US President-elect Donald Trump will nominate Robert F. Kennedy Jr. to be his Secretary of Health and Human Services (HHS), declaring that the former Democrat will ensure that “everybody will be protected from harmful chemicals [and] pollutants.”
Trump announced his choice in a social media post on Thursday evening. “For too long, Americans have been crushed by the industrial food complex and drug companies who have engaged in deception, misinformation, and disinformation when it comes to public health,” he wrote.
“HHS will play a big role in helping ensure that everybody will be protected from harmful chemicals, pollutants, pesticides, pharmaceutical products, and food additives that have contributed to the overwhelming health crisis in this country,” he continued. “Mr. Kennedy will restore these agencies to the traditions of gold standard scientific research… to Make America Great and Healthy Again!”
The New York Post claimed the previous day that some of Trump’s closest advisers were pushing for Kennedy to be given an advisory position, but that the former Democrat was “stubborn” in demanding control of HHS.
If confirmed, Kennedy would oversee the Centers for Disease Control and Prevention (CDC), Food and Drug Administration (FDA), National Institutes of Health (NIH), and other sub-agencies. Kennedy has been vocally critical of all of these agencies, and vowed to enact sweeping reforms if placed in charge of them.
A long-time vaccine skeptic and proponent of organic agriculture, Kennedy has promised to “get processed food out of school lunch immediately,” to recommend that fluoride be removed from the water supply, and to crack down on the use of chemical pesticides and herbicides in farming.
Kennedy announced last October that he would run for the presidency as an independent candidate, ending his bid to challenge President Joe Biden in the Democratic Party’s primary elections. He suspended his campaign and endorsed Trump in August, citing Trump’s support for free speech, his promise to end the Ukraine conflict, and his willingness to tackle what Kennedy called “the chronic disease epidemic” afflicting American children.
The thimerosal-free HibTITER pediatric vaccine marketed by Wyeth from 2003 through 2007 was associated with 19 different medical conditions, according to a study published Tuesday in the International Journal of Risk & Safety in Medicine.
The conditions include life-threatening side effects at rates “significantly higher” than other Hib vaccines.
The study, by Children’s Health Defense (CHD) researcher Karl Jablonowski, Ph.D., and Brian Hooker, Ph.D., CHD chief scientific officer, compared adverse events among children who received HibTITER to those among children who received other Hib vaccines.
Haemophilus influenzae type b (Hib) is a bacterium that can cause illnesses ranging from ear infections to pneumonia to meningitis. Vaccines for Hib in young children were first licensed in 1987. The Centers for Disease Control and Prevention (CDC) recommends Hib vaccines for infants at age 2 months.
Wyeth, now Pfizer, sold HibTITER from the time it was licensed in 1990 until 2007. In 2003, the company reformulated the vaccine to remove thimerosal, a type of mercury, after public outcry over the dangers of mercury in vaccines.
In 2007, Pfizer “quietly” pulled the reformulated HibTITER vaccine off the market, Hooker told The Defender — a move he said was concerning, in light of the vaccine’s “relationship to many adverse events in children.”
To assess those adverse events, Jablonowski and Hooker analyzed data from 277,484 children between 2003-2007 — when the thimerosal-free HibTiTER was available — using the publicly available Florida Medicaid database.
They corroborated their findings by analyzing data for the vaccine from the Vaccine Adverse Event Reporting System (VAERS), a passive public reporting system jointly administered by the CDC and the U.S. Food and Drug Administration (FDA).
The researchers identified medical conditions for infants vaccinated with any Hib vaccine within 30 days of the shot. The Medicaid data revealed 19 different diagnoses associated with HibTITER at frequencies significantly higher than those associated with other Hib vaccines. They also verified 14 of those diagnoses in VAERS.
The adverse events, ranging from mild to life-threatening, included respiratory, gastrointestinal, dermatologic and generalized infections; ear, nose and throat medical contitions; and other conditions.
None of the serious or even life-threatening conditions identified were listed as possible adverse events on the package insert for HibTITER.
The authors’ findings “have profound medical implications for the estimated 35 million Americans between the ages of 16 and 33 who received the vaccine,” they wrote.
VAERS ‘screaming’ problem with HibTITER for decades
The first Hib conjugate vaccine, which combines a weak antigen with a stronger one to elicit a more robust immune response to the weak antigen, was licensed in 1987 for children 18 months and older, and in 1990 for infants 2 months and older.
Following the approval of the first Hib conjugates, rates of Hib disease in young children dropped dramatically — 92%, from 37 per 100,000 in 1989 to 3 per 100,000 by 2008.
The clinical trial used to declare the vaccine’s safety consisted of investigators calling families 72 hours after vaccination to see how the infants were doing. On that basis, they concluded the vaccine was “safe and effective,” the authors wrote.
“Since VAERS first went live in July of 1990 the data started screaming that something was wrong with HibTITER,” Jablonowski told The Defender. “In VAERS’ first six months of existence, 30% of mortalities reported in children 6 months old or younger were HibTITER recipients.”
HibTITER dominated the Hib vaccine market between 1991 and 1994 when it began to share the market with other FDA-approved vaccines.
The license expired just after the Institute of Medicine’s Immunization Safety Review Committee published its 2001 safety review of thimerosal-containing vaccines and their link to neurodevelopmental disorders.
In that report, the Institute of Medicine found insufficient data to confirm or deny the link, yet the CDC recommended removing thimerosal from vaccines “as soon as possible.”
However, even when Wyeth began selling a reformulated non-thimerosal version of HibTITER in 2003, adverse events continued to occur at high rates.
“In the subsequent years, HibTITER accounted for a disproportionately larger number of emergency room visits, serious reports and reports of death,” Jablonowski said. “The FDA and CDC took no known action, and instead allowed the manufacturer, Wyeth, to choose to end production.”
The researchers estimated that approximately 35 million Americans received the HibTITER vaccine during its time on the market.
In 2011, vaccine maker Nuron Biotech Inc. acquired the HibTITER rights from Wyeth/Pfizer and announced it was preparing to rerelease the vaccine in the U.S. and some Asian markets.
However, the shot was never reintroduced to the U.S. market and the company no longer exists.
‘We were stunned at what the data revealed’
The investigators compared the frequencies of new diseases identified within 30 days of vaccination among 152,269 infants who received the thimerosal-free HibTITER to 125,215 infants who received any other Hib vaccine.
They employed the Fisher’s Exact Test statistical model to compare disease frequency in each cohort and used Bonferroni correction, a powerful statistical tool, to eliminate random results. They also set a high bar for statistical significance.
They identified 19 adverse outcomes with the “most prolific, significant signals” for infectious diseases, such as pulmonary tuberculosis, where 99.03% of diagnoses were among HibTITER recipients.
Other respiratory illnesses occurring within 30 days of HibTITER vaccination included asthma, acute upper respiratory infections, influenza and acute bronchiolitis. Additional diseases included laryngopharyngitis, common cold, colitis, enteritis and gastroenteritis.
Of the 19 adverse effects they identified, the most recent package insert for HibTITER named only two: fever and rash. Infectious diseases accounted for nine of the 19 adverse effects.
Jablonowski explained that the HibTITER doesn’t directly cause infections but can create conditions that facilitate them. The presence of so many infections “implicates significant and rapid immunological defense impairment,” he said.
Jablonowski added:
“While we had heard anecdotally of many adverse reactions to the HibTITER vaccine, we were stunned at what the data revealed.
“This vaccine should have been studied much more intensively before being allowed on the market. In fact, it shouldn’t have ever been allowed to be injected into infants in the absence of rigorous studies to support its safety.”
He said analyzing the adverse outcomes was “simple — high-school level math and basic database/programming skills kind-of-simple. There are literally millions of people in this country who could have performed the data science portion of this study, and none of them apparently work for the FDA or CDC.”
Peer-reviewed studies showing a link between brain cancer and cellphone radiation are piling up — contradicting a recent World Health Organization (WHO)-led study that claimed there’s no evidence of a link.
South Korean researchers — who analyzed 24 studies and published their report on Oct. 10 in Environmental Health — found significantly higher risks for malignant brain tumors, meningioma and glioma on the side of the head where cellphones were held.
They also found heavy, long-term cellphone use was linked to an increased risk of glioma.
The South Korean study brings the number of meta-analyses published since 2016 linking cellphone radiation to an increased risk of brain cancer to seven, wrote Joel Moskowitz, Ph.D., on his website.
Moskowitz — who directs the Center for Family and Community Health at the University of California, Berkeley — has conducted and disseminated research on wireless technology and public health since 2009.
“These seven peer-reviewed meta-analytic studies contradict the conclusion of the recent WHO systematic review,” he said.
“We encourage the WHO to revise its stance, unlikely as this may be. It’s more likely that the WHO and other captured agencies will label non-industry friendly science as misinformation, even if this puts the public further in danger.”
Lennart Hardell, M.D., Ph.D., a leading scientist who found a link between cellphone use and gliomas, agreed. He told The Defender it was “striking” that the South Korean researchers reached a conclusion that directly contradicted the findings by the authors of the WHO study.
“The WHO study authors should be responsible for their fraudulent behavior violating human health and the environment. Their lack of ethical principles in science gives a ‘green card’ to roll out this technology — and the misinformed layman is the victim.”
Brain tumor rates on the rise in Denmark
The South Korean study was published on the heels of new health data from Denmark showing that central nervous system tumors — including brain tumors — are on the rise.
The Danish Cancer Registry on Sept. 30 published a report on the number of new cancer cases in Denmark, Nilsson said. It shows that central nervous system tumors have been increasing among both men and women.
Nilsson compared Danish central nervous system cancer diagnosis rates since 1995. “The data show that tumors of the central nervous system, including brain tumors, are increasing and are among the cancers that have increased most rapidly over the past 10 years, between 2014 and 2023.”
Credit: Swedish Radiation Protection Foundation
The Danish statistics contradict the notion that the rate of brain tumors isn’t on the rise, Nilsson said. “That argument has been used to claim that cellphone use is not linked to an increased risk of brain tumors or cancers in general.”
A 2023 study on brain cancer rates worldwide from 1990-2019 found a significant rise in brain cancer among both men and women in nearly all parts of the world. The study authors noted that this increase was largely seen in Western countries.
In the U.S., overall brain and other nervous system cancer rates haven’t increased, according to the National Cancer Institute. However, there are many reasons tumors may go unreported in the U.S. and other countries, according to Moskowitz.
For instance, Hardell in a 2017 peer-reviewed study found indications of underreporting in the Swedish Cancer Register.
Although the incidence of reported glioma diagnoses in U.S. adults has remained steady, Moskowitz noted in a Sept. 25 webinar, there’s been an increase in glioblastoma — “the most common and most serious malignant brain tumor.”
“We have seen increases in brain tumor incidents among children and young adults,” he added. “Clearly, more research is needed to understand these increases in tumor incidents.”
Ellie Marks told The Defender she and her son founded the California Brain Tumor Association after discovering that her husband’s brain tumor was likely caused by long-term heavy cellphone use.
After the tumor diagnosis in 2008, Marks sent her husband’s medical and phone records to wireless radiation experts, including Hardell. “They got back to me and said, ‘Yes, he is the poster boy for the cellphone brain tumor correlation,’” she recalled.
Her husband survived, but it’s not easy living with a brain tumor — and her husband is far from alone, she said. “I know many others who have experienced brain cancer attributed to their cellphone use.”
FDA turned blind eye to research linking wireless radiation and cancer
The uptick in brain cancer cases isn’t surprising, Eckenfels-Garcia said, and U.S. health agencies saw it coming.
The U.S. Food and Drug Administration (FDA) claims there’s not enough scientific evidence to link cellphone use to health problems, including brain cancer — but it rejected the findings of a $30 million study it commissioned on the topic.
At the FDA’s request, the National Toxicology Program (NTP) did a multi-year study, concluding there was “clear evidence” that male rats exposed to high levels of wireless radiation like that used in 2G and 3G cellphones developed cancerous heart tumors, and “some evidence” of tumors in the brain and adrenal gland of exposed male rats.
When the NTP in 2018 released its findings, the FDA rejected the study and in February 2020, released an unsigned literature review that criticized the study.
Commenting on the increased incidence of brain tumors, Eckenfels-Garcia said, “So essentially this is an ‘I told you so’ moment. This is exactly what happens when our captured government agencies ignore science, as the FDA did with the NTP study.”
Moskowitz said the FDA should have followed up on the NTP study by conducting a formal risk assessment of wireless radiation, but that never happened. Instead, the U.S. government shut down NTP’s follow-up work on its 2018 study.
In April, CHD filed a Freedom of Information Act request with the National Institutes of Health (NIH) for documents and communications related to why the U.S. government stopped the work. The NIH has not responded to the request.
HART recently posted an article titled “The Witch Hunt continues”, which discussed self-censorship of doctors, General Medical Council (GMC) overreach, and how medical professionals are being erased from the medical register, despite no wrongdoing. Yet this is not a new phenomenon. If we delve into the history of how our existing ‘medical monopoly’ was established, with its roots firmly in America, it is an all too familiar disturbing playbook of censorship, corruption and subversion of ethics that spans over 130 years in the making. The existing medical monopoly was contrived by the Rockefeller family and their many contacts, which has been so successful in its takeover of medicine in America. Herein, I discuss an excellent book by Eustace Mullins titled “Murder by Injection: The Story of the Medical Conspiracy Against America”. Despite the book’s off putting title, Eustace’s careful research spanning over 30 years provides a detailed and shocking account of how billionaire tycoons have waged tyranny, economic depressions, wars and revolutions as part of a wider plan to usher in a medical care system to enslave the public through an entirely controlled medical monopoly. The whole book is free to download here.
Until the late 19th century, doctors were freelance practitioners who assumed all the risks associated with their medical decision-making. In 1832, the British Medical Association was chartered and provided the impetus for a similar organisation to be established in the United States (US), namely the American Medical Association (AMA), which was founded in 1847 with its headquarters in Chicago. From its inception, the AMA had one objective: to create a total medical monopoly of the practice of medicine, and ensure allopathy was the basis of its practice. Allopathic medicine required practitioners to receive training in a recognised academic school of medicine, which relied heavily on surgical procedures as well as medicines. Allopathy was to rival homoeopathy, which promoted non-toxic doses of natural remedies; in the mid-1800s, homoeopaths outnumbered allopaths two to one in the US – a statistic that had to be overturned when the AMA was created.
The reason this book is so pertinent in our troublesome times is that it catalogues the long, but very calculated and carefully planned demise of healthcare in America. It chronicles how the introduction of a monopoly through any means possible – including, racketeering, abuse, censorship and murder – enabled the takeover of health by federal agencies and governments, which were inextricably linked to industry and big pharma. How was such a monopoly to be achieved? It had to be orchestrated by the richest man in the world at that time, the monopolist John D. Rockefeller, who had triumphed in organising his oil monopoly. Backed by Rothschild and Wall Street colleagues, it was hoped the medical monopoly would provide even greater profits than oil, which has more than proved to be the case. Rockefeller appointed Frederick T. Gates (related to Mr Microsoft Bill Gates) as his ‘philanthropic’ agent, whose task was to dominate the entire medical education system.
In 1907, the AMA requested the Carnegie Foundation to conduct a survey of all medical schools in the US; the Foundation appointed Abraham Flexner to lead the study of medical schools. Coincidentally, Abraham Flexner’s brother, Simon, was head of the Rockefeller Institute of Medical Research, so this was an intentional cosy and conflicted setup from the outset. Flexner, a graduate of Johns Hopkins University, which was founded by Daniel Colt Gilman, completed his report in 1910. The report and AMA decided there were too many doctors and the solution was to create a medical educational system so elitist that most students would be prohibited from considering such a career. The undergraduate training was constructed so that allopathic medicine was central to its teaching, and by 1920 the number of medical schools had declined from 650 to 50 in number.
The book goes on to describe how ‘quackery’ was established, with three key players, Morris Fishbein, George Simmons and Albert Lasker, who all began their careers as journalists. Not one of them had any credentials of practising medicine, but their collective journalist and organisational talents propelled them to the heights of power, as full-time ‘quacks’. They utilised their connections with the corrupt AMA to stifle dissent and opposition. For instance, the AMA would grant pharmaceutical companies a ‘Seal of Approval’ for their products but only if they advertised in AMA-affiliated journals. Those that opposed this, such as Wallace Abbott, founder of Abbott Laboratories, soon found out the hard way that no products would be approved, and his reputation would suffer unless he ‘cooperated’. Simmons’ practices were particularly egregious, with one critic positing: “almost every branch of the Federal Government active in the field of medicine was completely dominated by the AMA”.
Ultimately, the monopolists forced government agencies to act against anyone who posed a threat to their monopoly, including arrests and prison sentences. Simmons and Fishbein collectively controlled the AMA for over half a century, through raising money and using political clout. Fishbein had total control over all publications of the AMA and selection of personnel in various committees. Moreover the AMA was instrumental in concealing beneficial (but non-lucrative) therapies, with products of high value being rejected or their acceptance enduring unwarranted delays. The extent of the corruption detailed in this history of American medicine is remarkable. Federal agents were solicited by charitable foundations to instigate police actions to hundreds of unsuspecting health practitioners throughout the US, in a ruthless operation to arrest and imprison people distributing leaflets about natural or herbal formulas, despite no evidence anyone had been injured or killed by these remedies. Terror raids against competitors were carried out, with heavily armed federal agents breaking doors and seizing any herbal stocks from people’s homes. The book describes terrorisation of anyone active in the alternative healthcare field. Thus, the AMA became an autocracy. Physicians were trained under the Rockefeller-based medical system, which had full control over the medical examination boards. So successful was this endeavour that Americans are now treated with expensive, overpriced, ineffective and potentially dangerous drugs, a corruption that has been routinely covered up by federal agencies.
In 1940, a bill for health insurance was introduced; although it initially suffered setbacks, the seed was sown to create an industry whereby the AMA would fight ‘socialised medicine’, which was the forerunner for Medicare and Medicaid. In the 1960s, the next target for annihilation was the chiropractic sector. No level of intimidation of censorship was spared and many high-profile speakers were forced to cancel lectures and lobby groups were set up to sanction and apply pressure on the Council on Chiropractic Education to the extent that the AMA Joint Committee on Accreditation of Hospitals barred chiropractors and refused accreditation of hospitals that had such practitioners. The AMA also forced the Veterans Administration to refuse payments to veterans for chiropractic services.
With their eyes set on further control, the medical monopolists realised that cancer was a lucrative endeavour and so established the next phase of the monopoly. In 1913, the same year President Woodrow Wilson signed the Federal Reserve Act, a group of doctors met at the Harvard Club in New York to establish a national cancer organisation, the American Society for the Control of Cancer (later renamed the American Cancer Society, ACS). The Rockefellers (with Rothschild and J. P. Morgan backing) funded the ACS. Similarly, funding for the Memorial Hospital (later to become the Memorial Sloan Kettering Cancer Center) was also linked with the National Radium Institute, which stipulated that further funds be permitted, only assuming all cancers were treated with radium. By 1922, more than 100 radiologists had died from X-ray induced cancer. Alfred Sloan, the President of General Motors and Charles Kettering, an inventive genius of electrical systems and auto ignition were deployed. Mullins chronicles in detail how huge industry directors and partners were all interlinked with each other, such as Squibb, Bristol Myers, Johnson & Johnson, Bell Telephone Laboratories, Lehman Brothers, Chase Manhattan Bank and National Geographic. Collaborations with ‘elected’ presidents, industry players, defence industries, CIA, chemical and drug firms go hand-in-hand.
Two key names in patent medicine and journalism were Albert Lasker and Elmer Bobst. One of Lasker’s greatest achievements was his national campaign to persuade women to smoke in public. Lasker became ill with cancer and died in 1952, but before his death, he set up the Albert and Mary Lasker Foundation, which made Mary (Albert’s daughter) the most powerful woman in American Medicine. It is also no coincidence that 18 members of the ACS Board of Directors were executive officers of banks. Pat McGrady, who served as editor of the ACS for 25 years stated “Medicine has become venal, second only to the law”. Since “the fight against cancer” is totally controlled by the Rockefeller medical monopoly, much of cancer research is bogus and filled with falsified results, albeit by well intentioned and unsuspecting researchers. Since Elmer Bobst played a crucial role in making it possible for Nixon to become President, it was not difficult to persuade him to authorise a new and expensive “war on cancer” in 1971.
The book explains how the ACS, AMA and FDA collaboratively staged a war of censorship and intimidation, preventing discussion of effective compounds, such as laetrile, for treating cancer. The ACS, for example, opposed the regulation of potential carcinogens, such as TRIS (trisaminomethane) and DES (diethylstilbestrol). Chemotherapy was promoted as a cancer treatment in the 1960s, despite evidence that it had many serious side effects and was shown to be highly toxic and carcinogenic in animal models, as well as immunosuppressive. Cancer is as much a disease of poor nutrition and one in which the multiplication of ‘simpler’ cells are unable to differentiate because the energy balance of the body is disrupted causing the disease. One of the Director’s of the National Cancer Institute is Mary Lasker, who has close ties with the Pharmaceutical Manufacturers Association, which is not a coincidence.
Mullins goes on to describe several instances of researchers who had discovered cancer cures either by detoxification or a diet low in salt, protein and fats, but the work was buried or destroyed to ensure the chemotherapy, radiation and surgical approaches to cancer were unchallenged. The Laskers built much of their fortune on the promotion of cigarette smoking. Although cigarette smoking is harmful and causes cancer, studies (cited in the book) have shown that there was no link between traditional air-dried tobacco and lung cancer. The tobacco industries, dominated by the Rothschilds, add chemicals and sugar to tobacco, which creates a carcinogenic substance in the nicotine tar. Air-dried tobacco lacks this carcinogen, as noted by the many primitive tribes who have smoked tobacco for thousands of years without any ill effects. Mullins explains that the ACS has vested interests in established forms of cancer treatment, for example owning 50% of the patent rights for the chemotherapy drug 5-fluorouracil. Dr Hardin James addressed the ACS in 1969, noting that “for a typical type of cancer, people who refuse treatment live an average of 12.5 years. Those who accepted surgery and other kinds of treatment, lived an average of 3 years. I attribute this to the traumatic effect of surgery on the body’s natural defence mechanisms.”
In the ‘holy church’ of allopathic medicine, there are what might be termed the four ‘holy waters’, which include immunisation, fluorination of water, use of fertilisers and contamination of the food chain. The practice of immunisation is the most pernicious in terms of its long-term effects. This practice goes directly against the discovery of modern holistic medical experts that the body has a natural immune defence against illness. The greatest heresy any clinician can commit is to publicly voice any doubt about any one of the four ‘holy waters’. The most deeply entrenched in the fabric of modern medical practice, as is glaringly apparent, is the vaccination programmes, as well as being one of the most profitable aspects of the medical monopoly. One physician, Dr Henry R. Bybee of Norfolk, Virginia, stated “My honest opinion is that vaccines are the cause of more disease and suffering than anything I could name.” Additionally, Dr Herbert Snow, a senior surgeon at a cancer hospital in London voiced similar concerns “In recent years, many men and women in the prime of life have dropped dead suddenly. I am convinced that some 80% of these deaths are caused by the inoculation or vaccination they have undergone.” The chilling accounts continue with another practitioner Dr W. B. Clarke of Indiana remarking “cancer was practically unknown until compulsory vaccination when the cowpox vaccine began to be introduced. I have had to deal with at least 200 cases of cancer, and I never saw a case of cancer in an unvaccinated person”. Is this not at least an observation worth exploring? It is unlikely modern medicine advocates will examine this alarming connection. Eventually, the outraged public will bring pressure to abandon the modern ritual of vaccinating children.
Another well-known practitioner from San Francisco, Dr J. M. Pebbles, revealed “The vaccination practice…has not only become the chief menace and the greatest danger to the health of the rising generation, but an outrage upon the personal liberties of the American citizen.” The book tells of how Wyeth laboratories was charged with $15 million in damages to an 8-year-old girl who suffered permanent brain damage after receiving a diphtheria-pertussis-tetanus vaccine. In the US, vaccines are actively and incessantly promoted as the solution for all infectious diseases. It is not a coincidence that agencies, such as the AMA, WHO, FDA, are in favour of the vaccine programmes given the revolving door that exists between Big Pharma and these agencies. It is well known that Edward Jenner ‘discovered’ the cowpox vaccine to purportedly prevent smallpox. However, smallpox was already declining before the introduction of the vaccine and many believe it would have disappeared by the end of the 19th century. After the cowpox vaccine became widespread in England, a smallpox epidemic ensued killing over 22,000 people. By 1872, 44,480 were killed, and the vaccine was finally banned in 1948. This trend is mirrored elsewhere: Japan introduced compulsory vaccination in 1872 and by 1892 there were 165,774 cases of smallpox resulting in nearly 30,000 deaths. Other European countries that submitted to compulsory vaccination saw similar high numbers of cases and deaths, whereas countries (such as Norway) who did not vaccinate had a fraction of the cases. Historians are reluctantly concluding that the 1918 ‘great flu epidemic’ was attributable to the widespread use of vaccines, as survivors were those who had refused the vaccines.
The book chronicles how dissenters and researchers who spoke out lost their jobs, had their laboratory notes seized and burned, and laboratory animals destroyed. In the 1970s, the swine flu vaccination campaign was ushered in, but insurance companies refused to cover against lawsuits as there were inadequate studies. This prompted a propaganda campaign by the monopolists to trick Americans into saving themselves by taking the vaccines, which resulted in billions in damage claims. The next iteration by Dr Jonas Salk in the 1950s was the polio vaccine, which Simon Flexner helped to recommend. It is disturbing that a national conference in Washington in 1988 declared that “all the cases of polio in America come from the vaccine. The naturally occurring (or wild type) polio virus has not been shown to cause a single case of polio in the US since 1979”. Even back in 1955, the Surgeon General of the US highlighted in the AMA conference that “no batch of vaccine can be proven safe before it is given to children”. Moreover, James R. Shannon of the NIH declared “the only safe vaccine is a vaccine that is never used.”
Importantly, the death by injection playbook is not new; rather, a well-orchestrated agenda has been implemented with calculated precision in multiple cycles to gradually harm and decimate populations across the globe. This book further discusses how fluorination of water has been another Rockefeller-deployed monopoly to poison millions of Americans by adding the poisonous chemical sodium fluoride to drinking water. Large quantities of fluorides are waste contaminants and byproducts from large agricultural firms, pesticides and chemical firms, such as Hooker Chemical. Predictably, Hooker Chemical became part of the Rockefeller unit when one of the Hooker family married into the Rockefeller family. Fluorides can cause serious chromosomal damage and animal model studies have shown it promotes cancer development, even at the one part per million threshold in drinking water that has detrimental consequences especially when consumed cumulatively over time. Soviet studies have further shown that fluorides were useful in inducing docile obedience in the general population. Combined with aluminium that was included in many foods, cooking pots and packaging, this has aided in slowly poisoning the mass population and of course produced Alzhiemer’s disease, in what constitutes a build up of toxic levels of aluminium, leading to cognitive and nervous system decline.
Not content with disrupting the medical and water supplies, the Rockefeller-based medical monopoly had its eye on the ‘green revolution’ and agricultural control through the contamination of crops using a ‘co-opted’ carefully constructed money laundering system. This time they developed ‘super crops’ or grains that would serve as an excellent cash cow for the US to sell to ‘developing’ nations. To achieve this goal required the soil to be pumped with huge quantities of fertiliser (the product of nitrates and petroleum), commodities controlled by the Rockefellers that helped to build an entire chemical empire. At the end of the second World War, a concerted effort was made by the monopolists to dump surplus nitrates into the American food chain. Farmers were instructed to increase their use of fertilisers, herbicides and pesticides and create a capital intensive payback scheme for the monopolists. The final sections of the book discuss how fertilisers have been used to reduce nutrients in the soil and how the food chain has been slowly contaminated. Chapter 9 lists and discusses the 18 largest drug firms and their close associations with major banking cartels and federal agencies, such as the CIA.
Collectively, these insidious links with Big Pharma and the medical monopoly, are not only a massive cash cow, but have maimed and decimated the population and continue to do so. Since the rest of the world is intimately tethered to the well-oiled Rockefeller US medical monopoly machine, it is not hard to see how the censorship, corruption and silencing of dissenters has become all too commonplace today.
As a requirement for discussing and appreciating the imperative of health freedom in the USA, we must first define what is meant by health freedom. A simple definition is: the right of every American to decide what medical interventions to put into or onto one’s body, the right to access and use the medical and healing modalities of one’s choice, the right to maintain one’s health according to one’s conscience, and the right to live free of involuntary medication be it via the food supply, the water supply, or something airborne.
In a free and moral society, health freedom is not simply a convenience, it’s an imperative. In this vein, in the event of injury or illness, all Americans must possess the absolute right to choose what medical interventions and treatments to accept and what medical or healing modalities to utilize in order to address illness or injury; Americans must be free to choose how to maintain their health whether that be through nutrition, supplements, herbs, drugs, or a myriad of healing modalities; Americans must have access to truthful information regarding how the seeds for plants and animal feed and the food in our food supply has been grown or developed, medicated, processed, and packaged; and Americans have the right to exist in a society free of water and airborne medications, insect vectors, and chemicals.
Health freedom can only exist in a free and moral society which values each and every member of that society. This prerequisite thus excludes medical mandates of any kind. It is immoral to force another individual to risk their life for the theoretical benefit of another. Moreover, government does not have the moral authority or power to dictate what medical products any American puts into or on his or her body. If anyone in government does possess that power, then no American is truly free, nor does he or she possess any meaningful right whatsoever – Americans are merely chattel.
In order to create a society based on true health freedom, the following policy shifts should be implemented, as a first step. There are many more changes which should be implemented as well, but these proposals would address some of the most glaring, pernicious anti-liberty and anti-health aspects of our system as it exists today:
1. Ban all Medical Mandates:
The Declaration of Independence states, “that all men are created equal, that they are endowed by their Creator with certain unalienable Rights, that among these are Life, Liberty and the pursuit of Happiness…” Medical mandates are prime facie violations of our founding documents.
Health freedom demands prior voluntary informed consent before a medical treatment or intervention is administered. Medical mandates are thus, by definition, antithetical to voluntary consent and therefore must be prohibited in a free and moral society. No single individual in government knows the medical history of any American, knows what is best for Americans, or has to live with the repercussions of any choices made by Americans, thus, medical mandates are never justified in any circumstance.
“The Bayh-Dole Act, formerly known as the Patent and Trademark Act Amendments, is a federal law enacted in 1980 that enables universities, nonprofit research institutions and small businesses to own, patent and commercialize inventions developed under federally funded research programs within their organizations.”
Under this program, government scientists may receive up to $150,000 per year on their patents.
In theory, Bayh-Dole incentivizes bright scientists to seek employment at federal health agencies rather than entering more lucrative private industry by allowing these taxpayer-funded scientists and other individuals and entities to retain the patent rights to intellectual property developed during their taxpayer-funded research and development activities.
In practice, this Act forever realigned the interests of taxpayer-funded scientists away from the American people and toward their own interests and profits and the profits of the private industries with which they collaborate. Dr. Anthony Fauci and his team at NIAID infamously owned half the Moderna Covid vaccine patent which incentivized the misguided covid era policies leading to a colossal violation of the rights of Americans demonstrating the perverse incentives created by Bayh-Dole and the necessity of repealing the act.
3. Repeal the Prescription Drug User Fee Act (PDUFA) of 1992:
“The Prescription Drug User Fee Act (PDUFA) was created by Congress in 1992 and authorizes FDA to collect user fees from persons that submit certain human drug applications for review or that are named in approved applications as the sponsor of certain prescription drug products. Since the passage of PDUFA, user fees have played an important role in expediting the drug review and approval process.”
In 2022 alone, the pharmaceutical industry paid $2.9 billion in user fees amounting to 46% of FDA’s entire budget including $1.4 billion or 66% for FDA’s drug approvers’ salaries and $197 million or 43% of the biologics (vaccines) program budget. As a direct consequence of PDUFA, the FDA has a vested interest aligned with the profits and success of the pharmaceutical industry rather than the health and wellbeing of the American people.
4. Repeal the Public Readiness and Preparedness Act (PREP Act) which authorizes the Secretary of the Department of Health and Human Services to issue a PREP Act declaration.
“The declaration provides immunity from liability (except for willful misconduct) for claims:
of loss caused, arising out of, relating to, or resulting from administration or use of countermeasures to diseases, threats and conditions
determined by the Secretary to constitute a present, or credible risk of a future public health emergency
to entities and individuals involved in the development, manufacture, testing, distribution, administration, and use of such countermeasures
A PREP Act declaration is specifically for the purpose of providing immunity from liability, and is different from, and not dependent on, other emergency declarations.”
The PREP Act desecrates the ethical principle of informed consent by protecting individuals from liability even when they expressly act contrary to patients’ wishes and instructions and must be repealed.
The Affordable Care Act anchors Americans to the pharmaceutical and drug-based medical paradigm even though a majority of Americans used at least one form of “alternative” medicine in 2021 and spent $30.6 billion in out of pocket expenses for those holistic medicine services in 2023 according to Statista. Instead, implement a health savings program which permits Americans to access the health and medical modalities of their choice which in turn would foster more competition and reduce the exorbitant health care costs in the US by breaking the extant monopolies held by the medical and insurance industries.
6. Repeal the National Childhood Vaccine Injury Act (NCVIA):
NCVIA shields vaccine makers and those who administer vaccines from liability (except for willful misconduct), creating a perverse incentive to industry to develop a never-ending stream of vaccines which are then mandated by the states and a perverse incentive to medical professionals to charge for and inject patients irrespective of the harm they may cause. Further, the NCVIA protects industry, medical professionals, and vaccine programs by creating a separate administrative federal court structure lacking due process and discovery, managed by “Special Masters” instead of judges, all in violation of the constitutionally protected right to due process. While NCVIA contains other provisions designed to protect American families and ensure the safety of the national vaccine supply, Congress is not conducting proper oversight and the promises made in 1986 at the time of the Act’s passage have not been upheld. As such, Americans who have been injured or killed by vaccines are left with astronomical medical bills and to fend for themselves.
7. Prohibit Private Donations to Government Entities:
Prohibit private individuals, foundations, corporations, contractors, any other person or entity from donating or otherwise giving money to any agency or entity of the federal government. FDA and the Centers for Disease Control and Prevention (CDC) accept money from private actors such as the Bill and Melinda Gates Foundation and Pfizer thus skewing the interests of the agency in favor of these private actors and away from the American public. Gates has collaborated with FDA and the CDC Foundation takes money from the pharmaceutical industry whose products CDC is responsible for monitoring for safety.
8. Cooling-off Period for Senior Federal Employees:
Enact a 5-year cooling-off period before which agency leadership, deputies, and other key officials may depart federal agencies in order to enter the companies they regulate in the private sector.
9. Prevent Conflicts of Interest:
Eliminate conflict of interest waivers so that no person serving on a health agency committee, board, or other regulatory entity may have a conflict of interest. Disclosure of conflicts of interest is insufficient to ensure the agencies pursue the interests of the American people. Individuals with financial or ideological conflicts of interest should not serve as decision makers in any capacity.
10. Prohibit Government Grants to Nonprofits:
Prohibit government from allocating taxpayer dollars to nonprofit. Nonprofits exists to serve the public interests and should be funded directly by American citizens. If a nonprofit has a worthwhile mission, the public will gladly support it. Government exists to protect our rights and should not be in the business of picking winners and losers nor should it be using third parties to pursue policies outside the reach and review of the public.
11. Ban Water Fluoridation:
While water fluoridation programs are broad spread, they are not only dangerous from a health standpoint, they are forced medication in violation of the ethical principle of informed consent. Research comparing the health outcomes and IQs of communities that do and do not fluoridate their water supply reveal that children in the fluoridated water communities have reduced IQs and therefore inferior prospects in life. Other research has documented the health hazards of fluoride, an industrial waste product.
In addition, as fluoride is added to municipal water supplies, residents of those communities have no way to opt out and therefore are subjected to involuntary forced medication. No one should be forced to consume drugged water in order to maintain a biological necessity.
12. Ban Release of Genetically Modified Insects
Two tenets of good health are abundant exposure to sunshine and fresh air, however in some states, the state governments have collaborated with private business to release genetically modified mosquitoes into communities. While these mosquitoes are often designed to breed with one another and eliminate the “dangerous” species going forward, the health impacts of humans being bitten by these insects is not well understood. Nor should a person have to be risk being bitten by one of these creatures in order to venture outside. This amounts to a form of forced medication absent any form of consent and must be ended.
These recommendations should be understood as necessary first steps to begin correcting the disastrous health policy environment that exists in the United States today and to restore true health freedom in the US which would allow all Americans to decide what medical interventions to allow into or onto one’s body, which health and medical modalities to utilize in maintaining their health, and the ability to live free of involuntary medication be it via the food supply, the water supply, or the air we breathe.
A vaccine approved in August by the U.S. Food and Drug Administration (FDA) for people deemed to be at “high risk” for mpox infection may cause more harm than good, according to the FDA’s own medication guide for the product.
ACAM2000 — made by Emergent BioSolutions, a company specializing in vaccines for biochemical warfare threats such as anthrax and smallpox — was approved for smallpox in 2007.
However, on Aug. 29, the FDA issued an expanded supplement approval for ACAM2000’s use against mpox.
Since then, social media users have been posting clips of the FDA’s ACAM2000 medication guide, which warns the vaccine may cause “serious complications” in both the vaccinated person and those with whom they come into close contact up to 6 weeks after getting the shot.
“You can call ACAM2000 a ‘vaccine,’ but its impact on the United States will be as a ‘disease,’” Jablonowski said.
He added:
“For instance, the drug’s package insert reveals (see Table 3) that the U.S. Department of Health and Human Services (HHS) found roughly 520 per million ACAM2000 recipients contracted myocarditis or pericarditis.
“That is about 1 in 2,000. But elsewhere in the package insert, the FDA acknowledges that — based on additional studies — the risk is actually 5.7 per 1,000 vaccinations.
“That’s about 1 in every 175 people. If the 262 million adults in the U.S. received this vaccine, an estimated 1,493,000 would contract the serious adverse reaction of myopericarditis.”
Dr. Meryl Nass, an internist and biological warfare expert, told The Defender that the CDC also acknowledged this same figure — myopericarditis in 5.7 per 1,000 primary ACAM2000 vaccinations — during a June 23, 2022, meeting.
“It’s a huge number,” Nass said. “The fact that the FDA and CDC are acknowledging it means no one should get the vaccine.”
She explained:
“Myopericarditis is a life-threatening condition. It lowers your life expectancy.
“Most people are never going to be exposed to mpox or smallpox. Vaccines are typically given to healthy people who are never even going to be exposed, therefore the risk posed by the vaccine needs to be low.
“That’s why vaccine safety is critical — even more than drugs, because drugs are given to people who are already sick.
“This risk — 1 in 175 — is higher than all other licensed vaccines for which the CDC acknowledges side effects. This is the worst.”
ACAM2000 can also cause fetal death when taken during pregnancy, the package insert states.
Additionally, the shot contains a “live vaccinia virus” that can be spread to — and possibly cause the death of — people who have close contact with the vaccinated person up to 6 weeks following vaccination, according to the medication guide.
The guide — which the FDA requires to be given to patients before they get the ACAM2000 vaccine — says, “ACAM2000 can cause serious complications in vaccinated individuals and in their close contacts to whom the vaccine virus has spread.”
Jablonowski said, “The spread of vaccinia virus is an infliction and an assault, as an unsuspecting person cannot possibly consent.”
“For good reasons you would not consent to this vaccine,” Jablonowski said, “even if you believed your benefits outweigh your risks, as you become a potential vector of a disease that is damaging to the heart and fatal to both fetus and infant.”
Risk of serious complications and death in vaccinated and those exposed to vaccinated individual
ACAM2000 is a single-dose vaccine administered using a bifurcated needle that’s been dipped into the vaccine solution, according to an Emergent BioSolutions press release.
In its Aug. 30 press release, the FDA stressed that “every person” who receives ACAM2000 is “required” to be given the drug’s FDA-approved medication guide.
“A Medication Guide is necessary,” the FDA said, “for safe and effective use of the vaccine because it could help prevent serious adverse events and inform the vaccine recipient of serious risks relative to benefit that could affect their decisions to be vaccinated.”
The guide lists serious possible complications, including: myocarditis, inflammation of the brain or spinal cord, serious skin infections, spreading the vaccine virus through the blood to other parts of the body and fetal death if taken during pregnancy.
According to the guide, “The risks for serious vaccine side effects are greater for people who:
have heart problems or a history of heart problems
are taking steroid eye drops or ointment
have a weakened immune system
have skin problems such as eczema, atopic dermatitis, burns, impetigo, contact dermatitis, chickenpox, shingles, psoriasis, or uncontrolled acne
are less than 1 year old
are pregnant or become pregnant within 6 weeks after vaccination.”
“Myocarditis and/or pericarditis, encephalitis, encephalomyelitis, encephalopathy, progressive vaccinia (vaccinia necrosum), generalized vaccinia, severe vaccinial skin infections, erythema multiforme major (including Stevens-Johnson syndrome), eczema vaccinatum, accidental eye infection (ocular vaccinia) which can cause ocular complications including keratitis and corneal scarring that may lead to blindness, and fetal death in pregnant women.”
The insert also goes into more detail about the risk of death:
“Historically, death following vaccination with live vaccinia virus is a rare event; approximately 1 death per million primary vaccinations and 1 death per 4 million revaccinations have occurred after vaccination with live vaccinia virus.
“Death has also been reported in unvaccinated contacts accidentally infected by individuals who have been vaccinated.”
U.S. stockpile contains more than 100 million doses
The FDA’s approval of ACAM2000 for use against mox followed just days after Emergent BioSolutions pledged to donate 50,000 doses to address the mpox outbreak in Africa.
On July 2, the U.S. Administration for Strategic Preparedness and Response at the HHS signed a $99.9 million deal with the drugmaker to obtain more ACAM2000 doses this year. Although the exact number of doses was not disclosed, Forbeson Sept. 8 reported that the U.S. currently has over 100 million doses.
HHS did not respond when The Defender asked if these doses are reserved for an emergency smallpox outbreak or are being made available as an mpox vaccine.
The Defender reached out to the Centers for Disease Prevention and Control (CDC) with the same question but was told by a CDC spokesperson, “We defer to the Administration for Strategic Preparedness and Response (ASPR) where the National Stockpile is housed.”
The CDC website on mpox vaccination states that ACAM2000 “has not been used in the ongoing clade II mpox outbreak that started in 2022″ but “has been made available for use against mpox in the clade II outbreak under an Expanded Access Investigational New Drug (EA-IND) protocol, which requires informed consent along with completing additional forms.”
When The Defender asked the CDC to clarify if the agency currently recommends ACAM2000 for mpox, an agency spokesperson said:
“It has not been used for U.S. civilians affected by the clade II global outbreak that began in 2022, and there are no plans to use it broadly during Mpox outbreaks.
“This is because JYNNEOS, the alternate to ACAM2000 in the United States, has fewer side effects.”
The Defender asked Emergent BioSolutions what it wants to tell members of the public who may be concerned about risks associated with ACAM2000 but did not receive a response by our deadline.
This article has been updated to clarify that both the FDA and CDC acknowledge that the myopericarditis risk for ACAM2000 is estimated at 5.7 per 1,000 primary vaccinations.
A team of researchers is developing a tool to track reports in the Vaccine Adverse Event Reporting System (VAERS), so vaccine-injured people can follow what happens to the reports they submit.
As part of a broader effort to hold public healthagencies accountable, the tool will also make it possible to audit the VAERS system by identifying what types of reports are deleted, insufficiently updated or contain errors.
The Centers for Disease Control and Prevention (CDC) and the U.S. Food and Drug Administration (FDA), which jointly oversee VAERS, have refused to do this work despite multiple appeals by advocates for the vaccine-injured, according to React19, the group leading the initiative.
React19, founded by a small group of medical professionals injured by COVID-19vaccines, works with institutions and providers to increase understanding and awareness of patients experiencing lasting effects following COVID-19 and/or COVID-19 vaccines.
The group is teaming up with computer programmer Liz Wilner, founder of OpenVAERS — a website that provides tools for more easily accessing and searching VAERS data — and Children’s Health Defense (CHD) to develop the tool.
The idea for developing the automatic VAERS report tracking tool came out of a VAERS audit the group conducted in 2022 to assess how the FDA and CDC were following up on COVID-19 vaccine injury reports.
React19 worked with outside experts to review a sample of 126 VAERS reports filed by some of its members who wanted to know what happened to their reports.
After tracking down each person’s reports and following them through the VAERS system, they “were kind of shocked at how bad it is,” members of React19 told The Defender.
They found that only 61% of the reports filed were correctly logged and published in VAERS. Twenty-two percent of the reports were never issued a permanent ID and are therefore not publicly visible, 12% were deleted and in 5% of the cases, a report couldn’t be filed or their report number remains unknown due to system errors.
That means more than 1 in 3 reports searched couldn’t be found in a database that is meant to be publicly accessible and transparent. It also suggests that problems of “omission of data and underreporting may be even greater than estimated,” according to the audit report.
The group also found that the medical status of the deleted reports, “by and large, had a worse outcome than the ones that were still in the system,” they said. For example, they said, in the public-facing VAERS system, 23% of reports were for permanent disabilities — but in the deleted reports, 53% were for permanent disability.
“One of the more alarming things we found out was that not all death reports are investigated,” Brianne Dressen, React19 founder, told The Defender.
The group brought this to the attention of public health officials in their meetings, sharing examples of reports that had been updated by people’s families when they died, but didn’t show up on the public system.
They also found that many follow-up reports containing updates on worsening symptoms were gone from the system.
At the time, the group was meeting regularly with top officials, including Peter Marks, M.D., Ph.D., director of the FDA’s Center for Biologics Evaluation and Research, to discuss vaccine injuries and why the agencies were doing nothing to address them.
In those meetings, according to Dressen and React19 member Dr. Joel Wallskog, when they raised the issue that the agencies weren’t following up on VAERS reports, the FDA told them VAERS wasn’t a reliable indicator for vaccine injuries, because anyone could file an injury complaint, including “Mickey Mouse or Michael Jackson.”
“We told them we know thousands of people that have not had any follow-up on their VAERS reports that are not Mickey Mouse, and they’re suffering it every single day waiting for you guys to get back to them to investigate what happened to them,” Dressen said.
“And of course then they never did anything. So we were like, OK, fine. If they’re not going to generate the evidence, then we will ourselves.”
The group submitted their findings to Marks during a meeting with him and his team. Based on their findings they also requested an external audit of the entire VAERS system and posed a series of questions listed on their audit report webpage.
They never heard from the agencies again.
“We were like, really?” Dressen said. “We were having these regular meetings with them every one month or every two months, and then after that, they wouldn’t meet with us anymore.”
Dressen, who was injured in the AstraZeneca clinical trials and whose diagnosis of post-vaccine neuropathy and other vaccine-related disorders was confirmed by the National Institutes of Health, said her own VAERS report is not visible to the public. The agencies haven’t told her why.
More recently, still hoping for accountability from the public health agencies, React19 submitted its audit and complaint to the Office of Inspector General at the U.S. Department of Health and Human Services.
The only response they received was an autoresponse confirming receipt of the complaint.
Attempt to ‘bring power back to the people’
In its small pilot audit, React19 found the VAERS system is “obviously broken from top to bottom.” According to Dressen, “One thing we can easily conclude is that the FDA and CDC have no interest in addressing these issues.”
Now, the group is scaling up the project to do a larger audit with more data.
With help from OpenVAERS and CHD, the team built a backend, automated administrative tracking system that eliminates the need to manually search for each report and its journey through VAERS — something the analysts had to do for the first iteration of their audit.
Participants will register on the React19 website and will be invited — if they are interested — to share their stories as part of the organization’s project to collect and publish vaccine injury testimonials.
Users can share any information they have about their VAERS report — their ID number if they have one, or if not, details about their case. Then they will receive a monthly email with the status of their report.
For example, someone who has a user ID and a public-facing report will be informed if their report disappears. In the case of those people who filed a VAERS complaint but never got an ID number, the system will search each month for the record and try to find the ID.
“We’ll be able to track these reports through the system and figure out what happens to them,” Wilner said. “Do they disappear? Do they appear and the person doesn’t get notified? Do they appear incorrectly?”
“So people will be able to track their own reports with less effort and React19 will be able to audit a much larger user base than they initially did.”
Wilner said auditing VAERS in this way also reveals details about how the agencies are “either lying or deliberately obfuscating the process.” In the first audit, it was clear there was no systematic or automated way that, for example, reports were deleted.
The tracker and the audit will provide valuable data that no one else has. Rather than having only the stories, Wilner said, they will have the data backing up those stories. “Now we have a group of injured people that are all talking with one voice.”
“Without more pressure and more discovery,” Wallskog said, “I don’t think we’re ever going to get the truth out. Ultimately, we want to get this information to the masses of people that just don’t know what’s happening, particularly with this data, and that we’ve all been duped.”
Dressen said the project is an attempt to “bring the power back to the people.”
The COVID-19 vaccine produced a large swath of vaccine injuries all at the same time, she said. Auditing the COVID-19 entries in VAERS will provide an opportunity “to show through massive numbers where those problems are, not just with the systems that are supposed to be monitoring vaccine safety, but also the actual harms themselves and what those are, but the government’s not doing their job on that.”
The two faces of VAERS and the problem of accountability
Wilner said Dressen’s injury report, sitting in VAERS limbo, spoke to one of the major issues around claims of transparency in the database — that there are two versions of VAERS, a public-facing database and a private one.
The BMJreported last year that it investigated the VAERS database and found that the public facing database contains only initial reports. And “a private, back end system containing all updates and corrections — such as a formal diagnosis, recovery, or death.”
The CDC told The BMJ that this was part of patient confidentiality, but the publication found that in the FDA’s Adverse Event Reporting System, they do update the database — “raising the question of why VAERS can’t do the same.”
And during the React19 audit, the group found that VAERS was sometimes deleting people’s legitimate reports or the more detailed updated reports that some people were submitting.
Another problem, Wilner noted, is that a lot of key information — such as race, pregnancy and report provider — is unnecessarily withheld from public VAERS reports. She also said the agencies sometimes leave reports on there that are clearly false or jokes, which then discredits the database in the public’s eyes.
On the CDC website, Wilner said, “you’re basically looking at a doctored set of books.”
Wallskog said the agencies “try to live on both sides of the fence” with VAERS, presenting it as a key tool for monitoring vaccine injuries. But when it shows a safety signal or an issue with vaccines, they discredit it as a problematic surveillance system with a lot of limitations that can’t be trusted.
“It’s incredibly frustrating for injured people,” he said.
The team working on the new VAERS tracking system and audit said they hope it will raise public awareness and force the public health agencies to take responsibility for the vaccine injuries.
“Rochelle Walensky said the CDC is charged with finding legitimate vaccine injuries and reporting them,” Wilner said. She added:
“If that’s the case, where is that? We don’t have access to the actual database to figure it out so we want to know where is the report from the CDC on the people that were actually injured by the COVID vaccine that the government accepts were legitimately injured? That report doesn’t exist.”
Bird flu is all the rage. As this issue heats up, here is a bit of information about each of the three bird flu (H5N1) vaccines licensed by the FDA.
First is Sanofi (National Stockpile),which was licensed for adults based on a clinical trial in which only 103 adults were vaccinated and 48 received the placebo. Worse, there were four serious adverse events in the vaccine group.
Next up is ID Biomedical,which was licensed for adults in a clinical trial in which the vaccine group had four times the rate of new immune-mediated diseases. The trial for ages 6 months to 17 years had only 838 children, making it underpowered and unable to adequately measure safety.
And last but not least is Seqirus, which was licensed for adults in a clinical trial in which 0.5% of the vaccinated group died but only 0.1% of the placebo group died. The trial for ages 6 months to 17 years had only 329 children, making it significantly underpowered and unable to adequately measure safety.
And that is a wrap. Needless to say, if you plan to get pricked, be informed!
Despite public statements by government officials affirming the safety and efficacy of COVID-19 vaccines in early 2022, documents obtained by Children’s Health Defense (CHD) reveal that, at that time, public health officials were increasingly concerned about vaccine-related adverse events.
The 300 pages of documents released on Aug. 22 contain private correspondence from 2021 and early 2022 between U.S. Food and Drug Administration (FDA) and National Institutes of Health (NIH) officials, and emails from vaccine-injured individuals to NIH scientists.
CHD requested the documents via a Freedom of Information Act (FOIA) request in 2022. In April 2023, CHD sued the NIH to obtain the records after the agency failed to respond. In an October 2023 settlement, the NIH agreed to produce 7,500 pages of documents at a rate of 300 pages per month.
Last month’s tranche of documents showed that in late 2021 and early 2022, FDA and NIH officials privately expressed concerns about the growing rate of adverse events related to the COVID-19vaccines — concerns that reached high-level FDA officials.
A Jan. 24, 2022, email (pages 239-240) to Dr. Janet Woodcock, the FDA’s principal deputy commissioner of food and drugs, and Peter Marks, M.D., Ph.D., director of the FDA’s Center for Biologics Evaluation and Research, alerted them to the existence of “scientific data” regarding adverse events.
The email, titled “Impromptu Meetup” and sent by an individual whose name is redacted, stated:
“We are in [Washington] DC the remainder of today and tomorrow. Some of our epidemiologists happen to be in town as well and would like to have the opportunity to review with you the scientific data they have.
“Also checking in to see what progress has been made with our researchers?”
In a reply later that day, Woodcock said, “We are evaluating the data and analyses that have been done on adverse events after vaccination, particularly neurologic AE’s” (adverse events).
However, she added that the FDA was “not having in person meetings” at that time but stated that “something could be set up for a discussion between the scientists but it would need to be scheduled to ensure the right people attend.” She did not clarify who the “right people” would be.
On the same day, Marks also responded to the email, stating that the FDA has “connected with” NIH researcher Dr. Avindra Nath — who was studying vaccine-related adverse events — and was “also working through contacting other physicians as well.”
Marks added that he “sent a note to our pharmacovigilance group to see if they can free up time today or tomorrow” but said that “setting up a virtual meeting at some point in the near future when there is more time to plan participants and the agenda may make sense.”
There is no indication as to whether this meeting ultimately took place.
The emails followed just months after another NIH scientist, Farinaz Safavi, M.D., Ph.D., of the NIH Division of Neuroimmunology and Neurovirology, appeared to acknowledge the potential dangers of COVID-19 boosters.
In a Sept. 30, 2021, email (page 129), Safavi told a vaccine-injured individual, “We do not have any data to suggest for or against booster shot [sic] but the consensus among our team is not to take if patient develop [sic] significant neurological complications post vaccine.”
The individual emailed Safavi earlier that day asking whether it was advisable to receive the then-new COVID-19 booster, despite saying that “nothing has really changed” regarding their symptoms.“I think my ears are still off, but I have gotten used to it.”
The injured person previously contacted Safavi earlier in 2021 complaining about injuries sustained following vaccination — describing in a March 26, 2021, email (page 136), “severe paresthesias in my face and scalp and tongue and chest band tightness,” and “severe muscle spasms in my scalp and jaw and even my gums and teeth hurt.”
Vaccine injury victims felt ‘very betrayed’
But while some people injured by the vaccines received replies and advice from NIH scientists, the latest documents showed that many others received no such replies. Some sent desperate emails to NIH scientists asking for help or an update.
For instance, in a Jan. 14, 2022, email (pages 234-235) to Nath, a vaccine-injured person praised Nath for his previous work helping the vaccine-injured, but then noted that he and other NIH scientists subsequently abandoned them. The email stated, in part:
“Dr. Safavi left a vaccine injured chat last September, something strange was going on. The active engagement from the spring and summer was replaced with distance and vague responses, then nothing. But then some people get telehealth visits, and vague responses … and others are told ‘there is no research’ and that’s it for them.
“I am sure you would understand now why the hundreds+ who were turned down for any assistance are now extremely upset after waiting for so long … many feel very betrayed. They have been waiting and waiting, all while suffering every single day. … The conversation isn’t happening. They are dying.”
Marks and other FDA officials appear to have met with vaccine-injured individuals a few months prior, according to an Aug. 18, 2021, email sent to Nath (page 283). In that email, the vaccine-injured person wrote:
“Our ‘injured’ MDs and I are meeting with peter marks and paul Richards [sic] at the FDA Monday morning. I have discussed this with Janet Woodcock and Paul for the last few weeks.
“Hopeful they will be willing to help us ‘nobodies’ in our quest to get medical help for people, or any sort of acknowledgement so people are able to begin dialogue with their home physicians.”
Some victims said Marks blew off scheduled meetings with them.
Dr. Danice Hertz, a retired gastroenterologist from California injured by the Pfizer-BioNTech COVID-19 shot she received in December 2020, previously told The Defender that she and a group of vaccine-injured individuals secured a Zoom meeting with Marks in early 2021 — which he then skipped.
Previously released documents from CHD’s lawsuit against the NIH contained emails showing that Marks and Woodcock were aware of reports about COVID-19 vaccine injuries in early 2021, including emails from injured people throughout 2021 and 2022 seeking help regarding their injuries.
Other documents indicate that, as early as January 2022, NIH researchers were aware of at least 850 peer-reviewed case reports and/or research articles about COVID-19 vaccine reactions.
In one email (name and agency redacted), NIH researchers were told the federal government was “saddled” with the “mess” of dealing with those injured by the COVID-19 vaccines, due to the liability shield enjoyed by vaccine manufacturers.
Marks, FDA still publicly claim COVID shots are safe and effective
Marks continues to promote the COVID-19 vaccines as safe and effective and downplay the extent and severity of vaccine-related adverse events.
Last month, he advised the public to get newly updated formulations of the COVID-19 shots, stating the new vaccines “meet the agency’s rigorous, scientific standards for safety, effectiveness, and manufacturing quality.” He said vaccination “continues to be the cornerstone of COVID-19 prevention.”
In a subsequent interview with NPR though, Marks hedged on the question of how effective the new vaccines are.
“The vaccine is not intended to be perfect,” Marks said. “It’s not going to absolutely prevent COVID-19. … But if we can prevent people from getting serious cases that end them up in emergency rooms, hospitals or worse — dead — that’s what we’re trying to do with these vaccines.”
During congressional testimony in February, Marks said, “There was a signal for myocarditis or pericarditis only after the primary vaccination series with the Pfizer mRNA vaccine in those 12 to 17 years of age, and that now that signal is not being seen more recently.”
Marks also claimed that numerous false reports are submitted to the Vaccine Adverse Event Reporting System (VAERS), though other experts have disputed this assertion.
However, Marks also acknowledged that the FDA was overwhelmed with adverse event reports after the COVID-19 vaccines became available, stating that “the avalanche of reports was tremendous.”
The attorney from the Department of Justice who defended the Food & Drug Administration in court admitted on undercover camera that the agency’s actions were an abuse of authority by the government during its public campaign against ivermectin to treat COVID-19.
A trio of doctors recently won a major legal victory in a multi-year lawsuit sparked by the FDA’s viral 2021 public health guidance advising against the use of ivermectin for treating COVID-19. The most notable offending tweet stated, “You are not a horse. You are a not a cow. Seriously, y’all. Stop it.”
Department of Justice trial lawyer, Isaac Belfer, defended the FDA in this suit brought by Drs. Mary Talley Bowden, Robert L. Apter, and Paul E. Marik. On undercover camera, Belfer admits to a Project Veritas journalist that his client’s legal loss was deserved because the agency overstepped its statutory authority when it publicly tweeted medical advice.
Belfer told our journalist, “So, what the agency has done… [is] unquestionably beyond its authority. Making a recommendation of what drugs to take or not to take, that’s the practice of medicine. And FDA can’t practice medicine.”
The FDA’s public relations campaign also failed to inform the public that the award-winning antiparasitic medicine had a decades-long track record of successful medical usage in humans.
During the COVID-19 pandemic, the doctors prescribed ivermectin to tens of thousands of patients and found the drug to be a cheap and effective treatment.
The doctors told Project Veritas that they suspect that the suppression campaign against ivermectin was motivated by the government’s interest in fast-tracking the experimental COVID-19 vaccination. This speedy vaccine roll-out could only be accomplished through the FDA’s emergency use authorization [EUA], and only if no other alternative medications existed to treat COVID-19.
The FDA’s tweets caused a deadly chain reaction. The agency’s pronouncements were swiftly enforced by national medical associations and regulatory agencies, pharmacists refused to fill prescriptions, insurance refused to pay for it, and doctors who prescribed it faced career ruin.
Drs Apter and Bowden told Project Veritas that suppression of ivermectin led to a prolonged pandemic, and potentially millions in excess COVID deaths.
Apter: “It’s not unreasonable to think that there have been a million unnecessary deaths from COVID in the United States because of the public health agency suppression of effective early treatment with repurposed inexpensive medications.”
Bowden: “If more people had access to early treatment in the form of ivermectin, monoclonal antibodies, hydroxychloroquine… we could have nipped the pandemic in the bud.”
As a result of the lawsuit, the FDA was forced to delete its social media posts warning against the use of ivermectin for treating COVID-19. Though the FDA removed its public statements, the agency did not change its policy or directives. Because major state and national medical governing authorities look to the FDA as an authoritative source on the appropriate use of drugs, pharmacies still refuse to prescribe ivermectin, and doctors face professional repercussions for prescribing it.
Dr. Talley Bowden was forced to resign her privileges from Houston Methodist Hospital; Apter was referred to the Washington Medical Commission and Arizona Medical Board for disciplinary proceedings; and Marik was forced to resign from his positions at Eastern Virginia Medical School.
Apter: “Because of my prescription of ivermectin for COVID I am still facing persecution by the medical licensing boards in spite of the fact that they have not been able to show a single adverse event in my care.”
Bowden: “I have a medical board coming after me because I tried to help a patient get ivermectin. We all had professional repercussions because of our use of ivermectin.”
Though the doctors continue to face professional consequences for their advocacy of ivermectin use for COVID-19, Belfer admits that the doctors dealt a significant blow to the government with their court victory. He told Project Veritas that the agency will think twice before issuing any misguided health advice in the future.
“I think going forward they’ll [FDA] probably be a bit more careful. They [the doctors] got an opinion that was good for them. That kind of limited FDA’s authority. It’s not okay to… actually tell people, ‘You should not take this drug.’”
Dr. Bowden says the fight against government overreach was worth it, because now doctors are vindicated in their years-long quest to protect the health of their patients.
Bowden: “One thing this case did is set a precedent. I think it permanently tarnished the reputation of the FDA. I think the public will takes the FDA little less seriously now, and it keeps them from making the same bold, reckless move in the future when it comes to telling patients what they can and cannot do. Like Isaac [Belfer] said, and we have all said, the FDA is not your doctor. The FDA has no business telling patients what they can take. And we proved in the court of law that they cannot do that.”
As I predicted, our new co-plaintiff Kennedy meets even the Supreme Court’s stringent standing requirements, the injunction against the government is back in play.
As I explained in a previous post, Robert F. Kennedy Jr.’s companion lawsuit Kennedy v. Biden has been consolidated by the court into our Missouri v. Biden case. Based upon documents we obtained on discovery, the court recently found that Kennedy meets the Supreme Court’s stringent standing criteria. We only need one co-plaintiff with standing to bring the case and the petition for the injunction. So the injunction is back in play, and we will likely find ourselves at the Supreme Court again in a few months. Unless SCOTUS invents another technicality on which to temporize, they will be forced to rule on the merits of the evidence against the government, which we believe is overwhelming.
On the issue of Kennedy’s standing, U.S. District Court judge Terry Doughty last week ruled: “There is not much dispute that both Kennedy and CHD [Kennedy’s nonprofit Children’s Health Defense] were specifically targeted by the White House, the Office of Surgeon General, and CISA, and the content of Kennedy and CHD were suppressed. Therefore, Kennedy must now show a substantial risk that in the near future, at least one platform will restrict the speech of Kennedy in response to the actions of one Government Defendant.” Citing evidence we uncovered in Missouri v. Biden, Doughty explained: “The Court finds that Kennedy is likely to succeed on his claim that suppression of content posted was caused by actions of Government Defendants, and there is a substantial risk that he will suffer similar injury in the near future.”
The latest ruling is not only significant for Kennedy but for the future of online speech. In June of this year, the Supreme Court ruled that the state attorneys general of Missouri and Louisiana did not have standing to bring their case on government directed mass censorship. Now that Kennedy and the CHD have been found to have standing in the matter, the Supreme Court will likely have an opportunity to judge the issue on its merits rather than on a technicality as it did when making its standing ruling on an injunction in June.
If Kennedy and his co-plaintiffs are able to demonstrate to judges that the Biden administration’s intrusion into the actions of major social media companies resulted in censorship, the country will be one step closer to a major legal ruling guaranteeing freedom to speak online without the censorious interference of the federal government.
In related news, Kennedy announced Friday that he is suspending his presidential campaign. While he has deep disagreements with Trump on several issues, he is endorsing Trump’s candidacy to advance the key issues on which they have substantial agreements—including stopping government censorship and propaganda. His 48-minute speech announcing this decision was an extraordinary moment in American politics and is worth watching. In addition to discussing the issue of government censorship, which seriously hamstrung his ability to campaign, Kennedy’s remarks focus also on the root causes of the current epidemic of chronic disease in the United States.
While there is online buzz that Trump may tap Kennedy as Attorney General, I anticipate if Trump is elected he will appoint Kennedy to his cabinet as Secretary of Health and Human Services, a department which includes the CDC, FDA, and NIH. This could prove a welcome opportunity for the reform of our public health agencies. I am currently working with a team of policy analysts and health freedom advocates on concrete policy proposals for just such reforms, and will keep you posted on our progress with that project.
New vaccines should be proven safe before they are accepted onto the Centers for Disease Control and Prevention (CDC) vaccine schedule.
Here is what is actually happening: Vaccine companies are doing studies that claim to demonstrate the safety of new vaccines but are carefully designed and conducted to intentionally hide the toxicity of these vaccines.
To see how this is done, read on.
What does an honest vaccine safety study look like?
An honest safety study must have a test group that gets the vaccine and a control group that gets a harmless placebo. Injuries and deaths are compared in the two groups.
If the test group has many more adverse events than the placebo control group, the vaccine is not safe.
Most people would be shocked to learn that none of the vaccines on the CDC vaccine schedule have been safety tested in this way.
What does a fraudulent vaccine safety study look like?
Rule No. 1 for conducting a fraudulent study: Do not have a placebo control group. Here is where the fraud is happening: The “control group” is deliberately given something that is as toxic as the vaccine being tested. It can be an older vaccine or the vaccine ingredients minus the antigen.
The results will show that the injuries and deaths are similar in both groups. That is because they are both receiving toxic ingredients. The new vaccine is then illogically declared safe.
If there is no placebo control group, the toxicity of the vaccine is hidden. This is both clever and diabolical. Can you see it?
The public is unaware of this subterfuge
“Turtles All The Way Down: Vaccine Science and Myth” is the most thorough and brutally honest book ever written about vaccines.
The authors tell us on page 81:
“As we have seen in this chapter, vaccine trials are designed and performed in such a way as to ensure that the true extent of adverse events is hidden from the public. There is not a single vaccine in the US routine childhood vaccination schedule whose true rate of adverse events is known.”
Two examples of how unsafe toxic vaccines got on the CDC vaccine schedule
Prevnar-13 (a pneumococcal vaccine) was given to the test group of children and the “control group” was given the older Prevnar vaccine.
Severe adverse events occurred in 8.2% (one out of every 12 children) in the test group. Severe adverse events also occurred in 7.2% (one out of every 14 children) of the control group.
What percent of a placebo control group would have had severe adverse events? Probably 0% because they would have received something harmless. We can’t know because the authors of this study chose not to have a placebo control group.
The Prevnar-13 vaccine was declared “safe” and was approved for use by the U.S. Food and Drug Administration (FDA). You don’t have to be a doctor or scientist to suspect that both the Prevnar and the Prevnar-13 vaccines are unsafe. “Turtles All The Way Down” covers this fraudulent vaccine safety study on pages 60 and 61.
Here is the second example, which the authors describe on pages 77 and 78:
“In one of the DTaP vaccine trials, 1 in every 22 subjects in the trial group was admitted to the hospital. A similar hospitalization rate was also reported in the ‘control group’ (which received the older-generation DTP vaccine).”
Again, there was no placebo control group. Both vaccines appear to be decidedly unsafe yet the newer DTaP vaccine made it onto the CDC vaccine schedule. DTP and DTaP vaccines contain antigens for diphtheria, tetanus and pertussis.
Why is this happening?
Ultimately, the answer is greed. It is enormously profitable to get a vaccine on the CDC schedule. Vaccine companies will do whatever it takes to accomplish this. If it takes a little scientific fraud, so be it.
The vaccine companies are cheating on vaccine safety studies by omitting placebo control groups, thereby lying about the safety of vaccines. The FDA and CDC are complicit because they are doing nothing to stop this fraud.
Corporate capture or regulatory capture
The FDA and CDC are regulatory agencies. The original function of these agencies was to protect the public from dangerous drugs and vaccines.
Unfortunately, these agencies have been captured by Big Pharma. They no longer focus on protecting the public. They focus on protecting and promoting the interests of pharma companies.
Can we compare the health outcomes of vaccinated versus unvaccinated children?
Theoretically, yes but not if we expect our health authorities or pharma companies to do these types of studies. Chapter 6 of the “Turtles” book is titled “The Studies That Will Never Be Done.”
On page 207 the authors tell us:
“No study that compares the health of vaccinated children to that of unvaccinated children has ever been done by the medical establishment.”
If such a study showed that vaccinated children are healthier than unvaccinated children, it would have been published and been headlined in every newspaper and been the lead story on the nightly news. That hasn’t happened. We suspect that such a study has been done internally at the CDC.
The unwanted conclusion that they won’t allow to see the light of day is that unvaccinated children are far healthier than vaccinated children. This study has likely been done and buried instead of published. Such a study is verboten because it would be a disaster for the vaccine companies.
Private studies show that unvaccinated children are healthier
Here are two privately funded studies:
“Relative Incidence of Office Visits and Cumulative Rates of Billed Diagnoses Along the Axis of Vaccination” by Dr. Paul Thomas and James Lyons-Weiler, Ph.D.
Another great resource is the book “Vax-Unvax: Let the Science Speak,” by Robert F. Kennedy Jr. and Hooker. They report on many studies where unvaccinated children have better health outcomes compared to vaccinated children.
Science is for sale
The book “Science for Sale: How the US Government Uses Powerful Corporations and Leading Universities to Support Government Policies, Silence Top Scientists, Jeopardize Our Health, and Protect Corporate Profits” by David L. Lewis, Ph.D., tells the story of how corporate profits can frequently trump true science.
This happens in many industries, not just in vaccines. It is not unusual for government agencies to take the side of the corporations. The author was fired from the EPA for revealing details of how this happens.
The health of the public is subverted by powerful corporations in these situations. Does that sound familiar? Lewis doesn’t cover vaccines in his book except in Chapter 7 where he describes how Dr. Andrew Wakefield was unjustly crushed for questioning the safety of the measles-mumps-rubella or MMR vaccine.
Are vaccines the main cause of autism?
If the answer is yes, that would be very bad for vaccine companies. The “Turtles” authors point out on page 209 how our health authorities are trying hard not to find the correct answer to this question:
“Over the past 15 years, dozens of epidemiological studies have been conducted examining the association between vaccines and autism, but not a single one compared the rate of autism in fully vaccinated and fully unvaccinated children.”
If they actually wanted to answer this question, they would do vax/unvax studies. Such studies are easy to do but our health authorities refuse to do them.
Why do health authorities favor epidemiological studies?
The “Turtles” authors provide the answer on page 198:
“Epidemiological studies are the tool of choice for health authorities and pharma companies to maintain a facade of vaccine safety science. They are cheap, relatively simple to conduct, and, above all, their results are easily manipulated.”
It is entirely possible to get an epidemiological study to conclude whatever its authors want it to conclude. These types of studies are not the gold standard.
What caused the drastic decline in infectious disease mortality?
We are supposed to believe that vaccines have been our saviors. Not true. The huge decline in infectious disease mortality was largely due to sanitation, hygiene and improved nutrition (the availability of fresh fruits and vegetables year-round).
The “Turtles” authors make this clear on page 293. They reference a report by the American Institute of Medicine, which states:
“The number of infections prevented by immunization is actually quite small compared with the total number of infections prevented by other hygienic interventions such as clean water, food, and living conditions.”
The claim that vaccines alone saved us is false and our health authorities know it is false.
Below is a simple graph that causes cognitive dissonance in those who believe that vaccines saved us from high rates of infectious disease mortality.
We can clearly see that deaths from measles were reduced to near zero by the interventions mentioned above BEFORE the measles vaccine was introduced.
Similar graphs for other infectious diseases are shown in the book “Dissolving Illusions: Disease, Vaccines, and the Forgotten History” by Dr. Suzanne Humphries and Roman Bystrianyk. The mortality rate for all infectious diseases was dropping rapidly before vaccines were introduced.
Do you smell a rat?
Yes. And it has been dead for quite a while. We have been bamboozled (deceived, cheated, swindled and defrauded).
Vaccines are now doing far more harm than good by causing a huge increase in chronic diseases like autism, asthma, attention-deficit/hyperactivity disorder or ADHD, Type 1 diabetes, learning disabilities, seizures and much more.
It is way past time to use honest unbiased science to sort it out. Imagine what will happen when honest science is applied to vaccine safety studies.
Here is how the ‘Turtles’ authors sum it up
On page 518:
“Science belongs to the people. It belongs to humanity, not to corrupt government agencies and pharmaceutical giants who collude to rewrite the principles of science in order to continue the decades-long cover-up of their crimes against humanity.
“The magnitude of these crimes is enormous — these entities are in way too deep to ever be able to admit any wrongdoing. They will do whatever is necessary to protect the great vaccine hoax. For them, it is a matter of life and death — literally. And so it is for us.”
The lie that vaccines are safe and effective and that serious adverse events are exceedingly rare is still believed by many people — yet trust in pharma and our coopted regulatory agencies is now rapidly eroding. For example, only a tiny percentage of people are continuing to take the COVID-19 vaccine boosters.
Also, the percentage of parents who are choosing to obtain an exemption to vaccines for their children is increasing. This can be done in almost all states.
It is becoming obvious to a growing number of people that we are being intentionally misled regarding vaccines and vaccine safety.
Introduction: For the greater part of a decade the US, the UK and the EU have been carrying out a campaign to undermine and overthrow the Russia government and in particular to oust President Putin. Fundamental issues are at stake including the real possibility of a nuclear war.
The most recent western propaganda campaign and one of the most virulent is the charge launched by the UK regime of Prime Minister Theresa May. The Brits have claimed that Russian secret agents conspired to poison a former Russian double-agent and his daughter in England, threatening the sovereignty and safety of the British people. No evidence has ever been presented. Instead the UK expelled Russian diplomats and demands harsher sanctions, to increase tensions. The UK and its US and EU patrons are moving toward a break in relations and a military build-up.
A number of fundamental questions arise regarding the origins and growing intensity of this anti-Russian animus.
Why do the Western regimes now feel Russia is a greater threat then in the past? Do they believe Russia is more vulnerable to Western threats or attacks? Why do the Western military leaders seek to undermine Russia’s defenses? Do the US economic elites believe it is possible to provoke an economic crisis and the demise of President Putin’s government? What is the strategic goal of Western policymakers? Why has the UK regime taken the lead in the anti-Russian crusade via the fake toxin accusations at this time?
This paper is directed at providing key elements to address these questions. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.

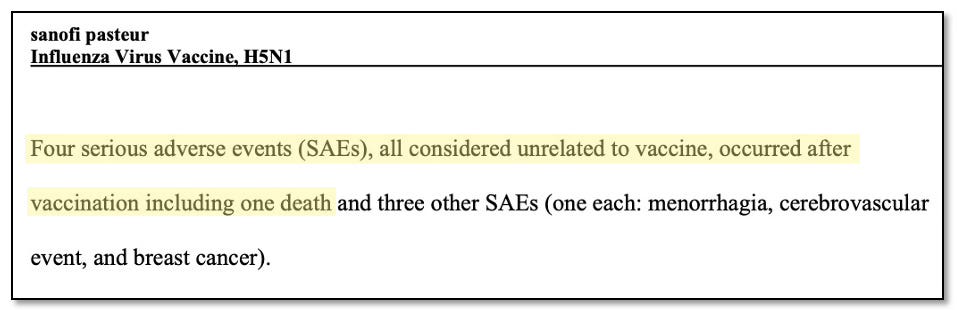

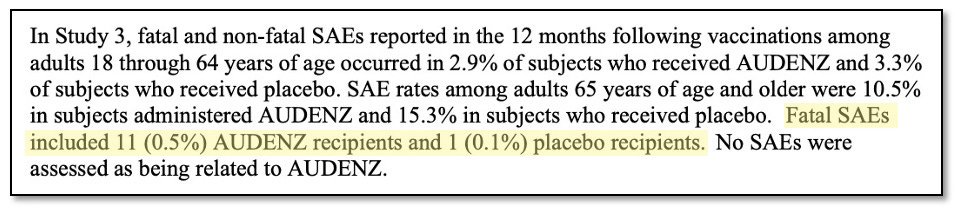


 Aletho News
Aletho News
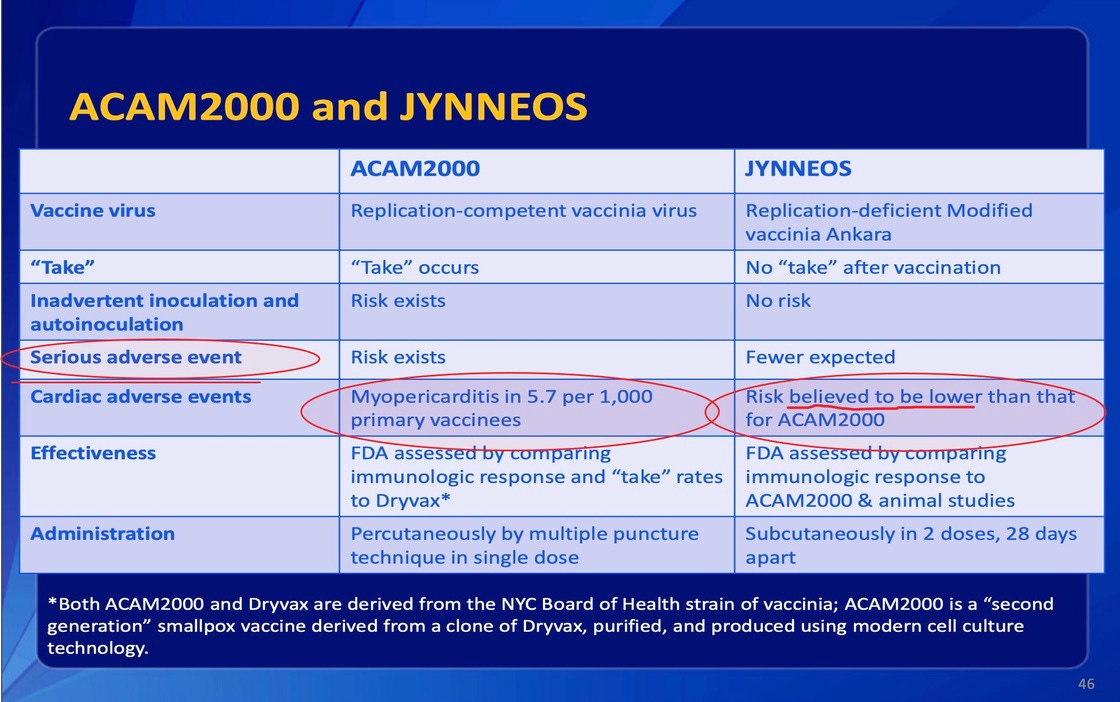{kind=link}