Greg Tucker-Kellogg publishes fraudulent study to attack ivermectin
Tucker-Kellogg aimed to review research conducted in Brazil and conclude that ivermectin was ineffective against Covid-19. In order to do so, he and his colleagues had to fabricate over 250 fatalities.
Illustration. Reproduction photo from Greg’s YouTube channel.
Médicos Pela Vida | August 17, 2023
Greg Tucker-Kellogg, from the Department of Biological Sciences at the National University of Singapore, who receives compensation from YouTube for creating content against scientific misinformation, along with two other authors, Ana Carolina Peçanha and Robin Mills, published a study on the Medrxiv platform on August 15th. The study used fraudulent data with the aim of undermining the research on ivermectin conducted in Itajaí, located on the coast of Santa Catarina, Brazil.
The study conducted in Itajaí, peer-reviewed and published in the prestigious Cureus journal in early 2022, concluded the effectiveness of ivermectin in its prophylactic use against COVID-19. The results were positive: among individuals who took ivermectin preventively, there were 68% fewer deaths, 56% fewer hospitalizations, and 44% fewer infections.
The False Data
Tucker-Kellogg and colleagues’ study, which aimed to recalculate and nullify the positive results, used fraudulent data to achieve its goal. In the article, they claim that the data is official.
The authors stated that 499 individuals died between July and December 2020, a period during which the effectiveness of ivermectin was studied in the city.
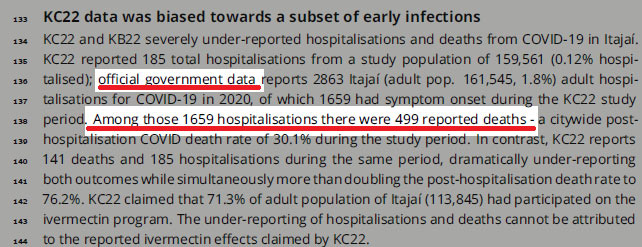
However, the data of 499 COVID-19 deaths during the six months of the study in Itajaí is indeed false. In order to achieve their desired outcome, the number of deaths had to be inflated. You can verify the original PDF of the reanalysis here on page 3.
How We Investigated
The purported 499 deaths in six months, used as a basis for the calculations, raised suspicions due to being an unusually high number for the period in a city with just over 200,000 inhabitants. Consequently, the first step we took was to research the city’s epidemiological bulletins during that timeframe.
The official epidemiological bulletin, published on the Itajaí city government’s website on December 28, 2020, stated that a total of 254 individuals had died since the beginning of the pandemic. This figure represents deaths from when the virus first spread in the city in early 2020. Therefore, the deaths between July and December were even fewer, far from the reported 499.
In a second attempt to verify the numbers, we accessed consolidated data from the Brazilian Unified Health System (Sistema Único de Saúde or SUS) through the OpendataSUS database, which is considered one of the most comprehensive and accurate in the world. As Brazil has a publicly funded healthcare system, data for all patients in the country is rigorously monitored.
The OpenDataSUS Numbers:
Deaths caused by Severe Acute Respiratory Syndrome (SARS), with dates ranging from July to December 2020, among residents of the city. Database downloaded on March 13, 2023.
Based on the date of hospitalization:
Total SARS-related deaths: 234
Deaths due to Covid-19 only: 222
Based on the date of symptom onset:
Total SARS-related deaths: 256
Deaths due to Covid-19 only: 237
Based on the date of data entry:
Total SARS-related deaths: 240
Deaths due to Covid-19 only: 222
The Numbers from Brasil.IO
According to the information from the Brasil.IO database, which compiles data from confirmed cases and deaths from the bulletins of the State Health Departments (Secretarias Estaduais de Saúde or SES), during the period of the Itajaí study, the data were as follows:
Total Covid-19 deaths: 227
Fraudulent Study Used for Attacks
The authors of the original study have a long history in science and impeccable reputations. Lucy Kerr, the lead author, is the daughter of the late Warwick Stevam Kerr, and she deeply values his legacy. Warwick was the Scientific Director of FAPESP, served as the president of the Brazilian Society for the Advancement of Science, and received the Order of Scientific Merit in the Grand Cross category. Other authors include Dr. Flavio Cadegiani, a researcher with several COVID-19 studies, Dr. Fernando Baldi, a professor at the São Paulo State University (UNESP), Dr. Pierre Kory, an American medical professor, and Dr. Jennifer A. Hibberd from the University of Toronto, among others.
Following the publication of the reanalysis with fraudulent data, the attacks on the authors’ reputations turned defamatory. “There are people who prefer to keep believing in charlatans,” said Chloé Pinheiro, a journalist from Veja, one of Brazil’s major magazines.
Leandro Tessler, a professor at Unicamp, who represents the respected university in classifying true or false news on the internet and has admitted to not reading studies on cheap, generic, and unpatented treatments that he criticized, claimed that the original positive study had “cooked data.” Furthermore, Leandro criticized the journal’s quality by saying, “It’s something for Cureus.”
“Statistical trickery,” said Julio Ponce, a doctor in epidemiology and host of the podcast “Escuta a Ciência,” in response to the positive results of the original study.
Isaac Schrarstzhaupt, coordinator of the Rede Análise, criticized the quality of the Cureus journal. He stated that the original publication falls among the “lesser journals,” and he phrased it this way “to avoid using other terms.“
Original Authors Always Prioritized Transparency
The authors of the original study on ivermectin in Itajaí, responding to a call from the BMJ – British Medical Journal, which requested the publication of public data from studies on medications and vaccines, decided to make their raw data available for reanalysis.
This action was highly praised. “It’s excellent that they have released their data anonymously. They have true confidence in the results of their analyses. This is how good science is carried out,” stated Dr. Harvey Risch, a professor of epidemiology at Yale University, USA, emphasizing that patients’ personal data had been preserved.
Previously, the scientific community had speculated that the authors would not make their data available.
The doctor has been attacking the authors for some time
Ana Carolina, one of the authors of the study, has been attacking Dr. Flavio Cadegiani for some time. He is also the author of other studies involving different medications against Covid-19, such as those involving proxalutamide. She claims that those researches are a “hoax.” Regarding the study she chose to reanalyze now, inserting fraudulent data, Ana Carolina had already committed in early 2022 to disqualify it. She referred to it as an “international embarrassment” at the time and used quotation marks to refer to the researchers, seemingly implying doubt about their work.
“They had already decided that ivermectin doesn’t work. So, they tried – and made a great effort – to find calculations that ‘fit’ their pre-established conclusion. This is the exact opposite of what science is, which involves accepting results whether they contradict or support the hypothesis. In their quest to find the desired data, they most likely forgot to look at their own analyses – and even worse, at basic numbers. Furthermore, it seems to me that they didn’t quite understand the study, as I couldn’t find analyses related to rates derived from infections, matched with Propensity Score Matching,” stated Dr. Flavio Cadegiani, one of the authors of the Itajaí study.
“The most important thing is that this ‘study,’ by demonstrating its inability to invalidate us, has only reinforced our findings, and for that, we cannot help but be grateful,” he added.
MPV Comment
Scientific fraud is presenting unverified data as if it were official. And this wasn’t a small error. It was the central data point used to generate the result. It’s not a minor mistake that wouldn’t affect the studied outcomes. In order for the authors to attack the study and arrive at the conclusion of inefficacy, they needed to increase the number of deaths.
All those who subsequently attacked, even labeling the authors as “charlatans,” supposedly had the capacity and training to spot the fraudulent numbers. They are doctors, professors, epidemiologists, and data scientists. They either didn’t see it or feigned ignorance.
So far, all the scientific frauds published during the pandemic have targeted inexpensive, generic, and unpatented medications, or they were frauds promoting expensive and patented drugs. Surely, this is just a coincidence.
This is the second time the Itajaí study has been attacked without valid scientific arguments. In June 2022, the USP – University of São Paulo journal attacked it, even spreading false information. Our analysis can be read here: “COVID-19: USP Journal Lies and Distorts Science to Attack Ivermectin. Read the full analysis.” (portuguese).
We, at MPV (Médicos pela Vida) – Doctors for Life, are grateful for the collaboration of Professor Daniel Tausk from USP, for compiling data from official databases. His collaboration was essential for the report. Additionally, we thank the French researcher Massimaux, who prefers to remain anonymous on Twitter, for quickly pointing out fraudulent data. According to him, it was a “sanity check.” It didn’t pass.
Sources
Data from OpendataSUS
Data from Brasil.IO
Epidemiological Bulletin of Itajaí
London City Hall Tries to Put Pressure on Scientists Who Doubted Climate Policy – Report
Sputnik – 20.08.2023
London Mayor Sadiq Khan’s office tried to “silence” scientists who called into question the effectiveness of the ultra-low emissions zone (Ulez) policy promoted by the head of the city, The Telegraph reported on Saturday.
Shirley Rodrigues, the London Mayor’s deputy for environment and energy, told in emails to Imperial College London professor Frank Kelly that she was “really disappointed” by scientists publishing results that cast doubt on the effectiveness of Ulez, the newspaper reported, adding that the corresponding complaint was sent in November 2021.
In particular, Rodrigues said that she was “deeply concerned” about the damage done to the credibility of the Mayor’s office and Ulez. In response, Kelly promised to write a Ulez-friendly report, the report added.
The report stated that since 2021, Kelly’s research group has received over 800,000 pounds ($1.018 million) from the mayor’s office. However, the publication by scientists led to a cooling in their relations with the London city hall. This, in turn, caused the reluctance of representatives of the scientific community to write any new materials about Ulez, the newspaper noted.
The Ulez initiative was first announced by then-Mayor of London Boris Johnson in 2015. Later, Khan launched an initiative that included, among other things, the installation of special traffic signs and cameras. Since 2020, the London authorities have had to spend over 850,000 pounds to rebuild infrastructure for the initiative, which has been repeatedly damaged by vandals.
Critics Slam JAMA Study Claiming 52 U.S. Doctors Spread COVID ‘Misinformation’
By Monica Dutcher | The Defender | August 18, 2023
Critics of a study published this week in JAMA concluding 52 doctors from across the U.S., propagated “COVID-19 misinformation about vaccines, treatments, and masks on large social media and other online platforms” called the study nothing more than “propaganda.”
“Ultimately, misinformation is just a weaponized term meaning nothing,” said Vinay Prasad, M.D., MPH. “People who use it are often completely ignorant of science and truth.
Prasad and others pointed to several flaws in the study, including the researchers’ definition of “misinformation,” the reported percentage of those with post-COVID-19 condition, or “long COVID” and the false claim that the Johnson & Johnson vaccine alone led to deaths — as deaths also have been linked to the Pfizer and Moderna mRNA vaccines.
The CDC as the arbiter of COVID truths
The University of Massachusetts researchers who produced the study defined misinformation as “assertions unsupported by or contradicting U.S. Centers for Disease Control and Prevention [CDC] guidance on COVID-19 prevention and treatment during the period assessed or contradicting the existing state of scientific evidence for any topics not covered by the CDC.”
But in an Aug. 16 Substack article, Prasad — a hematologist-oncologist and professor in the Department of Epidemiology and Biostatistics at the University of California, San Francisco — challenged the notion of using the CDC as the litmus test for pandemic-related information.
CDC “made many errors,” Prasad wrote, citing a paper he published in March, documenting 25 statistical or numerical errors made by the CDC that he said raised questions about the agency’s “real or perceived systematic bias.”
It’s also well documented that the agency constantly changed its mask guidance and published conflicting information about vaccine effectiveness.
Dominique Brossard, professor and chair of Life Sciences Communication at the University of Wisconsin-Madison, who studies medical misinformation, told USA Today, “The guidance kept on changing … Communication around the vaccine was horrible.”
Dr. Jeff Barke, an Orange County, California, primary care physician and founding member of America’s Frontline Doctors, called the CDC “a captured agency,” saying “it makes no sense whatsoever to recommend this toxic product [COVID-19 vaccines] to children.”
The CDC never came out with early treatment guidelines, Barke said. It was always about vaccines and masks. Barke recalled prescribing ivermectin to his patients and the pharmacists not filling it, asking him for the “diagnostic code” in order to proceed.
Barke told The Defender :
“The pharmacy never asks for a diagnostic code if you prescribe OxyContin for a patient. So it’s OK for a doctor to prescribe a Schedule II narcotic — no questions asked — but I can’t prescribe a product that has a proven safety record of 50 or 60 years.”
Barke is a co-plaintiff in a lawsuit to stop a California law that subjects the state’s doctors to discipline, including the suspension of their medical licenses, for sharing “misinformation” or “disinformation” about COVID-19 with their patients.
What exactly is ‘misinformation’?
The study’s authors identified four categories of “misinformation”:
- Claiming vaccines were unsafe and/or ineffective.
- Promoting unapproved medications for prevention or treatment.
- Disputing mask-wearing effectiveness.
- “Other misinformation,” to include conspiracy theories and the virus’s origins.
The authors reviewed COVID-19-related posts from doctors on the social media platforms Twitter (now X), Facebook, Instagram, Parler and YouTube between January 2021 and December 2022.
The researchers initially focused their Twitter review on America’s Frontline Doctors’ profile because of the organization’s “volume of COVID-19 misinformation in its tweets” and “large following.”
Physicians who followed America’s Frontline Doctors’ Twitter page were targeted on Twitter and other platforms.
Using the search terms “COVID,” “vaccine,” “doctor,” “physician,” “ineffective,” “pharmaceutical,” “ivermectin,” “hydroxychloroquine” and others, the authors of the study identified 52 doctors — 50 licensed and two unlicensed — who used social media to spread COVID-19 “misinformation.”
Results showed most of the 52 physicians (76.9%) who posted “misinformation” did so in more than one of the four categories identified. The majority posted vaccine “misinformation.”
Dr. Meryl Nass — who on Thursday sued the Maine Board of Licensure in Medicine and its individual members, alleging the board violated her First Amendment rights and her rights under the Maine Constitution — called the JAMA study “a piece of propaganda.”
Nass said:
“There is no science. They [the authors] are trying to make it look like they’re doing something quantitative when they’re not. There was a lot known about the ineffectiveness of the vaccines at the time they were working on this paper.”
Unpacking the misinformation in the misinformation study
The University of Massachusetts researchers said doctors’ claims that myocarditis was common in children who received the vaccine and that the risks of myocarditis outweighed the risk of vaccination were “unfounded.”
But myocarditis “does outweigh the benefits of vaccinations for some ages — in men — and some doses,” said Prasad, citing an article published in the Journal of Medical Ethics.
The paper, which focused on booster mandates at American universities, concluded the mandates were unethical because they could result in greater health risks, like booster-associated myocarditis, than benefits to healthy young adults.
Several other studies have shown either myocarditis deaths across all age groups, or elevated myocardial injury after vaccination.
The researchers also flagged any posts discussing pre-pandemic studies that definitively concluded masks do not prevent the spread of respiratory viral infections. And they deemed as misinformation any post that undermined the role of masks in slowing the spread of the infection and that pointed to rising cases in areas with mask mandates.
But a plethora of studies on mask ineffectiveness emerged during the time the Massachusetts team was conducting its research on physicians and “misinformation.”
There were also reports on “The Foegen effect” — the idea that deep re-inhalation of droplets and virions caught on facemasks might make COVID-19 infection more likely or more severe. German physician Dr. Zacharias Fögen introduced the concept in a study that concluded: “mask use might pose a yet unknown threat to the user instead of protecting them, making mask mandates a debatable epidemiologic intervention.”
“The totality of the evidence to date shows no benefit from community mask wearing,” said Prasad, who pointed to Cochrane’s multiple analyses.
According to the JAMA study, doctors who said the COVID-19 vaccines were ineffective at preventing COVID-19 spread or that the virus originated in a lab in China were propagators of misinformation.
Yet plenty of data show the vaccines did not prevent transmission, and scientists even testified to evidence that COVID-19 could have resulted from controversial gain-of-function research at the Wuhan Institute of Virology.
In the wake of the pandemic, multiple organizations have published guidelines on “medical misinformation” — including YouTube and the American Medical Association (AMA).
Last June, the AMA adopted a new policy to limit medical disinformation, including ensuring that medical licensing boards can take disciplinary action against health professionals who spread health-related disinformation.
In California, however, a judge ruled in January that the state does not have the power to penalize doctors who spread “misinformation” or “disinformation.”
“COVID-19 is a quickly evolving area of science that in many aspects eludes consensus,” the judge decided.
Monica Dutcher is a Maryland-based senior reporter for The Defender.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Can You Overdose on Ivermectin? Dr. Pierre Kory’s Answer Will Shock You
The Vigilant Fox | Vigilant News | August 17, 2023
“Of all the harmful misinformation spread over the past couple of years, one of the most disturbing false narratives was targeted at the Nobel-Prize-winning, human medicine ivermectin,” expressed filmmaker Mikki Willis in his ground-breaking documentary titled, Ivermectin: The Truth.
Ivermectin is “one of the safest and most effective medicines of this era. A medicine that, according to the numerous top scientists I’ve interviewed … could have ended the pandemic before it began.”
But Ivermectin is “horse dewormer,” the media said. “It could put you in a coma.” “It can kill you,” pundits warned.
But is this actually true?
Popular podcaster Greg Hunter, AKA USA Watchdog, asked Dr. Pierre Kory, one of the world’s leading experts on Ivermectin, straight-up, “Can I OD (overdose) on Ivermectin if I get two or three times the [standard] dose. Can I kill myself?”
“Let me answer scientifically. So there is a world-famous toxicologist named Jacques Descotes, and he’s French. And two years ago, he was commissioned to do a scoping review of the entire data on the safety of Ivermectin in its history. And his conclusion after doing this comprehensive review is that he does not believe that there has been one single case of anyone dying from an Ivermectin overdose.”

Prof. Jacques Descotes: Image – Academica.edu
“Oh, Lord,” reacted Greg Hunter. “How many pills have been given worldwide? I heard 4 billion, but it must be more than that.”
“Over 4 billion,” Dr. Kory confirmed. “Now, people have died where the deaths were reported as caused by Ivermectin. But when he [Prof. Jacques Descotes] reviewed those cases, he didn’t think those arguments [were] credible.”
Let’s dive deeper into Prof. Descotes’ analysis.
But first, a quick look at his impressive credentials. “Pr. Jacques Descotes, MD, PharmD, PhD, Professor Emeritus, Claude Bernard University of Lyon (France), [is] a world-known toxicologist with a 40-year track [record] as an independent consultant for the pharmaceutical industry as well as an advisor to regulatory bodies worldwide,” BusinessWire wrote.
In March 2021, he conducted a review of Ivermectin’s safety profile based on over 350 articles – plus accessible web sources. Here are his conclusions:
“Ivermectin has been administered orally to hundreds of millions of people throughout the world in the past three decades. The assessment of reported adverse events temporally associated with Ivermectin exposure shows that Ivermectin-induced adverse effects have so far been infrequent and usually mild to moderate.
“It is noteworthy that no deaths have seemingly ever been reported after an accidental or suicidal overdose of Ivermectin. No greater toxicity of Ivermectin has been substantiated in elderly people despite repeated assertions that an ageing blood-brain barrier might lead to increased Ivermectin toxicity level. The positive clinical experience accumulated with Ivermectin administration led many medical experts to break away from early adamant contra-indications in pregnant women. Finally, several national pharmacovigilance networks around the world released information and opinions to ascertain Ivermectin safety in human subjects. So far, there are no critical safety limitations to Ivermectin prescription in current indications.
I also want to point out that no severe adverse event has been reported in dozens of completed or ongoing studies involving thousands of participants worldwide to evaluate the efficacy of Ivermectin against COVID-19.”
“In order to overdose from Ivermectin, you have to take either a hundred or a thousand times the standard dose,” declared Dr. Kory.
“And there have been accidental poisonings where people have taken large amounts. But you know what happens every time? When they take these massive amounts of Ivermectin, it tends to affect them neurologically. They’ll get confused. They might be stumbling — uncoordinated. They go to the hospital, and there’s no treatment required. But within days, the patients return to normal. So, there’s been no life-ending injuries. No deaths reported with Ivermectin. So, that shows you why it’s one of the safest drugs in history, even at massive overdoses.
Greg Hunter’s full interview with Dr. Pierre Kory is available to watch.
Medical Board Chief who wanted Doctors delicensed for ‘misinformation’ in bed with PR firm tied to CDC, Pfizer, Moderna
By Michael Nevradakis, Ph.D. | The Defender | August 18, 2023
The head of a national medical organization who publicly called for doctors to lose their licenses unless they supported government narratives on COVID-19 treatments and vaccines concealed his relationship with a public relations firm whose client list also included Pfizer, Moderna and the Centers for Disease Control and Prevention (CDC).
Dr. Richard Baron, president and CEO of the American Board of Internal Medicine (ABIM) is a client of Weber Shandwick, investigative journalist Paul D. Thacker reported on Wednesday.
In late 2021, Baron publicly pushed for doctors who spread “misinformation” about COVID-19 and the vaccines to lose their license and certification. Baron said then that “putting out flagrant misinformation is unethical and dangerous during a pandemic.”
Weber, the world’s second-largest PR firm, has branded its team as “misinformation and disinformation” experts and says it provides clients with services to help manage any perceived threats posed by spreaders of such information.
The firm has organized conference panels on “medical misinformation” in which Baron participated.
Last year, Baron partnered with Weber Shandwick to propose a South by Southwest (SXSW) panel titled “When Doctors Prescribe Misinformation.” The proposal was subsequently accepted and the panel took place at SXSW in Austin, Texas, on March 13.
According to Thacker, “Weber Shandwick’s panel featuring Dr. Baron has been widely promoted by the PR firm’s employees,” including Sarah Mahoney, executive vice president, Healthcare Communications, Strategy & Planning for Weber Shandwick, who in a LinkedIn post, wrote she “can’t think of a more important topic right now.”
The CDC’s National Center for Immunization and Respiratory Diseases (NCIRD) in September 2020 awarded Weber a $50 million contract “to promote the vaccination of children, pregnant women and those at risk for flu and increase the general acceptance and use of vaccines,” according to the PR firm’s website.
Under the contract, Weber employees were embedded in the NCIRD to “communicate the risks and recommended actions for outbreaks and convey vaccine recommendations to healthcare providers,” according to Thacker.
Medicine has always been ‘in bed with Big Pharma’
Several doctors have faced disciplinary action by state medical boards for allegedly spreading “misinformation.” One of them is internist and biological warfare epidemiologist Dr. Meryl Nass, a member of Children Health Defense’s scientific advisory committee.
Nass on Thursday sued the Maine Board of Licensure, which suspended her license in January 2022.
The board’s suspension arose from its adoption of a position statement promulgated by the Federation of State Medical Boards (FSMB) threatening physicians “who generate and spread COVID-19 vaccine misinformation” with suspension or revocation of their medical license.
In 2021, ABIM and FSMB collaborated to create the statement used to discipline Nass.
Nass told The Defender that in order to get certified by organizations like ABIM, there are several requirements, primarily related to demonstrating competence in one’s field of specialization, including completing a residency, being certified by the residency director, and paying for and passing the board examinations.
Nass told The Defender that in order to get certified by organizations like ABIM, there are several requirements. She explained:
“You complete a medical residency in your field of specialization. Your residency director certifies your competence and moral character, and you must pay for and pass your board examination to demonstrate your command of your specialty.
“When you’ve paid them for board certification and successfully completed all the requirements, how can they change the rules 20 or 50 years later and say, ‘we’re going to decertify you now because we don’t like your viewpoint?’
“There was nothing in any documentation from the Board of Internal Medicine about misinformation, or any other standards that the board can impose apart from competency to practice when it issued certifications.”
Dr. Richard Eggleston, a retired ophthalmologist in Clarkston, Washington, also faces disciplinary action — by the Washington Medical Commission — arising from articles he published in a local newspaper in 2021, questioning the official narrative and medical advice related to COVID-19.
Doctors aren’t being targeted exclusively for spreading “misinformation” — some, like Dr. Mary Kelly Sutton, an integrative physician, were targeted for their less-than-100% support for COVID-19 vaccines.
Last month, the Massachusetts medical board revoked Sutton’s medical license, claiming she improperly exempted eight children from required school vaccinations. This came a year after California also revoked Sutton’s medical license.
Sutton told The Defender, “The voice of medicine today is determined by the marketing wisdom of Madison Avenue, not by what is sound information from scientific research.”
Sutton said the whole practice of medicine rests on sharing and providing information necessary for informed decisions and consent. When specialty boards issue vague accusations, they engage in “harassment,” and an “egregious overreach of power” and are obstructing the practice of medicine.
A California law aimed at punishing doctors for providing “misinformation” to their patients is now in “legal limbo” following conflicting rulings in state courts earlier this year, which could affect Sutton’s and other California doctors’ cases going through the courts.
This trail of evidence demonstrates medical boards are not simply acting on their own authority but in collusion with state governments, federal agencies and private companies.
“There’s no one who is a ‘misinformation’ or ‘disinformation’ expert whose opinion does not align with the government and with the corporations,” Thacker told The Defender. “That’s what makes them an ‘expert.’”
“What’s always been true is that medicine has been in bed with Big Pharma,” he added. “It’s now becoming a lot more transparent. These relationships are much more transparent.”
‘A very political attempt to shut down people from having alternative viewpoints’
According to Thacker, Baron began his “crusade for the biopharmaceutical industry” in September 2021. In a post for ABIM’s blog, Baron said, “I want to state unequivocally that ABIM can and does take action, independent of state licensing boards, to remove certification from physicians for unprofessional and unethical behavior.”
For Thacker, Baron’s concern about “misinformation” was first triggered when physicians spoke out against COVID-19 vaccine safety, efficacy and side effects. “These are the same concerns held by Weber Shandwick, who Pfizer and Moderna are paying big buck[s] to promote their vaccines,” he said.
“Baron’s relationship with Weber Shandwick was not disclosed” by JAMA, Thacker said, “nor in an accompanying viewpoint Baron wrote for JAMA.”
After an inquiry by Thacker, JAMA’s editor-in-chief, Kirsten Bibbins-Domingo, said, “We initiated our internal investigation earlier this week, in accordance with our standard processes for allegations of non-disclosure of conflicts.”
“It is notable that Baron has done his best to mislead the public and other physicians about what he is doing,” Nass said. “He claims the ABIM is trying to ‘protect the legitimacy of medical expertise’ rather than censoring viewpoints it does not like.”
Nass said Baron “conjures up examples of what the board might censure.” She pointed to a Feb. 23, 2023, New England Journal of Medicine (NEJM) article Baron co-authored with attorney Carl J. Coleman, which stated:
“When a licensed physician insists that viruses don’t cause disease or that COVID-19 vaccines magnetize people or connect them to cell towers, professional bodies must be able to take action in support of fact and evidence based practice.”
“Yet this is a fabrication,” Nass said, adding:
“Instead, Dr. Baron, who earns about $1.2 million yearly from the ABIM and the ABIM Foundation, has decertified Drs. Peter McCullough, Paul Marik and Pierre Kory — all highly celebrated, published and esteemed doctors in their fields.
“None of them have uttered any mumbo-jumbo about cell towers, magnetism or a non-viral etiology for COVID-19. All have had their board certifications revoked for the viewpoints they expressed — viewpoints that are supported by a preponderance of the medical literature.”
In a January 2022 article for Health Affairs, Coleman wrote, “Licensing boards are state agencies subject to the First Amendment, and as such they are limited in their ability to penalize physicians based on the content of their speech.”
Yet, a 2022 NEJM article co-authored by Baron argued that while “Differences of opinion in medicine are necessary for progress … there are some opinions that have been so thoroughly repudiated by existing evidence as to be considered definitively wrong.”
‘All this money is sloshing around now for misinformation research’
According to Thacker, “PR firms are now moving into the ‘disinformation’ space after decades of deceit on behalf of multiple industries,” with Weber Shandwick having “expanded into the disinformation space in late 2021,” promoting tactics that help “brands combat misinformation and disinformation that may implicate them.”
Speaking to Thacker, Dr. Aaron Kheriaty, director of bioethics at the Ethics and Public Policy Center, said, “The ABIM is clearly part of this ‘medical misinformation’ push, which is orchestrated by pharmaceutical companies and their PR allies” and which serves “the interests of Big Pharma.”
Remarking on the presence of a “medical misinformation” panel at SXSW, long known as a music, film and technology festival, Thacker told The Defender, “Anyone and everyone is getting involved in ‘misinformation’ and ‘disinformation.’”
“Baron has given a TED Talk, for instance. Why is TED Talks involved in this?” he asked.
In 2019 Baron delivered a talk at TEDx Chicago titled, “Please Don’t Confuse Your Google Search with My Medical Degree.”
For Thacker, the answer relates to financial interests. “All this money is sloshing around now for ‘misinformation’ research. Anyone can hop up and down saying ‘I’m an expert on misinformation and disinformation, get me a grant, get me on a panel,’” he said.
Weber embedded staffers within the CDC while representing Pfizer, Moderna
Thacker wrote that prior to discovering Baron’s ties to Weber Shandwick, he had confirmed the PR firm’s ties to COVID-19 vaccine manufacturers Pfizer and Moderna.
These ties did not prevent the CDC from awarding the $50 million contract to Weber Shandwick in September 2020 to push vaccines. The Daily Mail subsequently reported Thacker’s findings.
Medical Marketing and Media reported “Weber’s duties include providing 10 on-site health communications staffers, seven health comms specialists, two health research specialists and one social media specialist” to NCIRD, as well as “generating story ideas, distributing articles and conducting outreach to news, media and entertainment organizations.”
In October 2020, a blog post by Stacy Montejo, senior vice president at Weber Shandwick, disclosed that Pfizer is one of the firm’s clients. A month later, with Moderna’s COVID-19 vaccine awaiting Emergency Use Authorization, the company hired Weber Shandwick to handle the vaccine’s publicity, according to PR Week.
Such relationships have continued to the present. In June, Moderna announced a new communications strategy “to further educate the world about Moderna’s mRNA technology and its promise to transform the future of human health.”
The effort is led by Laura Schoen, “who is sometimes titled president of global healthcare at Weber Shandwick, and other times chief healthcare officer at IPG DXTRA, Weber Shandwick’s parent company,” Thacker wrote.
Lucy Rieck, a Weber Shandwick employee, previously publicly tweeted support for a panel Moderna proposed for this year’s SXSW, titled “COVID, Monkeypox, Disease X, What’s Next?” That proposal does not appear to have been accepted for presentation.
Conflicts of interest between Weber Shandwick, the CDC and NCIRD, and Pfizer and Moderna do not appear to have been disclosed.
In October 2022, Sen. Rand Paul (R-Ky.) sent a letter to the CDC inquiring about its relationship with Weber Shandwick and requesting “information regarding the nature of Weber’s work for the NCIRD.” It’s unclear whether the CDC complied with the request.
Todd S. Richardson, one of the attorneys representing Eggleston, told The Defender “While it is certainly understandable that governmental agencies will hire PR firms to help them get their message out … it becomes of real concern to me when those agencies, or people working within the agencies, try to silence those who disagree.”
According to Thacker, the web of relationships between Weber Shandwick doesn’t just extend to Big Pharma companies, the CDC and its agencies, or to doctors such as Baron. Academics such as Brown University’s Claire Wardle, Ph.D., a key figure in the “misinformation research” space, have participated in some of the firm’s events.
Wardle, a professor of the practice of Health Services, Policy and Practice at Brown University who has no scientific or medical credentials, participated in an online meeting organized by Weber Shandwick in October 2020 to discuss “election misinformation.”
Subsequently, Wardle played a key advisory role in the Biden administration, federal agencies, social media platforms and Ivy League institutions as they sought to censor content that ran counter to the government’s COVID-19 narrative.
According to Thacker, she “helped organize many of today’s campus disinformation groups … with funding from Google” and later sent Twitter a report aimed at countering the “growing threat of disinformation to trust in COVID-19 vaccines.”
Thacker said the biopharmaceutical industry is “the smartest at putting out disinformation. What other industry has bought off the medical community and the science community?” he asked. “They bought off the researchers, the government, the academic journals.”
Thacker said he believes much of what is labeled “misinformation” in medicine and academic research “is really just corporate PR,” and that “Congress needs to take a harder look at funding for ‘misinformation research.’“
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
“There Is No Climate Crisis”… 1600 Scientists Worldwide, Nobel Prize Laureate Sign Declaration
By P Gosselin | No Tricks Zone | August 15, 2023
1609 signatories recently signed a declaration that states there is no climate crisis, thus casting doubt over man’s alleged role in climate change and extreme weather.
Their doubt is based on data showing that natural factors are very much at play, the warming is slower than predicted, the models are unreliable, that CO2 has great benefits and weather disasters have not increased. The media hysteria and weather hype are not supported by data.
Climate science should be less political, while climate policies should be more scientific. Scientists should openly address uncertainties and exaggerations in their predictions of global warming, while politicians should dispassionately count the real costs as well as the imagined benefits of their policy measures.
Natural as well as anthropogenic factors cause warming
The geological archive reveals that Earth’s climate has varied as long as the planet has existed, with natural cold and warm phases. The Little Ice Age ended as recently as 1850. Therefore, it is no surprise that we now are experiencing a period of warming.
Warming is far slower than predicted
The world has warmed significantly less than predicted by IPCC on the basis of modeled anthropogenic forcing. The gap between the real world and the modeled world tells us that we are far from understanding climate change.
Climate policy relies on inadequate models
Climate models have many shortcomings and are not remotely plausible as policy tools. They do not only exaggerate the effect of greenhouse gases, they also ignore the fact that enriching the atmosphere with CO2 is beneficial.
CO2 is plant food, the basis of all life on Earth
CO2 is not a pollutant. It is essential to all life on Earth. More CO2 is favorable for nature, greening our planet. Additional CO2 in the air has promoted growth in global plant biomass. It is also profitable for agriculture, increasing the yields of crops worldwide.
Global warming has not increased natural disasters
There is no statistical evidence that global warming is intensifying hurricanes, floods, droughts and suchlike natural disasters, or making them more frequent. However, there is ample evidence that CO2-mitigation measures are as damaging as they are costly.
Climate policy must respect scientific and economic realities
There is no climate emergency. Therefore, there is no cause for panic and alarm. We strongly oppose the harmful and unrealistic net-zero CO2 policy proposed for 2050. Go for adaptation instead of mitigation; adaptation works whatever the causes are.”
Growing skepticism
Nobel Laureate in Physics Dr John F. Clauser also signed the manifesto.
The message is clear: there is no climate crisis. The number of critical scientists who no longer submit to the dogma of the alleged man-made climate catastrophe is growing.
Iran Commences Construction of Most Advanced-Ever Satellites
By Ilya Tsukanov – Sputnik – 18.08.2023
A fledgling space power with some of the best-developed space-based capabilities in the Muslim World, Iran’s space program has successfully launched over a dozen civilian and military satellites, created cosmodromes and built a range of homegrown space rockets using knowhow gained in the military sphere.
Iran has formally announced the start of design and construction work on two of its latest generation earth-imaging satellites.
“We had previously made promises regarding the construction of high-precision observation satellites, and today I proudly announce that the Iranian Space Agency has taken a significant step in designing and building domestic high-precision observation satellites. In this regard, the design and construction of two important projects, named Pars 2 and Pars 3, have officially commenced,” Iranian Space Agency chief Hossein Salariyeh told a media event Thursday.
The Pars 2 “is essentially a project to build an observation satellite with 4-meter imaging precision. The process of design and construction has begun for this satellite,” Salariyeh explained. As for the Pars 3, its development will provide Iran with its “most modern and highly accurate” imaging capabilities ever, with “an imaging precision of approximately 2 meters.”
The Pars series (lit. ‘Persia’ or ‘Iran’ in Persian) is one of Iran’s most ambitious satellite projects to date, with the remote-sensing spacecraft to be fitted with high-resolution earth imaging capabilities which can be used in agriculture, natural resource management, environmental and border monitoring, water sciences and mining.
Iran has one of the most advanced home-grown space programs in the Middle East, and in 2009 became the first Muslim nation to independently launch a satellite into orbit. The Iranian Space Agency has also engaged in deep cooperation with Russia and China, engaging in cooperative joint research programs, and piggybacking spacecraft on Soyuz rockets from the Baikonur Cosmodrome in Kazakhstan. Last year, a Russian rocket helped launch the Khayyam, a 600 kg remote sensing satellite which became fully operational and started its remote sensing activities last month.
Speaking at Thursday’s event, Iranian government spokesman Ali Bahadori Jahromi hailed the progress reached in Iran’s space endeavors, and said the country, whose peaceful space ambitions were born after the victory of the 1979 Revolution, is already reaping economic benefits from its space program.
Home to one of the world’s oldest continuous major civilizations, Iran has gifted the world with many of its earliest space scholars, including mathematicians and astronomers Omar Khayyam, Al-Khwarizmi, and Ibn al-Haytham. After the Muslim conquest of Persia during the 7th century, Ancient Persian astronomy became intermeshed with that of the wider medieval Islamic World, with Persian scholars contributing heavily to the creation of advanced mathematical formulas to calculate the movement of the Sun and planets in our solar system and the positions of various heavenly bodies. Persian contributions to ancient Islamic astronomical sciences helped spark the broader flourishing of the sciences in the Islamic World from the 8th through 13th centuries.
Modern Iran’s space-based efforts have been subject to derision by some US officials, with now former United States Space Command chief John Raymond once ridiculing the Islamic Republic’s Noor (‘Light’) satellite as a “tumbling webcam in space” unlikely to provide any useful intel. Several months later, the Noor, operated by the Islamic Revolutionary Guard Corps’ Aerospace Command, sent back detailed snapshots of Al-Udeid Airbase, largest US military facility in the Persian Gulf region.
Iran repeated the feat in 2022, with the Noor-2 sending back a panoramic image centered on the headquarters of the US Fifth Fleet in Bahrain.
Dr. Meryl Nass sues Maine Medical Board over suspension, alleges Board violated her first amendment rights
By Brenda Baletti, Ph.D. | The Defender | August 17, 2023
Dr. Meryl Nass today filed suit against the Maine Board of Licensure in Medicine and its individual members, alleging the board violated her First Amendment rights and her rights under the Maine Constitution.
The complaint alleges the board engaged in retaliatory conduct against Nass, a practicing internal medicine physician and member of the Children’s Health Defense (CHD) scientific advisory board, when the board suspended her medical license for publicly expressing her dissenting views on official COVID-19 policies, the COVID-19 vaccine and alternative treatments.
“Because she was outspoken, the board targeted Dr. Nass as someone to silence,” her attorney, Gene Libby told The Defender.
In fall 2021, the board issued a position statement, quoted in the complaint, stating that licensees could face disciplinary action if they “generate and spread COVID-19 vaccine misinformation or disinformation.”
In October 2021, soon after the statement was issued, the board received a complaint alleging Nass was spreading misinformation online and soon after launched an investigation.
The board suspended Nass’ medical license on Jan. 12, 2022, without a hearing, accusing her of engaging in “unprofessional conduct” by spreading “misinformation about COVID-19.”
It also accused her of improperly prescribing hydroxychloroquine and ivermectin for three patients for off-label uses of those drugs.
The board suspended Nass’ license and ordered a neuropsychological evaluation, implying she was mentally impaired or a substance abuser and incompetent to practice medicine.
“There were no grounds to order a mental health examination,” Libby said. “That was simply a means to communicate to the public that there was something wrong with Dr. Nass, to discredit her and tarnish her reputation.”
After Nass moved to have the board dismiss its complaint against her, alleging First Amendment violations, the board on Sept. 26, 2022, withdrew its accusations of “misinformation”, just prior to her first hearing date, Oct. 11, 2022.
The board’s case now rests on Nass’ alleged non-adherence to the medical “standard of care” as it pertained to ivermectin and hydroxychloroquine for treating COVID-19 and on the alleged “record-keeping” issues.
Nass told The Defender :
“The two primary complaints against me were that my statements were misleading and that I was prescribing drugs off-label. My speech — which I should note, was not simply opinion, it was an educated opinion developed after consulting the medical literature — is protected by the First Amendment.
“And prescribing drugs off-label is a perfectly legal thing to do, as explicitly stated on the FDA [U.S. Food and Drug Administration] website. Somewhere between 20-50% of drugs are prescribed off-label. The lawyers on the board staff know all of this. It’s their job to know the law with respect to medicine.
“They didn’t do this because they thought I had committed some kind of violation. They did it because they thought I’m older and I wouldn’t have the money to challenge them and so they could get away with it — they thought they could turn me into a poster child to scare all the doctors in the country.
“It is part of this broader attempt by the U.S. government and governments across the world to criminalize dissent by criminalizing so-called ‘misinformation.’”
Libby said the remaining allegations against Dr. Nass “are simply a pretext to discipline her. Because now, from an institutional standpoint, the board has to do something. She’s been under suspension for 19 months, which is the longest suspension that I’m aware of for any physician in the state.”
The board refused to schedule hearings on Nass’ suspension on consecutive days. Instead, it has held one day of hearings every other month. There have been six days of hearings so far over 10 months — and Nass’ license has been suspended the entire time.
“This is fundamentally unfair to Dr. Nass, but she’s within the grip of an institution that doesn’t want her speaking out,” Libby said.
In her lawsuit, Nass alleges the board and its members used their power to “crush dissenting views and chill disfavored speech.”
Nass is asking the court for declaratory relief, for an injunction to stop the board from continuing to retaliate against her and for monetary damages and legal fees.
CHD is providing financial and legal resources to Nass’ Maine-based legal team.
CHD President Mary Holland told The Defender :
“CHD is proud to support Dr. Nass’ lawsuit against the Maine medical board and its individual members.
“The board and its members have deprived Dr. Nass of her license and livelihood for over a year with no basis whatsoever. This kind of censorship, intimidation and punishment of doctors of conscience must stop.
“People need independent, thoughtful, caring physicians like Dr. Nass to be honored, not hounded as the board has done.
“I am pleased to see this case move forward in the courts in the interests of justice, for Dr. Nass, her patients and the broader society.”
Board provided resources to ‘combat spread of vaccine misinformation’
The Maine board’s Fall 2021 position statement expressed its support for a statement by the Federation of State Medical Boards (FSMB) — a private organization with no regulatory authority — which threatened physicians “who generate and spread COVID-19 vaccine misinformation” with suspension or revocation of their medical license.
According to the statement, physicians have a high degree of public trust and therefore a responsibility to “share information that is factual, scientifically grounded and consensus-driven for the betterment of public health.”
The Maine board’s statement endorsed the FSMB statement, encouraged physicians to address misinformation when encountered, directed physicians to use circulated materials from the American Medical Association (AMA) and said that questioning the COVID-19 vaccine qualifies as “misinformation,” according to the complaint.
The AMA materials provide scripts, talking points and strategies for “combating the spread of vaccine misinformation.”
The Maine board’s chair, Dr. Maroulla Gleaton, is also an FSMB director.
Nass is a widely recognized expert on the anthrax vaccine and biological warfare. She testified before Congress six times and was quoted in major media outlets including The New York Times, The Washington Post, the Los Angeles Times and the Chicago Tribune.
She has also been a prominent critic of governmental handling of the COVID-19 pandemic, the suppression of effective treatments such as ivermectin and hydroxychloroquine and the safety and risks of the vaccine — all topics she has discussed in her Substack, on the radio, in interviews and elsewhere.
But, the complaint notes, her positions have been in conflict with those asserted in the position statement and the resources it highlights as “supporting the fight against COVID-19 misinformation.”
This was merely an attempt by the board to justify its decision to immediately suspend Nass and to intimidate her, the complaint alleges.
Board’s only concern was ‘silencing’ Nass and ‘branding her as crazy’
When Nass questioned the board’s authority to investigate a complaint unrelated to the practice of medicine and instead “focused entirely on a statement made in her private life,” the board responded, on Oct. 14, 2021, that she was engaged in “alleged unprofessional conduct” by provisioning “misleading and/or inaccurate” information.
In the January board meeting where the board decided to suspend her license, the conversation focused on Nass’ “unprofessional conduct due to the spreading of misinformation about COVID-19.”
The board also cited three matters related to treating patients, alleging Nass improperly diagnosed a patient “over the phone,” that she had provided misinformation to a pharmacist about why she was prescribing ivermectin for a patient, and that she had improperly issued another prescription.
On Sept. 7, 2022, Nass moved to dismiss the complaint, alleging the board was violating her First Amendment rights.
The board responded by withdrawing all charges based on her speech, retaining only the charges related to the treatment of three patients.
Libby told The Defender that through the entire investigation and hearings, the board never even spoke to the three patients. It did not inform them their medical records had been subpoenaed, or ask them about their treatment by Dr. Nass.
“Yet the remaining disciplinary charges are all predicated on Dr. Nass’ consultation with and advice to these patients.”
Libby called the patients to testify in Nass’ hearings. They all made “glowing comments” about her availability, her medical advice and her handling of their cases and expressed anger that Nass was being targeted by the board for their cases.
Libby said he interpreted this to indicate the board’s singular focus was not to ensure patient well-being, but rather “silencing Dr. Nass and attempting to brand her as crazy.”
According to the complaint, the board’s animus against Nass is also demonstrated by the fact that it is flouting its own rules for selecting and paying expert witnesses.
Board guidelines stipulate that witnesses can be paid a maximum of $125/hour for preparation and $175/hour for testimony and that the witnesses should have the same specialty as the practitioner in question and be licensed to practice in Maine.
But the board is paying Dr. Jeremy Faust, an emergency room physician from Brigham & Women’s Hospital in Boston, $500/hour to testify.
And board member Gleaton, who has conflicts of interest because of her position as FSMB director and has acted in openly mocking ways, has refused to recuse herself.
The next medical board hearing is set for mid-September.
But in the meantime, Libby said “The actions of the board are so outrageous, they need to be acted on legally.”
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
‘A Fauci Clone’: New NIAID Director Oversaw Remdesivir Trials, Has Ties to Biosafety Lab Research

By Michael Nevradakis, Ph.D. | The Defender | August 15, 2023
When he retired in December 2022, Dr. Anthony Fauci, then-director of the National Institute of Allergy and Infectious Diseases (NIAID) was the highest-paid federal employee and the recipient of the largest federal retirement package in history.
Fauci’s successor, Dr. Jeanne M. Marrazzo, will soon take over leadership of the agency — and its $6.3 billion budget.
Fauci praised Marrazzo, telling CNN, “She’s very well-liked. She’s a really good person. I think she’s going to do a really good job.”
But some of her critics, including medical and public health experts interviewed by The Defender, questioned Marrazzo’s suitability for leading NIAID, citing her limited experience as a medical practitioner and her role in supervising clinical trials of remdesivir, a controversial drug used to treat hospitalized COVID-19 patients.
Critics also called out her steadfast support for strict restrictions and countermeasures during the pandemic, and her receipt, since 1997, of more than $20 million in grants from the National Institutes of Health (NIH) and payments from Big Pharma — including from Gilead, the manufacturer of remdesivir.
And lastly, some pointed to Marrazzo’s key administrative role in a University of Alabama (UAB) institution which houses a BSL3 (biosafety level 3) laboratory that conducts gain-of-function research.
Before being named director of the NIAID, Marrazzo was director of the Division of Infectious Diseases at the UAB at Birmingham. She will replace Dr. Hugh Auchincloss, who has served as NIAID’s acting director following Fauci’s departure.
Commenting on the appointment, Brian Hooker, Ph.D., senior director of science and research for Children’s Health Defense (CHD), said:
“It looks like Dr. Marrazzo will give us more of the same, unfortunately. Her flip-flopping, penchant for Big Pharma, and support of draconian public health (control) measures mean that she’ll take a reactionary posture to any ‘pandemic threat’ and may be as gleeful as Fauci at the prospect of new pandemics.
“I have dim hopes that she may learn some lessons while the investigations into Fauci lying to Congress play out. However, these bureaucrats don’t really believe that the law applies to them.”
The NIAID is the second largest center at the NIH. According to CNN, it “supports research to advance the understanding, diagnosis and treatment of infectious, immunologic and allergic diseases,” as well as “research at universities and research organizations around the United States and across NIAID’s 21 laboratories.”
“Marrazzo fits the mold of every public health leader so far that has led the charge during the pandemic,” Dr. Kat Lindley, president of the Global Health Project and director of the Global COVID Summit, told The Defender.
Lindley added:
“My concern with Marrazzo is actually her Big Pharma ties, her lack of clinical experience with COVID-19 in particular, and her blatant ignorance on early treatment and support for unproven, scientifically debunked measures, in particular masking.
“Any scientist or physician should understand that masking has never proven to be effective and, in the case of children, even detrimental.”
Touted remdesivir as ‘silver bullet’ for treating COVID
During her tenure at UAB, the university served as one of the clinical trial sites for remdesivir, an antiviral originally developed by Gilead Sciences as a treatment for Hepatitis C and respiratory syncytial virus (RSV).
According to the NIH, the trial was intended “to evaluate the safety and efficacy of the investigational antiviral remdesivir in hospitalized adults diagnosed with coronavirus disease 2019.” Marrazzo supervised the UAB trial site.
UAB has long served as a research site for remdesivir. A February 2021 UAB report states, “Gilead entered into collaboration with the UAB-led Antiviral Drug Development and Discovery Center … to study remdesivir against coronaviruses” in 2014.
“These earlier studies enabled remdesivir to more quickly be tested and approved for human use as a treatment for COVID-19 when the 2020 pandemic struck,” UAB stated.
The trial results, published in the New England Journal of Medicine (NEJM) in November 2020, found remdesivir shortened “the time to recovery in adults who were hospitalized with COVID-19 and had evidence of lower respiratory tract infection.”
Fauci later praised remdesivir as the “standard of care” for treating COVID-19.
However, according to investigative journalist Jordan Schachtel, studies “show that there are zero clinical benefits to injecting patients with remdesivir. Many studies show that remdesivir can severely injure vital organs such as the heart and kidneys.”
Yet, Marrazzo never disclosed a conflict of interest when publicly commenting on remdesivir, Schachtel said. She described it as a “silver bullet” in remarks shared with The Washington Post in July 2020, and in tweets praising the drug.
“Given the UAB-Gilead partnership, one would think that Dr. Marrazzo would refrain from commenting on issues through which she maintained a clear conflict of interest,” Schachtel wrote. “She did no such thing.”
According to the U.S. government’s Open Payments database, Marrazzo received seven payments from Gilead, totaling $2,474.93.
But as Marrazzo repeatedly praised remdesivir — and, according to Schachtel, has “never shown remorse” for this despite mounting evidence of the harm it has caused — she has repeatedly spoken out against hydroxychloroquine for treating COVID-19.
In June 2020, in reference to a study published in the NEJM claiming hydroxychloroquine is ineffective in protecting people from COVID-19, Marrazzo said these findings “should provide a very big nail in the coffin” for the use of this treatment.
The following month, Marrazzo called a video that went viral on social media describing hydroxychloroquine as a cure for COVID-19 “very irresponsible and despicable,” adding that she was “glad that video is hopefully not being shared very much.”
In October 2021, she said hydroxychloroquine and ivermectin hold “special appeal” to the unvaccinated.
Yet, in April 2020, prior to the conclusion of the remdesivir clinical trial, Marrazzo said, “We are using it [hydroxychloroquine] in our hospital … for a range of patients including when patients are beginning to deteriorate,” adding:
“And lots of media folks are asking what we think about hydroxychloroquine. And the reality is that we live and die by the evidence. And one issue is the argument about whether it’s even ethical to use these treatments when we don’t have the evidence.
“But I would get back to the compassionate use argument. When you have a patient who’s dying, you have to use what you can, what’s available.”
Cheerleader for COVID vaccines and Merck’s molnupiravir
Marrazzo has also praised COVID-19 vaccines and therapeutics. In May 2020, she was “hopeful” about the Moderna COVID-19 vaccine clinical trial — despite its enrollment of only eight volunteers, saying “We don’t have the luxury of time here in this case.”
In August 2021, she called the U.S. Food and Drug Administration’s approval of the Pfizer Comirnaty COVID-19 vaccine “great news,” saying, “Vaccines are our best weapon against this disease” and are “working incredibly well to prevent severe disease” and reduce hospitalizations.
In January 2022, Marrazzo said “Vaccination makes the biggest difference” in fighting COVID-19, adding that “boosters, of course, are going to augment that protection.”
And in October 2021, Marrazzo praised molnupiravir, Merck’s antiviral pill for COVID-19, stating it had “extraordinary potential.” Results of a preprint study later showed the drug may fuel the development of new and potentially deadly variants of COVID-19.
Marrazzo has received five payments from Merck, totaling $8,820.
Cardiologist Dr. Peter McCullough told The Defender Marrazzo “has been willfully blind to the failure of COVID-19 vaccines” and “appears incapable of mastering the four pillars of pandemic response to lead America through the next pandemic: 1) contagion control, 2) early treatment, 3) late treatment and 4) vaccination.”
A ‘slap in the face’ to vaccine, hospital protocol victims
During the COVID-19 pandemic, Marrazzo made frequent television appearances in which, according to a UAB statement, she “helped inform the world … sharing critical information and perspectives.” UAB touted Marrazzo as a COVID-19 expert during this period.
According to AL.com, Marrazzo was on Alabama Gov. Kay Ivey’s COVID-19 task force, supporting “emergency public health measures that closed business and mandated mask wearing.”
In March 2020, Marrazzo supported “flattening the curve,” calling on the public “to make personal sacrifices for the greater good.” In similar statements made on May 8, 2020, Marrazzo warned of a “backslide” if measures like social distancing were loosened.
In June 2020, she said masks can “change the trajectory of this epidemic.”
In a June 2020 YouTube video, “Why you should wear a mask,” Marrazzo said, “Masks have contributed to the control of this pandemic in other communities.” She called for masks for schoolchildren over age 6 and included mask-wearing in a list of “Three basic rules” along with hand washing and social distancing.
In an article she co-authored and in which she highlighted “the intersection of the COVID-19, HIV, and STI pandemics,” Marrazzo drew parallels between wearing masks and wearing condoms, writing:
“Condoms reduce transmission of HIV and bacterial STIs effectively, if used adequately and consistently, but lack of access to condoms or perhaps even personal preference limits their utility.
“As a correlate to barrier protection, masking has proven effective to reduce the expulsion of SARS-CoV-2 and other respiratory virus droplets.”
The paper also repeated claims regarding the “lack of benefit” of hydroxychloroquine, zinc and vitamins C and D in treating COVID-19. Conversely, referring to the COVID-19 vaccines, the authors stated, “There were few serious adverse events in either arm, and there were no deaths related to the vaccine.”
Blaming the unvaccinated
In May 2021, she criticized loosened Centers for Disease Control and Prevention (CDC) recommendations that the vaccinated do not need to wear masks, stating that because less than 50% were vaccinated in her community, she would still wear a mask indoors despite being fully vaccinated herself.
In July 2021 she warned of a “summer surge” that would be fueled by the unvaccinated.
In December 2021 Marrazzo again scolded the unvaccinated. “Your decision to get infected is unfortunately not just going to be affecting you,” she said. “It’s going to be serving a source of incredible infectiousness going forward.”
Dr. Scott Atlas, a member of the White House Coronavirus Task Force during the Trump administration, told KUSI News San Diego that Marrazzo “was completely wrong about COVID … Pushing pseudoscience, pushing … her belief that vaccines stopped the spread of the infection, that children have high risk, and that masks were efficacious.”
“Marrazzo represents everything that was done wrong in the handling of COVID,” said Gail Seiler, Texas chairperson, Projects and Content, for the FormerFedsGroup Freedom Foundation and a survivor of the CDC’s COVID-19 hospital protocols, including administration of remdesivir.
Seiler told The Defender that Marrazzo advocated for no early treatment until the patient “worsened to the point of hospitalization,” and at that point to give remdesivir, “a drug that she profits from.”
Seiler added:
“Because of people like Marrazzo, patients in the hospital were given no hope of survival. Because of her ignoring the evidence, over a million people died who shouldn’t have.
“Her selection to the NIAID is a slap in the face to every family whose loved ones were killed by the protocols she profited from. And it exemplifies why the general public has lost trust in agencies such as the NIAID.”
Financial ties to Big Pharma
Marrazzo received a total of $20,405,337 in NIH grants for 67 studies between 1997 and 2023, according to NIH data. These grants ranged between $6,000 and $2.82 million and averaged over $304,000 per grant.
Open Payments data show Marrazzo has received $28,761,36 across 37 “general payments” and $152,208.42 across seven payments for “associated research funding,” including $18,636.59 in consulting fees, $4,500 in honorariums, and payments from companies such as Merck, GlaxoSmithKline, Gilead, Janssen and Abbott Laboratories.
In December 2018, Marrazzo participated in a panel titled “Role of the Genital Tract Microbiome in Sexual and Reproductive Health,” during the Keystone Symposia Conference in South Africa, which was “made possible with funding from the Bill & Melinda Gates Foundation.”
Her employer, UAB, received at least two Gates Foundation grants pertaining to health-related research in recent years. This includes a June 2021 grant, “Modeling Impact of Service Delivery Redesign” totaling over $1.5 million, and a $124,921 grant in April 2020 for a project titled “COVID-19 CTA: HTS Core for screening compounds.”
UAB’s Division of Infectious Diseases boasts “an active research portfolio with approximately $39 million in external research funding.” Research specialties include “Pathogenesis of viral infections,” “Antiviral therapy,” “Travel medicine and international health” and “Host defenses and infectious diseases in immunocompromised patients.”
Big supporter of gain-of-function research
UAB also houses a BSL3 research laboratory, the Southeastern Biosafety Laboratory Alabama Birmingham (SEBLAB), funded in part by NIH. According to UAB, it is “one of a limited number of institutions,” adding that the university ranks “among the top 25 in funding from the National Institutes of Health.”
The university states that SEBLAB researchers are “able to bring their skills to bear on the SARS-CoV-2 pandemic, and other issues directly relevant to biodefense and emerging infectious disease,” with a focus on NIAID “priority pathogens” and discovery of “new treatments to prevent or combat” diseases caused by infectious agents.
These projects have also included “Testing drugs on SARS-CoV-2,” a process involving growing the virus in SEBLAB. According to UAB researcher Kevin Harrod, Ph.D.,“We grow the viruses, measure them and provide them to the BARDA [the U.S. government’s Biomedical Advanced Research and Development Authority] contractor.”
BSL3 and BSL4 laboratories across the U.S. and the world have been associated with controversial gain-of-function research, which some have said is responsible for the development and subsequent alleged leak from one such facility, the Wuhan Institute of Virology in China, leading to prominent calls to end such research.
According to Independent Institute, “Marrazzo’s views on the origin of COVID-19 are hard to find,” as are her views on gain-of-function research.
Francis Boyle, J.D., Ph.D., a professor of international law at the University of Illinois who drafted the Biological Weapons Anti-Terrorism Act of 1989, told The Defender that Marrazzo’s selection signals that the NIH and NIAID have no intention of stopping gain-of-function research at BSL3 and BSL4 facilities.
Boyle said:
“They will have her in place to deal with the next pandemic that they know is coming out of their own BSL3 and BSL4 labs, just as Fauci dealt with the COVID-19 pandemic that came out of the Wuhan BSL4 and the University of North Carolina BSL3 and that Fauci and [former NIH Director] Francis Collins funded.
“Under her auspices NIAID will continue to research, develop, manufacture and stockpile every hideous type of Nazi biological warfare weapon known to humanity … There will be no end to it and to these death scientists like her … unless and until we stop them by criminal prosecutions.”
Boyle called Marrazzo a “Fauci clone, not an original and independent thinker,” adding, “The Bidenites and the globalists and Big Pharma behind them picked her to continue the Fauci/NIAID policies and programs across the board.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
YouTube Greatly Expands Its Medical “Misinformation” Policies
New rules, largely determined by the WHO
By Christina Maas | Reclaim The Net | August 16, 2023
YouTube, the titan of online video content, has expanded its Covid misinformation policy to cover what it calls all forms of medical misinformation.
YouTube has also declared its plan to delist videos promoting “cancer treatments proven to be harmful or ineffective,” effectively disallowing content creators from encouraging natural cures.
The platform pledges to implement its medical misinformation policies when a topic exhibits high public health risks, is supposedly prone to misinformation, and when official guidance from health authorities is accessible to the public.
The changes also see YouTube recommitting to groups such as the WHO and other health bodies on what information is deemed to be acceptable for people to talk about on the platform – despite these institutions having recently received major blows to their credibility.
According to the policy update, YouTube will no longer host content that:
- Misinforms about prevention techniques or contradicts current health authority guidelines, including inaccuracies regarding the safety or efficacy of approved vaccines.
- Promotes treatments that local health bodies or the WHO have neither approved nor recognized as safe and effective. Moreover, it bans content that advocates for harmful substances or practices that have been scientifically proven to be detrimental.
- Denies the existence of specific health conditions.
As stated in its blog post, YouTube intends to punish content promoting not only what it believes to be overtly harmful treatments but also unproven ones that are audaciously offered as replacements for recognized alternatives.
For instance, influencers suggesting vitamin C supplements or garlic for cancer may have their content removed, the post states.
This marks a substantial escalation in the Google-owned platform’s ongoing crusade against what it believes to be the dissemination of medical misinformation, heavily catalyzed by the controversial experience of battling narratives about themes such as COVID-19 and vaccines, something YouTube was heavily criticized for as truthful content ended up being censored on the platform.
YouTube had targeted vaccine “misinformation,” such as demonetizing and deleting vaccine skepticism, thereby refining their approach in response to the global pandemic situation.
Doubt in Denmark
Another progressive country is having second thoughts about paediatric gender transition
BY BERNARD LANE | GENDER CLINIC NEWS | AUGUST 13, 2023
Denmark has taken a step towards caution in gender care by offering a form of counselling rather than medical treatments to the main patient group of teenagers with no childhood history of distress in their birth sex.
Official acknowledgment of a change in treatment policy was given on May 31 by the Liberal Party Health Minister Sophie Løhde during parliamentary debate of an unsuccessful resolution seeking a total ban on medical transition of minors.
Ms Løhde said that medical treatment at the Danish central gender clinic in Copenhagen—the Sexology Clinic—would only be offered “if the child or young person has had gender dysphoria since childhood.”
“If the gender dysphoria has started in connection with puberty, the young person may, among other things, be referred to a process of reflection or clarification,” she said.
“This process is often finalised without medical treatment, as the indication for treatment is not considered present.”
The dominant patient profile internationally is adolescent-onset dysphoria, chiefly affecting females, but the (limited and contested) evidence base for puberty blockers and cross-sex hormones for minors mostly derives from past studies of classic early childhood-onset dysphoria typically among males.
Gender distress that appears at or after the onset of puberty, often following online immersion and transgender identity declarations among school friends, is commonly referred to as Rapid-Onset Gender Dysphoria (ROGD) following the 2018 preliminary study of American public health researcher Dr. Lisa Littman.
Dr. Littman’s work is well known in Nordic countries. Sweden’s National Board of Health and Welfare last year referenced her 2021 detransitioners study and declared that the very low rate of treatment regret claimed by youth gender clinics “no longer stands unchallenged”.
Sweden and Finland are the most advanced in the post-2019 Nordic shift to caution, while health authorities in Norway are under pressure after the country’s independent healthcare investigation agency declared in March that medicalised gender change for young people was “experimental” and should be confined to clinical trials.
Systematic reviews of the evidence base undertaken in Finland and Sweden showed it to be weak (as did reviews in the United Kingdom).
“[Although in Denmark’s parliament] the issue of gender reassignment for children and other identity policy topics seems strongly divided into blocs, we feel that this is by no means the case in the general population, when the seriousness of the matter finally dawns on people. Many simply did not know that this was happening”—Danish Rainbow Council post, 2 March 2023
Denmark’s point of difference is that the call for an end to medical transition of minors is being spearheaded by a mainstream LGBT group, the Danish Rainbow Council, launched in 2022 under the leadership of transsexual Marcus Dib Jensen. The organisation is pledged to child safeguarding and recognition of gender dysphoria as a mental disorder, while opposing the extremes of gender ideology.
In May’s parliamentary debate, Minister Løhde faced pointed questions on gender medicine from politicians Mette Thiesen and Mikkel Bjørn, both members of the populist Danish People’s Party.
The minister presented the treatment policy change as an evolution influenced by developments in the field and clinical judgment. She was not specific about which medical treatment was being withheld from patients with adolescent-onset dysphoria (or ROGD), nor the timing of the policy change.
She noted that the Sexology Clinic had “become more reluctant to offer hormone treatment” to young people.
“This reluctance manifests itself particularly regarding young people with gender dysphoria that arises in connection with puberty.
“I think it is a positive thing that there is [such] a response to research and experience… both in Denmark, but also abroad, which we must follow closely. And this knowledge and experience lead to adjustments in the current treatment options.”
The group LGBT+ Danmark, whose slogan is “Global Queer Solidarity” and which campaigns for “better gender-confirming treatment”, told GCN that the minister’s remarks referred not to a change in general treatment guidelines but to “an adjustment in the practice” of the Sexology Clinic last year.
GCN put questions to the clinic and to Denmark’s health ministry.
Video: “You can be uncomfortable with reality, but it doesn’t change reality”—Marcus Dib Jensen, chairman of the Danish Rainbow Council
Big change
A recent commentary article on the minister’s remarks posted by the Danish Rainbow Council’s deputy chairman Jesper W. Rasmussen said:
“It is important to understand how significant it is that as many as 80 per cent of the children who previously underwent gender reassignment surgery will now, in the minister’s own words, no longer be able to undergo this controversial, irreversible treatment.
“Since [the minister’s comments], we have received several emails from relieved parents of ROGD children, and in the coming months we will keep a close eye on whether these children continue to be free from hormonal sex reassignment.
“We will do this by regularly requesting access to the treatment statistics from the Sexology Clinic [at the specialist hospital Rigshospitalet].”
The resolution for a total ban, put up in March by the populist New Right party after all other members of parliament had ignored apolitical appeals from the rainbow council, was not expected to pass in the government-controlled chamber.
But the council argued that the result was significant because public debate had been unleashed and the authorities were put under pressure.
The council suspected that the de-medicalisation of adolescent-onset (or ROGD) cases had been enacted without formal announcement in 2022, thereby explaining a sharp decline that year in the number of minors undergoing hormonal treatment.
Roughly 80 per cent of the 341 minors who had undergone medicalised gender change from 2015 to 2022 were believed to be in the ROGD category, the council said.
Since 2015, when Ms Løhde was also health minister, minors have been able to undergo irreversible medical gender reassignment without parental consent from the age of 15.
“A top [American] pediatric psychiatry organization has nixed at least three panels with leading European psychologists about Europe’s move away from chemical interventions for children with gender dysphoria, raising questions about the politicization of American medicine and underscoring a clinical divide between the United States and much of the world”—Aaron Sibarium, news report, The Washington Free Beacon, 11 August 2023
Future unknown
In 2021, Sexology Clinic consultant Dr. Mette Ewers Haahr gave an interview to the Dagbladet Information media outlet in which she acknowledged “a lack of research” relevant to today’s mostly teenage female patients and her concerns about why these girls wanted to change gender.
“We see that treatment helps young people in the short term. But we lack knowledge about what happens in ten and 20 years. Or when they want to have children. What happens when they fall in love and start to have an active sex life?” Dr. Haahr said.
“Transgender young people assigned female have, for the most part, no active sex life. Not even with themselves. How will their sex life develop and does this affect their perception of their gender? We have sometimes seen in young people that gender and sex life interact and change together.”
Dr. Haahr’s comments about the weak evidence base prompted the rainbow council to ask why the authorities had allowed such a confident regimen of paediatric transition to begin in 2015.
“As adults, we must dare to step up and say stop this madness. We castrate and sterilise children and physically destroy their otherwise healthy bodies to alleviate a psychological discomfort that is usually temporary and, if not, can be treated with a sex change on the other side of puberty,” the council’s June 2 comment said.
No surgery on minors
In May’s parliamentary debate, Minister Løhde also said that under new referral guidelines, it would no longer be permissible to offer transgender surgery such as mastectomy to children under age 18—“an option that, by the way, has never been used in Denmark.”
She said the country’s “entire guidance on health care for individuals with gender identity issues” was being reviewed.
GCN asked the Danish Health Authority if a systematic review of the evidence base would be undertaken.
A spokeswoman for the authority said: “We are in the process of updating the existing guideline and we will consult leading experts in that revision.”
In a post on a Danish study dealing with trans identity and suicide attempts, the Society for Evidence-Based Gender Medicine (SEGM) said:
“It remains to be seen whether the Danish Health Authority will take a cautious approach to the treatment of gender-dysphoric youth like the growing number of their European counterparts, or whether Denmark will choose to align with the current direction supported by a number of U.S. medical societies that assert that medical gender transition should be widely available for all youths who desire it.”
Copenhagen psychotherapist and former teacher Lotte Ingerslev, who writes the blog Transgender: the Fine Print and is a member of SEGM, told GCN that the Danish health minister’s May 31 remarks were “very, very important.”
She said the minister had represented this policy shift “as simply a result of the doctors ‘following the evidence’, and not a complete and utter break with their previous approach.”
Ms Ingerslev said this appeared to be a government tactic for “evading responsibility for the utter disregard for children’s bodies and lives.”
Nonetheless, she said the policy change meant “that teenagers will no longer be able to expect to get hormones as a quick fix for their loneliness, autism or inner homophobia.”
But she said these concessions to caution by the government and the Sexology Clinic were not enough and “the transing of children needs to be stopped completely.”
“Otherwise, the general public, schools, day-care centres and parents of gender-non-conforming children get a message from the state saying that gender-non-conformity is a sign that a child is ‘trans’, which goes against all evidence,” she said.
Opt-out females
In her 2021 media interview, the Sexology Clinic’s Dr. Haahr wondered aloud about why female patients are disproportionately represented in gender clinic caseloads.
She worried that for some girls, transition was more about “opting out of the feminine than opting into the masculine”, and more to do with physical discomfort than a different gender identity.
“When the birth-assigned girls reach puberty and their bodies change, some of them start to have these thoughts. Maybe the outside world has started to react differently to them because their bodies are suddenly sexualised,” Dr. Haahr said.
“They may not get as much speaking time, they’re belittled if they take up too much space, and certain girl things are expected of them that they can’t identify with. And then they feel really, really bad about their feminine bodies.
“Unlike the children [with early-onset dysphoria], who have experienced themselves as a different gender for as long as they can remember, we see that some of the [teenage] girls… have only had these thoughts for six months and are determined that they need body modification treatment. And then it becomes really difficult to figure out what it’s all about and what the right thing to do is.”
She said she paid particular attention to whether these girls had suffered traumatic experiences such as bullying, assault or sexual abuse.
“Abuse during adolescence and childhood can lead to alienation from one’s body. That’s where we need to be extra vigilant.”
She said today’s teenage female patients sometimes used formulaic language seemingly not their own when explaining why they wished to transition—it was like “listening to them read from a Facebook manual”.
She defended Dr. Littman’s 2018 ROGD study, which generated an international backlash from “gender-affirming” clinicians and trans activists, as well as pressure for the journal to issue a “correction” which in fact left the Littman hypothesis unchanged.
Dr. Haahr’s gender clinic colleague, chief physician Astrid Højgaard dismissed the ROGD hypothesis and objected that right-wing groups were enthusiastic about the idea of trans social contagion.
But Dr Haahr said:
“It is not my impression that Littman has done the research to appease the right wing or because she is transphobic, but because she thought the phenomenon should be studied.
“I think that if we can’t talk about this very large increase in the number of birth-assigned girls seeking to change their bodies during puberty, then it’s going to be a problem for all transgender people in the future.”
Featured Video

Ian Proud: Economic Reset with Russia to Save Europe
or go to
Aletho News Archives – Video-Images
From the Archives
Magic Hour for Gates
By Gary Jordan | Wake The F*** UP | March 15, 2021
Bill Gates wants to know everything about you.
He wants to control every aspect of your life.
His insatiable thirst for the supervision and scrutiny of every human being alive has sparked a US$1 billion investment that will blanket the earth in video surveillance satellites, providing real-time feedback with a mere one-second delay. He advocates for Orwellian digital tools to track your every move and has bankrolled US$1.7 billion to provide artificial intelligence that will be used to scan each and every visitor to major event venues worldwide. He wants to do away with end-to-end encryption, so he can snoop on your private conversations. He wants to know when and where you travel and who you travel with. He wants you to eat whatever he says you should eat, drink whatever he says you should drink, think how he wants you to think and know only what he wants you to know. Plus he wants to dictate what goes inside your body.
But he doesn’t want you to know a lot about him.
For instance… continue
Blog Roll
Recent Comments
 Aletho News
Aletho News- Keir Starmer-tied think tank paid PR firm to target The Grayzone
- ‘Israel’ threatens to genocide Gaza if Hamas refuses disarmament
- Apple Just Bought A Sinister ‘Pre-Speech’ Tech Company Implicated In Genocide
- Israel’s new West Bank registration process declares Palestinian land ‘state property’
- Two children killed in Palestinian Authority ambush in West Bank; Hamas slams attack as ‘black mark’
- Israel Needs Time Before Another Iran War—Here’s Why
- US seizes oil tanker for ‘defying Trump’s quarantine’
- Ian Proud: Economic Reset with Russia to Save Europe
- Senator Rand Paul Introduces Federal Bill to END Vaccine Makers’ Liability Shield
- The Hidden Map: US and Israel May Use Unexpected Neighbors to Attack Iran
- If Americans Knew
- In Gaza, “rats run over our faces” – Not a ceasefire Day 129
- Israel-backed border guards, GHF-linked aid – Not a ceasefire Day 128
- Israel battles Palestinian right of return, one Palestinian at a time – Not a ceasefire Day 127
- Noor’s short life of unimaginable suffering
- Israel Destroyed Gaza’s Hospitals. Now It’s Banning Doctors Without Borders.
- Is Spite of What Zionists Say, It’s a Good Thing to Criticize Governments
- Palestinian mother, daughter recount strip searches, harsh conditions in Israeli detention
- Israel used weapons in Gaza that made thousands of Palestinians evaporate
- ADL’s Stats Twist Israel’s Critics Into Antisemites
- Why Is the World Silent When the Gaza Genocide Is Not Over?
- No Tricks Zone
- New Study: A 4°C Warmer Beaufort Sea Had ‘No Sea Ice’ 11,700 – 8200 Years Ago
- Unfudging The Data: Dutch Meteorological Institute Reinstates Early 20th Centruy Heat Waves It Had Erased Earlier
- German Gas Crisis…Chancellor Merz Allegedly Bans Gas Debate Ahead of Elections!
- Pollen Reconstructions Show The Last Glacial’s Warming Events Were Global, 10x Greater Than Modern
- Germany’s Natural Gas Storage Level Dwindles To Just 28%… Increasingly Critical
- New Study Rebuts The Assumption That Anthropogenic CO2 Molecules Have ‘Special’ Properties
- Climate Scientist Who Predicted End Of “Heavy Frost And Snow” Now Refuses Media Inquiries
- Polar Bear Numbers Rising And Health Improving In Areas With The Most Rapid Sea Ice Decline
- One Reason Only For Germany’s Heating Gas Crisis: Its Hardcore-Dumbass Energy Policy
- 130 Years Later: The CO2 Greenhouse Effect Is Still Only An Imaginary-World Thought Experiment
