Journal Retracts Peer-Reviewed Study Linking COVID Vaccines to Cancer After Reuters ‘Fact Checks’ It
By Brenda Baletti, Ph.D. | The Defender | July 1, 2024
The journal Cureus last week retracted a Japanese study that found statistically significant increases in cancer mortality following COVID-19 vaccination, especially after the third COVID-19 shot.
The journal said on its website, “Upon post-publication review, it has been determined that the correlation between mortality rates and vaccination status cannot be proven with the data presented in this article.” This invalidated the results, prompting the retraction, the journal said.
Denis Rancourt, Ph.D., all-cause mortality researcher and former physics professor at the University of Ottawa in Canada, who also has published in Cureus, on X called the retraction “baseless.”
“Showing data in support of vaccine-induced cancer is not allowed: burn it,” he wrote.
EVIDENCE OF TURBO CANCER WILL NOT BE PUBLISHED
Another baseless owned editorial “retraction” of a published peer-reviewed article at @CureusMedical
Showing data in support of vaccine-induced cancer is not allowed: Burn it.
Among other problems, this suggests a dubious “business… pic.twitter.com/M4SW4c2kS1— Denis Rancourt (@denisrancourt) June 27, 2024
Other scientists also expressed frustration with the retraction.
“Unfortunately, one more scientific study that challenges the established narrative gets retracted,” Panagis Polykretis, Ph.D., a researcher at Italy’s Institute of Applied Physics at the National Research Council said in an email shared with The Defender. “One more outrageous and unjustified example of censorship takes place!”
The study, published in April, analyzed official Japanese government statistics to compare age-adjusted cancer mortality rates during the COVID-19 pandemic (2020-2022) with pre-pandemic rates.
The researchers found a 2.1% mortality increase in 2021 and a 9.6% increase In 2022.
They determined that age-adjusted death rates for leukemia, breast, pancreatic and lip/oral/pharyngeal cancers increased significantly in 2022 after a large portion of the Japanese population had received the third dose of an mRNA COVID-19 vaccine.
Overall, they found no significant cancer-related excess mortality in 2020, but a 1.1% increase in 2021 after the rollout of the first and second vaccine doses, and a 2.1% increase in 2022.
Mortality for some cancers increased by as much as 9.7%, according to the study.
The paper also discussed possible mechanisms by which multiple mRNA vaccines could influence cancer rates and called for further research into the issue.
The findings suggested the vaccines may be accelerating cancer deaths in patients with preexisting tumors, according to John Campbell, Ph.D., who discussed the study on his YouTube show.
The paper went through a “rigorous peer review process,” according to Polykretis, who detailed the retraction saga on his Substack, before Cureus accepted the paper on April 8.
Less than a month after the paper’s publication, Reuters issued a “fact check” of a social media post that cited the paper. Reuters called the analysis “flawed” and said the study “assumes without evidence that vaccines are the cause of the cancer death rates they observe.”

The “Fact Check” article also stated the paper offered no proof of “turbo cancers” — a claim the study authors don’t make.
On June 12, Graham Parker-Finger, director of publishing for the Cureus Journal of Medical Science, notified the authors about concerns with their paper, citing the Reuters Fact Check, Polykretis reported.
An “expression of concern” was posted that same day and about a month later the journal retracted the article.
The article has been viewed over 287,000 times.
Polykretis asked, since when does a scientific journal’s editorial board judge scientific studies “on the basis of poorly written, not backed by scientific data and not peer-reviewed fact-checking” articles?
M. Nathaniel Mead is co-author of the first peer-reviewed paper to provide an extensive analysis of COVID-19 mRNA vaccine trial data and post-injection injuries. Mead, whose article also was printed and then retracted by Cureus, told The Defender this latest retraction was “unfortunate but also quite revealing.”
He said:
“The Gibo et al. retraction makes it official: Even though Cureus has now published many counter-establishment narrative papers related to adverse events, it is clearly ‘unsafe’ for any authors presenting papers that expose the likely mortality risk of these gene-based prodrugs.
“As you will recall, our comprehensive ‘Lessons Learned’ review and analysis also was heavily focused on the mortality aspect. So that’s where Springer-Nature seems to be drawing the line — after they accept the paper.
“Scientists seeking to publish on mortality-related aspects of the Covid mod mRNA injections obviously need to be extra cautious when considering their publishing options. These weaponized, predatory retractions will likely continue for as long as these products remain on the market.”
Dr. John Adler at Stanford University and Dr. Alexander Muacevic at the University of Munich Hospitals co-founded Cureus in 2009 as a web-based, peer-reviewed, open-access general medical journal with low-cost barriers to publication.
The academic publishing giant Springer Nature bought Cureus in December 2022.
Springer Nature is a publishing conglomerate founded in 2015 through a merger of Nature Publishing Group, Palgrave Macmillian, Macmillan Education and Springer Science+Business Media.
The publisher generated 1.8 billion euros in 2022, showing continuous year-over-year growth since 2020.
The Defender asked the editors at Cureus and Springer Nature to comment on the retraction and the allegations of censorship.
Parker-Finger responded, “Concerns were raised following publication, so we undertook a post-publication review, in line with good publishing practice, which led us to conclude that retraction was warranted for the reasons outlined in the retraction note.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Finland to Offer Bird Flu Vaccine Despite Lack of Safety Testing and Human Infections
By John-Michael Dumais | The Defender | June 27, 2024
Finland is set to become the first country in the world to offer bird flu vaccinations to humans, sparking a heated debate about vaccine safety and necessity.
The Finnish Institute for Health and Welfare (Terveyden ja hyvinvoinnin laitos or THL) announced plans to begin administering H5N8 bird flu vaccines to select groups as early as next week, despite the absence of human infections in the country.
The unprecedented move comes as global health experts express conflicting views on the threat posed by avian influenza. While Finnish officials cite the need for preemptive protection, critics argue the vaccination program is premature and potentially dangerous.
The Finnish announcement comes just two weeks after the European Commission Health Emergency Preparedness and Response (HERA) program announced the purchase of 665,000 doses of CSL Seqirus’ H5N8 avian influenza vaccine, with an option to acquire another 40 million doses over the next four years. HERA has already obtained 111 million doses of GSK’s bird flu vaccine.
Finland’s vaccination plan
Finland plans to offer the CSL Seqirus H5N8 bird flu vaccine to approximately 10,000 people deemed at high risk of exposure to the virus.
Mia Kontio, a health security official at THL, told STAT News that the country was awaiting the arrival of 20,000 doses, with plans to administer them “as soon as the vaccines are in the country.”
According to THL’s press release, the target groups for vaccination include:
- Fur farm workers in contact with animals.
- Poultry workers in direct contact with birds.
- Veterinarians.
- Laboratory workers handling avian influenza samples.
- Bird ringers and those caring for wild birds.
- Workers in petting zoos and aviaries.
CSL Seqirus’ vaccine received the European Union’s (EU) marketing authorization in April. The vaccine requires a two-dose series, with the second dose administered at least three weeks after the first.
“The goal is to start vaccinations in the welfare areas as soon as possible, so that the two-dose vaccination series can be offered to the vaccinated before the start of the autumn flu season,” said THL’s expert doctor Anniina Virkku.
Besides protection from bird flu, the vaccination program aims to prevent simultaneous infection with the seasonal flu virus, “which could enable the emergence of a new type of virus.”
THL noted that the vaccination program is targeted at high-risk groups and is not a blanket recommendation for the staff of facilities without contact with infected birds or animals.
‘U.S. has never had a fatal human case of bird flu’
The H5N1 strain of bird flu has caused widespread concern among government health authorities in recent years, leading to the culling of hundreds of millions of poultry globally, according to Reuters.
The virus has expanded its reach, affecting not only birds but also an increasing number of mammals, including cows in the U.S.
In 2023, Finland experienced large-scale deaths of wild birds due to bird flu virus infections, THL said. The virus also spread widely to fur farms, causing high morbidity and mortality in animals.
However, the Finnish Food Agency reported that bird flu cases in wild birds have significantly decreased in 2024 compared to the previous year.
Globally, human infections remain rare. Since December 2021, only eight cases of bird flu have been reported in humans worldwide, according to the World Health Organization.
In the U.S., three dairy workers were diagnosed with confirmed infections tied to the recent outbreak among cattle, all experiencing mild symptoms, according to STAT News.
Despite the low number of human cases, health authorities remain concerned about the virus’s potential to mutate and become more transmissible between humans.
However, Dr. Peter A. McCullough, in his Substack post on Monday argued that even if the bird flu crossed to humans, it would be less dangerous. “Increased transmissibility of H5N1 has a tradeoff of decreased virulence,” he wrote.
He said the alarming statistics on human mortality rates are from long-ago cases in Southeast Asia and that such concerns are “not appropriate” for today’s strains.
Furthermore, the U.S. “has never had a fatal human case of bird flu,” he said.
A dangerous vaccine for a disease that does not exist’
Medical freedom advocates and health experts have voiced strong objections to the rapid deployment of the bird flu vaccine.
Internist and bioweapons expert Dr. Meryl Nass pointed out that the product information for the H5N8 bird flu vaccine recently purchased by the EU — the same one being deployed in Finland — includes no clinical data for this specific vaccine strain, meaning it has not been tested in humans.
STAT News reported that the European Medicines Agency approved the H5N8 bird flu vaccine based on immunogenicity studies rather than traditional efficacy trials, as the virus isn’t currently circulating among humans.
Nass noted that scientists don’t have a clear way to measure if the vaccine protects against H5 types of bird flu and that it’s unclear whether the vaccine would work against other similar strains of the virus.
She called the product “a dangerous vaccine for a disease that does not exist.”
Nass also noted that the vaccine contains the adjuvant MF59C.1, which includes squalene, polysorbate 80 and other compounds that could cause autoimmunity.
Jessica Rose, Ph.D., a vaccine analyst and biomathematics specialist, said she has several reservations about the program. “There’s no need for this vaccine, and it poses dangers including tolerization and autoimmune reactions from molecular mimicry,” she told The Defender.
Tolerization (or immunological tolerance) occurs when the immune system becomes less responsive to a particular antigen over time, potentially reducing the vaccine’s effectiveness.
Molecular mimicry refers to similarities between vaccine components and human proteins, which could lead the immune system to mistakenly attack the body’s own tissues, potentially triggering autoimmune disorders.
Rose also said, “Intramuscular injections are never the way to deal with pathogens that enter the body via respiration.”
McCullough warned that mass vaccination could lead to a “highly prevalent pandemic” because it “promotes resistant strains of the virus in the vaccinated.”
He suggested alternative strategies, including “dilute iodine nasal sprays and gargles, oseltamivir, hydroxychloroquine and other antivirals” for prevention and early treatment.
McCullough criticized what he called “fear-mongering promulgated by the Bio-Pharmaceutical Complex,” suggesting that it is “designed to promote mass vaccination of animals and humans with lucrative pre-purchased contracts to the vaccine manufacturers” and their nongovernmental organization sponsors.
Geert Vanden Bossche, DVM, Ph.D., voiced similar concerns. He told The Defender, “Any large-scale vax program using whatever vaccine administered during a pandemic or a panzootic transmissible to humans is at risk of causing large-scale Ab-[antibody-]dependent enhancement of disease and large-scale immune escape!”
Antibody-dependent enhancement is a phenomenon where antibodies produced by the immune system in response to a vaccine or previous infection can worsen a subsequent infection. Instead of protecting against the virus, these antibodies can help the virus enter cells more easily, potentially leading to more severe illness.
Regarding Vanden Bossche’s concerns over immune escape, he made the same argument for the COVID-19 vaccines, claiming their administration during the SARS-CoV-2 outbreak caused the evolution of more transmissible and dangerous viral variants.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
‘Stunning admissions’: White House pressured FDA to cut corners on COVID vaccine approvals in order to push mandates
By Brenda Baletti, Ph.D. | The Defender | June 28, 2024
The Biden administration pressured the U.S. Food and Drug Administration (FDA) to “change its procedures, cut corners, and lower agency standards,” to approve Pfizer’s COVID-19 vaccines and authorize boosters, according to a congressional report released earlier this week.
The approval was key to facilitating the Biden administration’s rollout of the fall 2021 vaccine mandates, despite safety concerns about the shots, according to the report.
“During the pandemic, politics overruled science at the government institutions entrusted with protecting public health,” Rep. Thomas Massie (R-Ky.) said in a press release announcing the report.
“The FDA abandoned its congressional directive to protect citizens from false claims and undisclosed side effects, and instead ignored its own rules to pursue a policy of promoting the vaccine while downplaying potential harms,” he added.
As a result, according to the report, “countless Americans” suffer from vaccine side effects and the FDA has lost credibility with the public.
Following the report’s release a U.S. House of Representatives Judiciary Subcommittee held a hearing Wednesday — “Follow the Science?: Oversight of the Biden Covid-19 Administrative State Response” — during which Dr. Philip Krause, former deputy director of the FDA’s Office of Vaccines Research and Review (OVRR) vaccine products provided evidence to support the report’s conclusions.
Krause testified that both he and OVRR Director Marion Gruber were relieved of their responsibilities overseeing the COVID-19 vaccines review process because the administration wanted to rush FDA approval on a faster timeline than their office could deliver and push forward the fall mandates, Vinay Prasad, M.D., MPH, reported.
The approval process was then pushed through by the director of the FDA’s Center for Biologics Evaluation and Research, Peter Marks, M.D., Ph.D., and then-Acting FDA Commissioner Janet Woodcock.
Documents obtained by Children’s Health Defense (CHD) through a Freedom of Information Act Request also showed that in early 2021, both Marks and Woodcock were aware of injuries linked to the vaccines.
Krause testified that the original timeline to complete the review process for Pfizer’s Biologics License Application (BLA) for its mRNA COVID-19 product was January 2022, but the team was already shooting to have the process completed earlier.
In early July 2021, “something had happened to completely change the opinion of Drs. Marks and Woodcock regarding the urgency of completing the BLA review,” Krause testified. “It was so important to them that they did not trust the experts who led the Office of Vaccines to do it, even with their help,” he said.
Krause told the committee that on July 19, he and Gruber were taken off the review process and Marks took it over himself.
He added:
“In this meeting, Drs. Woodcock and Marks expressed concern about the rising number of COVID cases in the US and globally, largely caused by the Delta variant and stated their opinion that, absent a license, states cannot require mandatory vaccination and that people hesitant to get an EUA authorized vaccine would be more inclined to get immunized if the product were licensed.”
Marks informed staff that the goal was to complete the review as rapidly as possible, Krause said. Pfizer’s Comirnaty COVID-19 vaccine was licensed on Aug. 23, 2021.
“As predicted by Drs. Woodcock and Marks, vaccine mandates followed immediately afterwards and were announced the same day for DoD [U.S. Department of Defense] and for New York State,” Krause said.
He said that the speed with which the mandates were implemented following authorization, “suggested that the rapid review of the vaccine was motivated more by a desire to mandate vaccines than by other public health considerations.”
Given that mandates are outside of the FDA’s purview, he added, the fact that Marks and Woodcock cited the need for mandates as a reason to speed the review “strongly implies that pressure to complete the review” more rapidly than planned came from outside of the FDA, he added.
When Krause and Gruber tried to implement a slower and more deliberative process, they were demoted, Prasad wrote.
As a result, they both left the agency at the end of 2021.
Prasad noted the mandates were issued only after the administration knew the vaccine couldn’t stop transmission and “as such, the mandates were unethical.”
“Krause’s testimony shows the Biden administration engaged in inappropriate political tampering with the FDA, and the FDA leaders — Woodcock and Marks — folded to political pressure,” he added.
Woodcock, now retired from the FDA, has since expressed regret about not doing more to respond to the concerns of the vaccine-injured, telling The New York Times she is “disappointed” in herself
Marks is still at the FDA, where Prasad said he “has been doing a bad job,” recently authorizing a product from Sarepta Therapeutics despite a failed study and a negative decision from reviewers.
Robert F. Kennedy Jr., independent presidential candidate and CHD’s chairman on leave, tweeted that Marks also made commercials for the vaccine, claiming it was safe and effective in pregnancy and for children. “Had Pfizer said that, it would have been a crime,” Kennedy said.
In his testimony, Krause also made a series of comments confirming early knowledge of myocarditis — with rates as high as 1 in 5,000 for young men in early studies — and the protection conferred by natural immunity.
He also said that he did not take a booster shot.
Chief Nerd called Krause’s comments “stunning admissions” and posted a video clip on X.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
‘Epic Waste of $500 Million’: Scientists Slam HHS Funding for ‘Next-Gen’ COVID Oral and Nasal Vaccine Trials
By John-Michael Dumais | The Defender | June 24, 2024
The U.S. Department of Health and Human Services (HHS) has announced up to $500 million in funding for clinical trials of three next-generation COVID-19 vaccine candidates, including two nasal sprays and an oral pill.
The initiative, part of the $5 billion Project NextGen, aims to develop innovative vaccines that are easier to administer and provide improved protection against the SARS-CoV-2 virus.
The funding, awarded through the Biomedical Advanced Research and Development Authority (BARDA) under HHS’ Administration for Strategic Preparedness and Response (ASPR), will support Phase 2b clinical trials for Vaxart‘s oral pill vaccine (up to $453 million) and CyanVac’s (up to $40 million) and Castlevax’s ($34 million) intranasal vaccines.
Each company’s phase 2b trials will recruit 10,000 volunteers to compare the safety and efficacy of the investigational vaccine against the existing mRNA vaccines.
ASPR Assistant Secretary Dawn O’Connell said in a news release that the new vaccines “may … be easier to administer through intranasal or oral delivery.” The announcement suggests the delivery methods have the “potential to improve vaccine access.”
However, the new delivery methods also raise unique concerns, especially the nasal vaccines, which use modified viruses as vectors.
Vaccine researcher Jessica Rose, Ph.D., told The Defender that she’s concerned about vaccine shedding and the possibility of pharmaceutical companies aerosolizing their products and administering them “without public knowledge as part of a ‘vaccination’ run.”
Brian Hooker, Ph.D., Children’s Health Defense chief scientific officer, echoed Rose’s concern about potential vaccine shedding, calling it a “nightmare like other live-virus vaccine formulations.”
Hooker told The Defender that because COVID-19 mutates rapidly, “immunity will still wane precipitously” for the new vaccine candidates, just as it did with the existing mRNA vaccines.
The new vaccines are “just more ‘me too’ technologies that are late to the party for COVID-19,” he said.
UGA spins off nasal vax biotech firm
University of Georgia (UGA) vaccine development spinoff CyanVac (an affiliate of Blue Lake Biotechnology) is set to begin phase 2b clinical trials for a new nasal COVID-19 vaccine, CVXGA. The study will be conducted through BARDA’s clinical studies network.
CyanVac founder Dr. Biao He, chair of veterinary medicine at UGA, leads the team behind CVXGA. He served on a White House panel in July 2022 advising on the future of COVID-19 vaccines, where he specifically promoted nasal vaccines.
CVXGA is a Parainfluenza virus 5 (PIV5)-based vaccine that encodes the spike protein of SARS-CoV-2.
Formally known as simian virus 5, PIV5 is often referred to as canine parainfluenza virus in the veterinary field, where it is a contributing factor to kennel cough in dogs. PIV5-based vaccines have been used to prevent kennel cough, reportedly without any safety concerns.
“PIV5 is a novel intranasal vaccine vector that has been shown to replicate safely in humans in clinical trials and stimulates all three pillars of immunity — cellular, mucosal, and humoral — with minimal uncomfortable side effects,” Dr. He said in the company’s press release.
Rose cautioned that some studies (here, here and here) have associated PIV5 with human diseases such as Creutzfeldt‐Jakob disease and multiple sclerosis, but noted that later research was unable to confirm PIV5 as the cause. “More research needs to be done before this is used as a viral vector in humans,” she said.
Currently, there are no licensed vaccines for humans that contain PIV5. However, besides the CVGXA COVID-19 vaccine, PIV5 is under development for vaccines targeting various human and animal infectious diseases, including Lyme disease, respiratory syncytial virus (RSV), influenza, rabies, tuberculosis and MERS-CoV.
Castlevax promises ‘game-changing’ spike protein vax
BARDA provided Castlevax, in collaboration with the Icahn School of Medicine at Mount Sinai in New York City, $34 million for its phase 2b trial of its intranasal vaccine candidate CVAX-01 beginning in Q4 2024.
The company is projected to receive as much as $338 million from BARDA for its COVID-19 “booster” vaccine.
Castlevax calls its vaccine “a next-generation COVID-19 vaccine with game-changing potential” with a design that “holds spike protein firmly in pre-fusion conformation, leading to more efficient induction of neutralizing antibodies.” It promises to “deliver reduced rates of breakthrough infections.”
Its vaccine, NDV-HXP-S, uses a recombinant Newcastle disease virus (NDV) that expresses the spike protein. The spike protein has been modified to contain six mutations by the HexaPro (HXP) technology developed at a University of Texas (UT), Austin laboratory.
HXP promises to make the spike protein more stable compared to older mRNA vaccines, which only contain two mutations. “Human antibodies recognize and respond to Hexapro better since the spike protein is less prone to shifting shapes,” according to a UT lab researcher.
The vaccine is grown in chicken eggs, a method commonly used to produce flu vaccines.
Castlevax boasts of having “multiple COVID-19 products in Phase 2 through Emergency Use Authorization, while we’re simultaneously developing a bivalent mucosal RSV+HMPV [human metapneumovirus] vaccine and a mucosal Norovirus vaccine.”
Promises and dangers of nasal vaccines
Hooker noted that nasal vaccines can be effective. “Mucosal immunity provides defenses at the mucous membrane level through a type of antibody called secretory IgA [immunoglobin A] along with humoral IgG and IgM antibodies,” he said.
But he cautioned that due to the observed rapid mutation in SARS-CoV-2 variants, “Long-term efficacy will be nil” for these vaccines.
Live virus nasal vaccines have been used for flu for years, he said, suggesting these latest entries are “looking for entry into the ‘annual’ COVID-19 vaccination market opportunity.”
Rose pointed out that EcoHealth Alliance’s 2018 DEFUSE proposal to the Defense Advanced Research Projects Agency (DARPA) included a plan to aerosolize bat vaccines and deliver them at the mouths of caves in China.
“They hired an aerosol tech company to find the best way to administer their products,” she said.
When she saw this part of the proposal, Rose speculated the technique could readily be used to vaccinate people without their consent. “Given that everything they’ve done so far has been from questionable to illegal, I really have to wonder.”
Hooker added that the three BARDA-funded projects use live-virus vaccines that are “notoriously bad for pregnant women.”
Oral pill targets epithelial cells
Vaxart will receive up to $453 million from BARDA to develop an oral pill vaccine, which is also just entering phase 2b clinical trials.
“Vaccine delivery has relied primarily on injection for more than 150 years,” said Steven Lo, Vaxart’s CEO in the press release. “This funding from BARDA will assist us in determining whether we can bring a transformational, next-generation approach to global vaccination.”
Vaxart’s pill, VXA-CoV2-1, uses an adenovirus vector to infect epithelial cells in the lower small intestine. The vaccine delivers the genetic material to create the spike protein. The company boasts that a special coating allows the oral pill to survive the low pH in the stomach.
Adenovirus vaccines reportedly cannot make you sick, and cannot replicate or be integrated into the host body’s DNA.
Johnson & Johnson’s (J&J) and AstraZeneca’s COVID-19 vaccines also used adenovirus vectors.
The use of J&J’s vaccine was paused in April 2021 due to reports of thrombosis with thrombocytopenia syndrome (TTS), a severe blood clotting disorder. In July 2021, the FDA warned about the risk of Guillain-Barré syndrome with the J&J vaccine after approximately 100 cases were reported among 12.8 million vaccine recipients. With existing doses of the J&J vaccine having expired in May 2023, the vaccine is no longer in use.
AstraZeneca’s COVID-19 vaccine also caused blood clots, resulting in temporary pauses in its use in several countries. With declining demand, it was also removed from the market in May 2023.
Trials set ‘a horribly low bar’
The two nasal and one oral vaccine candidates are all entering phase 2b trials where their safety and efficacy will be compared to the available FDA-approved mRNA vaccines.
Hooker said that this sets “a horribly low bar for comparison given that the ‘control’ group is now subjected to the vaccine that has the worst safety profile in history.”
He underscored that the mRNA vaccines offer “extremely limited and sometimes negative efficacy, and no utility in terms of prevention of transmission,” and argued that using them as comparators for the candidate vaccines would be next to useless.
“Basically, almost anything short of a vial of arsenic would perform comparably,” he said.
“Given the low morbidity/mortality of the currently circulating COVID-19 strains, this is an epic waste of $500 million,” he said. “Their ROI [return on investment] will essentially be a bunch of sick people with vaccine injuries.”
Rose said that long-term efficacy cannot be guaranteed “based on failure of maintained efficacy in COVID-19 product prototypes. This is precisely why they keep pushing ‘boosters.’”
Hooker also questioned the review and approval process for the new vaccines. He said:
“As far as independence, safeguards and transparency, those are now gone. Not because of this particular clinical trial entry, but because of the shamfest that FDA was and still is with the EUA [emergency use authorization] and approvals granted during the plandemic.
“All the tricks that they (Dr. Peter Marks and company) pulled like trying to prevent the release of clinical trial documents, approving without human trials, the joke that is CICP [Countermeasures Injury Compensation Program], etc., really spell death for any integrity in the approvals process.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Free Speech Legislation Gains Attention Following Supreme Court Siding with Biden in Social Media Censorship Case
By Didi Rankovic | Reclaim The Net | June 27, 2024
US House Judiciary Committee Chairman Jim Jordan has reacted to Wednesday’s ruling by the Supreme Court (SCOTUS) in the Murthy v. Missouri case, to call for new legislation that would, going forward, reinforce the rules, already contained in the First Amendment, meant to protect citizens from government-orchestrated censorship.
Jordan, whose Committee is probing alleged government-Big Tech collusion in violation of the First Amendment through the Select Subcommittee on the Weaponization of the Federal Government, noted that the US Constitution’s First Amendment is “first for a reason.”
According to the Republican congressman, free speech that this amendment protects (from government intervention) should extend to any government infringement – be it in Congress, or online.
Jordan said that while respectfully disagreeing with the SCOTUS ruling the Committee’s own oversight “has shown the need for legislative reforms.”
“While we respectfully disagree with the Court’s decision, our investigation has shown the need for legislative reforms, such as the Censorship Accountability Act, to better protect Americans harmed by the unconstitutional censorship-industrial complex,” Jordan wrote in a statement.
In other words, the increasingly pressing issue of how the government “interacts” with social platforms (because of their massive reach and therefore influence among the electorate) should be put into the hands of courts and their interpretations based on new and clear legislation to guide those decisions.
The Judiciary Committee chairman mentioned the Censorship Accountability Act – a bill that would let citizens launch legal action against federal employees suspected of colluding to suppress free speech.
Regardless of the SCOTUS decision, Jordan pledged that the Committee’s “important work will continue” – stating that the Subcommittee thus far has “uncovered how and the extent to which the Biden Administration engaged in a censorship campaign in violation of the First Amendment.”
Murthy v. Missouri – which sought to give the plaintiffs the right to pursue their legal case against the government, alleging it pressured social media to censor online user content, was thrown out by the Supreme Court in a 6-3 ruling as “lacking standing to sue.”
At the same time, the court canceled – at a particularly sensitive time, mere months before the upcoming US presidential election – an injunction that limited the way the government can “interact” with social platforms regarding a range of issues.
The collusion allegations for the most part refer to activities and communications between the government and Big Tech in the context of the previous vote that resulted in the installment of the current US administration.
We Now Have Proof The COVID Vaccines Damage Cognition
Examining the causes and treatments of the common neurological injuries caused by vaccination
A MIDWESTERN DOCTOR | THE FORGOTTEN SIDE OF MEDICINE | JUNE 20, 2024
Story at a Glance:
• Subtle and overt neurological injuries are one of the most common results of a pharmaceutical injury.
• The COVID-19 vaccines excel at causing damage to cognition, and many of us have noticed both subtle and overt cognitive impairment following vaccination that relatively few people know how to address.
• For a long time, the hypothesis that the vaccines impaired cognition was “anecdotal” because it was based on individuals observing it in their peer group or patients.
• Recently large datasets emerged which show this phenomenon is very real and that the severe injuries we’ve seen from the vaccines (e.g., sudden death) are only the tip of the iceberg.
• In this article we will review the proof that vaccines are doing this and explore the mechanisms which allow it to happen so we can better understand how to treat it.
Note: I originally published this article a year ago. I am republishing it now because a robust dataset emerged which regrettably validates the hypothesis I put forward then.
When the COVID-19 vaccines were brought to market, due to their design I expected them to have safety issues, and I expected over the long term, a variety of chronic issues would be linked to them. This was because there were a variety of reasons to suspect they would cause autoimmune disorders, fertility issues and cancers—but for some reason (as shown by the Pfizer EMA leaks), the vaccines had been exempted from being appropriately tested for any of these issues prior to being given to humans.
Since all new drugs are required to receive that testing, I interpreted it to be a tacit admission it was known major issues would emerge in these areas, and that a decision was made that it was better to just not officially test any of them so there would be no data to show Pfizer “knew” the problems would develop and hence could claim plausible deniability. Sadly, since the time the vaccines entered the market, those three issues (especially autoimmunity) have become some of the most common severe events associated with the vaccines.
At the start of the vaccine rollout, there were four red flags to me:
• The early advertising campaigns for the vaccines mentioned that you would feel awful when you got the vaccine, but that was fine and a sign the vaccine was working. Even with vaccines that had a very high rate of adverse events (e.g., the HPV vaccine), I had never seen this messaging before. This signified it was likely the adverse event rate with the spike protein vaccines would be much higher than normal.
• Many of my colleagues who got the vaccine (since they were healthcare workers they were able to get it first) posted on social media about just how awful they felt after getting the vaccine. This was also something I had never seen with a previous vaccine. After some digging, I noticed those with the worst vaccine reactions typically had already had COVID and that their reaction was to the second shot rather than the first, signifying that some type of increased sensitization was occurring from repeated exposures to the spike protein. Likewise, the published clinical trial about Pfizer’s vaccine also showed adverse reactions were dramatically higher with the second rather than first shot.
• Once the vaccine became available to the general public, I immediately had patients start showing up with vaccine reactions, many of whom stated they received their flu shot each year and never had experienced something similar with a previous vaccination. One of the most concerning things were the pre-exacerbation of autoimmune diseases (e.g., spots in their body they previously would occasionally have arthritis in all felt like they were on fire). After I started looking into this I realized people were seeing between a 15-25% rate of new autoimmune disorders or exacerbations of existing autoimmune disorders developing after the vaccine, a massive increase I had never seen any previous vaccine cause.
Note: this was demonstrated by a February 2022 Israeli survey which showed 3% of vaccine recipients experienced a new autoimmune disorder and that 24% experienced an exacerbation of a pre-existing one, a rheumatologic database published in the BMJ that found 4.4% of recipients experienced an exacerbation of a pre-existing autoimmune disease, and a survey by a private physician of 566 patients which found vaccination spiked their inflammatory markers, causing their five year risk of a heart attack to go from 11% to 25%.
• About a month after the vaccines were available to the public, I started having friends and patients share that they’d known someone who had unexpectedly died suddenly after receiving the vaccine (typically from a heart attack, stroke, or a sudden aggressive case of COVID-19).
This was also extremely concerning to me, because reactions to a toxin typically distribute on a bell curve, with the severe ones being much rarer than the moderate ones. This meant that if that many severe reactions were occurring, what I could already see was only the tip of the iceberg and far, far more less obvious reactions were going to be happening, to the point it was likely many people I knew would end up experiencing complications from the vaccine.
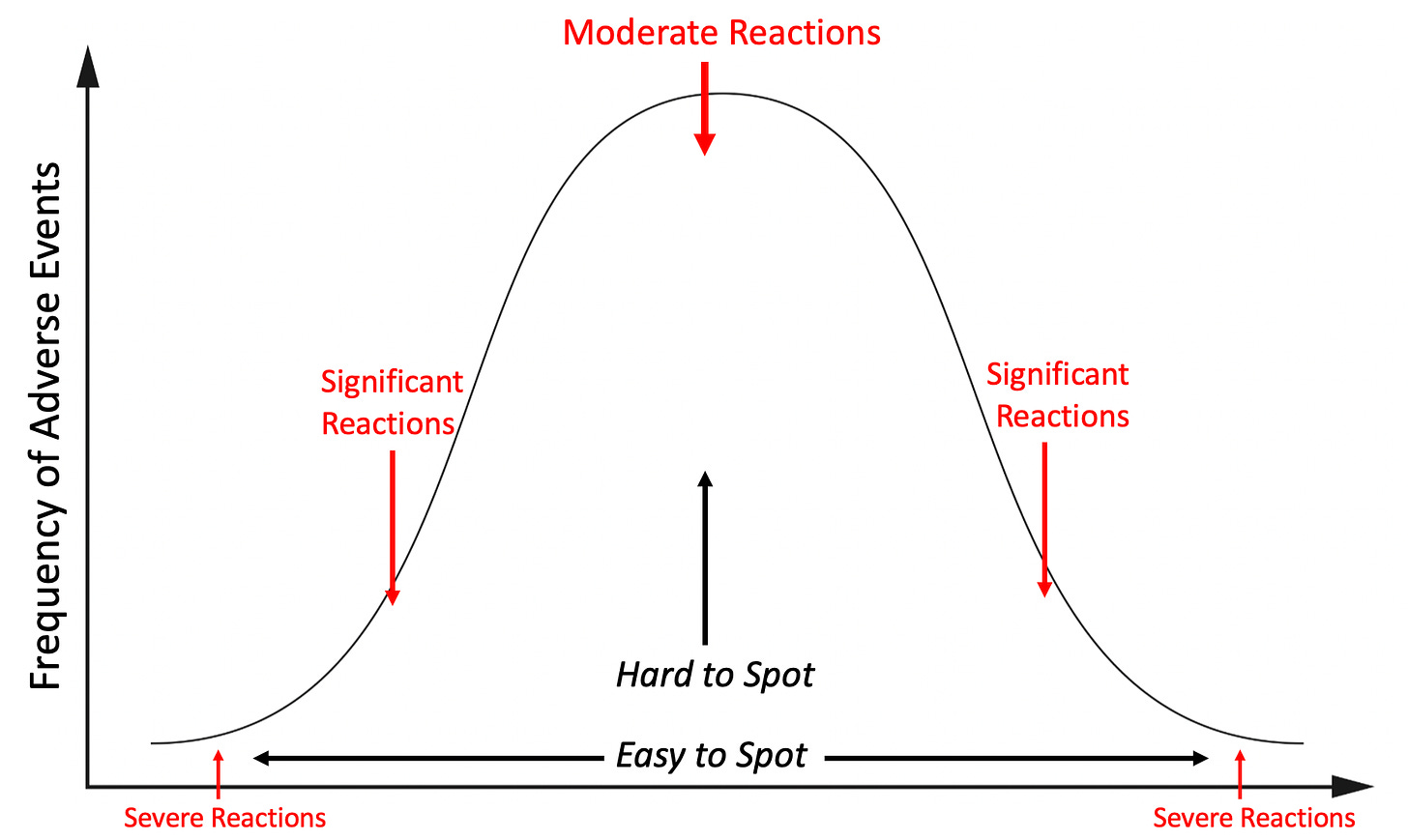
Note: the above graph is only illustrating one aspect of the picture as there will also be a much larger number of minor reactions, and even more invisible ones (e.g., a symptom occurs years down the road) or no reaction at all.
I tried to warn my colleagues about the dangers of this vaccine, but even when I pointed out Pfizer’s own trial admitted the vaccine was more likely to harm than help you, no one would listen to me. Not being sure what else to do, but not be willing to do nothing, I decided to start documenting all the severe reactions I came across so I could have some type of “proof” to show my colleagues.
This was something that was extremely important at the time since no one was willing to take on the personal risk of publishing something that went against the narrative (that vaccines were killing people) in the peer reviewed literature. Shortly after Steve Kirsch kindly helped launch my Substack, I decided to post the log I’d put together, and since there was a critical need for that information (as many had seen the same things I’d observed but no one was reporting them), the post went viral and created much of the initial reader base that made my Substack possible.
It was immensely time consuming to do the project (especially the verification of each story that was reported to me), so I ended the project after a year. During that time, I came across 45 cases of either a death (these comprised the majority of the 45 cases), something I expected to be fatal later on (e.g., a metastatic cancer) or a permanent and total disability. Additionally, in line with the previously described bell curve, I also came across many more serious but not quite as severe injuries.
What I found remarkable about this was that through a passive reporting system in my own limited social network (I learned of these cases because people reached out to me or someone off-handedly shared them with me), I alone found enough cases of severe vaccine injuries to justify pulling the COVID-19 vaccines from the market, yet, our healthcare authorities, who had access to thousands of times as much data as I did chose to pretend nothing was happening. Furthermore, from my own dataset (due to it being large enough to contain all the common COVID vaccine injuries), I accurately predicted most of the vaccine injuries that would be subsequently seen and only now (years later) are gradually being acknowledged.
In turn, we are now seeing clear signs that excess mortality has spiked across the globe, large polls are finding that one fifth of Americans know someone they believe were killed by the vaccines and because so much trust has been lost from this cover up, public health authorities are at last admitting there may be a problem—but they didn’t say anything until now because they “didn’t want to create vaccine hesitancy,” which coincidently is the same excuse which has been used for decades (e.g., Dr. Meier, a distinguished professor called out this behavior after the government unleashed an easily preventable polio disaster in 1955.
Patterns of Vaccine Injury
I’ve had a long term interest in studying pharmaceutical injuries because many of my friends and relatives have had bad reactions to pharmaceuticals. In most of these cases, ample data existed to show that reaction could happen (often to the degree it strongly argued against the pharmaceutical remaining on the market) and yet almost no one in the medical field was aware of those dangers, hence leading to my injured friends never being warned before they took the pharmaceutical or even while the injury was occurring (e.g., the doctor said they’d never seen anyone have those reactions, that whatever was happening was due to anxiety, and that they would soon end — when in reality it became a lifelong condition because the patient didn’t stop the drug in time).
My bell curve theory originally came about from examining all of their cases. I thus was interested to know if the distribution of adverse events from the spike protein vaccines would match what I had observed with previous dangerous pharmaceuticals and if what I saw personally did or did not match what everyone was reporting online (which is part of why I put so much work into making sure the log was both accurate and detailed).
One of the things that immediately jumped out at me during that logging process were the multiple cases of a friend’s parent in a nursing home receiving the vaccine, immediately undergoing a rapid cognitive decline which was “diagnosed” as Alzheimer’s disease and then dying not long after. At the time, I assumed these were most likely due to undiagnosed ischemic strokes as that was the most plausible mechanism to describe what I’d heard, but I was not certain as I could never examine any of these individuals for signs a stroke had indeed happened.
Note: despite many deaths in the nursing home population due to COVID and the vaccines, the number of people awaiting admission to a nursing home has significantly increased (shown by this large data set from the Netherlands). Given that individuals typically do not want to go to a nursing home unless they are no longe able to take care of themselves, this suggests that something new is causing the rapid development of debilitating cognitive impairment (e.g., dementia) in the adult population. Likewise, as Ed Dowd has repeatedly documented, there has been a large increase in physical and cognitive disability throughout the adult population which has significantly impacted the economy because of how many workers are being lost to vaccine injuries.
Steve Kirsch was contacted by a whistleblower who reported there has been a 25 fold increase in sudden dementia at the nursing home where she works. Similarly, like the cases shared with me, Kirsch has noted that (like me) he has frequently been contacted by relatives who reported a sudden onset of dementia in their beloved relative which was then swept under the rug. Furthermore, he has also collected numerous other forms of evidence corroborating this is indeed happening. These cases are really sad because the elders in nursing homes have very little ability to advocate for themselves, and most people will just write the cases off as “Alzheimers,” rather than seeing the red flag staring them in the face.
These cases were very concerning to me, as they signified (per the bell curve) that there was going to be a much larger portion of people who would develop less severe cognitive decline following vaccination.
Note: one of the most common types of injuries from pharmaceuticals are neurological injuries which both impair cognitive function and create psychiatric symptoms. This places patients in a difficult situation of being gaslighted by the medical system. This is because their doctors assume the psychiatric symptoms the patients are experiencing are the cause of their illness rather than a symptom of it, leading to the patient being told the illness is all in their head and continually referred for psychiatric help. One of the best examples of this occurred as a result of the abnormal heart rhythms (e.g., rapid anxiety provoking palpitations) caused by the vaccine damaging the heart which were consistently diagnosed as being a result of anxiety, even when a subsequent workup I requested showed heart damage was present. Remarkably, in the early era of vaccines, many doctors (as detailed here) acknowledged that vaccines caused neurological injuries which manifested as psychiatric symptoms, but now that recognition has been almost completely forgotten.
As I began seeing more and more signs of cognitive impairment following vaccination, I realized that what I observed mirrored what I had previously seen with chronic inflammatory conditions such as mold toxicity, HPV vaccine injuries, and lyme disease. Some of the examples included:
• Many people reported having a “COVID” brain where it was just harder for them to think and remember things. I sometimes saw this occur after more severe cases of COVID, but more frequently after vaccination, along with many instance of patients who per their timeline clearly developed it from the vaccine but nonetheless believed it had come from COVID.
• These issues tended to be more likely to affect older adults, but younger ones were more likely to notice (and complain) about them. In the case of older adults, I typically learned about them from someone else who had observed the cognitive decline rather than directly from the individual.
• I saw numerous cases of vaccine injured individuals who had trouble remembering or recalling the word they knew expressed what they were trying to communicate (this is also a common mold toxicity symptom).
• I had friends and patients who told me their brain just didn’t work the same since they’d received the vaccine. As an example, a few colleagues told me they started losing the ability to remember basic things they needed to practice medicine (e.g., medication dosages for prescriptions). They shared that they were very worried they would need to take an early retirement and that they thought it came from the vaccine but there was no one they could talk to about it (which understandably created a lot of doubt and anxiety).
• I saw cases of coworkers demonstrating noticeable (and permanent) cognitive impairment after I’d assumed they’d received the vaccine. Their impairment was never mentioned or addressed (rather the physician kept on working, did not perform as well, and in some cases retired).
• I met significantly injured vaccine injured patients who told me one of the primary symptoms was a loss of cognitive functioning they had taken for granted throughout their life. In many cases following treatment of their vaccine injury, their cognition also improved.
• Colleagues who treated vaccine injured patients told me cognitive impairment was one of the common symptoms they saw and was particularly noteworthy because they had never seen anything like that happen to young adults. To quote Pierre Kory:
In my practice of treating vaccine injuries, one of the three most common symptoms I see is brain fog. So many of my patients had been in the prime of their lives, can now barely function, have significant cognitive impairment and need a lot of help from our nurses to carry out their treatment plans. I never imagined I would see any of this in people far younger than me and instead I see it every day. I bear witness to an immense amount of suffering on a daily basis that is hard to put into words.
• One of my friends (a very smart immunologist) developed complications from the first two vaccines and based on their symptoms was able to describe exactly which parts of their immune systems were becoming dysregulated. Against my advice, they took a booster and reported they suffered a significant cognitive impairment never experienced before in their lifetime. I feel this case was important to share as it illustrates how an exacerbation of a vaccine injury can also cause an exacerbation of cognitive symptoms.
Note: I also saw significant cognitive impairment occur in individuals who were acutely ill with COVID-19. This was not as unusual since delirium is a well known complication in patients hospitalized with a systemic illness (e.g., sepsis), but it seemed to happen more frequently than usual. However, in almost all cases, COVID-19 cognitive impairment resolved after their illness (even when they had been critically ill and required hospitalization) whereas the cognitive impairment I saw from the vaccines was often permanent (unless it was treated).
I specifically wanted to write this article for two reasons.
First, unless you’ve talked to a lot of people who have been through this, it’s really hard to describe what it’s like to gradually lose your mind and the basic cognitive function you relied upon to navigate the world—especially if everyone around you is telling you that it’s not happening and it’s all in your head. I wrote this article to give a voice to those people.
Second, despite Alzheimer’s disease being the mostly costly disease for America, most providers know fairly little about it and instead use it as a blanket diagnosis for anytime a patient shows signs of impaired cognition. This, I in turn would argue has been because there is minimal interest in understanding the causes (and treatments) of Alzheimer’s disease as there is so much more money in “research” for it and productive expensive (but useless and harmful) drugs for it.
Evidence of Cognitive Impairment
At the same time I was observing these effects, many rumors were also swirling around online that the vaccines would cause severe cognitive impairment and that we would witness a zombie apocalypse from the vaccine injuries.
This apocalypse of course never happened (which again illustrates why it is so important to be judicious with what one pronounces will come to pass—as our movement has repeatedly damaged its credibility by making easily outlandish and easily falsifiable predictions). Nonetheless, many have observed a suspicion cognitive impairment was occurring. For example to quote Igor Chudov’s article on the topic:
I own a small business and deal with many people and other small businesses. Most provided reliable service, would remember appointments, followed up on issues, and so on. I noticed that lately, some people have become less capable cognitively. They forget essential appointments, cannot concentrate, make crazy-stupid mistakes, and so on.
In my own case, in addition to poorly performing colleagues, the most evident change I noticed was a worsening of drivers around me and had quite a few near misses from impaired driving.
The great challenge with these situations is that it’s very hard to tell if something is actually happening or your perception is simply a product of confirmation bias. For this reason, while I was comfortable asserting my belief the COVID-19 vaccines were causing the severe injuries on either end of the bell curve, I avoided doing so for many of the less impactful injuries in the middle where it was much more ambiguous if what I was observing was “real” or simply my own biased perception of the events around me. Because of this, amongst other things, I never mentioned the changes in driving I observed.
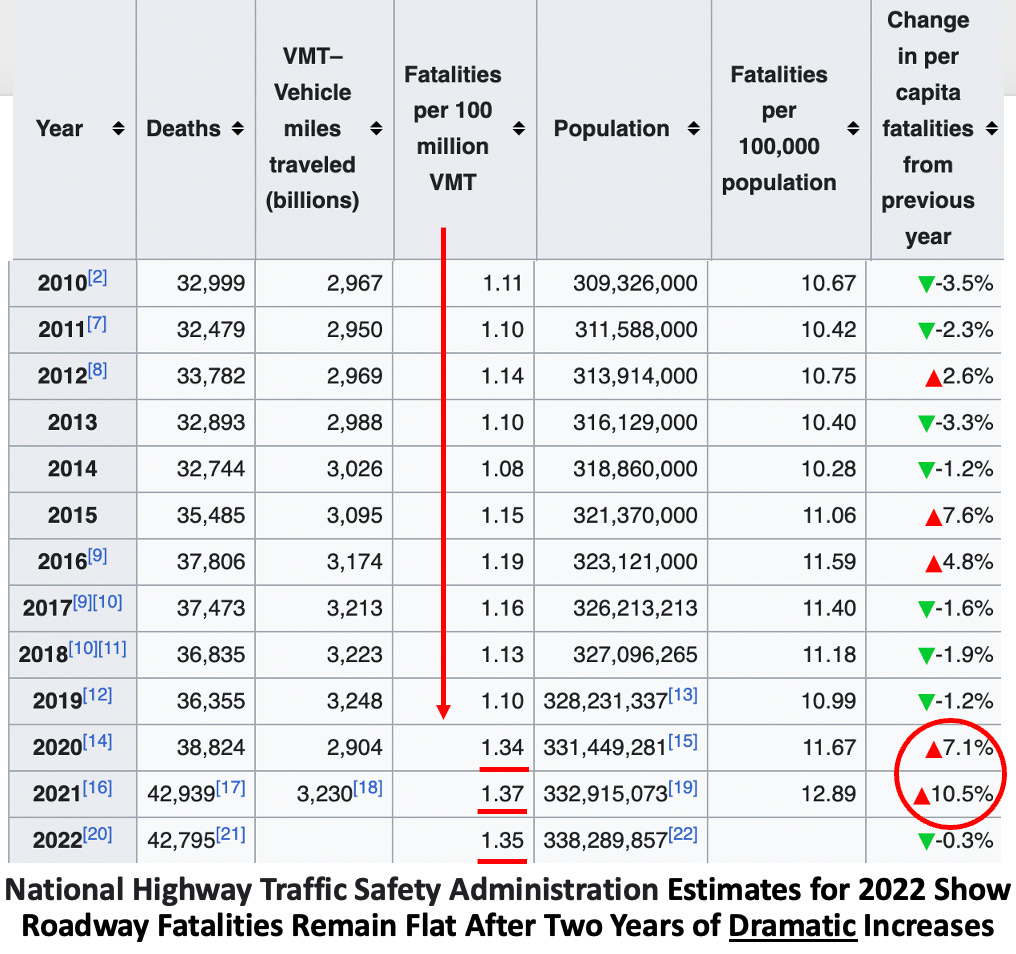
Note: after I posted the original article many of the readers stated they too had observed a significant worsening in the behavior of drivers around them. I was then pointed to this dataset, which suggests this issue was happening, but is difficult to properly assess because COVID-19 can also cause cognitive impairment and less people were driving in 2020 and because the dataset still has not been updated since 2022.
Recently, Igor Chudov was able to identify another dataset from the Netherlands which further corroborated that we were indeed facing a massive cognitive decline:
Primary care data for January to March 2023 showed that adults visited their GP more frequently for a number of symptoms compared to the same period in 2019. Memory and concentration problems were significantly more common than last year and in the period before COVID-19. Where these symptoms are concerned, the difference compared to 2019 is growing steadily in each quarter.
In the first quarter of 2023, there was a 24% increase in GP [general practioner] visits related to memory and concentration problems among adults (age 25 years and older) compared to the same period in 2020. This is evidenced by the latest quarterly research update from the GOR Network. The increase in memory and concentration problems of adults seems to be a longer-term effect of the coronavirus measures as well as SARS-CoV-2 infections.
More specifically they found:
• No increase was observed in adults under 25 years old.
• A 31% increase was observed in those 24-44 years old.
• A 40% increase was observed in those 45-74 years old.
• An 18% increase was observed in those over 75 years old.
Note: previous rounds of this survey, in addition to the cognitive issues described above, found that since 2019, the general population has also experienced worsening mental health (e.g, anxiety, depression or suicidal thoughts), sleep problems, tiredness, and cardiovascular issues (e.g., shortness of breath, dizziness or heart palpitation).
Typically, patients, less than 75 years old are unlikely to visit their doctors for cognitive issues. Taken in context with this data, it means there is a stronger case that the (massive) increases in cognitive issue for those under 75 were caused by something that happened after 2019. Additionally, since there were already a large number of visits for cognitive impairment in the elderly, the lower percentage increase is slightly misleading in quantifying the extent to which everyone was affected. For example to quote the previous report:
Primary care data showed that adults visited their GP somewhat more frequently for sleep problems in October–December 2022 than in the same period in 2019. This was particularly striking in the oldest age group (75 years and older).
Note: poor sleep is one of the primary causes of cognitive impairment (or dementia) and sadly also commonly impaired after COVID-19 vaccination.
All of this data put health officials in a bit of an awkward situation since publishing data demonstrating large scale cognitive impairment directly undermines the narrative they previous had committed themselves to. Nonetheless, the authors of the report were significantly more candid than many others before them:
The source of this increase in memory and concentration problems is unclear. A possible explanation could be that COVID-19 measures caused accelerated cognitive decline among people who were starting to have problems with memory and concentration (66 years on average).
COVID-19 was of course cited as a potential cause (which, as discussed above can sometimes cause long term cognitive impairment):
A supplementary explanation could be that some of these people have long-term symptoms after COVID-19. Various studies have shown that memory and concentration problems are common in post-COVID symptoms. Other infectious diseases, such as flu, can also cause these symptoms. However, recent studies have shown that long-term memory and concentration problems are much more common after COVID-19 than after flu. In addition, these symptoms are more common in older age groups. The figures provided by GPs are consistent with this expectation.
Fortunately, the authors acknowledged that long COVID could not be the primary explanation for what was occurring, and instead alluded to the elephant in the room—the vaccines.
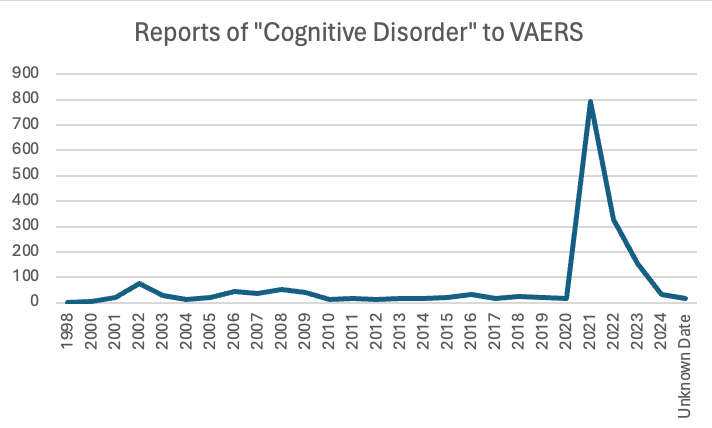
Finally, Ed Dowd has identified numerous government datasets demonstrating that widespread impairment and disability has occurred since the vaccine rollout. Likewise, VAERS detected a massive spike in cognitive issues being reported to it after the COVID vaccines hit the market.
Note: one of the key components of the COVID-19 vaccine push was to make it politically incorrect to raise any data-based objections to the vaccines, and thereby stifle any inconvenient discussions of the topic which would have exposed how dangerous these products were. Because of this, I repeatedly heard stories (like this one) of liberals (including famous ones) who had severe vaccine injuries but could not discuss them with their peers, as doing so meant being outcasted from their social group and being cut off from job opportunities, in effect placing them in a similar position to where gay men were in the early 1980s (as coming out often meant being ex-communicated by many close to you). Fortunately, things are now changing (as there are too many injuries to hide) and we are beginning to see more and more prominent individuals “come out of the closet” and admit they were vaccine injured.
Data Transparency
Making decisions has always been difficult and history is rife with catastrophic errors made by individuals who got it wrong. Because of this, a variety of solutions have been developed over the years (e.g., having a committee go through a process to decide something as it is unusual to have a leader who excels at making excellent decisions), all of which have serious short comings.
In recent years, we’ve had a push for data to become the means to making decisions. On one level, I think this is an excellent approach. For example in sales and the internet (which is where I suspect much of the push for data originated from), large amounts of data are used on a daily basis and constantly used to refine how a marketing campaign internet platform is set up so that it can maximize profits.
However, in many cases (e.g., those outside of business and sales), that same incentive to optimally utilize the data and adjust what’s being done due to the data does not exist. Because of this, while we have a large emphasis on gathering data, most of it is never utilized. For example, in medicine, we force our healthcare workers to do an immense amount of data entry, yet, we never combo the electronic health records to determine which drugs are unsafe or ineffective (which is very easy to do). I would argue this is because the healthcare system receives so much unconditional money they have no incentive to produce better results and because the pharmaceutical industry receives so much money for toxic drugs, it has every incentive to keep them on the market.
In order to enshrine this paradigm, industry had to both create the mythology that data should both be viewed as the ultimate authority we must all be subservient to, but simultaneously not be something that is publicly available. This in turn was done by arguing that data was “costly proprietary information and intellectual property must be protected” or that it “contained personal health information which could not ethically be disclosed to protect the patients.”
In turn, science has very much become us being expected to trust the team of “experts” who analyze a dataset, and not surprisingly, this process lends itself to corruption.
For example, the only publicly available vaccine injury database VAERS, exists because activists forced it to be required by law, and ever since it was made, the government (along with the medical establishment and the media) has done everything it can to undermine VAERS (discussed further here). Because VAERS reputation had been sullied, for the COVID vaccines, a new monitoring system, V-Safe, which was designed to address the short comings of VAERS was created. However, before long, activists discovered that V-safe did not allow the majority of adverse reactions to be reported in it, and furthermore would not make the data available for outside analysis. Instead, we were given access to a Lancet publication which concluded that:
Safety data from more than 298 million doses of mRNA COVID-19 vaccine administered in the first 6 months of the US vaccination programme show that most reported adverse events were mild and short in duration.
Reports of seeking medical care after mRNA vaccine were “rare”… Serious adverse events, including myocarditis, have been identified following mRNA vaccinations; however, these events are rare. Vaccines are the most effective tool to prevent serious COVID-19 disease outcomes and the benefits of immunisation in preventing serious morbidity and mortality strongly favour vaccination.
Through lawsuits, activists were eventually able to obtain the V-safe data where they then discovered the above study had lied and there were a lot of serious issues within that database. For example, the above article claimed 0.8-1.0% of vaccine recipients required medical care, whereas the raw V-safe data show 7.7% did—on average 2.7 times, which meant that every 4.8 vaccinations caused one medical visit.
Likewise, throughout the pandemic, we had almost all of the scientific journals refuse to publish anything which challenged the narrative (e.g., I’ve been in touch with numerous teams that have run into an endless number of roadblocks to publish contrarian data). Yet, simultaneously, those journals were willing to contort the existing (poor quality) data as much as possible if that supported the narrative (e.g., Pierre Kory has shown how multiple studies whose data demonstrated ivermectin benefitted patients concluded ivermectin was useless and then widely promoted for having debunked ivermectin).
Similarly, Deborah Birx and Anthony Fauci were essentially responsible for the disastrous COVID-19 response (e.g., useless but harmful mass testing, masking and lockdowns), as both within the White House and in the (fawning) media, they relentlessly and successfully pushed for those approaches regardless of how much protest they met. As both news clips and eye witnesses testimonies showed, Fauci and Birx constantly used “the data” to justify their their approach (e.g., when challenged, Birx would often say “I’m all about the data” while Fauci always cited “the data” whenever he advocated for a policy on national television).
However, Scott Atlas (who was with them on the White House COVID-19 task force) discovered that they both never presented scientific papers to the task force, lacked the ability to critically evaluate scientific research, they did not understand basic medical terminology, they would make patently absurd and non-sensical interpretations of their data, and adamantly refused to consider any of the data which challenged their narratives. In many cases, what he witnessed was so absurd he likened it to being in the Mad Hatter’s tea party from Alice and Wonderland, whereas I felt it was a real life version of this iconic Whitehouse scene from Idiocracy.
Because of the widespread lack of data transparency, a few different approaches exist.
First many (e.g., Drs. Peter Gøtzsche and Malcolm Kendrick) have gradually become experts in “data forensics” and being able to identify the tricks the pharmaceutical industry uses to doctor research so that the data always ends up supporting the sponsor’s desired conclusion. What I personally find depressing about this is that a fairly repetitive playbook is used to doctor studies, but the top medical journals consistently turn a blind eye to this, always publish that deceptive research, and in most cases refuse to correct it once the public points out the fraud.
Second, many (e.g., Steve Kirsch) argue that if data is not made publicly available, one must assume it’s incriminating and the data’s owners are lying about what’s in it (e.g., that the COVID vaccines are safe and effective). For example, for decades activists have been trying to get access to the data from the CDC’s Vaccine Safety Datalink (as it has the information which could definitively say if vaccines are safe or effective) but they’ve had no success—which in turn suggests that database is full of incriminating information for the vaccine program. Likewise, given the disconnect between what I was seeing with COVID-19 vaccine injuries and what the government was reporting (the only message we ever heard was “safe and effective!”) it was clear to me the government had very bad data and had made the decision to do whatever could be done to cover it up—a prediction which sadly has continued to hold true.
Third, we have to rely upon publicly available datasets which happened to capture the effects of vaccination programs (e.g., the one which tracks annual disability rates in the USA registered a huge spike after the COVID-19 vaccines hit the market). Unfortunately, while these clearly show that an issue exists which needs to be investigated, they do not definitively prove causality, and hence are often dismissed on that basis (much like VAERS is).
Fourth, we have to rely upon whistleblowers. Unfortunately, when this happens, the national government typically targets them for violating “patient confidentiality.” For instance, when a New Zealand whistleblower released fully anonymized data showing the vaccines were killing people, his government charged him with crimes carrying a maximum seven year prison sentence.
Note: the most recent example of government persecution of whistleblowers happened in Texas, where in February 2022, Texas’s government declared providing gender transitions to minors constituted child abuse, and June 2023, outlawed it. In response to this, in March of 2022, one of the largest Children’s hospitals in Texas (and where Peter Hotez exerts a significant amount of influence) announced it would stop providing transgender hormonal therapies. This however was a lie, so in April 2023, a concerned surgeon who had previously worked at the hospital convinced the hospital to give him access to their medical records, and then leaked anonymized medical records demonstrating that the hospital was continuing these practices, as in his opinion, under Texas law, this was child abuse he was required to report. In response to this, the Biden administration (not Texas) charged him with four felonies which carry a maximum penalty of 10 years in prison, which is very different from how other HIPPA violations have been handled. Likewise, more recently, after another nurse at the hospital exposed that the hospital was committing Medicaid fraud by billing for transgender care but labeling it as something else (as Texas’s Medicaid program does not permit for those practices to be reimbursed), after which the FBI was sent to interrogate (and likely intimidate) the nurse.
All of this hence leaves us in a very disorienting position—how do we know who to trust? In turn, I would argue one of the largest reasons so many people trust the audacious lies the government tells us is because the alternative (not knowing who or what to trust) is arguably even worse.
In my own case, I’ve developed a very simple rule for navigating the scientific literature (and many other sources of information as well).
Step 1. Determine the biases and conflicts of interest of the publication source (e.g., most medical journals and their editors take a lot of money from the pharmaceutical industry and hence do not want to upset their sponsors—an issue we sadly also see in the mainstream media).
Step 2. Determine if the conclusion of a published study agrees with, challenges, or is relatively neutral to it’s publisher’s bias.
Step 3 Use this formula:
• Agrees with publisher—high likelihood the study is wrong and it’s probably not worth your time to look into it.
• Disagrees with publisher—high likelihood the study is correct and that a very high bar had to be passed for it to be published (along with significant pressure being exerted behind the scenes).
• Relatively neutral for the publisher—you can take the paper at face value when you analyze its methods and conclusions to see if they had a reasonable way to derive their conclusion. Additionally, while the most prestigious medical journals are corrupt, this category is the one area they shine in and often ensure high standards were met for publication.
South Korea’s Data
In November 2023 and March 2024, some very interesting data emerged from a team of South Korean researchers where they looked at the electronic health records for a quarter and then half of the population in Seoul (2.2 million for the first study and then 4.3 million for the second) and then compared the rates of a variety of new (non-serious) medical conditions in those vaccinated and unvaccinated over three months. From this, they found a variety of medical conditions had a significant increase in the vaccinated. Those increases were as follows (with a range existing depending on how long after vaccination they were compared and which COVID vaccines they received).
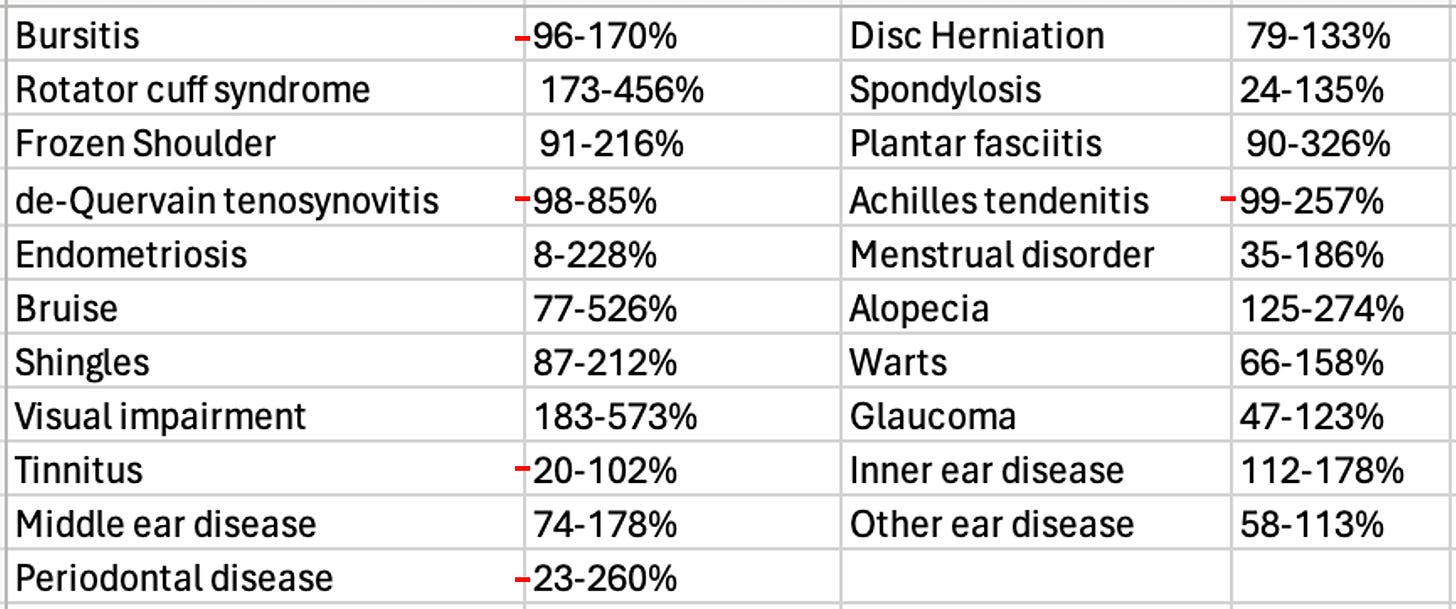
This was essentially a dataset we had been trying to get for over 2 years and it matched what we’d seen (e.g., many of these conditions such as shingles and alopecia [hair loss] appear to be strongly linked to vaccination). In turn, it both demonstrated that the vaccines were causing massive harm to society as millions of Americans suffer from these diseases and hence millions more developed them.
Unfortunately, after I analyzed them, I realized it was not appropriate for me to discuss them here as they were pre-prints rather than published articles, which either meant that they had fraudulent data (as it was quite extraordinary they got access to this data) or they were too politically incorrect for any journal to want to publish. While I felt the latter was much more likely, I was not sure which is was, so I avoided publishing that article (which was hard to do given how much time I’d put into it) as I did not want to fall into the trap of promoting something because it promoted my pre-existing biases and then misleading the audience here.
Note: if for some reason these studies disappear I have included the pre-prints below.
We hence tried to reach the authors (no success) and I patiently waited for the articles to leave the preprint server (which has still not happened).
However, recently. three other studies were published by the same team using the same dataset. The first one, (also from March 2024) analyzed the increase of ten common autoimmune disorders (autoimmune hepatitis, ankylosing spondylitis, hashimoto thyroiditis, hypertension, inflammatory bowel disease, primary biliary cholangitis, rheumatoid arthritis, graves, vitiligo, lupus).
This one stated only vitiligo was increased (by 174%), so it seemed plausible to me it could have been published, as it made a token admission the vaccines were bad (as they had a rare side effect from a disease most people don’t know about). Then, when I looked at the data, I noticed a few of the other conditions appeared to have also increased. In turn, since those increases weren’t mentioned in the article, I took that as a sign the article was deliberately omitting incriminating information from its conclusion so it could make it to publication (this happens a lot). Additionally, I was surprised the authors did not evaluate for polymyalgia rheumatica, as this seems to be one of the autoimmune disorders most distinctively associated with vaccination.
That article made me more confident the initial results were real—however since it was published in an obscure journal, I reserved judgement on it. Recently however, two very important ones came out.
Two weeks ago, the first was published in Nature (one of the top medical journals). It found that COVID vaccination resulted in a 68% increase in depression, a 44% increase in anxiety, dissociative, stress-related, and somatoform disorders, a 93.4% increase in sleep disorders, a 77% decrease in schizophrenia, and a 32.8% decrease in bipolar disorder. I was really surprised to see this be published, and took it as a sign there may have been a decision made to begin disclosing some of the harms of vaccination in the official medical literature. Additionally, I took this as an indication that this was an indirect admission neurologic issues also followed vaccination (due to the strong link between neurologic and psychiatric symptoms).
Note: the previously mentioned Israeli survey found that 4.5% of those who received a vaccine developed anxiety or depression, and 26.4% who already had either experienced an exacerbation of it.
Around the same time (three weeks ago) another article was published in a mainstream journal (or to be more exact “accepted for publication”). It analyzed individuals over 65 and found COVID vaccination increased the risk of mild cognitive impairment 138% and the risk of Alzheimer’s by 23%, and a smaller increase in vascular dementia and Parkinson’s disease the authors did not deem to be significant.
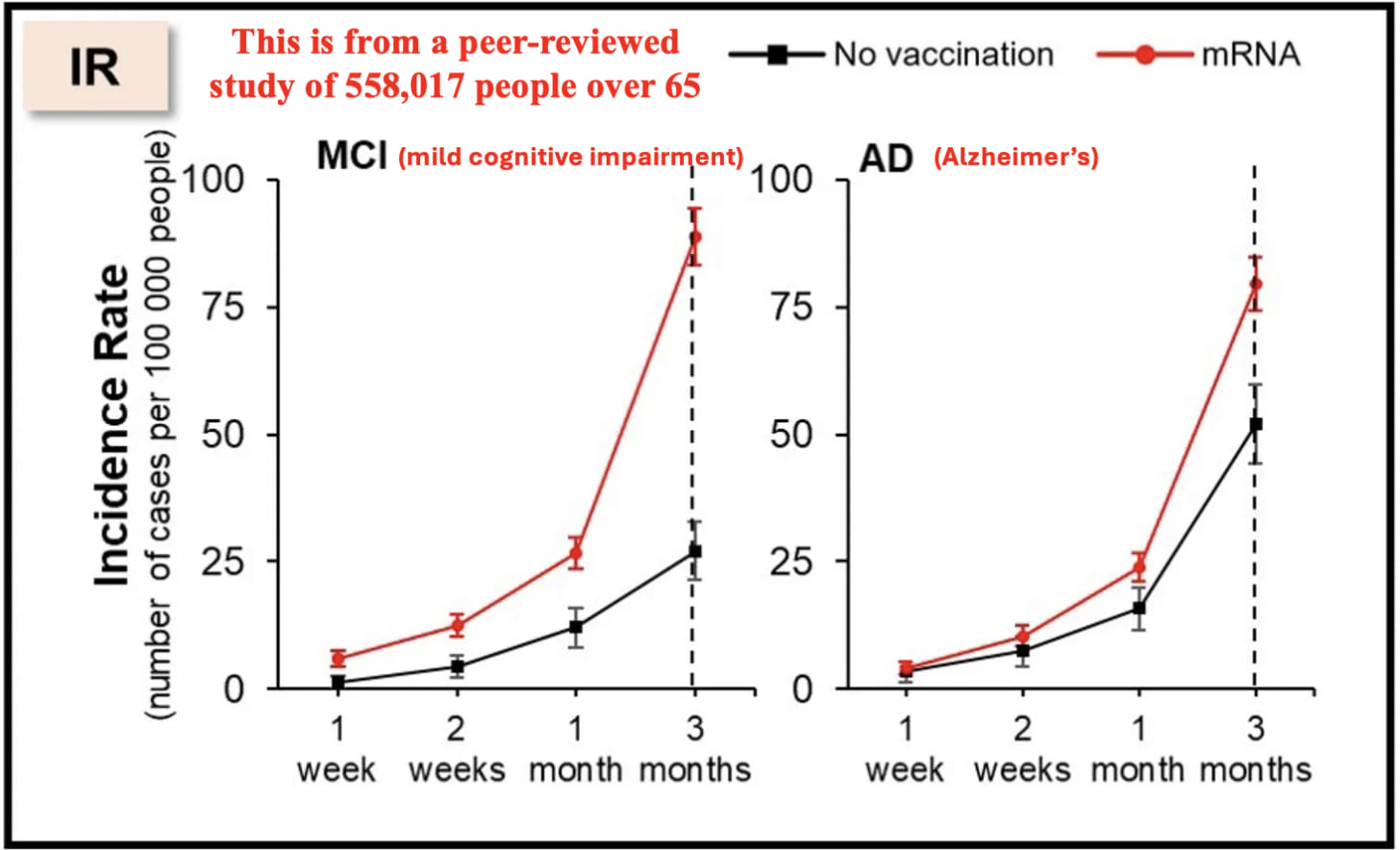
To put this in context, given that America spends over 300 billion dollars per year on Alzheimer’s disease, this single datapoint effectively means that the COVID vaccines cost the United States around 100 billion dollars. Additionally, as the authors only tracked the difference over 3 months (and it increased over time as these are both progressive diseases), the actual cost is likely greater, especially given that the elderly keep on receiving boosters. Likewise, it also makes a very strong argument for anyone who believes the vaccines damaged their cognition that this indeed happened.
Why Are The Vaccines Causing Cognitive Impairment?
My specific interest in studying spike protein vaccine toxicity arose because I suspected I would see many similarities to other pharmaceutical injuries I had observed previously and treatments that had developed for those injuries could be used to treat COVID-19 vaccine injuries. On Substack, I’ve tried to focus on explaining the areas that I believe are the most important to understanding this, zeta-potential, the cell danger response (CDR) and the treatments for Alzheimer’s disease. Note: Each of these is interrelated with and often causes the others.
Zeta Potential: Zeta potential (explained in detail here) governs if fluid in the body clumps together (e.g., forming a clot) or remains dispersed and capable of freely flowing. Additionally, it also influences if proteins will stay in their correct formation or misfold and clump together (with Alzheimer’s disease being characterized by misfolded proteins in the brain). Many different issues (discussed here) emerge when fluid circulation (be it blood, lymph, interstitial fluid or cerebrospinal fluid) becomes impaired. Since the spike protein is uniquely suited for impairing zeta potential, we have found restoring zeta potential (discussed here) often is immensely helpful during COVID-19 infections and for treating COVID-19 vaccine injuries. Many of those approaches in turn were initially developed from working with other vaccine injuries and cognitive decline in the elderly.
Note: the spike protein also has a prion forming domain, and many believe its responsible for the highly unusual amyloid (fibrous) blood clots seen in COVID-19 victims. Additionally, the COVID vaccines have been linked to extremely rare (and fatal) protein misfolding disorders such as the rapid dementia caused by CJD (discussed further here).
Cell Danger Response (CDR): When cells are exposed to a threat, their mitochondria shift from producing energy for the cell to a protective mode where the cell’s metabolism and internal growth shuts down, the mitochondria release reactive oxygen species to kill potential invaders, the cell warns other cells to enter the CDR and the cell seals off and disconnects itself from the body. The CDR (explained further here) is an essential process for cellular survival, but frequently in chronic illness, cells become stuck in it rather than allowing the healing response to complete.
Note: one common cause of impaired cognition are neurons becoming stuck in the CDR and hence not performing their cognitive tasks.
Understanding the CDR is extremely important when working with complex illnesses because it explains why triggers from long ago can cause an inexplicable illness, and why many treatments that seem appropriate (specifically those that treat a symptom of the CDR rather than the cause of it) either don’t help or worsen the patient’s condition. Many of the most challenging patients seen by integrative practitioners are those trapped within the CDR, but unfortunately, there is still very little knowledge of this phenomenon.
My interest was drawn back to the CDR after I realized that one of the most effective treatments for long COVID and COVID-19 vaccine injuries was one that systemically treated the CDR. Since many of the therapies that have been developed to revive nonfunctional tissue was developed by the regenerative medical field, I wrote an article describing how these approaches are applied to restore localized regions of dysfunctional tissue (which is sometimes needed to treat vaccine injuries) and another on the regenerative treatments that treat systemic CDRs (and are more frequently needed for vaccine injuries).
Alzheimer’s Disease (AD): since AD is one of the most costly disease in America, billions of dollars are spent each year in researching a cure for it. This research (which began in 1906) has had a very narrow focus on removing amyloid from the brain, and since the production of amyloid is a protective response from the brain, the decades of work to remove it have gone nowhere. Nonetheless, the FDA is presently working hand in hand with the drug industry to push forward ineffective, quite dangerous but highly profitable treatments for AD.
Remarkably, effective treatments do exist for AD and my colleagues have developed a few different methods that have successfully treated the condition. Additionally, one neurologist, Dale Bredesen developed a method for reversing AD that he proved worked in mulitiple publications (included a recent 2022 clinical trial)—something which no one else has done, but remarkably has been almost completely ignored by the neurological field.
All of these successful approaches utilize the following principles:
• Restore both the blood flow to the brain and the lymphatic drainage from it (which safely removes amyloid plaques). This often requires restoring the physiologic zeta potential and having a healthy sleep cycle. Additionally, AD is commonly linked to damage to the lining of the brain’s blood vessels, which is unfortunate because one of the most frequent toxicities of the spike protein is injury to the blood vessels (which has been shown in many autopsies—including within the brain).
• Treating the CDR (which causes chronic inflammation) and reactivating brain cells that became trapped in an unresolved CDR (which amongst other things requires reclaiming a healthy sleep cycle, providing the nutrients the brain needs to sustain itself, and mitigating the damage of neurotoxins like inhaled anesthetics).
Note: Bresden’s approach also emphasizes the importance of addressing chronically elevated blood sugar or insulin levels.
One of the most important things to recognize about AD is that it is a slowly worsening disease which often progresses over decades. In the early stages of AD (where it is the most reversible), minor cognitive changes occur, which (when possible to autopsy) correlate with tissue changes within the brain. In rarer instances, individuals can instead have a rapidly progressing form of Alzheimer’s (e.g., from Lyme) which strikes at a younger age and is often linked to the toxin exposure. Given how quickly the increase in AD appeared in both the patients I know and this dataset, I suspect it’s very likely the mechanisms behind the rapidly progressing forms of AD play a key role in the cognitive impairment and dementia we are seeing from these vaccines.
Conclusion
Many of the most successful people I know are willing to go against a crowd and act in spite of being afraid (e.g., they resisted the peer pressure to get the vaccine because they felt it was a good idea). Likewise, rather than looking to an authoritative source for advice, they tend to create preliminary assessments of what’s going on based on the limited data that’s available to them, and then act on it rather than waiting for a clear and definitive answer (or at least a safe one) to present itself.
In turn, as I’ve gotten to know many of the prominent dissidents in this movement, I’ve found they all had those traits in common (which likewise many of my extraordinary medical mentors did as well). For example, Steve Kirsch used this capacity to become a successful Silicon Valley entrepreneur. When the vaccines came out, he “trusted the science,” and immediately got one, but before long noticed numerous people he knew had had severe injuries from them, and rather than be in denial about it, recognized that chain of injuries was statistically impossible, began digging into it, realized the existing data showed we had a huge problem, and then began speaking out on it despite the fact much of the (left wing) peer group he’d belonged to for decades disowned him for doing so.
In my own case, for the COVID vaccines, I had initially come in with expectation (which formed as the virus broke out in Wuhan) that whatever “emergency” vaccine was pushed for it would have significant issues and the adverse events would be by and large covered up by the government (or only “discovered” years down the line). In turn, I concluded it was far more preferable for me to feel confident I could treat the infection when I eventually got it and develop natural immunity than it was to take a risk with the vaccines.
However, once I began seeing a high number of red flags the moment the vaccines hit the market, I realized that I had made a big miscalculation and these things were incredibly dangerous so I needed to shift my focus to preventing people from being harmed by them.
Furthermore, I took the bell curve theory into account and assumed that if I was seeing occasional deaths or severe cognitive degeneration following vaccination, it was likely that far more cases of cognitive impairment were occurring, and as this recent Korean study shows, that is indeed the case.
It is thus both quite tragic and remarkable that we now have a leadership which has so little accountability to produce quality results that things like the basic scientific process (which helped our country become one of the most powerful nations in history) is being completely disregarded and replaced with a dogmatic system which refuses to consider basic data points which more and more are proving themselves to be immensely costly to our nation.
Everything we are seeing now was incredibly predictable and represented a systemic failure in our system and a profound societal decline that must be reversed if we want our nation to be something which continues to provide the basic things we have taken for granted from it for most of our lives. I am especially worried as prior to COVID-19, our society was already struggling to reverse this decline, and since that time, we’ve been hit by a wave of cognitive impairment which can only further diminish our ability to address this.
College of Physicians and Surgeons of Saskatchewan suspends doctor for prescribing Ivermectin, fines him $44,784
Licence of Sask. doctor who prescribed Ivermectin for COVID-19 to be suspended
Dr. Tshipita Kabongo faced two sets of charges relating to unprofessional conduct, brought by the College of Physicians and Surgeons of Saskatchewan.
Author of the article: Brandon Harder
Published June 17, 2024
Regina doctor Tshipita Kabongo has admitted to unprofessional conduct in relation to two sets of charges brought against him by the oversight body for Saskatchewan physicians.
That’s according to Bryan Salte, associate registrar for the College of Physicians and Surgeons of Saskatchewan (CPSS).
Kabongo had one such charge brought against him in March of 2023 in relation to his failing to know and/or follow the CPSS Policy on Complementary and Alternative Therapies when he prescribed Ivermectin, an anti-parasitic drug, to treat COVID-19.
He also faced four additional professional charges, brought against him in March of 2024. Of those, three pertained to his work with specific patients, alleging he “failed to maintain the standard of practice of the profession,” while the fourth charge was in relation to billing for his services.
The 2024 charges also made reference to inappropriate prescription of Ivermectin, as well as cannabinoids, benzodiazepines, Vitamin B12, and supplements.
Charges brought by that oversight body are not criminal charges but pertain to conduct that does not comply with the rules that govern its members.
Salte advised, via email, that a hearing was held with regard to Kabongo’s matters in June, and a penalty was imposed on him.
With regard to penalty, the CPSS council decided Kabongo is to receive a written reprimand.
In addition, his licence is to be suspended for one month, starting Aug. 1, 2024.
He is to practice only under the supervision of “a duly qualified medical practitioner approved by the Registrar.”
“The requirement for supervision will continue until the Registrar concludes that Dr. Kabongo is no longer required to practise under supervision,” the council decision states.
The supervisor is to provide the CPSS with reports as to the status of Kabongo’s practice.
Kabongo is also directed to pay costs associated to the investigation and the hearing in the amount of $44,783.72. This amount is to be paid in 24 equal instalments, beginning August 1.
If he fails to pay these costs as required, his licence is to be suspended until he pays in full.
— with files from Pam Cowan
======
Regina doctor suspended for prescribing Ivermectin for COVID
Saskatoon / 650 CKOM
June 18, 2024
A Regina doctor has been suspended from practicing for a month this summer for prescribing Ivermectin for COVID-19.
The Saskatchewan College of Physicians and Surgeons found that over two years, between April 2020 and March 2022, Tshipita Kabongo prescribed the drug as either a treatment or to prevent COVID-19 at his practice in Regina
He was found to have engaged in unprofessional conduct.
In a decision released this month, the college said Kabongo failed to follow the its policy on alternative therapies, which says patients have a right to make decisions about their health care but doctors who choose to use complementary or alternative therapies have to do so in a way that’s informed by medical evidence and science.
“It is unethical to engage in or to aid and abet in treatment which has no acceptable scientific basis, may be dangerous, may deceive the patient by giving false hope, or which may cause the patient to delay in seeking conventional care until his or her condition becomes irreversible,” the policy states.
The college’s decision on Kabongo said one or more of the prescriptions he gave out weren’t medically necessary, he failed to recommend other evidence-informed treatment options, and he didn’t properly document the prescriptions in medical records.
As a result, Kabongo will be suspended from practising for one month in August. He’ll have to have someone supervise him when he returns to practising, and he’ll have to pay the cost of the investigation and hearing, which added up to $44,783.72.
Ivermectin is a drug meant to treat parasites as an oral medicine and rosacea as a topical medication. However, some on social media promoted it as a cure for COVID during the pandemic which began in 2020.
In the fall of 2021, Health Canada and several medical groups in Saskatchewan put out public messages warning people against the use of Ivermectin for COVID, particularly the stronger and more dangerous veterinary formulation.
“There is no evidence that Ivermectin works to prevent or treat COVID-19 and it is not authorized for this use. To date, Health Canada has not received any drug submission or applications for clinical trials for Ivermectin for the prevention or treatment of COVID-19,” explained a public notice from Health Canada issued in October, 2021.
A memo issued around the same time by the College of Physician and Surgeons, along with several other Saskatchewan medical groups, said that while there have been studies on Ivermectin, the study limitations like sample sizes and confounding factors mean that conclusions couldn’t be drawn, and so Ivermectin was disapproved of for the treatment or prevention of COVID-19.
DR. WILLIAM MAKIS MD | JUNE 23, 2024:
This is yet another example of criminal behavior by a College, this time by the College of Physicians and Surgeons of Saskatchewan.
It is time to start filing criminal charges against College Officials.
These Colleges, through their actions, have killed thousands of Canadians already and if Canadians don’t take the Colleges back, the Colleges will continue to take many more lives in the future.
Autopsy Study Linking COVID Shots to Deaths Finally Published, After Lancet Removed It
‘Unprecedented Censorship’
By Brenda Baletti, Ph.D. | The Defender | June 25, 2024
A systematic review of autopsy-related literature following COVID-19 vaccination found that 73.9% of the 325 deaths were linked to the shots, suggesting “a high likelihood of a causal link” between the shots and death.
The review, published on June 21 in the peer-reviewed journal Forensic Science International, was first posted on July 5, 2023, on The Lancet preprint server, SSRN, an open access research platform.
However, Preprints with The Lancet removed the study from the server within 24 hours, “because the study’s conclusions are not supported by the study methodology,” according to a statement on the SSRN page, The Daily Sceptic reported.
The paper had been viewed over 100,000 times.
Authors submitting papers to Lancet journals for review post their work to the SSRN to make it publicly available while it undergoes peer review.
University of Michigan researcher Nicolas Hulscher authored the study, along with Dr. William Makis, Peter A. McCullough, M.D., MPH, and several of their colleagues at The Wellness Company.
The authors said autopsies should be performed on all deceased people who have received one or more COVID-19 vaccines and that vaccinated people should be clinically monitored for at least one year following vaccination. They called for further research into the issue.
McCullough told The Defender :
“Our study faced unprecedented censorship from the Lancet SSRN preprint server and was taken down after massive downloads by concerned physicians and scientists across the globe.
“Lancet did not want the world to know that among deaths that were autopsied after COVID-19 vaccination, independent adjudication found that the vaccine was the cause of death in 73.9% of cases.
“The most common fatal vaccine syndromes were myocarditis and blood clots. Investigative journalists should probe Lancet to uncover who was behind unethical suppression of critical clinical information to the public.”
Makis announced the publication of the “Lancet censored” paper on X last week.
McCullough also noted the project was approved through the University of Michigan’s School of Public Health and used a standard scientific methodology to evaluate the studies for inclusion in the review.
The authors subsequently posted on the Zenodo preprint server, while the review underwent peer review at Forensic Science International. It was downloaded over 125,000 times.
Preprint servers were established to address inefficiencies in academic publishing. The peer-review process typically takes months or more, delaying the real-time sharing of scientific findings with the public.
Also, many journals are proprietary and can only be accessed through expensive personal or institutional subscriptions.
Preprint servers offer a location for scientific reports and papers to be available to the public while the paper goes through peer review — making scientific findings available immediately and for free and opening them up to broader public debate.
There is no peer-review process for preprints, although there is a vetting process.
Preprint servers are intended to be neutral and to post all research conducted with a clearly explained and reproducible methodology, according to Vinay Prasad, M.D., MPH, who reported last year that his COVID-19-related work was subject to similar censorship.
Thirty-eight percent of Prasad’s own lab’s submissions to preprint servers were rejected or removed — even though those same articles eventually were published in journals and extensively downloaded.
Preprint servers have become “gatekeepers” for what science gets published, Prasad said.
When The Lancet took down the paper, The Daily Sceptic’s Will Jones wrote that given the credentials of the authors, “It is hard to imagine that the methodology of their review was really so poor that it warranted removal at initial screening rather than being subject to full critical appraisal. It smacks instead of raw censorship of a paper that failed to toe the official line.”
The Lancet Preprints did not respond to The Defender’s request for comment.
Findings have wide-ranging implications
The authors searched the published literature archived in PubMed and ScienceDirect for all autopsy and necropsy — another word for autopsy — reports related to COVID-19 vaccination, where the death occurred after vaccination.
They screened out 562 duplicate studies among the 678 studies initially identified in their search. Other papers were removed because, for example, they lacked information about vaccination status.
Ultimately 44 papers containing 325 autopsies and one necropsy case were evaluated. Three physicians independently reviewed each case and adjudicated whether or not the COVID-19 shot was the direct cause or contributed significantly to the death reported.
They found 240 of the deaths (73.9%) were found to be “directly due to or significantly contributed to by COVID-19 vaccination” and the mean age for death was 70.4 years old.
Primary causes of death included sudden cardiac death, which happened in 35% of cases, pulmonary embolism and myocardial infarction, which occurred in 12.5% and 12% of the cases respectively.
Other causes included vaccine-induced immune thrombotic thrombocytopenia, myocarditis, multisystem inflammatory syndrome and cerebral hemorrhage.
Most deaths occurred within a week of the last shot.
The authors concluded that because the deaths were highly consistent with the known mechanisms for COVID-19 vaccine injury, it was highly likely the deaths were causally linked to the vaccine.
They said the findings “amplify” existing concerns about the vaccines, including those related to vaccine-induced myocarditis and myocardial infarction and the effects of the spike protein more broadly.
They also said the studies have implications for unanticipated deaths among vaccinated people with no previous illness. “We can infer that in such cases, death may have been caused by COVID-19 vaccination,” they wrote.
The authors acknowledged some potential biases in the article.
First, they said, their conclusions from the autopsy findings are based on an evolving understanding of the vaccines, which are currently different from when the studies evaluated were published.
They also noted that systematic reviews have bias potential in general because of biases that may exist at the level of the individual papers and their acceptance into the peer-reviewed literature.
They said publication bias could have affected their results because the global push for mass vaccination has made investigators hesitant to report adverse events.
They also said their research did not account for confounding variables like concomitant illnesses, drug interactions and other factors that may have had a causal role in the reported deaths.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Key Talking Points on Current Bird Flu Situation
Knowledge is Powerful Amidst Government False Narrative
By Peter A. McCullough, MD, MPH | Courageous Discourse | June 24, 2024
The McCullough Foundation, informative update on the current H5N1 global situation has received considerable attention and garnered valuable feedback. Here are the key takeaways:
- Practice of culling (mass destruction of entire healthy flocks) when a PCR test is found positive to “eradicate” the virus is futile and may work to constrain the food supply. The current strain H5N1 clade 2.3.4.4.b is not thus far causing necropsy or radiographic confirmed fatal pneumonia in birds or mammals.
- H5N1 host range expansion into migratory birds and mammals likely occurred as a result of gain-of-function serial passage research and a lab leak [or release].
- Increased transmissibility of H5N1 has a tradeoff of decreased virulence. Using legacy human mortality rates from cases in Southeast Asia is not appropriate. The US has never had a fatal human case of bird flu.
- Fear-mongering promulgated by the Bio-Pharmaceutical Complex is designed to promote mass vaccination of animals and humans with lucrative pre-purchased contracts to the vaccine manufacturers and their NGO backers. Mass vaccination into a highly prevalent pandemic promotes resistant strains of the virus in the vaccinated.
- If human-to-human spread occurs in the future as expected by many, it will be the product of gain-of-function research that has gone on for years with the goal of creating harm to human populations.
- Be prepared with early prevention and treatment strategies on hand. Courageous Discourse has covered dilute iodine nasal sprays and gargles, oseltamivir, hydroxychloroquine, and other antivirals. The Wellness Company has extended its Contagion Kit to cover the case of serious human avian influenza in the event it occurs.
Chinese Single Immunization with H5N1 Virus-like Particle Vaccine Protects Chickens Against H5N1 Influenza but Enables More Viral Shedding
By Peter A. McCullough, MD, MPH | Courageous Discourse™ | June 22, 2024
Poultry farmers are finding out that culling and vaccination of poultry may be futile as migratory water fowl spread H5N1 from farm to farm.
Kong, et al, from College of Veterinary Medicine, South China Agricultural University, Guangzhou, People’s Republic of China, tested a new poultry vaccine on 10 chickens. While the new product protected the birds from a lethal dose of the virus, the chickens retained it in the nasopharynx and were able to shed the virus theoretically to more animals.
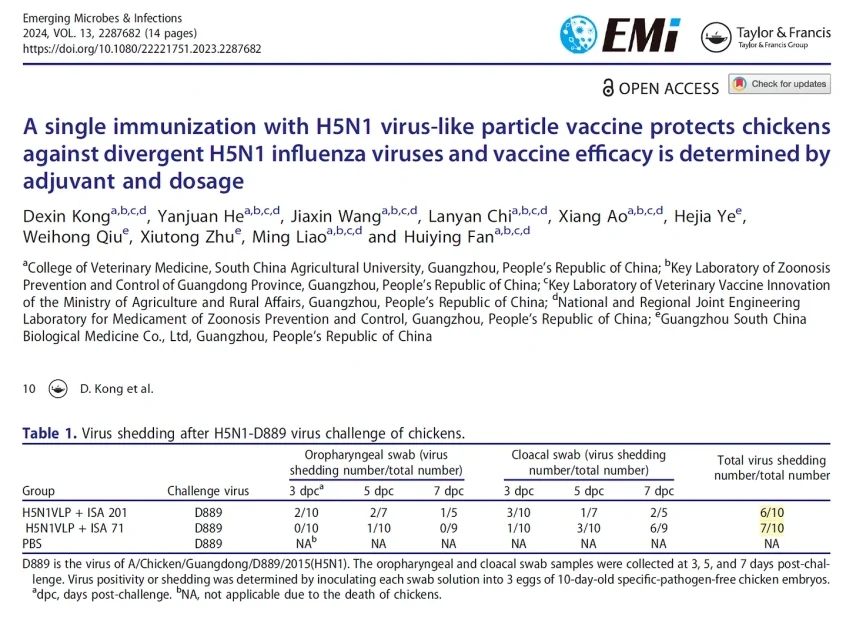
Kong D, He Y, Wang J, Chi L, Ao X, Ye H, Qiu W, Zhu X, Liao M, Fan H. A single immunization with H5N1 virus-like particle vaccine protects chickens against divergent H5N1 influenza viruses and vaccine efficacy is determined by adjuvant and dosage. Emerg Microbes Infect. 2024 Dec;13(1):2287682. doi: 10.1080/22221751.2023.2287682. Epub 2023 Dec 30. PMID: 37994795; PMCID: PMC10763850.
It appears the only method that will remain for farmers is to allow for natural immunity with wave after wave of bird flu expected as mallard ducks and other species spread H5N1 around the globe. Mass vaccination of birds and humans appears ill-advised with current products.
Featured Video

Alon Mizrahi: ‘Israel Must Be Dismantled’
or go to
Aletho News Archives – Video-Images
From the Archives
Allies Don’t Need Lobbies
By Jay Knott | Dissident Voice | September 24, 2013
In a recent article on Counterpunch, Rob Urie defended the traditional Marxist analysis of US policy in the Middle East. He argues that support for Israel is driven primarily by economic interest, not the Jewish lobby.
He starts by paying tribute to the idea that Western societies are uniquely racist. He says that the “Western narrative” claims there is an “Arab character”, and that this is “antique racist blather”. He gives no definition of these terms. Further, he establishes his credentials as part of the dominant current in the American left by claiming that “over a million people in Iraq died so ‘we’ in the West can drive SUVs.”1
When he tries to criticize bourgeois economics, he makes it clear he doesn’t understand the developments it has made since Marx’s day, using the mathematical discipline known as “game theory”. He dismisses the basic abstraction of economic theory, the idea of the rational individual, on the grounds that it is “devoid of history, culture and political context”. But abstractions are always devoid of something.
He defends a more concrete economic theory, mostly Marxist, with some input from another theorist of capitalist crisis, Hyman Minsky. This concrete theory leads him to the view that US activity in the Middle East is primarily driven by rational capitalist motives, the need to secure a supply of oil.
“Taking the totality of circumstance — former oil company executives launching war on an oil rich nation on a pretext they publicly proclaimed they didn’t believe shortly before taking office — and that upon launching their war proved to be non-existent, requires a willingness to overlook the obvious — that the war on Iraq was for oil, that is difficult to support.”1
Perhaps I’ve misunderstood him, but based on what he says in the rest of the article, this convoluted sentence seems to argue that, because president Bush and vice-president Cheney attacked Iraq on false premises, and they also said it was all about oil, and they are former oil executives, and Iraq has a lot of oil, it’s difficult to deny US attacks on Iraq are all about oil.
In fact, it’s not hard at all. As Urie points out, at times Bush and co. said that attacking Iraq was “protecting the world’s supply of oil.”1 But, as he also points out, they are congenital liars. Why should we believe them when they say they are trying to “protect” the oil supply? Protect it against what? When politicians “admit” attacks on Middle Eastern countries are wars for oil, they are parroting the neo-con party line, feeding the public, both left and right, with a plausible-sounding pretext. For right-wingers, “it’s a war for oil” is a reason to support war, and for leftists, it’s a way to feel better by complaining impotently about corporate greed. Both approaches help the war drive. … continue
Blog Roll
 Aletho News
Aletho News- US vs Iran: Kharg Island Talk — Bluff or Escalation? Ex-Military Officer Weighs In
- Zelensky unnecessarily involves Ukraine in the Middle East crisis
- Turkish tanker blacklisted by Ukraine hit in drone attack – media
- Canada, the U.S., and NATO: the inescapable trap
- Villains of Judea: Leonid Radvinsky
- Alon Mizrahi: ‘Israel Must Be Dismantled’
- Former Head Of MI6 Admits That The U.S. And Israel Are Losing The Iran War
- Scattered Thoughts on War and Peace
- Iran Threatens to Close Red Sea to Shipping in Response to Invasion
- Iran in excellent position to prevail in war with US, Israel: John Mearsheimer
- If Americans Knew
- Israel may be committing war crimes in Lebanon – Not a ceasefire Day 167
- In the West Bank, life is a constant battle – 3 articles
- Jacob Reses, one of the most powerful pro-Israel operatives in Trump’s Washington
- Israeli-US assaults kill or injure 87 children a day – Not a ceasefire Day 166
- ‘Forever live by the sword’: Understanding Israelis’ massive support for Iran war
- UN’s special rapporteur on human rights says Israel is systematically torturing Palestinians
- Trump White House plagiarized Iran war manifesto from Israel-aligned think tank
- Gaza says 6–10 patients die daily waiting for treatment abroad as Israel blocks medical evacuations
- ‘Substantial evidence’ of double-tap strike in killing of Gaza’s Hind Rajab
- ‘Do Not Want To Die For Israel’: Doubts About Trump’s Iran Strategy Spread Among Troops
- No Tricks Zone
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis
- New Study Documents A 20-Year Pause In Arctic Sea Ice Decline – Driven By Internal Variability
- Wake-up Call: Survey Shows Majority Of Germans Now Favor Postponing Climate Targets!
