
Before Dr. Vivek Murthy prescribed “community” as America’s cure, he helped engineer the policies that tore it apart.
When outgoing Surgeon General Dr. Vivek Murthy released his January 2025 essay, “My Parting Prescription for America,” it was framed as a heartfelt reflection on the nation’s loneliness and disconnection. The document reads like a sermon on “love,” “service,” and “community” — invoking Christian compassion, Hindu dharma, and African Ubuntu to offer a kind of spiritual healing for America’s fractured soul.
But beneath the soft prose lies a striking irony: the very official who now urges the nation to “choose community” presided over one of the most divisive and dehumanizing public health regimes in U.S. history. His tenure was marked by systematic censorship, defamation of independent scientists and health advocates, and the suppression of truthful reporting about vaccine injuries and deaths — all documented in federal court filings and corroborated by congressional investigation.
The Surgeon General Who Prescribed Silence
In 2021, Surgeon General Vivek Murthy partnered with the now-disgraced Center for Countering Digital Hate (CCDH) and its soon-to-be-deported founder, Imran Ahmed, to launch a campaign labeling “health misinformation” as a public threat and urging social media companies to “take more aggressive action” against those who questioned the official COVID-19 narrative.
As detailed in Finn v. Global Engagement Center (3:25-cv-00543) (Doc. 83), Murthy’s office collaborated with entities like the CCDH, the White House, and Big Tech platforms to pressure for the removal or throttling of lawful speech — including posts about natural immunity, vaccine injury, and early treatment protocols.
This coordination, which the complaint describes as a “fusion of state and private power to suppress disfavored viewpoints,” forms part of a broader transnational censorship enterprise now under legal scrutiny.
Murthy’s rhetoric about “protecting public health” masked an unprecedented effort to erase public testimony from the vaccine-injured and to delegitimize independent medical experts whose research contradicted pharmaceutical and government messaging. Many of those targeted — including myself — were falsely branded as part of the “Disinformation Dozen,” a defamatory construct disseminated to newsrooms worldwide through UK-linked NGOs and U.S. federal agencies.
Covering the Wounds He Helped Inflict
In his “Parting Prescription,” Murthy writes that “community is the formula for fulfillment” and that the modern epidemic of loneliness demands “love, courage, and generosity.”
Yet his own tenure systematically dismantled trust and belonging, dividing families, churches, and workplaces through moralized public health edicts.
Lockdowns, school closures, and vaccine mandates — all publicly championed by Murthy — fractured communities, creating the very isolation he now laments.
The Surgeon General who now preaches about “connection” was among those who ordered Americans to sever their most human bonds: to distance from loved ones, to shun the unvaccinated, and to treat dissenters as diseased threats.
His later call to “build a new social contract” founded on service and civic programs like the “Youth Mental Health Corps”is telling. It repackages the same surveillance-based public health infrastructure — behavioral tracking, centralized intervention, social credit by another name — in the language of compassion.
Weaponizing Psychology: Pathologizing Dissent
Murthy’s tenure advanced a subtle but potent form of psychological warfare: pathologizing dissent as sickness.
When he declares that division and distrust are symptoms of a “spiritual crisis,” he erases the political and moral legitimacy of resistance. Those who refused the experimental injections, questioned corporate capture of science, or defended medical choice are reframed not as engaged citizens but as patients in need of behavioral correction.
This framing, echoed by the World Health Organization and the Surgeon General’s “advisories,” lays the groundwork for the next phase of informational control — one cloaked not in censorship, but in therapeutic paternalism.
The Great Inversion: Coercion as Care
At the heart of Murthy’s “Prescription” is a moral inversion: coercion recast as compassion.
Throughout the pandemic, his messaging repeatedly equated compliance with virtue and questioning with harm. His Office’s partnership with the CDC and White House COVID Response Team normalized the language of “protecting others” — a phrase that justified censorship, job loss, and social exclusion.
Now, Murthy’s final reflection dresses that same ideology in the soft robes of empathy. His triad of “relationships, service, and purpose”reads less like a personal wellness philosophy than a state catechism — urging citizens to find meaning through collective obedience to approved narratives.
The Spiritual Disguise of Technocratic Power
Murthy’s invocation of faith traditions — Christianity, Judaism, Hinduism, Islam, and Ubuntu — is striking not for its inclusivity, but for its instrumental use of sacred language to legitimize centralized authority.
In merging spirituality with governance, Murthy mirrors a broader trend in global health policy: the conversion of care into control, where moral virtue is measured by conformity to bureaucratic “truth.”
The true crisis is not loneliness, but alienation from truth — a wound deepened by those who censored, shamed, and silenced the nation under the guise of saving it.
From Surgeon General to Social Engineer
Murthy closes his “Prescription” with a challenge:
“We are kin, not enemies… Good people with hearts full of love can change the world.”
But for the thousands of Americans censored, deplatformed, and defamed under his watch, and many more who were injured or killed by the experimental jabs he declared were necessary, those words ring as hollow as a pharmaceutical apology after the damage is done.
True love cannot coexist with coercion. True community cannot be built on lies.
The enduring legacy of Murthy’s public health tenure is not one of healing but of division, distrust, and epistemic violence — the destruction of the social immune system that protects a free people: open inquiry and dissent.
A Prescription Reversed
If Murthy’s farewell message was sincere, his repentance would begin with acknowledgment — of the vaccine-injured, of the silenced physicians, of the citizens whose livelihoods and voices were destroyed in the name of “safety.”
Until then, his “parting prescription” serves not as medicine, but as mirror — reflecting the psychological alchemy of a technocratic era that calls its injuries love.
Referendes
- Murthy’s My Parting Prescription for America (your uploaded PDF) — referenced for quotes and thematic contrast.
- Ji et al. v. Center for Countering Digital Hate et al. (Doc. 83 – Second Amended Complaint) — for legal and factual references regarding Murthy’s actions, coordination, and the broader censorship regime.
- Judicial and congressional context — including Missouri v. Biden and Kennedy v. Murthy, which form the legal frame for federal involvement in viewpoint suppression.
November 15, 2025
Posted by aletho |
Civil Liberties, Full Spectrum Dominance, Science and Pseudo-Science | United States |
Leave a comment
A recent article in The Guardian, “Change course now: humanity has missed 1.5C climate target, says UN head,” claims that the planet is in grave danger of passing climate “tipping points,” as it is now inevitable that 1.5°C warming will be breached. Although 1.5℃ of warming may be locked in if not already surpassed, the claim that it signifies a dangerous milestone is false. Not only is the tipping points narrative bunk, but there is no evidence that 1.5°C warming is any particular threat. The purported temperature threshhold was chosen arbitrarily and for political reasons rather than scientific ones.
The Guardian’s story focuses on comments made by United Nations Secretary General António Guterres, who in advance of the COP30 climate summit in Brazil, warned that it is “inevitable” that 1.5°C of warming will be breached, and it will result in “devastating consequences” for the planet. The Guardian says Guterres “urged the leaders who will gather in the Brazilian rainforest city of Belém to realize that the longer they delay cutting emissions, the greater the danger of passing catastrophic “tipping points” in the Amazon, the Arctic, and the oceans.”
There is no scientific basis for any so-called tipping points, and claiming otherwise is just fearmongering for political gain.
Beginning with the Amazon rainforest, the location of the next climate summit in November, Guterres reportedly warned that it could become a “savannah,” or a dry grassland. There is no evidence for this absurd claim. Like Guterres’ previous “boiling oceans” comment, it is purely fanciful hyperbole lacking any basis in fact. Guterres is referencing a period of drought suffered by parts of the Amazon basin in recent years, but that drought has not been historically unusual, and the recent localized areas of drought have not been more severe than previous drought periods. As discussed in the Climate Realism post “Media Outlets Continue Spreading False Amazon “Record Drought” Claims,” the Amazon has experienced periods of heavy rain and extended drought in the past that were worse than those we see now. Historic records do not show any worsening of drought in the Amazon. The threat that impacts tree cover is deforestation and clear cutting, not climate change.
The Arctic is also not approaching any dangerous tipping point. Should warming continue, ice extent will likely shrink, but it has not been happening at nearly as fast a rate as alarmists claim. Arctic sea ice extent has been stable since about 2010, indicating a new ice extent regime, and there is no telling how long that will last. If the past is any guide, sea ice might begin expanding again, as it has waxed and waned historically.
Finally, the ocean tipping point Guterres is referring to is the claim that coral reefs will die out as a result of ocean pH changes and higher temperatures, but again, science and paleo-history shows that corals are resilient to changes that are much more extreme than the modest warming of recent decades. As discussed repeatedly at Climate Realism, the world’s oceans are not at risk of becoming acidic and coral reefs are expanding their range and setting records for growth.
It is true that the “1.5°C threshold” is likely to be passed. But that does not mean anything, certainly nothing catastrophic. The 1.5°C warming limit was already passed in 2024 because of the El Niño conditions—with no cataclysm. This should not be of concern to anyone, because that limit is not a scientifically established value. The Guardian fearmongered about it in the past, which Climate Realism addressed here, and seems to have learned nothing. The 1.5°C number was arbitrary; established by an 11 member German political advisory board containing only one meteorologist. It is not a hard scientific threshold the way the boiling point of water is, though alarmists inappropriately treat it that way.
Guterres’ comments are not based on science, data, or even history. He is simply attempting to worry the public, with The Guardian’s complicity, in order to gain political leverage for negotiations at COP 30 even as a growing number of countries are downplaying climate concerns in the realistic assessment that other issues are more pressing and fossil fuels, for now, remain vital to prosperity.
November 13, 2025
Posted by aletho |
Fake News, Mainstream Media, Warmongering, Science and Pseudo-Science | The Guardian, United Nations |
Leave a comment
Today, Americans for Public Trust released a new report exposing how a group of foreign “charities” has spent almost $2 billion bankrolling U.S. policy fights and advancing an extreme climate agenda.
Click HERE to read the full report.
“It is extremely alarming that five foreign charities have quietly poured almost two billion dollars into advocating for the most extreme liberal policies and protests in the United States. Since current laws regulating foreign giving to U.S.-based nonprofit organizations are hindered by a lack of oversight and exploitable exemptions and loopholes, foreign actors have been able to advance their radical and dangerous interests virtually unchecked. Congress needs to address these serious shortfalls in our laws to protect American interests and keep foreign influence out of our politics.” — Caitlin Sutherland, Executive Director, Americans for Public Trust
Fast Facts:
- Five foreign charities have quietly funneled almost $2 billion into U.S. policy fights, litigation, research, protests, lobbying, and the nonprofit sector to advance their extreme, foreign, activist climate agenda. The groups support a radical green agenda including: the managed decline of oil and gas, climate protests, opposing the Keystone XL Pipeline, and more.
- Quadrature Climate Foundation (QCF): QCF, out of the United Kingdom has given $530 million in foreign money to 41 U.S.-based groups from 2020 to the present, including: ClimateWorks Foundation, Growald Climate Fund, The Grantham Foundation, Arabella’s Windward Fund, and the Sunrise Project.
- KR Foundation: The KR Foundation, a Danish charity, has given over $36 million in foreign cash to 53 U.S.-based groups from 2015 to 2024, including: The Conservation Law Foundation (CLF), Center for International Environmental Law (CIEL), Stop the Money Pipeline, Fossil Free Media, The Associated Press, and Oil Change International (OCI).
- Oak Foundation: OF, based in Switzerland, has given over $750 million in foreign money to 152 U.S.-based groups from 2014 to 2024, including: The Environmental Law Institute (ELI), Community Change – the fiscal sponsor for Free DC -, Rockefeller Philanthropy Advisors (RPA), Arabella’s New Venture Fund, Natural Resources Defense Council (NRDC), and The Tides Center.
- Laudes Foundation: Since 2020, The Laudes Foundation, another Swiss-based charity, has poured almost $20 million into 17 U.S.-based groups, including: The Pulitzer Center for Crisis, Ceres, Community Initiatives, and The World Resources Institute (WRI).
- Children’s Investment Fund Foundation: CIFF, based in the United Kingdom, has given over $553 Million in foreign money to 39 U.S.-based groups from 2014 to 2023, including: The Energy Foundation China (EFC), The Institute for Governance & Sustainable Development (IGSD), Environmental Defense Fund (EDF), and The Sunrise Project.
November 7, 2025
Posted by aletho |
Corruption, Science and Pseudo-Science | United States |
Leave a comment
A recent article in The Hill, “Climate change is not a ‘con job’,” claims that catastrophic, human-caused climate change is killing reefs via ocean heatwaves. This claim is false. In reality, corals have existed for millions of years, through warmer and colder periods, and in the recent past, coral reefs have recovered from bleaching events and even die-offs, proving to species to be adaptive and resilient in the face of climate change.
The Hill article, from Rebecca Vega Thurber, the director of the UC Santa Barbara Marine Science Institute, is framed by Thurber’s annoyance that President Donald Trump says climate change is a “con job.” She claims her personal research experience refutes his comment.
Thurber explains that pollution from fertilizer runoff can kill corals, which is true, but goes on to assert that “every result we have collected, in every one of these well intentioned and carefully designed experiments, was waylaid by the increasingly frequent and severe heat waves that have arisen in the last decades.” She says their efforts to mitigate pollution were “overwhelmed by high water temperatures driven by climate change or worse, climate change killed our whole experiment.”
Thurber claims marine heatwaves in the French South Pacific hampered her work by “transform[ing] these normally bountiful reefs from habitats where there was once 60 percent of the seafloor covered with healthy corals to barren plains with less than 1 percent live coral.”
In point of fact, one long-term study from 2019 showed that rather than a “barren plain” French Polynesian reefs have an “outstanding rate of coral recovery, with a systematic return to pre-disturbance state within only 5 to 10 years.”
A second study from 2024, published in Nature, sought to understand why reefs bounced back so readily after major heat waves, concluding that:
Over the past three decades, there have been five main warming events that have caused mass bleaching around Moorea and Tahiti, in 1994, 2002, 2007, 2016, and 2019. Despite bleaching levels up to 100% for some coral species, reefs experienced as high as ~76% recovery following each event. […]
It is currently unknown what controls the ability of coral coverage to recover quickly at these locations. It has been suggested that reefs may develop an increased tolerance to higher SSTs following each bleaching event, and that the increased resilience would allow for a shorter recovery period with less die-off under subsequent SST extremes.
In short, the scientific literature does not support Thurber’s contention in The Hill that coral reefs are dying off in vast numbers. Interestingly, just a few years ago The Hill published an article with a different tone, discussing the fact that coral reefs were thriving “despite warming seas,” but the outlet seems to have forgotten this.
What Thurber and The Hill also neglected to mention was that recent mass die offs did not just coincide with heatwaves alone. Rather a spate of tropical cyclones and crown of thorns starfish outbreaks occurred over the same period resulting in multiple coral colony declines. Multiple stressors are harder on a species than any of those dangers would be alone.
Thurber mentions that Australian reefs are another part of her area of research, but she does not mention that 2024 was the third year in a row where the Great Barrier Reef had record breaking coral coverage.
Unfortunately, close study of reef die backs barely existed in the early parts of the 20th century and before, so short term records like single-event tied die-offs do not stretch into the pre-industrial period for comparison. As a result it is all too easy for alarmists to assert, for example, that marine heatwaves are unprecedented when there are only a few decades of satellite data to work from. Longer term studies, and a knowledge of how coral reefs around the world are built over time, show, in fact, that coral death is part of the reef construction process.
Coral reefs have survived much hotter periods than today, like the Paleocene-Eocene Thermal Maximum which was 5-8°C hotter, as well as much colder glacial periods. One reason for this is that coral organisms are not immobile. Even if particular regions became too hot, which is highly unlikely in our lifetimes, corals could just migrate poleward, as research suggests they did in the past. Change like that might be uncomfortable for narrowly-focused researchers, but it is part of the Earth’s history.
The Hill did a disservice to its readers by publishing this article which served no other purpose than to frighten readers into ignoring Trump’s important point, that bad actors (particularly at the United Nations, where he made the comments) are using climate alarm to promote harmful leftist-favoring policies and enrich themselves. I am sure that Thurber is a “true believer” in the catastrophic warming narrative, but it does not help her case when essential facts are left out of the argument and when the multiple sources of data that do exist contradict her claims.
November 2, 2025
Posted by aletho |
Deception, Fake News, Mainstream Media, Warmongering, Science and Pseudo-Science, Timeless or most popular |
Leave a comment
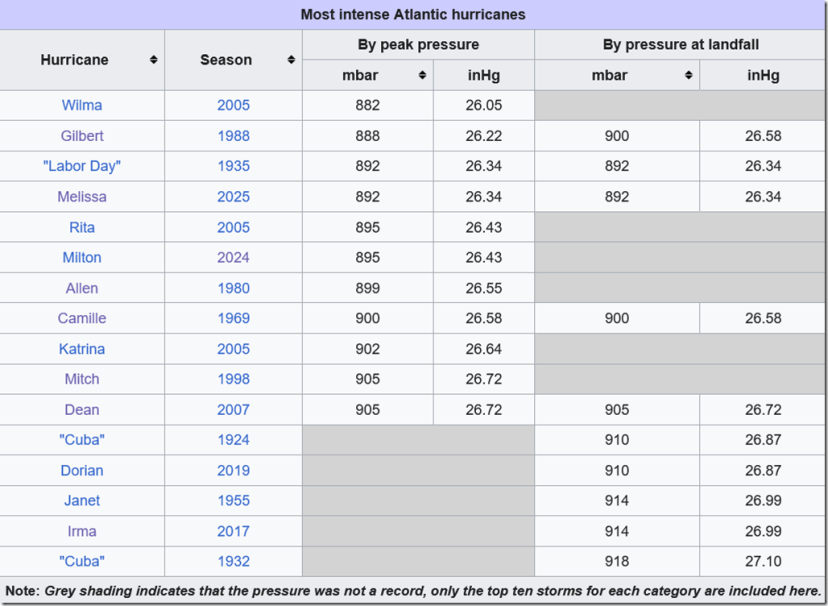
Melissa is now ranked tie 3rd most intense Atlantic hurricane at 892mb. We can look at it in graph format:
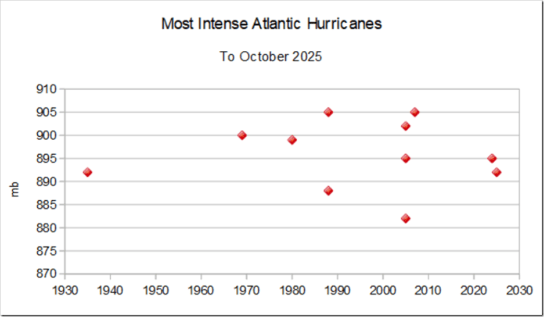
The picture is stark – nearly all of the eleven most intense have occurred in recent years, including the two most intense, Gilbert in 1988 and Wilma in 2005. Does this mean then that global warming really is making hurricanes more intense?
WHOA THERE!!!
Take another look at that table.
Of the eleven on the list, seven were logged out at sea. Of the other four, we already know that the Melissa reading was not at landfall, but occurred several hours before at sea.
Dean’s minimum pressure was measured at landfall, but was observed by hurricane hunters. The other two, Labor Day and Camille, were the only two genuinely recorded at the surface on land.
When we separate readings at landfall and at sea, we get a different story:
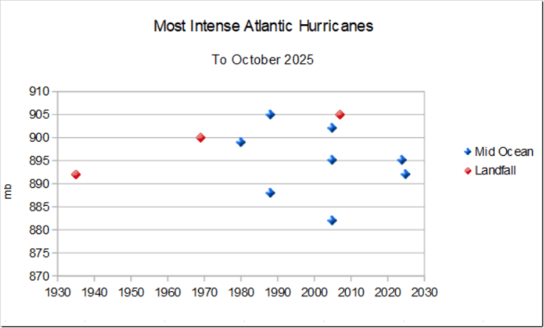
It is not a coincidence that mid ocean hurricanes did not feature before 1980, because proper technology did not exist then to measure them, whether satellites or aircraft.
We know that hurricanes almost invariably weaken as they approach land, so comparing mid-ocean intensities with landfall ones is a meaningless exercise.
But it gets worse.
On the Wikipedia table of most intense hurricanes at landfall, all of the modern entries were taken by hurricane hunters – Dean, Dorian and Irma.
Nowadays hurricane hunters are able to stay inside hurricanes for hours on end, able to seek out the highest wind speeds and lowest pressures. In contrast, measuring hurricanes like Camille relied on land based thermometers, which were extremely unlikely to be at the exact spot where pressure was lowest.
Scientists at the US Hurricane Research Division have done sterling work with their attempts to reanalyse past hurricanes. But as good scientists, they have to be conservative in their findings. They only estimate pressures and windspeeds that they can sensibly justify. Believing that a hurricane was probably more intense is not enough if you don’t have the data to back it up.
Many hurricanes only hit small islands – Dorian and Irma for example. Hurricane hunters are invaluable in getting measurements in these situations where previously there may have been no reliable land-based data.
Hundreds of catastrophic hurricanes have hit the Caribbean over the years. Just because we don’t have accurate data on them does not make them less catastrophic.
November 2, 2025
Posted by aletho |
Science and Pseudo-Science |
Leave a comment
In America, infants are dying at a rate of around 1,300 to 4,500 per year depending on the reporting source. Lives ended suddenly, unexplained with the greater medical system appearing to be okay with it as evidenced by their lack of deeper investigation into the ‘syndrome.’
Sudden Infant Death Syndrome (SIDS) has long-haunted parents and pediatricians alike. Defined traditionally as the sudden death of an apparently healthy infant under one year old for unknown reasons – scientific and legal momentum may be moving towards public understanding.
For decades, it was viewed as an enigmatic “diagnosis of exclusion,” often chalked up to environmental factors like prone sleeping, overheating and in extreme cases blaming the parents for abuse.
Yet, as of 2025, this static portrait is fracturing. Emerging research, landmark court rulings, and legislative reforms reveal SIDS not as a singular black box, but a tapestry of metabolic, genetic, and iatrogenic vulnerabilities—chiefly, immature detoxification pathways and post-vaccination inflammatory cascades.
Florida’s House Bill 188, filed for the 2026 legislative session, exemplifies this paradigm shift legislatively. The bill amends state statutes to mandate comprehensive autopsies for Sudden Unexpected Infant Deaths (SUID) and Sudden Death in the Young (SDY), explicitly requiring microscopic toxicology, full immunization records from the past 90 days, and reporting to the CDC’s national SUID/SDY Case Registry.
No longer optional, these protocols aim to unmask hidden contributors, such as vaccine excipients or genetic polymorphisms, that prior “undetermined” classifications obscured.
And the best part, the bill comes with penalties for noncompliance—fines up to $5,000 and potential license revocation—underscore a growing impatience with incomplete probes. By integrating immunization data with federal surveillance, HB 188 positions SIDS investigations as proactive risk-factor hunts, potentially reclassifying dozens of annual cases from “unexplained” to preventably-framed within the context of the largely untested infant CDC vaccine schedule.
This rigor finds stark validation in the 2023 U.S. Court of Federal Claims ruling on Sims v. Secretary of Health and Human Services (No. 15-1526V), a rare vaccine court triumph that dismantled SIDS as a default for post-vaccination fatalities.
An eleven-week-old infant succumbed just eight hours after receiving five routine shots after a well baby visit. Autopsy revealed cerebral edema [brain swelling] and pulmonary congestion.
The Special Master Christian Moran ruled the vaccines triggered a “Table” encephalopathy via cytokine storms breaching the blood-brain barrier, leading to herniation and arrest. Expert witnesses retained by the Sims family skillfully displayed and achieved the “preponderant evidence” standard under the National Vaccine Injury Compensation Program (NVICP) against all odds that the Department of Justice attornies and their expert witnesses fought to deny justice.
HHS Secretary Kennedy said during a 2025 interivew with Tucker Carlson:
“The lawyers in the Department of Justice, the leaders of it were corrupt. They saw their job as protecting the trust fund rather than taking care of people who made this national sacrifice.”
The Sims family vaccine court award of $300,000 has ignited momentum and advocacy. As detailed in Wayne Rohde’s June 2025 Substack analysis, the case—amid fewer than 5% NVICP death-claim successes—challenges the “coincidental” narrative, urging deeper scrutiny of ~100 pending infant petitions. With the appeal deadline passing without action, we may be witnessing a precedent-proof vaccine link in such cases, eroding SIDS’s explanatory monopoly.
Scientifically, the puzzle pieces align with revelations on cytochrome P450 (CYP450) enzymes, the liver’s metabolic gatekeepers. A 2025 paper by Dr. Gary Goldman has highlighted infants’ CYP450 immaturity: at birth, activity hovers at 30-60% adult levels, with preterm babies hit hardest by “poor metabolizer” genetics (15-40% prevalence).
These enzymes process vaccine adjuvants like aluminum (up to 3,350 mcg in year one) and polysorbate 80. A vicious circle appears as inflammation from shots further suppresses the detoxification ability prolonging toxin exposure.
VAERS data clusters 75% of SIDS-like reports within a week post-vaccination, peaking at day two—echoing the Sims timeline. In serotonin-deficient brains (flagged in 70% SIDS autopsies). In a node to Florida’s SB 188, Dr. Goldman’s study warns current toxicology protocols ignore these developmental gaps, fostering misclassifications.
Together, these threads weave a bolder SIDS narrative: less “syndrome,” more sentinel for systemic oversights. HB 188’s mandates, the Sims precedent, and CYP450 insights demand holistic federal and state-level probes—genetic screening, excipient dosing tiers, and inflammation biomarkers. As Rohde posits, transparency could halve misattributions, saving lives while honoring the unexplained’s gravity. In 2025, SIDS evolves from fatalism to fixable, urging science and policy to catch up before another crib goes silent.
November 1, 2025
Posted by aletho |
Science and Pseudo-Science | Florida, SIDS, United States |
Leave a comment
A chronological overview of leadership changes and the policy pivots that followed
From early 2020 onward, a repeating script unfolded: a head of state voiced skepticism of lockdowns, PCR testing, or experimental mRNA vaccines; international agencies scolded them; chaos or “illness” struck; and within weeks new officials delivered full compliance and suddenly unlocked frozen aid money. The alignment was worldwide—different cultures, same choreography.

1. Burundi – Pierre Nkurunziza
In Burundi, President Pierre Nkurunziza expelled the World Health Organization from his country in May 2020, saying foreign interference was undermining national sovereignty. He kept the nation open while neighboring states imposed severe restrictions. Merely two weeks after that decision he was dead, officially of a “heart attack,” though associates described him as being in vibrant health. His successor, Évariste Ndayishimiye, reversed course immediately, reopened WHO offices, and signed new vaccine and funding arrangements that brought Burundi back into the international fold.
- Backdrop: In spring 2020 the government halted WHO field work, accusing it of interfering with domestic affairs. Burundi rejected external pandemic restrictions and held public gatherings normally.
- Event: Nkurunziza died suddenly 8 June 2020 while still in office; official cause – cardiac arrest.
- Immediate shift: Successor Évariste Ndayishimiye re‑opened WHO offices, declared COVID‑19 a “national priority,” invited vaccine partnerships, and received roughly $24 million in rapid IMF assistance.
- Result: Burundi signed onto COVAX distribution in 2021 after having been one of the continent’s last hold‑outs.
2. Eswatini – Ambrose Dlamini
In Eswatini (formerly Swaziland), Prime Minister Ambrose Dlamini resisted extreme lockdown policies, insisting that starving citizens to stop a virus was immoral. In December 2020 he was taken to South Africa “for observation” and declared dead soon afterward. The royal government that replaced him moved quickly to impose strict curfews, accept COVAX vaccines, and collect foreign emergency aid.
- Backdrop: The businessman‑turned‑PM favoured balanced restrictions, warning that closing trade would worsen poverty.
- Event: Tested positive for SARS‑CoV‑2, transferred to South Africa, and died 13 Dec 2020.
- Aftermath: King Mswati III and his cabinet adopted curfews, mandatory masking, and joined regional COVAX planning.
- Economic follow‑up: The African Development Bank confirmed a $10 million grant under the COVID‑19 Response Support Programme in early 2021.
3. Ivory Coast – Hamed Bakayoko
A similar disappearance occurred in Ivory Coast. Hamed Bakayoko, the charismatic prime minister, had publicly encouraged herbal treatments and questioned the accuracy of PCR diagnostics. In March 2021 he died in Germany of “cancer,” barely eight months after his predecessor suffered a similar fate. His passing removed the last voice questioning WHO dependence. President Alassane Ouattara’s administration proceeded to import AstraZeneca doses through COVAX, and by summer the country was being praised for its “responsible leadership.”
- Backdrop: The popular Prime Minister promoted herbal remedies and localized treatment efforts while maintaining open borders for trade.
- Event: Died 3 Mar 2021 in Germany where he was under cancer treatment; preceded by the death of previous PM Amadou Gon Coulibaly eight months earlier.
- Aftermath: President Alassane Ouattara named Patrick Achi acting PM; by May, 504 000 AstraZeneca doses had been deployed through COVAX.
- Funding: World Bank approved $300 million for emergency health and education programmes that quarter.
4. Tanzania – John Magufuli
The next to fall was Tanzania’s John Magufuli, Africa’s most outspoken skeptic of mass testing and vaccines. He mocked the system by demonstrating that fruit and goats tested positive for COVID. After vanishing from public view in March 2021, the vice‑president announced that he had died of heart failure. His replacement, Samia Suluhu Hassan, promptly reversed every one of his policies, accepted a $600 million IMF “emergency” loan, reopened the gates to foreign pharmaceutical programs, and declared a massive vaccination drive before year’s end.
- Backdrop: Highly skeptical of PCR testing accuracy and mass vaccination; prioritized economic continuity.
- Event: Absent from view in March 2021 for two weeks; Vice President Samia Suluhu Hassan announced his death 17 March (heart failure).
- Aftermath: New administration reinstated public health briefings, reopened WHO cooperation, applied for IMF Rapid Credit Facility ($600 million approved Sept 2021).
- Policy transformation: Vaccine programmes, mask campaigns, and international data reporting began within ninety days.
5. Haiti – Jovenel Moïse
Then came Haiti, where Jovenel Moïse had rejected donated vaccine shipments, explaining that the country faced deeper issues of water and poverty. On July 7 2021, he was executed in his home by an armed team whose origins remain murky. Within three weeks, Haiti received half a million Moderna doses from COVAX and enjoyed renewed flows of Inter‑American Development Bank and USAID funding. The national policy flipped overnight.
- Backdrop: Refused early COVAX vaccine delivery, arguing sanitation and nutrition were greater priorities.
- Event: Assassinated 7 Jul 2021 by a commando team; political motives still contested.
- Aftermath: First COVAX shipment of 500 000 Moderna doses landed 14 July 2021.
- Financial context: Inter‑American Development Bank and USAID re‑released more than $60 million in suspended grants under the “COVID‑19 Recovery Program.”
6. Japan – Shinzo Abe → Yoshihide Suga → Fumio Kishida
In Japan, Prime Minister Shinzo Abe avoided harsh lockdowns and refused to make vaccination compulsory. In August 2020 he resigned citing chronic illness, a convenient exit for global interests irritated by Japan’s autonomy. His successor Yoshihide Suga approved emergency authorization for the Pfizer vaccine within weeks, and after political struggles Fumio Kishida continued the same line, expanding booster programs and digital health passes. When Abe, now a private citizen and public skeptic of global centralization, was assassinated in July 2022, the last independent conservative bastion in Japan’s establishment disappeared. The current government invested ¥4.5 trillion—about $40 billion—in mRNA infrastructure partnerships with Western firms.
- Backdrop: Abe resisted extreme lockdowns and mandatory passes; preferred voluntary distancing.
- Resignation: Aug 2020 due to chronic illness; Suga took over and immediately authorized Pfizer vaccine imports (Feb 2021).
- Transition: Kishida succeeded Suga Oct 2021 after election; expanded booster campaigns and health‑pass apps.
- Abe’s assassination: 8 Jul 2022 in Nara; investigation officially attributed to a personal grudge.
- Post‑event: Japan pledged ¥4.5 trillion (≈ $40 billion) in bio‑innovation investment partly for mRNA research.
7. Slovakia – Igor Matovič
Slovakia followed the pattern in March 2021 when Igor Matovič, who had attempted to purchase Russia’s Sputnik V vaccine outside the European Union’s centralized supply, was forced out after furious criticism from Brussels. His successor Eduard Heger rejoined the EU’s procurement framework and in return unlocked €6.3 billion in recovery funds.
- Backdrop: Purchased Sputnik V without EU approval to widen supply options.
- Event: Coalition crisis culminated March 2021 in his resignation.
- Aftermath: New PM Eduard Heger froze Sputnik imports, conformed to EU purchasing pool, and unlocked €6.3 billion EU Recovery Funds.
8. Czech Republic – Andrej Babiš
Nearby, the Czech Republic saw Prime Minister Andrej Babiš lose power at the end of 2021 after refusing to maintain endless pandemic states of emergency. His replacement Petr Fiala implemented vaccine passports and mass‑testing decrees soon afterward, bringing the nation into perfect accord with EU directives.
- Backdrop: Initially resisted heavy lockdowns, favored voluntary vaccination.
- Event: Lost October 2021 election amid strong pro‑mandate media push.
- Aftermath: Petr Fiala government mandated digital health passes (“Tečka” app) and extended state‑support contracts with Pfizer/Moderna.
9. Austria – Sebastian Kurz
Austria lost Sebastian Kurz the same year. Once a rising star who had questioned perpetual lockdowns, Kurz resigned under the weight of a corruption scandal in October 2021. Within days his successor announced Europe’s first universal vaccine mandate and qualified the country for €4.5 billion in European Stability Mechanism funding.
- Backdrop: Pushed for reopening and questioned perpetual emergency powers.
- Event: October 2021 resignation after prosecution alleged misuse of party funds.
- Aftermath: Successor Alexander Schallenberg announced universal vaccination January 2022; European Stability Mechanism distributed ≈ €4.5 billion in recovery funding.
10. United Kingdom – Boris Johnson
In the United Kingdom, Boris Johnson’s government had ended restrictions in mid‑2021 and refused to make vaccine passports a permanent condition of daily life. The press then exploded with “Partygate” scandals over gatherings during lockdown. Johnson resigned in 2022, replaced by Rishi Sunak, who restored Britain to full WHO cooperation and financed a £2 billion digital‑health‑ID system intended to prevent “misinformation.”
- Backdrop: Repealed many restrictions July 2021 (“Freedom Day”), angering zero‑COVID advocates.
- Event: Forced resignation mid‑2022 after “Partygate.”
- Aftermath: Rishi Sunak government supported the WHO pandemic‑treaty process and invested £2 billion in NHS digital ID infrastructure through Palantir‑backed data platforms. Within weeks of taking office, Downing Street announced negotiations with Moderna to establish a permanent mRNA‑manufacturing base — a 10‑year “strategic partnership” followed with construction of a mRNA vaccine research, development, and manufacturing centre in Harwell Science Park (Oxfordshire), projected to produce up to 250 million doses a year in a future outbreak. This collaboration was framed as part of the UK’s “100‑Day Mission” to deliver vaccines within 100 days of identifying a new pathogen; the mission itself originated from G7 and G20 pandemic‑preparedness pledges.
11. Sri Lanka – Gotabaya Rajapaksa
Half a world away in Sri Lanka, President Gotabaya Rajapaksa argued that global supply sabotage and debt were worse problems than COVID. By mid‑2022 coordinated protests and economic chaos forced him to flee abroad. Within weeks, the IMF approved a $3 billion bailout that required health‑security reforms and the adoption of digital‑surveillance frameworks under WHO supervision.
- Backdrop: Advocated reopening, claimed economic sabotage larger threat than virus.
- Event: Mass protests July 2022 amid fuel and food shortages.
- Aftermath: New interim government signed a $3 billion IMF agreement mandating fiscal reform and health‑security modernization.
12. Brazil – Jair Bolsonaro
Brazil completed the second‑wave phase of this storyline. President Jair Bolsonaro ridiculed mask mandates, called lockdowns a luxury for the rich, and questioned vaccine safety. After two furious years of constant hostility from media conglomerates and international NGOs, he lost the 2022 election. Lula da Silva took office, rejoined WHO initiatives, and secured a $1.2 billion World Bank “preparedness” loan.
- Backdrop: Dismissed lockdowns as “hysteria,” resisted vaccine coercion.
- Event: Lost 2022 election to Lula da Silva after two years of hostile media coverage.
- Aftermath: Brazil re‑entered WHO initiatives, COVAX procurement, and secured World Bank Preparedness Loan ($1.2 billion).
13. Madagascar – Andry Rajoelina
Along the African coast to Madagascar, President Andry Rajoelina had introduced his own herbal remedy, COVID‑Organics, and rejected Western pharmacology. In 2021 an attempted coup shook the island, and under global pressure Rajoelina signed new agreements restoring WHO cooperation that same year so donor funding could return.
- Backdrop: Promoted herbal tonic “COVID‑Organics” (artemisia‑based), claiming national self‑reliance.
- Event: July 2021 coup attempt; several senior officers arrested.
- Aftermath: Rajoelina accepted WHO cooperation and external medical aid later that year, restoring aid flows suspended in 2020.
14. Romania – Vlad Voiculescu Minister of Health
Appointed in December 2020 under Prime Minister Florin Cîțu, Voiculescu quickly became one of Eastern Europe’s most outspoken advocates for data transparency within the vaccine‑procurement process.
He questioned:
- why the European Commission’s contracts with Pfizer/BioNTech and Moderna were heavily redacted;
- the procedure for reporting adverse events and hospital bed usage;
- and financial allocation for Romania’s “Green Certificate” system.
In April 2021, Voiculescu alleged irregularities in the way national statistics on Covid mortality were reported (he said hospital figures were being “massaged” to fit EU targets).
Within 48 hours, Prime Minister Cîțu dismissed him (14 April 2021). That dismissal fractured the ruling coalition and was widely interpreted as pressure from Brussels and Bucharest business lobbies to restore “credibility” with EU health authorities.
- Backdrop: In 2021 Romanian minister objected to secrecy of EU vaccine contracts.
- Event: Dismissal and cabinet reshuffle.
- Aftermath:
- Florin Cîțu — Prime Minister (National Liberal Party), an economist trained in the US and a former banker, had emphasized cooperation with the European Commission’s Recovery Facility.
- Immediately after Voiculescu’s removal, Cîțu approved the formal implementation of the EU Digital COVID Certificate
- He signed Romania’s Recovery and Resilience Facility plan for €29 billion (approved September 2021).
- Cîțu later lost internal party support and was replaced by Nicolae Ciucă (2021 December).
- Raed Arafat — Secretary of State, Chief of the Department for Emergency Situations, a longtime figure in Romanian health management (specialist of Palestinian background), spearheaded the nationwide lockdown operations.
- He became polarizing — praised for emergency coordination but criticized for advocating strict curfews and mandatory digital passes.
- Through his influence, Romania aligned with EU Civil Protection Mechanisms and WHO technical advisories.
- Government enforced EU Digital COVID Certificates.
- Brussels released tranches of Recovery and Resilience Facility funds (€29 billion total plan).
15. Bulgaria – Kostadin Angov
Appointed during the closing months of Prime Minister Boyko Borisov’s third administration, acting Health Minister Kostadin Angov (2020 – 2021) faced severe criticism from Brussels for Bulgaria’s slow vaccine rollout and limited transparency regarding distribution data. Angov and Borisov’s cabinet were accused of delaying orders through the EU’s joint procurement scheme, preferring to wait for additional safety results before committing to large Pfizer/Moderna contracts.
By late March 2021, Bulgaria had one of the lowest vaccination rates in the European Union and was publicly rebuked by the European Commission for “failure to utilize allocated supply quotas.”
Backdrop: By early 2021, Bulgaria’s center‑right government under Boyko Borisov had lost support amid apparent corruption scandals unrelated to health policy but amplified by public anger over uneven lockdown enforcement and vaccine delays. Multiple cabinet ministers, including acting Health Minister Angov, were called before parliamentary committees to justify the government’s refusal to impose stricter green‑pass rules or to publish full statistics on vaccine deliveries.
Event: In April 2021, Borisov’s GERB party failed to form a coalition following a general election; the president appointed Stefan Yanev as caretaker prime minister, and Stoycho Katsarov — a former deputy minister and health‑reform activist — assumed the health portfolio. Katsarov announced immediate compliance with EU digital pass protocols and promised rapid adoption of the COVID Certificates system, stating that “communication with Brussels must be restored through transparency and vaccination.”
Aftermath: Within three months of the caretaker cabinet’s installation, Bulgaria joined the EU Digital Green Certificate scheme (July 2021), issued its own national app, and implemented tightened entry controls for public venues. The European Commission then approved Bulgaria’s €6 billion Recovery and Resilience Facility allocation (approved December 2021) after earlier postponements linked to “governance deficiencies.”
Katsarov and Yanev argued the shift was strictly technocratic, yet domestic media framed it as the price of unlocking EU funds frozen under Borisov. Moreover, WHO country officers held joint press briefings in Sofia throughout autumn 2021, publicly graduating Bulgaria from a “non‑compliant” to a “fully aligned EU‑health partner.” Later that year a second caretaker cabinet retained the same policies to preserve continued Brussels cooperation.
Government Outcome: By the end of 2021 Bulgaria had moved from partial defiance to complete compliance with EU and WHO health requirements. The turnover of Borisov’s administration and replacement with technocratic caretaker officials effectively cleared the way for release of European recovery funds for health‑system modernization and digital infrastructure projects.
Summary of Sequence
- Initial reluctance to join EU vaccine mandates and delays in accepting digital certificate standards.
- Electoral defeat of incumbent government after months of European pressure and domestic unrest.
- Caretaker administration’s rapid embrace of EU and WHO frameworks.
- Approval of €6 billion in Recovery Funds and re‑establishment of good standing with Brussels.
16. Paraguay – Mario Abdo Benítez
Paraguay’s experience exemplifies how smaller Latin American economies were forced to align pandemic policies with international credit conditions. President Mario Abdo Benítez’s government initially emphasized economic stability over draconian lockdowns, warning that strict restrictions would devastate informal workers who make up more than 60% of the labour market. However, as domestic protests intensified and foreign creditors tightened lending conditions, the administration conceded to the IMF’s stipulations that pandemic‑response financing be tied to specific “public‑health governance commitments.” Once those commitments were accepted, loan disbursements resumed, showing how financial contingency mechanisms coerced health‑policy conformity.
- Backdrop: Through 2020 and early 2021 Paraguay maintained one of South America’s least restrictive lockdown regimes. The government was reluctant to mandate vaccinations or fully close borders with Brazil and Argentina.
- Event: In March 2021 mass protests erupted in Asunción over shortages of medical supplies and alleged corruption in procurement; opposition parties launched a failed impeachment attempt against President Abdo Benítez.
- Aftermath: To restore credit stability, the finance ministry agreed to conditions attached to an IMF Rapid Financing Instrument (≈ $274 million) earmarked for health expenditure auditing and expansion of surveillance systems. By late 2021 Paraguay was fully aligned with WHO and Pan American Health Organization recommendations.
- Outcome: Government stability was restored after external financing resumed, but policy autonomy remained limited by credit conditionality.
17. South Africa – Cyril Ramaphosa
South Africa began as a reluctant participant in strict global pandemic protocols. President Cyril Ramaphosa voiced concerns that extended lockdowns could fuel unrest and economic collapse, and he pushed for Africa‑wide vaccine intellectual‑property waivers rather than Western purchases. Nevertheless, as international ratings agencies threatened downgrades and IMF/World Bank assistance was made contingent on “strengthened public‑health governance,” South Africa shifted its course, introducing some of the continent’s strictest workplace vaccine rules.
- Backdrop: From early 2020 to mid‑2021 Ramaphosa’s cabinet clashed with business unions and community organizations over the cost of lockdowns versus public‑health benefit. Debt pressures soared following a 10% GDP contraction in 2020.
- Event: The National Treasury secured a $4.3 billion IMF loan (July 2020) and a World Bank loan of $750 million (Jan 2022) containing performance benchmarks for pandemic containment and “human capital protection”.
- Aftermath: By December 2021 South Africa announced mandatory vaccination for public‑sector employees and participation in the WHO vaccine passport initiative. Foreign aid disbursement and sovereign bond ratings stabilized only after these steps.
- Outcome: Policy alignment improved credit access but deepened domestic inequality and led to significant civil‑liberty litigation and ongoing parliamentary inquiries into procurement transparency.
18. Mexico – Andrés Manuel López Obrador
Mexico under Andrés Manuel López Obrador (AMLO) presented one of the last major cases of gradual capitulation to WHO and multilateral financial pressures. Initially AMLO resisted mandatory lockdowns and booster campaigns, insisting that national public‑health policy should focus on nutrition and poverty reduction. However, a combination of supply‑chain disruption, dollar liquidity concerns, and lobbying from international philanthropic networks (CEPI, GAVI, and the Gates Foundation) eventually pushed Mexico toward full policy compliance by 2022.
- Backdrop: Throughout 2020 Mexico’s Health Secretary Jorge Alcocer and Under‑secretary Hugo López‑Gatell advocated moderate restrictions and non‑coercive vaccine rollout. The country’s mortality surged during mid‑2021, provoking foreign and domestic pressure for a policy shift.
- Event: Facing threat of credit downgrades, the Finance Ministry began talks with the World Bank and IMF for infrastructure loans linked to public‑health reform. In December 2021 Mexico signed a joint memorandum of understanding with WHO and CEPI for “bio‑pharmaceutical collaboration and vaccine development capacity”.
- Aftermath: Through 2022 Mexico aligned its vaccine certification systems with the COVAX framework and expanded digital health records for the Ministry of Health, unlocking up to $1 billion in World Bank Covid‑response financing.
- Outcome: By 2023 Mexico was publicly touted by WHO offices as a “model for integrated pandemic response,” demonstrating how international credit leverage transformed a once‑independent policy line into strict adherence with global health‑security standards.
Summary of Observable Trends
- Chronology: Deaths of Nkurunziza, Dlamini, Bakayoko, Magufuli, and Moïse opened the sequence (Jun 2020 – Jul 2021). Political collapses in Europe, Asia, and the Americas followed through 2022.
- Policy effect: Every successor endorsed WHO recommendations and entered international funding arrangements that had been unavailable under predecessors.
- Financial trigger: Aid packages—IMF Rapid Credit, World Bank preparedness loans, EU Recovery mechanisms—were routinely disbursed within 30–90 days of the leadership change.
Key Takeaway
From 2020 to 2022, the result was unmistakable: national autonomy collapsed beneath a synchronized agenda linking public‑health compliance to economic salvation. Countries that resisted early, especially in Africa, suffered the hardest blows—five sitting leaders dead in one year. More powerful nations experienced subtler coups through scandal, protest, or economic blackmail, all producing the same end state.
What emerged from these parallel crises was not medical harmony but political homogenization. Each successor declared a “renewed partnership with science,” welcomed new funding from the IMF, World Bank, or GAVI, and ushered in digital‑compliance systems that now define post‑pandemic governance.
By the end of 2022 nearly every government on Earth—rich or poor, democratic or autocratic—had been brought into alignment. Differing flags, languages, and histories no longer prevented one shared choreography: resistance punished, obedience financed, and sovereignty quietly exchanged for a coordinated global script.
- IMF Press Release – Rapid Credit Facility for Burundi (June 2020).
- Reuters / AP Report – Death of Eswatini Prime Minister (Dec 2020).
- African Development Bank – COVID‑19 Response Support Programme (2021).
- World Bank – Ivory Coast Emergency Support Project (2021).
- IMF Press Release No. 21/210 – Tanzania RFI (Sept 2021).
- Associated Press – “President of Haiti Assassinated at Home” (July 2021).
- IDB Official Statement on Haiti Relief Funding (2021).
- Japan Cabinet Office – Resignation of PM Abe (Aug 2020).
- Nikkei Asia – “Japan Invests in mRNA Manufacturing” (2022).
- 1European Commission – Next Generation EU Fund Allocation to Slovakia (2021).
- Czech News Agency – Election Results and Policy Changes (2021).
- Austrian Prosecution Service – Kurz Investigation Report (2021).
- EU Council Press Release – Austria ESM Allocation (2022).
- UK Parliamentary Record – Digital Health Infrastructure Funding (2022).
- IMF Staff Report – Sri Lanka Extended Fund Facility (March 2023).
- World Bank – Brazil Pandemic Preparedness Loan (2022).
- WHO Madagascar Country Office – Cooperation Agreement (2021).
- European Commission – Romania RRF Approval (2021).
- European Commission – Bulgaria RRF Approval (2021).
- IMF Country Report – Paraguay Pandemic Financing (2021).
- IMF Country Report – South Africa Fiscal Support Arrangements (2021).
- WHO / CEPI Press Release – Mexico Cooperation Agreement (2022).
- IMF Country Report – Paraguay Rapid Financing Instrument 2021.
- BBC News Latin America – “Protests Rock Paraguay Over Pandemic Supplies,” March 2021.
- Finance Ministry of Paraguay – Press Release on IMF Commitments April 2021.
- South African Reserve Bank Annual Report 2021.
- IMF Press Release No. 20/315 – South Africa Loan Approval; World Bank Loan Press Brief 2022.
- Reuters – “South Africa Adopts Mandatory Public‑Sector Vaccination Policy,” December 2021.
- El Universal – “López‑Gatell Sabemos que no habrá vacunación obligatoria,” 2020.
- WHO / CEPI – Memorandum on Mexico Vaccine Collaboration, December 2021.
- World Bank – “Mexico COVID‑19 Emergency Response Project,” 2022.
October 30, 2025
Posted by aletho |
Civil Liberties, Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine, Human rights |
Leave a comment
Consider this data
For anyone contemplating getting an influenza vaccine (flu shot) or planning to pressure or mandate someone else to get one:
A meta-analysis of existing flu shot studies of healthy children by Cochrane (effectively owned by vaccine zealot Bill Gates) concluded that despite decades of published studies, it “could find no convincing evidence that [flu] vaccines can reduce mortality, hospital admissions, serious complications, or community transmission of influenza.”
Read that carefully: no convincing evidence—none—that flu shots lowered the chances of dying, being admitted to the hospital, suffering serious complications from the flu, or transmitting the flu to others.
In fact, studies have found those vaccinated for flu have a statistically significant increased rate of respiratory illnesses. Meaning, it increases the risk of having other respiratory illnesses.
For example, a placebo-controlled efficacy (not safety) study by researchers at the University of Hong Kong compared children receiving influenza vaccine with those who did not receive the vaccine. The study found no statistical difference in the rate of influenza between the groups but did find the vaccinated had a four times increased rate of non-influenza infections (“recipients had an increased risk of virologically confirmed non-influenza infections (relative risk: 4.40; 95% confidence interval: 1.31-14.8)”).
As another example, researchers at Columbia University found that the risk of “influenza in individuals during the 14-day post-vaccination period was similar to unvaccinated individuals during the same period (HR 0.96, 95% CI [0.60, 1.52])” but that the risk of “non-influenza respiratory pathogens was higher [in the vaccinated individuals] during the same period (HR 1.65, 95% CI [1.14, 2.38]).”
A study by the Cleveland Clinic of 53,402 of its employees across multiple states even found an increased risk of influenza among those vaccinated for influenza, explaining that the “cumulative incidence of influenza was similar for the vaccinated and unvaccinated states early, but over the course of the study the cumulative incidence of influenza increased more rapidly among the vaccinated than the unvaccinated.”
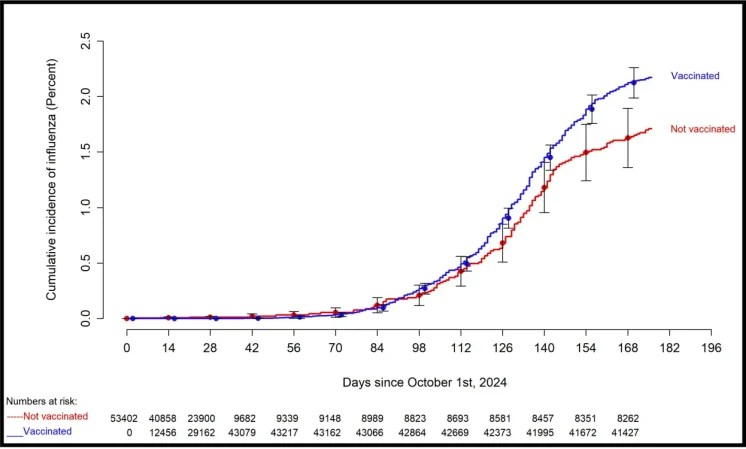
From the Cleveland Clinic study
I discuss these and other studies in my book, Vaccines, Amen.
That said: get a flu shot, don’t get a fu shot. That’s freedom. Everyone should be free to choose. But nobody should be coerced to get this or any medical product, especially, ironically, when the data reflects it has a net overall increase in infections.
If you do choose to get this product and are injured, you are always free to call our firm to represent you in the Vaccine Injury Compensation Program.
October 26, 2025
Posted by aletho |
Book Review, Science and Pseudo-Science, Timeless or most popular | Human rights, United States |
Leave a comment
A recent article at the BBC, “Government told to prepare for 2C warming by 2050,” claims that the United Kingdom needs to prepare for increasing extreme weather as the planet approaches 2°C warming. This is false in its framing. Although it’s always a good idea to harden infrastructure against weather, the UK is not suffering more extreme weather due to human emissions of carbon dioxide, and the recommendation of attempting to prevent temperature rise is not going to help anyone.
The BBC’s post discusses a letter written by the UK government’s “Climate Change Committee” (CCC), which the BBC reports said, “[t]he country was ‘not yet adapted’ to worsening weather extremes already occurring at current levels of warming, ‘let alone’ what was expected to come.”
The CCC asked the government to “set out a framework of clear long-term objectives” to prevent further temperature rise, with new targets every five years and departments “clearly accountable” for delivering those goals. It warned that “a global warming level of 2C would have significant impact on the UK’s weather, with extreme events becoming more frequent and widespread.”
These include increases in heatwaves, droughts, floods, and longer wildfire seasons.
These claims are fearmongering, and no amount of deindustrialization – which is what’s implied by the “objectives to prevent further temperature rise”—will stop bad weather from happening, nor will it have any measurable impact on global average temperature.
The simple fact is that the UK contributes a very small amount of carbon dioxide to the atmosphere, which would in theory contribute an even smaller amount to warming. According to emissions data, the global share of all UK carbon dioxide emissions is 0.88 percent. Not even 1 percent. Eliminating UK emissions would do absolutely nothing to slow or stop any amount of warming that could be connected to human emissions, if they are, in fact, driving temperature changes.
On top of that, data do not show that weather is becoming more extreme in the UK.
The BBC claims that global warming will increase the wildfire season in the UK, and presumably they believe it must have already done so during the past 150 years of planetary warming. A longer wildfire season should result in more fires. Available data, however, does not show that wildfires are getting more frequent or more intense in the UK. Satellite data from Copernicus show no trend at all.
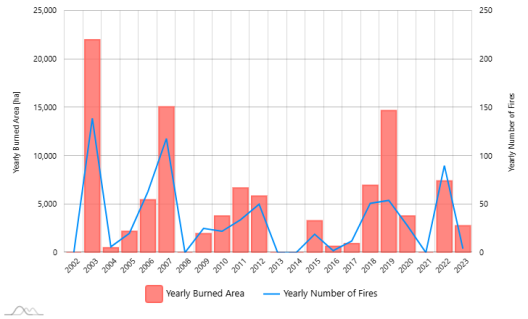
Chart of United Kingdom yearly burned area and number of fires from Copernicus
For another example, looking at Central England as this Climate Realism post did, the number of days per year breaching 25°C (77°F) show no rising trend, nor does the measured highest daily maximum.
Long term historical data for Europe show that drought is likewise not worse today than it was during the Renaissance, long before industrialization.
What is really notable is that Europe alone has actually already warmed 2°C since about 1820, according to historic European temperature averages, but no catastrophic change in weather has occurred. (See figure below)
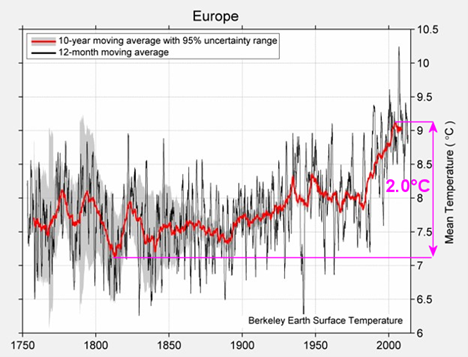
Berkeley Earth average European temperature showing a 2.0°C rise since about 1820. Source: http://berkeleyearth.lbl.gov/regions/europe
Weather isn’t getting worse, but bad weather does still happen. The UK’s largest industrial solar facility, for example, blighting the landscape of Anglesey, North Wales, was recently destroyed by a bad storm. That should be enough to give government agencies pause when it comes to at least some net-zero policies, but the real point is that hardening infrastructure against weather should be a priority regardless of climate change. Bad weather will occur, and it will wreck fragile facilities, including solar complexes.
Hardening against weather extremes, which always have and always will exist, is just common sense. As technology develops and new ways of protecting against bad weather are discovered (like the invention of air conditioning) they should be implemented where they can be, as they can be. Achieving net zero – especially for a country that emits negligible amounts of greenhouse gases anyway—will not save the UK from bad weather events.
As a news organization, the BBC should not carry water for its government or government advisory boards that want to continue wasting money on futile “objectives to prevent further temperature rise” when direct efforts to improve infrastructure and harden it against weather extremes, which have happened throughout history, would be far more effective in saving lives and reducing harm.
October 23, 2025
Posted by aletho |
Fake News, Mainstream Media, Warmongering, Malthusian Ideology, Phony Scarcity, Science and Pseudo-Science | UK |
Leave a comment
A coalition of city public health officials with ties to pharma investor George Soros is urging the public to “get vaccinated.”
In an open letter, the Big Cities Health Coalition accused federal officials of driving down vaccination rates and fueling an increase in dangerous infectious disease outbreaks by making “repeated false claims” about vaccines.
They wrote:
“Vaccines have eradicated devastating diseases and saved millions of lives. They keep classrooms safe and schools open. They allow children to spend time with friends and enjoy their favorite activities. They help parents and caregivers work to support their families.
The letter also addresses recent changes to the Centers for Disease Control and Prevention’s (CDC) recommended vaccine schedule for children and adults, though it does not mention U.S. Health Secretary Robert F. Kennedy Jr. or President Donald Trump by name.
The coalition, which represents 35 U.S. cities and about a fifth of the U.S. population, “has been working together to exchange ideas and address public health threats for more than two decades,” according to CNN, which first reported on the letter Monday.
Participating cities include New York, Los Angeles, Chicago, Boston, Houston, Dallas, Cleveland, Milwaukee and Seattle.
The group’s financial documents reveal support from billionaire financier Soros. Soros has also invested heavily in the pharmaceutical industry, including COVID-19 vaccine makers Pfizer and AstraZeneca, and Gilead Sciences, which produces remdesivir, a controversial antiviral treatment frequently given to COVID-19 patients.
Coalition attempted to scrub funding from Soros- and Gates-linked groups
The Big Cities Health Coalition was founded in 2002, according to a now-deleted webpage. The current version of its website contains little more than the group’s recent letter.
Links to the organization’s 2023 and 2024 annual reports are no longer active, but can be found on the Internet Archive and elsewhere. The reports show that Soros and other major healthcare-related organizations, including groups connected to Bill Gates, finance the coalition.
According to its 2023 annual report, the Open Society Foundations, founded by Soros, funded the coalition. Other funders include the Robert Wood Johnson Foundation, the W.K. Kellogg Foundation, healthcare provider Kaiser Permanente and the CDC Foundation.
In 2022, the Soros Economic Development Fund, an extension of the Open Society Foundations, partnered with Gavi, the Vaccine Alliance and MedAccess, a pharma-industry broker connected to the U.K. government, to invest $200 million in developing COVID-19 vaccines.
The Gates Foundation is a major funder of Gavi.
The Robert Wood Johnson Foundation has financially supported FactCheck.org, which previously flagged COVID-19-related “misinformation” for Facebook.
The CDC Foundation’s donor list includes the World Health Organization, the Gates Foundation and vaccine manufacturers including Pfizer, Merck and Johnson & Johnson.
According to internal medicine physician Dr. Clayton J. Baker, the coalition’s annual reports reveal clear conflicts of interest.
“It’s informative to look into the funding of organizations like the Big Cities Health Coalition,” Baker said. He noted that Kaiser Permanente paid patients $50 to get COVID-19 vaccines during the pandemic and fired employees who refused the shots, then tried to rehire them later when short-staffed.
According to the coalition’s Form 990 for fiscal year 2023, the organization spent $875,540 on “communications,” including engaging with “media, and federal policymakers about the importance of supporting local public health and health equity.”
The group also spent $433,703 on its “urban health agenda” and $147,397 on “equity/racial justice.”
The coalition’s members “meet periodically with Congressional staff” and “other federal government officials,” the filing states.
The organization’s schedule of contributors is listed as “restricted” in the filing.
Coalition blames unvaccinated for ‘deadly’ and ‘more frequent’ outbreaks
In its letter, the coalition blamed “declining” vaccination rates for “deadly outbreaks of diseases like measles and polio” and claimed that the outbreaks are “becoming more frequent.”
CNN reported that measles exposure at a South Carolina school led authorities to quarantine over 100 unvaccinated students, illustrating “one of the many reasons why Big Cities Health Coalition emphasizes the importance of vaccination.”
Research scientist and author James Lyons-Weiler, Ph.D., said that invoking measles and polio is a “manipulative framing device.” He said:
“Outbreaks of these diseases occur almost exclusively in highly vaccinated populations where immunity has waned, or where sanitation and migration variables are misattributed as ‘vaccine refusal.’
“By portraying every outbreak as proof of anti-vaccine rhetoric, the coalition seeks to recapture moral high ground based on presumptions of safety, without addressing the underlying immunologic and ecological data.”
The coalition’s letter also warned of a potential uptick of COVID-19 and flu infections in the “rapidly approaching” cold and flu season.
However, Baker said the coalition’s letter “contains absolutely zero genuine evidence” to support its claims. He said:
“The coalition’s statement is embarrassingly inane. They say, ‘We are united behind a simple message: get vaccinated.’ Vaccinated with what? They make no distinction between necessary or unnecessary, safe or unsafe, effective or ineffective shots. Just ‘get vaccinated.’ That’s like saying ‘get medicated.’ This is the asinine level of rhetoric to which vaccine fanatics are currently reduced.”
Emily Hilliard, press secretary for the U.S. Department of Health and Human Services (HHS), dismissed the coalition’s concerns.
“HHS is restoring the doctor-patient relationship so people can make informed decisions about their health with their providers,” Hilliard told The Defender.
Letter rooted in data, not ‘political ideology,’ coalition members say
Coalition members told CNN their letter is an attempt to restore public trust in science, not an effort to politicize public health recommendations.
“We have to make our public health decisions based on data and not on political ideology,” Dr. Philip Huang, director of the Dallas County Health and Human Services Department, told CNN. “We have to be the voices for that science and reason.”
Huang said the current CDC administration “seems more driven by political ideology than actual data and science, so it undermines the trust.”
Lyons-Weiler disputed the coalition’s claims, calling the letter “the opening salvo in an attempt to rebuild centralized narrative control over immunization policy.”
“Language such as ‘talk with your doctor’ and ‘tune out political noise’ is designed to sound apolitical while reinstating top-down message discipline,” he said.
CDC changes to vaccine policy spark pushback across U.S.
The coalition “is the latest group to take a strong public stand in support of vaccination as a direct response to concerns that the federal government is limiting access and raising doubts,” CNN reported.
Earlier this month, the CDC updated the childhood immunization schedule to recommend individual-based decision-making regarding COVID-19 vaccination for children 6 months and older, following the CDC’s Advisory Committee on Immunization Practices (ACIP) unanimous vote to adopt the recommendation.
Last month, ACIP also voted to recommend limiting the MMRV (measles, mumps, rubella and varicella, or chickenpox) vaccine to children ages 4 and older. And in June, the committee voted to stop recommending flu shots containing thimerosal — a preservative linked to neurodevelopmental disorders.
In response, 15 Democratic governors launched the Governors Public Health Alliance last week to coordinate their public health efforts independently of national public health agencies.
Previously, four Western states announced the formation of the West Coast Health Alliance, which aims to issue its own immunization guidelines.
In August, the American Academy of Pediatrics (AAP) issued “evidence-based” recommendations calling for COVID-19 shots for infants, young children and children in “high-risk” groups. In July, the AAP and five other medical organizations sued Kennedy over new COVID-19 vaccine guidance.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
October 23, 2025
Posted by aletho |
Deception, Science and Pseudo-Science | Boston, Chicago, Cleveland, Dallas, Gates Foundation, Houston, Los Angeles, Milwaukee, New York, Open Society Foundations, Seattle, United States |
Leave a comment
Yesterday, I took part in a panel discussion in Washington, D.C., on the weaponisation of science — specifically, how conflicts of interest, industry influence, and scientific deception have reshaped modern medicine.
It was an important conversation about how the scientific process has been hollowed out by financial incentives, regulatory capture, and institutional cowardice.
For me, this is not an abstract debate. I’ve spent much of my career investigating how science becomes distorted — not by a few rogue actors, but through an entire system built on commercial dependence.
Once you start pulling the threads of how evidence is produced, who funds it, who controls the data, and who polices the outcomes, you quickly realise that the corruption of science is structural and systemic.
The Statin Wars: a case study in deception
I first saw this clearly while investigating cholesterol-lowering drugs. My 2013 Catalyst documentary questioned whether statins were being overprescribed, and it unleashed a media firestorm.
The episode was pulled after industry outrage, and I was publicly attacked. None of the critics engaged with the evidence — they simply sought to silence it.
In 2018, I published a narrative review, “Statin wars: have we been misled by the evidence?”
The piece revealed that the raw data underpinning statin trials were held exclusively by the Oxford-based Cholesterol Treatment Trialists (CTT) Collaboration and had never been released.
The CTT group had signed confidentiality agreements with pharmaceutical sponsors, blocking independent access to the raw data and preventing verification.
Yet those same meta-analyses have shaped prescribing guidelines around the world — produced by a group that sits under Oxford’s Clinical Trial Service Unit, which receives millions in funding from statin manufacturers.
In my public talks, I’ve described the statin story as a case study in bias and censorship. The trials used well-worn techniques to amplify benefits and minimise harms.
For example, they use ‘run-in’ periods before the trial to weed out people who couldn’t tolerate the drug, thereby artificially lowering the adverse events detected during the trial.
Often the outcomes were reported in relative, not absolute, terms — effectively exaggerating benefits that were, in reality, minuscule to the individual patient.
The vast majority of statin trials are funded by the manufacturers, and almost all show benefit — except for one publicly funded study that showed the opposite.
So, who funds the trial matters. The system is captured, plain and simple.
Regulatory capture and the illusion of oversight
The same dynamics pervade drug regulation. In a 2022 BMJ investigation, I showed how drug regulators rely heavily on funding from the very industries they oversee.
In Australia, the Therapeutic Goods Administration derives 96% of its operating budget from industry fees.
In the U.S., the same conflict exists through the Prescription Drug User Fee Act (PDUFA), which allows the FDA to collect billions from drug companies.
Those “user fees” now fund roughly two-thirds of the agency’s drug-review budget — a structural conflict of interest described by one scholar as “institutional corruption.”
And it’s true.
Industry money drives the demand for faster approvals through “expedited pathways,” which often means weaker evidence, shorter trials, and looser post‑marketing obligations.
Regulators defend this as “innovation,” yet the drugs approved under these pathways are far more likely to later receive black-box warnings or be withdrawn from the market due to safety issues.
The result is a system that rewards speed and sales over safety and substance.
The illusion of effective drugs has become even clearer thanks to a landmark investigation this year by Jeanne Lenzer and Shannon Brownlee.
They reviewed more than 400 FDA drug approvals between 2013 and 2022, and found that 73% of the drugs failed to meet four basic scientific criteria for demonstrating effectiveness.
Cancer drugs were especially problematic: only 3 out of 123 met all scientific standards, most approved on surrogate endpoints with no evidence they improved survival.
It’s the perfect illustration of regulatory capture — an agency funded by industry fees and pressured by politics, approving drugs of uncertain benefit while calling itself the “gold standard.”
Antidepressant deception
The same playbook has unfolded in psychiatry — beginning with how clinical trials are designed and reported.
Study 329 is one of the best-known examples. It claimed that paroxetine (Paxil) was safe and effective for adolescents aged 12 to 18.
But when researchers reanalysed the original regulatory documents, they found that suicides and suicide attempts had been coded under misleading terms such as “emotional lability” or “worsening depression,” effectively erasing them from view.
A similar pattern emerged when regulatory documents for two fluoxetine (Prozac) trials in children and adolescents were re-examined. Suicide attempts were omitted or misclassified, making the drug appear safer than it was.
Both reanalyses were carried out under the Restoring Invisible and Abandoned Trials (RIAT) initiative, a project dedicated to “restoring” abandoned or misreported trials by publishing accurate versions of the data submitted to regulators.
Selective publication compounds the problem.
The FDA only requires two trials demonstrating a drug is better than placebo before it is approved – meaning multiple failed trials get buried.
Psychologist Irving Kirsch, using Freedom of Information requests, uncovered dozens of unpublished SSRI trials that had been withheld from the medical literature.
When those missing studies were included, the apparent benefit of antidepressants over placebo almost vanished — an average gain of less than two points on the Hamilton Depression Scale, far below the threshold for meaningful clinical benefit.
In other words, much of what appears to be a “drug effect” is, in reality, placebo.
For years, patients have also been sold the marketing myth that depression stems from a “chemical imbalance” in the brain — a debunked theory but an extraordinarily effective sales campaign.
In 2020, we analysed popular health websites across ten countries and found that about 74% falsely claimed depression was caused by a chemical imbalance and implied that antidepressants could correct it.
It may sound like harmless messaging, but its influence is profound.
An Australian study showed that 83% of people who were told they had a chemical imbalance were more likely to take an antidepressant, believing it would “fix” their brain chemistry.
A more recent review in Molecular Psychiatry synthesised the best available evidence and found no consistent link between depression and low serotonin levels or activity.
Together, these findings reveal how psychiatry’s modern narrative was constructed — through distorted trials and deceptive marketing — turning uncertainty into certainty, and speculation into “science.”
Fraud by omission
Recently, I reported on how journals can weaponise science.
The BMJ’s Peter Doshi raised serious concerns about the pivotal PLATO trial for the anti-clotting drug ticagrelor — including data irregularities and unexplained deaths. But the journal Circulation that published the trial, has refused to investigate.
This selective vigilance is telling. Journals will retract small hypothesis papers that challenge orthodoxy, but billion‑dollar drugs with questionable data remain untouchable.
We’ve seen an even more aggressive form of suppression in the vaccine arena.
The recent Covaxin case exposed the extent to which manufacturers will go to suppress inconvenient findings.
After Indian researchers published a peer‑reviewed post‑marketing study suggesting serious adverse events “might not be uncommon,” Bharat Biotech — the vaccine’s manufacturer — filed a defamation lawsuit against the 11 authors and the journal’s editor, demanding retraction and millions in damages.
Within weeks, the journal caved, announcing its intention to retract despite finding no scientific fraud or fabrication. The only “offence” was to suggest that further safety research was warranted.
It’s a chilling example of how corporate and political power now overrides the normal mechanisms of scientific debate — a new form of censorship disguised as quality control.
Punishing scientists
The weaponisation of science isn’t only about suppressing inconvenient ideas or studies—it extends to the scientists themselves.
During the Vioxx scandal, Merck was caught keeping an actual “hit list” of doctors and academics who criticised the drug’s cardiovascular risks.
Internal emails revealed executives discussing plans to “seek them out and destroy them where they live.” That’s how far industry will go to silence dissent.
Executives are no longer stupid enough to put such threats in writing, but the behaviour persists — now outsourced to lobby groups and front organisations that quietly destroy reputations.
I experienced a version of this myself after my ABC documentaries on statins and sugar.
Like Merck, the Australian Breakfast Cereal Manufacturers Forum – an industry front group – drew up an “active defence” plan to neutralise me for challenging the industry narrative.
And we’ve seen it again recently with the leaked BIO memo detailing a coordinated plan to undermine Health Secretary Robert F. Kennedy Jr. — by co-opting media influencers, partnering with think tanks, and shaping public perception.
Different industries, same playbook: when billions are at stake, dissent is dangerous, and science becomes a weapon.
Weaponised fact-checkers
Look at the rise of fact-checking as a weapon.
In 2024, for example, a peer‑reviewed Japanese study published in the journal Cureus that reported a statistical rise in certain cancers following the Covid‑19 mRNA vaccine rollout was retracted after a Reuters “fact check.”
The authors, led by Dr Miki Gibo, made no claim of causation and had explicitly called for further investigation, yet the journal retracted the paper after the media controversy, citing concerns about the scrutiny of fact checkers.
When journals begin outsourcing editorial judgment to media organisations with commercial or institutional conflicts, peer review itself collapses under the weight of narrative control.
This is what I mean by the weaponisation of science.
Fraud today isn’t only about fabricating data — it’s about what institutions choose to suppress. It’s selective enforcement designed to protect profits under the guise of integrity.
Can we restore scientific honesty?
I’m not going to pretend I have all the answers. Whether it’s cholesterol or serotonin, the science too often bends toward profit rather than truth.
Regulators, journals, and academic institutions have become so financially entangled with industry that truly independent science is now the exception, not the rule.
Retractions, fact-checks, and editorial bans are deployed selectively — not to correct fraud, but to erase debate under the banner of “scientific consensus.”
We’ve tried to fix this with transparency measures like open-data policies and the Sunshine Act, which expose payments from pharmaceutical companies to doctors.
But disclosure has become a box-ticking exercise and raw data is still hard to get. Meanwhile, the machinery of influence keeps turning.
The deeper problem is the absence of accountability. Without accountability, there can be no trust.
When Merck’s painkiller Vioxx was withdrawn after being linked to tens of thousands of deaths, not one executive went to jail. The company paid fines, issued statements, and carried on.
Lives were lost, and no one was held personally responsible. That isn’t justice — it’s the “cost of doing business,” and worse, the people who preside over these disasters are often rewarded for them.
Bonuses are paid, stock options soar, and departing CEOs collect multimillion-dollar severance packages — all while families are left to bury their dead.
If we’re serious about restoring trust, that has to change. CEOs and senior executives who knowingly conceal data or market dangerous drugs should face criminal penalties, not corporate settlements.
A few jail sentences at the top would do more to restore trust in medicine than a thousand press releases about a renewed commitment to safety.
Accountability must also extend to government.
The FDA and other regulators are structurally dependent on industry money. It’s baked into the system, and the only real solution is to rebuild — fund these agencies publicly, remove user fees, and make them independent again.
The barrier isn’t money — it’s political will, compromised by the same corporate lobbying and campaign donations that distort science.
True reform requires the courage to confront the pharmaceutical industry’s financial grip on both major parties, to end the political donations that buy silence, and to legislate for genuine independence in science and medicine.
Perhaps Secretary Kennedy is now best placed to begin dismantling industry’s hold on science. Systemic corruption didn’t happen overnight, and it won’t be undone overnight either.
Commercial conflicts of interest have become normalised — woven through our institutions, universities, journals, and political culture. Until that’s confronted directly, nothing will change.
Disclosure is necessary, but it is not sufficient. The antidote is open debate, public funding, and real accountability.
Science should never be about consensus; it should be about contestability. If we can’t test claims, challenge data, or ask uncomfortable questions without fear of retribution, then we no longer have science — we have marketing.
The weaponisation of science ends only when truth becomes more valuable than profit.
October 23, 2025
Posted by aletho |
Corruption, Deception, Science and Pseudo-Science, Timeless or most popular | Statins |
Leave a comment
Practitioners of rigorous scientific methodology — from the 17th century’s Galileo to 1965’s winner of the Nobel Prize in Physics, Richard Feynman — would consider today’s climate research an embarrassment, shaped by uncritical orthodoxy and zealotry rather than genuine testing of hypotheses.
Classical science welcomes skepticism. It thrives in an environment where debate and revision are encouraged. Today’s climate conformists declare the debate “settled” and label those with questions as deniers, effectively outlawing the skepticism that drives scientific progress.
Plenty of 21st-century scientists have objected to this travesty. Dr. Matthew Wielicki, formerly of the University of Alabama, put it bluntly: “Science should be self-correcting. Climate science isn’t. It’s self-preserving.”
Dr. Richard Lindzen of the Massachusetts Institute of Technology notes that climate dogma has little to do with evidence: “The narrative is a quasi-religious movement predicated on an absurd scientific narrative.”
In essence, modern climate science has been transformed into a political apparatus dominated by campaign-style advocacy, subverting the foundational principles of evidence-based inquiry.
Climate cultists treat every warming or cooling event as anthropogenic by default, ignoring millennia of natural variation. “While substantial concern has been expressed that emissions may cause significant climate change, measured or reconstructed temperature records indicate that 20th- and 21st-century climate changes are neither exceptional nor persistent, and the historical and geological records show many periods warmer than today,” say scientists writing to the American Physics Society.
Gregory Wrightstone, geologist and best-selling author of A Very Convenient Warming, says that the longer geological record reveals numerous epochs with much higher temperatures and levels of atmospheric CO₂, all predating the influence of modern human activity.
Wrightstone rejects descriptions of current conditions as dangerous, saying that “Earth is growing greener, and temperature-related deaths are declining.” The evidence indicates the planet is not imperiled but flourishing.
Deaths from natural disasters are at historic lows, life expectancy continues to climb, and global crop yields in both advanced and developing economies are at record highs. Rising atmospheric CO2 is associated with improved plant growth, not planetary degradation.
The much-hyped “disappearing islands” of the Pacific continue to exist. Many atolls have grown in size due to coral and sediment accumulation. Arctic sea ice, too, has refused to vanish; the 2025 minimum extent is nearly half a million square kilometers larger than 2007.
Yet none of these realities make it into school textbooks or U.N. briefings. The crisis narrative is perpetuated to sustain a trillion-dollar “green” industry dependent on fear, political support and publicly financed subsidies.
Error-riddled computer models that back doomsday predictions violate core tenets of scientific methodology. When tested against known outcomes, they routinely fail.
In 2014, Dr. Roy Spencer compared real-world satellite data with over 90 climate models. Nearly all the models exaggerated warming. Spencer summarized the absurdity: “If 95% of your models disagree with observations, the models are wrong — not reality.”
Dr. William Happer, a physicist at Princeton University and former scientific advisor to the U.S. government, notes: “Observations anchor our understanding and weed out the theories that do not work. This has been the scientific method for more than 300 years… computer models are not meant to replace theory and observation and to serve as an authority of their own.”
Yet these models drive the global policy agenda. The insistence on short time frames and cherry-picked data appear to support catastrophic scenarios; long-term geological records contradict them. Steve Milloy, author of JunkScience.com, described the phenomenon perfectly: “Climate science has become a political enterprise. The conclusion comes first; the data are adjusted later.”
Science belongs to critical thinkers, not to committees. The climate establishment will collapse as its funding dries up or the public stops believing its prophets. Reality will win — as it always does — but the longer the struggle, the higher the human cost of irrational policies.
Reason, empirical investigation and intellectual freedom have been undermined by a politically charged climate movement, which is a threat to science and civilization itself.
Vijay Jayaraj is a Science and Research Associate at the CO2 Coalition, Fairfax, Virginia. He holds an M.S. in environmental sciences from the University of East Anglia and a postgraduate degree in energy management from Robert Gordon University, both in the U.K., and a bachelor’s in engineering from Anna University, India.
October 20, 2025
Posted by aletho |
Malthusian Ideology, Phony Scarcity, Science and Pseudo-Science |
Leave a comment





