Dr. Paul Offit Lets Us Know ‘the Experts’ Have Officially Lost Their Minds
By Madhava Setty, M.D. | The Defender | July 5, 2023
I don’t have a big presence on Twitter. I don’t find the platform suitable for exploring and critiquing interesting ideas. You can say only so much in 280 characters. It’s great for inciting someone or dropping a witty comeback or link without much context.
At least that’s what I thought. Then I stumbled upon a tweet from Dr. Paul Offit. He’s taught me that you can convey a lot in a few short sentences.
Who is Dr. Paul Offit?
Offit is a big name in vaccines. Beyond what is listed below, he also sat on the Advisory Committee on Immunization Practices for the Centers for Disease Control and Prevention (CDC) and is presently a member of the Vaccines and Related Biological Products Advisory Committee for the U.S. Food and Drug Administration (FDA).
He’s had a say in the approval and/or authorization of many biologics, including the COVID-19 mRNA products.
Briefly, Offit is:
- Director of the Vaccine Education Center and professor of pediatrics in the Division of Infectious Diseases at Children’s Hospital of Philadelphia.
- Maurice R. Hilleman Professor of Vaccinology at the Perelman School of Medicine at the University of Pennsylvania.
- An internationally recognized expert in the fields of virology and immunology.
- A founding advisory board member of the Autism Science Foundation and the Foundation for Vaccine Research.
- A member of the Institute of Medicine and co-editor of the foremost vaccine text, “Vaccines.”
- The author or co-author of more than 150 papers in medical and scientific journals in the areas of rotavirus-specific immune responses and vaccine safety.
- The co-inventor of the rotavirus vaccine, RotaTeq®, recommended for universal use in infants by the CDC.
- A recipient of the Charles Mérieux Award from the National Foundation for Infectious Diseases.
His list of accomplishments goes on.
I don’t pretend to know more about vaccines than he does. I’m just an anesthesiologist and engineer. He must be a very smart person. Which is why this tweet is so baffling:
Why is Offit tweeting about placebos and saltwater right now?
It has to do with a truth bomb Robert F. Kennedy Jr. dropped at a town hall event last week.
According to Kennedy, chairman on leave from Children’s Health Defense, he and attorney Aaron Siri sued the U.S. Department of Health and Human Services (HHS) after HHS refused to meet their demand to produce at least one study comparing the safety of a vaccine on the childhood immunization schedule with a true placebo.
In a written response received more than a year later, the HHS did not cite a single such study, instead claiming:
“Inert placebo controls are not required to understand the safety profile of a new vaccine, and are thus not required.”
This stupefying claim made by Melinda Wharton, M.D., MPH, acting director of the National Vaccine Program Office, should be attacked on podcasts and publications everywhere.
How do you know that a new vaccine is safe if it isn’t tested against an inert placebo, Dr. Wharton?
If you are someone who is willing to abandon basic logic and trust every single word spewed by our public health agencies, ask yourself, why then does the FDA demand that medicines be tested against a placebo to ensure safety prior to licensure?
Twitter lit up around this pivotal topic. The tweet from one of the foremost vaccine experts in the world (Offit) was in response to Siri, who, according to Offit, asserted that virtually all vaccines on the childhood vaccination schedule, including RotaTeq (Offit’s brainchild), were not licensed by the FDA based on a placebo-controlled clinical trial.
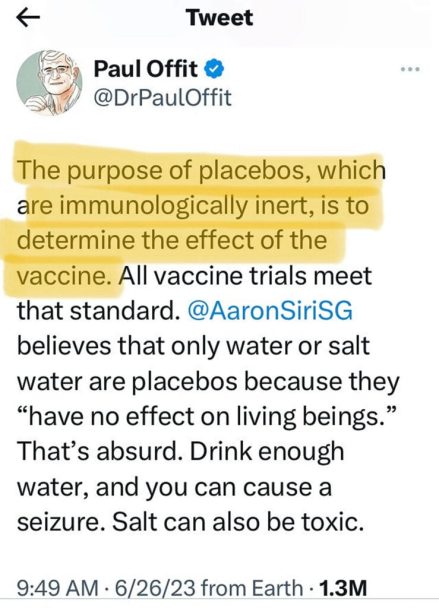
Let’s break down Offit’s attack on Siri. Offit states: “The purpose of placebos, which are immunologically inert, is to determine the effect of the vaccine.”
Yes, Dr. Offit, one purpose of a placebo is to determine the effect of the vaccine. In order to prove that it works, it must do better than an immunologically inert substance. In other words, it must exceed the so-called placebo effect.
But that’s not the only purpose placebos serve. With regard to safety, a new vaccine has to be compared to something that has the least possible chance of causing deleterious effects.
To be clear, those who eschew a vaccine do not get in line for a shot of an “immunologically inert substance.” They stay away from the vaccine clinic altogether and take their chances.
This is why the placebo must be a true placebo. The best we can possibly do is use saline, a saltwater solution that reasonably matches the sodium concentration in our plasma. It is what is used to dilute medications and replenish blood volume. It’s what you use to store your contact lenses.
Offit then adds this:
“[Aaron Siri] believes that only water or salt water are placebos because they ‘have no effect on living beings.’ That’s absurd. Drink enough water, and you can cause a seizure. Salt can also be toxic.”
Offit is saying that by drinking a large amount of water the plasma sodium concentration in a person can abruptly decrease which, in fact, can lower the seizure threshold. He’s not wrong, it does happen in pathological conditions, especially in the critically ill.
Can salt be toxic? Yes. Ingestion of a large amount of salt will stimulate properly functioning kidneys to increase the absorption of free water, thus mitigating the effect of the salt load. This can cause volume overload and put a person at risk for heart failure and pulmonary edema.
So what — if not 0.2 ml of saline — should we use for a placebo, Dr. Offit? A tiny aliquot of adjuvants (that can include elements like aluminum)? Pro-inflammatory lipid nanoparticles? Viral or toxin deactivators like formaldehyde? Preservatives like thimerosal that contain mercury, one of the most potent neurotoxins known (yes, mercury in this form is still in some flu vaccines according to the CDC)?
All of these substances are “immunologically inert.”
But why would you consider using them as a placebo control if not to mask the potential harm of the vaccine in question?
Is that how inventors of vaccines for our children view placebos? Is that how advisory committee members on the FDA view them? What about the other advisory board members of the Autism Science Foundation? Why would anyone trust any vaccine on the childhood immunization schedule after such comments?
You don’t have to be Maurice R. Hilleman Chair of Vaccinology at the Perelman School of Medicine to see that your comments here are misleading, disingenuous and purposefully inciting.
Moreover, they don’t make any sense.
What would other recipients of your long list of awards have to say about your comments on placebos? I don’t think they would approve, sir.
Your public statements also sully the excellent reputation of the Children’s Hospital of Philadelphia and those who were lucky to train there, like me.
Dr. Setty has been a board certified anesthesiologist since 2002 and has held various leadership positions in his clinical practice.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
RFK Jr. Dismantles Doctor’s Pro-Vaccine Stance in Town Hall Meeting
By Madhava Setty, M.D. | The Defender | June 29, 2023
Epistemology is the theory of knowledge. Epistemologists ask the foundational question, “How do we know what we know?”
Robert F. Kennedy Jr. on Wednesday appeared in a town hall meeting hosted by NewsNation and moderated by journalist Elizabeth Vargas.
The exchanges between Kennedy — chairman on leave from Children’s Health Defense — Vargas and Dr. Tariq Butt, a family medicine doctor in the audience, demonstrated the real quagmire the scientific community finds itself in.
Doctors and journalists cannot see the difference between believing and knowing. If we were in a rational world, there wouldn’t be the need for censorship and shadowbanning.
Nor would many of the vaccines on the childhood immunization schedule, as presently formulated and tested, have found their way into the arms of young human beings.
In 13 short minutes, Kennedy deftly demonstrated to the audience that our problem isn’t just a failure of epidemiology — it’s one of epistemology:
Vargas first framed the topic this way:
“The biggest controversy surrounding your candidacy is your stance on childhood vaccines. Nearly every scientific and medical organization including the CDC [Centers for Disease Control and Prevention], the FDA [U.S. Food and Drug Administration], the AMA [American Medical Association], the American Academy of Pediatrics, all say you’re wrong on this issue.”
Vargas opened the door for Kennedy to not only clarify his position — which he said has been distorted and misrepresented no matter how many times he has tried to set the record straight — but she also revealed how little thought and research she has done into the controversy.
Kennedy pointed out the reality of the situation. These are not organizations that have independently arrived at their conclusions. The AMA, the American Academy of Pediatrics and “nearly all scientific and medical organizations” take information coming from the CDC and FDA as gospel.
In other words, if the CDC and the FDA are wrong, the entire medical establishment is wrong.
There’s a difference between consensus and herd mentality — a fact that never seemed to register with Vargas.
Kennedy is immensely knowledgeable about vaccine science and the regulatory process, as well as its corruption by Pharma interests. Moreover, he is a seasoned litigator and is not careless in his delivery. He correctly asks Vargas for clarification: “On what issue?”
Vargas first alludes to the possibility that vaccines could be the cause of autism and harm.
Kennedy immediately asks the obvious, “So you are saying that these organizations claim that vaccines NEVER damage kids?”
Vargas is forced to backpedal:
“I don’t think anyone is saying they never have. There may be a child here [or there], but overall vaccines have saved millions and millions of lives.”
Vargas is demonstrating the lack of understanding the public has about the issue. How can anyone claim that vaccines have saved millions and millions of lives if proper prospective studies with matched unvaccinated controls have never been conducted?
Kennedy makes this abundantly clear in his response to Dr. Butt, who asks Kennedy this question:
“Eradication of chicken pox and polio in the U.S. and in many parts of the world is a result of regular vaccination. MMR [measles, mumps, rubella] and many diseases are preventable. There is little evidence of these diseases in the vaccinated population. Your vaccine stance is dangerous to the health and well-being of millions. Medical experts are deeply concerned about your message. How can we help you come to the side of science?”
Kennedy admits there is evidence that vaccines have reduced the risk of mortality and morbidity from the diseases they target. However, he argued, without long-term prospective studies around all-cause mortality/morbidity in vaccinated populations nobody — no matter how educated or how big an organization you represent, he said — can claim there is an overall benefit.
Kennedy’s answer to the question dismantles the issue to the very core, catching Dr. Butt off guard. His methodical response should have proven to the audience that the family medicine doctor has very little grasp of all the available evidence.
Dr. Butt clearly wasn’t aware of analyses like this one that concluded that a “Mass varicella vaccination is expected to cause a major epidemic of herpes zoster, affecting more than 50% of those aged 10-44 years at the introduction of vaccination.”
Should studies like this guide public policy in the U.S.? They certainly do in the U.K., where health officials do not recommend universal vaccinations against chickenpox for precisely the reason Kennedy states.
Of all the preventable diseases out there, why would Dr. Butt use chickenpox as an example of how Kennedy’s vaccine stance is dangerous to the health and well-being of millions? Could it be that a doctor with a microphone was unaware of the science?
Was Dr. Butt aware of the enormous tragedy caused by the DTP (diptheria, tetanus, pertussis) vaccine in Africa? After 30 years of observation, it was shown that children vaccinated with the DTP shot were dying of other causes at 10 times the rate of the unvaccinated. We would have never known about this if no one actually looked.
The devastation caused by the DTP vaccine is not limited to the continent of Africa. Kennedy informed the audience that the flurry of lawsuits against manufacturers of this vaccine led to the passing of the National Childhood Vaccine Injury Act of 1986, which has protected vaccine manufacturers from any liability.
As a concession to the public, this law also created the Vaccine Adverse Event Reporting System, or VAERS, to “protect” and warn the public of potential vaccine danger; a system that has been shown to underreport injuries as commonly as it gets ignored.
Though Kennedy did not discuss the MMR and polio vaccines, his point was clear: Unless proper, long-term, prelicensure placebo-controlled safety studies are done we cannot determine if more harm than good is being done.
Dr. Butt’s response to the likely damage caused by the varicella and DTP vaccines was all too predictable: “A person can take a medicine and then get involved in a motor vehicle accident.” In other words, correlation does not prove causation!
Dr. Butt has good intentions. He is also particularly skilled at picking the weakest examples to prove his point.
The issue with the varicella vaccine was the resulting increased risk of herpes zoster infection (shingles). The issue with the DTP vaccine was the increased risk of death from other prevalent diseases that proved to be more deadly for the kids who received the vaccine.
We are not talking about random traumatic injuries that have nothing to do with immune modulation.
Furthermore, was Dr. Butt aware that the “correlation does not equal causation” argument can be used to dismiss vaccine benefits as well?
This double standard is mindlessly applied by vaccine proponents. Trials don’t prove causation, only correlation. That goes for efficacy too. On what grounds can one say that a vaccine caused a decrease in the disease it targets while assuring us that it was only correlated with an increase in side effects?
Trials just measure the incidence of things in two (or more) groups of participants. It’s a mathematical comparison. No causation is ever proven.
Vargas took issue with Kennedy’s claim that not one vaccine on the childhood immunization schedule has been subjected to a prelicensured placebo-controlled trial.
Vargas: “Yes they have.”
Kennedy: “No.”
Vargas: “Yeah, they have!”
And later …
Vargas: “The FDA says, and in fact, on its website, you can clearly see vaccines go through three stages of testing against double-blind placebo. They already DO that testing.”
Kennedy: “Elizabeth, you can say that.”
Vargas: “I’m not saying that. The FDA is saying that.”
Kennedy: “The FDA is not saying that.”
Vargas: “Yes they do! They say that on their website!”
Kennedy: “They will not tell you that there’s a vaccine that has ever undergone a long-term placebo-controlled trial prior to licensing because it’s not true.”
The reason why this embarrassing (and mildly entertaining) spectacle is important to dissect is because of what it reveals about the stubbornness we have about being right. Did Vargas actually scour the FDA website prior to this public exchange?
She couldn’t have for the obvious reason that no such statement from them exists on their website as she maintained.
Why is she so sure that she is right? I would venture to say it is because someone whom she trusts more than Kennedy told her that.
But was she really listening to what Kennedy was saying? Kennedy demanded a citation from Dr. Anthony Fauci in a face-to-face meeting with him in 2016. Fauci couldn’t produce one but promised he would.
He never did — so Kennedy (and attorney Aaron Siri) sued him and the U.S. Department of Health and Human Services (HHS). After a year of litigation, they finally obtained a written statement from the HHS which still does not cite a single study but assures us that inert placebos are not required to demonstrate safety in childhood vaccines.
Of course, there is no reason Vargas should trust Kennedy if she has not visited the Children’s Health Defense website where the letter from the HHS is made available.
But at what point should she have paused and honestly asked herself about what she really knew and not just what she thought she did?
In this case, the spectacle arose not because Vargas was wrong, but because she was so sure she was right.
It’s also worthwhile to consider what was on the line for her, personally. Was she able to face the possibility that the vaccines we have been injecting into our own bodies and our children have never been tested against a placebo?
Her argumentative responses to Kennedy’s views, which he defended with several key citations off the top of his head, reflected the real impediments the public has toward seeing reality for what it is. What would it mean if Kennedy has been right all along?
As a veteran journalist for NewsNation and previously for Fox and A&E Networks, Vargas should have come prepared. Kennedy has previously made himself very clear that he is willing to change his mind. “Show me where I got it wrong.”
Kennedy asks Vargas to cite a single prelicensure, placebo-controlled vaccine study. She couldn’t because no one can. There aren’t any.
Kennedy pointed out the real issue: “We have a corrupt federal agency [FDA] that is lying to the AMA and all those agencies and all those doctors. But those agencies are controlled by Pharma. That is the problem.”
Without any studies to cite or any way to refute Kennedy’s damning allegations, Vargas chose to confront Kennedy with the fact that some of his family members disagree with his stance on vaccines.
Kennedy: “Does your family agree with everything that you say?”
Vargas: “Definitely not. You got me on that one.”
Madhava Setty, M.D. is senior science editor for The Defender.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Serious adverse events from Pfizer’s mRNA vaccine are not “rare”
Maryanne Demasi, reports | June 27, 2023
Drug regulators and public health agencies have saturated the airways with claims that serious harms following covid vaccination are “rare.”

But there has been very little scrutiny of that claim by the media, and I could not find an instance where international agencies actually quantified what they meant by the term “rare” or provided a scientific source.
The best evidence so far, has been a study published in one of vaccinology’s most prestigious journals, where independent researchers reanalysed the original trial data for the mRNA vaccines.
The authors, Fraiman et al, found that serious adverse events (SAEs) – i.e. adverse events that require hospitalisation – were elevated in the vaccine arm by an alarming rate – 1 additional SAE for every 556 people vaccinated with Pfizer’s mRNA vaccine.
According to a scale used by drug regulators, SAEs occurring at a rate of 1 in 556 is categorised as “uncommon,” but far more common than what the public has been told.

Therefore, I asked eight drug regulators and public health agencies to answer a simple question: what is the official calculated rate of SAEs believed to be caused by Pfizer’s mRNA vaccine, and what is the evidence?
The agencies were FDA, TGA, MHRA, HC, PEI, CDC, ECDC and EMA.
The outcome was startling.
Not a single agency could cite the SAE rate of Pfizer’s vaccine. Most directed me to pharmacovigilance data, which they all emphasised does not establish causation.
The Australian TGA, for example, referred me to the spontaneous reporting system but warned, “it is not possible to meaningfully use these data to calculate the true incidence of adverse events due to the limitations of spontaneous reporting systems.”
Both the German regulator (PEI) and European CDC referred me to the European Medicines Agency which, according to its own report, saw no increase at all in SAEs. “SAEs occurred at a low frequency in both vaccinated and the placebo group at 0.6%.”
The UK regulator MHRA went so far as to state it “does not make estimations of a serious adverse event (SAE) rate, or a rate for adverse reactions considered to be causally related for any medicinal product.”
The US FDA, on the other hand, did conceded that SAEs after mRNA vaccination have “indeed been higher than that of influenza vaccines,” but suggested it was justified because “the severity and impact of covid-19 on public health have been significantly higher than those of seasonal influenza.”
Despite analysing at the same dataset as Fraiman, the FDA said it “disagrees with the conclusions” of the Fraiman analysis. The agency did not give specifics on the areas of disagreement, nor did it provide its own rate of SAEs.
In response to the criticism, Joe Fraiman, emergency doctor and lead author on the reanalysis said, “To be honest, I’m not that surprised that agencies have not determined the rate of SAEs. Once these agencies approve a drug there’s no incentive for them to monitor harms.”
Fraiman said it’s hypocritical for health agencies to tell people that serious harms of the covid vaccines are rare, when they have not even determined the SAE rate themselves.
“It’s very dangerous not to be honest with the public,” said Fraiman, who recently called for the mRNA vaccines to be suspended.
“These noble lies may get people vaccinated in the short term but you’re creating decades or generations of distrust when it’s revealed that they have been misleading the public,” added Fraiman.
Dick Bijl, a physician and epidemiologist based in the Netherlands, agreed. “It goes to show how corrupted these agencies are. There is no transparency, especially since regulators are largely funded by the drug industry.”
Bijl said it’s vital to know the rate of SAEs for the vaccines. “You must be able to do a harm:benefit analysis, to allow people to give fully informed consent, especially in young people at low risk of serious covid or those who have natural immunity.”
Bijl said the mainstream media has allowed these agencies to make false claims about the safety of vaccines without interrogating the facts.
“The rise of alternative media is strongly related to the lies being told by the legacy media, which just repeats government narratives and industry marketing. In the Netherlands, there is a lot of discussion about the distrust in public messaging,” said Bijl.
Merck Knew Its Popular Asthma Drug Could Lead Kids to Commit Suicide, Lawsuits Allege
By Michael Nevradakis, Ph.D. | The Defender | June 27, 2023
Dozens of patients, including many children, died by suicide or suffered from neuropsychiatric problems after taking Singulair, Merck’s allergy and asthma medication, according to lawsuits that are finally proceeding, after decades of delays and legal challenges, Reuters reported.
Merck is accused of downplaying early evidence of Singulair’s impact on the brain. These claims “later faced intense scrutiny,” leading to “a raft of lawsuits alleging [Merck] knew … that the drug could impact the brain and that it minimized the potential for psychiatric problems in statements to regulators.”
Singulair, also known as montelukast, is available to adults and children as a medication for severe allergies and asthma. The drug “blocks chemicals, called leukotrienes, in the body,” according to Dr. Michelle Perro, a pediatrician. Leukotrienes “can be involved in the precipitation of asthma and can cause respiratory symptoms, as well as inflammation of the airways,” Perro told The Defender.
Numerous public comments about Singulair’s side effects were submitted in 2019, prior to the Sept. 27, 2019, joint meeting of the U.S. Food and Drug Administration’s (FDA) Pediatric and Drug Safety and Risk Management Advisory Committees charged with reviewing the drug’s safety.
Many of the comments were submitted by “vocal parents” of children adversely affected by Singulair.
Rolf Hazlehurst, senior staff attorney with Children’s Health Defense (CHD), told The Defender he “worked closely” with several of these parents.
The public comments, along with thousands of reports submitted over several years to the FDA Adverse Event Reporting System (FAERS) plus a 2015 research study finding that a “substantial amount” of Singulair entered the brain, forced the FDA to take action.
On March 4, 2020, the FDA required Singulair to carry a “black box” label — the FDA’s most serious warning, for “serious mental health side effects,” according to Drugwatch.
Black box warnings list “important side effect information surrounded by a thick black border and bold lettering to warn of permanent, serious or fatal side effects.”
In the case of Singulair, the label links the drug to “suicide, depression, aggression, agitation, suicidal thoughts and sleep disturbances.”
The black box label was at least two decades in coming, according to Hazlehurst, who said it “took over a decade’s worth of work by persistent parents, armed with overwhelming evidence of the serious neuropsychiatric side effects, urging the FDA to take action.”
According to Drugwatch, lawsuits now pending against Merck claim the drugmaker “knew or should have known before it started selling Singulair in 1998 that the drug could cause neuropsychiatric injuries during treatment and even after stopping.”
Dr. Liz Mumper, a pediatrician, said she has been “aware of the potential neuropsychiatric side effects of montelukast for many years,” adding that her patients “are instructed to stop the medicine if they notice a change in their mental health.”
“Over the years, parents have reported personality changes in their children, rapid changes in mood and irritability,” Mumper told The Defender. “Typically, these symptoms resolve once off montelukast.”
Since March 2020, when the FDA applied the black box warning to Singulair, numerous lawsuits have been filed against Merck. The lawsuits allege Merck designed “a defective drug,” in addition to claiming “negligence and failure to warn about the risk of mental problems,” according to Drugwatch.
A Reuters investigative report revealed the lawsuits also allege “that the company’s own early research indicated the drug could impact the brain but that Merck downplayed any risks in statements to regulators.”
The Reuters investigation states that plaintiffs faced a legal hurdle commonly used by Big Pharma — known as a “preemption defense” — based on a legal argument that federal law and federal regulations supersede state laws, including state product liability laws that traditionally served as the basis for lawsuits like those against Merck.
As a result, “companies increasingly argue that federally regulated products or services should be immune from lawsuits alleging state-law violations,” and plaintiffs “must often demonstrate that a company failed to disclose safety information to federal regulators — and that the information could have spurred new government restrictions or warnings before the alleged harm occurred.”
This has made it particularly difficult to sue manufacturers of generic versions of Singulair and other drugs, because generic drugmakers simply follow the primary manufacturer’s FDA-approved labeling, while the primary drugmaker can’t be sued by claimants if they or their family members took the generic version.
Perro told The Defender that a combination of an abrogation on the part of federal regulators, a lack of integrity on the part of drugmakers and complex legal maneuvering makes it difficult for doctors to prescribe safe treatments to their patients.
She said:
“A medical practitioner now needs to understand their patient, the illness, any prescribed medications, what Pharma reports about their drug, the real science behind the drug, and unfortunately, the legal doctrine of preemption, which is the principle based on federal law trumping state law.
“It is a dark time in medicine when the physician must question the integrity of what is written on the prescription pad.”
The FDA claims it has “diligently monitored reports of side effects possibly associated with montelukast, as well as communicated findings and taken regulatory action, when appropriate,” and that it “continues to monitor and investigate this important issue.”
Merck’s patent on Singulair expired in 2012, allowing generic drugmakers to begin producing and marketing the drug. Still, according to Reuters, Singulair “has provided Merck with about $50 billion in revenue.”
However, once Merck’s patent expired, “The number of patients prescribed the medicine climbed from about 7 million annually to more than 9 million” — with up to half of recipients age 16 or younger.
At least 82 suicides connected to Singular before FDA added black box warning
The Reuters investigation noted that “in the case of Singulair’s potentially deadly side effects, the FDA waited years, despite thousands of reported psychiatric problems, to require its most serious warning on the drug’s label.”
During this time, dozens of individuals taking Singulair committed suicide or faced other neuropsychiatric problems.
For instance, in 2017, 22-year-old Nicholas England, a Virginia resident, shot himself in the head less than two weeks after starting a generic version of the medication. He had no history of mental health problems — and his family had no legal recourse against Merck due to the preemption defense.
In 2007, a 15-year-old boy in New York committed suicide, 17 days after first taking Singulair. According to Reuters, this incident led Merck to propose — and the FDA to accept — an amendment to the drug’s label to add suicidal thinking and behavior to the product’s listed adverse events.
However, this adverse event “appeared in the middle of a list of more than three dozen side effects,” the Reuters investigation found. “Parent advocates argue the new label was grossly inadequate to warn of such a grave risk.”
“Neuropsychiatric side effects are listed in the documentation of potential side effects, but not always prominently,” Mumper told The Defender. And despite the new label, she said, parents searching for its package insert online will find older versions “without a prominent black box warning.”
According to Drugwatch, the change to Singulair’s label was made in August 2009, when the label was updated to also include other neuropsychiatric events including “postmarket cases of agitation, aggression, anxiousness, dream abnormalities and hallucinations, depression, insomnia, irritability, restlessness … and tremor.”
In 2008, the FDA said it was investigating “a possible association between the use of Singulair and behavior/mood changes, suicidality … and suicide,” Drugwatch reported.
In another example, the 3-year-old son of Jan Gilpin was prescribed Singulair for asthma in 2003. He “soon seemed withdrawn and sullen” and “started talking about death,” according to Reuters.
Gilpin initially did not suspect Singulair — until she discovered online posts by parents stating that their children were exhibiting similar behavior while on this medication. She pulled her son off Singular and soon “noticed he began to skip and laugh,” while his “obsessive thoughts about death disappeared after he quit the medicine.”
Indeed, “reports of related neuropsychiatric episodes piled up on internet forums and in the FDA’s early-warning detection system” starting in 1998, Reuters reported. Yet, by the time of England’s suicide in 2017, the FDA was still “reviewing” this data.
According to Reuters, in 2011, the FDA “rejected a petition from Gilpin and other parents seeking a black box warning, citing what it called insufficient evidence that the drug caused suicidal behavior.”
“Parents who argue Singulair endangered their children view the FDA’s 2020 decision to add a black box warning as vindication, but many still want to sue Merck for not acting sooner,” Reuters also reported.
In 2014, an FDA panel acknowledged that neuropsychiatric side effects among Singulair users were a “known safety issue,” but cited this reason and “feasibility concerns” in its decision not to order new studies, according to Reuters.
Yet, as reports of suicides continued to be filed — with 82 suicides linked to Singulair and its generic versions, including at least 31 involving people age 19 and younger, a new FDA advisory panel was convened in 2019.
According to Reuters, “agency staffers again said there was not enough evidence” to merit this. However, with Merck’s patent having expired, an FDA official told the advisory committee that the company may opt to pull Singulair from the market rather than fund expensive new studies to investigate the product’s safety.
This resulted in the March 2020 decision to add the black box label to Singulair.
‘Substantial amount’ of Singulair enters human brain
In its 2020 decision, the FDA cited independent research conducted in 2015 by cell biologist Julia Marschallinger and other researchers at Austria’s Institute of Molecular Regenerative Medicine.
They found that Singulair’s distribution into the brain was more significant than what was stated on the product label, which described its brain distribution as “minimal.”
Merck had claimed, in documents it submitted to FDA for the drug’s approval in 1998, that “only a trace amount” of the drug could be found in the brain and that its presence “declined over time.” Merck’s public marketing of the product later described side effects as “generally mild” and “similar to a sugar pill.”
However, Marschallinger’s team found that while Singulair’s presence decreased almost everywhere in the body within 24 hours after administration, the opposite was true in the brain, where “a substantial amount” of the drug was identified.
In its 1996 patent application for Singulair, Merck also claimed the drug could be used as a treatment for “cerebral spasms” — indicating “knowledge of the drug’s potential brain impacts.” Lawyers for plaintiffs filing Singulair lawsuits against Merck have cited this argument, as well as Marschallinger’s study.
The FDA has confirmed the study’s findings, acknowledging that claims regarding the declining presence of Singulair in all tissues “did not fully reflect the data.”
However, according to Reuters, the FDA also characterized findings of “a substantial amount” of the drug in the brain “a subjective characterization that is not necessarily incompatible with the ‘minimal’ descriptor in other contexts.”
“The FDA could have asked Merck to repeat the experiment or do it for an even longer period of time,” Marschallinger told Reuters. “It’s not hard to do.”
Perro said, “For those children who have been harmed by this drug,” due to the FDA’s 22-year delay in adding a black box warning, “there will not be any compensation because of pharmaceutical protection by our own government and liability shields.”
The FDA’s inaction has resulted in many deaths, Sue Peters, Ph.D., a CHD science fellow, told The Defender :
“The FDA has placed pharmaceutical profits over the safety and mental health of our children. It’s a never-ending cycle, with increased rates of chronic illness, like asthma, leading to pharmaceutical treatments which have not been properly safety-tested.
“These drugs put young people, with critical brain myelination continuing past 25 years of age, at risk of developing mental health disorders, leading to polypharmacy with psychiatric medications, and contributing to iatrogenic deaths as a leading cause of death in the U.S.”
Perro called for an overhaul of the FDA, telling The Defender :
“It is clear who our government — including the judicial system — is protecting. A solution to the lack of action by regulatory agencies? Overhaul.
“In the meantime, there are safer pharmaceutical alternatives for asthma in children. Not to mention, this is yet another reason to examine the root causes as to why so many children now have asthma, and address the real culprits, such as air pollution.”
For Mumper, a new approach to treating ailments such as asthma is needed. “Although montelukast is a valuable medication in my toolbox for treating allergies, the prescription should come after other measures, including working on gut health,” she said.
Similarly, Peters called for a “careful analysis” of the role of drugs in the treatment of common disorders and their role in precipitating mental health disorders and even deaths. She told The Defender :
“The tragic increase in the rate of mental health disorders in children in the United States, requires careful analysis of the role of iatrogenic death.
“Failing to consider the role of pharmaceutical drugs and medical treatments in the development of mental health disorders in children, has led to the loss of valuable research time, wasted research dollars, and ultimately the loss of life. Clearly, our current system is broken.”
Preemption defense lets Big Pharma avoid directly addressing safety claims
According to the Reuters investigative report, most of the Singulair lawsuits pending against Merck are still in their early stages.
Drugwatch reported that, as of May 16, “there have been no scheduled trials or court-approved global settlement in Singulair litigation.” Many of the suits against Merck were filed in New Jersey, where in January 2022, they were consolidated into multicounty litigation in the Superior Court of New Jersey Law Division: Atlantic County.
And in April, U.S. District Judge Timothy S. Hillman in Massachusetts denied Merck’s motion to dismiss a Singulair lawsuit “for lack of personal jurisdiction,” Drugwatch reported. Judge Hillman argued Merck manufactured, marketed and sold the drug in the state and allowed the case to continue.
Two U.S. Supreme Court rulings in 2011 and 2013 strengthened the preemption defense.
In Pliva, Inc. v. Mensing (2011), the Supreme Court held that state law requiring “generic drug manufacturers to provide adequate warning labels was preempted where federal law required manufacturers to use the same labels as their brand-name counterparts.”
And in Mutual Pharmaceutical Co. v. Bartlett (2013), the Supreme Court held that design-defect claims questioning the adequacy of a drug’s warnings under state law are preempted by the Federal Food, Drug, and Cosmetic Act and the Pliva v. Mensing ruling.
According to Reuters, the preemption doctrine rests on the U.S. Constitution’s Supremacy Clause, which states that the Constitution and federal law take precedence over state laws and state constitutions.
As a result, “Preemption defenses often deliver companies a swift procedural win, allowing them to avoid addressing the substance of plaintiffs’ allegations.”
While the defense has been used across multiple industries, it “has had a particularly profound impact in the pharmaceutical industry,” particularly as FDA data cited by Reuters indicates that generic drugs account for 91% of U.S. prescriptions.
Reuters, in its review of 257 U.S. Supreme Court and federal appeals court rulings since 2001, found that “judges ruled two-thirds of the time to weaken or kill lawsuits alleging deaths or injuries caused by corporate negligence or defective products.”
Moreover, “The number of potential lawsuits that were never filed” serves as “Another industry benefit” that “can’t be quantified,” according to Reuters.
Preemption defenses became a centerpiece of the George W. Bush administration — and FDA policy under his presidency, Reuters reports. This was part of the Bush campaign’s promise to address what it described as “frivolous” lawsuits.
Daniel Troy, the FDA’s chief counsel under the Bush administration, “interpreted preemption to mean that courts can’t undermine federal regulators based on alleged state-law violations,” Reuters reported, adding that he “aimed to make that argument in high-profile lawsuits” and briefed drug industry lawyers on the strategy in 2003.
Troy — who is now a pharmaceutical industry lawyer — told Reuters, “If you believe in a strong FDA, we can’t have state courts, especially juries, second-guessing and undercutting the FDA’s judgments.”
Hazlehurst told The Defender Troy’s argument is the same one used by Wyeth (Pfizer) before the Supreme Court in Bruesewitz v. Wyeth (2011). The Supreme Court’s decision in this case prohibited design defect lawsuits against vaccine manufacturers.
The U.S. Department of Health and Human Services, the parent agency of the FDA and the Centers for Disease Control and Prevention, supported Wyeth’s 2011 argument.
Similarly, Mumper told The Defender that pharmaceutical companies “have a history of avoiding liability through various legislative protection,” including the preemption defense and the National Childhood Vaccine Injury Act of 1986.
And in 2006, “The FDA formally changed its view of preemption in a 2006 regulation, stating the agency now believed that FDA labeling approval ‘preempts conflicting or contrary State law,’” Reuters reported.
Hazlehurst told The Defender, “CHD is proud to have played a role in advocating and assisting these parents on the journey to hold Merck accountable,” but “one thing rings loud and clear: the FDA is a captured agency, and this is a fundamental problem.”
Some parents have questioned whether the black box warning for Singulair was enough to save lives, citing the damage already done, continued legal obstacles, and Merck’s strong marketing campaign for the drug.
“Due to tremendous financial conflicts of interest, the pharmaceutical industry has tremendous influence over the FDA,” Hazlehurst said. “As a result, the FDA protects the pharmaceutical industry first and people second — this story is just one example.”
He added: “One must wonder, how many lives could have been spared if the FDA had timely done its job of properly investigating and regulating the pharmaceutical industry?”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Lethal Drones at the U.S.-Mexico Border?
By Laurie Calhoun | The Libertarian Institute | June 27, 2023
Fentanyl has caused many overdose deaths in recent years, and much of it has entered the United States through Mexico. A number of politicians have thrown their support behind a proposal to officially label narcotics traffickers based in Mexico as “terrorists.” Not all of the Republican lawmakers who support this idea have openly embraced the use of lethal drones to eliminate such persons, but that would be the inevitable policy implication of such labeling, given the wording of anti-terrorist legislation. At least one presidential candidate, Vivek Ramaswamy, has said the quiet part out loud: lethal drones should be deployed at the U.S.-Mexico border. There can be little doubt that the many other politicians declaring “war” on the cartels are well aware that lethal force will be used once the fentanyl producers have been designated terrorists, and the current tool of choice among self-styled smart warriors is the unmanned combat aerial vehicle (UCAV) or lethal drone.
The superficially plausible assumption behind this proposal is that if the flow of fentanyl is stanched, then the overdose deaths will subside. But the prospect of deploying lethal drones at the U.S.-Mexico border is a simplistic plan for addressing a very complicated problem. There are dozens of reasons for opposing this approach, on moral, legal, cultural, and geopolitical grounds. Most of those arguments, however, will fall on deaf ears and certainly not deter politicians from plundering ahead, expanding the domain of the killing machine once again, having been, in at least some cases, sincerely persuaded that they are acting not to enrich death industry profiteers but to defend the people of the United States from foreign enemies. The only way to prevent the deployment of lethal drones at the border from happening will be persuasively to demonstrate that the plan could never succeed, on purely tactical grounds. Two fatal flaws virtually guarantee that, if implemented, the plan would not have the desired effect, as can be seen through a consideration of the origins of the opioid crisis and the cross-border use of lethal drones in the Middle East.
The tragic drug overdoses of hundreds of thousands of people in the United States in recent years have had many causal factors, but the prime mover, which initiated the whole ugly mess, was the promiscuous overprescription of narcotics by doctors. Led by Purdue Pharma, drug industry giants aggressively marketed their opioid products as safe to use by anyone for anything, all blessed by the FDA (Food and Drug Administration), which permitted a package insert to be included in boxes of Oxycontin indicating that the time-release format made the product safe to use without concerns about addiction or abuse. This was a classic case of the commandeering by profiteers of a government agency established in order to protect citizens but used instead to promote the interests of those who come to enrich themselves through decisively shaping government policies. (An even more obvious case has been the capture of the Department of Defense by individuals beholden to companies in military industry, such as former Raytheon board member and current secretary of defense, Lloyd Austin.) Because most members of the populace believe that the FDA is their protector (again, just as they believe in the basic goodness of the Pentagon), many of them were taken in by this pharmaceutical industry scheme.
Doctors, too, were remarkably persuaded to believe that they could and should prescribe narcotics liberally, and patients consequently came to believe that they could and should empty their large amber vials. Preposterous though it may seem in retrospect, the pharmaceutical industry undertook aggressive public media campaigns to persuade politicians and their constituents that the nation was in the throes of a “pain epidemic,” for which narcotics were the solution. When clinicians expressed concern that their patients might be turning into addicts, they were tutored by “experts” tethered to the industry that the observed condition was in fact “pseudo-addiction,” the remedy for which would be even higher doses of narcotic drugs.
Prescription narcotics were oversupplied to perfectly ordinary patients suffering from even minor bouts of acute pain, who eventually discovered that they had become dependent on and were unable to function without the drugs. The opiates to which they found themselves hopelessly addicted were prescribed legally to them by physicians whom they had trusted as having their best interests in mind. In this way, people from all walks of life, including injured high school athletes who had never even been recreational drug users, were transformed into junkies.
Some of the working people who were prescribed narcotics for their various, often minor, ailments lost their jobs and, with them, their health insurance. During the early years of what would become the opioid overdose epidemic, addicts and others supported themselves by selling pills they acquired through “doctor shopping”. As a direct consequence of the pharmaceutical industry-created demand for more and more narcotics, mercenary but board-certified doctors teamed up with unscrupulous business persons to open “pain clinics,” which swiftly became places where addicts convened and collected drugs to be diverted for illegal sales. Massive quantities of narcotics were distributed by the now notorious pain clinics. Many of those drugs were sold on the streets for recreational use, thereby creating even more addicts. (For a concise and compelling summary of the government’s indisputable role in this tragic story, see director Alex Gibney’s two-part HBO series, The Crime of the Century [2021].)
Once the pain clinics were shut down, more and more addicts turned to the streets for supplies of their needed fix of whatever was available: diverted prescription pills, heroin, morphine, and most notoriously of all, fentanyl. Because it is so potent (about fifty times more than comparable drugs) and also cheap to produce, fentanyl was mixed or even used to replace other narcotics by unscrupulous dealers. The increased demand by addicts for opioids and the use by dealers of fentanyl to cut or replace heroin and other less dangerous surrogates has resulted in the deaths of many drug users who simply did not know what they were ingesting. At least some of the fentanyl deaths reported have been of non-addicts whose supplies of other drugs, too, were tainted with the highly concentrated and toxic substance.
Can eliminating supplies of fentanyl coming over the border to the United States from Mexico solve this problem? Will summarily executing suspected producers and distributors of fentanyl help to stem the tide of overdose deaths? Even setting aside concerns about procedural justice, the proposal to assassinate suspected drug dealers fails to take into account the etiology of the opioid crisis and, most importantly of all, the nature of drug dependency and the desperation of junkies to acquire the substances to which they are not only psychologically but physically addicted.
The opioid addiction crisis was not caused but seized upon opportunistically by Mexican drug cartels. The very fact that the fentanyl business has become so lucrative for illicit drug purveyors itself illustrates that there is a strong market demand for narcotics, whether natural or synthetic. If addicts cannot acquire cheap black tar heroin and/or fentanyl from Mexican producers and their network of distributors throughout the United States, then they will seek out and locate other sources of the drugs which their bodies crave. No one denies that the opioid addiction crisis is grave. But whacking drug dealers at the U.S.-Mexico border will simply produce more drug dealers, in different places.
We’ve seen a version of this story before, mutatis mutandis. What, after all, happened when war resisters transformed into jihadists on the ground in Iraq and Afghanistan were targeted by missiles? First, there was the hydra problem: targeting suspected militants often resulted in the deaths of innocent civilians, thus fueling the very anger requisite to the recruitment by Al Qaeda and other groups of new converts to violent retaliation. Other factors, beyond the illegal invasions themselves, contributed to the increased number of radical Islamist fighters as well, including the use of torture by the occupiers, along with a variety of other incompetent policies, which led to a general degradation in the quality of life for the inhabitants of occupied territories.
Second, and directly relevant to the proposed plan to execute suspects at the U.S.-Mexico border, as the ranks of the factional fighters increased, some of them fled to other parts of the Middle East to regroup and avoid being killed by occupying forces. The comportment of the dissidents who fled war zones was entirely rational. They believed that they were right, and they naturally wanted to succeed in their missions to eject the invaders from their lands, so they relocated and strategized about how to defeat what they had come to believe was “the evil enemy.” The lethal drones then followed the factional fighters to Pakistan, Syria, Somalia, Mali, Yemen, and beyond. As a result of this lethal creep, civilians in several different countries are now under constant threat of death by missiles launched by drones.
The Mexican drug cartels are not at this point engaged in a war with the U.S. military, but recalling how and why the “Global War on Terror” spread throughout the Middle East, we must soberly consider what is likely to ensue, should lethal drones be unleashed at the border as a way of curtailing the flow of fentanyl. It is quite plausible, given what happened in the Global War on Terror, that the more missiles which are fired on the U.S.-Mexico border, the fewer people there will be who choose to continue to live there. This should be a matter of common sense even to people ignorant of the details of the disastrous Global War on Terror, and yet the politicians pushing for a new “War on Drugs” somehow have not thought through the likely consequences of their plan, preferring instead to follow their usual “act tough” approach to garner political support for superficially appealing policies. No matter that Plan Colombia, intended to reduce the flow of cocaine to the United States, had the opposite effect and led to the militarization of drug traffickers throughout region, not the renunciation of their business activities. Just as the Global War on Terror has been all but forgotten by politicians keen to “move on” rather than acknowledge their role in creating humanitarian catastrophe throughout the Middle East, Plan Colombia has been memory-holed for the very same reason. Both were abject policy failures. Mistakes were made. Stuff happens. Nothing to see here; time to move on—to Ukraine!
Following the same logic used by both the radical jihadists in Afghanistan, and the cocaine cartels in Colombia, targeted groups at the U.S.-Mexico border who wish to continue to ply their trade, producing and distributing fentanyl and other drugs to the people of the United States, may well set up shop somewhere else, in places where they will be safe from the specter of lethal drones hovering above their heads. If fentanyl is easy to produce in Mexico, it is no less easy to produce wherever the same raw materials can be found. We can expect, then, that if lethal drones are used at the border, fentanyl production and distribution will migrate as a result. Some of the producers will move south, some may relocate to Canada, but it seems far more likely that many of them will opt to use the distribution apparatus they already have in place in the United States to begin or increase synthetic drug production in the very country where fentanyl is being sold.
The illicit drug purveyors may well reason that they will be safer moving their businesses to the United States, rather than further south in Mexico or other parts of Latin America, or up north to Canada. They may find it difficult to believe that the U.S. government would deploy lethal drones in the homeland, thereby directly endangering U.S. citizens. That assumption, however, is false. We already have precedents for such deployments abroad, and even the use of robotic means of homicide within the homeland against U.S. citizens.
The case of Anwar al-Awlaki, a U.S. citizen who was summarily executed by the U.S. government in Yemen without ever having been indicted for a crime, on the basis of evidence never made public to his fellow citizens that he was a “terrorist,” illustrates that the drone killers are ready and willing to inflict capital punishment upon citizens at the executive’s decree. Abdulrahman al-Awlaki, the sixteen-year-old son of Anwar al-Awlaki, was also destroyed, along with a group of his teenage friends, by a missile launched from a drone in Yemen, about two weeks after his father was eliminated, and shortly after the boy had turned sixteen, making him a “military-age male”. To this day, we do not know whether the son was killed because military analysts worried that he would be radicalized by his father’s assassination, for the U.S. government has never explained what happened on October 14, 2011.
It is possible, albeit implausible (given the government’s silence on the matter), that the drone strike which ended Abdulrahman’s life was a mistake, an incredible coincidence that the younger al-Awlaki happened to find himself at the receiving end of a missile intended for somebody else. But the case of U.S. citizen Warren Weinstein, who had been taken prisoner (along with an Italian, Giovanni Lo Porto) by a group of suspected Al Qaeda members, and was also destroyed by a lethal drone, illustrates that, in pursuing their targets, the technokillers are ready and willing to risk harming U.S. citizens not even suspected of criminal activity.
Lest anyone suppose that the U.S. government would draw the line with citizen suspects located abroad, it is important to recognize that the presumption against the use of intentional homicide against citizens has been significantly weakened in the homeland as well, arguably as a result of the U.S. military’s “shoot first, suppress questions later” conduct abroad everywhere on display throughout the Global War on Terror. That homicide should be used to resolve conflict has been normalized in the minds of not only military and political elites but also every random mass shooter who emerges out of nowhere to annihilate a group of people as a way of expressing his discontent. When Micah Xavier Johnson, the Dallas cop killer, was blown up on July 8, 2016, using a robotic device at the behest of David O’Neal Brown, the chief of the Dallas police, nearly no one questioned the wisdom of the decision, though it would have been a simple matter to load the robot with incapacitating sedatives instead. Both of these African American men had been indoctrinated to believe that the way to resolve conflict is to obliterate human beings. Johnson, a military veteran apparently suffering from PTSD, claimed that he felt the need to kill Dallas cops as a way of protesting their killing of innocent black men.
Given these precedents, it seems likely that once lethal drones are deployed in the latest doomed-to-fail War on Drugs, the “War on Fentanyl,” they will be used not only in Mexico, but also in the United States as fentanyl production migrates to the homeland along with those fleeing the missiles being fired near the border. In the face of the overdose epidemic, politicians, goaded by both angry and mourning constituents, feel the need to act, and they will likely be supported by many in the populace in their quest to send out lethal drones—until, that is, innocent family members and neighbors begin to be incinerated in the homeland. At that point, perhaps the nation will finally have its long overdue debate about the policy of summarily executing suspects and the labeling as “collateral damage” of any innocent person unlucky enough to be located within the radius of a missile’s effects. But revisiting the immorality and illegality of killing thousands of unarmed brown-skinned young men in the prime of their lives abroad, on the basis of sketchy evidence which would never hold up in a court of law, while perhaps salubrious for future foreign policy, will have no effect whatsoever on the overdose epidemic.
The only truly effective solution to the opioid crisis, given the manifest failure of both the War on Drugs and the Prohibition, will be to legalize all drugs, making it possible for addicts and recreational drug users alike to buy what they need or want, and to know what they are actually getting. Anyone who wishes to liberate himself from the chains of addiction and return to a semblance of normal life should be assisted in that endeavor. Every addict has a story, and rather than criminalizing all of them, we would do well to take seriously the genesis of the opioid crisis in the United States. Many well-meaning patients, leading perfectly ordinary, noncriminal lives, ended up as junkies because they trusted their doctors who, in turn, trusted the pharma-coopted FDA. To those who worry that legalizing drugs will create even more junkies, there is a ready-made, highly visible anti-narcotics abuse campaign currently underway in every major city in the United States. No rational person would freely choose to wind up in the sorry state of the zombies currently haunting our streets. Rather than pinning up posters of fried eggs captioned “Your brain on drugs,” parents need only to take their children to such scenes to dissuade them from making the mistakes which led to the creation of what appear now to be mere vestiges of human beings.
Unfortunately, instead of viewing the opioid crisis as the humanitarian disaster that it is, some of the very politicians who culpably condoned industry malfeasance for years by refusing to acknowledge its root cause—pharmaceutical industry greed and our captured federal agencies—have decided that the suppliers of fentanyl from Mexico are the latest “bad guys” who must be eradicated from the face of the earth. Stigmatizing drug purveyors as “terrorists” not only will not effectively address the overdose epidemic, but it will further undermine our already crumbling republic. If the use of lethal force against suspected drug dealers is undertaken at the border, it will only be a matter of time before the presumption of innocence in the homeland is inverted into a presumption of guilt, just as occurred in the thousands of drone strikes targeting suspects on the basis of hearsay and circumstantial evidence throughout the Global War on Terror abroad.
Laurie Calhoun is the Senior Fellow for The Libertarian Institute. She is the author of We Kill Because We Can: From Soldiering to Assassination in the Drone Age, War and Delusion: A Critical Examination, Theodicy: A Metaphilosophical Investigation, You Can Leave, Laminated Souls, and Philosophy Unmasked: A Skeptic’s Critique, in addition to many essays and book chapters. Questioning the COVID Company Line: Critical Thinking in Hysterical Times will be published by the Libertarian Institute in 2023.
FDA Approves 2 New Diabetes Drugs for Kids — Critic Says Clinical Trial Sample Was ‘Shockingly Low’
By Suzanne Burdick, Ph.D. | The Defender | June 23, 2023
The U.S. Food and Drug Administration (FDA) this week approved two drugs to treat Type 2 diabetes for children ages 10 and up, “as additions to diet and exercise,” the agency said.
The drugs — Jardiance (empagliflozin) and Synjardy (empagliflozin and metformin hydrochloride) — previously were approved for adults with Type 2 diabetes to improve blood sugar control.
They join metformin, approved in 2000 to treat Type 2 diabetes in children.
“Compared to adults, children with Type 2 diabetes have limited treatment options, even though the disease and symptom onset generally progress more rapidly in children,” said Michelle Carey, M.D., MPH, associate director for therapeutic review for the Division of Diabetes, Lipid Disorders, and Obesity in the FDA’s Center for Drug Evaluation and Research.
But critics like pediatrician Dr. Elizabeth Mumper said the agency’s action ignores the root causes of Type 2 diabetes in children while generating profits for pharmaceutical companies:
“Rather than doing the hard work of preventing chronic diseases by cleaning up multiple environmental sources of harm to children, we allow the pharmaceutical industry to spend millions to develop drugs that do not address root causes of conditions like diabetes but do create lifelong medicine customers.”
Mumper, the former medical director of the Autism Research Institute, said “a pill for every ill” is “not a good strategy for pediatric care.”
Type 2 diabetes used to be called “adult-onset diabetes” — but now we are seeing it in younger and younger ages, Mumper told The Defender. In her state of Virginia, 31% of children are overweight or obese, she said.
“This is a clear risk factor for insulin resistance progressing to Type 2 diabetes,” Mumper said, adding:
“We are redefining normal by assuming Type 2 diabetes is a reasonable condition in children to treat with medicine instead of attacking the root causes of this ever-increasing chronic condition.
“We continue to allow Big Food to sell food-like products which are devoid of nutritional value and filled with sugar and bad fats that are addicting and proinflammatory.”
‘System is rigged for Big Food and Big Pharma, with kids … as the losers’
Nina Teicholz, author, science journalist and founder of The Nutrition Coalition — a “non-profit, non-partisan educational organization that aims to improve health in America by ensuring that the public receives evidence-based nutritional advice” — also emphasized the importance of diet in successfully preventing and managing Type 2 diabetes.
Commenting on the FDA’s new drug approval, she said, “This is another Pharma victory, promoting drugs while ignoring diet,” adding:
“The system is rigged for Big Food and Big Pharma, with kids, getting fatter and sicker, as the losers.”
We’ve known for more than a decade that people can safely reverse their Type 2 diabetes through diet alone — “within a matter of just weeks,” Teicholz said. “But multiple government agencies ignore this lifesaving science while the FDA approves drugs instead.”
Adult participants in a 2017 peer-reviewed study who used a ketogenic diet to manage their blood sugar levels reported a 1.0% reduction in their hemoglobin A1c — while reducing their medications — and were still sustaining that reduction one year later, Teicholz said.
In contrast, the FDA safety and efficacy trial of empagliflozin — the active ingredient in the two newly approved products — showed the drug reduced the recipients’ hemoglobin A1c by 0.2% in 26 weeks.
According to the authors of a study released Thursday:
“Type 2 diabetes, which makes up the bulk of diabetes cases, is largely preventable and, in some cases, potentially reversible if identified and managed early in the disease course. However, all evidence indicates that diabetes prevalence is increasing worldwide, primarily due to a rise in obesity caused by multiple factors.”
The study, published in The Lancet, projected the number of adults with Type 2 diabetes will more than double — to 1.3 billion — by 2050.
‘Shockingly low’ clinical trial sample size makes it impossible to assess adverse events
Commenting on the FDA’s safety and efficacy trial for the drugs, Brian Hooker, Ph.D., P.E., senior director of science and research for Children’s Health Defense, told The Defender :
“The sample size for this clinical trial is shockingly low. Given that 157 patients were split into three separate treatment groups, it was impossible to properly assess adverse events from the drug.
“I would expect that the trial be at least 10 times larger with a longer period of follow-up than 26 weeks, given that these children would be on the drug indefinitely.”
According to the product’s website, Jardiance can have serious side effects, including increased ketones in blood or urine — which may be accompanied by nausea, vomiting, abdominal pain, tiredness and breathing difficulty, allergic reactions, dehydration, serious urinary tract infections, yeast infections, low blood sugar and necrotizing fasciitis.
Necrotizing fasciitis is “a rare but serious bacterial infection that causes damage to the tissue under the skin in the area between and around your anus and genitals (perineum),” the company said.
Synjardy listed the same possible side effects, plus a possible deficiency in vitamin B12 caused by using metformin for long periods of time.
The drugs are manufactured by insulin producer Eli Lilly and its partner Boehringer Ingelheim.
Eli Lilly’s revenue for the quarter ending March 31 was $6.960 billion.
The pharmaceutical industry in 2022 funded about 75% of the FDA’s drug division, The New York Times reported.
Meanwhile, the FDA said that based on the results of a “SEARCH for Diabetes in Youth” study involving more than 27,000 youth, the incidence of Type 2 diabetes in children increased by 4.8% per year from 2002 to 2015 and is expected to continue increasing.
The agency did not comment on why researchers believe the rate of Type 2 diabetes in kids is expected to rise but noted:
“As of 2017, there were approximately 28,000 cases of Type 2 diabetes in children in the U.S.
“By 2060, if current trends continue, that number is predicted to be approximately 220,000, with the majority of cases occurring in minority racial and ethnic groups such as Non-Hispanic Blacks and Hispanics.”
Additionally, the FDA last year approved the first drug designed to delay the onset of Type 1 diabetes for children as young as 8 years old.
Suzanne Burdick, Ph.D., is a reporter and researcher for The Defender based in Fairfield, Iowa. She holds a Ph.D. in Communication Studies from the University of Texas at Austin (2021), and a master’s degree in communication and leadership from Gonzaga University (2015). Her scholarship has been published in Health Communication. She has taught at various academic institutions in the United States and is fluent in Spanish.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
FDA responds to negative efficacy of variant boosters with another variant booster
By Daniel Horowitz – conservative review – June 21, 2023
The human experimentation of Operation Warp Speed was not an anomaly; it is the new normal, and the FDA is just getting started. The agency is now allowing the COVID vaccine manufacturers to change the formulation of their shots to continue to chase variants, themselves created by antigenic drift of the shots. And they continue to do so based on nothing more than measuring antibody titer levels. No human clinical trials necessary! Except, studies now show, and reality confirms, the more they chase variants, the more they create negative efficacy against the existing variant, thereby engendering a “need” for another formulation.
What was the response of the FDA to the increasing news of cataclysmic injuries and negative efficacy of the COVID shots for variants that are no longer dangerous? Last Thursday, the FDA’s VRBPAC unanimously approved a fall booster, advising Pfizer, Moderna, and Novavax to update their formulations for the so-called XBB.1.5 Omicron variant. So, officials pre-emptively approved a shot that doesn’t exist based on antibody level testing without human trials – all for a variant that not only is not dangerous but will actually be extinct by the time this poison reaches the market, just as they did with the bivalent formulation for the BA.4 and BA.4 variants.
To this day, the bivalent shot is the only one available, and according to the CDC, that variant doesn’t even exist! It is true that very few people are dumb enough to get this shot, but what they are trying to do is create an endemic schedule of COVID shots to time perfectly with the flu shots in the fall. They have already groomed people over the generation to “get their flu shot” every fall. So now the pharmacies will be waiting with the COVID needle to complete their seasonal updates.
So, what happens when you keep tricking the body to respond to a virus for strains that no longer exist? As the FDA approved these shots, the agency already had the peer-reviewed Cleveland Clinic study showing negative efficacy of the original COVID shots. Just days before this meeting, the Cleveland Clinic came out with a preprint showing negative efficacy for the bivalent booster shots too.
The study contrasted 11,990 employees of this venerable institution who chose to be “up to date” with the bivalent boosters compared to 36,344 employees who were “not up to date” and tracked their outcomes. It turns out that after about three and a half months, you were about 25% more likely to get COVID after having gotten the boosters as compared to the control group.

After adjusting for confounding factors between the groups, the study authors actually found a 33% rate of negative efficacy!
“This study’s findings question the wisdom of promoting the idea that every person needs to be ‘up-to-date’ on COVID-19 vaccination, as currently defined, at this time,” conclude the Cleveland Clinic researchers. They also observe, “It should be pointed out that there is not a single study that has shown that the COVID-19 bivalent vaccine protects against severe disease or death caused by the XBB lineages of the Omicron variant.”
The push for boosters comes at a time when more evidence proves a strong correlation between excess deaths and the vaccine take-up. A letter published in a peer-reviewed journal of Medicine and Clinical Science shows that Japan and Germany, two highly vaccinated countries, experienced sharp excess deaths coinciding with the vaccine take-up. They found very little excess death during the pandemic months before the vaccine was rolled out.
“It should be investigated to what extent the about 5%-10% highly significantly increased mortalities in Germany and Japan in 2021 and 2022 might be due to the pandemic countermeasures, including the vaccinations with their possibly underestimated immediate or protracted side effects,” concluded the researchers from Japan and Germany.
“From this point of view, it seems possible that a high vaccination rate has contributed to an increased all-cause mortality in some countries.”
The twisted irony is that, according to the CDC’s variant tracker, XBB.1.5 has gone from 80% of cases to less than 40% of cases in just a few months. It will clearly be obsolete by the fall. None of this was discussed at the FDA hearing. Of course, nothing about Pfizer’s own document showing five million cumulative reports of adverse events affecting every organ system was ever discussed. Hence, we have record injuries, negative efficacy, long-term immune imprinting causing the body to constantly respond inappropriately to wrong strains of the virus – all for a virus that is no longer deadly and for a population that has already gotten the virus!
That’s not just a lousy cost-benefit analysis; that is premeditated murder against the American people. What is the GOP plan to stop this? Or do Republicans even care? How can they continue to fund more COVID shots in the HHS appropriations bill, much less the broader FDA/CDC scheme to create new dangerous shots at warp speed?
Just how callously does the FDA regard human life? After its own VAERS system exploded with every adverse event imaginable, an outcome we now know officials anticipated, to this day they have not followed up on those safety signals. For example, according to the Informed Consent Action Network, the Standard Operating Procedures and Policies document for the FDA’s Vaccine Safety Team requires that its staff members identify VAERS adverse event reports that “need a rapid response and complex coordination,” after which they are supposed to “immediately” inform certain FDA management, who then alert other sub-agencies. Did that occur?
Well, more than a year after the ICAN’s record request, the agency responded, “A search of our records did not locate any documents responsive to your request.”
Where is the action from the House GOP? Why are they still only investigating the shutdown of schools in the past, but not the ongoing, premediated unleashing of deadly products on the American people?
From Florida’s Surgeon General, a devastating indictment of the vaccine and its pushers
By Neville Hodgkinson | TCW Defending Freedom | June 22, 2023
When it comes to error correction, the USA’s 50 sovereign states offer more opportunity for an authoritative challenge to the misuse of power than we enjoy in the UK. Dr Joseph Ladapo, the Florida Surgeon General, has made public a letter excoriating federal health officials over their promotion of the mRNA Covid vaccines. The government, he said, ‘has relentlessly forced a premature vaccine into the arms of the American people with little or no concern for the adverse ramifications’.
The letter was to Drs Robert Califf, head of the Food and Drug Administration, and Rochelle Walensky, director of the Centers for Disease Control and Prevention. Lapado wrote: ‘Your ongoing decision to ignore many of the risks associated with mRNA Covid-19 vaccines, alongside your efforts to manipulate the public into thinking they are harmless, have resulted in deep distrust in the American health care system.’
As reported here earlier this year, senior American scientists have called for a ‘bipartisan, scientifically minded Covid-19 commission so the public health disaster of the past three years is not repeated’. They face an uphill struggle in achieving that aim, but Ladapo’s no-holds-barred letter means that at least some of Florida’s 22.6million citizens have a chance of knowing the jabs are not ‘safe and effective’, as the British public are constantly being told.
Ladapo would surely have been less forthright if Ron DeSantis, Florida’s Republican governor and a possible future US president, were not also on the warpath over the Biden administration’s handling of the pandemic. The Florida Supreme Court has approved DeSantis’s request to convene a grand jury to investigate ‘wrongdoings’ associated with the vaccines.
But DeSantis is not alone. The Texas Attorney General has launched an investigation into whether Pfizer, Moderna and Johnson & Johnson, the companies producing the jabs, misrepresented their safety and efficacy and manipulated trial data. The investigation could open the door to lawsuits by people injured by the mRNA products.
Meanwhile, what hope of redress do Britons have, not just for vaccine damage but for the lives shattered by cruel and unprecedented lockdowns?
The public inquiry led by Baroness Hallett looks likely to be worse than useless, as Laura Dodsworth, author of the best-selling A State of Fear: How the UK Government Weaponised Fear During the Covid-19 Pandemic, has described.
It is in ‘the wise and noble tradition of the great British public inquiry’, Rod Liddle commented in the Sunday Times last weekend. That is, keep the public away from it for as long as possible, and say nothing useful or meaningful unless ‘at least 20 years after whatever it is that they are inquiring about, at which point most of the relevant people are stiff as a stoat’.
The headline on Liddle’s article declared: ‘The data is clear: lockdowns are useless. But you won’t hear that from the inquiry.’
Sadly, neither the Sunday Times nor its daily stablemate, nor just about any of the mainstream media in the UK, have yet ventured into questioning the ‘safe and effective’ narrative about the vaccines. So let’s look at what Ladapo, who as state surgeon general can hardly be dismissed as a conspiracy theorist, has told the American public.
‘Data are unequivocal,’ Ladapo wrote. ‘After the Covid-19 vaccine rollout, the Vaccine Adverse Events Reporting System (VAERS) reporting increased by 1,700 per cent, including a 4,400 per cent increase in life-threatening conditions.
‘Dismissing this pronounced increase as being solely due to reporting trends is a callous denial of corroborating scientific evidence also pointing to increased risk and a poor safety profile. It also fails to explain the disproportionate increase in life-threatening adverse events for the mRNA vaccines compared to all adverse events.
‘Based on the CDC’s own data, rates of incapacitation after mRNA vaccination far surpass other vaccines.’
Ladapo cited a recent study which found an excess risk of serious adverse events ‘of special interest’ for 1 in 550 people after mRNA vaccination. He wrote: ‘As you are aware, this is extraordinarily high for a vaccine. In comparison, the risk of serious adverse events after influenza vaccination is much lower. For you to claim that serious adverse events such as these are “rare” when Pfizer and Moderna’s clinical trial data indicate they are not, is a startling exercise in disinformation.
‘I want to re-emphasise that these questions could have been answered if you had required vaccine manufacturers to perform and report adequate clinical trials . . . I anticipate with regret that you will repeat past mistakes and prematurely promote new therapies to Americans without accurately and truthfully weighing data on risks and benefits.’
Ladapo then asked Califf and Walensky to answer 12 questions relating to the safety data, and concluded: ‘Your organisations are the main entities promoting vaccine hesitancy – Florida promotes the truth. It is our duty to provide all information within our power to individuals so they can make their own informed health care decisions. A lack of transparency only harms Americans’ faith in science.’
Regular readers of TCW as well as The Daily Sceptic know that numerous scientists support Ladapo’s position, such as reported here, here, here, here, here, here and here.
At present, however, the FDA and CDC, like the NHS, continue to ignore such reports, asserting that ‘the known and potential benefits of these vaccines clearly outweigh their known and potential risks, and that ‘being up to date on vaccinations saves lives compared with individuals who did not get vaccinated’.
FDA admits it has no records indicating covid-19 vaccine safety protocols were followed
By Aaron Siri | ICAN | June 9, 2023
From early in the pandemic, the government has been promising the public that it was taking COVID-19 vaccine safety “very seriously,” and that the vaccines had been subject to “the most intense safety monitoring program in U.S. history.” ICAN likes to confirm these claims for itself but when it tried to do just that, it uncovered that the FDA actually deviated from long-standing protocols concerning vaccine safety.
Since May 9, 2008, the FDA has had vaccine safety procedures in place detailed in a Standard Operating Procedures and Policies (SOPP) document. This document “describes the procedures that the [FDA] staff should routinely follow to coordinate rapid responses to complex vaccine safety issues,” and discusses a Vaccine Safety Team whose “key purpose” is to “coordinate [FDA] rapid responses to vaccine safety issues … and to serve as a resource [] to identify data and policy needs pertaining to vaccine safety.”
One office in the FDA is crucial to this goal and acts as the “official contact for VAERS and is responsible for processing and review of the reports,” as well as “for forwarding those reports to the appropriate contacts within CBER for further action and follow-up.” For example, its staff members identify VAERS adverse event reports that “need a rapid response and complex coordination,” after which they are supposed to “immediately” inform certain FDA management who then alert other sub-agencies.
Given the lofty talk by federal health agencies claiming that COVID vaccines were subject to “the most rigorous – and accurate – review processes globally,” one would think that the FDA, at a minimum, subjected them to at least these already ridiculously weak pre-existing standards for vaccine safety monitoring.
But, after ICAN’s attorneys submitted records requests to the FDA seeking documents on the FDA’s policies concerning the identification of VAERS reports requiring a “rapid response,” as well as documents showing that the FDA had actually followed up on the individual VAERS reports that required a “rapid response,” the FDA replied more than year later with an incredible response: “A search of our records did not locate any documents responsive to your request.”
In a nutshell, the FDA has essentially admitted that it is not following even its own set of already watered-down procedures for vaccine safety monitoring that were in place prior to COVID.
When the curtain is pulled back on the purported “thorough” and “intense” safety monitoring, there is yet again nothing to see. So much for the FDA’s promise to look out for the American people. ICAN will continue to monitor the FDA and share any important updates.
See below for more instances where ICAN uncovered instances where “health” agencies made unsupported claims to the public:
Featured Video
Iran War Is Accelerating the End of US Dominance
or go to
Aletho News Archives – Video-Images
From the Archives
Why the UK, the EU and the US Gang-Up on Russia
By James Petras :: 03.20.2018
Introduction: For the greater part of a decade the US, the UK and the EU have been carrying out a campaign to undermine and overthrow the Russia government and in particular to oust President Putin. Fundamental issues are at stake including the real possibility of a nuclear war.
The most recent western propaganda campaign and one of the most virulent is the charge launched by the UK regime of Prime Minister Theresa May. The Brits have claimed that Russian secret agents conspired to poison a former Russian double-agent and his daughter in England, threatening the sovereignty and safety of the British people. No evidence has ever been presented. Instead the UK expelled Russian diplomats and demands harsher sanctions, to increase tensions. The UK and its US and EU patrons are moving toward a break in relations and a military build-up.
A number of fundamental questions arise regarding the origins and growing intensity of this anti-Russian animus.
Why do the Western regimes now feel Russia is a greater threat then in the past? Do they believe Russia is more vulnerable to Western threats or attacks? Why do the Western military leaders seek to undermine Russia’s defenses? Do the US economic elites believe it is possible to provoke an economic crisis and the demise of President Putin’s government? What is the strategic goal of Western policymakers? Why has the UK regime taken the lead in the anti-Russian crusade via the fake toxin accusations at this time?
This paper is directed at providing key elements to address these questions. … continue
Blog Roll
 Aletho News
Aletho News- Trump White House plagiarized Iran war manifesto from Israel-aligned think tank
- Western media whitewashes Israel’s attempted murder of British journalist in Lebanon
- Israel-linked arms facility set ablaze in EU
- IRAN: The Three Islands Unmaking American Unipolar Sea Power in the Persian Gulf
- Trump’s dispatch of Marine Expeditionary Unit signals desperation for any symbolic success
- Iran Proposes Creating Middle East Security Structure With All Regional States – President
- Iran’s weapons industry still churning out missiles despite war: IRGC
- Washington approves billions in new arms sales to Gulf states as concerns grow over stocks of air defenses
- Iran War: Pentagon’s $200B Budget Could Run Out in Just Five Months
- Seven US allies endorse Hormuz ‘coalition,’ offer ‘no commitment’ for military action
- If Americans Knew
- Meet the former fashion blogger and shady doctor behind the ‘30,000 dead’ Iran psy-op
- Vatican Secretary of State to Trump, Israel: End the war as soon as possible
- The Majority of Americans Believe War Against Iran Benefits Israel More Than US
- Efforts to shut down pro-Palestinian speech face series of setbacks in court
- What has Israel done to my brother?
- Eid without worship in Al Aqsa – Not a ceasefire Day 161
- Trump: Israel attacked Iranian gas field without US knowledge. No more such attacks!
- America’s friends must help extricate it from an unlawful war
- Democratic Nat’l Committee’s Kneejerk Backing of Israel Is Political and Moral Failure
- Major revelations from former counterterrorism chief Joe Kent’s extensive interview
- No Tricks Zone
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis
- New Study Documents A 20-Year Pause In Arctic Sea Ice Decline – Driven By Internal Variability
- Wake-up Call: Survey Shows Majority Of Germans Now Favor Postponing Climate Targets!
- Televised! Leading German Political Candidate Tells Schoolchildren CO2 Makes Sun Hotter!
- New Study: A Century Warming Of 1.1°C Is ‘Commonplace’ And ‘Not Unusual’ During This Interglacial
- New Study: ‘Internal Noise’ And Volcanic Forcing Can Trigger 10-15°C Warming Within Decades
