Crossword clues and bullying – the influence of Australia’s pro-Israel lobby unveiled
Michael West Media | October 3, 2021
The intimidating power of Australia’s pro-Israel lobby limits what mainstream media outlets dare publish about Israel and forces self-censorship on editors and journalists alike, writes John Lyons in his latest book Dateline Jerusalem: Journalism’s toughest assignment. Kim Wingerei reports.
In 2019, Fairfax Media’s Sydney and Melbourne mastheads made an error. In the daily crossword section, the answer to the clue “Holy land” turned out not to be six letters starting with an I, as some would expect, but nine letters: Palestine. So affronted was the Australia/Israel and Jewish Affairs Council (AIJAC) that they demanded an investigation.
Fairfax acceded, blamed the error on an external contractor and apologised to Colin Rubenstein, executive director of the AIJAC.
This is just one of many examples which John Lyons uses to illustrate the power of a lobby group so influential it can force changes to Government policy, hound journalists out of their jobs and pressure the ABC board to justify the appointment of foreign correspondents.
… there are only three people who can tell the editors of The Australian what they can or can’t use: Rupert Murdoch, Lachlan Murdoch and Colin Rubenstein. – John Lyons
 John Lyons is an experienced journalist. Currently the head of investigative journalism at the ABC, his 40 years in the media include being editor of the Sydney Morning Herald, Middle East correspondent for The Australian and winning one of his three Walkley Awards for “Stone Cold Justice”, a Four Corner’s episode which exposed the human rights abuses in Israel military courts.
John Lyons is an experienced journalist. Currently the head of investigative journalism at the ABC, his 40 years in the media include being editor of the Sydney Morning Herald, Middle East correspondent for The Australian and winning one of his three Walkley Awards for “Stone Cold Justice”, a Four Corner’s episode which exposed the human rights abuses in Israel military courts.
His earlier book Balcony over Jerusalem covered his six years of witnessing the tragedies and contradictions of a region which has suffered more armed conflict than any other since World War II.
In his latest book released this weekend (at 85 pages, it’s closer to essay size), Lyons focuses entirely on the Israel-Palestine conflict and specifically how pro-Israel lobbyists seek to control the narrative for the Australian audience.
He makes the point several times that the press in Israel is far more overtly critical of the policies of Israel’s Government than is the media in Australia, including how the regular flare-ups in the West Bank are covered.
To the AIJAC it’s a war of words. It is a battle to control how and what is said.
For example, Colin Rubenstein and his fellow lobbyists are particularly sensitive about using the word “occupation” in reference to Israel’s occupation of Palestinian Territories. But as the lieutenant colonel responsible for Israel’s army operations in the occupied territories quips:
If this is not occupied then the media has missed one of the biggest stories of our time, (Israel’s) withdrawal from the West Bank! – LC Eliezer Toledano, Israel Army
The pro-Israel lobby has even developed a special dictionary. The Global Language Dictionary was funded by The Israel Project to “guide politicians and journalists on the language to use to win support for settlement expansion.”
Merely using the word Palestine can land a journalist in trouble. Jennine Khalik, a Palestinian Australian and former journalist at The Australian recounts in the book how she was yelled at by a sub-editor for referring to a refugee and singer as coming from Palestine:
PALESTINE DOES NOT EXIST … Palestine is NOT a place … What kind of journalist are you, using the word Palestine?
For Jennine Khalik this was the last straw, she left the paper shortly after, following what had been a concerted campaign by the pro-Israel lobby, including diplomats from the Israel embassy questioning her editors about the appointment of “a Palestinian activist”.
In another example of the tactics used to control the narrative, Lyons refers to a story told by former The Age editor, Andrew Holden, where Colin Rubenstein and Mark Leibler – lawyer and well known leader of the Jewish business community – marched into his office and complained loudly about the paper’s coverage of the 2014 Gaza war.
Anyone who thinks that such a display by an esteemed member of the Australian community doesn’t have a chilling effect is kidding themselves. I have seen its effect in the years since in hesitancy on the part of editors and trepidation about any story which may show Israel in a negative light. – John Lyons
Lyons himself has also been subjected to threats and intimidation over the years for his reporting on Israel and Palestine. Like many who have dared to criticise the Israeli Government, he has been called an anti-semite, but also a “Goebbels” and “a Hamas smelly used tampon”.
It is a tactic he says is used persistently by those in Australia agitating for positive coverage of Israeli government actions.
I think the aim is to make journalists and editors decide that, even if they have a legitimate story that may criticise Israel it is simply not worth running, as it will cause more trouble than it’s worth. – John Lyons
As a result, most Australians don’t know much about the plight of the Palestinian people. They don’t know about the 101 permits that Palestinians need to obtain from Israel to be able to work and live in what they believe is their own land. They don’t know that Palestinians don’t enjoy free speech, freedom of movement or equality before the law.
In April 2021, Human Rights Watch (HRW) released its landmark report “A Threshold Crossed: Israel Authorities and the Crimes of Apartheid and Persecution”. It was largely ignored by mainstream media in Australia. “Including by my own organisation, the ABC,” says Lyons.
Abusive Israeli policies constitute crimes of apartheid, persecution
The pro-Israel lobby is so effective it has achieved the ultimate aim of information suppression – self-censorship.
John Lyons: Dateline Jerusalem: Journalism’s Toughest Assignment – now available from Monash University Publishing
Kim Wingerei is a businessman turned writer and commentator. He is passionate about free speech, human rights, democracy and the politics of change. Originally from Norway, Kim has lived in Australia for 30 years. Author of ‘Why Democracy is Broken – A Blueprint for Change’.
Gagged Australian Nurses Form Whistleblower Group to Expose What’s Really Happening with COVID-19 Vaccine Injuries

By Brian Shilhavy | Health Impact News | September 27, 2021
Reignite Democracy Australia, which was started by journalist Monica Smit, an outspoken critic on authoritarian lockdowns in Australia who was just released from jail on bond last week, has started a group called “Nurses Speak Out” where gagged nurses are speaking out about the truth of what is currently going on inside of hospitals with people suffering from vaccine injuries.
They are posting these stories on their Telegram channel as well.
This is an Anonymous whistleblowing channel for Nurses & Healthcare workers in Australia. We will share verified experiences from frontline workers who see firsthand the damage caused by COVID-19 vaccinations.
These submissions have been vetted by a collective of health professionals. Some details may be omitted, your identity will be protected. AHPRA has gagged, coerced and threatened anyone who comes forward – let’s save some lives.
This channel is dedicated to all frontline workers around the world. This is Australia. This is for you.
Here are some of their stories that have just been published.
Hi,
I’m a community RN on the —— , Qld.
I am seeing and caring for adversely affected clients who have had the vaccines and are quite literally dying. Our palliative care is increasing at an exponential rate, people are getting diagnosed with terminal conditions and dying quickly. We (community nurses) are seeing 2-3 palliative clients per day each, this is a massive increase from 1-2 each per week. Other palliative clients who haven’t been vaxxed, then their families talk them into the vax, die more quickly than expected.
Have noted that those who are vaxxed that their clinically ‘weak’ areas are being exacerbated. Appears to be at 3, 5 then 12 week patterned intervals. Not one of them associate with the C19vax.
Had one man in his 70’s in very stable remission with leukemia for years. Within 3 weeks of having ‘the vaccine’ his white cell count dropped so he had neutropenia. He suddenly developed in 24 hours bilateral cellulitis to both legs up to thighs. 9 weeks later, he is dead.
Those with rheumatoid arthritis who have been jabbed experiencing related consistency of flare ups. Getting all sorts of skin infections for no obvious reasoning. They’re having constant medication reviews and increasing analgesia.
3 x clients with healing venous ulcers, all 3 had the jab, 3 weeks later all developed septicemia all with hard to treat bacteria.
Those with cardiac conditions who were clinically stable on medication for years, suddenly no longer stable. Arrhythmias, unstable blood pressure, syncope, falls, increased hospitalisations.
Cancers: seeing massive increase in skin cancers. They’re growing very quickly and aggressively.
Cognition: clients who have been vaxxed and predisposed to some memory issues, increasing episodic bouts of confusion with accompanying amnesia and increasing STML.
Of my nursing colleagues who have been vaxxed, noticing increasing sick leave being taken.
Sincerely,
Veronica
Community RNTriage Admin, Emergency Department.
Hi,
I work in Emergency Department as an admin clerk at triage and I can tell you the reason I will not be having this vaccine is that every third or fourth patient is coming in with an adverse reaction.
Some complaining that their heart is beating so hard and is squeezing out of their chest, I’ve seen vision changes, numbness , skin problems , cellulitis young men and women diagnosed with pericarditis myocarditis, clots , tumors even my colleagues have had Bell’s palsy there is so much more.
What amazes me with all this is that no one can see it! Young patients being told it’s just anxiety 😥, nurses at triage rolling their eyes saying things like “can’t they just stay home and take a panadol” !
Then to top it all off our double jabbed nurses at triage test positive to Covid and are admitted and are sick but they are saying “at least I’m vaccinated I could have been a lot worse”, there are 5 unvaccinated clerks at the front desk at triage and we have worked through this pandemic but now we are a danger to the other other staff
UNBELIEVABLE! So we now have received the letter saying no jab no job we’ve got till the 30th 😟 Also would like to add the influx of nursing home patients that are coming in is ridiculous, falls vertigo generally declining quickly after jab, I’m not a medical person but I can see what’s going on it’s very sad 😞
Hi,
I am a Physiotherapist with 40 years of Private Practice experience – Some of the clients I see I have been seeing them and their families for different things for decades.
On Thursday I had four of the jabbed ones in. They all had the same set of symptoms.
Their original injury that I treated them for occasionally — maybe once every few years over the last few decades has returned with a vengeance and is excruciatingly painful. Additionally all four of them had pain all over in ankles, wrists, knees, hips, backs all over… and they all had a severe headache.
They are not relating this to the jab.
I have been seeing this new presentation of pain over the last couple of weeks.
However, on Thursday with them all coming in on the same day with the same symptoms I now KNOW it is a pattern of pain for the jabbed.
This evening I went out with a Nurse friend who is jabbed and she has the same thing happening to her. Neck, arm and wrist pain, swollen feet and foot pain, and she kept saying she felt old, and her body was breaking down… She is 15 years younger than me and could barely walk home from dinner.
These people are my friends and long term clients — it is difficult to watch them suffer.
(Response to #0003)
25/09/2021
Private Practice PhysiotherapistsHi,
We’re also a group of private practice physios of similar vintage and have seen this pattern of presentation in the jabbed ones.
Headaches feature prominently. In addition, we’ve noticed discoloured feet (purple-red), swollen joints (one young patient with Crohn’s disease resorted to a walking stick), swollen and tight calves, recurrence of old injuries as well as new joint aches snd pains.
When dry needling, our acupuncture needles are now “swimming” in tissue because there’s just so much generalised inflammation of the muscles. Patients are reluctant to report these symptoms because they’re doctors have told them “the shots are safe”!
Student Nurse, Rural.
Hi,
I’m a student nurse working in a rural hospital.
I’ve had several people walk into the hospital with flaring pains all over their body, on my last shift there were 9 patients who whispered to me that they were sure that their condition was caused by the COVID vaccine they got but they were afraid to tell the registered nurse for fear of being ostracised. They got the jab because everyone else was getting it rather then making the decision for medical treatment.
I have seen many nurses and doctors laughing about these people in the break room. Calling these patients Anti-vaxers and wishing they could kick them out for the real patients in need. I told my student supervisor and the nurses stopped talking about it when I was on break but I have the feeling they still had those conversations behind my back.
RN. Aged Care, NSW.
Hi,
I am (was) a Registered Nurse in Aged Care in NSW.
I was terminated from my job there over a week ago now for declining the jab.The facility had a covid clinic where the masses received Pfizer.
On the day as they had left over stock the staff were then offered jabs which many of them didn’t feel comfortable but got because the management where there on the day saying things like “come on just get it, don’t be ridiculous, if you can’t trust the science what can you trust” one staff member declined twice, the third time she was pushed into getting it (all on the same day) I seen this as pure bullying and coercion, she submitted and got the jab.
The next day a resident died (nobody batted an eyelid) within three days post jab another two residents died.
Over the course of the next three weeks we lost in total 6 residents all who had significantly declined overall and not to mention a lot of other residents declining overall and becoming unwell.
The second jab clinic, within the first week, we had five people end up in hospital who then died, shortness of breath, heart issues, others the residence getting rashes not being able to lift their arm up, acting as delirious state, within the next week after that another 5 residents died.
In total within the 3 months roll out of the jab, we had 14 deaths of vaccinated residents.
In a nursing home with 90 residents most of the staff are commenting on how unheard of this amount of death was but when questioned in relation to the jab many were in denial stating it couldn’t be from that.
Over the course of three months watching the staff who had been injected so many staff off on sick leave a few staff members ended up in the hospital one for heart reasons the other one had blistering rashes all over her body she ended up being admitted twice, mass reports of headaches lasting days to weeks, dizziness, just generally reporting to not feeling right since having it. The fear in the eyes of the staff is something I will never forget. Other staff feeling completely deflated as they could lose there jobs and had to submit to the jab, In which some after were crying to me at how much they just felt defeated. I have many things to say in relation to this, I could write a novel.
I know just within the week and a half of not being there they are struggling to fill shifts, which sadly impacts on everyone, residents and staff the only people it doesn’t effect is the management.
I love being a nurse but I just can’t do it in this current situation it no longer aligns with what I believe health to be. It is a sad and devastating time.
RN, Emergency Department. NSW.
I am a Registered Nurse from NSW,
I have a young colleague, also a nurse who did not want the vaccine.
Due to the mandate she got the shots. After her first shot she had searing pain down her arm. Unrelenting pain. After her second shot, she was bedridden for an entire week. She could not sit up straight. She was so sick, unable to move and constant chest pain.
After the week of being bedridden she returned to work with chest pain. She finally has been admitted to hospital with myocarditis.
She is early 20’s. Before the vaccines she was healthy with nil health issues. Now she has cardiac issues and may need medication for the rest of her life.Each day we are seeing the emergency department full of patients with stroke, Pulmonary embolisms, cardiac arrhythmias, Myocarditis, endocarditis. The increase of strokes is exponentially growing. Patient after patient with PE’s, cardiac issues. Most in previously healthy patients. Doctors are denying connections to the vaccines.
RN, 40years. Palliative Care.
AHPRA Verified ✅Hi,
I am an RN of 40 years, presently my work is in Palliative care where I have worked for 8.5 years permanently in ——-.
I am seeing patients developing increased effects from Palliative radiation, which is commonly prescribed for reducing various conditions arising from cancers. Our patients are deteriorating more quickly with increasing weaknesses, breathlessness (?PEs) facial droops (Palsy or stroke), neuropathys in hands or feet.
The cancers some only recently diagnosed, seem to have metastisised very rapidly. This needs to be looked into carefully. We as nurses are commenting those going for radiation are very much at risk; a death sentence which hastens their deterioration towards death. As Palliative patients, their downturns are passed as expected, while we see them as alarming.
I have many colleagues took the jab out of sheer fear of losing their job and incomes. Also one other colleague after she recieved her 1st pfizer jab was off work with encephalitis and remains very unwell having diffuculty with headaches and dizzy spells.
I am ordered to leave from September 30th, a job I am passionate about and feel have been valued. While now 61 years old I hoped to continue my work for 5 more years and feeling very sad to be forced to leave.
I think the radiation perhaps is accentuating the vaccinations, namely the graphene components.
Sincerely.
EN. Brisbane, QLD.
Hi, Enrolled Nurse from Brisbane…
I work in Private health, so don’t often get to see initial reason for presentation to emergency, as they are usually transferred from public to us later.
I nursed a man in his 60’s recently that got vaxed…he had a knee replacement 3 months prior (fully healed).
Came in to hospital again due to severe bleeding and needing surgery… post-surgery his knee haemorrhaged quite badly… then got a vacc dressing…ended up nursing him again in a Rehab ward a week later… told me it happened after vaccination but surgeon didn’t report it or link it with vaccine.
Another older lady presented as very disordered after vaccination.. couldn’t walk properly, ended up 2 assist with a FASF… on Lyrica 150 BD for nerve pain… frequently complained of headaches and chronic ear ache.. ended up going home after a long rehab stint..
I won’t be getting the jab so will probably be unemployed in the next month or so… One of our Doctors is very over the draconian crap..his words.. he is fully vaxed and furious we are still wearing masks.
Remedial Massage Therapist, QLD.
Part 1 of 2.
Hello,
I am a Remedial Massage Therapist operating out of Wellness Clinic in an exclusive seaside town in —— Qld, Australia.
Over the past 12months the majority of my regular clients have received both shots of either AZ or Pzizer and I have observed and felt the changes in their bodies. I will also add that not only have the changes happened in their bodies but also their personalities.
Over the past 2 months I have also listened to them telling me of their sudden medical issues that are happening to them. This has been so disturbing for me that I am closing my business and am taking the time to heal myself both physically and mentally.
Their bodies over the past 12months have changed. They have no movement, elasticity anymore. It is like they are turning to lead. I have 3 clients, all retirees and golfers who now have tears in their supraspinatus. This is on their left hand side from swinging the golf club.
(1) One client, male retiree who has been rushed to hospital 4 times last week unable to urine or make bowel release. The Doctors have told him that he has kidney stones. Hmmm… He also had a large burning and itchy rash all over his back. He said it was that painful he had his wife put metho on his back to ease the pain as nothing else was working.
(2) One retired lady advised me that she had a cyst forming behind her knee and when she would have a shower it would burst and the blood that came out was uncontrollable. This happened twice within a couple of weeks. She went to the Doctors he said it was a bakers cyst. She returned saw another Doctor who said it was a BCC. The third time she came to me her leg is now swollen all the way and she is in a lot of pain.
(3) Another lady, a Doctor herself advised that she had an electrical like pain run across her back. She couldn’t quite explain it. Never had anything like it before and now has a sore neck and headaches. I felt her neck and there was a pulsing feeling at the rear. She couldn’t feel it. I went back to that site 2 more times and I could feel it. She couldn’t.
Cont…
Part 2 of 2.
… (4) A retired lady told me she had burning and itching skin on her chest and that she was in a lot of pain. I asked her if I could see it. It covers a large area between her breasts and underneath her bra line. She said it is getting worse each day. It was very red and raw.
(5) Another regular client has markings all through her lower back on the left side. She was unaware. I took a pic and showed her. She said that she had been putting an electric heat pack in that location at night to warm her up. She went to the Doctors and the skin clinic and they didn’t know what it was. She came back to see me 5 weeks later and the markings are still there.
I have attached the pics (redacted) for you to view. and the list goes on..I have regularly massaged these clients over the past 2-3 years and I find it extremely troubling. These haven’t happened straight after their shots but over the 3, 4 , 5 months following so they are not connecting it to their shots. I am unable to say anything to them as their once friendly personalities have also changed. They are more aggressive and talk at you, not to you and will defend these shots.
The man I mentioned above even said to me that he will be getting the booster shot if and when it comes out next year. When you hear from your clients all day, every client, not 1 or 2 then this is a concern for all people who have had this shot. They are not the same people, on any level anymore. Like I mentioned above this has traumatised me to the point that I am now unable to continue my passion for the foreseeable future and I am now focusing on healing me, physically, mentally and spiritually. Take care everyone and be safe.
Radiographer, Private Practice, Rural.
Hi,
I work as a Sonographer for a private rural practice. We mostly see outpatients but the occasional patient via ED.
I work three days a week and I would say I see at least one patient per shift with an injury directly related to the vaccine. Some examples:
89 yo F haemathrosis to left shoulder at injection site one week post vaccine.
No blood thinners. Healthy72 yo F (mother in law)
Very healthy, fit. No medical problems.
Profoundly deaf in both ears over a period of days. Had vax 10 months ago. No cause found.56 yr old M
Testicular ultrasound showed epididymis one week post vax.Lots of unexplained abdominal pain, headaches, shoulder pain and inability to use arm at injection site.
Hope that’s helpful.
Regards. ——RN, 39years.
Hi,
I am an RN with almost 40years experience.
We looked after one of the first AZ blood clot patients
Male, 45yo. 8 days post his 1st AZ shot he complained of dreadful stomach pains. Went to ED.
Scans showed a massive blood clot in his bowel.
It took 3-4 days before they could operate, as his Coags were all over the place.The clot was finally removed along with almost 2 metres of necrotic bowel.
When out of ICU, he came to our ward. A beautiful man, who was black and blue all over with bruising. He was on an anti-coagulant drip, with a drug I’d never heard of (still can’t remember the name).
He was transferred to our Haematology ward, and unsure what happened to him.
Admitted a pt yesterday, who had been in ED for 10 hrs. Quite casually he told me that he couldn’t believe the numbers of young guys coming in with side effects from the vaccine. I asked him how he knew this, and he said he could hear the conversations.
I asked re the side effects and he said chest pains, breathing problems!Nursed a female pt, fully vaxxed, with pancreatic issues, but she’s had increasing weakness in her legs?? All Neuro tests are NAD. She can no longer weight bear, and has been told it’s because she’d been in ICU and was deconditioned???
I’m not so sure….Will no doubt lose my job end of October, as no jab for me!😥😥
RN. Emergency Department, Melbourne, VIC.
Hi,
I am an Emergency Department RN based in Melbourne’s east and have similar experiences to the other whistleblowers.
We have young, healthy men in their 20’s-30’s coming in every single day due to chest pain after the vaccine. Pathology is usually fairly normal (Trops and d-Dimer) and doctors write it off as either psychological or unrelated to the vaccine. Even when they admit it’s probably vaccine related, it is never reported. Ever.
I have looked after a young, healthy female who felt coerced in to getting it due to her job in healthcare, who suffered from severe headaches ever since, and nothing seemed to help. She was sent home basically left to hope that it resolves eventually. Doctors did not report it.
Another patient came in with multiple blood blisters, and petechiae on his arms. He was diagnosed with ITP which is a known adverse effect of the Pfizer vaccine. His platelets were literally completely wiped out. Doctors did not think it was linked to the vaccine he had 3 days earlier, and so it was not reported.
If science was being respected, people would be followed up properly, and the cause of the chest pain for example would be getting investigated, but it isnt.
None of these things were discovered during the purportedly thorough and complete clinical trials. None of the patients were made aware of the possibility of these effects, which means they could not give proper informed consent.
Now they want to force us to take it or lose our job? Who knows what other problems will be uncovered in the future?
No risk/reward analysis is being done in regards to age demographics. Many experts are saying young adults have greater risk from the vaccine than the virus. No formal studies have been done that I’m aware of, but I suspect that is true. And it is definitely true for children. The government now wants to vax all children despite their risk of harm from covid being almost zero, and the risk from the vax being comparatively high.
Medical treatment is supposed to have a favourable risk/benefit analysis, and it absolutely does not in this case.
The medical field is about to lose staff who are capable of thinking for themselves and standing up for themselves, and healthcare for patients will be much worse because of it.
RN. Brisbane Hospital, QLD.
AHPRA Verified ✅Hi there,
I am a nurse at one of the major hospitals in Brisbane. Had my first Pfizer shot back in April – suffering pericarditis, numbness and tingling in both arms, ceased menstruation, elevated insulin levels.
Will not get second.
No Covid at our hospital. Have seen many adverse reactions from Covid vaccine. Mainly block clots, strokes, heart problems.
AIN. Aged Care, NSW.
AHPRA Verified ✅I work as an AIN (Assistant in Nursing) in aged care in rural NSW.
One of my colleagues in her mid 30s went home sick the day after her second Pfizer shot. She went white and nauseaus and faint. This was in March and she has not been back to work since (its September now). After ages of going to Doctors etc she was diagnosed with myocarditis, she says she can hardly do anything. She was fine and healthy before, slim, physically active and on a good diet. Whenever the other staff talk about it, the narrative goes: oh she must have had something else before that, surely it’s not from the vaccine.
Two residents died within 2-3 weeks after first Astra-Zeneca shots, however were overall in bad condition before.
Residents are not allowed to leave the facility and nobody is allowed to see them except on compassionate grounds (basically if someone becomes really unwell). This causes some of the people to be really mentally unwell. There has not been one Covid Case in our town for the whole course of the pandemic since 2020.
We are told we have a “choice” to either get the flu and covid shot or we can’t work here. Another colleague had 40 years experience in emergency nursing and refused the flu shot, she was subjected to sitting at the door doing covid checks for about six months (even when there was no flu season) until she gave up and resigned. She had never had a flu shot for her entire career.
RN. Clinical Call Handler, COVID Vaccine Adverse Events, VIC.
AHPRA Verified ✅Hi,
I am a registered nurse in Melbourne with almost 33 years experience.
I currently have a role as a clinical call handler for people that are experiencing side effects from covid vaccines.
The adverse events that have been reported to me are extremely concerning in both the types of reactions and the frequency of them.
Apart from the usual expected side effects of over, pain etc for 1 to 2 days, some of the reactions that have been reported to me multiple times include
*Delayed anaphylactic reactions involving respiratory distress, facial and tongue swelling, usually a rash, but not always , with onset occurring usually around 2 days after vaccine, but has been up to 4 days post vaccine.
* Chest heaviness, stabbing chest pains, palpitations and shortness of breath is reported to me several times a day every day usually in young people (male and female) post Pfizer 1st and 2nd dose.
* Heart palpitations are very commonly reported across all age groups( usually Pfizer)
* ongoing shortness of breath for 6 plus weeks post vaccination with no explanation
* unusual rashes that appear days to weeks after vaccination
* unexplained bruising that appear days to weeks after vaccination with both Pfizer and AZ ( commonly reported extensive bruising on legs)
* swollen, painful varicose veins
* persistent headaches for weeks after vaccination, sometimes severe but usually just annoyingly persistent
* heavy vaginal bleeding in post menopausal women ( mid to late 50’s) and menstrual disruption/ irregularities in younger women
* Blood noses post Pfizer is extremely common
* Burning pain in limbs, in several cases the pain is so severe that the person is unable to walk.
* numbness and tingling in arms and legs is very commonly reported up to 6 weeks post vaccination with both Pfizer and AZ
* leg / foot pain and swelling( symptoms strongly suggestive of DVT however I don’t get to follow up)
* severe vertigo and tinnitus ( Pfizer)
* numbness down one side of face (this is surprisingly common)
* uncontrollable muscle twitching/ spasms
* extreme lethargy that persists for months after vaccine.
* Exacerbation of old injuries such as previously broken or sprained joints flare up or old scars become red and inflamed again.
* older Australians that have had Astrazeneca vaccine and have been ok but then had flu vaccine and have been extremely unwell since. I do believe there is a correlation between the 2 given within weeks of each other that is causing significant health decline in older people.
* people that have had stable auto immune disease but then once vaccinated their symptoms are markedly exacerbated or others with no previous history of immune disorders, I suspect develop an immune disorder post vaccine
I am certain that these vaccines are causing immune, neurological and blood clotting disorders resulting in significant harm to an unacceptably large amount of people.
There is more specific cases that I am aware of but for anominity I will not disclose them here. I am aware of ICU admissions post Pfizer vaccination in 3 different people as well as deaths of elderly nursing home residents within 24 hours of vaccination.
I am both concerned and frustrated that the medical profession is either unaware that these side effects are happening, or in many cases, not prepared to admit that they are in fact a result of the covid vaccines, (often medically gaslighting and putting down to anxiety), leaving these poor affected people desperately seeking help and answers, that in most cases, they probably won’t get either. I have tried to raise this issue on more than one occasion, but it falls on deaf ears.
RN/Critical Care Nurse. Rural, NSW.
Hi,
Love your idea by the way! It’s too hard for us to speak out and keep our jobs 😔
I watched many of my fellow colleagues suffer side effects. I was one of them too! When you talk about it so many stories come out and quite a few of us have ongoing issues to this day.
Within my workplace in a rural Emergency department I find myself as a team leader at times. I have been overwhelmed with patients post vaccination suffering side effect. Some short term such as chest pain amongst 20 -40yr olds to abdominal pain. Then the more serious long term stokes, heart attacks, guillian barre and pulmonary embolism.
For those nurses around me that have not had their vaccination yet, they are terrified!! For us that have had a reaction…..never again!Very little are reported and knowing how a proper clinical trial is conducted for my many years at university…this roll out is terribly wrong!
I understand COVID can make you quite sick (even if I have never seen it in my nursing career) but I believe this vaccination is no better! We need to go back to the drawing board and admit defeat instead of pushing forward.
The politics running this with no medical knowledge should be ashamed!
RN. Palliative Care Ward, Melbourne. VIC. AHPRA Verified ✅
.I’m a RN working on a Palliative Care ward in a major Melbourne hospital.
We never had Covid patient as they stay on the acute wards, obviously we need to protect our non-Covid patients.However we have had a number of patients coming to our ward and subsequently dying with sudden onset of unusual symptoms. Of course no connection has been made to the jab what so ever.
One male 70-something had his second AZ jab and a few days later suddenly collapsed with seizures. He was brought into hospital, ICU, had a number of CT’s, MRI’s and other investigations done, was intubated for a number of weeks. Everytime he was extubated, he was having seizures despite being on high doses of anticonvulsant (anti-seizer medication). The medical team decided he might have Autoimmune encephalitis (=autoimmune brain inflammation) eventhough the EEG and blouds did not confirm this conclusively.
(1). A man in that age group suddenly having an autoimmune disease? Eventually the decision was made to palliate him, which is when he was transferred to our ward. He somehow stabilised on our ward but was bedbound and definetly not like himself. Now here’s the twist. All along in his medical history the diagnoses was documented as “autoimmune encephalitis vs. vaccine injurie post AZ”. At one stage during the weekly meeting I actualy asked if he was going to be a Coroners case, since it’s unclear what his cause of death would be.
I was looked at realy strange, my concern was dismissed, I was told no it’s clear that he suffers from Autoimmune Encephalitis. After that the above comment was removed and his diagnoses remained Autoimmune encephalitis. To me this was a trigger to start looking at each patients history deeper.
(2). Female 65 years old and healthy was transferred to us after she’d suddenly collapsed at home for unknown reasons. ICU, intubated, again seizures from unkown reasons. They had done all the tests available under the sun(whole body MRI, CT, EEG, Autoimmune tests, etc). Medical team unable to find a cause of her severe deterioration. Decision was made to palliate. Transferred to us and then died after a couple of weeks. At least this one was a Coroners, as the cause of death was unclear.
A number of other patients were transferred to us, mostly with some sort of seizure that led to a collapse, or Stroke that led to more strokes and collapses. Sometimes one has to dig a bit to find info of recent vaccination with Covid vaccine!
I am genuenly concerned for every single person that had or will have the jab! Please don’t take it!
Physiotherapist, Private Practice.
Hi.
Thanks for giving us somewhere safe to speak out. I am a physio in private practice and previously contracted to aged care.
I have seen several deaths in aged care facilities in 12-24hours following the vaccination in people who were previously stable. Each time the entire file has been completely removed from the system and any notes by staff related to vaccine were deleted prior to the file being returned.
I actually retained proof of this from the first time I saw it happen as I could not believe what I had seen happen given how strict they are on no modification of record keeping being made in ANY other circumstance. This was not normal protocol when a death occurred in the facilities.
In private practice I have seen and heard of many side effects – similar to all those listed in the other accounts (persistent sharp headaches, increased previous injury flares, auto-immune disorder flares)
Probably the worst 2 were a patient with Parkinsons who I have been seeing for several years and had been symptomatically stable the entire time despite other health challenges. Post second vaccination they had a debilitating increase in freezing episodes and pain through their lower limbs. Their specialist denied this would have any connection to the vaccination so they did not question it any further.
Another client attended an appointment reporting they were completely bedridden for 3 weeks with extreme dizziness, lack of appetite and fatigue post initial vaccine (AZ). They were still breathless and very fatigued on the day they saw me. They are normally very well and active with no history of prior health issues. Again when they contacted the GP regarding the issues following the vaccine they were informed that what they had experienced the equivalent of “mild” symptoms of COVID and that was all to be expected with the vaccine. When I queried if they were going to return for their second dose, they reported they were so afraid as the GP had told them catching COVID would be much worse than what they were currently going through so they definitely needed to ensure they returned for their second dose. 😥😥
RN, Cardiology Ward, Major Hospital.
27/09/2021 AHPRA Verified ✅Hi,
I work on a busy cardiology ward.
Overall in the medical notes Doctors aren’t connecting the dots and not even considering the jab as a reason for the illness. Whether that is intentional or not I don’t know.
I have seen young adults come onto the ward for cardiac monitoring after collapsing after the jab.
(1). A lady with an autoimmune disease came in with a pericardial effusion after her jab.
(2). One lady had chest pain for weeks after the second astrazeneca dose, she had myocarditis. She was quite sick when she was on the ward, she had fevers, and all of her face was swollen, her eyelids were that swollen she could barely open them and inside her eyes were all glassy.
(3). Another was a young guy, healthy as, post jab had severe cellulitis to one side of his face, his ear was Triple the size.
(4). Another guy in his 20s had his first pfizer and the day after was febrile, and after a TOE was diagnosed with infective endocarditis. He also developed acute kidney injury to the point of needing dialysis. All kidney scans came back normal but still his kidneys were failing. In his notes when he was in ED it was mentioned that this started post jab but then on the ward after being reviewed by multiple specialists (infectious disease, renal, cardiac) not once was the jab mentioned.
What I am finding disturbing in my area is that it’s not even being considered as a potential cause. Even though problems start after the jab.
RN, Community GP Practice, Former Vaccinator. AHPRA Verified ✅
Part 1 of 2..
Hi,
I’m an RN who was working in a GP clinic and guilty of being a covid vaccinator.
I had raised concerns on a number of occassions and could no longer give it when I started to see what was happening. During this time I have seen and heard things which lead me to believe the vaccines are not safe.
I have heard many people saying they were spaced out and dizzy for days.I can’t count how many times I heard “spaced out”. Older people coming back and saying they were off balance and having falls when this hasn’t happened to them before.
Also heard people say loss of bladder control, arthritis flare ups, eczemea and skin rashes, strange blister, out of control diabetes, unhealing wounds and enhanced pain of old injuries. A man reported that he had visual problems and thought he almost went blind for a month but went to the optometrist instead of a dr and he said he had reported it to the report link provided which he said they had “pretty much dismissed it”.
I have sent a man off in the ambulance with anaphylaxis reaction, uncontrollable shaking and tingling around his mouth, unable to walk. I have had 40y old man crying half hr post vaccination saying he didnt feel right, was dizzy, headache, heart palpatations and jitters, he did not believe it was anxiety as they said.
I’ve since realised there was an older man who didnt come back for second jab and I had reported this to the report line. I remember he had walked back into the treatment room the day after his jab and he was anxious, glassy eyed, said he was sick and had been falling over that night. I did his obs and his ecg wasnt right, offered for him to go in ambulance but he declined. He missed his second appointment I wouldn’t be surprised if he died.
I have seen a man with cancer go down hill very quickly after his jab.
I have heard patients tell me there family has told them they have to get the shot or they wont pay for a ventilator. Also a pt tell me that her old neighbour told her he thinks he has killed himself getting the jab and he hasnt been the same since.Cont…
I have heard of a nurse pressured to get the jab who had diabetes under control is now on insulin. Another nurse I know didn’t want it but said she has brain fog and memory loss and sudden onset of menopause..she also admits to seeing patients at a seperate clinic she works at go down hill since getting the shots.
I have a nurse friend who has 2 family members, 1 with bells palsy and the other with myocarditis. She also knows a fit healthy 30yr old who had a heart attack.
My sisters 60yr old neighbour is in a coma after second shot. Her mother in law keeps passing out and her father in law has been showing aggression.
My brother in law also knows a guy in a coma and somebody else with blood clots in his bowel.
My sister in law had kidney stones the day after her second shot.Another thing I have noticed is personality changes in patients and people I know or have worked with where a number of them seem to become aggressive, lack empathy and logical sense.
In comparing my findings with other nurses we have all noticed similiar patterns where we agree that comorbidities seem to become worsened and mortality is being sped up.
We are very concerned and worried sick, especially that they want to give these to our children who will be at much greater risk from the jab than the virus.
We disagree with the mandates, we believe the cases of injuries and deaths to be under reported and the jabs are unsafe and unethical and should be ceased immediately.
RN, Major Hospital.
27/09/21 AHPRA Verified ✅I work on a rehab ward
I know of 3 patients who had a stroke 7-8 days post jab.
(1). 1 Pt with bell’s palsy.
(2). 1 Pt with Guillain-Barré syndrome.
(3). 1 man experienced an unresponsive episode following his 2nd jab. Diagnosed with hypo delirium and pneumonia! 3 weeks in hospital so far and at what financial cost?
Nothing documented in notes. Family told it was nothing to do with the jab.Also possibly seeing vac shedding too.
Bels palsy, shingles causing encephalitis, lots of falls.Lots of PE’s, but unsure of vac status.
Interesting that recently the federal gvt was trying to amend the NDIS Act! It would be interesting to see the statistics of new NDIS applications.
And, what happened to influenza?? Vanished?
Reported by REGISTERED NURSE from Regional NSW:
(1). 62 year old with blood clot on lung post AstraZeneca- ICU admission
(2). 35 year old with severe headaches and blood clot on brain- ICU admission 2 weeks- sent home to have MRIs every 2 weeks as followup
(3). 27 Year old Male- Pericarditis following Pfizer
(4). 19 Year old female- cardiac arrest 3 days post pfizer (deceased)
…and many others.V status not being consistently asked or documented in eMR- medical team not looking to make correlation. Medical team worried about AHPRA and their careers if they speak out.
This is not what we signed up for!
MD. RN. 46years.
27/09/2021. AHPRA Verified ✅
Part 1 of 2.Hi,
Im an RN of 46 yrs practicing as an acute peri/post operative care nurse.
I no longer practice. The following is an account of a close nursing colleague. She experienced: Pfizer x no1 jab- “headache from hell”.
No 2 pfizer jab- awoke in the night totally paralysed for 4-6 hrs(estimated as time unknown on waking). She could not move a muscle, cough, speak, take a deep breath or nudge her husband to call ambulance until it resolved. Only eyes would open and blink..at one point she wished she would die she felt so terrible.On return to duty when recovered much later, she reported incident in writing to hear similar affects with 6 other nurses in total at her hospital. Date 2/6/21. Still has not been interviewed face to face as normal protocol, 10 weeks later.
What is going on? We must all ask ourselves and our superiors?
The Hippocratic oath- to do no harm? Are the medicos brain dead? Is it mind control? Surely no one could need the $ that badly. That is only one example…Cont…
MD. RN. 46years.
27/09/2021. AHPRA Verified ✅
Part 1 of 2.Hi,
Im an RN of 46 yrs practicing as an acute peri/post operative care nurse.
I no longer practice. The following is an account of a close nursing colleague. She experienced: Pfizer x no1 jab- “headache from hell”.
No 2 pfizer jab- awoke in the night totally paralysed for 4-6 hrs(estimated as time unknown on waking). She could not move a muscle, cough, speak, take a deep breath or nudge her husband to call ambulance until it resolved. Only eyes would open and blink..at one point she wished she would die she felt so terrible.On return to duty when recovered much later, she reported incident in writing to hear similar affects with 6 other nurses in total at her hospital. Date 2/6/21. Still has not been interviewed face to face as normal protocol, 10 weeks later.
What is going on? We must all ask ourselves and our superiors?
The Hippocratic oath- to do no harm? Are the medicos brain dead? Is it mind control? Surely no one could need the $ that badly. That is only one example…Cont…
No 2 this is anecdotal from a jab victims daughter-in-law:
An 80 r yr old independant lady, no comorbidities in nursing home. Family expressly forbade- face to face with 2 staff members, her having the jab( I can’t call it a vaccine as it isnt). The army turned up to jab the residents. When they came to this 80 yr old, the residential nurse on duty told the army nurse the said woman was not to have the injection. She ignored the nurse and gave it (az) anyway- that was on a Thursday.On the Friday the relative came to see her mother in law, having been informed via phone of the misdeed. She found the woman in an unusually hyped up state- as if high on something- unusual for this quiet woman.
On the Saturday, the injected woman asked her nurse to return her to her room as she felt unwell. According to the relative who had been told the following, as she walked down the hallway she collapsed and died instantly. This was day 2 after first az.
The attending physician refused to sign the death certificate as he thought his now deceased patient had NOT died of a cardiac arrest as staff assumed. Deceased was sent to coroner in a large city nearby. The coroner only scanned the body, decided it was heart attack and declined to perform a full post mortem. The lady has since been cremated so no body to exume? We all know what to call such an incident!
Life should never be this cheap!
Enough is enough. This must be stopped.
We all know there is power in numbers. Everyone, seem to be impotent to act on this critical and existential crisis in the making.In fact this is threatening humanity’s very survival.
Childless Gladys should read these ‘testimonials’. She is some one else’s child too! Unwitting guilt abounds. The people responsible including medico’s, who ignore what they must be re-cognising, cannot plead ” I didn’t know” for too much longer, surely?? Bring on Nuremberg!
M. D. RN
Senior Clinical Nurse Specialist, Metropolitan Hospital, NSW.
27/09/21.Hi there,
I am a senior Nurse (CNS2) in a metropolitan hospital, NSW.My usual role is in Cardiology.
My lengthy career is ending this week, after decades in the acute sector.I have seen many patients both in ED and Cardiology with vaccine SE’s .
These are LARGELY under-recognised, and RARELY reported. I have told relatives to make their own TGA reports as reporting in the acute sector is NOT HAPPENING.Doctors are RARELY attributing the various conditions to vaccination, but when you take a history it is very easy to join the dots.
Heart attacks (all ages), acute myocarditis / pericarditis, DRASTIC deterioration in EF (ejection fraction – index of heart’s pumping strength), ie worsening in heart failure.
I understand that many are presenting with strokes, and other neurological complications.
Diabetes has been far more unstable in some, and difficult to manage, with very labile BSLs.
I have seen colleagues with gastrointestinal SE, recurrent pneumonias
Many non- injected, including myself have experienced symptoms from spike protein transmission (shedding).
GI pain (severe), headaches, migraines, sleep disturbance.
I have seen bizarre changes in pathology, huge drops in haemaglobin, and derangements in biochemistry (Na, kidney function).I had a secondment in Aged Care and after the vaccination was rolled out in Facilities, saw MANY acute deteriorations, with increases in death rates above normal
Loss of speech, loss of mobility, chest infections.My sister in law works in community aged care, and has seen MANY SE as well. Renal Failure, siezures, acute loss of mobility with resultant falls.
Many of the elderly she has cared for and knows well have had their death hastened, or had to move into residential care as they now cannot manage at home.Thanks for helping us to get our stories out there.
RN, 40 years experience, NSW.
27/09/21. AHPRA Verified ✅Hello,
I am an RN with over 40 years experience, mostly in the public sector.I am currently employed on a casual basis.
I received a letter from NSW Health last week stating I “ must have” my first “ vaccination” by the 30th September to continue to work.
If I don’t I will not be able to work for NSW Health and will be placed on unpaid leave.All of the nurses in my ward( except a pregnant one) acquiesced to the “ vaccine” even though some were
dead against it.One nurse experienced loss of sensation in both legs below the knees which eventually resolved.
Another staff member( clerical) had a mini stroke and ended up in ED.
Both these episodes were not reported as vaccine injury.Indeed, one Physician said it definitely is not vaccine related.
I will now be forced not to work as I do not want the “vaccine”.
I believe NSW Health system will be in dire straights after 30th September and beyond as very experienced staff leave.I am a Registered Nurse working for a large public hospital in Melbourne.
A significant amount of our patients have had the covid vaccine and are presenting to us as transfers from ED, presenting with chest pain, shortness of breath, neurological symptoms , headaches and fevers. These patients are being found to have confirmed mini strokes (TIA), Pulmonary Embolisms, neurological disorders, severe headaches and deranged pathology resulting particularly often in acute kidney injury.
The most concerning of these presentations is the fact that majority of these patients range from 20-70 years old. One female patient in her 30’s presented with a body temperature of 40 degrees and has since been found to have multiple bilateral PE’s.
There has been no documentation or discussion from Doctors linking these patients symptoms with their recent covid vaccination. These patients were healthy and fully functioning people pre vaccination.
We’re also having to palliate patients at a concerning rate due to acute deterioration. Most of these patients are dying from respiratory failure or suffering a massive stroke.
All nurses in my clinical area have now been vaccinated besides myself. Some have told me they were coerced into getting it by management.
I am counting down the days now until I’m fired for not wanting the vaccine.Our current staffing is awful, I hate to think how bad it will be after October 15th when unvaccinated nurses are mercilessly terminated from employment. I feel for the patients who will fall through the gaps of our already stressed healthcare system.
Registered Midwife, WA.
28/09/2021
AHPRA Verified ✅Hello, Thank you so much for the work you are doing.
I’m a Registered Midwife in W.A. and until I resigned on Wednesday Sep 21, I had been working at the biggest hospital in the South West region. When RANZCOG and the ACM came out with their guidelines stating the c19 vax was safe for pregnancy, the directive from the hospital was to promote it hard.
At the hospital clinic I know of 2 women that received their first doses and they subsequently lost their babies;
1st dose at 34 weeks and 2 days, fetal death in utero at 36 weeks
1st dose 28+2, fetal death in utero 29 weeks I know of other women in the community under 20 weeks as reported to me by midwives that work with General Practice obstetricians;
1st dose 12+6, miscarriage 13 weeks
1st dose 17 +5, miscarriages 18 weeks
1st dose 12 weeks, miscarriage 12+2
Now, I know correlation does not mean causation, but it certainly should be investigated. Only one of the above cases have been reported. I fear many won’t be and they will be lumped into the 1:4 pregnancy loss statistic.
It’s not something that is asked (vaccine status) when women come to the hospital with a loss, so many may fall through and be missed.
I mentioned it to a doctor and they didn’t see the connection. I’m so sad to leave a job I love, but this isn’t health. This is something entirely different.
Registered Midwife, Small Rural Hospital.
28/09/21. AHPRA Verified ✅Hi,
I’m a Midwife in a small rural hospital.
We recently admitted a woman who’s baby had unfortunately died in utero and was subsequently stillborn. She was in her third trimester and she’d had her 2nd dose of Pfizer just 3 days before she stopped feeling the baby moving.
When I questioned my manager if this was going to be reported to the TGA she talked to the doctor and he said no, because there was no evidence of the two being linked.
I can’t help but wonder…what if nobody else is reporting events like this either because they all think there is no evidence?
contact us: nursesspeakout@pm.me
COVID-19: Vaccinating kids – the debate heats up
By Maryanne Demasi, PhD | September 23, 2021
5- to 11-year-olds
This week, the Australian Federal Health Minister announced a commitment to COVID-19 vaccines for kids aged 5 to 11 years pending TGA-approval, after Pfizer claimed, in a press release, that it had obtained “favourable” results.
Pfizer’s ongoing Phase 2/3 trial apparently showed the vaccine “was safe, well tolerated and showed robust neutralising antibody responses”. However, the results were not submitted to the drug regulator, nor were they published in a medical journal, so for now, we must take their word for it.
Pfizer registered the trial plan, showing that it tested a lower dose (10µg) as well as two higher doses (20µg and 30µg) in 5- to 11-year-olds. Whether the vaccine can provide protection against symptomatic disease or severe COVID-19 remains to be seen.
The manufacturer also claimed that the vaccine had a “favourable safety profile”, however, it is important to note that the trial has not enrolled enough children (2,268) to detect any rare but serious harms that might arise from the vaccine
Only healthy kids were recruited in the trial – children with known or suspected immunodeficiency, a history of autoimmune disease, any condition associated with prolonged bleeding, anyone receiving treatment with immunosuppressive therapy or corticosteroids were excluded from the trial.
Notably, these are the same cohort of children who have been prioritised for the vaccine.
Despite little to no data available for its safety and efficacy, the Israeli Ministry of Health gave the green light to start vaccinating high risk 5- to 11-year olds with the lower-dose (10µg) of the vaccine.
Pfizer senior vice-president Dr Bill Gruber said he felt “a great sense of urgency” in the process, and Pfizer’s CEO Albert Bourla said trial data would be submitted to the various international drug regulators for “immediate authorisation.”
The language of Pfizer executives, the frenzied press coverage, and the political will of Governments, is all designed to pressure drug agencies to fast-track authorisations.
Younger than 5 years old?
Pfizer announced that trial data involving children under 5 are expected later this year.
Last week, Cuba began vaccinating toddlers as young as 2, using its homegrown vaccine, the Soberana 02, from the Finlay Vaccine Institute administered at adult doses. To my knowledge, there has been no data from Phase III trials published in the peer-reviewed literature in children as young as 2 with this vaccine.
China’s drug agency has cleared three COVID-19 vaccines produced by Sinopharm and Sinovac and is vaccinating children aged 3 years and older, under emergency use authorisation.
12- to 15-year-olds
Most major western nations have authorised COVID-19 vaccines for those aged 12 years and older.
In Australia for example, children aged 12 to 15 years began receiving the mRNA vaccines last week. According to the NSW Premier, 20% of children in the state of NSW have already had their first jab.
They require a two-dose regimen, the same dose given to adults, which aligns with the US FDA and Health Canada advisories on vaccines for this age group. (See my previous analysis for 12-15yr olds)
This does not align with the UK’s more cautious approach. After significant political and media pressure, UK chief medical officers recommended a single dose of the Pfizer vaccine, because of concerns about rare side effects such as heart inflammation.
Brazil appears to be an outlier at the moment. It was reported that the Minister for Health called for the suspension of the COVID-19 immunisation of people aged 12 to 17 after the death of a 16-year old girl named Isabelli Borges Valentim, eight days after she received the Pfizer shot. Authorities are still investigating the incident but the drug regulator denies any link to the vaccine.
Myocarditis/Pericarditis
This issue has stirred up some heated debate.
Now that real world data is becoming widely available, myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the membrane surrounding the heart) are being reported as rare harms related to the Pfizer & Moderna mRNA vaccines.
Israel, because of its fast vaccine roll-out, was first to raise the alarm – 148 cases of myocarditis were reported within 30 days of immunisation, more commonly after the second jab. It prompted the Israeli Ministry of Health to launch an investigation into any possible link between these cases of myocarditis and vaccination.
Since then, other countries such as the UK, the US and Canada have corroborating data.
In June, the US FDA decided that the link between the mRNA vaccines and myocarditis, particularly in young males, was sufficiently clear that it revised its vaccine fact sheets to include a warning.
The CDC released data showing the incidence of “expected” versus “observed” incidences of myocarditis and pericarditis and found a significant increase in the observed rates. The graph shows the higher rates in red (see table numbers circled in red).

Another study, published in JAMA which looked at data from 40 hospitals in the US showed a similar pattern to the CDC, although at higher incidences, suggesting that the vaccine’s adverse events were being underreported.
Researchers then took a more granular look at the database for reported adverse events (VAERS database) between 1 January and 18 June, and found boys aged 12-15 years vaccinated with their second shot of the mRNA vaccine, with no underlying medical conditions were 4 to 6 times more likely to develop a cardiac adverse event, than ending up in hospital with COVID-19.
The study was published as a pre-print online but it ignited a twitter storm, with critics claiming the study ‘over-estimated’ the risk and it was biased because one of the authors belonged to a group that did not support making vaccines compulsory.
Sceptics say that most of the myocarditis cases are mild, and that children recover quickly from hospitalisation. Others are not so quick to dismiss the potential risk of ‘sub-clinical disease’ (myocarditis without symptoms) in children.
Notably, a retrospective multi-centre study across 16 US hospitals including patients <21 years of age with a diagnosis of myocarditis following COVID-19 vaccination, found concerning abnormalities in heart tissue (the left ventricle) (See image with yellow arrows).
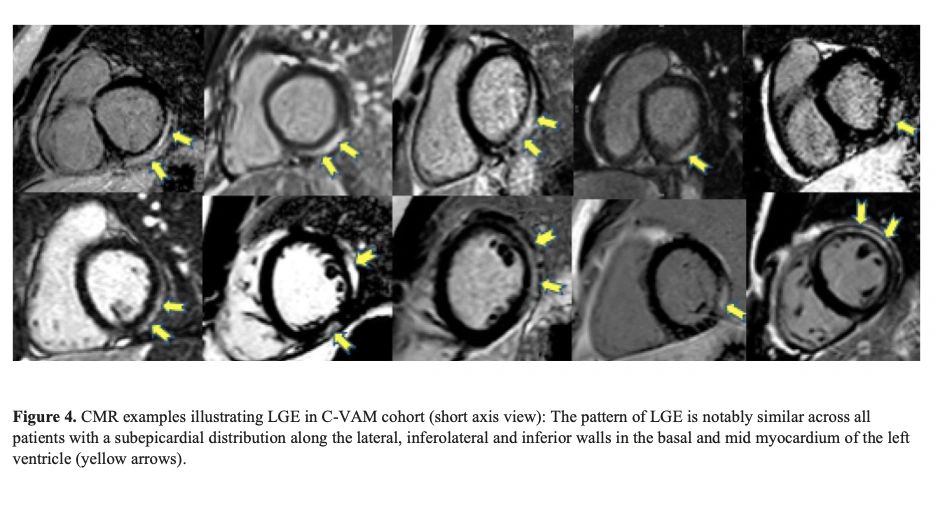
Jain SS, et al doi: 10.1542/peds.2021-053427.
Careful monitoring is required to see if these abnormalities lead to fibrosis, which can have long-term implications for young patients.
Early findings suggest that post-vaccination myocarditis could be mediated by the toxicity of ‘spike protein’ on heart muscle cells or from circulating spike proteins in plasma after vaccination.
The risk of myocarditis associated with contracting COVID-19 infection may be higher than that after vaccination, but more research is needed to weigh harms against benefit.
If we don’t vaccinate kids, what about long COVID?
The fear of long-COVID has been a major impetus behind vaccinating kids.
A recent review by Monash University, analysing 14 international studies on long COVID in children and adolescents, found no difference in the symptoms reported by those who had experienced COVID-19 and those who had not.
Lead researcher on the study, Professor Nigel Curtis told newsGP the review’s findings should be reassuring for parents and carers.
Similarly, a webinar hosted by The BMJ revealed the results of the largest citizen-scientist participation study to date in young children. It used a smartphone app to monitor the illness and symptoms of children after testing positive to COVID-19.
The researchers found that the median duration of illness was 6 days. Only 4.4% of children had illness duration >28 days and 1.8% had symptoms >56 days. Encouragingly, their symptom ‘burden’ was greatly reduced by this time (none became worse) with the most common symptoms being headache and fatigue.
The researchers looked at neurological symptoms such as epileptic seizures, convulsions, impaired attention and concentration, but none were reported.
Lead investigator on the study, Prof Emma Duncan from Kings College in London concluded “Long illness duration of COVID-19 in children is uncommon.”
Vaccine Mandates for kids
Despite COVID-19 vaccine mandates for teachers in places such as New York and Australia (Victoria and New South Wales), no Federal government has announced plans to make the vaccines compulsory for children (yet).
Canadian and English professors have argued that making COVID-19 vaccines mandatory for children, will “encourage uptake”.
U.S. Surgeon General Vivek Murthy has also suggested that COVID-19 vaccine mandates for students could happen at the state and local level in the US, once they have been approved for paediatric use by the US FDA.
In a surprise announcement this week, the Los Angeles public school system said students aged 12 and older will now have to be double-vaccinated by the end of the year, to attend classes on campus or take part in sports and other extracurricular activities. It remains to be seen whether other school districts will follow.
Consent from kids
Before the age of 14, minors are generally thought to lack the cognitive capacity and maturity to make rational judgments about their health.
In fact, most US state laws presume that minors lack medical decision-making capacity and therefore require parental consent for most health care decisions, including vaccination, with some exceptions.
However, in the case of COVID-19, under what is termed ‘Gillick competency’, those under 16 years can make independent decisions about a medical treatment if they can demonstrate they have the capacity to consent, even if their parent withholds consent.

This applies to every Australian state and territory as part of the ‘common law’ and in the UK.
The Victorian government has produced ‘communication packs’ for teachers and educators on how to ‘promote’ COVID-19 vaccines to minors.
Hopefully, the conversations about COVID-19 vaccines, between health professionals and minors, are conducted without coercion, pressure or judgment.
Not surprisingly, this has raised the age-old question about who is better placed to determine the best medical treatment for a child – a parent or a Government minister?
The debate will continue and experts will need to wade through muddy waters to find a balance between protecting children’s health and the uncertainty over the long-term harms of the vaccine.
Pending International Treaty Empowering The WHO
By Dr Urmie Ray B.A., M.A., Mmath, Ph.d. | Principia Scientific | September 23, 2021
Between 29 November and 1 December 2021, member states are meeting in a special session with the World Health Organisation to discuss, possibly sign, a new treaty on pandemic preparedness and response.
This decision was taken in March 2021 and backed by 26 nations, among which Australia, Canada, Iceland, Norway, Republic of Korea, South Africa, Ukraine, United Kingdom, United States, Uruguay and Member States of the European Union.1
To be noted is the absence of Russia, China, and India among these 26.
The International Health Regulations (2005)[i] signed by 196 countries already provide States the legal right to:
“– review travel history in affected areas;
– review proof of medical examination and any laboratory analysis;
– require medical examinations;
– review proof of vaccination or other prophylaxis;
– require vaccination or other prophylaxis;
– place suspect persons under public health observation;
– implement quarantine or other health measures for suspect persons;
– implement isolation and treatment where necessary of affected persons;
– implement tracing of contacts of suspect or affected persons;
– refuse entry of suspect and affected persons;
– refuse entry of unaffected persons to affected areas; and
– implement exit screening and/or restrictions on persons from affected areas.”
In other words, all the measures applied round the world since 2020, including mandatory vaccination, are in effect legal under this former treaty.
In particular, it critically changes the definition of “quarantine” from that in the 1969 IHR. There, it is used only in the expression “in quarantine” defined to be a “state or condition during which measures are applied by a health authority to a … means of transport or container, to prevent the spread of disease, reservoirs of disease or vectors of disease from the object of quarantine”.[i]
The 2005 revised IHR use the term by itself, and define it as “the restriction of activities and/or separation from others of suspect persons who are not ill or of suspect baggage, containers, conveyances or goods in such a manner as to prevent the possible spread of infection or contamination”.
This represents a subtle but critical shift from protection of the community to restriction of individual liberties.
The implementation of quarantine and other coercive measures on all, including surveillance and vaccination, is legalized: the expression “suspect persons” criminalizes every individual, both healthy and unhealthy.
Indeed, it covers anyone “considered by a State Party as having been exposed, or possibly exposed, to a public health risk and that could be a possible source of spread of disease”. Of significance is the use of “possibly” and “possible”, hence not just anyone definitely known to be a risk factor.
So Why The Need For A New Treaty?
The answer was given by WHO Director-General Tedros Adhanom Ghebreyesus. “It’s the one major change, Tedros said, that would do the most to boost global health security and also empower the World Health Organization.”[i]
The 2005 revised IHR still leave some authority to States and require certain conditions for a health event in a particular State to be considered sufficiently serious globally for the State to be forced to communicate it to WHO. Once communicated, it becomes the prerogative of the director general of WHO to determine whether it “constitutes a public health emergency”, but in collaboration with that particular State.
Although it should be added that in case of disagreement, the director general decides after consultation with the emergency committee of WHO, and passed a certain period no State can reject or emit reservations about the IHR or any later amendments. Still, to some extent, measures implemented remain the result of a dialogue between “IHR focal points” in each country and “WHO IHR contact points”.
What is particularly important is that the above listed measures, although rendered legal by the IHR, can under this treaty, only be recommended by the WHO, not imposed, and that it is up to the States to proceed towards their imposition, and to verify they are followed by means already existing in their respective countries.[ii]
The new treaty would address the above “weaknesses” of the IHR as they are considered to be, by ensuring “independent verification, monitoring, and compliance”. Given the clearly expressed end of empowering the WHO, should one conclude that “independent” means under the authority of WHO rather than the States themselves?[i]
Further the IHR cover “public health hazards and public health emergencies of international concern”, whereas the treaty will concern “all hazards”, not just pandemics. In the latter case, it would take over from the IHR once a pandemic is officially declared by the WHO.[ii]
This said, the treaty would presumably also make clear the idea expressed in the 2007 CDC “Interim Pre-pandemic planning guidance”,[i] namely overruling the need of a pandemic to implement restrictive measures. All that would be needed would be for an event to be declared a “public health emergency of pandemic potential”.
Given that any future event is always hypothetical, does this enable the maintenance of the measures for an indeterminate period? For it can always be claimed that a pandemic will occur especially were the measures lifted. This raises many questions, all the more so as the event would no long need to be of “international concern as in the current IHR”. “Measures”, as advised, should also go beyond the current scope of IHR”, in particular to cover the production and supply of vaccines, diagnostics, and treatments”.[ii]
The treaty would unlike the IHR also go beyond sanitary issues and allow the implementation of measures against “social and economic disruptions” as well as “broader disaster risk”.[i]
Would this in effect not only make it legal to put an end to criticisms, and thus to the freedom of expression, and make it possible to control any public antagonism against restrictive measures through “urgent international assistance”,[ii] namely not just by national police or military forces, but international ones?
In short, would the treaty not provide the international legal framework for derogation from the civil and political rights guaranteed “even in time of emergency threatening the life of the nation” by The Syracuse Principles on the Limitation and Derogation Provisions in the International Covenant on Civil and Political Rights drafted in 1984,[iii] namely:
“the right to life; freedom from torture, cruel, inhuman or degrading treatment or punishment, and from medical or scientific experimentation without free consent; freedom from slavery or involuntary servitude; the right not be be imprisoned for contractual debt; the right not to be convicted or sentenced to a heavier penalty by virtue of retroactive criminal legislation; the right to recognition as a person before the law; and freedom of thought, conscience and religion. These rights are not derogable under any conditions even for the asserted purpose of preserving the life of the nation”?
For the Syracuse Principles only ensure that “No state party shall” in any circumstance “derogate from the Covenant’s” above guarantees”. However, according to the new treaty, would the WHO, possibly together with the help of other international bodies, not become an occupying planetary power, with each State a collaborating subservient unit, like France in 1940, and hence without any power to ensure that non-derogable rights are protected?
Last but not least, “[t]rying to revise the IHR would be a long process and take several years. … In addition, any amendment made to the IHR will enter into force only two years after its adoption. A world in crisis cannot afford to wait this long.”[i] Why such a rush to get the treaty ratified?
It should not be forgotten that among the main contributors of WHO are the Bill and Melinda Gates foundation and the vaccine alliance (GAVI). It established in 2000 and whose initial funding it essentially provided – a “unique public-private partnership … bring[ing] together key UN agencies, governments, the vaccine industry, private sector and civil society”.[i]
References
[1] https://apps.who.int/gb/ebwha/pdf_files/WHA74/A74_ACONF7-en.pdf
[1] https://www.who.int/health-topics/international-health-regulations#tab=tab_1
[1] https://www.who.int/csr/ihr/WHA58-en.pdf
[1] https://www.who.int/csr/ihr/WHA58-en.pdf
[1] Ibid.
[1] https://www.centerforhealthsecurity.org/cbn/2007/cbnreport_02072007.html
[1] Ibid.
[1] Ibid.
Elderly Australian woman knocked down & Pepper-Sprayed by police during protest against lockdowns

RT | September 19, 2021
An elderly woman believed to be in her 70s was attacked by Melbourne police and pepper-sprayed while she was on the ground during a protest against Covid-19 lockdowns on Saturday.
As she held an Australian flag and stood on the road facing toward a group of approaching police, one officer shoved the woman, sending her tumbling to the ground. Another officer then pepper-sprayed the woman as she laid motionless and unable to protect herself.
Seconds after the attack – with the offending officers having already moved on – another group of police officers came to the woman’s aid and attempted to help her up.
Videos of the attack from multiple angles went viral on social media this weekend, with many Australians accusing the Melbourne officers of police brutality.
Australian MP Craig Kelly called the attack “despicable,” “disgusting,” and “ILLEGAL,” and tweeted, “This is not my Australia… We cannot accept Police in Australia pushing to the ground an unarmed 70 yr old woman (or anyone) who presents no threat & then have 2 officers pepper spray the unarmed, defenceless person in the face while on the ground.”
Former New South Wales Senator David Leyonhjelm also condemned the attack, calling the officers “gutless,” while journalist Ky Chow wrote, “I’ve watched several videos of this, and it’s hard to see how the Vic cops defend this.”
Several other incidents of violence between police and protesters broke out during the protest in Melbourne on Saturday and 235 people were reportedly arrested.
Melbourne police were also caught on camera pepper-spraying dozens of other Australians who were involved with the “unauthorized protest.”
Both Melbourne and Sydney have experienced repeated protests over the past few months in response to Covid-19 lockdown restrictions in the two cities. In August, a man from the state of Victoria was sentenced to a maximum of eight months in prison for helping to organize a protest in Sydney, New South Wales.
A Sad and Shameful Day for Australian Medicine
By Professor Robert Clancy | Quadrant | September 13, 2021
September 10, 2021, was a black day, the day a group of faceless bureaucrats known as the “Advisory Committee for Medicines Scheduling”, through its effector arm, the Therapeutic Goods Administration (TGA), compromised medical practise and the health of their fellow Australians. The TGA used its regulatory muscle to prevent doctors at the COVID-19 pandemic’s coalface from prescribing ivermectin (IVM), the one therapy available that is safe, cheap and which reduces mortality in the order of 60 per cent. This poorly conceived action threatens the high standards of medical practise we have achieved in Australia, and the credibility of the administrative structure within which medicine operates.
The immediate consequence of the TGA Notice means patients contracting COVID-19 are left to hear, “Sorry, no treatment for COVID-19 is legally available. Just go to hospital when you get very sick.” In the longer term it means that bureaucrats can change the way medicine is practised for whatever reason without review by, or discussion with, the medical community. It is important for Australians to consider two issues that follow the TGA’s decision: first, it adds risk to those exposed to COVID-19, putting additional pressures on health-care facilities; second, it drives a wedge into the fault lines that have appeared in medical practise during the course of the COVID-19 saga.
Looking at the first issue, the decision by the TGA to prevent general practitioners from prescribing IVM to manage COVID-19, the Notice is flawed and misleading, although giving clues to its political motivation. The evidence that IVM is safe and effective in both preventing and treating early (pre-hospital) COVID-19 is overwhelming, as has been laid out in four Quadrant articles published through 2021. Despite this evidence, every artifice has been used to quash IVM’s use and to do so in unprecedented fashion. The causes for the suppression include political agendas, pressures from pharmaceutical companies, ideology and breakdown in medical communication. This latest blow by the TGA follows its previous form in shutting down use of hydroxychloroquine, another safe, effective and cheap COVID-19 therapy. Every experienced doctor prescribes drugs for “off-label” indications. It is anathema and dangerous that the doctor-patient relationship can now be over-ridden by government agendas.
The driving source of “evidence” that IVM has unproven therapeutic value is the Cochrane Review, which concluded from a single meta-analysis that the benefit in treating COVID-19 was “unproven”. This was out of line with a series of supportive meta-analyses by non-conflicted competent epidemiologists. Yet results from Cochrane have singularly been adopted without criticism or discussion, initially by the National COVID Clinical Evidence Taskforce (NCCET), then by diffusion via various professional and regulatory bodies while being fanned by an even less critical mainstream press. Thus IVM is seen by many, including some medical professionals, as the snake-oil of our age. What is not discussed is the validity of the Cochrane Review and the advisory messages from the NCCET. The influence of vested interest parties on Cochrane has been previously raised. The circumstances of generating the review by an unknown German group when experienced epidemiologists were available needs explanation. More immediately, critiques of the Cochrane analysis and the NCCET by unaligned British epidemiologists show defective methodology, cherry-picked data and exclusion of a raft of supportive data.
The information source used to formulate policy in Australia is both out of kilter with conclusions from over 60 controlled clinical trials and the positive experience recorded when IVM was used in national and regional programmes. Cochrane is an incomplete and unreliable basis for decision making on COVID-19 management in an Australian context. The views of international experts are trumped by unknown local bureaucrats.
Surprisingly, the reasons given by the TGA for their decision on IVM are not the usual mantra of “unproven”, based on Cochrane, although that is left hanging as a “given”. The reasons are even less defensible: “supply may become limited” (incorrect, but this nevertheless demonstrates there is a need for the drug); “concerns re toxicity due to dosage determined by social media” (this concern is easily remedied by controlling usage through front-line doctors), and, lastly, the real reason: “It may interfere with the vaccination programme”. What an extraordinary statement!
The reason for “vaccine hesitancy” has nothing to do with IVM use. Doctors promote IVM as complementing the vaccine programme, which, given concerns regarding vaccine resistance caused by Delta strain of the virus and waning of post-vaccine immunity, makes early drug treatment more needed than ever. It is irresponsible to exclude IVM as a drug to control high numbers of infections that will be encountered as Australia moves out of its “bubble”, irrespective of the level of vaccination. The only parts of the world not experiencing a “third wave” of infection are those where lockdowns have been avoided, such as Sweden, or where IVM is used throughout the community, as is seen in parts of South America, Mexico and India.
The real cause of “vaccine hesitancy” is lack of transparency and discussion. Where is the discussion that death from COVID-19 is one thousand times greater than reported deaths linked to the vaccine? That is a fact easily understood. There are genuine concerns about experimental genetic vaccines, yet discussion is suppressed, and these issues are treated as “best kept secrets” by authorities. Failure to openly discuss these concerns in the context of a plan for a safe future vaccine strategy is reason in itself for uncertainty and conspiracy theories. It is unacceptable to shift blame onto IVM for “hesitancy”. Both vaccines and IVM are urgently needed, and suppression of IVM simply leads to unnecessary deaths and a postponed public reaction when evidence supporting the value of both becomes more widely known. Have we learnt nothing from the preventable thousand deaths that followed refusal in the US to allow cheap, safe prophylaxis against Pneumocystis infection in AIDS patients until a randomised clinical trial (RCT) was completed in the 1990s?
What is the influence of pharmaceutical companies? They have actively conspired against IVM while accepting hundreds of millions of government dollars to develop their versions of “early treatments”; in this they have been supported by the TGA that has now regulated against IVM. Meanwhile, the TGA recently registered a monoclonal antibody, Sotrovimab, based on a single small trial. This drug has a similar protection profile to IVM but costs $4,000 a dose (I support its registration, although it is hard to see how it could be superior to IVM). The TGA approved Remdesivir following one study showing its only benefit was four days less hospitalisation. Three subsequent RCTs failed to confirm benefit, yet the TGA allows the drug’s continued use in Australian hospitals. Just a week ago, the TGA reported with enthusiasm discussions with Merck about “son-of Remdesivir”, Molnupiravir, which comes with no clear clinical benefit noted from what are incomplete studies. The US government has bought millions of doses at $1000 per dose. Whose interests are being protected?
Second, the implications for medical practise are a more sinister and subtle consequence of the TGA decision. Preventing general practitioners prescribing IVM for early COVID-19, when there is evidence of safety and benefit, sends a concerning message to community-based doctors. It threatens the “doctor-patient relationship”, as patients with COVID-19 are also aware that drugs are available which could save their lives. It also challenges the traditional role of senior medical advisers, most of whom are hospital-based with no experience of early COVID-19, and are influenced by expert bodies such as the NCCET, and of course Cochrane reports.
Cochrane is promoted as the foundation stone of Evidenced Based Medicine (EBM), the holy grail of contemporary medical practice. Dr. Dave Sackett was the “father of EBM” at Canada’s McMaster University, where he and I led medical-admission teams for five years. We had numerous discussions of EBM, then in its formative stage, anticipating it would have an integrating role in medical practise. Dave died in 2015, which saved him the disappointment of seeing what has happened during COVID-19, where a limited Cochrane review is used as a lever to achieve political outcomes to the disadvantage of patients. The unravelling of well-established professional relationships between community doctors, their medical advisory structures and government bodies has not been helped by the confusion, the lack of organised education activities and the isolation enforced by the pandemic.
The authoritarian and poorly conceived interference by the TGA in the effective running of clinical medicine, and its broader implications, is a further splintering event. This is a time when everyone needs to be on message to counter a devastating pandemic. The use of blunt legal tools to threaten and bully doctors with de-registration, legal action for “advertising” and even with jail terms for striving for the transparency and common sense that has served medicine so well compromises the rules of science and the doctor-patient relationship upon which our profession is built. The answer is transparency and communication around agreed goals based on science. We should again involve all levels of health care and the public we serve. The decision-making process should include clinicians familiar with the problem to ensure the pragmatic and common-sense approach needed to get us through this pandemic with minimum damage.
Rather than create the chaos and loss of respect for an important institution that will follow continued enforcement of the current Notice, the TGA should initiate a working party that includes frontline doctors to establish an agreed treatment protocol that includes dosage, with monitoring of the outcomes. We live in dangerous times that call for new ideas able to address a real world crisis that is out of control and will only get worse without a different way of thinking.
Emeritus Professor Robert Clancy AM MB BS PhD DSc FRACP FRCP(A) RS(N) is Foundation Professor Pathology, Medical School University Newcastle, Clinical Immunologist and (Previous) Head of the Newcastle Mucosal Immunology Group, with special interest in airways infection and vaccine development.
Australia’s Labor Party asks Google what “misinformation” censorship plans it has for the next election

By Christina Maas | Reclaim The Net | September 17, 2021
Australia’s Labor Party wants Google to explain the steps it has taken to ensure its platforms are not “exploited for misinformation” ahead of the next general election. The party says it fears its rivals will use “misinformation” to gain an edge in the upcoming election.
According to The Guardian, Labor’s national secretary Paul Erickson sent a letter to Google Australia’s managing director Mel Silva, asking if the company has improved its systems since the last election in 2019 to “ensure its platforms and advertising capabilities are not exploited for misinformation.”
In the letter, Erickson mentions Craig Kelly and businessman Clive Palmer for their criticism of the strict COVID-19 measures. He notes several videos posted by Kelly on his YouTube account “in which Mr Kelly promotes ivermectin and hydroxychloroquine as effective treatments for COVID-19 or claims that Covid-19 vaccines are unsafe,” according to The Guardian.
Kelly, a former member of the Liberal Party, formed his own party, the United Australian Party (UAP).
Erickson’s letter further asks Google how it plans to handle “the elevated risk of misinformation in the context of the upcoming federal election, including in relation to content uploaded by the UAP.”
The Labor leader notes that the UAP “is already spending hundreds of thousands of dollars on political advertising, including on Google’s platforms.” He insisted that it was crucial for Google’s platforms not to be “misused” amid a pandemic, “including by those with a track record of spreading politically motivated misinformation in the lead-up to the next federal election.”
“Regrettably, the response of digital platforms was wholly inadequate,” Erickson wrote. “These mistakes should not be repeated.”
The Labor party was the victim of a misinformation campaign relating to the “death tax” in the last election.
Kelly slammed Erickson for the letter.
“It is a disgrace and a new low that a political party would ask a foreign oligarch to censor freedom of speech in Australian politics,” the MP told The Guardian Australia. “The idea that an alternate opinion of an expert is misinformation is a claim I categorically reject.”
The UAP leader described Erickson’s letter as “silencing of genuine debate, and that will leave the public misinformed.”
Australia: Petition EN3196 – Alternate treatment options for Covid 19
Petition Request
Millions of Australians are extremely concerned about the federal government’s push to force hastily approved and poorly tested novel vaccines on the population, when adequate long term safety data is unavailable.
It is also is of great concern that many notable doctors and medical researchers reporting successful treatment using cheap, safe generic anti viral drugs appear to be ignored by the government and TGA, due to these generic drugs being of little commercial value and not sponsored by pharmaceutical companies for approval by the TGA.
We therefore ask the House to formally request that the TGA assess the use of Ivermectine and Hydroxycloriquine, in the recommended dosages and combination with complimentary drugs, based on the peer reviewed studies and data, and the recommendation of notable Australian medical researchers such as Professor Thomas Borody and Professor Robert Clancy.
We ask that the house requests this of the TGA in the absence of sponsorship by a pharmaceutical corporation, seeing as both of these drugs are generic and of little commercial value to an individual company, and due to the conflict of interest many of these companies have with competing patented vaccines of far higher commercial interest.
We believe that if this is performed thoroughly and transparently it will restore public faith in the federal government, and also provide confidence to the public that all options for treatment are being honestly explored.
The petition is currently open for signatures. [until September 29th]
To see more and sigh the petition, see here: aph.gov.au
The tragedy of Australia
By Paul Collits | TCW Defending Freedom | September 10, 2021
The writer is in Australia
THE British historian Guy de la Bédoyère claims that ‘Australia is falling apart’. Off Guardian suggests that we are ‘going full fascist’. Daily reports in France, Russia and everywhere in between and beyond, hover between pity, amusement and disbelief. How did this happen – in Australia? The overseas storytelling can barely keep up with the never-ending stream of new announcements designed to grind us into the ground. But on and on it goes.
There is, at last, a book-length account of Australia’s eighteen months of madness that will either warm the hearts of Covid realists, remind us of all the Covid policy absurdities or perhaps simply provide yet more chilling evidence of the sinister forces at work that are changing us irrevocably.
Unfolding Catastrophe: Australia (Sense of Place Publishing, 2021), by John Stapleton, restores – though perhaps only a little – the faith we ought to have in the journalist class, so utterly diminished by their sitting out the crushing of our lives (at best) and their active collaborating in the spread of Covid propaganda (at worst).
Recognising early on the biggest story of all of our lives, Stapleton set out to record in graphic detail and with authenticity the developing catastrophe, from the toilet paper crisis at the start to the emerging apartheid regime for those who refuse the State Injectible.
Stapleton records with palpable astonishment the now familiar litany of harms that have been done, not only to the body politic, but to our core values, indeed, to our very sense of our country. Our place. They include the impositions of lockdowns that do not work but cause harm beyond telling; the ‘wildly inaccurate’ modelling that predicted catastrophe and instead merely delivered fame and riches for those involved; the succession of non-medical interventions with no basis in science and without popular understanding that this is the case; the low information voter; the punitive policing; the absence of real leadership in the crisis; the incoherent messaging from the top; the disaster that is ‘National Cabinet’; magic money tree economics; the relentless announcables; the Covid cronyism; the entrenching of power by the political class.
This all amounts to ‘a radical social experiment going against decades of epidemiological wisdom’. It has been, Stapleton suggests, ‘demonic’. Not just stupid and deranged, but evil. It has caused, as we now see in all our empty churches, ‘spiritual damage’. Earthly lives gone, and souls lost. A sad tale of deceit and compliance, of induced fear, isolation, economic deprivation, destroyed friendships and civil fracture. A creepy but unmistakable feel of the Biblical End Times, the streets empty. Astonishing submissiveness. A story of manufactured narratives, of a ‘disinformation feedback loop’ as Stapleton reports, his previous faith in the scepticism of his countrymen utterly destroyed. Societal dysfunction. Many ‘conspiracy theories’ across the internet have proved to be spot on.
The book draws upon a broad range of expert observers, who include journalists of every colour and distinguished academics such as the Spectator’s Ramesh Thakur, a breath of fresh air amid the fetid atmosphere of secular decline. Ramesh’s call on the Covid response, as reported by Stapleton: ‘The greatest mistake in history’. World War One is right up there, but this call is no exaggeration.
Rational argument simply does not work with our rulers. Copious evidence relating to the policy disasters of the pandemic never breaches the walls of the bubble. As Stapleton said in an interview with Sydney Criminal Lawyers, ‘it all fell on deaf ears’.
Is the tide of opinion turning against the ever-increasing crush of medical technocracy? Stapleton has cautious optimism. Speaking up for those of us who, mercifully, live outside the cities, he says: ‘But there are no cases or virtually no cases in this area. Nobody knows anybody who has died.’ Pennies may, at last, be dropping. Crisis? What crisis? It is a case-demic of a very mild strain of the initial virus, without the remotest hospitalisation crisis
Chillingly, as Stapleton says, ‘All of this has been done in secret, and in our name.’ The parliaments rarely sit. Public Health Orders trump democratic processes. Reasons are never given for policy actions beyond formulaic tosh. We never signed up for this.
Steve Waterson, one of the few consistently sane voices in the corporate media, describes the book as a ‘devastating indictment of Australia’s response to the Covid pandemic’. I am glad Waterson didn’t confine himself to ‘Australian governments’, for we are, all of us, complicit in this truly diabolical attack on everything we have all lived for. Stapleton uses the term ‘manipulated’ and ‘held hostage’ to describe our corporate media’s role in the fiasco.
Stapleton, alone, it seems, among our publishers and authors, has taken a stand – for freedom, common sense, perspective and Aussie values. His is a stand for life itself. His work shames his colleagues who have chosen to sit quietly in the corner these past eighteen months, or worse, to join in the chanting for the Covid Fascist State. This book is the methodical work of a brave truth-teller who is willing to call a spade a bloody shovel, in the best tradition of fair-dinkum journalism.
As the first draft of history, this magnificent book should be marked ‘essential reading’. Normally one might add here: ‘Send a copy to your member of parliament’. Alas, I fear, in this case, such a course of action would be pointless. Our rulers are in and settled, on a good wicket, and they intend to bat on.
A ‘signal collapse and rearrangement of society’? Who on earth could disagree?
Australia helped CIA in toppling Chile’s Allende, records show

Press TV – September 11, 2021
Australian government documents have revealed that the country assisted the US Central Intelligence Agency (CIA) in launching a coup against Chilean President Salvador Allende.
On September 11, 1973, an American-orchestrated military coup against Allende’s government resulted in a long-time dictatorship led by the coup leader Augusto Pinochet.
On the eve of the 48 anniversary of the coup, declassified documents published by the National Security Archive reveal that spies from the Australian Secret Intelligence Service (ASIS) assisted in the destabilization of Allende’s leftist government.
At the request of the CIA, ASIS established a secret base in Santiago in the fall of 1970.
Liberal Party Foreign Minister William (Billy) McMahon had reportedly approved the cooperation of ASIS agents with the CIA.
The base operated for approximately 18 months and involved Australian agents and equipment alongside several Chilean s[pies recruited by the CIA in Santiago.
The group gathered intelligence that was relayed to CIA headquarters in Langley, Virginia.
According to one of the declassified documents, Austalia’s then-Prime Minister Gough Whitlam, elected in December 1972, was “uncomfortable” with the participation of Australia, because if the acts of international espionage were made public it would be “extremely difficult” to justify their presence there.
Whitlam ordered ASIS director at the time, William Robertson, to dissolve the den of spies that Australia set up in Chile to assist the Americans to topple Allende’s democratically-elected government.
Despite Whitlam’s order, an Australian intelligence agent reportedly stayed in Santiago until after the US-led coup.
Another report also noted that the prime minister “was well aware of the importance of this (operation) to the Americans” and “was very concerned that the CIA should not interpret this decision (of the closure of the base) as a hostile gesture towards the US in general or towards the CIA in particular. “
Numerous crimes against humanity, persecution of opponents, political repression, and state terrorism were committed by the Chilean armed forces, members of Carabineros de Chile, and agents of the secret police of the Pinochet regime from 1973 to 1990.
Sydney doctor who criticized medical censorship online is suspended from practicing medicine
By Cindy Harper | Reclaim The Net | September 11, 2021
On social media, a Sydney doctor questioned whether vaccines and lockdowns would be effective in ending the pandemic while also scrutinizing how medical authorities were handling treatment. As a result of his postings, New South Wales medical authorities have taken action against Dr. Paul Oosterhuis by suspending him.
Oosterhuis’ social media activities have garnered at least two anonymous complaints to the medical council, the group confirmed on September 2nd.
“Over the last 18 months, I have been increasingly concerned about the misinformation and censorship creeping into science and medicine,” the doctor had stated.
Oosterhuis recommended that medical authorities advise COVID-19 patients to take vitamin D and zinc and to treat them with ivermectin and hydroxychloroquine.
He called the lockdowns “totalitarian” and causing “massive damage to society-wide.”
In a post, he wrote. “The risk of antibody-dependent enhancement of disease… driven by immune escape from the selective evolutionary pressure of vaccinating with a non-sterilizing agent is a real and present danger and needs to be discussed. The danger to millions is distressing me, and discussing that danger is, I believe, unarguably in the public interest.”
According to the Medical Council of New South Wales, Oosterhuis’s social media activity was flagged. He was asked to attend an “immediate action panel” on September 3rd and the anesthetist was questioned by the MCNSW.
“The Council deals with individual doctors whose conduct, performance or health may represent a risk to the public and works with them, where possible, to reduce that risk by for example, placing conditions on their medical registration. Section 150 or immediate action panels are held by the Council when a complaint or notification prompts serious concerns about risk to public safety or the need to otherwise act in the public interest. Panel members include community representatives as well as medical practitioners,” the MCNSW statement read.
The MCNSW provided Reclaim The Net with this full statement here
Ultimately, the MCNSW chose to suspend Dr Oosterhuis’ later that day.
Medical practitioners can be suspended by the medical council under New South Wales’ Health Practitioner Regulation National Law (NSW). The New South Wales Medical Council collaborates with the state Ministry of Health to investigate and resolve complaints about specific doctors and other medical specialists.
According to the council, this law does not give it the power to de-register Oosterhuis or revoke his license and they have no authority to punish him. However, despite his almost 30 years of experience in medicine, his suspension has already barred him from practicing in the medical profession.
Oosterhuis has responded by stating that he will not adjust his behavior to be more compliant. He stated that he intends to challenge the suspension, saying:
“I am very disappointed by the Medical Council’s decision to suspend my registration.
“The material I submitted in support of my evidence-based concerns was not considered. I intend to appeal the decision.
“The council drew upon s150 powers to demand an urgent hearing into some posts I have shared on Facebook on the importance of early treatment, particularly the low hanging fruit of vit D, Zinc, Quercetin, vit C and the repurposed drugs Ivermectin.
“I’m pro choice, pro informed consent… it’s always been a key ethical principle… you need to be able to discuss all the risks, benefits, and alternatives of any medical intervention.”
He later added, “Censorship kills. My responsibility to the Hippocratic oath, and basic ethics compels me to share data that I believe is definitely in the public interest.”
Despite an initial public statement, the MCNSW failed to make any further statements on this issue.
Featured Video

The Attack on Pearl Harbor Was No Surprise (Part V)
or go to
Aletho News Archives – Video-Images
From the Archives
Iran Delenda Est
By Stephen J. Sniegoski • Unz Review • July 25, 2019
After Carthage had been significantly weakened by Rome in the Second Punic War (218 to 201 BC), Cato the Elder, a leading Roman senator, is said to have ended all his speeches with the words: “Carthago delenda est!” (“Carthage must be destroyed!”). This destruction ultimately took place in the Third Punic War (149–146 BC). A somewhat similar situation exists today in the United States, where war hawks demand that Iran–which in no way could effectively attack the United States, or even conquer America’s Middle East so-called allies—be stripped of its ability to protect itself.
Of course, what makes the American situation different from ancient Rome’s is that Rome sought to eliminate Carthage for its own interests whereas the United States is largely acting to advance the military interests of Israel… continue
Blog Roll
Recent Comments
eddieb on The Old Testament and the Geno… papasha408 on Trump’s war posturing against… Coronistan on This is How We Should Have Res… Coronistan on NO MANDATES, NO PROFITS: MODER… Lutz Barz on Russia Vows to Protect Its Oil… loongtip on Russia Vows to Protect Its Oil… loongtip on Hamas never agreed to lay down… eddieb on Conspiracy Denial eddieb on WEF Calls for ‘Cultural Revolu… loongtip on Trump wanted to play peacemake… Coronistan on EU member to sue bloc over ‘su… loongtip on Vicious
 Aletho News
Aletho News- The Attack on Pearl Harbor Was No Surprise (Part V)
- How Human Rights Watch Shattered Yugoslavia
- Hamas rejects Israeli accusations as “lies meant to justify its massacres in Gaza”
- Interior ministry: Israeli strike on police building in Gaza shows disregard for mediators
- West’s hypocrisy over Iran and Gaza proves a regime-change operation in Tehran
- Trump’s war posturing against Iran traces back to Bush’s infamous 2002 ‘axis of evil’ speech
- The Streetlight Effect
- NO MANDATES, NO PROFITS: MODERNA CEO TELLS THE TRUTH
- UK Health Officials Covered Up Reports of Heart Damage Linked to AstraZeneca Vaccine
- This is How We Should Have Responded to COVID-19
- If Americans Knew
- Is Israel opening the Rafah border to depopulate Gaza? – Not a ceasefire Day 113
- NBA Star Stephen Curry’s Ties To Israeli Military Intelligence
- ‘Apocalyptic wasteland’: Biden admin. blocked warning on deteriorating Gaza situation after Oct. 7
- Why Israeli counterterrorism tactics are showing up in Minnesota
- Israel Went to Extremes to Return Ran Gvili’s Body. Why Doesn’t It Accord Dead Palestinians the Same Respect?
- Across the West, speaking for Palestine is now a crime
- A West Bank Bus Trip Through ‘the Best Documented Ethnic Cleansing in History’
- Mike Huckabee’s distorted theology does not speak for Christians worldwide
- CBS Evening News” With Tony Dokoupil Is Ellisons’ & Weiss’s Pro-Israel Show
- A Generation on Hold: Inside Gaza’s Collapsing Education System
- No Tricks Zone
- One Reason Only For Germany’s Heating Gas Crisis: Its Hardcore-Dumbass Energy Policy
- 130 Years Later: The CO2 Greenhouse Effect Is Still Only An Imaginary-World Thought Experiment
- New Study Affirms Rising CO2’s Greening Impact Across India – A Region With No Net Warming In 75 Years
- Germany’s Natural Gas Crisis Escalates … One Storage Site Near Empty …Government Silent
- Polar Colding…Antarctica Saw Its Coldest October In 44 Years!
- New Study: Sea Levels Rose 20 Times The Modern Rate During The Roman Warm Period
- As German Gas Storage Dips Dangerously Low…Shortage Hardly Avoidable
- New Study: Brazil’s Relative Sea Level Was 2+ Meters Higher And SSTs 3-4°C Warmer 6000 Years Ago
- Philosopher Schopenhauer: Climate Science Certainty Stems From Stupidity, Ignorance
- New Study: Species Extinction Rates Declining Since 1980 – ‘Climate Change Is Not An Important Threat’
