While America panics, Europe quietly recalibrates Covid-19 vaccine policy
Maryanne Demasi, PhD | September 3, 2025
As of 1 September, Sweden no longer recommends Covid-19 vaccination for children unless an individual medical assessment finds they are at increased risk of severe disease.
Even then, it is only available with a doctor’s prescription.
Adults are eligible for a single dose only if they are 75 and older, or belong to defined risk groups.
It is a strikingly cautious policy — yet in Sweden, there is no sense of crisis. Public health officials describe it as a proportionate step, aligned with the evidence.
By contrast, in the United States, the temperature has been rising over the narrowing of Covid-19 vaccine policy. The medical establishment has long been hostile toward Health Secretary Robert Kennedy Jr, but in recent weeks the attacks have escalated.
This week in the New York Times, nine former directors of the Centers for Disease Control and Prevention (CDC) warned that his decisions mean “children risk losing access to lifesaving vaccines.”
On ABC TV, outgoing CDC official Dr Demetre Daskalakis intensified the rhetoric, claiming he “only sees harm coming” for America’s children. The language was deliberately alarming and intended to signal an emerging catastrophe.

Dr Demetre Daskalakis, former director, CDC National Center for Immunization & Respiratory Diseases.
In reality, though, the policies under review in the US look more like a belated effort to bring American practice closer to what Europe has already done.
The CDC’s own data illustrate why recalibration makes sense.
Figures show that the risk of children dying from Covid-19 equates to roughly 1 in 810,000 per year (0.000123%) — an infinitesimally low risk.
It’s even lower for children without underlying conditions, closer to 1 in 1.75 million (0.000057%).
Despite these tiny mortality figures, Daskalakis warned that half of infants hospitalised for Covid-19 last season had “no underlying conditions.”
But that claim paints a distorted picture.
A Covid-19 hospitalisation is defined as “a positive SARS-CoV-2 test ≤14 days before admission or during hospitalisation,” meaning any child treated for a broken arm or routine surgery but testing positive, is still counted as a Covid case.
When researchers examined hospital charts more closely, they found roughly 30% of paediatric Covid-19 admissions were ‘incidental’ – in other words, they were hospitalised with Covid, not for Covid.
CDC’s adult data showed a similar pattern.
Other countries ahead of the curve
Across Europe and beyond, other nations are moving in the same direction as Sweden.
The United Kingdom has also tightened eligibility as it heads into autumn, limiting Covid boosters to people over 75, nursing-home residents, and those with weakened immune systems.
Its guidance notes that “in the current era of high population immunity to Covid-19, additional Covid-19 doses provide very limited, if any, protection against infection and any subsequent onward transmission of infection.”
These are targeted, risk-based policies aligned to measurable benefits.
Australia, too, has shifted. In May, the Department of Health quietly updated its immunisation handbook to state that healthy children and adolescents under 18 without medical conditions no longer need the Covid-19 vaccine.
There was no press conference, no ministerial statement, no media blitz. And most notably, no outrage from the medical establishment.
Taken together, these changes show nations with advanced health systems are adjusting policies in response to the evidence.
Unlike in the US, no one accuses countries like Sweden, Britain, or Australia of ‘sacrificing children’ by narrowing access to Covid-19 vaccines.
Hepatitis B on the radar
On September 18-19, the CDC’s Advisory Committee on Immunization Practices (ACIP) will meet to vote on various issues, including the current hepatitis B schedule.
Daskalakis warned that at its upcoming meeting, ACIP might “try to change the birth dose,” arguing that public health only gets “one bite of that apple” to vaccinate newborns against hepatitis B.
But several advanced European programs already do not give a universal day-one dose.
Instead, they target it to babies of mothers who test positive for hepatitis B, since most are screened in hospital, and begin routine doses later in infancy.
Denmark follows this approach. It is mainstream policy, endorsed by national health authorities, and no one suggests Danish babies are being left unprotected.
Scrutiny, not sabotage
The criticism of ACIP has been fierce.
Current members are branded as “dangerous” or anti-vaccine when their real offense is pressing for increased scrutiny and asking difficult questions. That is what an advisory committee is meant to do.
Kennedy is accused of sabotaging access to vaccines, but his approach is simply a call for the ‘gold standard’ science that Americans were promised by this administration.
As FDA Commissioner Marty Makary said this week, the CDC is a “broken” agency. That is why proportional policies and humility matter.
The way forward is not to alarm Americans with talk of bans or lost access to vaccines. It is to deliver risk-based, evidence-driven recommendations, as peer nations already do, and to be candid about uncertainty.
That is how public health begins to rebuild trust…the trust Kennedy says he now hopes to restore.
Wrong, CBS and Other Media Outlets, Abrupt Antarctic “Climate Shifts” Are Not New or Necessarily Catastrophic
By Anthony Watts and H. Sterling Burnett | ClimateRealism | August 29, 2025
A recent CBS News article, “Abrupt Antarctic climate shifts could lead to ‘catastrophic consequences for generations,’ experts warn,” claims that Antarctica is on the brink of irreversible collapse due to climate change, warning that sea levels could rise by meters and that “catastrophic consequences for generations” are looming. This is false or, at best, deeply misleading. The actual data and history of Antarctic ice show that “abrupt changes” are neither unprecedented nor a reason to panic. Natural variability and cyclical shifts are being ignored in favor of sensational headlines pushing the increasingly untenable climate crisis narrative.
CBS was not alone in pushing the Antarctic climate crisis narrative. On 21 August 2025, The Australian Broadcasting Corporation (ABC) joined the chorus of media outlets with alarming headlines warning of pending ice collapse, publishing a report claiming Antarctica is undergoing “rapid, self-perpetuating changes” that are “potentially irreversible.” Each of the reports cited a new Nature review led by Professor Nerilie Abram, as the source of the information for their alarming articles.
ABC’s article presents Antarctica as being in a state of runaway decline, with imminent threats to emperor penguins and global sea levels, parroting language from the Abram paper as if it were observed fact, rather than the speculative synthesis of research papers that the Nature study cites. CBS, ABC, and other media outlets are covering this story as if a tipping point is upon us—but a closer look at the evidence reveals otherwise.
CBS News warns:
Abrupt and potentially irreversible changes in Antarctica driven by climate change could lift global oceans by meters and lead to ‘catastrophic consequences for generations,’ scientists warned Wednesday. … After increasing slightly during the first 35 years that satellite data was available, Antarctic sea-ice cover plunged dramatically over the last decade.
Australia’s ABC News, meanwhile, uncritically repeats Abram’s claims and, describing the Antarctic as “rapidly, self-perpetuating” on the cusp of collapse, while offering little discussion of data—leaning instead on worst-case modeling and literature reviews.
Antarctic data and an examination of its history show that such events have happened previously, long before anyone was worried about human-caused climate change, and they are not self-perpetuating but rather, seem cyclical in nature.
The CBS article claims that “Antarctic sea-ice cover plunged dramatically over the last decade,” citing a “regime shift” since 2014. ABC News, echoing the same theme, refers to a sudden and supposedly “irreversible” decline. But both articles omit key facts, among them:
- The “Abrupt” Decline Follows Decades of Expansion. Satellite measurements of Antarctic sea-ice began in late 1978. For most of the next 36 years, Antarctic sea-ice was stable or increasing, setting multiple record highs between 2007 and 2014. In October 2014, the National Snow and Ice Data Center (NSIDC) reported: “Antarctic sea-ice extent set an all-time record high for the third straight year.” This expansion occurred for more than 30 years during the period when the Earth was warming, contradicting claims that warming inevitably reduces Antarctic sea-ice.
- The recent sharp declines since 2016 are real, but as the most robust satellite records show, these represent a regime shift within a variable system—not evidence of permanent or “runaway” collapse as one recent paper detailed.
- Evidence of Antarctica’s history shows that natural variability dominates changes in Antarctica. Longer reconstructions, stretching back to 1905, confirm that Antarctic sea-ice has experienced periods of large growth and subsequent declines over the past century. One 2020, study demonstrated that natural variability, including the influence of atmospheric and oceanic circulation, have likely played a role in any recent changes, as they drove such changes in the past.
As importantly as all this is, concern for the recent decline in sea ice is largely misplaced since, as even CBS news acknowledged in its story, [f]loating sea ice does not significantly add to sea level when it melts . . ..” As a result, neither the “record setting” expansion of sea-ice spanning the late 20th and early 21st century nor the recent decline significantly effect sea levels.
Perhaps that’s why the new stories tried to tie the sea-ice decline to rising seas indirectly saying the sea ice retreat, “ . . . does replace white surfaces that reflect almost all of the sun’s energy back into space with deep blue water, which absorbs the same amount instead.”
The problem here is, there is no evidence the earlier multidecade expansion of sea-ice or the recent decline has a causal connection to ice growth or expansion on mainland Antarctica, the latter of which could impact sea levels. Indeed, the record indicates that for some of the period when sea-ice was expanding, Antarctica was losing mass, and now, while it is in decline, Antarctica is gaining ice on net, reducing sea level rise.
Shifting focus from sea-ice to Antarctica’s mainland, the CBS and ABC News shift attention to recent ice losses on the West Antarctic ice sheet and in particular the declining Thwaites glacier.
When discussing ice sheets, both outlets repeat claims that the West Antarctic Ice Sheet has crossed a point of no return. But they fail to mention that West Antarctica sits atop a tectonic rift system with elevated geothermal heat flux, which drives melting from below, regardless of atmospheric conditions. In short, subsurface volcanic activity or heating from tectonic shifts is melting the region’s ice from below, and causing increased flow into the sea.
Indeed, Direct borehole measurements, aeromagnetic surveys, and radar-based research confirm anomalously high heat flow in the region from beneath the mass. This subglacial influence helps explain why areas like Amundsen and Thwaites behave differently from the stable East Antarctic.
Also, the northern Antarctic Peninsula, which is frequently highlighted for its instability, extends north of the Antarctic Circle into sub-Antarctic latitudes. Its climate and dynamics cannot be generalized to the rest of the continent according to NASA Earth Observatory in 2014.
Climate Realism has previously discussed the causes and consequences of ice loss on the Antarctic peninsula and in the West Antarctic multiple times previously, here and here, for example, in each case debunking a media claim that humans are behind the loss.
Antarctica’s ice loss is important, CBS and ABC tell us, because the Antarctic Ice Sheet’s collapse could “raise sea levels by meters,” threatening “hundreds of millions.” But the actual rate of global sea level rise, measured by satellites and tide gauges, is about 3 millimeters per year as detailed in Climate at a Glance: Sea Level Rise. At this rate, it would take 333 years to reach even a single meter of rise.
The idea of meters of sea level rise by 2100 is rooted in computer models, not observation. Even the Intergovernmental Panel on Climate Change (IPCC) concedes that melting the East Antarctic Ice Sheet would require thousands of years and temperature increases far beyond any plausible scenario this century:
Loss of the East Antarctic Ice Sheet (EAIS) is very unlikely over this century and beyond under scenarios of greenhouse gas emissions considered in this report. Complete loss of the EAIS would require sustained global warming significantly above the levels projected for this century, and would take thousands of years.
Putting the supposed amount of Antarctic glacier loss in context is important, because as a percentage of the continent’s total ice volume, recent reported losses from the continent are miniscule, contrary to media hype. See the figure below, as presented at Climate at a Glance Antarctic Ice Melt.
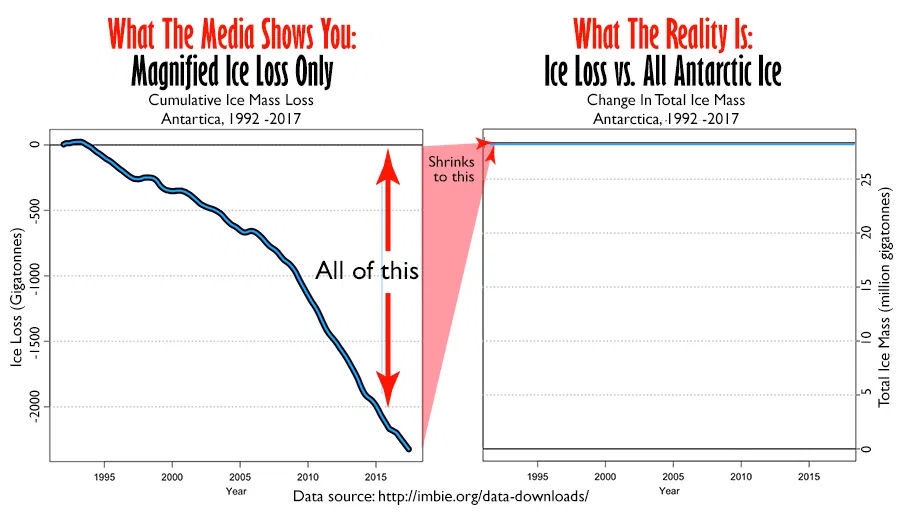
Figure: Comparison of satellite data for Antarctic ice mass loss. Cumulative ice mass loss on the left and that same data compared to the total mass of ice on the right.
Data source: http://imbie.org. Graphs originally by Willis Eschenbach, adapted and annotated by Anthony Watts.
Describing the ice changes in Antarctica as “irreversible” or “runaway” is nothing more than alarming speculation that ignores evidence to the contrary.
CBS, ABC, and the other mainstream media outlets touting the study’s warnings about the future also ignore the fact that contrary to the implication of the study, Antarctica is actually gaining ice at present and has for the past couple of years.
As discussed at Climate Change Weekly, In late April and early May, mainstream media outlets ran dozens of stories discussing the findings of a recent study that showed Antarctica’s ice mass was growing. The outlets called the ice and snow gain “astonishing,” “surprising,” and “shock[ing]” and said it “startled the scientific community.” That’s right, recent research shows that the Antarctic has not warmed over the past seven decades and that the vast bulk of Antarctica experienced substantial ice growth in the past couple of years, reversing the decline reported in Nature that ABC, CBS, and other outlets are writing about. Glacial melt which had been contributing to sea level rise reversed itself over a period of three years, adding mass and cutting Antarctica’s contribution to sea level rise.
Any reporting that omits the physics, history, and current trends is incomplete and misleading. And any story that blames global warming for glacier melt in Antarctica and subsequent sea level rise, when the continent has not experienced warming, glaciers on the whole are growing and thus reducing sea level rise, is just false.
Both ABC and CBS also point to emperor penguin breeding failures as a result of climate change, implying an existential threat across the species. Yet the 2025 study making these claims conducted a regional and local survey of selected colonies from 2009 to 2024, reporting a 22 percent decline in those specific locations. It didn’t look at the health of emperor penguin colonies across Antarctic as a whole. The authors themselves specifically cautioned that their results may not represent the entire Antarctic coastline—a vital caveat that ABC and CBS’s stories lack. With emperor penguins living for decades, a 15-year record is simply too short to establish population trajectories. These penguins have survived warm and cold phases across the Holocene. To suggest continent-wide extinction risk by 2100 is not supported by the available evidence.
In the end, history shows that the expansion and contraction of Antarctic sea-ice are natural features of a highly variable system. Short-term losses are not proof of a “runaway” tipping point; rather, they are well within known ranges of natural variability.
CBS, ABC, and other media outlets are constructing a narrative of Antarctic collapse by cherry-picking short-term declines, ignoring decades of stability and increase, omitting key physical context, and leaning on speculative reviews. Climate Realism has factually debunked similar media scare stories in the past, here and here. The actual Antarctic observational record reveals a dynamic system—one that expands and contracts, shaped by natural variability, oceanic and atmospheric cycles, and unique geographic barriers.
The catastrophic claims ABC and CBS are parroting are not only unsupported, they fly in the face of decades of data and scientific understanding. Had the mainstream media displayed a little investigative curiosity, it would have questioned the recent study’s findings, since the evidence clearly shows Antarctic “climate shifts” are not a harbinger of doom but another chapter in a long story of natural change.
RFK JR. LAUNCHES HHS PROBE INTO SSRIS, SCHOOL SHOOTINGS
The HighWire with Del Bigtree | August 28, 2025
The tragic mass shooting at a Minneapolis Catholic school by a 23-year-old shooter, who identified as transgender, has reignited concerns about a possible connection between SSRIs and violent mass shootings. HHS Director Robert F. Kennedy Jr. announced that the National Institutes of Health will investigate whether these widely prescribed antidepressants may play a role in fueling such acts of violence.
IPCC Likely to Start Blaming Humans For Weather as Friederike Otto Takes Key Role
The foxes are now firmly in charge of the chicken coop
By Chris Morrison | The Climate Skeptic | August 24, 2025
Last December the Daily Sceptic published an article reporting that the Intergovernmental Panel on Climate Change (IPCC) could be preparing to start blaming humans for individual bad weather events. Straws-in-the-wind stuff, based on an IPCC press release claiming a century of burning hydrocarbons had resulted in “more frequent and intense extreme weather events”. To date, the IPCC has failed to detect that humans using hydrocarbons have led to worse bad weather on the simple scientific ground that it is impossible, with current data sources, to remove the overwhelming role of natural variation. Our story was prescient. It’s all change at the IPCC, with the appointment of Attribution Queen Friederike Otto and a troop of fellow attributionists to take charge of writing a new chapter on extreme weather for its forthcoming seventh climate science assessment report. With the foxes now in charge of the chicken coop, political order can be restored, with the IPCC science more closely aligned with current Net Zero political requirements.
Dr Otto, who runs the Green Blob-funded World Weather Attribution (WWA) operation out of Imperial College, has been appointed the co-leader of the extreme weather chapter. “It will be a lot of work, but it also gives a lot of opportunity to shape the structure and focus of the chapter”, she notes. WWA paymasters who include the Grantham, European Climate and Bezos Earth foundations will no doubt be delighted with this news. Helping her shape the narrative going forward will be a number of writers who are all in on the single event attribution game. The science writer Roger Pielke Jr notes that the team is “stacked” with people who focus on extreme event attribution (EEA) – “far out of proportion to their presence in the field”. Few of the authors, if any, he adds, have expertise in the IPCC’s conventional framework for detection and attribution (D&A), and some have no publications on either detection or attribution. He points out that nine out of 20 of the authors focus their research on EEA, including two of the three coordinating leads.
One-off weather attribution is a pseudoscience based mostly on the flimsy findings of computer models. Two imaginary atmospheres with different levels of carbon dioxide are compared, and, hey presto, claims are made that a weather event is x times more likely to be caused by humans.
Complete with a suitable large multiple, the results are distributed to ‘join-the-dots’ merchants such as Jim Dale, as well as mainstream media climate desks. Worldwide publicity is given to ‘science’ findings that obviously fail the Popperian principle in that they cannot be tested and falsified. The non-peer-reviewed information is pushed out quickly in a press release, with the disaster fresh in the media minds. Climate fear levels in the general population are kept nicely topped up – job done. Climate ‘deniers’ can be dismissed with a head-in-the-hands sigh and a “can’t you even see the evidence outside your own window?” Of course, the entire unquestioning media meltdown is based on the false notion that computer models produce ‘evidence’, when in reality they just supply opinions.
In 2019, the former BBC Today editor Sarah Sands wrote a foreword for a WWA journalist guide to reporting extreme weather. She recalled the time when the UK politician Nigel Lawson managed to slip into a BBC broadcast that there had been no increase in extreme weather. “I wish we had this guide for journalists to help us mount a more effective challenge to his claim,” she gushed. These days, she enthused, attribution studies have given us significant insight into the horsemen of the climate apocalypse.
In the past, the IPCC has failed to detect and attribute most extreme weather to human involvement, and it did not expect to do so for the rest of the century. It is becoming increasingly obvious that computer models are poor at replicating the complex atmosphere and offer little guidance for future climate projections. Detecting changes in the climate requires many decades of observation. The idea that one event can shortcut an understanding of a long-term trend, when there is no way of knowing if it is a statistical outlier, is for the birds. Collecting one-offs from a number of different weather types and claiming that humans control the weather would just be silly if it wasn’t designed to induce mental anguish and screw oil and gas firms in court.
With many of the poster scares of climate collapse having to be retired – even melting Arctic sea ice has gone on strike for 20 years – the desperation of activists is getting noticeably worse. One of the last throws of the dice is running bad weather scares. Net Zero is dead in the United States, and a recent official government report stated that computer models offered “little guidance” on how the climate responds to higher CO₂ levels. It also noted that most extreme weather events are not increasing, while weather attribution claims are challenged by natural climate variation, along with an admission that they were originally designed with ‘lawfare’ in mind.
WWA was set up in 2014 by Otto and Dr Geert Jan van Oldenborgh, with Green Blob-funded Climate Central providing support and help with securing funding. These days, the operation notes that its methods have been developed over time and “peer reviewed in dedicated methods publications”. A link to the claimed peer review is helpfully provided on its website, and this brings up a paper titled ‘Pathways and Pitfalls in Extreme Event Attribution.’ Interestingly, the first peer reviewer is Dr Geert Jan van Oldenborgh, while the fifth is Dr Friederike Otto.
In 2022, a group of four Italian scientists led by Professor Gianluca Alimonti published a paper in Nature based on data used by the IPCC that concluded there had been little change in extreme weather events. Such findings and data are easy to find, although mainstream media is mostly absent from the search. On the basis of their factual findings, the Italians suggested there was not a climate crisis. All hell subsequently broke loose, and an alliance of activists, journalists and scientists managed to get the paper retracted a year later. One of those activists was Otto who said the authors were “of course” not writing their paper in good faith. “If the journal cares about science they should withdraw it loudly and publicly, saying that it should never have been published”, she added. At the time of the infamous affair, Pielke observed: “The abuse of the peer-reviewed process documented here is remarkable and stands as a warning that climate science is as deeply politicised as ever with scientists willing to exert influence on the publication process both out in the open and behind the scenes”.
Chris Morrison is the Daily Sceptic’s Environment Editor. Follow him on X.
‘Medically Reckless’: AAP Pushes Mental Health Screenings for Kids as Young as 6 Months Old
‘Parents must know they have the right to refuse these screenings’
By Jill Erzen | The Defender | August 27, 2025
Children as young as 6 months old should begin regular screenings for mental or developmental issues at every well-child visit, the American Academy of Pediatrics (AAP) said in a clinical report released Aug. 25.
Critics of the report fear the recommendations will lead to misdiagnosing and further overmedicating children.
“It is alarming that pressure is being put on pediatricians by the AAP to actively look for signs of depression in a 2-year-old,” Stephanie Seneff, Ph.D., a senior research scientist at MIT, told The Defender.
Pushing mental health screening for children leads to the expectation of psychiatric problems being woven into standards of care, said Robert Whitaker, author of “Anatomy of an Epidemic: Magic Bullets, Psychiatric Drugs, and the Astonishing Rise of Mental Illness in America.”
“And the screening instruments the pediatricians will employ will have been constructed to identify a certain percentage of children as being in need of treatment,” he said.
The AAP report, published online in the journal Pediatrics, recommends that mental health screening begin at 6 months old and continue as part of well-child visits at ages 1, 2 and 3. After age 3, screening would continue annually.
The report said as many as 1 in 5 children in the U.S., including kids as young as 2, have mental or behavioral issues such as depression, anxiety, ADHD (attention-deficit/hyperactivity disorder) or suicidal thoughts.
However, studies show mental health issues are commonly misdiagnosed. Depression has been falsely diagnosed 66% of the time, and generalized anxiety disorder has been incorrectly assessed 71% of the time.
“Parents should be more than just skeptical,” said Whitaker. “They should be alarmed by this push for ‘early detection.’ Screening of children, starting when they are very young, will of course lead a significant percentage to be diagnosed with one disorder or another.”
That diagnosis then “serves to pathologize the child, and that diagnosis may stick to the child for years, possibly through childhood and into adulthood,” he said. And a diagnosis “often will lead to a prescription for a psychiatric drug, and the scientific evidence on this is quite clear: over the long term, this will harm the child.”
Whitaker added:
“Or to put it another way, while screening and early detection is presented to the public as an effort to help the child, in reality it serves as an assault on the child’s right to be — to grow up without being tagged as ‘abnormal’ and forced to take a drug that will change the child’s capacity to experience the world.”
Screening toddlers for psychiatric disorders is ‘medically reckless’
The AAP claims rates of mental, emotional and behavioral problems in the U.S. are rising, and early detection will lead to intervention.
However, an August 2022 study in Preventive Medicine concluded that screening adolescents for depression does not reduce their treatment for suicidal behaviors.
A 2017 review found no evidence that screening children improves mental health outcomes, but instead raises the risk of potential harm and wasted resources.
“Screening babies, toddlers and schoolchildren for psychiatric disorders is medically reckless,” said Jan Eastgate, president of Citizens Commission on Human Rights (CCHR) International, a mental health industry watchdog.
She added:
“The questionnaires are based on a subjective and unscientific diagnostic system that pathologizes normal childhood behavior. Instead of helping families, they funnel children into a pipeline of psychiatric drugging — substances that can be addictive, damage the heart, and even drive them to suicide.”
The AAP, which represents 67,000 pediatricians in the U.S., stated that pediatricians are best equipped to work with families to identify issues early and provide children with the necessary help.
The AAP is also a lobbying organization. It spent between $748,000 and $1.18 million annually over the previous six years to advocate for its members, according to Open Secrets.
Some of the AAP’s biggest financial contributions come from major pharmaceutical companies, including Eli Lilly, GSK, Merck, Moderna and Pfizer.
In January 2024, an AAP study published in Pediatrics found that more children were being subjected to restraint drugs — antipsychotics used to sedate — because more children were being admitted to mental health facilities.
During the 2016-2021 study period, the analysis found a 141% increase in the use of restraint drugs overall, and longer inpatient stays. Pharmacological restraints tend to be used with greater frequency on autistic children, low-income children and children of color.
According to the mail-order pharmacy Express Scripts, prescriptions for antidepressants for teenagers increased 38% from 2015-2019.
The AAP has been diagnosing and medicating children for decades, and the data show it doesn’t benefit children, Whitaker said.
He added:
“Early detection will just amplify the harm that is already being done to so many children by diagnosis plus drug treatment.
“What we should be doing if so many of our children are struggling, starting at an early age, is fixing the environment for raising children in our country. The children’s struggles don’t tell of a problem within the child, but within our society, and diagnosing the child just puts the blame inside the child.
“This promotion of early detection. … It’s an assault on our children.”
‘Alarming list of serious side effects’
Selective serotonin reuptake inhibitors (SSRIs) are a first-line medication for children diagnosed with moderate to severe depression and anxiety. However, these medications carry a black box warning for a potential, though low, increased risk of suicidal thoughts, according to the AAP’s webpage, Antidepressants: Pediatric Mental Health Minute Series.
“SSRIs have an alarming list of serious side effects, the most egregious of which might be serotonin syndrome, which can cause death,” Seneff said. SSRIs raise levels of serotonin — a hormone and neurotransmitter that regulates mood.
While common side effects of SSRIs include diarrhea, headache, sleepiness and weight gain, the medications are also associated with serious adverse events, including heart rhythm changes, bleeding and thoughts of suicide or self-harm.
The risks of prescribing antidepressants are greater in children than in adults, Seneff said:
“A child’s developing brain will respond to these drugs in unpredictable ways. Early exposure to SSRIs could lead to permanent but currently unknown disruptions in brain development. We should rather be devoting our efforts to figuring out why so many kids are so emotionally disturbed today.”
Studies show benefits don’t outweigh risks
A 2025 study examined the link between antidepressant medications and fatal heart events. Researchers reviewed the death records of every adult ages 18-90 living in Denmark in 2010. In all age groups, the longer people used antidepressants, the more likely they were to die from sudden cardiac death.
In June 2022, the International Journal of Risk Safety Medicine published a study raising concerns about the first U.S.-approved SSRI antidepressant, fluoxetine. The authors reviewed several core studies used as the basis for the drug’s approval, and found that “the two pivotal trials showed that fluoxetine is unsafe and ineffective.”
Fluoxetine is the only SSRI antidepressant approved by the U.S. Food and Drug Administration (FDA) for treating major depression in patients as young as 8 years old. Yet, the FDA warns that children treated with antidepressants should be closely observed for agitation, irritability, suicidality and unusual changes in behavior.
The benefits of SSRIs have not been shown to outweigh the risks.
In 2022, FDA researchers published an extensive review of antidepressant studies in the BMJ. In total, the data from 1979-2016 covered 73,388 patients with diagnosed depression.
The analysis found that antidepressants outperformed placebo in just 15% of patients, and the benefit was almost entirely limited to people with the most severe forms of depression. For everyone else, the improvement was likely due to belief and expectation, not the drug itself.
The AAP recommendation for mental health screening was announced just weeks after Illinois became the first state to mandate mental health screenings for students in grades 3-12.
The Illinois law, set to take effect in the 2027-2028 school year, requires schools to conduct self-screenings annually using either digital or paper forms.
CCHR International said such subjective screening has shown an 84% “false positive” rate that could lead to teens being prescribed antidepressants, which in turn have been linked to an increase in suicide and/or acts of violence.
The source of such screening questionnaires can also be suspect, according to CCHR International.
The Patient Health Questionnaire-9 (PHQ-9) was first developed in 2001 and administered as a universal intervention in high schools to identify and treat depression, according to CCHR International. It was developed through a grant from Pfizer, the manufacturer of the antidepressant Zoloft (sertraline).
In 2010, the company made both its PHQ-9 and General Anxiety Disorder questionnaire available to primary care doctors “without copyright restriction and at no charge.” Prescriptions of sertraline jumped 33%, from almost 29 million prescriptions in 2004 to over 38 million in 2020.
“Parents must know they have the right to refuse these screenings,” Eastgate said. She added:
“Signing an ‘Opt-Out’ form is essential to protect their child from being falsely labeled with a mental disorder and drugged. Informed consent belongs to parents — not to a psychiatric screening checklist that has no scientific foundation and is often developed by pharmaceutical interests.”
Related articles in The Defender
How the American Academy of Pediatrics Betrayed Children Everywhere
By Clayton J. Baker, MD | Brownstone Institute | August 25, 2025
The prime directive of Western medicine, its golden rule, is expressed by the Latin maxim primum non nocere – first, do no harm. Unfortunately, the Covid era taught us that from the patient’s point of view, a better motto for our times might be caveat emptor – let the buyer beware.
Every medical student is taught that, first and foremost, they should not cause harm to their patients, and every doctor is familiar with this maxim. It is echoed in the Hippocratic Oath, and it forms the basis for the four pillars of medical ethics: autonomy, beneficence, nonmaleficence, and justice.
This rule, and the core tenets of medical ethics that it underpins, were all abandoned during the Covid era. They were replaced with a brutal, inhumane, and unethical martial-law-as-public-health approach to medicine. The results were unconstitutional lockdowns, prolonged school closures, suppression of early treatment, mandated vaccinations, and silencing of dissenting views. These abuses were justified by constant propaganda and lies from public health authorities, the medical establishment, the mainstream media, and medical professional associations.
Enter the American Academy of Pediatrics.
The American Academy of Pediatrics (AAP) is the largest professional association for pediatricians in the United States. Nearly one hundred years old, the AAP’s motto is “Dedicated to the Health of All Children.” But as with so much of the medical establishment, the Covid era revealed that the AAP has abandoned its stated mission, and in the process, it has betrayed children everywhere.
During the Covid era, no group was harmed more – or more unnecessarily – than children, who lost multiple years of education, socialization, and normal growth and development. Many millions of kids also received the fraudulently tested, toxic, experimental mRNA-based injections that were coercively imposed upon the population at large. Countless children have been harmed or killed by these products, with myocarditis being only the most universally acknowledged of the many toxicities associated with the shots.
Adding insult to injury, it was known from the beginning of the pandemic that the gain-of-function-produced SARS-CoV-2 virus affected children very mildly, rarely causing severe illness, and almost never killing them. Even at the height of the pandemic, an article in the preeminent journal Nature described pediatric Covid deaths as “incredibly rare.” A very large population-based Korean study from 2023 found the case-fatality rate in children from Covid to be well under 1 death in every 100,000 cases.
If no segment of the population was harmed more egregiously than children during the Covid era, few medical organizations betrayed their patient population more thoroughly than the American Academy of Pediatrics.
While the AAP has for many years taken questionable stances on a variety of issues, including the ever-enlarging pediatric vaccine schedule, “gender reassignment,” and others, at one early point during Covid, the AAP did attempt to advocate appropriately in the interest of children. It didn’t last long, however, and a review of this incident shows how the AAP, like so many other medical professional organizations, effectively sold its soul during Covid.
Summer 2020: The AAP Changes Its Tune on In-School Learning
From mid-March 2020, when the Covid lockdowns began, until the end of that school year in June, most American schoolchildren had been kept completely out of school. On July 9, 2020, the AAP released a statement arguing forcefully for the return of American schoolchildren back:
The AAP strongly advocates that all policy considerations for the coming school year should start with a goal of having students physically present in school. The importance of in-person learning is well-documented, and there is already evidence of the negative impacts on children because of school closures in the spring of 2020.
The July AAP statement went on to say that school closure “places children and adolescents at considerable risk of morbidity and, in some cases, mortality.” It went even further to state that:
… the preponderance of evidence indicates that children and adolescents are less likely to be symptomatic and less likely to have severe disease resulting from SARS-CoV-2 infection. In addition, children may be less likely to become infected and to spread infection.
All of these claims the AAP made in July 2020 were known to be true to those who did the proper research (as the AAP apparently had done), and they have been repeatedly and definitively confirmed in the following years.
I was acutely aware of that July 9, 2020, AAP statement. I used it as an important resource in my own advocacy during the summer of 2020 to try to get schools reopened for full-time learning in New York State by the fall. The July AAP document was a well-researched, well-constructed, and well-argued advocacy tool that supported all children’s best interests.
So far, so good. Very soon thereafter, however, the AAP shamefully succumbed to pressure from public health officials, teachers’ unions, and others pushing for continued school closures. By August 19, 2020, with school reopening imminent, the AAP suddenly “revised” their recommendations. The AAP dramatically changed its tune, stating that they would go along with whatever measures public health officials decreed:
… many schools where the virus is widespread will need to adopt virtual lessons and [AAP] is calling for more federal funding to support both models.
“This is on us – the adults – to be doing all the things public health experts are recommending to reduce the spread of the virus,” said AAP President Sara “Sally” H. Goza, M.D., FAAP.
In an act of cowardice and dereliction of duty, the AAP surrendered. It abandoned the strong and sound advocacy for normalizing children’s education contained in its July document. As a physician actively following the issues of the day surrounding Covid and publicly fighting for school reopening, I can testify that nothing changed regarding our knowledge of the virus that justified the AAP’s abdication of its responsibility to children. In fact, multiple foreign countries had already returned children to school without ill effect. The AAP’s capitulation significantly undermined school reopening efforts, especially in Blue states.
The AAP’s sudden and craven volte-face regarding in-school learning was just one of many disgraceful acts committed by medical associations during the Covid era, and it acted to the severe harm of schoolchildren across the nation. Millions of American schoolchildren continued to languish in “remote” or “hybrid” learning for the entire 2020-2021 school year. Many thousands simply dropped out of school, never to return.
In retrospect, the AAP cannot claim that they “didn’t know” enough to push for school reopening. Their July 2020 document proves they knew the correct course of action – before caving in to the establishment’s false narrative, and then subsequently devolving into just one more shameless shill organization, pushing for the mass inoculation of children with the toxic Covid mRNA injections.
Why would the AAP have done such a thing?
Money, for one thing. And plenty of it.
The AAP’s Federal Funding Windfall During Covid
As the Covid vaccine push intensified, the AAP became one of the trusted legacy medical associations that was handsomely rewarded to “push vaccines and combat ‘Misinformation’.” By 2023, the year for which data is most available, the AAP was absolutely raking it in.
As journalist Michael Nevradakis explains:
AAP… received $34,974,759 in government grants during the 2023 fiscal year, according to the organization’s most recent tax disclosure. The grants are itemized in the AAP’s single audit report for 2023-2024. Documents show some of the money was used to advance childhood vaccination in the U.S. and abroad, target medical “misinformation” and “disinformation” online, [and] develop a Regional Pediatric Pandemic Network.
In summary: in July 2020, the AAP ever-so-briefly and correctly sided with the lockdown dissenters, in service of its self-proclaimed motto to serve “the health of all children.” But by mid-August, the AAP switched sides and subsequently got a massive payout to do so. In fiscal 2023 alone, the AAP was receiving $35 million of tax money, much of it directly tied to pushing the Covid mRNA shots in children and to silence dissenters, whom it knew were telling the truth.
Unfortunately, this is unsurprising. Years before Covid, the AAP had already morphed into a highly compromised organization, straying far from its stated goal of being “dedicated to the health of all children.”
The Dinosaurs Sell Themselves to Survive
The business model for the old establishment medical professional organizations, like the AAP, is a dinosaur. The value of paid membership to these organizations has disappeared over the years, causing income from membership fees to fall. Individual paid subscriptions to their flagship journals have nosedived as well. Their financial survival increasingly relies upon Big Pharma largesse and, as we saw above for the AAP during Covid, government payouts.
In return for Big Pharma and government money, these professional organizations function less and less as champions for their professional members and their patients. They become mouthpieces for government initiatives and advertisers for Pharma. If you’ll pardon the mixed metaphor, they have become a strange species of dinosaur-prostitutes.
The AAP in particular is deeply tied to and heavily subsidized by Big Pharma, especially in the area of vaccine promotion.
Starting with the 1986 National Childhood Vaccine Injury Act (NCVIA), which effectively eliminated tort liability for vaccine manufacturers, the CDC pediatric vaccine schedule has ballooned from 7 vaccines in 1985 to 23 vaccines (and over 70 total doses!) in 2024. Since then, the AAP has largely been in the vaccine promotion business.
In accordance with the CDC vaccine schedules, the Federal government purchases huge quantities of the recommended vaccines from pharmaceutical companies. The shots are promoted to the public and to physicians through well-paid organizations like the AAP, and administered by pediatricians, many of whom receive payment – essentially kickbacks – to do so. Every step of the way, palms are greased.
As a result, American children have become what Dr. Meryl Nass calls “a delivery system to transfer taxpayer funds to big pharmaceutical companies, via your child or grandchild’s arm.”
As HHS Secretary Kennedy recently noted, the AAP posts on its own website its financial indebtedness to its corporate “donors.” Lo and behold, the four top vaccine manufacturers for the products on the pediatric vaccine schedule – Merck, Pfizer, Moderna, and Sanofi – stand at the top of the AAP’s corporate “donor” list. (The total amounts of the payouts the AAP receives are not disclosed.)
The AAP, originally created a century ago to advocate for pediatricians and their patients, has devolved into an advertiser and lobbyist for the corporate interests that fund their operations. So much for “dedicated to the health of all children.”
The AAP Goes All-In Against Reform
Fast forward to the present. The second Trump Administration and its reconstituted Department of Health and Human Services (HHS) under Secretary Robert F. Kennedy, Jr., are attempting to implement much-needed reforms to the corrupt and thoroughly captured Federal regulatory systems for healthcare.
HHS has begun to review and revise the Centers for Disease Control and Prevention’s recommended vaccine schedules, including the pediatric schedule. As mentioned above, since the passage of the NCVIA, which provided broad legal immunity to vaccine manufacturers, the pediatric schedule has exploded, from 7 recommended shots in 1986 to an incredible 23 in 2024. For over 3 decades, the AAP has agreed with the recommendations of the CDC with regard to the recommended pediatric vaccines, without argument.
Absolutely no cumulative safety testing for this bloated schedule has ever been performed, and products based on the highly controversial mRNA platform, including annual recommended shots for Covid, have recently been added to the schedule. The CDC pediatric schedule is much larger than those of most other developed countries, many of which boast significantly better pediatric (and general population) health than the United States.
Kennedy’s HHS replaced the members of the Advisory Committee on Immunization Practices (ACIP) that reviews vaccines for the schedules, due to documented conflicts of interest that many prior members were found to have.
In May 2025, Kennedy’s HHS announced changes to the Covid-19 vaccination recommendations for children. The changes are in fact modest. Regarding the Covid shots, CDC currently recommends “shared clinical decision-making” between parents and providers for healthy children ages 6 months to 17 years.
How has the American Academy of Pediatrics responded? With actions so blatantly pro-Pharma, and so spitefully anti-parent, anti-patient, and anti-child, that their August 2020 betrayal of schoolchildren seems like, well, child’s play in comparison.
On July 28, 2025, in its flagship journal Pediatrics, the AAP released a policy statement calling for a nationwide end to all religious and other nonmedical exemptions for all mandated vaccinations for children, announcing “The AAP advocates for the elimination of nonmedical exemptions from immunizations as contrary to optimal individual and public health.”
Note that the AAP calls for a blanket ban. It makes no distinction between different vaccines, different educational settings, or different reasons for seeking exemptions. According to the AAP, all mandated vaccines are equally essential to both “individual and public health.” All nonmedical exemptions are totally invalid.
The lead author of the policy statement, one Dr. Jesse Hackell, told MedpageToday that
“We recognize that excluding a child from public education does have problems, and yet, we reach the conclusion that, on balance, assuring the safety of the school and daycare environment outweighs that risk because there are other educational opportunities available.”
What an appalling shift in the AAP’s attitude toward in-school learning. What happened to their July 2020 stance, when barring kids from school “places children and adolescents at considerable risk of morbidity and, in some cases, mortality?”
The AAP’s message to parents and children is crystal clear. They don’t give a damn about your beliefs, your personal autonomy, your Constitutional rights, or even your well-being. You want to go to school? Shut up, line up, and take the shots we tell you to take. Every last one of them. On August 19, 2025, the AAP released its own pediatric vaccination schedule, which is at variance with the Kennedy HHS’s current schedule. The AAP’s website states:
“The biggest difference between the AAP and CDC schedules is around COVID-19 vaccination. The CDC no longer recommends routine vaccination for healthy children, although children can get vaccinated after a conversation with their doctor. In contrast, the AAP recommends all young children ages 6-23 months get vaccinated.”
It is telling that after decades of placid agreement with the CDC as the pediatric vaccine schedule continually expanded, the AAP has decided to take the drastic step of releasing its own childhood vaccination schedule, at variance with the CDC’s, over the issue of “shared decision-making.” Apparently, only slavish adherence to mandatory vaccination suffices for the AAP.
This is the AAP’s stance, despite rapidly declining uptake of the Covid shots in the population, the miniscule risk of Covid to children, and the mountains of evidence building that demonstrate the toxicity of these shots. In addition to myocarditis, peer-reviewed studies are demonstrating numerous autoimmune and immune system toxicities in children receiving these shots. Michael Nevradakis lists some of these:
According to a peer-reviewed study published in Pediatric Rheumatology in May, children and adolescents who received at least one Covid-19 vaccine had a 23% higher risk of developing autoimmune disease compared to unvaccinated children.
A study published in the journal Immunity, Inflammation and Disease in April found that young adults who received a Pfizer Covid-19 vaccine showed elevated spike protein production a year or more after vaccination — significantly longer than the spike protein was expected to remain in the body.Children ages 5-11 who received two doses of Pfizer’s Covid-19 vaccine had heightened levels of a type of antibody suggestive of an altered immune system response one year after vaccination, according to a peer-reviewed study published last year in the Pediatric Infectious Disease Journal.
Regarding the Covid injections and the CDC vaccine schedule in general, the AAP holds a weak hand, and yet their leadership is going all-in anyway. The AAP’s insistence on annual Covid shots for children is absurd at best, and murderous at worst. As public relations, it appears arrogant, mercenary, and utterly tone deaf. Morally and ethically, it is indefensible.
The Betrayal Is Complete
The leadership at the American Academy of Pediatrics has apparently decided that they would rather torch any residual credibility on the altar of vaccinology than acknowledge any past or present mistakes, or suffer the pain of needed reform. In so doing, with their arrogant and grossly irresponsible attitude to the safety of children, they demonstrate that primum non nocere is not in their vocabulary, and that their motto “dedicated to the health of children” is, quite frankly, a lie.
Such destructive (and self-destructive) actions reveal the AAP’s near-total dependency on the vaccine industry, and its desperation to perpetuate that gravy train at any cost. The American Academy of Pediatrics has sold its soul. Sooner or later, the devil will come to collect.
The AAP’s deep betrayal of its stated core purpose is hardly unique. The AAP is just the poster child for the corruption and corporate capture that have consumed other legacy medical professional associations (the American Medical Association and the American College of Gynecology come to mind).
The Federal Government must stop all funding to medical professional organizations like the AAP. This was always bound to corrupt them, and hard experience has demonstrated that it has. Furthermore, these organizations should be prohibited from accepting Pharma largesse, or at the very least be required to publicly disclose all income from such sources.
Perhaps some of these organizations will choose to reform. Public admission of past wrongdoing, complete divestiture of all Pharma support, and eliminating government subsidy would be the essential, bare-minimum steps to re-establishing independence and credibility.
More likely, the dinosaurs will be replaced by a species of smaller, independent, and uncompromised organizations that incorporate safeguards against the corruption that destroyed their predecessors.
Any legacy medical professional organizations that do not thoroughly and sincerely reform do not deserve the support of physicians, credibility in the eyes of the public, or trust of patients. May they go the way of the dinosaur.
C.J. Baker, M.D., 2025 Brownstone Fellow, is an internal medicine physician with a quarter century in clinical practice. He has held numerous academic medical appointments, and his work has appeared in many journals, including the Journal of the American Medical Association and the New England Journal of Medicine. From 2012 to 2018 he was Clinical Associate Professor of Medical Humanities and Bioethics at the University of Rochester.
HHS REINSTATES VACCINE TASK FORCE
The HighWire with Del Bigtree | August 21, 2025
Aaron Siri reveals how ICAN has fought HHS since 2017, relentlessly exposing and litigating the agency’s decades-long neglect of its legal duty under the 1986 Act to ensure vaccine safety. After disbanding its safety task force in 1998—following just one report—and failing to submit even a single required biannual report to Congress, HHS is finally being forced back to the table. Now, with RFK Jr. at the helm of HHS, the task force is being revived—and ICAN is ready with decades of overdue recommendations.
DR. PAUL THOMAS VS. THE CDC
CDC Hit With Lawsuit Over Failure to Test Cumulative Effect of 72-Dose Childhood Vaccine Schedule
By Michael Nevradakis, Ph.D. | The Defender | August 18, 2025
Two doctors who lost their medical licenses because they questioned the CDC’s vaccine recommendations for children are suing the agency for failing to test the cumulative effect of the 72-dose schedule on children’s health.
Drs. Paul Thomas and Kenneth P. Stoller and Stand for Health Freedom filed the lawsuit last week in federal court, alleging the lack of safety testing violates federal law and children’s constitutional rights.
The lawsuit names Susan Monarez, Ph.D., in her official capacity as director of the Centers for Disease Control and Prevention (CDC).
Attorney Rick Jaffe, who represents the plaintiffs, said the lawsuit “goes to the heart of the CDC’s childhood immunization program — a 72-plus dose medical intervention schedule that has never been tested.”
According to the complaint, the CDC’s childhood immunization schedule “is only based on an evaluation of short-term individual vaccine risks,” as the CDC “has never studied the combined effects and the accumulating dangers of administering all of the vaccines.”
The lawsuit states:
“The facts establish a continuing public health outrage hiding in plain sight: America administers more vaccines than any nation on earth while producing the sickest children in the developed world. Yet CDC demands proof of harm while refusing to conduct the studies that could provide it.”
The HighWire with Del Bigtree | August 21, 2025
Dr. Paul Thomas, author of Vax Facts, opens up about his controversial “vaxxed vs. unvaxxed” study, which showed healthier outcomes in unvaccinated children. After publishing the data, his license was suspended — but he continues to speak out, now suing the CDC over its untested vaccine schedule. He warns that pediatricians have become blind enforcers of pharma policy, while parents are waking up to the harms.
In 6 years, have any healthy Alabama students died from Covid?
I’ve gone back through my Covid archives and want to make sure everyone remembers how ridiculous the school lockdowns were
By Bill Rice, Jr. | August 12, 2025
The late Will Fowler overcame serious disabilities to become an honor’s student and band member at Cullman High School. This young man was the only named K-12 student in Alabama I can find who reportedly died “from Covid.” The lone source is a Facebook post made by his cousin who said Will tested positive for Covid before his death in the second year of Covid.

I’m working on a story that will try to debunk a non-sensical and specious claim made by the Alabama Education Association that “sixty five” Alabama educators died from Covid in the fist 18 months of the pandemic.
While researching this story, I decided to take another stab at ascertainingwhat the real Covid mortality rate for Alabama students has been over the past six years.
***
According to Google AI, approximately 814,000 students attend K-12 public and private schools in my state every year.
Since approximately 374,000 students have graduated from K-12 schools in the last six years, this means approximately 1.2 million current and former Alabama students could have contracted and died from Covid in the past six years.
Regarding the Covid Infection Fatality Rate (IFR) for Alabama students, I have found only two students who may have reportedly died from Covid in the past five-plus years.
If one assumes that 85 percent of students have now contracted the original Covid or its many variants, this would mean that approximately 1 million Alabama students have already had a “case” of Covid.
If only two students (allegedly or reportedly) died from this disease, this translates to a COVID IFR for Alabama students of approximately 1-in-500,000 (0.0002 percent).
Alabama’s only known Covid student death had serious co-morbid conditions …
I should note that I researched these two Covid deaths and was able to come up with the name of only one former student who passed away “from Covid.”
On August 17, 2021, Will Fowler, who was going to be a senior at Cullman High School, passed away and, in a Facebook post, his cousin said Will had “tested positive for Covid.”
Will seems to have been an inspiring young man as he battled severe, life-altering medical conditions his entire life. He suffered from Muscular Dystrophy and was confined to a wheel chair and also, like many children with severe disabilities, was extremely heavy.
Per logic, I also deduced that Will had not contracted Covid from classmates or from anyone at his school as he died (presumably in the hospital) only five days after school had started at Cullman High (and, one assumes, must have been ill and not at school in the days before his death).
I also found one other quote from the superintendent of Birmingham City Schools who said a student at Jackson Olin High School had “died from Covid” but I could find no name or article providing any details about this student’s death.
This is par for the course
Indeed, in five-plus years researching Covid cases and victims, I’m struck by the almost universal absence of key medical details about alleged victims of Covid.
For example, readers seeking important information might be interested in learning when a victim first developed Covid symptoms. What were these symptoms? What was the period of time from the appearance of first symptoms to death? When did the victim(s) test positive for Covid? What treatment protocols did medical staff administer (or fail to administer)?
Were family members of victims present during hospital or ICU stays or were they kept away from their loved one?
I assume, at some point, most alleged Covid victims did “test positive” for Covid, but was it really Covid that caused their deaths?
Needless to say, I’d also like to know who did and didn’t get a Covid vaccine and, also, how many victims might have gotten a flu shot before they developed “flu-like symptoms.”
A key ‘Covid death’ with virtually no important details provided
An example of this lack of details would be the circumstances of the death of Robert Thacker, Jr., the only crew member of the USS Teddy Roosevelt air craft carrier who reportedly “died from Covid” after an “outbreak” on that ship in March and April 2020.
(Note: Positive antibody tests in late April 2020, showed that at least 60 percent of the crew of 4,800 had previously had Covid. A U.S. destroyer and a French aircraft carrier also had outbreaks at the same time with similar positive rates and no fatalities. The Covid IFR on these three vessels was approximately 1-in-4,500, which is 4.5x lower than the flu IFR of 1-in-1,000.)
While I’ve performed a diligent search, all I’ve learned is that this ordnance specialist tested positive for Covid on March 30th, 2020 was placed in quarantine quarters in Guam and was later “found unresponsive” in a wellness check (a couple of days after he’d been to the local hospital, where he’d been discharged).
To this day, no member of the public knows the full and comprehensive details of this 41-year-old crew member’s medical crisis, which is common with the vast majority of “Covid victims.” For me at least, it seems like the only sailor who died after “outbreaks” on three large Naval vessels should have been the focus of copious media attention.
One great oddity of “Covid cases” is the public almost never learns such details as it’s apparently taboo to ask such common-sense questions.
Expressed differently, if evidence exists that someone, perhaps, didn’t really directly die from Covid, this evidence isnot going to be revealed by corporate journalists or pubic health officials.
Disparate lethality numbers among the young and older …
I should also note that, via an email query, I asked the Alabama Department of Public Health (ADPH) media affairs spokesperson “how many Alabama students have died from Covid?” and was told this information was not available or the ADPH didn’t know – a non-answer which strikes me as extremely odd.
Maybe I imagined it, but I seem to recall a somewhat heated debate over whether school should be cancelled and how long schools should remain closed. It seems to me that a firm answer on the number of students who had died from Covid would be very important information for the public to know.
As it is, I’m left with the apparent conclusion that maybe just two Alabama K-12 students have died “from Covid” in the entire pandemic … although I’m not sure if Covid actually caused their deaths (because no reporter ever wrote an in-depth story on particulars of these cases).
Assuming these figures are correct and the deaths of these two students can only be explained by Covid, I still can ascertain the dramatic difference in Covid deaths among students and “educators.”
Approximately 65 educators allegedly died from Covid (out of 89,000 to 100,000 educators in our state). Only two students – out of 1.2 million – reportedly died from the same disease.
If educators were contracting Covid from students, they were contracting this disease from a virus that very possibly had a 0.0000 percent mortality rate for “healthy” students.
In Alabama, the simple mortality rate for “healthy” students seems to be 1-in-1.2 million (as Will Fowler had numerous life-altering medical conditions and could not have been considered a “healthy student.” For purposes of this illustration, I’m assuming the unknown other student might have been in perfect health before his/her death).
Context for a hypothetical ‘informed consent’ conversation …
Per Google AI, I learned that the probability a random citizen will be struck by lightning in a given five-year period is approximately 1-in-200,000
This would mean that “healthy” Alabama K-12 students were approximately five times more likely to be struck by lightning as they were to expire from Covid in the last five years.
This “context example” would seem to be very relevant in any “informed consent” conversation parents might have with doctors before getting their children vaccinated.
Doctor: “Mrs. Jones, I can tell you that your child has a 1-in-200,000 chance of being struck by lightning in the coming five years and an approximately 1-in-1-million chance of dying from Covid.
“Still, on advice of the American Pediatric Association, I strongly recommend your child get today’s shot and stay current with future boosters every year.”
Of course, it’s doubtful any APA dues-paying doctor will tell parents what their child’s chances of death from all causes will be in the next five years if they get this shot.
Or, even more likely, the chance a child might develop any serious adverse event(s) over the next five years if a child goes ahead and gets his “life-saving” injection.
As noted, in Alabama, I’m pretty sure I know the odds any healthy child will die from Covid is approximately 1-in-1-million.
The odds a vaccinated male child might develop myocarditis are maybe 1-in-17,000 to 1-in-34,000 (and this is just one life-threatening adverse event.)
As I’ve noted repeatedly, we now live in a “crazy world,” so my guess is that if many parents think they can reduce the odds their child might die from Covid from 1-in-1 million to 0-in-1-million, they are going to take their pediatrician’s advice and reduce those terrifying (sarc) odds.
Most parents will also never ask their doctor, “how many vaccinated people later died from Covid?”
If a bold parent did ask this question, the doctor would probably lie and reply “zero” and tell this inquisitive mother that the shots are “100-percent effective at preventing Covid deaths.”
Part 2 …
In my next story, I’m going to show that the vast majority of the 65 Alabama educators who allegedly died from Covid died in the fall of 2021 – well after most educators had already been vaccinated and, bizarrely, in the second year of this pandemic.
Also, I’ll show that all Alabama educators were wearing (mandatory) masks every day for seven hours, meaning most educators were allegedly double protected (mask and vaccines).
Part 2 of this story will also show that most of these educators clearly didn’t get Covid from their students.
In fact, I think almost all 65 probably died from a combination of iatrogenic hospital protocols, vaccine injuries and perhaps got sick and had to go to the “killing zones” (hospitals) after they’d gotten that year’s flu shot, which might explain many ILI and Covid symptoms.
I also think most teachers were NOT afraid of this virus. IMO, what clearly transpired was an orchestrated spin campaign originating from state and national teachers’ unions, which were key actors in a global Psy-Op designed to produce mass fear.
Students certainly faced no mortality risk from being in school. In fact, the only parents terrified of a virus that posed 0.000-percent mortality risk to their children must have been products of the intentionally dumbed-down education they’d once received in the same schools.
The good news is that some parents somehow got a quality education and could identify “Covid theater” fear-mongering when they saw it.
Why is America’s paediatric academy still pushing Covid vaccines for children?
The American Academy of Pediatrics has broken ranks with the CDC, issuing its own “evidence-based” immunisation schedule—but whose interests is the AAP really serving?
By Maryanne Demasi, PhD | August 19, 2025
The American Academy of Pediatrics (AAP) has just urged that all children aged 6 – 23 months receive a Covid-19 vaccine, regardless of prior infection, and extended that recommendation to older children deemed high risk.
Their guidance directly conflicts with the US Centres for Disease Control and Prevention (CDC), which recently withdrew broad recommendations to vaccinate healthy children and pregnant women in favour of “shared clinical decision-making.”
Now, for the first time, the AAP has broken ranks — issuing its own “evidence-based immunization schedule” that places it squarely alongside its biggest corporate donors, the very companies whose products it promotes.
The boycott
The rupture began in June 2025, when Health Secretary Robert F. Kennedy Jr dismissed the CDC’s old Advisory Committee on Immunization Practices (ACIP) and replaced it with a leaner panel.
The AAP, which had held a privileged liaison seat at ACIP for decades, responded by boycotting the meeting.
AAP president Dr Susan Kressly declared, “We won’t lend our name or our expertise to a system that is being politicised at the expense of children’s health,” branding the restructured ACIP “no longer a credible process.”
But credibility cuts both ways. At the June meeting, ACIP member Cody Meissner — himself an establishment veteran — rebuked the boycott.
“I think it’s somewhat childish for them not to appear,” he said. “It is dialogue that leads to the best recommendations for the use of vaccines.”
The AAP’s absence wasn’t about protecting children from politics. It was about rejecting a forum it could no longer control.
Following the money
The AAP insists its funding has no bearing on policy. But the Academy advertises its dependence on the very companies whose products it recommends for children.
On its own website, the Academy thanks its top corporate sponsors: Moderna, Merck, Sanofi and GSK. These companies produce nearly every vaccine on the childhood schedule — and now the AAP is demanding more of their products be given to babies.

Financial filings show corporate contributions make up a substantial slice of the Academy’s revenue. Even its flagship journal, Pediatrics, carries the fingerprints of industry support.
This isn’t independence, it’s entanglement. When an organisation funded by vaccine makers issues recommendations that boost those same companies’ sales, it is impossible to pretend this is solely about children’s health.
Parents have already rejected the shots
The problem for the AAP is that parents have already walked away. CDC data show that among toddlers, the rate is a mere 4.5%.
The public’s verdict could not be clearer: most families do not want these vaccines for their children.
The AAP knows this — yet it presses ahead regardless. Its recommendations are now performative, directed less at parents than at its corporate benefactors.
Kennedy strikes back
Kennedy seized on the contradiction.
Posting a screenshot of the AAP’s donor list, he wrote: “These four companies make virtually every vaccine on the CDC’s recommended childhood vaccine schedule,” after the Academy released its own list of “corporate-friendly vaccine recommendations.”

Kennedy accused the Academy of running a “pay-to-play scheme” on behalf of “Big Pharma benefactors” and demanded full disclosure of conflicts in its leadership and journal.
He warned that recommendations diverging from the CDC’s official list are not protected under the 1986 Vaccine Injury Act. For now, Covid-19 products remain under a separate regime — the PREP Act and the Countermeasures Injury Compensation Program (CICP), which HHS has extended through to 2029.
Kennedy cast this as a red line for the future: if the AAP keeps inventing its own vaccine schedule, it risks dragging doctors and hospitals into legal jeopardy.
This is no longer about one product but about who dictates the rules of childhood vaccination — government regulators or an industry-backed lobby group.
The deeper problem
This dispute isn’t really about Covid vaccines because parents, even healthcare workers, have already rejected them in overwhelming numbers. It is about who controls the institutions that speak in the name of children’s health.
The AAP claimed it boycotted ACIP in June to resist politicisation. In reality, it walked away from a process no longer stacked with the industry-aligned figures it had long relied on. That was the real affront.
The deeper problem is that the AAP is not a neutral guardian of child health. It is a lobbying arm entangled with corporate sponsors, issuing pronouncements that align with donor interests while ignoring the families it claims to represent.
AAP says it represents 67,000 paediatricians, and by extension America’s children. But its actions tell a different story. It represents the companies that fund it.
Children’s health is jeopardised when those entrusted with protecting it are compromised. The AAP’s latest recommendations are not science-based safeguards. They are corporate advocacy in disguise.
It is not just disappointing — it is harmful.
AAP’s full vaccine schedule [LINK]
Beware Universal Mental Health Screening
By Cooper Davis, Jeffrey Lacasse | Brownstone Institute | August 21, 2025
How would your child score on a common mental health screening?
A mental health professional might view the results and conclude that your child has a mental health problem… that needs to be psychiatrically diagnosed and treated, even medicated.
Will this help your child thrive? Or will it reshape their identity in undesirable ways? Will you be comfortable with your child taking medications that alter their developing brains and could perturb their sexuality? When your child reaches adulthood, will they be able to withdraw from these drugs, or will they despair to find out that their body and brain have adapted to them, making this difficult or maybe even impossible?
For any parent with even minor reservations about our current medical and mental health system, these aren’t theoretical questions. A new public policy has just made them very salient.
Illinois Governor J.B. Pritzker has signed a new law mandating universal mental health screenings for every child in public school. This includes healthy children with no signs of behavioral problems. Parents can theoretically opt out, but they’ll have to do so repeatedly, as the screenings will be given at least once a year from grades 3-12.
Media coverage has been laudatory, expounding on the importance of “getting kids the help and support they deserve.” But do you know what a mental health screen is and how it works? Before sounding the applause, parents need to understand what these screenings are, how they’re used, and what the potential outcomes of their use might be.
The new law does not specify how children will be screened, what questionnaires will be used, or what procedures will be followed when a child’s answers are seen as troubling. But to get a sense of the ground that self-report mental health questionnaires cover, you can screen your kids right now with a commonly used questionnaire:
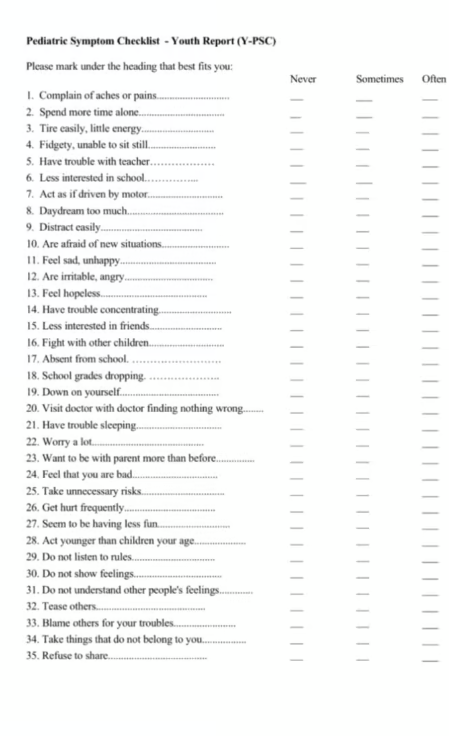
While this is a self-assessment, the questions are the same whether you’re a parent or teacher filling this out on behalf of a child. Each of the 35 questions can be answered “never,” “sometimes,” or “often.” The scoring is simple:
- 0 = “never”
- 1 = “sometimes”
- 2 = “often”
If the total score is at or above 28, professionals will consider it likely that your child has a mental health problem. The law doesn’t define what happens next. Ideally, there would be a lengthy (and costly) multi-hour clinical assessment for each such child that views these results skeptically, and heavily considers normal developmental issues and transitory problems. In the real-world mental health system, it’s hard to imagine that actually happening.
Unfortunately, the bias of the current system is towards overmedicalization, overdiagnosis, and overtreatment. The implementation of universal screening is likely to worsen these problems.
In the past, some physicians gave annual chest X-rays to smokers. This was a form of universal screening in response to concerns about lung cancer. At first blush, this sounds reasonable. The problem? False-positive results. Studies showed that annual X-rays did not prevent mortality. They did cause anxiety in patients. And incidental findings were common, causing unnecessary biopsies, procedures, and interventions.
Current screening guidelines now target high-risk individuals. This is an example where the medical establishment carefully weighed the risks and benefits of universal screening and concluded that it was not in the interests of patients, and with a well-defined disease in mind, lung cancer.
Mental health diagnosis is not like cancer. It is a fuzzy, subjective enterprise. We don’t have blood tests or brain scans; we have flawed checklists and clinical judgment. And obviously, being improperly identified as having a mental disorder comes with a real cost for the child.
Screening every single child makes it inevitable that some healthy children will be thrust into the mental health pipeline. Even assuming that the questionnaires work reasonably well, a 15% false-positive rate is likely. Combine this false-positive rate with twice-a-year universal screening from grades 3-12, and your child will have 20 separate chances to be wrongly identified as having a mental health problem…at which point the government ostensibly gets involved in the mental health of your child.
It’s easy to imagine the catastrophic results. A child’s mental health screen inaccurately identifies a mental health problem; the busy therapist confirms a diagnosis; there’s eventually a referral to a psychiatrist, who prescribes psychotropic medication. Out of 20 screenings, this only has to happen once to alter your child’s life forever.
I (C.D.) know, because it happened to me.
I was caught up in a similar diagnostic dragnet in 1991, when my teacher read about Ritalin in Time magazine and began “identifying” students she believed might have the condition, which at the time was known as “ADD” (the “H”, for hyperactivity, came later). My parents chose not to medicate me, but did send me to a psychologist and a pediatric psychiatrist. From them, I learned that my constant chair-tipping, foot-tapping, wiggling, and inability to tolerate boredom — the very traits that drove me to act out in class and leave little space between impulse and action — weren’t just part of me, but symptoms of a medical condition. It was presented as both permanently part of my nature and “acceptable,” yet somehow also extrinsic to me and framed primarily as a “deficit.” (At that time, ADD was not as widely viewed as a full disability as it is today.)
At 17, when I was legally able to decide for myself — though I now view the “informed” part as questionable — I chose to begin drug treatment. Even without the drugs, however, the diagnosis had already shaped my sense of self: diminishing my agency, reinforcing a feeling of abnormality, and feeding the belief that my more organized, conscientious, and inconspicuous peers possessed something essential that I never would. You can hear a fuller account in The Atlantic’s Scripts podcast series (“The Mandala Effect,” Episode 2, on YouTube).
My experience is just one example of how a single screening can lock a child into a lifelong diagnostic identity — and once that process starts, there are few real off-ramps. Surely no one in favor of this law wants that scenario to come true for any child.
But with 1.4 million schoolchildren in Illinois, we’re talking about dealing with the results of up to 28 million separate mental health screenings in the decade after implementation. Will the mental health professionals dealing with this deluge approach the medicalization of your child’s supposed problems carefully, gingerly, sensitively? A 2004 study found that screening 1,000 children for ADHD using the American Psychiatric Association’s DSM criteria would result in 370 false positives. And it’s common for children to be prescribed psychotropic medication at their first consultation with their physician or psychiatrist.
A comprehensive, in-depth psychological assessment for each child might help reduce false positives — but it would also mean spending 3-6 hours assessing each child, which represents a high burden in terms of both time and money. School districts in Illinois already report that a lack of time, expertise, and financial resources presents challenges to implementing universal mental health screening. The law passed anyway.
It’s hard to argue that attempts to identify and measure human misery, suffering, and emotional pain are a bad thing, etc.—especially when the goal is “getting people the help they need.” It sounds right. But the kids who will be screened every year in Illinois? They have many kinds of problems: social, relational, environmental, academic, psychological, and physical problems. Children today have issues navigating a modern life dominated by endless screens, scrolling, and even more endless data.
And also, they have some problems that you’re supposed to have—problems that have been a critical part of growing up since the dawn of time.
Our culture is currently debating the medicalization of human problems, the credibility of medicine, the influence of the pharmaceutical industry, and the ethics of imposing medical authority as state policy. Covid lockdowns were a prime example of this, and, similar to universal mental health screening, they were imposed without consideration of the unintended consequences.
Mandatory Covid vaccinations also led many Americans to rethink the role of government in their bodily autonomy, and to consider how arbitrary social policy could be when it claimed to be for the greater good (e.g., insisting that those with immunity to Covid must still get vaccinated). For those who have grown skeptical of medical authority, universal mental health screening will likely be viewed as another overextension of the government into the lives (and minds) of their children. Children aged 12-17 can already receive psychotherapy in Illinois without parental consent; universal screening offers a new on-ramp to this process.
The new Illinois law seems almost tone deaf, out of step with the lessons learned from Covid. This critique is cultural, social, and ethical in nature. But universal mental health screening is supposedly based on science. The new Illinois law does not give details; it just authorizes universal screening as if it is an unmitigated good. The devil (and the science, or lack thereof) will be in these details – how the policy is implemented. Assuming that the rationale for universal screening is scientific, we present critically important questions that should be addressed as procedures are developed:
- What is the evidence that universal mental health screening improves real-world outcomes for children? Is there evidence that it could cause harm? The scientific rationale for the program needs to be stated clearly, citing compelling data, and explicitly addressing the measures taken to avoid harm.
- Given that Illinois has already implemented universal mental health screening in some school districts, what were the outcomes for the children? After testing positive for a mental health condition, how many were further assessed, and how much time was spent on each child? How many ended up in psychotherapy or on medication? Usually, a pilot program tests the effectiveness of an intervention, and it is only adopted on a wide scale if it is shown to be effective and not harmful – where is that data?
- How many children a year does Illinois expect to inaccurately identify as having a mental health problem (e.g., how many false positives)? How many children will make it from 3rd to 12th grade without ever screening positive? What measures will address the known issue of false-positive results in universal screening? Do Illinois public schools have the time, money, and expertise to carefully assess each child who screens positive for multiple hours to ensure that they do not overdiagnose and overtreat Illinois children? If universal screening results in a surge of children who ultimately end up on psychiatric medication, how will the public know? Implementing this program without addressing these issues ignores the potential harm of universal screening.
- How will Illinois taxpayers know if this program is a success? What metrics will be tracked? The easy out is to focus on the implementation of the program, and if a high proportion of children are screened, call it a success, never mind the details or outcomes. But using the screening of children as a measure of success for a universal screening program is tautology; data must be collected that demonstrates that the program helps children measurably and does not harm them.
There are good reasons to object to the new Illinois program based on general principles. If the issues above go unaddressed, or if sufficient resources are not provided to allow careful and precise identification of children in distress, it has the potential to be a disaster.
Cooper Davis is an advocate, speaker, and writer. He is the Executive Director of Inner Compass Initiative (ICI), a 501(c)(3) nonprofit organization that advocates for mental health system reform and helps people make informed choices about psychiatric diagnoses, drugs, and drug withdrawal.
Featured Video

or go to
Aletho News Archives – Video-Images
From the Archives
Israel Would Have No Qualms About USS Liberty-Style FALSE FLAG If Iran Campaign Falters – Analysts
By Ilya Tsukanov – Sputnik – 18.06.2025
Donald Trump is mulling whether or not to join Israel’s aggression against Iran as Tel Aviv faces problems sustaining its defenses against growing counterstrikes, and apparently lacks a realistic game plan for an end to hostilities after failing to achieve its goals. Analysts told Sputnik how the US could be ‘nudged’ into the conflict.
“The US is already assisting Israel with supplies, intel, refueling support, etc. One of the many US posts in the region could be attacked for a casus belli,” former Pentagon analyst Karen Kwiatkowski explained.
“If Trump doesn’t comply with Israel’s demand” and join its aggression voluntarily, “a false flag may be needed” to drag the US in, Kwiatkowski, retired US Air Force Lt. Col.-turned Iraq War whistleblower, fears.
Netanyahu has a diverse array of options at his disposal, according to the observer, including:
- a false flag against US assets abroad blamed on Iran or one of its Axis of Resistance allies, like the Houthis
- a US domestic attack or assassination blamed on Iran
- Iranian air defenses ‘accidentally’ hitting a civilian jetliner carrying Americans
- use of a dirty bomb or nuclear contamination somewhere in the region blamed on Iran
- even blackmailing by threatening to use nukes against Iran if the US doesn’t join the fight
Kwiatkowski estimates that Israel probably has “enough blackmail power” against President Trump and Congress to avoid the necessity of a false flag operation, but a “USS Liberty-style” attack, targeting the soon-to-be-retired USS Nimitz supercarrier that’s heading to the Middle East, for example, nevertheless cannot be ruled out entirely, she says. … continue
Blog Roll
 Aletho News
Aletho News- Outlasting the Superpower: The Reasons Why Iran is Beating uhe US and Israel
- Top PMU commander, over a dozen fighters killed in new US strikes on Iraq
- Is Netanyahu’s war gamble threatening the future of ‘Israel’?: FT
- Smotrich calls for annexation of South Lebanon to Litani River
- Echos of Gallipoli? Hormuz and the Geography of Hubris
- Pakistan PM backs Iran’s right to self-defense amid tensions
- Hungary blasts ‘fake’ EU accusation
- SAFE Debt Trap: Poland’s €43.7 Billion Bet on Unipolar Illusion
- War on Iran threatens global Gulf capital flows: FT analysis
- Mossad De Facto Admits To Inciting Riots In Iran
- If Americans Knew
- Instead of taking Joe Kent’s claims seriously, the media is disregarding him as an antisemite
- Joe Kent’s Explosive Interviews about his Resignation over the Iran War
- Israel poised to take over southern Lebanon; settlers wreak havoc in West Bank – Not a ceasefire Day 165
- From Sde Teiman, the truth about Israel’s military justice system has been set free
- Child denied life-saving bone marrow transplant by Israel ‘because he is from Gaza’
- Raffi Berg: BBC Middle East Editor Exposed as CIA, Mossad Collaborator
- Jerusalem Archbishop Rebukes Netanyahu’s Statements on Christianity
- US to embed Palantir AI across entire military: Report
- Israeli-US war on Iran to drag on “a few more weeks” – Not a ceasefire Day 164
- Lebanon deaths top 1,200; Palantir AI to be embedded across US military – Not a ceasefire Day 163
- No Tricks Zone
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis
- New Study Documents A 20-Year Pause In Arctic Sea Ice Decline – Driven By Internal Variability
- Wake-up Call: Survey Shows Majority Of Germans Now Favor Postponing Climate Targets!
