NEW FAUCI EMAILS EXPOSE ATTACK ON NATURAL IMMUNITY
The HighWire with Del Bigtree | January 22, 2026
Newly revealed emails show Dr. Anthony Fauci privately acknowledged that natural immunity may provide stronger protection than COVID vaccination, even as he publicly dismissed it during the mandate period. As Senator Rand Paul calls for criminal referrals, the larger issue is whether the DOJ will pursue Fauci—or protect the COVID-era establishment instead.
American Academy of Pediatrics Hit With Federal RICO Lawsuit for Vaccine Safety Fraud
By Nicolas Hulscher, MPH | Focal Points | January 21, 2026
For decades, the American Academy of Pediatrics (AAP) has been treated like an untouchable authority on child health — the gold standard that parents, doctors, schools, and lawmakers were told to trust without question. But today, that image collapses. Children’s Health Defense (CHD) and multiple plaintiffs just filed a federal lawsuit alleging the AAP spent decades running a racketeering operation that sold parents false safety assurances about the childhood vaccine schedule.
This isn’t another “vaccine debate” lawsuit. It’s a RICO fraud case—the same legal weapon used against organized crime and the tobacco industry. The allegation is blunt and devastating: the AAP allegedly manufactured false certainty around vaccine schedule safety, shut down legitimate scientific scrutiny, and promoted sweeping assurances that were never validated through rigorous real-world safety testing—while operating within a system shaped by vaccine-manufacturer funding and financial incentives tied to high pediatric vaccination rates.
One of the most explosive points in the complaint is what it forces into the open. The cumulative childhood schedule has never been safety-tested the way any reasonable parent would assume it has. The lawsuit points to Institute of Medicine findings from 2002 and 2013 calling for more research and acknowledging the lack of proper vaccinated vs. unvaccinated comparisons. Yet the AAP continued portraying the schedule as thoroughly tested and unquestionably safe, shaping pediatric care nationwide through repetition, authority, and pressure—not proof.
The complaint also describes what parents have learned the hard way. This system doesn’t merely recommend vaccines. It demands compliance. Physicians who questioned the schedule or deviated from AAP protocols were professionally targeted, disciplined, and financially crushed. The message was clear: follow the script, or lose your career.
The lawsuit further argues that the AAP’s public reassurances were built on “theoretical” talking points that became institutional doctrine, including the infamous claim that infants could tolerate an extreme number of vaccines at once. According to the plaintiffs, this wasn’t evidence—it was marketing disguised as medical authority, repeated in clinics to silence questions and keep the assembly line moving.
Then there’s the part that makes it all make sense: money. The complaint highlights conflicts of interest and financial entanglements with vaccine manufacturers and aligned institutions. The AAP presents itself as independent and science-first, while operating in a world of corporate sponsorships, incentives, and industry relationships that would be unacceptable in any genuinely transparent public health organization.
This is why the lawsuit matters. It’s not about a single product. It challenges the entire protection racket that has propped up the pediatric vaccine industry for decades. AAP’s model has relied on one rule: the schedule is safe because we say it’s safe—and anyone who demands real proof gets smeared, censored, or destroyed.
The lawsuit seeks financial damages for the families and physicians harmed, demands disclosure of the lack of comprehensive safety testing behind the cumulative schedule, and aims to stop the AAP from making blanket, unqualified claims that the schedule is “safe and effective” as if that question has already been settled.
If this case advances, discovery alone could expose what the public has been denied for decades—and that would be a historic victory for medical transparency, informed consent, and accountability in pediatrics. For years, parents were told to “trust the experts,” while legitimate safety questions were mocked, censored, or punished. Now those questions are headed to the one place the system can’t silence them with talking points: federal court.
Summary
- CHD and multiple plaintiffs filed a federal RICO lawsuit against the AAP, accusing the organization of long-term fraud and racketeering tied to vaccine safety claims.
- The lawsuit alleges the AAP violated RICO by engaging in a sustained pattern of deceptive safety messaging about the CDC childhood vaccine schedule, while operating within a financial ecosystem tied to vaccine-manufacturer funding and incentive-driven pediatric vaccination practices.
- The lawsuit alleges the AAP repeatedly promoted false certainty that the childhood vaccine schedule is thoroughly tested and safe.
- The complaint highlights the absence of proper vaccinated vs. unvaccinated comparisons for cumulative schedule safety, referencing IOM reports calling for more research.
- Plaintiffs argue the AAP relied on theoretical reassurance (not real-world schedule safety trials) to shut down scrutiny and concerns.
- The suit includes physicians claiming they suffered professional and economic harm for deviating from AAP vaccine orthodoxy or questioning safety claims.
- It also includes families alleging severe injury or death following routine vaccination and describes how medical judgment was allegedly overridden by rigid AAP-driven standards.
- The complaint raises concerns about conflicts of interest, alleging financial ties and aligned incentives undermined the credibility of AAP’s public safety assurances.
- The lawsuit seeks financial damages, mandatory disclosure about safety-testing gaps, and to stop the AAP from making unqualified vaccine safety claims.
Epidemiologist and Foundation Administrator, McCullough Foundation
Medicalized Motherhood (2026)

Unbekoming | January 15, 2026
A healthy woman downloads a fertility app before she’s even trying to conceive. The algorithm tells her she’s “irregular,” suggests she might have a problem, builds a referral pathway to a fertility clinic directly into the interface. She arrives at pregnancy already a patient—monitored, tested, supplemented, optimized. Forty weeks later, she’s induced for passing an arbitrary due date, monitored continuously, confined to bed, augmented with synthetic hormones, numbed with an epidural, and delivered by cesarean for “failure to progress.” Her newborn is immediately clamped, separated, injected, tested, and supplemented with formula. A year later, her baby has a diagnosis for falling below the 10th percentile on a growth chart. Five years later, she’s still in the system—annual screenings, ongoing surveillance, carrying diagnoses that originated in pregnancy. She entered healthy. She never exits.
Medicalized Motherhood: From First Pill to Permanent Patient documents 123 medical interventions that operate through a single logic: each one creates conditions requiring the next. The induction requires monitoring. The monitoring requires confinement. The confinement slows labor. The slowed labor requires drugs. The drugs intensify pain. The pain requires anesthesia. The anesthesia impairs pushing. The impaired pushing requires surgery. This isn’t system failure—it’s the system functioning exactly as designed, converting healthy women into lifelong patients while generating revenue at every step. The book maps this cascade across six phases: pre-conception capture, pregnancy surveillance, labor management, immediate newborn intervention, infant pathologizing, and postpartum capture. No other single resource traces how a fertility tracking app connects to a cesarean scar connects to a “failure to thrive” diagnosis connects to permanent patient status.
The book is written for women entering this system, not researchers studying it. Every intervention is documented with evidence—Cochrane reviews, clinical studies, manufacturer warnings, professional guidelines—but translated into direct language that can be read during pregnancy, shared with partners, used in conversations with providers. The goal is informed participation, not reflexive refusal. Genuine emergencies exist; some women need cesareans; some babies need intervention. What doesn’t need to happen is the routine application of 123 interventions to healthy women and babies who would do better without them. The cascade can be interrupted. The questions that create space—What happens if we wait? What are the alternatives? Is this required or recommended?—are simple to ask and difficult for the system to dismiss.
This is my first book, and I’m proud of it. I think it offers something that didn’t exist before: the complete map, from first pill to permanent patient, written for the women who need it most. I’m offering it free to reach those women—but 226 pages is a commitment not everyone can make. So I’ve given it the Unbekoming summary treatment: comprehensive Q&A, the key arguments distilled, and a deep dive audio file available to everyone, not just paid subscribers. Consider this your entry point. If the summary resonates, the full book goes deeper into each of the 123 interventions with the evidence behind them. If a woman entering the system reads this and asks one question she wouldn’t have asked otherwise, the book did its job.
Medicalized Motherhood: From First Pill to Permanent Patient
![]()
Medicalized Motherhood Edition 1
2MB ∙ PDF file
Disruptive science (part two)

By Dr Malclom Kendrick | January 17, 2026
My son tends to dismiss the idea of watching any film from before about say, the year 1990. Terrible special effects, he informs me, and just too old. As for anything in black and white … no, just, no. Why watch old stuff, it’s rubbish. The fool.
In science there also seems to be a tendency to think that things are constantly moving forward, building on what has gone before. Old research and ideas, become obsolete, and fade from memory. There is no need to look back. We can learn little, or nothing, from things we did a hundred or more years ago.
True? Let me take you back to a land that seems far away and long, long ago. A place where the sun was used as a powerful ‘medicine’. Patients with tuberculosis (TB), or those with non-healing wounds, or mental illness, and many other things. They were wheeled into solariums to make the most of the sun’s rays. Many hospitals had great big windows to let in sunlight.
Years ago I read a fascinating book on this called ‘The healing sun’ which looked at how the sun was used to treat many illnesses. Often with impressive results. It certainly awakened my interest in the area. And, because I have an obsessive interest in heart disease, I focussed on nitric oxide (NO), which is synthesised when the skin is exposed to the sun. [This is not the only way NO is created in the body, but it is important].
Nitric oxide is a molecule that is now understood to be critical for cardiovascular health, although it was not known to have any role a hundred years ago. Until recently it was not known to exist inside the body. in fact, the idea that such a highly reactive compound could have a positive role to play was considered bonkers. Super-reactive – and damaging.
I would like to point out that sunlight does many more things than create nitric oxide and, of course, vitamin D. Mostly good. With so many potential benefits why did the era of ‘solar treatment’ fade into darkness? I think it is almost entirely due to the arrival of antibiotics. A whole bunch of terrible infections, which killed so many millions became treatable – virtually overnight. Sunlight was no longer required, or so it appeared. We had a new solution. Faster, and more effective.
And then came the slow, but inexorable, one-hundred-and-eighty-degree turn. The sun began to be viewed as dangerous. From ‘healing sun’ to ‘bringer of death’. Has this been a good move? In my opinion, absolutely not. Let me show you a graph from a long-term study done in Sweden. It looks at probability of death, in three groups.
- Those who avoid sun exposure.
- Those with moderate sun exposure.
- Those who actively sought out the sun1.
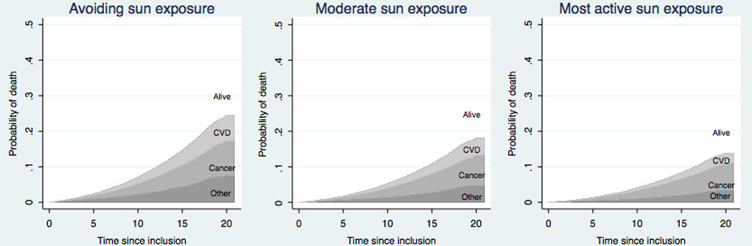
Over a twenty-year time period, those who actively sought the sun were ten per cent less likely to die – of anything, than those who avoided it. This was an absolute, not a relative risk.
On the basis of this study, sunlight would be considered a miracle drug. Everyone in the world urged to take it, every day, without fail. The pharmaceutical company with a patent for any such medicine would become rich beyond the wildest dreams of avarice. You would never hear the last of it.
I make this somewhat bold statement because there is no medication, nothing else at all, that comes close to this level of overall health benefit, and life extension. Nothing … at all. Stopping smoking would be almost as good, providing about eight to ten years of added life. But that is not really the same thing.
That paper was published ten years ago. A more recent one, from 2020, had pretty much exactly the same thing to say about sunlight. The title says it all, really:
‘Insufficient Sun Exposure Has Become a Real Public Health Problem.’
‘This article aims to alert the medical community and public health authorities to accumulating evidence on health benefits from sun exposure, which suggests that insufficient sun exposure is a significant public health problem.
Studies in the past decade indicate that insufficient sun exposure may be responsible for 340,000 deaths in the United States and 480,000 deaths in Europe per year, and an increased incidence of breast cancer, colorectal cancer, hypertension, cardiovascular disease, metabolic syndrome, multiple sclerosis, Alzheimer’s disease, autism, asthma, type 1 diabetes and myopia.’ 2
Eight hundred and twenty thousand deaths a year … seems a lot. Their figures, not mine.
My own view is that the big bright thing up in the sky … Well, it has been shining down on all life forms – all of them on land at least – for five hundred million years – give or take. And for most of our existence, humans have spent the majority of daylight hours outside. Thus, from an evolutionary perspective, it is probably not a great idea to avoid the ‘giver of life’, as I now like to call it. We may be missing out on something, or several somethings, which are rather important.
Over the years, there have been many studies demonstrating that sun exposure is really important for our health and wellbeing. But none of them had the slightest effect … on anything. Instead, we are increasingly told to cower away in terror. In Australia, land of ‘slip slap and slop’, they are now creating massive sunshades around schools, so that children who dare to go outside and play will be protected from the sun at all times. Hoorah. Good job.
My previous blog was about disruptive science. An area where there has been a drastic contraction over the last fifty years. Why? Well, one of the main reasons is that disruptive science seems to have little, to no, effect. ‘My mind is made up, do not confuse me with the facts.’ Why bother going against the mainstream view when it achieves the square root of bugger all.
The mainstream view in this area is that sun exposure causes skin cancer. Which means that any discussion on potential benefit is shut down immediately. Yes, there is some robust research to show that fair skinned people, living in hot and sunny lands, are more likely to develop skin cancer.
However, the evidence that there is an increased risk from malignant melanoma is far from clear. There are many different forms of skin ‘cancer(s)’, and most are very easily spotted and easily treatable, and removed. Whilst unpleasant, most of these are not remotely life threatening.
Australia has been banging the ‘anti-sun’ drum for decades. To great effect?
- In 1982, 596 people died of malignant melanoma.
- In 2023 1,527 people died of malignant melanoma
That represents a 2.6-fold increase. In case you were wondering.
The population of Australia went up by 1.8-fold during the same time period. Although I am informed by Google AI that ‘The age-standardised mortality rate for malignant melanoma in Australia has generally remained stable or decreased over the last twenty years.’ You think?
I think 2.6 is a bigger number than 1.8. Thirty per-cent bigger. Yes, I know you can play statistical games to create ‘age-standardized’ rates, whereby 1.8 becomes a larger number than 2.6. ‘Bibbity bobbity boo.’ Or. ‘War is peace, freedom is slavery…etc.’
Leaving such, reality distorting statistical manipulation aside, there are many other diseases that you can die of including, let me think: breast cancer, colorectal cancer, hypertension, cardiovascular disease, metabolic syndrome, multiple sclerosis, Alzheimer’s disease, autism, asthma, type 1 diabetes …etc.
If you protect against one thing, but in so doing, increase the risk of many others, you have just done significantly far more harm than good. To look at just one of the other potential forms of death that sun exposure could protect us from – colorectal cancer:
Gorham et al examined five studies on association of serum 25(OH)D (vitamin D) and colorectal cancer risk. A meta-analysis indicated a 104% higher risk associated with serum 25(OH)D <30 nmol/L compared to >82 nmol/. 3
- Malignant melanoma kills around two thousand five hundred people a year in the UK.
- Colorectal cancer kills around seventeen thousand people a year in the UK.
This ratio of around one, to eight, is pretty much the same in most other countries. So, dear reader, which of these forms of cancer should you be more interested in preventing?
Simple sum here – assuming ‘best/worst case’ scenarios in either direction:
- Malignant melanoma kills 2,500 per year. If avoiding the sun prevented this completely, we could save 2,500 lives.
- Colorectal cancer (CRC) kills 17,500 per year. If avoiding the sun increases the risk of death by 104%, we have caused 18,200 excess deaths.
Would the figures change as dramatically as this? Almost certainly not, nowhere near. My figures represent a thought experiment. However, here is what Google AI informs me about colo-rectal cancer:
‘There’s a significant and concerning rise in bowel cancer among young people in the UK, with rates in those under 50 increasing by around 50% since the mid-1990s.’ This is a trend seen around the world. As for Australia. ‘Yes, there’s a significant and concerning rise in bowel cancer among young Australians (under 50), with Australia having the world’s highest rates for this age group.’
Highest rates of CRC in the country where sun exposure is dreaded more than any other? Has anyone even suggested sun exposure, or the lack of it, may play a role? Nope, complete and utter silence on the matter. Can’t even be mentioned, it seems.
Moving on from bowel cancer, I feel the need to make the point that the most significant impact on dying, if you avoid the sun, appears to be on heart disease. This kills 175,000 people each year in the UK. Reduce that number by one and half per-cent you will have saved as many lives as can possibly die of malignant melanoma. Logic, where art though?
How can the concern about one disease trump all others so completely? Primarily, I believe, it is because dermatologists have managed to gain dominance in the world of sun exposure, with their very simple message. ‘Sunshine damages the skin and causes skin cancer, and so it must be avoided at all costs.’
Focussing on one thing to the exclusion of all else is a cognitive bias known as the focusing effect/illusion. For a dermatologist malignant melanoma is their number one issue/disease. Any suggestion that the sun may be good for us is ruthlessly stomped on. ‘Your ideas are killing people’ is the normal line of attack – believe me, I know this line of attack well.
And the public have been convinced. And the medical profession has become convinced – as has almost everyone in the entire world. Try telling the average person that sun exposure is extremely good for you, and they look at you as if you were mad, bad, and dangerous to know.
I don’t find this type of concrete, straight line, focussed thinking, strange anymore. Over the years I have stumbled across many areas of medicine where bad ideas have taken hold, and simply cannot be shifted. Indeed, they only seem to strengthen under attack.
I have been banging on about saturated fat for decades. The evidence that saturated fat is bad for you has always been weak, to non-existent, to totally contradictory. Yet, and yet, the idea continues to hold sway over most of the population. With little sign that it is losing its grip. One day, perhaps, I can dream.
Salt … if there is any good evidence on this, it suggests that salt is good for you. But the idea that salt is harmful is also immovable, and unchanging. Evidence that it reduces life expectancy, there is none. And I mean … none.
So, what does it take to change thinking. If I knew how to sweep aside wrong ideas, I would have managed it by now. Disruptive science? Disruptive evidence? It is actually out there, but no-one pays much attention to it. In general, it is first mocked, then attacked, then dismissed.
Somehow, somehow, we have to think in different ways. I was going to say better ways, but that sounds a little on the elitest side. ‘I think better than you.’ When it comes to sunshine, it really isn’t difficult to change the thinking, is it?
I cannot find any evidence, anywhere, that it is anything other than extremely good for us. Ergo, hiding away from the sun is bad for us. One of the worst things we can possibly do, and it is also one of the easiest, and most pleasurable things, to rectify. Go out and sunbathe. [Yes, of course, I have to add, but do not burn. As if everyone in the world is a complete idiot that cannot understand even the simplest idea.]
But, but, but … instead, we have all been – made to be – terrified of skin cancer. A condition which kills very few people each year. It seems impossible to move the thinking beyond this barrier … bonkers. And very harmful indeed.
In my next blog on disruptive science, I will look again at sunshine, from a different perspective, including the question. Does it actually increase the risk of malignant melanoma?
1: https://pubmed.ncbi.nlm.nih.gov/26992108/
2: https://www.mdpi.com/1660-4601/17/14/5014 3: https://www.sciencedirect.com/science/article/abs/pii/S0749379706004983
Congratulations On Your Diagnosis
A welcome letter

By Dr. Roger McFillin | Radically Genuine | January 12, 2026
Dear Valued Patient,
Welcome.
We’re so pleased you found us. Or rather, that we found you, though you may not remember exactly how it happened. Perhaps you mentioned sadness that lasted more than two weeks. Perhaps you admitted to worry. Perhaps a teacher noticed your child had too much energy, or not enough, or the wrong kind at the wrong time. No matter. You’re here now. That’s what counts.
First, let us assure you: this is not your fault. You have a condition. A real, medical condition, confirmed by a checklist, validated by a billing code, and now officially part of your permanent record. You’re not weak. You’re not broken. You’re sick. Doesn’t that feel better already?
We know you may have once believed that your suffering had meaning. That grief was love’s receipt. That anxiety was wisdom trying to speak. That your child’s wildness was life itself looking for room to move. We’ve heard all of this before. We’ve noted it in your file. It falls under “Resistance to Treatment” and “Poor Insight,” both of which, interestingly, are also symptoms. But here’s what science has discovered: feelings that persist are symptoms. Experiences that disrupt are disorders. And the body’s ancient signaling system, the one that kept your ancestors alive long enough to produce you? A chemical error. Fortunately, we now have chemicals to fix the chemicals. You’re welcome.
What You’ve Gained
As a member of our industry, you now have access to:
- A name for what’s wrong with you (selected from our current catalog)
- Medications clinically proven to reduce the intensity of being alive
- A support team who will monitor your progress toward feeling less
- Periodic check-ins to adjust dosage based on how much of yourself remains
You may notice some changes. Colors may seem less vivid. Music may stop reaching you the way it once did. Orgasms may become a memory you’re not sure you’re remembering correctly. These are signs the treatment is working. Please do not confuse returning aliveness for wellness. That feeling you had before, the one that brought you here, that was the disease.
Frequently Asked Questions
How long will I need treatment? Most patients require lifelong management. Think of it like insulin, except for your soul.
What if I feel worse? This is common. It means we haven’t found the right combination yet. Stay the course. There are many options. We can always add more.
What if I want to stop? We’d ask you to examine that impulse carefully. The desire to feel your feelings again is often a sign of relapse. Your brain has been corrected. Going back now would be like choosing disease.
Can I ever be cured? We don’t use that word. But with compliance, you can achieve something even better: symptom management with minimal breakthrough emotion.
Share Your Journey
Now that you have a diagnosis, it’s time to tell the world.
Post it. Pin it to your bio. Add it to your Instagram highlights. Change your Twitter handle. You are no longer just a person with a name. You are a person with a condition, and conditions deserve visibility.
Use the hashtags. Join the communities. Find your tribe. You’ll discover thousands of others just like you, sharing their medication selfies, their symptom lists, their before-and-after stories. You will be seen. You will be validated. Strangers will leave heart emojis beneath your pain. Isn’t that what healing looks like?
Don’t be shy. Vulnerability is currency now. The more you share, the more you belong. And if anyone questions your diagnosis, remember: that’s stigma. Block them. They are part of the problem.
Your disorder is your story. Your story is your brand. Your brand is your identity. And your identity, as we’ve discussed, is permanent.
So go ahead. Tell everyone. We’ll be here when you get back.
A Note on Gratitude
You’re lucky, you know. In another era, you might have been told to sit with it. To feel your way through. To let grief crack you open. To treat your anxiety as a messenger rather than a malfunction. You might have been surrounded by people instead of professionals. You might have been asked what happened to you rather than what’s wrong with you.
But you live now. And we have built an entire world to catch you. Billboards. Commercials. Sponsored content. Quizzes that always confirm what you already suspected. Doctors with ten minutes and a prescription pad. Pharmacies on every corner. A pipeline so smooth you’ll barely notice you’re inside it.
We’ve made it so easy. Your insurance covers it. Your employer encourages it. Your friends will understand. And someday, when you’re sitting in a room, feeling very little, wondering if something got lost along the way, you can comfort yourself with this: at least you weren’t difficult.
Welcome to the industry.
We’re so glad you’re ours.
Warmly,
The Psychiatric Industry
P.S. If this letter has stirred any strong feelings, please contact your provider immediately.
Lessons Learned from Thirty Years CT Heart Scans and Coronary Calcium Scores: The Role of Vitamin D
William Davis , MD | January 8, 2026
My 30+ years of involvement with CT heart scans and coronary calcium scores has yielded many important lessons on how to halt, then reverse, the accumulation of coronary atherosclerotic plaque and thereby risk for heart attack, need for heart procedures, and sudden cardiac death.
Here, I discuss the crucial importance of vitamin D and how, by addressing this issue, it was the first time I saw actual reductions in coronary calcium scores.
*Disclaimer:* The information presented in my books, blog posts, YouTube videos, podcasts, and other content is for informational and educational purposes only. The content I share should not be interpreted as medical advice, diagnosis, or treatment. Always consult with your personal physician or qualified healthcare professional before making any changes to your diet, medication, lifestyle, or healthcare regimen. Your individual health needs should be evaluated by a professional who is familiar with your unique medical history.
My new book is Super Body: A 3-Week Program to Harness the New Science of Body Composition and Restore Your Youthful Contours Available on Amazon and other bookstores: https://www.amazon.com/SUPER-Body-Com…
If you are new to my microbiome discussions, see my Super Gut book that includes recipes for L. reuteri and SIBO Yogurts: https://www.amazon.com/Super-Gut-Four…
Also see my Revised & Expanded Wheat Belly book that contains the entire Wheat Belly program, all updated with new information, more recipes, more success stories. Available on Amazon and other bookstores: https://www.amazon.com/Wheat-Belly-Re…
span class=”yt-core-attributed-string yt-core-attributed-string–white-space-pre-wrap” dir=”auto”>About Dr. Davis:
Dr. Davis practiced conventional cardiology for 25 years but became discouraged with the predatory and exploitative practices of modern healthcare. He now devotes his efforts to helping people regain magnificent health without doctors or hospitals with results that are SUPERIOR to that obtained through conventional healthcare. His Wheat Belly books have sold 4 million copies in 40 countries.
We draw from the health information of the world, collaborate, share experiences, collect data, and show how to apply new health tools to achieve levels of health that you may have thought unattainable. We do all this at a time when conventional healthcare costs have become crippling.
In addition to the Wheat Belly, Undoctored, and Super Gut books, find more of Dr. Davis’ conversations at: Dr. Davis Infinite Health http://www.DrDavisInfiniteHealth.com
The 15 Most Devastating Truths About the PSA Screening Disaster
Lies are Unbekoming | October 26, 2025
The prostate-specific antigen (PSA) test has screened 30 million American men annually for over three decades. The man who discovered PSA in 1970, Richard Ablin, now calls mass screening “a public health disaster.” Two landmark 2012 studies found no survival benefit from radical surgery compared to watchful waiting. The U.S. Preventive Services Task Force concluded PSA screening does more harm than good. Yet the $3 billion annual industry continues largely unabated.
These revelations emerge from three insider accounts: Ablin’s The Great Prostate Hoax, urologist Anthony Horan’s The Rise and Fall of the Prostate Cancer Scam, and oncologist Mark Scholz’s Invasion of the Prostate Snatchers. Together they document how a test meant to monitor existing cancer patients became a screening juggernaut that has left millions of men incontinent, impotent, or dead from unnecessary treatment.
The numbers are staggering. Since 1987, when PSA screening exploded nationwide, over one million American men have undergone radical prostatectomies. Studies show 40 to 50 men must be diagnosed and treated to prevent one death from prostate cancer. The other 39 to 49 men receive no benefit but face permanent side effects. Medicare and the Veterans Administration fund most of this treatment, pouring billions into a system that prominent urologists privately acknowledge has failed.
What follows are the most damaging truths about how PSA screening became entrenched despite overwhelming evidence of harm, why it persists against scientific consensus, and what this reveals about American medicine’s inability to abandon lucrative practices even when they damage patients.
1. The Test’s Creator Calls It a “Public Health Disaster”
Richard Ablin discovered prostate-specific antigen in 1970 while researching cryosurgery’s effects on prostate tissue. He never intended PSA as a screening test for healthy men. The test cannot distinguish between the cancers that kill and those that remain harmless. Ablin has spent decades publicly denouncing mass screening, including a 2010 New York Times op-ed titled “The Great Prostate Mistake.”
Ablin compares PSA screening’s specificity to “a coin toss” – hardly the precision expected from a medical test that determines whether men undergo surgery or radiation. He testified before Congress, published papers, and gave countless lectures warning against screening’s misuse. The medical establishment ignored him. In his book, he writes that watching his discovery become “a hugely expensive public health disaster” has been “painful.” The man who found PSA receives angry emails from men whose lives were destroyed by unnecessary treatment triggered by elevated PSA levels.
2. 75% of Men with Elevated PSA Don’t Have Cancer
A PSA level above 4.0 triggers the treatment cascade, yet three-quarters of these men have no cancer. Infections, enlarged prostates, bicycle riding, and recent ejaculation all elevate PSA. The test measures inflammation as readily as malignancy. This 75% false positive rate means millions undergo invasive biopsies needlessly.
The Prostate Cancer Prevention Trial found that 15% of men with PSA under 4.0 – the “normal” range – actually had prostate cancer, including aggressive forms. Meanwhile, only 25% with elevated PSA had cancer at all. No blood test with such poor specificity would gain approval today. Yet once PSA became standard practice, removing it from clinical use proved impossible despite its fundamental unreliability.
3. The $3 Billion Annual PSA Gold Rush
PSA screening generates at least $3 billion annually, with Medicare and the Veterans Administration covering most costs. Each abnormal PSA triggers a cascade: repeat tests, biopsies, imaging, surgery or radiation, plus years of follow-up. A single radical prostatectomy bills $15,000 to $30,000. Radiation therapy can exceed $50,000. These procedures require expensive equipment, specialized facilities, and teams of providers.
Hospital systems depend on this revenue stream. Urology practices built business models around screening and treatment. Medical device companies profit from surgical robots, radiation equipment, and biopsy tools. This economic ecosystem resists evidence showing most treatment is unnecessary. When the U.S. Preventive Services Task Force recommended against routine screening in 2012, medical associations mobilized massive lobbying efforts to preserve the status quo. Money, not medicine, drives the screening machine.
4. 30 Million Tests, 1 Million Unnecessary Biopsies Per Year
Annual PSA screening of 30 million American men triggers approximately one million prostate biopsies. Since most elevated PSAs are false positives, at least 750,000 of these biopsies find no cancer. Each biopsy involves 12 to 18 needle cores punched through the rectal wall into the prostate. Serious infections requiring hospitalization occur in 1-4% of cases. Sepsis can be fatal.
Even negative biopsies don’t end the cascade. Urologists often recommend repeat biopsies for persistently elevated PSA, subjecting men to multiple rounds of needles, infection risk, and anxiety. Some undergo four, five, even six biopsies chasing ghost cancers that either don’t exist or would never threaten their lives. The psychological toll – months of fear between tests, the dread of results, the pressure to “do something” – devastates men and families. This suffering serves no medical purpose for the vast majority subjected to it.
5. The “Arbitrary” 4.0 Cutoff That Changed Everything
The PSA threshold of 4.0 ng/mL that triggers intervention was, according to New York Times reporting, chosen “just sort of arbitrarily.” William Catalona’s influential 1991 New England Journal of Medicine article established this cutoff without reporting false positive rates – a basic requirement for screening tests. The entire world adopted this number uncritically.
No scientific process determined that 4.0 represented a meaningful boundary between health and disease. The number could have been 3.0 or 5.0 or 6.5. Each choice would have swept millions more or fewer men into the treatment vortex. This arbitrary threshold, selected without rigorous validation, has determined the fate of millions. Men with 4.1 undergo biopsies while those with 3.9 are deemed safe, though this 0.2 difference has no biological significance. A random number became medical dogma, and challenging it meant confronting an entire industry built on its foundation.
6. 2,600 Post-Surgery Deaths at the 1992 Peak
Radical prostatectomy deaths peaked at 2,600 in 1992, five years after PSA screening exploded nationally. These men died from surgical complications – bleeding, infections, blood clots, anesthesia reactions. They underwent surgery for cancers that, in most cases, would never have threatened their lives. The operation killed them before their cancer could.
Anthony Horan documents how radical surgery was “revived without new evidence” in the 1980s after being largely abandoned. The combination of PSA screening and renewed surgical enthusiasm created a perfect storm. Thousands died on operating tables for a disease that grows so slowly most men die with it, not from it. These deaths represent only immediate surgical mortality – not the men who died months later from complications, or whose lives were shortened by surgical trauma. Each death was preventable had screening not detected their harmless cancers.
7. Radical Surgery Shows No Survival Benefit Over Watchful Waiting
Two randomized controlled trials reported in 2012 found no difference in cancer-specific mortality between radical surgery and watchful waiting. The Prostate Cancer Intervention Versus Observation Trial (PIVOT) followed 731 men for up to 15 years. The Scandinavian trial tracked men for over 20 years. Both reached the same conclusion: surgery doesn’t save lives compared to monitoring.
These studies destroyed the rationale for early detection. If removing the entire prostate doesn’t extend life compared to doing nothing, then finding cancer early serves no purpose except to subject men to treatment side effects. The medical establishment largely ignored these findings. Surgery rates declined modestly but remained far higher than evidence justified. Mark Scholz writes that these studies should have “removed the rationale for early diagnosis with PSA” entirely. Instead, the industry adapted its messaging while continuing essentially unchanged.
8. The FDA Approval Based on 3.8% Detection Rate
The FDA approved PSA for screening in 1994 based primarily on a study showing it could detect 3.8% more cancers than digital rectal examination. This marginal improvement became justification for testing millions annually. The agency relied heavily on this single statistic while downplaying false positive rates and overdiagnosis risks.
Alexander Baumgarten, one of FDA’s own expert advisers, warned officials: “Like Pontius Pilate, you cannot wash the guilt off your hands.” Susan Alpert, who directed FDA’s Office of Device Evaluation during approval, later acknowledged the decision’s problems. The agency never required studies showing screening actually saved lives or improved quality of life. This regulatory failure, approving a test based on detection rates rather than patient outcomes, enabled the disaster that followed. The FDA has never revisited its decision despite overwhelming evidence of harm.
9. Prostate Cancer Grows So Slowly Most Men Die WITH It, Not FROM It
Autopsy studies reveal that 30% of men in their 40s and 70% in their 70s have prostate cancer cells. Most never knew and were never affected. The cancer’s typical growth rate means decades pass between initial cellular changes and potential lethality. A 65-year-old diagnosed with early-stage prostate cancer has less than 3% chance of dying from it within 15 years if left untreated.
Men diagnosed at 75 almost certainly will die of something else first – heart disease, stroke, other cancers. Yet screening doesn’t discriminate by age or life expectancy. Elderly men in nursing homes receive PSA tests and undergo biopsies. Some receive radiation or surgery in their 80s for cancers that could never outlive them. This fundamental biological reality – that most prostate cancers are clinically insignificant – undermines screening’s entire premise. Finding these cancers serves only to transform healthy men into cancer patients unnecessarily.
10. The Biopsy Train: 18-Gauge Needles and Serious Infections
Modern prostate biopsy involves 12 to 18 hollow-bore needles, each 18-gauge in diameter, fired through the rectal wall. The needles extract tissue cores while potentially spreading bacteria from the bowel into the prostate and bloodstream. Fluoroquinolone-resistant bacteria have made infections increasingly dangerous. Some men develop sepsis requiring intensive care.
Richard Ablin receives emails from men describing their biopsy experiences as “spinning out of control,” having “panic attacks,” and living in a “nightmare.” The procedure’s violence – needles punching through tissue, the sound of the spring-loaded gun, blood in urine and semen for weeks – traumatizes men regardless of results. Those with negative biopsies face pressure to repeat the procedure if PSA remains elevated. Some endure annual biopsies for years, each carrying infection risk, each failing to find cancer that likely isn’t there or doesn’t matter. The biopsy itself becomes a recurring assault that serves no medical purpose.
11. Incontinence and Impotence: The “Acceptable” Side Effects
Radical prostatectomy leaves 20-30% of men with permanent urinary incontinence requiring pads or diapers. Erectile dysfunction affects 60-80%, depending on age and surgical technique. These rates come from centers of excellence; community hospitals report worse outcomes. Surgeons routinely minimize these risks, calling them “acceptable” trade-offs for cancer treatment.
For men whose cancers would never have threatened them – the majority who undergo surgery – these side effects represent pure harm. They lose sexual function and bladder control to treat a disease that required no treatment. Their marriages suffer. Depression is common. Some become recluses, afraid to leave home without knowing bathroom locations. The medical profession’s casual acceptance of these devastating outcomes reflects a stunning disregard for quality of life. No other medical specialty would tolerate routinely destroying normal function to treat non-threatening conditions.
12. PSA Isn’t Even Prostate-Specific
Despite its name, prostate-specific antigen isn’t specific to the prostate. Breast tissue produces PSA – it’s a normal component of breast milk. Salivary glands make it. Some lymphomas produce PSA. Women have measurable PSA levels. This basic biological fact undermines the test’s fundamental premise.
Anthony Horan notes he personally reported PSA production in B-cell lymphomas. The protein’s presence throughout the body means elevated levels can reflect numerous non-prostatic processes. Yet the medical establishment treats PSA as if it were a precise prostate cancer marker. This scientific sloppiness – naming and using a test based on false assumptions about specificity – exemplifies the intellectual bankruptcy underlying mass screening. If PSA were discovered today with current knowledge, it would never be approved for screening healthy men.
13. The Veterans Administration’s Role in the Screening Epidemic
The Veterans Administration extensively promoted and funded PSA screening, making it routine for millions of veterans. The VA’s electronic medical records prompted doctors to order PSA tests, created quality metrics based on screening rates, and facilitated the treatment cascade. Veterans, trusting their government healthcare, underwent screening at higher rates than the general population.
The VA spent billions on screening, biopsies, and treatment. Veterans suffered disproportionately from overdiagnosis and overtreatment. Many underwent surgery or radiation at VA hospitals with limited experience in these procedures, likely experiencing higher complication rates. The government that sent these men to war later subjected them to medical harm through systematic overscreening. Only after the 2012 USPSTF recommendation did the VA begin moderating its approach, too late for hundreds of thousands of veterans already harmed.
14. Why Urologists Can’t Stop Screening Despite the Evidence
Urologists understand the evidence against screening yet continue promoting it. Professional self-interest explains this cognitive dissonance. Prostate cancer diagnosis and treatment represent major revenue sources for urology practices. Academic urologists depend on prostate cancer research grants. Professional status derives from surgical volume and technical expertise in procedures that shouldn’t be performed.
Mark Scholz describes the “surgeon personality” that sees every problem as requiring surgical solution. Urologists train for years to perform radical prostatectomies. Abandoning these procedures means acknowledging that much of their training and practice caused unnecessary harm. The psychological and economic barriers to accepting screening’s failure prove insurmountable. Even urologists who privately acknowledge the problem continue participating in the system. Professional conferences feature token debates about screening while exhibit halls showcase million-dollar surgical robots. The specialty cannot reform itself when its economic survival depends on perpetuating harm.
15. Active Surveillance Works for 99% of Low-Risk Cases
Multiple studies demonstrate that active surveillance – monitoring without immediate treatment – works for virtually all low-risk prostate cancers. Memorial Sloan Kettering reported that fewer than 1% of men on surveillance die from prostate cancer over 15 years. Johns Hopkins found similar results. These men avoid treatment side effects while maintaining the option to treat if their cancer progresses.
Despite this evidence, most men with low-risk disease still receive immediate treatment. Doctors present surveillance as “doing nothing” rather than an active management strategy. Patients fear leaving cancer untreated, not understanding their cancer’s indolent nature. The medical system’s financial incentives favor treatment over monitoring. Each patient choosing surveillance represents lost revenue. This proven alternative that could spare hundreds of thousands from unnecessary treatment remains underutilized because it threatens the economic foundation of prostate cancer care.
Conclusion
The PSA screening disaster exposes American medicine’s darkest impulses: the primacy of profit over patient welfare, the persistence of harmful practices despite overwhelming evidence, and the medical establishment’s inability to acknowledge error. Thirty years of mass screening has transformed millions of healthy men into cancer patients unnecessarily, subjecting them to treatments that left many incontinent, impotent, or dead.
The men who exposed this scandal from within – Richard Ablin who discovered PSA, Anthony Horan who practiced urology during screening’s rise, Mark Scholz who treats screening’s victims – deserve recognition for their courage in challenging their profession’s orthodoxy. Their accounts reveal not isolated mistakes but systematic failure: arbitrary thresholds adopted without validation, regulatory approval based on minimal evidence, and an entire medical specialty economically dependent on perpetuating harm. Until American medicine can abandon lucrative practices that damage patients, the PSA disaster will repeat in other forms, with other tests, harming other victims who trusted their doctors to first do no harm.
References
Ablin, Richard J., with Ronald Piana. The Great Prostate Hoax: How Big Medicine Hijacked the PSA Test and Caused a Public Health Disaster. New York: Palgrave Macmillan, 2014.
Horan, Anthony H. The Rise and Fall of the Prostate Cancer Scam. 3rd ed. Broomfield, CO: On the Write Path Publishing, 2019.
Scholz, Mark, and Ralph H. Blum. Invasion of the Prostate Snatchers: An Essential Guide to Managing Prostate Cancer for Patients and Their Families. Revised ed. New York: Other Press, 2021.
FLU FEAR VS. FLU FACTS
The HighWire with Del Bigtree | January 8, 2026
Alarmist media coverage and public health messaging have branded this season’s flu a so-called “super flu,” but surveillance data from both the U.K. and the U.S. tell a more measured story. While reports of influenza-like illness (ILI) have risen—as they typically do during winter—rates of laboratory-confirmed influenza remain within normal seasonal levels. The distinction is often blurred in headlines, with ILI frequently conflated with confirmed flu infections. Even public health officials acknowledge these limitations, along with the well-documented constraints of flu vaccine effectiveness, raising questions about whether the current narrative reflects the data.
Offshore wind turbines steal each other’s wind: yields greatly overestimated
By Bert Weteringe – clintel – December 30, 2025
The energy yields of offshore wind turbines are overestimated by up to 50% in national policy documents. This conclusion is based on an analysis of operational data from 72 wind farms.
In order to meet the net-zero targets set out in the European Green Deal, offshore wind turbines will have to make a significant contribution to Europe’s future energy supply – at least, that is the plan of European governments. However, these plans are facing setbacks due to high investment costs and uncertainty about returns, as demand is lower than expected. On October 30, outgoing Minister Hermans of the Dutch Ministry of Climate & Green Growth (KGG) announced in a letter to the House of Representatives that no applications for a permit had been received for the tender for the Nederwiek I-A wind farm, which has an installed capacity of 1–1.15 gigawatts. This is a trend that is not limited to the Netherlands. In August, for example, there were no bids for the ten gigawatts of tenders that the German government had put out for offshore wind projects. On top of that, there is now another setback: the energy yields of offshore wind turbines appear to be much lower than assumed in most national policy plans.
“National policy targets show expectations of energy production up to 50% higher than can realistically be achieved”, concludes Carlos Simao Ferreira, professor of Wind Energy Science at Delft University of Technology. He published, together with Danish colleagues Gunner Chr. Larsen and Jens Nørkær Sørensen from the Technical University of Denmark (DTU), an article in the latest journal Cell Reports Sustainability, on November 21. “This study establishes a physically grounded upper limit on wind farm performance, demonstrating that aerodynamic constraints impose a fundamental ceiling on the energy extractable from the marine Atmospheric Boundary Layer”, the scientists continue.
According to the article, the ever-growing wind farms, which are also becoming increasingly denser, extract energy from the lower part of the atmospheric boundary layer, affecting this boundary layer up to several kilometres above the Earth’s surface. The energy extracted from the airflow must be replenished from the higher layers of the atmosphere, but this is only possible to a limited extent due to atmospheric limitations determined by physical principles known from meteorology and geophysics. This means that wind turbines literally steal each other’s wind, which means that the efficiency of wind turbines will decrease even further as their number increases. The scientists demonstrate this with a validated analytical model that defines the physical upper limit of offshore wind farm production.
They built their model based on the actual yields of 72 large wind farms in the United States, the United Kingdom, Germany, France, Belgium and the Netherlands, and compared the actual yields of the wind farms with the theoretically expected yields set out in national policy documents in a number of case studies. In seven of the nine case studies, the national policy targets for offshore wind yields turned out to be way overestimated. Two German wind farms were slightly underestimated.
The limitations of offshore wind revealed in the publication are not new. Scientists from the Danish university and the German Max Planck Institute have previously warned that the expected yields from offshore wind energy could fall by a third or more if offshore wind is scaled up further. In a 2020 publication by the German organization Agora Energiewende, an interdisciplinary and international team that develops scientifically sound and politically feasible strategies for the transformation towards climate neutrality, they showed how the efficiency of wind turbines decreases as the use of wind energy increases in scale. In addition, Axel Kleidon, physicist and group leader at the Max Planck Institute, states in a 2021 publication in the ‘Meteorologische Zeitschrift’ that the energy yields of areas with wind turbines covering more than 100 square kilometres, are up to twelve times lower than those of small wind farms in prominent locations, regardless of the technological advances made in wind turbines. The Cell Reports publication now confirms these earlier findings with hard figures.
The Netherlands stands out most conspicuously: with an overestimation of revenues of 49%, the scientists have labelled the Dutch government’s policy as “internally inconsistent”. The North Sea Wind Energy Infrastructure Plan (WIN), published by the Dutch government in July, assumes a capacity factor of 51 to 56 percent—this is the ratio between the actual electricity production of a wind turbine and the maximum possible yield in the same period. This is despite figures from Statistics Netherlands (CBS) showing that the capacity factor of wind turbines in the Dutch part of the North Sea was 37% and 38% in 2023 and 2024, respectively. The Delft publication cites this as a striking example of how “changing targets, spatial planning, and assumed performance can become misaligned with physical constraints.”
“Such overestimation not only hides true energy costs but also underestimates power variability, integration, and curtailment risks, and it distorts policy pathways”, the scientists argue. They further note that the resulting shortfall in electricity revenues “could have a profound impact on society and the economy.” The effectiveness of large-scale investments in the flexibility of the power grid and in wind energy storage—such as batteries and hydrogen production—depends to a large extent on the actual capacity factor of offshore wind turbines. According to the scientists, the underutilization of these investments in the future will have an impact on several generations. “The heavy demands on society, the economy, and the environment mean that corrective paths may become costly or unfeasible for a country or region”, they state.
Simão Ferreira et al., A theoretical upper limit for offshore wind energy extraction, Cell Reports Sustainability (2025), https://doi.org/10.1016/j.crsus.2025.100573
 Bert Weteringe is a Dutch aeronautical engineer and the author of the book Downwind (2023), in which he informs readers about the devastating effects of the climate agenda on society and nature, specifically the impact of large-scale energy generation using wind turbines. As an independent investigative journalist, his focus is primarily on the energy transition. Through his website, he publishes news about the energy transition and wind turbines in particular.
Bert Weteringe is a Dutch aeronautical engineer and the author of the book Downwind (2023), in which he informs readers about the devastating effects of the climate agenda on society and nature, specifically the impact of large-scale energy generation using wind turbines. As an independent investigative journalist, his focus is primarily on the energy transition. Through his website, he publishes news about the energy transition and wind turbines in particular.
Is the Psychiatric Drugging of Children a Form of Child Abuse?
A case that becomes harder to dismiss the longer you look
By Dr. Roger McFillin | Radically Genuine | December 18, 2025
Let me be direct about something before we go any further.
We call them psychiatric “medications.” We say children are being “medicated” for their “conditions.” This language is a lie.
These are drugs. Chemical compounds made in a factory. They do not correct any known abnormality. They do not heal anything. They are not medicinal in any meaningful sense of the word. They are chemicals that alter brain function that numb, restrict, and sedate.
We need to stop hiding behind medical language that implies these interventions are “therapeutic” and healing. They are not. They are chemical management of behavior with the potential for severe health consequences. Once we are honest about what we are actually doing to children, the ethical questions become unavoidable.
The Question We Must Answer
I have spent fifteen years in private practice as a clinical psychologist. Before that, I worked in psychiatric hospitals, community mental health, public schools and the juvenile justice system. I have watched what we do to young people in the name of treatment, and it’s a moral and ethical failure.
Federal law defines child abuse as “any act or failure to act on the part of a parent or caretaker which results in death, serious physical or emotional harm” or “an act or failure to act which presents an imminent risk of serious harm.”
The question I want to pose is straightforward: Does the prescription of mind-altering and mood-altering drugs, which carry significant potential for harm and frequently cause it, meet this legal definition?
I believe it does. Here is why.
Rationale #1: No Identifiable or Measurable Biological Foundation for Mental Disorders Exists
If we could identify a biological abnormality that a drug effectively corrects, we would have reasonable justification for the risks involved. We could measure responses empirically and adjust treatment accordingly.
But no such abnormality has been identified. Not for ADHD. Not for depression. Not for anxiety. Not for any psychiatric diagnosis given to children.
Psychiatric diagnoses fail the most basic standards of scientific measurement. They lack both reliability and validity.
Reliability means consistency. If a diagnostic system is reliable, different clinicians evaluating the same child should arrive at the same diagnosis. This does not happen in psychiatry. Studies repeatedly demonstrate that clinicians disagree at alarming rates. One psychiatrist sees ADHD. Another sees anxiety. A third sees oppositional defiant disorder. The same child, the same behaviors, wildly different labels depending on who is in the room. Field trials for the DSM-5 found that many diagnoses failed to reach acceptable reliability thresholds. The system cannot even produce consistent results.
Validity means the diagnosis corresponds to something real and distinct in the world. A valid diagnosis identifies a specific condition with a known cause, predictable course, and targeted treatment. Psychiatric diagnoses meet none of these criteria. There are no biomarkers. No lab tests. No imaging findings. No way to confirm or disconfirm the diagnosis through objective measurement. These categories were created by committees of psychiatrists voting on clusters of behaviors. They are descriptive labels masquerading as medical diagnoses.
The honest history is this: the Diagnostic and Statistical Manual was developed primarily to facilitate insurance billing within the broader healthcare system. It provided codes so that psychiatrists could be reimbursed like other physicians. The appearance of medical legitimacy was the point. Scientific validity was never established because it was never the priority.
The chemical imbalance theory has been formally abandoned. The former director of the National Institute of Mental Health publicly stated that psychiatric diagnoses lack scientific validity. Yet physicians continue telling parents their children have brain disorders based on no objective test whatsoever.
Consider the psychological impact on a child who begins to identify with a psychiatric label. They internalize the message that something is fundamentally wrong with how they think and feel. They believe they are different from other children. They conclude they need drugs to be normal.
Is this not a form of emotional harm?
Any genuine medical disease underlying psychiatric symptoms would be reclassified as a medical condition. If obsessive-compulsive symptoms stem from a streptococcal infection, we treat the infection with antibiotics. If attention problems result from nutritional deficiencies, we address the deficiencies through diet and supplementation.
When we affix psychiatric labels to children without objective confirmation, we drug them with chemicals that cause significant adverse effects and health concerns.
Rationale #2: No Psychiatric Drug Has Been Proven to Objectively Improve the Assigned Mental Disorder
I have spent fifteen years studying psychiatric drug trials, the FDA approval process, and the mechanisms through which these chemicals reach the market. What I have learned disturbs me deeply.
These trials typically last six to twelve weeks. Researchers measure effectiveness through symptom checklists, quantifying whether reported symptoms decrease. The critical problem is that many of these drugs primarily induce emotional numbing or sedation. A person who feels disconnected from their emotions will report fewer symptoms on a checklist. This is not the same as improvement.
The objective is to create enough of a drug effect to generate a statistical difference compared to placebo. That statistical variance should not be mistaken for evidence that a drug treats depression or stabilizes mood. By the same logic, alcohol could be considered an approved treatment for social anxiety.
Pharmaceutical companies have encountered significant challenges demonstrating that antidepressants and other psychiatric drugs outperform placebos in meaningful ways. The illusion that we possess effective pharmacological treatments for childhood emotional and behavioral challenges must be dispelled.
If we are honest about what happens in clinical practice, the primary approach involves attempting to induce emotional numbness and detachment in developing children. This truth is rarely communicated to families.
I hear the same descriptions from young people in my practice over and over. “I feel like a zombie.” “I feel nothing.” “I cannot cry anymore.” “I do not feel like myself.”
This is not treatment. This is chemical suppression of the full range of human emotion in a developing brain. And we call it medicine.
Rationale #3: Psychiatric Drugs Are Proven to Create Harm
Every psychiatric drug approved for children carries a substantial list of side effects. Many are severe. Some are potentially fatal.
Do you want to know the long term effects? Well so do I! However, if you fail to study the long term problems of a drug you do not have to report on it.
Selective Serotonin Reuptake Inhibitors, the most commonly prescribed class of drugs for childhood anxiety and mood disorders, carry a black box warning. This represents the most stringent cautionary label the FDA can issue. The purpose of black box warnings is to alert the public and healthcare providers to grave side effects, including risks of injury or death.
The FDA requires black box warnings when compelling evidence indicates a drug can trigger severe adverse reactions, when benefits do not outweigh risks, when the drug requires restricted usage to protect public safety, or when the drug poses heightened dangers to specific populations, including children.
The black box warning on SSRIs states that these drugs increase suicidality in children and adolescents.
I need you to fully absorb that statement. The drugs most commonly prescribed to treat depression in young people can increase their desire to end their own lives.
I have witnessed this pattern repeatedly in clinical practice. A teenager who was struggling but stable starts an antidepressant. Within weeks, they are engaging in self-harm. They are making suicide plans. They are hospitalized.
In the hospital, the response is often to adjust the drug or add another. The adverse reaction becomes evidence of how sick they truly were.
Within clinical settings, physicians frequently combine drugs in ways that have never been adequately studied. Polypharmacy in pediatric psychiatry is common practice, not the exception. The combinations given to children have often never been evaluated even in adult populations.
This is experimentation. It is conducted on those least able to advocate for themselves.
Rationale #4: Psychiatric Drug Reactions Are Misinterpreted as Mental Disorders, Leading to More Diagnoses and More Drugs
This is perhaps the most insidious aspect of the current system. It creates a self-perpetuating cycle that transforms episodic struggles into chronic disability.
The pattern begins when a physician attributes emotional or behavioral challenges to a simplistic chemical imbalance. Drugs are prescribed that alter brain chemistry and can create genuine neurological changes. When the child displays adverse reactions, these responses are interpreted as manifestations of mental illness.
The misinterpretation becomes justification for additional drugs, additional diagnoses, and further deterioration.
A child enters the system because her parents are divorcing and she is sad. Understandable. Her world has been disrupted. She is prescribed an antidepressant. It makes her agitated and unable to sleep. A second drug is added for the agitation. That causes weight gain and lethargy. A stimulant is added to counteract the lethargy. The stimulant triggers anxiety. A benzodiazepine is added for the anxiety.
Within a few years, this child is taking five psychiatric drugs. She has accumulated diagnoses of major depressive disorder, generalized anxiety disorder, and bipolar disorder. She has been hospitalized. She has dropped out of school. She believes she is fundamentally broken and will need psychiatric management for the rest of her life.
She did not have five psychiatric disorders. She had one: an adverse reaction to psychiatric drugs that was misinterpreted at every turn.
This system transforms episodic and even typical variations in behavior into chronic disabilities. It creates the very conditions it claims to treat.
This Is Child Abuse
I use this language deliberately.
When we label children with psychiatric disorders based on no objective biological evidence, we cause emotional harm.
When we prescribe drugs that carry black box warnings for suicidality, that cause neurological changes, sexual dysfunction, metabolic disruption, and emotional blunting, we cause physical harm.
When we interpret adverse drug reactions as evidence of worsening mental illness and respond with additional drugs, we perpetuate harm.
When we transform children experiencing normal human responses to difficult circumstances into lifelong psychiatric patients, we cause profound harm to their identity, their development, and their future.
The fact that this occurs in medical settings does not change what it is.
The fact that it is performed by credentialed professionals does not change what it is.
The fact that insurance covers it does not change what it is.
We are systematically harming children while calling it care. And until we name it clearly, nothing will change.
AWAKEN
I would not have dedicated my career to exposing these problems if I did not believe alternatives exist.
Children do not need to be diagnosed and drugged. They need to be understood.
Anxiety is not a disorder. It is information. A child’s nervous system communicates that something requires attention in their environment, their relationships, their nutrition, their sleep, their sense of safety and belonging. Many need to LEARN how to face and tolerate fear, uncertainty and anxiety provoking situations. It’s part of the journey.
Address the root causes. Create genuine safety. Build authentic connection. Teach skills for understanding and navigating difficult emotions. Support the family system. Examine what the child is eating, how they are sleeping, whether they are moving their bodies, whether they have purpose and meaning. If you are on your phone for 8 plus hours a day I guarantee you are going to be miserable. You do not have a genetic condition called “Major Depressive Disorder” and “ADHD”.
We have collectively lost our minds.
I have watched children labeled treatment-resistant transform when we stopped drugging their symptoms and started addressing their lives. Not occasionally. Repeatedly. Consistently.
The psychiatric system does not want families to know this is possible. Healthy children do not generate recurring revenue.
But it is possible. And families deserve to know.
A Challenge
If you are a prescriber who puts developing children on psychiatric drugs without exhausting other options, without providing genuine informed consent about the risks, without a clear plan for eventual discontinuation, I ask you to reconsider what you are participating in.
If you are a parent who was told your child has a brain disease requiring lifelong medication, please know that you were not given accurate information. Seek other opinions. Explore other approaches. Your child’s future may depend on it.
If you are a young person who was drugged into compliance and told there was something fundamentally wrong with you, I want you to hear this: There was not. There is not. You were a human being having a human experience within a system that profits from your suffering.
The psychiatric drugging of children is one of the defining moral failures of our era. I will continue saying so until something changes.
Featured Video

Total War – Attacking Nuclear Plants, Desalination & Infrastructure
or go to
Aletho News Archives – Video-Images
From the Archives
Strike on Israel Shows US Bases Near Iran Are ‘Achilles Heel’
By Svetlana Ekimenko – Sputnik – 14.04.2024
Fears of a greater Middle East escalation were triggered after Iran launched a massive drone and missile attack against Israel, aided by Hezbollah and the Yemeni Houthis. Iran said the attack was in response to Israel’s bombing of the Iranian consulate in Damascus, Syria, which killed seven members of the elite Revolutionary Guard Corps.
Iran’s massive retaliatory attack on Israel from its own territory is a sign that the conflict could “escalate out of control.”
Michael Maloof, a former senior security analyst in the office of the US secretary of defense, told Sputnik that the first ever direct Iranian attack on Israel set a dangerous precedent.
“My concern is that this could easily escalate into something not only between Iran and Israel, but beyond the Middle East region,” he said.
Iran’s assault, which it stated was an act of “self-defense” after the Israeli strike on its consulate in Damascus, was originally intended to be a “limited” one, said Maloof.
Iran first sent in “swarms of drones with lights on as a sign of psychological warfare,” but sending in cruise and ballistic missiles by Tehran was a “distinct escalation,” said Maloof.
The scale of Iran’s attack on Israel suggests that Tehran was sending a message, demonstrating that it possesses “extraordinary capabilities,” said Maloof. … continue
Blog Roll
 Aletho News
Aletho News- Pakistan PM backs Iran’s right to self-defense amid tensions
- Hungary blasts ‘fake’ EU accusation
- SAFE Debt Trap: Poland’s €43.7 Billion Bet on Unipolar Illusion
- War on Iran threatens global Gulf capital flows: FT analysis
- Mossad De Facto Admits To Inciting Riots In Iran
- Tehran: World grown thoroughly exhausted with US-Israeli ‘false flag storylines’
- Trump ‘stuck between a rock and a hard place’, lacks Iran war strategy: Ex-CIA chief
- Trump’s bombardment of fake news so far is working quite well. But where is it heading?
- Iran to Mine Sea Lanes in Persian Gulf in Case of Attack – Defense Council
- Barak blasts Netanyahu: ‘Stop lying – you can’t destroy Iran’s nuclear, missile capabilities’
- If Americans Knew
- From Sde Teiman, the truth about Israel’s military justice system has been set free
- Child denied life-saving bone marrow transplant by Israel ‘because he is from Gaza’
- Raffi Berg: BBC Middle East Editor Exposed as CIA, Mossad Collaborator
- Jerusalem Archbishop Rebukes Netanyahu’s Statements on Christianity
- US to embed Palantir AI across entire military: Report
- Israeli-US war on Iran to drag on “a few more weeks” – Not a ceasefire Day 164
- Lebanon deaths top 1,200; Palantir AI to be embedded across US military – Not a ceasefire Day 163
- Israel’s assassination game: Take all pragmatists off the board
- Food shortages return to Gaza as Israel tightens aid restrictions under the cover of its war on Iran
- Trump demands trillions in payments from Gulf countries, billions from Harvard – Not a ceasefire Day 162
- No Tricks Zone
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis
- New Study Documents A 20-Year Pause In Arctic Sea Ice Decline – Driven By Internal Variability
- Wake-up Call: Survey Shows Majority Of Germans Now Favor Postponing Climate Targets!
- Televised! Leading German Political Candidate Tells Schoolchildren CO2 Makes Sun Hotter!
