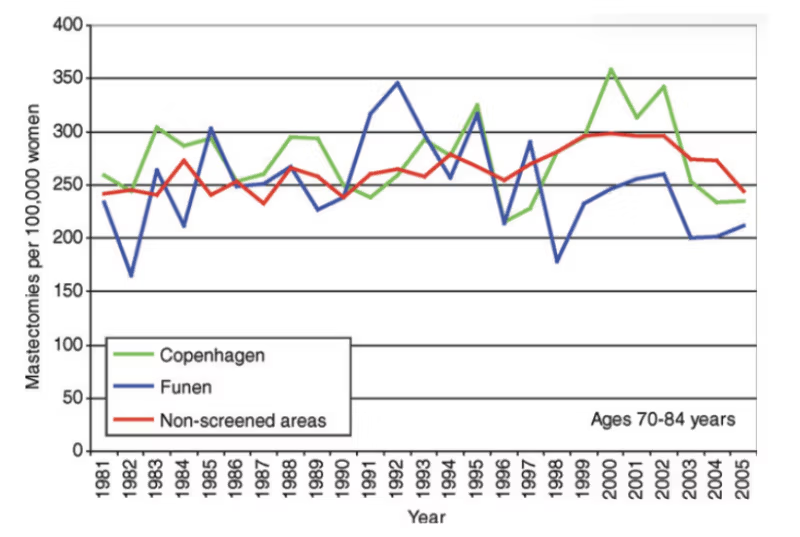
Moreover, as the next graph shows, there is no compensatory drop in old age groups:22
Yet women are told that screening leads to less invasive surgery, with fewer mastectomies. This is disinformation in the extreme.
The most commonly used trick used to disinform the women about this issue is to report percentages instead of numbers.3 Imagine a town with a certain level of crime. You divide the crimes into serious and less serious ones. Over a period of time, the rate of serious crime increases by 20% and the rate of less serious crime by 40%. This is a development for the worse. But although more people are exposed to serious crime and more people are exposed to less serious crime as well, a trickster would say that, as there are now relatively fewer cases of serious crime, the situation has improved.
It is deplorable that people who know better – screening researchers, cancer charities, national boards of health, etc – have lied to the public this way3 and still do, in direct contrast to logic and the scientific evidence.
The Final Layers of Dishonesty
The mammography screening area is riddled with dishonesty. So much that I needed to write a whole book detailing all the elaborate ways in which researchers and others had made it look like the Emperor was dressed when in fact he was naked.3
The deception is total because it always continued after I had pointed out in letters to the editor what the researchers had done wrong, and to which they responded.3,14 They therefore cannot claim they didn’t know that they continued to manipulate the data and to deceive the public.
Three of the most dishonest and most prolific authors are László Tabár, Stephen Duffy, and Robert Smith. Over many years, they aggressively attacked my extensive research on mammography screening but never with convincing arguments3,14 – they excel at ad hominem arguments.
László Tabár was the primary investigator for the Swedish Two-County study, an early trial that reported a huge effect of screening, a 31% reduction in breast cancer mortality.23 This trial was instrumental for introducing screening. However, there are so many serious discrepancies in numbers, and some of the findings are so implausible and incompatible with reported tumour characteristics, that it looks like scientific misconduct.3,6,24-27 Tabár has made a fortune on mammography screening and has a habit of threatening with litigation whenever anyone gets too close to his secrets.3,14,23
One would not think that Stephen Duffy is a professor of statistics because he has bent the data beyond belief and beyond what is appropriate in many creative and obscure ways.3,6,14 Robert Smith was once the Director of Cancer Screening at the American Cancer Society.
This triumvirate reported a 63% reduction in breast cancer mortality in an observational study.28 I pointed out some of the problems with their study,29 but in their reply,30 they compared women who attended screening with women who didn’t, although it is clear from their own paper that they were aware that such comparisons are seriously misleading.
These authors claimed, based on the Two-County study data, that they had found a “statistically significant 13% reduction in mortality in association with an invitation to screening.”31,32 This is plain wrong and totally impossible. Even if screening was 100% effective and prevented all deaths from breast cancer, it could not reduce total mortality by 13%.
They furthermore predicted that when a screening programme had been running for some time, one could expect a reduction of 3-4% in total mortality.31 This is also impossible unless screening prevents all breast cancer deaths. The lifetime risk of dying from breast cancer is 2.5-3%,33 and it was 3-4% in many countries before screening was introduced.
I dryly remarked in my book that if they continued their line of research for other diseases, they may find the recipe for eternal life.3 I also noted that the problem with lying is that
sooner or later people usually contradict themselves, which they did in relation to a study they had published in The Lancet.3
A common way of duping the readers is to say that early detection of breast cancer “reduces mortality”34 without specifying what kind of mortality this is, which makes the reader believe that screening saves lives.
The most common error in the screening literature could be that people falsely translate a recorded effect on mortality from a cancer into an effect on all-cause mortality. We see claims everywhere that common cancer screening tests save lives but a systematic review of the randomised trials found that the only screening test with a significant lifetime gain was sigmoidoscopy. It extended life by 110 days on average, and as the 95% confidence interval went from 0 to 274 days, this result was on the verge of not being statistically significant.35
Another common trick is to use hypothetical statements when we have certain knowledge. For example, authors may write – even in our most esteemed medical journals – that overdetection “may” occur for invasive cancers and that it “may” cause harm through unnecessary labelling and treatment of patients who, without screening, “might” never have been diagnosed.34 These are not hypothetical possibilities; they are inevitable consequences of screening.
Final Remarks
Starting in 2000, I have published numerous scientific articles, letters to the editor, newspaper articles, and two books about mammography screening that do not leave a shred of doubt that this intervention is very harmful.37
Even though I know that no one will ever be convicted, I consider it a crime that women have been systematically lured into believing that screening is good for them. According to the principles for informed consent, people must be fully informed about the most important benefits and harms of interventions they are offered, but this ethical requirement has been brutally ignored. To such a degree that in many countries, women receive an “invitation” to mammography screening with a pre-allotted time for a mammogram they never asked about.1 This makes them believe it is very important that they show up and puts pressure on them to cancel the appointment if they don’t want a mammogram taken. If they refuse, they are often subjected to highly coercive and paternalistic follow-up letters.
Here are some examples of the deeply unethical practice:1
“We have reserved a time… If the time is very inconvenient, we ask you to contact the mammography screening centre as soon as possible;” “I am concerned that you have not yet responded to our recent invitation for a screening mammogram;” “If you would like to avoid participation, we ask you to fill out a form. You obtain this form by calling the breast-diagnostic centre;” “During the past two years, over 340,000 Queensland women have benefited from taking part in the BreastScreen Queensland Programme,” “You can take a positive step to decrease your own risk, and help us achieve our goal, by deciding to take part.”
What matters is to ensure a high uptake, “our goal,” not that the women understand what they are being subjected to.
I advise women in all countries to not go to mammography screening and to do nothing if they are “invited,” which my wife did. She had no obligation to decline an “invitation” with a pre-allotted time she never asked for, and the letter made her angry.
Screening is harmful in many other ways than those I have mentioned here, e.g. between one quarter and one half, depending on the country, of all women attending screening repeatedly will experience at least one false positive result, which can be distressful for several years.36 It therefore constitutes another tremendous harm.6,14
As I have explained elsewhere,38 the Cochrane Collaboration refused to allow us to update our Cochrane review on mammography screening last year, even though I had updated it three times before and the update was only about adding more deaths to two of the trials.
Absurdly, the ”Sign-Off Editor” noted that our review might create a potentially damaging firestorm of misinformation and we were accused of having pre-conceived ideas about no benefit of screening “rather than considering it may actually have benefit not detected.” We were also forbidden to use the term overdiagnosis even though this is standard and appears in other Cochrane reviews of cancer screening, including our own.6,12
When I first published the Cochrane review, in 2001, there was a huge scandal39 because Cochrane forbade us from publishing our data on the most important harms of screening, overdiagnosis, and overtreatment.3 This should have made the Cochrane leaders handle our update professionally, but they preferred to support the prevailing dogma about screening rather than telling the women the truth.
Only one question remains: Which country will be the first to show a little sanity and respect for the science and abandon screening?
References
1 Jørgensen KJ, Gøtzsche PC. Content of invitations to publicly funded screening mammography. BMJ 2006;332:538-41.
2 Gøtzsche P, Hartling OJ, Nielsen M, Brodersen J, Jørgensen KJ. Breast screening: the facts – or maybe not. BMJ 2009;338:446-8.
3 Gøtzsche PC. Mammography screening: truth, lies and controversy. London: Radcliffe Publishing; 2012.
4 Mammography Saves Lives. American College of Radiology 2026; Feb 27.
5 American Cancer Society Recommendations for the Early Detection of Breast Cancer. 2026; Feb 27.
6 Gøtzsche PC, Jørgensen KJ. Screening for breast cancer with mammography. Cochrane Database Sys Rev 2013;6:CD001877.
7 Miller AB, Wall C, Baines CJ, et al. Twenty five year follow-up for breast cancer incidence and mortality of the Canadian National Breast Screening Study: randomised screening trial. BMJ 2014;348:g366.
8 Duffy SW, Vulkan D, Cuckle H, et al. Effect of mammographic screening from age 40 years on breast cancer mortality (UK Age trial): final results of a randomised, controlled trial. Lancet Oncol 2020;21:1165-72.
9 Gøtzsche PC. Relation between breast cancer mortality and screening effectiveness: systematic review of the mammography trials. Dan Med Bull 2011;58:A4246.
10 Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancer screening: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med 2002;137(5 Part 1):347-60.
11 Baum M. Harms from breast cancer screening outweigh benefits if death caused by treatment is included. BMJ 2013;346:f385.
12 Gøtzsche PC, Nielsen M. Screening for breast cancer with mammography. Cochrane Database Syst Rev 2006;4:CD001877.
13 Gøtzsche PC, Jørgensen KJ, Zahl PH, Maehlen J. Why mammography screening has not lived up to expectations from the randomised trials. Cancer Causes Control 2012;23:15-21.
14 Gøtzsche PC. Mammography screening: the great hoax. Copenhagen: Institute for Scientific Freedom; 2024 (freely available).
15 Jørgensen KJ, Gøtzsche PC. Overdiagnosis in publicly organised mammography screening programmes: systematic review of incidence trends. BMJ 2009;339:b2587.
16 Nielsen M, Thomsen JL, Primdahl S, et al. Breast cancer and atypia among young and middle-aged women: a study of 110 medicolegal autopsies. Br J Cancer 1987;56:814-9.
17 Welch HG, Black WC. Using autopsy series to estimate the disease reservoir for ductal carcinoma in situ of the breast. Ann Intern Med 1997;127:1023-8.
18 Kricker A, Smoothy V, Armstrong B. Ductal carcinoma in situ in NSW women in 1995 to 1997. National Breast & Ovarian Cancer Centre 2000;April 15.
19 Patnick J. NHS Breast Screening Programme: annual review 2011. NHS Breast Screening Programme 2012.
20 Dixon JM. Breast screening has increased the number of mastectomies. Breast Cancer Res 2009;11(Suppl 3):S19.
21 Jørgensen KJ, Zahl P-H, Gøtzsche PC. Overdiagnosis in organised mammography screening in Denmark: a comparative study. BMC Womens Health 2009;9:36.
22 Jørgensen KJ, Keen JD, Gøtzsche PC. Is mammographic screening justifiable considering its substantial overdiagnosis rate and minor effect on mortality? Radiology 2011;260:621-7.
23 Tabár L, Fagerberg CJ, Gad A, et al. Reduction in mortality from breast cancer after mass screening with mammography. Randomised trial from the Breast Cancer Screening Working Group of the Swedish National Board of Health and Welfare. Lancet 1985;1:829-32.
24 Zahl P, Kopjar B, Mæhlen J. Mammografistudier. Tidsskr Nor Lægeforen 2001;121:2636.
25 Gøtzsche PC, Mæhlen J, Zahl PH. What is publication? Lancet 2006;368:1854–6.
26 Zahl P-H, Gøtzsche PC, Andersen JM, Mæhlen J. Results of the Two-County trial of mammography screening are not compatible with contemporaneous official Swedish breast cancer statistics. Dan Med Bull 2006;53:438-40.
27 Gøtzsche PC. Whistleblower in healthcare (autobiography). Copenhagen: Institute for Scientific Freedom 2025 (freely available).
28 Tabár L, Vitak B, Chen HH, Yen MF, Duffy SW, Smith RA. Beyond randomized controlled trials: organized mammographic screening substantially reduces breast carcinoma mortality. Cancer 2001;91:1724-31.
29 Gøtzsche PC. Beyond randomized controlled trials. Cancer 2002;94:578.
30 Tabár L, Duffy SW, Smith RA. Beyond randomized controlled trials. Authors’ reply. Cancer 2002;94:581–3.
31 Tabár L, Duffy SW, Yen MF, Warwick J, Vitak B, Chen HH, Smith RA. All-cause mortality among breast cancer patients in a screening trial: support for breast cancer mortality as an end point. J Med Screen 2002;9:159–62.
32 Duffy SW, Tabár L, Vitak B, Yen MF, Warwick J, Smith RA, Chen HH. The Swedish Two-County trial of mammographic screening: cluster randomisation and end point evaluation. Ann Oncol 2003;14:1196–8.
33 Office of Population Censuses and Surveys. Mortality Statistics: cause 1988. London: HMSO; 1990. (Series DH2 no. 15. Table 2).
34 Irwig L, Houssami N, Armstrong B, Glasziou P. Evaluating new screening tests for breast cancer. BMJ 2006;332:678-9.
35 Bretthauer M, Wieszczy P, Løberg M, et al. Estimated lifetime gained with cancer screening tests: a meta-analysis of randomized clinical trials. JAMA Intern Med 2023;183:1196-1203.
36 Brodersen J, Siersma VD. Long-term psychosocial consequences of false-positive screening mammography. Ann Fam Med 2013;11:106–15.
37 Gøtzsche PC. Mammography screening is harmful and should be abandoned. J R Soc Med 2015;108:341-5.
38 Gøtzsche PC. Cochrane on a suicide mission. Brownstone Journal 2025; June 20.
39 Horton R. Screening mammography – an overview revisited. Lancet 2001;358:1284-5.
Dr. Peter Gøtzsche co-founded the Cochrane Collaboration, once considered the world’s preeminent independent medical research organization. In 2010 Gøtzsche was named Professor of Clinical Research Design and Analysis at the University of Copenhagen. Gøtzsche has published over 100 papers in the “big five” medical journals (JAMA, Lancet, New England Journal of Medicine, British Medical Journal, and Annals of Internal Medicine). Gøtzsche has also authored books on medical issues including Deadly Medicines and Organized Crime.
Sorry, The New Republic, Climate Change Isn’t Causing Somali Migration. Blame Civil Strife and Poverty.

By Linnea Lueken | Climate Realism | March 10, 2026
The New Republic (TNR) posted an article titled “Somali Immigrants Fled Climate Change. Now They’re Facing ICE,” claiming that Somali migrants in the United States have been driven out of their country by climate-change caused drought. This is false, or at least incomplete. Drought is a natural part of the region, even multi-year drought, and the present one is no different than the region has experienced with some regularity historically. It is civil strife and government corruption, resulting in continued poverty, that is leading Somalis to flee their homeland. With present governing institutions and security, they have been unable to improve water handling practices. Climate change has nothing to do with Somali emigration elsewhere in the region or to the United States, as even those interviewed for the article acknowledge.
TNR undermines its titular claim that unprecedented man-made climate change has forced Somalians to migrate by admitting that Somalian culture has “deep-rooted traditions of movement and migration.” TNR goes on to say that “Somalis have been caught in civil war and unrest for decades, and many have migrated to Kenya, Ethiopia, Europe, and the United States.”
Somehow not noticing the actual central point of that statement, that Somalians often move and that political strife has kept them destabilized, TNR says that climate change plays a “pervasive role” in the migration.
TNR claims that a multi-year drought “made a hundred times more likely due to warming caused by fossil fuel emissions—is affecting Somali people’s decisions to either relocate internally or migrate across international borders.”
Incredibly, later in the article, TNR refutes its own suggestion that this drought is worse, and pushing unprecedented migration, by explaining that this is how farmers have long dealt with drought in Somalia:
Traditionally, Somali pastoralists had resilient ways to deal with changes in rainfall and drought patterns, where families migrated and moved on a regular basis, even crossing borders in the process. But the nature of climatic changes—and conflict—overwhelmed their traditional capacities, leading to more rural-urban migration within the country and in East Africa.
That’s right, severe drought is something Somalians have dealt with for ages, long enough to have known traditions regarding adaptation to the dry periods.
There is no evidence that this drought is worse than those that drove historic migration.
The cited claim that recent drought in Somalia was made “a hundred times more likely” by climate change is not based on sound science. It comes from an attribution study from World Weather Attribution that specifically seeks to tie various weather conditions to human-caused climate change, they do not come to any other conclusions. Climate Realism has gone into the specifics of how unscientific World Weather Attribution studies are here, here, and here.
The TNR piece says that “[f]rom 2020 to 2023, the East Africa region had five failed rainy seasons, an unprecedented drought and climatic episode not seen in 40 years, which led to 70 percent crop loss, three million livestock deaths, and the displacement of about 2.9 million people in Somalia, according to some estimates.”
Admitting that a weather event also happened 40 years ago should tell a writer that their argument about something being “unprecedented” – meaning, without precedent, or never happened before—is faulty.
In fact, studies and data show a long history of swings between severe drought and monsoon floods in the region, and they show that nothing about modern drought is unprecedented. Paleo studies, including one published in Science, show that “intervals of severe drought lasting for periods ranging from decades to centuries are characteristic of the monsoon and are linked to natural variations in Atlantic temperatures.”
Climate Realism has covered this very claim before: In Anthony Watts’ “No, CBS News, Drought in Somalia is Not Being Driven by Climate Change,” he compared natural weather-driving patterns like the Atlantic Meridional Oscillation (AMO) and recent drought in Somalia and found repeated patterns of drought that were similarly severe.
Somalia is part of the Sahel region, and Watts shared this graphic of the region’s rainfall index since 1900, which shows that the rainfall in the Sahel varies widely over time:
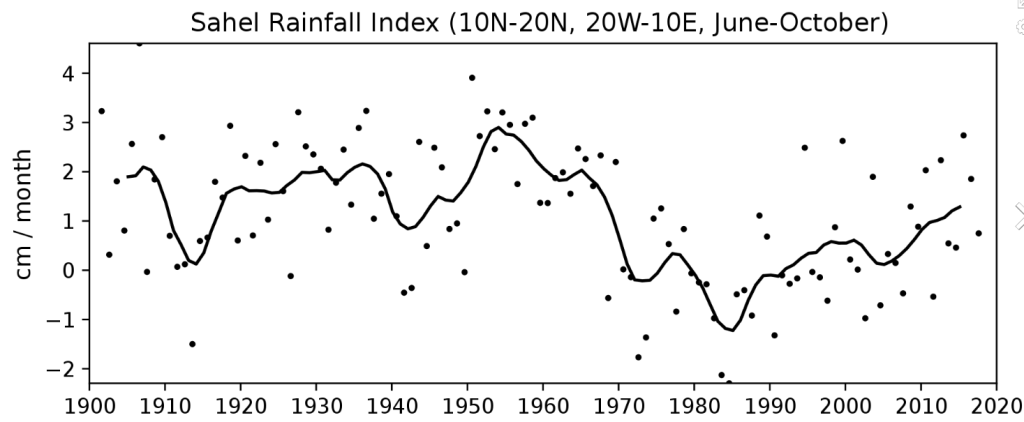
Figure 1: More than a century of rainfall data in the Sahel show an unusually wet period from 1950 until 1970 (positive index values), followed by extremely dry years from 1970 to 1991. (negative index values). From 1990 until present rainfall returned to levels slightly below the 1898–1993 average, but year-to-year variability was high. Source: Benedikt Seidl – based on JISAO data
Additionally, comparing crop production data between Somalia and neighboring countries like Ethiopia and Kenya reveals that even when drought impacts East Africa, Somalia is uniquely incapable of maintaining agricultural production. During the same period in which Ethiopia and Kenya saw increasing production in vital cereal crops, UN Food and Agriculture Organization (FAO) data show Somalia declining. (See figure below)
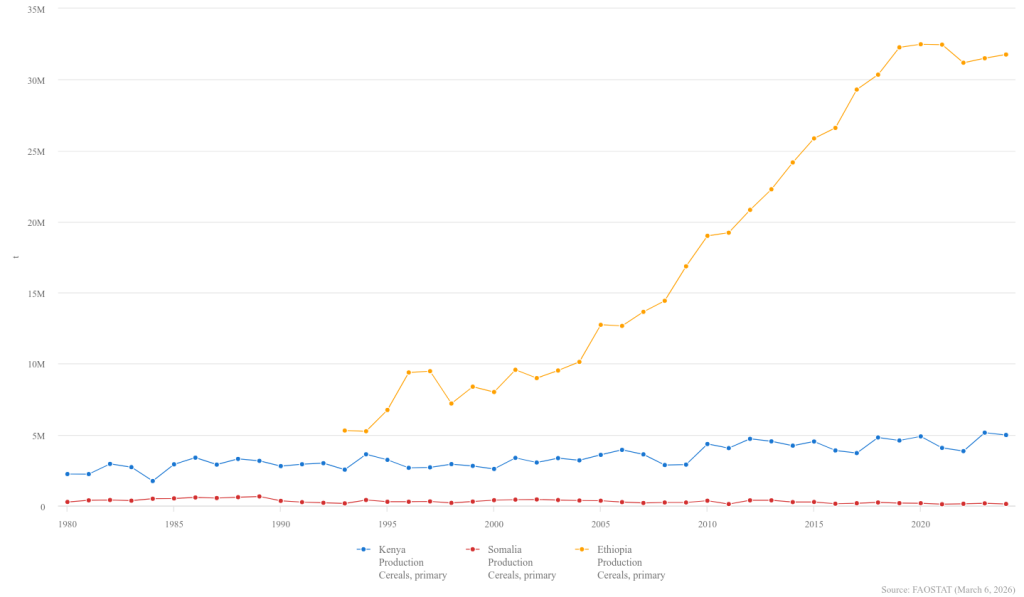
Is climate change not hitting Kenya and Ethiopia? What is the difference?
While Somalia has a long history of severe, recurring droughts, the worst drought in the past 50 years was the “Long-tailed Drought” from 1973 to 1975. That drought, and a subsequent similarly deadly drought in the early 1980s, occurred when the Earth was in a cooling spell and atmospheric carbon dioxide was much lower than today.
Somalia’s civil war and resulting destruction and corruption is the prime force behind Somalia’s emigration. Ironically, one of the interviewees in the TNR piece says as much:
Drought does not necessarily lead to famine and does not always lead to migration,” said Abdi Samatar, a Somali scholar and geographer at the University of Minnesota […] Somalis were unable to “put Humpty Dumpty back together in their country,” and in the absence of government support, “people have to do what they can for themselves,” Samatar added.
We at Climate Realism could not have said it better ourselves, though we have explained as much in past articles where mainstream outlets tried to link climate change and Somalia’s migration issue.
The New Republic’s effort to tie Somalians fleeing their country for the United States to climate change was a flawed, agenda-driven effort from the start. Even when those interviewed by TNR link the mass exodus of residents from Somali to other factors, TNR persists in pushing the narrative that climate change is playing a “pervasive role.”
It is true that Somalia is suffering through a severe, life threatening drought. It is also true that such droughts are not unprecedented but have been common throughout the region’s history. The nation’s unstable government and the ongoing, long-standing, civil war bear far more of the blame than climate change, especially since there is little or no evidence that Somalia’s climate has changed much over the past century.
The current drought is hitting Somalia’s populace worse than those of nearby countries in the region because of the political instability there. The New Republic was told this by the experts they interviewed but chose to ignore it to advance a climate scare story. Evidently, it’s too much to hope for honest journalism at The New Republic.
Linnea Lueken is a Research Fellow with the Arthur B. Robinson Center on Climate and Environmental Policy.
EPSTEIN FILES REVEAL POWER BROKERS IN SCIENTIFIC PUBLISHING
The HighWire with Del Bigtree | March 26, 2026
Newly surfaced documents and reporting are fueling questions about whether a small network of powerful players including Bill Gates, Jeffrey Epstein, and individuals linked to Robert Maxwell’s scientific publishing legacy sought outsized influence over how research is distributed and amplified. Emails, investments, and media-funding ties are being cited as potential indicators of an effort to shape which scientific ideas rise to prominence and which get sidelined. The broader issue: who controls the pipelines of modern science—publishing, PR, and perception—and what transparency is owed to the public when power concentrates behind the scenes.
The Mandelson Molecule: Exposing the Architecture of Cross-Border Political Suppression
By Freddie Ponton | 21st Century Wire | February 18, 2026
The resignation of Peter Mandelson as UK ambassador to Washington in February 2026 revealed more than a scandal—it exposed the architecture of a parallel governance system operating through deniable channels. The Epstein files, the Center for Countering Digital Hate (CCDH) censorship apparatus, and the Mandelson intelligence pipeline are not separate stories. They are component parts of a transatlantic mechanism that converts private access into public control, with enforcement mechanisms that now reach across sovereign borders to silence American citizens.
Jeffrey Epstein was a convicted sex offender with deep ties to political and financial elites on both sides of the Atlantic. Peter Mandelson is a former UK power‑broker and ambassador to Washington, now under investigation for secretly sharing government information with Epstein. This article shows how their relationship connects to a wider system of online censorship and private global‑health finance.
The Intelligence Pipeline: Real-Time Treasury Briefings to a Convicted Sex Offender
The Mandelson-Epstein correspondence reveals something far more systematic than indiscreet friendship. It documents a private intelligence channel operating at the highest levels of UK and US financial policy.
In December 2009, while serving as Business Secretary, Mandelson forwarded Treasury positions on the bankers’ bonus tax to Epstein within hours of receiving them, with Epstein requesting advance notice “before Jes” and Mandelson replying simply: “Treasury”. By March 2010, the pattern had escalated—Mandelson forwarded notes from a meeting between UK Chancellor Alistair Darling and US Treasury Secretary Larry Summers to Epstein within five minutes, followed by his own meeting with Summers the next day. Those notes were forwarded within two minutes.
The content was market-moving intelligence: Dodd-Frank implementation, hedge fund taxation, derivatives regulation, and Bank of England quantitative easing strategy during the credit crunch. Mandelson advised Epstein that JPMorgan’s CEO should “mildly threaten” Chancellor Darling over policy. This systematic extraction of live government intelligence for private financial advantage can hardly be construed as incidental corruption.
DOCUMENT: Peter Mandelson leaked No 10 documents to Epstein, who then helped him pursue multi-million dollar jobs (Source: Tax Policy Associates)
The Censorship Architecture: From Anti-Corbyn Operations to American Deplatforming
The same censorship machine that produced the Biden White House’s authoritarian campaign against the so-called “Disinformation Dozen” in 2021 had emerged from the notorious Room 216, Brixton, where Israeli loyalist and architect of Keir Starmer’s rise to power, Morgan McSweeney, along with Imran Ahmed, built the “Labour Together” operation to dismantle Jeremy Corbyn. It was a CCDH list of 12 named individuals, which the White House then pushed Facebook to censor. The March 2021 “Disinformation Dozen” report was not independent research—it was unequivocally the identical playbook redeployed. The Biden White House directly cited CCDH’s report to pressure Facebook into censoring American health publishers, with internal documents showing the platform’s “secretly demoted” users, including alleged “anti-vaxxers”, and Twitter accounts of targeted individuals. When Facebook pushed back that the “majority of the accounts in question were not spreading misinformation,” the White House persisted.
Among those branded the “Disinformation Dozen” by the CCDH in March 2021: Robert F. Kennedy Jr. (Children’s Health Defense), physician Joseph Mercola, and Sayer Ji—whose investigative work exposing the Mandelson intelligence pipeline appears later in this report.
The method was documented in internal strategy papers: cultivate “seemingly independent voices to generate and share content to build up a political narrative,” infiltrate opposition spaces to extract decontextualised content, and feed narratives to sympathetic media. The “antisemitism crisis” that destroyed UK Labour Party leader Jeremy Corbyn was, as Labour Party files confirm, instrumentalised by this same faction.
Morgan McSweeney was CCDH’s founding director and subscriber for 18 months, operating from the same Brixton office that produced Labour’s anti-Corbyn operation. When he resigned in April 2020 to become Starmer’s chief of staff, Ahmed inherited an apparatus already proven effective at demonetising political opposition.

Morgan McSweeney, founding director of the CCDH, and former British Prime Minister Keir Starmer’s Chief of Staff. (Source: The Edge | Business news)
The March 2021 “Disinformation Dozen” report was not independent research—it was unequivocally the identical playbook redeployed. The Biden White House directly cited CCDH’s report to pressure Facebook into censoring American health publishers, with internal documents showing the platform “secretly demoted” affiliated accounts and Twitter accounts of targeted individuals. When Facebook pushed back that the “majority of the accounts in question were not spreading misinformation,” the White House persisted.
Project Molecule: The Financial Infrastructure of Private Governance
The August 2011 JPMorgan “Project Molecule” blueprint reveals the financial architecture that made this system durable. The $150 million fund Epstein pitched to JPMorgan CEO Mary Erdoes was designed to operate “across sovereign borders, into specific countries, for specific biological interventions”—with no elected officials, no treaty obligations, and no public accountability beyond its own audit committee.
DOCUMENT: JPMorgan “Project Molecule” blueprint (Source: DOJ Epstein File Library | EFTA01301114)
Epstein operated as Bill Gates’s representative under a written agreement, with the explicit purpose of securing “additional money for vaccines” while creating a “permanently governed, privately controlled, transnational system”. The budget allocated $40M for polio vaccines in Afghanistan, $40M in Pakistan, $20M specifically for “financing the surveillance network in Pakistan,” and $30M for rotavirus vaccines in Latin America.
This is the governance model: private intelligence (Mandelson-Epstein), private finance (Project Molecule’s offshore vaccination funds), and private enforcement (CCDH’s deplatforming operations) operating in substitutional parallel to democratic institutions.
The Enforcement Layer: Cross-Border Suppression of American Speech
What transforms influence operations into censorship is enforcement. The original investigation documents the apparatus reaching into foreign legal proceedings against American journalists—cross-border enforcement without due process, extradition treaties, or congressional oversight.
The pattern is now confirmed by US government action. In December 2025, Secretary of State Marco Rubio barred Imran Ahmed from entering the United States, citing his role in “leading organised efforts to coerce American platforms to punish American viewpoints they oppose”. Ahmed was one of five Europeans sanctioned under a visa policy targeting foreigners responsible for censoring protected speech in America.
The CCDH is now reportedly under DOJ investigation for potential violations of foreign agent registration laws, given its coordination with UK Labour operatives while targeting US political speech. Labour’s deployment of approximately 100 operatives to US swing states during the 2024 election—conducted by McSweeney’s network—has generated formal FEC complaints alleging direct electoral interference.
After days of parliamentary theatre about “transparency,” Westminster has craftily moved to bury the Mandelson-Epstein papers—not in open sunlight, but inside the Intelligence and Security Committee, a body three of whose members have already stuffed with cash from pro-Israel lobbyists.
In Britain, Downing Street originally wanted veto power over anything “prejudicial to national security”, but the documents will now be reviewed by the Parliament’s Intelligence and Security Committee (ISC). Critics argue that this allegedly independent oversight body could be compromised. In effect, three sitting members—Deputy Chair Sir Jeremy Wright, Sir John Hayes, and Labour’s Derek Twigg—have all taken money from the pro-Israel lobby, which by some estimates bankrolls roughly a quarter of British MPs. This can be verified in the excellent Declassified UK report published in June 2024.
The bottom line is that the Epstein file, which details how Mandelson piped classified Treasury intelligence to a convicted sex offender, and how British power brokers and Wall Street criminals traded backroom briefings, will now be “vetted” by politicians on the take from foreign influence networks. Forget transparency—it was never on the table.
The Architecture of Manufactured Consensus
The critical insight is structural: these networks exploit the gap between formal democratic institutions and actual governance. Mandelson’s Treasury briefings to Epstein occurred through informal channels. Project Molecule’s sovereign surveillance programs were designed to operate offshore. CCDH’s censorship operations, though effective at capturing White House policy, occurred through a nonprofit rather than state agencies. According to reports, George Soros is said to have donated $250,000 to the CCDH, which is working to censor conservative news outlets and to undermine Musk’s Twitter.
When the same personnel (McSweeney as CCDH founder, then Starmer’s chief of staff), the same infrastructure (Brixton operations), and the same methods (crisis amplification, media laundering, financial pressure) appear across Corbyn’s destruction, COVID censorship, and US electoral operations, we are not observing a coincidence. We are witnessing a system.
The switchboard is not the scandal. The switchboard is the system, and it is now being dismantled by the very government it sought to influence.
The Original Investigation
This synthesis builds upon the groundbreaking investigative work of Sayer Ji, founder of GreenMedInfo and author of the Switchboard series—including the first publication to connect the Mandelson-Epstein intelligence pipeline to the CCDH censorship apparatus. Ji’s research, conducted under direct legal and professional pressure from the very networks he was exposing, documented how British political operatives built a cross-border enforcement mechanism capable of weaponising foreign courts against American journalists.
His original reporting on Room 216, the Brixton operations, and the emergence of “disinformation” as a tool for political suppression predates mainstream coverage by years, and has now been validated by the Epstein disclosures, the Rubio sanctions against Ahmed, and the DOJ’s investigation into CCDH’s foreign agent activities.
Read the complete investigation series and supporting documentation at Sayer Ji Substack…

Sayer Ji reports on Substack…
The Switchboard: From Epstein to Mandelson to McSweeney to Ahmed — How a British Machine Became America’s Censorship Engine
How the Epstein Files Reveal the Architecture Behind Censorship, Crisis Finance, and What Happened When I Investigated It – Part 3 in a Series
Peter Mandelson, “the Prince of Darkness,” Keir Starmer’s hand-picked ambassador to Washington, the most powerful unelected figure in British politics, resigned from Parliament this week, one step ahead of legislation to eject him. The Metropolitan Police opened a criminal investigation. The Prime Minister apologised to Jeffrey Epstein’s victims for believing Mandelson’s lies.
The press is treating this as a story about a politician’s downfall. It is not. It is a story about what he was connected to — and what was built to make sure you never found out.
Key Findings:
- The censorship machine that targeted American speech during COVID was built inside a Labour Party factional operation. Morgan McSweeney and Imran Ahmed created the Center for Countering Digital Hate (CCDH) from the same office, using the same staff, and the same dark-money infrastructure they used to destroy Jeremy Corbyn — then redeployed the identical playbook against U.S.-based health publishers and independent media.
- CCDH’s founder and political patron is a protégé of Peter Mandelson, who was simultaneously routing confidential UK and U.S. government intelligence to Jeffrey Epstein. Mandelson forwarded Treasury readouts on the Volcker Rule, Dodd-Frank, and derivatives regulation to Epstein within minutes of receiving them — intelligence worth billions to Epstein’s Wall Street clients. The same political culture of deniable backroom operations that made the Epstein network functional also produced CCDH.
- Epstein’s network was not just criminal — it was architectural. Project Molecule, a $150M JPMorgan blueprint produced the same month Epstein sketched a private global health fund, reveals the institutional machinery: offshore vaccination funds, sovereign biological surveillance programs, and governance structures designed to bypass elected oversight entirely.
- The enforcement layer is not theoretical — it has already been deployed against named individuals. CCDH’s “Disinformation Dozen” list led directly to platform deplatforming. In at least one documented case, CCDH-originated material was entered into foreign legal proceedings to seek an ex parte arrest warrant against a U.S.-based journalist for lawful American speech — cross-border enforcement with no due process, no extradition treaty, and no congressional oversight.
- The same network is now the subject of a formal FEC complaint alleging direct electoral interference. McSweeney — Mandelson’s protégé, CCDH’s political architect, and now Starmer’s chief of staff — was named in a formal FEC complaint for dispatching approximately 100 Labour operatives to U.S. swing states during the 2024 presidential election. The censorship pipeline and the electoral interference pipeline share the same personnel, the same infrastructure, and the same assumption: that British political operatives can shape American outcomes without accountability.
‘Fox guarding the henhouse’: AMA, Vaccine Integrity Project to conduct their own vaccine safety and efficacy reviews
By Suzanne Burdick, Ph.D. | The Defender | February 11, 2026
The American Medical Association (AMA) is teaming up with the Vaccine Integrity Project to conduct its own review of vaccine safety and efficacy, claiming that advisers to the Centers for Disease Control and Prevention (CDC) are no longer doing a good enough job.
The groups said Wednesday in a press release that “for decades,” the CDC’s Advisory Committee on Immunization Practices (ACIP) had “served as the engine of evidence-based vaccine policy” for the U.S. “That system has now effectively collapsed.”
U.S. Department of Health and Human Services (HHS) Press Secretary Emily G. Hilliard told The Defender the claim that ACIP’s evidence-based process has collapsed is “categorically false.” She said:
“ACIP continues to remain the nation’s advisory body for vaccine use recommendations driven by gold standard science. While outside organizations continue to conduct their own analyses and confuse the American people, those efforts do not replace or supersede the federal process that continues to guide vaccine policy in the United States.”
The Vaccine Integrity Project, based at the University of Minnesota’s Center for Infectious Disease Research and Policy (CIDRAP), says it is dedicated to “safeguarding vaccine use in the U.S.”
The AMA will work with the project to review vaccines for the 2026-2027 respiratory virus season. These include immunizations against COVID-19, influenza and respiratory syncytial virus (RSV), according to the press release.
CIDRAP Director Michael Osterholm said in a statement that the goal is “to restore peace of mind for clinicians and patients by ensuring that experts are continuously evaluating vaccine safety and effectiveness using transparent, evidence-based methods.”
Children’s Health Defense (CHD) General Counsel Kim Mack Rosenberg said it’s unlikely that the groups will restore people’s peace of mind about vaccines. She said:
“Unfortunately, the AMA and the Vaccine Integrity Project support a narrative about vaccines that is being exposed more and more as problematic and contradicted by what people are seeing with their own eyes.
“The system is broken and efforts to prop it up from the inside are being exposed for conflicts of interest and flawed analyses.”
The groups’ review process looks similar to how the ACIP traditionally worked, but they won’t issue recommendations. Instead, they will share their review results with medical societies, which can write recommendations for their patient demographic.
The AMA and the Vaccine Integrity Project said they will also involve medical societies and public health and healthcare organizations to craft policy questions.
Review members will disclose “relevant” conflicts of interest, according to the press release. However, “relevant” was left undefined.
The AMA and Vaccine Integrity Project said in a statement:
“The goal of this work is to ensure a deliberative, evidence-driven approach to produce the data necessary to understand the risks and benefits of vaccine policy decisions for all populations — the approach traditionally used by the federal government.”
The effort may generate more confusion among Americans who are torn between looking to the federal government or medical societies for vaccine guidance, according to Trial Site News.
“The country is no longer operating with a single, uncontested center of vaccine-policy gravity,” Trial Site News wrote.
‘Like asking the fox to guard the henhouse’
The Vaccine Integrity Project, launched in April 2025, is funded by an unrestricted gift from iAlumbra, a nonprofit founded by Walmart heiress and philanthropist Christy Walton.
The Robert Wood Johnson Foundation, The Greenwall Foundation and Lasker Foundation are also listed among the project’s funders.
The Vaccine Integrity Project declined The Defender’s request for a list of donation amounts and names of any individual donors.
Former CDC Director Rochelle Walensky serves as the Vaccine Integrity Project’s adviser of medical affairs. In 2022, Walensky admitted the CDC gave false information about COVID-19 vaccine safety monitoring.
Already, the Vaccine Integrity Project released a review of the hepatitis B vaccine that supported vaccinating all newborns at birth, rather than delaying when the mother has tested negative for hepatitis B. The project is currently reviewing the human papillomavirus (HPV) vaccine.
“Trusting the AMA and the Vaccine Integrity Project to objectively review vaccine safety feels a lot like asking the fox to guard the henhouse,” said Nebraska chiropractor Ben Tapper.
Mack Rosenberg said the repeated failures of such organizations to “truly and comprehensively” analyze vaccine safety data have led to “increasing distrust among the public — and with good reason.”
AMA ‘a political force,’ not a ‘neutral medical association’
In 2025, the AMA spent nearly $24 million on lobbying, making it one of the top 10 groups trying to influence government policy, according to OpenSecrets.
“This is not the behavior of a neutral medical association. It is the strategy of a political force,” wrote Jason Altmire in an op-ed for RealClearHealth.
Altmire, a former hospital and health insurance executive who served in the U.S. House of Representatives, is an adjunct professor of healthcare management at the Texas Tech University Health Sciences Center.
Tapper questioned whether the AMA and the Vaccine Integrity Project would sufficiently assess the safety of vaccines.
For many people, the concern isn’t that vaccines can have benefits, he said. “The concern is whether safety data is fully transparent, whether adverse event reporting is thoroughly investigated, whether conflicts of interest are disclosed and whether risk-benefit analyses are stratified appropriately by age and health status.”
The AMA, which touted 2024 revenues of $546 million, was criticized during the COVID-19 pandemic for deferring to political ideology rather than medical facts.
Its “AMA COVID-19 Guide: Background/Messaging on Vaccines, Vaccine Clinical Trials & Combatting Vaccine Misinformation” encouraged doctors to use certain words and avoid others. For instance, “stay-at-home order” replaced “lockdown,” and “deaths” replaced “hospitalization rates.”
The AMA in August 2025 was disinvited from the CDC’s vaccine advisory committee’s workgroups.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Epstein Pitched JPMorgan Chase on Plan to Get Bill Gates ‘More Money for Vaccines’
By Michael Nevradakis, Ph.D. | The Defender | February 10, 2026
In the years leading up to the COVID-19 pandemic, Bill Gates and key figures from the Gates Foundation regularly interacted with Jeffrey Epstein, discussing ways to finance and develop a global pandemic preparedness and vaccination network.
The communications between Gates and Epstein were included in the “Epstein Files” released Jan. 30 by the U.S. Department of Justice (DOJ). Last year’s passage of the bipartisan Epstein Files Transparency Act prompted the release.
Sayer Ji told The Defender the files show that Epstein “functioned as a switchboard” connecting “hedge funds, central banks, billionaires, academic institutions and global health initiatives.”
Ji published his analysis of health- and medical-related information in the files in a series of Substack articles and posts on X.
Seamus Bruner, director of research at the Government Accountability Institute, said the files revealed the workings of a network of “Controligarchs on steroids, but with shocking new receipts.”
Bruner said the files showed that Epstein helped develop “the architecture for pandemic profiteering” years before the COVID-19 pandemic.
The documents largely date from the 2010s — after Epstein’s 2008 conviction for soliciting underage sex and his inclusion on a registry of sex offenders.
Ji noted that months before the start of the COVID-19 pandemic, many of the same actors who appear in the Epstein files participated in Event 201 — a simulation of a global pandemic caused by a coronavirus.
The pandemic preparedness infrastructure built in the years before the pandemic helped lead to this simulation, Ji wrote.
According to The Hill, members of the U.S. Congress began reviewing unredacted versions of the documents on Monday.
Rep. Thomas Massie (R-Ky.), who co-sponsored the Epstein Files Transparency Act along with Rep. Ro Khanna (D-Calif.), told The Defender the documents’ release is about justice, not politics.
“Rep. Ro Khanna and I have tried to keep the Epstein files from being political. The Democrats want to make it about Trump, and the Republicans want to make it about the Clintons. We want to make it about the survivors and getting them justice and transparency,” Massie said.
Gates, Epstein and the ‘architecture behind pandemics as a business model’
Ji’s series of Substack posts revealed what he described as “a 20-year architecture behind pandemics as a business model — with Bill Gates at the center of the network,” along with multinational financial institutions like JPMorgan Chase.
The documents, dating from 2011 to 2019, illustrate an “architecture whose foundations predate the COVID-19 era by more than a decade,” Ji wrote. He said they constitute evidence of “a major Wall Street bank asking a convicted sex offender to define the architecture of a Gates-linked charitable fund.”
The documents included several emails outlining the development of a Gates-led charitable fund. A Feb. 17, 2011, email from JPMorgan Chase’s Juliet Pullis to Epstein included questions from the “team that is putting together some ideas for Gates.”
Epstein’s reply outlined how this fund could be structured. The proposal would be developed further in the following months.
In a July 26, 2011, email from Epstein to JPMorgan Chase executive Jes Staley, on which Boris Nikolic, Gates’ chief science and technology adviser, was copied, described a “silo based proposal that will get bill [Gates] more money for vaccines.”
By Aug. 17, 2011, Staley and Mary Erdoes, then-CEO of JPMorgan Asset and Wealth Management, were discussing more details of the proposed fund, including developing “an offshore arm — especailly for vaccines” and projecting “billions of dollars” in donations within two years.
In a response later that day, Epstein said Gates was “terribly frustrated” at the slow pace of establishing the fund. He said Gates was insistent that “additional money for vaccines” be included in an upcoming presentation about the fund.
By Aug. 31, 2011, JPMorgan Chase had apparently developed a proposal called “Project Molecule,” where the bank would partner with the Gates Foundation to develop a perpetual charitable fund for pandemic preparedness and surveillance, vaccine promotion and disease eradication.
According to Ji, the proposal contains many of the ideas Epstein had previously discussed with JPMorgan Chase executives. It also contained plans to spend millions of dollars to purchase oral polio vaccines for Afghanistan and Pakistan, a rotavirus vaccine for Latin America, and a meningitis vaccine for Africa.
The proposal suggested that Melinda Gates chair the fund’s strategic program/grant and distribution committee and that Erdoes, Warren Buffett, Jordan’s Queen Rania and Seth Berkley, CEO of Gavi, the Vaccine Alliance, also participate. The Gates Foundation funded Gavi’s launch in 1999 and holds a permanent seat on its board.
Ji wrote that while Epstein’s name does not appear in the Project Molecule proposal, it acts as the “institutional translation of the architecture he was sketching informally.”
By 2013, these efforts appear to have led to the launch of the Global Health Investment Fund. A confidential Sept. 23, 2013, briefing described the fund as “the first investment fund focused on global health drug and vaccine development.” The fund promised investors annual returns of 5%-7%.
Among the attendees at the fund’s September 2013 launch were JPMorgan Chase CEO Jamie Dimon and representatives of Pfizer, Merck and GlaxoSmithKline (now GSK).
Gates could ‘work with anyone on earth’ but ‘chose a registered sex offender’
According to Ji, Nikolic’s involvement is significant. In August 2013, Gates and Epstein signed an agreement, in which Gates “specifically requested” that Epstein “personally serve” as Nikolic’s representative. The letter noted Epstein’s “existing collegial relationship” with Gates.
“This agreement was executed five years after Epstein’s conviction for soliciting a minor for prostitution,” Ji wrote. “Gates had the resources to work with anyone on earth. He chose a registered sex offender — and put it in writing.”
The documents showed that a month earlier — on July 18, 2013 — Epstein authored a draft email apparently intended for Gates. It references Epstein’s friendship with Gates, his disappointment that Gates sent him an “unfriendly strongly worded email,” and referenced sordid communications the two apparently previously shared.
“TO add insult to the injury you them implore me to please delete the emails regarding your std, your request that I provide you antibiotics that you can surreptitiously give to Melinda and the description of your penis,” Epstein wrote.
In a video posted on X, Michael Kane, director of advocacy for Children’s Health Defense, said that while it’s unknown whether Epstein ever sent that email to Gates, “the next month they’re in a contract together.”
“I think Bill Gates got the message,” Kane said.
In November 2023, a federal judge approved a $290 million settlement between JPMorgan Chase and over 100 women who accused Epstein of sexual abuse. The women alleged that JPMorgan Chase continued doing business with Epstein despite internal warnings over a span of several years.
“JPMorgan banked Epstein for years despite clear red flags — over $1 billion in suspicious transactions flagged internally and ignored. They knew. They didn’t care,” wrote The Truth About Cancer.
Did Epstein play role in launch of the ‘biosecurity state’?
According to Ji, the documents provide a roadmap for how a pandemic preparedness infrastructure was developed and how it helped make Event 201 possible.
“By the time Event 201 convened, the architecture … was no longer conceptual. It had been funded, structured, bonded, insured, staffed, and legally papered. What remained was the rehearsal,” Ji wrote.
September 2014 documents show that Gates disclosed his upcoming meeting with President Obama to Epstein, just as an adviser to then-Israeli Prime Minister Ehud Barak sent Epstein an invitation to a private, off-the-record reception with Obama the following month.
Ji said the communications occurred during “the week Ebola was formally reclassified as a threat to international peace and security.” He said the timing is significant, as this “was the week the biosecurity state was born.”
According to Ji, these developments helped activate the infrastructure outlined in Project Molecule, where Epstein acted as a node for Ebola-related project proposals.
This included Epstein receiving a United Nations (U.N.) diplomat’s proposal for the development of a “Nexus Centre for peace and health” that would take “into account the serious impact of Ebola,” and a proposal by a group of scientists for a pre-symptomatic Ebola detection system using PCR testing.
The scientists behind the proposal — affiliated with a U.S. military biolab at Fort Detrick, the Centers for Disease Control and Prevention and the National Institutes of Health — asked Epstein to send the proposal to Gates and the Gates Foundation.
By October 2014, Epstein was warning Kathy Ruemmler, then White House counsel to Obama, of the political cost if Obama didn’t take action on Ebola. By 2015, Epstein was acting as an intermediary in efforts to convene global experts who would “discuss how we can most effectively address and prevent pandemics.”
The proposal, by the International Peace Institute’s Terje Rød-Larsen, led to the convening of a May 2015 closed-door meeting in Geneva, Switzerland, titled “Preparing for Pandemics: Lessons Learned for More Effective Responses.” The World Health Organization (WHO), World Bank and U.N. were involved with the meeting.
The meeting’s agenda included sessions addressing “how pandemics should be anticipated, how authority should be exercised, how multiple stakeholders should be coordinated, and — critically — what legal, institutional, and financial mechanisms must be put in place in advance to enable rapid, centralized response,” Ji wrote.
According to Ji, the COVID-19 pandemic response has its roots in the 2014 Ebola response, as Ebola “was the first disease to formally justify the suspension of normal political and sovereign constraints on a global scale. … When the next global health emergency arrived — COVID-19 — the playbook was already written.”
“Epstein appears in the background of precisely these formative conversations — serving as a connector between global finance, philanthropic capital, and biological risk governance,” Ji told The Defender.
Epstein involved in ‘strain pandemic simulation’ two years before COVID
By 2017, these conversations led to proposals for pandemic simulations.
In a January 2017 iMessage thread between Epstein and an unidentified physician seeking help in finding a new job, the physician cited “expertise with public health security.”
The physician, who had experience at the U.N., WHO, Gates Foundation and World Bank, said he “just did pandemic simulation,” which could become a “big platform.”
Referring to Gates, the physician told Epstein, “He hates mental health but he’s crazy about vaccines and autism stuff. That could be start to a more broad conversation.”
A March 2017 email chain, which included Epstein and Gates, discussed efforts by the then-bgC3, Gates’ private strategic office, to develop “Follow-up recommendations and/or technical specifications for strain pandemic simulation.”
Ji noted that in 2017, the Coalition for Epidemic Preparedness Innovations (CEPI) was launched at the World Economic Forum (WEF), with Gates Foundation funding and a goal of creating “pandemic-busting vaccines” within 100 days. Later that year, the World Bank issued the first-ever pandemic bonds.
Event 201, held just six weeks before the first publicly acknowledged COVID-19 cases were announced, involved the Gates Foundation, WEF and the Johns Hopkins Center for Health Security. Global financial institutions, media organizations and intelligence agencies also participated.
The simulation focused on the response to a novel coronavirus outbreak by governments, pharmaceutical companies, media outlets and social media platforms.
Ji said the Epstein Files don’t show that COVID-19 was planned or manufactured, or that Event 201 led to COVID-19. Instead, they prove that “the institutional infrastructure to capitalize on exactly this kind of crisis was already built, tested, staffed, and insured.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
No, Al-Jazeera, Climate Change Hasn’t Altered African Flood and Drought Patterns
By Anthony Watts | Climate Realism | February 3, 2026
Al Jazeera (AJ) recently published an article titled “Drought in the east, floods in the south: Africa battered by climate change” by Haru Mutasa, in which the reporter details recent experiences of drought in East Africa and flooding in southern Africa, asserting that those weather events are proof that climate change is battering the continent. This is false. The article relies on flimsy content such as personal observation, interviews, and evocative imagery to imply causation, ignoring data and trends that show no appreciable changes in flood or drought patterns over time.
Mutasa asserts that “rising seas and intensifying storms” and shifting rainfall patterns are already devastating livelihoods, citing the author’s personal field observations as evidence of a broader climate crisis. Readers are shown photos of dry riverbeds, dead livestock, submerged neighborhoods, and distressed residents, then invited to connect these scenes directly to global warming. The emotional impact is real, but emotion is not evidence.
Let us start with AJ’s most basic error: weather is not climate. Climate is defined by long-term patterns measured over decades, typically 30 years or more. A drought in one region followed by floods in another over a few weeks or months says nothing about a durable climate trend. Africa’s climate has always been highly variable, with sharp swings driven by ocean–atmosphere cycles such as the El Niño–Southern Oscillation and the Indian Ocean Dipole. Short-term extremes—sometimes back-to-back—are a known feature of the region, not a recently discovered diagnostical proof of climate change.
The historical record bears this out. Southern and eastern Africa experienced severe droughts and catastrophic floods long before modern greenhouse gas emissions rose. Mozambique’s Limpopo River basin, featured prominently in the article’s flood imagery. The area has a long history of major inundations, including the devastating 2000 Mozambique floods, which displaced hundreds of thousands and occurred during a strong El Niño year. East Africa’s Horn has likewise seen repeated, multi-year droughts throughout the twentieth century, interspersed with episodes of extreme rainfall. These precedents matter because they show that today’s events are consistent with a long pattern of variability rather than proving a novel climate regime.
In fact, science has shown a 50-year seasonal variability across centuries in East African droughts and floods recorded in lake sediments.
When measured data are consulted instead of anecdotes, the alarm bells fade. Climate at a Glance summarizes the global evidence in “Floods” and “Drought,” explaining that there is low confidence in any increasing trend of global flood frequency or magnitude and that drought trends are regionally mixed, not universally worsening. These conclusions align with the cautious language used by the Intergovernmental Panel on Climate Change (IPCC) Sixth Assessment Report (AR6), which emphasizes uncertainty and regional variability rather than blanket claims of intensification.
The AJ article substitutes interviews for analysis. Quoting local residents and aid workers about hardship may document suffering, but it does not diagnose cause. Infrastructure deficits, land-use changes, deforestation, river management, dam releases upstream, population growth in floodplains, and limited early-warning systems all play decisive roles in disaster outcomes across Africa. Climate Realism has repeatedly shown how media coverage overlooks these factors while attributing complex events to climate change by default, as catalogued in its Africa-related reporting and extreme-weather analyses accessible via Climate Realism’s search on floods and droughts and Climate Realism’s coverage of drought claims.
Even within the article’s narrative, local management issues loom large. Mutasa notes dam releases in South Africa’s Mpumalanga province sent additional water downstream into Mozambique—an operational decision with immediate hydrological consequences that has nothing to do with global temperature or climate change. Treating such factors as footnotes while elevating climate change as the primary driver of flooding misinforms readers about where real risk reduction lies.
Serious climate reporting distinguishes between events and trends, and between personal experiences and measured evidence.
By presenting interviews and moment-in-time scenes as confirmation of a continent-wide climate verdict, Al Jazeera is misleading its audience by making a causal connection where data show none. Africa’s vulnerability to climate and weather extremes is real, but the causes are multifaceted and long-standing. Ignoring historical precedents and measured trends in favor of an alarming narrative certainty does not inform the public; it misleads it with false headlines.
Bad Science, Big Consequences
How the influential 2006 Stern Review conjured up escalating future disaster losses
By Roger Pielke Jr. | The Honest Broker | February 2, 2026
For those who haven’t observed climate debates over the long term, today it might be hard to imagine the incredible influence of the 2006 Stern Review on The Economics of Climate.1
The Stern Review was far more than just another nerdy report of climate economics. It was a keystone document that reshaped how climate change was framed in policy, media, and advocacy, with reverberations still echoing today.
The Review was commissioned in 2005 by the UK Treasury under Chancellor Gordon Brown and published in 2006, with the aim of assessing climate change through the lens of economic risk and cost–benefit analysis. The review was led by Sir Nicholas Stern, then Head of the UK Government Economic Service and a former Chief Economist of the World Bank, from the outset giving the effort unusual stature for a policy report.
As the climate issue gained momentum in the 2000s, the Review’s conclusions that climate change was a looming emergency and that virtually any cost was worth bearing in response were widely treated as authoritative. The Review shaped climate discourse far beyond the United Kingdom and well beyond the confines of economics.
One key aspect of the Stern Review overlaps significantly with my expertise — The economic impacts of extreme weather. In fact, that overlap has a very surprising connection which I’ll detail below, and explains why back in 2006 I was able to identify the report’s fatal flaws on the economics of extreme weather in real time, and publish my arguments in the peer-reviewed literature soon thereafter.
But I’m getting ahead of myself.
I have just updated through 2025 the figure below that compares the Stern Review’s prediction of post-2005 increases in disaster losses as a percentage of global GDP with what has actually transpired.
Specifically, the figure shows in light grey the Stern Review’s prediction for increasing global disaster losses, as a percentage of GDP, from 2006 through 2050.2 These values in grey represent annual average losses, meaning that over time for the prediction to verify, about half of annual losses would lie above the grey bars and about half below.
The black bars in the figure show what has actually occurred (with details provided in this post last week). You don’t need fancy statistics to see that the real world has consistently undershot the Stern Review’s predictions over the past two decades.
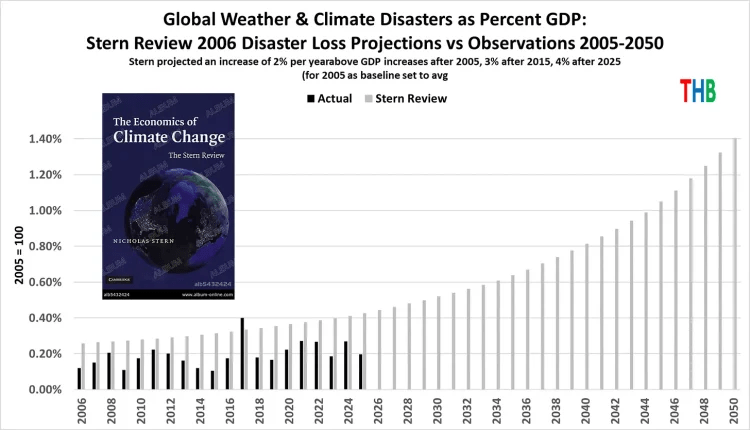
The Stern Review forecast rapidly escalating losses to 2050, when losses were projected to be about $1.7 trillion in 2025 dollars. The Review’s prediction for 2025 was more than $500 billion in losses (average annual). In actuality losses totaled about $200 billion in 2025.
The forecast miss is not subtle.
How did the Stern Review get things so wrong?
The answer is also not subtle and can be summarized in two words: Bad science.
Let’s take a look at the details. The screenshot below comes from Chapter 5 of the Review and explains its source for developing its prediction, cited to footnote 26.

As fate would have it, footnote 26 goes to a white paper that I commissioned for a workshop that I co-organized with Munich Re in 2006 on disasters and climate change.
That white paper — by Muir-Wood et al. — is the same paper that soon after was played the starring role in a fraudulent graph inserted into the 2007 IPCC report (yes, fraudulent). You can listen to me recounting that incredible story, with rare archival audio.
But I digress . . . back to The Stern Review, which argued:
If temperatures continued to rise over the second half of the century, costs could reach several percent of GDP each year, particularly because the damages increase disproportionately at higher temperatures . . .
The report presented its prediction methodology in the footnote 27, shown in full below, which says: “These values are likely underestimates.”

Where do these escalating numbers come from? Who knows.
They appear to be just made up out of thin air. The predictive numbers do not come from Muir-Wood et al., who do not engage in any form of projection.
The 2% starting point for increasing losses — asserted in the blue highlighted passage in the image above — also does not appear in Muir-Wood et al. which in fact says:
When analyzed over the full survey period (1950 – 2005) the year is not statistically significant for global normalized losses. . . For the more complete 1970-2005 survey period, the year is significant with a positive coefficient for (i.e. increase in) global losses at 1% . . .
The Stern Review seems to have turned 1% into 2% and failed to acknowledge that over the longer-period 1950 to 2005, there was no increasing trend in losses as a proportion of GDP. The escalating increase in annual losses from 2% to 3%, 4%, 5%, 6% every decade is not supported in any way in the Stern Review, nor is it referenced to any source.
When the Stern Review first came out, I noticed this curiosity right away, and did what I thought we scholars were expected to do when encountering bad science with big implications — I wrote a paper for peer review.
My paper was published in 2007 and clearly explained the Muir-Wood et al. and other significant and seemingly undeniable errors in the Stern Review.
Pielke Jr, R. (2007). Mistreatment of the economic impacts of extreme events in the Stern Review Report on the Economics of Climate Change. Global Environmental Change, 17(3-4), 302-310.
I explained in that paper:
This brief critique of a small part of the Stern Review finds that the report has dramatically misrepresented literature and understandings on the relationship of projected climate changes and future losses from extreme events in developed countries, and indeed globally. In one case this appears to be the result of the misrepresentation of a single study. This cherry picking damages the credibility of the Stern Review because it not only ignores other relevant literature with different conclusions, but it misrepresents the very study that it has used to buttress its conclusions.
Over my career in research, I’ve had some hits and some misses, but I’m happy to report that I got this one right at the time and it has held up ever since. Of course, perhaps a more significant outcome of this episode, and a key part of my own education in climate science, is that my paper was resoundingly ignored.
One reason that science works is that scientists share a commitment to correct errors when they are found in research, bringing forward reliable knowledge and leaving behind that which doesn’t stand the test of time.
I learned decades ago that in areas where I published, self-correction was often slow to work, if not just broken. Over the decades that pathological characteristic of key areas of climate science has not much improved (e.g., see this egregious example).
The Stern Review helped to launch climate change into top levels of policy making around the world. Further, we can draw a straight line from the Review to the emergence of (often scientifically questionable) “climate risk” in global finance a decade later. It still rests on a foundation of bad science.
1 My ongoing THB series on insurance and “climate risk” in finance prompted me to revisit the 2006 Stern Review, hence this post.
2 Note that the Review explicitly referenced the tabulation of global economic losses from extreme weather events as tabulation by Munich Re, which is the same dataset that I often use, such as in last week’s THB post on global disaster losses. The comparison here is thus apples to apples.
Featured Video

Total War – Attacking Nuclear Plants, Desalination & Infrastructure
or go to
Aletho News Archives – Video-Images
From the Archives
Strike on Israel Shows US Bases Near Iran Are ‘Achilles Heel’
By Svetlana Ekimenko – Sputnik – 14.04.2024
Fears of a greater Middle East escalation were triggered after Iran launched a massive drone and missile attack against Israel, aided by Hezbollah and the Yemeni Houthis. Iran said the attack was in response to Israel’s bombing of the Iranian consulate in Damascus, Syria, which killed seven members of the elite Revolutionary Guard Corps.
Iran’s massive retaliatory attack on Israel from its own territory is a sign that the conflict could “escalate out of control.”
Michael Maloof, a former senior security analyst in the office of the US secretary of defense, told Sputnik that the first ever direct Iranian attack on Israel set a dangerous precedent.
“My concern is that this could easily escalate into something not only between Iran and Israel, but beyond the Middle East region,” he said.
Iran’s assault, which it stated was an act of “self-defense” after the Israeli strike on its consulate in Damascus, was originally intended to be a “limited” one, said Maloof.
Iran first sent in “swarms of drones with lights on as a sign of psychological warfare,” but sending in cruise and ballistic missiles by Tehran was a “distinct escalation,” said Maloof.
The scale of Iran’s attack on Israel suggests that Tehran was sending a message, demonstrating that it possesses “extraordinary capabilities,” said Maloof. … continue
Blog Roll
 Aletho News
Aletho News- Hungary blasts ‘fake’ EU accusation
- SAFE Debt Trap: Poland’s €43.7 Billion Bet on Unipolar Illusion
- War on Iran threatens global Gulf capital flows: FT analysis
- Mossad De Facto Admits To Inciting Riots In Iran
- Tehran: World grown thoroughly exhausted with US-Israeli ‘false flag storylines’
- Trump ‘stuck between a rock and a hard place’, lacks Iran war strategy: Ex-CIA chief
- Trump’s bombardment of fake news so far is working quite well. But where is it heading?
- Iran to Mine Sea Lanes in Persian Gulf in Case of Attack – Defense Council
- Barak blasts Netanyahu: ‘Stop lying – you can’t destroy Iran’s nuclear, missile capabilities’
- Trump backs down on Iran strikes; Tehran denies any talks
- If Americans Knew
- From Sde Teiman, the truth about Israel’s military justice system has been set free
- Child denied life-saving bone marrow transplant by Israel ‘because he is from Gaza’
- Raffi Berg: BBC Middle East Editor Exposed as CIA, Mossad Collaborator
- Jerusalem Archbishop Rebukes Netanyahu’s Statements on Christianity
- US to embed Palantir AI across entire military: Report
- Israeli-US war on Iran to drag on “a few more weeks” – Not a ceasefire Day 164
- Lebanon deaths top 1,200; Palantir AI to be embedded across US military – Not a ceasefire Day 163
- Israel’s assassination game: Take all pragmatists off the board
- Food shortages return to Gaza as Israel tightens aid restrictions under the cover of its war on Iran
- Trump demands trillions in payments from Gulf countries, billions from Harvard – Not a ceasefire Day 162
- No Tricks Zone
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis
- New Study Documents A 20-Year Pause In Arctic Sea Ice Decline – Driven By Internal Variability
- Wake-up Call: Survey Shows Majority Of Germans Now Favor Postponing Climate Targets!
- Televised! Leading German Political Candidate Tells Schoolchildren CO2 Makes Sun Hotter!
