New Study Rebuts The Assumption That Anthropogenic CO2 Molecules Have ‘Special’ Properties
By Kenneth Richard | No Tricks Zone | February 6, 2026
The Intergovernmental Panel on Climate Change (IPCC) has for decades advocated net-zero governmental policies to reduce anthropogenic CO2 (aCO2) emissions.
This advocacy is rooted in the non-physical assumption that aCO2 molecules are special, as they remain in the atmosphere for decades to centuries.
Proponents of the anthropogenic global warming (AGW) narrative even claim aCO2 removal can “take up to several hundreds of thousands of years.”
While AGW proponents insist that “once in the atmosphere, carbon dioxide can continue to affect climate for thousands of years,” they (and the IPCC) simultaneously acknowledge the residence time of “natural” or non-anthropogenic CO2 is only about 4 years.
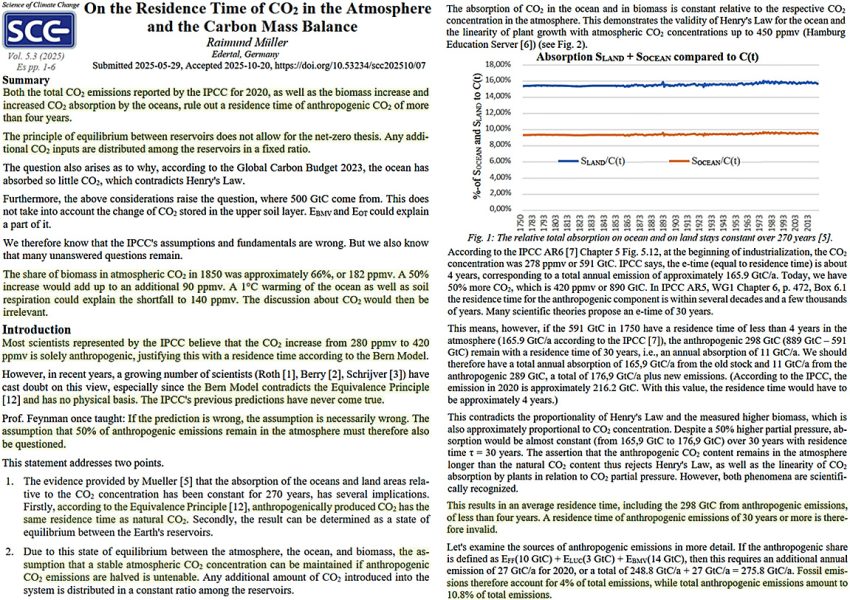
In reality, a new study references the Equivalence Principle in emphasizing nature’s sinks indiscriminately and equivalently absorb both aCO2 and natural CO2 in about 4 years (Müller, 2025). There is no physical reality for IPCC claims of “specialized” absorption time for aCO2 vs. natural CO2 molecules.
The IPCC assumes exactly 50% of aCO2 emissions remain in the atmosphere for decades to millennia. It is consequently assumed net-zero policies that propose to halve aCO2 emissions will lead to the stabilization of atmospheric CO2 concentrations. Because “anthropogenic CO2 has the same [4-year] residence time of natural CO2,” this assumption is physically invalid.
Net-zero policies will literally have no detectable effect on atmospheric CO2 concentrations. In sum, “the IPCC’s assumptions and fundamentals are wrong.”
When Threats Replace Evidence
What an Australian Newspaper Article Reveals About the Vaccine Compliance Machine
Lies are Unbekoming | February 5, 2026
The Sydney Morning Herald wants you to know the penalties. Doctors and nurses who falsify vaccination records face suspension, deregistration, and jail. Parents who seek them out face fraud investigations through Services Australia. The article names specific dollar amounts ($2,500 per child), quotes the Health Minister expressing shock and outrage, and reminds readers that AHPRA—the regulatory body that controls whether medical professionals can earn a living—is watching.
The article reads less as journalism than as a warning to anyone considering dissent.
The Herald is one of Australia’s oldest and most influential newspapers, the rough equivalent of the New York Times in reach and establishment credibility. When it publishes a piece like this, it speaks with institutional authority. The January 2026 article, “Parents are paying $2500 to falsify vaccine records,” arrives at a particular moment in Australian public health: vaccine uptake has “stalled below national targets,” mandate enforcement is creating a black market for exemptions, and parents are organising in Facebook groups 40,000 members strong.
To understand the context, American readers need to know what Australia built. Between 2014 and 2019, five Australian states—New South Wales, Victoria, Queensland, South Australia, and Western Australia—rolled out “no jab, no play” laws, which bar unvaccinated children from childcare and preschool enrollment entirely. The only exemptions are medical, and these require documented life-threatening allergic reactions or severe immunocompromise—conditions so narrow that most families cannot qualify no matter their concerns.
The coercion is not subtle—and it violates the government’s own rules. Australia’s Immunisation Handbook states that valid consent must be given “voluntarily in the absence of undue pressure, coercion or manipulation.” Denying a child access to childcare unless the parents comply is textbook duress. The government has built an enforcement apparatus that fails its own stated ethical standards.
The system was designed to make non-compliance economically devastating and socially impossible. And for years, it worked. But now that system is encountering mass resistance, and the Herald article’s purpose is to make examples—to signal what happens to doctors who help parents escape a coercive system, and to parents who refuse to comply.
Buried beneath the threats is a dead baby. Riley Hughes, 32 days old, is the emotional payload. His story opens the piece, provides the moral frame, and transforms regulatory enforcement into righteous protection of the innocent. Without Riley, this article is just an inventory of punishments. With Riley, non-compliance becomes child murder.
The story requires examination.
Riley developed “mild cold symptoms” at three weeks old. His mother took him to a doctor, who said he appeared “perfectly fine.” When he stopped feeding, she took him to the children’s hospital. By day three, doctors “suspected” whooping cough. By day four, he had pneumonia. By day five, he was on life support. He died at 32 days old. Riley died in February 2015—eleven years before this article was published. The Herald reached back over a decade to find its dead baby.
The article states that “The Bordetella pertussis bug had overwhelmed his tiny body.” This is presented as fact. But reading carefully, the diagnosis was never confirmed—doctors “suspected” whooping cough. The journalist’s assertion that pertussis killed Riley is not attributed to any medical source. It is simply declared.
More striking is what the article omits entirely: what happened during those five days of hospitalisation. What interventions were administered to a three-week-old infant? What antibiotics? What was the “life support” that preceded his death? The hospital’s role in Riley’s deterioration is invisible. The medical system appears only as the place where heroic efforts were made to save him from the disease that (we are told) the unvaccinated community gave him.
The article describes Riley as “too young” to be vaccinated against whooping cough, which is given at six to eight weeks in Australia. But it does not mention that under Australian guidelines, Riley would have received the Hepatitis B vaccine within 24 hours of birth. He was not an unvaccinated child. He was a vaccinated child who had not yet received this particular vaccine.
If Riley had been completely unvaccinated, that would be the story. “Unvaccinated baby dies of preventable disease” writes itself. Instead, the article performs a subtle shift: a vaccinated infant dies after five days of hospital intervention, and an entire class of people—parents who refused to vaccinate—are scapegoated to protect the system that failed him.
None of this can be stated with certainty. We do not have Riley’s medical records. We do not know what drugs were administered, what procedures were performed, what his body endured in those five days. But that is precisely the point: neither does the Herald, and neither do its readers. The article presents a story with a hole at its centre and fills that hole with a villain—the unvaccinated community—while the institution that actually had custody of Riley during his decline remains unexamined.
What we do know: Riley was vaccinated. He received the Hepatitis B vaccine at birth, as per Australian protocol. He then spent five days in hospital care before he died. This is a vaccinated child who died after days of medical intervention—and the article repurposes his death as a case against vaccine refusal.
The mother, Catherine Hughes, is quoted: “My son would likely be alive today if everyone in my community had been fully vaccinated against whooping cough.”
This is a grieving mother’s belief, given to her by a medical system that needed someone to blame. She has since founded the Immunisation Foundation of Australia and become a professional advocate for vaccination mandates. What the Herald does not disclose: as journalist Alison Bevege has documented, her foundation received $170,000 from Sanofi in 2023 and $100,000 from GSK in 2025. Hughes herself appears in GSK press releases promoting their products. The article presents her as a spontaneous voice of bereaved motherhood. She is a paid pharmaceutical spokesperson.
The article’s foundational premise—that unvaccinated children endanger the community—is not merely unexamined. Even within the mainstream framework of germ theory and disease transmission, the published science contradicts it.
In 2014, researchers at the FDA published a study using baboons to examine how the acellular pertussis vaccine actually works. The results, within the germ theory framework the researchers operated in, were unambiguous: vaccinated baboons exposed to Bordetella pertussis showed few symptoms but became colonised with the bacteria. They were then placed in cages with unvaccinated baboons—and by the researchers’ own account, the vaccinated animals passed the bacteria to the unvaccinated ones. The study’s conclusion: “acellular pertussis vaccines protect against disease but fail to prevent infection and transmission.”
A 2015 study by Althouse and Scarpino went further. Using epidemiological, genetic, and mathematical modelling data, they argued that asymptomatic spread from vaccinated individuals “provides the most parsimonious explanation for the observed resurgence of B. pertussis in the US and UK.” Vaccinated individuals who show no symptoms carry and spread the bacteria—according to the very framework the public health establishment operates within. The authors noted that this also explains the documented failure of “cocooning”—the strategy of vaccinating family members to protect newborns. By their own logic, it doesn’t work because the vaccinated family members become silent carriers.
Even by the establishment’s own standards, the pertussis vaccine does not prevent colonisation. It does not prevent spread. What it does, according to their own researchers, is suppress symptoms in the vaccinated individual while allowing them to pass the bacterium to others, including infants too young to be vaccinated.
These are peer-reviewed studies published in the Proceedings of the National Academy of Sciences and BMC Medicine. The FDA conducted the baboon study.
Meanwhile, within this same framework, the bacterium has apparently evolved under vaccine pressure. A 2014 Australian study found that between 30% and 80% of circulating pertussis strains during a major outbreak were “pertactin-deficient”—lacking the protein the vaccine targets. The authors observed that “pertussis vaccine selection pressure, or vaccine-driven adaptation, induced the evolution of B. pertussis.”
The pertussis vaccine suppresses symptoms. Whether it also creates asymptomatic carriers who spread an apparently evolving pathogen, as the establishment’s own researchers claim, remains their narrative to defend. But even within that narrative, the unvaccinated are not the problem—the vaccine is.
When the Herald article quotes a professor warning about “one of the kids there has whooping cough or measles, and it spreads through the childcare, putting your child at risk,” the establishment’s own science suggests the spreader is more likely to be a vaccinated child with no visible symptoms than an unvaccinated child who would be home sick.
Even within the establishment’s own framework, if Riley had pertussis, the most likely source—according to their own research on asymptomatic carriage—would be a vaccinated person, perhaps someone in his own family who had been “cocooned” as the health authorities recommend. The article does not explore this possibility. It cannot, because the entire enforcement apparatus rests on the premise that the unvaccinated are the danger.
The article is not confused about the science. It is not interested in the science. Its function is compliance enforcement, and its vectors are specific.
The first vector targets medical professionals. The article names a Perth nurse charged with fraudulently recording vaccines—though the case was dropped for lack of evidence. It names a Victorian doctor whose registration was suspended. It quotes AHPRA warning that practitioners found acting fraudulently face suspension or deregistration. The message to any doctor or nurse who might help parents escape the system: we are watching, and we will destroy your career.
This is not new. In December 2020, Dr. Paul Thomas, a Portland paediatrician who had practiced for 35 years, published a peer-reviewed study comparing health outcomes in vaccinated versus unvaccinated children in his practice. The data showed unvaccinated children were significantly healthier across multiple metrics. Within days of publication, the Oregon Medical Board issued an “emergency order” suspending his licence, claiming his “continued practice constitutes an immediate danger to the public.”
The Board’s letter accused Thomas of “fraudulently” asserting that his vaccine-friendly protocol improved health outcomes—the very thing his peer-reviewed data demonstrated. His paper was later retracted under circumstances its authors describe as dubious. Thomas eventually surrendered his licence rather than continue fighting the Board’s conditions, which prohibited him from consulting with parents about vaccines or conducting further research.
The pattern is consistent. Produce evidence that challenges the orthodoxy, lose your ability to practice medicine. The threat in the Herald article is not abstract. Medical professionals in Australia have seen what happens to dissenters.
The second vector targets parents. The article reminds readers that Services Australia investigates Medicare and Centrelink fraud. Parents who pay for falsified records are not just endangering children (according to the article’s framing)—they are committing crimes against the Commonwealth. The article implies that seeking workarounds exposes parents to criminal liability, transforming a decision about their child’s medical care into a prosecutable offence.
The third vector is reputational. The article quotes the Health Minister: “I am shocked and appalled that any doctor or nurse would falsify vaccination records.” Parents in the Facebook groups are framed as reckless conspirators, their concerns about vaccine safety transmuted into selfish endangerment of babies like Riley. The 2025 study cited in the article notes that 47.9% of parents with unvaccinated children “did not believe vaccines are safe” and 46.7% “would not feel guilty if their unvaccinated child got a vaccine-preventable disease.” These statistics are presented as moral indictments.
What the article does not mention: the same study found that nearly 40% of these parents “did not believe vaccinating children helps protect others in the community.” Given the published science on pertussis—even within the establishment’s own framework—these parents have a point.
In 2004, Glen Nowak, the CDC’s director of media relations, gave a presentation to the National Influenza Vaccine Summit titled “Increasing Awareness and Uptake of Influenza Immunization.” His slides explained that vaccine demand requires “concern, anxiety, and worry” among the public. “The belief that you can inform and warn people, and get them to take appropriate actions or precautions with respect to a health threat or risk without actually making them anxious or concerned,” Nowak explained, “is not possible.”
His recipe for demand creation included medical experts stating “concern and alarm” and predicting “dire outcomes” if people don’t vaccinate. References to “very severe” and “deadly” diseases help motivate behaviour. Pandemic framing is useful.
The Herald article follows this template precisely. It opens with a dead baby. It features a professor warning about diseases “spreading through childcare.” The Health Minister invokes “serious complications, hospitalisation, and in some cases, death.” The 14 measles cases since December are presented ominously, without context about how many of those cases involved vaccinated individuals or resulted in any serious illness.
The article also quotes Dr. Niroshini Kennedy, president of the paediatrics and child health division at the Royal Australasian College of Physicians, warning about “vaccine hesitancy.” What the article does not mention: the RACP has a foundation that partners with GSK, a major pertussis vaccine manufacturer. The expert voice warning about hesitancy has institutional financial ties to a company that profits from vaccination.
The financial stakes are not abstract. GSK’s pertussis products Boostrix and Infanrix generated $2.3 billion in 2023. Sanofi’s pertussis vaccine revenue hit $1 billion in 2024, up 10.8% on the previous year, driven by booster demand. When the Herald runs a story demonising vaccine refusers, it serves an industry measured in billions.
The article acknowledges, briefly, that public health experts warned in 2019 that “vaccine mandates can backfire, and simply induce parents to seek loopholes, and, worse, fuel negative attitudes towards vaccination.” This warning has proven accurate. Australia’s escalating mandate regime has not produced the desired compliance. It has produced a $2,500 black market and Facebook groups with 40,000 members sharing strategies for resistance.
The system’s response is not to reconsider the mandates. It is to escalate enforcement and amplify fear. The article is part of that escalation.
The escalation itself is diagnostic. Systems that can defend their policies on evidence do not need to inventory punishments in the newspaper. They do not need to reach back eleven years for a dead baby. They do not need AHPRA warnings and Health Minister quotes and reminders about criminal prosecution. They make their case and let the data persuade.
What the Herald article reveals, beneath its institutional authority, is a system that has run out of persuasive tools. The sequence tells the story: first came the information campaigns, which did not produce sufficient uptake. Then came the mandates—no jab, no play—which produced compliance but also resistance. Then came enforcement against the resisters, which produced a black market. Now comes the threat display in the national press, designed to frighten the black market into submission. Each escalation is a concession that the previous level of coercion failed. Each one is more desperate than the last.
A system confident in its science would welcome questions. A system confident in its products would publish the safety data that parents are asking for. A system confident in its outcomes would point to the evidence and let parents decide. This system prosecutes nurses, deregisters doctors, denies children access to childcare, and runs articles designed to make examples of anyone who dissents. That is not the behaviour of an institution operating from strength. It is the behaviour of an institution that knows it cannot survive scrutiny—and is scrambling to ensure that scrutiny never arrives.
What parents are waking up to, slowly and in growing numbers, is that the fundamental promise—vaccinate your children and they will be protected, vaccinate enough children and the community will be protected—is not supported by the evidence, even within the framework that public health authorities operate in. What they are discovering is that asking questions produces hostility rather than answers. What they are learning is that doctors who support informed consent are being systematically removed from practice, leaving parents with no one in the medical system willing to have honest conversations.
The 40,000 parents in that Facebook group are not there because they read misinformation. They are there because they asked questions their doctors couldn’t answer, or because their child had a reaction that was dismissed, or because they did the research the system told them not to do and found that the confident assurances didn’t match the published science.
The Herald article treats these parents as a problem to be solved through enforcement. It does not entertain the possibility that they might be responding rationally to real information. It cannot, because that would require examining the science—and the science does not support the policy.
Australia has constructed a system where parents lose childcare access if they do not vaccinate, where doctors lose their licences if they support parental choice, where asking questions about vaccine safety is framed as “misinformation,” and where a dead baby is deployed to transform regulatory non-compliance into moral monstrosity.
The article calls this public health. A more accurate description: this is what happens when a policy built on faulty premises meets a population that is beginning to see through it. Unable to defend the science, the system defends itself through threats, fear, and the weaponisation of grief.
Riley Hughes deserved better than to become a propaganda tool for the companies that fund his mother’s foundation. The parents seeking exemptions deserve honest information about what vaccines can and cannot do. The doctors trying to practice informed consent deserve to keep their licences.
None of them are served by an article whose purpose is to frighten dissenters into silence.
The system is telling parents: comply or be punished, and don’t ask questions. The parents are responding: we have questions, and your threats are not answers.
That tension will not be resolved by more enforcement. It will be resolved when someone in authority has the courage to address the questions honestly—or it will continue to escalate until the system’s credibility collapses entirely.
Forty thousand parents in one Facebook group suggest which direction this is heading.
References
The Article Under Discussion:
Olaya, K. (2026, January 31). Parents are paying $2500 to falsify vaccine records. It’s endangering babies like Riley. The Sydney Morning Herald. https://www.smh.com.au/national/parents-are-paying-2500-to-falsify-vaccine-records-it-s-endangering-babies-like-riley-20260127-p5nxah.html
Catherine Hughes Financial Disclosures:
Bevege, A. (2026, February 4). ‘Baby-Killers’ – Nine Newspapers falsely claim unvaccinated people killed a baby by spreading whooping cough. Letters from Australia. https://alisonbevege.substack.com/
RACP-GSK Partnership:
GSK Australia. RACP Foundation partnership announcement. Referenced in Bevege (2026).
Vaccine Revenue Figures:
GSK. (2024). Annual Report 2023. Boostrix and Infanrix/Pediarix revenue figures.
Sanofi. (2025). Fourth Quarter 2024 Earnings Report. Polio/pertussis/HiB vaccine sales.
Pertussis Vaccine and Asymptomatic Carriage:
Warfel, J. M., Zimmerman, L. I., & Merkel, T. J. (2014). Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model. Proceedings of the National Academy of Sciences, 111(2), 787-92. https://doi.org/10.1073/pnas.1314688110
Althouse, B. M., & Scarpino, S. V. (2015). Asymptomatic transmission and the resurgence of Bordetella pertussis. BMC Medicine, 13(1), 146. https://doi.org/10.1186/s12916-015-0382-8
Pertussis Vaccine Evolution and Waning Immunity:
Lam, C., Octavia, S., et al. (2014). Rapid increase in pertactin-deficient Bordetella pertussis isolates, Australia. Emerging Infectious Diseases, 20(4), 626-33. https://doi.org/10.3201/eid2004.131478
Tartof, S. Y., Lewis, M., et al. (2013). Waning immunity to pertussis following 5 doses of DTaP. Pediatrics, 131(4), e1047-52. https://doi.org/10.1542/peds.2012-1928
van Boven, M., Mooi, F. R., et al. (2005). Pathogen adaptation under imperfect vaccination: implications for pertussis. Proceedings of the Royal Society B, 272(1572), 1617-24. https://doi.org/10.1098/rspb.2005.3108
Dr. Paul Thomas Case:
Oregon Medical Board. (2020). In the Matter of: Paul Norman Thomas, MD. License Number MD15689: Order of Emergency Suspension. https://omb.oregon.gov/Clients/ORMB/OrderDocuments/e579dd35-7e1b-471f-a69a-3a800317ed4c.pdf
Lyons-Weiler, J., & Thomas, P. (2020). Relative Incidence of Office Visits and Cumulative Rates of Billed Diagnoses Along the Axis of Vaccination. International Journal of Environmental Research and Public Health, 17(22), 8674. [Retracted 2021]
Hammond, J. R. (2021). The War on Informed Consent: The Persecution of Dr. Paul Thomas by the Oregon Medical Board. Skyhorse Publishing.
CDC Fear-Based Messaging:
Nowak, G. (2004). Increasing Awareness and Uptake of Influenza Immunization. Presentation at the National Influenza Vaccine Summit, Atlanta, GA.
Vaccine Mandates and Backfire Effects:
Ward, J. K., et al. (2019). France’s citizen consultation on vaccination and the challenges of participatory democracy in health. Social Science & Medicine, 220, 73-80.
Suppression of Vaccine Dissent:
Martin, B. (2015). On the Suppression of Vaccination Dissent. Science and Engineering Ethics, 21(1), 143-57. https://doi.org/10.1007/s11948-014-9530-3
Australia’s No Jab, No Play Laws:
Australian state governments. No Jab, No Play legislation (2014-2019). New South Wales, Victoria, Queensland, South Australia, Western Australia.
Australian Immunisation Handbook — Consent Requirements:
Australian Government Department of Health. Australian Immunisation Handbook. Section: Valid Consent. https://immunisationhandbook.health.gov.au/
Is Canada Really Warming?
By Tom Harris | American Thinker | January 30, 2026
Is Canada really warming at double the global average rate, as the Canadian government says it is? A new report says no, because the data Environment and Climate Change Canada (ECCC) uses are apparently corrupted by fundamental mistakes, mistakes so severe that when corrected, all the supposed warming of the past six or seven decades vanishes.
Given that Canada represents a large fraction of global land surface area, one naturally wonders if the world is warming at anything like we are told it is.
This discovery should have generated mainstream media headlines across Canada. After all, the mistakes in the Canadian temperature data were discovered over four years ago by Dr. Joseph Hickey, a highly qualified Canadian data scientist, and the group I lead, the International Climate Science Coalition – Canada, has been publicizing the story for the past month.
But don’t expect mainstream media in the Great White North to say anything about this. Most of Canada’s press are heavily subsidized by the federal and provincial governments, which would probably not appreciate the story being covered. Dr. Dave Snow, Associate professor in political science at the University of Guelph, writes:
“Canada has created a bevy of policies, ranging from subsidies to tax breaks to mandated contributions from foreign tech companies, that undoubtedly constitute a major portion of news outlets’ revenue and journalists’ salaries — potentially upwards of 50 percent.”
Publicly questioning government narratives on something as significant as climate change is a risky proposition for any editor when doing so leaves their paymasters with egg on their faces.
Here’s what governments in Canada — and the media outlets reliant on their largess — would rather you never heard. On December 23, the report “Artificial stepwise increases in homogenized surface air temperature data invalidate published climate warming claims for Canada” was released by Dr. Joseph Hickey, a data scientist with a PhD in Physics. The report was published by CORRELATION Research in the Public Interest regarding a significant error in Canada’s temperature data.
Using the data from ECCC for hundreds of stations across the country, scientists had previously calculated that the surface air temperature has increased 1-2 degrees Celsius over the past six to seven decades in Canada. Yet in 1998, the exact year in which 72 Canadian reference climatological stations were first added to the Global Climate Observing System, a sudden stepwise increase of approximately 1 degree Celsius occurred at most stations across the country.
Numerous studies in scientific literature assert that sudden temperature jumps like this are not due to real climactic change but instead are caused by temperature measurement artifacts corrupting the data. They contend that this data should therefore be removed from the record. Even though one of the studies explaining this was authored by Dr. Lucie A. Vincent, the senior Environment Canada Research Climatologist, the temperature jump was left in ECCC’s data and is still there to this day. Hickey concludes, “The reported climate warming of Canada appears to be entirely from a temperature measurement artifact.”
Hickey first discovered this in 2021 when he was as an analyst for the Bank of Canada and so was barred from sharing his findings with the public. After leaving the bank, he secured his communications with Environment Canada via an access to information, which is why we know what happened next.
In that year Hickey alerted Environment Canada to the problem and explained in detail to Vincent that the sharpness of the temperature increase, and its magnitude, indicate that it is not due to real climactic change. He also laid out a thorough analysis of potential sources of the artifact, which could include land use changes and instrumentation changes. Both of these could easily cause a one-degree shift in the temperature data. Moreover, he explained, “there are no other similar large and geographically widespread discontinuities in the AHCCD dataset [Environment Canada’s flagship temperature dataset] at other years.” This increase could be responsible for almost all the claimed warming calculated for Canada over the past six or seven decades.
Vincent essentially brushed him off, did not provide an explanation for the step increase, and said that the shift “is probably due to climate variability only.”
So, Canada is spending hundreds of billions of dollars to fight climate change largely based on data that the government scientist most involved in its generation can only say is “probably” indicative of warming.
Hickey was not the only Bank of Canada employee to find fault with ECCC’s temperature data. In his December report, he writes:
“On December 7, 2020, Bank of Canada Economist Julien McDonald-Guimond sent an email to Environment Canada researchers with an inquiry about the … daily temperature records, noting he had found some cases in which the daily minimum temperature was greater than the daily maximum temperature for the same day and for the same AHCCD station.”
In fact, there were more than 10,000 instances of days for which the daily minimum temperature was greater than the daily maximum temperature.
Environment Canada Climate Data Analyst Megan Hartwell replied to McDonald-Guimon, saying that “We were quite surprised by the frequency of the issue you reported, and have taken some time to go through the data carefully.”
That ECCC were surprised by McDonald-Guimond’s finding is cause enough to worry. But the fact that they now “have taken some time to go through the data carefully” begs the question: didn’t they go through the data carefully before releasing it the first time?
Environment and Climate Change Canada have yet to respond to Hickey’s December report. They have some explaining to do.
Tom Harris is Executive Director of International Climate Science Coalition – Canada.
Climate Scientist Who Predicted End Of “Heavy Frost And Snow” Now Refuses Media Inquiries
By P Gosselin | No Tricks Zone | February 3, 2026
More than two decades ago, renowned climate scientist Mojib Latif of Germany’s Max Planck Instiute for Meterology, based in Hamburg, warned the climate-ambulance chasing Der Spiegel that, due to global warming, Germany would likely no longer experience harsh winters with heavy frost and snow as it had in previous decades.
In light of the current severe winter weather in Germany, Latif’s statements are facing renewed scrutiny. An article appearing in the Berliner Zeitung notes that Latif’s prophecy has “aged poorly” and he appears to want to have nothing to do with them.
Hiding from the media
According to the Berliner Zeitung, the former Max Planck Institute scientist has recently stopped responding to media inquiries regarding his past claims. Critics argue that such drastic predictions damage the credibility of climate science, while others point out that extreme weather events—including intense cold snaps—can still occur within the broader context of climate change.
No Easter snow as well
Latif also claimed he recalled snow in the past occurring at Easter time, implying this no longer happens today. But that too was a false claim. perhaps prof. Latif will answer phone calls in April?
‘Fact-checking’ as a disinformation scheme: The Brazilian case of Agência Lupa
By Raphael Machado | Strategic Culture Foundation | February 7, 2026
Since the term “fake news” emerged in the world of political journalism, we have been confronted with a new angle through which the establishment attempts to reinforce its hegemony in the intellectual and informational sphere: by simulating ideology as science, data, or fact.
A fundamental aspect of hegemonic liberalism in the “rival-less” post-Cold War world is the transition of ideology into the diffuse realm of pure facticity. What decades earlier was clearly identified as belief comes to be taken as “data,” that is, as indisputable, not open for debate. This is the case, for example, with the myth of “democracy,” the myth of “human rights,” the myth of “progress,” and the myth of the “free market.” And today, we could extend this to the dictates of “gender ideology” and a series of other beliefs of ideological foundation, which are nevertheless taken as scientific facts.
“Fact-checking” has thus become one of the many mechanisms used by the establishment to reinforce systemic “consensus” in the face of the emergence of alternative perspectives following the popularization of the internet and independent journalism. The “authoritative” distinction made by a self-declared “independent” and “respectable” agency between what would be “fact” and what would be “fake news” has become a new source of truth.
Some liberal-democratic governments, like the USA, have gone so far as to create special departments dedicated to “combating fake news,” thus acting as authentic “Ministries of Truth” of Orwellian memory.
However, even within the “independent” sphere, we rarely encounter genuine independence. On the contrary, in fact, Western “fact-checking agencies” tend to be well-integrated into the constellation of NGOs, foundations, and associations of the non-profit industrial complex, which, in turn, is permeated by the money of large corporations and the interests of liberal-democratic governments. Even their staff tend to be revolving doors for figures coming from the NGO world, mainstream journalism, and state bureaucracy.
Although the phenomenon is of Western origin, Brazil is not exempt from it. “Fact-checking agencies” also operate here — most of them engaged in the same types of disinformation operations as the governments, newspapers, and NGOs that sponsor them.
A typical example is Agência Lupa.
Founded in 2015, its founder Cristina Tardáguila previously worked for another disinformation apparatus disguised as “fact-checking,” Preto no Branco, funded by Grupo Globo (founded and owned by the Marinho family, members of which are mentioned in the Epstein Files). Lupa was financially boosted by João Moreira Salles, from the billionaire banker family Moreira Salles (of Itaú Unibanco).
Despite claiming independence from the editorial control of Revista Piauí, also controlled by the Moreira Salles family, Agência Lupa continues to be virtually hosted by Piauí’s resources, where Tardáguila worked as a journalist from 2006 to 2011. Furthermore, she also received support from the Instituto Serrapilheira, also from the Moreira Salles family, during the health crisis to act as a mechanism for imposing the pandemic consensus in what was one of the largest social experiments in human history.
In parallel, it is relevant to mention that the same João Moreira Salles was involved decades ago in a scandal after it was revealed that he had financed “Marcinho VP,” one of the leaders of the drug trafficking organization Comando Vermelho. Moreira Salles made a deal with the justice system to avoid being held accountable for this involvement.
Tardáguila was also the deputy director of the International Fact-Checking Network, an absolutely “independent” “fake news combat” network, yet funded by institutions such as the Open Society, the Bill & Melinda Gates Foundation, Google, Meta, the Omidyar Network, and the US State Department, through the National Endowment for Democracy.
Today Tardáguila no longer runs Lupa, but her “profile” on the official page of the National Endowment for Democracy (notorious funder of color revolutions and disinformation operations around the world) states that she is quite active at the Equis Institute, which counts among its funders the abortion organization Planned Parenthood, and aims to conduct social engineering against “Latino” populations.
Lupa is currently headed by Natália Leal. Contrary to the narrative of “independence,” the reality is that she has worked for several Brazilian mass media outlets, such as Poder360, Diário Catarinense, and Zero Hora, in addition to also writing for Revista Piauí, from the same Moreira Salles. Leal is less “internationally connected” than Tardáguila, but she was “graced” with an award from the International Center for Journalists, an association of “independent journalists” that, in fact, is also funded by the US State Department’s National Endowment for Democracy, the Bill & Melinda Gates Foundation, Meta, Google, CNN, the Washington Post, USAID, and the Serrapilheira Institute itself, also from Moreira Salles.
Quite clearly, it is somewhat difficult to take seriously the notion that Lupa would have sufficient autonomy and independence to act as an impartial arbiter of all narratives spread on social networks when it and its key figures themselves have these international connections, including at a governmental level.
But even on a practical level, it is difficult to take seriously the self-attributed role of confronting “fake news.” Returning to the pandemic period, for example, the differentiated treatment given by the company to the Russian Sputnik vaccine and the Pfizer vaccine is noteworthy. The former is treated with suspicion in articles written in August and September 2020, both authored by Jaqueline Sordi (who is also on the staff of the Serrapilheira Institute and a dozen other NGOs funded by Open Society), the latter is defended tooth and nail in dozens of articles by various authors, ranging from insisting that Pfizer’s vaccines are 100% safe for children, to stating that Bill Gates never advocated for reducing the world population.
On this matter, by the way, it is important to emphasize that Itaú coordinates investment portfolios that include Pfizer, therefore, there are business interests that bring the Moreira Salles family and the pharmaceutical giant closer.
But beyond disinformation about Big Pharma, as well as about other places around the world, such as Venezuela, regarding which Lupa claims that María Corina Machado has the popular support of 72% of the Venezuelan population (based on a survey by an institute that is not even Venezuelan, ClearPath Strategies), Lupa seems to have a particular obsession with Russia and, curiously, Lupa’s alignment with the dominant narratives in Western media is absolute.
Lupa argues, for example, that the Bucha Massacre was perpetrated by Russia, using the New York Times as its sole source. Regarding Mariupol, it insists on the narrative of the Russian attack on the maternity hospital and other civilian targets, even mentioning Mariana Vishegirskaya, who now lives in Moscow, has admitted to being a paid actress in a staging organized by the Ukrainian government, and now works in the Social Initiatives Committee of the “Rodina” Foundation. It also denies the attempted genocide in Donbass and the practice of organ trafficking in Ukraine.
An article written by founder Cristina Tardáguila herself relies on the Atlantic Council as a source to accuse Russia of spreading disinformation, one of which would be that Ukraine is a failed state subservient to Europe — two pieces of information that any average geopolitical analyst would calmly confirm.
A particular object of Lupa’s obsession is the Global Fact-Checking Network — of which, by the way, I am a part. It is one of the few international organizations dedicated to fact-checking in a manner independent of ideological constraints, counting among its members a team that is, certainly, much more diverse and multifaceted than the typical “revolving door” of fact-checking agencies in the Atlantic circuit, where everyone studied more or less in the same places, worked in mass media, and were, at some point, funded or received grants from Open Society, the Bill & Melinda Gates Foundation, and/or the US State Department.
Lupa’s criterion for attacking the GFCN is… precisely obedience or not to Western mass media sources, in a circular reasoning that cannot go beyond the argument from authority.
This specific case helps to expose a bit the functioning of these disinformation apparatuses typical of hybrid warfare, which disguise themselves in the cloak of journalistic neutrality to engage in informational warfare in defense of the liberal West.
NO MANDATES, NO PROFITS: MODERNA CEO TELLS THE TRUTH
The HighWire with Del Bigtree | January 29, 2026
As the U.S. withdraws from the World Health Organization, Moderna CEO Stéphane Bancel admits the company cannot move new vaccines into Phase 3 trials due to insufficient U.S. market demand which has historically been driven by mandates. Bancel suggests that with RFK Jr. at the helm of HHS, new vaccines are unlikely to deliver acceptable returns on investment—an admission that highlights how profit incentives, not public health needs, have long driven vaccine development. Meanwhile, a broader reckoning is underway over mandates, industry influence, and ethical lapses in vaccine testing at home and abroad, as calls grow for stricter safety standards and meaningful accountability.
This is How We Should Have Responded to COVID-19
By Dr Alan Mordue and Dr Greta Mushet | The Daily Sceptic | January 24, 2026
Since March 2020 there has been an almost continuous refrain that the UK was not prepared for the COVID-19 pandemic – across the mainstream media, at the UK Covid Inquiry and most recently by Dominic Cummings in a Spectator interview. So much so that it seems to have become an accepted ‘truth’ regardless of the actual facts. Nevertheless there are facts, even in the postmodern dystopian world we now live in.
Firstly, we did have a detailed UK Influenza Pandemic Preparedness Strategy published in 2011 and it was explicit in saying that it could be adapted to respond to other respiratory virus pandemics, and gave as an example the first Severe Acute Respiratory Syndrome virus (SARS). Secondly, there was further national guidance in 2013 and 2017 to update the strategy. Thirdly, this national guidance helped all four nations and each local health board or authority to develop their own pandemic plans which were regularly reviewed and updated. Fourthly, we had many systematic reviews of the evidence for non-pharmaceutical interventions (NPIs) to minimise transmission, one published only a few months before the COVID-19 pandemic started. And finally, the UK scored second in a global assessment of countries’ pandemic preparedness in 2019.
So, the ‘unprepared’ mantra was not the whole truth and arguably we were comparatively well prepared. However, in the event all this preparation did prove to be useless – but only because we decided to abandon it all in March 2020. We binned our pandemic plans and ignored the careful reviews of the evidence and the experience gained responding to previous pandemics. No doubt the UK strategy will be updated, but whatever is produced could be just as easily discarded next time. So what can be done?
Perhaps what we need is something more accessible, something that reflects the ethical and democratic foundations of our country, and, given how important this is for the whole of society, something that is shared widely – well beyond public health departments, the office of the Chief Medical Officer (CMO), the Scientific Advisory Group for Emergencies (SAGE) and the NHS. Core principles on how we should respond to a pandemic that are shared, understood and agreed with the public, perhaps through their representatives in Parliament, might give us some scientific, ethical and governance guardrails. They might help to improve and protect accountability and also stand a better chance of surviving beyond a few weeks when the next pandemic hits.
If so, what might such principles contain? Here we offer some suggestions with commentary on how they were applied, or not, during the Covid-19 pandemic, grouped under four headings – epidemiological, medical, ethical, and democratic. Many of these principles don’t appear in the UK Strategy, or those of the four nations or local pandemic plans … and for very understandable reasons. Prior to 2020 they were taken for granted, they were so obvious that they did not need stating, they were the principles and codes that the public health specialty and the medical profession had followed for decades if not centuries, they were the way we conducted ourselves in our liberal democratic society. The Covid-19 pandemic response changed all that – we now clearly need to restate our commitment to core, indeed fundamental, principles.
Epidemiological principles

The first task in epidemiology is to assess the scale and severity of a new disease or health problem, examine how it varies by time, place and person (age, sex, occupation etc.), and compare it with other diseases. This helps to ensure that any response is proportionate and identifies those at greater and lower risk, as well generating hypotheses about potential causes.
In the context of a respiratory viral pandemic, data on case and infection fatality ratios are paramount. These were available early in the COVID-19 pandemic and before the first UK lockdown. Instead of these data being reported accurately, compared to previous pandemic data and carefully explained to the population (for example here), public messaging was alarmist and seemed designed to instil fear not reassure, and made little reference to those at lower risk (see Laura Dodsworth’s 2021 book A State of Fear). In a future pandemic the public should expect such data, the media should demand them, the CMO should have a responsibility to identify and collate them, and government responses should be calibrated based upon them.
Then to ensure accurate monitoring of the developing pandemic within the country and valid comparison to earlier pandemics the standard definitions for confirmed cases, hospitalisations and deaths should be employed. This did not happen in the COVID-19 pandemic with new definitions adopted, definitions that for all three exaggerated the statistics. This was compounded by inappropriate widespread testing using a PCR test insufficiently specific and using inappropriate cycle thresholds.
There was a further concern that arose during the pandemic response on the epidemiological front: the use and impact of modelling studies. Whilst such studies can be helpful they cannot be interpreted without understanding their underlying inputs, assumptions and methods. They are ‘what if’ studies – for example, what if we assume that the number of cases will grow exponentially without any seasonal effect, what if we assume no existing immunity in the population from other coronaviruses, etc. The Imperial College modelling study published in March 2020 seems to have had a significant impact on the push for the first lockdown, but it had not been peer-reviewed and seems to have been insufficiently debated and challenged; of course, it is now widely considered to have been flawed. Modelling studies are not reality, they are not facts, they are not evidence, they are better viewed as ‘what if’ scenarios and their assumptions and results should be rigorously challenged. Their presentation to politicians without critical analysis and careful interpretation amounts to professional negligence.
Medical principles

Science and medicine only develop through open debate and a willingness to consider alternative views, even if they are contrary to the current orthodoxy. This did not happen during the COVID-19 pandemic, as the oft repeated term ‘The Science’ demonstrates. There is no such thing: there is rarely a consensus and science is never settled, we only ever have the current disputed theories which remain until better ones come along. Any pandemic response should be open to challenge and wide debate so that we are not limited to the knowledge and experience of only a few prominent scientific and medical government advisors. The thoughtful and detailed letters addressed to the Medicines and Healthcare Products Regulatory Agency (MHRA) and Joint Committee on Vaccination and Immunisation (JCVI) from often in excess of 100 doctors and scientists on the merits or otherwise of Covid vaccination of children were a case in point, and were ignored or summarily dismissed. Public health messages to the population certainly need to be clear and if possible consistent to maximise understanding, but this does not preclude an open and vigorous debate within the medical and scientific community, something that is essential if we are to develop an optimal response.
In 1979 Archie Cochrane, widely regarded as the father of evidence-based medicine, made his famous comment that: “It is surely a great criticism of our profession that we have not organised a critical summary, by speciality or subspeciality, adapted periodically, of all relevant randomised controlled trials.” The international Cochrane Collaboration, named after him and designed to address this criticism, produced a series of systematic reviews on the effectiveness of physical interventions to interrupt or reduce the spread of respiratory viruses such as school and business closures, social distancing measures and restrictions on large gatherings. Despite the limited evidence for effectiveness and the relatively poor quality of the evidence from these reviews and similar conclusions from a WHO review published in September 2019, almost all these measures were applied to the whole population from March 2020, including a ‘lockdown’ of healthy people.
We copied the response of a totalitarian state despite a lack of evidence and despite the fact that these same systematic reviews drew attention to the widespread harms that would be caused by implementing these measures across the whole population. These harms are beginning to be appreciated across multiple areas – in terms of mortality and physical health particularly of older people, the social development of young children, the mental health and education of young people, businesses across the country as well as jobs, the economy and the benefits system.
An evidence-based approach also required a thorough review of the evidence on the benefits and harms for the prevention and treatment of COVID-19 in individuals. The limited data on the effectiveness of the novel gene technology ‘vaccines’ (and see Clare Craig’s 2025 book Spiked – A Shot in the Dark) and on their side-effects, with no data at all on long term harms, pointed clearly towards their use only in those at higher risk with full disclosure on what was known and what was not. In the event, of course, they were recommended and pushed on most of the population including those at insignificant risk. Furthermore, ‘safe and effective’ was far from a full disclosure of the evidence on benefits and risks.
By contrast, the use of re-purposed drugs such as ivermectin with known anti-viral and anti-inflammatory effects, extensive evidence on effectiveness and a well-documented safety profile, was actively discouraged.
In all these areas, doctors should be acting as advocates for their patients, informing them as best they can and helping them to make decisions on their treatment and care, as required by the General Medical Council’s guidance ‘Good Medical Practice.’ However, as already discussed, the informing was cursory and partial, and the contact often non-existent or via leaflet or video-call.
If they are to regain public trust the medical profession and public health authorities must do better next time, and patients and the public must demand better information and better discussion and engagement with medical staff to help them make decisions.
Ethical principles – informed consent for individuals

The Greek philosopher and physician Hippocrates developed his Oath around 400 BC. It urged doctors to act with beneficence – that is, to help their patients and prevent harm – and non-maleficence – that is to do no harm themselves or primum non nocere. The term appropriateness brings these two concepts together – an appropriate treatment is one that has been chosen because its benefits outweigh its harms in the particular patient.
As outlined above, evidence-based medicine involves the careful assessment of the evidence, ideally from randomised controlled trials, to quantify these benefits and harms. Whilst the patient advocacy role of doctors involves them in informing and supporting their patients to make informed decisions on their treatment and care.
Although this process sounds simple and straightforward, it is not. It seems to be taken more seriously in surgical practice, after notable legal cases, but less so in medical practice with the prescribing of drugs and vaccines. Certainly in the pandemic consenting practices for vaccination were cursory, to the point of being non-existent – public information heralding the ‘safe and effective’ vaccines was at best partial, and coercion was widespread via national advertising that deliberately sought to shame and manipulate, via vaccine mandates, and via bans from venues without proof of vaccination (or negative Covid antigen tests).
Large relative risk reductions of 70% for the Astra Zeneca ‘vaccine’ and 95% for the Pfizer ‘vaccine’ were trumpeted, but not the smaller, less convincing absolute risk reductions of around 1-2%. And there was no attempt to directly compare benefits and risks and harms, the key information a patient needs to give fully informed consent.
The wholesale abandonment of standard codes of practice for informed consent during the pandemic was truly shocking. To regain public trust the medical profession needs to take this key responsibility more seriously and particularly improve practice in relation to long term medications and vaccinations.
Democratic principles

The UK Strategy of 2011 did emphasise the importance of accurate and timely information to the public, and stressed that uncertainty and any alarmist reporting in the media could create additional pressures on health services. Despite this, the early epidemiological data on the scale and severity of the COVID-19 pandemic, a comparison with previous pandemics and clear identification of those at higher and lower risk were not shared with the public and carefully explained. The data that were given were far vaguer and the messages seemed designed to raise anxiety rather than contain it and modulate it to appropriate levels. Government advisors seem to have entirely lost sight of these crucial epidemiological data that are so essential to enable the government to calibrate its response and ensure it was proportionate. Data reflecting reality seem to have been overshadowed by modelling data reflecting potential future scenarios – fiction rather than fact influenced key decisions.
Whatever national response is being contemplated to a pandemic, there needs to be a clear separation of the medical and scientific evidence on the benefits and risks of specific interventions on the one hand, and the political value judgements and decisions on the other. Governmental advisors must present options and their benefits, risks, harms and likely costs to ministers, and in a democracy it is for ministers to decide as they are accountable to the electorate. This relationship is akin to the doctor-patient relationship – the doctor informs the patient and supports him or her to make his or her own decision but does not lead or coerce. This line may have been blurred during the COVID-19 pandemic. Moreover, government advisors seemed reluctant to identify, and where possible quantify, the risks, harms and costs that might flow from the options they put to ministers despite some, like lockdowns, being unprecedented in their severity and scope.
In turn ministers and politicians more generally have a responsibility to ensure that their advisors present them with the epidemiological data and the data on the benefits, risks and costs of recommended options. Ministers also have a responsibility to ensure that differences of opinion on how best to respond within the medical and scientific community are fully aired and discussed. This is crucial to arrive at an optimal response and to avoid groupthink. Only if ministers do these things can they take decisions on behalf of their population and give fully informed consent.
Crucially ministers have a particular responsibility to protect the basic freedoms we enjoy in a democratic society – freedom of speech, association and movement and individual bodily autonomy when it comes to medical treatments. Any infringement of such basic freedoms demands a clear, unambiguous and overwhelming justification, must be subject to challenge in Cabinet and Parliament, and must be the least restrictive as is possible to achieve the aim – in extent, impact and time. This is such a fundamental issue that we perhaps need to develop a framework to guide and constrain actions: defining the types of evidence and high thresholds that are required; limiting powers in terms of their impact, duration and the number of people affected; and outlining checks and balances, with perhaps an automatic independent review afterwards. We have such a clear and rigorous framework for compulsory detention under the Mental Health Acts when one individual is affected: we need at least as rigorous a framework when the freedom of millions is at stake.
There has also been considerable criticism of how the usual democratic governance systems were subverted and avoided during the pandemic, including the use of emergency legislation by the executive without appropriate challenge within Parliament. These governance systems are essential to enable questioning and challenge by MPs and select committees with the aim of improving decision making, and to ensure a clear justification for measures taken and transparency to facilitate accountability. This did not happen during the COVID-19 pandemic as clearly outlined in The Accountability Deficit by Kingsley, Skinner and Kingsley (2023).
In all of these four areas – epidemiological, medical, ethical and democratic – principles were violated during the COVID-19 pandemic with dire consequences for health, basic freedoms, quality of life, education, business and the economy, and for democracy and society itself. Before 2020 it would have seemed unnecessary to state such core principles. Now, having set a precedent when we abandoned them, it seems absolutely essential not only to restate them but to discuss them widely and if possible to reaffirm our commitment to uphold them before another pandemic hits.
Dr Alan Mordue is a retired consultant in public health medicine and Dr Greta Mushet is a retired consultant psychiatrist and psychotherapist.
The UK Covid Inquiry: Propaganda to protect the ‘pandemic’ narrative
By Gary L. Sidley | Propaganda In Focus | January 9, 2026
On the 20th of November, 2025, the UK Covid Inquiry published a report on Module 2 of its ongoing review titled, ‘Core decision-making and political governance’. Despite, to date, spending around £192 million of taxpayers’ money on an in-depth investigation into the management of the 2020 ‘pandemic’, this 800-page tome indicates that the overarching conclusion of the Inquiry will most likely be that the unprecedented and net harmful government responses (lockdowns, mask mandates, vaccine coercion) were all necessary, and the only problems related to the timings of the interventions and process failures. As such, this Module 2 report can be reasonably construed as a propaganda exercise primarily intent on preserving the core elements of the dominant, fundamentally flawed, covid narrative.
In the words of the oft-quoted Edward Bernays, propaganda involves ‘the conscious and intelligent manipulation of the organized habits and opinions of the masses’. It is clear that this Module 2 report, and the UK Covid Inquiry as a whole, strive to do just that. With the primary goal of protecting the ‘pandemic’ story – that in early 2020, a uniquely lethal pathogen spread carnage across the world, and unprecedented and draconian restrictions on our day-to-day lives were essential to prevent Armageddon – the inquiry has incorporated a range of manipulation techniques designed to promulgate this state-sanctioned ideology. The two most prominent opinion-shaping strategies deployed by the Inquiry have been the suppression of dissenting perspectives, and a narrowing of the Overton window.
Suppression of dissenting perspectives
In her initial selection of ‘core participants’ for the Inquiry, Chairperson Baroness Hallett signalled her intention to marginalise voices that were likely to be critical of the official covid narrative. Those granted core status benefitted from the opportunity to make opening and closing statements, and to suggest lines of questioning to the witnesses, whereas those groups excluded were limited to submitting written evidence in the hope that it would be considered by the Inquiry team. Organisations who had been openly opposed to the mainstream public health responses during the covid event – for example, Us For Them (who repeatedly highlighted the devastating impact of the restrictions on our nation’s children) and the Health Advisory & Recovery Team (a group of scientists and clinicians concerned about ‘pandemic’ policy and guidance recommendations) – were unsuccessful in their applications.
Consideration of those groups who were permitted to be core participants for Module 2 clearly shows a preponderance of stakeholders who were highly likely to be on board with the central tenets of the official covid narrative. In addition to the expected establishment figures (representatives from various government departments, the Office of the Chief Medical Officer, the UK Health Security Agency) and four ‘Covid-19 Bereaved Families for Justice’ groups, it is difficult not to conclude that other core participants were selected on account of their fervour for more and earlier restrictions. For instance, despite ‘long covid’ being a highly contested concept, three groups representing the victims of this assumed malady were awarded core status. Similarly, the British Medical Association (who energetically campaigned for longer lockdowns and stricter mask mandates) also managed to secure a place in Baroness Hallett’s inner circle.
Despite this crude censorship, a significant amount of critical commentary did reach the Inquiry, in the form of both live testimony and written statements. Crucially, however, these counter narratives were de-emphasised by the Inquiry team and – subsequently – were not reflected in its conclusions. One blatant example of a dissenting voice being prematurely curtailed was the interview with Carl Heneghan, Professor of Evidence-Based Medicine and longstanding critic of the dominant covid narrative. When Heneghan asserted that expert interpretation of published research constitutes valid evidence for the Inquiry, Hallett retorted, ‘Not in my world it doesn’t … if there is anything further, please submit it in writing’. This abruptness contrasts sharply with the deferent, sometimes sycophantic, way establishment witnesses were managed by the Inquiry team.
Narrowing the Overton window
It was apparent from the start of the UK Covid Inquiry that Baroness Hallett and her legal team had decided which public health decisions made during the covid event were open to critical scrutiny and which were not. This contraction of the Overton window ensured that crucial elements of the official narrative were shielded from critical analysis.
To illustrate, three pre-determined assumptions – foundational to the official covid story – seemed to fall into this protected category:
1. Lockdowns were necessary
The headline-grabbing conclusion in the Module 2 report was that locking down a week earlier would have saved 23,000 lives. This absurd deduction was not based on robust science or real-world studies, but drawn from the fantasy realm of mathematical modelling. An in-depth analysis of covid-era decision making (which is what the Inquiry was supposed to be) would have given prominence to a detailed cost-benefits evaluation of lockdowns, a process that would have revealed the substantial harms of this unparalleled pandemic restriction. The key reason for the omission of this vital analysis was the Inquiry’s premature assumption that lockdowns were an effective public health tool, essential for the containment of a – purportedly – novel virus.
More specifically, Baroness Hallett and her team adopted a classic propaganda strategy, commonly referred to as ‘unanimity’. With the presumption that all right-thinking people recognise that lockdowns save lives, the Overton window was squeezed to become merely a question of timing; any testimony straying outside of this range of acceptability was ignored – or, at best, reduced to background noise – while, in contrast, speculations about the life-saving benefits of an earlier societal shutdown were amplified.
2. The mass vaccination programme was a great success
Despite increasing recognition that the covid vaccines were less efficacious, and more harmful, than initially claimed, the Inquiry appears to have adopted the foundational assumption that these novel products were safe and effective, and anyone who believed otherwise must constitute a deviant minority at odds with the unanimous opinion of right-thinking people. Indications for the constant presence of this guiding notion are brazen. Thus, Hugo Keith KC (the lead counsel to the Inquiry) has, at various points during his interactions with witnesses, described the vaccines as ‘entirely effective… undoubted successes… with lifesaving benefits that vastly outweighed the very rare risk of serious side effects’. Similarly, Baroness Hallett – at the press conference announcing the findings of Module 2 – hailed the vaccine programme as a ‘remarkable achievement’.
3. Community masking was not associated with any appreciable negative consequences
It was evident at an early stage in the Inquiry that another untouchable premise was that the masking of healthy people in community settings was a sensible precaution that could only have net benefits. Thus, when Professor Peter Horby, the chair of NERVTAG (a high-profile SAGE advisory group), gave evidence in October 2023 he reiterated his group’s 2020 conclusion that the evidence for mask effectiveness in reducing viral transmission was ‘weak’; Lady Hallett interjected, saying, ‘I’m sorry, I’m not following … if there’s a possible benefit, what’s the downside? Horby responded to this challenge by suggesting that respect for institutional science was at stake – in keeping with the majority of the establishment scientists, he failed to highlight the considerable harms associated with routine masking.
The Inquiry’s pre-formed assumption that compelling people to wear face coverings was a public health intervention free of negative consequences was confirmed by the Module 2 report with its emphatic conclusions that:
‘The experience of the Covid-19 pandemic has shown that wearing a face covering has minimal disadvantage for the majority of the population.’
‘In any future pandemic where airborne transmission is a risk, the UK government and devolved administrations should give real consideration to mandating face coverings for the public in closed settings.’ (p. 288)
In conclusion, the overarching take-home message from the Inquiry to date is that public health strategy adopted by the government in response to the emergence of a novel virus in 2020 was essentially the correct one, and any criticism of the official covid narrative should be confined to process issues, such as the timing of restrictions. Devoid of any forensic analysis of their costs and benefits, Lady Hallett and her team have concluded that lockdowns, mRNA vaccines, and mask mandates all achieved positive outcomes and should therefore be repeated when we encounter the next ‘pandemic’. By amplifying voices supportive of the official covid narrative, while marginalising critical viewpoints, the Inquiry has succeeded in strengthening its – apparently pre-determined – perspective that, irrespective of any harms caused, the restrict-and-jab approach was, ultimately, for the greater good.
Most commentators who have been sceptical of the official covid narrative will not be surprised by the Inquiry’s conclusions. Given that the political elites, along with prominent public health mandarins, enthusiastically endorsed the calamitous restrictions and vaccine rollout (and continue to do so) the damage to the establishment of drawing different, more condemnatory, inferences would have been immense. From the perspective of our global leaders, the Inquiry to date is – no doubt – serving its primary purpose of concealing the true ramifications of the covid response from the general population.
Gary Sidley, PhD, is a former NHS consultant clinical psychologist with over 30-years’ experience of clinical, professional and managerial practice in adult mental health. In 2000, he obtained his PhD for a thesis exploring the psychological predictors of suicidal behaviour and has multiple mental health publications to his name, including academic papers, book chapters, and his own book, ‘Tales from the Madhouse: An insider critique of psychiatric services). Since the start of the covid event, he has written many articles critiquing the government’s nudge-infused messaging and mask mandates, including pieces for the Spectator, the Critic and Self & Society. More of his articles can be found on his ‘Manipulation of the Masses’ Substack.
Scientists accuse Cochrane Reviews of using biased studies to claim HPV vaccine prevents cancer
‘Completely misleading’
By Brenda Baletti, Ph.D. | The Defender | January 26, 2026
The prestigious Cochrane Library in November 2025 published two reviews touting the safety and efficacy of the HPV vaccine.
In a press release, Cochrane claimed the reports showed that girls vaccinated before age 16 were 80% less likely to develop cervical cancer, and that there was no evidence the human papillomavirus (HPV) vaccine caused any serious adverse events.
Cochrane is widely cited as the “gold standard” of systematic reviews. Major news organizations, from NBC News to The BMJ, repeated claims made in the press release.
The BMJ wrote that the researchers wanted to “share high quality data to counter misinformation spread on social media, which has had a massive impact on vaccination rates.”
The two reviews were published together. One assessed evidence from clinical trials, the other examined observational studies.
Co-author Nicholas Henschke declared that based on the reviews, “We now have clear and consistent evidence from around the world that HPV vaccination prevents cervical cancer.”
Co-author Hanna Bergman told Cochrane that the evidence from the clinical trials confirmed that HPV vaccines are “highly effective” and “without any sign of serious safety concerns.”
However, experts who analyzed the reviews in detail told The Defender that based on their analyses of the reviews, they determined that the authors relied on a small number of studies with a high risk of bias for their claim that the HPV vaccine prevented cancer.
The experts said they identified similar patterns when they analyzed other outcomes cited by the researchers.
“We know that the meta-analysis can only be as good as the quality of the studies included in the meta-analysis,” Lucija Tomljenovic, Ph.D., a biochemist, said.
Yet the vast majority of the studies the authors relied on to make their most dramatic conclusions about cancer and cancer-related lesions were at “serious or critical risk of bias,” according to the study authors themselves, she said.
“If this is not a gross misinterpretation of evidence, I don’t know what is,” Tomljenovic said.
A systematic review is a “study of studies,” a high-level research method that reviews, synthesizes and critically appraises the available body of evidence for a given disease or health topic in a standardized and systematic way.
Healthcare policymakers often use them to guide their decision-making.
Researchers use a crucial metric — “risk of bias” — to evaluate the studies and determine whether to include them in a systematic review.
Risk of bias indicates the likelihood that a study contains a systematic error that could cause its results to deviate from the truth, which could lead to an over- or underestimation of the effect of an intervention — in this case, the HPV vaccine.
Authors draw ‘completely misleading’ conclusions based on the evidence with high risk of bias
Although the two Cochrane reviews claimed to find an 80% reduction in cancer rates, the review of clinical trials stated that the studies evaluated “were not of sufficient duration for cancers to develop. Four studies reported on cancer. No cancers were detected.”
The observational review, which evaluated different studies to assess the impact of HPV vaccination on the general population, claimed there was “moderate‐certainty evidence” from 20 studies that HPV vaccination reduces the incidence of cervical cancer.
However, Tomljenovic said that only four of the 20 studies had a moderate risk of bias. The other 16 studies had either serious or critical risk of bias.
Of the four studies with a moderate risk of bias, one did not even include cervical cancer as an endpoint, and the follow-up was only seven years — which is not enough time for cancer to develop. Instead, the studies measured persistent HPV infections, Tomljenovic said.
As a proxy for cancer, many studies examined precancer outcomes, focusing on the reduction in CIN3+ — or cervical squamous intraepithelial neoplasia 3 — which are abnormal cells found on the cervix that may be precancerous and are caused by a high-risk HPV type.
Tomljenovic also found that of the 23 eligible studies included in the meta-analysis investigating CIN3+ lesions, only a single study was overall at moderate risk of bias. The other 22 had serious or critical risk of bias.
On this shaky basis, she said, the authors concluded, “There are now long-term outcome data from different countries and from different study designs that consistently report a reduction in the development of high-grade CIN and cervical cancer in females vaccinated against HPV in early adolescence.”
Tomljenovic called that conclusion “completely misleading.” She said that the authors of the Cochrane reviews themselves judged the vast majority of studies that “consistently” report reduction in cervical cancer and high-grade CIN lesions to be at serious and critical risk of bias.
“The best evidence for reduction from only a handful of studies was at a moderate risk of bias rather than low,” she added.
Lancet study conclusions, cited by Cochrane, are ‘patently absurd’
The Cochrane review of observational studies included the widely cited 2021 study in The Lancet, which investigated the impact of HPV vaccination in England. The Lancet study claimed to offer first direct evidence of prevention of cervical cancer using the Cervarix vaccine — not available in the U.S.
The Lancet study claimed an 87-97% relative reduction in cervical cancer rates and CIN3 lesions in girls vaccinated at ages 12-13 compared to unvaccinated girls.
The authors claimed that vaccination “has almost eliminated cervical cancer and cervical precancer up to age 25,” Tomljenovic said. However, her own analysis of U.K. cervical cancer statistics from Cancer Research UK tells a different story.
Tomljenovic found that data show that since the early 1990s, cervical cancer incidence rates decreased by 25% in females in the U.K., and have remained stable over the last decade.
She found that cervical cancer incidence rates reached their lowest point somewhere between 2004 and 2007 — a year before the HPV vaccine was introduced in the U.K.
“Since then, the incidence rates of cervical cancer have actually slightly increased, not decreased,” Tomljenovic said. “Therefore, these data completely contradict the conclusions of The Lancet study.”
In light of the cervical cancer incidence in the U.K. over time, she said, the claim by the The Lancet study authors that HPV vaccination with high coverage in 12-13-year-old girls has almost eliminated cervical cancer and cervical precancer up to age 25 “is patently absurd.”
Screening, healthy practices prevent cervical cancer, and affect study outcomes
Children’s Health Defense Senior Research Scientist Karl Jablonowski said, “The HPV vaccines are pushed, because they allegedly prevent cancer. Yet, a comprehensive review of the world’s literature on HPV vaccinations concludes an insufficient body of evidence exists.”
Dr. Sin Hang Lee, a pathologist and expert in molecular diagnostics who has extensively studied the HPV vaccine, told The Defender that most HPV infections — even high-risk types — are cleared by the immune system. He said cervical cancer is a predictable and preventable disease because it can be identified early through regular pap screenings and treated.
“With proper gynecological care, no woman should have cervical cancer or die of cervical cancer,” Lee said.
According to Lee, the cohort studies assessed in the Cochrane review that reported a reduced risk of cervical cancer following the HPV vaccine were conducted in countries where it is less likely that gynecologists may remind patients to do pap screening follow-ups.
The basic flaw of using observational cohorts to detect efficacy, he said, is that “observational studies are subject to healthy user effect and healthy adherer effect, which may lead to erroneous conclusions,” and create a statistical bias.
That means women who choose to receive a vaccine to prevent cervical cancer are also more likely to seek other preventive services and practice healthy behaviors that affect cervical cancer. This includes exercising more, eating a healthier diet, having fewer sex partners, and avoiding tobacco, excessive alcohol intake and illicit drugs.
“A healthy lifestyle is known to affect the rate of clearance of HPV infections,” Lee added.
Observational studies typically compare these women to women who did not get the vaccine, “which may lead to erroneous conclusions.”
No serious adverse effects?
The Cochrane authors also claimed their findings dispute claims about serious adverse effects “reported on social media.”
However, social media isn’t the only place where serious adverse events, including autoimmune conditions like POTS [postural orthostatic tachycardia syndrome] and POI [primary ovarian insufficiency], have been reported.
The vaccine adverse event databases (VAERS and VigiBase) contain reports of serious adverse events. So do numerous case studies and Merck’s own internal data — as revealed in court documents from hundreds of lawsuits filed in state and federal courts against Merck, the maker of the Gardasil HPV vaccine.
Writing in response to the Cochrane findings in a letter to The BMJ, Dr. Peter Gøtzsche, ousted founder of the Cochrane Collaboration and founder of the Institute for Scientific Freedom, wrote that his own research group conducted a peer-reviewed systematic review that found “the HPV vaccines increased serious nervous system disorders significantly.”
Gøtzsche said that as an expert witness in a case against Merck, he documented that Merck “had hidden cases of serious neurological harms on Gardasil from the drug regulators.” Gøtzsche published his findings in a recent book.
Other research studies have identified similar adverse events. This includes a study published in Human Vaccines and Immunotherapeutics in July 2025. The study, which analyzed reports in the VAERS database related to Gardasil between 2015 and 2024, used multiple statistical signal-detection methods to identify safety signals for the Gardasil vaccine.
The researchers identified signals for certain neurological and autoimmune-related conditions, including POTS, eye movement disorders, autoimmune thyroiditis and posture abnormality — none of which are isted on the vaccine’s label.
U.S. regulators taking a closer look at HPV vaccines?
When the Centers for Disease Control and Prevention (CDC) earlier this month reduced the number of recommended routine childhood vaccines, the agency left the controversial HPV vaccine on the schedule.
However, the CDC now advises a single dose of the HPV vaccine, instead of the previous two-dose regimen. In making the new recommendations, the U.S. Department of Health and Human Services cited a growing global consensus that one shot is effective at protecting against HPV.
Investigative reporter Maryanne Demasi, Ph.D., reported last week that after nearly two decades on the childhood immunization schedule, the HPV vaccine is being subjected to closer scrutiny.
The CDC’s Advisory Committee on Immunization Practices (ACIP) convened a new workgroup to reexamine the vaccine from the ground up — including its effectiveness, dosing, safety and long-term population impact.
Massachusetts Institute of Technology Professor Retsef Levi, a current ACIP member who has repeatedly called for longer safety follow-up and greater transparency about uncertainty in vaccine science, is leading the workgroup, Desmasi wrote.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Vicious
Lies are Unbekoming | January 25, 2026
The waiting room is clean. The receptionist is polite. The forms ask reasonable questions. Nothing in the physical environment suggests danger. The magazines are current. The hand sanitizer dispenser works. Someone has chosen calming colors for the walls.
A pregnant woman sits in a chair designed for her comfort. She has been told to be here. Not ordered—no one orders. Recommended. Strongly recommended. Everyone does this. Her mother did this. Her friends did this. The women in her prenatal group compare notes about their appointments the way they compare notes about nursery furniture. Which provider did you choose? What tests have you had? The questions assume the answers. The answers assume the questions.
She will be offered things today. Offered is the word used. The offers will come with information sheets that list risks and benefits in tabular form. She will sign consent documents. Everything will be voluntary in the legal sense. No one will hold her down. No one will threaten her. She will choose, and her choices will feel like choices, and she will leave feeling she has done the responsible thing.
What she will not feel is the weight of what has been arranged before she arrived. The scheduling software that ensures the appointment is short enough to be profitable. The protocol that determines which tests are “standard” regardless of her individual circumstances. The liability calculations that make defensive intervention safer for the provider than watchful waiting. The training her provider received, which did not include the word “cascade” and did not question the premises. The pharmaceutical representative who visited last month. The professional guidelines written by committees with financial ties to the interventions they recommend. The insurance code that reimburses procedures but not conversations. The architecture of the building itself, which presumes birth is a medical event requiring medical facilities.
None of this is secret. All of it is documented, published, occasionally debated in journals that no one outside the profession reads. The machinery operates in plain sight. It has operated for so long that its operation feels like nature—the way medicine works, the way pregnancy is managed, the way responsible people behave.
She cannot see it because she is inside it. The water she swims in. The air she breathes. The climate of her experience.
For years I used the word “predatory” to describe this system. Predatory captured something true—the targeting, the extraction, the conversion of healthy people into revenue streams. The pharmaceutical company identifying a market. The screening program generating patients. The intervention that creates the need for the next intervention. Predation implies a hunter and prey, a calculation, a strategy.
But predatory is not quite right. A predator needs its prey. A predator pays attention to what it hunts. A predator, in some sense, respects the thing it consumes—respects it enough to study it, track it, understand its patterns. The lion watches the gazelle. The con artist studies the mark.
This system does not watch. It does not study. It processes.
The word that came to me after documenting 123 medical interventions across the arc of pregnancy and birth is different. Starker. Less strategic and more indifferent.
Vicious.
Viciousness is not cruelty, though cruelty may be one of its expressions. Cruelty requires attention. The cruel person watches suffering and derives something from it—pleasure, power, confirmation. Cruelty is a relationship, however deformed.
Viciousness requires no such relationship. A vicious mechanism can operate without anyone watching the effects. A vicious system can grind through populations while everyone involved believes they are helping. The viciousness is in the structure, not the intention. It emerges from the interaction of parts, none of which are vicious in isolation.
The doctor who follows the protocol is not vicious. The protocol is not vicious. The committee that wrote the protocol is not vicious. The pharmaceutical company that funded the research the committee relied on is not vicious—or rather, its viciousness is diffused through so many quarterly earnings reports and shareholder meetings and marketing budgets that no single person experiences themselves as causing harm. The regulator who approved the product is not vicious. The politician who mandated its use is not vicious. The parent who complies is not vicious. The neighbor who judges the parent who doesn’t comply is not vicious.
And yet.
A 13-year-old girl in London, who declined a vaccine, is being pressured about a screening test she is not eligible for. The vaccine was Gardasil, marketed as preventing cervical cancer. The screening is the smear test—cervical screening that begins at age 25 in the UK, designed to detect what the vaccine supposedly prevents. The two programs are presented as separate, but they function as a single apparatus: refuse our prevention and you must submit to our surveillance. I have documented elsewhere, in my essay The HPV Lie: Pap Smears, Gardasil, and a Cancer Caused by Something Else, why the foundational claim—that HPV causes cervical cancer—does not survive scrutiny. But for the purposes of this essay, the truth of the claim matters less than the machinery built on it.
The pressure comes from somewhere. It reaches her through channels—through school, through health messaging, through the questions of peers whose parents made different choices. No single person decided to punish her. No committee met to discuss her case. The system does not know her name.
The pressure is automatic. It is the system maintaining itself, closing gaps, ensuring that even those who refuse one element remain captured by another. The vaccine and the screening are presented as separate programs, but they function as a single apparatus. Refuse the prevention and you will be reminded, persistently, of your need for surveillance.
She is 13. The screening she is being pressured about begins at 25. There is no medical reason for anyone to be discussing it with her. The pressure is not medicine. It is correction. It is the system registering a deviation and applying force to resolve it.
No one in her life who transmits this pressure experiences themselves as being vicious. The teacher who mentions it is concerned. The nurse who brings it up is following guidelines. The friends who ask why she didn’t get the shot are simply curious, or perhaps uncomfortable with difference. Everyone is doing what people do. Everyone is being normal.
The viciousness is in the normal. The viciousness is that “normal” has been constructed, over decades, through thousands of small decisions, each one defensible, none of them examined, until the accumulated weight presses down on a 13-year-old whose only crime was asking questions.
The system is vicious. Say it plainly.
The government that approves the products, mandates their use, shields manufacturers from liability, and funds the campaigns that manufacture consent—the government is vicious.
The society that has been engineered to enforce compliance through social pressure, to treat refusal as deviance, to make the unvaccinated child a problem and the questioning mother a danger—this society is vicious.
But here is where the analysis must be careful. “The system” is an abstraction. “Government” is an abstraction. “Society” is an abstraction. These words make it easy to express outrage while leaving everyone blameless. If the system is vicious, I am not. If government is the problem, I am just a citizen. If society has been engineered, I am merely a victim of the engineering.
This is too easy. It is also untrue.
The system is made of people. Every protocol was written by a person. Every guideline was approved by persons sitting in a room. Every prescription is written by a hand attached to a body that contains a mind capable of doubt. The government is not a machine. It is people who could choose differently and do not. Society is not weather. It is the accumulated choices of everyone who participates in it—which means everyone.
The viciousness is emergent. No one designed the full harm. But the viciousness is also composed. Each component is a human decision. The emergence does not erase the composition. The fact that no one intended the complete picture does not mean no one is responsible for their corner of it.
This is the moral difficulty the essay cannot resolve, because reality does not resolve it. The harm is everyone’s and no one’s. The choices are individual and the outcome is collective. A woman loses her uterus to a surgery she did not need, and the surgeon who performed it was following the standard of care, and the standard of care was set by a committee, and the committee relied on studies, and the studies were funded by companies that profit from the surgery, and the companies are owned by shareholders who never think about uteruses, and the shareholders include pension funds, and the pension funds include the retirement savings of nurses who work in the hospitals where the surgeries are performed.
Where does blame land? Everywhere and nowhere. This is not an evasion. This is a description of how the viciousness actually works. It is distributed so thoroughly that it becomes atmospheric. It becomes the milieu. It becomes the climate that everyone moves through and no one feels responsible for, because the mechanisms of responsibility have been dissolved in the general weather.
Ivan Illich saw this decades ago. He described how institutions reshape the milieu—the environment people move through—until alternatives become unthinkable. A radical monopoly, he called it. Not a monopoly that corners a market, but a monopoly that disables people from doing things on their own. When hospitals “draft all those who are in critical condition,” he wrote, “they impose on society a new form of dying.” The institution does not merely provide a service. It reshapes reality so that the service becomes necessary.
This is what has happened with birth. With childhood. With the female body across its entire reproductive arc. The medical system has not merely offered services. It has reshaped the milieu so that moving through pregnancy without those services becomes an act of deviance. The services are not chosen from a range of options. They are the water in which choice occurs.
A woman who declines the standard interventions is not making a different choice within a shared framework. She is refusing the framework itself. This is why she is treated not as someone with different preferences but as someone who is failing—failing to be responsible, failing to care for her baby, failing to be the kind of mother the system has defined as acceptable.
The viciousness is in that definition. The system defines acceptable, and acceptable means compliant, and compliant means captured.
I documented 123 interventions across six phases of the reproductive timeline. Pre-conception capture. Pregnancy surveillance. Labor interventions. Immediate newborn procedures. Infant pathologizing. Ongoing medical capture. Each intervention has its own literature, its own justification, its own defenders. Each one, examined in isolation, can be made to seem reasonable—or at least not obviously harmful.
The viciousness becomes visible only when you see the whole arc.
A woman begins birth control at 16. The pill alters her hormonal environment for a decade or more. She stops the pill to conceive. She has difficulty conceiving—perhaps because years of synthetic hormones have disrupted her natural cycles, perhaps for other reasons. She seeks fertility treatment. The treatment works. She is pregnant.
Now she is in the system.
She receives prenatal testing that identifies risks, some real, most statistical. The risk identification generates anxiety. The anxiety generates more testing. The testing generates findings. The findings generate interventions. She is induced before her body was ready because a measurement crossed a threshold. The induction is long and painful because her body was not ready. She receives an epidural because the pain is unbearable. The epidural slows labor. She receives Pitocin to accelerate it. The baby shows distress. She receives a cesarean.
The cesarean is recorded as necessary. It was necessary—given everything that preceded it. Each step created the conditions for the next. The cascade operated exactly as designed.
Her baby is taken to the warmer for evaluation. Eye drops are administered. Vitamin K is injected. Hepatitis B vaccine is given—for a disease transmitted through sex and IV drug use, to a newborn who will do neither. The baby is observed in the nursery. Feeding is scheduled rather than on-demand. Supplementation is suggested because the baby lost weight—as all babies lose weight in the first days, a fact that would resolve with continued nursing but which becomes a problem requiring intervention.
She goes home with a baby she is not sure she knows how to feed, a body she is not sure she recognizes, a mind clouded with hormonal disruption and sleep deprivation and the particular loneliness of having been processed rather than supported.
She returns for postpartum visits. She is screened for depression. She may receive medication. The medication helps, or seems to. She continues it. She is now a psychiatric patient as well as a surgical patient. Her records follow her. Her risk profile follows her. The next pregnancy, if there is one, will be managed with reference to this one.
At no point was she mistreated in any way she could name. Everyone was professional. Everyone followed protocols. Everyone was trying to help.
The viciousness was in the protocols. The viciousness was in the accumulation. The viciousness was in the fact that no one—not one person across dozens of encounters—ever said: you could do none of this. You could wait. You could trust your body. You could go home.
No one said it because no one could say it. The milieu does not permit those words. A provider who speaks them risks liability, peer censure, loss of hospital privileges. The words are not forbidden. They are simply outside the weather. They are not rain or sun or wind. They do not exist in the climate the system has made.
Anyone who asks questions is doing something dangerous. They are noticing the weather. Asking why the sky is this particular color, why the wind blows this particular direction, why everyone walks leaning at this particular angle.
Most people never ask. The weather is just the weather. You dress for it. You complain about it. You do not inquire into its origins. You do not ask who made it, because weather is not made. Weather simply is.
But this weather was made. Every element of it was chosen. The clinical guidelines were written by people who could have written different ones. The regulatory approvals were granted by people who could have demanded different evidence. The liability structures were established by legislatures that could have established different ones. The insurance codes were set by committees that could have set different ones. The training curricula were designed by faculties that could have designed different ones.
Each choice was made by humans. Each human could have chosen otherwise. That none of them did—that the choices accumulated into a system that now operates with the indifference of weather—does not change the fact that the choices were made.
Anyone who asks questions threatens to make the choices visible. This is why they are pressured. Not because anyone decides to pressure them, but because the system cannot tolerate the visibility of its own construction. The weather must remain weather. The moment it becomes choices, it becomes contestable. The moment it becomes contestable, it can be refused.
If you have read this far, you are no longer fully inside the weather.
This is not a comfortable position. It is easier not to see. It is easier to move through the waiting room, sign the forms, accept the offers, go home feeling responsible. The system is designed for this ease. It has made compliance comfortable and refusal exhausting. The path of least resistance leads directly into the machinery.
Seeing the machinery does not stop it. One person’s recognition changes nothing about the protocols, the guidelines, the insurance codes, the training curricula. The 123 interventions will continue to be applied to the women who come after, regardless of what any individual understands.
But recognition changes what is possible.
A woman who sees the cascade can make different choices within it—can refuse this test, delay that intervention, ask questions that disrupt the automatic sequencing. She cannot escape the milieu, but she can move through it differently. She can refuse to be weather.
More importantly, she can speak. She can tell other women what she saw. She can name the viciousness, which is the first step toward refusing to participate in it. The system maintains itself partly through silence—through the assumption that everyone experiences the same thing and no one objects. Each voice that breaks the silence makes the next voice easier.
This is modest. It is not a revolution. It will not dismantle the system or defund the institutions or rewrite the guidelines. But the system depends on billions of small compliances, and each small refusal is a friction. Enough friction, accumulated over enough time, and the machinery begins to slow. Begins to be noticed. Begins to require justification rather than assuming it.
The girl in London who asked questions did something her grandmother could not do for her. She refused to accept the weather as weather. She noticed that she was being pressured and asked why. The pressure will continue—systems do not stop because one person notices them. But she has seen something that cannot be unseen.
This is what recognition makes possible: not escape, but awareness. Not freedom from the milieu, but movement within it that is no longer automatic. The end of innocence is not the same as the end of the system. But it is the end of participation without knowledge. It is the beginning of refusal.
The system is vicious. The viciousness is made of choices. The choices can be seen. Once seen, they can be refused.
One refusal at a time. One woman at a time. One conversation at a time.
The weather was made. It can be unmade. Not quickly. Not easily. Not by any individual alone. But the alternative is to keep swimming without noticing the water, keep breathing without noticing the air, keep walking at the angle the wind requires and calling it freedom.
The 13-year-old noticed. That is where it begins.
Book: Medicalized Motherhood: From First Pill to Permanent Patient
Available as a free download. 123 interventions documented across six phases—from pre-conception capture through postpartum surveillance. Includes practical tools: birth plan template, provider interview questions, quick reference card, and a new chapter on interrupting the cascade. Download it, share it with someone facing their first prenatal appointment, their induction date, their cesarean recommendation. The cascade works because women don’t see it coming. This book makes it visible.
Featured Video

Total War – Attacking Nuclear Plants, Desalination & Infrastructure
or go to
Aletho News Archives – Video-Images
From the Archives
Strike on Israel Shows US Bases Near Iran Are ‘Achilles Heel’
By Svetlana Ekimenko – Sputnik – 14.04.2024
Fears of a greater Middle East escalation were triggered after Iran launched a massive drone and missile attack against Israel, aided by Hezbollah and the Yemeni Houthis. Iran said the attack was in response to Israel’s bombing of the Iranian consulate in Damascus, Syria, which killed seven members of the elite Revolutionary Guard Corps.
Iran’s massive retaliatory attack on Israel from its own territory is a sign that the conflict could “escalate out of control.”
Michael Maloof, a former senior security analyst in the office of the US secretary of defense, told Sputnik that the first ever direct Iranian attack on Israel set a dangerous precedent.
“My concern is that this could easily escalate into something not only between Iran and Israel, but beyond the Middle East region,” he said.
Iran’s assault, which it stated was an act of “self-defense” after the Israeli strike on its consulate in Damascus, was originally intended to be a “limited” one, said Maloof.
Iran first sent in “swarms of drones with lights on as a sign of psychological warfare,” but sending in cruise and ballistic missiles by Tehran was a “distinct escalation,” said Maloof.
The scale of Iran’s attack on Israel suggests that Tehran was sending a message, demonstrating that it possesses “extraordinary capabilities,” said Maloof. … continue
Blog Roll
 Aletho News
Aletho News- Pakistan PM backs Iran’s right to self-defense amid tensions
- Hungary blasts ‘fake’ EU accusation
- SAFE Debt Trap: Poland’s €43.7 Billion Bet on Unipolar Illusion
- War on Iran threatens global Gulf capital flows: FT analysis
- Mossad De Facto Admits To Inciting Riots In Iran
- Tehran: World grown thoroughly exhausted with US-Israeli ‘false flag storylines’
- Trump ‘stuck between a rock and a hard place’, lacks Iran war strategy: Ex-CIA chief
- Trump’s bombardment of fake news so far is working quite well. But where is it heading?
- Iran to Mine Sea Lanes in Persian Gulf in Case of Attack – Defense Council
- Barak blasts Netanyahu: ‘Stop lying – you can’t destroy Iran’s nuclear, missile capabilities’
- If Americans Knew
- From Sde Teiman, the truth about Israel’s military justice system has been set free
- Child denied life-saving bone marrow transplant by Israel ‘because he is from Gaza’
- Raffi Berg: BBC Middle East Editor Exposed as CIA, Mossad Collaborator
- Jerusalem Archbishop Rebukes Netanyahu’s Statements on Christianity
- US to embed Palantir AI across entire military: Report
- Israeli-US war on Iran to drag on “a few more weeks” – Not a ceasefire Day 164
- Lebanon deaths top 1,200; Palantir AI to be embedded across US military – Not a ceasefire Day 163
- Israel’s assassination game: Take all pragmatists off the board
- Food shortages return to Gaza as Israel tightens aid restrictions under the cover of its war on Iran
- Trump demands trillions in payments from Gulf countries, billions from Harvard – Not a ceasefire Day 162
- No Tricks Zone
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis
- New Study Documents A 20-Year Pause In Arctic Sea Ice Decline – Driven By Internal Variability
- Wake-up Call: Survey Shows Majority Of Germans Now Favor Postponing Climate Targets!
- Televised! Leading German Political Candidate Tells Schoolchildren CO2 Makes Sun Hotter!
