Evidence presented to the Scottish Inquiry
Tragic testimonies ignored by mainstream media
Health Advisory & Recovery Team | July 30, 2024
The Scottish Inquiry has heard repeated testimonies on a wide range of topics, but what has been said in relation to what happened in care homes during lockdown is particularly striking. The stories are those of neglect, abuse, denial of healthcare and repeated misuse of end of life medication resulting in deaths. Witness after witness has given concurring evidence.
These stories have only really reached our attention thanks to the work of an independent citizen journalist (“Dave”) on Twitter and Substack. Neil Oliver has been the only mainstream journalist to have reported on these stories on his show in GB News, including interviews with our two co-chairs, Dr Clare Craig and Dr Jonathan Engler.
Here we publish a summary of the evidence from one woman which manages to encompass almost every aspect of the harm caused in care homes. It is the story of her grandmother who was admitted to a care home for mild dementia in autumn 2020.
“My gran was a very mischievous little old lady who was great fun and very talkative. She used to be a very active person when she was younger and tried to keep that up when she was older but, in her later years, she was less active due to widespread pain, and she was unsteady on her feet.”
After a fall “Social Services then intervened and said that they felt my gran should be in a more regimented type setting.”
“I actually took her to the home and that was very difficult as I just had to hand her over to a care home staff member and leave her as I was not allowed in.”
The staff called her by the wrong name but she didn’t know because she depended on lip reading and they were all masked.
~1st Nov 2020:
Positive test result for covid they called to say “my gran had tested positive but that she was fine and that they would keep us updated.”
2nd Nov 2020:
Granddaughter asked to authorise Do Not Resuscitate:
“My answer first of all was, ‘Well, why are you asking me that, as you said she only had mild Covid?’. My second point was that this was not a decision I would make at the moment as my grandmother was lucid, still talking and it would be a discussion to have with her.”
Despite this, a DNR was put in place without proper authorization.
3rd Nov 2020:
They proposed giving her a “mild sedative” to keep her from removing her nasal cannula. The family agreed, not realising it was Midazolam, which can suppress respiratory function.
“On the 3rd November 2020, about 3 o’clock in the afternoon the care home contacted my mother to explain that her (grandmother’s) oxygen saturation had dropped but that it was generally due to the fact that she had a nasal cannula and that every time she went to the toilet she kept forgetting to put it back in.”
“At this point my grandmother was eating and drinking by herself, moving to the toilet herself, that there was only mild symptoms and that they were giving her the nasal oxygen just as a precaution as her stats were a little low but, with the cannula in, she was fine. Her stats had actually improved from the previous day according to her medical records.”
“I later found out my grandmother was on a full end of life protocol put on place by the doctor “just in case”. I don’t understand why this was administered as we were at no point informed that she was end of life and if we had been then why had we not been called to be with her? The way I look at it is that I think they have looked at her notes and seen the medication from the earlier shift and thought that she was “end of life”. My mum was never told it was Midazolam when the home asked if they could give my gran a mild sedative.”
4th Nov 2020:
Granddaughter received a call at 4:11 am saying her grandmother had deteriorated. When she arrived at 4:30 am, she was told her grandmother had died at 4:20 am and went in.
“there were only three staff members, including one nurse, caring for 26 residents”
“She was stone cold and, in my opinion, she had been dead a lot longer than twenty minutes.”
“There was no cannula or oxygen tank in the room.”
“The funeral was also difficult because of the numbers that were allowed. I think a lot more would have been there in normal times. The people there had masks and there was no singing. My gran had loved music and she liked singing. Years before, my gran had given me full instructions for her funeral and I could only follow some of them. When you can’t fulfil somebody’s dying wishes because of rules, it’s hard. To go there and not be able to hug your mum or your dad or your brother is really difficult.”
It’s shocking to imagine one person experiencing all these horrific events. Now consider the reality: each of these horrors has actually happened to countless individuals. This widespread suffering is even more disturbing.
Shocking testimony regarding Remdesivir
Health Advisory & Recovery Team | July 30, 2024
Some rather shocking testimony has emerged from the USA.
An American doctor working in Everett, Washington (just north of Seattle) called James Miller, recently published an attestation which can be downloaded from here.
This was written to be filed as evidence with some attorneys who are petitioning state Attorney Generals to investigate hospital administrations and others responsible for what some regard as homicides. More about that can be read here.
The whole statement is worth reading, but in our view the following in particular stands:
From just that small extract, the following can be surmised:
- treatment was entirely protocol-driven — this person was well enough to be in a car and her “covid-19” was incidental; there were, however, recommendations in place that notwithstanding that, she should receive remdesivir just because a protocol said so
- usually these protocols were followed, regardless of clinical need, but just because a person had a positive test
- the protocols, however, could be flexibly applied and in this case a doctor decided that a valid criterion for making a decision was how “nice” the patient was
- a treatment was actively avoided here “because she was nice” — indicating that the doctors knew that per-protocol they ought to be giving treatments which they themselves knew to be harmful
The core departure from medical norms on display here from which this fortunate patient escaped — the rigid application of “protocols” by compliant unquestioning doctors resulting in harmful treatment being given — is an extremely disturbing phenomenon. It would be naive to think this only happened in the USA, and was seen only in association with the particular treatment — remdesivir — mentioned here.
It’s worth noting that the tenacious Jessica Hockett has written this article in which she suggests a series of further questions she’d like to ask Dr Miller.
Largest Study of Its Kind Finds Excess Deaths During Pandemic Caused by Public Health Response, Not Virus
By Brenda Baletti, Ph.D. | The Defender | July 19, 2024
A study released today of excess mortality in 125 countries during the COVID-19 pandemic found the major causes of death globally stemmed from public health establishment’s response, including mandates and lockdowns that caused severe stress, harmful medical interventions and the COVID-19 vaccines.
“We conclude that nothing special would have occurred in terms of mortality had a pandemic not been declared and had the declaration not been acted upon,” the authors of the study wrote.
Researchers from the Canadian nonprofit Correlation Research in the Public Interest and the University of Quebec at Trois-Rivières analyzed excess all-cause mortality data prior to and during the COVID-19 pandemic, beginning with the March 11, 2020, World Health Organization (WHO) pandemic declaration and ending on May 5, 2023, when the WHO declared the pandemic over.
The results, presented in a detailed 521-page analysis, establish baseline all-cause mortality rates across 125 countries and use those to determine the variations in excess deaths during the pandemic.
The researchers also used the baseline rates to investigate how the individual country variations in excess death rates correlated to different pandemic-related interventions, including vaccination and booster campaigns.
Not all of the results on a country-by-country basis were the same. For example, in some countries, mortality spikes occurred before the vaccines were rolled out, while in other places, the mortality spikes tracked closely with vaccine or booster campaigns.
In some places, excess mortality rates returned to baseline or close to baseline in 2022, while in others, the rates persisted well into 2023. Denis Rancourt, Ph.D., lead author of the study, told The Defender the disparities result from the complex nature of pandemic measures — and the data — in different areas.
Once Rancourt’s team was able to establish the baseline and excess mortality data for each place, they clustered and examined the data through different filters to interpret it, and drew several conclusions.
Data ‘incompatible with a pandemic viral respiratory disease as a primary cause of death’
The researchers established that there was significant excess mortality worldwide between March 11, 2020, and May 5, 2023.
Overall excess mortality during the three years in the 93 countries with sufficient data to make an estimate is approximately 0.392% of the 2021 population — or approximately 30.9 million excess deaths from all causes.
The conventional explanation for the excess mortality during the COVID-19 pandemic, Rancourt said, is that the SARS-CoV-2 virus caused virtually all deaths — and there would have been even more deaths if there hadn’t been a vaccine.
The variations in excess all-cause mortality rates across space and time, the authors wrote, “allow us to conclude that the Covid-period (2020-2023) excess all-cause mortality in the world is incompatible with a pandemic viral respiratory disease as a primary cause of death.”
They said the theory that the virus caused the deaths is propped up by mass virus-testing campaigns that should be abandoned.
‘Idea that vaccines saved lives is ridiculous’
Rancourt and his team cited several factors they believe disprove the theory that the virus caused a spike in all-cause mortality.
For example, they wrote that excess mortality surged almost simultaneously across several continents when a pandemic was declared, while there were no comparable surges in areas that had not yet declared a pandemic.
This suggests that pandemic interventions like lockdowns, which were implemented synchronously across many countries, likely caused the surges.
The researchers also pointed out the significant variation in mortality rates during the pandemic in all time periods, even across different political jurisdictions directly adjacent to each other. If the virus caused the deaths, it would follow that the infection fatality rate would be the same, or at least similar across political boundaries.
The researchers also found a lot of variability in death rates within countries over time, which also would not be an expected outcome if those deaths were caused by a pathogen.
Rancourt said they found “the idea that the vaccine saved lives is ridiculous,” and based on flawed modeling as he and colleagues also showed in a previous paper.
Here again, they found no systematic or statistically significant trends showing that vaccination campaigns in 2020 and 2021 reduced all-cause mortality.
Instead, they found that in many places, there was no excess mortality until the vaccines were rolled out, and most countries showed temporal associations between vaccine rollouts and increases in all-cause mortality.
Medical interventions — including denial of treatment — caused premature deaths
Rancourt said the excess deaths his team identified are strongly associated with the combination of two major factors — the proportion of elderly in a country’s population and the number of people living in poverty. Both factors increased peoples’ vulnerability to “sudden and profound structural societal changes” and “medical assaults.”
While the proximal cause of death may be classified on death certificates as a respiratory condition or infection, the researchers noted, they argue the true primary causes of death are actually biological stress, non-COVID-19-vaccine medical interventions and the COVID-19 vaccination rollouts.
The study provides an overview of plausible mechanisms for this hypothesis, including research showing that some people experienced severe biological stress from measures like mandates and lockdowns.
“If you structurally change the society by preventing people from moving, breathing, working, having their lives, having to stay at home, lock them in. If you do all these incredibly huge changes, structural changes in society, that is going to induce biological stress,” Rancourt told The Defender.
“There’s very compelling scientific evidence that biological stress is a massive killer,” he added.
Rancourt also pointed out that the stress of lockdowns affected poor people quite differently than it did people who could easily work from home, have food delivered and live relatively comfortably.
The authors also pointed to extensive evidence showing that medical interventions — including denial of treatment — caused premature deaths.
Such interventions included but were not limited to the denial of antibiotics and ivermectin against bacterial pneumonia, the systematic use of mechanical ventilators, experimental treatment protocols, new palliative medications and overdoses, isolation of vulnerable people and encouraged voluntary or involuntary suicide.
The March-April 2020 COVID-19 peak they identified in several countries is difficult to explain without such medical interventions, they wrote.
17 million excess deaths tied to COVID vaccines
Finally, the researchers projected that 17 million of the excess deaths they identified were associated with the COVID-19 vaccines, confirming the findings of their previous research on a smaller sample of countries.
Those vaccine-related estimations were based on analyses of places that had large spikes immediately following vaccination or booster campaigns and also by examining the numbers of vaccine doses and their relation to deaths over time.
Thirty percent of the countries they analyzed had no excess deaths until either the vaccine rollouts or the booster campaigns. And there were significant correlations between COVID-19 vaccine rollouts and peaks or increases in excess all-cause mortality. Ninety-seven percent of countries showed a late-2021 or early-2022 peak in excess all-cause mortality temporally associated with booster rollouts.
It is highly unlikely, the researchers wrote, that the vaccine-mortality associations are coincidental.
Rancourt noticed that people critical of this idea point to the fact that in some places, there are sometimes campaigns or booster campaigns that aren’t associated with spikes in excess mortality.
However, he said vaccination campaigns don’t always lead to such spikes because vaccination was not related to death in the same way in every situation. Vulnerability factors like the age of those vaccinated, the health of the population and other sociological factors related to stressors on the immune system change how they are affected by vaccine toxicity or the vaccines’ effects on the immune system.
Based on their analysis and interpretations, they concluded, “We are compelled to state that the public health establishment and its agents fundamentally caused all the excess mortality in the Covid period.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
British Columbia Royal College of Physicians and Surgeons Defeated on Judicial Notice
Case of Dr. Charles Hoffe Kills Deferral to Government Offices as Agents of “Truth”
Courageous Discourse™ | July 6, 2024
This was written by Canadian attorney Lee Turner after discussion with Dr. McCullough.
Dr. Charles Hoffe is a family and (former) emergency room physician in British Columbia who is the subject of disciplinary proceedings before the College of Physicians and Surgeons of British Columbia for making public statements about SARS-CoV-2, the safety and efficacy of the COVID-19 vaccines, and other alternative treatments including ivermectin. Hoffe has successfully defeated an application made by the College seeking judicial notice of the truth of facts alleged by the College concerning these issues. In its efforts to discipline the physician, the College has alleged that the statements made by the physician are misleading, incorrect or inflammatory and constitute professional misconduct. The College asked the discipline panel to take judicial notice of the following facts and thereby prevent the doctor from presenting any contrary evidence in his defence:
- The Covid virus kills or causes other serious effects;
- The virus does not discriminate;
- Vaccines work;
- Vaccines are generally safe and have a low risk of harmful effects, especially in children;
- Infection and transmission of the COVID-19 virus is less likely to occur among fully vaccinated individuals than for those who are unvaccinated; vaccines do not prevent infection, reinfection or transmission, but they reduce the severity of symptoms and the risk of bad outcomes;
- Health Canada has approved COVID vaccines, and regulatory approval is a strong indicator of safety and effectiveness;
- Health Canada has not approved ivermectin to treat COVID-19; and
- Health Canada advises that Canadians should not consume the veterinary version of ivermectin.
In its June 29, 2024 decision, the disciplinary panel of the College of Physicians and Surgeons of British Columbia declined to take judicial notice of items 2-5, did take judicial notice of items 7-8 (the straightforward ivermectin claims), and took judicial notice of a revised version of items 1 and 6.
The panel was prepared to take judicial notice of item 1 that reads: “COVID-19 can kill or cause other serious effects”.
The College explained their rationale for taking judicial notice of a revised version of item 1 by referencing evidence presented by the doctor in his defence that included the following:
- risk of severe disease and death from COVID-19 is extremely skewed to those above 70 years of age, especially those with multiple comorbidities. The average age of persons that died from COVID-19 in Canada was approximately 84 years old;
- very low proportion of COVID-19 related deaths in Canada occurred in those under 50 years of age-the data shows very high (although not 100%) survival rates for those under 70;
- average rate of lethality from COVID-19 for Canadians is much lower than estimates given by public health officials; and
- reported hospitalizations and deaths from COVID-19 have been over-counted, because many hospitalizations and deaths “with, and not from” COVID-19 were wrongly attributed to COVID-19
With respect to item 6, the panel endorsed findings of an earlier provincial Court of Appeal decision that held the safety and efficacy of any drug is always relative and as a rule the safety and efficacy of a pharmaceutical product cannot be discussed in such blunt fashion as to say that it “is” or “is not” safe and effective. The panel held that the issues raised in the citation should be determined based upon the evidence that is tested through cross-examination rather than by taking judicial notice of one party’s assertion of the facts, and in this case, based upon statements made by public health officials or public health agencies. The panel held that it was prepared to take judicial notice of the fact that Health Canada had approved the COVID – 19 vaccines, but declined to take judicial notice that Health Canada’s approval was a strong indicator of safety and effectiveness.
This decision on the issue of judicial notice, is consistent with the June 28, 2024 decision of the US Supreme Court in Loper Bright Enterprises et al. v. Raimondo Secretary of Commerce et. al. which overturned the landmark 1984 decision in Chevron v. Natural Resources Defense Council. The Chevron decision had given rise to what is commonly referred to as the Chevron deference doctrine. Under this doctrine, federal agencies had the power to interpret a law that they administer when that law is vaguely written, and courts were required to defer to the agency’s interpretation of a statute. In Loper, the US Supreme Court rejected the Chevron deference doctrine calling it “fundamentally misguided.” They said court should rely on their own interpretation of ambiguous laws rather than having to accept the agency’s interpretation. Commentators have suggested that the Chevron deference doctrine gave the powerful – the people who control the agencies like the FDA, CDC and FCC – a significant advantage in court making them essentially the ultimate decision-makers in interpreting ambiguous laws. Commentators have pointed out that many of these agencies are captive agencies with close ties, including financial ties, to the industries that they are charged with regulating and therefore they lack objectivity with respect to those industries. The ruling in Labor means that federal judges now have more authority to interpret these laws. The decision by the British Columbia Disciplinary Panel of the College of Physicians of Surgeons of British Columbia prevents regulatory bodies from saying “it is so because we say it is so”. They have to prove the facts they assert and those who disagree will be allowed to challenge those facts and present contrary evidence.
The case against Dr. Hoffe is far from over. This development is significant in that a government agency cannot make the rules, interpret them, and claim they hold the truth on an evolving scientific or medical issue.
Lee C. Turner, Partner, Doak Sherriff Lawyers, LLC, Kelowna BC V1Y 2A9
(Professional Law Corporation)
We Now Have Proof The COVID Vaccines Damage Cognition
Examining the causes and treatments of the common neurological injuries caused by vaccination
A MIDWESTERN DOCTOR | THE FORGOTTEN SIDE OF MEDICINE | JUNE 20, 2024
Story at a Glance:
• Subtle and overt neurological injuries are one of the most common results of a pharmaceutical injury.
• The COVID-19 vaccines excel at causing damage to cognition, and many of us have noticed both subtle and overt cognitive impairment following vaccination that relatively few people know how to address.
• For a long time, the hypothesis that the vaccines impaired cognition was “anecdotal” because it was based on individuals observing it in their peer group or patients.
• Recently large datasets emerged which show this phenomenon is very real and that the severe injuries we’ve seen from the vaccines (e.g., sudden death) are only the tip of the iceberg.
• In this article we will review the proof that vaccines are doing this and explore the mechanisms which allow it to happen so we can better understand how to treat it.
Note: I originally published this article a year ago. I am republishing it now because a robust dataset emerged which regrettably validates the hypothesis I put forward then.
When the COVID-19 vaccines were brought to market, due to their design I expected them to have safety issues, and I expected over the long term, a variety of chronic issues would be linked to them. This was because there were a variety of reasons to suspect they would cause autoimmune disorders, fertility issues and cancers—but for some reason (as shown by the Pfizer EMA leaks), the vaccines had been exempted from being appropriately tested for any of these issues prior to being given to humans.
Since all new drugs are required to receive that testing, I interpreted it to be a tacit admission it was known major issues would emerge in these areas, and that a decision was made that it was better to just not officially test any of them so there would be no data to show Pfizer “knew” the problems would develop and hence could claim plausible deniability. Sadly, since the time the vaccines entered the market, those three issues (especially autoimmunity) have become some of the most common severe events associated with the vaccines.
At the start of the vaccine rollout, there were four red flags to me:
• The early advertising campaigns for the vaccines mentioned that you would feel awful when you got the vaccine, but that was fine and a sign the vaccine was working. Even with vaccines that had a very high rate of adverse events (e.g., the HPV vaccine), I had never seen this messaging before. This signified it was likely the adverse event rate with the spike protein vaccines would be much higher than normal.
• Many of my colleagues who got the vaccine (since they were healthcare workers they were able to get it first) posted on social media about just how awful they felt after getting the vaccine. This was also something I had never seen with a previous vaccine. After some digging, I noticed those with the worst vaccine reactions typically had already had COVID and that their reaction was to the second shot rather than the first, signifying that some type of increased sensitization was occurring from repeated exposures to the spike protein. Likewise, the published clinical trial about Pfizer’s vaccine also showed adverse reactions were dramatically higher with the second rather than first shot.
• Once the vaccine became available to the general public, I immediately had patients start showing up with vaccine reactions, many of whom stated they received their flu shot each year and never had experienced something similar with a previous vaccination. One of the most concerning things were the pre-exacerbation of autoimmune diseases (e.g., spots in their body they previously would occasionally have arthritis in all felt like they were on fire). After I started looking into this I realized people were seeing between a 15-25% rate of new autoimmune disorders or exacerbations of existing autoimmune disorders developing after the vaccine, a massive increase I had never seen any previous vaccine cause.
Note: this was demonstrated by a February 2022 Israeli survey which showed 3% of vaccine recipients experienced a new autoimmune disorder and that 24% experienced an exacerbation of a pre-existing one, a rheumatologic database published in the BMJ that found 4.4% of recipients experienced an exacerbation of a pre-existing autoimmune disease, and a survey by a private physician of 566 patients which found vaccination spiked their inflammatory markers, causing their five year risk of a heart attack to go from 11% to 25%.
• About a month after the vaccines were available to the public, I started having friends and patients share that they’d known someone who had unexpectedly died suddenly after receiving the vaccine (typically from a heart attack, stroke, or a sudden aggressive case of COVID-19).
This was also extremely concerning to me, because reactions to a toxin typically distribute on a bell curve, with the severe ones being much rarer than the moderate ones. This meant that if that many severe reactions were occurring, what I could already see was only the tip of the iceberg and far, far more less obvious reactions were going to be happening, to the point it was likely many people I knew would end up experiencing complications from the vaccine.
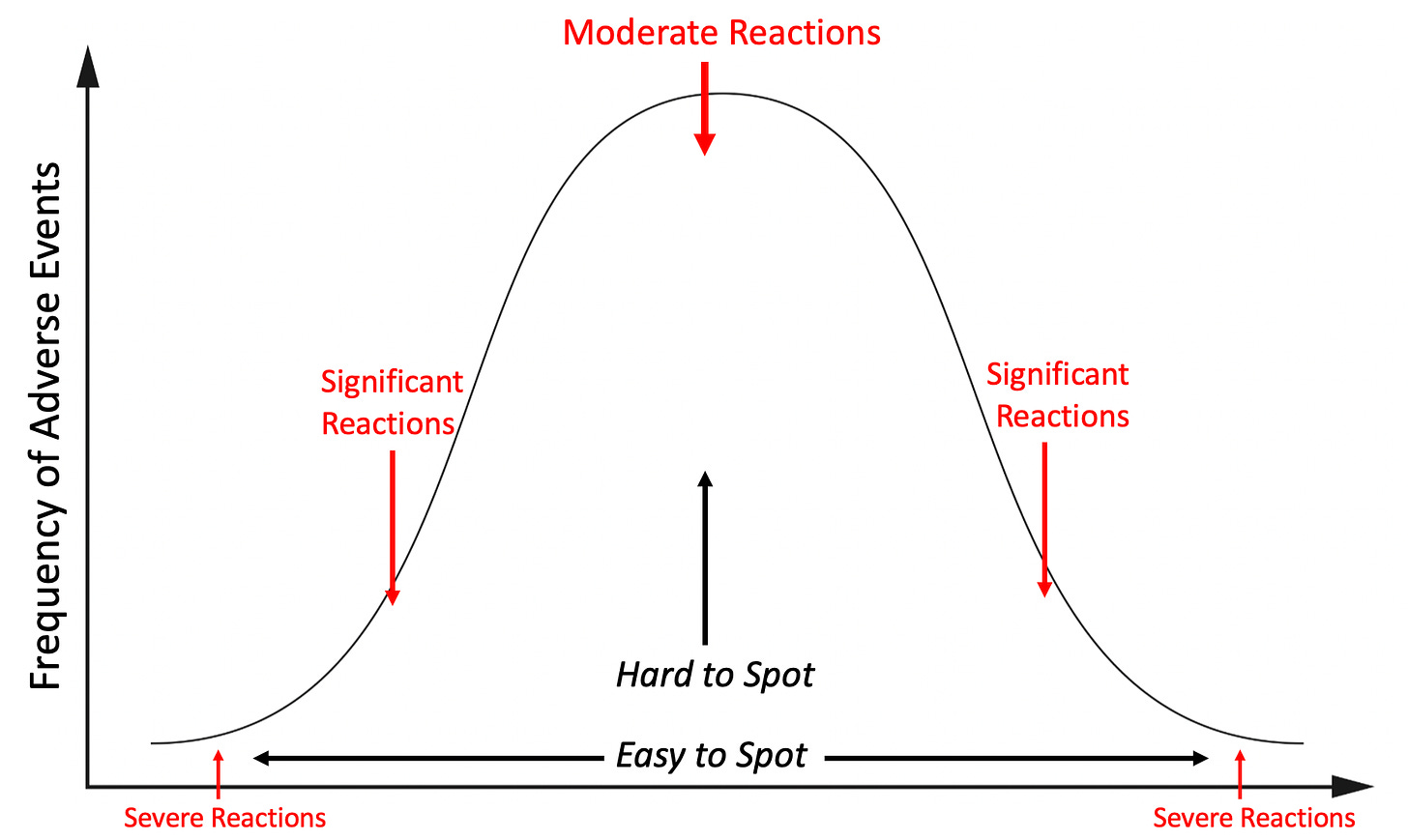
Note: the above graph is only illustrating one aspect of the picture as there will also be a much larger number of minor reactions, and even more invisible ones (e.g., a symptom occurs years down the road) or no reaction at all.
I tried to warn my colleagues about the dangers of this vaccine, but even when I pointed out Pfizer’s own trial admitted the vaccine was more likely to harm than help you, no one would listen to me. Not being sure what else to do, but not be willing to do nothing, I decided to start documenting all the severe reactions I came across so I could have some type of “proof” to show my colleagues.
This was something that was extremely important at the time since no one was willing to take on the personal risk of publishing something that went against the narrative (that vaccines were killing people) in the peer reviewed literature. Shortly after Steve Kirsch kindly helped launch my Substack, I decided to post the log I’d put together, and since there was a critical need for that information (as many had seen the same things I’d observed but no one was reporting them), the post went viral and created much of the initial reader base that made my Substack possible.
It was immensely time consuming to do the project (especially the verification of each story that was reported to me), so I ended the project after a year. During that time, I came across 45 cases of either a death (these comprised the majority of the 45 cases), something I expected to be fatal later on (e.g., a metastatic cancer) or a permanent and total disability. Additionally, in line with the previously described bell curve, I also came across many more serious but not quite as severe injuries.
What I found remarkable about this was that through a passive reporting system in my own limited social network (I learned of these cases because people reached out to me or someone off-handedly shared them with me), I alone found enough cases of severe vaccine injuries to justify pulling the COVID-19 vaccines from the market, yet, our healthcare authorities, who had access to thousands of times as much data as I did chose to pretend nothing was happening. Furthermore, from my own dataset (due to it being large enough to contain all the common COVID vaccine injuries), I accurately predicted most of the vaccine injuries that would be subsequently seen and only now (years later) are gradually being acknowledged.
In turn, we are now seeing clear signs that excess mortality has spiked across the globe, large polls are finding that one fifth of Americans know someone they believe were killed by the vaccines and because so much trust has been lost from this cover up, public health authorities are at last admitting there may be a problem—but they didn’t say anything until now because they “didn’t want to create vaccine hesitancy,” which coincidently is the same excuse which has been used for decades (e.g., Dr. Meier, a distinguished professor called out this behavior after the government unleashed an easily preventable polio disaster in 1955.
Patterns of Vaccine Injury
I’ve had a long term interest in studying pharmaceutical injuries because many of my friends and relatives have had bad reactions to pharmaceuticals. In most of these cases, ample data existed to show that reaction could happen (often to the degree it strongly argued against the pharmaceutical remaining on the market) and yet almost no one in the medical field was aware of those dangers, hence leading to my injured friends never being warned before they took the pharmaceutical or even while the injury was occurring (e.g., the doctor said they’d never seen anyone have those reactions, that whatever was happening was due to anxiety, and that they would soon end — when in reality it became a lifelong condition because the patient didn’t stop the drug in time).
My bell curve theory originally came about from examining all of their cases. I thus was interested to know if the distribution of adverse events from the spike protein vaccines would match what I had observed with previous dangerous pharmaceuticals and if what I saw personally did or did not match what everyone was reporting online (which is part of why I put so much work into making sure the log was both accurate and detailed).
One of the things that immediately jumped out at me during that logging process were the multiple cases of a friend’s parent in a nursing home receiving the vaccine, immediately undergoing a rapid cognitive decline which was “diagnosed” as Alzheimer’s disease and then dying not long after. At the time, I assumed these were most likely due to undiagnosed ischemic strokes as that was the most plausible mechanism to describe what I’d heard, but I was not certain as I could never examine any of these individuals for signs a stroke had indeed happened.
Note: despite many deaths in the nursing home population due to COVID and the vaccines, the number of people awaiting admission to a nursing home has significantly increased (shown by this large data set from the Netherlands). Given that individuals typically do not want to go to a nursing home unless they are no longe able to take care of themselves, this suggests that something new is causing the rapid development of debilitating cognitive impairment (e.g., dementia) in the adult population. Likewise, as Ed Dowd has repeatedly documented, there has been a large increase in physical and cognitive disability throughout the adult population which has significantly impacted the economy because of how many workers are being lost to vaccine injuries.
Steve Kirsch was contacted by a whistleblower who reported there has been a 25 fold increase in sudden dementia at the nursing home where she works. Similarly, like the cases shared with me, Kirsch has noted that (like me) he has frequently been contacted by relatives who reported a sudden onset of dementia in their beloved relative which was then swept under the rug. Furthermore, he has also collected numerous other forms of evidence corroborating this is indeed happening. These cases are really sad because the elders in nursing homes have very little ability to advocate for themselves, and most people will just write the cases off as “Alzheimers,” rather than seeing the red flag staring them in the face.
These cases were very concerning to me, as they signified (per the bell curve) that there was going to be a much larger portion of people who would develop less severe cognitive decline following vaccination.
Note: one of the most common types of injuries from pharmaceuticals are neurological injuries which both impair cognitive function and create psychiatric symptoms. This places patients in a difficult situation of being gaslighted by the medical system. This is because their doctors assume the psychiatric symptoms the patients are experiencing are the cause of their illness rather than a symptom of it, leading to the patient being told the illness is all in their head and continually referred for psychiatric help. One of the best examples of this occurred as a result of the abnormal heart rhythms (e.g., rapid anxiety provoking palpitations) caused by the vaccine damaging the heart which were consistently diagnosed as being a result of anxiety, even when a subsequent workup I requested showed heart damage was present. Remarkably, in the early era of vaccines, many doctors (as detailed here) acknowledged that vaccines caused neurological injuries which manifested as psychiatric symptoms, but now that recognition has been almost completely forgotten.
As I began seeing more and more signs of cognitive impairment following vaccination, I realized that what I observed mirrored what I had previously seen with chronic inflammatory conditions such as mold toxicity, HPV vaccine injuries, and lyme disease. Some of the examples included:
• Many people reported having a “COVID” brain where it was just harder for them to think and remember things. I sometimes saw this occur after more severe cases of COVID, but more frequently after vaccination, along with many instance of patients who per their timeline clearly developed it from the vaccine but nonetheless believed it had come from COVID.
• These issues tended to be more likely to affect older adults, but younger ones were more likely to notice (and complain) about them. In the case of older adults, I typically learned about them from someone else who had observed the cognitive decline rather than directly from the individual.
• I saw numerous cases of vaccine injured individuals who had trouble remembering or recalling the word they knew expressed what they were trying to communicate (this is also a common mold toxicity symptom).
• I had friends and patients who told me their brain just didn’t work the same since they’d received the vaccine. As an example, a few colleagues told me they started losing the ability to remember basic things they needed to practice medicine (e.g., medication dosages for prescriptions). They shared that they were very worried they would need to take an early retirement and that they thought it came from the vaccine but there was no one they could talk to about it (which understandably created a lot of doubt and anxiety).
• I saw cases of coworkers demonstrating noticeable (and permanent) cognitive impairment after I’d assumed they’d received the vaccine. Their impairment was never mentioned or addressed (rather the physician kept on working, did not perform as well, and in some cases retired).
• I met significantly injured vaccine injured patients who told me one of the primary symptoms was a loss of cognitive functioning they had taken for granted throughout their life. In many cases following treatment of their vaccine injury, their cognition also improved.
• Colleagues who treated vaccine injured patients told me cognitive impairment was one of the common symptoms they saw and was particularly noteworthy because they had never seen anything like that happen to young adults. To quote Pierre Kory:
In my practice of treating vaccine injuries, one of the three most common symptoms I see is brain fog. So many of my patients had been in the prime of their lives, can now barely function, have significant cognitive impairment and need a lot of help from our nurses to carry out their treatment plans. I never imagined I would see any of this in people far younger than me and instead I see it every day. I bear witness to an immense amount of suffering on a daily basis that is hard to put into words.
• One of my friends (a very smart immunologist) developed complications from the first two vaccines and based on their symptoms was able to describe exactly which parts of their immune systems were becoming dysregulated. Against my advice, they took a booster and reported they suffered a significant cognitive impairment never experienced before in their lifetime. I feel this case was important to share as it illustrates how an exacerbation of a vaccine injury can also cause an exacerbation of cognitive symptoms.
Note: I also saw significant cognitive impairment occur in individuals who were acutely ill with COVID-19. This was not as unusual since delirium is a well known complication in patients hospitalized with a systemic illness (e.g., sepsis), but it seemed to happen more frequently than usual. However, in almost all cases, COVID-19 cognitive impairment resolved after their illness (even when they had been critically ill and required hospitalization) whereas the cognitive impairment I saw from the vaccines was often permanent (unless it was treated).
I specifically wanted to write this article for two reasons.
First, unless you’ve talked to a lot of people who have been through this, it’s really hard to describe what it’s like to gradually lose your mind and the basic cognitive function you relied upon to navigate the world—especially if everyone around you is telling you that it’s not happening and it’s all in your head. I wrote this article to give a voice to those people.
Second, despite Alzheimer’s disease being the mostly costly disease for America, most providers know fairly little about it and instead use it as a blanket diagnosis for anytime a patient shows signs of impaired cognition. This, I in turn would argue has been because there is minimal interest in understanding the causes (and treatments) of Alzheimer’s disease as there is so much more money in “research” for it and productive expensive (but useless and harmful) drugs for it.
Evidence of Cognitive Impairment
At the same time I was observing these effects, many rumors were also swirling around online that the vaccines would cause severe cognitive impairment and that we would witness a zombie apocalypse from the vaccine injuries.
This apocalypse of course never happened (which again illustrates why it is so important to be judicious with what one pronounces will come to pass—as our movement has repeatedly damaged its credibility by making easily outlandish and easily falsifiable predictions). Nonetheless, many have observed a suspicion cognitive impairment was occurring. For example to quote Igor Chudov’s article on the topic:
I own a small business and deal with many people and other small businesses. Most provided reliable service, would remember appointments, followed up on issues, and so on. I noticed that lately, some people have become less capable cognitively. They forget essential appointments, cannot concentrate, make crazy-stupid mistakes, and so on.
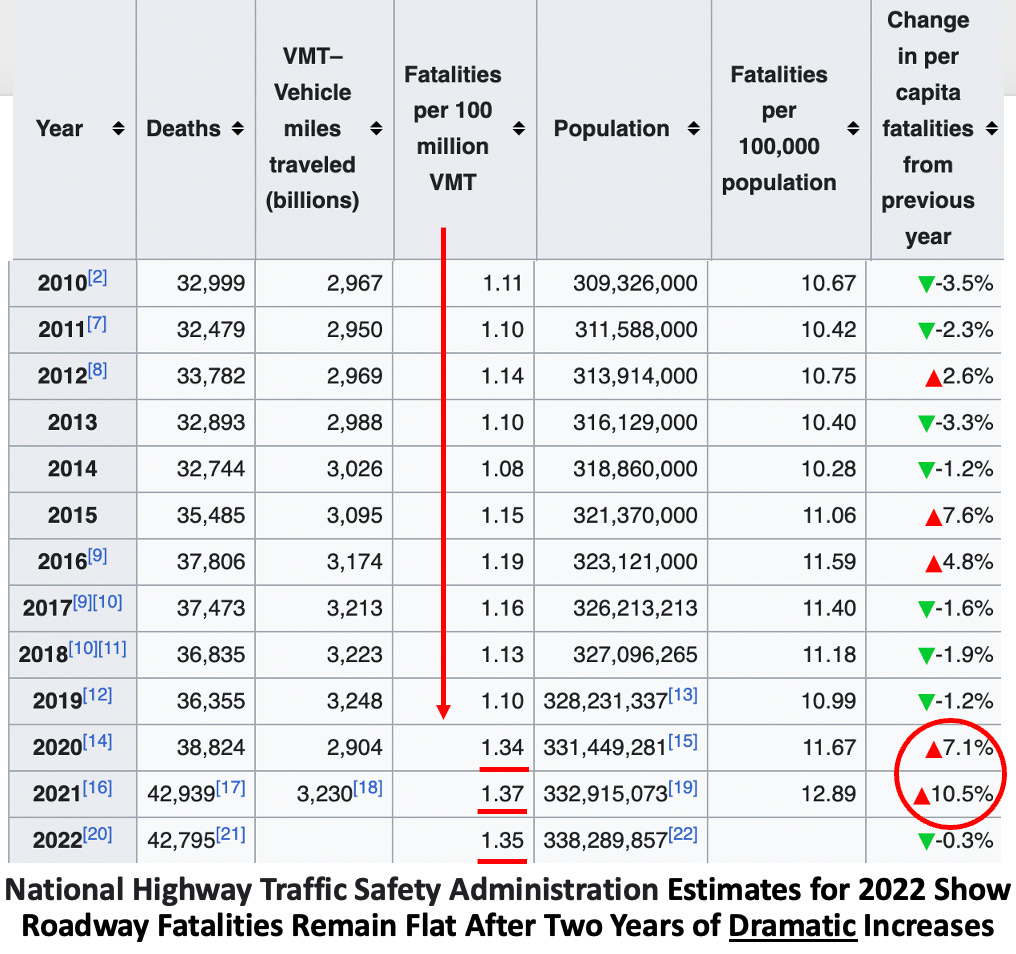
In my own case, in addition to poorly performing colleagues, the most evident change I noticed was a worsening of drivers around me and had quite a few near misses from impaired driving.
The great challenge with these situations is that it’s very hard to tell if something is actually happening or your perception is simply a product of confirmation bias. For this reason, while I was comfortable asserting my belief the COVID-19 vaccines were causing the severe injuries on either end of the bell curve, I avoided doing so for many of the less impactful injuries in the middle where it was much more ambiguous if what I was observing was “real” or simply my own biased perception of the events around me. Because of this, amongst other things, I never mentioned the changes in driving I observed.
Note: after I posted the original article many of the readers stated they too had observed a significant worsening in the behavior of drivers around them. I was then pointed to this dataset, which suggests this issue was happening, but is difficult to properly assess because COVID-19 can also cause cognitive impairment and less people were driving in 2020 and because the dataset still has not been updated since 2022.
Recently, Igor Chudov was able to identify another dataset from the Netherlands which further corroborated that we were indeed facing a massive cognitive decline:
Primary care data for January to March 2023 showed that adults visited their GP more frequently for a number of symptoms compared to the same period in 2019. Memory and concentration problems were significantly more common than last year and in the period before COVID-19. Where these symptoms are concerned, the difference compared to 2019 is growing steadily in each quarter.
In the first quarter of 2023, there was a 24% increase in GP [general practioner] visits related to memory and concentration problems among adults (age 25 years and older) compared to the same period in 2020. This is evidenced by the latest quarterly research update from the GOR Network. The increase in memory and concentration problems of adults seems to be a longer-term effect of the coronavirus measures as well as SARS-CoV-2 infections.
More specifically they found:
• No increase was observed in adults under 25 years old.
• A 31% increase was observed in those 24-44 years old.
• A 40% increase was observed in those 45-74 years old.
• An 18% increase was observed in those over 75 years old.
Note: previous rounds of this survey, in addition to the cognitive issues described above, found that since 2019, the general population has also experienced worsening mental health (e.g, anxiety, depression or suicidal thoughts), sleep problems, tiredness, and cardiovascular issues (e.g., shortness of breath, dizziness or heart palpitation).
Typically, patients, less than 75 years old are unlikely to visit their doctors for cognitive issues. Taken in context with this data, it means there is a stronger case that the (massive) increases in cognitive issue for those under 75 were caused by something that happened after 2019. Additionally, since there were already a large number of visits for cognitive impairment in the elderly, the lower percentage increase is slightly misleading in quantifying the extent to which everyone was affected. For example to quote the previous report:
Primary care data showed that adults visited their GP somewhat more frequently for sleep problems in October–December 2022 than in the same period in 2019. This was particularly striking in the oldest age group (75 years and older).
Note: poor sleep is one of the primary causes of cognitive impairment (or dementia) and sadly also commonly impaired after COVID-19 vaccination.
All of this data put health officials in a bit of an awkward situation since publishing data demonstrating large scale cognitive impairment directly undermines the narrative they previous had committed themselves to. Nonetheless, the authors of the report were significantly more candid than many others before them:
The source of this increase in memory and concentration problems is unclear. A possible explanation could be that COVID-19 measures caused accelerated cognitive decline among people who were starting to have problems with memory and concentration (66 years on average).
COVID-19 was of course cited as a potential cause (which, as discussed above can sometimes cause long term cognitive impairment):
A supplementary explanation could be that some of these people have long-term symptoms after COVID-19. Various studies have shown that memory and concentration problems are common in post-COVID symptoms. Other infectious diseases, such as flu, can also cause these symptoms. However, recent studies have shown that long-term memory and concentration problems are much more common after COVID-19 than after flu. In addition, these symptoms are more common in older age groups. The figures provided by GPs are consistent with this expectation.
Fortunately, the authors acknowledged that long COVID could not be the primary explanation for what was occurring, and instead alluded to the elephant in the room—the vaccines.
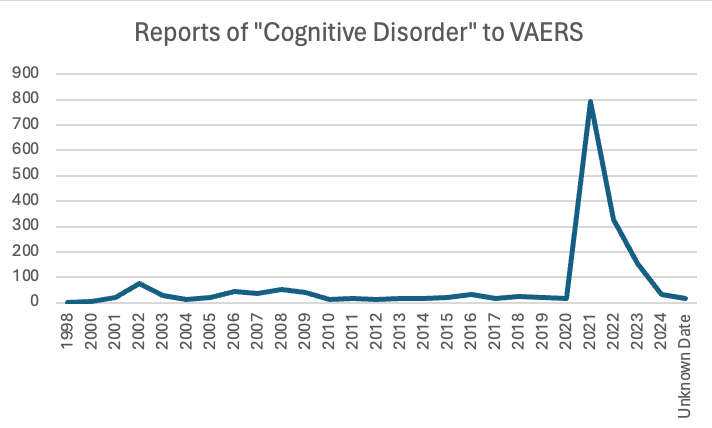
Finally, Ed Dowd has identified numerous government datasets demonstrating that widespread impairment and disability has occurred since the vaccine rollout. Likewise, VAERS detected a massive spike in cognitive issues being reported to it after the COVID vaccines hit the market.
Note: one of the key components of the COVID-19 vaccine push was to make it politically incorrect to raise any data-based objections to the vaccines, and thereby stifle any inconvenient discussions of the topic which would have exposed how dangerous these products were. Because of this, I repeatedly heard stories (like this one) of liberals (including famous ones) who had severe vaccine injuries but could not discuss them with their peers, as doing so meant being outcasted from their social group and being cut off from job opportunities, in effect placing them in a similar position to where gay men were in the early 1980s (as coming out often meant being ex-communicated by many close to you). Fortunately, things are now changing (as there are too many injuries to hide) and we are beginning to see more and more prominent individuals “come out of the closet” and admit they were vaccine injured.
Data Transparency
Making decisions has always been difficult and history is rife with catastrophic errors made by individuals who got it wrong. Because of this, a variety of solutions have been developed over the years (e.g., having a committee go through a process to decide something as it is unusual to have a leader who excels at making excellent decisions), all of which have serious short comings.
In recent years, we’ve had a push for data to become the means to making decisions. On one level, I think this is an excellent approach. For example in sales and the internet (which is where I suspect much of the push for data originated from), large amounts of data are used on a daily basis and constantly used to refine how a marketing campaign internet platform is set up so that it can maximize profits.
However, in many cases (e.g., those outside of business and sales), that same incentive to optimally utilize the data and adjust what’s being done due to the data does not exist. Because of this, while we have a large emphasis on gathering data, most of it is never utilized. For example, in medicine, we force our healthcare workers to do an immense amount of data entry, yet, we never combo the electronic health records to determine which drugs are unsafe or ineffective (which is very easy to do). I would argue this is because the healthcare system receives so much unconditional money they have no incentive to produce better results and because the pharmaceutical industry receives so much money for toxic drugs, it has every incentive to keep them on the market.
In order to enshrine this paradigm, industry had to both create the mythology that data should both be viewed as the ultimate authority we must all be subservient to, but simultaneously not be something that is publicly available. This in turn was done by arguing that data was “costly proprietary information and intellectual property must be protected” or that it “contained personal health information which could not ethically be disclosed to protect the patients.”
In turn, science has very much become us being expected to trust the team of “experts” who analyze a dataset, and not surprisingly, this process lends itself to corruption.
For example, the only publicly available vaccine injury database VAERS, exists because activists forced it to be required by law, and ever since it was made, the government (along with the medical establishment and the media) has done everything it can to undermine VAERS (discussed further here). Because VAERS reputation had been sullied, for the COVID vaccines, a new monitoring system, V-Safe, which was designed to address the short comings of VAERS was created. However, before long, activists discovered that V-safe did not allow the majority of adverse reactions to be reported in it, and furthermore would not make the data available for outside analysis. Instead, we were given access to a Lancet publication which concluded that:
Safety data from more than 298 million doses of mRNA COVID-19 vaccine administered in the first 6 months of the US vaccination programme show that most reported adverse events were mild and short in duration.
Reports of seeking medical care after mRNA vaccine were “rare”… Serious adverse events, including myocarditis, have been identified following mRNA vaccinations; however, these events are rare. Vaccines are the most effective tool to prevent serious COVID-19 disease outcomes and the benefits of immunisation in preventing serious morbidity and mortality strongly favour vaccination.
Through lawsuits, activists were eventually able to obtain the V-safe data where they then discovered the above study had lied and there were a lot of serious issues within that database. For example, the above article claimed 0.8-1.0% of vaccine recipients required medical care, whereas the raw V-safe data show 7.7% did—on average 2.7 times, which meant that every 4.8 vaccinations caused one medical visit.
Likewise, throughout the pandemic, we had almost all of the scientific journals refuse to publish anything which challenged the narrative (e.g., I’ve been in touch with numerous teams that have run into an endless number of roadblocks to publish contrarian data). Yet, simultaneously, those journals were willing to contort the existing (poor quality) data as much as possible if that supported the narrative (e.g., Pierre Kory has shown how multiple studies whose data demonstrated ivermectin benefitted patients concluded ivermectin was useless and then widely promoted for having debunked ivermectin).
Similarly, Deborah Birx and Anthony Fauci were essentially responsible for the disastrous COVID-19 response (e.g., useless but harmful mass testing, masking and lockdowns), as both within the White House and in the (fawning) media, they relentlessly and successfully pushed for those approaches regardless of how much protest they met. As both news clips and eye witnesses testimonies showed, Fauci and Birx constantly used “the data” to justify their their approach (e.g., when challenged, Birx would often say “I’m all about the data” while Fauci always cited “the data” whenever he advocated for a policy on national television).
However, Scott Atlas (who was with them on the White House COVID-19 task force) discovered that they both never presented scientific papers to the task force, lacked the ability to critically evaluate scientific research, they did not understand basic medical terminology, they would make patently absurd and non-sensical interpretations of their data, and adamantly refused to consider any of the data which challenged their narratives. In many cases, what he witnessed was so absurd he likened it to being in the Mad Hatter’s tea party from Alice and Wonderland, whereas I felt it was a real life version of this iconic Whitehouse scene from Idiocracy.
Because of the widespread lack of data transparency, a few different approaches exist.
First many (e.g., Drs. Peter Gøtzsche and Malcolm Kendrick) have gradually become experts in “data forensics” and being able to identify the tricks the pharmaceutical industry uses to doctor research so that the data always ends up supporting the sponsor’s desired conclusion. What I personally find depressing about this is that a fairly repetitive playbook is used to doctor studies, but the top medical journals consistently turn a blind eye to this, always publish that deceptive research, and in most cases refuse to correct it once the public points out the fraud.
Second, many (e.g., Steve Kirsch) argue that if data is not made publicly available, one must assume it’s incriminating and the data’s owners are lying about what’s in it (e.g., that the COVID vaccines are safe and effective). For example, for decades activists have been trying to get access to the data from the CDC’s Vaccine Safety Datalink (as it has the information which could definitively say if vaccines are safe or effective) but they’ve had no success—which in turn suggests that database is full of incriminating information for the vaccine program. Likewise, given the disconnect between what I was seeing with COVID-19 vaccine injuries and what the government was reporting (the only message we ever heard was “safe and effective!”) it was clear to me the government had very bad data and had made the decision to do whatever could be done to cover it up—a prediction which sadly has continued to hold true.
Third, we have to rely upon publicly available datasets which happened to capture the effects of vaccination programs (e.g., the one which tracks annual disability rates in the USA registered a huge spike after the COVID-19 vaccines hit the market). Unfortunately, while these clearly show that an issue exists which needs to be investigated, they do not definitively prove causality, and hence are often dismissed on that basis (much like VAERS is).
Fourth, we have to rely upon whistleblowers. Unfortunately, when this happens, the national government typically targets them for violating “patient confidentiality.” For instance, when a New Zealand whistleblower released fully anonymized data showing the vaccines were killing people, his government charged him with crimes carrying a maximum seven year prison sentence.
Note: the most recent example of government persecution of whistleblowers happened in Texas, where in February 2022, Texas’s government declared providing gender transitions to minors constituted child abuse, and June 2023, outlawed it. In response to this, in March of 2022, one of the largest Children’s hospitals in Texas (and where Peter Hotez exerts a significant amount of influence) announced it would stop providing transgender hormonal therapies. This however was a lie, so in April 2023, a concerned surgeon who had previously worked at the hospital convinced the hospital to give him access to their medical records, and then leaked anonymized medical records demonstrating that the hospital was continuing these practices, as in his opinion, under Texas law, this was child abuse he was required to report. In response to this, the Biden administration (not Texas) charged him with four felonies which carry a maximum penalty of 10 years in prison, which is very different from how other HIPPA violations have been handled. Likewise, more recently, after another nurse at the hospital exposed that the hospital was committing Medicaid fraud by billing for transgender care but labeling it as something else (as Texas’s Medicaid program does not permit for those practices to be reimbursed), after which the FBI was sent to interrogate (and likely intimidate) the nurse.
All of this hence leaves us in a very disorienting position—how do we know who to trust? In turn, I would argue one of the largest reasons so many people trust the audacious lies the government tells us is because the alternative (not knowing who or what to trust) is arguably even worse.
In my own case, I’ve developed a very simple rule for navigating the scientific literature (and many other sources of information as well).
Step 1. Determine the biases and conflicts of interest of the publication source (e.g., most medical journals and their editors take a lot of money from the pharmaceutical industry and hence do not want to upset their sponsors—an issue we sadly also see in the mainstream media).
Step 2. Determine if the conclusion of a published study agrees with, challenges, or is relatively neutral to it’s publisher’s bias.
Step 3 Use this formula:
• Agrees with publisher—high likelihood the study is wrong and it’s probably not worth your time to look into it.
• Disagrees with publisher—high likelihood the study is correct and that a very high bar had to be passed for it to be published (along with significant pressure being exerted behind the scenes).
• Relatively neutral for the publisher—you can take the paper at face value when you analyze its methods and conclusions to see if they had a reasonable way to derive their conclusion. Additionally, while the most prestigious medical journals are corrupt, this category is the one area they shine in and often ensure high standards were met for publication.
South Korea’s Data
In November 2023 and March 2024, some very interesting data emerged from a team of South Korean researchers where they looked at the electronic health records for a quarter and then half of the population in Seoul (2.2 million for the first study and then 4.3 million for the second) and then compared the rates of a variety of new (non-serious) medical conditions in those vaccinated and unvaccinated over three months. From this, they found a variety of medical conditions had a significant increase in the vaccinated. Those increases were as follows (with a range existing depending on how long after vaccination they were compared and which COVID vaccines they received).
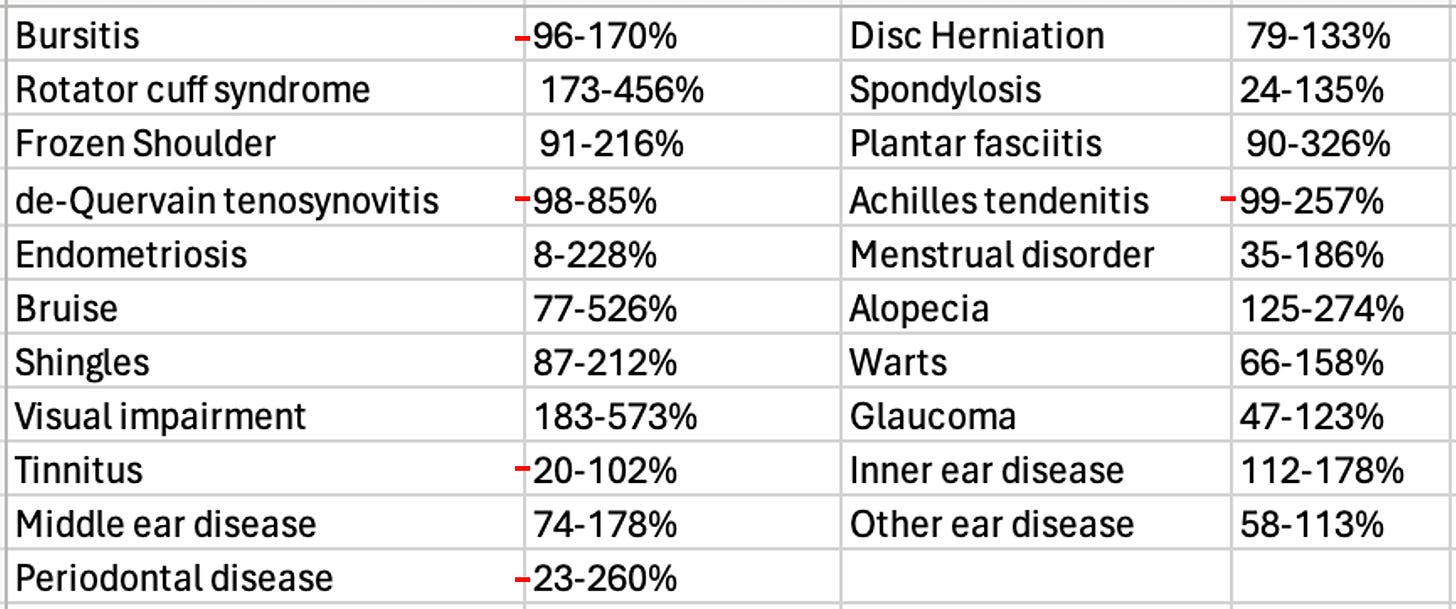
This was essentially a dataset we had been trying to get for over 2 years and it matched what we’d seen (e.g., many of these conditions such as shingles and alopecia [hair loss] appear to be strongly linked to vaccination). In turn, it both demonstrated that the vaccines were causing massive harm to society as millions of Americans suffer from these diseases and hence millions more developed them.
Unfortunately, after I analyzed them, I realized it was not appropriate for me to discuss them here as they were pre-prints rather than published articles, which either meant that they had fraudulent data (as it was quite extraordinary they got access to this data) or they were too politically incorrect for any journal to want to publish. While I felt the latter was much more likely, I was not sure which is was, so I avoided publishing that article (which was hard to do given how much time I’d put into it) as I did not want to fall into the trap of promoting something because it promoted my pre-existing biases and then misleading the audience here.
Note: if for some reason these studies disappear I have included the pre-prints below.
We hence tried to reach the authors (no success) and I patiently waited for the articles to leave the preprint server (which has still not happened).
However, recently. three other studies were published by the same team using the same dataset. The first one, (also from March 2024) analyzed the increase of ten common autoimmune disorders (autoimmune hepatitis, ankylosing spondylitis, hashimoto thyroiditis, hypertension, inflammatory bowel disease, primary biliary cholangitis, rheumatoid arthritis, graves, vitiligo, lupus).
This one stated only vitiligo was increased (by 174%), so it seemed plausible to me it could have been published, as it made a token admission the vaccines were bad (as they had a rare side effect from a disease most people don’t know about). Then, when I looked at the data, I noticed a few of the other conditions appeared to have also increased. In turn, since those increases weren’t mentioned in the article, I took that as a sign the article was deliberately omitting incriminating information from its conclusion so it could make it to publication (this happens a lot). Additionally, I was surprised the authors did not evaluate for polymyalgia rheumatica, as this seems to be one of the autoimmune disorders most distinctively associated with vaccination.
That article made me more confident the initial results were real—however since it was published in an obscure journal, I reserved judgement on it. Recently however, two very important ones came out.
Two weeks ago, the first was published in Nature (one of the top medical journals). It found that COVID vaccination resulted in a 68% increase in depression, a 44% increase in anxiety, dissociative, stress-related, and somatoform disorders, a 93.4% increase in sleep disorders, a 77% decrease in schizophrenia, and a 32.8% decrease in bipolar disorder. I was really surprised to see this be published, and took it as a sign there may have been a decision made to begin disclosing some of the harms of vaccination in the official medical literature. Additionally, I took this as an indication that this was an indirect admission neurologic issues also followed vaccination (due to the strong link between neurologic and psychiatric symptoms).
Note: the previously mentioned Israeli survey found that 4.5% of those who received a vaccine developed anxiety or depression, and 26.4% who already had either experienced an exacerbation of it.
Around the same time (three weeks ago) another article was published in a mainstream journal (or to be more exact “accepted for publication”). It analyzed individuals over 65 and found COVID vaccination increased the risk of mild cognitive impairment 138% and the risk of Alzheimer’s by 23%, and a smaller increase in vascular dementia and Parkinson’s disease the authors did not deem to be significant.
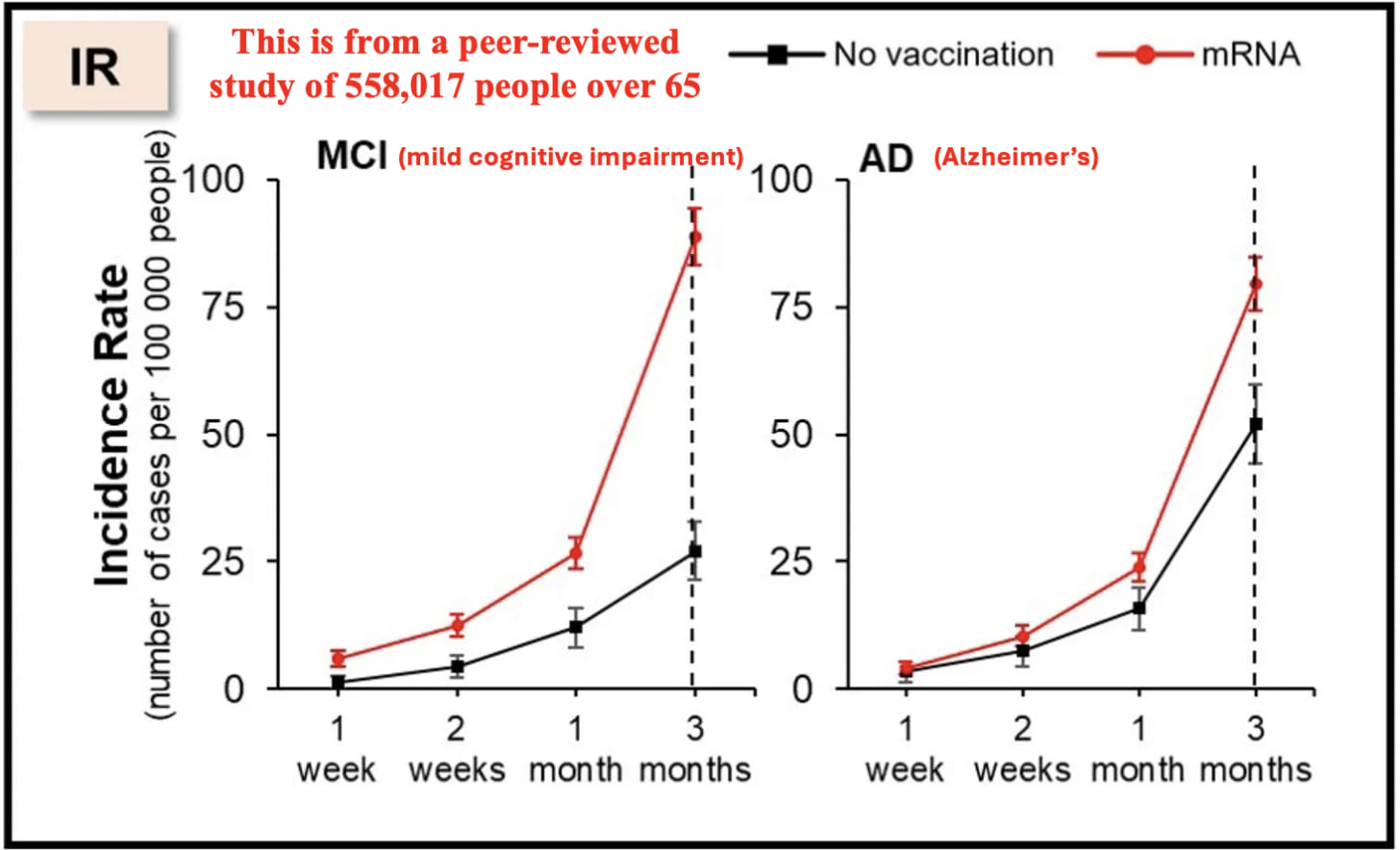
To put this in context, given that America spends over 300 billion dollars per year on Alzheimer’s disease, this single datapoint effectively means that the COVID vaccines cost the United States around 100 billion dollars. Additionally, as the authors only tracked the difference over 3 months (and it increased over time as these are both progressive diseases), the actual cost is likely greater, especially given that the elderly keep on receiving boosters. Likewise, it also makes a very strong argument for anyone who believes the vaccines damaged their cognition that this indeed happened.
Why Are The Vaccines Causing Cognitive Impairment?
My specific interest in studying spike protein vaccine toxicity arose because I suspected I would see many similarities to other pharmaceutical injuries I had observed previously and treatments that had developed for those injuries could be used to treat COVID-19 vaccine injuries. On Substack, I’ve tried to focus on explaining the areas that I believe are the most important to understanding this, zeta-potential, the cell danger response (CDR) and the treatments for Alzheimer’s disease. Note: Each of these is interrelated with and often causes the others.
Zeta Potential: Zeta potential (explained in detail here) governs if fluid in the body clumps together (e.g., forming a clot) or remains dispersed and capable of freely flowing. Additionally, it also influences if proteins will stay in their correct formation or misfold and clump together (with Alzheimer’s disease being characterized by misfolded proteins in the brain). Many different issues (discussed here) emerge when fluid circulation (be it blood, lymph, interstitial fluid or cerebrospinal fluid) becomes impaired. Since the spike protein is uniquely suited for impairing zeta potential, we have found restoring zeta potential (discussed here) often is immensely helpful during COVID-19 infections and for treating COVID-19 vaccine injuries. Many of those approaches in turn were initially developed from working with other vaccine injuries and cognitive decline in the elderly.
Note: the spike protein also has a prion forming domain, and many believe its responsible for the highly unusual amyloid (fibrous) blood clots seen in COVID-19 victims. Additionally, the COVID vaccines have been linked to extremely rare (and fatal) protein misfolding disorders such as the rapid dementia caused by CJD (discussed further here).
Cell Danger Response (CDR): When cells are exposed to a threat, their mitochondria shift from producing energy for the cell to a protective mode where the cell’s metabolism and internal growth shuts down, the mitochondria release reactive oxygen species to kill potential invaders, the cell warns other cells to enter the CDR and the cell seals off and disconnects itself from the body. The CDR (explained further here) is an essential process for cellular survival, but frequently in chronic illness, cells become stuck in it rather than allowing the healing response to complete.
Note: one common cause of impaired cognition are neurons becoming stuck in the CDR and hence not performing their cognitive tasks.
Understanding the CDR is extremely important when working with complex illnesses because it explains why triggers from long ago can cause an inexplicable illness, and why many treatments that seem appropriate (specifically those that treat a symptom of the CDR rather than the cause of it) either don’t help or worsen the patient’s condition. Many of the most challenging patients seen by integrative practitioners are those trapped within the CDR, but unfortunately, there is still very little knowledge of this phenomenon.
My interest was drawn back to the CDR after I realized that one of the most effective treatments for long COVID and COVID-19 vaccine injuries was one that systemically treated the CDR. Since many of the therapies that have been developed to revive nonfunctional tissue was developed by the regenerative medical field, I wrote an article describing how these approaches are applied to restore localized regions of dysfunctional tissue (which is sometimes needed to treat vaccine injuries) and another on the regenerative treatments that treat systemic CDRs (and are more frequently needed for vaccine injuries).
Alzheimer’s Disease (AD): since AD is one of the most costly disease in America, billions of dollars are spent each year in researching a cure for it. This research (which began in 1906) has had a very narrow focus on removing amyloid from the brain, and since the production of amyloid is a protective response from the brain, the decades of work to remove it have gone nowhere. Nonetheless, the FDA is presently working hand in hand with the drug industry to push forward ineffective, quite dangerous but highly profitable treatments for AD.
Remarkably, effective treatments do exist for AD and my colleagues have developed a few different methods that have successfully treated the condition. Additionally, one neurologist, Dale Bredesen developed a method for reversing AD that he proved worked in mulitiple publications (included a recent 2022 clinical trial)—something which no one else has done, but remarkably has been almost completely ignored by the neurological field.
All of these successful approaches utilize the following principles:
• Restore both the blood flow to the brain and the lymphatic drainage from it (which safely removes amyloid plaques). This often requires restoring the physiologic zeta potential and having a healthy sleep cycle. Additionally, AD is commonly linked to damage to the lining of the brain’s blood vessels, which is unfortunate because one of the most frequent toxicities of the spike protein is injury to the blood vessels (which has been shown in many autopsies—including within the brain).
• Treating the CDR (which causes chronic inflammation) and reactivating brain cells that became trapped in an unresolved CDR (which amongst other things requires reclaiming a healthy sleep cycle, providing the nutrients the brain needs to sustain itself, and mitigating the damage of neurotoxins like inhaled anesthetics).
Note: Bresden’s approach also emphasizes the importance of addressing chronically elevated blood sugar or insulin levels.
One of the most important things to recognize about AD is that it is a slowly worsening disease which often progresses over decades. In the early stages of AD (where it is the most reversible), minor cognitive changes occur, which (when possible to autopsy) correlate with tissue changes within the brain. In rarer instances, individuals can instead have a rapidly progressing form of Alzheimer’s (e.g., from Lyme) which strikes at a younger age and is often linked to the toxin exposure. Given how quickly the increase in AD appeared in both the patients I know and this dataset, I suspect it’s very likely the mechanisms behind the rapidly progressing forms of AD play a key role in the cognitive impairment and dementia we are seeing from these vaccines.
Conclusion
Many of the most successful people I know are willing to go against a crowd and act in spite of being afraid (e.g., they resisted the peer pressure to get the vaccine because they felt it was a good idea). Likewise, rather than looking to an authoritative source for advice, they tend to create preliminary assessments of what’s going on based on the limited data that’s available to them, and then act on it rather than waiting for a clear and definitive answer (or at least a safe one) to present itself.
In turn, as I’ve gotten to know many of the prominent dissidents in this movement, I’ve found they all had those traits in common (which likewise many of my extraordinary medical mentors did as well). For example, Steve Kirsch used this capacity to become a successful Silicon Valley entrepreneur. When the vaccines came out, he “trusted the science,” and immediately got one, but before long noticed numerous people he knew had had severe injuries from them, and rather than be in denial about it, recognized that chain of injuries was statistically impossible, began digging into it, realized the existing data showed we had a huge problem, and then began speaking out on it despite the fact much of the (left wing) peer group he’d belonged to for decades disowned him for doing so.
In my own case, for the COVID vaccines, I had initially come in with expectation (which formed as the virus broke out in Wuhan) that whatever “emergency” vaccine was pushed for it would have significant issues and the adverse events would be by and large covered up by the government (or only “discovered” years down the line). In turn, I concluded it was far more preferable for me to feel confident I could treat the infection when I eventually got it and develop natural immunity than it was to take a risk with the vaccines.
However, once I began seeing a high number of red flags the moment the vaccines hit the market, I realized that I had made a big miscalculation and these things were incredibly dangerous so I needed to shift my focus to preventing people from being harmed by them.
Furthermore, I took the bell curve theory into account and assumed that if I was seeing occasional deaths or severe cognitive degeneration following vaccination, it was likely that far more cases of cognitive impairment were occurring, and as this recent Korean study shows, that is indeed the case.
It is thus both quite tragic and remarkable that we now have a leadership which has so little accountability to produce quality results that things like the basic scientific process (which helped our country become one of the most powerful nations in history) is being completely disregarded and replaced with a dogmatic system which refuses to consider basic data points which more and more are proving themselves to be immensely costly to our nation.
Everything we are seeing now was incredibly predictable and represented a systemic failure in our system and a profound societal decline that must be reversed if we want our nation to be something which continues to provide the basic things we have taken for granted from it for most of our lives. I am especially worried as prior to COVID-19, our society was already struggling to reverse this decline, and since that time, we’ve been hit by a wave of cognitive impairment which can only further diminish our ability to address this.
College of Physicians and Surgeons of Saskatchewan suspends doctor for prescribing Ivermectin, fines him $44,784
Licence of Sask. doctor who prescribed Ivermectin for COVID-19 to be suspended
Dr. Tshipita Kabongo faced two sets of charges relating to unprofessional conduct, brought by the College of Physicians and Surgeons of Saskatchewan.
Author of the article: Brandon Harder
Published June 17, 2024
Regina doctor Tshipita Kabongo has admitted to unprofessional conduct in relation to two sets of charges brought against him by the oversight body for Saskatchewan physicians.
That’s according to Bryan Salte, associate registrar for the College of Physicians and Surgeons of Saskatchewan (CPSS).
Kabongo had one such charge brought against him in March of 2023 in relation to his failing to know and/or follow the CPSS Policy on Complementary and Alternative Therapies when he prescribed Ivermectin, an anti-parasitic drug, to treat COVID-19.
He also faced four additional professional charges, brought against him in March of 2024. Of those, three pertained to his work with specific patients, alleging he “failed to maintain the standard of practice of the profession,” while the fourth charge was in relation to billing for his services.
The 2024 charges also made reference to inappropriate prescription of Ivermectin, as well as cannabinoids, benzodiazepines, Vitamin B12, and supplements.
Charges brought by that oversight body are not criminal charges but pertain to conduct that does not comply with the rules that govern its members.
Salte advised, via email, that a hearing was held with regard to Kabongo’s matters in June, and a penalty was imposed on him.
With regard to penalty, the CPSS council decided Kabongo is to receive a written reprimand.
In addition, his licence is to be suspended for one month, starting Aug. 1, 2024.
He is to practice only under the supervision of “a duly qualified medical practitioner approved by the Registrar.”
“The requirement for supervision will continue until the Registrar concludes that Dr. Kabongo is no longer required to practise under supervision,” the council decision states.
The supervisor is to provide the CPSS with reports as to the status of Kabongo’s practice.
Kabongo is also directed to pay costs associated to the investigation and the hearing in the amount of $44,783.72. This amount is to be paid in 24 equal instalments, beginning August 1.
If he fails to pay these costs as required, his licence is to be suspended until he pays in full.
— with files from Pam Cowan
======
Regina doctor suspended for prescribing Ivermectin for COVID
Saskatoon / 650 CKOM
June 18, 2024
A Regina doctor has been suspended from practicing for a month this summer for prescribing Ivermectin for COVID-19.
The Saskatchewan College of Physicians and Surgeons found that over two years, between April 2020 and March 2022, Tshipita Kabongo prescribed the drug as either a treatment or to prevent COVID-19 at his practice in Regina
He was found to have engaged in unprofessional conduct.
In a decision released this month, the college said Kabongo failed to follow the its policy on alternative therapies, which says patients have a right to make decisions about their health care but doctors who choose to use complementary or alternative therapies have to do so in a way that’s informed by medical evidence and science.
“It is unethical to engage in or to aid and abet in treatment which has no acceptable scientific basis, may be dangerous, may deceive the patient by giving false hope, or which may cause the patient to delay in seeking conventional care until his or her condition becomes irreversible,” the policy states.
The college’s decision on Kabongo said one or more of the prescriptions he gave out weren’t medically necessary, he failed to recommend other evidence-informed treatment options, and he didn’t properly document the prescriptions in medical records.
As a result, Kabongo will be suspended from practising for one month in August. He’ll have to have someone supervise him when he returns to practising, and he’ll have to pay the cost of the investigation and hearing, which added up to $44,783.72.
Ivermectin is a drug meant to treat parasites as an oral medicine and rosacea as a topical medication. However, some on social media promoted it as a cure for COVID during the pandemic which began in 2020.
In the fall of 2021, Health Canada and several medical groups in Saskatchewan put out public messages warning people against the use of Ivermectin for COVID, particularly the stronger and more dangerous veterinary formulation.
“There is no evidence that Ivermectin works to prevent or treat COVID-19 and it is not authorized for this use. To date, Health Canada has not received any drug submission or applications for clinical trials for Ivermectin for the prevention or treatment of COVID-19,” explained a public notice from Health Canada issued in October, 2021.
A memo issued around the same time by the College of Physician and Surgeons, along with several other Saskatchewan medical groups, said that while there have been studies on Ivermectin, the study limitations like sample sizes and confounding factors mean that conclusions couldn’t be drawn, and so Ivermectin was disapproved of for the treatment or prevention of COVID-19.
DR. WILLIAM MAKIS MD | JUNE 23, 2024:
This is yet another example of criminal behavior by a College, this time by the College of Physicians and Surgeons of Saskatchewan.
It is time to start filing criminal charges against College Officials.
These Colleges, through their actions, have killed thousands of Canadians already and if Canadians don’t take the Colleges back, the Colleges will continue to take many more lives in the future.
Supreme Court Rules 6-3 That Biden Regime Pressuring Platforms To Censor Speech Doesn’t Violate First Amendment
By Dan Frieth | Reclaim The Net | June 26, 2024
The US Supreme Court has ruled in the hotly-awaited decision for the Murthy v. Missouri case, reinforcing the government’s ability to engage with social media companies concerning the removal of speech about COVID-19 and more. This decision, affirming that these actions do not infringe upon First Amendment rights, delineates the limits of free speech on the internet, dealing a massive blow to freedom of expression online and the interpretation that the First Amendment prevents the government from pressuring platforms to remove legal speech.
The verdict, decided by a 6-3 vote, found that the plaintiffs lacked the standing to sue the Biden administration. The dissenting opinions came from conservative justices Samuel Alito, Clarence Thomas, and Neil Gorsuch.
We obtained a copy of the ruling for you here.
John Vecchione, Senior Litigation Counsel at NCLA, responded to the ruling, telling Reclaim The Net, “The majority of the Supreme Court has declared open season on Americans’ free speech rights on the internet,” referring to the decision as an “ukase” that permits the federal government to influence third-party platforms to silence dissenting voices. Vecchione accused the Court of ignoring evidence and abdicating its responsibility to hold the government accountable for its actions that crush free speech.
Jenin Younes, another Litigation Counsel at NCLA, echoed Vecchione’s sentiments, labeling the decision a “travesty for the First Amendment” and a setback for the pursuit of scientific knowledge. “The Court has green-lighted the government’s unprecedented censorship regime,” Younes commented, reflecting concerns that the ruling might stifle expert voices on crucial public health and policy issues.
Further expressing the gravity of the situation, Dr. Jayanta Bhattacharya, a client of NCLA and a professor at Stanford University, criticized the Biden Administration’s regulatory actions during the COVID-19 pandemic. Dr. Bhattacharya argued that these actions led to “irrational policies” and noted, “Free speech is essential to science, to public health, and to good health.” He called for congressional action and a public movement to restore and protect free speech rights in America.
This ruling comes as a setback to efforts supported by many who argue that the administration, together with federal agencies, is pushing social media platforms to suppress voices by labeling their content as misinformation.
Previously, a judge in Louisiana had criticized the federal agencies for acting like an Orwellian “Ministry of Truth.” However, during the Supreme Court’s oral arguments, it was argued by the government that their requests for social media platforms to address “misinformation” more rigorously did not constitute threats or imply any legal repercussions – despite the looming threat of antitrust action against Big Tech.
Here are the key points and specific quotes from the decision:
Lack of Article III Standing: The Supreme Court held that neither the individual nor the state plaintiffs established the necessary standing to seek an injunction against government defendants. The decision emphasizes the fundamental requirement of a “case or controversy” under Article III, which necessitates that plaintiffs demonstrate an injury that is “concrete, particularized, and actual or imminent; fairly traceable to the challenged action; and redressable by a favorable ruling” (Clapper v. Amnesty Int’l USA, 568 U. S. 398, 409).
Inadequate Traceability and Future Harm: The plaintiffs failed to convincingly link past social media restrictions and government communications with the platforms. The decision critiques the Fifth Circuit’s approach, noting that the evidence did not conclusively show that government actions directly caused the platforms’ moderation decisions. The Court pointed out: “Because standing is not dispensed in gross, plaintiffs must demonstrate standing for each claim they press” against each defendant, “and for each form of relief they seek” (TransUnion LLC v. Ramirez, 594 U. S. 413, 431).The complexity arises because the platforms had “independent incentives to moderate content and often exercised their own judgment.”
Absence of Direct Causation: The Court noted that the platforms began suppressing COVID-19 content before the defendants’ challenged communications began, indicating a lack of direct government coercion: “Complicating the plaintiffs’ effort to demonstrate that each platform acted due to Government coercion, rather than its own judgment, is the fact that the platforms began to suppress the plaintiffs’ COVID–19 content before the defendants’ challenged communications started.”
Redressability and Ongoing Harm: The plaintiffs argued they suffered from ongoing censorship, but the Court found this unpersuasive. The platforms continued their moderation practices even as government communication subsided, suggesting that future government actions were unlikely to alter these practices: “Without evidence of continued pressure from the defendants, the platforms remain free to enforce, or not to enforce, their policies—even those tainted by initial governmental coercion.”
“Right to Listen” Theory Rejected: The Court rejected the plaintiffs’ “right to listen” argument, stating that the First Amendment interest in receiving information does not automatically confer standing to challenge someone else’s censorship: “While the Court has recognized a ‘First Amendment right to receive information and ideas,’ the Court has identified a cognizable injury only where the listener has a concrete, specific connection to the speaker.”
The case revolved around allegations that the federal government, led by figures such as Dr. Vivek Murthy, the US Surgeon General, (though also lots more Biden administration officials) colluded with major technology companies to suppress speech on social media platforms. The plaintiffs argue that this collaboration targeted content labeled as “misinformation,” particularly concerning COVID-19 and political matters, effectively silencing dissenting voices.
The plaintiffs claim that this coordination represents a direct violation of their First Amendment rights. They argue that while private companies can set their own content policies, government pressure that leads to the suppression of lawful speech constitutes unconstitutional censorship by proxy.
The government’s campaign against what it called “misinformation,” particularly during the COVID-19 pandemic – regardless of whether online statements turned out to be true or not – has been extensive.
However, Murthy v. Missouri exposed a darker side to these initiatives—where government officials allegedly overstepped their bounds by coercing tech companies to silence specific narratives.
Communications presented in court, including emails and meeting records, suggest a troubling pattern: government officials not only requested but demanded that tech companies remove or restrict certain content. The tone and content of these communications often implied serious consequences for non-compliance, raising questions about the extent to which these actions were voluntary versus compelled.
Tech companies like Facebook, Twitter, and Google have become the de facto public squares of the modern era, wielding immense power over what information is accessible to the public. Their content moderation policies, while designed to combat harmful content, have also been criticized for their lack of transparency and potential biases.
In this case, plaintiffs argued that these companies, under significant government pressure, went beyond their standard moderation practices. They allegedly engaged in the removal, suppression, and demotion of content that, although controversial, was not illegal. This raises a critical issue: the thin line between moderation and censorship, especially when influenced by government directives.
The Supreme Court ruling holds significant implications for the relationship between government actions and private social media platforms, as well as for the legal frameworks that govern free speech and content moderation.
Here are some of the broader impacts this ruling may have:
Clarification on Government Influence and Private Action: This decision clearly delineates the limits of government involvement in the content moderation practices of private social media platforms. It underscores that mere governmental encouragement or indirect pressure does not transform private content moderation into state action. This ruling could make it more challenging for future plaintiffs to claim that content moderation decisions, influenced indirectly by government suggestions or pressures, are tantamount to governmental censorship.
Stricter Standards for Proving Standing: The Supreme Court’s emphasis on the necessity of concrete and particularized injuries directly traceable to the challenged government action sets a high bar for future litigants. Plaintiffs must now provide clear evidence that directly links government actions to the moderation practices that allegedly infringe on their speech rights. This could lead to fewer successful challenges against perceived government-induced censorship on digital platforms.
Impact on Content Moderation Policies: Social media platforms may feel more secure in enforcing their content moderation policies without fear of being seen as conduits for state action, as long as their decisions can be justified as independent from direct government coercion. This could lead to more assertive actions by platforms in moderating content deemed harmful or misleading, especially in critical areas like public health and election integrity.
Influence on Public Discourse: By affirming the autonomy of social media platforms in content moderation, the ruling potentially influences the nature of public discourse on these platforms. While platforms may continue to engage with government entities on issues like misinformation, they might do so with greater caution and transparency to avoid allegations of government coercion.
Future Legal Challenges and Policy Discussions: The ruling could prompt legislative responses, as policymakers may seek to address perceived gaps between government interests in combating misinformation and the protection of free speech on digital platforms. This may lead to new laws or regulations that more explicitly define the boundaries of acceptable government interaction with private companies in managing online content.
Broader Implications for Digital Rights and Privacy: The decision might also influence how digital rights and privacy are perceived and protected, particularly regarding how data from social media platforms is used or shared with government entities. This could lead to heightened scrutiny and potentially stricter guidelines to protect user data from being used in ways that could impinge on personal freedoms.
Overall, the Murthy v. Missouri ruling will likely serve as a critical reference point in ongoing debates about the government’s ability to influence and shut down speech.
Hey, Jim Jordan: Ask Fauci Who His Bosses Were!
To get to the bottom of Covid censorship, we must understand who was in charge of the global pandemic response.

llustration by Anthony Freda
By Debbie Lerman | June 13, 2024
As recently reported by Reclaim the Net, Anthony Fauci is being called to testify by House Judiciary Committee Chairman Jim Jordan for his “alleged role in the Biden White House’s censorship initiatives.”
Right away a glaring issue emerges: The censorship of dissenting COVID narratives started all the way back in late January-early February 2020, with Fauci implicated in the censorship as early as February 2, 2020. The Committee tacitly acknowledges this by requesting documents dating back to 2019, even as it frames the inquiry politically as a “Biden Administration censorship” problem.
In fact, the entire disastrous, unscientific lockdown-until-vaccine pandemic response was initiated and insidiously perpetrated by the Task Force, which was housed in the Trump White House, in the Office of the Vice President (OVP).
The group responsible for pandemic policy within the Task Force was not HHS or NIAID, where Fauci worked, or any other public health agency. It was the National Security Council (NSC).
All communications about Covid had to go through OVP/NSC.
We know from the Twitter files and subsequent investigations that the Intelligence Community (FBI, CIA, DHS, CISA) was heavily involved in censoring Americans on many issues, starting at least as far back as 2016. Foreign military/intelligence agencies of allied countries collaborated on censoring the U.S. population.
So if anyone is truly interested in who initiated and enforced censorship of dissenting Covid voices, they should ask the following questions of Fauci under oath:
We know from official government documents that Covid pandemic policy was set by the National Security Council (NSC), NOT the public health agencies. But who exactly on the NSC was in charge? Who wrote the policy?
- Dr. Fauci: Did you participate in crafting the pandemic response policy with the National Security Council, including censorship of dissenting views?
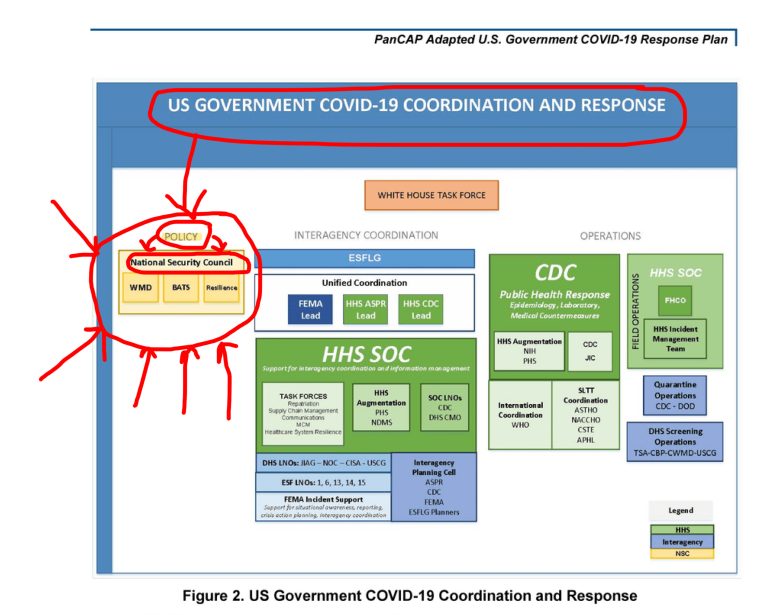
Why were Covid meetings classified?
On March 11, 2020 Reuters reported that “The White House has ordered federal health officials to treat top-level coronavirus meetings as classified.” Reuters sources said “the National Security Council (NSC), which advises the president on security issues, ordered the classification.”
Furthermore, government officials said “dozens of classified discussions about such topics as the scope of infections, quarantines and travel restrictions have been held since mid-January.”
- Dr. Fauci: Why were the Covid response meetings classified? Were you present in those meetings? Were censorship plans discussed in those meetings?
According to the US Government’s COVID-19 Response Plan, starting on February 28, 2020 “all federal communication and messaging” about the pandemic had to go through the Office of the Vice President, which housed the Task Force, which was led by the National Security Council.
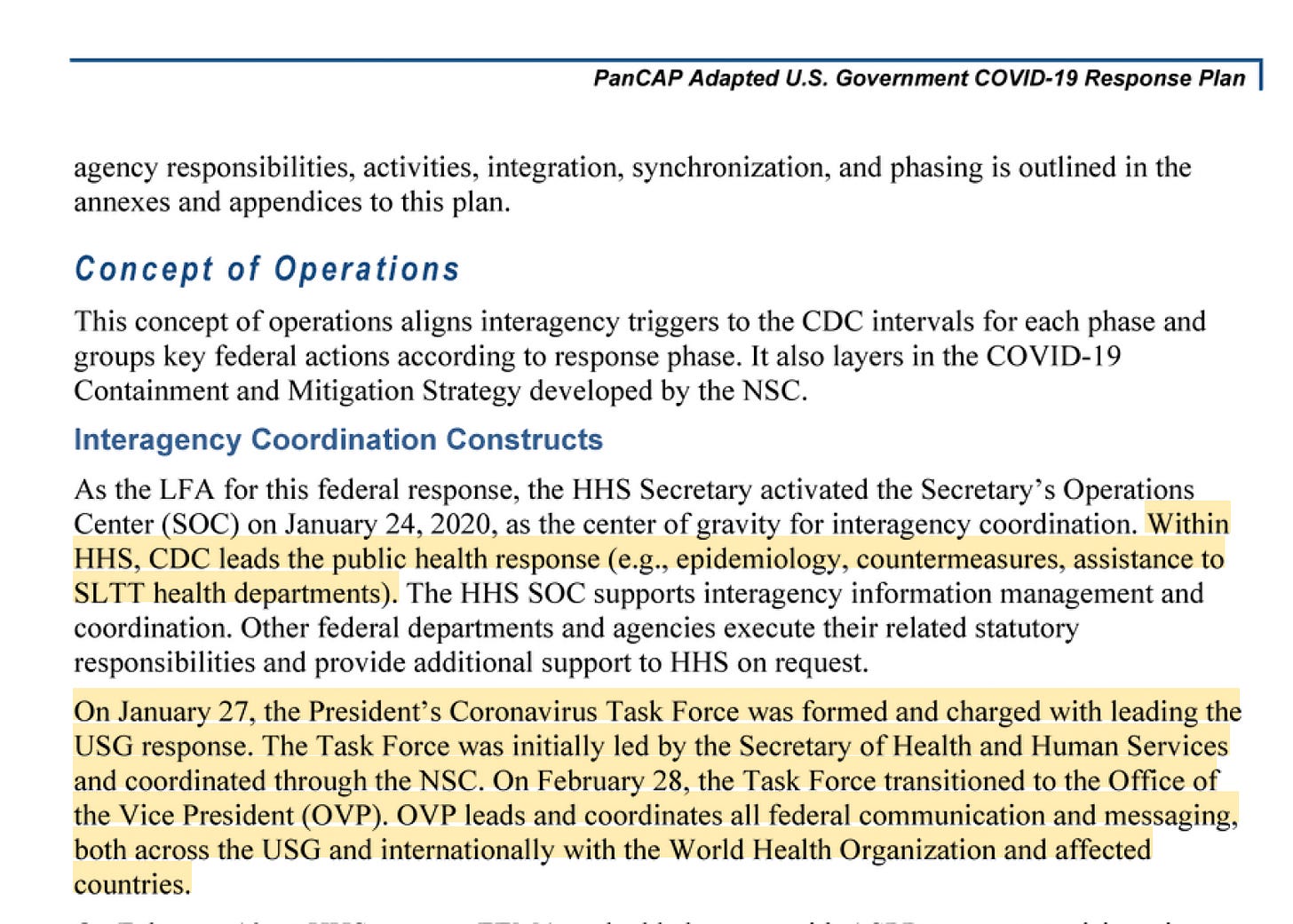
- Dr. Fauci: In your role on the Task force, were you in charge of crafting the communications about the pandemic? If not, who on the Task Force was in charge of messaging?
- Were you in charge of efforts to censor messaging that questioned or contradicted Task Force/NSC policy?
- If not, who was in charge of designing and enforcing the censorship efforts on behalf of the Task Force/NSC?
Why was the CDC forbidden from communicating about the pandemic?
Although it was supposed to play a leadership role in pandemic communications, starting on February 28, 2020 the CDC was actually “not permitted to conduct public briefings,” according to a Senate report.

It sounds like the agency that was supposed to be in charge of communicating with the public about the pandemic was itself being CENSORED by the Task Force/NSC.
- Dr. Fauci, who forbade the CDC from conducting public briefings about the pandemic?
- Why were CDC communications with the public completely shut down?
- Was this part of the overall efforts by the Task Force/NSC to censor any messaging that contradicted their policy?
Why was the intelligence community so heavily involved in Covid censorship?
Many deeply and carefully investigated reports show extensive involvement of military/intelligence agencies and personnel in Covid censorship efforts.
Here are just a few examples:
How Twitter Rigged the Covid Debate, by David Zweig
Pentagon Was Involved in Domestic Censorship Scheme, by Alex Gutentag
The Virality Project Was a Government Front to Coordinate Censorship, by Andrew Lowenthal and Alex Gutentag
- Dr. Fauci, were you coordinating with the FBI, CIA, DHS, CISA or any other intelligence entity to censor messaging that questioned or contradicted Task Force/NSC policy?
- Why were intelligence agencies involved in censoring Covid messaging?
Were international NGOs and the WHO involved in censorship of American citizens?
Here’s one of the earliest known instances of Covid censorship from all the way back in February 2020, in which the following international cast participated:
- Anthony Fauci of the U.S. NIAID and Francis Collins of the U.S. NIH
- Jeremy Farrar, then head of the British Wellcome Trust (the wealthiest nonprofit in the UK that prospered during Covid and gave money to EcoHealth Alliance, among other Covid-related orgs) now Chief Scientist at the WHO
- Tedros Ghebreyesus, head of the World Health Organization (WHO) and Bernhard Schwartlander, the WHO representative in China (about whom little info is available online – and who requires more investigation).
As reported by US Right To Know :
on Sunday, February 2, 2020 at 11:28am
Farrar flagged a ZeroHedge article [now archived] in an email to Fauci and Collins, raising the possibility of virus=bioweapon. In the email, he mentioned that the WHO leaders were in the process of making an important decision. He said they might “prevaricate” which means “avoid telling the truth.”
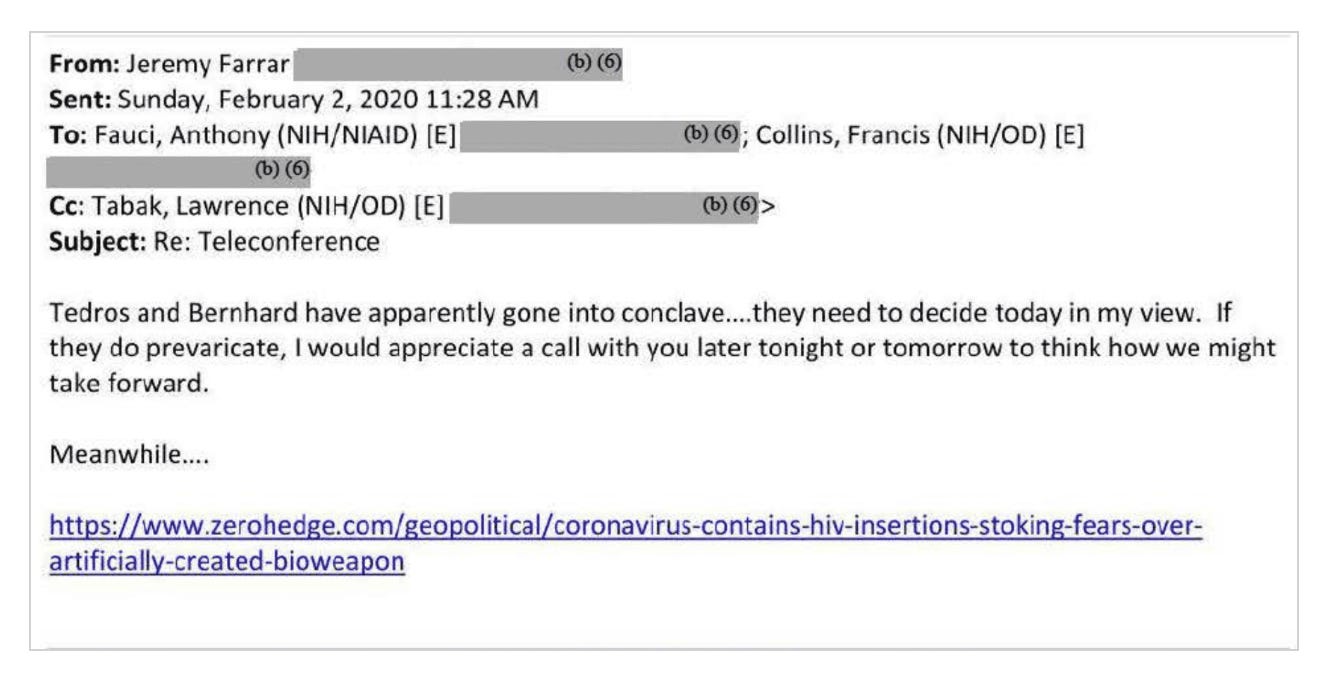
Regardless of whether they prevaricated or not, just two and a half hours later, at approximately 1:57pm ZeroHedge was suspended on Twitter.
- Dr. Fauci, was your correspondence with Farrar, involving the leaders of the World Health Organization, in any way related to the suspension of ZeroHedge on Twitter?
- If so, which of you was responsible for conveying the message to Twitter about the suspension?
- Were international organizations like the WHO, and NGOs including the Wellcome Trust, involved in Covid censorship activities in coordination with U.S. officials/agencies?
- Were you involved in any international Covid censorship activities?
Featured Video
The Iran War has destroyed fertilizer markets and farmers everywhere, almost
or go to
Aletho News Archives – Video-Images
From the Archives
Truth, History and Integrity
By Gilad Atzmon | March 13, 2010
… As devastating as it may be, at a certain moment in time, a horrible chapter was given an exceptionally meta-historical status. Its ‘factuality’ was sealed by draconian laws and its reasoning was secured by social and political settings. The Holocaust became the new Western religion. Unfortunately, it is the most sinister religion known to man. It is a license to kill, to flatten, no nuke, to wipe, to rape, to loot and to ethnically cleanse. … Read full article
Blog Roll
 Aletho News
Aletho News- Iran moved to change the US-Iran equation yesterday
- Former Israeli soldier: I left the Gaza war with shame and regret
- The UK Government Will Persecute Those Vocal about Israel, But Not War Criminals
- Is Hungary about to give Ukraine the EU green light?
- EU pushing Armenia to expel Russian Orthodox Church – intel service
- From Evo Morales to Rodrigo Paz: Bolivia’s Dramatic Shift Toward Israel
- Iran rejects US assassination claim, says Washington trying to whitewash its own crimes against Iranians
- The Iran War has destroyed fertilizer markets and farmers everywhere, almost
- Capitulate or Die: The Gaza ‘peace process’ and Western propaganda
- FSB Blows Lid on Western Plot to Hack Russian Officials’ Phones — But Here’s the Shocker
- If Americans Knew
- The Faustian Bargain of Journalists Embedding with the Israeli Military in Gaza
- AIPAC: Defending the Indefensible
- “You Either Leave Right Now or You Die”—Israel’s Ethnic Cleansing of a Village in Lebanon
- Selling American dead bodies to the US Navy for Israeli military training?
- AIPAC affiliate has funded lavish trips to Israel for dozens of Congress members since 7 October, filings reveal
- Trump called Netanyahu crazy, stopped Israel attack on Beirut: three articles
- ISRAELI MEDIA: Israel’s Education System Isn’t Broken. It’s Doing Exactly What It Was Built to Do
- UN experts alarmed by escalating settler terror and displacement in West Bank
- Israeli soldiers halt Catholic festival preparations in West Bank Christian village
- Congress Is Quietly Making Israel a Permanent Pillar of U.S. Military Modernization
- No Tricks Zone
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
- Germany’s AfD Party Calls Debunked Climate Scenarios “Greatest Fraud In Human History”
- Researchers Find Rapid Global Warming Phase At End Of Last Ice Age (Ca.18,000 Years Ago)
- Even The DNA Of Single-Celled Plankton Can Upend Alarmist Arctic Sea Ice Melt Claims
- Scandal: Although Climate Panic Is Canceled By IPCC, Europe’s Policymakers Continue With Their Crushing Policies
- How Once Hardcore Climate Alarmist Lucy Biggers Realized It Was All A Scam, Brainwashing
