Evidence Against COVID-19 Vaccines in Medical Journals Continues to Grow
BY DR RAPHAEL LATASTER | THE DAILY SCEPTIC | SEPTEMBER 7, 2023
As a university academic, and former pharmacist, whose speciality is misinformation, disinformation and fake news, I have been very active of late in collecting (and writing) papers appearing in medical journals that provide evidence and arguments against the COVID-19 vaccines. Below is a summary of some of the recent papers I find to be most concerning.
Vaccine effectiveness and safety exaggerated
An article appearing in the Journal of Evaluation in Clinical Practice, including BMJ Editor Peter Doshi amongst its authors, discusses several biases that, if not accounted for, indicate that the effectiveness of the mRNA COVID-19 vaccines in observational studies is being heavily exaggerated. The most important appears to be one many of us have worried about from the beginning, the dubious ‘case-counting window bias’, which concerns the seven days, 14 days or even 21 days after the jab where we are meant to overlook jab-related issues, particularly poor effectiveness, as “the vaccine has not had sufficient time to stimulate the immune system”. In an example using some data from Pfizer’s clinical trial, the authors show that thanks to this bias, a vaccine with effectiveness of 0%, which is confirmed in the hypothetical clinical trial, could be seen in observational studies as having effectiveness of 48%.
In a follow-up article in the same journal I revealed ways in which the situation may even be worse. The aforementioned ‘case-counting window bias’ is often accompanied by a ‘definitional bias’, whereby the Covid cases in the vaccinated are not just ignored, but shifted over to the unvaccinated. So building on the above example, a vaccine with 0% effectiveness can actually be perceived as having 65% effectiveness. My article also shows, touching on the intriguing (horrifying?) issue of negative effectiveness, “a vaccine with minus-100% effectiveness, meaning that it makes symptomatic COVID-19 infection twice as likely, can be perceived as being 47% effective”. Furthermore, “Repeated calculations will show that moderate vaccine effectiveness is still perceived even with actual vaccine effectiveness figures of minus-1,000% and lower”. I also explained that this exaggeration could equally apply to studies on vaccine safety, which would be important when comparing the overall health of the vaccinated and unvaccinated, as may be appropriate when looking into the mysterious rise in non-Covid excess deaths post-pandemic.
Doshi, joined by one of his earlier co-authors, decided to produce another article in the same journal, a follow-up to my follow-up, shifting the focus from observational studies to the clinical trials. They found that case counting “only began once participants were seven days (Pfizer) or 14 days (Moderna) post Dose 2, or approximately four to six weeks after Dose 1”. The obvious implication:
Decisions on when to initiate the case counting window affected calculations of vaccine efficacy. Because cases occurring in the four to six weeks between Dose 1 and the case counting window were excluded, reported vaccine efficacy against COVID-19 (the primary endpoint) at the time of Emergency Use Authorisation was higher than what would have been calculated had all COVID-19 cases after Dose 1 been included, as in a conventional Intent-to-Treat analysis.
They also found that “different case counting windows” were used at different times, ‘coincidentally’ yielding better results.
Not yet published, though under peer review, is my intended fourth and final article in this unofficial ‘series’. Firstly, I justify my earlier concern of exaggerated safety in observational studies, or studies built on observational data and models rather than data from controlled trials, by discussing a recently published paper in another journal, noting how the authors only count vaccine adverse effects from 14 days after the second dose (or seven days after the latest booster shot), and stopping the count at around four to five months. As if to highlight the potential magnitude of safety exaggeration with so many adverse effects being overlooked, the study, flawed as it is, showed only a very slight net benefit to vaccination. A more complete view of adverse effects (as well as cases in the ‘partially vaccinated’) could easily lead to the conclusion that the risks of COVID-19 vaccination outweigh the benefits. I also explain that there are issues with the adverse effect counting windows in the clinical trials in relation to their short length. The safety monitoring ends mere months after vaccination, though adverse effects can manifest clinically years later.
Vaccine-induced myocarditis and young males
In the latter article, and in a rapid response published by BMJ Open, I also discuss recent evidence and journal articles on myocarditis, with one finding a “Covid vaccine-induced myocarditis incidence rate of around one in 100,000, and around one in 19,000 for males between the ages of 12 and 17 years”. These authors also found that a significant number of people with Covid vaccine-induced myocarditis end up dead soon afterwards. Go ahead and contrast this with the U.K. Government’s determination of numbers needed to vaccinate to prevent a severe Covid hospitalisation being in the hundreds of thousands for young ‘no risk’ groups.
In research I hope to be published soon, I show how Pfizer estimates an even greater incidence of myocarditis in young males, and it also estimates that one million vaccinated will result in zero to one saved lives. Yes, zero is included as a real possibility. By Pfizer. It would appear that, at least for certain groups, this one adverse effect alone undoes the claim that the ‘risks outweigh the benefits’. The risk of vaccine-induced myocarditis may indeed be very small, but the risk of serious Covid in the young and healthy is smaller still. If you’re a young male and if you’ve received one of these novel COVID-19 vaccines, it may be worthwhile testing for preclinical myocarditis.
Negative effectiveness
I couldn’t leave you hanging after dangling this juicy but horrifying morsel in front of you earlier. I managed to get another rapid response published, in the BMJ proper this time, on the topic of negative effectiveness. While rapid waning of effectiveness and exaggeration of effectiveness is concerning enough, particularly as we learn more about the adverse effects, the phenomenon of COVID-19 vaccine negative effectiveness could completely end the discussion as to whether the COVID-19 vaccines are net useful or not. There is increasing evidence for this phenomenon (in relation to infections, hospitalisations and deaths), with one study revealing a dose-dependent relationship. The more COVID-19 jabs, the more the risk of COVID-19. If that sounds concerning to you, well, quite. My rapid response effectively refuted an article in the BMJ trying – and failing horribly – to explain this phenomenon away. If negative effectiveness is occurring, there is no such thing as ‘risks vs benefits’. There is only ‘risks plus risks’. We need explanations from the manufacturers and regulators, as a matter of urgency.
Dr. Raphael Lataster is an Associate Lecturer at the University of Sydney, specialised in misinformation, and a former pharmacist. This summary is adapted from several entries originally appearing in Lataster’s Substack newsletter, Okay Then News. Read more on his research and legal actions, including his recent win against the healthcare vaccine mandate in New South Wales.
The Government’s Reassurances on 5G Safety Fail to Persuade

BY GILLIAN JAMIESON | THE DAILY SCEPTIC | SEPTEMBER 10, 2023
Wouldn’t you think that if the Government wanted to “make the U.K. a world-leader in 5G” that its ministers would know some basics about how the regulatory organisation they follow, the International Commission on Non-Ionising Radiation Protection (ICNIRP), arrived at its recommendations for safe exposure?
Recently I wrote to my MP, Rishi Sunak, to alert him to my situation in needing to avoid radio-frequency radiation (RFR) or electromagnetic fields (EMF), due to health damage I sustained 20 years ago when I lived 15 metres from a mobile phone mast. Before, dear reader, you tell me that my conclusion is pure speculation, let me tell you that this likely explanation only occurred to me after the death of a second neighbour from motor neurone disease and after months of my suffering with flu-like symptoms and heavily swollen neck glands, followed by health problems, with which I will not bore you.
Anyway, Mr. Sunak, very diligently, put my concerns to two ministerial colleagues, while telling me in the meantime that he proposed to blanket the U.K. with the fastest wireless coverage available. My reply to the latter remark was as follows:
1.The Government purportedly stands by the results of the Stewart Report 2000 and states here “adults should be able to make their own choices about reducing their exposure should they so wish, but be able to do this from an informed position”. How will this be possible if the country if blanketed? Smart devices, phone masts and WiFi are now everywhere where there are people. Will you inform people where coverage is lightest, if they wish to reduce exposure? Will you make sure that non-smart transactions are always possible? Will you ensure that some areas will always have landlines and are smart meter and smart camera free? And so on.
2. If the country is blanketed, what happens to the rights of those disabled by electromagnetic hypersensitivity (EHS) in terms of section 6 of the Equality Act? A case has already been won in the U.K., where a local authority has been mandated to provide RFR/EMF free education for a child with EHS.
Be that as it may, when the ministerial replies arrived, I was genuinely shocked by the level of ignorance they betrayed.
Steve Barclay, the Secretary of State for Health and Social Care wrote: “The ICNIRP guidelines apply to the whole population, including children and people of varying health status, which may include particularly susceptible groups or individuals.”
This is simply wrong. What ICNIRP actually says is:
Some exposure scenarios are defined as outside the scope of these guidelines. Medical procedures may utilise EMFs, and metallic implants may alter or perturb EMFs in the body, which in turn can affect the body both directly and indirectly… As medical procedures rely on medical expertise to weigh potential harm against intended benefits, ICNIRP considers such exposure managed by qualified medical practitioners, as beyond the scope of these guidelines. (emphasis mine)
In other words, these guidelines do not apply to anyone with a metal implant or anyone undergoing a medical procedure utilising EMFs. That is a large population group. It is left to doctors to advise on this, but, in fact, in the U.K. doctors are not trained in the health effects of non-ionising radiation. And the implication of this statement is that ICNIRP has no medical expertise. Indeed on examining the profiles of ICNIRP members, I have not found anyone with a medical qualification.
But even more alarming is this statement by Sir John Whittingdale OBE, the Minister for Data and Digital Infrastructure:
The ICNIRP… guidelines… are based upon a large amount of research carried out over many years.
This is nonsense, I am afraid. The guidelines are based on behavioural studies of eight rats and five monkeys, which were irradiated for up to an hour and also by measuring heating effects on a plastic model of a man’s head. Criticisms of the methodology used for deciding the guidelines have been made by the International Commission on the Biological Effects of Electromagnetic Fields (ICBE-EMF) in a recent article and by James Lin, a highly qualified ex-member of ICNIRP, who laid out his objections in the IEEE Microwave magazine.
In actual fact, far from being the basis of the guidelines, the opposite is true. Studies on the biological health effects of EMFs are largely dismissed by ICNIRP with the comment “more research needs to be done”.
Sir John went on to state:
Reviews carried out by the independent Advisory Group on Non-Ionising Radiation (AGNIR) found no convincing evidence that radiofrequency field exposures below guideline levels cause health effects.
He did not mention that this review was carried out back in 2012 and was discredited by Dr. Sarah Starkey who found that the report omitted and distorted scientific evidence leading to wrong and misleading conclusions. She also pointed out how many personnel had dual roles and conflicts of interests by being in more than one of these regulatory bodies at the same time.
And indeed, since that time, there have been two very large animal studies (the NTP study and the Ramazzini study) showing a link between RFR and cancer as well as a large epidemiological review In 2019 by an international expert team led by Canada’s most senior cancer epidemiologist Professor Tony Miller, reporting human epidemiological evidence linking human breast and brain tumours, male reproductive outcomes and child neurodevelopmental conditions to RFR exposures. It also found compelling evidence of carcinogenesis, especially in the brain and acoustic nerve, as well as the breast, from strong RFR exposures to previous generations of mobile phone transmissions.
AGNIR was disbanded in 2017 and its remit adopted by the Committee on Medical Aspects of Radiation in the Environment (COMARE). Unfortunately COMARE has never produced a report on the health effects of non-ionising (radio-frequency) radiation, because our Government has never asked it to do so, according to an email sent to me by its secretariat.
What a contrast to the U.S. New Hampshire Commission, which gathered a large group of experts together and conducted a thorough investigation into the health effects of RFR a couple of years ago.
In June this year, at a conference at the Royal Society of Medicine in London, its findings were described with great clarity by Professor Kent Chamberlain, the Professor Emeritus of the Department of Electrical and Computer Engineering at the University of New Hampshire. His talk included a discussion of the methods used to set the ICNIRP safety exposure guidelines, a review of the peer-reviewed literature on adverse health effects of RFR and the highlighting of key findings, such as the increased risk of cancer if you live within 1,000 metres of a mast.
The Royal Society of Medicine conference was organised by the International Commission on the Biological Effects of Electromagnetic Fields (ICBE-EMF) and was based around an important paper, examining the 14 false assumptions of those creating the ICNIRP safety guidelines. I introduced the expert speakers in a previous DS article and they include Dr. Erica Mallery-Blythe, Professor Kent Chamberlain, Professor James Lin and Professor John Frank in an event ably introduced by David Gee, who co-authored Late Lessons, Early Warnings for the European Environmental Agency.
Short written highlights, presentation slides and videos of the event are now available to view on an ICBE-EMF webpage and I’d say that these are essential viewing and reading for anyone interested in this subject and particularly for our Government ministers and their researchers.
Just when will our Government do its due diligence? And how certain do we need to be about causation before exercising caution and catering for those who already know they are affected by RFR exposure?
Autopsy Confirms Infant Died From Over-Vaccination
Maine Mom, RN, Paid Ultimate Price Trusting Her Doctors
By Jennifer Margulis | Vibrant Life | September 9, 2023
A toxicology report shows that a new mom in Maine was right. Her baby, Sawyer, died when he was just eight weeks and six days old, just 34 hours after being vaccinated.
On October 20, 2022, Melissa, who herself is a registered nurse, took her baby to the pediatrician. Baby Sawyer had a rash around his torso that just wouldn’t go away. The pediatrician diagnosed him with a viral infection, which was causing the rash.
The doctor gave her Eucerin cream and told her to monitor her son’s temperature for a possible fever.
Seven days later, on October 27, 2022, Melissa went to the same pediatrician for her son’s well-child check-up. At that two-month check-up, Melissa asked the doctor if they should wait on the two-month vaccinations because her baby was still sick.
The doctor said no.
Although Baby Sawyer still had a rash, he didn’t have a fever. And Since Baby Sawyer didn’t have a fever during the appointment, the doctor insisted it would be perfectly safe for the baby to get all his recommended vaccines.
Even though her intuition, as both a nurse and a mom, was that they should wait until the baby was feeling better, Melissa trusted her doctor.
That turned out to be the biggest mistake of her life.
At that visit, the baby was given:
Rotateq
Prevnar 13
Pediarix (a combination vaccine that contains DTaP, IPV, and hepatitis B)
It’s worth noting that a new version of Pediarix was approved by the FDA in 2019, making this formulation one of the newer vaccinations on the market.
By the time Melissa got home that day, Baby Sawyer was screaming like he had never screamed before.
More experienced moms, moms whose babies have suffered brain damage, would recognize that heartbreaking sound as the “DTP scream”—a high-pitched uncontrollable almost inhuman expression of agony.
Melissa’s pediatrician had told her during the appointment to give the baby acetaminophen to help make him more comfortable. Even though Baby Sawyer didn’t have a fever, Melissa gave him a partial dose of baby Tylenol for discomfort.
The next morning, on October 28, 2022, the baby was still acting fussy and uncomfortable.
Melissa gave him more Tylenol, held him, and rocked him. He drank five ounces of expressed breastmilk from a bottle.
When her husband got home from work, they put the baby down in his bassinette for a nap. This was around 5:30 p.m. Her husband then ran out to get some food for dinner.
Melissa, who worked remotely, heard the baby fussing around 6:15 p.m. Her husband went in to check on him. He readjusted him, and rubbed his back as Fathers do. Baby Sawyer fell back to sleep.
Sawyer was asleep off and on for about four hours, during which time she and her husband both checked on him. They also had a baby monitor and it was easy to hear the baby anyway because their home is small.
But the last time Melissa went to check on Baby Sawyer, the baby wasn’t moving or breathing. She picked him up out of the bassinette and the baby was completely limp and lifeless. Melissa started screaming. Her husband, who was the last one to see him alive, rushed in to help his wife.
They immediately called 911.
When the emergency medical technicians arrived, they did everything they could to revive the baby. But they were unable to save him.
Baby Sawyer was pronounced dead at 10:51 that night.
His tiny body was put in a body bag and taken away by the Brookings-Smith Funeral Home.
The Penobscot County Sheriff’s office and the state police had also responded to investigate. Because it was an infant death, the state of Maine opened a formal investigation and ordered an autopsy.
The autopsy was performed the next day, on October 29, 2022.
The Chief Medical Examiner, Dr. Mark Flomenbaum, determined that the cause of death was “asphyxiation due to inappropriate sleep position and environment.”
His report essentially blamed the parents, citing a “sub-optimal sleeping environment,” for purportedly causing their infant’s death.
At this point, law enforcement began questioning Melissa and her husband as if they were murder suspects.
One asked Melissa if she thought her husband could have hurt the baby, implying that her husband might have suffocated their son on purpose.
She was also asked her if her husband had been drinking and whether he had a problem with alcohol.
However, the investigators found no evidence of foul play.
According to the pathology report, the child was “well developed” and had no signs of injury or bruising on his body.
Baby Sawyer’s death was ruled an accident and the case was closed.
Melissa, who was devastated, mentioned to anyone who would listen that her son had just been vaccinated.
Though she did not know why her son had died, she did not understand how the timing could be coincidental.
Her intuition would not allow her to ignore the fact that her healthy baby had a viral infection, got four vaccines against eight illnesses, and died the next day.
How could that possibly be a coincidence?
Researching on-line, Melissa found a pathology protocol, a list of recommended tests for infants when over-vaccination is a suspected culprit.
She emailed the state medical examiner, Dr. Mark Flomenbaum. She formally requested that the tests on the protocol list she’d found be performed to explore if vaccinations may have played a role in her son’s death.
Here’s the email Melissa sent to the Medical Examiner. I have reprinted it in its entirety:
“I am writing to you to formally request the following additional pathology assays, analyses and tests be performed on my son Sawyer DOB 8/27/22 post-mortem blood and tissue samples and to preserve the samples and data they reveal for my legal counsel to review.
Infant Vaccines Autopsy Tests
· CRP (C-reactive protein: if inflammation is high, that would indicate vaccines were to blame as a small infant or toddler could not generate such results) This would indicate severe brain inflammation.
· Test for liver enzymes
· Test for heavy metals, especially Hg and Al in blood and brain tissue
· Test for formaldehyde and Formalin–in particular, which would come from vaccines. Even though the body manufactures a little formaldehyde, large amounts would implicate formaldehyde, or Formalin, especially in vaccines.
· Test brain tissue for Hg and Al, which would indicate those metals crossed the blood brain barrier and may have been the precipitating factor in the child’s demise, as they are potent neurotoxins and can cause encephalopathy.
Cytokine panel:
1. Interleukin-1 beta (IL-1β) — IL-1beta is one of the key mediators of the inflammatory response to physical stress.
2. Interleukin-6 (IL-6)
3. Interleukin-8 (IL-8)
4. Tumor necrosis factor alpha (TNF-α) TNF-α is a growth factor for immune cells and osteoclasts, the cells that break down bone.
5. Fibrinogen
6. Vitamin C assay
7. Titer levels on all the vaccines. If they are sky high, that could make a case for molecular mimicry causing death.
Sincerely,
Parents of deceased infant Sawyer”
Flomenbaum’s office, which has come under scrutiny several times in the past, refused to perform any of the tests Melissa requested.
Sandra Slemmer, Medicolegal death investigator for the State of Maine, explained to Melissa via email that:
“Dr. Flomenbaum and I reviewed your correspondence to Office of Chief Medical Examiner (OCME). I will do my best to address all of your requests and concerns. If you have more questions, please feel free to contact me.”
Slemmer’s email, in a screenshot below, asserts that heavy metals do not cause SIDS, so additional testing was not necessary.
However, Slemmer’s office did not list the cause of Baby Sawyer’s death as SIDS.
But their emailed response further claims that if there were heavy metals in his system, the amounts would be “so small” that these metals would not be a contributing factor in his demise.
The email also claims that the description of the baby’s sleeping environment was “compelling,” and therefore they saw no reason to perform any additional tests.
The entire email suggests that before they even did any testing on Baby Sawyer’s body, the Medical Examiner’s office had already determined the cause of his death.

Since she was unable to get the Medical Examiner to do any further investigation of her baby’s death, Melissa reached out to Health Choice Maine.
Health Choice Maine is a statewide non-profit that works to protect families and restore medical freedom in Maine. I spoke at their conference, Find Your Light, a year ago.
Tiffany Kreck, Health Choice Maine’s Executive Director, met with Melissa and helped her to build a timeline of evidence and documentation. They decided they needed to find a new pathologist, someone willing to order additional testing.
Health Choice Maine started an exhaustive search to find a competent pathologist.
“We searched the entire country,” Kreck told me when I spoke to her by phone. “We came up empty handed. No medical professional wants to touch this issue. They are terrified of losing their career and their ability to support their families.
”It took four months,” she continued, “utilizing every network we had. We finally found one person who, seeing the grief of the mother, agreed to order the tests.”
Working with the fluid and tissue samples collected by the state medical examiner, this pathologist did as many of the suggested tests as he could.
The results of this report were shared with the family and with Health Choice Maine on August 3, 2023.
In the meantime, trying to deal with the unfathomable grief of losing her only child, Melissa went to a psychiatrist in March of 2023, five months after her son died.
Instead of sympathy, however, Melissa was met with a cold diagnosis.
She was told she was having an “adjustment disorder.”
The therapist recommended mood stabilizers and anti-depressants. Melissa left the therapist’s office crying. She felt like she was going crazy. Was she a bad mom? Had she done something wrong? Was there something wrong with her because she couldn’t let it go and was still grieving?
The aluminum concentration in the baby’s blood was at adult toxicity levels.
Baby Sawyer had 95 micrograms per liter, which far, far exceeds safety amounts.
Several of the vaccines Baby Sawyer received, including Hib and Pediarix, contained high amounts of aluminum.
So the medical examiner’s office was wrong in assuming (without ever testing it) that heavy metals did not contribute or even cause the death.
“This additional pathology report shows how much our medical examiners don’t know because they won’t look. How many other parents have been blamed for their infants’ death that were innocent?” Kreck said.
“These tests must be standard in all unexplained infant death.”
Health Choice Maine is working with attorneys to find out how to challenge the cause of death listed on Baby Sawyer’s death certificate and file a Vaccine Injury Compensation Program (VICP) claim.
“Follow your instincts, even when everyone’s telling you you’re wrong,” Kreck says.
“Vaccines are implicated far more often in infant deaths than parents realize.”
About the Author
Jennifer Margulis, Ph.D., is an award-winning investigative journalist and book author.
The Childhood Vaccination Schedule – Part One: The First Vaccine – Hepatitis B
By Michael Bryant | 21st Century Wire | September 5, 2023
Introduction
As more vaccines are added to the US childhood immunization schedule it’s imperative that there be a broader public discussion about the prominence of vaccines in public health policy, what benefits they convey and a forthright assessment of the risks involved.
Though vital to both the short and long term health of children, exploratory questions, in-depth rational discussion and comprehensive analysis about vaccines are considered off-limits for the mainstream medical establishment.
In the conventional narrative it is accepted as an article of faith that vaccines are miraculous discoveries responsible for global disease eradication and are the most important medical product for disease prevention.
For today’s pediatricians promoting and implementing the childhood immunization program has become their primary duty.
It is widely believed that if we stopped, or even reduced vaccinations, we would be going back to the dark ages. Any individual that challenges this vaccine orthodoxy is seen as a heretic.
Despite the deeply ingrained belief system of the vaccine ideology a growing number of parents and health advocates are beginning to ask many of the questions which have been swept under the rug for years.
Are all of these vaccines necessary? Are they safe? Are the diseases they are supposed to prevent truly diseases of concern?
Does the claim that vaccines are responsible for reductions in disease, disability, and death from a variety of infectious diseases fit with the facts when scrutinized?
Why such an increase in the number of vaccinations through the years? Has this escalating vaccine program produced an accompanying improvement in health outcomes?
What happens if I don’t give my child all of these vaccines? What happens if I don’t give my child any of these vaccines? What happens to children who don’t get vaccinated?
These are some of the questions parents are not supposed to ask and precisely the questions that need to be addressed.
While the information presented in this series is publicly available it is denied admittance into the public discourse by means of systematic indoctrination by a compromised media apparatus and a medical establishment which has created a mystique around vaccines while persuading the public they are the holiest of all medicinal products.
As an antidote to this institutional programming we embark upon a series of articles which take a close look at each of the vaccines on the childhood schedule and the diseases they are designed to prevent.
Our series begins with an overview of the US Childhood Immunization Schedule and a detailed look at the initial shot given to infants on the first day of life- the Hepatitis B vaccine.
The United States Childhood Immunization Schedule – An Overview
In the past few decades the childhood vaccine schedule in the United States has exploded into what is now the most aggressive childhood vaccination schedule in the world. It wasn’t always this way. Most baby boomers likely had only 2 or 3 vaccinations- polio, smallpox and DTP with never more than one shot given per visit.
With the recent addition of the COVID-19 vaccines to the childhood schedule the number of recommended injections ballooned to a regimen of 72 injections of 90 antigens by age eighteen for any child that undergoes the full immunization schedule circa 2023.
To understand how this came to pass we need to understand the history of how we got here.
The first vaccine mandate in the United States was enacted in Massachusetts in 1810 and was centered on smallpox. The legislation was essentially an ad hoc law which gave local health boards the authority to require vaccination.
The first public school mandate was issued in Massachusett in the 1850’s. At that time the only vaccine of interest was for smallpox. By the end of the 1800s most states in New England had smallpox vaccine requirements for children attending public schools.
The next significant stride in vaccine recommendations and requirements for children would arrive a century later in 1954, focusing on the polio vaccine developed by Jonas Salk.
By 1955, the polio vaccine was fully licensed and through the Polio Vaccine Assistance Act Congress appropriated funds to provide federal grants for states to purchase the vaccine and for the costs of planning and conducting vaccination programs.
This Act would become the template for the utilization of federal funds to cover various costs of vaccine programs and would provide the impetus for a mass inoculation campaign for polio.
At this time there were no codified mechanisms to mandate vaccine uptake, doctors recommendations were considered just that- guidance with no strict obligation or enforcement for adherence.
In 1962 the Vaccine Assistance Act would establish a permanent mechanism to provide ongoing financial support to state and local health departments. This Act would allow the CDC to appropriate federal funds for the provision of vaccines and establish an advisory group to assist in managing vaccination programs.
To this day the 1962 Act remains one of the most important mechanisms for aligning local and state health department immunization activities with federal funds to deliver vaccines to children.
In 1964 the Advisory Committee on Immunization Practices (ACIP) was created under the US Public Health Service. Its mission was to review the science and evidence of vaccines given to children and to make recommendations on when those vaccines should be given and at what age.
The 1960s and 1970s saw a wave of new vaccines hit the market. A second type of polio vaccine was developed along with the first Hepatitis B vaccine. Measles vaccines were developed as a single vaccine and then combined with the mumps and rubella vaccines to create the “MMR” vaccine.
Paralleling the increase in the volume of vaccines came the creation of global immunization programs. In 1974 the World Health Organization established the Expanded Programme on Immunization which was designed to ”strengthen vaccine programmes, supply, and delivery, and ensure universal access to all relevant vaccines for all populations across the life course.”
These changes radically altered the business landscape of vaccine manufacturing. What was once a cottage industry of small pharmaceutical companies, individual investigators and physician scientists evolved into the mega corporations that exist today.
By 1977, the U.S. federal government had set up the Childhood Immunization Initiative which sought to increase vaccination rates in children against seven diseases (diphtheria, measles, mumps, pertussis, poliomyelitis, rubella, tetanus) for which vaccines had been developed. This began the process by which all 50 states would adopt mandatory school vaccinations.
In the 1980s, vaccines against Hepatitis B, Haemophilus influenzae type b, and pneumococcal disease were recommended for children at different ages. By 1983 the number of recommended injections had increased to 23 doses of 7 vaccines by age six.
In 1986, the National Childhood Vaccine Injury Act created a system of passive and active surveillance for cases of adverse reactions to vaccines as well as a mechanism to compensate any persons injured by vaccines.
With the passage of the 1986 Act and its implementation in 1988, a liability shield for pharmaceutical companies was created. On the heels of the 1986 Act the number of vaccines placed on the CDC schedule would escalate.
Even as the list of available vaccines was growing local and state health boards had differing opinions on when to give vaccines, which children should get them and how many should be given.
In order to standardize vaccine uptake, the first “harmonized” childhood immunization schedule was issued in 1995 by the Advisory Committee on Immunization Practices (ACIP), the American Academy of Pediatrics (AAP), and the American Academy of Family Physicians (AAFP). combining recommendations of all three national groups.
This initial schedule included diphtheria, tetanus, pertussis, measles, mumps, rubella, polio (oral), Haemophilus influenzae type b, and Hepatitis B vaccines. (The DTP and MMR vaccines were combination vaccines for diphtheria, tetanus, pertussis; and measles, mumps, rubella.)
Since then, the schedule has been adjusted as new vaccines have been developed, taken off the market or the risk profile for children changed.
Today, according to the National Conference of State Legislatures (NCSL), all 50 states have legislation requiring specific vaccines for students with exemptions varying from state to state.
These laws apply not only to children attending public schools but also to those attending private schools and day care facilities.
There are 45 states and Washington D.C. that grant religious exemptions for people who have religious objections to immunizations and 15 states which allow for philosophical exemptions.
All school immunization laws grant exemptions for medical reasons.
Six states (California, Connecticut, Maine, Mississippi, New York, and West Virginia) do not allow religious or philosophical exemptions from vaccination requirements as of 2021.
NCSL also states that the laws and regulations on vaccine requirements in all 50 states and DC follow the vaccine schedule set forth by CDC.
The trajectory of this vaccine program would result in 54 injections of 72 antigens by 2019 for US children by age eighteen who adhered to the full CDC schedule- with even more shots added as the Covid vaccines were placed on the child immunization schedule.
This dizzying array of injections in the childhood immunization schedule begins on a child’s first day of life with the Hepatitis B vaccine.
Hepatitis B – The Disease: A Case Study In Manufacturing Public Perception
The first question every parent should ask when considering the Hepatitis B vaccine is, “Does my child need a vaccine for Hepatitis B on the first day of life?”
Given the low risk of newborns acquiring the HepB infection and the ease with which pregnant mothers can be screened it’s fair to ask why a newborn would need the HepB vaccine?
Before arriving at that answer we look back at how Hepatitis B, the disease, was transformed from a relatively obscure disease which impacted a limited population into a widespread public health predicament.
The conventional characterization of Hepatitis B is as a type of viral hepatitis which causes acute and chronic liver infection. It is generally accepted that in order to contract HepB direct contact with infected blood or other body fluids is required. Transmission routes that by any standards pose little or no risk to infants.
This is in fact how public health officials characterized the disease back in 1981 when the Hepatitis B vaccine initially gained approval. The CDC’s own Fact Sheet on HepB the disease does not include newborn babies as a risk group for that disease.
The risk groups listed are, “injection drug users, homosexual men, sexually active heterosexuals, infant/children of immigrants from disease-endemic areas, sexual/household contacts of infected persons, infants born to infected mothers, health care workers and hemodialysis patients.”
What was it that changed the CDC’s earlier 1982 recommendation, which targeted only a small “at-risk” population, into a set of more aggressive policies that would result in the 1991 recommendation that all infants get three doses of HBV by 18 months of age?
And how did the HepB vaccine become compulsory for all schoolchildren in 47 states by the year 2000 even as the CDC admits that they lack proof of HepB being transmitted in a school setting?
In large part the answer to these questions lies in how the public’s perception of HepB was radically altered through orchestrated media messaging and deliberately provocative depictions of the disease by industry and public health officials. Notably the change in HepB’s image came immediately following the vaccine’s development, licensure and introduction.
In the late 1970s and early 1980s, prior to the approval of the vaccine, HepB was a disease which had little to no relevance to most Americans and nowhere to be found on the media radar. Before the Hepatitis B vaccine was developed and marketed most Americans had little reason to view the disease as a threat to their health.
New cases of HepB were quite low in the 1970’s, began to rise in the 1980’s, concurrent with the AIDS crisis, and then began to fall again in the 1990’s.
By its own admission the CDC attributed this decline to, “reduction of transmission among men who have sex with men and injection-drug users, as a result of HIV prevention efforts.”
As scientific discoveries leading to the vaccine moved forward HepB acquired a more public image.
The advent of the AIDS crisis in the early 1980s, the development of genetically-engineered pharmaceuticals in the late 1980s, and the political push for health reform in the early 1990s all led to changes in how HepB was presented to Americans.
The media, medical and scientific community would all contribute in altering the image of HepB through the 1980s and 1990s. Media outlets would often conflate HepB with HIV/AIDS in order to arouse public attention and induce fear towards this obscure disease.
Provocative headlines and stories began to surface with claims that Hepatitis B was similar to HIV and possibly worse.
The historical medical view that HepB was a disease which only impacted a narrow subset of the population was replaced by hysterical media representations that anyone could be at risk of Hepatitis B.
In her article, “Do We Really Need Hepatitis B on the Second Day of Life?”, Vaccination Mandates and Shifting Representations of Hepatitis B, history of health sciences professor Elena Conis chronicles some of this history:
“Outlets from the Philadelphia Tribune to Good Housekeeping reported that a third of people with the disease were not in any of the known risk groups. Redbook warned readers that hepatitis was “spreading fast,” and the Boston Globe noted that hepatitis was spread by sharing gum, food, toothbrushes, and razors and by body piercing. New York magazine, in a feature titled, “The Other Plague,” recounted the stories of a young woman who contracted a fatal case by getting her ears pierced, a young man who was infected when mugged at knife-point, and a woman infected at a nail salon. Frequent mention of the prevalence of asymptomatic carriers heightened the sense of an immediate health threat: in the words of the New York magazine reporter, anyone could be one of the U.S.’s 1.5 million “Typhoid Marys,” unwittingly transmitting hepatitis B to people unaware of their risk.”
Such media reports citing HepB disease statistics would normally originate with statements generated by officials at the CDC.
Most of the inflated disease statistics found in the media reports were generated in the very same ACIP Morbidity and Mortality Weekly Report (MMWR) which called for mass vaccination with hepatitis B vaccine.
In that report the CDC stated that there are an “estimated 1 million-1.25 million persons with chronic hepatitis B infection in the United States” and that, “each year approximately 4,000-5,000 of these persons die from chronic liver disease” and that, “an estimated 200,000-300,000 new [Hepatitis B] infections occurred annually during the period 1980-1991.”
To generate those statistics the CDC, in what at best would be considered duplicitous, circled back to itself citing an MMWR 1990 report as the basis for their claims. Nowhere in either report were scientific references used to support those claims.
Despite the media campaign, vaccine uptake for HepB was not rising to desired levels as vaccinating high-risk adults was proving to be difficult. This would result in a more systematic strategy at the national level.
In September of 1991 the Immunization Practices Advisory Committee (ACIP) would develop and codify a national program for the HepB vaccine- Hepatitis B Virus: A Comprehensive Strategy for Eliminating Transmission in the United States Through Universal Childhood Vaccination.
In 1992 the World Health Organization (WHO) would follow suit recommending that “all infants should receive their first dose of hepatitis B vaccine as soon as possible after birth, preferably within 24 hours, even in countries where Hepatitis B virus is of low endemicity.”
Acknowledging children were not in the at-risk group for HepB the ACIP committee lamented that “HBV transmission cannot be prevented through vaccinating only the groups at high risk of infection.”
Using this rationale they declared a blanket vaccination policy for all newborns- “a comprehensive strategy to prevent HBV infection, acute hepatitis B, and the sequelae of HBV infection in the United States.”
Earlier that year, June 11,1991 in a Boston Globe article titled, “U.S. To Urge All Children Be Vaccinated for Hepatitis B,” an official from the CDC admitted, “We do not feel that targeting adults for vaccination has worked. This will be the first time that a vaccine is recommended for children to prevent a disease that primarily occurs in adults.”
In testimony before Congress Michael Belkin summed it up neatly, “So in the CDC and ACIP’s own words, almost every newborn US baby is now greeted on its entry into the world by a vaccine injection against a sexually transmitted disease for which the baby is not at risk -because they couldn’t get the junkies, prostitutes, homosexuals and promiscuous heterosexuals to take the vaccine.”
Not to be swayed by logic, the CDC would effectuate a comprehensive HepB vaccine program and a medical product with an initial target population of drug addicts and homosexuals would become compulsory for every child in the country.
The Hepatitis B Vaccine Clinical Trials- The Devil’s In the Details
It is a near certainty that few physicians will study the details of a vaccine clinical trial found in the package inserts of each vaccine. Rarely will a pediatrician or physician initiate a conversation with a patient or parent about what those trials entailed and what else the package insert reveals.
Yet that is exactly the first place one should go to get a clear picture of the safety profile for any vaccine.
In 2017 the Informed Consent Action Network (ICAN) received a tip from a supporter that the clinical trials used by the FDA to license the two children’s HepB vaccines, Engerix-B and Recombivax HB, only reviewed safety data for a few days after injection.
ICAN was so stunned by this revelation that they assumed the supporter was making false claims. Upon reviewing the package inserts for both vaccines ICAN found the claims to be true.
The package insert for GlaxoSmithKline’s Energix-B vaccine, approved in 1989, acknowledges that the subjects were monitored for only 4 days after administration of the vaccine. By any standards 4 days of post-injection data is inadequate to assure a product’s safety. As noted by ICAN, “the review period for a vaccine given to infants and young children should be longer as neurological and developmental disorders are often discovered until the child is a few years old.”
A 2019 study authored by researchers at the FDA and Duke University confirmed ICAN’s position, stating that compared to licensing time period for adults, “data on drug efficacy and safety in children may require an additional 6 years.”
Another troubling facet of GSK’s pre-licensure clinical trials is that ENGERIX-B was administered to 5,071 healthy adults and children. Of the 13,495 doses administered in 36 clinical trials nowhere is it listed how many of those subjects were adults, how many were children and how many were infants.
As there were no specifics on how many individuals from each age group were involved the results of these trials are uninterpretable with respect to the risks of vaccinating infants.
While the trials for Energix-B were certainly less than rigorous the pre-licensure trials for Merck’s Recombivax HB vaccine might hold the dubious distinction for being the most unscrupulous and underpowered trials in the annals of the Pharmaceutical Industry.
In only three clinical studies, 434 doses of RECOMBIVAX HB, 5 mcg, were administered to a whopping 147 healthy infants and children (up to 10 years of age) who were monitored for a mere 5 days after each dose.
Along with the fact that 147 subjects is a grossly insufficient number upon which to base any determination on vaccine safety, the ages of the trial participants are not even listed. How many infants were in the study? Was there even a single newborn in the study?
Additionally, as is the case with virtually all vaccine clinical trials, neither of these two HepB trials used a proper randomized placebo-controlled clinical trial.
Beyond the untrustworthy nature of the composition and execution of these trials there is also the nagging problem with the difference between the noted outcomes of the clinical trials versus the post marketing experience.
In the clinical trials, effects are only studied for a few days immediately following vaccination, (with no true placebo), and only minor adverse reactions such as irritability, fever, diarrhea, fatigue/weakness and injection site pain are mentioned.
But in the “post marketing data”, which means post-approval injections in the general population, a laundry list of more serious adverse reactions such as Guillain-Barré syndrome, multiple sclerosis, encephalitis, thrombocytopenia, meningitis, Stevens-Johnson syndrome, tachycardia and many more are reported.
This is one of the elemental tricks the Pharmaceutical Industry uses to conceal the nature and extent of injuries which may be attributable to the shots.
More serious adverse reactions are swept under the rug by asserting that “no causal link has been established” between the injection and these reactions.
In the trials subjects are observed for only a few days and nothing is found to cause concern.
But when the general public starts reporting real world serious adverse events, these are dismissed as no long term studies are done which could establish causal relations.
ICAN’s lawyer Aaron Siri in a 9 hour deposition brought these many problems to the attention of Stanley Plotkin, the ‘Godfather of Vaccines’, who authored what is considered the bible on vaccines,
In the deposition Siri gets Plotkin to admit that the Hepatitis B vaccine (given to babies on their first day of life), has not had an adequate safety study:
Siri asked, “How long does it say that safety was monitored after each dose?”
Dr. Plotkin responded, “Five days.”
Siri responded, “Is that long enough to detect an autoimmune issue that arises after five days?”
Dr. Plotkin stated, “No.”
Siri then asked, “Was there any control group in this trial?”
Dr. Plotkin, who had just argued how important control groups are to cause and effect, answered, “It does not mention any control group, no.”
Based on the weight of the evidence ICAN is currently petitioning the FDA to withdraw the licensure of these Hepatitis B vaccines and asserts that these vaccines should never have been approved.
Given that the utility of the Hep B vaccine for toddlers is unsubstantiated and the clinical trials are at best problematic it would seem incumbent upon the manufacturers to at least provide ironclad evidence for the safety of these products.
Is this the case?
The data tell a different story.
Dangers of the HepB Vaccine- An Open Secret
In the first months of life a child’s brain and biological systems are at critical stages of development. Throughout pregnancy parents are bombarded with directives from their physician telling them a multitude of vaccinations will be essential to protect their child from the pending torrent of infectious diseases.
In addition to the medical stipulations given by their pediatrician, parents understand that they will be faced with mandates for day care and schooling as well as ever-present societal pressures. The combination of these forces create a climate of fear and coercion intended to bring about automatic compliance.
Little to no information about vaccines are volunteered at most pediatric visits. Parents are expected to obediently trust their physician and place their faith in a medical system that assiduously claims vaccinations are necessary, safe and effective. Questions challenging the utility and safety of a vaccine are typically discouraged and dismissed.
In the United States the journey into this world of mass vaccination begins on the day of birth with the Hepatitis B vaccine.
To the extent that Hepatitis B is a danger to anyone, that risk is understood to be through sexual contact or sharing needles. A sexually transmitted risk or a needle exchange risk means there is little to no chance of Hepatitis B infection for infants calling into question the fundamental rationale for this vaccine.
Less than one percent of all HepB cases occur in children under 15 years old. In North America, Europe and Australia a mere one-tenth of one percent are said to be carriers of HepB. Of adults infected, 90-95% clear the virus on their own, without intervention.
While it is thought that infants born to mothers who are infected with HepB carry a greater risk of contracting the disease, pregnant women can easily be screened for this disease if there is a concern.
Given this risk profile, as infants and young children receiving this vaccine face little to no chance of hepatitis B infection, we have to ask, Is this vaccine worth the potential risk of neurodevelopmental disorders or other adverse impacts associated with this vaccine?
The answer to those questions can be found in answering the most important question for any medical product, “Is it safe?”
From the earliest days of development and production safety concerns have dogged the various iterations of the Hepatitis B vaccine.
The original HepB vaccine, Heptavax B, manufactured by Merck Sharp & Dolme and approved by the FDA in 1981, was unlike previous vaccines in that it contained inactivated virus collected from plasma of HepB-infected donors rather than live, weakened virus or killed, denatured virus.
Maurice Hilleman hypothesized that he could make a HepB vaccine by injecting patients with Hepatitis B surface protein using three treatments of blood serum together with rigorous filtration. To obtain the necessary plasma Hilleman collected blood from gay men and intravenous drug users—groups said to be at risk for viral hepatitis.
Hilleman believed the immune system would recognize the surface proteins as foreign, and manufacture specific antibodies which would destroy these proteins. His theory went that if the patient were infected with HepB in the future the immune system would produce protective antibodies which would destroy the viruses.
On November 16, 1981, CBS Evening News reporter Dan Rather touted Hilleman’s vaccine as the “first completely new viral vaccine in 10 years,” and hailed it as, “the first vaccine ever licensed in the United States that is made directly from human blood.”
Though lauded as a revolutionary medical achievement at the time, the original plasma derived HepB vaccine was not intended for widespread use in the US due to the fact that liver cancer was relatively uncommon in the US at the time and the cost of the vaccine was seen as prohibitive.
Excitement surrounding this novel plasma vaccine soon dissipated due to a public relations problem. It came to light that the clinical trials which tested the vaccine in the 1970s had included only gay men who had been identified as being at high risk of the infection.
The approval of the serum derived vaccine had the added misfortune of coinciding with the AIDS crisis which heightened concerns over the safety of using potentially contaminated human serum in vaccines due to fears of transmission of live HepB or other blood-borne pathogens.
As gay men and injection drug users were frequent blood donors for the vaccine this brought about fears that blood plasma could be infected and the vaccine itself could become a carrier for HIV/AIDS.
These concerns of potential contamination with human viruses led to the 1986 introduction of a second hepatitis B vaccine, Recombivax-HB. This new type of vaccine, known as a recombinant vaccine, manufactured by Merck Sharp & Dolme, was the first vaccine produced using recombinant DNA technology.
The creation of this new type of vaccine entailed inserting the gene of the HepB virus protein envelope into yeast cells, eliminating the risk of viral contamination from using human serum to produce the vaccine.
Frank E. Young, FDA Commissioner at the time, heralded this development as yet another medical marvel declaring, “This vaccine opens up a whole new era of vaccine production. These techniques should be able to be extended to any virus or parasite to produce other vaccines that normally cannot be propagated in the laboratory.”
Noting that the plasma-derived vaccine had annual sales of only $45 million, Edward E. Penhoet, president of Merck’s collaborator Chiron Corp., suggested that the new recombinant HepB vaccine would be more profitable for Merck as genetically engineered vaccines are “cheaper to produce” than those derived from human blood.
By 1989, a second recombinant hepatitis B vaccine, Engerix-B manufactured by The SmithKline Beecham Company, was approved for use in the U.S.
While the new HepB vaccines tempered anxieties surrounding the previous plasma-based vaccines a different set of problems materialized in the manufacturing processes and with certain ingredients in the HepB recombinant vaccines.
A 2005 French study, Multiple sclerosis and hepatitis B vaccination: Adding the credibility of molecular biology to an unusual level of clinical and epidemiological evidence, highlighted issues with HepB virus polymerase contamination asserting, “We reviewed evidence showing that hepatitis B vaccine HBV has a marked potential to induce auto-immune hazards, neurological as well as non-neurological. We emphasized that for a drug used as a prevention, HBV was remarkable by the unusual frequency, severity and variety of its hazards.”
The authors came to the stark conclusion that, ‘‘the principle of precaution’’ should urgently be applied [with] regard to the tiny benefit (if any) of large HepB vaccination in low-endemic countries. In addition, the benefit/ratio of this costly prophylaxis should be seriously re-assessed even in countries where the frequency of HepB is higher.”
Soon issues surrounding genetically modified yeast proteins used in the HepB vaccines cropped up.
Links to yeast-containing vaccinese and autoimmune disease were observed, creating concerns that the genetically engineered yeast in the HepB vaccines may cause children with an allergy to yeast to react severely to the vaccine.
Bioinformatics and epidemiological evidence link the yeast protein found in the Hepatitis B vaccines to numerous autoimmune disorders. Part of the study’s stark conclusion was, “Vaccine makers have refused to perform such checks, resulting in devastating consequences.”
The Hepatitis B Foundation warned, “The vaccine may not be recommended for those with documented yeast allergies or a history of an adverse reaction to the vaccine.”
The CDC’s Pinkbook on Hepatitis B identified another potential problem with latex packaging in the vaccines observing, “Some presentations of HepB vaccines contain latex, which may cause allergic reactions.”
As the first dose of the HepB vaccine is recommended and usually given on the day of birth this presents a conspicuous problem. How is it possible to know if a newborn has an allergy to yeast or latex or any of the other vaccine ingredients?
While certainly not insignificant, even more alarming safety concerns than yeast and latex allergies have been identified with certain ingredients found in the HepB vaccine.
Until the early 2000s the original gene based HepB vaccines, Recombivax and Engerix, contained the mercury preservative thimerosal, a mercury- and thiosalicylate-containing organic compound with antiseptic, bactericidal, and fungicidal properties. Certain exposures to thimerosal are known to be toxic to the central nervous system, kidneys, liver, spleen, and bone marrow. Some believe that even the tiniest amounts of methylmercury, found in thimerosal, carry a risk of adverse neuropsychological outcomes.
A 2016 longitudinal study of the relationship between Thimerosal-containing hepatitis B vaccination and developmental delays made an assessment that, “During the decade in which Thimerosal-HepB Vaccines (T-HBVs) were routinely recommended and administered to US infants (1991–2001), an estimated 0.5–1 million additional US children were diagnosed with specific delays in development as a consequence of 25 μg or 37.5 μg organic Hg from T-HBVs administered within the first 6 months of life.”
The study added, “[This] study provides compelling new evidence to confirm and extend previous epidemiological studies finding a significant relationship between organic Hg exposure from Thimerosal-containing childhood vaccines and the subsequent increased risk of a diagnosis for specific delays in development.”
A 2018 cross-sectional study published in the International Journal of Environmental Research and Public Health strongly suggested that the 1990s-era thimerosal-containing HepB vaccine caused considerable harm to children concluding, “This cross-sectional study provides new evidence consistent with and extends the results from previous epidemiological and biological studies on the adverse effects of Hg exposure from Thimerosal-containing childhood vaccines. This study supports a significant about nine-fold increase in the risk of adverse effects as measured by receipt of special education services among boys receiving infant Thimerosal-containing hepatitis B vaccination.”
The study added to the chorus of voices demanding thimerosal be removed from all vaccines given to pregnant women and children.
The Food and Drug Administration (FDA) Modernization Act of 1997 called for the FDA to review and assess the risk of all mercury-containing food and drugs.
In 1999 the FDA determined that, “under the recommended childhood immunization schedule, infants might be exposed to cumulative doses of ethylmercury that exceed some federal safety guidelines established for ingestion of methylmercury, another form of organic mercury (Ball et al., 2001). In July 1999, the American Academy of Pediatrics (AAP) and the U.S. Public Health Service (PHS) issued a joint statement recommending the removal of thimerosal from vaccines as soon as possible.”
The statement also recommended, “a temporary suspension of the birth dose of hepatitis B vaccine for children born to low-risk mothers until a thimerosal-free alternative became available.”
Merck responded by making a new vaccine available immediately, gaining FDA approval for its thimerosal-free Recombivax HB vaccine on August 27, 1999 with distribution beginning in September.
SmithKline Beecham reformulated its thimerosal-free Engerix-B which the FDA approved in 2000.
Neal Halsey, M.D., director of the Institute for Vaccine Safety, assured the public the new Engerix-B contained only trace amounts of thimerosal (<1 mcg), which will “have no clinically relevant effects making it equivalent to a thimerosal-free product.”
While recommending newborns and infants up to the age of six months avoid vaccinations with thimerosal the CDC still allowed those over the age of six months to receive the thimerosal-containing HepB vaccines.
Even as thimerosal was being phased out of children’s vaccines, safety concerns surrounding ingredients in the Hepatitis B vaccine persisted. Disturbing reports relating to aluminum adjuvants found in the vaccines emerged and continue to this day.
In a 2008 article in Mothering magazine pediatrician Robert Sears sounded alarm bells about the dangers of vaccinations which contained aluminum adjuvants.
While embarking upon an inquiry to see if anyone had actually tested and scientifically assessed “safe” levels of injected aluminum he discovered an FDA document on aluminum toxicity which warned:
“Aluminum may reach toxic levels with prolonged parenteral administration [i.e., injected into the body] if kidney function is impaired. Research indicates that patients with impaired kidney function, including premature neonates [i.e., babies], who received parenteral levels of aluminum at greater than 4 to 5 micrograms per kilogram of body weight per day, accumulate aluminum at levels associated with central nervous system and bone toxicity. Tissue loading [i.e., toxic buildup in certain body tissues] may occur at even lower rates of administration.”
A second document produced by the American Society for Parenteral and Enteral Nutrition (ASPEN) also emphasized a daily limit of 4 to 5 mcg of aluminum per kilogram (2.2 lbs) of body weight for babies being fed an IV solution containing aluminum.
While neither of these documents mentioned vaccines specifically, both the ASPEN group and the FDA agreed that all injectable solutions for children should be limited to a maximum amount of 25 mcg of aluminum within a 24-hour period.
The FDA’s Code of Federal Regulations explicitly states, “The aluminum content of large volume parenteral (LVP) drug products used in total parenteral nutrition (TPN) therapy must not exceed 25 micrograms per liter ([micro]g/L).”
The unsettling fact regarding the HepB vaccine in regards to aluminum is that each dose, given at birth, 2 months and 6 months, is laced with 250 mcg of aluminum– far exceeding the recommended safe levels for large volume parenteral (LVP) drug products.
In a 2011 study Canadian scientists Professor Christopher Shaw and Dr. Lucija Tomljenovic asked the question, Aluminum Vaccine Adjuvants: Are they Safe?
The answers they discovered are worth quoting at length:
“Aluminum is an experimentally demonstrated neurotoxin and the most commonly used vaccine adjuvant. Despite almost 90 years of widespread use of aluminum adjuvants, medical science’s understanding about their mechanisms of action is still remarkably poor.
Experimental research, however, clearly shows that aluminum adjuvants have a potential to induce serious immunological disorders in humans. In particular, aluminum in adjuvant form carries a risk for autoimmunity, long-term brain inflammation and associated neurological complications and may thus have profound and widespread adverse health consequences.”
…
“Given that multiple aluminum-adjuvanted vaccines are often given to very young children (i.e., 2 to 6 months of age), in a single day at individual vaccination sessions, concerns for potential impacts of total adjuvant-derived aluminum body burden may be significant. These issues warrant serious consideration since, to the best of our knowledge, no adequate studies have been conducted to assess the safety of simultaneous administration of different vaccines to young children.” [Bold Added]
In a 2013 study, Aluminum in the Central Nervous System: Toxicity in Humans and Animals, Vaccine Adjuvants, and Autoimmunity, Shaw and Tomljenovic concluded, “In young children, a highly significant correlation exists between the number of pediatric aluminum-adjuvanted vaccines administered and the rate of autism spectrum disorders. Many of the features of aluminum-induced neurotoxicity may arise, in part, from autoimmune reactions, as part of the autoimmune/inflammatory induced by adjuvants (ASIA) syndrome.”
UK Professor Christopher Exley, known as Mr. Aluminum, has devoted much of his life to studying the dangers of aluminum, with a particular focus on the use of aluminum adjuvants in childhood vaccines.
With numerous studies and papers to his credit Exley is particularly recognized for his discovery which proved that cells known to populate a vaccine injection site actually take up aluminum adjuvant into their cell bodies.
Accompanying this finding was his pioneering revelation that antigens and adjuvants are taken up as separate particles. Both discoveries have implications for the possible role of aluminum adjuvants in instigating serious adverse events distant from the vaccine injection site.
Multiple studies have aligned with Exley’s findings that the intramuscularly injected aluminum vaccine adjuvant is absorbed into the systemic circulation and travels to different sites in the body such as the brain, joints and the spleen where it accumulates and is retained for years post-vaccination.
Cui Bono?
According to statistics, Hepatitis B causes death in fewer than one quarter of one percent of those infected. It is a near certainty that even that rate is an overestimate since deaths of hepatitis B infected drug addicts and alcoholics is more likely due to their habits which destroy their liver and other vital organs and not the disease.
In 1986, five years before the CDC began pushing for vaccination of all newborns, the US had documented fewer than 280 cases of hepatitis B infection in children under age 14. Newborns are probably the least likely human beings on the planet at risk of actually getting hepatitis B.
Given that most infants are not at risk for Hepatitis B in the United States and given the copious documentation linking the Hepatitis B vaccine to various pathologies (here, here and here) we return to the question: Why the fanatical push for universal HepB vaccination for children?
If we look at the HepB childhood vaccination program from a perspective of health and “saving lives” we are confronted with a world of contradictions and manipulations- none of it makes sense.
If looked at it through the lens of power, money and control everything makes perfect sense.
A 2005 letter written by Dr. Marc Girard to the Director General of the World Health Organization referenced a correspondence he had with an Indian colleague, Dr J. Puliyel, on the false data being disseminated by the WHO about the epidemiology of hepatitis B in India.
This exchange gives us insight into the processes by which a once non-existent threat is turned into a public health crisis and the motives behind this.
Girard noted that, “the mechanisms of the deception described by Dr Puliyel were exactly comparable to those I observed in my own country — and of course with the same results: a plea of “experts” to include hepatitis B vaccination in the national vaccination program, in spite of its costs and, its unprecedented toxicity.” [Emphasis added]
Dr. Girard went on to state: “It is blatant that in the promotion of the hepatitis B vaccination, the WHO has never been more than a screen for an undue commercial promotion, in particular via the Viral Hepatitis Prevention Board (VHPB), created, sponsored and infiltrated by the manufacturers.
In Sept 1998, while the dreadful hazards of the campaign had been given media coverage in France, the VHPB met a panel of “experts”, the reassuring conclusions of which were extensively announced as reflecting the WHO’s position: yet some of the participants in this panel had no more “expertise” than that of being employees of the manufacturers.” [Emphasis added]
Girard also drew attention to a 1997 interview published in the French journal Sciences et Avenir in which GlaxoSmith Beecham’s business manager admitted, “We started increasing the awareness of the European Experts of the World Health Organization (WHO) about Hepatitis B in 1988. From then to 1991, we financed epidemiological studies on the subject to create a scientific consensus about hepatitis being a major public health problem. We were successful because in 1991, WHO published new recommendations about hepatitis B vaccination.”
This cynical admission by one of the primary manufacturers of the Hepatitis B vaccine offers a glimpse into how the time honored strategy of problem-reaction-solution is applied in the Pharmaceutical Industry
The disease itself is seen as superfluous, all that is necessary is to create the perception that there is a widespread public health crisis which requires a heroic and international medical intervention in the form of a vaccine which, curiously, was already in production leading into the “crisis.”
Such a frank admission reinforces the facts surrounding the history of Hepatitis B, there was little to no problem with this disease until after the vaccine became available and for marketing reasons they had to change the image of the disease.
Tracing the breadcrumbs of the entire production of the Hepatitis B vaccine campaign a pattern emerges which appears to be a non-medical agenda that leads to the reliable predictor-follow the money.
For years vast amounts of financial and political capital were invested in the Hepatitis B vaccine as well as enormous amounts of resources allocated towards research and development. Each new HepB vaccine was hailed as a medical wonder.
Despite these efforts the medical industry couldn’t get people to take the vaccine which meant meager returns on these enormous investments.
To solve this dilemma, and address the sunk costs, the pharmaceutical industry, through its cadre of captured policy makers, invented regulations fashioned to make the vaccines compulsory thusly creating a captured customer base and guaranteeing revenue.
The “at-birth” vaccines have the added benefit, from the manufacturers perspective, of providing “vaccine training wheels” for new parents, conditioning them for a steady routine of immunization appointments.
The 12 million doses of Hepatitis B vaccine administered to children each year in the US alone represents a substantial annual income stream for vaccine manufacturers.
The NY Times reported that the average cost to fully vaccinate a child to the age of 18 in a private doctor’s office soared from $100 in 1986 to $2,192 by 2014.
To get every dose of every recommended vaccine in a private pediatricians office circa 2023 that cost now exceeds a staggering $3,000.
Heading into the 21st century the commercialization of vaccines has expanded into a colossal and profitable global enterprise, and according to International Monetary Fund chief Kristalina Georgieva, vaccine policy is now one of the most important drivers of global economic policy.
A Final Word
In two separate hearings in 1999 Michael Belkin, whose daughter died of Sudden Infant Death Syndrome (SIDS) immediately after receiving a Hepatits B vaccine dosage, called the HepB vaccine policy a ”bureaucratic vaccination program that is on auto-pilot flying into a mountain” and accused CDC bureaucrats of “hav[ing] a vested interest in the status quo.”
Mr. Belkin’s conclusions merit reciting in full:
-
Newborn babies are not at risk of contracting the hepatitis B disease unless their mother is infected.
-
Hepatitis B is primarily a disease of junkies, gays, and promiscuous heterosexuals.
-
The vaccine is given to babies because health authorities couldn’t get those risk groups to take the vaccine.
-
Adverse reactions out-number cases of the disease in government statistics.
-
Nothing is being done to investigate those adverse reactions.
-
Those adverse reactions include numerous deaths, convulsions and arthritic conditions that occur within days after
-
Hepatitis B vaccination. The CDC is misrepresenting hypothetical, estimated disease statistics as real cases of the disease.
-
The ACIP is recommending new vaccines for premature infants without having scientific studies proving they are safe.
-
The U.S. vaccine recommendation process is hopelessly compromised by conflicts of interest with vaccine manufacturers, the American Academy of Pediatrics and the CDC.
While Mr. Belkin was addressing the Hepatitis B vaccination specifically as an injection which may present risks for health complications, the risks of toxicity and adverse reactions for all vaccines is a question that demands far more rigorous scrutiny than has been provided to date.
We hope that this series will provide a framework for a long overdue assessment of this highly contentious medical issue.
Our next installment takes a look at the Rotavirus vaccine.
The Truth: No Vaccines Are Safe For Children
Dr Tess Lawrie, MBBCH, PHD | A Better Way to Health | September 10, 2023
This week the World Council for Health (WCH) issued an official caution against all vaccines on the childhood vaccination schedule. I’ve re-published the statement below.
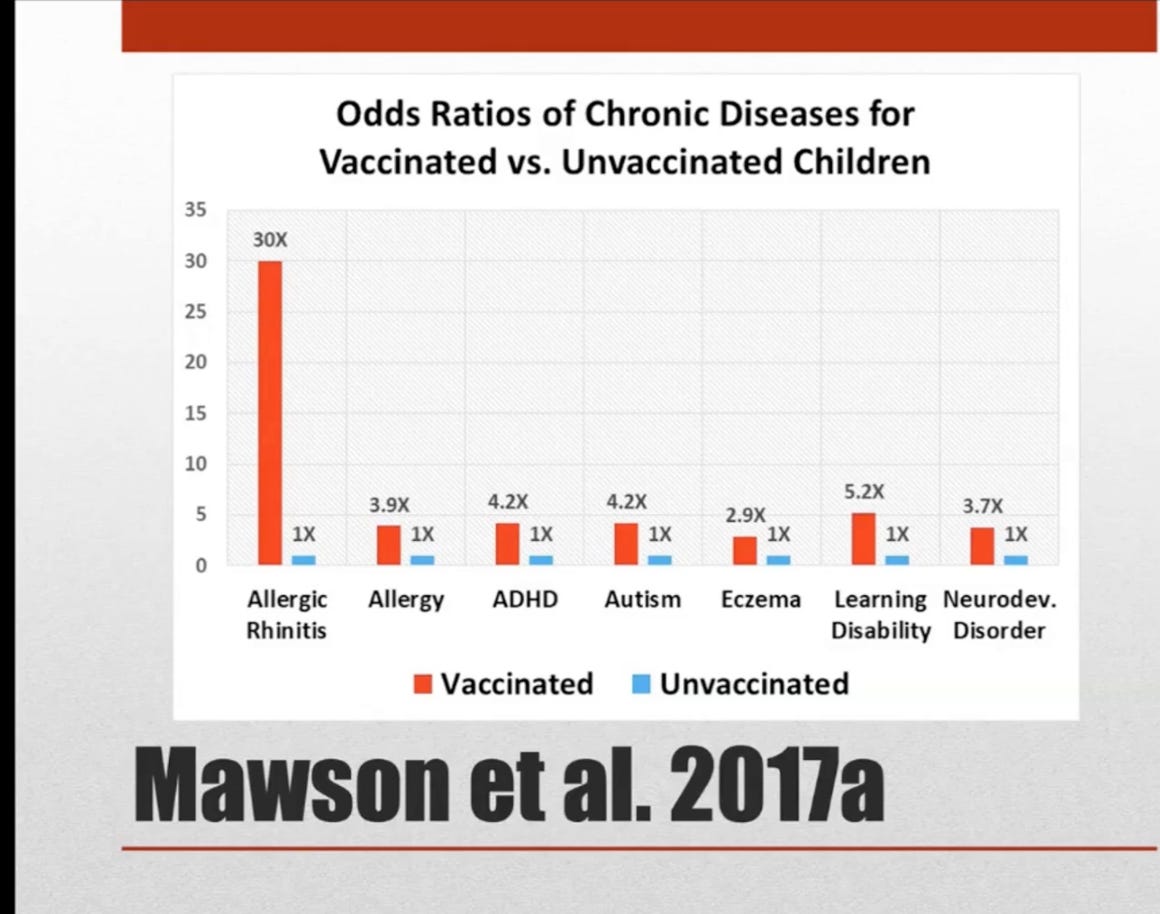
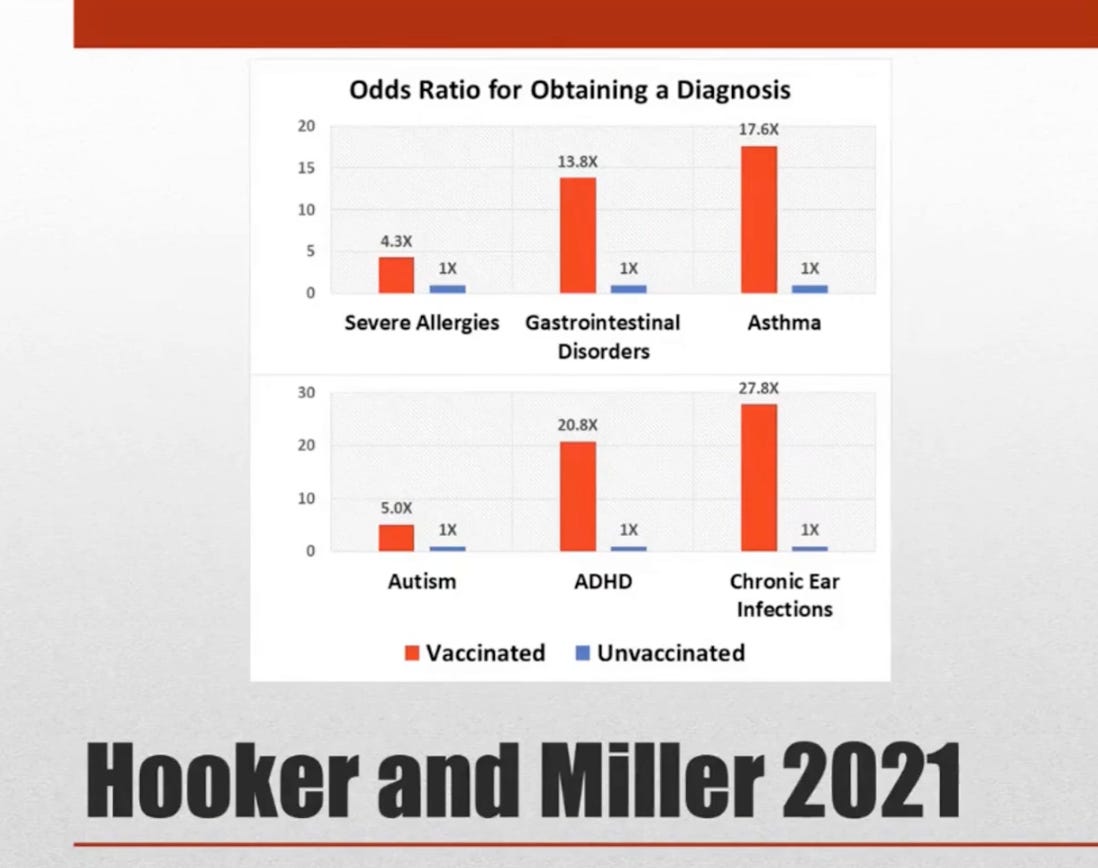
The following images have been taken from WCH General Assembly Meeting #101 in which Prof. Brian Hooker presented the latest research:



World Council for Health | September 5, 2023
The number of vaccines given to babies and children has increased dramatically without the necessary due diligence by regulatory authorities. Parents are urged to adopt a common-sense, ‘Safer to Wait” approach.
Growing international concerns about vaccine regulatory processes and vaccine safety have emerged following the widespread regulatory failure of Covid-19 vaccines. The Covid-19 crisis has demonstrated that regulatory bodies, once public watchdogs, are now at best incompetent and at worst have been deeply corrupted by pharmaceutical industry interests.
In the context of emerging revelations of regulatory body incompetence and corruption, e.g. The Perseus Report, the WCH Health and Science Committee notes that:
- Several research studies now indicate that vaccinated children have far worse health outcomes with higher rates of many chronic diseases than non-vaccinated children.
- The integrity of scientific research and the regulatory process of childhood vaccines, including the new nasal ‘flu’ vaccine, now being administered en masse in schools is in question.
- Pharmaceutical corporations have a long-standing history of misrepresenting products that cause injuries and deaths. Pfizer, for instance, has paid the largest criminal settlement in history for drug fraud. The childhood vaccination schedule provides these unscrupulous corporations with unregulated access to the bodies of our children.
- Modern society is experiencing unprecedented rates of autism, asthma, allergies, inflammatory bowel disease, diabetes, obesity, depression and more, for which the root cause/s have not been established.
- Much of what we have been told about the success of early vaccines, including smallpox and polio vaccines is emerging as untrue. Clean water, modern plumbing, hygiene, refrigeration, and improved nutrition are real factors that have correlated with the dramatic reduction in many infectious diseases over the past century.
- National regulatory agencies have never done the necessary evaluation to determine whether vaccines given to children alone or together according to the ever-expanding childhood vaccination schedules are associated with poor health outcomes compared with children who are not vaccinated.
- National regulatory agencies have been turning a blind eye to the mounting evidence linking childhood vaccination with autism that has emerged since a possible link was first suggested in 1998.
- National regulatory agencies have also been turning a blind eye to the mounting evidence linking childhood vaccination with other diseases, including asthma, allergies, and bowel disease.
- The vast majority of children find vaccination with needles painful and long-term psychological harms, including disruption to breastfeeding and maternal bonding, have not been properly evaluated.
- There are serious concerns among experts that existing childhood vaccines will be converted to mRNA technology, which has never been proven safe for use in vaccines for adults let alone children, and that this will be done without public awareness, consent and a robust research and regulatory process.
- With regard to Covid-19 vaccination, evidence from independent experts and official international databases show that the Covid-19 vaccines are not effective and are not safe, raising serious questions around the authorisation of the Covid-19 vaccines for babies and children.
In addition to these specific considerations, the burgeoning vaccination schedule for children needs to be viewed in the context of the following supranational developments in global health policy:
- The World Health Organisation (WHO) and its private and state stakeholders have financial and ideological interests in the provision of vaccines and has committed to providing 500 vaccines by 2030.
- The WHO and its stakeholders are working for the pharmaceutical industry and creating legislation that would give them the power to mandate injections by force for you and your children.
- The WHO supports gain-of-function research, facilitating the creation of dangerous pathogens as well as the vaccines to combat newly created pathogens, thus creating a self-perpetuating vaccine industry based on fear.
In the current circumstances, the World Council for Health urges parents to consider childhood vaccination very carefully and adopt a common-sense, “Safer to Wait” approach to the vaccination of your boys and girls.
For the sake of all children and a healthy society it is time that we all question our blind faith in vaccines, the corporations that produce them, and the regulatory bodies and supranational organisations that enable and profit directly or indirectly through their authorisation.
The World Council for Health will continue to bring you supportive information and resources to help you optimize your family’s health naturally. Be assured that reducing infectious disease and maximizing your children’s health is rooted in wholesome nutrition, good physical and mental hygiene, a healthy outdoor lifestyle and your unconditional love.
- WCH meeting #101, August 28th 2023. https://worldcouncilforhealth.org/multimedia/brian-hooker-vax-unvax/
- Anthony R. Mawson et al., “Preterm Birth, Vaccination and Neurodevelopmental Disorders: A Cross-Sectional Study of 6- to 12-Year-Old Vaccinated and Unvaccinated Children,” Journal of Translational Science 3, no. 3 (2017): 1-8, doi:10.15761/JTS.1000187.
- Anthony R. Mawson, et al., “Pilot Comparative Study on the Health of Vaccinated and Unvaccinated 6 to 12-year-old U.S. Children,” Journal of Translational Science 3, no. 3 (2017): 1-12, doi:10.15761/JTS.1000186.
- Brian Hooker and Neil Z. Miller, “Analysis of Health Outcomes in Vaccinated and Unvaccinated Children: Developmental Delays, Asthma, Ear Infections and Gastrointestinal Disorders,” SAGE Open Medicine 8, (2020): 2050312120925344, doi:10.1177/2050312120925344.
- Brian Hooker and Neil Z. Miller, “Health Effects in Vaccinated versus Unvaccinated Children,” Journal of Translational Science 7, (2021): 1-11, doi:10.15761/JTS.1000459.
- James Lyons-Weiler and Paul Thomas, “Relative Incidence of Office Visits and Cumulative Rates of Billed Diagnoses along the Axis of Vaccination,” International Journal of Environmental Research and Public Health 17, no. 22 (2020): 8674, doi:10.3390/ijerph17228674.
- Wakefield AJ, et al. Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children. The Lancet. 1998. doi.org/10.1016/S0140-6736(97)11096-0.
- Turtles All The Way Down. Vaccine Science and Myth. 2022. Editor: Zoey O’Toole. Foreword by Mary Holland.
- Kirsch S.If vaccines don’t cause autism, then how do you explain all this evidence? May 2023.
- Vax-Unvax. Let the Science Speak. August 2023. Robert F. Kennedy Jr and Brian Hooker, PhD.
- Countering the WHO’s “Big Catch-up” Global Campaign and Immunization Agenda 2030. WCH Statement. May 12, 2023.
- Rejecting Monopoly Power over Global Public Health. WCH Policy Brief. May 2023.
CDC’s New ‘Wild to Mild’ Ad Campaign Hypes Flu Vaccines for Kids, Pregnant Women
John-Michael Dumais | The Defender | September 8, 2023
The Centers for Disease Control and Prevention (CDC) this week launched a new “Wild to Mild” ad campaign to “tame skepticism about flu vaccines,” CNN Health reported.
The campaign, which will run on the radio and social media platforms starting this week, targets pregnant women and parents of young children “because vaccination rates are down in both of those high-risk groups,” said CNN.
Experts who spoke with The Defender, however, questioned the efficacy of flu vaccines and cautioned about their potential harms.
The CDC ads feature cute animal images, including one that depicts a tiger (“a ferocious animal”) and a kitten (“something that’s not scary”) designed to promote the idea that the flu vaccine, rather than preventing influenza altogether, will inhibit severe symptoms and yield a milder course of the illness.
The CNN article cited CDC data showing flu vaccination rates for pregnant women are down more than 16% since 2019 and 7% for children under 18. “That means more than 3.7 million people were unprotected during pregnancy over the past winter” along with “an estimated 32 million children,” CNN reported.
Erin Burns, M.A., associate director for communications for the Influenza Division at the CDC, told CNN the progress made to vaccinate pregnant women after the 2009 H1N1 pandemic has been “completely wiped out in the years since COVID-19.”
Focus groups run by the CDC showed that “most of the pregnant women had no intention of getting a flu vaccine and no awareness of the benefits it could bring them or their baby,” Burns said.
Dr. William Schaffner, infectious disease specialist at Vanderbilt University and a member of the CDC’s Advisory Committee on Immunization Practices, told CNN that “something was amiss” if doctors were not adequately informing pregnant women about the risks of the flu.
“Women who get influenza who are pregnant may have rates of complication that rival that of senior citizens,” Schaffner said, adding “They [doctors] have to get these messages out to women who come to them right now.”
Burns said mothers in focus groups found it “extremely motivating” when health educators explained that antibodies induced by flu shots could transfer to their babies and protect them after birth.
While seniors tend to understand their higher risk from the flu and therefore keep up with their shots, moms need more nudging, CNN reported.
Ad campaign tempers expectations about respiratory vaccines
According to CNN, Burns said the CDC felt cautious about claiming flu vaccines could attenuate illness, but since deepening its vaccine surveillance network, it found “strong and growing evidence” that the vaccine could “blunt a bout with the flu” and reduce doctor visits.
Schaffner said comparing the effectiveness of the flu vaccine to vaccines designed to eradicate diseases like measles, polio and whooping cough confuses people about what flu shots can do.
“With these respiratory viruses,” he said, “the vaccines aren’t very good at preventing milder disease. [But] we have to say … ‘here’s the benefit.’”
According to the CDC, all flu vaccines for the 2023-2024 season will be quadrivalent (i.e., targeting four different strains).
“Most will be thimerosal-free or thimerosal-reduced vaccines (91%), and about 21% of flu vaccines will be egg-free,” states the CDC website.
Hundreds of peer-reviewed studies show that thimerosal is a developmental neurotoxin.
The CDC is recommending the flu and respiratory syncytial virus, or RSV, vaccines this fall for everyone, and also the COVID-19 vaccine or booster for people 6 months and older.
‘Basically, it does not work’
The CDC states that flu vaccine effectiveness can vary, citing studies over the past 10 years showing between 19% and 54% effectiveness. The major factors influencing vaccine effectiveness are a person’s age and health and how well the vaccines match the circulating virus strains.
Dr. Meryl Nass told The Defender the CDC claims that flu shots reduce flu severity “cannot be relied on” when the shots “fail to work to prevent infection.”
Nass pointed to four studies the CDC uses to support its new contention that flu shots reduce flu severity even if they do not prevent flu. “All four published studies have CDC authors, so the CDC cites itself to make this claim.”
Two of the papers, published in the journal Vaccine in 2018 and 2021, said Nass, start by acknowledging that the effect of influenza vaccination on influenza severity remains uncertain.
Dr. Anthony Fauci, former head of the National Institute for Allergy and Infectious Diseases, in a paper published in January with co-authors Dr. David M. Morens and Jeffery K. Taubenberger, M.D., Ph.D., said that vaccines for respiratory diseases are “decidedly suboptimal” and that new types of vaccines need to be developed.
“’Wild to Mild’ is a propaganda strategy to throw up against the facts,” Nass said, “that efficacy is often poor, that flu shots have never been shown to prevent deaths and that even Fauci has now admitted this.”
Commenting on the campaign, Dr. Peter McCullough told The Defender, “In the last several years the estimated vaccine efficacy of the influenza vaccine was statistically insignificant. Basically, it does not work.”
‘No data’ on safety of flu shots for pregnant women and their babies
According to Nass, in the past flu shots were not approved for pregnancy.
“They used to be labeled ‘Category C,’ which meant ‘no data in pregnancy,’” she said. “That system of specifying the pregnancy risk was junked to make way for verbiage instead.”
As an example of this “verbiage,” Nass referred to the U.S. Food and Drug Administration’s (FDA) risk summary for the flu vaccine FLULAVAL, which states:
“All pregnancies have a risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
“There are insufficient data on FLULAVAL in pregnant women to inform vaccine-associated risks.”
The flu vaccines’ effect on lactation also is unknown, according to Nass. “Despite CDC recommending use in pregnancy for well over 10 years, they just have not looked,” she said.
According to the FDA, “Data are not available to assess the effects of FLULAVAL on the breastfed infant or on milk production/excretion.”
Brian Hooker, Ph.D., senior director of science and research at Children’s Health Defense and co-author of “Vax-Unvax: Let the Science Speak,” reviewed a 2021 study published in JAMA Network on flu vaccination during pregnancy.
The retrospective cohort study reviewed live births in Nova Scotia, Canada, from 2010-2014, with a follow-up in 2016. The authors concluded that “maternal influenza vaccination during pregnancy was not significantly associated with an increased risk of adverse early childhood health outcomes.” But, according to Hooker, the study failed to consider several key points.
The first shortcoming was that diagnoses considered in the study were based on emergency visits and hospitalizations only, not outpatient settings such as practitioner offices, where most diagnoses are made.
To support his criticism of this diagnostic bias, Hooker noted the study found only 1.1% cases of asthma while for the overall Canadian population, the asthma rate was 9.5%.
The study also inaccurately reported on the rates of ear infections in unvaccinated versus vaccinated groups, with the latter experiencing significantly higher rates.
The study showed a significant association between lower respiratory infection in babies for mothers vaccinated in the third trimester versus unvaccinated mothers, but “these results were summarily ignored by the study authors,” Hooker said.
Finally, the study’s “control diagnosis,” which it defined as “all-cause injuries,” showed a significantly higher incidence for children whose mothers were vaccinated, which, Hooker said, “casts a shadow of doubt on any conclusions made from this study.”
Hooker expressed concern that physicians would use the study to provide a “false assurance of safety” to pregnant women considering the flu vaccine.
Nass said the majority of claims filed and compensated in the National Vaccine Injury Compensation Program (NVICP) — which has paid out over $4 billion to date — are for injuries from the flu vaccine.
NVICP is part of the 1986 National Childhood Vaccine Injury Act. It was passed to exempt vaccine manufacturers from product liability, based on the legal principle that vaccines are “unavoidably unsafe” products.
John-Michael Dumais is a news editor for The Defender. He has been a writer and community organizer on a variety of issues, including the death penalty, war, health freedom and all things related to the COVID-19 pandemic.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Breast Cancer in Women Under 50 on the Rise — Could Cellphones Play a Role?
By Suzanne Burdick, Ph.D. | The Defender | September 6, 2023
Early-onset breast cancer is on the rise in younger women in the U.S., according to two new peer-reviewed studies, leading some experts to wonder if cellphone use could be at least partially to blame.
The authors of an Aug. 16 study in JAMA Network Open looked at the health data from 2010 to 2019 of more than half a million people in the U.S. under 50 who reported having some kind of early-onset cancer.
They concluded breast cancer in 2019 had the highest incidence rate, with 12,649 new cases reported that year.
Meanwhile, the authors of a study published Sept. 5 in BMJ Oncology looked at worldwide cancer trends from 1990-2019. Breast cancer was responsible for the largest number of cases and associated deaths among younger people, with rates of 13.7 cases and 3.5 deaths per 100,000 people, they said.
Devra Davis, Ph.D., MPH, a toxicologist and epidemiologist who for more than 40 years has studied trends in cancer and who published more than 200 peer-reviewed articles, said she found the reports “very troubling.”
Davis is the president of Environmental Health Trust (EHT), a scientific research and education nonprofit, and founding director of the Board on Environmental Studies and Toxicology of the U.S. National Research Council at the National Academy of Sciences.
She told The Defender, “A trend in cancer cannot prove what is causing it. The trend is simply a fact. So the fact is that cancer among younger Americans, particularly women, is on the rise.”
Indeed, the American Cancer Society in 2022 estimated there were 47,550 cases of breast cancer in U.S. women younger than 50.
“But,” Davis added, “there’s clear compelling evidence that electromagnetic fields [EMFs] accelerate the growth of breast cancer cells.”
EMFs can accelerate growth of breast cancer cells
“We have known for nearly 30 years that EMFs can accelerate the growth of MCF-7 breast cancer cells,” Davis said. “There’s no debate about that.”
According to Davis, MCF-7 is an estrogen receptor-positive cancer cell that has been cultured for many years and is used as a standard assay in the laboratory.
Davis said prior research showed radiofrequency (RF) radiation emitted by cellphones moves easily through fat and fluid — “and the breast is nothing but fat and fluid,” she said.
Additionally, a 2020 peer-reviewed study found that excessive smartphone use “significantly increased” the risk of breast cancer, with those using cellphones for more than 4.5 minutes before bedtime having a 5.27-fold increased risk of breast cancer compared to those using a smartphone for less time.
The study authors said:
“To the best of our knowledge, we are the first to find that excessive smartphone use significantly increased the risk of breast cancer, particularly for participants with a smartphone addiction, who maintained a close distance between the breasts and smartphone, and who had the habit of smartphone use before bedtime.”
Staring at a cellphone screen before bedtime can also suppress the natural release of melatonin, a hormone that plays a role in sleep.
Melatonin appears to protect against breast cancer, Davis said. “We know this most especially from studies of blind women because blind women naturally have very high levels of melatonin and they have half the rate of breast cancer of sighted women,” she said.
Some research, however, suggests more thorough studies must be done before the link between melatonin and decreased risk of breast cancer can be proven.
Davis and several co-authors in February 2023 published a review of the latest science on pediatric health, EMFs and RF radiation in which they noted that RF radiation can act like an endocrine disruptor:
“It appears that non-ionizing RFR has all the classic hallmarks of endocrine disruptors that affect reproduction, development of the hypothalamic-pituitary-gonadal axis (HPG) and alter normal male and female reproductive endpoints.”
According to Davis, endocrine disruptors can cause “a host of biological consequences, including breast cancer.”
EHT in 2020 collaborated with the Massachusetts Breast Cancer Coalition to create an educational module for K-12 schools on the health impacts of daily RF radiation exposure and ways to reduce one’s exposure, Davis said.
‘We’re going to see a whole cluster of young people with breast cancer’
According to Davis, there have been at least five case reports of women developing breast cancer tumors where they routinely kept their cellphones in their bras.
One of the case report’s authors, Dr. John West, is a former breast surgeon who more than a decade ago predicted there would be an uptick in breast cancer cases.
West told CBS News in Nov. 2012, “If there is a risk and we don’t find out about it for five or ten years from now, we’re going to see a whole cluster of young people with breast cancer.”
West and his co-authors in 2013 published their case report of four women who carried their smartphones in their bras for up to 10 hours a day for several years, and who “developed tumors in areas of their breasts immediately underlying the phones.”
“These cases,” West and his co-authors said, “raise awareness of the lack of safety data of prolonged direct contact with cellular phones.”
In 2016, West wrote a book about breast cancer prevention, “Prevent, Survive, Thrive: Every Woman’s Guide to Optimal Breast Care,” with a chapter entitled, “Your Bra: A No-Phone Zone.”
That same year, Dr. Otis W. Brawley, the ACS’ former chief medical officer, highlighted the potential link between cellphone radiation and cancer in a May 27, 2016, press release citing the National Toxicology Program (NTP) multi-year $30 million study showing “clear evidence” that RF radiation is associated with cancer and DNA damage. He said:
“For years, the understanding of the potential risk of radiation from cell phones has been hampered by a lack of good science. This report from the National Toxicology Program (NTP) is good science.”
Brawley said the NTP’s report “marks a paradigm shift in our understanding of radiation and cancer risk.”
But the “paradigm shift” Brawley referenced never took hold after the U.S. Food and Drug Administration (FDA) in 2020 dismissed the NTP study.
According to Davis, the FDA’s rejection of the NTP study was “deeply flawed” and “deeply hypocritical.”
The FDA in 1999 requested the NTP study cellphone radiation, she said. FDA officials were intimately involved in reviewing the study design plans.
“Then when the results came out and some people didn’t like it, the FDA began to trash talk their own study,” Davis said.
To this date, the FDA still claims there is not enough scientific evidence to link cellphone use to health problems, including cancer.
Breast cancer is the most common type of cancer worldwide, excluding non-melanoma skin cancer, with 2.26 million cases in 2020 noted by the World Health Organization.
Suzanne Burdick, Ph.D., is a reporter and researcher for The Defender based in Fairfield, Iowa. She holds a Ph.D. in Communication Studies from the University of Texas at Austin (2021), and a master’s degree in communication and leadership from Gonzaga University (2015). Her scholarship has been published in Health Communication. She has taught at various academic institutions in the United States and is fluent in Spanish.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Bio-Pharmaceutical Censorship Complex Attacks Spike Detoxification Protocol
Syndicate Fact Checkers Confirm Empiric Regimen is Valuable for Post-Acute Sequelae after SARS-CoV-2 Infection and COVID-19 Vaccination
By Peter A. McCullough, MD, MPH | Courageous Discourse | August 31, 2023
It took less than a day since our Base Spike Protein Detoxification Protocol was published for the Biopharmaceutical Complex to come out with syndicate social media allies discrediting the most hopeful news long-COVID and vaccine suffers have heard since the start of their misery.
Syndicate fact checker Science Feedback, issued an unsupported false counterclaim on Instagram given below.
![]()
Science Feedback, a science and climate blogging organization with no foundation in peer-reviewed medical publications, is not advised by prominent physicians working in the COVID-19 field. Their major donor is former Microsoft and Apple executive Eric Michelman who is also a noted Democrat supporter, donating money to the Presidential campaigns of Barack Obama and Joe Biden. Michelman is also a climate change activist, founding a climate change advocacy organization and publicly supporting a carbon tax.
LinkedIn pulled a post indicating the COVID-19 vaccine causes more post-acute sequelae than SARS-CoV-2 which is my clinical opinion supported by the data. Base Spike Detoxification is an approach a to both problems. LinkedIn uncredentialed anonymous content moderators obviously disagreed and continue to push the false narrative indicating that long-COVID is unassailable and the only answer is more genetic shots.

I have found it interesting that the fact checkers have never made claims against a myriad of drugs or supplements that were ineffective during the pandemic. They have exclusively targeted therapies with preclinical and clinical studies demonstrating signals of benefit and acceptable safety (iodine/xylitol nasal washes, vitamin D, hydroxychloroquine, ivermectin, budesonide). In a perverted way, the Biopharmaceutical Complex has confirmed Base Spike Detoxification is the path forward for so many patients suffering from long-COVID and or regretting the jab.
Peter A. McCullough, MD, MPH
President, McCullough Foundation
Featured Video

Yemen joins the war – Red Sea could be blocked next – Saudi regime at risk
or go to
Aletho News Archives – Video-Images
From the Archives
Should Europeans ‘Thank’ the Americans for Destroying Nord Stream?
By Robert Bridge | Strategic Culture Foundation | September 29, 2022
With an investigation continuing into the destruction of the Nord Stream gas pipeline that provided energy supplies to Europe from Russia, there appears to be just one prime suspect, and that should surprise nobody.
Following the sabotage of the Nord Stream 1 and 2 gas pipelines, former Polish Foreign Minister Radoslaw Sikorski already seemed to know the identity of the perpetrator when he tweeted out: “Thank you, USA.”
At first glance, it seemed that Sikorski was speaking sarcastically, berating Washington for carrying out an attack that will have severe repercussions for the people of Europe. After all, how could anyone see any good coming from the termination of Europe’s primary source of gas reserves with winter just around the corner? It was Sikorski’s homeland of Poland, after all, that urged its citizens to collect firewood in the face of dwindling gas reserves.
In fact, the Polish diplomat was speaking one-hundred percent literally… continue
Blog Roll
 Aletho News
Aletho News- Russian Oil Tanker Arrives in Cuba Amid U.S. Blockade
- America Racing to Strategic Defeat in Iran: Lt Col Daniel Davis
- FTC Warns Visa, Mastercard, PayPal, Stripe Over Political Debanking
- Russian tanker approaches Cuba despite US oil blockade
- Marandi: Yemen joins the war – Red Sea could be blocked next – Saudi regime at risk
- Pro-Palestinian French member of European Parliament denied entry to Canada
- Pakistan to Host US-Iran Talks
- How Indonesia’s tilt toward the US left it stranded in the Strait of Hormuz
- US has no choice but to retreat from Iranian borders: Top commander
- Iran Retaliation Strikes Chemical Plant Near Dimona
- If Americans Knew
- Israeli police block Catholic cardinal from entering Church of the Holy Sepulchre on Palm Sunday
- Israel is assassinating journalists again, more than any other nation, anywhere, ever – Not a ceasefire Day 170
- Over 300 US service members wounded, majority have brain injuries – Not a ceasefire Day 169
- Researchers at Human Rights Watch Resign Over Blocked Report on Palestinian Refugee Return
- Jewish Groups Are Backing a War Americans Don’t Want
- Eric Fingerhut Thinks He’s the President of the Jews
- Top Jewish Philanthropists, Rabbis Urge Israeli President to Take Action Against ‘Jewish Extremists’
- Don’t Be Fooled. Zionist Leaders Have Always Wanted to Control Southern Lebanon
- Israel’s widespread use of torture is a core element of its genocide against the Palestinian people
- In Israel’s War on Iran, Many Middle East US Bases Rendered “All But Uninhabitable”
- No Tricks Zone
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis
