NEW VARIANTS TRIGGER CALLS FOR RETURN TO LOCKDOWNS
The Highwire with Del Bigtree | August 24, 2023
Mass media is calling for the reinstitution of COVID restrictions due to new variants, with no conversation about the efficacy or the harm they’ve caused. Jefferey Jaxen connects all the dots, which appears to be pointing to a Pandemic 2.0.
Fauci declares lockdowns were ‘absolutely justified’ and suggests they should be used again to force vaccinations
Retired government bureaucrat says that tragedy in Maui was due to climate change
By Jordan Schachtel | The Dossier | August 22, 2023
Recently retired government bureaucrat Anthony Fauci just appeared at a university virtual event titled, “Pandemic Lessons and Role of Faculty in Pandemic Preparedness with Dr. Anthony Fauci.” During the conversation, Fauci, who is now affiliated with Georgetown University, made it clear that he still supports locking down society in the name of a virus, adding that lockdowns are a great tool to forcibly “vaccinate” people.
I’ll save you 40 minutes of your life and quote some of the “highlights” from the interview, in which a Wayne State University professor asks Fauci about what he’s learned from his time overseeing a “pandemic response.” The video of the chat is available via YouTube below:
Fauci falsely claimed that New York City was overrun and had “cooler trucks outside because they had no places to put the bodies.”
“You had to have something to immediately shut down the tsunami of infection,” he states, adding, “that lockdown was absolutely justified.”
“Lockdown has a purpose,” the pseudoscientist continued. “One of the purposes, if you don’t have a vaccine, it’s to get more ventilators, get the hospitals better prepared … until you decompress the pressure on the hospitals.
Fauci wasn’t done yet. Here comes the truly evil insanity…
“If you have a vaccine available, you might want to lock down temporarily so you can get everybody vaccinated,” he suggests.
Rejecting the idea that lockdowns are a moral question, he added that “lockdowns have a place, but they are not a permanent solution.”
The conversation continued, with the longtime NIAID chief declaring that “climate change” is “playing a role” in causing outbreaks.
He then calls for an “international commitment to decrease the carbon imprint in society so you don’t have the kinds of crazy weather we’re having in this country.”
Yes, that’s a real quote.
He went on to blame the tragedy in Maui on climate change. “It’s completely, really amazing what’s happened with climate change,” he concludes.
‘Unvaccinated’ Does Not Mean Unprotected
The False Claims (Pseudoscience) Provided by Governments and Doctors over the Last Three Years
By Judy Wilyman Phd | Vaccination Decisions | August 24, 2023
Not only are you not unprotected due to natural immunity if you did not get the COVID injections, but the COVID injections were NOT vaccines. Therefore, you are also not ‘unvaccinated’ or an ‘antivaxxer’. Here are the reasons why the genetically engineered COVID injections were NOT vaccines:
Question 1: How can a synthetic (man-made) drug be claimed to be ‘safe and effective’ or that the benefits far outweigh the risks, without this long-term data?
Question 2: Why did governments claim that it “would prevent people getting COVID disease” from the beginning of the roll out, when it was never tested in clinical trials, to see if it prevented COVID disease?
Welcome to the first Vaccination Decisions Substack. I have been writing newsletters for over a decade attempting to provide the knowledge that people need to understand the influence of the pharmaceutical companies and the UN’s World Health Organisation (WHO), in the Australian government’s decisions on public health policy.
This became necessary because the diversity of media ownership laws in Australia were removed over the last two decades, and this has led to a lack of independent vaccine information being provided to the general public.
Democracy only exists when the people can hold their government to account. This ability is removed once there is a lack of independence in the media. In Australia we have a corporate-sponsored media that is ~80% owned by Murdoch News Corp.
In this situation reality can be inverted as you have seen over the last three years: black becomes white due to the mis- and disinformation presented when governments collaborate with a corporate-sponsored media to control the information you receive. This is also described as public-private partnerships. Australia’s politicians are heavily influenced by corporate lobby groups, financial bonus’s and being required to present the government narrative through party policy.
Australia is in a Pre-Police State (Independent, Andrew Wilkie, Australian Parliament 10th September 2015)
Currently, the Australian government is attempting to further this censorship by pushing through new legislation in the Australian Communications and Media Authority (ACMA) Amendment (Mis and Disinformation) Bill 2023. This bill will allow the government to continue promoting the medical fraud that the UN/ WHO is directing (with financial incentives) to all member countries in global health policies.
There is a clause in this ACMA amendment bill that exempts politicians from being censored for the mis or disinformation that they provide on social media platforms. This legislation will completely remove the façade of democracy that still exists in Australia.
I have provided below a list of some of the false claims that governments and the medical-industry have made over the last three years that are now putting global populations at risk. It is time for everyone who has this knowledge to stand up visibly for the truth to ensure that ethics and principles can be restored to our society and institutions.
“If we lose courage we lose the truth and without the truth there is no other virtue” (Sir Walter Scott).
The False Claims Provided by Governments and the Medical industry in 2020-22:
- Humans would not have any natural immunity to this new mutated Coronavirus 2019 (False). (The family of Coronaviruses cause the common cold, so the correct assumption is that we would have some natural immunity to a new mutation).
- The PCR test can be used in people without symptoms to diagnose COVID disease (False). (It is a supportive tool and can only be used to assist in diagnosis when someone has symptoms. The PCR test is being misused and misinterpreted).
- A healthy person can be diagnosed as an ‘asymptomatic case of disease’ using a PCR test (False). (A PCR test cannot be used to diagnose disease in people without symptoms: finding a virus in a person does not indicate they will ever get a disease because viruses only cause disease symptoms if there is a poor environment (terrain). A healthy person should never be classified as a ‘case of disease’ and isolated from society).
- An ‘asymptomatic infection’ is a ‘case of disease and a ‘risk to the community’ (False). (This is an infection without symptoms and can only be identified with an antibody test (not a PCR test). A positive antibody test shows you have gained natural immunity to an infection without any disease symptoms. You are not a risk to others and healthy people should never be tested to see if they have a respiratory virus. There are hundred’s of viruses that cause ‘flu-like symptoms’.
- Flus and colds disappeared in 2020-22 (False). (They were re-classified as a new disease called ‘COVID’ based only on a PCR test that was misused in healthy people. The diagnosis was not based on symptoms, or systematic testing for any other virus, bacteria or medication that cause the same symptoms).
- These COVID mRNA injections are ‘vaccines’ (False). (They are genetically-engineered modified mRNA drugs until they are proven to prevent disease and that the benefits far outweigh the risks).
- COVID ‘vaccines’ would prevent you getting COVID disease (False). (These genetically-engineered COVID injections were never tested to see if they prevent COVID disease and they are causing COVID disease.
- COVID ‘vaccines’ would reduce the severity of COVID disease (False). (Hospitalisations and Deaths increased when the COVID injections were implemented in 2021-22 and UK data also shows that 92% of alleged COVID deaths were triple vaccinated).
- COVID ‘vaccines’ are ‘safe and effective’ (False). (Many deaths and illnesses were recorded in the short-term trials and in post-marketing surveillance).
- Adverse events are ‘rare’ (False). (How can they be claimed to be ‘rare’ when the injections had not been studied in the genetically diverse population when they were marketed in 2021?).
- The COVID ‘vaccines’ stimulate the immune system to produce a ‘Coronavirus spike protein’ (False). (They stimulate the immune system to produce a recombinant synthetic (man-made) protein that is foreign to our bodies and is being called a ‘spike protein’. This foreign protein can result in autoimmune diseases such as Multiple Sclerosis, Lupus, Chronic Fatigue Syndrome, Arthritis, Diabetes, Graves Disease, Guillain Barre Syndrome etc.
The book “Slaying the Virus and Vaccine Dragon” by John O’Sullivan et el, exposes the psychological strategies that were used by governments (directed by the WHO’s public-private partnerships) to predict and manipulate a global ‘pandemic’ based only on an industry-designed mathematical model that had hidden assumptions about viruses and vaccines. (Book Review).
References exposing these false government claims are:
1. Dr. Paul Marik, the Truth about the Shots
2. The mRNA Vaccines are Neither Safe Nor Effective
3. Pfizer, FDA, CDC Hid Proven Harms to Fertility from Vaccine Ingredients.
The Royal Society Lockdown Report Authors Understand That by Ignoring the High Quality Evidence they Reach the Politically Acceptable Conclusion
BY DR CARL HENEGHAN AND DR TOM JEFFERSON | THE DAILY SCEPTIC | AUGUST 25, 2023
This week saw the publication of a suite of systematic reviews by the Royal Society (RS) on the effect of non-pharmaceutical interventions in the pandemic.
Politico headlined with ‘Top review says Covid lockdowns and masks worked, period’. The Guardian led with ‘Lockdowns and face masks “unequivocally” cut the spread of Covid, report finds’, and the i newspaper stated: ‘Masks and social distancing did reduce Covid infections, new report shows, proving lockdown sceptics wrong.’
So there you have it, a slam dunk, sceptics, you were all wrong. You should have masked up and stayed in lockdown.
Even more so when you listen to the Chair of the report’s group, Mark Walport, who said: “There is sufficient evidence to conclude that early, stringent implementation of packages of complementary NPIs was unequivocally effective in limiting SARS-CoV-2 infections.”
Four systematic reviews informed the effectiveness of non-pharmaceutical interventions in the Covid pandemic. However, here is some of what these reviews report.
A systematic review on environmental control measures:
Many of these studies were assessed to have critical risk of bias in at least one domain, largely due to confounding factors that could have affected the measured outcomes. As a result, there is low confidence in the findings.
One study, an RCT, showed that daily testing of contacts could be a viable strategy to replace lengthy quarantine of contacts. Based on the scarcity of robust empirical evidence, we were not able to draw any firm quantitative conclusions about the quantitative impact of TTI interventions in different epidemic contexts.
Effectiveness of face masks for reducing transmission of SARS-CoV-2:
We analysed 35 studies in community settings (three RCTs and 32 observational) and 40 in healthcare settings (one RCT and 39 observational). Ninety-one percent of observational studies were at ‘critical’ risk of bias (ROB) in at least one domain, often failing to separate the effects of masks from concurrent interventions.
Effectiveness of international border control measures during the COVID-19 pandemic:
There is little evidence that most travel restrictions, including border closure and those implemented to stop the introduction of new variants of concern, were particularly effective.
The report makes the same errors that the UKHSA and Public Health England did. They ignored the critical biases and the confounders when drawing conclusions. Some of the comments misunderstand the evidence required for making healthcare decisions.
Chris Dye, Professor of Epidemiology at the University of Oxford, who led the review on masks for the Royal Society, said if they had only looked at randomised controlled trials, they would have come to the same conclusion as the Cochrane review. However, the researchers behind the paper released Thursday chose to analyse a larger body of studies and found strong evidence that masks work.
So, if we ignore high-quality evidence, we arrive at the conclusion we want – they fully understand the politics. Low-quality evidence means the estimated effect will differ substantially from the actual effect – we’ve known this for quite some time, and it is fundamental to the delivery of evidence-based interventions. An approach that uses low-quality evidence shouldn’t inform healthcare, and it doesn’t. That’s why we have NICE, which uses the best available evidence to develop recommendations that guide health, public health and social care decisions.
Did the reviewers, for instance, ask if there was a protocol for any of these studies – something we have previously pointed out. There were none, despite protocols being essential for robust research.
There is something we do agree with in the report, that the “future assessments should also consider the costs as well as the benefits of NPIs, in terms of their impacts on livelihoods, economies, education, social cohesion, physical and mental wellbeing, and potentially other aspects”. However this report looked at none of that. The single focus on one outcome, ignoring harms, further hinders informed decision-making.
The RS report wants us to believe that RCTs are impossible during a pandemic: “While RCTs should not be discounted, it is highly likely that most information in a future pandemic will continue to be observational.”
Yet the pandemic has re-emphasised the importance of high-quality randomised clinical trials and highlighted the need for preparation, coordination and collaboration.
The Royal Society review shows that some academics are losing their ability to think critically. Instead of retrofitting evidence to preconceived conclusions, it would be much better to report the uncertainties and set out those questions that need addressing. Refusal to acknowledge uncertainties does a disservice to society and undermines public trust in research.
Staying at home decreases your risk of all sorts of hazards – in the short term, you won’t get run over and you’ll reduce the risk of an infection or an accident. But what matters is the costs of what happens when you reemerge.
The Digital Services Act Will Give the EU Sweeping New Censorship Powers, Forcing X and Facebook to Remove Content that Challenges Mass Migration, Transgender Ideology or Net Zero
BY DR FREDERICK ATTENBOROUGH | THE DAILY SCEPTIC | AUGUST 25, 2023
The European Union’s Digital Services Act (DSA) comes into force today, obliging “very large online platforms” to swiftly take down what unelected European Commission bureaucrats decide to define as ‘disinformation’.
As Laurie Wastell points out in the European Conservative, the DSA obliges online platforms to swiftly take down so-called disinformation. From today, the EC has at its disposal an aggressive enforcement regime, such that if Big Tech companies fail to abide by the EU’s ‘Strengthened Code of Practice on Disinformation’, which requires swift censorship of mis- and disinformation, then they can be fined up to 6% of their annual global revenue, investigated by the Commission, and potentially even prevented from operating in the EU altogether.
So, who is to say if something is misinformation? In the case of social media platforms operating within the EU, the EC is the arbiter of that, since it is the Commission that will decide if platforms like X and Facebook are doing enough to combat it. (It is the EU’s executive body, the EC, that is invested by the DSA with the exclusive power to assess compliance with the Code and apply penalties if a platform is found wanting.)
And what kind of speech is the DSA expected to police? The Code defines disinformation as “false or misleading content that is spread with an intention to deceive or secure economic or political gain and which may cause public harm”. That sounds innocent and apolitical enough. Yet the European Digital Media Observatory (EDMO), which was launched by the EC in June 2020 and aims to “identify disinformation, uproot its sources or dilute its impact”, appears to adopt a much broader, deeply politicised understanding of the term “misleading content”.
Consider, for instance, some of the key “disinformation trends” listed in the EDMO’s recent 2023 briefing on disinformation in Ireland. They include “nativist narratives” that “oppose migration”, “gender and sexuality narratives” that touch on drag queens and trans issues as “part of a wider ‘anti-woke’ narrative that mocks social justice campaigns”, and “environment narratives” that criticise climate-change policies and Greta Thunberg.
Clearly, what is common to such narratives is not that they constitute disinformation in the sense outlined in the Code — that is, “false information intended to mislead”. Rather, they represent opposition by members of the public to unpopular policies favoured by European elites — in this case, mass migration, transgender ideology and Net Zero.
In the words of EC President Ursula von der Leyen, it is vital that companies censor disinformation of this kind to “ensure that the online environment remains a safe space”. Safe for whom, one wonders — politicians or citizens?
Well worth reading in full.
Dr. Frederick Attenborough is the Communications Officer of the Free Speech Union.
Free Speech Union Highlights New Risk to Free Speech in the Workplace: Carbon Literacy Training
BY TOBY YOUNG | THE DAILY SCEPTIC | AUGUST 25, 2023
The Free Speech Union has just published a briefing on carbon literacy training by Thomas Harris, its Director of Data and Impact. The FSU is concerned that it will have a chilling effect on free speech in the workplace in the same way that unconscious bias training and anti-racism training does, with employees reluctant to challenge the ideas behind it for fear of jeopardising their careers.
Carbon literacy training is spreading rapidly across UK offices and places of study, with over 67,000 citizens certified as ‘carbon literate’ according to the Carbon Literacy Project (CLP), the main organisation behind the initiative. (Between financial year-end September 2021 and September 2022, CLP’s income grew from £183.8k to £637.7k, an increase of nearly 250%.) The training takes it for granted that we’re in the midst of a ‘climate emergency’ and recommends that employees embrace various radical solutions, including net zero.
The Free Speech Union is concerned that this training is embedding a particular orthodoxy about climate change in British workplaces, leaving employees feeling unable to challenge it. While it’s indisputable that average global temperatures have increased since the mid-19th Century people hold a range of views about the causes and severity of climate change and that in turn influences their opinion about the best way to tackle it – or, indeed, whether tackling it is possible or necessary. Different solutions to the problems created by climate change are informed by different values and recommending one approach over another inevitably involves making a political choice. There is no-such thing as an apolitical, ‘scientific’ solution. Consequently, employees should not be put under pressure to endorse a particular approach or threatened with disciplinary action if they fail to adjust their behaviour to follow this approach, particularly in their private lives.
In those companies seeking accreditation as a ‘Carbon Literate Organisation’ (CLO), up to 80% of staff are expected to become ‘carbon literate’. Carbon literate accreditation requires employees to embrace a particular view about climate change and identify at least one action they can take to reduce their own carbon footprint, as well as at least one action involving other people. The FSU fears that employees may be penalised if they refuse to comply with these requirements because they do not share a particular point of view.
The FSU first became aware of this new threat to free speech in the workplace when it was contacted by a member who is concerned about his career after he challenged the carbon literacy training provided by his employer. The FSU believes he was right to be concerned. To secure CLP’s platinum, gold, and silver CLO accreditation, companies are expected to embed carbon literacy in the annual targets of staff members and evaluate their performance accordingly. This means that employees who don’t subscribe to a particular view on climate change could find themselves missing out on pay awards or promotion unless they self-censor or pretend to hold convictions they don’t have.
If you’re being forced to undergo carbon literacy training in your workplace and are worried you might get into trouble for challenging the climate activist agenda behind it, you can contact Thomas Harris at the Free Speech Union here. And if you’re not already a member of the FSU, you can join here.
Kaiser Family Foundation Finds Many Believe COVID-19 Mass Vaccination Responsible for Sudden Deaths
Poll Statistics Reveal America Waking Up to Immunization Debacle
By Peter A. McCullough, MD, MPH | Courageous Discourse | August 23, 2023
The Kaiser Family Foundation is a pro-vaccine organization that has an biased polling system aimed at showing satisfaction and benefit of mass vaccination among other family issues. The May 23 through June 12, 2023 poll reveals some shocking new data. A substantial minority of Americans believe the COVID-19 vaccines have caused great harm. Here are the results.
![]()
As you can see it is roughly a third of Americans are awake and understand the COVID-19 vaccines have failed, cause great harm, and pose a giant safety risk to Americans. It is also interesting to note a quarter of respondents have been awakened to the link between childhood hyper vaccination and autism spectrum disorder. I wonder what the actual sentiment is on vaccines if Kaiser had asked the questions in a more unbiased manner and did not load up their survey with charged words such as “false” and “misinformation”.
Those Doctors Calling for Spreaders of Covid Misinformation to be Punished Should be Careful What they Wish For
Many of their Claims – that the Vaccinated Couldn’t Infect Others, For Instance – Turned Out to be False
BY NIGEL WILSON | THE DAILY SCEPTIC | AUGUST 24, 2023
The Journal of the American Medical Association recently published a review of alleged ‘misinformation’ about COVID-19 that physicians were responsible for, either on social media and in other news sources.
In the paper, the corresponding author, Dr. Sarah L. Goff, MD PhD, defined misinformation. She surveyed social media platforms and news sources for anything written by other physicians that fits her selected examples of both. She then proposes that physicians guilty of writing what she judges to be misinformation should be “regulated and disciplined”.
Dr. Goff and her co-authors define misinformation as “false, inaccurate or misleading information according to the best evidence available at the time” and disinformation as “having an intentionally malicious purpose”.
Dr. Goff states: “We conservatively classified inaccurate information as misinformation rather than disinformation because the intent of the propagator cannot be objectively assessed.”
Dr. Goff identified four major themes of alleged misinformation. These included: (1) vaccines were unsafe and/or ineffective; (2) masks and/or social distancing did not decrease risk for contracting COVID-19; (3) other medications for prevention or treatment were effective despite not having completed clinical trials or having been FDA approved, and (4) other misinformation.
Dr. Goff includes a brief discussion of vaccine safety and effectiveness and mask effectiveness, but does not attempt to undertake a full review of the published evidence in these areas. Instead, she seems to assume that her readers will agree that any suggestion that vaccines or masks were ineffective or unsafe are self-evidently false.
Dr. Goff states that the American Medical Association has called for disciplinary action for physicians propagating COVID-19 misinformation. She laments the fact that “few physicians appear to have faced disciplinary action” for alleged sins against Covid orthodoxy.
I am not an expert in analysis of published medical research. I don’t work in a School of Public Health like Dr. Goff. I have worked as a licensed physician in England for over 40 years as a family doctor and an occupational physician and I have over 40 years’ experience reading the medical peer review literature. I retired from full time medical practice in 2017. I have a reasonable understanding of English, maths, logic and critical thinking. I don’t pretend to have read all the published research on masks or vaccinations. However, I continue to read leading medical journals on a regular basis.
I understand the concept of truth and how hard it is to establish an absolute truth in science. I understand the enlightenment principles that any ideas can be discussed, that nobody has a veto on ideas and that it is important to doubt and test all of our ideas continually. There is no indication from her writing that Dr. Goff understands how important it is to doubt, question and test the effectiveness and safety of interventions such as vaccines and masks.
From my reading of the peer review literature, for illustration purposes, I identified the following four publications as examples of publications which should raise concerns and questions about COVID-19 vaccines and masks.
In 2019, the World Health Organisation (WHO) published a report entitled ‘Non-pharmaceutical public health measures for mitigating the risk and impact of epidemic and pandemic influenza’. The WHO concluded: “There are a number of high-quality randomised controlled trials demonstrating that personal measures (e.g. hand hygiene and face masks) have at best a small effect on transmission.”
In February 2023 a Cochrane review into the effectiveness of masks concluded: “Compared with wearing no mask in the community studies only, wearing a mask may make little to no difference in how many people caught a flu-like illness/Covid-like illness.”
A study from the Department of Infectious Diseases in Cleveland, Ohio, in December 2022 found that “the bivalent COVID-19 vaccine only offered modest effectiveness”.
A study from the University of Queensland in September 2022 concluded: “Never in vaccine history have 57 leading scientists and policy experts released a report questioning the safety and efficacy of a vaccine. They not only questioned the safety of the current COVID-19 injections but were calling for an immediate end to all vaccination. Many doctors and scientists around the world have voiced similar misgivings and warned of consequences due to long-term side effects.”
These four publications are examples which give us a legitimate reason to question the use of masks and the Covid vaccines and to look further for evidence. Are we not allowed to raise questions about these issues without being threatened with disciplinary procedures? Not to ask any questions would be lacking in curiosity in the extreme, especially for practising physicians concerned about the safety of their patients and the integrity of their advice. These publications do not prove anything conclusively, but they should not be ignored. Expressing doubt and asking questions about the safety and effectiveness of vaccines and masks is not false, inaccurate or misleading, to use the definition adopted by Dr. Goff. If questions arise in my mind, why don’t similar questions arise in the minds of Dr. Goff and her co-authors? How did Dr. Goff reach such a degree of certainty about the effectiveness of masks and vaccines against COVID-19 that she can classify any statement to the contrary as misinformation worthy of disciplining a colleague? Why does she conclude that a colleague who disagrees with her does not have the right to be heard? Why would she seek to silence those who disagree with her?
Inaccurate information which is not deliberately intended to deceive is simply inaccurate. In science and medicine there are many inaccurate statements made in good faith by researchers who are presenting their data or their theories as accurately and honestly as possible. It is important that all theories and all research data can be published, even when the data or the theory are wrong. Disciplinary action for any statement which turns out to be inaccurate or false would surely suppress a large proportion of all scientific and medical discourse. Is this what Dr. Goff wants?
It could be argued that the examples of misinformation used by Dr. Goff are themselves misinformation. To suggest that anyone who states that the Covid vaccines were unsafe and/or ineffective is guilty of misinformation is to ignore significant evidence which raises questions about the vaccines. To suggest that anyone who states that masks did not decrease risk for contracting COVID-19 is guilty of misinformation is also to ignore evidence to support this view. It could be argued that Dr. Goff is using false, inaccurate or misleading examples of misinformation in her study in order to suppress dissenting views.
Dr. Goff appears to have very little humility. She does not appear to be in any doubt that she and her co-authors are infallible in relation to masks and vaccines. She seems to think she is the ultimate arbiter of truth, and that she is immune from being regulated or disciplined for her views in the way she promotes for others. I would not propose disciplining or applying regulatory sanctions to Dr. Goff or her colleagues if her publication includes false, inaccurate or misleading statements. Instead, I would propose respectful dialogue with her to debate her proposal, offering arguments to the contrary with a view to educating her and myself.
In England, medical doctors are obliged to respect colleagues’ skills and contributions, and to treat colleagues fairly. We must create a working environment in which it is safe to ask questions and raise concerns. I believe in these principles. Failure to adhere to these standards can lead to disciplinary action against medical doctors. I understand that similar professional obligations apply to medical doctors in the United States. Dr. Goff does not appear to respect the skills and contributions of colleagues who disagree with her. She seems to be promoting a working environment in which it is not safe for those who disagree with whatever the orthodoxy within the medical profession is at any one time to ask questions and raise concerns. Does she not realise that this may make it unsafe for her to raise concerns and ask questions in due course?
Dr. Goff acknowledges in her final sentence that “a coordinated response by federal and state governments and the profession that takes free speech carefully into account is needed”. This tiny nod towards free speech is somewhat undermined by her attempts to censor her colleagues’ right to disagree with her. Free speech is nothing if it is not accorded to those with whom we disagree.
Frederick Douglass, the American social reformer said: “To suppress free speech is a double wrong. It violates the rights of the hearer as well as those of the speaker.” If Dr. Goff persuades those in power to regulate or discipline those who disagree with her, then their right to free speech is violated and our right to hear them is violated. Does Dr. Goff not have a glimmer of doubt about her omniscience? Does she not think there is even a faint possibility that physicians who disagree with her might have something useful to say?
Why do some physicians think that the best response when another physician disagrees with them is to censor their colleague? How could any physicians achieve such unshakeable certainty in their own omniscience? When did they forget the fundamental principles of the enlightenment, that all ideas can be discussed and that nobody has a veto on any ideas? How did the principles of treating colleagues with respect and upholding the free speech of those with whom we disagree become so degraded?
Dr. Goff and her co-authors should be careful what they wish for. They seek to discipline colleagues for daring to disagree with their orthodoxy. If they succeed, the cancel police may be coming for them next.
Dr. Nigel Wilson MRCGP FFOM is a retired consultant occupational physician.
CDC Now Refusing New COVID Vaccine Adverse Event Reports in Its V-Safe Program
By David Gortler | Brownstone Institute | August 24, 2023
The Centers for Disease Control and Prevention (CDC) V-safe website quietly stopped collecting adverse event reports with no reason or explanation. The V-safe website simply states: “Thank you for your participation. Data collection for COVID-19 vaccines concluded on June 30, 2023.” If you go there today, V-safe directs users to the FDA’s VAERS website for adverse event reporting, even though officials continually derided VAERS as “passive” and “unverified.”
VAERS and V-safe are mutually exclusive safety collection databases operated by the FDA and CDC, respectively. VAERS is an older way of collecting safety data where one can fill out a form online, or manually, or by calling a toll-free number, whereas V-safe is a device “app” which requires online registration. Both VAERS and V-safe collect personal information, lot numbers, dates and associated information, but V-safe was an active collection system geared towards a younger app-using demographic.
Does this mean that the CDC believes that the mRNA Covid-19 injections are so safe, there is no need to monitor adverse event reports any longer? What is the argument against continued monitoring, especially since the V-safe website was already up and paid for?
While CDC’s V-safe was stealthily and abruptly turned off, refusing to accept new safety reports, to this very day the CDC continues to urge everyone ages 6 months and older to stay up to date with COVID-19 vaccines and boosters.
As a drug safety expert, I personally can’t cite another example of any agency or manufacturer halting collection of safety data. It seems even worse because mRNA technology is relatively new with long-term manifestations unknown. On top of this, both manufacturers and the FDA refuse to share the list of ingredients, such as lipid nanoparticles, which could affect individuals differently and take a long time to manifest clinically.
Safety Data Collection Should Never Stop:
Now, contrast that with the fact that the National Highway Traffic and Safety Administration (NHTSA) will still accept a safety report for a 30-year-old Ford Bronco II. Indeed, this is an oddly specific example, but only because I drove this exact vehicle as a family hand-me-down as a student, through my residency, fellowship, for my tenure as a Yale professor on the mean streets of New Haven and even during my years at the FDA as a medical officer /senior medical analyst.
Like mRNA shots, Bronco IIs are still available on the market and people are still using them up to this very day. My Bronco became an intermittent topic of conversation with friends and FDA colleagues. One day, I was informed by a patrolling security guard at the FDA that it was the oldest car on campus.
I didn’t know much about cars (or mRNA technology) back then, but when a fellow FDA-er informed me that my Bronco II had noteworthy safety problems and that the NHTSA still had their eye on this vehicle (rollover accidents were more common and more fatal) I addressed the problem: I got rid of the reliable relic, even though I really liked it. NHTSA Is still accepting safety reports three decades later.
CDC No longer accepting safety reports despite rapidly increasing safety findings:
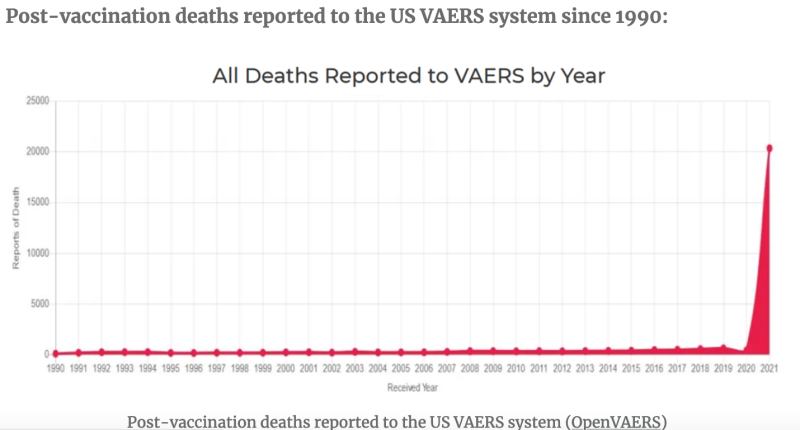
Unlike my old Bronco, mRNA injections have only been on the market for about two years, and according to the FDA Vaccine Adverse Event Reporting System (VAERS) database, mRNA “vaccines” have been named the primary suspect in over 1.5 million adverse event reports, of which there are >20,000 heart attacks and >27,000 cases of myocarditis and pericarditis just in the USA alone. Worldwide numbers would be greater. According to many references, including an FDA-funded study out of Harvard, VAERS reports represent fewer than 1 percent of vaccine adverse events that actually occur.
Interestingly, the NHTSA link above on my Ford Bronco II only shows: one parts recall, one investigation and 23 complaints, and still features a button in the upper right hand corner for submitting new complaints.
Wikipedia defines an humanitarian crisis or humanitarian disaster as a: “singular event or a series of events that are threatening in terms of health, safety or well-being of a community or large group of people.” Based on VAERS and previous V-safe findings, adverse events from mRNA shots in the USA alone could be considered a humanitarian crisis.
Despite those alarming clinical findings, the CDC has concluded that collecting new safety reports is somehow no longer in the interest of America’s public health. Existing data from the V-safe site showed around 6.5 million adverse events/health impacts out of 10.1 million users, with around 2 million of those people unable to conduct normal activities of daily living or needing medical care, according to a third-party rendering of its findings. In other words, despite mRNA shots still being widely available and the CDC promoting its continued use, it’s “case closed” with regards to collecting new safety reports, under today’s federal public health administration.
Will the CDC opine on the existing data or justify its halting of collecting new safety data? To the best of my knowledge, stopping the collection of public health information doesn’t have a clinical justification or scientific precedence — especially when it comes to an actively marketed product.
In George Orwell’s 1984, characters were told by The Party to “reject the evidence of your eyes and [your] ears.” Now, the CDC isn’t even allowing that evidence to be collected for viewing (and prospective rejecting). It’s a terrible idea for any product, let alone novel mRNA technologies.
Dr. David Gortler, a 2023 Brownstone Fellow, is a pharmacologist, pharmacist, research scientist and a former member of the FDA Senior Executive Leadership Team who served as senior advisor to the FDA Commissioner on matters of: FDA regulatory affairs, drug safety and FDA science policy. He is a former Yale University and Georgetown University didactic professor of pharmacology and biotechnology, with over a decade of academic pedagogy and bench research, as part of his nearly two decades of experience in drug development. He also serves as a scholar at the Ethics and Public Policy Center.
Featured Video

The Most Important Bet You’ve Never Heard Of
or go to
Aletho News Archives – Video-Images
From the Archives
The Occupied Mentality Syndrome
Saudi Arabia on the American chessboard – Part 2
By B. J. Sabri | American Herald Tribune | April 19, 2016
Since the Korean War, but particularly since the Iranian Revolution of 1979 until today, the United States has been steadily escalating its military presence in the Persian Gulf. Taking advantage of many colossal events of the past 36 years, [1] the hyper-empire has institutionalized its massive presence on land and sea, and expanded its objectives to include the unambiguous physical control of the area, as well as the clear understanding that local Arab governments should abide by them. The pretext is always the same: in “defense” of the national interests and security of the United States. From observing how the United States has been interacting with the governments of the region, and by judging from the size of its expeditionary force, we could reach a basic conclusion. The United States is occupying, de facto, the entire Arabian Peninsula. (Yemen, devastated by Saudi and American jets is yet to be conquered. Oman? Britain returned not as colonial ruler but as a soft occupying power.)
Under this articulation, Saudi Arabia, Qatar, Kuwait, and the United Arab Emirates are virtually occupied countries. If we compare this type of occupation to the mandate and protectorate regimes of the past, the results might be identical—the nations affected by it lose sovereignty. When Arab governments comply with the objectives of a foreign power that station military forces on their national milieu, then that power controls them in multiple ways including how they react to policy deliberations and what decisions they intend to take on specific issues. A good method to verify the concept of effective occupation is this: take notice of what the United States says and wants, and then compare it to what the gulf rulers do in response. (I shall discuss this detail at some point in the upcoming parts.)
If the presence of US forces or other means of political pressure are a factor in Saudi Arabia’s interventionist Arab wars, then we need to debate this issue. However, from the history of resistance to colonialism, we learnt: if a powerful state imposes its order on a nation by military means or other forms of coercion, and if this nation does not resist that imposition, then a mental subordination to the powerful state will ensue. This is especially true in the case of Saudi Arabia. One single event, 9/11, has transformed it from a US “ally” into an instant political hostage of the American Empire. … continue
Blog Roll
 Aletho News
Aletho News- Trump and the debris of Iran war
- IRGC hits US tech giant Oracle’s data center, computing site in UAE over new assassinations
- Bombing Iran Back Into the Stone Age /Lt Col Daniel Davis & Jim Jatras
- UAE rejects report claiming it is ready to join war on Iran to reopen Hormuz
- A New Resistance Front: How Does Syria Factor into the Regional War?
- Gulf states weigh pipeline expansion plans, hoping to bypass Hormuz
- Iran sets up ‘tollbooth’ system in Strait of Hormuz
- Wave 90: IRGC strikes US-linked industrial sites in Gulf
- Iran Says US-Israeli Claims of Its Military Strength Are Wrong
- Trump’s April Fools’ Address to the nation
- If Americans Knew
- ‘War crime’: Global condemnation as Israeli ministers celebrate death penalty law targeting Palestinian prisoners
- 7 Ways Israel Is Turning Lebanon Into Gaza
- World’s Leading Football Bodies Under Fire Over Israel Policies
- Experts warn of possible use of nukes against Iran
- Israeli invasion of Lebanon could be worse than 1982, warn European officials
- Passover: Liberation and collective punishment
- Trump says the quiet part out loud: (Israel’s) war on Iran > Americans’ health – Daily Update
- Gaza families reunite years after babies evacuated amid Israel’s war
- International Rescue Committee warns Gaza’s children face grave protection risks
- Iran’s Alleged 47-Year War on America: Debunking the 1,050 American Deaths Canard
- No Tricks Zone
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
