Top 10 NHS dietary advice FAILS (from a doctor)
Dr Philip Bosanquet | August 4, 2023
The NHS dietary guidelines are not fit for purpose (in my opinion).
Buy The Concise Nutrition and Lifestyle Guide: https://www.bosanquethealth.com/book-… (available worldwide via Amazon).
Visit Bosanquet Health: https://www.bosanquethealth.com The 10 fails are:
10. Approaching healthy eating / nutrition from a calories-in vs calories-out energy balance focus (failing to take into account Leptin).
9. Basing meals on starchy carbohydrates (failing to understand the root cause of insulin resistance, number one driver of obesity and chronic disease).
8. Minimising fat intake (due to it’s calorie density).
7. Promoting seed oils (vegetable oil, rapeseed oil, sunflower oil) as healthy, whilst stating saturated fat is bad / causes cardiovascular disease (papers on this are listed below, see also video on animal fat:  • Why ANIMAL FAT is the ultimate SUPERF… ).
• Why ANIMAL FAT is the ultimate SUPERF… ).
6. Advising people not to delay or skip meals, including breakfast (failing to appreciate time restricted eating / intermittent fasting).
5. Advice of healthy snacks.
4. Advice on artificial sweeteners as a substitute for sugar.
3. No mention of the gut microbiome, of organic food being better for humans and the environment than non-organic food, of minimally processed or unprocessed foods in preference to overly processed foods, or the quality or nutritional density of food choices.
2. Switching from full cream / full fat / whole milk to semi skimmed / reduced fat milk to help kids lose weight (!). Failing to take into account fat soluble vitamins including vitamin D.
1. Some of the recipe examples given.
Links to papers on saturated fat: https://pubmed.ncbi.nlm.nih.gov/28864…
https://pubmed.ncbi.nlm.nih.gov/24723…
https://pubmed.ncbi.nlm.nih.gov/26268…
https://pubmed.ncbi.nlm.nih.gov/34796…
https://pubmed.ncbi.nlm.nih.gov/34547…
https://pubmed.ncbi.nlm.nih.gov/34717…
https://pubmed.ncbi.nlm.nih.gov/34509…
https://pubmed.ncbi.nlm.nih.gov/27071…
https://pubmed.ncbi.nlm.nih.gov/23386…
https://pubmed.ncbi.nlm.nih.gov/34290…
Dr Philip Bosanquet The Low-Tech Lifestyle Medic
content (except quotes) copyright to Dr Philip Bosanquet 2023 ©
New Study: ‘Carbon Dioxide And A Warming Climate Are Not Problems’
Instead, warmth and elevated CO2 are a boon for humanity
By Kenneth Richard | No Tricks Zone | July 8, 2024
A new peer-reviewed paper published in The American Journal of Economics and Sociology (May and Crok, 2024) counters the prevailing “wisdom” that says a warmer climate and greener vegetation are problematic.
The authors detail the horrors of the much colder Little Ice Age that destroyed civilizations (crop failures, summerless years). Half the population of Finland and 15% of Scotland’s citizens died off in the 1690s due primarily to the cold-induced famines and frozen-over water supplies.
Elevated CO2 and warmth are 70% and 8% responsible, respectively, for a much greener, more vegetated landscape across the world since the 1980s.
The incidence and severity of storms, hurricanes, floods, and extreme weather in general have undergone flat to declining trends over the last several decades. Thus, “it is hard to find any unusual weather or weather-related disaster that can be blamed on climate change, whether natural or anthropogenic.”
“52 of 53 studies of disaster losses due to extreme weather were unable to attribute the events to human causes…”
The US government estimates the warming since 1950 has reduced the country’s gross domestic product by less than 0.5%, and an estimated 3°C of warming by 2100 still only reduces the GDP by less than 1%. Considering the US economy grew by 800% from 1950 to present, this means any assumed “damage” from warmth and elevated CO2 would not be detectable.
The quest to “save” the world from warming and elevated CO2 is devoid of scientific and socio-economic merit.
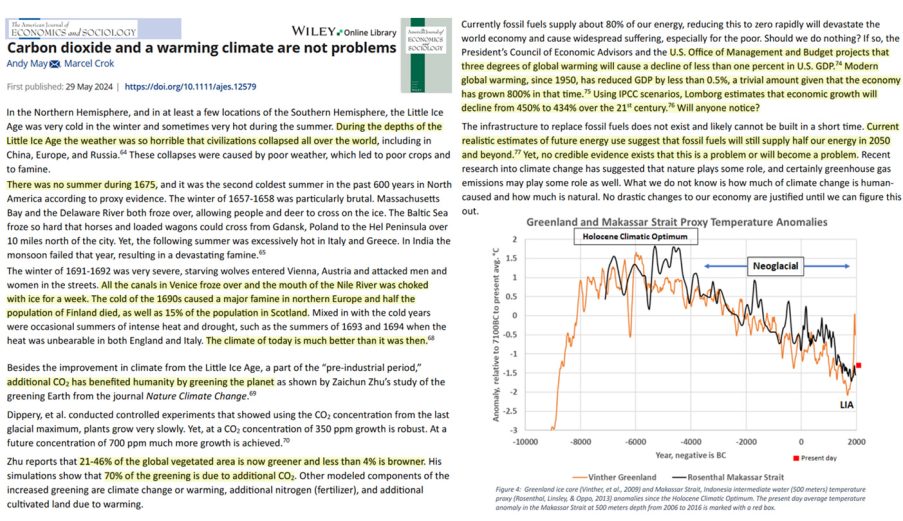
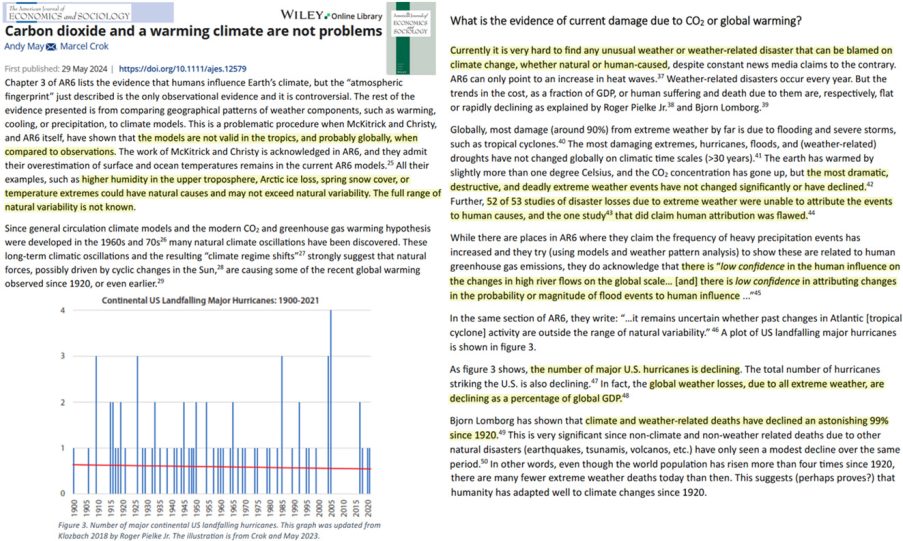
Image Source: May and Crok, 2024
COVID-19 Modified mRNA “Vaccines”: Lessons Learned from Clinical Trials, Mass Vaccination, and the Bio-Pharmaceutical Complex, Part 1
Mead et al Deliver Counter-Punch after Springer Nature Unethical Retraction of High-Impact Paper
By Peter A. McCullough, MD, MPH | Courageous Discourse™ | July 8, 2024
Every major development in medicine evolves over years with peer-reviewed manuscripts and published correspondence along the lines of arguments and scientific discourse. Never had we seen a new technology and mass mandated line of medical products be introduced with no allowance for proper scientific discourse. Not until mRNA.

Mead and co-workers found themselves at the center of a controversy when Springer Nature CUREUS Journal of Biomedical Sciences retracted their paper calling for global market withdrawal of mRNA vaccines. The retraction violated the COPE (Committee on Publication Ethics Guidelines) for retraction and became a news story garnering even more attention. Other papers continued to cite Mead creating a stinging reverberation for Springer who was hoping to silence the paper.
Now epidemiologist M. Nathaniel Mead and six co-authors have punched back with the manuscript divided into two parts for a greater depth of data and analysis on the safety and theoretical efficacy of modified mRNA COVID-19 vaccines. In Part I, Mead discloses censorship of the first paper by the Bio-Pharmaceutical Complex, a working syndicate that is hell-bent on suppressing any scientific information on COVID-19 side effects.
You may ask what should have occurred? Springer Nature should have never retracted the paper. Rather letters to the editor and responses to the letters from authors should have been published as proper scientific interchange. The new normal is now unethical retraction, massive publicity, and republication with greater amplification of the message—precisely what the Bio-Pharmaceutical Complex is trying to squelch.
Mead MN, Seneff S, Wolfinger R, Rose J, Denhaerynck K, Kirsch S, McCullough PA. COVID-19 mRNA Vaccines: Lessons Learned from the Registrational Trials and Global Vaccination Campaign. Cureus. 2024 Jan 24;16(1):e52876. doi: 10.7759/cureus.52876. Retraction in: Cureus. 2024 Feb 26;16(2):r137. doi: 10.7759/cureus.r137. PMID: 38274635; PMCID: PMC10810638.
COVID-19 Modified mRNA “Vaccines” Part 1: Lessons Learned from Clinical Trials, Mass Vaccination, and the Bio-Pharmaceutical Complex. (2024). International Journal of Vaccine Theory, Practice, and Research , 3(1), 1112-1178. https://doi.org/10.56098/fdrasy50
British Columbia Royal College of Physicians and Surgeons Defeated on Judicial Notice
Case of Dr. Charles Hoffe Kills Deferral to Government Offices as Agents of “Truth”
Courageous Discourse™ | July 6, 2024
This was written by Canadian attorney Lee Turner after discussion with Dr. McCullough.
Dr. Charles Hoffe is a family and (former) emergency room physician in British Columbia who is the subject of disciplinary proceedings before the College of Physicians and Surgeons of British Columbia for making public statements about SARS-CoV-2, the safety and efficacy of the COVID-19 vaccines, and other alternative treatments including ivermectin. Hoffe has successfully defeated an application made by the College seeking judicial notice of the truth of facts alleged by the College concerning these issues. In its efforts to discipline the physician, the College has alleged that the statements made by the physician are misleading, incorrect or inflammatory and constitute professional misconduct. The College asked the discipline panel to take judicial notice of the following facts and thereby prevent the doctor from presenting any contrary evidence in his defence:
- The Covid virus kills or causes other serious effects;
- The virus does not discriminate;
- Vaccines work;
- Vaccines are generally safe and have a low risk of harmful effects, especially in children;
- Infection and transmission of the COVID-19 virus is less likely to occur among fully vaccinated individuals than for those who are unvaccinated; vaccines do not prevent infection, reinfection or transmission, but they reduce the severity of symptoms and the risk of bad outcomes;
- Health Canada has approved COVID vaccines, and regulatory approval is a strong indicator of safety and effectiveness;
- Health Canada has not approved ivermectin to treat COVID-19; and
- Health Canada advises that Canadians should not consume the veterinary version of ivermectin.
In its June 29, 2024 decision, the disciplinary panel of the College of Physicians and Surgeons of British Columbia declined to take judicial notice of items 2-5, did take judicial notice of items 7-8 (the straightforward ivermectin claims), and took judicial notice of a revised version of items 1 and 6.
The panel was prepared to take judicial notice of item 1 that reads: “COVID-19 can kill or cause other serious effects”.
The College explained their rationale for taking judicial notice of a revised version of item 1 by referencing evidence presented by the doctor in his defence that included the following:
- risk of severe disease and death from COVID-19 is extremely skewed to those above 70 years of age, especially those with multiple comorbidities. The average age of persons that died from COVID-19 in Canada was approximately 84 years old;
- very low proportion of COVID-19 related deaths in Canada occurred in those under 50 years of age-the data shows very high (although not 100%) survival rates for those under 70;
- average rate of lethality from COVID-19 for Canadians is much lower than estimates given by public health officials; and
- reported hospitalizations and deaths from COVID-19 have been over-counted, because many hospitalizations and deaths “with, and not from” COVID-19 were wrongly attributed to COVID-19
With respect to item 6, the panel endorsed findings of an earlier provincial Court of Appeal decision that held the safety and efficacy of any drug is always relative and as a rule the safety and efficacy of a pharmaceutical product cannot be discussed in such blunt fashion as to say that it “is” or “is not” safe and effective. The panel held that the issues raised in the citation should be determined based upon the evidence that is tested through cross-examination rather than by taking judicial notice of one party’s assertion of the facts, and in this case, based upon statements made by public health officials or public health agencies. The panel held that it was prepared to take judicial notice of the fact that Health Canada had approved the COVID – 19 vaccines, but declined to take judicial notice that Health Canada’s approval was a strong indicator of safety and effectiveness.
This decision on the issue of judicial notice, is consistent with the June 28, 2024 decision of the US Supreme Court in Loper Bright Enterprises et al. v. Raimondo Secretary of Commerce et. al. which overturned the landmark 1984 decision in Chevron v. Natural Resources Defense Council. The Chevron decision had given rise to what is commonly referred to as the Chevron deference doctrine. Under this doctrine, federal agencies had the power to interpret a law that they administer when that law is vaguely written, and courts were required to defer to the agency’s interpretation of a statute. In Loper, the US Supreme Court rejected the Chevron deference doctrine calling it “fundamentally misguided.” They said court should rely on their own interpretation of ambiguous laws rather than having to accept the agency’s interpretation. Commentators have suggested that the Chevron deference doctrine gave the powerful – the people who control the agencies like the FDA, CDC and FCC – a significant advantage in court making them essentially the ultimate decision-makers in interpreting ambiguous laws. Commentators have pointed out that many of these agencies are captive agencies with close ties, including financial ties, to the industries that they are charged with regulating and therefore they lack objectivity with respect to those industries. The ruling in Labor means that federal judges now have more authority to interpret these laws. The decision by the British Columbia Disciplinary Panel of the College of Physicians of Surgeons of British Columbia prevents regulatory bodies from saying “it is so because we say it is so”. They have to prove the facts they assert and those who disagree will be allowed to challenge those facts and present contrary evidence.
The case against Dr. Hoffe is far from over. This development is significant in that a government agency cannot make the rules, interpret them, and claim they hold the truth on an evolving scientific or medical issue.
Lee C. Turner, Partner, Doak Sherriff Lawyers, LLC, Kelowna BC V1Y 2A9
(Professional Law Corporation)
Tale Of Two Weather Stations
By Paul Homewood | Not A Lot Of People Know That | July 3, 2024
Below are photos of two weather stations in Hull.
One is run by the University of Hull’s Environmental Department, the other is used by the Met Office for climatological purposes and typically runs two degrees hotter.
It does not take a genius to work out which is which!

…

Met Office Still Opening Junk Weather Stations
By Paul Homewood | Not A Lot Of People Know That | July 5, 2024
As we know, 77.9% of the Met Office’s temperature station network is junk Class 4 and 5.

But how many of these have been added in recent years?
The Met Office have now sent me a full list of stations, showing both Class and opening date. Since 2000, 58 stations have been added, out of a current total of 380. However only nine are acceptable Class 1 and 2s:
| Class | No |
| 1 | 1 |
| 2 | 8 |
| 3 | 5 |
| 4 | 29 |
| 5 | 15 |
| Total | 58 |
One Class 4 station was opened as recently as last year at Arthog in Wales.
It is one thing having poorly sited stations which have been around for decades. But I personally find it unacceptable that the Met Office have deemed it appropriate to carry on opening so many more, which they know full well should not be used for climatological purposes.
It is surely not beyond their wit to build a few pristine Class 1 sites. Which leads us to the conclusion that they are doing it deliberately.
Meanwhile in other news, the hottest place in the UK yesterday was ……………… HEATHROW!!
The Supreme Court’s Superb Dissenting Opinion
At least three justices understand what is at stake here
By Aaron Kheriaty, MD | Human Flourishing | July 5, 2024
Three justices of the Supreme Court actually read and understood the record in our case. Justice Alito, joined by Gorsuch and Thomas, wrote an important dissenting opinion. I’d like to share a few highlights here, as it provides a roadmap to ultimately prevailing in our case.
The three dissenting justices clearly recognize that we the plaintiffs were victims of the government’s unconstitutional censorship activities:
Among these victims were two States, whose public health officials were hampered in their ability to share their expertise with state residents; distinguished professors of medicine at Stanford and Harvard; a professor of psychiatry at the University of California, Irvine School of Medicine; the owner and operator of a news website; and Jill Hines, the director of a consumer and human rights advocacy organization. All these victims simply wanted to speak out on a question of the utmost public importance.
Echoing the district court and circuit court opinions, the dissenting justices indicate the landmark importance of this free speech case:
If the lower courts’ assessment of the voluminous record is correct, this is one of the most important free speech cases to reach this Court in years. Freedom of speech serves many valuable purposes, but its most important role is protection of speech that is essential to democratic self-government, and speech that advances humanity’s store of knowledge, thought, and expression in fields such as science, medicine, history, the social sciences, philosophy, and the arts.
Unlike the majority opinion, which took the government’s claim to be combating “misinformation” at face value, the dissenting opinion recognized that much of the speech that the government suppressed was true:
The speech at issue falls squarely into those categories. It concerns the COVID–19 virus, which has killed more than a million Americans. Our country’s response to the COVID–19 pandemic was and remains a matter of enormous medical, social, political, geopolitical, and economic importance, and our dedication to a free marketplace of ideas demands that dissenting views on such matters be allowed. I assume that a fair portion of what social media users had to say about COVID–19 and the pandemic was of little lasting value. Some was undoubtedly untrue or misleading, and some may have been downright dangerous. But we now know that valuable speech was also suppressed. That is what inevitably happens when entry to the marketplace of ideas is restricted.
The majority opinion suggested, without evidence, that our censorship was the result of the actions of social media platforms, who may have censored us even in the absence of government coercion. The dissenting opinion explains the flaws with this unwarranted assumption:
Of course, purely private entities like newspapers are not subject to the First Amendment, and as a result, they may publish or decline to publish whatever they wish. But government officials may not coerce private entities to suppress speech, see National Rifle Association of America v. Vullo, 602 U. S. 175 (2024), and that is what happened in this case.
The record before us is vast. It contains evidence of communications between many different government actors and a variety of internet platforms, as well as evidence regarding the effects of those interactions on the seven different plaintiffs.
Alito focuses on Facebook and co-plaintiff Jill Hines as the clearest example (though by no means the only example) to illustrate the nature of the problem:
Here is what the record plainly shows. For months in 2021 and 2022, a coterie of officials at the highest levels of the Federal Government continuously harried and implicitly threatened Facebook with potentially crippling consequences if it did not comply with their wishes about the suppression of certain COVID–19-related speech. Not surprisingly, Facebook repeatedly yielded. As a result Hines was indisputably injured, and due to the officials’ continuing efforts, she was threatened with more of the same when she brought suit. These past and threatened future injuries were caused by and traceable to censorship that the officials coerced, and the injunctive relief she sought was an available and suitable remedy.
It’s hard to know how much more harm the Supreme Court would need to see before agreeing that at least one of the plaintiffs has standing. These examples could be multiplied. By refusing to examine the record and rule on the merits, Alito suggests that the Court actually provides a roadmap for future government censorship efforts:
This evidence was more than sufficient to establish Hines’s standing to sue, and consequently, we are obligated to tackle the free speech issue that the case presents. The Court, however, shirks that duty and thus permits the successful campaign of coercion in this case to stand as an attractive model for future officials who want to control what the people say, hear, and think.
That is regrettable. What the officials did in this case was more subtle than the ham-handed censorship found to be unconstitutional in Vullo, but it was no less coercive. And because of the perpetrators’ high positions, it was even more dangerous. It was blatantly unconstitutional, and the country may come to regret the Court’s failure to say so. Officials who read today’s decision together with Vullo will get the message. If a coercive campaign is carried out with enough sophistication, it may get by. That is not a message this Court should send.
Alito then echoes arguments I published in The Federalist following oral arguments, regarding the key differences between newspapers and social media companies in terms of their interactions with government:
Internet platforms, although rich and powerful, are at the same time far more vulnerable to Government pressure than other news sources. If a President dislikes a particular newspaper, he (fortunately) lacks the ability to put the paper out of business. But for Facebook and many other social media platforms, the situation is fundamentally different. They are critically dependent on the protection provided by §230 of the Communications Decency Act of 1996, 47 U. S. C. §230, which shields them from civil liability for content they spread. They are vulnerable to antitrust actions; indeed, Facebook CEO Mark Zuckerberg has described a potential antitrust lawsuit as an “existential” threat to his company. And because their substantial overseas operations may be subjected to tough regulation in the European Union and other foreign jurisdictions, they rely on the Federal Government’s diplomatic efforts to protect their interests.
This dynamic sets social media companies up to be vulnerable to government coercion, in precisely the way we argued before the Court:
For these and other reasons, internet platforms have a powerful incentive to please important federal officials, and the record in this case shows that high-ranking officials skillfully exploited Facebook’s vulnerability. When Facebook did not heed their requests as quickly or as fully as the officials wanted, the platform was publicly accused of “killing people” and subtly threatened with retaliation.
Not surprisingly these efforts bore fruit. Facebook adopted new rules that better conformed to the officials’ wishes, and many users who expressed disapproved views about the pandemic or COVID–19 vaccines were “deplatformed” or otherwise injured.
Alito perfectly describes how this abusive Stockholm Syndrome dynamic played out between Facebook and the White House:
What these events show is that top federal officials continuously and persistently hectored Facebook to crack down on what the officials saw as unhelpful social media posts, including not only posts that they thought were false or misleading but also stories that they did not claim to be literally false but nevertheless wanted obscured. And Facebook’s reactions to these efforts were not what one would expect from an independent news source or a journalistic entity dedicated to holding the Government accountable for its actions. Instead, Facebook’s responses resembled that of a subservient entity determined to stay in the good graces of a powerful taskmaster. Facebook told White House officials that it would “work . . . to gain your trust.” When criticized, Facebook representatives whimpered that they “thought we were doing a better job” but promised to do more going forward. They pleaded to know how they could “get back to a good place” with the White House. And when denounced as “killing people,” Facebook responded by expressing a desire to “work together collaboratively” with its accuser. The picture is clear.
Here we have a major social media platform responding as though they are entirely subservient to government interests. The more they try to please the government by ramping up censorship, the more abusive and demanding the government becomes.
To the dubious claim that plaintiffs cannot allege potential future injuries because—on their word—the White House has backed off the social media companies, Alito (in contrast to the majority opinion) calls the government’s bluff:
The White House threats did not come with expiration dates, and it would be silly to assume that the threats lost their force merely because White House officials opted not to renew them on a regular basis.
As Alito later quips, “death threats can be very effective even if they are not delivered every day.”
Drawing an analogy to another free speech case (Vullo) that was heard on the same day as ours, Alito explains:
In Vullo, the alleged conduct was blunt. The head of the state commission with regulatory authority over insurance companies allegedly told executives at Lloyd’s directly and in no uncertain terms that she would be “‘less interested’” in punishing the company’s regulatory infractions if it ceased doing business with the National Rifle Association. The federal officials’ conduct here [in Murthy] was more subtle and sophisticated. The message was delivered piecemeal by various officials over a period of time in the form of aggressive questions, complaints, insistent requests, demands, and thinly veiled threats of potentially fatal reprisals. But the message was unmistakable, and it was duly received.
The Supreme Court majority was ready to knock down ham-fisted censorship (in Vullo) but gave a pass—at least for now—to sophisticated and debonair censorship (in Murthy).
The government’s defense of its behavior included the argument that it had the right to use the bully pulpit to “persuade” social media companies to do its bidding—”the government has free speech rights, too, don’t you see?” Alito sees right through this ruse:
This argument introduces a new understanding of the term “bully pulpit,” which was coined by President Theodore Roosevelt to denote a President’s excellent (i.e, “bully”) position (i.e., his “pulpit”) to persuade the public. But [Rob] Flaherty, [Andy] Slavitt, and other [White House] officials who emailed and telephoned Facebook were not speaking to the public from a figurative pulpit. On the contrary, they were engaged in a covert scheme of censorship that came to light only after the plaintiffs demanded their emails in discovery and a congressional Committee obtained them by subpoena. If these communications represented the exercise of the bully pulpit, then everything that top federal officials say behind closed doors to any private citizen must also represent the exercise of the President’s bully pulpit. That stretches the concept beyond the breaking point.
In any event, the Government is hard-pressed to find any prior example of the use of the bully pulpit to threaten censorship of private speech.
To repeat what I have said many times before: this case is not about constraining the government’s speech—as they falsely claim; it’s about stopping the government from constraining the speech of U.S. citizens.
The dissenting justices argue that the majority opinion applies a “new and heightened standard” of traceability in our case (p.20). Alito explains, again using the case of co-plaintiff Jill Hines, that she clearly has standing to bring the case (and we only need one plaintiff with standing to prevail):
Here, it is reasonable to infer (indeed, the inference leaps out from the record) that the efforts of the federal officials affected at least some of Facebook’s decisions to censor Hines. All of Facebook’s demotion, content-removal, and deplatforming decisions are governed by its policies. So when the White House pressured Facebook to amend some of the policies related to speech in which Hines engaged, those amendments necessarily impacted some of Facebook’s censorship decisions. Nothing more is needed. What the Court seems to want are a series of ironclad links—from a particular coercive communication to a particular change in Facebook’s rules or practice and then to a particular adverse action against Hines. No such chain was required in the Department of Commerce case, and neither should one be demanded here.
Furthermore, the Court’s majority opinion developed a novel, higher standard of repressibility of potential future harms to avoid ruling on the merits of our case:
As with traceability, the Court applies a new and elevated standard for redressability, which has never required plaintiffs to be “certain” that a court order would prevent future harm.
Having established that the Court should have found that we have standing, Alito proceeds to analyze the record on the merits, using the following legal framework:
The principle recognized in Bantam Books and Vullo requires a court to distinguish between permissible persuasion and unconstitutional coercion, and in Vullo, we looked to three leading factors that are helpful in making that determination: (1) the authority of the government officialswho are alleged to have engaged in coercion, (2) the natureof statements made by those officials, and (3) the reactions of the third party alleged to have been coerced. 602 U. S., at 189–190, and n. 4, 191–194. In this case, all three factors point to coercion.
Although the government tries to spin their interactions with social media platforms as fairly benign, examination of the record in this regard leaves no doubt: “The totality of this record—constant haranguing, dozens of demands for compliance, and references to potential consequences—evince ‘a scheme of state censorship.’” Lest there be any doubt in this regard, “Facebook’s responses to the officials’ persistent inquiries, criticisms, and threats show that the platform perceived the statements as something more than mere recommendations.” Alito concludes, “In sum, the officials wielded potent authority. Their communications with Facebook were virtual demands. And Facebook’s quavering responses to those demands show that it felt a strong need to yield.”
From here we return to the District Court in Louisiana for trial, where we have an excellent judge (Terry Doughty). We will be granted additional discovery, in which we anticipate getting enough additional “smoking guns” to cross the high standing bar set by the majority Supreme Court opinion. The District court has combined our case with an analogous case filed by Robert F. Kennedy, Jr., who is clearly named and targeted in several government censorship missives—so between Hines and Kennedy there should be no questions on the issue of standing, even under the novel and strict criteria that SCOTUS requires in this case.
In other words, we will prevail in the end. I anticipate being back at the Supreme Court in another year or two for the final ruling. At that point, SCOTUS will not be able to temporize or look away as they did this time. And when judges examine the record in our case, they have only reached one conclusion: the government engaged in unconstitutional censorship on a mass scale. And it has to stop.
Trump Goes Full RFK Jr., Targets Chronic Childhood Illness, Big Pharma As Campaign Pledge
By Jefferey Jaxen | July 3, 2024
In a recent video, former President Donald Trump signaled he would establish a “special presidential commission of independent minds” to determine what is causing the increase in chronic illness.
“This conversation is long overdue… it’s time to ask what’s going on” stated Trump.
Many involved in this space demanding investigation and justice for years, and even decades, have seen several opportunities pass by to ask ‘what’s going on’ with little change ever occurring.
Meanwhile, one of the major pillars of RFK Jr.’s 2024 campaign is to investigate chronic illness in children – a message that he has been consistent on through his career.
With the Democratic party currently engulfed in uncertainty, the unofficial RFK Jr. – Trump alliance found on this topic is hopeful for several reasons. It increases the percentage that something will actually get changed as more attention begins to focus on this topic. It puts Big Pharma on notice while upping the chances whoever is the next president is will carve out a space to aggressively approach chronic childhood illness by any means necessary.
Despite presidential candidates dipping their toes into this conversation, it has been parents who have carried the torch for decades seeking answers and raising awareness to the increasing chronic illness and disease that have plagued their children.
Ten days before Trump took office in 2017, he met with RFK Jr. to discuss forming a commission on vaccine safety and scientific integrity to which he would lead.
“The President-elect is exploring the possibility of forming a committee on Autism, which affects so many families; however no decision have been made at this time,” his transition team said in a statement provided to The New York Times. “The President-elect looks forward to continuing the discussion about all aspects of Autism with many groups and individuals.”
For reasons still unknown to this day, the Trump team decided not to green-light the commission which may have proven useful going into the early stages of COVID vaccine development.
Why look at vaccine safety and it’s link to chronic illness?
A formal exchange between attorneys at the Informed Consent Action Network and US Health and Human Services in 2018 states:
“… the increase in HHS’s childhood vaccine schedule over the last 30 years from 8 vaccine injections to 50 vaccine injections (plus 2 injections during pregnancy) has occurred in lockstep with the increase in the rate of autoimmune, developmental and neurological disorders in children from 12.8% to 54%. HHS has no explanation for why U.S. children today are plagued with a chronic disease and disability epidemic.”
Meanwhile, safety review periods in clinical trials for vaccines are too short, often days or weeks, to detect most chronic health conditions further hamstringing an entire body of health and research.
Why is this a campaign issue?
The economic burden of America’s chronic illness problem began to get much-needed attention with a 2018 report from the Milken Institute estimating $1.1T in direct costs and $3.7T [in indirect costs].
The COVID response torpedoed the mainstreaming and critical mobilization of the medical and research communities into the burden of chronic disease, especially among children. Closed off was this investigative avenue to the funding and national effort needed to address this problem.
One only needs to look at how the dominant culture went to war with the benefits of vitamin D, sunlight, and fresh air during the COVID response to see the lengths those from corporate media to heads of regulatory agencies will go to silence simple, lifesaving information when it protects power, control and pharmaceutical product lines.
Yet it’s not all about the shots.
An article from Politico titled, How Washington Keeps America Sick and Fat states, “the federal government has devoted only a tiny fraction of its research dollars to nutrition… Studying the relationship between diet and health is such an afterthought that Washington doesn’t even bother tracking the total amount spent each year.“
After reviewing the federal budget documents, Politico found, “the National Institutes of Health and the Agriculture Department — the two agencies that fund the majority of government-backed nutrition science — share of research dollars devoted to nutrition has stayed largely flat for at least three decades, and pales in comparison to many other areas of research.“
Pharma outspends all other industries in lobbying. Meanwhile, there is no major lobbying force behind boosting nutritional research funding. America’s sick-care, pharmaceutical product-based ‘health’ paradigm appears rooted, driven, and amplified by the lobbying efforts of corporate interests.
Profit-driven industry is happy to let accurate and beneficial information about nutrition and the harms of their products die on the vine of public awareness. Channeling their efforts more into protecting their products from much-deserved bad press and the outing of known harms into the public conversation.
For American children to thrive, these malevolent, corporate-influence cartel networks, wherever they operate within the medical, nutrition, agriculture, or environmental sectors must be splintered in a thousand pieces and scattered to the winds. Political alliances in efforts to better this situation is a much needed step forward.
How Pfizer’s Original mRNA Trial Hid a 66% Increase in Cardiovascular Death Rate Amongst the Vaccinated
PharmaFiles by Aussie17 | June 29, 2024
Thanks to Dr. Clare Craig for highlighting this clip from Dr. David White on Twitter/X today. It’s important for people to understand how Pfizer manipulated the categorization of deaths in their original trial, which led to politicians using the “safe and effective” narrative. Everyone should carefully watch this, as it not only raises concerns about Pfizer or Moderna’s mRNA vaccines but also highlights the broader corruption of medical information that prioritizes profit over safety.
Dr. David White, a retired general practitioner from the UK, masterfully breaks down the concerning aspects of the Pfizer BNT162b2 trial. He walks us through the intricate details and demonstrates how Pfizer may have “adjusted” the categorization of participant deaths to make it appear as though there were fewer cardiovascular deaths in the vaccine group than there actually were.
To recap, a total of 29 deaths from all causes were reported in the trial within six months, as published in the New England Journal of Medicine. The original trial showed that deaths were about 7% higher in the vaccine group, with 15 deaths, compared to 14 deaths in the placebo group. However, many “fact-checkers” and pharma shills “scientists” claim that this difference is not statistically significant.
This is intriguing because, according to a Lancet paper, there were 44,000 more deaths in England in 2022, driven by a sharp increase in cardiovascular deaths among the middle-aged, which rose by 33%. He wonders if cardiovascular deaths in the trial’s vaccine group were also 33% higher. This question is important because it seeks to determine if the higher death rate in the vaccinated group is related to the rise in cardiovascular deaths seen in the general population.
He walks us through four mysterious “causes of deaths” categorized in the paper:
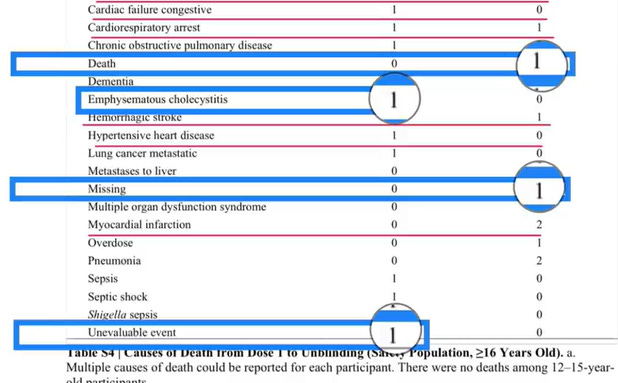
- An “Unevaluable Event” on a vaccinated death, which was found to be a sudden cardiac death confirmed via autopsy.
- A “Missing” entry categorized as a “placebo” death, which was later found to be a “vaccinated” death.
- “Emphysematous Cholecystitis,” which is a cardiovascular death but Pfizer said let’s put something that sounds really complicated and hope nobody knows its a cardiovascular death.
- “Death” for participant #10841470. First of all categorizing a “cause of death” as “Death”, are you kidding? Anyway this participant died after taking a Moderna mRNA vaccine, but was categorized as a placebo death. I wrote about this issue here.
In conclusion, after recategorizing the deaths, all-cause deaths were 15% higher in the vaccine group. There were 10 cardiovascular deaths in the vaccine group and six in the placebo group, indicating that cardiovascular deaths were 66% higher in the vaccine group.
Dr. White highlights that these figures, particularly the increased all-cause mortality in the vaccine group, clearly point to safety signals. He stresses that informed consent is a fundamental ethical principle in medicine, necessitating the open discussion of such safety concerns. It is crucial to ensure that participants are fully informed about the potential risks associated with the vaccine to maintain trust and transparency within the medical community.
Watch full video:
Featured Video

Did the 9/11 Hijackers Really Fly the Planes?
or go to
Aletho News Archives – Video-Images
Book Excerpt
Biden’s Closed Circle on Russia
An excerpt from ‘The Great Betrayal’
By James W. Carden | The Realist Review | June 14, 2026
Joe Biden’s presidency may ultimately come to be seen as a cautionary tale. Here was a president who showed little interest in entertaining arguments that might have contradicted his most deeply held assumptions.[1] And there were precious few within the upper ranks of the administration who might have attempted to do so, after all, only policy hands and political operatives who had come up through the ranks of the Clinton and Obama administrations or had longstanding ties to the citadels of the foreign policy community were invited into the fold. … continue
Blog Roll
 Aletho News
Aletho News- CDC Awards Pfizer $1.24 Billion for COVID Vaccines for Kids and Adults
- Historic blow to South Korea’s military intelligence agency
- Russian frigate fires warning shots in English Channel
- Radio Free Europe, the Cold War ‘Weapon’ Congress Still Funds
- UN: Israel continues to violate Lebanon airspace in defiance of Iran-US MoU
- Araghchi: Israeli occupation of Lebanese land a violation of MoU
- Hezbollah fighters confront intruding Israeli forces in southern Lebanon
- The Straight of Hormuz is Open for Iranian Business… Oil is Moving and Iran is Getting Paid
- Biden’s Closed Circle on Russia
- Lebanon Accuses Israel Of Violating The Chemical Weapons Convention By Spraying Toxic Herbicide Over Farmland
- If Americans Knew
- Israeli army ‘murdered child’ in Gaza and then dumped body on a roadside
- The Forward’s Hit Piece on Thomas Massie and USS Liberty Veterans
- Israel’s former defense minister compares settler ideology to Nazism
- The Pro-Israel Lobby’s Quiet Cash Shuffle
- Trinity Broadcasting Network (TBN) Propagandizes for Israel’s Wars
- A grim milestone: Gaza’s death toll surpasses 73,000 – Daily Update
- Jared Kushner’s Israel-linked island, and other dubious projects
- Why Are Crypto Billionaires and AIPAC Spending $8+ Million to Elect Adrian Boafo?
- Why the Mainstream Media Should Stop Using the ADL as Their Go-To Antisemitism Source
- Censorship and Thuggery Won’t Save Israel’s Reputation
- No Tricks Zone
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
