WHO Official Admits Vaccine Passports May Have Been a Scam
By Paul D. Thacker | The DisInformation Chronicle | April 12, 2024
The World Health Organization’s Dr. Hanna Nohynek testified in court that she advised her government that vaccine passports were not needed but was ignored, despite explaining that the COVID vaccines did not stop virus transmission and the passports gave a false sense of security. The stunning revelations came to light in a Helsinki courtroom where Finnish citizen Mika Vauhkala is suing after he was denied entry to a café for not having a vaccine passport.
Dr. Nohynek is chief physician at the Finnish Institute for Health and Welfare and serves as the WHO’s chair of Strategic Group of Experts on immunization. Testifying yesterday, she stated that the Finnish Institute for Health knew by the summer of 2021 that the COVID-19 vaccines did not stop virus transmission
During that same 2021 time period, the WHO said it was working to “create an international trusted framework” for safe travel while EU members states began rolling out COVID passports. The EU Digital COVID Certificate Regulation passed in July 2021 and more than 2.3 billion certificates were later issued. Visitors to France were banned if they did not have a valid vaccine passport which citizens had to carry to buy food at stores or to use public transport.
But Dr. Nohynek testified yesterday that her institute advised the Finnish government in late 2021 that COVID passports no longer made sense, yet certificates continued to be required. Finnish journalist Ike Novikoff reported the news yesterday after leaving the Helsinki courtroom where Dr. Nohynek spoke.

Dr. Nohynek’s admission that the government ignored scientific advice to terminate vaccine passports proved shocking as she is widely embraced in global medical circles. Besides chairing the WHO’s strategic advisory group on immunizations, Dr. Nohynek is one of Finland’s top vaccine advisors and serves on the boards of Vaccines Together and the International Vaccine Institute.
The EU’s digital COVID-19 certification helped establish the WHO Global Digital Health Certification Network in July 2023. “By using European best practices we contribute to digital health standards and interoperability globally—to the benefit of those most in need,” stated one EU official.
Finnish citizen Mika Vauhkala created a website discussing his case against Finland’s government where he writes that he launched his lawsuit “to defend basic rights” after he was denied breakfast in December 2021 at a Helsinki café because he did not have a COVID passport even though he was healthy. “The constitution of Finland guarantees that any citizen should not be discriminated against based on health conditions among other things,” Vauhkala states on his website.
Vauhkala’s lawsuit continued today in Helsinki district court where British cardiologist Dr. Aseem Malhotra will testify that, during the COVID pandemic, some authorities and medical professionals supported unethical, coercive, and misinformed policies such as vaccine mandates and vaccine passports, which undermined informed patient consent and evidence-based medical practice.
You can read Dr. Malhotra’s testimony here.
CDC Demonstrates Failure of Public Health Management of the COVID-19 Pandemic
BY DR. HARVEY RISCH | APRIL 1, 2024
In so many words—and data—CDC has quietly admitted that all of the indignities of the Covid-19 pandemic management have failed: the masks, the distancing, the lockdowns, the closures, especially the vaccines, all of it failed to control the pandemic. It’s not like we didn’t know that all this was going to fail, because we said so as events unfolded early on in 2020, that the public health management of this respiratory virus was almost completely opposite to principles that had been well established through the influenza period, in 2006. The spread of a new virus with replication factor R0 of about 3, with more than one million cases across the country by April 2020, with no potentially virus-sterilizing vaccine in sight for at least several months, almost certainly made this infection eventually endemic and universal.
Covid-19 starts as an annoying, intense, uncomfortable flu-like illness, and for most people, ends uneventfully two-three weeks later. Thus, management of the Covid-19 pandemic should not have relied upon counts of cases or infections, but on numbers of deaths, numbers of people hospitalized or with serious long-term outcomes of the infection, and of serious health, economic and psychological damages caused by the actions and policies made in response to the pandemic, in that order of decreasing priorities. Even though numbers of Covid cases correlate with these severe manifestations, that is not a justification for case numbers to be used as the actionable measure, because Covid-19 infection mortality is estimated to range below 0.1% in the mean across all ages, and post-infection immunity provides a public good in protecting people from severe reinfection outcomes for the great majority who do not get serious “long-Covid” on first infection.
Nevertheless, once the Covid-19 vaccines were rolled out, with a new large wave of the delta strain spreading across the US in July-August 2021 even after eight months of the vaccines taken by half of Americans, instead of admitting policy error that the Covid vaccines do not much control virus spread, our public health administration doubled down, attempting then to compel vaccination on as many more people as could be threatened by mandates. That didn’t work out too well as seen when the large Omicron wave hit the country during December 2021-January 2022 in spite of some 10% more of the population getting vaccinated from September through December of 2021.
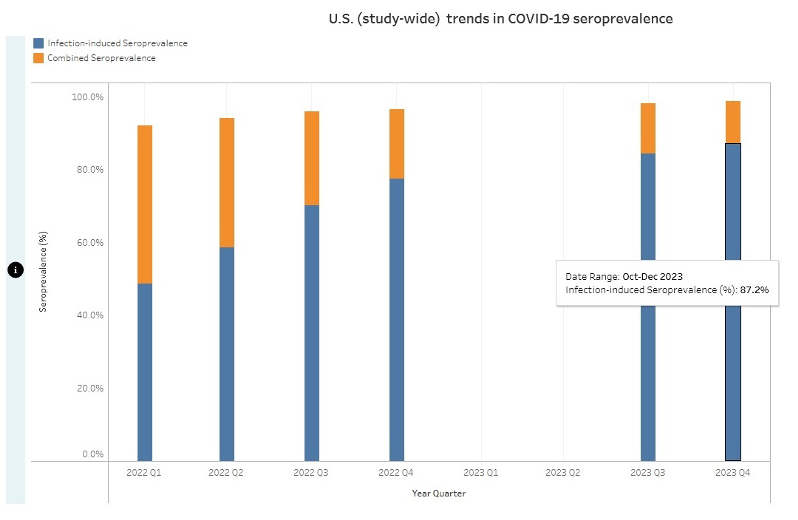
A typical mandate example: in September 2021, Washington Governor Jay Inslee issued Emergency Proclamation 21-14.2, requiring Covid-19 vaccination for various groups of state workers. In the proclamation, the stated goal was, “WHEREAS, COVID-19 vaccines are effective in reducing infection and serious disease, and widespread vaccination is the primary means we have as a state to protect everyone … from COVID-19 infections.” That is, the stated goal was to reduce the number of infections.
What the CDC recently reported (see chart below), however, is that by the end of 2023, cumulatively, at least 87% of Americans had anti-nucleocapsid antibodies to and thus had been infected with SARS-CoV-2, this in spite of the mammoth, protracted and booster-repeated vaccination campaign that led to about 90% of Americans taking the shots. My argument is that by making policies based on number of infections a higher priority than ones based on the more serious but less common consequences of both infections and policy damages, the proclaimed goal of the vaccine mandate to reduce spread failed in that 87% of Americans eventually became infected anyway.
In reality, neither vaccine immunity nor post-infection immunity were ever able fully to control the spread of the infection. On August 11, 2022, CDC stated, “Receipt of a primary series alone, in the absence of being up to date with vaccination through receipt of all recommended booster doses, provides minimal protection against infection and transmission (3,6). Being up to date with vaccination provides a transient period of increased protection against infection and transmission after the most recent dose, although protection can wane over time.” Public health pandemic measures that “wane over time” are very unlikely to be useful for control of infection spread, at least without very frequent and impractical revaccinations every few months.
Nevertheless, infection spread per se is not of consequence, because count of infections is not and should not have been the main priority of public health pandemic management. Rather, the consequences of the spread and the negative consequences of the policies invoked should have been the priorities. Our public health agencies chose to prioritize a failed policy of reducing the spread rather than reducing the mortality or the lockdown and school and business closure harms, which led to unnecessary and avoidable damage to millions of lives. We deserved better from our public health institutions.
Harvey A. Risch, MD, PhD
References Cited
1. Inglesby TV, Nuzzo JB, O’Toole T, Henderson DA. Disease mitigation measures in the control of pandemic influenza. Biosecur Bioterror. 2006;4(4):366-75. https://www.liebertpub.com/doi/10.1089/bsp.2006.4.366
2. Ramirez VB. What Is “R-naught”? Gauging Contagious Infections. Healthline, June 14, 2023. https://www.healthline.com/health/r-naught-reproduction-number
3. Worldometer. United States Coronavirus Cases. March 28, 2024. https://www.worldometers.info/coronavirus/country/us/
4. Gupta S. Was I wrong about the Covid infection fatality rate?. UnHerd, April 5, 2023. https://unherd.com/newsroom/how-wrong-was-i-on-covid-ifr/
5. Inslee J. PROCLAMATION BY THE GOVERNOR AMENDING PROCLAMATIONS 20-05 and 20-14: 21-14.2. COVID-19 VACCINATION REQUIREMENT. Issued September 27, 2021. https://governor.wa.gov/sites/default/files/proclamations/21-14.2%20-%20COVID-19%20Vax%20Washington%20Amendment%20(tmp).pdf
6. CDC. 2022-2023 Nationwide COVID-19 Infection- and Vaccination-Induced Antibody Seroprevalence (Blood donations). March 22, 2024. https://covid.cdc.gov/covid-data-tracker/#nationwide-blood-donor-seroprevalence-2022
7. Our World in Data. Total number of people who received at least one dose of COVID-19 vaccine. Downloaded March 27, 2024. https://ourworldindata.org/grapher/people-vaccinated-covid
8. Massetti GM, Jackson BR, Brooks JT, Perrine CG, Reott E, Hall AJ, Lubar D, Williams IT, Ritchey MD, Patel P, Liburd LC, Mahon BE. Summary of Guidance for Minimizing the Impact of COVID-19 on Individual Persons, Communities, and Health Care Systems – United States, August 2022. MMWR Morb Mortal Wkly Rep. 2022;71(33):1057-1064. https://www.cdc.gov/mmwr/volumes/71/wr/mm7133e1.htm
Dr. Harvey A. Risch MD, PhD is a Professor Emeritus of Epidemiology at the Yale School of Public Health and a guest contributor for Peter Navarro’s Taking Back Trump’s America
Austrian officials must have known all along that “covid” was a nothing-burger
Startling disclosures from official documents
BY JONATHAN ENGLER | APRIL 08, 2024
A colleague in HART has drawn my attention to this article on “TKP”, an Austrian sceptical website. As usual, machine translation does a good enough job to discern the gist for us non-German speakers.
It is reported that in an official government report entitled Virus Epidemiological Information No. 18/20 published in April 2020:
Prof. Judith Aberle reported on evidence of immunity against SARS-CoV-2 through T cells in blood samples from Austria going back to 2018 and in some other countries even as far back as 2015. It would probably have been the duty of the MedUni Vienna to make the public aware of the findings about widespread immunity.
The article goes on to state that Prof. Aberle disclosed that:
… in studies from the USA, Singapore, Germany, the Netherlands and Great Britain, SARS -CoV- 2 specific T -Cells were detected:
“Depending on the study, T cells against SARS-CoV-2 could be detected in 20 to 50 percent of blood donors. In Austria, too, in our previous studies we found T cells against various SARS-CoV-2 proteins in 30 percent of the blood samples from 2018-2019, i.e. before the pandemic.”
The actual reports in question are available here, and the specific one cited above (report 18-20) here.
Sure enough, Google translate confirms the Professor states the following:
Interestingly, T cells against SARS-CoV-2 can also be found in some pPeople who have not yet had contact with the new coronavirus. Show that several international studies from the USA, Singapore, Germany, the Netherlands and Great Britain. Those used for these investigations Blood samples come from healthy people from 2015-2018, i.e. a long time before SARS-CoV-2 first appeared in China. Depending on the study, 20 to 50 percent of blood donors have T cells detected against SARS-CoV-2 become. In our previous studies in Austria we have also found 30 Percent of blood samples from 2018-2019, i.e. before the pandemic, T cells found against various SARS-CoV-2 proteins. We now know about it Studies from the USA and Germany show that it is primarily about memory T cells are involved in infections with those four known Coronaviruses have been formed that cause relatively mild respiratory infections cause. They are called HCoV-OC43, -229E, -HKU1 and -NL63, occur worldwide and cause around 30% of colds However, you can get it back every year.
So, she is basically suggesting that the T cell reactivity comes from previous exposure to other coronaviruses.
However, as the article states:
The other explanation, which is at least as plausible, would be that SARS-CoV-2 spread significantly before 2020.
Whether “the virus” was “novel” or not seems to be an academic question, unless the new virus was causing lots of extra illness or death. But – as would be expected for something for which so many people seemed able to mount an adequate immune defence – it wasn’t.
The article then links to a piece from a few days ago about a recent episode of a TV show held in “Hangar 7” in which various state officials either maintained that covid was a terrible disease or that it couldn’t have been known back in spring 2020 that it wasn’t.
But, as the article points out:
- In an 9 April 2020 edition of the same program John Ioniodis’s data suggesting very low mortality was discussed.
- On April 10th , a TKP article was published in which not only Ionnidis’ findings were presented, but also the French study by Didier Raoult with the telling title ” SARS-CoV-2: fear versus data “, as well as a study from Wuhan with similar infection mortality.
- Even the decidedly mainstream vienna.at on April 7, 2020 reported that: “Analysis shows: Covid-19 victim curve corresponds to “normal” mortality”, concluding: “The Covid-19 victim curve in Austria roughly corresponds to the “normal” mortality for men and women in the individual age groups”.

Translated: Analysis shows: Covid-19 victim curve corresponds to “normal” mortalitySo the article states plainly that:
So the facts were well known, people knew about it.
It goes on to quote Dr Christian Fiala of the Karolinska Institut:
Ultimately, the alleged danger of the virus was only “scaled up” in order to get the mRNA into people. The virus was pretty insignificant and I think the many discussions about its laboratory origin were smoke grenades or media hype to attribute a meaning to the virus that it didn’t even have. It was never about the virus, it was about the mRNA.
This business concept is now obvious.
It will be interesting to see if these revelations result in any more indignation in the Austrian population than we are seeing in other countries – where, considering the scale of the lies and harms caused, voices are extraordinarily muted.
Fauci’s Inquisition Against Safe and Effective Anti-COVID-19 Drugs

By Richard Gale and Dr. Gary Null | Global Research | April 6, 2024
A question needs to be asked. Were the novel experimental drug treatments for SARS-CoV-2 viral infections that Anthony Fauci, the CDC and FDA advocated for and funded responsible for worsening the contagion and countless deaths?
However, at that time there were plenty of studies confirming there were pre-existing safe, inexpensive medications known to have highly effective antiviral properties to treat Covid-19 patients. Among these were ivermectin and hydroxychloroquine (HCQ).
There were also specific nutrients such as vitamin D and zinc, known to strengthen the immune system against viral infection and yet there was no recommendation from the government about the benefits of proper nutrition. So why did Fauci along with other federal health officials choose to intentionally ignore the scientific evidence and rather condemn these repurposed drugs? In Fauci’s case, over a year and half into the pandemic, he continued to lie outright on CNN that “there is no clinical evidence whatsoever that [ivermectin] works.”[1] And could millions have been saved if these generic medications were prescribed rather than the feds doing nothing but recommending social isolation and quarantines as the world awaited an experimental Covid-19 vaccine to enter the market?
To date, between ivermectin and HCQ alone, there have been 670 published studies, analyses and papers involving over 9,800 scientists and over 682,000 patients supporting the use of these drugs over and beyond those the FDA has approved under Emergency Use Authorization (EUA) statutes. Despite this, four years later, the FDA continues to fiercely deny ivermectin’s and HCQ’s efficacy and safety under proper administration. Why this blatant cover-up?
Every CDC effort to approve a novel drug treatment for SARS-CoV-2 infections has been a dismal failure. Aside from monoclonal antibody therapy, only three anti-Covid-19 drugs have been approved under an EUA in the United States. None met their promised expectations from either the manufacturer or our federal health agencies. With their poor efficacy rates, safety profiles and a black box warning slapped upon Pfizer’s anti-Covid-19 drug Paxlovid, the CDC is scrambling to find new viable alternatives in the pharmaceutical pipeline. Bloomberg amplifies the fake Covid-19 treatment crisis by lamenting that repurposed drugs such as ivermectin are gaining global popularity as “the world needs effective Covid drugs.”[2]

Shortly after the pandemic was formally announced, the FDA recommended the cheap over the counter anti-malarial drug hydroxychloroquine but then quickly reversed its decision after Fauci publicly announced the future arrival of Gilead Sciences’ novel intravenous drug Remdesivir. The FDA’s and European Union’s approvals of Remdesivir baffled many scientists, according to the journal Science, who questioned its therapeutic value and kept a close watch on the drug’s clinical reports about a “disproportionally high number of reports of liver and kidney problems.”[3] Even an earlier Chinese study published in The Lancet found that remdesivir had no impact on the coronavirus. The Science article notes that the “FDA never consulted a group of outside experts that it has at the ready to weigh in on complicated antiviral drug issues.”[4] Six months before remdesivir received EUA approval, Anthony Fauci had already hailed the drug as a major breakthrough that would establish a new “standard of care” in Covid-19 treatment.[5]
Today, remdesivir is being increasingly recognized as a debacle in antiviral therapeutic care. Even the WHO released a “conditional recommendation against the use of remdesivir in hospitalized patients, regardless of disease severity, as there is currently no evidence that remdesivir improves survival and other outcomes in these patients.” An Italian study observed a 416 percent increase in hepatocellular injuries among hospitalized Covid-19 patients treated with Remdesivir.[6] And a smaller Taiwanese study of hospitalized unvaccinated patients reported a 185 percent higher mortality during late remdesivir treatment.[7]
Earlier this year, Pfizer’s novel oral Covid-19 medication Paxlovid was given an FDA black box warning for clinically significant adverse reactions that can potentially be fatal. Because the company does not permit independent random-controlled trials to investigate its drug, other than retrospective studies, we only have Pfizer’s own data to rely upon. Nevertheless, The Lancet published a study by a team of Chinese scientists at Shanghai Jiao Tong School of Medicine that managed to look at Paxlovid’s use among critically ill patients hospitalized with Covid-19. The study reported a 27 percent higher risk of the infection progressing, a 67 percent increased risk in requiring ventilation, and 10 percent longer stays in ICU facilities.[8]
Paxlovid is a combination of a novel SARS-CoV-2 protease inhibitor and the HIV protease inhibitor ritonavir. The FDA approved Paxlovid under a EUA with the claim it was safe. However, on the government’s HIV.gov website for ritonavir it is clearly stated that the drug “can cause serious life-threatening side effects. These include inflammation of the pancreas (pancreatitis), heart rhythm problems, severe skin rash and allergic reactions, liver problems and drug interactions.”[9] Perhaps due to the drug’s serious side effects, it is no longer used solely against HIV, but rather is given in smaller doses as a booster for AZT-related drugs. Being highly toxic, ritonavir is also not recommended for pregnant women and has been shown to interfere with hormone-based birth control efficacy.
Paxlovid only received FDA EUA approval in May 2023. At that time, the agency claimed there was no evidence that patients who were treated with the drug rebounded and came down with Covid. However, shortly thereafter this was determined to be untrue.[10] A Harvard analysis found that 21 percent of Paxlovid recipients will remain contagious and likely succumb to a viral rebound compared to only 1.8 percent who did not take the drug.
Merck’s anti-Covid-19 drug molnupiravir (Lagevrio) also has an FDA black box warning for potential fetal harm when administered to pregnant women. Why the drug was ever approved under an EUA seems to be an enigma. The drug’s antiviral activity is based upon a metabolite known as NHC, which for many years has been known to create havoc in an enzyme crucial for viral replication by inserting errors into the virus’ genetic code. The theory is: produce enough errors and the virus kills itself off. However, molnupiravir can cause hundreds of mutations thereby “supercharging” the manufacturing of new Covid-19 viral strains. Moreover, according to a Forbes article, the drug’s mutagenic powers may also interfere with our own body’s enzymes and DNA.[11] Another Forbes article points out that Merck’s clinical trial only enrolled around 1,500 participants, which is far too “small to pick up on rare mutagenic events.”[12]
Molnupiravir has a poor efficacy rate across the board including viral clearance, recovery, and hospitalizations/death (68 percent).[13] One trial, funded by Merck, concluded the drug had no clinical benefit.[14] More worrisome, the drug also has life-threatening adverse effects including mutagenic risks to human DNA and mitochondria, carcinogenic activity and embryonic death.[15]

Each of these drugs have been outrageous cash cows for their manufacturers. Remdesivir is priced at $3,120 per treatment and earned Gilead $5.6 billion in sales for 2021.
Pfizer’s Paxlovid is priced at $1,390 per treatment. Last year, the company’s revenues for its Covid products—Paxlovid and the Comirnaty vaccine—came in at $12.5 billion, and, according to Fierce Pharma, Pfizer wrote off an additional $4.7 billion on its overstocked Paxlovid inventory.[16] Merck’s molnupiravir’s sales for 2022 cashed in almost $5.7 billion. Despite their profits, none of these drugs have been shown convincingly to have measurably lessened the pandemic nor the spread of SARS-CoV-2.
Despite all the attention and medical hype about novel experimental antiviral drugs to treat Covid-19, Anthony Fauci and other federal officials had full knowledge that other FDA-approved drugs existed that could have been quickly repurposed at minimal expense to effectively treat Covid-19 infections. Repurposing existing drugs to treat illness is a common occurrence. The antiparasitic and antiviral drug Ivermectin best stands out. Its effectiveness was observed to be so remarkable and multifaceted that researchers started to investigate its potential.
The mainstream media, including many liberal news sources who pride themselves on their independence, continue to channel the voices of Anthony Fauci, the CDC and FDA to demonize ivermectin and other generic drugs for treating Covid-19 and to reduce hospitalization and deaths. This propaganda campaign, however, has completely ignored the large body of medical literature that shows ivermectin’s statistically significant efficacy against symptomatic and asymptomatic SARS-2 infections.
Originally developed for veterinarian use, in 1987, the FDA approved ivermectin for treating two parasitic diseases, river blindness and stronglyoidiasis, in humans. Since then an enormous body of medical research has grown showing ivermectin’s effectiveness for treating other diseases. Its broad range of antiviral properties has shown efficacy against many RNA viruses such avian influenza, zika, dengue, HIV, West Nile, yellow fever, chikungunya and earlier severe respiratory coronaviruses. It has also been shown to be effective against DNA viruses such as herpes, polyomavirus, and circovirus-2.[17]
Unsurprisingly, ivermectin’s inventors Drs. William Campbell and Satoshi Omura were awarded the 2015 Nobel Prize in Physiology and Medicine.
It has been prescribed to hundreds of millions of people worldwide. Given its decades’ long record of in vitro efficacy, it should have been self-evident for Fauci’s NIAID, the CDC and the WHO to rapidly conduct in vivo trials to usher ivermectin as a first line of defense for early stage Covid-19 infections and for use as a safe prophylaxis.
For example, if funding were devoted for the rapid development of a micro-based pulmonary delivery system, mortality rates would have been miniscule and the pandemic would have been lessened greatly.[18] Repurposing ivermectin could have been achieved very quickly at a minor expense.[19] However, despite all the medical evidence confirming ivermectin’s strong antiviral properties and its impeccable safety record when administered properly, we instead witnessed a sophisticated government-orchestrated campaign to declare war against ivermectin and another antiviral drug, hydroxychloroquine (HCQ), in favor of far more expensive and EUA approved experimental drugs. Unlike the US, other nations were eager to find older drugs to repurpose against Covid-19 and protect their populations. A Johns Hopkins University analysis offered the theory that a reason why many African countries had very few to near zero Covid-19 fatalities was because of widespread deployment of ivermectin. In February 2020, the National Health Commission of China, for example, was the first to include hydroxychloroquine in its guidelines for treating mild, moderate and severe SARS-2 cases. Eight Latin American nations distribute home Covid-19 treatment kits that include ivermectin.[20] Why did the US and most European countries swayed by the US and the WHO fail to follow suit?
Early in the pandemic, physicians in other nations where treatment was less restricted, such as Spain and Italy, shared data with American physicians about effective treatments against the SARS-2 virus. In addition, there was a large corpus of medical research indicating that older antiviral drugs could be repurposed. Doctors who started to prescribe drugs such as ivermectin and HCQ, along with Vitamin D and zinc supplementation, observed remarkable results. Unlike the dismal recovery and high mortality rates reported in hospitals and large clinics that relied upon strict isolation, quarantine, and ventilator interventions, this small fringe group of physicians reported very few deaths among their large patient loads. Even reported deaths were more often than not compounded by patients’ comorbidities, poor medical facilities and other anomalies.
Very early into the pandemic, medical papers indicated ivermectin was a highly effective drug to treat SARS-2 infections.
In April 2020, less than a month after the WHO declared Covid-19 as a global pandemic, Australian researchers at the Peter Doherty Institute of Infection and Immunity published a paper demonstrating that a single ivermectin dose can control SARS-CoV-2 viral replication within 24-48 hours.[21] Monash University’s Biomedicine Discovery Institute in Australia had also published an early study that ivermectin destroyed SARS-2 infected cell cultures by 99.8 percent within 48 hours. But no American federal health official paid any attention.
As of March 2024, a database for all studies and trials investigating ivermectin against Covid-19 infections records a total of 248 studies, 195 peer-reviewed, and 102 involving controlled groups reporting an average 61 percent improvement for early infections, a 39 percent success rate in treating late infections, and an 85 percent average success rate for use as a preventative prophylaxis.[22] Moreover, prescribing ivermectin reduced mortality by 49 percent, compared to remdesivir’s 4 percent, Pfizer’s Paxlovid’s 31 percent, and molnupiravir’s 22 percent. Even hydroxychloroquine well outperforms these drugs mortality risk for early treatment at 66 percent.
A noteworthy study conducted in Brazil and published in the Cureus Journal of Medical Science prescribed ivermectin in a citywide prophylaxis program in a town of 223,000 residents. 133,000 took ivermectin. The results for a population of this size are indisputable in concluding that ivermectin is a safe first line of defense to confront the pandemic. Covid mortality was reduced 90 percent. There was also a 67 percent lower risk of hospitalization and a 44 percent decrease in Covid cases. Garcia-Aquilar et al reports a Mexican in vitro analysis showing a definitive interaction between ivermectin and the SAR-CoV-2 spike protein, which would account for its high efficacy in Covid-19 cases.[23]
The All India Institute for Medical Science (AIIMS) and the Indian Council of Medical Research (ICMR), two of India’s most prestigious institutions, acted against the WHO and launched an ivermectin treatment campaign in several states. In Uttar Pradesh there was a 95 percent decrease in morality (a decline from 37,944 to 2,014). The Indian capital of New Delhi witnessed a 97 percent reduction. During the same time period, the state of Tamil Nadu, which followed the WHO’s ban on ivermectin, had a 173 percent increase in deaths (from 10,986 to 30,016 deaths).
There have been many concerted efforts to discredit ivermectin and other repurposed drugs’ effectiveness. Most notable is the large TOGETHER Trial Brazil study published in the New England Journal of Medicine (NEJM) that concluded both ivermectin and another repurposed drug fluvoxamine showed no beneficial signs for treating Covid-19 patients. The study was widely reported in the mainstream media. However, a Cato Institute analysis discovered the study in fact showed its benefits and the results were in agreement with 87 percent of other clinical trials investigating ivermectin. The Cato analysis identifies many odd anomalies in how the trial was conducted including an unspecified placebo—although it is suspected it was Vitamin C, which has itself been shown to be mildly effective against the SARS-CoV-2 virus, and protocol changes as the study was underway including inclusion/exclusion criteria. By his own admission the TOGETHER Trial’s principal investigator Dr. Ed Mills at McMaster University in Ontario “designs clinical trials, predominantly for the Bill and Melinda Gates Foundation.”[24] In a McMaster University press release, the Gates foundation is listed as a funder for the study to debunk ivermectin and fluvoxamine.[25] Oddly, Gates is nowhere listed among the several funders in the NEJM study’s disclosure. In addition, TOGETHER Trials is owned by the Canadian for profit startup Purpose Life Sciences, founded by Mills; legal documents showed Mills’ PLS is largely funded and controlled by Sam Bankman Fried’s FTX who invested $53 million into the project. Administrators of FTX’s bankruptcy are suing PLS for fraud.[26]
In short, the ivermectin/fluvoxamine TOGETHER Trial was a complete medical sham and intentionally designed for one single purpose: to fuel media disinformation in order to undermine ivermectin’s superior efficacy and safety profile to Big Pharma’s more profitable designer drugs.
In 2004, the US Congress passed an amendment to the Federal Food, Drug and Cosmetic Act known as Emergency Use Authorization (EUA). This piece of legislature legalized an anti-regulatory pathway to allow experimental medical interventions to be expedited and bypass standard FDA safety evaluations in the event of bioterrorist threats and national health emergencies such as pandemics. At the time, passage of the EUA amendment made sense because it was partially in response to the 2001 anthrax attacks and the US’s entry into an age of international terrorism. However, the amendment raises some serious considerations. Before the Covid-19 pandemic, EUAs had only been authorized on four occasions: the 2005 avian H5N1 and 2009 H1N1 swine flu threats, the 2014 Ebola and the 2016 Zikra viruses. Each of these pathogen scares proved to be false alarms that posed no threat of pandemic proportions to Americans. The fifth time EUAs were invoked was in 2020 during the Covid-19 pandemic, which at the time seemed far more plausible.
Before the government can authorize an EUA to deploy an experimental diagnostic product, drug or vaccine, certain requirements must be fulfilled. First, the Secretary of the Department of Health and Human Services (HHS) must have sufficient proof that the nation is being confronted with a serious life-threatening health emergency. Second, the drug(s) and/or vaccine(s) under consideration must have sufficient scientific evidence to suggest they will likely be effective against the medical threat. The evidence must at least include preclinical and observational data showing the product targets the organism, disease or condition. Third, although the drug or vaccine does not undergo a rigorous evaluation, it must at least show that its potential and known benefits outweigh its potential and known risks. In addition, the product must be manufactured in complete accordance with standard quality control and safety assurances.
When we look back at the government’s many debacles during the Covid-19 pandemic, other EUA requirements warrant the spotlight. On the one hand, an EUA cannot be authorized for any product or intervention if there is an FDA alternative approved product already available, unless the experimental product is clearly proven to have a significant advantage. Moreover, and perhaps more important, EUAs demand informed consent. Every individual who receives the drug or vaccine must be thoroughly informed about its experimental status and its potential risks and benefits. Recipients must also be properly informed about the alternatives to the experimental product and nobody should be forced to take it.
Finally, an EUA requires robust safety monitoring and reporting of adverse events, injuries and deaths potentially due to the drug or vaccine. This is the responsibility not only of the private pharmaceutical manufacturers but also the FDA, physicians, hospitals, clinics and other healthcare professionals.
Obviously important cautions must be considered after approving a medical intervention under the EUA requirements. Foremost are the inherent health risks of any rapid response of experimental medical interventions, especially novel drugs and vaccines. As we observed during the FDA approval process and roll out of Pfizer’s and Moderna’s mRNA Covid-19 jabs, no long-term human trials were conducted to even estimate a reliable baseline of their relative efficacy and safety. The American public has blindly placed its trust in our federal health authorities decision-making. It is expected that under a national health emergency, the authorities would be completely transparent and act only by the highest ethical standards. However our institutions betrayed public trust and either ignored or transgressed cautions underlying EUA approved medical interventions in every conceivable way. Moreover, conflicts of interests have been discovered to have plagued the entire EUA review process.
Although the EUA amendment provides some protections to authorized drug and vaccine manufacturers, it was the Public Readiness and Emergency Preparedness Act (PREP) in 2005 that expanded liability protections. In addition to protecting private corporations, PREP also shields company executives and employees from claims of personal injury or death resulting from the administration of authorized countermeasures. The only exceptions for liability are if the company or its executive offices are proven to have engaged in intentional and/or criminal misconduct with conscious disregard for the rights and safety of those taking their drugs and vaccines.
During the pandemic, the FDA issued widespread EUAs with liability immunity for the PCR diagnostic kits for SARS-2, the mRNA vaccines and the anti-Covid-19 drugs. Curiously, the Secretary of the Department of Health and Human Services invoked the PREP Act on February 4, 2020 giving liability protections; this was over a month before the pandemic was officially announced, which raises serious questions about prior-planning before the viral outbreak in Wuhan, China.
From the pandemic’s outset, Fauci embarked on the media circuit to promise Americans that federal health agencies were doing everything within their means to get a vaccine on the market because there was no available drug to clear the SARS-2 virus. As we have seen with respect to ivermectin alone, this was patently false. Rather the government placed an overriding emphasis on vaccination with a near total disregard for implementing very simple preventative measures to inhibit viral progression. Once mass vaccinations were underway, we were promised that the SARS-2 virus would be defeated and life would return to normal. In retrospect, we can look back and state with a degree of certainty that American health authorities and these products’ corporate manufacturers may have violated almost every EUA requirement. Everything that went wrong with the PCR kits, the experimental mRNA vaccines and novel drugs could have been avoided if the government had diligently repurposed effective and safe measures as pandemic countermeasures. Very likely, hundreds of thousands of lives, perhaps millions, would have been saved.
Similarly the FDA issued a warning statement against the use of ivermectin. Even ivermectin’s manufacturer Merck discredited its own product. Shortly after ridiculing its drug, the Alliance for Natural Health reported, “Merck announced positive results from a clinical trial on a new drug called molnupiravir in eliminating the virus in infected patients.”[27]
And still the FDA considers these novel patented drugs to be superior to ivermectin. Favoring a vaccine regime and government-controlled surveillance measures to track every American’s movements, American health officials blatantly neglected their own pandemic policies’ severe health consequences. Ineffective lockdowns, masks, social isolation, unsound critical care interventions such as relying upon ventilators, and the sole EUA approvals of the costly and insufficiently effective drugs brought about nightmares for tens of millions of adults and children. This was all undertaken under Fauci’s watch and the heads of the US health agencies in direct violation of the EUA requirements to only authorize drugs and medical interventions when no other safe and effective alternative is available. Alternatives were available.
The 4-year history of the pandemic highlights a sharp distinction between dependable medical research and pseudoscientific fraud. The CDC adopted a common Soviet era practice to redefine the very definition of a vaccine and the parameters of vaccine efficacy in order to fit economic and ideological agendas. This explains Washington’s aggressive public relations endeavors to silence medical opponents. According to cardiologist Dr. Michael Goodkin’s private investigations, several of the most cited studies discrediting ivermectin’s antiviral benefits were intentionally manipulated in order to produce “fake” results.[28] These studies were then widely distributed to the AMA, American College of Physicians and across mainstream media to author “hit pieces” to demonize ivermectin and other repurposed drugs. The government’s belligerent and reactive diatribes, brazenly or casually advocating for censorship, were direct violations of scientific and medical integrity and contributed nothing towards developing constructive policies for handling a pandemic with a minimal cost to life. The consequence has been a less informed and grossly naïve public, which was gaslighted into believing lies.
The FDA’s EUAs for the Covid-19 vaccines and novel experimental drugs were in fact an attack on the amendments and PREP directives. Neither the vaccines nor drugs warranted emergency authorization because effective and safe alternatives were readily available. No doubt a Congressional investigation would uncover criminal misconduct and conscious fraud. Moreover, these violations of the PREP Act may have the potential to lead directly into medical crimes against humanity as outlined in the Nuremberg Code.
Although the Nuremberg Code has not been officially adopted in its entirety as law by any nation or major medical association, other international treaties, such as the Universal Declaration of Human Rights, the World Medical Association Declaration of Helsinki (which is not legally binding), the International Covenant on Civil and Political Rights (ICCPR) and the International Ethical Guidelines for Biomedical Research on Human Subjects incorporate some of Nuremberg’s main principles that aim to protect people from unethical and forced medical research. Although the US signed the ICCPR as an intentional party, the US Senate never ratified it. The ICCPR’s Article 7 clearly states, “No one shall be subject to torture or cruel, inhuman or degrading treatment or punishment,” which can legally be interpreted to include forced medical experimentation implied as cruel, inhuman treatment. Other ICCPR articles, 6 and 17, are also applicable to medical experimentation to ensure ethical conduct, obtaining proper informed consent and the right to life and privacy. For a moment, consider the numerous senior citizens in nursing homes and hospitals who were simply administered experimental Covid-19 vaccines without full knowledge about what they were receiving. And now how many children are being coerced by the pseudoscience of health officials’ lies to be vaccinated without any knowledge of these mRNA products’ risk-benefit ratio?
The US is also a signatory to the Helsinki Declaration, which, although not directly aligned with Nuremberg, shares much in common. The Declaration shares some common features with the EUA amendment and PREP Act. These include voluntary informed consent—which is universally accepted, adequate risk and benefit information about medical interventions, and an emphasis on the principle of medical beneficence (promoting well-being and the Hippocratic rule of doing no harm). It also guarantees protections for vulnerable groups, especially pregnant women and children, which the US government and vaccine makers directly violated by conducting trials on these groups with full knowledge about these vaccines’ adverse events in adults. In addition, weighing the scientific evidence to assess the risk-benefit ratios between prescribing ivermectin and HCQ over the new generation of novel experimental drugs conclusively favors the former. This alone directly violates the ethical medical principles noted above.
However, the failure to repurpose life-saving drugs is less criminal than the questionable unethical motivations to usher a new generation of genetically engineered vaccines that have never before been adequately researched in human trials for long term safety. This mass experimentation, which continues to threaten the health and well-being of millions of people, is global and can legally be interpreted as a genocidal attack on humanity.
If the emerging data for increasing injuries and deaths due to the Covid-19 vaccines is reliable—and we believe it is—the handling of the pandemic can be regarded as the largest medical crime in human history. In time, and with shifting political allegiances and public demands to hold our leaders in government and private industry accountable, the architects of this medical war against civilization will be brought to justice.
*
Richard Gale is the Executive Producer of the Progressive Radio Network and a former Senior Research Analyst in the biotechnology and genomic industries.
Dr. Gary Null is host of the nation’s longest running public radio program on alternative and nutritional health and a multi-award-winning documentary film director, including his recent Last Call to Tomorrow.
Notes
[1] https://www.cnn.com/videos/health/2021/08/29/dr-anthony-fauci-ivermectin-covid-19-sotu-vpx.cnn
[4] https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31022-9/fulltext
[6] https://www.dldjournalonline.com/article/S1590-8658(21)00923-3/fulltext
[8] https://www.thelancet.com/action/showPdf?pii=S2666-6065%25252823%25252900012-3
[9] https://clinicalinfo.hiv.gov/en/drugs/ritonavir/patient
[10] https://www.yalemedicine.org/news/13-things-to-know-paxlovid-covid-19
[13] https://www.medrxiv.org/content/10.1101/2023.01.20.23284849v1.full.pdf
[14] https://evidence.nejm.org/doi/pdf/10.1056/EVIDoa2100044
[15] https://c19early.org/waters.html
[17] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7290143/
[18] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7539925/
[19] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7564151/
[21] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7129059/
[22] https://c19ivermectin.com
[23] https://www.mdpi.com/1422-0067/24/22/16392
[25] https://www.eurekalert.org/news-releases/855535
[26] https://c19ivm.org/tallaksen.html
[27] https://anh-usa.org/fda-ensures-pharma-profits-on-covid/
[28] https://www.trialsitenews.com/a/are-major-ivermectin-studies-designed-for-failure
Rogues’ Gallery
Never forget that they’re a bunch of liars

By John Leake | Courageous Discourse™ | April 5, 2024
Maddow, Walensky, and Biden may plead ignorance, as they apparently don’t understand anything, but Fauci, Gates, and Bourla certainly knew they were lying. As Fauci himself noted in a November 2022 paper:
… non-systemic respiratory viruses such as influenza viruses, SARS-CoV-2, and RSV tend to have significantly shorter incubation periods (Table 1) and rapid courses of viral replication. They replicate predominantly in local mucosal tissue, without causing viremia, and do not significantly encounter the systemic immune system or the full force of adaptive immune responses, which take at least 5–7 days to mature, usually well after the peak of viral replication and onward transmission to others. …
Taking all of these factors into account, it is not surprising that none of the predominantly mucosal respiratory viruses have ever been effectively controlled by vaccines.
Fauci already knew this about influenza and coronaviruses before 2020, and it quickly became apparent that SARS-CoV-2 was no different in this respect.
Never forget this Rogues’ Gallery of liars and the lies they told the world in order to justify tyranny based on fraudulent assertions.
In New Bird Flu Scare Comes Tacit Admission Coronavirus Was Not a Big Deal
By Adam Dick | Peace and Prosperity Blog | April 5, 2024
“Bird flu pandemic could be ‘100 times worse’ than COVID, scientists warn.” That is the headline at the New York Post for one of many media reports out Thursday spreading the latest pandemic scare.
Note the “100 times worse” comparison. Why not “nearly as bad,” “as bad,” or even “twice as bad” as coronavirus? The answer is that the fearmongers know that most people are on to the coronavirus hoax whereby a run-of-the-mill health threat was exaggerated to justify tyrannical measures including forcing termination of a vast amount of in-person interaction, mandating mask wearing, and even pushing and mandating experimental “vaccine” shots marketed as safe and effective despite being both dangerous and ineffective. All the while, good early treatment options were suppressed, resulting in greater sickness and death as well as expansive use of dangerous medical procedures and pharmaceuticals for people whose serious illness could have been prevented.
The world could be turned upside down over coronavirus because of a concerted effort of government and media to paint coronavirus as both extremely dangerous to everyone and something for which there were not already available good medical countermeasures. Both of those assertions were false. But, at the time, many people bought into the charade and trusted that “the science” propounded by the government and media selected “experts” required radical changes in human behavior, widespread participation on novel medical experimentation, and extreme restraints on liberty.
But now it is a new day. Looking back on the coronavirus scare, increasingly people realize, including some who are ashamed to discuss the matter, that they were duped. And they don’t want to be duped again. “Fool me once, shame on you; fool me twice, shame on me,” the saying goes.
Yet, trickery is a go-to tactic for expanding power. The government and its business allies in medical and other fields aren’t about to give up on that tactic that reaped such huge gains during the coronavirus scare. Thus the ploy of tacitly admitting what has become common knowledge — that coronavirus was way overblown — so that the repression and profit process can be repeated anew to deal with a threat that, trust us, is this time really, really, really bad.
And what scientist does the New York Post article quote to support the claim that scientists say the bird flu is “100 times worse than COVID” declared in the article’s title? His name is John Fulton, described in the article as “a pharmaceutical industry consultant for vaccines.”
Oh brother: Here we go again. Or do we? If enough people stand up and say “no you don’t this time,” this new dangerous charade can be stopped in its tracks.
America Has Paid a Total of $38,893 to Avalanche of COVID Vaccine Injured Citizens
By Jefferey Jaxen | March 29, 2024
What Americans were sold during the COVID vaccine rollout hype was an injection to return to normal – medical blackmail. A two-dose series turned into multiple boosters, as high as nine now recommended by the CDC if you are counting. As many capitulated, no public spokesperson or mainstream media outlet marketing the shot uttered a word about its safety or what would happen if someone was harmed by the rushed, experimental product…a tactic called strategic silence.
A ‘black hole’ for COVID vaccine injury claims was the title of a June 29, 2021 Reuters article describing the Countermeasure Injury Compensation Program, or CICP, run by the Health Resources and Services Administration. A program few Americans ever knew existed and probably still don’t.
This is the program people who are injured by the COVID shot get tossed into if they are educated enough to recognize the harm from the shot and their doctor understands and is courageous enough to file a claim. And here are a few other stipulations that matter:
- No attorney & medical expert fee reimbursement
- 1-year statute of limitations (from the date of administration)
- No reimbursement for future medical care
- No pain & suffering damages
- No appeal to a higher court in the CICP
- No medical testimony or hearings. You vs Sec’y of HHS
- Lack of transparency on reporting of decisions
It’s been three years since the COVID vaccine rollout and hundreds of millions of doses later, injury compensation is still lacking to the point it borders on criminal. The CICP has recently released their monthly updated injury compensation numbers – three weeks late for those keeping an eye on them.

11 claims compensated…

For a grand total of… $38,893.
Proponents of COVID vaccine safety will use this number, 11, as proof the vaccine is indeed safe ignoring how the CICP is monumentally unfit for its current purpose.
Speaking to Wayne Rohde, author of The Vaccine Court and host of Right on Point podcast about the the CICP program, he said, “The CICP was never designed for a long-term, nationwide pandemic public health crisis.”
Meanwhile, as the public tries to piece together the true human damage caused by the COVID shots, we take a look at another broken, unfit program in the CDC’s Vaccine Adverse Event Reporting System (VAERS). Can you spot an issue once the COVID shots began going into American arms on an industrial scale in 2021?

In addition to the deaths, there have been 214,906 hospitalizations, 154,245 urgent care visits, 242,537 doctors office visits, 10,767 cases of anaphylaxis, 17,688 cases of Bell’s palsy, 5,115 miscarriages, 21,524 heart attacks, 28,215 cases of myo/per-carditis, 69,936 cases of ‘permanently disabled,’ and 39,544 ‘life-threatening’ and so many more reports to VAERS after the COVID shot. In all, a total of 1,630,913 reports.
Let’s take a moment to do some math here. VAERS is a system that is notorious for underreporting. A study of the system found “fewer than 1% of vaccine adverse events are reported.” Assuming the current number of VAERS reports of 1,630,913 is only 1%, the true number may be closer to something like 163,091,300.
Last month FDA director of the Center for Biologics Evaluation and Research Dr. Peter Marks appeared before the Select Subcommittee on the Coronavirus Pandemic to discuss possible issues with the fast-tracking of the COVID shots.
When asked by Chairman Brad Wenstrup if the government was prepared for such an avalanche of reports to VAERS, Marks replied, “We tried to be prepared for that but the avalanche of reports was tremendous.”
So on one side with VAERS, we have a broken government intake program getting overwhelmed on the front end while the other (CICP) sees the outflow of compensation for damages and cases awarded administratively throttled. Caught in between are untold numbers of Americans left hanging in the wind shouldering unsettled medical harms and the bills to follow. America can do better.
The entire vaccine damage infrastructure needs a historic overhaul. From education for medical professionals to recognize and encourage reporting of harms from the shots to greater research on why some are more susceptible than others to vaccine injury while addressing decades of ignored scientific research.
Most importantly, a true compensation mechanism for the injured beyond CICP’s pittances and the long-broken National Vaccine Injury Compensation Program. The beginning of a fair compromise should, at the very least, end the product liability shield for vaccine manufacturers.
“Drug companies should be liable in civil court for vaccine injuries and deaths and so should anyone giving vaccines to people being denied the human right to informed consent to medical risk-taking,” said NVIC co-founder and president Barbara Loe Fisher. “There is an urgent need to hold vaccine manufacturers and doctors accountable in civil court for the safety of vaccines and how they are being given.”
More Young People Getting Cancer — What’s Behind the New ‘Public Health Crisis’?
By Suzanne Burdick, Ph.D. | The Defender | March 27, 2024
Catherine, Princess of Wales, who on March 22 announced she has cancer, “is part of an unfortunate new trend of more and younger cancer cases,” according to Dr. Pierre Kory and journalist Mary Beth Pfeiffer.
Kory and Pfeiffer addressed Princess Catherine’s diagnosis in an op-ed published Tuesday in The Washington Times, in which they said there’s evidence suggesting that the marked increase in cancers among young people may be linked to COVID-19 mRNA vaccines and pandemic policies, such as lockdowns and vaccine mandates.
“We are facing an emerging toll of illness and death in the young,” they wrote. “We cannot shirk from asking what is causing it.”
Kory — president and chief medical officer of the Frontline COVID-19 Critical Care Alliance — told The Defender that early-onset cancer and excess deaths are “poised to become the next public health crises that our medical system is not equipped to manage.”
This latest op-ed is Kory and Pfeiffer’s fourth. Their three prior op-eds — which appeared in USA Today, Newsweek and The Hill — also called attention to excess mortality and disability rate spikes occurring after the global COVID-19 vaccine campaign.
“Our intention for writing the op-eds is to raise the profile of this important issue to prepare for a future crisis and advance the conversation on possible causes and treatments,” Kory said.
In their latest op-ed, Kory and Pfeiffer said an “unthinkable twist” in cancer rates is occurring and it has garnered the attention of the American Cancer Society, Yale Medicine and the Harvard Gazette.
According to the American Cancer Society’s 2024 report, about 2 million people in the U.S. will develop malignancies this year — and a larger share of the more than 600,000 who are estimated to die will be younger than before.
CDC data show ‘red flags’
Kory and Pfeiffer cited cancer death records through 2023 from the Centers for Disease Control and Prevention (CDC) that included data two years beyond what was in the American Cancer Society report.
“The later data, which is provisional,” they wrote, “shows a cancer pattern that appears to have gone from slow simmer to rapid boil in the heat of a pandemic.”
They found that cancer deaths across all ages rose by 2% from pre-pandemic 2019 to 2023 — and in people 15-44 years old, cancer-related mortality rose at double that rate.
“Why is this happening now?” Kory and Pfeiffer asked. “Moreover, what will be done to address it?”
They saw additional “red flags” in the CDC data including:
- Deaths from colorectal cancer rose 17% among people ages 15-44 in 2019-2023 — 4 times the population-wide increase.
- Uterine cancer deaths rose 37% among people ages 25-44 from 2019-2023, and 15% overall.
- There were much larger increases, from 2019-2022, in liver and pancreatic cancer mortality in young adults than in the overall population.
The U.S. Society of Actuaries also reported 76% and 101% increases in death claims among insured workers ages 25-34 and 35-44. “COVID-19 was ruled out as the cause,” Kory and Pfeiffer said.
The public needs to explore the role of lockdowns, top-down treatment protocols and vaccines that were often mandated as a condition of employment, they said.
“By top-down treatment protocols,” Kory told The Defender, “I’m referring to how the public health and medical authorities made edicts on treatments that had to be followed and could not be questioned without consequence.”
“These same authorities were not open to understanding the novel treatments showing promise on the frontlines and instead allowed information to flow only one way — from the top down,” he said.
‘Just a tragic coincidence?’
In a March 27 Substack post about the data exposed in the op-ed, Kory said he and Pfeiffer compiled and interpreted these and other data from government and professional society sources after “bearing witness to so much medical carnage.”
“Just a few weeks ago,” he said, “a 20-year-old patient of mine died of glioblastoma.”
He added:
“If that is not tragic enough, her parents told me that a 20 year-old man in her college friend group had died of the same a few weeks earlier. Unsurprisingly, their university had a vaccine mandate.
“Just a tragic coincidence right?”
But reviewing cancer facts and figures has convinced Kory that such cases aren’t just a coincidence.
“We believe that the data strongly if not definitively implicates the COVID mRNA vaccine as the most proximate cause.”
Suzanne Burdick, Ph.D., is a reporter and researcher for The Defender based in Fairfield, Iowa.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Featured Video

Rewriting the risk? Inside the government’s vaccine safety messaging
or go to
Aletho News Archives – Video-Images
Book Review
“Davos Can Really Replace the UN”
Inside the book that maps the architecture behind global governance — from the Epstein files to the Pact for the Future
Lies are Unbekoming | April 1, 2026
On June 13, 2019, the United Nations and the World Economic Forum signed a partnership deal to “accelerate the implementation of the 2030 Agenda for Sustainable Development.” That same evening, WEF president Börge Brende — Norway’s former Foreign Minister — had dinner with Jeffrey Epstein at Epstein’s Manhattan townhouse. The Epstein files, released January 2026, contain an exchange between the two from the previous year. Epstein to Brende: “Davos can really replace the UN. C21, cyber, crypto . genetics… intl coordination.” Brende back to Epstein: “Exactly — we need a new global architecture. World Economic Forum (Davos) is uniquely positioned — public private.”
The next day, the UN General Assembly adopted the framework for restructuring global governance.
That sequence — the partnership signing, the Epstein dinner, the candid admission about replacing the UN with a public-private architecture, and then the formal adoption — opens Jacob Nordangård’s The Digital World Brain. Pages two and three. Footnoted to the UN resolution number, the Epstein files, and the General Assembly record.
I keep coming back to it because it captures what this book does that almost nothing else in the independent research space manages. I’ve followed Jacob’s work for years now and interviewed him about his research. Each book peels back another layer of the same institutional architecture, and each time I think he’s reached the limit of what can be documented, the next one goes further. Nordangård doesn’t speculate. He doesn’t editorialize much. He lays institutional actions next to each other in chronological order and lets the pattern announce itself. … continue
Blog Roll
 Aletho News
Aletho News- How I fell foul of the BBC thought police
- The End of NATO
- 37 days of war on Iran cost US staggering $42bln, tracker shows
- Baghdad tells Asian refiners, traders to begin loading Iraqi crude amid Iranian exemption
- Under fire, Moscow and Tehran close ranks
- Iran, US receive Pakistan-mediated plan for ceasefire then final deal
- Iran submits demands for end to war as mediators scramble ahead of Trump deadline
- Iran Threatens Retaliatory Strike on Stargate AI Project in UAE
- US sent ‘a lot’ of arms to Iranian protesters – Trump
- Barak Ravid Launders Deception To Allow Trump To Back Off Of His Power Plant Threat – Again
- If Americans Knew
- Israel’s Latest Genocide Is Against the Shias of Lebanon. Why Is the World Silent?
- How Eliot Cohen’s influence over U.S. war-making paved the way for Trump’s war crimes in Iran
- Israelis don’t pay for the weapons we ‘sell’ to them — US taxpayers do
- While Distancing from AIPAC, Most 2028 Democratic Hopefuls Are Still Embracing Israel
- A brief history of the Israeli nuclear program, the open secret at the heart of the Iran war
- Israeli Settlers Killed a Palestinian Farmer on His Own Land, in Front of His Father. Yes, Again
- The US-Israeli War on Science is an Assault on our Future
- 100+ International Law Experts Say US Strikes on Iran Violate UN Charter, Could Be War Crimes
- ‘Vile, Horrifying, Evil’: Trump Threatens to Bomb Nation of 90 Million People ‘Back to the Stone Ages’
- The Axis of Resistance: Islamic Liberation Theology and the Struggle for Freedom
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
