The Lies We Were Told
How long does it take to conclude some authority is lying? We don’t know this answer yet … apparently many years.
BY BILL RICE, JR. | JULY 11, 2023
I recently discovered an excellent Substack Newsletter authored by a registered nurse (Dee Dee) who has treated many (alleged) Covid patients. This nurse finally had enough and decided to share her stories and thoughts via her own Substack, which she started May 25th.
From reading a couple of her pithy posts, my take-away is Nurse Dee must feel like the main character in Joseph Heller’s classic novel Catch 22.
In that novel the experiences and observations of a fictional WW II bombardier tell readers the guidance and logic used by his superiors is complete madness.
Dee’s observations prompted my own question: When do citizens or employees finally realize that every supposedly-true thing they’ve been told is, in fact, a brazen lie?
For most people, at least with Covid proclamations, the answer seems to be “never.”
In other words, for many people, being lied to over and over doesn’t matter.
To put it mildly, such a revelation is a tad disconcerting.
Dee Dee’s observations from a June 2nd dispatch might show readers why I thought of “Catch-22,” where the message to bomber crews was “just do what you are told;” don’t try to figure out the logic.
With Covid, Nurse Dee identifies the goal of all orders. Instead of just “fly the dangerous mission,” the key message is: “Just take the shot.”
“The logic surrounding COVID-19 was circular. Every dictated premise, required blind faith and the goal was always the same; to take the shot.
“… You could not question the narrative and remain a good citizen …The mantra erupted, this is a pandemic of the unvaccinated.
“No argument could be interjected in the logic. It didn’t matter if you had not seen a new illness with unique symptoms … It didn’t matter if the science didn’t make sense. It didn’t matter if the measures were opposite to all your previous medical training.
… It didn’t matter that the vaccine did not stop transmission, and it didn’t matter if you had natural immunity. Essentially, we were told to accept every claim without evidence or reason. The orders had been given, just take the shot.”
In a recent dispatch, Dee listed about 30 truisms she (and all of us) were told. A few examples:
We were told the vaccine wouldn’t be mandatory.
We were told there would be two shots.
We were (then) told a booster was needed.
We were (then) told another booster was needed.
We were told there had been clinical trails conducted by the pharmaceutical companies that proved safe and effective.
We were told the vaccine would prevent the COVID-19 illness.
We were then told the vaccine would prevent serious illness.
We were told if everyone would just take the shot, it would be over.
We were (then) told there were breakthrough cases, where the vaccinated person became sick with COVID-19.
We were told even if you weren’t sick, you could give the disease to grandma.
We were told the unvaccinated are spreading the virus and creating mutations.
We were told, this is a “pandemic of the unvaccinated.”
We were told vaccine passports were the new normal and would be required.
We were told the vaccine was mandatory for employment.
We were told nurses who refused the shot were stupid …”
Back to me: Forget the pronouncements of the CDC experts, of Dr. Fauci, or of Nurse Dee’s hospital supervisors … just think about people you’ve interacted with in your own life.
At some point, when someone has told you one falsehood after another, do you stop believing them?
For most people, three big lies and you’re out.
“Fool me once, shame on you; fool me twice, shame on me …”
At some point, villagers did stop listening to the little boy who kept screaming, “A wolf is coming!”
Even politicians can take lying too far.
Here I recall John Edwards, a former U.S. Senator who was almost elected vice president of the United States.
Edwards lied repeatedly about an affair and then about fathering a baby with his mistress. Even when he “came clean” in a TV interview, his “confession” was replete with more lies.
I don’t know what John Edwards is doing with his life today, but I know he’s not running for political office. If he did, he’d be laughed off the podium. Everyone now gets that they can’t trust John Edwards.
The question I’m grappling with today is how many lies does someone have to tell before people conclude they’re listening to a serial liar? Is there a quota for one-lie-too-many, or a lie cut-off point?
In every-day normal life, it only takes a couple big whoppers before a friend becomes a “former friend,” a person to be avoided at all costs.
But not with our Covid liars. Apparently, there’s no limit to how many lies “trusted authorities” can tell … and still be considered “trusted” authorities.
In her very fist post, Nurse Dee wrote:
“Thrust upon our population was a labyrinth of lies. There were new daily mandates offering no explanation, making little if any, medical sense.
“… The medical interventions … coupled with preposterous statements from our leading experts, led me to personally, question everything. One question led to many questions until one day, I came to the realization, there were no answers.
“My questions met a variety of responses that included silence, laughter, and hostility. This was my first experience of being discouraged from asking questions.”
How does a person continue to function – as a sane human being – in a world that’s apparently insane?
Somehow, Nurse Dee (and me and you) … are still here, but we’ve had to adopt a new survival mechanism and are now functioning in a surreal new matrix where we know we have to live with insane notions; where we realize a never-ending cascade of “accepted” lies is our New Normal.
After reading Dee’s “Catch-22” anecdotes, I also had this question: How do serial liars keep telling all these lies? How do they get away with it?
This answer seems clear. Except for people like Dee, very few people call them out on their lies. (Thank you, mainstream media “watchdog” journalists).
Also, as I learned from a big story making the rounds today, the lying officials just keep doubling down on their lies.
An organization called the International Coalition of Medicine Regulatory Authorities (ICMRA) just issued a big press release telling everyone that the vaccines are still safe and effective and, just like we’ve all been told a million times … everyone should keep getting their next rounds of shots.
It’s clear to me that the purpose of this document is to counter the growing “spread” of world citizens who might, finally, be starting to question the pronouncements of trusted health authorities.
A few of the “Key messages from this group, which “brings together 38 medicines regulatory authorities from every region in the world, with the WHO as an observer” (In other words, a centralized, clearinghouse of expert liars):
* “False and misleading information about the safety of COVID-19 vaccines on social media often exaggerates the frequency and severity of side effects. Misinformation also wrongly attributes unrelated medical events to the vaccines.”
* “There is no evidence that COVID-19 vaccines have contributed to excess mortality during the pandemic …”
* Under the header, “Benefits of COVID-19 Vaccination,” the public is told that
“Millions of lives are estimated to have been saved by COVID-19 vaccination …”
I learned of this document from colleagues at the Brownstone Institute’s writer group.
A fellow Substacker added the link with this note: “A meticulous and immaculately supported take-down of this statement is needed. It’s been all over MSM today.”
I read the propaganda and immediately posted this reply:
“You could debunk/challenge every sentence …”
Two seconds before I made my post, another colleague posted this:
“Wow. Every single bullet point is a lie.”
Key take-away: The lies Nurse Dee was told every day – or almost immediately figured out on her own – are still being told today.
The damn liars have simply worn us down. I could debunk every one of those bullet points, but I’m growing tired of writing the same rebuttals over and over.
And as Dee observes, what’s the point? Even if someone does debunk all of these whoppers, these people are just going to keep lying … and keep telling us what to do.
The only conclusion I can make is that – especially regarding topics that might involve “life and death” – people, for some surreal reason, simply want to keep believing the liars.
Most people in the world must feel “safer” believing lies, lies that have killed and injured millions of their fellow citizens, including family members, friends and neighbors.
In our “Catch-22” world, the bigger the lies – and the more often serial lies prevaricate, the better.
For the liars, the benefits of lying are impressive. For the world’s skeptics, the costs of calling out liars are quite unpleasant.
Anyway, the lies aren’t going to stop.
‘Covid Censorship Proved to be Deadly’
BY BILL RICE, JR. | JULY 8, 2023
I wanted to make a quick post to recommend an exceptional and important essay published by The Wall Street Journal’s Opinion section.
In a brief essay (“Covid Censorship Proved to be Deadly”) author Brett Swanson shows how the Censorship Industrial Complex – or what he perfectly describes as “full spectrum censorship” – has effectively caused the unnecessary deaths (and misery) of huge numbers of world citizens.
As the essay makes clear, “truth” and “facts” have become “false narratives” or “dangerous misinformation” …. while false beliefs have become accepted as gospel/infallible truths.
Claims that are wrong, dangerous or dubious cannot be challenged.
As Swanson points out, the masses on social media quickly gleaned the speech they could not make (this shows the toxic effects of “self censorship.”)
The opinions of those who believe the “experts” might be “ignorant” were censored or not allowed to reach large numbers of people. Because of this, “falsehoods” could NOT be “dispelled.”
Swanson points out such a surreal template is the exact opposite of real science, which exists to challenge dubious claims.
A technology (the Internet) that could and should have been used to save many lives – and rebut many falsehoods – was instead used to bully and silence skeptics, who were really just trying to save lives and prevent outcomes that ultimately produced mass misery and devastating consequences for billions of world inhabitants.
The censored, bullied and demonetized skeptics are the real altruistic heroes, not the villains.
Theme fits perfectly with my next big story ….
I’m currently working on a story regarding the Covid outbreak aboard the USS Theodore Roosevelt aircraft carrier.
The true/vital lesson from this case study should have been that Covid does NOT threaten “everyone.” Per the lessons of the Roosevelt outbreak, this virus certainly doesn’t pose any real mortality risk to the young and middle aged.
But the “false narrative” quickly became that Covid threatens “everyone” … that younger adults and children were also “vulnerable.”
The truth – which would have eliminated irrational fear in most people – could NOT be disseminated as it would threaten the most important (false) narratives/initiatives.
As Swanson points out, the real goal in all of this “full spectrum censorship” is to PROTECT “authority.”
It would have constituted a “crisis” for those in authority if their pronouncements were exposed as “ignorance.”
The bottom line is that the massive and coordinated Censorship Industrial Complex was created to protect the power, wealth and continued control of those in authority.
At least The Wall Street Journal published this essay ….
… Also, The WSJ op-ed section deserves kudos for publishing this piece.
The author didn’t have the space to document the evidence of the huge spike in all-cause (non-Covid) excess deaths, but he still worked those points into his essay.
This by itself is a “win” for our side.
Shocking numbers of “vaccine” deaths/injuries and iatrogenic deaths/injuries are the giant elephants in the room in the mainstream media.
The reason most every-day citizens aren’t shocked by these scandals/truths … is that this story has been … censored. That is, this is NOT a “story.”
But at least The WSJ acknowledged this by publishing Swanson’s superlative essay.
Maybe the “news” division of the WSJ will follow-up on the author’s points and do some real journalism on these taboo topics?
Somehow I doubt this … but, still, the needle exposing the false narratives is moving in the right direction.
Blueprint for the New World Order

MERYL NASS | JULY 10, 2023
The UN has put out a number of concerning policy briefs and documents in the past 2 years and I will share them with you. This is the first :
First, now is the time to re-embrace global solidarity and find new ways to work together for the common good. This must include a global vaccination plan to deliver vaccines against COVID-19 into the arms ofthe millions of people who are still denied this basic lifesaving measure. Moreover, it must include urgentand bold steps to address the triple crisis of climate disruption, biodiversity loss and pollution destroying our planet.
 Second, now is the time to renew the social contract between Governments and their people and within societies, so as to rebuild trust and embrace a comprehensive vision of human rights. People need to see results reflected in their daily lives. This must include the active and equal participation of women and girls, without whom no meaningful social contract is possible. It should also include updated governance arrangements to deliver better public goods and usher in a new era of universal social protection, health coverage, education, skills, decent work and housing, as well as universal access to the Internet by 2030 as a basic human right. I invite all countries to conduct inclusive and meaningful national listening consultations so all citizens have a say in envisioning their countries’ futures.
Second, now is the time to renew the social contract between Governments and their people and within societies, so as to rebuild trust and embrace a comprehensive vision of human rights. People need to see results reflected in their daily lives. This must include the active and equal participation of women and girls, without whom no meaningful social contract is possible. It should also include updated governance arrangements to deliver better public goods and usher in a new era of universal social protection, health coverage, education, skills, decent work and housing, as well as universal access to the Internet by 2030 as a basic human right. I invite all countries to conduct inclusive and meaningful national listening consultations so all citizens have a say in envisioning their countries’ futures.
Third, now is the time to end the “infodemic” plaguing our world by defending a common, empirically backed consensus around facts, science and knowledge. The “war on science” must end. All policy and budget decisions should be backed by science and expertise, and I am calling for a global code of conduct that promotes integrity in public information.
Fourth, now is the time to correct a glaring blind spot in how we measure economic prosperity and progress. When profits come at the expense of people and our planet, we are left with an incomplete picture of the true cost of economic growth. As currently measured, gross domestic product (GDP) fails to capture the human and environmental destruction of some business activities. I call for new measures to complement GDP, so that people can gain a full understanding of the impacts of business activities and how we can and must do better to support people and our planet. [So clever how the wordsmiths portray the globalists’ desire to get rid of measures of economic activity as if this is linked to preventing environmental destruction!—Nass ]
Fifth, now is the time to think for the long term, to deliver more for young people and succeeding generations and to be better prepared for the challenges ahead. Our Common Agenda includes recommendations for meaningful, diverse and effective youth engagement both within and outside the United Nations, including through better political representation and by transforming education, skills training and lifelong learning. I am also making proposals, such as a repurposed Trusteeship Council, a Futures Lab, a Declaration on Future Generations and a United Nations Special Envoy to ensure that policy and budget decisions take into account their impact on future generations. We also need to be better prepared to prevent and respond to major global risks. It will be important for the United Nations to issue a Strategic Foresight and Global Risk Report on a regular basis, and I also propose an Emergency Platform, to be convened in response to complex global crises.
Sixth, now is the time for a stronger, more networked and inclusive multilateral system, anchored within the United Nations. Effective multilateralism depends on an effective United Nations, one able to adapt to global challenges while living up to the purposes and principles of its Charter. For example, I am proposing a new agenda for peace, multi-stakeholder dialogues on outer space and a Global Digital Compact, as well as a Biennial Summit between the members of the Group of 20 and of the Economic and Social Council, the Secretary-General and the heads of the international financial institutions. Throughout, we need stronger involvement of all relevant stakeholders, and we will seek to have an Advisory Group on Local and Regional Governments.
For 75 years, the United Nations has gathered the world around addressing global challenges: from conflicts and hunger, to ending disease, to outer space and the digital world, to human rights and disarmament. In this time of division, fracture and mistrust, this space is needed more than ever if we are to secure a better, greener, more peaceful future for all people. Based on this report, I will ask a High-level Advisory Board, led by former Heads of State and Government, to identify global public goods and other areas of common interest where governance improvements are most needed, and to propose options for how this could be achieved…
Prion Disease and the mRNA Shots: Some Light in the Dark
By John-Michael Dumais | The Defender | July 6, 2023
In a 2022 paper, Stephanie Seneff, Ph.D., Peter McCullough, M.D., MPH, and others discussed how the COVID-19 mRNA vaccines produce G-quadruplexes and microRNAs that can lead to prion disease.
The effect becomes significantly worse after the second dose of the Pfizer shot.
Prions are pathogenic agents that can induce the abnormal folding of cellular proteins, leading to diseases such as bovine spongiform encephalopathy (mad cow disease), Creutzfeldt-Jakob disease (CJD) and Alzheimer’s.
In his June 20 Substack post, researcher Adam Gaertner provides an accessible mini-tutorial on the complex and inspirational nature of cellular proteins. He addresses the structure and function of prions, the mechanisms by which they form, and how they can wreak havoc on any organ, especially the brain.
Prion disease can lead to a number of rare, progressive neurodegenerative disorders such as dementia, ataxia and spasticity before it becomes fatal, typically within just a few years of diagnosis.
Gaertner challenges the orthodoxy that there is no cure for prion disease by discussing several recent discoveries that offer “some unexpectedly good news.”
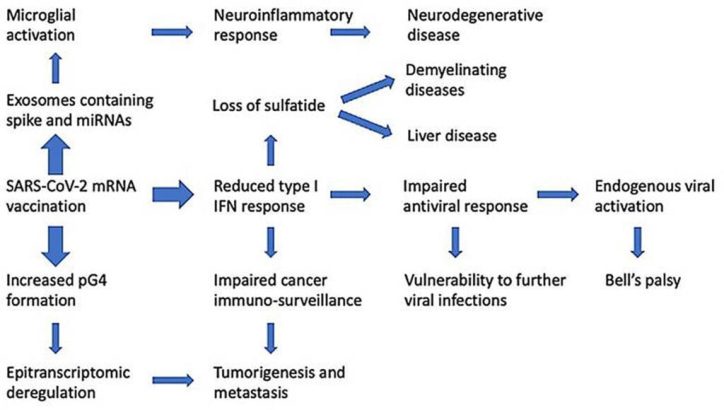
Innate immune suppression by SARS-COV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes and micrornas. Credit: Seneff, Nigh, Kyriakopoulos and McCullough.
Further investigation into mRNA and CJD
Gaertner began his research work into potentially useful therapeutics for prion disease and has also funded the development of a non-invasive prion blood test.
He even undertook his own study of people who were diagnosed with or died of CJD-like symptoms (n=60) after receiving the (mostly Pfizer) mRNA jab.
Nevertheless, he readily admits that he has yet to establish absolute proof of causation.
In a European Union document related to the approval of the vaccine, Gaertner discovered what could be the smoking gun: The liquid nanoparticles used to encase the mRNA came primarily from cow fat. According to Gaertner, the document in question even admitted mRNA’s potential to cause prion protein contamination.
Nearly a year after Gaertner publicized his discovery — which convinced some but not all researchers — a paper by Jean-Claude Perez documented 26 cases of “a new form of CJD” observed within a few days of the Pfizer, Moderna or AstraZeneca vaccinations.
Of these, 20 people died within less than five months of the injection. (At the time of the paper’s publication, only one of the 26 had survived.)
The ‘good news’
While admitting that “there is not, ordinarily, a whole lot of good news to be had concerning prion diseases,” Gaertner outlined a mechanism by which “residues on the spike [protein] bind to the many and varied amyloidogenic proteins,” thus resulting in the blood clots observed by more than a few embalmers since the introduction of the mRNA shots.
He explained how this process can “bind up” the prionic proteins:
“So, what we essentially have here is, instead of a silently cascading apocalypse, buried deep inside parts of the brain that we will never reach, we likely, instead, have these long, stringy, vein-shaped agglomerations of the various amyloid proteins, binding together wherever they meet, and apparently at least somewhat resistant to being broken down by the body’s natural processes for dealing with such eventualities.”
The “really good news” comes from the way ivermectin binds directly to the spike protein — which has itself been described as a “prion-like” protein — thus blocking the spike from connecting to the ACE-2 receptor and “preventing the key from ever entering the keyhole.”
According to Gaertner, ivermectin also prevents the “amyloidogenic aggregations to the spike protein,” thereby arresting the production and proliferation of the prionic proteins. He adds:
“Ivermectin is, without a shadow of a doubt at this point, a true miracle drug: With so many applications, from antiviral, to cancer treatment, to anti-inflammatory, and of course in its originally recognized anti-parasitic application, there should be little wonder why the powers that be have done their best to diminish it as ‘horse paste.’”
Gaertner also notes that in a “very unscientific poll” he conducted on Twitter, 80% of respondents reported that a single, low dose of ivermectin significantly improved “brain fog,” a common post-COVID-19 symptom.
He described a number of “relevant investigational therapeutics” for use against the spike protein and its effects, including serrapeptase, quercetin, methylene blue and resveratrol, some of which demonstrate a “very broad range of useful actions.”
Expressing his belief that the lack of progress on therapeutics for neurodegenerative diseases is likely due to “your run-of-the-mill Pharma and charity corruption,” Gaertner nonetheless found cause for optimism.
“There’s been a lot of progress, on a lot of fronts, and more comes regularly as the world continues waking up,” he said.
John-Michael Dumais is a news editor for The Defender. He has been a writer and community organizer on a variety of issues, including the death penalty, war, health freedom and all things related to the COVID-19 pandemic.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Now that government COVID malfeasance is exposed, what will the GOP do about it?
By Daniel Horowitz – conservative review – July 6, 2023
We are now 2+ years into consuming reams of information showing the vaccines were devastating to humanity. What will Republicans do about it other than whine about censorship? Refusing to focus on vaccine injury and the perfidy of the government-vaccine complex is an act of self-censorship.
There is a bizarre dynamic unfolding as it relates to GOP sentiment toward the vaccine. All Republicans recognize and decry the growing evidence of the government’s collaboration with big tech to censor all information about vaccine injury. Yet they seem to be more upset about the censorship of the information than about the information itself. Why is there no push from Republicans to defund the vaccines and fix the regulatory and legal structures that allowed Operation Warp Speed to occur and that continue to gaslight the next iteration of rushed, dangerous vaccines?
In an extraordinary ruling on Independence Day itself, Louisiana federal Judge Terry Doughty issued a broad injunction against all government agencies on working with social media companies to censor politically unfavored speech. Citing “substantial evidence” of government’s “dystopian” violations of the First Amendment, Judge Doughty prohibited the federal government from “encouraging, pressuring, or inducing in any manner the removal, deletion, suppression, or reduction of content containing protected free speech.” The injunction not only includes the HHS agencies censoring COVID information, but also the FBI, the Cybersecurity and Infrastructure Security Agency, the State Department, the DOJ, and the White House censoring all forms of protected speech.
This ruling comes a week after the House Judiciary committee produced a preliminary report showing DHS’ CISA was behind the censorship enterprise. It turns out that CISA funded a nonprofit group to work with social media on a process, known as “switchboarding,” which would “trigger content moderation” to “ensure priority treatment of misinformation reports.”
Republicans seem united in combating this censorship and plan to include provisions in the relevant appropriations bills for fiscal year 2024 to block funding for these surveillance and censorship programs. However, where is the same degree of outrage about the dangers of the vaccines themselves?
We now have over two years of information showing ubiquitous injury stemming from damage to all parts of the body, particularly cardiac and neurological. Whether it’s VAERS, European data, countless independent studies, epidemiological data, excess deaths and “died suddenly” mysteries correlating with the take-up of the vaccines, health insurance data, life insurance data, or disability data – we have enough evidence to convict this shot for murder if it were a human standing for trial. Yet not only have these vaccines not been defunded, the same framework that rushed their approval has already been used for countless other new vaccines.
The government’s new shell game is to concede the existence of these problems, but play semantics with the term “rare” when describing their risk. Science Insider published a piece acknowledging the “rare link between coronavirus vaccines and Long Covid–like illness,” including blood clotting, heart inflammation, and neurological disorders. Even Peter Marks, the man at the center of Operation Warp Speed, admitted, “We can’t rule out rare cases.”
“If a provider has somebody in front of them, they may want to take seriously the concept [of] a vaccine side effect,” admits the director of the FDA’s Center for Biologics Evaluation and Research, two years after emails show he ignored concerns of rushing the vaccine amidst a pileup of adverse event reporting.
However, what is rare? The CDC’s own pharmacovigilance program showed a 7.7% rate of clinical-level injury. Coupled with the underreporting rate in VAERS, there were likely millions of severe and long-term injuries, including several hundred thousand deaths in the U.S. So yes, we can suggest that 92% of people didn’t experience clinical levels of injury and 98%-99% didn’t experience long-term and deadly injuries. In that sense, I guess you can say it’s rare. But how many people are we talking about when 5.5 billion people were given at least one dose? Potentially, millions of deaths and hundreds of millions of injuries! Just consider the fact that 25% of injuries reported to VAERS and about a third reported by the European Medicines Agency are considered serious, well beyond the standard of 15%.
House Republicans can no longer ignore the problem with the vaccines. They must also stop ignoring the endless approvals of monkeypox and RSV shots based on dubious data and the same rushed framework. To that end, Speaker McCarthy should take the following actions.
- Defund all COVID shots in the HHS, DOD, and FDA funding bills.
- Create a commission of members of Congress to examine the rationale, safety, and efficacy data of all vaccines, beginning with the new ones recently approved and in the pipeline.
- Refuse to sign off on the Senate version of the Pandemic and All-Hazards Preparedness Act unless major reforms are enacted curtailing pandemic authorities.
- Bar any involvement in a WHO pandemic treaty or expansion of the International Health Regulations.
- Repeal immunity for vaccine manufacturers, including the provision in the 21st Century Cures Act of 2016 that extends the immunity to vaccines offered to pregnant women.
To this day, we still can’t get Republicans to shake their support for the V-word even in red states. Last week, Ohio Gov. Mike DeWine, the consummate COVID fascist governor, used his line-item veto to strike a provision from the budget ending vaccine mandates in colleges. “University and college dormitories and student housing are congregate settings where such policy may be of great importance to ensure resident safety,” said DeWine of vaccine mandates in his veto message. It takes a new level of cognitive dissonance to support mandates on those who don’t want the shot out of fear of harming those who did supposedly get the protection that evidently fails to protect unless the other person gets it!
Republicans all agree that our government engaged in an unprecedented operation to cover up the truth about vaccines. How come their curiosity stops at the degree of exposing the cover-up with no interest in delving into what exactly they are trying to cover up? After all, this is the only product that automatically goes into every arm of every baby multiple times after birth with a set schedule mandated by schools. Certainly the COVID shots are proven to be poison, but is there no interest in uncovering the broader truth?
© 2023 Blaze Media LLC. All rights reserved.
Lancet Study on Covid Vaccine Autopsies Finds 74% Were Caused by Vaccine – Journal Removes Study Within 24 Hours
BY WILL JONES | THE DAILY SCEPTIC | JULY 6, 2023
A Lancet review of 325 autopsies after Covid vaccination found that 74% of the deaths were caused by the vaccine – but the journal removed the study within 24 hours.
The study, a pre-print that was awaiting peer-review, is written by leading cardiologist Dr. Peter McCullough, Yale epidemiologist Dr. Harvey Risch and their colleagues at the Wellness Company and was published online on Wednesday on the pre-print site of the prestigious medical journal.
However, less than 24 hours later, the study was removed and a note appeared stating: “This preprint has been removed by Preprints with the Lancet because the study’s conclusions are not supported by the study methodology.” While the study had not undergone any part of the peer-review process, the note implies it fell foul of “screening criteria”.
The original study abstract can be found in the Internet Archive. It reads (with my emphasis added):
Background: The rapid development and widespread deployment of COVID-19 vaccines, combined with a high number of adverse event reports, have led to concerns over possible mechanisms of injury including systemic lipid nanoparticle (LNP) and mRNA distribution, spike protein-associated tissue damage, thrombogenicity, immune system dysfunction and carcinogenicity. The aim of this systematic review is to investigate possible causal links between COVID-19 vaccine administration and death using autopsies and post-mortem analysis.
Methods: We searched for all published autopsy and necropsy reports relating to COVID-19 vaccination up until May 18th, 2023. We initially identified 678 studies and, after screening for our inclusion criteria, included 44 papers that contained 325 autopsy cases and one necropsy case. Three physicians independently reviewed all deaths and determined whether COVID-19 vaccination was the direct cause or contributed significantly to death.
Findings: The most implicated organ system in COVID-19 vaccine-associated death was the cardiovascular system (53%), followed by the hematological system (17%), the respiratory system (8%) and multiple organ systems (7%). Three or more organ systems were affected in 21 cases. The mean time from vaccination to death was 14.3 days. Most deaths occurred within a week from last vaccine administration. A total of 240 deaths (73.9%) were independently adjudicated as directly due to or significantly contributed to by COVID-19 vaccination.
Interpretation: The consistency seen among cases in this review with known COVID-19 vaccine adverse events, their mechanisms and related excess death, coupled with autopsy confirmation and physician-led death adjudication, suggests there is a high likelihood of a causal link between COVID-19 vaccines and death in most cases. Further urgent investigation is required for the purpose of clarifying our findings.
The full study does not appear to have been saved in the Internet Archive, but can be read here.
Without further detail from the Lancet staff who removed the paper it is hard to know what substance the claim that the conclusions are not supported by the methodology really has. A number of the authors of the paper are at the top of their fields so it is hard to imagine that the methodology of their review was really so poor that it warranted removal at initial screening rather than being subject to full critical appraisal. It smacks instead of raw censorship of a paper that failed to toe the official line. Keep in mind that the CDC has not yet acknowledged a single death being caused by the Covid vaccines. Autopsy evidence demonstrating otherwise is clearly not what the U.S. public health establishment wants to hear.
Dr. Clare Craig, a pathologist and co-Chair of the HART pandemic advisory group, says that in her view the approach taken in the study is sound. She told the Daily Sceptic:
The VAERS system [of vaccine adverse event reporting] is designed to alert to potential harms without necessarily being the best way of measuring the extent of those harms.
Quantifying the impact of deaths can be done by looking at overall mortality rates in a country.
However, this is imperfect as a deficit of deaths would be expected after a period of excess deaths, making the accuracy of any baseline dubious.
An alternative approach of auditing such deaths through autopsy is sound.
There may be a bias [in the study] towards reporting the autopsies of deaths where there was evidence of causation and the likelihood of causation might be exaggerated by that bias. For example, 19 of the 325 deaths were due to vaccine-induced immune thrombocytopenia and thrombosis (VITT) but these reports may be overrepresented because of the regulators’ willingness to acknowledge such deaths.
Nevertheless, it is important that attempts are made to quantify the risk of harm and censorship of these attempts, rather than open scientific critique, does nothing to help reassure people.
Walensky Warns Public to Beware of ‘Misinformation’ and ‘Politicized Science’
By Brenda Baletti, Ph.D. | The Defender | July 5, 2023
As she ended her tenure last week as director of the Centers for Disease Control and Prevention (CDC), Dr. Rochelle Walensky warned the American public to be on guard against “misinformation” and the “politicization of science.”
Walensky told The Wall Street Journal she hopes Americans will make health decisions based on “their own risk assessment and their own personal risks, but not through politics,” emphasizing that public health recommendations also shouldn’t be politicized.
“Ironically, this comes after two-and-a-half years of Walensky misinforming the public and politicising the science,” investigative journalist Maryanne Demasi, Ph.D., wrote on her Substack.
Demasi and many others took to Twitter to remind people of Walensky’s false statements and politicized decision-making.
Walensky last week published a farewell op-ed in The New York Times, in which she wrote that public health is critically important in the U.S., and yet she “fear[s] the despair from the pandemic is fading too quickly from our memories.”
She complained that “the agency [CDC] has been sidelined, chastened by early missteps with Covid and battered by persistent scrutiny.”
She also told the WSJ that public health shouldn’t fall along partisan lines.
Yet stark political partisanship defined her time at the CDC. The WSJ reported that a recent KFF poll showed political affiliation was the strongest demographic predictor of COVID-19 vaccination. And about one-quarter of Americans don’t trust the CDC’s health recommendations, according to a 2022 survey published in the journal Health Affairs.
Walensky acknowledged “missteps in communicating” by the CDC, which, she said, “could have done a better job” making it clear to the public that the agency’s message could change during the pandemic.
But, she told the WSJ, the CDC has a plan to regain public trust in the future — by working directly with media organizations to discuss how to best shape public opinion prior to releasing scientific information to the public.
She said the CDC plans to use a method called “prebunking,” where they will communicate directly with media organizations before they release information to let the media know which details about public health might be “misconstrued.”
According to The Associated Press (AP) “prebunking” by public health agencies allows the agencies to define something as “misinformation” before readers have an opportunity to encounter it elsewhere as possibly true.
Then search engines such as Google prioritize “credible websites” like the U.S. Food and Drug Administration’s (FDA) or the CDC’s in its searches.
FDA Commissioner Robert Califf, the Virality Project and Google are among those who have promoted prebunking as a way to combat misinformation.
Journalist Kim Iversen proposed a different approach Walensky might take to restoring public trust in the CDC.
She said:
“Well, the way to do it is to apologize, to own up to your lies, to own up to the mistakes that you made and to discuss why you did that, why the agency followed such political partisanship when they should have been following science, why they ignored the science that was right in front of them.”
CDC broadcast a long list of ‘misinformation’ during Walensky’s tenure
Throughout her tenure at the CDC, which began when Biden took office in January 2021, Walensky made a series of public statements that have proven to be false.
Evidence has since emerged that Walensky knew many of these statements were false when she made them.
In March 2021, Walensky famously told Rachel Maddow, that “vaccinated people do not carry the virus, don’t get sick.”
The CDC was forced to walk back her statements a few days later. But that message was the basis for vaccine mandates imposed later that year by the Biden administration, businesses, universities and public venues throughout the country.
In a mid-June congressional hearing, Walensky defended her March statements, claiming they were true at the time.
But the Washington Examiner reported on June 20 that emails obtained through a Freedom of Information Act request showed Walensky and Dr. Francis Collins were aware of and discussed “breakthrough cases” of COVID-19 in January 2021 — just before the vaccines became widely available — and yet continued to tell the public the vaccines would prevent transmission.
In that same congressional testimony, Walensky also defended the mask mandates, saying that the summary of Cochrane’s review — which found wearing masks in the community “probably makes little to no difference” in preventing viral transmission — had been “retracted.”
But it was neither retracted nor had the authors of the review changed the language in the summary, Demasi reported.
In June 2021, Walensky told “Good Morning America” that the risk of myocarditis was extremely rare, and there was overwhelming data the vaccines were safe for children — even after hundreds of cases of myocarditis had been reported and the CDC had been aware of a safety signal since February.
Under Walensky, the CDC also gave false information on vaccine safety monitoring, added the COVID-19 vaccines to the childhood vaccine schedule despite known harms, withheld data on boosters from the agency’s own advisers and told pregnant women the vaccine was safe — just days after Pfizer reportedly finalized a report demonstrating it wasn’t.
In a March study by Krohnert and others, researchers compiled instances of errors in data presented by the CDC during the COVID-19 pandemic in publications, press releases, interviews and Twitter. The authors reported 25 instances where the agency under Walensky promoted demonstrably false numbers.
In most (80%) cases, the CDC exaggerated the severity of the pandemic. For example, Walensky gave a briefing on June 23, 2022, during which she claimed COVID-19 was a “top 5 cause of death” in children, which was untrue.
Most recently, the House Select Subcommittee on the Coronavirus Pandemic gave Walensky until July 12 to turn over phone records involving American Federation of Teachers (AFT) President Randi Weingarten. The House is investigating potential political interference on the part of AFT with the CDC’s school reopening recommendations during the COVID-19 pandemic, The Defender reported.
Walensky warns of ‘future threats’
Walensky warned at the end of her Times op-ed:
“I want to remind America: The question is not if there will be another public health threat, but when. The C.D.C. needs public and congressional support if it is going to be prepared to protect you from future threats.”
To take on these “future threats” the Biden administration nominated Dr. Mandy Cohen, an internal medicine physician and former state health secretary of North Carolina, to replace Walensky.
But critics warn Cohen is “a public health COVID authoritarian” who is “fully entrenched in the ‘bio-pharmaceutical complex.’”
Dr. Peter McCullough told The Defender that during the COVID-19 pandemic, Cohen failed to recognize therapeutics and natural immunity, and supported lockdowns, vaccine mandates and masking.
Cohen comes to the CDC from the private sector, where she is executive vice president of Aledade and CEO of Aledade Care Solutions, whose executive leadership and board of directors includes people with connections to the World Economic Forum and the Bill & Melinda Gates Foundation.
Walensky congratulated Cohen on her nomination, describing her as “a respected public health leader who helped North Carolina successfully navigate” COVID-19, and whose “unique experience and accomplished tenure in North Carolina … make her perfectly suited to lead CDC as it moves forward by building on the lessons learned from COVID-19 to create an organization poised to meet public health challenges of the future.”
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Exposed, the multi-billion-dollar illusion of ‘HIV’: Part 1
Readers of TCW will be familiar with Neville Hodgkinson’s critical reporting of the ‘Covid crisis’ since December 2020, notably his expert, science-based informed alarm about the mass ‘vaccine’ rollout, so absent from mainstream coverage. What they may be less aware of is the international storm this former Sunday Times medical and science correspondent created in the 1990s by reporting a scientific challenge to the ‘HIV’ theory of Aids, presaging the hostile response to science critics of Covid today. In this series, written exclusively for TCW, he details findings that form the substance of his newly updated and expanded book, How HIV/Aids Set the Stage for the Covid Crisis, on the controversy. It is available here.
By Neville Hodgkinson | TCW Defending Freedom | July 3, 2023
Three years into the Covid crisis, many are now aware of the disastrous advice on which so many governments blindly acted. False predictions of spread, fearmongering propaganda, lockdowns damaging young and old, suppression of cheap treatments to make way for a dangerous, experimental vaccine . . . so much of ‘the science’ turned out to be fiction, hugely profitable for a few but harmful for billions.
These failures have brought back into focus claims that the syndrome known as HIV/Aids was – and still is – being similarly mishandled and exploited by the worlds of medical science, public health and Big Pharma. Robert Kennedy Jr documents this in detail his best-selling 2021 book The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health.
What few people know however is that for almost 40 years a small group of scientists has deconstructed almost every aspect of the theory that Aids is caused by a lethal, sexually transmitted virus known as HIV. Their critique goes beyond questioning HIV as the cause of Aids. They say ‘HIV’ has never even been proved to exist. And the reason you have probably never heard of their work is that, like the doctors and scientists who challenged Covid insanities, they have been silenced at every turn.
With Covid, pressure to conform came through government-directed appeals to our higher nature through slogans such as ‘Stay at home. Protect the NHS. Save Lives’ and ‘Every vaccination gives us hope’. The implied claim was that anyone who thought differently was either an idiot or a murderer.
Similarly with Aids, advocates of the deadly virus theory sought to make those who questioned it sound as though they were lacking in compassion, irresponsible or stupid.
I was working as medical correspondent of the London Sunday Times in the 1980s when Aids suddenly became big news after American government scientists claimed to have identified a previously unknown virus as the cause of a mysterious cluster of symptoms related to severely depleted immunity. They included Kaposi’s sarcoma, a cancer affecting the skin and internal organs; severe candidiasis; and pneumonia caused by an out-of-control fungus. The symptoms proved resistant to treatment, and fatal in a number of cases.
The first victims were groups of gay men who were challenging long-standing homophobic attitudes in American society through what came to be known as the ‘fast-track’ gay lifestyle. This involved multiple sex partners and heavy drug use.
The partying was fun, I was later told, but it caused disease microbes to become pooled among participants such that almost every encounter carried a risk of infection. Prophylactic use of antibiotics staved off some illnesses but contributed to an underlying deterioration, and in some cases complete collapse, of the immune system.
The crisis at first met an unsympathetic response from the right-wing Reagan administration. The common histories of the victims led to dismissive descriptions of Aids as a ‘gay plague’. As numbers increased, however, outrage and anger grew. Those involved had often already suffered greatly from discriminatory attitudes and behaviour, and their efforts to end this bigotry through the Gay Lib movement looked to be under threat.
That was the context in which US biomedical researcher Robert Gallo found immediate acceptance when in 1984 he claimed to have identified a deadly virus, new to humanity, as the cause of Aids. The theory took off like wildfire and by the end of 1984 had come to be accepted by virtually everyone. The microbe Gallo said he had found became known as the Human Immunodeficiency Virus, or HIV.
It brought virologists, drug companies and public health experts to centre stage. Taxpayer dollars, eventually reaching hundreds of billions, were poured into Aids research and treatment through the US National Institutes of Health, in particular the National Institute of Allergy and Infectious Diseases (NIAID) under the leadership of Dr Anthony Fauci. Well-funded NGOs and activist groups sprang up with the aim of contributing to the fight against the disease.
Religious leaders warmed to the theory because it discouraged sleeping around. Politicians liked it because it put in place a new ‘enemy within’ against which they could claim to offer protection with advertising campaigns such as the UK’s ‘Aids: Don’t Die of Ignorance’ – a precursor of the intense propaganda inflicted on us with the advent of Covid-19.
Media people – including me, I am ashamed to say – vigorously promulgated warnings that the virus put at risk everyone and anyone who had sex. It felt good to be not just selling newspapers, but helping to sound the alert.
Young people were less readily taken in. James Delingpole has recalled how the ad campaign put a dampener on his sex life, though after the initial shock it became increasingly clear to him that the government had been overstating the case.
In fact, as the late Nobel Prize-winning chemist Kary Mullis and other scientists were to point out, there never was a body of scientific evidence demonstrating the validity of the ‘deadly new virus’ idea. That remains the case today, despite hundreds of thousands of papers having been published over the years predicated on the HIV belief system.
Henry Bauer, a retired professor of science studies who has drawn on numerous sources in documenting The Case Against HIV, says: ‘Anyone open to looking at the actual data . . . can find an enormous amount of evidence that the diagnosis of HIV as cause of AIDS is simply wrong.’
One lasting outcome of the theory was that by ‘democratising’ Aids, with the message that the disease did not discriminate and so everyone was at risk, it prevented the feared setbacks for the Gay Lib movement. Lesbian and gay rights became firmly established in American society, and in some other parts of the world.
In many other ways, however, the global hysteria to which the theory gave rise has had disastrous consequences, some of which continue to this day.
A failed cancer drug called AZT, pulled off the shelf by American government researchers because of an apparent anti-HIV effect, killed and injured thousands. It was administered in high doses not just to people with Aids but to gay men, haemophiliacs and others thought to be HIV-infected, earning hundreds of millions of pounds for the US drug company Burroughs Wellcome and its British parent, the Wellcome Foundation (later taken over by Glaxo). American and British government institutions promoted it vigorously as the ‘gold standard’ of Aids treatment. Doctors who stepped publicly out of line were hounded out of the profession.
Although later generations of drugs can genuinely help to support a failing immune system, 40 years of research has failed to bring either a vaccine or cure for the purported ‘HIV’ infection. Taken over long periods, the drugs themselves can kill, contributing significantly to the 800 or so deaths reported annually of ‘people living with HIV’ in the UK.
The most widespread and long-lasting harm, however, has been to the countless people around the world, especially in Africa and of African descent, terrorised with a false belief that they are victims of a sexually transmitted virus which only Western medicine has the means to hold at bay. The World Health Organization (WHO) claims that more than 80million people have been infected, and that about 40million have died from HIV. Three-fifths of purported new HIV infections are said by WHO to be in the African region. African Americans are eight times more likely to be diagnosed with HIV infection compared with the white population.
American taxpayers in particular have been burdened with the huge expense of maintaining an industry that has grown up around HIV/Aids. The US government spends more than $28billion a year on the domestic response, and expenditure globally between 2000 and 2015 totalled more than half a trillion dollars ($562.6billion), according to a University of Washington study. Yet the Joint United Nations Programme on HIV/AIDS (UNAIDS), in a never-ending plea for more money, says the pandemic continues to take a life every minute.
In this series of articles I am going to describe the fruits of years of painstaking work by scientists based in Perth, Western Australia, collating evidence challenging almost every aspect of the ‘HIV’ theory. The essence of their case is that there is no ‘HIV’ epidemic, and there never will be a vaccine or cure, because there is no ‘HIV’.
If you find this hard to believe, I am with you entirely in the sense that it took me years to accept fully how wrong I had been in my early reporting on Aids. I documented this painful journey of discovery in my book AIDS: The Failure of Contemporary Science, published in 1996 by Fourth Estate.
If you ask how it could be possible that for 40 years the scientific and medical worlds have failed to correct a belief in a mythological virus, the answer is more sociological than scientific.
Solidarity with the suffering of the gay community played a part – although genuine kindness, such as Louise Hay demonstrated in her early healing work with people with Aids, strongly and successfully challenged the medical view that they were certain to die. An arrogant, but ill-informed, neocolonial drive by countless NGOs to ‘do good’ in poorer parts of the world also contributed. But probably the most powerful and detrimental element in maintaining the deception was the money and influence involved, as governments went into partnership with the hugely profitable pharmaceutical industry. The resources poured into HIV/Aids created thousands of jobs, buying loyal collaboration and stifling dissent.
Highly experienced scientists who spoke out against the theory were ridiculed, defunded, gaslighted, and accused of killing people by weakening the public health message.
I experienced this pressure myself when I began to examine alternative ways of looking at Aids in the early 1990s, when I was working as Sunday Times science correspondent. Joan Shenton of Meditel, producers of prize-winning but much criticised documentaries on the issue, alerted me to the fact that several distinguished scientists had challenged the idea that HIV could be doing all the damage attributed to it.
Andrew Neil, editor of the Sunday Times, which had serialised Michael Fumento’s 1990 book The Myth of Heterosexual Aids, supported my reports on an ever-deepening scientific challenge to the theory. Over a three-year period, condemnation came from just about every quarter. The deeper the critique went, the shriller the protests became.
In 1993, with the HIV/Aids industry still pointing to Africa as proof of how millions could become infected, Neil told me to go there to find out what was happening. Over six weeks, travelling through Kenya, Zambia, Zimbabwe and Tanzania, it became increasingly plain to me that the entire pandemic was an illusion arising from diseases of poverty being reclassified as ‘HIV/Aids’.
My reports to this effect proved too much for the scientific establishment, and Nature – supposedly one of the top scientific journals in the world – declared that we must be stopped. Having decided that picketing our offices would be impractical, the magazine mounted a campaign of ridicule. The UK’s Health Education Authority started an Aids journalism award specifically in my dishonour. They said it was to counter the newspaper’s dangerously misleading coverage. There was incomprehension and abuse from all three main political parties, as well as from scientific and medical chiefs.
But we also heard from many doctors, health workers, gay men, and specialists on Africa, thanking the newspaper for its challenging coverage. An ‘HIV’ diagnosis at that time could still have the power of a witch-doctor’s hex, and people who had tested positive wrote to say that our reports were like a breath of fresh air.
Andrew Neil was undeterred by the hostile bluster, while insisting the paper was ready to publish any evidence that countered the dissident case we were presenting. In 1994 he left the paper for New York, and I left too after his successor John Witherow made it plain that he did not want me to continue this line of reporting. The literary agent David Godwin had been in touch, suggesting a book on the controversy, and this took shape over the following year.
When Fourth Estate published it in 1996, however, it became an early victim of ‘cancel culture’. The late American gay activist Larry Kramer, at first a bitter critic of Fauci but later his friend and ally, was in the UK at the time of publication to address a conference on Aids. He picked up a copy at a pre-conference gathering, tore several pages, and spat in it, telling his audience: ‘Do the same if you come across this book. They will soon stop stocking it.’ It quickly disappeared from view, subsequently topping a list of ‘Books You’re Not Supposed to Read’ in a work on political incorrectness in science.

(From The Politically Incorrect Guide to Science, by Tom Bethell, Regnery, 2005)
I am republishing it now, with additional material including a summary of where the science of ‘HIV’ went wrong, because the story is so redolent of the misunderstandings, mishandling and downright lies surrounding Covid-19. As with Aids, huge grants from Big Pharma and ‘philanthropic’ foundations to researchers, medical associations, consumer groups, and civil rights organisations fuelled the Covid illusions.
There is one important difference. At first I thought the Covid fearmongering was as ill-conceived as that over ‘HIV’ and Aids. It soon became clear, however, that unlike ‘HIV’ this was a genuine pathogen. A disgracefully suppressed paper by the UK’s Professor Angus Dalgleish, working with Norwegian colleagues including a biowarfare expert, demonstrated beyond reasonable doubt the genetically-engineered nature of SARS-CoV-2 (see here and here).
Panic measures to try to hide its laboratory origin confirm that view. These were led by the Chinese, from whose Wuhan laboratory the virus almost certainly escaped, and by Fauci, whose NIAID had part-funded the work. Sir Jeremy Farrar, then director of the UK’s Wellcome Trust and now WHO chief scientist, also played a leading role in the cover-up.
Many are now aware of the adverse social, economic and health consequences of the Covid hysteria into which Fauci and others led us. Billions of people meekly accepted and even welcomed unprecedented lockdowns and other fearmongering measures, along with mass administration of the mRNA gene products. TCW Defending Freedom has been one of few voices constantly critical of the mishandling of Covid over the past three years, despite high-level, far-reaching efforts to silence and defund the site.
Much less widely understood is the way Aids became subject to similar mismanagement 40 years ago, with adverse consequences lasting until today.
Laid Low by the COVID Vaccine, Now They’ve Got a Bad Case of Federal Unresponsiveness
By Christian Britschgi | RealClear Investigations | June 28, 2023
In April 2021, Adele Fox received a single shot of the Johnson & Johnson COVID-19 vaccine. Within a few hours, the 60-year-old resident of Portsmouth, New Hampshire, started feeling shooting pains in her legs, arms, and neck. The pain didn’t abate over the next few days. Instead, it got worse and was accompanied by nausea and debilitating fatigue.
Within a few weeks, neurologists affiliated with Massachusetts General Hospital diagnosed her with several serious conditions they say were a result of her COVID-19 vaccine, including small-fiber neuropathy (which causes a painful tingling in the extremities) and Sjögren’s Syndrome (which leaves patients pained and fatigued, and in extreme cases, can damage internal organs).
This shot, which was supposed to get Fox back to normal, instead left her with diminished ability to work and enjoy life. Persistent physical therapy and experimental treatments she’s taken since have done little to alleviate her symptoms.
“I used to do so much, and now it’s a struggle,” she says. “Sometimes you just get down.”
With her medical bills mounting and her condition not improving, Fox sought compensation for her damaged health. Federal liability protections prevent the vaccine-injured from directly suing vaccine manufacturers like Johnson & Johnson. Instead, claimants have to go to the federal government for compensation.
But as Fox would soon learn, the government has two starkly different injury programs for vaccines. One operates like a civil court with a neutral judge, lawyers on both sides, and a guaranteed right of appeal. In recent decades, it has approved about 75% of claims and pays out hundreds of millions of dollars per year.
The other, which handles COVID-19 vaccines, has rejected almost every claim brought to it, awarding less than $10,000 since the pandemic. And in a nation nearly numb to the pandemic’s toll and its scandals, the program is adding seething frustration atop lasting injury to Fox and people like her in a little reported aftermath to the government’s much criticized performance on vaccines – ranging from erratic booster advice to broad-brush vaccine mandates that cost people their jobs.
Fox filed her claim two years ago, submitting hundreds of pages of medical documents about her condition and diagnoses. She’s nevertheless one of the 10,887 people still waiting on a decision. “You’re not even hearing anything from the organization that’s supposed be helping you,” she says. “The phone keeps ringing, no one is emailing, nobody is doing anything.”
The federal agency overseeing the program, the Health Resources and Services Administration, said in a statement to RealClearInvestigations that the current number of claims “significantly exceeds the previous volume in the program” and that the program has “hired additional staff to address this growth in claims, and the President’s budget requests additional funding to support the additional staffing needed to process claims.”
Tale of Two Compensation Programs
The government’s two contrasting vaccine compensation programs are similarly named and thus easily confused. The first, Vaccine Injury Compensation Program (VICP) was created in the 1980s and covers most routine vaccines. The second, the Countermeasures Injury Compensation Program (CICP), is a result of war-on-terror legislation in 2005 and now covers COVID-19 vaccines. Their bureaucratic differences help explain why a nation that has spent trillions of dollars on COVID relief programs has provided almost no assistance to people harmed by the vaccines that the government encouraged, and sometimes required, them to take.
The earlier program was supposed to shore up pharmaceutical companies’ willingness to make childhood vaccines in the face of persistent vaccine injury lawsuits, while also giving the vaccine-injured a fair and expedited process for compensation.
The vaccine-injured would not sue pharmaceutical companies. Instead, they’d petition the government in Federal Claims Court, where special masters (judges) would decide cases. Compensation came from a government-administered trust fund paid for by excise taxes levied on vaccine manufacturers.
Between 2006 and 2021, this court adjudicated cases from 10,602 petitioners and issued compensation to 7,618 of them. The compensation trust fund sits at $4 billion and pays out about $200 million in compensation and attorneys’ fees each year.
This earlier program bears little resemblance to the Countermeasures Injury Compensation Program, where the COVID-vaccine cases of Fox and many others are languishing.
It was meant to incentivize pharmaceutical companies to be part of the federal response to one-off, one-in-a-million events like a bioweapon attack or an outbreak of a deadly pandemic. Although almost one billion doses of COVID-19 vaccines have been administered in the United States, and health authorities say boosters could become as common as the annual flu shot, it remains the only way people harmed by the shot can receive compensation.
It’s far from guaranteed they’ll get it.
Before the pandemic, this program received a little over 500 claims and had paid out compensation to only 30 people – mostly for H1N1 (swine flu) vaccine injuries. In just the past two years, it has been asked to make decisions on over 10,000 injury claims related to COVID countermeasures.
As of June, it made decisions on just 919 of these COVID-related claims and rejected 894 of them. It has so far paid out only $8,593 in compensation to just four people who were injured by a COVID vaccine. The program has deemed another 20 people eligible for compensation, but has yet to pay them.
It’s not a judicial process either. Rather, it’s an administrative process overseen by Health Resources and Services Administration, which is housed within Department of Health and Human Services (HHS). People file a claim and government medical reviewers decide whether to pay out or not. That’s an awkward arrangement, given that HHS is deciding whether to pay for damages caused by products it approved and in some cases mandated.
Because it’s an administrative process, there’s no right to counsel and no neutral arbitrator. A denied claimant can file for reconsideration with HRSA, but otherwise has no right to appeal.
Unlike the earlier program, the CICP offers no compensation for pain and suffering and doesn’t pay attorneys’ fees. Most successful claimants have received compensation totaling a few hundred dollars or a few thousand dollars. The highest award for a COVID-19 vaccine injury sufferer was $3,957.66 to a person who got myocarditis (a heart condition) from a vaccine.
It also has shorter filing deadlines. People have to file a claim within one year of vaccination, a much shorter window than the earlier program’s standard of three years from the onset of symptoms. Of the 894 claims that CICP has rejected, 444 of them were for missing the filing deadline.
CICP also only awards compensation in cases where there’s “compelling, reliable, valid, medical, and scientific evidence” that someone’s injury is linked to a covered countermeasure. HRSA describes this as “a high evidentiary standard.” Renée Gentry, a practicing vaccine injury lawyer who directs the Vaccine Injury Litigation Clinic at George Washington University, says it’s a much higher bar than what the earlier vaccine injury compensation program requires, which contributes to a much lower rate of successful claims.
The Countermeasures Injury Compensation Program’s nature as a small emergency program has seen its capacity strained by a flood of COVID-related injury claims. Of the 11,806 COVID-related claims filed, 10,887 are still pending. Those four cases where COVID compensation was paid out didn’t come until after April 2023, over two years since the first vaccines were administered.
Pain and Suffering
The shortcomings of CICP are all too apparent for the people who are forced to wade through it. Even folks who seem to have done everything right are left waiting or disappointed by the program.
Fox filed her claim in May 2021, which was relatively early in the immunization campaign. She also had clear diagnoses from well-credentialed doctors linking her conditions to her COVID-19 vaccination. Fox says she provided the program with no shortage of documentation as well.
After filing all that paperwork, she hasn’t been idle either. After months of not hearing anything back from CICP, Fox started to reach out repeatedly to anyone she thought might be able to move the needle. She spoke repeatedly with representatives from Sen. Jeanne Shaheen’s and Rep. Chris Pappas’ offices. She also kept calling program administrators, trying to figure out what was taking so long.
“I’m sure they saw my number, and said ‘Ah, Fox, oh no, not her [again]’,” she jokes.
Her congressional representatives did reach out to CICP on her behalf. That was at least effective at getting program administrators to call Fox personally twice, once in July 2022 and again in June 2023. But each time, they could only offer her reassurance that her paperwork had been received. On both calls, Fox says she was told that the program was vastly overburdened by the flood of COVID-19 claims it had received. She, like thousands of others, would have to wait.
The few decisions on COVID-19 claims that have trickled out haven’t offered much relief to the people who’ve received them. That includes Cody Flint, one of the 894 people who’ve had their COVID-related claims rejected.
Flint was vaccinated in February 2021, when he received a single Pfizer dose. He says that he started to feel headaches and had affected vision within 30 minutes of the shot. He was still experiencing symptoms two days later when he headed to his job as a crop-dusting pilot.
While flying that day, he started to experience extreme tunnel vision, followed by a sensation he describes as “a bomb [going] off in my head.” He barely managed to get his plane back to his runway, where his coworkers found him slumped over his controls and shaking.
He was diagnosed with perilymphatic fistula (or tear of the inner ear) caused by elevated intracranial pressure – which could only be relieved through repeated draining of his spinal fluid. Given the timing of his symptoms and the fact that he’d passed a flight physical just a couple weeks prior, his doctors said his condition was almost certainly caused by the vaccine. His injury prevented him from returning to work as a pilot, and his mounting medical bills saw him draw down all of his savings.
In April 2021, Flint filed a claim. In May 2022 – just a few weeks after Sen. Cindy Hyde-Smith asked HHS Secretary Xavier Becerra about his case specifically in a committee hearing – Flint’s claim was rejected. The program’s medical reviewers told Flint that it was more likely his injuries were caused by barotrauma from flying a plane.
He petitioned for a reconsideration of his case. His doctors argued that there was no way he’d have experienced barotrauma from flying just a few hundred feet off the ground. Commercial airliners, they noted, are pressurized at 6,000 to 8,000 feet of elevation. Flint’s lawyers also submitted recent studies linking the symptoms he’d experienced to COVID-19 vaccinations.
Nevertheless, a separate medical reviewer at HRSA upheld the CICP’s initial denial in January 2023. That letter succinctly stated that HHS has “no appeals process beyond this reconsideration” and “there is no judicial review of a final action concerning CICP eligibility.”
Efforts at Reform
The federal government’s liability protections for COVID-19 vaccines aren’t scheduled to expire until the end of 2024. Once they do, those claiming a vaccine injury will be able to pursue claims against vaccine manufacturers in state courts.
While liability protections remain in effect, the federal program is injured claimants’ only potential source of compensation.
Whether or not the HRSA succeeds in boosting staffing in line with its statement to RCI, those seeking compensation have started to get organized. They’ve formed the group React19, which is dedicated to advocating for additional research into the side effects of COVID-19 vaccines. It’s grown into a network of tens of thousands of people who say they suffered adverse injuries from the shot. Flint, the pilot, is on its board of directors.
“It’s a very pro-vaccine community,” says Christopher Dreisbach, the group’s legal affairs director. “You say anything about vaccine injuries, you’re branded as anti-vaxxers. We are pro-science, we are not political. We’re just dealing with a very politicized issue.”
He says the politicization of vaccines has made their efforts at compensation reform a challenge.
When the CICP, and the 2005 Pandemic Response and Emergency Preparedness (PREP) Act that created it, were first being debated, Republican lawmakers were its main advocates, while its main critics were Democrats. The partisan politics of the program and liability protections for pharmaceutical companies has done a 180 since COVID.
In 2005, Rep. Sheila Jackson Lee argued during the House floor debate on the PREP Act that the law’s liability shield would leave injured healthcare workers with little protection or chance of compensation. Come 2023, she would return to the floor of the House to argue in favor of mandating those same healthcare workers receive a vaccine covered by the PREP Act’s liability shield.
The PREP Act’s harshest critics during COVID, meanwhile, have mostly been Republicans.
“I call the PREP Act medical malpractice martial law,” says Rep. Thomas Massie, who complains that its liability shield is both incredibly broad and improperly preempts state law. “I think it’s sort of anathema to the way our government is set up. I found it hard to believe that Congress would pass something, much less that a Republican president would invoke it.”
In March 2022, Sen. Mike Lee introduced a bill that would have amended CICP to give claimants the same framework for pursuing compensation as the VICP. They could file in Federal Claims Court and receive an expedited, judicial adjudication of their injury claim.
Gentry argues that it would be far simpler to just move the COVID-19 vaccines into the VICP program, which already has a successful track record of adjudicating injury claims. In order for that to happen under the law that created the VICP, the CDC needs to recommend the vaccines for routine administration to children (which has already happened) and vaccine manufacturers would have to start paying excise taxes. That latter condition will require action from Congress.
VICP needs a number of updates as well, says Gentry, including expanding the number of special masters to handle the backlog of cases and increasing the available levels of compensation (which haven’t been updated since the 1980s).
Increasing the number of special masters is particularly important if the VICP program is going to be expected to process tens of thousands of COVID claims, she says. But she argues it’s the best way of getting the vaccine injured out of CICP and into a program that will work for them. “If you’re taking away someone’s constitutional right to sue, you really have to give them a reasonable and meaningful alternative and that’s what this program is, for all of its faults,” says Gentry.
While efforts at reform in Washington lumber on, React19 has started a privately funded compensation program that’s thus far paid out $552,000.
“Is that making a meaningful difference to all the vaccine injured everywhere? No, that’s not enough,” says Dreisbach, but he notes that it’s far more than what CICP has paid out. “That should be pretty embarrassing to the federal government.”
Featured Video
Chinese jet fuel and the myth of energy independence
or go to
Aletho News Archives – Video-Images
Book Review
Former Insiders Criticize Iran Policy as U.S. Hegemony
By GARETH PORTER | CounterPunch | February 27, 2013
“Going to Tehran” arguably represents the most important work on the subject of U.S.-Iran relations to be published thus far.
Flynt Leverett and Hillary Mann Leverett tackle not only U.S. policy toward Iran but the broader context of Middle East policy with a systematic analytical perspective informed by personal experience, as well as very extensive documentation.
More importantly, however, their exposé required a degree of courage that may be unparalleled in the writing of former U.S. national security officials about issues on which they worked. They have chosen not just to criticise U.S. policy toward Iran but to analyse that policy as a problem of U.S. hegemony. … continue
Blog Roll
 Aletho News
Aletho News- Why no power can undermine Iran’s eternal dominance over the Strait of Hormuz
- Is The War Against Iran Over?
- Iran war will leave long-term ‘scar’ on Wall Street, investors warn
- How Iran decimated US power projection in West Asia: Military lessons of 40-day war
- Iran’s report details US-Israeli war crimes in targeting schools, hospitals, livelihoods
- NATO’s Slow Fracture: How Trump’s Iran War Exposed the Instrument of Hegemony
- Chinese jet fuel and the myth of energy independence
- Ukraine Sea Drone Fired From Libya Hit Russian Tanker in Mediterranean
- IRGC: Iranian forces launched no attacks during ceasefire hours
- Trump Administration Moves To Automate U.S. Military Draft Registration
- If Americans Knew
- TCN: Is Israel Blackmailing President Trump?
- Israel killed at least 303 Lebanese yesterday – who were they? Daily Update
- Amnesty: Urgent – Protect Lebanese civilians from brutal escalation in Israeli attacks
- Is The War Against Iran Over?
- Inside the Israeli army’s propaganda wing
- Hundreds of Gaza Amputees Stranded in Legal Limbo
- The gallows law: Israel moves toward executing Palestinian children
- Tucker Carlson: The Path to Peace requires ending ‘special alliance’ with Israel
- This is ceasefire? Israel’s biggest massacre yet in Lebanon, another journalist killed in Gaza – Daily Update
- Tucker Carlson on Israel: This Is the Behavior of an Ally? Really?
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
