Serious adverse events from Pfizer’s mRNA vaccine are not “rare”
Maryanne Demasi, reports | June 27, 2023
Drug regulators and public health agencies have saturated the airways with claims that serious harms following covid vaccination are “rare.”

But there has been very little scrutiny of that claim by the media, and I could not find an instance where international agencies actually quantified what they meant by the term “rare” or provided a scientific source.
The best evidence so far, has been a study published in one of vaccinology’s most prestigious journals, where independent researchers reanalysed the original trial data for the mRNA vaccines.
The authors, Fraiman et al, found that serious adverse events (SAEs) – i.e. adverse events that require hospitalisation – were elevated in the vaccine arm by an alarming rate – 1 additional SAE for every 556 people vaccinated with Pfizer’s mRNA vaccine.
According to a scale used by drug regulators, SAEs occurring at a rate of 1 in 556 is categorised as “uncommon,” but far more common than what the public has been told.

Therefore, I asked eight drug regulators and public health agencies to answer a simple question: what is the official calculated rate of SAEs believed to be caused by Pfizer’s mRNA vaccine, and what is the evidence?
The agencies were FDA, TGA, MHRA, HC, PEI, CDC, ECDC and EMA.
The outcome was startling.
Not a single agency could cite the SAE rate of Pfizer’s vaccine. Most directed me to pharmacovigilance data, which they all emphasised does not establish causation.
The Australian TGA, for example, referred me to the spontaneous reporting system but warned, “it is not possible to meaningfully use these data to calculate the true incidence of adverse events due to the limitations of spontaneous reporting systems.”
Both the German regulator (PEI) and European CDC referred me to the European Medicines Agency which, according to its own report, saw no increase at all in SAEs. “SAEs occurred at a low frequency in both vaccinated and the placebo group at 0.6%.”
The UK regulator MHRA went so far as to state it “does not make estimations of a serious adverse event (SAE) rate, or a rate for adverse reactions considered to be causally related for any medicinal product.”
The US FDA, on the other hand, did conceded that SAEs after mRNA vaccination have “indeed been higher than that of influenza vaccines,” but suggested it was justified because “the severity and impact of covid-19 on public health have been significantly higher than those of seasonal influenza.”
Despite analysing at the same dataset as Fraiman, the FDA said it “disagrees with the conclusions” of the Fraiman analysis. The agency did not give specifics on the areas of disagreement, nor did it provide its own rate of SAEs.
In response to the criticism, Joe Fraiman, emergency doctor and lead author on the reanalysis said, “To be honest, I’m not that surprised that agencies have not determined the rate of SAEs. Once these agencies approve a drug there’s no incentive for them to monitor harms.”
Fraiman said it’s hypocritical for health agencies to tell people that serious harms of the covid vaccines are rare, when they have not even determined the SAE rate themselves.
“It’s very dangerous not to be honest with the public,” said Fraiman, who recently called for the mRNA vaccines to be suspended.
“These noble lies may get people vaccinated in the short term but you’re creating decades or generations of distrust when it’s revealed that they have been misleading the public,” added Fraiman.
Dick Bijl, a physician and epidemiologist based in the Netherlands, agreed. “It goes to show how corrupted these agencies are. There is no transparency, especially since regulators are largely funded by the drug industry.”
Bijl said it’s vital to know the rate of SAEs for the vaccines. “You must be able to do a harm:benefit analysis, to allow people to give fully informed consent, especially in young people at low risk of serious covid or those who have natural immunity.”
Bijl said the mainstream media has allowed these agencies to make false claims about the safety of vaccines without interrogating the facts.
“The rise of alternative media is strongly related to the lies being told by the legacy media, which just repeats government narratives and industry marketing. In the Netherlands, there is a lot of discussion about the distrust in public messaging,” said Bijl.
CDC Panel Recommends Pfizer Pneumococcal Vaccines for Infants, RSV Vaccines for Adults
By Michael Nevradakis, Ph.D. | The Defender | June 26, 2023
Advisers to the Centers for Disease Control and Prevention (CDC) last week recommended newly approved vaccines for respiratory syncytial virus (RSV) — despite concerns about the efficacy and safety of the new vaccines, potentially harmful interactions with the flu and COVID-19 vaccines and the unspecified cost for the vaccines.
In a three-day meeting that ended Friday, the CDC’s Advisory Committee on Immunization Practices (ACIP) also:
- Recommended a new pneumococcal conjugate vaccine as an “option” for children.
- Discussed COVID-19 bivalent vaccines and vaccines for meningitis, polio, dengue, monkeypox and chikungunya vaccines.
- Discussed proposals regarding the vaccine schedule.
- Suggested the removal of egg allergies as a contraindication to vaccines made in eggs.
For Dr. Meryl Nass, an internist, biological warfare epidemiologist and member of the Children’s Health Defense (CHD) scientific advisory committee, last week’s proceedings lacked the due diligence needed to fully ascertain the safety of the vaccines and treatments being reviewed.
Writing on her blog, Nass stated:
“The mission of CDC and the ACIP members is to sign off on all possible vaccines as safe and effective, and to never turn over any stones that could reveal anything different. Then to roll all vaccines out to as broad a group of humans as humanly possible.”
ACIP says seniors ‘may’ get RSV vaccine, but overlooks other safety concerns
According to MedPage Today, ACIP recommended the new RSV vaccines for older adults on Wednesday “but opted not to give their strongest endorsement,” instead recommending “a talk with [a] medical provider first.”
STAT reported that ACIP recommended “anyone 60 and over should be able to get one of the new [RSV] vaccines … if they and their physicians think it would be worthwhile.”
According to STAT, ACIP was initially slated to vote on a broader recommendation that would have “urged all people 65 and older to get vaccinated” for RSV.
However, “that recommendation was watered down” after “several members of the committee expressed serious concerns about the decisions they were being asked to make based on the data the companies had provided.”
Reuters reported that while some committee members wanted to stick with the broader recommendation, “others had concerns that there was not enough data about how effective the vaccines are in people over the age of 75 and other high-risk groups.”
Two votes followed. In one, ACIP was asked whether “adults 65 years of age and older are recommended to receive a single dose of RSV vaccine.” The committee voted 9-5 to recommend that those age 65 and over “may” get an RSV vaccine after consultation with a doctor or pharmacist.
The other vote asked ACIP’s members whether “individual adults ages 60-64 may receive a single dose of RSV vaccine, using shared clinical decision-making” — that is, consultation with a doctor or pharmacist. Here, the result was 13-0 in favor, with one abstention.
ACIP’s recommendations are headed to the desk of outgoing CDC Director Rochelle Walensky, who is expected to sign off on them early this week. Her last day as head of the CDC is June 30. However, ACIP recommendations are not considered final until they are published in the Morbidity and Mortality Weekly Report.
The FDA recently approved the two vaccines — Pfizer’s Abrysvo and GSK’s Arexvy.
According to STAT, “It is expected both companies will provide vaccines to the market in time for the next RSV season.” However, the mild recommendations from ACIP “will likely lead to a lower uptake of the new vaccines than the manufacturers might have expected.”
Nass noted that data presented to ACIP indicated that out of 40,000 participants in the RSV vaccine clinical trials, six developed Guillain-Barré syndrome (GBS), a rare disorder in which the immune system attacks the nerves or a GBS-type illness. This was compared to no GBS cases in the control group.
According to CNN, some ACIP members expressed concern that few adults over 75 and older were enrolled in the Pfizer and GSK clinical trials, even though they represent the group most at risk from RSV.
The immunocompromised and those living in “settings such as nursing homes are also at elevated risk but were not enrolled in the studies,” STAT reported.
In addition, according to MedPage Today, approvals of the two RSV vaccines “were based on efficacy data spanning a single RSV season.” At the ACIP meeting, Pfizer and GSK representatives “presented data showing that vaccine efficacy largely held up through the first part of the second RSV season, but did drop slightly.”
Some concerns were also raised regarding the concurrent administration of RSV vaccines alongside flu and COVID-19 shots.
According to STAT, “these vaccines will likely be given at the same time of the year … and it’s not yet clear if giving the vaccines at the same time undermines the immune responses they generate” because studies of concomitant administration of COVID and RSV vaccines are still underway.
GSK claimed that when its RSV vaccine was administered along with a flu vaccine, “It was safe and well-tolerated,” CNN reported.
The cost of the vaccine also drew criticism. According to MedPage Today, Pfizer and GSK proposed a range of prices spanning between $180 and $295, but according to STAT, “Both companies resisted strong pressure from the committee to commit to a firm price.”
According to Reuters, “Pfizer and GSK have said they expect RSV vaccines to eventually become multibillion-dollar sellers.” However, Fierce Pharma reported that ACIP’s “tepid endorsement for the vaccines could hinder sales.”
For 2023, GSK “expects the U.S. market to be in the range of 10 million to 15 million people, a fraction of the size of the expected flu or COVID-19 market,” Reuters stated.
Pneumococcal vaccine approved as ‘option’ for infants as young as 2 months old
ACIP voted unanimously in favor of adding Pfizer’s new 20-valent pneumococcal conjugate vaccine (Prevnar, or PCV20) — currently administered only to adults — as an “option” for children, MedPage Today reported.
According to the AAP, “Pfizer’s PCV20 adds serotypes 8, 10A, 11A, 12F, 15B, which are not covered in PCV15,” a previously existing vaccine.
ACIP voted in favor of:
- Routine use of either PCV20 or PCV15 in children aged 2-23 months.
- Administration of either PCV15 or PCV20 in children aged 24-59 months with incomplete PCV vaccination status, and in children aged 24-71 months with certain underlying conditions and incomplete PCV vaccination status.
- Vaccination of children between 2 and 18 years of age with PCV20, or with pneumococcal polysaccharide vaccine (PPSV23) if they previously had only received PCV13 or PCV15.
- A single dose of PCV15 or PCV20 to children between 6 and 18 years of age with any risk condition who have not received any dose of PCV13, PCV15 or PCV20. If PCV15 is administered, the committee said it should be followed by a dose of PPSV23 at least eight weeks after the initial vaccination.
According to Nass, PPSV23 is “very inflammatory” and it is “unclear how well/if it works.”
Moreover, according to MedPage Today, ACIP expanded its definition of high-risk children to include conditions such as moderate persistent and severe persistent asthma, chronic kidney disease (excluding dialysis patients), chronic liver disease and those with renal failure on maintenance dialysis.
Some committee members “expressed concern over the lack of clinical data for the new vaccines,” MedPage Today reported, including “no effectiveness and no efficacy data on either PCV15 or PCV20.”
Nass noted that “the CDC presented no good data on these new vaccines,” instead presenting “economic models” in lieu of this data, adding, though, that “reliable data to plug into the models” is lacking.
Despite this missing data, an ACIP member quoted by Nass said, “Our CDC colleagues are masters at epidemiology surveillance that will give us the answer in [the] future” — “In other words,” Nass said, “‘we won’t know if it works unless we give it to millions of children, so what are we waiting for?’”
Third monkeypox vaccine dose not recommended — for now
ACIP considered, but rejected, recommending a third dose of the Jynneos vaccine for monkeypox.
However, the committee did encourage “2-dose vaccinations among persons who do not have immunity and optimizing immune function … ideally before mpox exposure.”
ACIP also recommended “persons eligible for vaccination, particularly those with advanced HIV and other immunocompromising conditions, should receive two doses of Jynneos vaccine,” adding that “Additional research on the durability of Jynneos vaccine-induced immunity is needed.”
In response, Nass remarked, “Let me remind you that monkeypox is essentially like shingles … It is a mild disease and there is no need for a vaccine for 99.9% of people; and if you get it, you will probably have real immunity afterwards.”
“CDC is willing to give it along with COVID vaccines, even though that probably magnifies the risk of myocarditis,” Nass added.
The committee also discussed, but did not act on, proposals to expand the use of Jynneos to children and pregnant and breastfeeding women.
Other vaccines also on ACIP’s agenda, but no decisions made
According to APP, “ACIP members reviewed data on Friday regarding the safety of aluminum in vaccines,” reviewing the results of a study finding a possible link between aluminum and childhood asthma.
However, it was determined that the study had “important limitations” and that its findings “do not prove causation,” although “a follow-up study with a larger group of children and longer follow-up time” will subsequently be performed. Ultimately, ACIP “did not recommend changing the vaccine schedule.”
Nass noted that links between aluminum, and diabetes and eczema, were also discussed, with a “small positive association” found in the case of eczema and asthma.
ACIP members also examined the possibility of “simplifying COVID vaccine recommendations for children ages 2-4 years,” according to the APP, looking “at the possibility of requiring only one dose for this group instead of two to three.”
ACIP’s COVID-19 vaccine work group said “it would support a single, potentially annual, dose for children ages 2 years and older, while maintaining multiple doses for those under 2.” However, no vote was taken.
Some committee members argued that “Simplifying the recommendations also may lead to more children getting vaccinated,” citing low uptake in children under age 2.
A new pentavalent meningococcal vaccine, combining two existing vaccines into one, was also discussed — a vaccine which, according to Nass, “is not needed.” No discussion of the safety of the existing meningitis vaccines took place at the meeting, Nass said.
Also on ACIP’s agenda was a recommendation under consideration for a single polio shot for all individuals who are unsure whether they were fully vaccinated as children or who expect to visit high-risk environments. Again, no decisions were made.
Vaccines for dengue and chikungunya — two mosquito-borne diseases which are rare in the U.S. — were also discussed by ACIP, with no outcome arising from the meeting.
Reactogenicity got magically turned into safety, and safety got thrown away’
ACIP also voted 14-0 that it is no longer necessary for individuals with egg allergies to receive their flu vaccine in a medical setting, noting that “immunization best practice guidelines already call for all vaccine providers to be equipped to handle anaphylaxis,” as reported by the American Academy of Pediatrics (AAP).
“Any flu vaccine appropriate for the person’s age and health status can be used regardless of whether it is egg-based,” AAP stated. This decision awaits CDC approval.
“CDC has been trying to get rid of vaccine contraindications for the past five years, despite lack of supportive evidence,” Nass said. Following ACIP’s vote, “egg allergies as a contraindication or precaution for flu shots is about to disappear.”
Nass told The Defender that while “there used to be three things a vaccine had to be tested for — purity, potency and safety,” safety has now “morphed into sterility” — meaning it doesn’t contain “outside germs,” according to a new definition from the U.S. Department of Health and Human Services.
“There used to be a word — reactogenicity — for acute reactions to a vaccine,” Nass said, referring to the physical manifestation of the body’s inflammatory response to vaccination. She also noted that “safety” was “primarily concerned with longer-term or non-resolving side effects,” including “serious side effects.”
“But reactogenicity got magically turned into safety, and safety got thrown away.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
mRNA: Vaccine or Gene Therapy? The Safety Regulatory Issues
Dr. Helene Banoun Elucidates the History of Misguided Use of Genetic Code for Vaccination
By Peter A. McCullough, MD, MPH | Courageous Discourse | June 26, 2023
I have been impressed with the quality of scholarship from independent academic researchers during the pandemic. During this time there has been a silence from academia in terms of any viewpoints that deviate from the mainstream scientific narrative. Dr. Helene Banoun is an independent researcher, former research fellow at INSERM (French Institute for Health and Medical Research), Marseille, France. She has published several very important review papers during the crisis.
Dr. Banoun has recently published an analysis on the mRNA vaccines in consideration of definitions and regulations that apply to gene therapy. For most people vaccinated, it was the first time they had been injected synthetic genetic code for a potentially lethal foreign protein (Wuhan Spike protein). A perfectly compliant American who started the COVID-19 vaccination program on time is on their seventh mRNA injection—an astonishing observation given the lack of any safety information concerning the cumulative effect of frequent, serial administrations. Banoun makes the case that they should be classified as gene therapy products. I have heard no counter arguments to the contrary.

Banoun, H. mRNA: Vaccine or Gene Therapy? The Safety Regulatory Issues. Int. J. Mol. Sci. 2023, 24, 10514. https://doi.org/10.3390/ijms241310514
Banoun goes on to state: “The wide and persistent biodistribution of mRNAs and their protein products, incompletely studied due to their classification as vaccines, raises safety issues. Post-marketing studies have shown that mRNA passes into breast milk and could have adverse effects on breast-fed babies. Long-term expression, integration into the genome, transmission to the germline, passage into sperm, embryo/fetal and perinatal toxicity, genotoxicity and tumorigenicity should be studied in light of the adverse events reported in pharmacovigilance databases.”
This is important for discussants and litigators to have this predicate. Genetic vaccines are gene therapy products, all the regulations, laws, and safety protections should be called for and pointed out when missing in the discussion on the next steps to be taken on mRNA genetic vaccines.
Aluminium and Breast Cancer
Building the scientific case
BY DR CHRISTOPHER EXLEY | JUNE 20, 2023
In my recent book I write about building a case for an aetiological role for aluminium in breast cancer. Herein I will revisit the chapter in my book and examine the case for aluminium anew.
My interest in breast cancer was sparked by the research of oncologist Philippa Darbre linking breast cancer incidence and occurrence with the regular use of antiperspirants. My interest in these ‘cosmetics’ went back much further and I was concerned that antiperspirants were significant contributors to the body burden of aluminium. Please read my book for an account of the history, but to cut a long story short, I collaborated with Darbre and we showed that breast tissue biopsies obtained from women with breast cancer contained aluminium. Of particular interest was that breast tissues closest to the underarm consistently contained a higher content of aluminium. Of course, our research was ignored by the breast cancer community and campaigned against by breast cancer charities, including the charity that provided the breast tissue biopsies used in our study! However, it was followed up by a number of research groups in Europe and the US and evidence began to be put forward to support aluminium as a carcinogen in breast cancer. Perhaps foremost amongst these groups is research led by Stefano Mandriota in Switzerland. Mandriota, an oncologist of some repute, showed that mouse mammary epithelial cells underwent malignant transformations upon exposure to aluminium. Aluminium-induced tumours were the result of genomic instability. The most recent publication from this group highlights the importance of chromosome instability in aluminium’s carcinogenicity. Mandriota’s meticulous cell and animal studies are building the case for a role for aluminium in breast cancer. These studies continue today and deserve our full support.
A role for aluminium in breast cancer is not dependent upon a link to the regular use of antiperspirants. However, the most definitive clinical trial yet to fully investigate such a link makes a very compelling case. The study found both significantly increased concentrations of aluminium in breast tissue in breast cancer and a significant increased risk of breast cancer in women who used an antiperspirant several times a day. Confirmation of increased content of aluminium in breast tissue in breast cancer asks the question at least as to the role played by aluminium-based antiperspirants in the accumulation of aluminium in breast tissue. Note that contrary to the information repeatedly reported by the antiperspirant industry these ‘cosmetics’ do not prevent sweating by simply acting as plugs in the sweat gland. These ‘cosmetics’ prevent sweating by inhibition of the activity of the sweat gland by aluminium. The industry is well aware of this but cannot admit to such since this would change the categorisation of antiperspirants from simple cosmetics to a medicine. The latter requiring authorisation through clinical trials demonstrating both safety and efficacy. (Well, this used to be the case prior to covid vaccines.) Since sweating is a significant route of excretion of aluminium from the body, inhibiting sweating in the underarm region is likely to promote accumulation of aluminium in the surrounding tissue.
The industry actively ignores the science and attempts to defend itself by funding studies that desperately look to minimise the role of antiperspirants in the accumulation of aluminium in breast tissue. Let me be frank about such published work. I do not believe them. They set out to prove a point and, hey presto, the results prove their point. The recent study I have highlighted is wholly funded by the antiperspirant industry, its interpretation is wholly dependent upon the premise that antiperspirants are simply acting as plugs in sweat glands and as a clue to its bias one can notice that it only cites industry publications and completely ignores all previous independent research in this field. One can only surmise that the journal editor and manuscript referees are either stupid or, perhaps more likely, industry affiliates.
I have built a case for a role for aluminium in breast cancer and I will continue to watch with interest the new and independent research that tests this role. In the meantime those who are interested might like to visit the website of my good friend Eileen whose untiring work endeavours to bring this story to a wider audience.
Clinical Trial to License RotaTeq, Like Almost All Childhood Vaccines, Did Not Use a Placebo Control
Those attacking RFK are wrong
BY AARON SIRI | INJECTING FREEDOM | JUNE 25, 2023
Robert F. Kennedy, Jr. is on record stating that almost all childhood vaccines were licensed based on clinical trials that did not include a placebo control. He is correct.
Nonetheless, numerous news outlets, such as Stat News in its article titled “Correcting Robert F. Kennedy Jr.’s vaccine ‘facts’”, are stating Mr. Kennedy is wrong because they claim the clinical trial relied upon to license the rotavirus vaccine, RotaTeq, did include a placebo control. They are wrong.
A placebo is defined by the CDC as a “substance or treatment that has no effect on living beings.” This means a saline injection or water drops in mouth.

RotaTeq is administered via oral drops. A “placebo” would have been water drops in the mouth. The control used in the trial, however, included bioactive ingredients including almost all the ingredients in the RotaTeq vaccine itself.
How do I know this? Because in 2018, on behalf of ICAN, we were investigating the control used in each clinical trial relied upon by the FDA to license each childhood vaccine.
In that review, we found that while the package insert for the RotaTeq vaccine says the control in its clinical trial was a “placebo,” when we read the FDA’s clinical trial review for RotaTeq, the ingredients of this so-called “placebo” were redacted:
So, on behalf of ICAN we submitted a Freedom of Information Act Request to the FDA for “Documents sufficient to identify the ingredients of the ‘placebo’ in the prelicensure clinical trials identified in Section 6.1 of the package insert for RotaTeq.”
In a response dated June 14, 2018, the FDA provided the requested documents which clearly show that the control was not a placebo. Rather, it included polysorbate-80, sodium citrate, sodium phosphate, and sucrose.
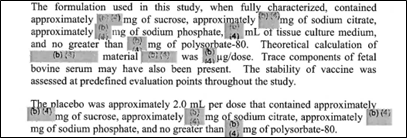
These same four ingredients are also contained in RotaTeq. The only difference between the vaccine and the control is that RotaTeq also included tissue culture medium and rotavirus reassortments. So, bottom line: the control used in the RotaTeq clinical trial was not a placebo since it included bioactive ingredients.
For example, here is what the NIH explains about sodium phosphate, one of the ingredients in the control:
Sodium Phosphate can cause serious kidney damage and possibly death. In some cases, this damage was permanent, and some people whose kidneys were damaged had to be treated with dialysis (treatment to remove waste from the blood when the kidneys are not working well). Some people developed kidney damage within a few days after their treatment, and others developed kidney damage up to several months after their treatment.
And as these studies and data sheet make clear, polysorbate-80 is far from an inert substance, is bioactive, and can have safety concerns, especially when given to infants.
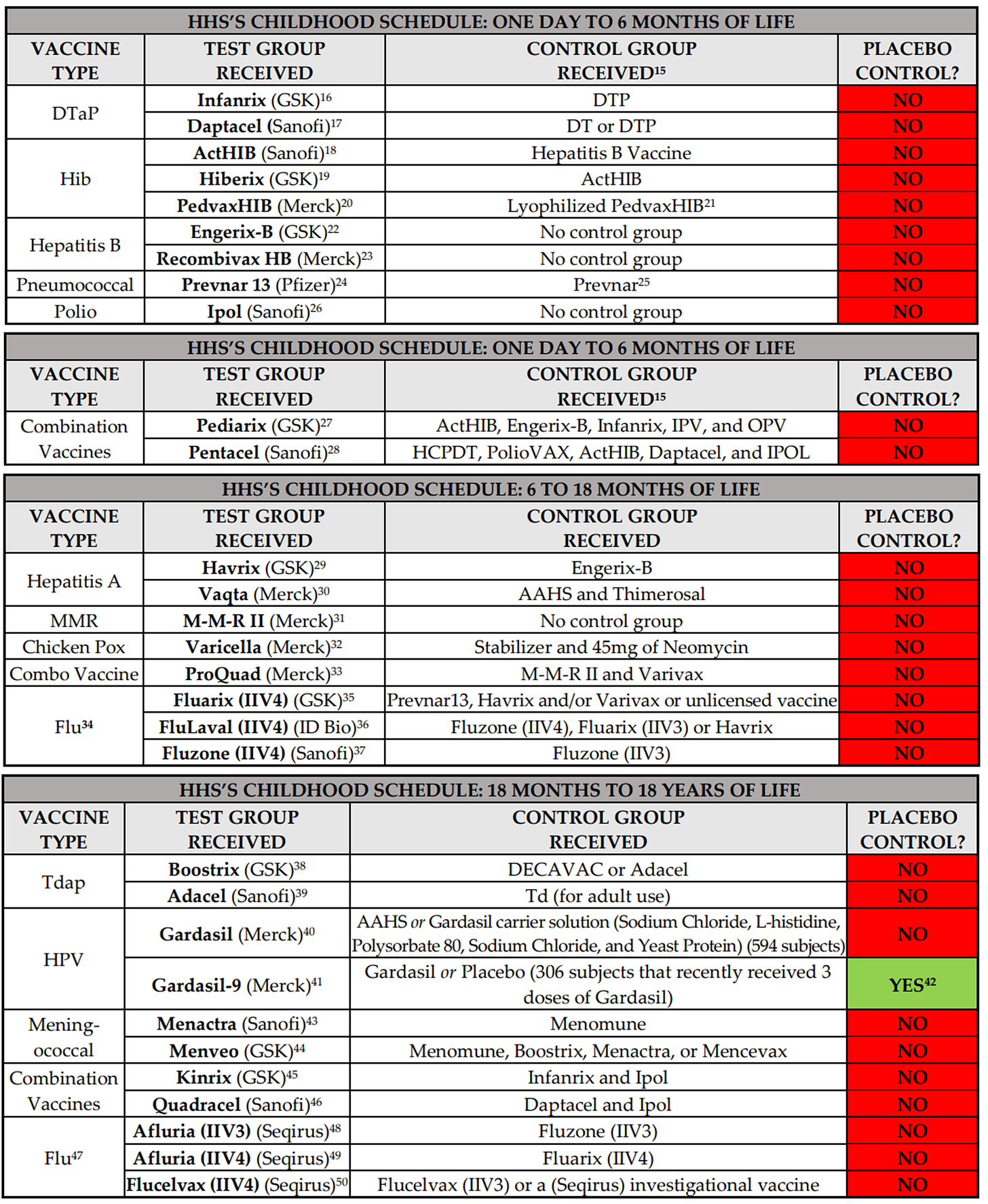
Bottom line, Robert F. Kennedy, Jr.’s claim that virtually all childhood vaccines were licensed based on clinical trials that did not include a control group that received a placebo is correct. The undisputable evidence for this claim, all from FDA or pharma sources, is detailed on pages 3 to 7 of a response we sent to HHS on December 31, 2018. (In sharp contrast to virtually all other childhood vaccines, the clinical trial relied on to license Pfizer’s Covid-19 vaccine for teenagers 12 to 17 years of age appears to have had a placebo control group, though we are still reviewing that claim.)
Here are copies of the charts from that 2018 response to HHS which show what the control group received in each clinical trial for each childhood vaccine:
It is also why the following claim by Dr. Paul Offit in his article “Should Scientists Debate the Undebatable” is categorically false: “All vaccines are tested in placebo-controlled trials before licensure.”
I would more than welcome a public debate with Dr. Offit on this point and would welcome being proven wrong – would gladly prefer that products injected into babies not have this safety gap. Oh, but wait, Dr. Offit says it is undebatable, which again shows precisely why there must always be complete, uncoerced choice when it comes to any medical product.
What is really incredible about the attacks on Mr. Kennedy is that he has made clear he has no intention of changing anyone’s right to obtain vaccines. Everyone who wants to keep vaccinating will be free to do so. He just wants to assure freedom of choice and help those who are injured by these products.
The media and medical profession’s attack on this position is callous. Just as they care about those injured by infectious disease, as Mr. Kennedy certainly does, they should also care about those injured by vaccines. Mr. Kennedy is clear that we can and should do both. And to his amazing credit, no amount of insult or attack has moved him from his position that we must protect every American, including those injured by these pharma products.
Was SARS-CoV-2 entirely novel or particularly deadly?
BY THOMAS VERDUYN, DR TODD KENYON, DR JONATHAN ENGLER | PANDA | JUNE 22, 2023
As part of our inquiry into the drivers of excess deaths, we take a step back and address the central theme of the Covid-era narrative: that SARS-CoV-2 is a novel virus that is so deadly that drastic measures were needed to contain it.
In the previous articles of this mini series about excess deaths we looked at how effective the Covid shots were at arresting Covid [1, 2] and also how bad the “first wave” in New York city was.[3] There are good reasons behind why we chose to address these two topics first. One reason is that an honest look at these issues helps establish a balanced understanding of what might be driving excess deaths since 2020. Another reason is that both topics were central to the official narrative emanating from government sources and the mainstream media. We were told that the whole point of the lockdowns was to delay the spread of SARS-CoV-2 until a vaccine could be developed that would spare us from overwhelmed hospitals like what happened in places like New York and Italy.
As has been shown, and to put it mildly, the Covid shots did not perform nearly as well as promised. Sadly, the burden of the adverse events caused by the experimental shots turned out to be worse than the disease.[4] Furthermore, by a close examination of excess deaths in New York city in early 2020, and in particular by a comparison to what happened on the Diamond Princess, it was concluded that the tragedy in New York was not compatible with the spread of a virus such as SARS-CoV-2, let alone any other generally mild respiratory virus.
All of this presses us to take a step back and address the central theme of the Covid-era narrative, namely the idea that SARS-CoV-2 is a novel virus that is particularly deadly; so deadly that drastic measures were needed to contain it. We begin with a look at the idea that the virus is novel.
1. How novel is SARS-CoV-2?
In the field of virology, the term “novel virus” typically means that the virus was recently discovered. This definition, of course, tells us nothing at all about when the virus first existed. Thus, for instance, the first human-coronavirus was found in 1961.[5] It was labeled B814 and identified as a cause of the common cold. This does not mean that this particular cold-causing coronavirus suddenly appeared in that year. No, and much to the rather, it only means someone finally found it. The ability to isolate, identify and sequence RNA viruses is a relatively new science. The patent on the process used in PCR machines was first granted in 1987.[6] It was in 2003, only 20 years ago, that the first human reference genome was sequenced. Despite all the efforts by many scientists, mankind has not yet sequenced every virus on planet earth. It is quite possible we never will. As a result, we are hardly in a position to assert when a particular virus (or strain of a virus) first appeared. Even if sequencing of a virus could prove beyond reasonable doubt that it was made in a laboratory, unless we had lab records to prove when it was made, it would still be nearly impossible to determine when it first infected someone. At best we might be able to estimate a timeframe by using antibody tests applied to stored specimens. The fact that SARS-CoV-2 is a relatively mild virus with symptoms similar to that caused by the flu only compounds the challenge. All we know for certain about this virus is that labs first began testing for it in early 2020.
The real problem with all of this is that during the Covid era the term “novel virus” was used by many outlets (including universities, journals, the media, and government officials) to mean something quite different from “recently discovered.”[7] For example, the GoodRx website has an article in which the authors say that “SARS-CoV-2, the virus that causes COVID-19, is a “novel coronavirus.” This means it’s different from all viruses like it.” They go on to say that “In medicine, novel refers to a virus or bacteria that wasn’t known to affect humans. This means that the bug is either brand new or was only found in animals or other life forms.” [8] Likewise, Dr. Tam, the chief medical officer of Canada, recently wrote, “In March 2020, Canada was faced with a… virulent pathogen… for which there was no natural immunity… and no effective antivirals.” So we see that the official narrative was not only that SARS-CoV-2 was recently discovered, but that it did not exist before late December 2019, was different from other viruses, was newly capable of infecting humans, was entirely new to our immune system, and was outside the scope of what doctors knew how to treat.
Are any of these claims true? Other than the fact that it was recently identified, the other claims are either false or dubious at best. It is useful to examine each claim on its own. We begin with a brief investigation into the possibility that SARS-CoV-2 existed before December 2019. Actually, there is growing evidence that SARS-CoV-2 was around long before it suddenly acquired international attention. For instance, by searching through the public sequencing data archives, a group of researchers found that soil samples collected in Antarctica between Dec 2018 and Jan 2019 contained “sequence fragments matching the SARS-CoV-2 reference genome…” [9] This was so contrary to the official narrative that the authors later suggested that it had to be on account of laboratory contamination issues. But their findings were not unique. For example, by examining human blood samples taken in Italy before the Covid era, researchers found that already by September of 2019 some individuals (none of whom were sick at the time) had SARS-CoV-2 specific antibodies in their blood.[10 11] Other studies have found similarly.[12] Therefore, there is good evidence that the virus existed long before it garnered any attention.
Second, was SARS-CoV-2 that different from other viruses? The very fact that the virus was named “SARS-CoV-2” informs us that virologists think it is similar enough to SARS that it didn’t even warrant an entirely new name. Indeed, the two viruses are said to share “79.5% sequence identity.” [13] Despite the 20.5% difference, and notwithstanding the 17 year time lapse, studies have shown that people that were infected with SARS “possess long-lasting memory T cells… that displayed robust cross-reactivity to the N-protein of SARS-CoV-2.”[14] Therefore, although possessing differences, it cannot be said that this virus is that different from other coronaviruses.
Third, was this virus newly capable of infecting humans? To answer this question, it may help to consider RaTG13, a bat coronavirus that is said to be the closest to our virus. The two viruses are reported to be 96% similar.[15] Although it is commonly assumed that bat coronaviruses cannot infect humans without either a modification to its RNA or via an intermediate host, it is possible that bat coronaviruses jump to humans all the time, only without making us sick. For instance, a study done in 2018 found good evidence to conclude that bat coronaviruses are capable of infecting humans regularly, noting also that the “infections were subclinical or caused only mild symptoms.” [16] Conversely, experiments with blood samples of health care workers known to have had Covid demonstrated efficient neutralization of RaTG13.[15] Of particular significance in this regard is the little known fact that the PCR test for Covid, as designed by Drosten, was initially verified by making sure it detected coronaviruses from “bats in Europe and Asia.”[17] In other words, a positive PCR test may have indicated nothing more or less than the presence of a harmless bat coronavirus already endemic among humans. Although the Drosten test was later superseded by other tests, the official narrative emerged rapidly out of case detection using the Drosten test. Unfortunately, it is not clear to what extent this influenced early test results. In any case, it is certainly not novel that a virus of this sort could infect humans.
Fourth, is this virus entirely new to our immune system? Certainly not, for it was known from early on in the Covid-era that a significant percentage of people were immune to this supposedly novel virus. We previously observed that only 19% (712 of 3711) of the people on board the Diamond Princess cruise ship tested positive for the virus, and of these only a smaller fraction yet actually became ill.[4] Similarly, a group of researchers from Singapore “detected SARS-CoV-2 specific T cells in individuals with no history of SARS [or] Covid-19.” Remarkably, they also detected T cells in people that had no known contact with anyone that had had either SARS or Covid.[14] Likewise, a study in the UK found that many health care workers repeatedly tested negative despite repeated exposure to Covid.[18] The authors of that study concluded that “some individuals may clear subclinical infection before seroconversion.” Why did so many people never get Covid? Multiple researchers have concluded that it was likely a result of memory T-cells from a previous infection with a common cold or flu.[19, 20, 21, 22]
What percentage of people had sufficient prior immunity to prevent illness? Those same researchers found it was about 50%. For instance, a study by Grifoni et al “detected SARS-CoV-2-reactive CD4+ T cells in ~ 40% – 60% of unexposed individuals, suggesting cross-reactive T cell recognition between circulating ‘common cold’ coronaviruses and SARS-CoV-2.” [23] In other words, about half the population was destined to never become noticeably ill from Covid for the simple reason that they recently had a cold. Nor is this particularly surprising since it was known that the original SARS virus had also cross-reacted with other coronaviruses.[24] Thus, the virus was not entirely novel to our immune system.
Fifth, was this virus new to doctors? As may be gathered from the fact that Covid was around long before March 2020, it is almost certain that before doctors were told that they were dealing with a novel virus that they supposedly did not know how to treat, they must have unknowingly treated Covid as if it was any normal respiratory or influenza-like-illness. To the best of our knowledge, there is no record of doctors reporting an unusual increase in untreatable respiratory disease, at least not until the WHO officially declared Covid a pandemic. Even after doctors were advised it was an entirely new disease, treatment protocols were rapidly developed in multiple places.[25, 26, 27]
In summary, SARS-CoV-2 was “novel” only in the sense that it was first discovered in early 2020. It is certain that it existed globally for at least six months before this. Already by January 2020 about half the world’s population was immune to this virus. Nor was Covid outside the parameters of known treatments available for respiratory diseases. These facts should have been front and center in the media, and should have had a strong influence on government policies. Sadly, all this information was buried.
Of course, if Covid was not novel, it is impossible that it should have caused any excess deaths in 2020. It follows from this sobering conclusion that any and all excess deaths had to have been caused by other factors.
2. How deadly was Covid?
As was just pointed out, at least half of the population was essentially immune to Covid. For these people Covid was a non-issue. What about the other half? How lethal was it for them? Central to a proper answer of this question is the fact that our immune system is confronted with novel proteins all the time. Our survival does not depend on us having seen them or anything similar before. Rather, the immune system learns from all foreign material, remembers the experience, and serves to make future encounters less noteworthy. If at some point in the future a virus should arise that was both novel to our immune system and untreatable, even this would not necessarily mean that the virus was something to fear; certainly not to the extent of causing a cataclysm like we have recently witnessed.
In a previous article of this series [1] we made mention of a World Health Organization bulletin that estimated the Infection Fatality Rate (IFR) of Covid to be 0.23%.[28] That same bulletin also advised it might be substantially less than this. As data accumulated, the IFR was indeed found to be lower, eventually converging on a global average of about 0.15%.[29] For people under 70 years old, the average IFR of Covid drops down to 0.07%.[30] Of course these estimates were determined using information from death certificates and PCR test results, which (as shall be explained below) may have introduced significant inflationary errors into the results. The IFR of Covid may therefore be much less than 0.15%.
Moreover, it is well established that severe Covid illness is generally linked to those with underlying medical conditions, meaning it is rare in healthy individuals. For instance, a study looking at more than half a million people hospitalized in the USA with Covid found that 94.9% “had at least 1 underlying medical condition.” [31]
Nevertheless, for the sake of argument let us accept these estimates at face value and proceed to ask how Covid compares with the flu? The IFR of influenza is generally considered to be about 0.1%, and in a typical season about 8% of Americans get sick from the flu.[32] As for Covid, despite the unprecedented numbers of people that were tested for this virus, the total number of Covid cases in the USA during 2020 totaled 19.2 million,[33] or about 5.7% of the population. Thus, by all metrics it would appear that Covid in 2020 was on par with or less than a normal flu season.
The fact that Covid is not a particularly lethal disease was known since early 2020. For instance, the UK government officially declared that “as of 19 March 2020, Covid-19 is no longer considered to be an HCID in the UK.” [34] The acronym HCID stands for “high consequence infectious diseases.” Therefore, for the vast majority of people, the wonderful and immensely complicated human immune system was more than adequate to fight off a Covid infection.
If in fact Covid was only as bad as a normal flu season, why did it garner so much attention? And why have government dashboards suggested that Covid is causing millions of excess deaths in the world? The answer to the first of these two questions will have to be postponed for a future article. As for the second question, it is helpful to look a little closer at excess deaths in 2020. A recent study by Levitt et al analyzed all-cause mortality rates in 33 countries from 2009 to 2021. They found that during this 13 year window, the year 2020 was the worst year with the highest mortality for only four countries: “UK, Italy, Spain and Belgium.” [35] Another 10 countries had “the highest mortality in 2021.” (USA and Poland were the worst). As for the remaining 19 countries, either 2009 or 2010 had the highest mortality.
Was there anything particularly special about 2009 that made it the worst year for more than half these countries? Actually, it was found to be the worst for two simple reasons: mortality rates have in general been decreasing over time, and 2009 is as far back as the study went. Of interest is that in 2009 the WHO declared a pandemic on account of the H1N1 virus. Nothing special came of it, however, for “the total number of influenza-related deaths worldwide… proved similar to the number in a relatively mild year of seasonal influenza.” [36]
The fact that 2020 was the worst year for only 4 of these 33 countries lends support to our conclusion that Covid was about as bad as a normal flu season. The fact that 2021 was the worst year for 10 countries helps reinforce our previous findings that the Covid shots did very little to prevent Covid deaths and instead caused a great deal of deaths from adverse events.
3. Covid Data Issues
How is it possible that a mortality analysis seems to contradict reports about millions of Covid cases and deaths? There are several good reasons for this apparent discrepancy. For starters, and as was mentioned in a previous article,[1] on April 20, 2020 the WHO mandated changes to the way death certificates were to be filled out. The document stated that “a death due to Covid-19 is defined for surveillance purposes as a death resulting from a clinically compatible illness.” [37] In other words, since influenza typically has identical symptoms to Covid, flu deaths were to be labeled as Covid deaths. While this may be useful for “surveillance purposes,” it does not help us determine if Covid caused any excess deaths. Nor is it useful for making accurate comparisons between Covid and the flu. And it most definitely makes it difficult to calculate the IFR of Covid.
The WHO document went on to say: “A death due to Covid-19 may not be attributed to another disease (e.g. cancer)… Always apply these instructions whether they can be considered medically correct or not.” Therefore, even if cancer was the actual cause of death, if the person so much as tested positive for Covid, the death certificate was to say that Covid was the cause of death. The end result of this change in policy is that the number of deaths caused by Covid has been significantly over-counted in most countries.[38, 39, 40, 41] What was not affected by the protocol change was how many people died from all causes. This is why all-cause mortality studies are so relevant during the Covid-era.
Another issue muddying the waters is the PCR test used to identify a Covid case. Despite the fact that the PCR test is based on remarkable technology, it has various shortcomings when used as it was to establish a Covid case. Very briefly, a few such issues are:
- If the cycle threshold is too high, it will return a high number of false positives.[42]
- As disease prevalence decreases, the risk of false positives increases.[43, 44]
- The number and type of primers used for identifying the presence of SARS-CoV-2 has the potential to pick up fragments originating from some other source.[45, 46] (As we saw above, harmless bat coronaviruses may give a false positive.)
- The PCR test is capable of finding virus fragments,or intact virus in the airway, but is not capable of determining if a person is actually infected with Covid. Since clinical symptoms were not required to be present, many uninfected individuals falsely tested positive. [47, 48]
Every issue listed above has the tendency to inflate Covid deaths.
4. Covid in Canada
To put things into perspective, and to tie all these ideas together, it is appropriate to consider one particular country in more detail as an example. Let us consider Canada. Statistics Canada records that 16,151 deaths in 2020 were attributed to Covid.[49] This is slightly more than twice the number of deaths attributed to “Influenza and Pneumonia” in an average year in Canada (7304 deaths/yr). How is it possible that Covid was more than twice as deadly as the flu if the two illnesses are about the same?
The answer is either that the number of Covid deaths was overcounted due to all the issues just mentioned or that influenza deaths were underdiagnosed in the past. Unfortunately, it is now nearly impossible to determine the exact error rate. Nevertheless, by considering only the last of the issues in the above list, it is possible to demonstrate how significant the inflation factor really is.
Dr. Bullard, head of the provincial laboratory in Winnipeg Manitoba, testified that PCR tests do not verify infection and were never intended to be used to diagnose respiratory illness.[50] He went on to say that about 56% of positives in Canada belonged to people that were not infected with Covid. If we accept this percentage, in all likelihood at least 56% of the deaths attributed to Covid in Canada were a result of a false positive. Applying this error rate to Covid deaths in Canada in 2020 brings the number of deaths down to 7,106. It is duly noted that this number is slightly lower than the yearly average for influenza deaths in the preceding four years. If we use this adjusted amount, and plot mortality in Canada in 2020 by the top 15 leading causes of death, we can see the relative significance of Covid in Canada.

Figure 1. Source: Statistics Canada. Table 13-10-0392-01
Covid mortality was adjusted down by 56% to account for false positives.
In Figure 1 above, cancer and heart issues dwarf all other causes of death. The number of deaths attributed to flu and pneumonia is several thousand below average. This resulted from the fact that, according to the WHO mandate, many deaths that would normally have been classified as influenza were labeled as Covid because the two are clinically compatible illnesses. Also, Canadian labs changed the way they tested for the flu: “changes in laboratory testing practices as a result of the public health response to… Covid-19… may affect the comparability of data to previous… seasons.” [51] What is clear from this chart is that Covid was not particularly lethal, was no worse than a normal flu season, and certainly unworthy of the unprecedented attention it received.
Conclusion
In conclusion, it is safe to say that SARS-CoV-2 was “novel” in early 2020 solely because of the simple fact that that is when it was first detected. Not only was Covid treatable, but at least 50% of people had sufficient immunity from a previous common cold to prevent noticeable illness. It can also be said that Covid was not unusually lethal, since the mortality burden was only as bad as a normal flu season. Covid mortality (when adjusted for only one of several factors) ranked ninth among the leading causes of death in Canada, the same rank normally held by influenza and pneumonia.
Of course, it could be argued that the reason Covid deaths were this low is because government mandated lockdowns and other non-pharmaceutical interventions prevented a Covid catastrophe. It is this important topic that we plan to cover in our next article of this series.
References
- Kenyon, Todd et al, “It is impossible that the vaccines saved 14 million lives in 2021,” Panda, 2023, https://pandata.org/drivers-of-excess-deaths-part1/
- Verduyn et al, “How many lives were actually saved by the Covid-19 vaccines?” Panda, 2023, https://pandata.org/how-many-lives-were-actually-saved-by-the-covid-19-vaccines/
- Kenyon, Todd et al, “What the Diamond Princess tells us about NYC in spring 2020,” Panda, 2023, https://pandata.org/what-the-diamond-princess-tells-us-about-nyc-in-spring-2020/
- Verduyn, Thomas et al, “Did side effects from the Covid shots cause an excess mortality?” Panda, 2023, https://pandata.org/did-side-effects-from-the-covid-shots-cause-any-excess-mortality/
- Akronson, Jeffrey, “Covid-19: First coronavirus was described in The BMJ in 1965,” BMJ 2020;369:m1547
- Mulley, Kary, US Patent, 1987, http://patentimages.storage.googleapis.com/cc/f0/3e/dc51b1fb4af2e6/US4683202.pdf
- Morris, Dylan, “Novelty Means Severity: The Key To the Pandemic,” Insight, 2021, https://www.theinsight.org/p/novelty-means-severity-the-key-to
- Billingsley, Alyssa, Pinto-Garcia, Patricia, “The Novel Coronavirus: What Are Novel Viruses, and How Do They Impact Public Health?” GoodRx Health, 2023, https://www.goodrx.com/conditions/covid-19/what-does-novel-coronavirus-mean-science-medical-definition
- István Csabai, Krisztián Papp, Dávid Visontai et al. “Unique SARS-CoV-2 variant found in public sequence data of Antarctic soil samples collected in 2018-2019,” 23 December 2021, PREPRINT (Version 1) available at Research Square https://doi.org/10.21203/rs.3.rs-1177047/v1
- Apolone G, Montomoli E, Manenti A, et al. “Unexpected detection of SARS-CoV-2 antibodies in the prepandemic period in Italy.” Tumori Journal. 2021;107(5):446-451. doi:10.1177/0300891620974755
- Antonella Amendola, et al, “Molecular evidence for SARS-CoV-2 in samples collected from patients with morbilliform eruptions since late 2019 in Lombardy, northern Italy,” Environmental Research, Volume 215, Part 1, 2022, 113979,ISSN 0013-9351, https://www.sciencedirect.com/science/article/pii/S0013935122013068
- Jones, Will, “The Evidence COVID-19 Was Spreading Silently Around the World in Late 2019,” 2022, The Daily Sceptic, The Evidence COVID-19 Was Spreading Silently Around the World in Late 2019 – The Daily Sceptic
- Rossi GA, Sacco O, Mancino E, Cristiani L, Midulla F. “Differences and similarities between SARS-CoV and SARS-CoV-2: spike receptor-binding domain recognition and host cell infection with support of cellular serine proteases.” Infection. 2020 Oct;48(5):665-669. doi: 10.1007/s15010-020-01486-5. Epub 2020 Jul 31. PMID: 32737833; PMCID: PMC7393809
- Le Bert, N., Tan, A.T., Kunasegaran, K. et al. “SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls.” Nature 584, 457–462 (2020). https://doi.org/10.1038/s41586-020-2550-z
- Cantoni, D., Mayora-Neto, M., Thakur, N. et al. “Pseudotyped Bat Coronavirus RaTG13 is efficiently neutralised by convalescent sera from SARS-CoV-2 infected patients.” Commun Biol 5, 409 (2022). https://doi.org/10.1038/s42003-022-03325-9
- Wang, N., Li, SY., Yang, XL. et al. “Serological Evidence of Bat SARS-Related Coronavirus Infection in Humans, China.” Virol. Sin. 33, 104–107 (2018). https://doi.org/10.1007/s12250-018-0012-7
- Corman, Victor M et al, “Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR,” Eurosurveillance, 25, 2000045 (2020), https://doi.org/10.2807/1560-7917.ES.2020.25.3.2000045
- Swadling, L., Diniz, M.O., Schmidt, N.M. et al. “Pre-existing polymerase-specific T cells expand in abortive seronegative SARS-CoV-2.” Nature 601, 110–117 (2022). https://doi.org/10.1038/s41586-021-04186-8
- Jose Mateus et al., “Selective and cross-reactive SARS-CoV-2 T cell epitopes in unexposed humans.” Science, 370,89-94(2020). DOI:10.1126/science.abd3871
- Lipsitch, M., Grad, Y.H., Sette, A. et al. “Cross-reactive memory T cells and herd immunity to SARS-CoV-2.” Nat Rev Immunol 20, 709–713 (2020). https://doi.org/10.1038/s41577-020-00460-4
- Humbert, Marion et al, “Functional SARS-CoV-2 cross-reactive CD4+ T cells established in early childhood decline with age,” PNAS, 2023, https://doi.org/10.1073/pnas.2220320120
- Mahajan, S., Kode, V., Bhojak, K. et al. “Immunodominant T-cell epitopes from the SARS-CoV-2 spike antigen reveal robust pre-existing T-cell immunity in unexposed individuals.” Sci Rep 11, 13164 (2021). https://doi.org/10.1038/s41598-021-92521-4
- Grifoni, Alba et al, “Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals,” Cell, 2020, DOI:https://doi.org/10.1016/j.cell.2020.05.015
- Patrick, David et al, “An Outbreak of Human Coronavirus OC43 Infection and Serological Cross-Reactivity with SARS Coronavirus,” Canadian Journal of Infectious Diseases and Medical Microbiology, 2006, https://doi.org/10.1155/2006/152612
- Front Line Covid Critical Care Alliance, Treatment Protocol, https://covid19criticalcare.com/treatment-protocols/
- Heart Advisory & Recovery Team, Ivermectin, https://www.hartgroup.org/category/ivermectin/
- McCullough PA, et al, “Multifaceted highly targeted sequential multidrug treatment of early ambulatory high-risk SARS-CoV-2 infection (COVID-19).” Rev Cardiovasc Med. 2020 Dec 30;21(4):517-530. doi: 10.31083/j.rcm.2020.04.264. PMID: 33387997.
- Ioannidis, John P A. (2021). “Infection fatality rate of COVID-19 inferred from seroprevalence data.” Bulletin of the World Health Organization, 99 (1), 19 – 33F. World Health Organization. http://dx.doi.org/10.2471/BLT.20.265892
- Ioannidis, John P A. “Reconciling estimates of global spread and infection fatality rates of COVID-19: An overview of systematic evaluations,” European Journal of Clinical Investigation, 2021, https://doi.org/10.1111/eci.13554
- Pezzullo AM, Axfors C, Contopoulos-Ioannidis DG, Apostolatos A, Ioannidis JPA. “Age-stratified infection fatality rate of COVID-19 in the non-elderly population.” Environ Res. 2023 Jan 1;216(Pt 3):114655. doi: 10.1016/j.envres.2022.114655. Epub 2022 Oct 28. PMID: 36341800; PMCID: PMC9613797.
- Kompaniyets, Lyudmyla et al, “Underlying Medical Conditions and Severe Illness Among 540,667 Adults Hospitalized With COVID-19, March 2020–March 2021,” CDC 2021, DOI: http://dx.doi.org/10.5888/pcd18.210123external icon
- Anonymous, “Key Facts About Influenza (Flu),” CDC 2022, https://www.cdc.gov/flu/about/keyfacts.htm
- Anonymous, Our World In Data, Coronavirus (COVID-19) Cases – Our World in Data
- Anonymous, “Guidance High consequence infectious diseases (HCID),” UK government, 2020, https://www.gov.uk/guidance/high-consequence-infectious-diseases-hcid
- Levitt, M., Zonta, F. & Ioannidis, J.P.A. “Excess death estimates from multiverse analysis in 2009–2021.” Eur J Epidemiol (2023). https://doi.org/10.1007/s10654-023-00998-2
- Fineberg, Harvey, “Pandemic Preparedness and Response — Lessons from the H1N1 Influenza of 2009,” N Engl J Med 2014; 370:1335-1342 DOI: 10.1056/NEJMra1208802
- Anonymous, “International Guidelines for Certification and Classification (coding) of Covid-19 as Cause of Death,” World Health Organization, 2020, https://cdn.who.int/media/docs/default-source/classification/icd/covid-19/guidelines-cause-of-death-covid-19-20200420-en.pdf (pg 3)
- Audie, Joseph, “Using CDC data and death certificate standards to propose a preliminary estimate for the number of US COVID-19 associated deaths that were caused by or contributed to by SARS-CoV-2 infection,” Research Gate, 2020, https://www.researchgate.net/publication/344228032_Using_CDC_data_and_death_certificate_standards_to_propose_a_preliminary_estimate_for_the_number_of_US_COVID-19_associated_deaths_that_were_caused_by_or_contributed_to_by_SARS-CoV-2_infection
- Fenton, Norman & Neil, Martin & McLachlan, Scott. (2021). What proportion of people with COVID-19 do not get symptoms?. 10.13140/RG.2.2.33939.60968.
- Jensen, Scott, 2023, https://www.youtube.com/watch?app=desktop&v=PHxj_Luclxs&feature=youtu.be
- Beaudoin, John, “500,000 Death Certificates Tell of Signals, Fraud, and Unlawful Deaths,” 2023, https://rumble.com/v2a7wtk-john-beaudoin-500000-death-certificates-tell-of-signals-fraud-and-unlawful-.html
- La Scola B, Le Bideau M, Andreani J, Hoang VT, Grimaldier C, Colson P, Gautret P, Raoult D. “Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards.” Eur J Clin Microbiol Infect Dis. 2020 Jun;39(6):1059-1061. doi: 10.1007/s10096-020-03913-9. Epub 2020 Apr 27. PMID: 32342252; PMCID: PMC7185831.
- Anonymous, “WHO Information Notice for Users 2020/05: Nucleic acid testing (NAT) technologies that use polymerase chain reaction (PCR) for detection of SARS-CoV-2,” World Health Organization, 2021, https://www.who.int/news/item/20-01-2021-who-information-notice-for-ivd-users-2020-05
- Deeks, John, “Why the school testing regime needs to change,” The Post, 2021, https://unherd.com/thepost/why-the-school-testing-regime-needs-to-change/
- Neil, Martin, “Put to the test: use of rapid testing technologies for covid-19,” BMJ 2021; 372 doi: https://doi.org/10.1136/bmj.n208
- Neil, Martin, “UK lighthouse laboratories testing for SARS-COV-2 may have breached WHO Emergency Use Assessment and potentially violated Manufacturer Instructions for Use.” Probability and Risk, 2021, https://probabilityandlaw.blogspot.com/2021/02/uk-lighthouse-laboratories-testing-for.html?m=1
- Deeks, Jonathan, “Operation Moonshot proposals are scientifically unsound,” BMJ 2020; 370 doi: https://doi.org/10.1136/bmj.m3699
- Pollock A M, Lancaster J. “Asymptomatic transmission of covid-19” BMJ 2020; 371 :m4851 doi:10.1136/bmj.m4851
- Anonymous, Statistics Canada. Table 13-10-0392-01 “Deaths and age-specific mortality rates, by selected grouped causes” DOI: https://doi.org/10.25318/1310039201-eng
- Anonymous, “Manitoba Chief Microbiologist and Laboratory Specialist: 56% of positive “cases” are not infectious,” JCCF, 2021, https://www.jccf.ca/manitoba-chief-microbiologist-and-laboratory-specialist-56-of-positive-cases-are-not-infectious/
- Government of Canada, “FluWatch annual report: 2019-2020 influenza season,” 2021, https://www.canada.ca/en/public-health/services/publications/diseases-conditions/fluwatch/2019-2020/annual-report.html
FDA responds to negative efficacy of variant boosters with another variant booster
By Daniel Horowitz – conservative review – June 21, 2023
The human experimentation of Operation Warp Speed was not an anomaly; it is the new normal, and the FDA is just getting started. The agency is now allowing the COVID vaccine manufacturers to change the formulation of their shots to continue to chase variants, themselves created by antigenic drift of the shots. And they continue to do so based on nothing more than measuring antibody titer levels. No human clinical trials necessary! Except, studies now show, and reality confirms, the more they chase variants, the more they create negative efficacy against the existing variant, thereby engendering a “need” for another formulation.
What was the response of the FDA to the increasing news of cataclysmic injuries and negative efficacy of the COVID shots for variants that are no longer dangerous? Last Thursday, the FDA’s VRBPAC unanimously approved a fall booster, advising Pfizer, Moderna, and Novavax to update their formulations for the so-called XBB.1.5 Omicron variant. So, officials pre-emptively approved a shot that doesn’t exist based on antibody level testing without human trials – all for a variant that not only is not dangerous but will actually be extinct by the time this poison reaches the market, just as they did with the bivalent formulation for the BA.4 and BA.4 variants.
To this day, the bivalent shot is the only one available, and according to the CDC, that variant doesn’t even exist! It is true that very few people are dumb enough to get this shot, but what they are trying to do is create an endemic schedule of COVID shots to time perfectly with the flu shots in the fall. They have already groomed people over the generation to “get their flu shot” every fall. So now the pharmacies will be waiting with the COVID needle to complete their seasonal updates.
So, what happens when you keep tricking the body to respond to a virus for strains that no longer exist? As the FDA approved these shots, the agency already had the peer-reviewed Cleveland Clinic study showing negative efficacy of the original COVID shots. Just days before this meeting, the Cleveland Clinic came out with a preprint showing negative efficacy for the bivalent booster shots too.
The study contrasted 11,990 employees of this venerable institution who chose to be “up to date” with the bivalent boosters compared to 36,344 employees who were “not up to date” and tracked their outcomes. It turns out that after about three and a half months, you were about 25% more likely to get COVID after having gotten the boosters as compared to the control group.

After adjusting for confounding factors between the groups, the study authors actually found a 33% rate of negative efficacy!
“This study’s findings question the wisdom of promoting the idea that every person needs to be ‘up-to-date’ on COVID-19 vaccination, as currently defined, at this time,” conclude the Cleveland Clinic researchers. They also observe, “It should be pointed out that there is not a single study that has shown that the COVID-19 bivalent vaccine protects against severe disease or death caused by the XBB lineages of the Omicron variant.”
The push for boosters comes at a time when more evidence proves a strong correlation between excess deaths and the vaccine take-up. A letter published in a peer-reviewed journal of Medicine and Clinical Science shows that Japan and Germany, two highly vaccinated countries, experienced sharp excess deaths coinciding with the vaccine take-up. They found very little excess death during the pandemic months before the vaccine was rolled out.
“It should be investigated to what extent the about 5%-10% highly significantly increased mortalities in Germany and Japan in 2021 and 2022 might be due to the pandemic countermeasures, including the vaccinations with their possibly underestimated immediate or protracted side effects,” concluded the researchers from Japan and Germany.
“From this point of view, it seems possible that a high vaccination rate has contributed to an increased all-cause mortality in some countries.”
The twisted irony is that, according to the CDC’s variant tracker, XBB.1.5 has gone from 80% of cases to less than 40% of cases in just a few months. It will clearly be obsolete by the fall. None of this was discussed at the FDA hearing. Of course, nothing about Pfizer’s own document showing five million cumulative reports of adverse events affecting every organ system was ever discussed. Hence, we have record injuries, negative efficacy, long-term immune imprinting causing the body to constantly respond inappropriately to wrong strains of the virus – all for a virus that is no longer deadly and for a population that has already gotten the virus!
That’s not just a lousy cost-benefit analysis; that is premeditated murder against the American people. What is the GOP plan to stop this? Or do Republicans even care? How can they continue to fund more COVID shots in the HHS appropriations bill, much less the broader FDA/CDC scheme to create new dangerous shots at warp speed?
Just how callously does the FDA regard human life? After its own VAERS system exploded with every adverse event imaginable, an outcome we now know officials anticipated, to this day they have not followed up on those safety signals. For example, according to the Informed Consent Action Network, the Standard Operating Procedures and Policies document for the FDA’s Vaccine Safety Team requires that its staff members identify VAERS adverse event reports that “need a rapid response and complex coordination,” after which they are supposed to “immediately” inform certain FDA management, who then alert other sub-agencies. Did that occur?
Well, more than a year after the ICAN’s record request, the agency responded, “A search of our records did not locate any documents responsive to your request.”
Where is the action from the House GOP? Why are they still only investigating the shutdown of schools in the past, but not the ongoing, premediated unleashing of deadly products on the American people?
Never in my wildest dreams…
… or never in my wildest nightmares?
Health Advisory & Recovery Team | June 23, 2023
This was the opening phrase in a Twitter post from Dr Lisa Iannattone,on 15 June. The whole Tweet read, “Never in my wildest dreams could I have predicted a future where a new virus would become the #1 infectious disease killer of children and that medical leadership would decide the vaccine for this virus is NOT important for kids, and NOT promote it”
Those of us at HART might rephrase this, “Never in my wildest NIGHTMARE could I have predicted a future where, for a virus with such a low impact on children, medical leadership would decide that a novel-technology vaccine with NO long-term safety data IS important for kids to take and WOULD promote it — and in some countries even mandate it — in a vain attempt to protect their grandparents”.
The tweet was linked to this news item from Oxford University dated 31st January 2023 so it seems to have taken Dr L several months to read it! “A new study led by researchers at the University of Oxford’s Department of Computer Science has found that, between 2021 and 2022, COVID-19 was a leading cause of death in children and young people in the United States, ranking eighth overall. The results demonstrate that pharmaceutical and public health interventions should continue to be applied to limit the spread of the coronavirus and protect against severe disease in this age group.”
The study itself used publicly available US data to look at deaths in children and young people (CYP) aged 0-19, where COVID-19 was ‘the underlying cause of death’ and to look at rankings of causes of death from 2019 onwards. The finding emphasised in the Tweet was that COVID-19 ranked “first in deaths caused by infectious or respiratory diseases.” The next sentence, unsurprisingly omitted from the Tweet, is however vital when putting this into context “COVID-19 deaths constituted 2% of all causes of death in this age group.”
A group looking at data in England from March 2020 to March 2021, found that deaths of children with a positive PCR test gave a similar 2% of all childhood deaths. However, unlike the more recent US study, this study did a thorough notes review for all the deaths and found that in less than half of the cases was COVID-19 either the underlying or a contributory cause of death, accounting for only 0.8% of total deaths for this age group. Fortunately, child deaths are rare and a Child Death Review system has been in place in England and Wales since 2008 to look for preventable causes, so the idea of looking at cases in detail is nothing new.
Like the importance of looking at absolute risk reduction rather than relative risk reduction for judging vaccine efficacy, it is vital to look at the absolute risk of a child dying from COVID-19. Whilst any child death is a tragedy for the family concerned, the risk of death from a respiratory virus is small compared with risks of say accidental death or suicide, which are also conditions the reduction of which should be the concern of Public Health departments. People, including children, dying of other conditions also find it harder to fight off viral infections. It is therefore inevitable that excessive testing will link viruses to dying children. However, the idea that these deaths could have been prevented has no basis in evidence.
It is noteworthy that the number of deaths in under 20s in the US, did not diminish with the arrival of the vaccines — one could even be forgiven for thinking they have increased.

Peter Hotez: Why He Won’t Debate
Another Sign that We’re Winning
By Fed Up Texas Chick | Dr. Tenpenny’s Eye on the Evidence | June 24, 2023
“Peter, if you claim what RFK Jr. is saying is misinformation, I am offering you $100,000 to the charity of your choice to debate him on my show with no time limit.”
And the little worm squirmed.
The worm I am referring to is Dr. Peter Hotez, and the quote above is from Joe Rogan. At the writing of this article, Joe Rogan’s challenge to Hotez has been viewed over 25 million times on Twitter. The money is being crowdsourced and has grown to $2.6 million thus far. Apparently, a lot of folks want to see this debate.
It all started with a long three-hour podcast interview between Joe Rogan and his guest, Robert F. Kennedy Jr., who has done incredible work with the Children’s Health Defense and is an outspoken opponent of vaccines. If you missed it podcast, here is an unedited version.
RFK Jr. expressed all sorts of opinions, which is any American’s right, about autism, the COVID vaccines, and the CIA’s involvement in the murder of his father and uncle President JFK. In particular, he touted the use of the anti-parasitic drug ivermectin and the anti-malaria drug hydroxychloroquine to treat COVID in lieu of the vaccines.
Apparently, Hotez took issue with this, which is very interesting, given that he is the dean for the National School of Tropical Medicine at Baylor College of Medicine in Houston’s Texas Medical Center. His personal website says he leads a team that is “developing new vaccines for hookworm infection, schistosomiasis, leishmaniasis, Chagas disease, and SARS/MERS/SARS-2 coronavirus diseases.” Naturally, he promotes global access to vaccines, because he directly benefits financially. If anyone should know about antiparasitic and antimalarial drugs, it’s Hotez, right? Why wouldn’t he be able to hold his own in a debate on tropical medicine?
Hotez knows about the value of ivermectin, because he wrote a paper on it in 2007 that was published in New England Journal of Medicine that discussed the history of the drug’s effectiveness. But rather than engaging in the challenge to debate RFK and “bury him once and for all,” Hotez took to Twitter. He promptly asked for a $50 million endowment because Rogan and Kennedy are so stinkin’ rich. He tried to get money from them to continue his work “making low-cost patent-free vaccines for the world’s poor.”
Hotez also asked for a public apology from RFK Jr.
Mostly, Hotez is pissed about RFK Jr’s anti-vax status, challenging his work and making him non-essential. Hotez has too good of a gig, actually, and doesn’t want anyone interfering with his gravy train. Let’s explore that gravy train…
Pfizer
Hotez has been in lock step with Pfizer for decades. Redacted News reporter Dan Cohen did a two part deep dive into Hotez and his past; I highly recommend watching it. Cohen reveals that Hotez started receiving money from Pfizer straight out of college, and he hasn’t stopped. And Hotez seems to only appear on Pfizer-backed channels, such as MSNBC.
This explains why Hotez praised Pfizer’s Covid-19 clinical trial results for children aged 12 to 15 as “pretty impressive”. The trial showed 100% efficacy, but we now know that Pfizer lied.
Lofty Colleagues: Gates and Fauci
Hotez also has an international status to protect. In 2022, he and colleague Dr. Maria Elena Bottazzi were nominated for the Nobel Peace Prize for their work to develop and distribute a low-cost COVID-19 vaccine “to people of the world without patent limitation.”
According to his personal bio, Hotez has been developing recombinant protein coronavirus vaccines for SARS and MERS for more than a decade at Texas Children’s Hospital.
In 2020, he developed the first recombinant protein COVID-19 through microbial fermentation in yeast. Hotez has a connection to researcher Zhengli Shi, more commonly known as the Wuhan Institute of Virology “bat lady.” They worked together to develop a lab-generated (i.e. man-made) chimeric SARS-related coronavirus. Their work was was funded through an NIH grant, a grant that also provided funding for two of Shi’s staff.
Hmmm. Is this gain of function research? How about this hot new revelation from Kanekoa News :
In a groundbreaking revelation, it has come to light that Dr. Peter Hotez has been entangled in a web of funding, collaboration, and research with Chinese military scientists potentially involved in the development of COVID-19. The intricate tale weaves together key Chinese military virologists and culminates in the smoking gun evidence surrounding COVID-19’s notorious furin cleavage site.
So far, Hotez’s jab technology has been sent to four countries:
- India (Biological E, CORBEVAX),
- Indonesia (BioFarma, CORONAVAC),
- Bangladesh (Incepta) and
- Botswana (ImmunityBio).
More than 100 million doses have been administered in India and Indonesia. Gosh, he sounds like Bill Gates, doesn’t he? Maybe that’s because they also work together.
Here is an article from 2021 that starts,
“The Bill Gates-funded doctor is very displeased that you aren’t blindly genuflecting before his unassailable brilliance.” This is another article that is definitely worth reading.
There are many videos on the internet where Bill Gates is singing Hotez’s praises. This is blatant propaganda: Hotez is a salesman, not a scientist.
Lately, Hotez’s messaging has turned militant. What is he militant about? Anti-vaxxers. And anti-science promoted by anti-vaxxers, people like RFK Jr. You would think he would be chomping at the bit at the chance to debate him. He sticks to Twitter.
For example, his December 2022 Tweet where the WHO prominently features his militant attitude: Hotez says that anti-vaxxers have become a global killing force, and that anti-science kills more people than “gun violence, global terrorism, nuclear proliferation and cyberattacks.”
Wow, just wow.
He is particularly militant about, and protective of, Dr. Anthony Fauci. After Fauci stepped down from NIH late last year, Hotez was on the short list as a likely successor. In fact, Children’s Health Defense re-published an article, originally written by Dr. Joseph Mercola, wondering if he would assume Fauci’s role. Mercola’s article is a deep dive into Hotez’s world, and highly recommended reading.
In 2021, Hotez actually said it should be a federal hate crime to criticize Fauci and other government-funded scientists. Yes, he really said that. But we know that name-calling is the last resort for those who have no grounds for an argument.
The Clintons and Obama
It is actually perplexing that Hotez didn’t take Rogan up on a chance at a large charity donation, particularly since Hotez has such a penchant for nonprofit work. After all, he worked for the Clinton Global Health Initiative and, in 2006, that helped him found the Global Network for Neglected Tropical Diseases to “provide access to essential medicines for hundreds of millions of people.” This is not anti-science; it comes from his own bio, linked above.
Take a gander at the rest of Hotez’s resume. From 2014 to 2016, he served in the Obama Administration as a US envoy to focus on vaccine diplomacy between the US government and North Africa and countries in the Middle East.
I literally could go on and on and write an 8,000-word expose on Hotez, but I won’t.
Hotez is a self-proclaimed saint who ‘toils tirelessly’ to develop vaccines for the world’s poor. At the same time, he wants to criminalize the questioning of vaccine safety and use cyberwarfare against anti-vaxxers to literally snuff them out. Journalist Paul Thacker wrote a great piece (2022) entitled, “Peter Hotez Sees Aggression Everywhere But in the Mirror.”
Hotez is a paradox, but many see his true colors. Is Hotez a scientist or a salesman? Is he a prominent physician or a political operative peddling propaganda? Is he a Mother-Theresa-like figure helping the world’s poor, or is he one of the most hateful and dangerous people in medicine today?
You be the judge.
Fed Up Texas Chick is a contributing writer for The Tenpenny Report (at http://www.Vaxxter.com) She’s a rocket scientist turned writer, having worked in the space program for many years. She is a seasoned medical writer and researcher who is fighting for medical freedom for all of us through her work.
Featured Video

Rewriting the risk? Inside the government’s vaccine safety messaging
or go to
Aletho News Archives – Video-Images
Book Review
“Davos Can Really Replace the UN”
Inside the book that maps the architecture behind global governance — from the Epstein files to the Pact for the Future
Lies are Unbekoming | April 1, 2026
On June 13, 2019, the United Nations and the World Economic Forum signed a partnership deal to “accelerate the implementation of the 2030 Agenda for Sustainable Development.” That same evening, WEF president Börge Brende — Norway’s former Foreign Minister — had dinner with Jeffrey Epstein at Epstein’s Manhattan townhouse. The Epstein files, released January 2026, contain an exchange between the two from the previous year. Epstein to Brende: “Davos can really replace the UN. C21, cyber, crypto . genetics… intl coordination.” Brende back to Epstein: “Exactly — we need a new global architecture. World Economic Forum (Davos) is uniquely positioned — public private.”
The next day, the UN General Assembly adopted the framework for restructuring global governance.
That sequence — the partnership signing, the Epstein dinner, the candid admission about replacing the UN with a public-private architecture, and then the formal adoption — opens Jacob Nordangård’s The Digital World Brain. Pages two and three. Footnoted to the UN resolution number, the Epstein files, and the General Assembly record.
I keep coming back to it because it captures what this book does that almost nothing else in the independent research space manages. I’ve followed Jacob’s work for years now and interviewed him about his research. Each book peels back another layer of the same institutional architecture, and each time I think he’s reached the limit of what can be documented, the next one goes further. Nordangård doesn’t speculate. He doesn’t editorialize much. He lays institutional actions next to each other in chronological order and lets the pattern announce itself. … continue
Blog Roll
 Aletho News
Aletho News- Iran Threatens Retaliatory Strike on Stargate AI Project in UAE
- US sent ‘a lot’ of arms to Iranian protesters – Trump
- Barak Ravid Launders Deception To Allow Trump To Back Off Of His Power Plant Threat – Again
- REWRITING THE RISK? INSIDE THE GOVERNMENT’S VACCINE SAFETY MESSAGING
- “Davos Can Really Replace the UN”
- NIAID/NIH and USDA Fund Bioengineered Chimeric Influenza Viruses Built Using Pandemic H1N1 Components: Journal ‘Science Advances’
- Hezbollah hits Israeli warship off Lebanon’s coast, sets it aflame
- Iran slams US strikes on B1 bridge, Mahshahr petrochemical plants as ‘blatant acts of state terrorism’
- In letter to UN chief, Araghchi warns of dire consequences of US-Israeli attacks on Iran’s nuclear facilities
- Why the CIA conspiracy to invade Iran with Kurdish militias failed
- If Americans Knew
- In Iran, Israel-US take aim at “reason, research, and freedom of thought” – Daily Update
- US loses planes over Iran, Israel downgrades Lebanon war goals – Daily Update
- Israel Is Blocking Palestinians from Easter at Church Where Jesus Resurrected
- Plot to assassinate Palestinian activist follows harassment campaign promoted by Zionist groups and elected officials
- Prominent New York synagogue hosts presentation on why U.S. Jews should support the ethnic cleansing of Gaza
- Tapper vs. Piker: Is the CNN Anchor Auditioning for David Ellison?
- Shouldn’t Democrats Be Able to Condemn Genocide?
- Israel-US kill negotiators, destroy civilian structures, but Iran’s military capabilities still largely intact – Daily Update
- ‘War crime’: Global condemnation as Israeli ministers celebrate death penalty law targeting Palestinian prisoners
- 7 Ways Israel Is Turning Lebanon Into Gaza
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
