In a precedent-setting victory last month, a New York State Supreme Court judge ruled that 10 New York City school teachers fired for refusing the COVID-19 vaccine on religious grounds must be reinstated with back pay, benefits, seniority and attorney fees.
But the city immediately appealed the decision, so none of those teachers have returned to their jobs or received any payments.
“These workers absolutely did win reinstatement and back-pay,” Sujata Gibson, the teachers’ attorney told The Defender. “Unfortunately, in New York State courts, the government is entitled to an ‘automatic stay’ of any such relief pending resolution of the appeal.”
Gibson also said:
“CHD [Children’s Health Defense] is supporting us in our fight to defend these wins on appeal, and we are pursuing additional options to try to speed this process up and secure relief for additional plaintiffs. But the fight is not over yet.”
Nearly 7,000 New York City Department of Education (DOE) workers who sought religious accommodation from the COVID-19 vaccine mandate in 2021 were denied based on standards that a federal court later ruled unconstitutional.
The suit also sought class-action certification for all DOE workers who were denied religious exemptions. Judge Ralph Porzio denied the motion to grant class status, a ruling the plaintiffs are appealing.
Regardless, Gibson said the decision was “a precedent-setting victory, and a watershed moment in the teachers’ fight.”
Thousands of workers were subjected to the very same processes the judge ruled were “arbitrary and capricious,” and they could sue individually based on that precedent, if it is upheld by the appeals court, Gibson said.
Michael Kane, one of the plaintiffs and a member of Teachers For Choice, told The Defender that after filing the appeal, the city has six months to take the next step in the case — so even though they won with the last ruling, the fired teachers will have to continue to fight for their rights and the relief they are entitled to.
The struggle continues, despite confusion on social media
Last week, a Fox News story from Oct. 25, 2022, “New York Supreme Court reinstates all employees fired for being unvaccinated, orders backpay” was picked up and celebrated on social media by influential figures and their followers. It circulated on X, formerly Twitter, and Instagram, where hundreds of thousands of social media users “liked” the posts, Kane said.
The story itself was vague — it did not cite the actual case that had been ruled on and it gave the impression that all New York City workers fired for refusing vaccination would be returning to work with back pay.
In fact, the story was posted after the state’s Supreme Court ruled in favor of plaintiffs George Garvey and 15 other New York City Department of Sanitation employees who were fired by the city for non-compliance with the mandate.
That historic ruling was applicable not only to the 16 workers who sued but also to all public employees in New York City, including the police and fire department.
But in that case, the city also appealed the ruling and the appeals process is ongoing.
New York City workers, with substantial public support, continue to fight, Kane said.
He added:
“This isn’t just for us, it’s for our kids and our grandkids. This is laying the groundwork. It took over 50 years for Plessy v. Ferguson to be overturned by Brown v. Board of Education. Civil rights battles are long, protracted struggles, and that’s what we’re in. It’s not fun, but that’s what we’re in.”
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
What is “shedding” and what are the implications for our health? Tonight, host Betsy Ashton will be joined by Dr. Pierre Kory and Scott Marsland, FNP-C for this important discussion.
My clinical practice is loaded with patients who took one or two vaccines early in 2021 and realized like most of us that the the mRNA products were not safe. A common question is: “doctor when does this shot get out of my body?”
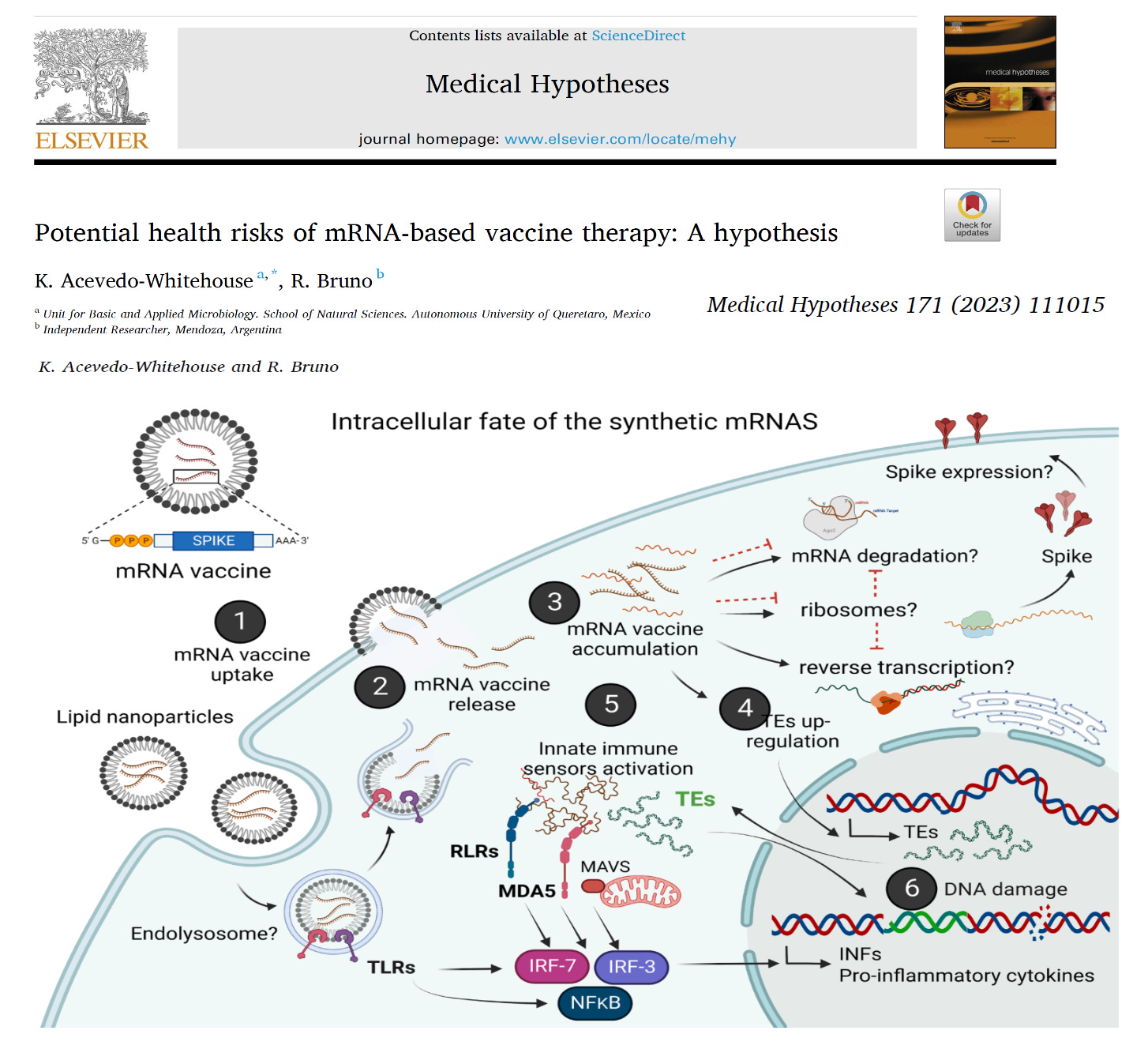
Acevedo-Whitehouse and Bruno raise this point in a recent peer reviewed publication concerning the entire mRNA vaccine product pipeline.
Therapeutic applications of synthetic mRNA were proposed more than 30 years ago, and are currently the basis of one of the vaccine platforms used at a massive scale as part of the public health strategy to get COVID-19 under control. To date, there are no published studies on the biodistribution, cellular uptake, endosomal escape, translation rates, functional half-life and inactivation kinetics of synthetic mRNA, rates and duration of vaccine-induced antigen expression in different cell types. Furthermore, despite the assumption that there is no possibility of genomic integration of therapeutic synthetic mRNA, only one recent study has examined interactions between vaccine mRNA and the genome of transfected cells, and reported that an endogenous retrotransposon, LINE-1 is unsilenced following mRNA entry to the cell, leading to reverse transcription of full length vaccine mRNA sequences, and nuclear entry. This finding should be a major safety concern, given the possibility of synthetic mRNA-driven epigenetic and genomic modifications arising.
These are stunning revelations. I have called for a halt on mRNA research development until these fundamental questions can be answered. If synthetic mRNA cannot be broken down by the human body, there were be no way to shut off potentially dangerous antigens such as the Spike protein of SARS-CoV-2, Influenza virus hemagglutinin (HA), or any other toxin produced from the genetic code. To make matters worse, it appears that all of these proteins will be expressed on the cell surface and cause auto-immunity with any new mRNA vaccine. This alone is a show stopper for me in my practice. I am advising NO mRNA vaccines for my patients.
The following fictional story may or may not bear resemblance to events in real life.
Imagine, if you will, that you are a first-generation high tech gazillionaire. In fact, at one time you were said to be the richest man on earth, although that is no longer the case. Nevertheless, you remain unimaginably wealthy, with all the responsibilities and burdens that such wealth brings. (Given the extremely unusual circumstances of this tale, to make it more relatable, we will assign you a fictional name.) Your birth certificate reads Gilbert Harvey Bates III, but the world knows you as Gil Bates.
Gil Bates’s erstwhile net-worth preeminence (stolen as it was by an upstart online retailer named Biff Jezos) is not the only important loss he has suffered. Also in the rearview mirror is his youth, his marriage, and his position as CEO of the behemoth tech company he created, MacroHardTM.
After Gil Bates stepped down as CEO of MacroHardTM, he focused on his philanthropic work. The centerpiece of this work is the immensely well-funded (and therefore immensely influential) Bates Foundation. The Foundation’s scope may be mind-bogglingly broad, but one problem especially consumed Bates: there are far too many people on the planet.
In his youth, Gil Bates read a controversial book called The Overpopulation Bomb, written by a visionary scientist named Saul Derelicht. That alarming book, a huge bestseller in its day, described a neo-Malthusian hell on earth resulting from human overpopulation, and proposed mass sterilization and other aggressive population reduction techniques as the solution.
Gil Bates became convinced, and remains convinced – especially as the worldwide human population has soared beyond 8 billion units – that Homo sapiens have obscenely overpopulated the planet. Once Bates had sold software packages to the great majority of them, he vowed that this existential threat to the planet must be addressed.
But what was to be done? How could this great affront to Gaia be reconciled? When it comes to a responsibility so great, a task so immense, no single man – not even Gil Bates – could hope to accomplish it alone.
Fortunately for the future of Earth, Bates knew a host of like-minded, enlightened elites, pre-eminent individuals of great wealth, power, and worldwide influence. Among the most important:
A dour Teutonic economist named Kraut Schlob. The son of an ambitious industrialist who built flamethrowers for the Third Reich, Schlob is the founder and chairman of the World Enslavement Forum. The Forum has become the premier worldwide gathering of hyper-elites who wish to discuss globalist policies, and enjoy the company of high-end prostitutes, free from the prying eyes of commoners.
An immensely powerful – if embarrassingly vertically challenged – American health bureaucrat named Dr. Fantoni Auci. For decades, Dr. Auci controlled the overwhelming majority of US Government medical research funding. As such, no one in the vast American network of hospitals, research institutes, or universities dares to cross Dr. Auci, and he wields similar influence internationally. In fact, he oversees funding for multiple secret virology research laboratories, as far away as China.
A mysterious veterinarian named Adalbert Ghoula. Ghoula is the CEO of Kaiser, Inc., the world’s largest and most rapacious pharmaceutical company, which Ghoula has grown into a veritable modern day IG Farben. In his earlier days, Ghoula oversaw the development of a vaccine that successfully induces the chemical castration and sterilization of swine.
The consensus, reached after lengthy consultations with these men and other luminaries, was that the worldwide human population must be reduced from 8 billion to 500 million units.
But how? Several possible avenues were proposed.
War has been used for millennia to reduce populations, and while highly effective locally or regionally, it would be entirely ineffective at removing the necessary fifteen-sixteenths of people on Earth. After all, the deadliest war in history, World War II, resulted in a mere 80 million deaths, just 3 percent of the world’s population at the time.
The use of a bomb was considered a special kind of bomb, reminiscent of the “neutron bomb” of yore, which would supposedly reduce populations while sparing infrastructure. This seemed closer to the mark than all-out war, but ultimately it was determined that setting off bombs would be both impractical and far too obvious. After all, even herd animals will not consent to being openly and massively slaughtered, no matter how necessary the culling may be. The herd must be kept forever in the dark.
A plague, a pestilence, a pandemic seemed more promising. Past naturally occurring pandemics had reduced human populations much more successfully than wars. The Black Death of 1346-53 may have reduced the world population by as much as 25 percent, a much more encouraging number than the measly 3 percent from World War II. As an added economic bonus, the Black Death served as a very effective concentrator of wealth for the survivors, as it caused minimal collateral property loss.
However, a more detailed review of historical worldwide population estimates demonstrated that a pandemic alone could only serve as a temporizing measure at best. Most estimates show that by 1400, the worldwide population had unfortunately returned to its pre-plague total.
Clearly, the necessary 94 percent reduction in population could not be achieved by culling the herd alone. Sterilization would be needed as well. But how to achieve such mass sterilization? Many H. sapiens possess an intense desire to procreate – that’s the source of the problem, after all. Unfortunately, prior historical initiatives for mandatory sterilization – even those of limited scale and scope, such as those targeting the mentally deficient – have met great opposition, at least in the so-called “free” nations.
However, a vaccine could be used for mass sterilization. Ghoula’s earlier work at Kaiser was proof of this. But a fundamental problem remained: how to get the unsuspecting population – specifically, its children and young adults – to take the stealth-sterilizing inoculation?
The solution, when it came, was a thing of beauty, sublimely subtle and symmetrical. The answer was a two-step process: a pandemic and a vaccine. One population reduction device would be released, presented as a worldwide plague. It would be followed by a second population reduction device, presented as the cure.
And the technology was already in place to make it happen. It merely had to be perfected, then enacted.
Employing the Black Magic of gain-of-function virology research, an animal respiratory virus, previously never infecting humans, was genetically engineered to readily infect and spread amongst humans. At a key moment in political history, when a particularly bothersome populist American President named T. Ronald Dump was running for reelection, the virus was released from a Chinese laboratory into the human population.
As the new virus spread, reports of the death and devastation it wrought were spread as well. In actuality, the virus had been engineered so that it was deadly only to the frail, chronically ill, and very old. It was cleverly propagandized, however, as a threat to persons of all ages, a modern day Black Death of sorts.
The US deep state, desperate to disrupt the Dump presidency and remove him from office, were willing partners to manage the control and manipulation of the population through propaganda, and to enforce unprecedented, prolonged lockdowns of society. Remarkably, they even convinced President Dump to sanction the lockdowns, and to fund the development of the vaccine. Most other countries followed suit.
The new virus rapidly killed off many of the oldest and sickest members of society, as would be expected of a novel respiratory virus. However, the locked-down and isolated populations were barraged with media messages that stirred up mass terror of the virus. Businesses were closed, save for those deemed “essential.” Schools were closed, though children were already known to be at statistically zero risk of death. Dissenters were harassed, scapegoated, and punished.
Then, a solution to the pandemic was presented: the vaccine. The vaccine was the savior, the only way out of this crisis.
A few irritating, contrarian dissenters fought back. They protested for civil rights. They stressed the near impossibility of producing an effective vaccine against a rapidly mutating respiratory virus. They identified numerous “safety signals” found in the vaccine trials, and tried to expose these as best they could. But the mainstream media drowned them out, the social media companies (controlled by the deep state) censored them ruthlessly, and after all, once the vaccines were mandated, most people took at least a couple of doses.
And the joke was on the dissenters in another, more important respect. These meddlesome do-gooders were indeed intelligent enough to identify the toxicities inherent in the vaccines. But they decried them as “safety signals.” The fatal toxicities they identified still seemed to them to be flaws, mistakes, and the unfortunate results of a hasty and mad rush to make money off of the pandemic.
Imagine the naïvete.
Early in the vaccine “rollout,” young women reported abnormal vaginal bleeding and other menstrual problems after receiving the vaccines, raising concerns about potential unintended consequences to female reproduction. Pathologists found ovaries infiltrated with multiple toxins from the vaccines, both the dreaded “spoke” protein of the virus and “lucid nanoparticles” from the vaccine’s delivery system. Even occluded Fallopian tubes were identified.
Soon thereafter, reports appeared in the alternative media of dramatically increased numbers of sudden deaths, primarily in young men, after receiving the vaccine. It often visibly occurred in athletes while on the playing field. This caused considerable alarm, impossible as it was to hide.
In a masterful demonstration of the “limited hangout,” officials acknowledged the sudden death phenomenon, but would not even allow mention of the vaccine as a possible cause within the mainstream medical community. Instead, protocols and clinics for this sudden epidemic of heart disease in the young were established, but strangely without any official curiosity as to the cause. All they knew for sure was that it couldn’t be the vaccine.
Of course, the infamous “spoke” protein, the same viral antigen chosen by the vaccine’s designers to induce the vaccinated patient’s body to produce in quantity, just happens to be the most toxic part of the virus. The “spoke” protein deposits itself in tissues throughout the body, wreaking havoc wherever it goes. It has a particular affinity for the heart muscle, causing the inflammatory process known as myocarditis that leads to cardiac arrests.
“Spoke” doesn’t stop with the heart, however. It is a remarkably versatile toxin, a sort of Swiss Army monkey wrench in the human body. It causes gigantic, gruesome, rubbery blood clots in the vasculature, seizures in the central nervous system, the aforementioned deposits in ovaries and Fallopian tubes (and testes, for that matter), etcetera, etcetera. What a stroke of genius to choose “spoke” as the antigen the vaccines induce replication of!
The vaccines held another nasty little secret, which even the pathetic, naïve resistance only recognized much later. The vaccines were “contaminated” with plasmids containing MV-40 and MV-40-like DNA sequences. Yes, that MV-40, the monkey virus known to cause cancer in multiple animal species.
Could the appearance of so-called “turbo cancers” in vaccinated persons somehow be related to this “contamination?” Well, another limited hangout, this time courtesy of Healthcare Canada, took care of that.
Excess death rates rose dramatically after the vaccine rollout. Birth rates plummeted. To the do-gooders, refuseniks, and dissidents, this was a scandal.
But what did they know? To use a phrase all-too-familiar to the seasoned software developer, these toxicities were not bugs, but features. The vaccines were working exactly as they were supposed to work.
Silly plebes! The “vaccines” were actually a deliberate, multi-pronged, population reduction device. They were designed to kill a percentage of young people – mostly male – outright, to poison and disable the female reproductive system at multiple points, and to insert teratogenic plasmids into recipients’ cells, to pick off others at undisclosed, later dates. They were merely packaged and marketed as a vaccine against a (lab-manufactured) flu-like illness.
As successful as they have been, there remains so much more work yet to be done.
A definite lull occurred in the population’s acceptance of repeated injections of the vaccine. The dissidents may be naïve, but they are persistent, and sometimes effective to a degree. But ultimately they will fail.
The general population is lazy, uneducated, and easily terrified. (Some say they are being done a favor by being culled.) They are accustomed to the precedents set by other vaccines. Their reluctance will be worn down with time. Of course respiratory viruses are imperfect targets for vaccines. Once again, that’s not a bug, it’s a feature! It only means that a new booster of the vaccine will be needed every year – at least.
With each new round of boosters, a new population of girls and young women will be rendered infertile. A new group of boys and young men will suffer cardiac arrest – a very quick and painless way to die, really.
Countless others will contract cancers – turbo cancer, to use the current term for these rapidly progressing and deadly malignancies, often of unusual types – bone cancers, muscle cancers, and other former rarities. Not an easy way to die, admittedly. But these tumors mercifully progress to end stage very swiftly, and their value as a population reduction device is undeniable.
Have no fear. It is only a matter of time; only a matter of lather, rinse, repeat. As long as the herd allows itself to be sent through the sheep dip whenever and however often the shepherds proclaim is necessary, H. sapiens will get to 500 million. All courtesy of a type of bomb after all, but in this case a microscopic bomb that is released in each person via a tiny little injection: The Depopulation Bomb.
Happy Halloween!
C.J. Baker, M.D. is an internal medicine physician with a quarter century in clinical practice. He has held numerous academic medical appointments, and his work has appeared in many journals, including the Journal of the American Medical Association and the New England Journal of Medicine. From 2012 to 2018 he was Clinical Associate Professor of Medical Humanities and Bioethics at the University of Rochester.
Dr Keith Berkowitz is a founding member, with Dr Pierre Kory, of the Front Line Covid-19 Critical Care Alliance (FLCCC). He is treating a lot of vaccine-injured patients at his practice in midtown Manhattan. Dr Berkowitz was kind enough to answer a few questions on the Covid vaccine and the vaccine injured.
***
Who is most at risk for vaccine injury?
One thought is that if someone had Covid first, and then got the vaccine after being sick, the rates of vaccine injury were higher because they already had an antibody response, their immune system was already revved up, and then they got an injection of another antigen. Another group I see is people with autoimmune disease, they seem to be more triggered. I have several cases of people who had dormant autoimmune disease, such as ulcerative colitis and rheumatoid arthritis, and post vaccine it got retriggered. What people forget about vaccines is that they have an immunosuppressive effect. So in that two- to three-week period, the immune system takes a hit, which makes the body vulnerable to other illnesses. The third group I see that are most at risk of vaccine injury are people with high histamine levels.
What are the most common symptoms of vaccine injury?
Mildest is probably loss of taste and smell, mild digestive issues, or a cough. More severe are the autoimmune responses, the neurological symptoms, like brain fog, and tinnitus (which is one of the toughest to treat), myocarditis and pericarditis (inflammation of the heart), cancer, which I would call the most severe.
Is that new cancers, or cancers that have returned?
I’m seeing both.
Which autoimmune diseases are you seeing?
First, autoimmune disease is what I’m seeing most in vaccine injury. Specifically thyroid disease, more than anything else. What’s interesting is that I’m seeing normal thyroid function, and positive thyroid antibodies. So typically we wouldn’t check for thyroid antibodies if thyroid function was normal. So that group is often missed for that reason.
Would you say any vaccine was worse than the others?
It seems to be batch-related. That’s the question. There’s a theory that 10 per cent of the batches, roughly, caused 90 per cent of the issues. If you look at the original technology, the mRNA was created at a 70 per cent purity. There’s speculation that, because of manufacturing issues, they weren’t able to create that level of purity, and achieved only 50-55 per cent purity. So does one really know if that level of purity works? Especially being that it was never tested.
Why is there so much denial around vaccine injury?
I think there was a blind trust of the government and the pharmaceutical companies, coupled with a fear aspect of Covid (remember people thought that 50 per cent of hospitalised Covid patients died, when it was more like less than 1 per cent). Fear made people not think any more, and now they’re in denial about the choice they made. Another thing I can’t figure out: If you’re vaccinated, how does an unvaccinated person put you at risk? Also, why did doctors not do their own research? It was blind faith. Medications all have side effects – why was this one different?
How do you respond to the proponents of the vaccine who say, regarding vaccine injury, correlation is not causation?
That’s true, but why are they not even looking into it? If they are so confident, then just study it. What do they have to lose? Why not disprove it? Why is disproving it a major issue for them? If you don’t agree with me, prove me wrong.
Traditionally, vaccines take 10-15 years to get approval, because all that time they are studying long-term effects. The Covid vaccine, which was administered as soon as it was created, is still only about three years old. Therefore, have we yet to see the potential damage it can cause?
Absolutely. Do you know what percentage of drugs approved by the US Food and Drug Administration are withdrawn within five years? 31 per cent. One out of three drugs are taken off the market within five years. That’s incredibly high. That tells me we’re not checking properly. Now with this vaccine, one of my biggest questions is why did we decide to use new technology? Is a pandemic the right time to test new technology? I would argue probably not. And why did some countries around the world, like China and Russia, not use this technology? And at the end of the day we have to ask, was the treatment worse than the problem? And should medical products be tied to financial incentives? That creates a huge conflict. There were incentives to use the vaccine. If a drug or a treatment was really that good, would you need to push it like that?
Any final comments?
This is going to take years to figure out. It isn’t going away any time soon. I feel bad for the people who took something which they thought they were doing for the right reason, and now they are suffering. And they’re not being helped. Why does the government create a long Covid initiative, but not a vaccine-injured initiative? Why are we ignoring these patients? And why are we [in the US] approving a product for over six-month-olds when other countries are saying over 65 years? Another thing that doesn’t make sense is a study on teenagers showed that we have to vaccinate a million young men to prevent one hospitalisation. And the potential in a million doses is 1,000 with side effects. So the hospital to side effect rate is one to a thousand. It doesn’t make any sense! My worry is the trust in the medical system may never come back. And I’m not sure that it’s not deserved.
Sen. Ron Johnson (R-Wis.) accused federal public health agencies of displaying an “appalling” lack of transparency with the American public during the pandemic, depriving them of “the benefit of informed consent.”
In a letter sent Oct. 25 to the heads of the U.S. Department of Health and Human Services, the U.S. Food and Drug Administration (FDA), the Centers for Disease Control and Prevention (CDC) and the National Institutes of Health, Johnson said that even now, “As new and alarming information continues to come to light, federal health agencies continue to stonewall and gaslight Congress and the public.”
The lawmaker pointed to an FDA-funded study published this month that identified a potential safety signal linking mRNA COVID-19 vaccines to seizures in children ages 2-5.
Johnson questioned whether the CDC was aware of these findings last month when it recommended everyone 6 months of age and older be vaccinated to protect against COVID-19 this fall and winter.
As a result, they “have not even come close to ensuring that doctors can provide informed consent on a new gene therapy masquerading as a ‘vaccine’ that was rushed to market without adequate safety or efficacy testing,” he said.
In his letter, the lawmaker wrote that the agencies’ refusal to respond to the “vast majority” of his questions and information requests “only heightens [his] level of suspicion.”
He listed over a dozen letters he sent requesting information on the COVID-19 vaccines that the agencies “have failed to adequately address.”
These included requests for data about vaccine lots linked to high rates of adverse events, information suppression on social media and the Countermeasures Injury Compensation Program.
Johnson listed 11 other outstanding requests he made regarding the other aspects of the pandemic.
But these make up only a partial list of over 60 public letters Johnson said he has sent to government agencies concerning various aspects of the pandemic.
“It is well past time for U.S public health agencies to be transparent,” he said.
Johnson requested the agencies respond by Nov. 8 to questions about what they knew about the risks COVID-19 vaccines posed to children, when they knew it and how they plan to address those issues.
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
Dr. Kulvinder Kaur Gill is a pediatric allergist in Toronto. She condemned COVID rules as irrational, political, harmful, and inconsistent with scientific data. In the eyes of the College of Physicians and Surgeons of Ontario (CPSO), Gill was dangerous.
In 2021, the CPSO issued three “cautions” (formal warnings) against her. In 2022 it began disciplinary proceedings. The College alleged that she was undermining confidence in public health measures. Its senior counsel wrote that her communications were unprofessional and unbalanced. In its persecution of Gill, the CPSO has made the case for its own demise. Self-regulated monopolies do not work. The CPSO and other professional regulators need competition.
Gill’s inquisition was not an isolated case. Like other medical regulators in North America, the CPSO forbade its doctors from publicly contradicting COVID orders and recommendations. Its Discipline Tribunal revoked the licence of Patrick Phillips, one of several Ontario doctors pursued for their COVID dissent.
The Nova Scotia medical college investigated Dr. Chris Milburn for writing an op-ed on the death of personal responsibility in the criminal justice system. The Ontario College of Psychologists ordered Jordan Peterson to undergo re-education on the use of social media for tweeting about politics. The BC College of Nurses seeks to discipline Amy Hamm for believing in the biology of two sexes.
The Law Society of Ontario compelled its members to state their concurrence with the ideology of “equity, diversity, and inclusion” until a group of rebel lawyers (of whom I was one) managed to repeal it, although the agenda remains. In British Columbia and Alberta, law societies are instituting politically laden “cultural competency” requirements. Teachers, occupational therapists, engineers, and accountants cannot safely voice doubts about transgenderism or “anti-racist” agendas.
This regulatory bullying is occurring within self-regulated professions. Like “ordinary” regulation, self-regulation is coercive. The state delegates authority to their governing bodies. Some doctors rule over other doctors. A licence from the CPSO is voluntary only in the sense that a driver’s licence is voluntary. You don’t get fines or prison time if you don’t get one, but then you can’t drive or practice medicine. Gill’s livelihood was on the line.
Civil servants do not run self-governing professional bodies, but they are part of the executive branch of government nonetheless. Legislation creates them and they are subject to the constitution. Self-regulation exists only for as long as the legislature says that it does.
Legislatures delegate authority, the theory goes, because professionals have the expertise to ensure competence and ethical practice in the public interest. Your surgeon should know how to cut. Your corporate lawyer should be able to draft articles of incorporation and not skim funds off your trust account. But focusing on technical competence and honest conduct no longer satisfies professional regulatory bodies.
We live in a managerial age. As C.S. Lewis wrote:
“The greatest evil is not now done in those sordid ‘dens of crime’ that Dickens loved to paint. It is not done even in concentration camps and labour camps. In those we see its final result. But it is conceived and ordered (moved, seconded, carried, and minuted) in clean, carpeted, warmed, and well-lighted offices, by quiet men with white collars and cut fingernails and smooth-shaven cheeks who do not need to raise their voices.”
Professions have become managerial cartels. Governing bodies are their godfathers, permitting only proper people and perspectives. Their purpose is not to ensure public access to a variety of professional opinions. Instead, they seek to herd people into “correct” attitudes and behaviors. Propaganda is not evil, but merely a tool to facilitate right results.
Ironically, managerial cartels turn out to be terrible managers. They excel at exercising control but not at producing good outcomes. During COVID, even propaganda was patently incoherent. Yet Gill was one of a scant few doctors and scientists to decry the public health debacle unfolding in front of them. As her lawyer Lisa Bildy wrote in response to the College’s accusations, Gill provided the public with substantiated facts on lockdowns, masking, and COVID vaccines, relying on credible and respected scientific sources and opinions.
The College had scheduled a two-week disciplinary hearing for early 2024. But in September 2023, it abruptly cancelled the hearing with no explanation. Gill’s disciplinary ordeal had come to an end, although her formal warnings remain. Bildy will challenge their validity by judicial review in spring 2024.
Self-regulation protects professions from government interference. That is ironic, given the CPSO’s insistence that their members toe the government line. But self-regulation does not protect individual professionals from the oppression of their peers. A different model beckons: multiple, private regulators competing for members, credibility, and public trust.
Professional cartels benefit the bullies who run them. There’s no reason to grant them the power of monopoly.
Bruce Pardy is executive director of Rights Probe and professor of law at Queen’s University.
Dr. Malik writes:
My name is Ahmad Malik and I am an honest surgeon passionate about free speech and medical ethics.
I have been suspended without pay and cancelled because I dare to challenge the Government narrative, defend informed consent, oppose mandates and lockdowns, question experimental jabs and insist that there are only two biological sexes.
I am raising funds to take legal action against the hospital to lift my suspension and stop the attempts by organisations to censor me.
It will set a precedent that organisations cannot bully, harass and censor those that speak up for medical ethics, and encourage others to speak out.
I am up against large organisations and my case is complex. Legal costs will easily run into the thousands. I need a decent fighting fund which will give me the best chance of being successful.
Pfizer-BioNTech delayed reporting vaccine-associated deaths among BNT162b2 clinical trial participants until after the U.S. Food and Drug Administration (FDA) issued an Emergency Use Authorization (EUA) for the product.
The vaccine makers also failed to account for a large number of subjects who dropped out of the trial.
The authors of the paper described it as a “forensic analysis,” defined by the U.S. National Institute for Standards and Technology as “the use of scientific methods or expertise to investigate crimes or examine evidence that might be presented in a court of law.”
What the analysis shows
Corinne Michels, Ph.D., retired distinguished professor of biology at Queens College, New York, led the DailyClout Pfizer/BioNTech Documents Investigations Team on what the authors claim was the first independent examination of original data from the Pfizer-BioNTech COVID-19 mRNA vaccine (BNT162b2) clinical trial.
Investigators looked at each of the 38 deaths occurring between July 27, 2020, the start of phase 2/3 of the Pfizer-BioNTech vaccine trial, and March 13, 2020, the end date culminating in Pfizer-BioNTech’s 6-month interim report.
This trial phase involved 44,060 subjects. Half received a dose of BNT162b2, half got a placebo consisting of an inactive sterile salt solution.
The trial was unusual because at week 20 after the FDA issued the EUA for the vaccine, trial subjects in the placebo group were allowed to switch to the vaccinated group and receive their first BNT162b2 shot.
Switching from the placebo to the vaccinated group — or “unblinding” — normally occurs when the benefit of the drug is so great that not treating subjects becomes unethical. For example, investigators might consider unblinding a cancer trial if at some point all untreated patients deteriorated or died but all treated patients improved.
Unblinding conditions may be specified in the study design, but they usually involve input or review from medical ethicists.
Of 20,794 unblinded placebo subjects in the Pfizer trial, 19,685 received at least one dose of BNT162b2.
Normally the decision to unblind a vaccine trial would be based on the product’s safety and effectiveness in reaching certain endpoints or objectives. Endpoints for a drug to prevent viral infections might be a positive test or self-reported COVID-19 illness (the “case” numbers that drove much of COVID-19 policy), illness requiring hospitalization or death.
But, perhaps unexpectedly, after 33 weeks the data revealed no significant difference between deaths in the vaccinated and placebo groups for the initial 20-week placebo-controlled portion of the trial.
After week 20, after most former placebo subjects had received the vaccine, deaths among those in the vaccine group continued unabated.
The authors revealed “inconsistencies” between data presented in Pfizer-BioNTech’s 6-month interim report and subsequent publications by Pfizer-BioNTech trial site administrators:
“Most importantly, we found evidence of an over 3.7-fold increase in the number of deaths due to cardiac events in the BNT162b2 vaccinated individuals compared to those who received only the placebo.”
This means that 79% of relevant deaths were not recorded in time to be included in Pfizer’s regulatory paperwork.
By not including relevant subject deaths in the case report, Pfizer obscured cardiac adverse event signals, allowing the EUA to proceed unchallenged.
How did Pfizer get around legal, ethical obligations?
The Pfizer-BioNTech data, obtained through a Freedom of Information Act lawsuit, uncovered four additional deaths in the vaccine group and one more in the placebo group — but Pfizer failed to include these data in their FDA submission despite an explicit study design requirement to do so.
These data, and how they differ from what Pfizer-BioNTech reported in their applications, are summarized in Table 3 of Michels’ study.
One case involved a 63-year-old woman who died 41 days after receiving the shot, but whose death only entered the data pool 37 days later. Another was a 58-year-old woman whose death 72 days after vaccination went unreported for 26 days.
Had Pfizer-BioNTech met their legal and ethical obligation to report all serious adverse events their data would have shown equal deaths in placebo and vaccine groups — which would have shown no clear benefit for the vaccine.
How were they able to skirt those obligations?
For one, they were able to hide behind the the 2005 Public Readiness and Emergency Preparedness (PREP) Act, which provided an almost impenetrable liability shield for vaccine manufacturers for “medical countermeasures” in response to any “public health emergency.”
Second, because COVID-19 was viewed as a national health emergency, regulators abandoned the established, patient-centered, safety-based approval process requiring years of preclinical animal testing — and Pfizer-BioNTech unsurprisingly went along.
Timing of death reports raises questions
Michels also raised issues regarding total death reports and their timing.
Since the death total from both study groups, 38, appeared “surprisingly low” to study authors — particularly during a pandemic — they undertook their own analysis based on population mortality expectations at the time.
Assuming that age-adjusted death rates for the study subjects were similar to those of the general population, they estimated that 222 subjects should have died from July 27, 2020, to March 13, 2021. The reported number, 38, is just 18% of the expected number.
Michels explained this by the large number, 4.2% of “discontinued subjects.” The most concerning of these were subjects “lost to follow-up,” which means missing scheduled visits or other required activities.
Pfizer-BioNTech tried to reach these subjects via phone, certified mail or through their emergency contact but despite their efforts could not account for 395 subjects who had dropped out.
The authors wrote:
“These are not insignificant numbers and could easily account for the low number of deaths reported in this safety period of the trial. Given the importance of knowing the status of each trial subject, there should have been greater effort to locate these individuals.
“Additionally, Pfizer/BioNTech was responsible for oversight of the trial sites. Sites with excessive numbers of lost to follow-up should have been evaluated for performance.”
Michels was also concerned over how certain trial centers had many dropped-out subjects while others had none or just a few.
Ninety-six of 153 trial sites (63%) reported 0 or 1 subjects lost to follow-up and 34 (22%) reported 2-5 dropouts. But four sites reported more than 20 subjects lost to follow-up, amounting to about 5% of all trial subjects.
Since the vaccine makers were responsible for trial site oversight, the authors wrote, “Sites with excessive numbers of lost to follow-up should have been evaluated for performance.”
Finally, based on the data, it appears Pfizer-BioNTech was in no hurry to enter death reports before the EUA submission deadline, particularly for the BNT162b2 group.
Of the 38 reported deaths only one case was added on the day the subject died. Delays of 20+ and 30+ days were common.
One death took 72 days to find its way into the database, and all were entered as occurring on the reporting day, not on the actual date of death.
Of the eight subjects in the vaccine group that should have been reported by Dec. 10, 2020, the EUA application cutoff, the average reporting delay was 17.5 days for subjects in the vaccine group, but just 5.9 days for deaths among subjects in the placebo group.
Angelo DePalma, Ph.D., is a science reporter/editor for The Defender.
Many COVID vaccine skeptics reported an unusual number of “sudden deaths” happening lately.
Such reports are always dismissed as “biased.” And, perhaps, they are biased. I have to admit that I am biased, too, and that keeps me from blaming Covid vaccines for various isolated incidents that I know of.
However, we now have Peter Hotez, one of the most rabid Covid vaccine promoters, unwittingly join the “reporting unusual sudden deaths” club.
Professor Hotez’s today’s tweet laments the sudden passing of his “close colleagues and friends.” Peter mentions that they were “still active when they passed,” so he means sudden deaths.
His suddenly deceased friends were “champions of global health”; tireless Covid vaccine advocates like himself. Professor Hotez is not sure what to blame. Overwork? Exhaustion? – he asks.
I am also not sure; perhaps it is climate change or stress his friends experienced from seeing vaccine misinformation online.
This is the same Stephen Colbert who almost every night took great joy in making fun of people like myself, the national vermin who never got one shot.
But the joke is on Stephen Colbert. I’ve never had Covid and I’ve never gotten one jab.
Actually, I think I probably had “early Covid” in January 2020, which we can’t talk about. Still, this non-Covid did produce stellar natural immunity for myself and my two kids, who were also sick before they were supposed to be and who also have never contracted official (PCR-test) Covid.
And I think Jimmy Kimmel is a Covid multi-timer too.
Anyway, it’s good to see Late Night Karma at work.
… This short post also gives me an opportunity to share this fun graphic that Covid contrarian scientist Dr. Harvey Risch posted at the Brownstone Institute’s Writer Group. One good graphic is worth a thousand words.
The White House and the Centers for Disease Control and Prevention (CDC) knew in April 2021 that the Pfizer COVID-19 mRNA vaccine was linked to heart damage on an unprecedented scale for a vaccine — but they hid that knowledge from the public while pushing vaccine mandates, according to emails obtained by DailyClout through a Freedom of Information Act (FOIA) request.
The emails show the White House communications team struggling to craft a cover-up message on email chains that included Dr. Anthony Fauci, then-director of the National Institute of Allergy and Infectious Diseases (NIAID) and chief medical advisor to President Biden; CDC Director Rochelle Walensky; Dr. Janet Woodcock, then-acting commissioner of the U.S. Food and Drug Administration (FDA), U.S. Surgeon General Vivek Murthy and Dr. Francis Collins, then-director the National Institutes of Health (NIH).
A number of high-level public health officials worked with upper-echelon leadership to craft a “Myocarditis Email” that minimized the relationship between COVID-19 mRNA vaccines and myocarditis,” said Amy Kelly, program director for the War Room/DailyClout Pfizer Documents Analysis Project.
According to Kelly, the officials included: Ian Sams, COVID-19 response and special assistant to the president and senior advisor and spokesman for the White House; Abbigail Tumpey, then-associate director for communication science for the CDC’s Public Health Infrastructure; and Dr. Dana Meaney-Delman, CDC lead on maternal immunization and CDC chief of Infant Outcomes Monitoring Research and Prevention Branch.
The FOIA emails were obtained by Edward Berkovich, one of 250 volunteer attorneys Kelly oversees on the DailyClout and War Room Project to analyze the court-ordered, FDA-released 450,000 pages of Pfizer’s records on its mRNA COVID-19 vaccine — records the drug maker tried unsuccessfully to keep private for 75 years.
The War Room-DailyClout Project was founded by bestselling author and journalist Naomi Wolf, a former advisor to the Clinton campaign, in collaboration with Steve Bannon, former advisor to President Trump and podcaster on “The War Room.”
In addition to volunteer attorneys, Kelly oversees approximately 3250 volunteer doctors, nurses, scientists and others who are reviewing the documents. They’ve issued 89 investigative reports, including the Oct. 18 report on the myocarditis cover-up evident in FOIA emails.
“Astonishingly, the emails reveal that the most senior of leaders, all the way up to the White House, knew about heart damage linked to mRNA vaccines,” Kelly said. “Yet they “colluded behind the scenes to conceal this side effect from the American people.”
Anyone can study the three FOIA releases of emails at dailyclout.io, Kelly said.
“What I think most important is to see who all is involved,” she said. “I believe 105 different people are on the emails, a whole slew of people at the White House, CDC, U.S. Department of Health and Human Services, NIAID, Pfizer, some children’s hospitals and organizations and some other external people,” Kelly said.
“My takeaway from seeing this is that everyone, all over the public health agencies, knew there was an issue” with myocarditis dangers linked to the COVID-19 vaccines, Kelly said. Yet “when you read through the emails, you see they are crafting messages to downplay the significance of myocarditis and the vaccines, all the the way up to the White House.”
“They said, ‘We’re seeing a myocarditis signal and we’re happy to share information with you,’” she said. “The CDC actually didn’t even respond to the first email as far as I can tell. So the Israeli Ministry of Health emailed again March 2, ‘Hey we’re seeing this myocarditis signal, we’re concerned, let’s discuss it if you want.’”
White House created 17-page script to ‘keep everyone on message’
The FOIA email trove was a frequent topic of discussion Saturday at the “Summit for Truth,” which brought together leaders of the health freedom movement at the Bethel Christian Fellowship church and community center in downtown Rochester, New York.
Wolf was the keynote speaker in a lineup that included Dr. Robert Malone, Dr. Ryan Cole, attorney Bobbie Ann Cox, and Brownstone Institute publisher and writer Jeffrey Tucker.
Wolf spoke about her journey from feminist icon to outcast from the liberal media establishment when she questioned the safety of the COVID-19 shots.
She has written two books on her experience investigating and reporting on the pandemic. They include, “The Bodies of Others: The New Authoritarians, COVID-19 and the War Against the Human,” and the forthcoming “Facing the Beast: Courage, Faith, and Resistance in a New Dark Age.”
During a panel discussion Saturday, Wolf called the White House involvement in a cover-up of vaccine dangers “absolutely shocking.”
Berkovich’s FOIA request was aided by “a whistleblower at the CDC,” Wolf said, who was “throwing the White House under the bus.”
“In addition to the pages he had asked for, he got 46 pages he didn’t request that showed the White House communications team was “freaking out at the highest levels in April of 2021, because news of blood clots and heart damage had reached them,” Wolf said.
“Instead of coming clean with the American people and pulling this injection off the market, they looped in Dr. Fauci, Dr. Collins, Dr. Walensky and created a script,” she said.
It was “a 17-page script, their word, which is wholly redacted, to keep everyone on message and downplay the dangers. And in fact if you recall from 2021, rather than pulling this injection off the market, they mandated it. They doubled down and mandated it.”
Wolf said the emails reveal “a massive crime.”
They show a template was prepared to email to “POTUS, which stands for president of the United States,” to keep the president up to date on the email discussions among the top U.S. public-health officials on myocarditis and vaccines, Wolf said.
“Dr. Wallensky was on the emails, Dr. Fauci, Dr. Collins,” she said. “The entire White House communications team was driving the discussion.”
“They were reacting to the fact that blood clots and heart damage had been presented to them at scale and that the American Association of Pediatrics was warning them about myocarditis in teens, a serious, sometimes fatal disease that needs constant management. Instead of coming clean with the American people… they doubled down and made a strategy to cover it up.”
Public-health officials went ahead with mandates for the Pizer COVID-19 vaccine, “knowing it was killing people,” Wolf said.
Dr. Peter McCullough, one of the most highly published cardiologists in the world, said the Pfizer COVID-19 vaccines should have been pulled from the market in January 2021, after “no more than 50 deaths” — the previous government standard to guarantee the safety of a biologic product.
McCullough said FDA records show the agency expected a myocarditis risk from the mRNA COVID-19 vaccines as early as Oct. 22, 2020.
“If they had reported these deaths, there would have been a three- to four-fold excess cardiovascular risk with Pfizer in the core slides at the Dec. 10, 2020 meeting and Pfizer would never have been approved,” he said.
McCullough said the myocarditis cover-up has killed untold thousands of Americans.
He pointed to his research paper with other scientists including Dr. William Makis. They performed a systematic review of “all published autopsy reports involving COVID-19 vaccination-related myocarditis” through July 3, 2023.
The paper concluded “there is a high likelihood of a causal link between COVID-19 vaccines and death from suspected myocarditis in cases where sudden, unexpected death has occurred in a vaccinated person.”
McCullough and colleagues concluded that “urgent investigation is required for the purpose of risk stratification and mitigation in order to reduce the population occurrence of fatal COVID-19 vaccine-induced myocarditis.”
Dr. Bruce Boros, a Key West, Florida cardiologist who was one of the first American physicians to use ivermectin for early COVID-19 treatment based on his resarch of the emerging literature, said recent studies show that the RNA from the COVID-19 vaccines “goes right to the heart.”
A study that applied the Moderna and Pfizer vaccine to heart muscle cells in culture “showed direct evidence that within 48 hours there was heart dysfunction, mechanical and electrical chaos,” Boros said.
Young athletes dropping dead from heart failure at unprecedented rates are “almost assuredly suffering” myocarditis symptoms brought on by the shots, he said.
“Everybody who received the shot had some damage to the heart muscle,” Boros said. “They knew it in the preclinical studies and they covered it up. All the signals were there, the FDA went ahead and approved it anyway.
“It’s all a money game, a eugenics game, and they’re continuing to say you need to get a booster,” Boros said. “Now every child in the world should get this shot for a virus that has been falsely normalized as dangerous when the risk, especially for children, is essentially zero when it comes to death,” he said.
“It saddens me,” Boros concluded. “We need to remember this was created as a bioweapon, and hold our government accountable.”
Mike Capuzzo is the managing editor of The Defender. He is a former prize-winning reporter for The Philadelphia Inquirer and The Miami Herald, a science writer, and a regional magazine founding editor and publisher who has won more than 200 journalism awards as a writer, editor and publisher.
People commonly ask me for “comprehensive” publications on vaccine side effects. It is fair to point out that the SARS-CoV-2 Spike protein is contained in the virus and it is uncontrollably produced by the mRNA and adenoviral DNA COVID-19 vaccines. Because the vaccines failed to stop COVID-19, most vaccinated persons have had the illness, thereby having multiple Spike protein exposures.
Parry, et al, published a comprehensive review on the litany of Spike-protein diseases that occur after its widespread distribution in the body. Here are some of their evidence based teaching points:
SARS-CoV-2 spike protein is pathogenic, whether from the virus or created from genetic code in mRNA and adenovector DNA vaccines.
Biodistribution rodent study data show lipid nanoparticles carry mRNA to all organs and cross blood-brain and blood-placenta barriers. Some of these tissues are likely to be impervious to viral infection; therefore, the biohazard is particularly from vaccination.
Lipid-nanoparticles have inflammatory properties.
The modification of mRNA with N1-methylpseudouridine for increased stability leads to the production of spike proteins for months. It is uncertain how many cells and from which organs mRNA spike proteins are produced, and therefore, the exact effective dose delivered per vaccine vial is unknown.
The long-term fate of mRNA within cells is currently unknown.
The mRNA and adenovector DNA vaccines act as ‘synthetic viruses’.
In the young and healthy, and even in many older individuals with vulnerable comorbidities, the encoding-based COVID-19 vaccines will likely transfect a far more diverse set of tissues than infection by the virus itself.
Evidence suggests reverse transcription of mRNA into a DNA copy is possible. This further suggests the possibility of intergenerational transmission if germline cells incorporate the DNA copy into the host genome.
Production of foreign proteins such as spike protein on cell surfaces can induce autoimmune responses and tissue damage. This has profoundly negative implications for any future mRNA-based drug or vaccine.
The spike protein exerts its pathophysiological effects (‘spikeopathy’) via several mechanisms that lead to inflammation, thrombogenesis, and endotheliitis-related tissue damage and prion-related dysregulation. Interaction of the vaccine-encoded spike protein with ACE-2, P53 and BRCA1 suggests a wide range of possible biological interference with oncological potential.
Adverse event data from official pharmacovigilance databases, an FDA-Pfizer report obtained via FOI, show high rates and multiple organ systems affected: primarily neurological, cardiovascular, and reproductive.
Pfizer and Moderna mRNA COVID-19 vaccines’ clinical trial data independently interpreted has been peer-review and published to show an unfavourable risk/benefit, especially in the non-elderly. The risks for children clearly outweigh the benefits.
Repeated COVID-19 vaccine booster doses appear to induce tolerance and may contribute to recurrent COVID-19 infection and ‘long COVID’.
“The SARS-CoV-2 pandemic has revealed deficiencies in public health and medicines regulatory agencies. A root cause analysis is needed for what now appears a rushed response to an alarming infectious disease pandemic. Treatment modalities for ‘spikeopathy’-related pathology in many organ systems, require urgent research and provision to millions of sufferers of long-term COVID-19 vaccine injuries. We also advocate for the suspension of gene-based COVID-19 vaccines and lipid-nanoparticle carrier matrices, and other vaccines based on mRNA or viral-vector DNA technology. A safer course is to use vaccines with well-tested recombinant protein, attenuated or inactivated virus technologies, of which there are now many for vaccinating against SARS-CoV-2.”
The Omission of Israeli Terrorism in the Occupied Palestinian Territories
By Karin Brothers | Global Research | December 6, 2014
… The Israeli settlements — all of which are illegal – have been identified as a major impediment to peace. The refusal of a major “global” terrorism report to name the Israeli settlers as one of the groups most responsible for terrorism not only misrepresents a major source of regional violence but exposes the Global Terrorism Index as a propaganda tool that supports a U.S. agenda.
In recent years, governments have been attempting to thwart terrorism by blocking supportive fund-raising. When it comes to Israeli settlements, however, the US and Canada actually encourage fund-raising by giving organizations (such as Christian Friends of Israeli Communities (CFOIC) and the Jewish National Fund) financial support in the form of donor tax-deductions.
Charities which provide funds for the Israeli settlements should be regarded as terror-financing organizations. They should not only lose their tax-deductible status, but they should be banned because they support the violation of international humanitarian law. The terror-financing laws that are being strictly enforced for Muslim charities should be applied to Christian and Jewish charities as well. … Read full article
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.