A majority of Americans now officially meet the definition of “anti-vaxxer”
By Aaron Siri | Injecting Freedom | July 29, 2024
The Merriam-Webster dictionary defines an “anti-vaxxer” as “a person who opposes the use of some or all vaccines, regulations mandating vaccination, or usually both”:
So, to be an “anti-vaxxer,” per the dictionary, a person needs to only oppose receiving some vaccines. Meaning, a person that opposes receiving a COVID-19 vaccine or an influenza vaccine is an anti-vaxxer. And guess what? The majority of Americans now oppose receiving both of these vaccines.
In fact, according to the CDC, despite spending billions of dollars wildly promoting these products, less than half of Americans received an influenza vaccine, RSV vaccine, and the updated COVID-19 vaccine. In fact, less than 23% of the adult population in the U.S. has received an updated COVID-19 vaccine despite a relentless multi-billion-dollar national promotion campaign.
Not only do a majority of Americans oppose receiving these vaccines, an even greater percentage of Americans no doubt (including some that receive these vaccines) oppose mandating one or more of these products.
The irony is that deciding against being injected with a product after reviewing its clinical trials, post-licensure safety record, lack of liability, etc., is an informed, thoughtful decision. Yet those that mindlessly get every vaccine are the ones painted as making informed, thoughtful decisions?! Hats off to Big Pharma/CDC for convincing so many that up is down and down is up.
The next time someone calls you an “anti-vaxxer” because you have made an informed decision to not receive a medical intervention, let them know that, yes, you did make an informed, independent medical decision. And wish them luck doing the opposite!
You can also let them know that since “anti-vaxxers” are now the majority, you understand their insecurity and hostility. But they shouldn’t worry: the anti-vax majority is not interested in taking away the rights of the pro-vax minority. They can feel free to get (or not get) as many vaccines as they want. We in the majority just ask that they respect our right to do the same.
Vaccine Advocate Peter Hotez Calls for Use of Police, Military Against ‘Anti-vaccine Aggression’
By Michael Nevradakis, Ph.D. | The Defender | July 26, 2024
Vaccine advocate and pharmaceutical industry insider Dr. Peter Hotez, long a proponent of the COVID-19 vaccine, said he favors deploying police and military powers against “anti-vaxers,” whom he blamed for causing hundreds of thousands of deaths during the pandemic.
During an interview July 5 at the Simposio Internacional de Actualización en Pediatría (International Symposium of Pediatric Updates) in Cartagena, Colombia, Hotez suggested organizations such as the World Health Organization (WHO), the U.S. Department of Homeland Security and NATO should target “anti-vaccine aggression.”
Hotez said:
“What I’ve said to the Biden administration is, the health sector can’t solve this on its own. We’re going to have to bring in Homeland Security, the Commerce Department, Justice Department to help us understand how to do this.
I’ve said the same with — I met with Dr. Tedros [director general of the WHO] last month … to say, I don’t know that the World Health Organization can solve this on our own. We need the other United Nations agencies. NATO. This is a security problem because it’s no longer a theoretical construct or some arcane academic exercise. Two hundred thousand Americans died because of anti-vaccine aggression, anti-science aggression.
The full interview was available on YouTube until Wednesday evening, when it was removed. The Defender obtained a video recording of the full interview.
Hotez is dean of the National School of Tropical Medicine at Baylor University College of Medicine and director of the Center for Vaccine Development at Texas Children’s Hospital, one of the sponsors of the symposium, which was organized by the Colombian Pediatric Society.
Aside from being a vaccine proponent and developer — he helped develop the Corbevax COVID-19 vaccine which was administered in India and has received at least $30 million in vaccine development grants from the Bill & Melinda Gates Foundation — Hotez has crusaded against so-called “misinformation” about vaccines.
In March, The Hill reported that Hotez has found a “‘parallel career’ fighting misinformation.”
Hotez “finds his efforts to combat misinformation to be ‘meaningful,’” and says “pushing back on the anti-vaccine movement is just as important as developing vaccines,” The Hill wrote.
Hotez also holds six patents on the hookworm (helminth) vaccine, and has several listed patent applications as well, including those for SARS-CoV2 vaccines.
“Peter has cashed in significantly on the COVID-19 pandemic and gets a lot of money when shots go into arms,” said Brian Hooker, Chief Scientific Officer for Children’s Health Defense (CHD).
In his July 5 interview, Hotez called for more stringent action against “anti-vaxers,” whom he connected to entities such as the Russian government, and called for medical schools to educate new doctors about anti-vaccine sentiment.
“‘Anti-science’ and ‘anti-vaxxer’ are propaganda terms Hotez uses to establish a power dynamic over anyone who disagrees with him,” said cardiologist Dr. Peter McCullough.
“Now Hotez is calling for a security state to enforce his propaganda instead of engaging in much needed dialogue over vaccine safety with a critical appraisal of short- and long-term side effects from the routine childhood vaccine schedule, including the COVID-19 shots,” McCullough added.
According to Harvey Risch, M.D., Ph.D., professor emeritus and senior research scientist in epidemiology (chronic diseases) at the Yale School of Public Health:
“Hotez has spent his entire career developing vaccines which have not achieved success in commercial use. His demands to impose public health martial law are reminiscent of the ‘Comité de salut public’ — ‘Committee of Public Safety’ — that Robespierre used to murder his political opponents [during the French Revolution].”
For Francis Boyle, J.D., Ph.D., professor of international law at the University of Illinois, Hotez’s suggestions are a call to violate established international human rights law.
“Coercing vaccines upon human beings without their informed and voluntary consent violates the Nuremberg Code on Medical Experimentation, which is a crime against humanity,” Boyle said. “What we see at work here with Hotez is the Nazi mentality that pervades so many vaccinologists like him. Hotez is revealing his true colors.”
Independent journalist Paul D. Thacker has investigated Hotez for his site, The Disinformation Chronicle. He said, “This crackpot idea that we should deploy military forces to deal with moms worried about vaccine side effects and children … doesn’t that speak for itself?”
Dr. Sukharit Bhakdi, a microbiologist, questioned Hotez’s scientific credentials:
“Simple fact: Hotez is not a real scientist. He has never published any research article based on true scientific research. His publications transmit his personal opinions and beliefs. He has not conducted a single valid vaccine trial and has zero data to back his claims.
“He has been on the globalist team together with [Dr. Anthony] Fauci et al. and is now turning to violence to silence all dissenters. This very fact disqualifies him as a physician.”
“His evolution over the course of the pandemic is curious as he has become more and more shrill as time goes on,” Hooker said. “It seems he is trying to extend his 15 minutes of fame by ‘jumping the shark’ and inciting gestapo-like measures against ‘anti-vaxers’ and ‘science deniers.’ His definition of science is very ‘Fauci-esque’ indeed.”
Claim that unvaccinated caused ‘hundreds of thousands’ of deaths ‘an obvious untruth’
During his July 5 interview, Hotez asserted that the unvaccinated were responsible for hundreds of thousands of deaths during the COVID-19 pandemic. He said:
“There’s anti-vaccine activity in every country, and each has its own unique national flavor. But the part that I’m worried about now is something very dark and accelerating in the United States.
“And the most dramatic evidence for that is what happened during the COVID pandemic … My estimate is 200,000 Americans died needlessly because they refused COVID vaccines in 2021, 2022.”
Hotez did not provide evidence supporting this figure, but it was similar to claims made by Dr. Anthony Fauci during Congressional testimony last month. Without citing evidence, Fauci said the unvaccinated are “probably responsible for an additional 200,000-300,000 deaths” in the U.S.”
Risch called this claim “an obvious untruth.”
“In the face of repeated major empirical CDC [Centers for Disease Control and Prevention] evidence and CDC’s public acknowledgement that the mRNA vaccines largely failed to reduce COVID transmission, Hotez absurdly claims that people choosing not to vaccinate themselves have contributed more to deaths from COVID than all of the large-scale breakthrough infections among vaccinated people,” Risch said.
McCullough said, “Hotez presumes COVID-19 vaccines are safe and effective as any vaccinologist would dream. Sadly, his fantasy was over before it started. The COVID-19 vaccines were unsafe and failed to reduce hospitalization and death in prospective randomized trials or in valid observational studies. They never stopped transmission.”
“All experts, including Hotez, agreed theoretical protection from COVID-19 vaccines was just a few months, requiring frequent boosters,” McCullough added.
Hotez calls parents who choose not to vaccinate their children ‘victims’
In his interview, Hotez called for action — including more censorship — to counter what he called a “dark and accelerating” and “dangerous” anti-vaccine movement in the U.S. and globally that is “expanding and extending to childhood immunizations in the United States.”
“My worry is that this anti-vaccine movement, and it’s not misinformation or [an] infodemic, as many call it, it’s organized, it’s deliberate, it’s well-financed and it’s politically motivated … I worry that’s now globalizing to other countries on the African continent, in Asia and even Latin America,” he added.
On the topic of childhood vaccinations, Hotez said, “Parents who choose not to vaccinate their kids are victims” of this campaign, and called for medical schools to train doctors on how to respond to parents who oppose vaccinations.
“Pediatricians need to understand what the anti-vaccine ecosystem is, how it’s organized, how it operates, and to get educated about it,” he said. “I think that’s a first step … in our medical schools, in our pediatric residency training, in our conferences like this, being able to describe what this anti-vaccine monster looks like.”
But for journalist Rodney Palmer, formerly of the Canadian Broadcasting Corporation, the increasing reluctance of parents to vaccinate their children is due to mounting concerns about vaccine safety. He said:
“The rising movement questioning the safety and efficacy of COVID-19 vaccines appears to be based on mounting evidence from government health data collection agencies and the life insurance industry.
“The fraud and cover-up of ivermectin as an effective prevention and treatment of COVID-19 caused a segment of the population to question the official guidance around vaccines — more so once they were mandated.”
Hotez blamed legacy and traditional media, as well as foreign governments, for fueling anti-vaccine sentiments.
“Fox News is now a source of anti-vaccine disinformation,” Hotez said. “If the parents are watching Fox News every night … They are going to be coming into your practice believing disinformation.”
Turning to social media, Hotez said, “Twitter, since Elon Musk has taken it over, has become an anti-vaccine site dominated by anti-vaccine groups and individuals who are monetizing the internet. They’re selling fake autism cures because they say vaccines cause autism, which they don’t.”
Hotez continues to be active on X.
Adversarial foreign governments are also to blame for propagating anti-vaccine rhetoric, according to Hotez. “For instance, the Russian government, the Putin government, is spreading anti-vaccine propaganda. The goal of this is to destabilize society and to have caused people to question authority,” he said.
Hotez did not provide any information to support this claim. Russia produces the Sputnik V COVID-19 vaccine, under the auspices of the Russian Direct Investment Fund and The Gamaleya National Center of Epidemiology and Microbiology — an arm of the Russian federal government.
Hotez calls ‘anti-vaccine movement’ a tool of the ‘far-right’
Hotez also used the interview as an opportunity to plug his upcoming book, “The Deadly Rise of Anti-Science: A Scientist’s Warning.” He said the book “describes [the anti-vaccine] ecosystem and its political leanings in detail.”
According to the book’s publisher, Johns Hopkins University Press, Hotez “explains how anti-science became a major societal and lethal force” and how “the anti-vaccine movement became a tool of far-right political figures around the world.”
In 2022, Hotez fiercely criticized looming Congressional hearings into a possible lab-leak origin of COVID-19 and whether the National Institutes of Health (NIH) prematurely discredited the hypothesis, dismissing this as an “outlandish conspiracy.”
However, Hotez’s own 2012 to 2017 NIH grant — totaling $6.1 million — for the development of a SARS vaccine had the aim of responding to any “accidental release from a laboratory,” in addition to a possible zoonotic (or natural) spillover of the virus.
In a June 2023 interview with Robert F. Kennedy Jr., CHD’s chairman on leave, podcaster Joe Rogan offered to donate $100,000 to a charity of Hotez’s choice if he agreed to debate Kennedy.
Hotez — with the support of several legacy news media outlets and the American Medical Association — refused Rogan’s offer. He later claimed on social media that a “couple of anti-vaxers” “stalked” and “taunted” him outside his home after he declined the offer to debate Kennedy.
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
EU Refuses Support to Hungary, Slovakia on Russian Oil Transit Dispute With Ukraine
Sputnik – 25.07.2024
The European Union has denied its support to Hungary and Slovakia after they sought to force Ukraine to restore Russian oil transit to the bloc, the Financial Times reported citing sources familiar with the matter.
EU Trade Commissioner Valdis Dombrovskis told the FT that Brussels would need more time to gather evidence and assess the legal situation. Eleven of the EU nations attending a meeting of trade officials on Wednesday backed his stance and none took the side of Budapest and Bratislava, diplomats told the FT.
Hungarian Foreign Minister Peter Szijjarto said on Monday that Hungary and Slovakia had asked the European Commission to launch consultations with Ukraine after it stopped the transit of oil through the Druzhba pipeline. Szijjarto also said that Hungary would not approve the allocation of 6.5 billion euros ($7 billion) for arms sent to Ukraine through the European Peace Facility until the issue was resolved.
Ukraine’s trade agreement reportedly contains a clause that provides for the possibility of suspending oil transit. An EU diplomat was quoted as saying by FT that disruption in Russian oil supplies would have a “huge impact” on the central European nation.
Last week, Szijjarto said that Ukraine stopped the transit of Lukoil’s oil. The Slovak Economy Ministry confirmed that the country was no longer receiving oil from the Russian oil giant, which was sanctioned by Ukraine. Slovakia’s Slovnaft refinery imports Russian crude from another supplier, but the country is discussing the current situation with Ukraine.
U.S. Government ‘Saddled’ With COVID Vaccine Injury ‘Mess’ — While Vaccine Makers Avoid Liability
By Michael Nevradakis, Ph.D. | The Defender | July 18, 2024
As early as January 2022, National Institutes of Health (NIH) researchers were aware of at least 850 peer-reviewed case reports and/or research articles about COVID-19 vaccine reactions, according to emails obtained by Children’s Health Defense (CHD).
In one email (name and agency redacted), NIH researchers were told the federal government was “saddled” with the “mess” of dealing with those injured by the COVID-19 vaccines, due to the liability shield enjoyed by vaccine manufacturers.
The emails, part of a 309-page batch of documents released to CHD on June 21, originated from a U.S. Food and Drug Administration (FDA) request to NIH researchers for input on a report highlighting several injuries common among people who received the vaccines.
CHD requested the documents via a Freedom of Information Act (FOIA) request to the NIH in November 2022. When the NIH hadn’t responded by April 2023, CHD sued the agency.
In an October 2023 settlement, the NIH agreed to produce up to 7,500 pages of documents at a rate of 300 pages per month.
The batch of documents released in June — which include emails to Peter Marks, M.D., Ph.D., director of the FDA’s Center for Biologics Evaluation and Research — revealed that by fall 2021, key NIH researchers were aware of scientific studies on serious adverse events, including persistent neurological symptoms, following COVID-19 vaccines.
As with prior releases of the NIH documents, June’s tranche also included several emails from vaccine-injured individuals to NIH researchers, seeking help for their symptoms — with one person asking, “Why aren’t you studying vaccine injuries?”
‘Tinnitus … was a freight train in my head for the first four months’
On Jan. 10, 2022, NIH researcher Dr. Avindra Nath was forwarded an email from someone whose name is redacted, with the subject line: “Followup [sic] Jan 4th Meeting” (pages 281-289).
The original email, dated Jan. 9, 2022, was sent to FDA officials including Marks and Dr. Janet Woodcock, principal deputy commissioner of food and drugs, who apparently participated in a meeting on this topic on Jan. 4, 2022.
The Jan. 9, 2022 email included a list of “persistent symptoms following the Covid vaccines” and the names of researchers who were studying these conditions, which included dysautonomia, neuropathy, tinnitus, multisystem inflammatory syndrome (MIS), myocarditis, blood clots and parasthesias.
The email was accompanied by a spreadsheet listing approximately 850 “peer-reviewed case reports/research articles about Covid vaccine reactions.”
Regarding dysautonomia — a nervous system disorder that disrupts automatic bodily functions — the email stated that the condition is “grossly under diagnosed” and “is not diagnosed in ERs or ICUs” but in “autonomic specialty labs.”
The email noted that such labs are less likely than hospitals to file reports with the Vaccine Adverse Event Reporting System (VAERS) and added that there “likely are issues with identifying this syndrome if only looking through VAERS or similarly reported databases.”
As a result, the email suggested “it would be reasonable to approach autonomic specialists / long covid specialists about their observations.”
A 2011 Harvard study found that less than 1% of all adverse events are reported to VAERS.
The Jan. 9, 2022, email also noted unusual trends regarding diagnoses of neuropathy — a set of neurological symptoms that includes numbness and tingling in the hands or feet, and a burning, stabbing or shooting pain in affected areas.
According to the email, “Historically, neuropathy presents in the predominantly male population aged 59+. However as discussed previous [sic], neuropathy in our case is predominantly female, aged 29-40.”
As with dysautonomia, the email noted that neuropathy is “likely to be inadequately reported through the VAERS and BEST [Biologics Effectiveness and Safety] systems because of the circumstances previously mentioned for dysautonomia.”
The Jan. 9, 2022 email also acknowledged that tinnitus was a common post-vaccination injury, noting, “Our findings are that this is not just J&J [the Johnson & Johnson, or Janssen, COVID-19 vaccine] … not by a long shot.”
According to the email, “This symptom is more proportionate to the general neuro symptoms by brand as previously reported in our patient led survey of 500 participants.”
The email’s author also noted that, “in my case yes, I have tinnitus now and it was a freight train in my head for the first four months.”
‘Is it reasonable to dismiss … 20 new symptoms … in a single person post vaccine?’
According to the email, myocarditis and blood clots were already “acknowledged by the FDA and CDC” (Centers for Disease Control and Prevention).
“Every person in our groups that have one of these two conditions, also have accompanying neuro issues like those of us who are not currently acknowledged by the FDA and CDC,” the email said.
The conditions included postural orthostatic tachycardia syndrome (POTS), “brain fog/memory loss, and inflammation (MCAS)” — mast cell activation syndrome.
“Even the perfectly healthy very fit young males with the lasting myocarditis are struggling with the POTS and inflammation/brain fog/memory loss. Makes me suspect that somehow these all are a result of the same mechanism of action,” the email stated.
The Jan. 9, 2022, email also acknowledged parasthesia — a condition that causes a burning, prickling sensation — and MIS, a condition in which numerous organs become inflamed, as concerns.
The email openly questioned why more wasn’t being done to connect these conditions in the vaccinated, to the COVID-19 vaccines themselves, noting that vaccinated people were frequently demonstrating multiple rare symptoms:
“While we understand that correlation does not equal causation, we also find a strong correlation with the change in our blood that mirrors long-haul, and symptomology that mirrors long-haul.
“Because of this, I have to ask what is the process by which Covid PASC [post-acute sequelae of SARS-CoV-2 infection, or long COVID] symptoms have been so readily tied back to Covid, whereas the same symptoms due to the Covid vaccines have not?
“Also, while it may be coincidental to have one or maybe two strange symptoms pop up, is it reasonable to dismiss 10, 15, 20 new symptoms that occur in a single person post vaccine.”
‘Insanely challenging for these people suffering … to walk this path alone’
In the Jan. 10, 2022, email to Nath an NIH researcher wrote, “The FDA has asked once again for us to provide any input from those who have experience with this disease. Very prompt responses and more active engagement on their part lead me to believe they will now examine these problems with some effort.”
The author also asked Nath if he knew researchers “who could fill in the gaps” and asked him if he would “kindly be willing to discuss with Peter Marks?”
“The gov has conveniently absolved the drug companies of any liability, and the federal government is now saddled with the responsibility of figuring out this mess,” the email continued. “I am happy to orchestrate a meeting of the minds with NDR [non-disclosure] agreements if that would get the discussion started in a way that is similar to how previous new diseases have been investigated.”
The email also noted talks with public health officials in Germany and France.
“It has been insanely challenging for these people suffering to have to walk this path alone. They grow more and more desperate by the day. Knowing there is someone, somewhere looking into this makes a big difference for these people to just hang on.”
Even though public health agencies were aware of this information and were discussing vaccine injuries in early 2022, official government advice to the public continued to claim the COVID-19 vaccines were “safe and effective,” including statements by Dr. Anthony Fauci in November 2022.
And in testimony before Congress in February, Marks dismissed the COVID-19 vaccine injury reports filed with VAERS, stating that numerous false reports are submitted to the database — a claim some experts have disputed.
As of today, the CDC continues to recommend the COVID-19 vaccines “for everyone ages 6 months and older, including people who are pregnant, breastfeeding, or might become pregnant in the future.”
NIH researchers aware of vaccine injury studies in fall of 2021
The June 2024 tranche of NIH documents also revealed that, at least as early as fall 2021, researchers with the agency were aware of scientific studies and surveys highlighting serious adverse events following COVID-19 vaccination.
In a Sept. 2, 2021, email (pages 109-121), Farinaz Safavi, M.D., Ph.D., of the NIH Division of Neuroimmunology and Neurovirology was sent the results of the “Covid Vaccine Persistent Symptoms Survey” conducted by React19, a group advocating on behalf of COVID-19 vaccine injury victims.
The version of the survey included in the email was accurate as of Aug. 31, 2021, and contained the results of 382 questionnaires submitted by people “suffering persistent neurological symptoms after receiving the Sars-CoV2 Vaccine in the United States.”
According to those results, 71% of respondents said they had no preexisting health conditions prior to the symptoms they developed following their COVID-19 vaccination, and 94% said they had never previously experienced a reaction to other vaccines.
The most commonly reported symptoms included paresthesia, tinnitus, heart palpitations, tachycardia, chest pain, visual disturbance or loss, muscle twitching, joint pain, muscle aches, brain fog, fatigue and anxiety attacks.
Almost all respondents said these symptoms began less than two weeks following vaccination.
In a Nov. 15, 2021, email (pages 300-305), Nath was sent a scientific paper, “Neurological side effects of SARS-CoV-2 vaccinations,” authored by Austrian researcher Josef Finsterer, M.D., Ph.D.
According to this paper, “The most frequent neurological side effects of SARS-CoV-2 vaccines are headache,” Guillain-Barré syndrome, venous sinus thrombosis and transverse myelitis.
“Safety concerns against SARS-CoV-2 vaccines are backed by an increasing number of studies reporting neurological side effects. … Healthcare professionals, particularly neurologists involved in the management of patients having undergone SARS-CoV-2 vaccinations, should be aware of these side effects and should stay vigilant to recognize them early and treat them adequately,” the paper concluded.
Nath received a review copy of this paper, which has since been published in Acta Neurologica Scandinavica.
And in a May 17, 2021, email (pages 292-299), Nath was sent a preprint of “Sudden Onset of Myelitis after COVID-19 Vaccination: An Under-Recognized Severe Rare Adverse Event,” co-authored by William E. Fitzsimmons, doctor of pharmacy, and Dr. Christopher S. Nance.
According to the preprint, “Myelitis has been reported as a complication of COVID-19 infection. However, it has rarely been reported as a complication of COVID-19 vaccination.”
The paper focused on the example of one of Fitzsimmons’ patients, a 63-year-old previously healthy male who developed myelitis after his second dose of the Moderna COVID-19 vaccine — and treatment that was effective in his case.
Other emails apparently sent by Fitzsimmons highlighted the injuries and the progression of treatment of this 63-year-old man (pages 145-150).
‘A blood clot as a cause of your paralysis would make the most sense’
In an email chain to Nath beginning Sept. 20, 2021, (pages 228-233) with the subject “Paralyzed after J&J Covid Vaccine,” the author (whose name is redacted) said that less than 24 hours following vaccination, the patient “lost bladder control.” He later developed a blood clot and erectile dysfunction, before becoming paralyzed.
In a response that day, Nath told the patient, “The temporal association of the symptoms with the vaccine does make is [sic] suspect, but I do not know of any way how to sort it out.”
In a follow-up email that day, Nath said, “A blood clot as a cause of your paralysis would make the most sense, however, proving cause and effect related to the vaccine in a single patient is virtually impossible.”
In a Dec. 13, 2021, email to Nath (pages 234-236), another vaccine injury victim, who “was healthy prior to vaccination,” described injuries following both doses of the Pfizer-BioNTech COVID-19 vaccine, including paresthesia, tachycardia, severe tinnitus, intractable insomnia and “POTs-like symptoms.”
“I have been diligent and determined in seeking care near and far, but have continued to face skepticism, half-interest, and an inability to know how best to treat,” this person wrote.
And in a series of emails beginning Jan. 24, 2022, (pages 246-247), a “woman who was completely healthy before taking the Pfizer vaccines” told Nath about a series of neurological symptoms and inflammation she experienced following her second dose, in addition to symptoms like tinnitus, insomnia and brain fog.
“Why isn’t the NIH doing research on this?” she asked in a follow-up email on Jan. 25, 2022.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
New German Study Shocks: “Significant Positive Correlation Between Excess Mortality, COVID 19 Vaccinations
100,000 excess German deaths in 2 years… suggests link to COVID vaccines
By P Gosselin | No Tricks Zone | July 21, 2024
To me, it seems a lot of people in Germany have been reporting sick this summer due to a colds and grippe. Normally the flu season starts in the fall. Something has changed.
Moreover, there have been lots of reports out there (mostly gone uncovered by the media) of mysterious excess mortality occurring in many countries. Germany as well has been hit by excess mortality.
Now a new preprint paper by Christof Kuhbandner of the University of Regensberg and Matthias Reitzner of the University of Osnabrück looked at the influence of COVID 19 on mortality in the 16 German states.
The paper found over 100,000 excess deaths occurring in 2021 and 2022. Recall the vaccine was introduced in early 2021.

Source: Differential Increases in_Excess Mortality in the German Federal States During the_COVID-19 Pandemic
In the paper’s conclusion, the authors found a “significant positive correlation between the increase of excess mortality and COVID 19 vaccinations.”
Largest Study of Its Kind Finds Excess Deaths During Pandemic Caused by Public Health Response, Not Virus
By Brenda Baletti, Ph.D. | The Defender | July 19, 2024
A study released today of excess mortality in 125 countries during the COVID-19 pandemic found the major causes of death globally stemmed from public health establishment’s response, including mandates and lockdowns that caused severe stress, harmful medical interventions and the COVID-19 vaccines.
“We conclude that nothing special would have occurred in terms of mortality had a pandemic not been declared and had the declaration not been acted upon,” the authors of the study wrote.
Researchers from the Canadian nonprofit Correlation Research in the Public Interest and the University of Quebec at Trois-Rivières analyzed excess all-cause mortality data prior to and during the COVID-19 pandemic, beginning with the March 11, 2020, World Health Organization (WHO) pandemic declaration and ending on May 5, 2023, when the WHO declared the pandemic over.
The results, presented in a detailed 521-page analysis, establish baseline all-cause mortality rates across 125 countries and use those to determine the variations in excess deaths during the pandemic.
The researchers also used the baseline rates to investigate how the individual country variations in excess death rates correlated to different pandemic-related interventions, including vaccination and booster campaigns.
Not all of the results on a country-by-country basis were the same. For example, in some countries, mortality spikes occurred before the vaccines were rolled out, while in other places, the mortality spikes tracked closely with vaccine or booster campaigns.
In some places, excess mortality rates returned to baseline or close to baseline in 2022, while in others, the rates persisted well into 2023. Denis Rancourt, Ph.D., lead author of the study, told The Defender the disparities result from the complex nature of pandemic measures — and the data — in different areas.
Once Rancourt’s team was able to establish the baseline and excess mortality data for each place, they clustered and examined the data through different filters to interpret it, and drew several conclusions.
Data ‘incompatible with a pandemic viral respiratory disease as a primary cause of death’
The researchers established that there was significant excess mortality worldwide between March 11, 2020, and May 5, 2023.
Overall excess mortality during the three years in the 93 countries with sufficient data to make an estimate is approximately 0.392% of the 2021 population — or approximately 30.9 million excess deaths from all causes.
The conventional explanation for the excess mortality during the COVID-19 pandemic, Rancourt said, is that the SARS-CoV-2 virus caused virtually all deaths — and there would have been even more deaths if there hadn’t been a vaccine.
The variations in excess all-cause mortality rates across space and time, the authors wrote, “allow us to conclude that the Covid-period (2020-2023) excess all-cause mortality in the world is incompatible with a pandemic viral respiratory disease as a primary cause of death.”
They said the theory that the virus caused the deaths is propped up by mass virus-testing campaigns that should be abandoned.
‘Idea that vaccines saved lives is ridiculous’
Rancourt and his team cited several factors they believe disprove the theory that the virus caused a spike in all-cause mortality.
For example, they wrote that excess mortality surged almost simultaneously across several continents when a pandemic was declared, while there were no comparable surges in areas that had not yet declared a pandemic.
This suggests that pandemic interventions like lockdowns, which were implemented synchronously across many countries, likely caused the surges.
The researchers also pointed out the significant variation in mortality rates during the pandemic in all time periods, even across different political jurisdictions directly adjacent to each other. If the virus caused the deaths, it would follow that the infection fatality rate would be the same, or at least similar across political boundaries.
The researchers also found a lot of variability in death rates within countries over time, which also would not be an expected outcome if those deaths were caused by a pathogen.
Rancourt said they found “the idea that the vaccine saved lives is ridiculous,” and based on flawed modeling as he and colleagues also showed in a previous paper.
Here again, they found no systematic or statistically significant trends showing that vaccination campaigns in 2020 and 2021 reduced all-cause mortality.
Instead, they found that in many places, there was no excess mortality until the vaccines were rolled out, and most countries showed temporal associations between vaccine rollouts and increases in all-cause mortality.
Medical interventions — including denial of treatment — caused premature deaths
Rancourt said the excess deaths his team identified are strongly associated with the combination of two major factors — the proportion of elderly in a country’s population and the number of people living in poverty. Both factors increased peoples’ vulnerability to “sudden and profound structural societal changes” and “medical assaults.”
While the proximal cause of death may be classified on death certificates as a respiratory condition or infection, the researchers noted, they argue the true primary causes of death are actually biological stress, non-COVID-19-vaccine medical interventions and the COVID-19 vaccination rollouts.
The study provides an overview of plausible mechanisms for this hypothesis, including research showing that some people experienced severe biological stress from measures like mandates and lockdowns.
“If you structurally change the society by preventing people from moving, breathing, working, having their lives, having to stay at home, lock them in. If you do all these incredibly huge changes, structural changes in society, that is going to induce biological stress,” Rancourt told The Defender.
“There’s very compelling scientific evidence that biological stress is a massive killer,” he added.
Rancourt also pointed out that the stress of lockdowns affected poor people quite differently than it did people who could easily work from home, have food delivered and live relatively comfortably.
The authors also pointed to extensive evidence showing that medical interventions — including denial of treatment — caused premature deaths.
Such interventions included but were not limited to the denial of antibiotics and ivermectin against bacterial pneumonia, the systematic use of mechanical ventilators, experimental treatment protocols, new palliative medications and overdoses, isolation of vulnerable people and encouraged voluntary or involuntary suicide.
The March-April 2020 COVID-19 peak they identified in several countries is difficult to explain without such medical interventions, they wrote.
17 million excess deaths tied to COVID vaccines
Finally, the researchers projected that 17 million of the excess deaths they identified were associated with the COVID-19 vaccines, confirming the findings of their previous research on a smaller sample of countries.
Those vaccine-related estimations were based on analyses of places that had large spikes immediately following vaccination or booster campaigns and also by examining the numbers of vaccine doses and their relation to deaths over time.
Thirty percent of the countries they analyzed had no excess deaths until either the vaccine rollouts or the booster campaigns. And there were significant correlations between COVID-19 vaccine rollouts and peaks or increases in excess all-cause mortality. Ninety-seven percent of countries showed a late-2021 or early-2022 peak in excess all-cause mortality temporally associated with booster rollouts.
It is highly unlikely, the researchers wrote, that the vaccine-mortality associations are coincidental.
Rancourt noticed that people critical of this idea point to the fact that in some places, there are sometimes campaigns or booster campaigns that aren’t associated with spikes in excess mortality.
However, he said vaccination campaigns don’t always lead to such spikes because vaccination was not related to death in the same way in every situation. Vulnerability factors like the age of those vaccinated, the health of the population and other sociological factors related to stressors on the immune system change how they are affected by vaccine toxicity or the vaccines’ effects on the immune system.
Based on their analysis and interpretations, they concluded, “We are compelled to state that the public health establishment and its agents fundamentally caused all the excess mortality in the Covid period.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Ministers Were Informed Of mRNA Lies During Mandates, Cardiologist Reveals
Dr Aseem Malhotra had a direct line of communication to the Health Secretary

By JJ Starky | The Stark Naked Brief | July 19, 2024
We’ve had another mainstream breakthrough.
Yesterday, Dr. Aseem Malhotra appeared on TalkTV to discuss the UK government’s Covid response in light of Baroness Hallett’s report on the first module of the Covid Inquiry.
Commentators were surprised. Most predicted that the Covid Inquiry chair’s report would echo sentiments seen during proceedings, suggesting that lockdowns, despite all credible evidence, were the only viable solutions for dealing with Covid.
So when Hallett’s team concluded that “the imposition of a lockdown should be a measure of last resort… indeed, there are those who would argue that a lockdown should never be imposed,” it almost seemed strange.
During the interview, much like his January 2023 appearance on the BBC where he pivoted from discussing statins to linking Covid vaccines to cardiovascular issues, Malhotra shifted the focus to vaccines.
He covered a lot of detail in quick succession. He argued that the term “vaccine” used for mRNA products is misleading, as they are better described as gene technologies. He cited peer-reviewed reanalysis of Moderna and Pfizer’s clinical trials, which showed an adverse event rate closer to 1-in-800, a figure that outweighed Covid hospitalisation risk. He also mentioned that Israel saw a 25% increase in cardiac events among people aged 16-39 during the vaccine rollout.
But the standout moment came when Malhotra discussed his involvement in a court case in Finland concerning an entrepreneur who was denied entry to a café because he was unvaccinated.
Malhotra revealed that he witnessed a World Health Organisation (WHO) chief scientist testify under oath that by December 2021, the mRNA vaccine offered zero protection against Covid. He then disclosed that he had texted Sajid Javid, the UK Secretary of State for Health and Social Care, informing him of this testimony, but Javid effectively ignored it.

Former UK Secretary State for Health and Social Care Sajid Javid
It has been difficult to gauge what certain officials knew at what time. However, now we have an indication that some were categorically made aware that their policies were illogical and at direct odds with the evidence-base.
Press releases show that Javid’s department finally revoked the Covid vaccine mandate for health and social care staff on March 15, 2022, months after Malhotra made contact.
In November 2021, a survey of industry leaders estimated that up to 20,000 carers had already quit or been sacked over mandatory jabs. Given the mandate carried on to March the following year, that could be a vast underestimate.
Malhotra, who once advocated for everyone to receive the vaccines before his father reportedly passed away from them, notably said, “This is the biggest corporate crime committed by the drug the industry.”
TalkTV did not post the interview on YouTube as the platform continues to issue strikes to channels discussing the topic. So here it is in full.
Summary of Hallett’s Report on the Covid Inquiry:

- Ad Hoc Intervention: Epidemiologist Professor Mark Woolhouse described lockdown as an ad hoc intervention with no prior planning, guidelines, or clear expectations.
- Lack of Scrutiny on Consequences: The novelty of the lockdown approach meant there was no time to scrutinise its potential side effects, leading to ill-prepared policies with unknown consequences.
- Significant Economic Impact: The report highlights the 25% drop in GDP between February and April 2020 due to lockdowns, representing a major gap in the UK’s assessment of pandemic risk.
- Missing Topics: The report does not discuss the UK government’s evidence that the Test and Trace system had minimal impact on reducing Covid infections despite its high cost.
- Balancing Factors in Health Emergencies: The report emphasises the need for a balanced approach in health emergencies, considering economic impact, social wellbeing, and effects on education, as advocated by former chief medical officer Sally Davies.
- Exclusion of Certain Testimonies: Testimonies from Chief Medical Officer Chris Whitty are notably absent, indicating a potential shift from previously dominant perspectives during the pandemic.
- Real Story of the Report: The report suggests that the UK was not prepared for the “wrong pandemic”, but rather that it resorted to an unprecedented policy without a proper evidence base or risk assessment. It advocates that lockdowns should be a measure of last resort, and perhaps never used at all.
EU Commission Hid Vaccine Contract Details From Public, Court Rules
By John-Michael Dumais | The Defender | July 17, 2024
The European Union‘s (EU) top court today ruled that the European Commission’s decision to heavily redact key portions of COVID-19 vaccine contracts with pharmaceutical companies during the pandemic violated the commission’s transparency obligations.
The European Court of Justice found that the commission failed to provide sufficient public access to COVID-19 vaccine purchase agreements, in a ruling that could deal a blow to Commission President Ursula von der Leyen on the eve of her re-election bid, according to The Associated Press (AP).
The ruling came in response to legal challenges brought by EU lawmakers and private citizens seeking fuller disclosure of the multibillion-euro vaccine deals.
It highlights ongoing concerns about the secrecy surrounding the EU’s vaccine procurement process, a contentious issue since the early days of the pandemic.
“The Commission did not give the public wide enough access to the contracts for the purchase of COVID-19 vaccines,” the court said in its judgment, pointing to several areas where the executive body fell short in being sufficiently transparent.
In response to the ruling, the commission wrote, “The Commission needed to strike a difficult balance between the right of the public, including MEPs [Members of the European Parliament], to information, and the legal requirements emanating from the COVID-19 contracts themselves, which could result in claims for damages at the cost of taxpayers’ money.”
Green MEP Tilly Metz, one of the deputies who submitted the original request, said, “This ruling is significant for the future, as the EU Commission is expected to undertake more joint procurements in areas like health and potentially defence,” Euractiv reported.
“The new European Commission will have to adapt their handling of access to documents requests to be in line with today’s ruling,” Metz said.
However, Dutch attorney Meike Terhorst told The Defender that the court ruling is not the victory it seems. She argued that the EU court has given the commission a “giant loophole” to keep parts of the contracts secret “to protect ‘business interests.’”
“It is not possible to both protect public health and full transparency and at the same time protect the business interests of the supplier,” Terhorst said. “We, the public, will not get the access to the information we need. The cat and mouse play continues.”
The commission, which has two months to appeal the decision, said it would “carefully study the Court’s judgments and their implications” and that it “reserves its legal options.”
Scale and speed of purchases unprecedented
In 2020 and 2021, von der Leyen negotiated purchase agreements for COVID-19 vaccines with several pharmaceutical companies, including Pfizer, Moderna and AstraZeneca, according to the AP.
EU member states mandated the European Commission organize the joint procurement of vaccines and lead negotiations with manufacturers.
The scale and speed of these purchases were unprecedented. According to the court, approximately 2.7 billion euros ($2.95 billion) was quickly mobilized to place firm orders for more than 1 billion doses of vaccines. This joint procurement approach allowed for the rapid acquisition of vaccines for all 27 EU member states.
Initially, von der Leyen received praise for her leadership during the COVID-19 crisis, particularly for her role in securing collective vaccine access for EU citizens. However, the spotlight quickly shifted to concerns about the negotiations’ lack of transparency.
In 2021, several members of the European Parliament requested full details of the agreements. The commission, citing confidentiality reasons, agreed to provide only partial access to certain contracts and documents, which were placed online in redacted versions.
The commission also refused to disclose how much it paid for the billions of doses it secured.
Concerns over secret deals with Pfizer
Pfizer CEO Albert Bourla twice in 2022 refused to testify before the European Parliament’s special committee on COVID-19. Bourla was expected to face tough questions about secretive vaccine deals and negotiations between Pfizer and the European Commission.
Of particular interest were text messages between Bourla and von der Leyen that preceded a multibillion-euro vaccine contract. In January 2023, The New York Times sued the European Commission over its failure to release the messages.
That suit followed a January 2022 inquiry by the EU ombudsman charging the commission with maladministration over its handling of a previous request for the messages.
In June, a Belgian court took up the issue of the secret negotiations between Bourla and von der Leyen, with a former lobbyist for the EU Parliament claiming “destruction of public documents” and alleging von der Leyen violated the commission’s code of conduct.
Commission officials argued the messages didn’t contain any important information and have thus far refused to provide them, according to the AP.
European Public Prosecutor’s Office (EPPO) in 2022 opened an investigation into the acquisition of COVID-19 vaccines in the EU during the pandemic. This investigation stems from a criminal complaint filed by an individual, with the governments of Hungary and Poland later joining the lawsuit, euronews reported. EPPO adjourned the case until December.
Implications for the European Commission and von der Leyen
The court’s ruling comes at a critical time for von der Leyen, just one day before the European Parliament is set to vote on her reappointment as commission president.
Von der Leyen had previously won backing from a majority of EU leaders in June. To secure her position, she now needs to garner support from at least 361 MEPs in the 720-seat European Parliament, WIONews reported.
This ruling presents a dilemma for the Greens, who initiated the legal challenge against the commission’s redactions. In recent days, von der Leyen has been courting the Greens to shore up support for her nomination ahead of the vote.
During a press conference in Strasbourg on Wednesday, Manon Aubry, a French MEP from the Left group, expressed strong concerns about the European Commission’s “lack of transparency.”
On the heels of the EU court ruling, German MEP Christine Anderson today said she would call for the removal of von der Leyen and the continuation of the criminal investigation of her actions.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Australians in shock over former President of AMA Prof. Kerryn Phelps’ leaked audio on vaccine injuries
PharmaFiles by Aussie17 | July 9, 2024
Australians have been left in a state of shock after more leaked audio emerged from the censored 7News segment “After COVID,” which I wrote about here and here. This time, we have the full, alarming statements by former President of the Australian Medical Association, the largest professional body for doctors in Australia, Professor Kerryn Phelps, in response to host Michael Usher when he asked, “Is there anything to learn from people who’ve had side effects that both of you are describing in detail?”
In the recording, Phelps exposes the disturbing rise in mRNA vaccine side effects and the gross negligence by both the government and pharmaceutical companies in addressing these issues.
“I mean I’ve never seen so many young people having cardiac MRIs in my entire career. There are people who’ve had heart damage, myocarditis, they’ve had heart problems, gastrointestinal problems, dysautonomia.” – Professor Kerryn Phelps
The conversation, hosted by Michael Usher on “Spotlight,” is now available on YouTube. The official version, unfortunately, removed many “controversial” remarks that 7News doesn’t want the public to hear, exposing the shocking incompetence and indifference displayed by the authorities. This blatant censorship is nothing short of an insult to the public’s right to know the truth.
According to Phelps, this dismissive attitude points to an acute lack of medical curiosity and engagement when investigating adverse reactions. The Therapeutic Goods Administration (TGA) takes in reports—estimated at 144,000 adverse reactions and 22,000 serious adverse reactions(deaths, permanent disabilities, hospitalizations, miscarriages, and other life-threatening conditions.) — but this figure significantly underrepresents the actual problem, as Phelps said it is only “a drop in the ocean”.
Just to emphasize again, based on the population of Australia, which is approximately 25.7 million, the 144,000 adverse reaction reports represent approximately 0.56% of the population, equating to about 1 in every 179 people. When considering the 22,000 serious adverse reactions, this represents approximately 0.086% of the population, or about 1 in every 1,168 people. This is also roughly in line with Fraiman et al., who found at least 1 in 800 serious adverse reactions.
This is extremely high. For context, the 1976 swine flu vaccine recall in the United States was initiated after it was linked to Guillain-Barré syndrome, a rare neurological disorder. The vaccine was associated with approximately 1 case of Guillain-Barré syndrome per 100,000 vaccinations. This event led to the suspension of the vaccine program. The current figures for adverse reactions to the COVID-19 vaccines far exceed the threshold that prompted the swine flu vaccine recall.
Furthermore, Phelps critiques the TGA’s management of adverse reactions. “The TGA never gets back to anybody. They compile this data but they don’t actually follow up. They don’t know how long these vaccine injuries have gone on for. They don’t go back to people and say, you know, ‘Are you still suffering? What’s happening with you now?'” she reveals.
For many Australians, this isn’t just a “conspiracy theory” anymore. Hearing these concerns from the former Australian Medical Association President, Professor Kerryn Phelps, makes it clear that this issue is real. It’s time for real action and support for those affected.
COVID-19 Modified mRNA “Vaccines”: Lessons Learned from Clinical Trials, Mass Vaccination, and the Bio-Pharmaceutical Complex, Part 1
Mead et al Deliver Counter-Punch after Springer Nature Unethical Retraction of High-Impact Paper
By Peter A. McCullough, MD, MPH | Courageous Discourse™ | July 8, 2024
Every major development in medicine evolves over years with peer-reviewed manuscripts and published correspondence along the lines of arguments and scientific discourse. Never had we seen a new technology and mass mandated line of medical products be introduced with no allowance for proper scientific discourse. Not until mRNA.

Mead and co-workers found themselves at the center of a controversy when Springer Nature CUREUS Journal of Biomedical Sciences retracted their paper calling for global market withdrawal of mRNA vaccines. The retraction violated the COPE (Committee on Publication Ethics Guidelines) for retraction and became a news story garnering even more attention. Other papers continued to cite Mead creating a stinging reverberation for Springer who was hoping to silence the paper.
Now epidemiologist M. Nathaniel Mead and six co-authors have punched back with the manuscript divided into two parts for a greater depth of data and analysis on the safety and theoretical efficacy of modified mRNA COVID-19 vaccines. In Part I, Mead discloses censorship of the first paper by the Bio-Pharmaceutical Complex, a working syndicate that is hell-bent on suppressing any scientific information on COVID-19 side effects.
You may ask what should have occurred? Springer Nature should have never retracted the paper. Rather letters to the editor and responses to the letters from authors should have been published as proper scientific interchange. The new normal is now unethical retraction, massive publicity, and republication with greater amplification of the message—precisely what the Bio-Pharmaceutical Complex is trying to squelch.
Mead MN, Seneff S, Wolfinger R, Rose J, Denhaerynck K, Kirsch S, McCullough PA. COVID-19 mRNA Vaccines: Lessons Learned from the Registrational Trials and Global Vaccination Campaign. Cureus. 2024 Jan 24;16(1):e52876. doi: 10.7759/cureus.52876. Retraction in: Cureus. 2024 Feb 26;16(2):r137. doi: 10.7759/cureus.r137. PMID: 38274635; PMCID: PMC10810638.
COVID-19 Modified mRNA “Vaccines” Part 1: Lessons Learned from Clinical Trials, Mass Vaccination, and the Bio-Pharmaceutical Complex. (2024). International Journal of Vaccine Theory, Practice, and Research , 3(1), 1112-1178. https://doi.org/10.56098/fdrasy50
British Columbia Royal College of Physicians and Surgeons Defeated on Judicial Notice
Case of Dr. Charles Hoffe Kills Deferral to Government Offices as Agents of “Truth”
Courageous Discourse™ | July 6, 2024
This was written by Canadian attorney Lee Turner after discussion with Dr. McCullough.
Dr. Charles Hoffe is a family and (former) emergency room physician in British Columbia who is the subject of disciplinary proceedings before the College of Physicians and Surgeons of British Columbia for making public statements about SARS-CoV-2, the safety and efficacy of the COVID-19 vaccines, and other alternative treatments including ivermectin. Hoffe has successfully defeated an application made by the College seeking judicial notice of the truth of facts alleged by the College concerning these issues. In its efforts to discipline the physician, the College has alleged that the statements made by the physician are misleading, incorrect or inflammatory and constitute professional misconduct. The College asked the discipline panel to take judicial notice of the following facts and thereby prevent the doctor from presenting any contrary evidence in his defence:
- The Covid virus kills or causes other serious effects;
- The virus does not discriminate;
- Vaccines work;
- Vaccines are generally safe and have a low risk of harmful effects, especially in children;
- Infection and transmission of the COVID-19 virus is less likely to occur among fully vaccinated individuals than for those who are unvaccinated; vaccines do not prevent infection, reinfection or transmission, but they reduce the severity of symptoms and the risk of bad outcomes;
- Health Canada has approved COVID vaccines, and regulatory approval is a strong indicator of safety and effectiveness;
- Health Canada has not approved ivermectin to treat COVID-19; and
- Health Canada advises that Canadians should not consume the veterinary version of ivermectin.
In its June 29, 2024 decision, the disciplinary panel of the College of Physicians and Surgeons of British Columbia declined to take judicial notice of items 2-5, did take judicial notice of items 7-8 (the straightforward ivermectin claims), and took judicial notice of a revised version of items 1 and 6.
The panel was prepared to take judicial notice of item 1 that reads: “COVID-19 can kill or cause other serious effects”.
The College explained their rationale for taking judicial notice of a revised version of item 1 by referencing evidence presented by the doctor in his defence that included the following:
- risk of severe disease and death from COVID-19 is extremely skewed to those above 70 years of age, especially those with multiple comorbidities. The average age of persons that died from COVID-19 in Canada was approximately 84 years old;
- very low proportion of COVID-19 related deaths in Canada occurred in those under 50 years of age-the data shows very high (although not 100%) survival rates for those under 70;
- average rate of lethality from COVID-19 for Canadians is much lower than estimates given by public health officials; and
- reported hospitalizations and deaths from COVID-19 have been over-counted, because many hospitalizations and deaths “with, and not from” COVID-19 were wrongly attributed to COVID-19
With respect to item 6, the panel endorsed findings of an earlier provincial Court of Appeal decision that held the safety and efficacy of any drug is always relative and as a rule the safety and efficacy of a pharmaceutical product cannot be discussed in such blunt fashion as to say that it “is” or “is not” safe and effective. The panel held that the issues raised in the citation should be determined based upon the evidence that is tested through cross-examination rather than by taking judicial notice of one party’s assertion of the facts, and in this case, based upon statements made by public health officials or public health agencies. The panel held that it was prepared to take judicial notice of the fact that Health Canada had approved the COVID – 19 vaccines, but declined to take judicial notice that Health Canada’s approval was a strong indicator of safety and effectiveness.
This decision on the issue of judicial notice, is consistent with the June 28, 2024 decision of the US Supreme Court in Loper Bright Enterprises et al. v. Raimondo Secretary of Commerce et. al. which overturned the landmark 1984 decision in Chevron v. Natural Resources Defense Council. The Chevron decision had given rise to what is commonly referred to as the Chevron deference doctrine. Under this doctrine, federal agencies had the power to interpret a law that they administer when that law is vaguely written, and courts were required to defer to the agency’s interpretation of a statute. In Loper, the US Supreme Court rejected the Chevron deference doctrine calling it “fundamentally misguided.” They said court should rely on their own interpretation of ambiguous laws rather than having to accept the agency’s interpretation. Commentators have suggested that the Chevron deference doctrine gave the powerful – the people who control the agencies like the FDA, CDC and FCC – a significant advantage in court making them essentially the ultimate decision-makers in interpreting ambiguous laws. Commentators have pointed out that many of these agencies are captive agencies with close ties, including financial ties, to the industries that they are charged with regulating and therefore they lack objectivity with respect to those industries. The ruling in Labor means that federal judges now have more authority to interpret these laws. The decision by the British Columbia Disciplinary Panel of the College of Physicians of Surgeons of British Columbia prevents regulatory bodies from saying “it is so because we say it is so”. They have to prove the facts they assert and those who disagree will be allowed to challenge those facts and present contrary evidence.
The case against Dr. Hoffe is far from over. This development is significant in that a government agency cannot make the rules, interpret them, and claim they hold the truth on an evolving scientific or medical issue.
Lee C. Turner, Partner, Doak Sherriff Lawyers, LLC, Kelowna BC V1Y 2A9
(Professional Law Corporation)
How Pfizer’s Original mRNA Trial Hid a 66% Increase in Cardiovascular Death Rate Amongst the Vaccinated
PharmaFiles by Aussie17 | June 29, 2024
Thanks to Dr. Clare Craig for highlighting this clip from Dr. David White on Twitter/X today. It’s important for people to understand how Pfizer manipulated the categorization of deaths in their original trial, which led to politicians using the “safe and effective” narrative. Everyone should carefully watch this, as it not only raises concerns about Pfizer or Moderna’s mRNA vaccines but also highlights the broader corruption of medical information that prioritizes profit over safety.
Dr. David White, a retired general practitioner from the UK, masterfully breaks down the concerning aspects of the Pfizer BNT162b2 trial. He walks us through the intricate details and demonstrates how Pfizer may have “adjusted” the categorization of participant deaths to make it appear as though there were fewer cardiovascular deaths in the vaccine group than there actually were.
To recap, a total of 29 deaths from all causes were reported in the trial within six months, as published in the New England Journal of Medicine. The original trial showed that deaths were about 7% higher in the vaccine group, with 15 deaths, compared to 14 deaths in the placebo group. However, many “fact-checkers” and pharma shills “scientists” claim that this difference is not statistically significant.
This is intriguing because, according to a Lancet paper, there were 44,000 more deaths in England in 2022, driven by a sharp increase in cardiovascular deaths among the middle-aged, which rose by 33%. He wonders if cardiovascular deaths in the trial’s vaccine group were also 33% higher. This question is important because it seeks to determine if the higher death rate in the vaccinated group is related to the rise in cardiovascular deaths seen in the general population.
He walks us through four mysterious “causes of deaths” categorized in the paper:
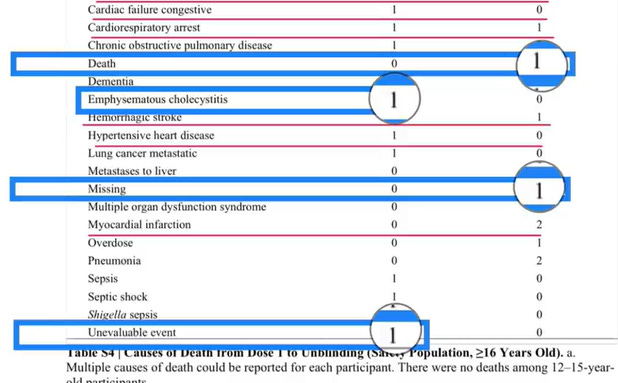
- An “Unevaluable Event” on a vaccinated death, which was found to be a sudden cardiac death confirmed via autopsy.
- A “Missing” entry categorized as a “placebo” death, which was later found to be a “vaccinated” death.
- “Emphysematous Cholecystitis,” which is a cardiovascular death but Pfizer said let’s put something that sounds really complicated and hope nobody knows its a cardiovascular death.
- “Death” for participant #10841470. First of all categorizing a “cause of death” as “Death”, are you kidding? Anyway this participant died after taking a Moderna mRNA vaccine, but was categorized as a placebo death. I wrote about this issue here.
In conclusion, after recategorizing the deaths, all-cause deaths were 15% higher in the vaccine group. There were 10 cardiovascular deaths in the vaccine group and six in the placebo group, indicating that cardiovascular deaths were 66% higher in the vaccine group.
Dr. White highlights that these figures, particularly the increased all-cause mortality in the vaccine group, clearly point to safety signals. He stresses that informed consent is a fundamental ethical principle in medicine, necessitating the open discussion of such safety concerns. It is crucial to ensure that participants are fully informed about the potential risks associated with the vaccine to maintain trust and transparency within the medical community.
Watch full video:
Featured Video

Rewriting the risk? Inside the government’s vaccine safety messaging
or go to
Aletho News Archives – Video-Images
Book Review
“Davos Can Really Replace the UN”
Inside the book that maps the architecture behind global governance — from the Epstein files to the Pact for the Future
Lies are Unbekoming | April 1, 2026
On June 13, 2019, the United Nations and the World Economic Forum signed a partnership deal to “accelerate the implementation of the 2030 Agenda for Sustainable Development.” That same evening, WEF president Börge Brende — Norway’s former Foreign Minister — had dinner with Jeffrey Epstein at Epstein’s Manhattan townhouse. The Epstein files, released January 2026, contain an exchange between the two from the previous year. Epstein to Brende: “Davos can really replace the UN. C21, cyber, crypto . genetics… intl coordination.” Brende back to Epstein: “Exactly — we need a new global architecture. World Economic Forum (Davos) is uniquely positioned — public private.”
The next day, the UN General Assembly adopted the framework for restructuring global governance.
That sequence — the partnership signing, the Epstein dinner, the candid admission about replacing the UN with a public-private architecture, and then the formal adoption — opens Jacob Nordangård’s The Digital World Brain. Pages two and three. Footnoted to the UN resolution number, the Epstein files, and the General Assembly record.
I keep coming back to it because it captures what this book does that almost nothing else in the independent research space manages. I’ve followed Jacob’s work for years now and interviewed him about his research. Each book peels back another layer of the same institutional architecture, and each time I think he’s reached the limit of what can be documented, the next one goes further. Nordangård doesn’t speculate. He doesn’t editorialize much. He lays institutional actions next to each other in chronological order and lets the pattern announce itself. … continue
Blog Roll
 Aletho News
Aletho News- Barak Ravid Launders Deception To Allow Trump To Back Off Of His Power Plant Threat – Again
- REWRITING THE RISK? INSIDE THE GOVERNMENT’S VACCINE SAFETY MESSAGING
- “Davos Can Really Replace the UN”
- NIAID/NIH and USDA Fund Bioengineered Chimeric Influenza Viruses Built Using Pandemic H1N1 Components: Journal ‘Science Advances’
- Hezbollah hits Israeli warship off Lebanon’s coast, sets it aflame
- Iran slams US strikes on B1 bridge, Mahshahr petrochemical plants as ‘blatant acts of state terrorism’
- In letter to UN chief, Araghchi warns of dire consequences of US-Israeli attacks on Iran’s nuclear facilities
- Why the CIA conspiracy to invade Iran with Kurdish militias failed
- Why Are Upbeat US Claims About Mission to Rescue Pilot ‘Highly Questionable’?
- Aircraft destroyed during US ‘rescue’ of downed F-15 pilot cost more than $100 million each
- If Americans Knew
- In Iran, Israel-US take aim at “reason, research, and freedom of thought” – Daily Update
- US loses planes over Iran, Israel downgrades Lebanon war goals – Daily Update
- Israel Is Blocking Palestinians from Easter at Church Where Jesus Resurrected
- Plot to assassinate Palestinian activist follows harassment campaign promoted by Zionist groups and elected officials
- Prominent New York synagogue hosts presentation on why U.S. Jews should support the ethnic cleansing of Gaza
- Tapper vs. Piker: Is the CNN Anchor Auditioning for David Ellison?
- Shouldn’t Democrats Be Able to Condemn Genocide?
- Israel-US kill negotiators, destroy civilian structures, but Iran’s military capabilities still largely intact – Daily Update
- ‘War crime’: Global condemnation as Israeli ministers celebrate death penalty law targeting Palestinian prisoners
- 7 Ways Israel Is Turning Lebanon Into Gaza
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
