New Book: Covid Through Our Eyes
Review by Maryanne Demasi, PhD | September 28, 2025
 When Covid hit, governments, health agencies and the media marched in lockstep. Their united front was sold as “consensus.”
When Covid hit, governments, health agencies and the media marched in lockstep. Their united front was sold as “consensus.”
In reality, it was compliance by coercion. Dissenters were punished, questions suppressed, and the public was fed slogans instead of science.
Covid Through Our Eyes tears away that façade.
This collection of essays—written by doctors, scientists, lawyers, journalists, economists and ordinary Australians whose lives were upended—restores the voices silenced during the pandemic.
Each chapter forms part of a collective testimony. And in a final act of principle, not a cent of the book’s sales goes to the authors; all proceeds support Australia’s vaccine injury class action.
A chorus of voices
Editors Robert Clancy, an immunologist, and Melissa McCann, a physician, have gathered an extraordinary range of perspectives.
Among them, British oncologist Angus Dalgleish describes patients relapsing into aggressive cancers after years in remission. He argues that repeated boosters and chronic spike protein exposure created a “pro-cancer milieu.”
Vaccinologist Nikolai Petrovsky recounts how his homegrown vaccine, built on decades of expertise, was cast aside in favour of untested mRNA technology.
Statistician Andrew Madry lays out devastating evidence of excess mortality and the government’s refusal to investigate the causes.
Other contributors highlight phenomena dismissed at the time: immune system imprinting, shifts in antibody subclasses, and persistence of mRNA in the body.
Regulatory expert Philip Altman details how the Therapeutic Goods Administration ignored clear safety signals, choosing convenience over caution.
Lawyers and doctors tell of their battles in the courts and on the streets against vaccine mandates—small victories, bitter defeats, and governments that seemed more determined to silence critics than to defend their policies with evidence.
Clancy himself turns a sharp eye on Australia. Once a nation of independent scientists—from Burnet to Fenner, with pandemic plans crafted at the Commonwealth Serum Laboratories—by 2020 it had surrendered to bureaucracy.
He argues that recovery depends on restoring the doctor–patient relationship and returning vaccine development to proven antigen platforms, not experimental technologies rushed to market.
The media that failed
My own chapter in the book examines how mainstream media collapsed.
Newsrooms abandoned their adversarial role and parroted government lines. Contradictory evidence was buried. Scientists who asked questions were branded fringe. Patients who reported harm were cast as public health risks.
The press did not simply fail; it became an enforcer. That betrayal corroded trust, and the damage persists today.
Stories of loss
The most haunting chapters are personal.
Antonio DeRose, left in a wheelchair after transverse myelitis, describes doctors who refused to acknowledge the cause.
Queenslander Caitlin Gotze died six weeks after her second Pfizer dose, with her myocarditis misdiagnosed as asthma.
Actor and writer Katie Lees collapsed from clotting linked to AstraZeneca; her death was reduced to a single line on a regulator’s website.
These are stories of grief, stark reminders of what happens when agencies, designed to protect, instead deny responsibility.
This book matters
Covid may have slipped from the headlines, but its consequences have not.
Excess deaths remain unexplained. Injured families still fight for recognition. Trust has been squandered. And this nation has yet to hold a Royal Commission into Covid.
Covid Through Our Eyes is essential reading for anyone who wants to understand what really happened to Australians—a nation of people once known for their laid-back spirit, now grappling with a legacy of coercion and injury.
Buy it, read it, and judge for yourself.
AN INCONVENIENT STUDY: THE PUSHBACK
The HighWire with Del Bigtree | September 25, 2025
Del confronts legal pushback from Henry Ford Medical over the upcoming film “An Inconvenient Study,” which highlights what we believe is a significant study showing health outcomes between vaccinated and unvaccinated children. Watch to see the new trailer, highlighting hidden camera footage from the study’s lead author.
Media’s psyop against climate scientists
By Vijay Jayaraj | American Thinker | September 23, 2025
A coordinated offensive unfolded with precision September 2 against five scientists questioning the popular media’s most sacred bogeyman — the hypothesis that human-induced emissions of carbon dioxide threaten to overheat the planet.
The scientists attacked had written a report published in July by the U.S. Department of Energy (DoE), “A Critical Review of Impacts of Greenhouse Gas Emissions on the U.S. Climate.”
Delivering virtually identical narratives, proclaiming that 85 “climate experts” had discredited the DoE report, were CBS, NPR, ABC, CNN, The New York Times, Los Angeles Times, Reuters and others.
Language in the news reporting was nearly indistinguishable, and the focus identical: a number (“85” or “dozens”), a designated group (“scientists” or “experts”) and a verdict (“flawed,” “lacks merit,” “full of errors”). This is not the natural variance of independent newsrooms pursuing a story. This is the result of a shared press release, a common source or a backroom agreement to push a common storyline.
It was a master class in singing the same tune that would make any propaganda ministry proud — a calibrated flash mob of climate-fear messaging in an explicitly partisan tone.
Fooling the Public
The first volley of the assault was a classic ad hominem attack. The authors of the DoE report, five of the world’s most distinguished and academically rigorous researchers of climate issues, were immediately branded as the “Trump Team.”
This is a deliberately dishonest tactic. The authors — doctors John Christy, Judith Curry, Steven Koonin, Ross McKitrick, and Roy Spencer — are not political operatives. They are scientists with decades of experience and hundreds of peer-reviewed publications.
Dr. Koonin served as Undersecretary for Science in the Department of Energy under President Obama, a fact conveniently omitted from most of the media’s hit pieces. Drs. Christy and Spencer are world-renowned for developing the first global temperature dataset from satellites, for which they received NASA’s Medal for Exceptional Scientific Achievement.
No mention that Ross McKitrick is a Canadian academic with no political ties. No mention that Judith Curry stepped away from academia partly because of the politicization of climate research and previously had been much sought after for her research into hurricane intensity.
Most critically, the authors themselves have stated that there was no oversight or compulsion from anyone in any government department during the creation of their report. They say they crafted the report independently, with no interference from Energy Secretary Chris Wright. But the media gloss over that. Instead, the scientists are derided as the “Trump team.”
In stark contrast to the vilified DoE authors, the 85 individuals who signed the critical letter were anointed as “climate experts” and “leading scientists.” Yet, the list of signers is padded with individuals whose specializations are, to put it generously, tangential to the core issues of climate science.
The strategy is clear: assemble a gaggle of academics, label them “climate experts” and use the sheer number to create an illusion of overwhelming scientific consensus against the DOE report.
Sell Lies, Instill Fear With a ‘Black Mirror’
Adding to the theater, the National Academies of Sciences, Engineering, and Medicine (NASEM) has announced a panel to review the DoE report. But here’s the twist: The panel is headed not by a climate scientist, but by a biologist. Out of the panel’s members, only a few have direct expertise in atmospheric science. Yet the announcement was trumpeted as if the nation’s top climate experts were mobilized.
Predicting catastrophe is a media business model. NPR warned of “irreversible” sea-level rise in 2023, ignoring tide gauge records that show no acceleration beyond historical norms. News outlets regularly report on “unprecedented” floods, yet data indicate no uptick in floods due to climate change.
If everybody believed climate impacts were manageable, the case for sweeping carbon taxes, bans on fossil fuels and subsidies for wind and solar energy would collapse. That’s why the DoE report — noting forecasting uncertainty, adaptation possibilities and economic trade-offs — is so threatening. It undermines a narrative of an “existential” threat or imminent collapse. So, the media did not debate the five scientists; they sought to destroy them and their report. Not with data, but with labels.
This is a psyops initiative like that depicted in the Netflix dystopian series “Black Mirror.” The media outlets are not mirrors reflecting reality; they are black screens projecting a manufactured one. They have become instruments of a political agenda, sacrificing journalistic integrity to enforce a specific viewpoint on climate change. They operate not as individual watchdogs but as a wolf pack. They decide what you should think and seek to broadcast it in unison until you do.
I’d encourage you to read the DoE report for yourself or at least countervailing opinions of it. Scrutinize the credentials of those who attack it. Ask the hard questions that the journalists refuse to. The black mirror can only hold power over you if you consent to stare into it. It is time to look away and see the world as it is, not as they tell you it is.
Vijay Jayaraj is a Science and Research Associate at the CO2 Coalition, Fairfax, Virginia. He holds an M.S. in environmental sciences from the University of East Anglia and a postgraduate degree in energy management from Robert Gordon University, both in the U.K., and a bachelor’s in engineering from Anna University, India.
Will Vaccines Prevent 1.1 million Deaths? No.
More CDC junk science
Injecting Freedom by Aaron Siri | September 18, 2025
At my recent Senate hearing, the minority witness submitted testimony claiming that “The CDC estimates that vaccines given to children born between 1994 and 2018 will prevent … 936,000 deaths over their lifetimes.” That claim has also been levied against Secretary Kennedy. Here is why it is a junk claim. (Note that portions of this response are taken directly from my new book Vaccines, Amen.)
Newsletter + Selection Bias
First, this claim is an updated version of a 2014 MMWR report. MMWR is essentially CDC’s newsletter. CDC’s own guidelines for the MMWR only permit publishing articles that align with CDC policy, which results in the worst form of selection bias. As explained by the CDC’s policies for publishing an MMWR report: “By the time a report appears in MMWR, it reflects, or is consistent with, CDC policy.” Hence, this article would only be published until it was massaged to assure that it aligned with the CDC’s policy that vaccines are safe and effective. That approach is not science — it is the perversion of science.
No Confidence Intervals
Second, like the WHO advertising report I discussed yesterday, this is an “advertising report” for CDC’s immunization program and has no confidence intervals for its estimates. This is because they are just unreliable guesswork. The true rate could be that the vaccines caused 2 million deaths between in the United States from 1994 to 2023 because the report provides no bounds for its claims. Again, absent bounds for its claims, it could be equally true that vaccines resulted in causing 2 million extra deaths instead of a net saving in lives.
Ignores All Confounders
Third, it’s even worse, because the 2023 report explains that “factors other than immunization (e.g., hygiene…) might have contributed to lower disease risks in recent decades, and reductions resulting from these contributions have not been incorporated into the model” (emphasis added). Meaning, it did not account for any other advancement or factor that may have improved health outcomes. Nothing. This alone renders this CDC promotion “study” junk science. It is also why it has no bounds for its estimates because it cannot calculate them with any confidence.
The Hard Data Shows The 1.1 Million Claim Is Nonsense
Finally, just a simple review of the data shows how preposterous the numbers are. While it claims vaccines saved 1.1 million lives between 1994 and 2023, it takes only looking at the actual real-world data to see this figure is nonsense. Let’s look at three diseases the report claims account for almost the entire 1.1. million lives purportedly saved: diphtheria, hepatitis B, and measles.
Diphtheria
Around 750,000 of the 1.1. million lives (over 68%) that CDC claims were prevented are from diphtheria. That means that it claims 25,000 lives were saved per year by this vaccine. That figure is nonsensical. Here is why.
The first vaccine for diphtheria was introduced in 1926. Between 1900 and 1926, as the population rose, the death rate from this disease had already declined 81%, from 40.3 to 7.8 deaths per 100,000 individuals. A vaccine had nothing to do with this sharp decline since no vaccine of any kind for diphtheria existed until 1926. The further decline from 1926 until at least the mid-1940s also had little or nothing to do with the vaccine because it was rarely, if ever, used outside of certain demographics in major cities, and diphtheria mortality declined at a similar rate in areas with or without its use.[1]
Below is an official government chart reflecting same. So, even as the population increased, the data clearly shows an 81% mortality decline from 1900 to 1926, a 97.3% decline from 1900 to 1940, and a 97.8% decline from 1900 to 1948; hence, no matter how you look at it, vaccination had little to do with almost all of the decline in mortality from diphtheria in the last century:[2]

Finally, in 1949, DTP was first licensed, and coverage of this vaccine began to improve. The year prior, in 1948, there was a total of 634 deaths from diphtheria. Yet, this MMRW report nonsensically claims the diphtheria vaccine is now saving 25,000 lives a year in the United States. (Also note that in 1985, the coverage for only three doses, let alone the six recommended today, was still only 63.6%.)
This claim becomes more absurd when you consider that even after six childhood doses, adults require a booster dose every ten years in adulthood, and about 40% of adults skip these boosters. Despite a large portion of adults not receiving boosters, the last case of respiratory diphtheria in the United States was nearly three decades ago. This almost certainly reflects the extensive literature which supports that any harmful effects by the diphtheria toxin are counteracted by iron, vitamin C, and vitamin B3, and deficiencies of these vitamins and minerals have mostly been eliminated in developed countries.
There are diseases that had a high mortality in the United States that disappeared without a vaccine. For many of these diseases, researchers sought to develop a vaccine but failed. For example, scarlet fever was one of the deadliest infectious diseases for children in 1900, with a death rate of 9.6 deaths per 100,000 children. Researchers furiously sought to develop a vaccine but repeatedly failed. By the 1950s, deaths from scarlet fever had significantly declined and by the late 1900s, deaths from scarlet fever were essentially non-existent.
Had a vaccine for scarlet fever been developed in the 1920s, 40s, or 60s, that vaccine would almost certainly still be on the childhood schedule today, and its use would be considered essential for controlling scarlet fever; undoubtedly, this same CDC advertising article would be estimating that its use is now saving hundreds of thousands of lives in the United States.
In fact, scarlet fever and diphtheria are similar in that each is caused by a bacterium that releases a potentially harmful toxin when the bacterium has been “infected” by a certain virus. Both diseases cause sore throats, and many doctors, without a lab test, will confuse diphtheria with scarlet fever, and vice versa. These two diseases also have something else in common: both declined at nearly the same rate beginning in 1900. The primary reason why public health officials and the medical community behave differently with regard to these two diseases is that a vaccine was developed for diphtheria, but not for scarlet fever. If a vaccine for diphtheria had not emerged, this disease would have likely gone the way of scarlet fever and other childhood diseases that effectively disappeared without a vaccine.
Even if it would not have disappeared on its own, the article’s claim that 750,000 lives have been saved from diphtheria between 1994 and 2023 is absurd given the failure to account for the actual mortality data, other factors that reduced morality from diphtheria, the lack of any bounds to its claim, the lack of population-wide immunity and disappearance of the disease anyway, and the objective big picture reality regarding this disease; it truly requires a true religious fervor that suspends all reason and thinking to conclude that this vaccine has saved 25,000 lives per year between 1994 and 2023. The reality, based on the real-world data, is likely far closer to what occurred with scarlet fever absent vaccination.
Hepatitis B
As another example, the CDC advertisement article claims Hep B vaccines saved over 90,000 lives from 1994 to 2023, amounting to over 3,000 lives purportedly saved per year. This claim again defies data and reason. By way of background, the first Hep B vaccine was introduced in 1981 and was made with human blood plasma from donors who were chronically infected with the Hep B virus; and in 1986, a new Hep B vaccine using recombinant DNA technology without human blood was licensed. With that background, the mortality from Hep B climbed after introduction of the 1981 vaccine, continued to climb after the introduction of the 1986 vaccine, and has never returned to pre-vaccination levels. In 1980, there were 294 deaths in the United States from Hep B. Today, there are around 1,700 deaths per year. Yet, somehow, CDC claims that Hep B vaccine has saved over 3,000 lives per year between 1994 and 2023. It defies reason.
Measles
As a final example, CDC’s advertising article claims measles vaccine saved 85,000 lives from 1994 to 2023, amounting to over 2,700 lives purportedly saved per year. This claim again defies data. The first measles vaccine came on the market in 1963. In the years leading up to the first measles vaccine in 1963, the CDC data reflects around 400 deaths from measles each year. There were also around 4.2 million births each year in the late 1950s and early 1960s, whereas there was around 3.8 million births each year between 1994 and 2023. Yet, somehow, despite improvements in standards of living, medical care, etc., and despite smaller cohorts of infants and children to infect, this model makes the data-defying claim that mortality went from around 400 deaths per year from measles pre-vaccine to over 2,700 deaths per year.
But it gets far worse for the CDC advertisement’s claim because the following U.S. government chart shows the decline in the measles death rate by over 98% from 1900 to 1960, three years before the first measles vaccine was introduced in the United States in 1963. Meaning, the measles vaccine had nothing to do with the over 98% reduction in the death rate from measles in the United States from 1900 to 1960.
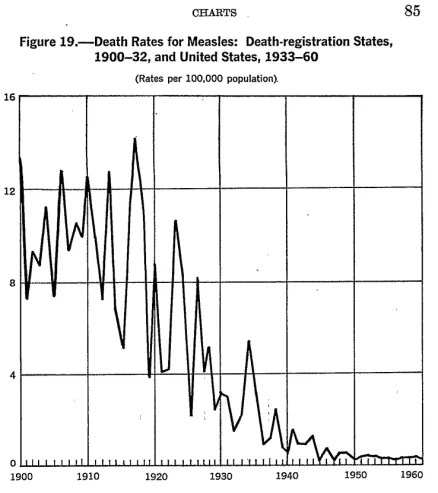
Taking a closer look, the CDC data reflects that in 1900, the rate of mortality from measles was 13.3 deaths per 100,000 individuals. By 1960, it was 0.2 deaths per 100,000 individuals. The same was true for 1961 and 1962. And as noted above, a similar decline of over 99% in measles deaths occurred between 1900 and 1967 in England and Wales, and it was only after that decline that the first measles vaccine was introduced there in 1968—five years after its introduction in the United States.
Hence, the same factors that caused measles mortality to decline by over 98% from 1900 to 1962 would, absent the vaccine interrupting the ecology of measles, likely have continued to cause a further reduction in the measles mortality rate after 1962. Meaning, at least a portion of the decline in the 400 deaths per year after the vaccine was available is no doubt attributable to the same factors that caused a steady decline in the measles death rate for decades prior to the introduction of the measles vaccine. Therefore, even without the measles vaccine, the death rate would have, no doubt, continued to decline after 1963.
In pockets of the country with poor nutrition, sanitation, and water, deaths from any pathogen, including measles, can occur at a higher rate. Those conditions still existed in some pockets of the United States in the early 1960s. As living conditions in those pockets of America improved with the introduction of clean water, improved sanitation, and better living conditions, deaths from measles declined, which is what typically occurs when these conditions improve. Let’s also not ignore that health care, especially the management and treatment of acute infections, has vastly improved since the 1960s. Doctors readily concede this point, unless you are talking about vaccines.
Yet, CDC claims that measles vaccines would have saved a data defying over 2,800 lives a year from measles in the United States between 1994 and 2023. CDC’s advertisement study, of course, also doesn’t account for the increase in deaths from heart disease and cancer due to the elimination of measles, as discussed in my previous post and reflected by studies that did not engage in estimates.
In sum, this CDC self-promotion article, that is not peer-reviewed and must conform to CDC policy to be published, does not account for any external factors, does not account for actual mortality data related to these diseases, and lacks any confidence intervals because its claims have zero reliability. Anyone citing this study claiming 1.1 million lives were saved is spreading propaganda. Not science.
[1] https://pmc.ncbi.nlm.nih.gov/articles/PMC1997101/pdf/pubhealthreporig01174-0001.pdf (“The simultaneous decline in diphtheria morbidity and mortality rates in all age groups of individual States located in different sections of the country, which began after a cyclic increase in incidence between 1915 and 1925, suggests the operation or influence of other factors besides, or in addition to, artificially induced immunity. Studies such as that included in the 1930 White House Conference on Child Health and Protection indicated that immunization programs were reaching a relatively large proportion of children in some areas or cities and a very low proportion in others as late as 1930. In spite of this wide variation, both morbidity and mortality began to decline rapidly after 1925 in all States simultaneously.”); https://www.cdc.gov/pinkbook/hcp/table-of-contents/chapter-7-diphtheria.html (“[D]iphtheria toxoid-containing vaccines became available in the 1940s” and “universal childhood vaccination program which included diphtheria toxoid-containing vaccines beginning in the late 1940s.”).
[2] The death rate per 100,000 individuals in the United States in 1900, 1940, and 1948 for diphtheria was 40.3, 1.1, and 0.4, respectively, for tetanus it was 2.4, 0.4., and 0.3, respectively, and for pertussis it was 12.2, 2.2, and 0.8, respectively. https://www.cdc.gov/nchs/data/vsus/vsrates1940_60.pdf.
The Pandemic of Fake Psychiatric Diagnoses
By Peter C. Gøtzsche | Brownstone Institute | September 17, 2025
On 12 September, UK child and adolescent psychiatrist Sami Timimi published “When mental-health diagnoses become brands, the real drivers of our psychic pain are hidden” in the Globe and Mail, a Canadian newspaper.
In his superb article, Sami carefully explains how he arrives at his painful conclusion:
You see there is a truth that we (in the mental-health business) hope no one will notice – we literally don’t know what we are talking about when it comes to mental health.
An obvious problem is that all definitions of psychiatric disorders are subjective. They are not objective facts such as a broken bone is. This means they can be expanded in a myriad of ways to capture a kaleidoscope of distress, alienation, and dissatisfaction, and that psychiatric diagnoses are consumer brands, not medical diseases.
In medicine, a diagnosis is aimed at determining which disease explains a person’s symptoms and signs, which enables effective matching of a treatment to address specific disease processes.
This is not the case in psychiatry. And all psychiatric drugs have nonspecific effects that are not directed against some cause of a disease. Their effects are similar to those of alcohol, narcotics, and other brain-active substances.
But, as Sami explains, increasingly, youngsters are getting diagnosed with ADHD, trauma, depression, anxiety, PTSD, autism, and often several such diagnoses. Their conversations may address gender identity, neurodiversity, and “having” a mental health disorder such as ADHD.
The facts are that virtually no one is in doubt about whether they are male or female; neurodiversity is a meaningless concept used by psychiatrists to impress the public about how knowledgeable they are but it just means that all people are not the same; and one cannot “have” ADHD, which is just a name for a subjective description of rather common behaviours and therefore cannot explain anything.
What people should realise is that it is part of being human to have difficulties that can be handled better if we don’t give people psychiatric diagnoses and drugs. Difficulties often have a cause that has nothing to do with being ill, e.g. poverty, trauma, inadequate housing, social injustice, marital problems, discrimination, exclusion, bereavement, unemployment, and financial insecurity. Life is not easy, but if you have difficulty coping with its challenges, you can easily get one or more psychiatric diagnoses.
There is a lot of misinformation that leads people astray, in scientific articles, newspapers, TV, radio, and social media. When youngsters look up descriptions of people who say they “have” ADHD on social media, they may be convinced they “have” it too and may even self-diagnose. There is an element of social contagion in this, and the criteria for ADHD are so vague and ludicrous that when I lecture and ask people to use the adult ADHD test on themselves, it never fails that one quarter to half the audience test positive.
Often, authoritative information is also seriously misleading or even mendacious, which I have documented in my books and articles, most recently in my freely available book, “Is psychiatry a crime against humanity?” and in the freely available article, “The only medical specialty that survives on lies.”
Sami mentions a patient information leaflet on antidepressants produced by a British national mental health service that includes the following advice:
It can sometimes take weeks, months or even years, to get the right medicine at the right dose for you. Think of it as a bit like dating. Some make you feel sick or sleepy; some are great to start with but wear off; others may not be much to start with but after a while grow on you. Then you might have found the one that makes you feel good long-term. So don’t lose hope if the first one doesn’t work.
It is an illusion to think that if you wait long enough and try enough drugs, one will work for you. Most mental health issues become better with time, without any treatment, which is misinterpreted as a drug effect, and research has shown that it doesn’t help to change drugs or increase the dose of drugs (see my freely available “Critical Psychiatry Textbook”).
The illusion that it helps to try several antidepressant drugs comes from the STAR*D trial, a $35 million fraud funded by the US National Institute of Mental Health.
Sami writes that he is impressed by the extraordinary ability of even the most severely afflicted of the young patients he sees to recover functionality and meaning in their lives. His advice to parents with troubled kids is that they should not agree to having their children assessed for ADHD, autistic spectrum disorder, or anxiety (or depression, as depression drugs double suicides). We should be able to talk about how we feel without jumping into panic mode and imagining that what we’re describing could be the onset of some mental disorder. Sami goes on to say that,
As we are launched into a seemingly never-ending search for the right diagnosis and treatment, we start collecting labels and accompanying interventions. Each step in this journey has the potential to make it harder to accept your child (or yourself) just the way they are with all their uniqueness and the mysterious wonderful variety of ways they might thrive in this maddening world. Be patient and categorize psychological problems in the sphere of the ordinary and/or understandable… Our duty as parents (and to each other as adults) is not to prevent our children from experiencing distress (which is impossible), but to be there and take the time and have the patience to be with them and support them when they do.
Beware of concept creep. As what I call the Mental Health Industrial Complex has burrowed its way into day-to-day language and “common sense,” concepts have been popularized that encourage us to view behaviours and experiences in pathological ways. We no longer become sad or miserable, we get depressed… You and your children’s experiences nearly always sit in the realm of the ordinary and/or understandable… Arming yourself with some knowledge to help you avoid the prolific spread of scientism (faith masquerading as science) could save you or your child becoming another number in the growing crowds of those who are deemed to have lifelong and incapacitating mental disorder/illness. These conditions were never meant to be a life sentence.
If all doctors heeded Sami’s advice, fewer people would kill themselves and fewer people would become permanently disabled. But in a world where healthcare is heavily influenced by the drug industry’s corruption of doctors, it is reasonable to ask: Are psychiatrists more mad than their patients? I have responded in the affirmative.
Like me, Sami is a member of the Critical Psychiatry Network based in England. My experience with lecturing for psychiatrists has led me to believe that over 99% of psychiatrists are uncritical towards their practice. Think about it. This is why psychiatric drugs are the third leading cause of death and why psychiatry as a profession does far more harm than good.
Don’t our kids and friends deserve better than this?
Dr. Peter Gøtzsche co-founded the Cochrane Collaboration, once considered the world’s preeminent independent medical research organization. In 2010 Gøtzsche was named Professor of Clinical Research Design and Analysis at the University of Copenhagen. Gøtzsche has published more than 97 over 100 papers in the “big five” medical journals (JAMA, Lancet, New England Journal of Medicine, British Medical Journal, and Annals of Internal Medicine). Gøtzsche has also authored books on medical issues including Deadly Medicines and Organized Crime.
‘Shut out’: Journal fires editor after publishing research refuting ‘warming climate’
By Gabriel Zylstra – The College Fix – September 17, 2025
The American Journal of Economics and Sociology recently removed special editor Marty Rowland from his position for publishing a paper refuting climate change argument about carbon dioxide, according to the paper’s authors.
“The standard response of the mainstream climate science community these days to papers that somewhat challenge the CO2-is-dangerous-narrative is to immediately ask for retraction,” Marcel Crok, a co-author of the paper and director of the climate science group Clintel, told The College Fix.
“It’s a strategy because it gives the signal that the paper is really bad and most people don’t have the time and knowledge to assess the situation,” Crok said in an email Tuesday.
The paper in question, “Carbon dioxide and a warming climate are not problems,” was published in the journal in May 2024. Crok co-authored it with Andy May, a retired petrophysicist and developmental geologist who worked for Exxon and other oil and energy companies.
Rowland, a lecturer at the Henry George School of Science and environmental engineer, was the editor at the journal who approved it.
According to May’s blog, the journal fired Rowland in August, and the reason it gave was “his publication of our paper.”
An archived version of the journal editorial board webpage shows Rowland was the special editions editor at least since 2023. The current page no longer lists him as an editor.
The Fix reached out to the editorial team at the American Journal of Economics and Sociology several times by email over the past two weeks to ask about the reason for Rowland’s departure. None responded.
Since being published, the paper has been cited 25 times according to google scholar, and scientists David Wojick, Kenneth Richard, and H. Sterling Burnett gave positive reviews, according to May’s blog.
“In short there was no legitimate reason to fire Dr. Rowland for publishing our fully peer-reviewed, and well received, paper,” May wrote.
May told The Fix via email this week that the paper was peer-reviewed prior to publication.
“The two scientists that liked the paper, both are very famous scientists with decades of climate science publications and well over 16,000 citations between them, had many suggestions and I made all their suggested changes to the paper and the changes improved the paper a lot,” May said.
“Post-publication, the response was mostly favorable, but there was a lot of published criticism,” he told The Fix. “But, these critical responses to our paper are swamped by the favorable critiques. The paper is very popular and in the top 0.1% of all papers followed by Wiley… It is also the #2 paper published in AJES.”
Crok told The Fix that others responded to its publication with calls for retraction.
However, May said none of the critics “identified any errors” in their article, which is why it hasn’t been retracted.
The publisher, Wiley, “disagreed with our conclusions and wanted to censor our paper, thankfully the board did not do that, but they did fire Marty, which was a very bad move” May told The Fix.
May told The Fix, “The pressures are huge. Basically, if a climate researcher does not toe the ‘consensus’ line he will receive no funding for his work and will be ostracized. He or she is then often forced to resign or fired.”
Crok agreed, saying scientists whose research does not fit the predominant climate change narrative often are unfairly maligned.
These include Dutch scientist Hessel Voortman, “who published a paper in 2023 about sea level rise along the Dutch coast (showing no acceleration), which led to a group of Dutch scientists asking for retraction,” Crok said.
Clintel, Crok’s foundation based in the Netherlands, focuses on climate education and policies from the standpoint that climate science should be less political. In 2023, Clintel organized a petition of more than 1,600 scientists world-wide, including Nobel Laureates, that argues there is no climate change crisis.
Meanwhile, environmental policy expert H. Sterling Burnett expressed similar concerns about Rowland’s firing when contacted by The College Fix.
“Unfortunately, I’m not surprised at all by the American Journal of Economics and Sociology (AJES) firing of Dr. Rowland,” Burnett said. He is the director of the Arthur B. Robinson Center on Climate and Environmental Policy at The Heartland Institute.
“If anything, I’m surprised at how brave he was in publishing the study,” he said.
Burnett said the field of climate research is heavily censored and not open to dispute. “No one should suffer for their belief in open inquiry that is at the heart of the scientific endeavor, but in the field of climate science, far too many academics do.”
According to Burnett, academics are commonly ostracized or fired “for daring to raise perfectly legitimate questions about the causes and consequences of climate change, and about the policies proposed by the ‘settled science’ community as a response to climate change.”
Burnett said climate research was relatively open to dissenting views up until about 20 years ago when “influential climate alarmists moved to shut down continued debate and discussion about the causes and consequences of climate change, by having open minded journal editors removed from their positions or reined in by journal publishers.”
“[C]limate skeptics were increasingly shut out of the peer review process, and papers openly skeptical of the anthropogenic climate disaster narrative found it nearly impossible to get published in top journals,” he said.
Burnett told The Fix that politicians and media also contributed to disenfranchising so-called “climate deniers” under the guise of protecting scientific consensus.
When asked about claims of consensus to justify scientific censorship, he responded, “Consensus is a political term, not a scientific one and should have no legitimate place in scientific discovery. ” He said that science “is a method, a way of explaining phenomena and discovering facts, not a conclusion set in stone for all time.”
Burnett expressed hope that things are starting to change for the better following the publication of a recent report by the U.S. Department of Energy that pushes back on “climate alarmists.”
The report “is forcing alarmists to address, rather than dismiss out of hand because the ‘science is settled,’ realists long-standing questions, concerns, and critiques of the argument that humans are causing dangerous climate change,” he said.
Crok also mentioned the DOE report in his interview with The Fix, noting that the authors are now facing “severe,” negative pressure for their work.
“This battle will go on, they will try to get the report retracted as well,” Crok said. “This is a worrisome trend in which the mainstream instead of engaging with skeptical scientists simply try to get skeptical papers removed immediately.”
Former CDC Officials Take Aim at RFK Jr. During Senate Hearing
By Suzanne Burdick, Ph.D. | The Defender | September 17, 2025
The U.S. Senate hearing that began today as an investigation into the firing of the CDC director and the resignations of other key agency officials morphed quickly into a forum for accusing U.S. Health Secretary Robert F. Kennedy Jr. of posing a threat to public health.
“Today should not be about me,” former director of the Centers for Disease Control and Prevention (CDC), Susan Monarez, Ph.D., told senators. “Today should be about the future of trust in public health.”
Monarez testified that she was fired for “holding the line of scientific integrity.” Dr. Debra Houry, former chief medical officer of the CDC who resigned after Monarez’s firing, also testified.
“Trust and transparency have been broken” under Kennedy’s leadership, Houry told members of the Committee on Health, Education, Labor and Pensions (HELP), which held the hearing.
She criticized Kennedy’s handling of the recent measles outbreak and the changes to COVID-19 vaccine recommendations.
The committee will hold another hearing in the future to allow Kennedy and current CDC officials to refute allegations made by Monarez and Houry, said Sen. Bill Cassidy (R-La.), the committee chair. “I want President Trump to have the best CDC in our nation’s history,” he said.
According to Sen. Bernie Sanders (I-Vt.), minority chair, the hearing was really about Kennedy’s “dangerous war on science, public health and the truth itself.”
Sanders praised Monarez for standing up for the “scientific method” and refusing to “rubber-stamp” Kennedy’s “dangerous agenda.”
Monarez testified that “vaccines are not controversial because they work.”
She also recounted how the CDC was attacked by a gunman who, in her words, was “driven by vaccine distrust.”
Sen. Roger Marshall (R-Kan.) called out the agency for creating public distrust during the COVID-19 pandemic. “The CDC is the cause of vaccine hesitancy,” he said.
Sanders refuses to have Monarez, Houry sworn in
The hearing came as no surprise. The day Monarez was fired, Cassidy posted on X that the sudden departure of top CDC officials “will require oversight” by the committee.
Cassidy wanted Monarez and Houry to be sworn in before their testimony. However, Sanders — whose approval was needed as minority leader — refused, saying Kennedy wasn’t sworn in at a prior hearing.
When another senator challenged Sanders’ refusal, Cassidy pointed out that Kennedy would be sworn in for future hearings related to today’s testimony.
Sanders still refused.
Cassidy reminded the witnesses that it’s illegal to lie to senators, even without explicitly vowing to tell the truth. Yet throughout the hearing, several senators questioned whether Monarez and Houry were being honest.
A U.S. Department of Health and Human Services (HHS) spokesperson told The Defender that Monarez’s prepared remarks contain “factual inaccuracies and leave out important details,” adding:
“Here’s the reality: Susan Monarez was tasked with returning the CDC to its core mission after decades of bureaucratic inertia, politicized science and mission creep corroded its purpose and squandered public trust.
“Instead, she acted maliciously to undermine the President’s agenda and was fired as a result. Some of her biggest offenses include neglecting to implement President Trump’s executive orders, making policy decisions without the knowledge or consent of Secretary Kennedy or the White House, limiting badge access for Trump’s political appointees, and removing a Secretarial appointee without consulting anyone. When she refused to acknowledge her insubordination, President Trump fired her.”
Children’s Health Defense CEO Mary Holland said Monarez represented the CDC’s “old guard” and that her termination was “necessary and proper.” She said:
“Monarez is assiduously following the pharma-funded script to attempt to oust Kennedy as HHS Secretary. Yet the obvious reality is that the CDC has lost the trust of the nation and the world, and radical reform is absolutely required if the agency is to continue at all.”
Senators, Monarez dispute details surrounding her firing
Senators at the hearing attempted to clarify disputed details surrounding Monarez’s firing.
The White House confirmed on Aug. 27 that she was fired after Kennedy tried to force her resignation and she refused to leave. Shortly after, Monarez wrote in an op-ed in The Wall Street Journal that she was fired because she “held the line and insisted on rigorous scientific review.”
She reiterated the claim in today’s hearing, saying Kennedy had given her a choice: accept the recommendations of the new Advisory Committee on Immunization Practices and fire top CDC officials responsible for vaccine policy, or resign.
According to Kennedy, he fired her because she responded “no” when he asked her, “Are you a trustworthy person?”
Monarez said the conversation went differently. “He told me he couldn’t trust me,” she said. “I told him that if he could not trust me, he could fire me.”
Sen. Markwayne Mullin (R-Okla.) pressed Monarez on details of the conversation, saying it had been recorded. However, he reportedly backtracked on the claim. “If HHS has a recording, I ask them to release it,” Cassidy said.
Cassidy also asked for all documentation related to the conversation for the committee to review.
Houry testified that she resigned because Kennedy “censored CDC science, politicized its processes and stripped leaders of independence.”
Andrew G. Nixon, an HHS spokesman, told The New York Times that Kennedy “has insisted that decisions be evidence-based, open to scrutiny and free from the kind of closed-door processes that undermined confidence in the C.D.C. during the pandemic.”
Monarez evasive on COVID and Hep B vaccines
Sen. Rand Paul (R-Ky.) asked Monarez if the COVID-19 vaccine prevented transmission or reduced children’s risk of hospitalization or death.
She replied, “It can.”
Paul cited research contradicting Monarez’s answer. He pointed out that children who get the COVID-19 shot face a heightened risk of myocarditis, and the shot fails to lower their risk of hospitalization or death.
James Lyons-Weiler, Ph.D., criticized Monarez in a Substack post, saying she was unable to provide substantive answers to Paul’s questions.
Lyons-Weiler also noted that Monarez offered “no credible defense” when Paul asked why it was important for newborns to get the hepatitis B vaccine if their mother was hepatitis B negative.
The CDC’s vaccine advisory panel is expected to vote Thursday on certain childhood vaccine recommendations, including the hepatitis B (Hep B) vaccine.
Critics have long raised concerns about the safety and necessity of giving the vaccine to newborns, particularly those not at risk for the disease. Today, the Hep B vaccine contains at least 250 micrograms of aluminum, and aluminum exposure has been linked to autism.
Paul asked Monarez, “What is the medical, scientific reason and proof for giving a newborn a hepatitis B vaccine if the mom is Hep B negative?”
Monarez refused to answer the question.
Paul called out Monarez for evading questions about specific vaccines and hiding behind vague assertions that all vaccines are “safe and effective.”
He said the burden should be on the CDC and its staff to prove that the benefits of giving babies COVID-19 and Hep B vaccines outweigh the risks. “That’s what the debate ought to be about,” he said. “Not on whether all vaccines are good.”
Monarez repeatedly said that the CDC doesn’t “mandate” vaccines; the agency only makes “recommendations.”
While technically correct, her answer overlooks the reality that many states use the agency’s recommendations when mandating vaccines for school entry.
Monarez was first CDC director in 70 years without medical degree
In March, Trump nominated Monarez for director of the CDC, where she had served as acting director until her nomination.
She was the first CDC director confirmed under a law passed in 2023 that requires Senate confirmation for the position. She was also the first person, in more than 70 years, without a medical degree to serve in the role. She has a doctorate in microbiology and immunology.
Trump nominated Monarez after withdrawing the nomination of Dr. Dave Weldon, who reportedly failed to secure enough votes because of comments he made suggesting a possible link between autism and vaccines.
Monarez, a biosecurity veteran, was previously deputy director of the Advanced Research Projects Agency for Health (ARPA-H), an agency within HHS created by the Biden administration to accelerate “high-risk, high-reward” biomedical research.
ARPA-H is modeled after the U.S. military’s Defense Advanced Research Projects Agency or DARPA. Monarez also previously held positions with the U.S. Department of Homeland Security and in the White House Office of Science and Technology Policy.
During her confirmation hearing before the Senate committee, Monarez affirmed her belief that “vaccines save lives,” and pledged to prioritize vaccine availability. She said mRNA vaccines are “safe and with demonstrated efficacy,” and she said she was unaware of any confirmed scientific link between vaccines and autism.
In her WSJ op-ed about why she was fired, Monarez said:
“Those seeking to undermine vaccines use a familiar playbook: discredit research, weaken advisory committees, and use manipulated outcomes to unravel protections that generations of families have relied on to keep deadly diseases at bay.”
Mark Crispin Miller, Ph.D., professor of media studies at New York University, told The Defender that Monarez is playing an old trick called “accusation in the mirror,” in which a person accuses their enemy of doing what the person has been doing.
He said:
“The trick usually works because it’s so disorienting, and most people have a hard time believing that anybody as ‘respectable’ as Susan Monarez — a woman with a Ph.D., who worked at CDC — could be so utterly dishonest. The only way to fight it is to call it out immediately, loud and clear.”
Watch the hearing here.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Fugitive Scientist Behind Vaccine and Autism Studies Arrested for Stealing $1 Million From CDC
By Brenda Baletti, Ph.D. | The Defender |September 16, 2025
Danish scientist Poul Thorsen, who co-authored influential papers in 2002 and 2003, used to argue against the link between vaccines and autism, was arrested in Germany and may be extradited to the U.S. on charges of stealing nearly $1 million in research money, Breitbart News reported.
Thorsen was listed as a fugitive on the U.S. Office of the Inspector General’s most wanted list for over a decade.
He reportedly was arrested in June following an Interpol Red Notice, a request to international law enforcement to locate and provisionally arrest a wanted person. The U.S. Department of Justice (DOJ) is working with German authorities to extradite him to the U.S., an unnamed DOJ official told Breitbart.
Thorsen allegedly absconded with over $1 million from the Centers for Disease Control and Prevention (CDC) as part of a scheme to steal grant money awarded to governmental agencies in Denmark for autism research.
A federal grand jury indicted Thorsen in Atlanta in 2011 on 22 counts of wire fraud and money laundering. However, Denmark previously refused to extradite him, so he wasn’t prosecuted, Forbes reported.
‘Number one’ on the HHS most wanted list
Thorsen’s research, allegedly “debunking” the link between autism and the measles-mumps-rubella or MMR vaccine and other thimerosal-containing vaccines, was cited by the Institute of Medicine (IOM) as proof of no link.
His research was also used as evidence in the National Vaccine Injury Compensation Program’s (VICP) proceedings to deny the injury claims of more than 5,000 families.
Thorsen’s findings have been widely criticized by safe vaccine advocates as seriously flawed and potentially fraudulent.
“Thorsen has been number one on the Health and Human Services (HHS) most wanted list for the past 10 years,” HHS Secretary Robert F. Kennedy Jr., a long-time critic of Thorsen’s studies, told Breitbart following reports of Thorsen’s arrest.
HHS did not respond to The Defender’s request to confirm whether Thorsen had been detained.
Author James Grundvig told The Defender that Thorsen’s arrest has the potential to expose a long history of misconduct within the CDC.
Grundvig wrote “Master Manipulator: The Explosive True Story of Fraud, Embezzlement, and Government Betrayal at the CDC,” which details the story of Thorsen’s alleged role in a broader CDC manipulation of vaccine safety studies.
“It is not just Thorsen,” Grundvig said. “It won’t be just taking down one guy.” If Thorsen is compelled to testify, “he will be pointing fingers and naming names.”
Children’s Health Defense Chief Scientific Officer Brian Hooker said:
“I really want to emphasize that this crime is much bigger than Thorsen. His collaborators need to be brought to justice as well. They partied on the backs of many autistic children. Frankly, jail time is too good for Thorsen and the many other fraudsters at CDC, IOM and the VICP!”
Thorsen used grant money to buy home, motorcycle, cars
Beginning in the 1990s, Thorsen, who worked as a visiting scientist at the CDC when the agency was soliciting grant applications for research about infant disabilities, advocated for grants on behalf of Danish scientists and institutions.
Between 2000 and 2009, the CDC awarded over $11 million to two Danish government agencies to study the relationship between vaccines and autism, and other infant developmental issues, according to a 2011 press release by the U.S. Attorney’s Office for the Northern District of Georgia and Grundvig’s book.
In 2002, Thorsen relocated to Denmark to serve as principal investigator on the grant, overseeing the distribution of research money. The research was done by Aarhus University and Odense University Hospital in Denmark.
Between 2004 and 2008, Thorsen allegedly submitted more than a dozen fraudulent invoices on CDC letterhead to the medical facilities conducting the research for costs incurred for work related to the grant.
The facilities transferred hundreds of thousands of dollars in payments to fake CDC accounts at the CDC Federal Credit Union in Atlanta. However, the money actually was deposited into Thorsen’s personal accounts.
Thorsen allegedly used the money to purchase a home in Atlanta, a Harley Davidson motorcycle and cars, among other items. Overall, he withdrew more than $1 million, according to reports.
The indictment charged Thorsen with 13 counts of wire fraud and nine counts of money laundering, each carrying potentially long prison sentences and heavy fines. It also sought forfeiture of all property purchased with the fraudulently obtained funds.
Fabricated results seem ‘all but certain’ in research involving Thorsen
Mainstream media writers have mocked the long-term critiques of Thorsen’s work as “conspiracy theories,” and argued that, as a co-author, his contributions to the papers didn’t skew the results.
In a Substack post detailing Thorsen’s history and the studies he co-authored, scientist James Lyons-Weiler, Ph.D., said Thorsen’s influence on the research was concerning and the studies themselves were flawed.
He said:
“Although his scientific findings must be evaluated on their own merits, including data sources, design, and replicability, his case may be critical in revealing decision-making and could produce evidence of wrong-doing by Thorsen and others. Defrauding the US Government of research dollars is a crime. (This includes misuse and scientific fraud).
“Results fabrication in the Danish registry results seems all but certain given the clear evidence of those practices in other studies on the topic of vaccines and autism.”
The Danish government, since 1968, has maintained an extensive registry of birth and health records on all of its citizens. This provided a rich database for research on childhood disabilities, Grundvig said.
According to Lyons-Weiler, the Danish registry studies published by Thorsen and others were riddled with methodological flaws, including vulnerability to confounding variables over time, shifting diagnostic categories that distorted the data, misclassification and reporting biases and conflicts of interest.
Lyons-Weiler called for greater transparency in that research, including access to the original datasets, registries, study methods and peer review processes.
He said the studies should be replicated, the policies derived from them should be reexamined, and the public should be provided clarity on which studies Thorsen influenced.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Is It Safe to Get 3 Vaccines at Once? Vaccine Makers Say Yes, But FDA Wants Proof
By Michael Nevradakis, Ph.D. | The Defender | September 8, 2025
Is it safe to get a COVID-19, RSV and flu vaccine at the same time? The answer is yes, according to many medical experts and the CDC and HHS websites — but that’s about to change.
According to an Aug. 25 memo, the U.S. Food and Drug Administration (FDA) now says vaccine makers must conduct clinical trials to study the potential adverse effects of simultaneously giving multiple shots for respiratory viruses before they can market the vaccines as “safe and effective” when received at the same time.
The FDA said it “cannot affirm that concurrent administration is both safe and effective,” as coadministration has not been thoroughly studied.
Some medical and scientific experts welcomed the new policy, first reported last week by The Washington Post.
Dr. Clayton J. Baker, an internal medicine physician, said:
“There is urgent need for scientifically sound, non-Pharma-conducted studies regarding the safety of all simultaneously administered vaccines.
“This practice is widely used and dangerously under-evaluated. The greatest risk is to young children during co-administration of the many different vaccines listed on the current, bloated Centers for Disease Control and Prevention [CDC] pediatric schedule.”
Last month, two doctors who lost their medical licenses because they questioned the CDC’s vaccine recommendations for children sued the agency for failing to test the cumulative effect of the 72-dose schedule on children’s health.
Research scientist and author James Lyons-Weiler, Ph.D., said, “Properly controlled and sufficiently powered trials are the gold standard,” promised by U.S. Health Secretary Robert F. Kennedy Jr., and that such trials are “the correct approach for any clinical intervention.”
“It’s about time the gold standard of science is applied to vaccines,” he said.
In a statement shared with The Defender, Emily G. Hilliard, press secretary for the U.S. Department of Health and Human Services, said the department “does not comment on future or potential policy decisions.”
Prasad: Past studies ‘incapable of adequately documenting safety signals’
According to Fierce Pharma, the Biden administration “supported vaccine coadministration as a means to increase immunization rates.”
Dr. Vinay Prasad, director of the FDA Center for Biologics Evaluation and Research (CBER), has publicly criticized this strategy due to a lack of evidence supporting it, the Post reported.
The Post cited 2021 guidance from the World Health Organization, which found that coadministration of the COVID-19 and flu vaccines is safe and “has potential advantages.”
A survey of the scientific literature, published in March in the journal Influenza and Other Respiratory Viruses and cited by the Post, found that “Adult vaccine coadministration is safe for all the combinations we assessed,” with adverse events that were “generally mild to moderate and of short duration.”
The Post also cited a 2022 CDC study published in JAMA Network Open, which found that “simultaneous administration of COVID-19 mRNA booster and influenza vaccines may be associated with increased likelihood of systemic reactions.” Yet, according to the Post, “those reactions were mostly mild and went away quickly.”
In the FDA memo, Prasad said past determinations regarding the safety of coadministering respiratory virus vaccines were made on the basis of small randomized studies. “Such small trials are inherently incapable of adequately documenting safety signals,” he said.
Baker agreed:
“At least two of the studies showed statistically significant increases in systemic reactions when the vaccines were coadministered. To dismiss this finding without further evaluation — as was done — is both irresponsible and tendentious in favor of ‘just giving’ the shots.”
Lyons-Weiler said the relevant studies “support convenience and short-term tolerability,” but “do not deliver the decisive evidence needed for label-level claims about clinical benefit or the absence of interaction-driven risk.”
Giving multiple vaccines at once is convenient, profitable — but not necessarily safe
Dr. Ashish Jha, the White House’s former coronavirus coordinator during the Biden administration and now dean of the Brown University School of Public Health, told the Post that the millions of doses of respiratory virus vaccines coadministered over the years prove they are safe.
“The burden of proof is not on manufacturers to be able to do something that clearly has been done millions of times safely,” Jha said.
Karl Jablonowski, Ph.D., senior research scientist at Children’s Health Defense, said Jha “is partaking in a fallacy that past actions were safe and warranted,” as “historic data of dubious record does not constitute a safety study.”
Jablonowski said:
“That it has been administered millions of times does not make vaccines safe; it makes them profitable. That we administered vaccines to our most vulnerable — during pregnancy and to 6-month-old infants — doesn’t make them safe, it makes us reckless.”
Baker agreed, saying, “Jha is correct in stating that the coadministration of multiple vaccines for respiratory viruses ‘clearly has been done millions of times.’ But how ‘safely’ has it been done? Jha doesn’t know, because nobody knows.”
Jablonowski said looking at vaccination data retrospectively is problematic because “there is no experimental control.”
He cited the case of a 6-month-old in Iowa who received multiple respiratory virus vaccines concurrently in 2022 and was “found pulseless” in his crib 10 days later, according to a report in the U.S. government-run Vaccine Adverse Event Reporting System or VAERS.
“Which vaccine, if any, likely killed him? We don’t know, because we don’t have the safety studies for combinations,” Jablonowski said.
Jablonowski also referred to a 2023 paper published in The BMJ on the safety of the mRNA COVID-19 booster shots. His analysis of the study’s data found that people who received a flu vaccine along with their fourth COVID-19 booster dose had a 62.5% higher risk of stroke within 28 days of vaccination.
The 2022 CDC study does, in fact, show “a compounding or synergy of adverse reactions,” Jablonowski added.
The study states:
“Compared with administration of COVID-19 mRNA booster vaccines alone, simultaneous administration of COVID-19 mRNA booster and seasonal influenza vaccines was associated with significant increases in reports of systemic reactions during days 0 to 7 following vaccination.”
Jablonowski analyzed the study’s results. He found that people who received Pfizer or Moderna COVID-19 vaccines concurrently with a flu vaccine were more likely to experience a systemic or injection-site reaction or to be unable to work or attend school following vaccination.
FDA policy ‘could have implications’ beyond cold and flu season
CDC guidance, current as of Aug. 18, states, “Flu, COVID-19, and RSV vaccines may be co-administered (given at the same visit)” and “may also be co-administered with other vaccines.”
According to the Post, Prasad’s memo “could have implications that go beyond the fall respiratory vaccination season.”
While the memo “does not prevent pharmacies and doctors from providing coronavirus and flu vaccines in the same visit,” the Post suggested that immunization rates may decline if more than one visit is required to receive multiple respiratory virus vaccines, or longer intervals are required between shots.
The memo comes as national pharmacy chains, including CVS and Walgreens, have begun limiting access to COVID-19 vaccines in response to new federal guidelines enacted last month ending emergency use authorization of the COVID-19 shots and restricting them to people at higher risk for severe illness.
According to the Post, Pfizer responded to Prasad’s memo by sending a letter to healthcare providers stating that some batches of its COVID-19 vaccine contain “unapproved prescribing information inside the cartons,” indicating the company intends to add a warning about coadministration of the vaccine to its product label.
According to the Post, the FDA’s policy change may also lead to new recommendations for respiratory vaccines — potentially stemming from the CDC’s vaccine advisory panel, the Advisory Committee on Immunization Practices (ACIP).
CDC vaccine advisers to meet next week
ACIP is scheduled to meet Sept. 18 to vote on COVID-19 vaccine recommendations for the upcoming cold and flu season.
In June, Kennedy retired all 17 members of ACIP to eliminate conflicts of interest. Shortly after, Kennedy named eight researchers and physicians to the committee, but one nominee declined to participate. Fierce Pharma reported last week that Kennedy plans to nominate seven additional members to the committee.
The new FDA policy is part of a broader series of shakeups at the FDA and CDC.
Prasad resigned from his position on July 29 amid pressure from vocal critics, but returned to his position two weeks later.
In May, Prasad replaced Peter Marks, M.D., Ph.D., as head of CBER. Marks had overseen Operation Warp Speed and the rapid development and approval of the COVID-19 vaccines. He resigned in March under pressure from Kennedy.
On Aug. 27, the White House confirmed the firing of CDC Director Susan Monarez, after she refused to resign amid clashes with Kennedy.
During a contentious U.S. Senate hearing Thursday, Kennedy said Monarez had indicated she would refuse to endorse any ACIP recommendations, even before the committee met to make them.
On Sept. 1, President Donald Trump suggested that the CDC and Big Pharma have not been fully forthcoming about COVID-19 vaccine safety data. Trump demanded they “clear up this mess.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Featured Video

or go to
Aletho News Archives – Video-Images
From the Archives
Israel Would Have No Qualms About USS Liberty-Style FALSE FLAG If Iran Campaign Falters – Analysts
By Ilya Tsukanov – Sputnik – 18.06.2025
Donald Trump is mulling whether or not to join Israel’s aggression against Iran as Tel Aviv faces problems sustaining its defenses against growing counterstrikes, and apparently lacks a realistic game plan for an end to hostilities after failing to achieve its goals. Analysts told Sputnik how the US could be ‘nudged’ into the conflict.
“The US is already assisting Israel with supplies, intel, refueling support, etc. One of the many US posts in the region could be attacked for a casus belli,” former Pentagon analyst Karen Kwiatkowski explained.
“If Trump doesn’t comply with Israel’s demand” and join its aggression voluntarily, “a false flag may be needed” to drag the US in, Kwiatkowski, retired US Air Force Lt. Col.-turned Iraq War whistleblower, fears.
Netanyahu has a diverse array of options at his disposal, according to the observer, including:
- a false flag against US assets abroad blamed on Iran or one of its Axis of Resistance allies, like the Houthis
- a US domestic attack or assassination blamed on Iran
- Iranian air defenses ‘accidentally’ hitting a civilian jetliner carrying Americans
- use of a dirty bomb or nuclear contamination somewhere in the region blamed on Iran
- even blackmailing by threatening to use nukes against Iran if the US doesn’t join the fight
Kwiatkowski estimates that Israel probably has “enough blackmail power” against President Trump and Congress to avoid the necessity of a false flag operation, but a “USS Liberty-style” attack, targeting the soon-to-be-retired USS Nimitz supercarrier that’s heading to the Middle East, for example, nevertheless cannot be ruled out entirely, she says. … continue
Blog Roll
 Aletho News
Aletho News- Top PMU commander, over a dozen fighters killed in new US strikes on Iraq
- Is Netanyahu’s war gamble threatening the future of ‘Israel’?: FT
- Smotrich calls for annexation of South Lebanon to Litani River
- Echos of Gallipoli? Hormuz and the Geography of Hubris
- Pakistan PM backs Iran’s right to self-defense amid tensions
- Hungary blasts ‘fake’ EU accusation
- SAFE Debt Trap: Poland’s €43.7 Billion Bet on Unipolar Illusion
- War on Iran threatens global Gulf capital flows: FT analysis
- Mossad De Facto Admits To Inciting Riots In Iran
- Tehran: World grown thoroughly exhausted with US-Israeli ‘false flag storylines’
- If Americans Knew
- From Sde Teiman, the truth about Israel’s military justice system has been set free
- Child denied life-saving bone marrow transplant by Israel ‘because he is from Gaza’
- Raffi Berg: BBC Middle East Editor Exposed as CIA, Mossad Collaborator
- Jerusalem Archbishop Rebukes Netanyahu’s Statements on Christianity
- US to embed Palantir AI across entire military: Report
- Israeli-US war on Iran to drag on “a few more weeks” – Not a ceasefire Day 164
- Lebanon deaths top 1,200; Palantir AI to be embedded across US military – Not a ceasefire Day 163
- Israel’s assassination game: Take all pragmatists off the board
- Food shortages return to Gaza as Israel tightens aid restrictions under the cover of its war on Iran
- Trump demands trillions in payments from Gulf countries, billions from Harvard – Not a ceasefire Day 162
- No Tricks Zone
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis
- New Study Documents A 20-Year Pause In Arctic Sea Ice Decline – Driven By Internal Variability
- Wake-up Call: Survey Shows Majority Of Germans Now Favor Postponing Climate Targets!
