The Truth: No Vaccines Are Safe For Children
Dr Tess Lawrie, MBBCH, PHD | A Better Way to Health | September 10, 2023
This week the World Council for Health (WCH) issued an official caution against all vaccines on the childhood vaccination schedule. I’ve re-published the statement below.
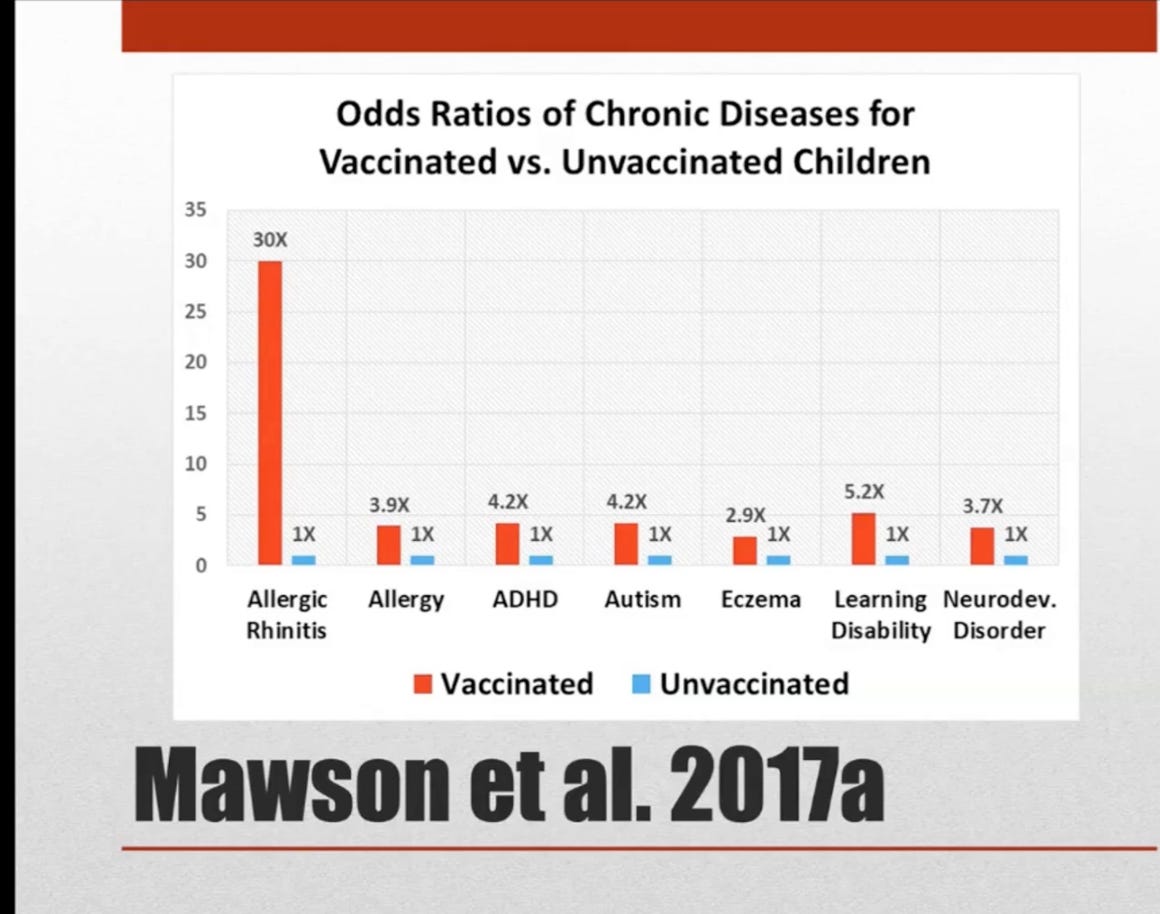
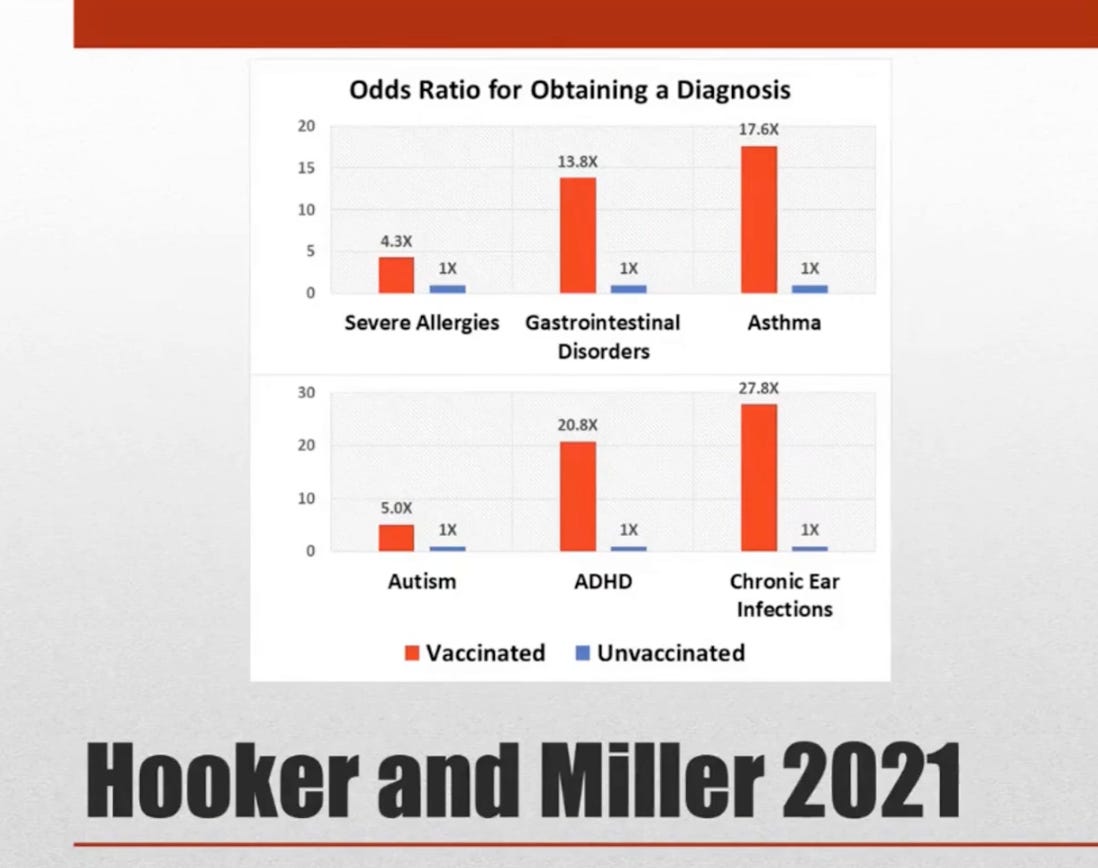
The following images have been taken from WCH General Assembly Meeting #101 in which Prof. Brian Hooker presented the latest research:



World Council for Health | September 5, 2023
The number of vaccines given to babies and children has increased dramatically without the necessary due diligence by regulatory authorities. Parents are urged to adopt a common-sense, ‘Safer to Wait” approach.
Growing international concerns about vaccine regulatory processes and vaccine safety have emerged following the widespread regulatory failure of Covid-19 vaccines. The Covid-19 crisis has demonstrated that regulatory bodies, once public watchdogs, are now at best incompetent and at worst have been deeply corrupted by pharmaceutical industry interests.
In the context of emerging revelations of regulatory body incompetence and corruption, e.g. The Perseus Report, the WCH Health and Science Committee notes that:
- Several research studies now indicate that vaccinated children have far worse health outcomes with higher rates of many chronic diseases than non-vaccinated children.
- The integrity of scientific research and the regulatory process of childhood vaccines, including the new nasal ‘flu’ vaccine, now being administered en masse in schools is in question.
- Pharmaceutical corporations have a long-standing history of misrepresenting products that cause injuries and deaths. Pfizer, for instance, has paid the largest criminal settlement in history for drug fraud. The childhood vaccination schedule provides these unscrupulous corporations with unregulated access to the bodies of our children.
- Modern society is experiencing unprecedented rates of autism, asthma, allergies, inflammatory bowel disease, diabetes, obesity, depression and more, for which the root cause/s have not been established.
- Much of what we have been told about the success of early vaccines, including smallpox and polio vaccines is emerging as untrue. Clean water, modern plumbing, hygiene, refrigeration, and improved nutrition are real factors that have correlated with the dramatic reduction in many infectious diseases over the past century.
- National regulatory agencies have never done the necessary evaluation to determine whether vaccines given to children alone or together according to the ever-expanding childhood vaccination schedules are associated with poor health outcomes compared with children who are not vaccinated.
- National regulatory agencies have been turning a blind eye to the mounting evidence linking childhood vaccination with autism that has emerged since a possible link was first suggested in 1998.
- National regulatory agencies have also been turning a blind eye to the mounting evidence linking childhood vaccination with other diseases, including asthma, allergies, and bowel disease.
- The vast majority of children find vaccination with needles painful and long-term psychological harms, including disruption to breastfeeding and maternal bonding, have not been properly evaluated.
- There are serious concerns among experts that existing childhood vaccines will be converted to mRNA technology, which has never been proven safe for use in vaccines for adults let alone children, and that this will be done without public awareness, consent and a robust research and regulatory process.
- With regard to Covid-19 vaccination, evidence from independent experts and official international databases show that the Covid-19 vaccines are not effective and are not safe, raising serious questions around the authorisation of the Covid-19 vaccines for babies and children.
In addition to these specific considerations, the burgeoning vaccination schedule for children needs to be viewed in the context of the following supranational developments in global health policy:
- The World Health Organisation (WHO) and its private and state stakeholders have financial and ideological interests in the provision of vaccines and has committed to providing 500 vaccines by 2030.
- The WHO and its stakeholders are working for the pharmaceutical industry and creating legislation that would give them the power to mandate injections by force for you and your children.
- The WHO supports gain-of-function research, facilitating the creation of dangerous pathogens as well as the vaccines to combat newly created pathogens, thus creating a self-perpetuating vaccine industry based on fear.
In the current circumstances, the World Council for Health urges parents to consider childhood vaccination very carefully and adopt a common-sense, “Safer to Wait” approach to the vaccination of your boys and girls.
For the sake of all children and a healthy society it is time that we all question our blind faith in vaccines, the corporations that produce them, and the regulatory bodies and supranational organisations that enable and profit directly or indirectly through their authorisation.
The World Council for Health will continue to bring you supportive information and resources to help you optimize your family’s health naturally. Be assured that reducing infectious disease and maximizing your children’s health is rooted in wholesome nutrition, good physical and mental hygiene, a healthy outdoor lifestyle and your unconditional love.
- WCH meeting #101, August 28th 2023. https://worldcouncilforhealth.org/multimedia/brian-hooker-vax-unvax/
- Anthony R. Mawson et al., “Preterm Birth, Vaccination and Neurodevelopmental Disorders: A Cross-Sectional Study of 6- to 12-Year-Old Vaccinated and Unvaccinated Children,” Journal of Translational Science 3, no. 3 (2017): 1-8, doi:10.15761/JTS.1000187.
- Anthony R. Mawson, et al., “Pilot Comparative Study on the Health of Vaccinated and Unvaccinated 6 to 12-year-old U.S. Children,” Journal of Translational Science 3, no. 3 (2017): 1-12, doi:10.15761/JTS.1000186.
- Brian Hooker and Neil Z. Miller, “Analysis of Health Outcomes in Vaccinated and Unvaccinated Children: Developmental Delays, Asthma, Ear Infections and Gastrointestinal Disorders,” SAGE Open Medicine 8, (2020): 2050312120925344, doi:10.1177/2050312120925344.
- Brian Hooker and Neil Z. Miller, “Health Effects in Vaccinated versus Unvaccinated Children,” Journal of Translational Science 7, (2021): 1-11, doi:10.15761/JTS.1000459.
- James Lyons-Weiler and Paul Thomas, “Relative Incidence of Office Visits and Cumulative Rates of Billed Diagnoses along the Axis of Vaccination,” International Journal of Environmental Research and Public Health 17, no. 22 (2020): 8674, doi:10.3390/ijerph17228674.
- Wakefield AJ, et al. Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children. The Lancet. 1998. doi.org/10.1016/S0140-6736(97)11096-0.
- Turtles All The Way Down. Vaccine Science and Myth. 2022. Editor: Zoey O’Toole. Foreword by Mary Holland.
- Kirsch S.If vaccines don’t cause autism, then how do you explain all this evidence? May 2023.
- Vax-Unvax. Let the Science Speak. August 2023. Robert F. Kennedy Jr and Brian Hooker, PhD.
- Countering the WHO’s “Big Catch-up” Global Campaign and Immunization Agenda 2030. WCH Statement. May 12, 2023.
- Rejecting Monopoly Power over Global Public Health. WCH Policy Brief. May 2023.
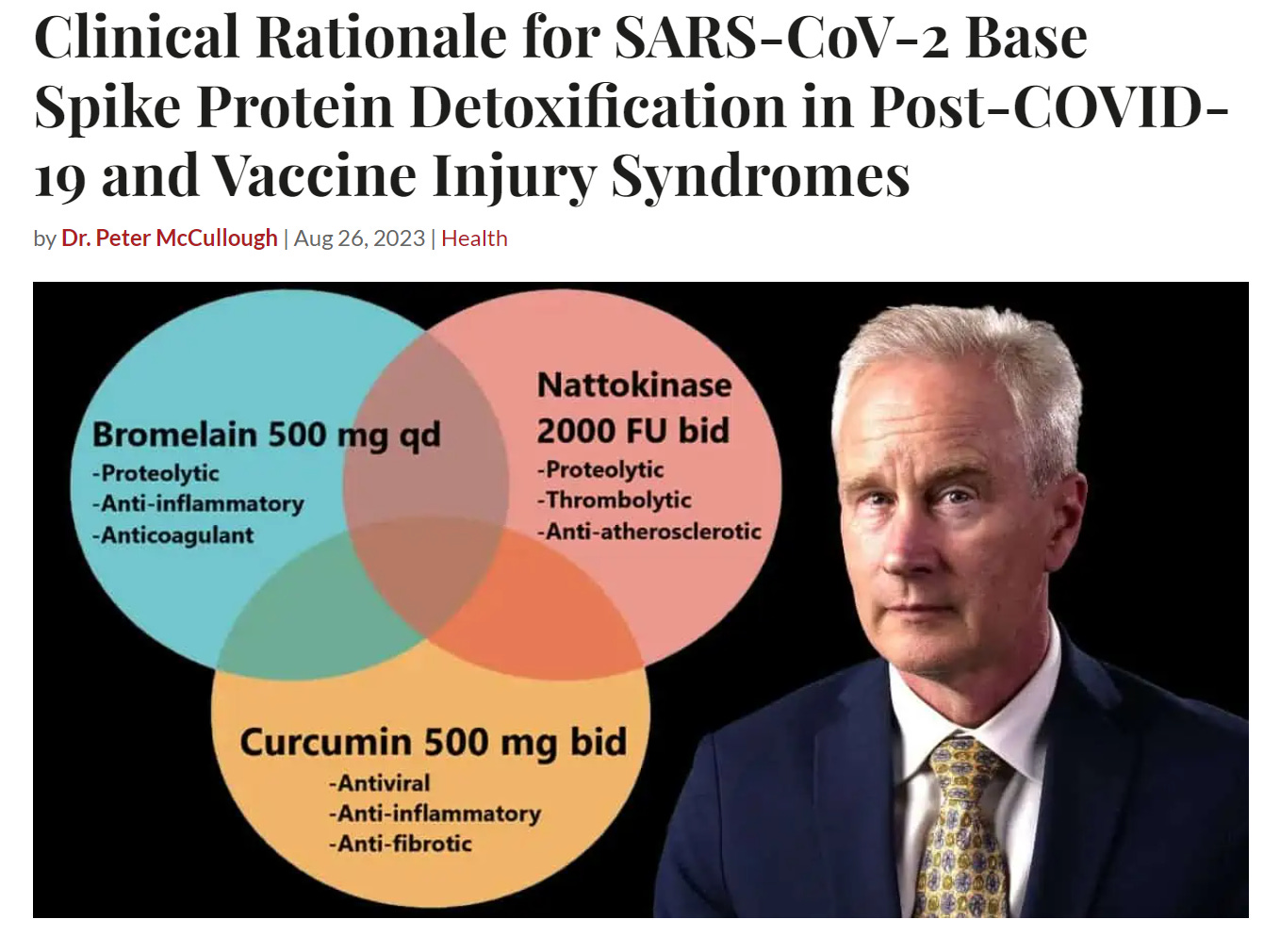
Bio-Pharmaceutical Censorship Complex Attacks Spike Detoxification Protocol
Syndicate Fact Checkers Confirm Empiric Regimen is Valuable for Post-Acute Sequelae after SARS-CoV-2 Infection and COVID-19 Vaccination
By Peter A. McCullough, MD, MPH | Courageous Discourse | August 31, 2023
It took less than a day since our Base Spike Protein Detoxification Protocol was published for the Biopharmaceutical Complex to come out with syndicate social media allies discrediting the most hopeful news long-COVID and vaccine suffers have heard since the start of their misery.
Syndicate fact checker Science Feedback, issued an unsupported false counterclaim on Instagram given below.
![]()
Science Feedback, a science and climate blogging organization with no foundation in peer-reviewed medical publications, is not advised by prominent physicians working in the COVID-19 field. Their major donor is former Microsoft and Apple executive Eric Michelman who is also a noted Democrat supporter, donating money to the Presidential campaigns of Barack Obama and Joe Biden. Michelman is also a climate change activist, founding a climate change advocacy organization and publicly supporting a carbon tax.
LinkedIn pulled a post indicating the COVID-19 vaccine causes more post-acute sequelae than SARS-CoV-2 which is my clinical opinion supported by the data. Base Spike Detoxification is an approach a to both problems. LinkedIn uncredentialed anonymous content moderators obviously disagreed and continue to push the false narrative indicating that long-COVID is unassailable and the only answer is more genetic shots.

I have found it interesting that the fact checkers have never made claims against a myriad of drugs or supplements that were ineffective during the pandemic. They have exclusively targeted therapies with preclinical and clinical studies demonstrating signals of benefit and acceptable safety (iodine/xylitol nasal washes, vitamin D, hydroxychloroquine, ivermectin, budesonide). In a perverted way, the Biopharmaceutical Complex has confirmed Base Spike Detoxification is the path forward for so many patients suffering from long-COVID and or regretting the jab.
Peter A. McCullough, MD, MPH
President, McCullough Foundation
Dr. Pierre Kory: New York Times Guide to Fall Vaccine Shots Is ‘Disinformation’
By Michael Nevradakis, Ph.D. | The Defender | September 6, 2023
The New York Times on Sept. 1 published a “guide to fall vaccine shots,” which included recommending the general public get COVID-19, flu and RSV (respiratory syncytial virus) vaccines, and infants 6 months and older receive COVID-19 shots this fall.
Written by Times senior writer David Leonhardt, the guide warns about rising COVID-19 cases and the approaching flu season, before offering, “The good news is that there are vaccines and treatments that reduce risks from all major viruses likely to circulate this season.”
According to the Times, “This year, we should take a broader approach,” rather than “obsess over COVID.”
Peter Hotez, M.D., Ph.D., dean of the National School of Tropical Medicine at the Baylor College of Medicine — described by the Times as a “vaccine expert” — echoed that appeal. “It’s not only COVID you have to think about,” he said.
Hotez, Nirav Shah, M.D., J.D., principal deputy director of the Centers for Disease Control and Prevention (CDC), and other public health officials and experts quoted by the Times recommended Americans prepare for the upcoming fall and winter by getting the trio of COVID-19, flu and RSV vaccines.
None of these experts, however, addressed any of the potential safety risks posed by these vaccines.
Medical and public health experts who spoke with The Defender took a different view and questioned the Times’ guide, citing concerns about the safety and efficacy of vaccines for respiratory illnesses.
“Vaccines against respiratory illnesses have failed miserably,” said cardiologist Peter McCullough M.D., MPH. “America is wary of vaccines at this point, wanting to get on with life free of menacing vaccines, and are willing to seek early treatment, which is always the best way to handle infections, vaccinated or not.”
Pediatrician Dr. Liz Mumper, president and CEO of the Rimland Center for Integrative Medicine, told The Defender, “There have been no studies examining the effects of giving RSV vaccine, flu vaccine and COVID vaccine at the same time.”
“If you follow the advice in The New York Times article,” Mumper said, “be aware that your child will be part of post-marketing experimentation.”
Times still pushing vaccine propaganda
According to the Times, “The best defenses against COVID haven’t changed: vaccines and post-infection treatments,” which are “especially important for vulnerable people, like the elderly and immunocompromised.”
The federal government is “on track” to approve updated COVID-19 shots, designed to combat recent variants, in mid-September, the Times reported. Once they are available, “all adults should consider getting a booster shot.”
“COVID can still be nasty even if it doesn’t put you in the hospital,” the Times states. “A booster shot will reduce its potency.”
Hotez resurrected a claim heard often during 2021 and 2022, telling the Times, “Overwhelmingly, those who are being hospitalized are unvaccinated or undervaccinated.”
Experts who spoke with The Defender disagreed.
Harvey Risch, M.D., Ph.D., professor emeritus and senior research scientist in epidemiology (chronic diseases) at the Yale School of Public Health, citing data from U.K. Public Health, said, “All-cause deaths ages 18+ are disproportionately among vaccinated people, whether one, two or three doses, compared to unvaccinated people.”
“The statistic quoted by Dr. Hotez is false,” Risch said.
Brian Hooker, Ph.D., senior director of science and research for Children’s Health Defense (CHD) said, “The new booster simply hasn’t been tested to affirm any assertion of protection. The original trials on children were laughable as they looked at antibody titers rather than actual disease prevention.”
McCullough told The Defender, “The COVID-19 vaccines have been a safety debacle with record cases of myocarditis, blood clots, stroke, and all-cause mortality.”
Despite the injury and mortality reports and the Times’ admission that the risk of COVID-19 to young children is “very low,” Shah nonetheless recommended children as young as 6 months of age get the COVID-19 booster shots this fall.
“Do you want to see your grandpa … [and] grandma?” Shah asked in the Times. “Are you really sure you’re not going to give COVID to them?”
Experts who spoke with The Defender refuted Shah’s advice.
Dr. Pierre Kory, president and chief medical officer of the Front Line COVID-19 Critical Care Alliance (FLCCC), said “There is no medical justification for a healthy 6-month-old or older child to be vaccinated for COVID-19,” adding:
“There is so little data available on the safety of the COVID-19 vaccine in children that to give blanket recommendations like Shah is doing creates an unnecessary risk to children’s health.
“We simply do not know enough about the COVID-19 vaccines to make such broad recommendations. Additionally, COVID-19 is highly treatable in children and poses very little risk to a healthy child.”
Mumper told The Defender, “Any official who advocates that children take a vaccine to protect grandparents has not read the medical literature carefully.” She said, “After doing a deep dive on the risks and benefits of COVID vaccines in children, I remain steadfastly opposed to their use in healthy children,” adding:
“Any immunity from COVID shots is short-lived and follows a period of immune suppression. Very worrisome adverse events like inflammation of the heart, triggering autoimmunity, interfering with autonomic functions and reproductive toxicity are well described in the medical literature.”
Not all countries following suit
Some countries began limiting COVID-19 vaccination for children last year. In April 2022, Denmark ended its blanket COVID-19 vaccination recommendation, including for children.
Now, Denmark recommends “booster-vaccination” only for people “aged 50 years and above and selected target groups.”
Earlier in 2022, public health authorities in Sweden and Norway opted not to recommend COVID-19 vaccines for children between the ages of 5 and 11.
Sweden now recommends COVID-19 vaccination only for those 50 and above (18 and above for high-risk groups), while Norway is still only recommending COVID-19 vaccines for those 65 and older (and as young as 5 for high-risk groups).
In March of this year, the World Health Organization (WHO) said healthy children and adolescents ages 6 months to 17 years have a “low disease burden” and are therefore low priority for vaccination.
In June, Australian public health officials said Moderna’s COVID-19 vaccine is “no longer available” for children under 12, and in January, U.K. public health authorities ended their booster program for those under 50.
COVID vaccine recommendations ‘not science, not medicine, not public health’
Dr. Meryl Nass, an internist and member of CHD’s scientific advisory committee, told The Defender that while public health authorities and the media continue to recommend COVID-19 vaccines, none of them have been fully licensed in the U.S., as all such vaccines are available under Emergency Use Authorization (EUA) only.
In May 2022, the U.S. Food and Drug Administration (FDA) said that COVID-19 vaccines for kids under 6 would not have to meet the agency’s 50% efficacy threshold required to obtain an EUA.
CDC data released in September 2022 showed that more than 55% of children between 6 months and 2 years old had a “systemic reaction” after their first dose of the Pfizer-BioNTech or Moderna COVID-19 vaccines.
“The CDC, criminally, claims the (authorized) vaccines are ‘safe and effective,’” Nass said, adding:
“That is a term of art that is only allowed to be used for licensed vaccines and drugs. No licensed COVID-19 vaccine is available in the U.S. Public health is supposed to balance benefit and risk.
“This is not science. Not medicine. Not public health.”
Flu vaccines have demonstrated ‘declining efficacy’
According to the Times, “The most immediate step worth considering involves R.S.V.” On Sept. 5, the CDC issued a health advisory warning of rising RSV cases in parts of the U.S., particularly among children and babies.
Last month, the CDC signed off on the first-ever monoclonal antibody vaccine Beyfortus for the prevention of RSV, for babies up to 8 months old.
Also last month, the FDA approved an RSV vaccine for pregnant women, despite concerns raised by some medical experts about premature births identified during clinical trials. In May, the FDA approved Pfizer’s Abrysvo and GlaxoSmithKline’s Arexvy RSV vaccines for people 60 and older.
The Times quoted Ashish Jha, M.D., MPH, former White House COVID-19 adviser and now dean of Brown University’s School of Public Health, who said, “If you’re 60 or over, you don’t want to get into November without having an RSV vaccine.”
And though there is no RSV vaccine approved for administration to children, the Times said that “parents may want to ask their pediatrician” about monoclonal antibody treatment for children under 8 months of age.
According to Hooker, “the RSV vaccine given to pregnant women could not even make a 20% threshold for protection (as specified by the FDA) against lower respiratory RSV infection.”
Supporting the push for the flu vaccine, the Times and experts such as Jha said, “The flu officially kills about 35,000 Americans in a typical year,” but “the flu’s toll would be lower if more people got a vaccine shot,” noting that “In recent years, less than half of Americans have done so.”
Jha added, “We underestimate the impact that respiratory viruses have on our population. The flu can knock people out for weeks, even younger people.” Jha pointed out that flu can make heart attacks and strokes more common as well.
Kory, however, told The Defender that the COVID-19 vaccines have made people more susceptible to other respiratory illnesses, like the flu and RSV:
“In my practice, we treat many vaccine-injured patients who are now more susceptible to the flu, RSV and many other viruses. The COVID vaccines cause many to present as if they have an autoimmune disease and now respond with more severe symptoms to common viruses like the flu.”
Risch, meanwhile, said, “Traditional flu vaccines are considered to be safe for most people” and may be a “reasonable” option for them, but “this should be discussed with one’s healthcare provider.”
“The flu vaccines seem to have had declining benefit over the last 10-15 years, to the point now that they may confer only a 30% benefit,” Risch added.
And according to Hooker, “The flu shot is also notoriously bad at protection against the flu and there are very few data regarding this season’s flu shot efficacy.”
‘Ludicrous’ public health messaging
Shah’s recommendation that children as young as 6 months get a COVID-19 shot this fall follows in a long line of questionable advice and claims disseminated by public health officials, some of which were later contradicted.
In a May 2021 MSNBC interview, Dr. Anthony Fauci, then-head of the National Institute of Allergy and Infectious Disease (NIAID), said:
“Although you don’t like to see breakthroughs, the fact is, this is one of the encouraging aspects about the efficacy of the vaccine. It protect you completely against infection. If you do get infected, the chances are that you’re going to be without symptoms, and the chances are very likely that you’ll not be able to transmit it to other people.”
Fauci’s statements, however, failed to account for the many examples of breakthrough infections with severe symptoms and hospitalization.
After years of official “safe and effective” claims, in YouTube’s new “medical misinformation” policy introduced Aug. 15, “Claims that any vaccine is a guaranteed prevention method for COVID-19” are prohibited. Fauci’s videos from 2021, notably, are still up on YouTube.
In April 2020, Fauci said that remdesivir will become the “standard of care” for treating COVID-19. But numerous victims of COVID-19 hospital protocols prescribed by the CDC have come forward in recent months claiming that remdesivir was administered without permission of the patients or their families and contributed to further injury or death.
Similarly, former CDC Director Rochelle Walensky said in March 2021 “Our data from the CDC today suggests … that vaccinated people do not carry the virus, don’t get sick … can’t transmit it to others.” She doubled down on these statements during a House Select Subcommittee on the Coronavirus Pandemic hearing in June, asserting that her statement “was generally accurate.”
Hooker said these statements were “obviously patently false, as the vaccines distributed in the U.S. at that time [in 2021] were not tested for transmission and there was evidence of ‘breakthrough’ infections even in the clinical trials.”
“This obviates any protection to ‘Grandma and Grandpa’ through children getting vaccinated against COVID-19,” Hooker added.
Also in 2021, Walensky recommended wearing pantyhose over a mask to ensure a tight fit.
Nass called such public health messaging “ludicrous,” noting that Walensky’s pantyhose recommendation “quickly disappeared” because it “had connotations the CDC was not willing to deal with.”
Kory criticized the Times’ fall vaccine guide, characterizing it as an example of “disinformation.”
“The New York Times is carrying the disinformation that continues to come from the CDC and other government health agencies,” he said. “This is one of the reasons that the public continues to lose trust in the media and our government.”
As a result, public health officials “create a mockery of how medical and scientific evidence is used to inform patient care decisions and public health policy,” Kory said.
Other experts who spoke with The Defender suggested taking vitamins to boost one’s immune system, rather than a series of vaccinations.
“For the immune system to defend against respiratory viruses, all people should take daily vitamin D to achieve blood levels of 50 or greater,” Risch said. “This is typically 5,000 units per day for a 150-lb person, but can be adjusted up or down according to body weight.”
“Serious RSV infections generally occur only in the youngest young and the oldest old. People in these categories should discuss this with their doctors,” he added.
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Unvaxxed Haiti Recorded 0% Covid Deaths

By Hunter Fielding – N/A – September 5, 2023
The vast majority of the population of Haiti is unvaccinated for COVID-19 but the impoverished Caribbean nation recorded virtually no deaths from the virus.
Haiti remains one of the least vaccinated countries in the world while also showing the lowest Covid death rate.
As of the end of April, just 254 people have died in Haiti from what authorities agree constitutes Covid, according to reports.
However, this figure is likely overblown considering SARS-CoV-2 has never even been isolated and proven to exist.
Compared to the United States, which currently has a COVID-19 death rate of around 1,800 per one million people, Haiti has a Covid death rate of just 22 per one million people, or 0.0022% – basically 0 percent.
NPR admits in a report about Haiti that Covid restrictions were never enforced there.
Nobody there wears a mask, people are mostly unvaccinated, and daily life is normal with busy and crowded buses and markets.
For most Haitians, the pandemic never happened.
“And Haiti hasn’t yet administered a single COVID-19 vaccine,” NPR‘s Jason Beaubien further reveals.
It turns out that Haiti had its own version of Tony Fauci, a man named Dr. Jean “Bill” Pape, who headed up a commission during the “pandemic” to deal with the fallout. In the end, however, the commission was dissolved because Haiti was, and continues to be, COVID-free.
“The reason mainly is because we have very, very few cases of COVID,” Pape said about why the commission was ultimately disbanded.
GHESKIO, the local health agency that Pape heads, also closed its COVID units last fall due to a lack of patients.
While the Western world is stricken with hordes of “fully vaccinated” people who are now sick as dogs, Haiti is back to normal thanks to its rejection of the shots.
“Sometimes it’s two, sometimes zero, sometimes it’s 20 cases,” Pape said.
“But we are not seeing a second wave as we thought would happen.”
Unlike much of the rest of the world, Haiti remained open during the “pandemic.”
Outdoor markets were never closed, and people there continued working because sheltering in place and remote employment are not things that the average Haitian can afford.
“Most people don’t wear a mask,” Pape added, noting that Haitians continued working as normal throughout the pandemic because “if they don’t work, they don’t eat – their family doesn’t eat.”
When AstraZeneca tried to peddle its COVID injection in Haiti, the Haitian government denied a shipment of it.
It turns out that the medical community in Haiti heard about all the “rare” side effects of the jab and thus rejected it.
“COVID did not impact us as badly,” said Dr. Jacqueline Gautier, who serves on the national technical advisory group on COVID vaccination in Haiti.
“People don’t think [the vaccine] is worth it, actually.”
Another factor that makes Haiti an incredible success story compared to other nations is the fact that its population is very young.
The average age in Haiti is around 23, while in the United States, it is closer to 40.
Younger people tend to have stronger immune systems than older people.
And without COVID jabs to destroy them, Haiti’s millions of unvaccinated people fared well compared to the rest of the world.
“Also, there are many other major problems the country is facing,” Gautier added.
“So people don’t see COVID as our major, as a major, problem for us.
“And who can blame them?”
South Africa ‘held to ransom’ over Covid vaccine deals – NGO
RT | September 7, 2023
An investigation into South Africa’s procurement of Covid-19 vaccines has found that the country’s health officials purchased supplies from global pharmaceutical companies at inflated prices compared to many Western nations.
The Health Justice Initiative (HJI), an independent body formed during the pandemic to monitor the South African healthcare system’s handling of the crisis, said during a news conference this week that the government was “bullied” into accepting unfavorable vaccine deals via one-sided “ransom negotiations.”
“The [vaccine] contracts contain unusually hefty demands and conditions, including secrecy, a lack of transparency, and very little leverage against late or no delivery of supplies or inflated prices,” the HJI said in a statement on Tuesday. It added that this system led to “gross profiteering” and an “inability to plan properly in a pandemic.”
The terms agreed by South Africa’s government with companies such as Pfizer and Johnson & Johnson for the purchase of Covid-19 vaccines were the subject of a legal challenge by the HJI last month under the country’s Promotion of Access to Information Act.
A Pretoria court subsequently ruled in favor of the HJI, compelling the South African government to release the vaccine contracts in the interest of transparency and accountability.
The documents detailed that South Africa was liable for vaccine payments of $734 million. The terms of the agreements included no guarantees of a timely delivery or penalties for late arrival. It was also found that Johnson & Johnson charged South Africa $10 per dose of its vaccine – some $1.50 more than EU countries paid.
“The country was forced to overpay for vaccines, paying 33% more than the African Union price from the Pfizer-BioNTech vaccine and paying the Serum Institute of India 2.5 times more for a generic version of the Oxford-AstraZeneca vaccine compared to the United Kingdom,” the HJI said.
The group claimed that the government’s practices throughout the pandemic “signals a dangerous precedent for future pandemic readiness,” and that “we were bullied into unfair and undemocratic terms in contracts that were totally one-sided. Put simply, pharmaceutical companies held us to ransom.”
According to publicly available data, South Africa has recorded 102,595 deaths from Covid-19 since the start of the pandemic. As of May 2023, approximately 65% of South Africans have received a vaccine against the virus.
Viral RFK Jr. Video Gets Deleted By “X”: Here’s What They Didn’t Want You to See
The Pfizer clinical trials were a disaster. Robert F. Kennedy, Jr. explains why.
The Vigilant Fox | September 4, 2023
“Freedom of speech, not reach,” is taking effect more than ever as Twitter (“X”) regresses to its 1.0 days. Ever since Elon Musk hired CEO Linda Yaccarino, who has close ties to the World Economic Forum, things have taken a turn for the worse.
In short, “lawful but awful” accounts and external links (especially Substack) are getting brutally deboosted. And permanent suspensions, which were promised to be reserved for unlawful speech only, have made a big comeback.
Now, Twitter (“X”) is taking further action by making undesirable videos unplayable.
What type of videos in particular? Well, mine…
After this article garnered lots of attention, the video in the tweet is now working for many people, but not everyone. X has not personally reached out or made a comment on why the video became unplayable several hours after it was uploaded.
Users also reported X was “blocking” them from retweeting. Now, that’s something reminiscent of 2021 and early 2022 — BEFORE Elon took over the platform. So, this is concerning.
So, what did Robert Kennedy Jr. say that crossed the line?
The video was a clip of RFK Jr. breaking down the Pfizer clinical trials with podcast host Brian Rose. And what he exposed, according to Pfizer’s own data, was that people who received Pfizer’s COVID vaccine showed a 23.5% GREATER likelihood of dying than the placebo group after six months.
Here’s the full breakdown, per Robert F. Kennedy, Jr.:
• In the Pfizer clinical trials, they gave 22,000 people two COVID injections and 22,000 people fake vaccines.
• Of the 44,000 in total, one person died of COVID in the vaccine group, and two people died of COVID in the placebo group. So Pfizer, with the misleading measure of relative risk reduction, called their vaccine “100% effective” because two is 100% greater than one. But from the angle of absolute risk, it took 22,000 vaccines to save just one life from COVID.
• And over a 6-month period, 21 of the vaccinated people died of all causes, whereas only 17 people died in the placebo group, a 23.5% difference.
So, what was killing those people in the vaccine group?
“It was cardiac arrest,” answered Kennedy.
“There were five cardiac arrest deaths in the vaccine group and only one in the placebo group. What that means is that if you take that vaccine, you’re [five times] more likely to die from a fatal cardiac arrest over the next six months than if you don’t. What it also means is that for every life they save by preventing a death from COVID, they are killing four people from cardiac arrest.”
“The all-cause mortality of the vaccine group was 23% higher than the all-cause mortality of the placebo group. And what do we have today currently running in the US for excess mortality? 23%, according to our numbers. I just find that curious.”
So when Pfizer presented this data to the FDA, the FDA was supposed to assess all-cause mortality, give Pfizer’s vaccine a failing grade, tell them to make a better product, and not come back until they could show it saves more lives than it kills. But instead, they rubberstamped the shots through, gave them the green light, and fast-tracked a vaccination campaign that inoculated the world with 13.46 billion doses of this stuff.
Data analyst Edward Dowd corroborated Kennedy’s findings when he did his own deep dive on the Pfizer clinical trials.
Spike Protein Linked to Alzheimer’s Acceleration
SARS-CoV-2 Spike amyloid fibrils specifically and selectively accelerates amyloid fibril formation
BY JOHN LEAKE | COURAGEOUS DISCOURSE | SEPTEMBER 5, 2023
During the last two years, several people in my broad social circle have told me that one or more of their parents seemed to experience a rapid cognitive decline during this time period. A British friend’s recent account is typical. On a trip home to visit her parents, she was stunned to learn that her father was just diagnosed with Alzheimer’s, as he’d seemed perfectly alert, engaged, and intellectually lively just two years ago. What could account for his precipitous decline? She confirmed that her father had received COVID-19 vaccines and multiple boosters since early 2021.
This anecdote was consistent with my general perception that the SARS-CoV-2 spike protein—to which our bodies are exposed from COVID-19 infection and COVID-19 vaccination and boosters—may be accelerating underlying, inflammatory disease processes such as arteriosclerosis and Alzheimer’s. In this scenario, a man who was destined to have a fatal heart attack at 74 due to his underlying arteriosclerosis has one at the age of 54 because the spike protein produced by the COVID-19 vaccine and boosters, has markedly accelerated the disease. A similar acceleration of the Alzheimer’s disease process of amyloid fibril formation in the brain struck me as plausible.
With my British friend’s anecdote fresh on my mind, I read with keen interest a paper—published on a preprint servicer by Larson, Hellstrand, et al. at Linkoeping University in Sweden—titled SARS-CoV-2 Spike amyloid fibrils specifically and selectively accelerates amyloid fibril formation of human prion protein and the amyloid β peptide.
As is now typical of our infernally corrupt academic medical establishment, the authors only mention exposure to the SARS-CoV-2 spike during COVID-19 infection, and mention nothing about massive, uncontrolled exposure to the spike from COVID-19 vaccines and boosters.
As Dr. McCullough frequently emphasizes, those who are at the greatest risk of developing disease syndromes caused by the SARS-CoV-2 spike protein are people who are repeatedly exposed to it through the vaccine, boosters, and infections. Because the COVID-19 vaccines do NOT prevent infection and may even impair natural immunity, those who continue to receive these shots are simply increasing their repeated exposure to the dangerous spike.
Have we only seen the tip of the iceberg for mRNA vaccine harms?
A slow-motion car crash

Health Advisory & Recovery Team | September 5, 2023
To those of us well-versed in the biology and emerging safety data relating to the injections referred to as “covid vaccines”, what is playing out before us is like a slow-motion motorway pile-up: we can see it unfolding, causing immense harm, have no idea when it will stop, and feel powerless to do much about it.
At present, it is unknown for how long this ghastly experiment will continue and how much further harm will be caused.
However, unfortunately there are reasons to believe the following may well be the case:
- It will take much longer for the harms caused to be acknowledged by the “establishment” and so the injections will continue to be administered for some time yet – albeit to smaller and smaller groups as time progresses, and with varying degrees of enthusiasm in different locations.
- Even if the injections were to stop now, it is unknown how much the harms caused thus far have actually come to light, and how much may manifest over the ensuing years or even decades.
One category of reasons for the above is essentially political. We are referring here to the complete failure on the part of those we previously relied upon to ensure pharmaceutical interventions are safe. The reasons for this are willful blindness on the part of our regulatory authorities, combined with the by now rather obvious capture of these institutions by two different interested parties:
- Politicians who will apparently stoop to anything, including installing transnational coordinated censorship regimes, to keep their monumental errors hidden; and
- Big Pharma, desperate to ensure that their bonanza continues as long as possible.
But as well as the above there are some inherent biological reasons which may hinder and delay the ending of this unprecedented catastrophe.
For a variety of reasons which are listed below, many uncertainties remain concerning the biological action of repeated doses of the mRNA products. However, what is known suggests that many of the harms they cause are mediated by inflammatory and autoimmune processes induced (potentially) throughout the body.
To recap the principal mode of action, the lipid nanoparticles carry mRNA into some of the recipient’s cells. These cells express spike protein – which is foreign to the body. The body’s immune system creates antibodies to that protein, as well as attacking and destroying the cells which express the protein.
In contrast to the original claims made – that the product would be broken down in the deltoid (shoulder) muscle with little or no distribution throughout the body, it turns out that the product DOES become widely distributed – potentially to every organ system. Of course, this should not have been surprising, since the whole point of the lipid in the lipid nanoparticles is to make them able to cross membranes and become distributed, to help with their original role as conveyors of targeted drugs to cancerous cells.
Moreover:
- The amount of spike protein produced is uncontrolled and uncontrollable, as is the duration over which it is produced. High levels of spike antibodies have been found many months after injection, suggesting continued creation of the protein.
- The spike protein produced has inbuilt differences compared to the natural version – the replacement of uridine by pseudouridine – designed to ensure the mRNA is less degradable. Other changes (eg codon optimisation) may well alter the folding characteristics of the protein produced – with unknown consequences.
- It is thought that the spike protein my translocate to the nuclei of cells… cancer
- The repeated creation of spike from multiple injections may have deleterious effects, both on the ability to fight similar viruses (so-called “tolerance” created through changing the type of antibody created) through to immune exhaustion (reducing the body’s ability to fight other pathogens or cancers)
- The LNPs themselves (notwithstanding their “payload”) may well be pro-inflammatory in themselves…
- The significance of above-tolerance levels of DNA contamination left-over from the bacterial plasmids used in the high-volume manufacturing process are as yet unknown.
Much of the harm observed appears to be inflammatory or auto-immune in nature. Both these processes are usually chronic, not acute problems. It is perfectly possible that once started, they continue for months or even years. Notably, chronic inflammation is thought to have a central role in many of the chronic pathologies increasingly suffered by Westerners over the past few decades.
Hence the tail of visible harm could manifest over a long timeframe. Moreover, because chronic inflammatory and autoimmune processes, by their nature, build slowly over time, the individual is likely to become habituated to ill effects, until a critical event occurs after some longer period.
A good example of this is with coronary artery disease. It is thought that inflammation is an important part of the pathophysiology in which a “plaque” builds up in the arterial wall. This may be asymptomatic until it ruptures causing a total blockage resulting in a “heart attack”. If the injections are accelerating this inflammatory process, the course of the pathological process may appear identical to that previously seen in many people, although it has been brought on and accelerated beyond what that person would otherwise have experienced; however, because it is within the range of possible or even probable illnesses observed, it gets dismissed as “one of those things”.
Cigarette manufacturers used to deny their products caused lung cancer by pointing out non-smokers who suffered the same fate. It was, in fact, only by rigorous epidemiological analysis that the link could be unequivocally proven. For the covid injections, it is deeply concerning that authorities seem to be doing everything possible to hinder access to the data which would permit such analyses to be performed.
Another reason why harms may be difficult to identify is that in some cases the pathological processes may be merely reducing physiological reserve, something which can go unnoticed for years or decades. Most of the body’s systems have significant inbuilt redundancy, which is why a kidney, or a significant part of the liver, can be lost while still maintaining good physiological and biochemical control. But if someone loses a kidney, they are more likely to suffer renal failure as they get older and the efficiency of their kidneys declines, and the available reserve falls away. Likewise, if part of the heart is damaged when young (eg through myocarditis), they may well make a full recovery in the short term in the sense of being physiologically normal, but be more vulnerable to suffering from heart failure (where the heart can’t pump blood around the body sufficiently) after losing some more heart muscle tissue after – say – a heart attack in middle age.
Finally, it should be noted that because of the wide distribution throughout the body (something rather obvious given the wide range of reports in the various adverse event databases), the harms appear to be manifesting in an extremely wide variety of symptoms and disorders. These will be problematic to diagnose, requiring lengthy and complex investigation, with multiple pathologies being possible. Such profiles of types of harms have not generally been observed with pharmaceutical products before; in most cases, the adverse effects are more limited in scope, and more closely temporally related to dosing (though there are some exceptions).
In conclusion
It is not possible to say whether we are at the beginning, or near the end of, the harms caused by these agents.
A combination of what may be termed “political” reasons, together with the inherent biological characteristics of the mRNA “vaccines”, all mitigate against the injections being identified and accepted anytime soon as being the causative agent of significant and sustained harms being experienced by an unacceptably large number of people.
Moreover, it remains likely that they will continue to be administered for some time yet – at least to certain groups in certain places – prolonging and exacerbating the harms already caused.
Featured Video
Chinese jet fuel and the myth of energy independence
or go to
Aletho News Archives – Video-Images
From the Archives
The Dirty Little Secret behind the “Global Terrorism Index”
The Omission of Israeli Terrorism in the Occupied Palestinian Territories
By Karin Brothers | Global Research | December 6, 2014
… The Israeli settlements — all of which are illegal – have been identified as a major impediment to peace. The refusal of a major “global” terrorism report to name the Israeli settlers as one of the groups most responsible for terrorism not only misrepresents a major source of regional violence but exposes the Global Terrorism Index as a propaganda tool that supports a U.S. agenda.
In recent years, governments have been attempting to thwart terrorism by blocking supportive fund-raising. When it comes to Israeli settlements, however, the US and Canada actually encourage fund-raising by giving organizations (such as Christian Friends of Israeli Communities (CFOIC) and the Jewish National Fund) financial support in the form of donor tax-deductions.
Charities which provide funds for the Israeli settlements should be regarded as terror-financing organizations. They should not only lose their tax-deductible status, but they should be banned because they support the violation of international humanitarian law. The terror-financing laws that are being strictly enforced for Muslim charities should be applied to Christian and Jewish charities as well. … Read full article
Blog Roll
 Aletho News
Aletho News- Chinese jet fuel and the myth of energy independence
- Ukraine Sea Drone Fired From Libya Hit Russian Tanker in Mediterranean
- IRGC: Iranian forces launched no attacks during ceasefire hours
- Trump Administration Moves To Automate U.S. Military Draft Registration
- Spain orders reopening of Tehran embassy, condemns Israel’s carpet bombing of Lebanon
- Israel faces ‘unsustainable’ strategic crisis following 40-day war against Iran: Analyst
- Iran restricts Hormuz access to 15 vessels per day under ceasefire terms: Report
- The ‘Opposition Party’ Has Done Nothing to Stop the Iran War and Much to Goad Trump Into Continuing It
- Moscow backs Tehran on status of Lebanon in US-Iran deal
- How UK Regulator Ofcom Quietly Bypassed International Law to Police American Speech
- If Americans Knew
- Amnesty: Urgent – Protect Lebanese civilians from brutal escalation in Israeli attacks
- Is The War Against Iran Over?
- Inside the Israeli army’s propaganda wing
- Hundreds of Gaza Amputees Stranded in Legal Limbo
- The gallows law: Israel moves toward executing Palestinian children
- Tucker Carlson: The Path to Peace requires ending ‘special alliance’ with Israel
- This is ceasefire? Israel’s biggest massacre yet in Lebanon, another journalist killed in Gaza – Daily Update
- Tucker Carlson on Israel: This Is the Behavior of an Ally? Really?
- Gazans face a triple crisis: severe shortages of water and bread, healthcare in tatters
- NY Times reports how Netanyahu took the US into Iran War
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
