The Next Step for the World Economic Forum

BY ROGER KOOPS | BROWNSTONE INSTITUTE | FEBRUARY 20, 2022
It has been obvious since early 2020 that there has been an organized cult outreach that has permeated the world as a whole. It’s possible that this formed out of a gigantic error, rooted in a sudden ignorance of cell biology and long experience of public health. It is also possible that a seasonal respiratory virus was deployed by some people as an opportunity to seize power for some other purpose.
Follow the money and influence trails and the latter conclusion is hard to dismiss.
The clues were there early. Even before the WHO declared a pandemic in March 2020 (at least several months behind the actual fact of a pandemic) and before any lockdowns, there were media blitzes talking about the “New Normal” and talk of the “Great Reset” (which was rebranded as “Build Back Better”).
Pharmaceutical companies such as Pfizer, Johnson & Johnson, Moderna, and Astra-Zeneca were actively lobbying governments to buy their vaccines as early as February 2020, supposedly less than a month after the genetic sequence (or partial sequence) was made available by China.
As a person who spent his whole professional career in pharmaceutical and vaccine development, I found the whole concept of going from scratch to a ready-to-use vaccine in a few months simply preposterous.
Something did not add up.
I knew of the names with which everyone has become familiar. Bill Gates, Neil Ferguson, Jeremy Farrar, Anthony Fauci, and others had either been lobbying for or pursuing the lockdown strategies for many years. But still, the scope of the actions seemed too large to even be explained by those names alone.
So, the fundamental questions that I have been asking myself have been why and who? The “Why” seems to always come back to issues besides public health. Of course the “Who” had the obvious players such as the WHO, China, CDC, NIH/NIAID, and various governments but there seemed to be more behind it than that. These players have been connected to the “public health” aspect but that seemed to be only scratching the surface.
I am not an investigative journalist and I would never claim that role, but even I can do some simple internet searches and start to see patterns evolve. The searches that I have done have yielded some very interesting “coincidences.”
If I give you the names of the following people – Biden, Trudeau, Ardern, Merkel, Macron, Draghi, Morrison, Xi Jinping – what do you think that they have in common? Yes, they are all pampered and stumble over themselves, but that is also not the connection.
One can see very quickly that these names certainly connect to lockdown countries and individuals who have ignored their own laws and/or tried in some way to usurp them. But, there is more to it than that and I will give a hint by providing a link with each name.
- Joseph Biden, President, United States
- Boris Johnson, PM of United Kingdom
- Jacinda Ardern, PM of New Zealand
- Angela Merkel, Former PM of Germany
- Emmanuel Macron, President of France
- Justin Trudeau, PM of Canada
- Xi Jinping, CCP Leader, China
- Mario Draghi, PM of Italy
- Scott Morrison, PM of Australia
They are all associated with the World Economic Forum (WEF), a “nonprofit” private organization started (in 1971) and headed by Klaus “You will own nothing and be happy” Schwab and his family. This is a private organization that has no official bearing with any world governance body, despite the implication of the name. It could just as well have been called the “Church of Schwabies.” The WEF was the origin of the “Great Reset” and I would guess that it was the origin of “Build Back Better” (since most of the above names have used that term recently).
If you think that the WEF membership ends with just leaders of countries, here are a few more names:
- Gavin Newsom, Governor of California
- Jay Inslee, Governor of Washington State
- Anthony Fauci, Director NIAID
- Nancy Pelosi, Speaker of the House
Allow me to introduce more of the WEF by giving a list of names for the Board of Trustees.
- Al Gore, Former WP of the US
- Mark Caney, UN Special Envoy for Climate Action
- T. Shanmugaratnam, Seminar Minister Singapore
- Christine Lagarde, President, European Central Bank
- Ngozi Okonja-Iweala, Director General, WTO
- Kristalian Georggieva, Managing Director, IMF
- Chrystia Freeland, Deputy Minister of Canada
- Laurence Fink, CEO, BlackRock
You can see a cross section of political and economic leaders on the board. The leader of the organization, that is the leader of the Board, is still Klaus Schwab. He has built an impressive array of followers.
If you want to really see the extent of influence, go to the website and pick out the corporate name of your choice; there are many to choose from: Abbott Laboratories, Astra-Zeneca, Biogen, Johnson & Johnson, Moderna, Merck, Novartis, Pfizer, Serum Institute of India, BASF, Mayo Clinic, Kaiser Permanente, Bill and Melinda Gates Foundation, Wellcome Trust, Blackrock, CISCO, Dell, Google, Huawei, IBM, Intel, Microsoft, Zoom, Yahoo, Amazon, Airbus, Boeing, Honda, Rakuten, Walmart, UPS, Coca-Cola, UBER, Bank of China. Bank of America. Deutsche Bank, State Bank of India, Royal Bank of Canada, Lloyds Banking, JP Morgan-Chase, Equifax, Goldman-Sachs, Hong Kong Exchanges, Bloomberg, VISA, New York Times, Ontario (Canada) Teacher’s Pension Plan
The extent of reach is huge even beyond the worldwide leader network. For example, we all know what Bill Gates has been doing with his wealth via the Bill and Melinda Gates Foundation (BMGF). But, the Wellcome Trust is equal to the task. Who is the Director of the Wellcome Trust? One named Jeremy Farrar, of the United Kingdom SAGE and lockdown fame – arguably the architect of the US-UK lockdowns in 2020 – is closely associated with WEF.
Concerning the reach that can occur, let me give some examples from the BMGF alone, and it comes from the time that I spent in 2020 reading their extensive funding list.
A few years ago, the BMGF awarded the Institute for Health Metric Evaluation (IHME) a ten-year, almost $280 million award. IHME (associated with the University of Washington in Seattle) was at the forefront of the computer modeling that was driving the lockdowns and the nonpharmaceutical Interventions during 2020. People have seen their name often in print or on MSNBC or CNN.
In 2019, IHME awarded the Editor of the Lancet (Dr. Richard Horton) a $100,000 award and described him as an “activist editor.” The Lancet, once considered one of the best medical journals, has been at the forefront of censoring opposing scientific viewpoints since 2020 and publishing “papers” that were not fit to be published. I never could understand what it meant to be an “activist” editor in a respected scientific/medical journal because, stupid me, I always thought that the first job of the editor was to be impartial. I guess I learned in 2020 how wrong I was.
Of course, the Lancet is also heavily funded from pharmaceutical companies such as Pfizer (also a member of the WEF).
But, the BMGF reach goes far beyond just IHME and these connections have been quite recognizable. Here are some examples of the organizations and moneys received during 2020 alone broken down by areas.
Bill and Melinda Gates Foundation Grants 2020
| Organization Name | Amount USD |
|---|---|
| Johns Hopkins Bloomberg School of Public Health | 20+ million |
| World Health Organization (WHO) | 100+ million |
| Oregon Health Sciences Univ. | 15+ million |
| CDC Foundation | 3.5+ million |
| Imperial College of London | 7+ million |
| Chinese CDC | 2+ million |
| Harvard TH Chan School of Public Health | 5+ million |
| Institute of Health Metric Evaluation (IHME) | 28 million (part of a 10 yr/279 million USD grant) |
| Nigeria CDC | 1.1 million |
| Deutsche Gesellschaft für Internationale Z. (Gmbh) | 5+ million |
| Novartis | 7+ million |
| Lumira Dx UK LTD | 37+ million |
| Serum Institute of India | 4+ million |
| Icosavac | 10 million |
| Novavax | 15 million |
| BBC | 2 million |
| CNN | 4 million |
| Guardian | 3+ million |
| NPR | 4 million |
| Financial Times LTD | 0.5 million |
| National Newspaper Publishers Assoc. | 0.75 million |
Bill Gates has also invested heavily in Moderna and his investments have paid out nicely for him. The BMGF has also given close to $100 million to the Clinton Health Access Initiative.
The questions now have to be asked:
- Is this some beginning of a controlled authoritarian society intertwined via the WEF?
- Has the Covid panic been staged to set the stage? Please note, I am not a “Covid Denier” since the virus is real. But, has a normal seasonal respiratory virus been used as an excuse to activate the web?
The next questions, for those of us who at least pretend to live in “Democratic” societies, have to be:
- Is this what you expected and/or want from the people you elect?
- How many people knew of the “Associations” of the people that they voted for? (I certainly did not know of the associations until I did the searches but maybe I am just out of touch)
Can we anticipate their next moves? There may be some hints.
The Next Move
Jeremy Farrar of The Wellcome Trust recently wrote an article for the WEF with the CEO of Novo Nordisk Foundation, Mads Krogsgaard Thomsen. It is a summary of a larger piece written for and published by the Boston Consulting Group.
In this article, they propose that the way to “fix” the problem of antibiotic resistant bacteria is via a subscription service. That is, you pay a fee and when you need an antibiotic, presumably an effective one will be available for you.
My guess is that they have the same philosophy for vaccines and that certainly seems to be the approach with Coronavirus. Keep paying for and taking boosters.
In view of this philosophy, the vaccine mandates make sense. Get society “addicted” to an intervention, effective or not, and then keep feeding them. This becomes especially effective if you can keep the fear going.
This approach is so shortsighted, from a scientific viewpoint, it astounds me. But, like much of recent history, I think science has little to do with it. The goal is not scientifically founded but control founded.
After the discovery of penicillin almost one century ago, there were scientists who warned that antibiotic usage should be considered very carefully in practice because evolutionary pressures would lead to antibiotic resistant species of bacteria. At that time, they were considered to be rogue scientists; after all, didn’t we suddenly have a miracle cure for many deadly problems?
From the time of discovery, it took over a decade before fermentation methods were developed to produce sufficient quantities of antibiotics to be practical. These methods allowed for the use of penicillin on the battlefield towards the end of WWII and undoubtedly saved many lives then and later in subsequent wars (Korea and Vietnam) by preventing serious infections resulting from wounds sustained during battle.
However, it did not take long before the medical establishment was handing out antibiotics like candy. I experienced this myself when I was a child in the 1960s. It seemed like every time we went to the doctor, no matter what the problem, I was given a series (not just one) of injections of penicillin. There were never any attempts to determine if I had a virus, bacteria, or even an allergy. The answer was: in with the needle. I cannot count how many times I was “jabbed” as a child.
It didn’t take long before resistant species started to appear. The result was that more and more money was pumped into R&D for antibiotics. When I was in graduate school during the 1980s, one sure way to get some NIH funding was to tie the research into the “antibiotic” search. Antibiotics became big business.
We now have several classes of antibiotics that are used for specific cases. We have Aminoglycosides (Streptomycin, Neomycin, etc.), Beta-Lactams Cephalosporins (four generations including Cefadroxil-G1, Cefaclor-G2, Cefotaxime-G3, Cefepime-G4 , Beta-Lactams Penicillins (including Ampicillin, Amoxicillin, and Penicillin), Other Beta-Lactams (Meropenem), Fluoroquinolones (Levofloxacin, Gemifloxicin, etc.), Macrolides (Azithromycin, Clarithromycin, etc.), Sulfonamides (Sulfisoxazole, etc.), Tetracyclines, and others such as Clindamycin and Vancomycin (typically reserved for resistant bacteria). All in all, physicians have over 50 different choices for antibiotics.
The most common place to encounter antibiotic resistant bacteria is in a hospital. Most people who get some sort of infection in the normal routine of life, like a sinus infection or skin infection, will not likely encounter an antibiotic resistant species.
Except there has been another source of the problem and that has been in the food supply. Antibiotics have become very popular with large scale meat production facilities of all types including beef, poultry, swine, and even fish. These include actual farms where the animals are raised as well as in the processing of the meat. The overuse of antibiotics in these industries has also produced resistant forms of bacteria.
For example, in attempts to limit the bacteria e. coli, common to mammalians, antibiotics have been used and this has resulted in some antibiotic resistant forms of e. coli. An infection via e. coli (antibiotic resistant or not) can be avoided by proper cooking and handling of meats. However, sometimes that does not happen and there are e. coli outbreaks (also from improperly washed vegetables that may use contaminated irrigation water).
For most healthy people, experiencing e. coli (either resistant or not) is only a passing discomfort that includes intestinal cramps, diarrhea, and other GI complaints. Depending on the amount of contamination, a person may suffer for a day or two or for several days.
But, with some people, it can be serious or deadly (such as in elderly people in poor health and young children). If that occurs, then the presence of an antibiotic resistant form can be a serious matter. Presence of a non-resistant form can be treated more readily.
A few years ago I had pneumonia; a relatively mild case. I was given a choice of in-patient treatment or out-patient and it was a no-brainer. If I wanted to make sure that my pneumonia could be handled by the normal course of antibiotics (I was given a quinolone), staying at home and away from the hospital was important. I knew that hospital-acquired pneumonia could be a much more serious situation. So, I stayed at home and easily recovered. That did not mean I was guaranteed getting a more serious resistant form in the hospital but I understood that the risk was much greater.
Producing more antibiotics and giving them on subscription to the users is not the answer. That will only lead to more resistant forms and there will be this continuing loop of antibiotic use. But, if the actual goal is societal addiction to antibiotics out of fear, just like addiction to universal Covid vaccines out of fear, then it makes sense.
Finding a few universal antibiotics that deal with the resistant forms is important and it is also important to use those sparingly and only as a last resort. In addition, better management of antibiotic use in our society would go a long way to attenuating the problem.
There is nothing particularly controversial about that observation. It was accepted by nearly every responsible health professional only two years ago. But we live now in different times of extreme experimentation, such as the deployment of world-wide lockdowns for a virus that had a highly focused impact, with catastrophic results for the world.
It was the WEF on March 21, 2020 that assured us “lockdowns can halt the spread of Covid-19.” Today that article, never pulled much less repudiated, stands as probably the most ridiculous and destructive suggestion and prediction of the 21st century. And yet, the WEF is still at it, suggesting that same year that at least lockdowns reduced carbon emissions.
We can easily predict that the WEF’s call for a universal and mandated subscription plan for antibiotics – pushed with the overt intention of shoring up financial capitalization of major drug manufacturers – will meet the same fate: poor health outcomes, more power to entrenched elites, and ever less liberty for the people.
Roger W. Koops holds a Ph.D. in Chemistry from the University of California, Riverside as well as Master and Bachelor degrees from Western Washington University. He worked in the Pharmaceutical and Biotechnology Industry for over 25 years. Before retiring in 2017, he spent 12 years as a Consultant focused on Quality Assurance/Control and issues related to Regulatory Compliance. He has authored or co-authored several papers in the areas of pharmaceutical technology and chemistry.
How a false hydroxychloroquine narrative was created, and more

Meryl Nass, MD
Alliance for Human Research Protection | June 28, 2020
Below, Dr. Meryl Nass reviews a long list of corrupt practices that undermine the integrity of medical science and the practice of medicine during the current medical crisis. The coronavirus crisis has been made significantly worse by stakeholders who are preventing doctors from prescribing for their patients, existing, safe and effective medicines, because the stakeholders are invested on garnering projected future profits from not-yet-developed vaccines and “countermeasures” specifically developed against COVID-19.
The stakeholders who influence and issue medical practice guidelines, include public health officials, global public health institutions, government advisory committees, and clinical trialists who design trials to provide commercially beneficial results. Editors of prestigious high impact, medical journals contribute to the corruption of medicine by publishing fraudulent studies, and reports of clinical trials that were designed to cause foreseeable deaths, The focus of Dr. Nass’ J’Accuse post are clinical trials that deliberately subjected some patients to toxic doses of Hydroxychloroquine. [Dr. Nass is a longtime member of the AHRP Board of Directors].
These collaborators engaged in an orchestrated effort to prevent physicians from utilizing an existing, off-patent, cheap and affordable drug, that thousands of clinicians attest to its therapeutic benefit.
- The problem with Hydroxychloroquine, a drug with a 70-year safety track record, is that there is no profit to be made from this cheap, off-patent drug!
*****************
It is remarkable that a series of events taking place over the past 3 months produced a unified message about hydroxychloroquine, and produced similar policies about the drug in the US, Canada, Australia, NZ and western Europe. The message is that generic, inexpensive hydroxychloroquine is dangerous and should not be used to treat a potentially fatal disease, Covid-19, for which there are no (other) reliable treatments.
- Hydroxychloroquine had been used safely for 65 years in millions of patients. And so the message was crafted that the drug is safe for its other uses, but dangerous when used for Covid-19. It doesn’t make sense, but it seems to have worked.
Were these acts carefully orchestrated? You decide.
Might these events have been planned to keep the pandemic going? To sell expensive drugs and vaccines to a captive population? Could these acts result in prolonged economic and social hardship, eventually transferring wealth from the middle class to the very rich? Are these events evidence of a conspiracy?
Here is a list of what happened, in no special order. Please help add to this list if you know of additional acts I should include. This will be a living document. I have penned this as if it is the “to do” list of items to be carried out by those who pull the strings. The items on the list have already been carried out. One wonders what else might be on their list, yet to be carried out, for this pandemic.
1. You stop doctors from using the drug in ways it is most likely to be effective (in outpatients at onset of illness). You prohibit use outside of situations you can control.
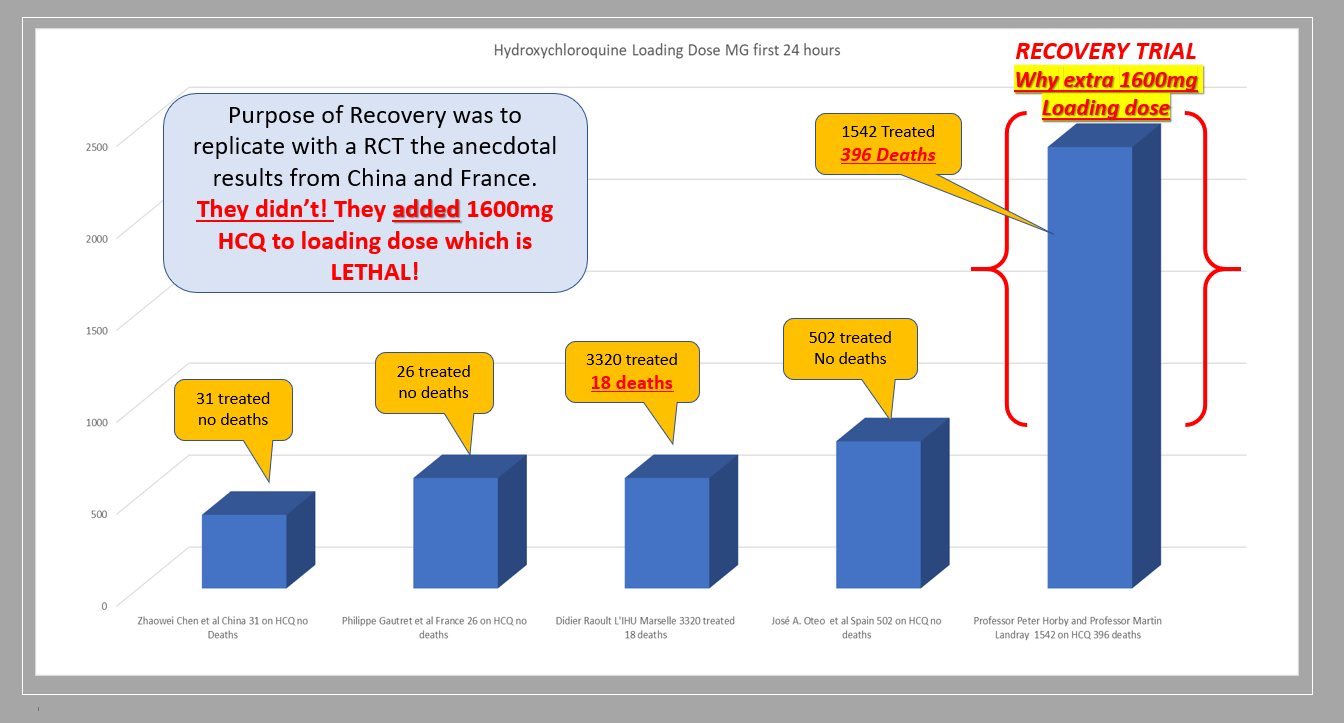
Situations that were controlled to show no benefit included 3 large, randomized, multi-center clinical trials (Recovery, Solidarity and REMAP-Covid), which are generally believed to yield the most reliable evidence. However, each of them used excessive doses that were known to be toxic; see my previous articles here and here.
2. You prevent or limit use in outpatients by controlling the supply of the drug, using different methods in different countries and states. In NY state, by order of the governor, hydroxychloroquine could only be prescribed for hospitalized patients. France has issued a series of different regulations to limit prescribers from using it. France also changed the drugs’ status from over-the-counter to a drug requiring a prescription.
3. You play up the danger of the drug, emphasizing side effects that are very rare when the drug is used correctly. You make sure everyone has heard about the man who died after consuming hydroxychloroquine in the form of fish tank cleaner.
4. You limit clinical trials to hospitalized patients, instead of testing the drug in outpatients, early in the illness, when it is predicted to be most effective.
5. You design clinical trials to give much too high a dose, ensuring the drug will cause harm in some subjects, sufficient to mask any possible beneficial effect. You make sure that dozens of trials in dozens of countries around the world use these dangerous doses.
6. You design clinical trials to collect almost no safety data, so any cause of death due to drug toxicity will be attributed to the disease instead of the drug.
7. You issue rules for use of the drug based on the results of the unethical, overdosing Recovery study.
8. You publish, in the world’s most-read medical journal, the Lancet, an observational study from a huge worldwide database that says use of chloroquine drugs caused significantly increased mortality. You make sure that all major media report on this result. Then 3 European countries announce they will not allow doctors to prescribe the drug. And Sanofi announces it will no longer supply the drug for use with Covid, and will halt its own clinical trials, based on a fabricated study.
9. Even after hundreds of people renounce this observational study due to easily identified fabrications–which, as James Todaro, MD, wrote was a “study out of thin air“–the Lancet held firm for two weeks, serving to muddy the waters about the trial, until finally 3 of its 4 coauthors (but not the journal) retracted the study. You make sure few media report that the data were fabricated and the “study” a fraud. You let people believe the original story: that hydroxychloroquine routinely kills.
10. You ensure federal agencies like FDA and CDC hew to your desired policies. For example, FDA advised use only in hospitalized patients (too late) or in clinical trials (which are limited, are difficult to enroll in, or use excessive doses). As of mid June, FDA now advises patients and doctors to only use the drug in a clinical trial!
Another example: you have FDA make unsubstantiated and false claims, such as: “Hospitalized patients were likely to have greater prospect of benefit (compared to ambulatory patients with mild illness)” and claim the chloroquine drugs have a slow onset of action. If that were really true, they would not be used for acute attacks of malaria or in critically ill patients with Covid. (Disclosure: I once dosed myself with chloroquine for an acute attack of P. vivax malaria, and it worked very fast.). Providing no other treatment advice, CDC refers clinicians to the NIH guidelines, discussed below.
11. You make sure to avoid funding/encouraging clinical trials that test drug combinations like hydroxychloroquine with zinc, with azithromycin, or with both, although there is ample clinical evidence that such combinations provide a cumulative benefit to patients.
12. You have federal and UN agencies make false, illogical claims based on models rather than human data. For example, you have the FDA state on June 15 that the dose required to treat Covid is so high it is toxic, after the Recovery and Solidarity trials have been exposed for toxic dosing. This scientific double-speak gives some legal cover to the clinical trials that overdosed their patients.
According to Denise Hinton, RN, the FDA’s Chief Scientist, or a clumsy FDA wordsmith:
”Under the assumption that in vivo cellular accumulation is similar to that from the in vitro cell-based assays, the calculated free lung concentrations that would result from the EUA suggested dosing regimens are well below the in vitro EC50/EC90 values, making the antiviral effect against SARS-CoV-2 not likely achievable with the dosing regimens recommended in the EUA. The substantial increase in dosing that would be needed to increase the likelihood of an antiviral effect would not be acceptable due to toxicity concerns.”
13. You have a WHO report claim toxic doses are needed. This of course is nonsense since
a) CDC researchers showed strong effects against SARS-1 at safely achievable concentrations,
b) the drug at normal doses is being tested in over 30 different medical conditions (see clinicaltrials.gov), and
c) reports from many different countries say that the drug is effective for Covid-19 at normal doses, while
a high dose chloroquine treatment arm was halted in Brazil and a preprint of the study was posted April 11, after finding the toxic effects were causing ventricular arrhythmias and deaths.
- Toxicity was noted after only 3 days of treatment, during which 3.6 grams of chloroquine were administered. But the Solidarity (3.2 grams of hydroxychloroquine in 3 days), Recovery (3.6 grams of hydroxychloroquine in 3 days) and REMAP-Covid trials (3.6 grams of hydroxychloroquine in 3 days) continued overdoing patients until June, despite Brazil’s evidence of deaths by overdose.
- Tellingly, JAMA editor Gordon Rubenfeld wrote about the Brazilian study, “if you are prescribing HCQ after these JAMA results, do yourself and your defense lawyer a favor. Document in your medical record that you informed the patient of the potential risks of HCQ including sudden death and its benefits (???).”
14. You create an NIH Guideline committee for Covid treatment recommendations, in which 16 members have or had financial entanglements with Gilead, maker of Remdesivir. The members were appointed by the CoChairs. Two of the three CoChairs are themselves financially entangled with Gilead. Are you surprised that their guidelines recommend specifically against the use of hydroxychloroquine and in favor of Remdesivir, and that they deem this the new “standard of care”?
15. You frighten doctors so they don’t prescribe hydroxychloroquine, if prescribing it is even allowed in their jurisdiction, because prescribing outside the “standard of care” leaves them open to malpractice lawsuits. You further tell them (through the FDA) they need to monitor a variety of lab parameters and EKG when using the drug, although this was never advised before, which makes it very difficult to use the drug in outpatients. You have the European Medicines Agency issue similar warnings.
16. You manage to control the conduct of most trials around the world by designing the WHO-managed Solidarity trials, currently conducted in 35 countries. WHO halted hydroxychloroquine clinical trials around the world, twice.
The first time, May 25, WHO claimed it was in response to the (fraudulent) Lancet study.
The second time, June 17, WHO claimed the stop was in response to the Recovery trial results.
Recovery used highly toxic doses of hydroxychloroquine in over 1500 patients, of whom 396 died.
You stop the trial before the data safety monitoring board has looked at your data, a move that is unlikely to be consistent with trial protocol. WHO’s trial in over 400 hospitals overdosed patients with 2.0 g hydroxychloroquine in the first 24 hours.
WHO’s trial in over 400 hospitals was unlikely to provide useful results, as it too overdosed patients with hydroxychloroquine. The trial was halted days after the toxic doses were exposed.
17. You have the WHO pressure governments to stop doctors prescribing hydroxychloroquine.
18. You have the WHO pressure professional societies to stop doctors prescribing hydroxychloroquine.
19. You make sure that the most-consulted medical encyclopedia, UptoDate, provides bad guidance to physicians, advising them to restrict hydroxychloroquine to only patients in clinical trials, citing the above sources of information.

Anthony Fauci, MD
20. You have the head of the Coronavirus Task Force, Dr. Tony Fauci, insist the drug cannot be used in the absence of strong evidence… while he insisted exactly the opposite in the case of the MERS coronavirus outbreak several years ago, when he recommended an untested drug combination for use… which had been developed for that purpose by his agency.
And while he was bemoaning the lack of evidence, he was refusing to pay for trials to study hydroxychloroquine. And he was changing the goalposts on the Remdesivir trial, not once but twice, to make Remdesivir show just a tiny bit of benefit, but no mortality benefit. And don’t forget, Fauci was thrilled to sponsor a trial of a Covid vaccine in humans before there was any data from animal trials. So much for requiring high quality evidence before risking use of drugs and vaccines in humans!
21. You convince the public that the crisis will be long-lasting. You have the 2nd richest man in the world, and biggest funder of the WHO, Bill Gates, keep repeating to the media megaphone that we cannot go back to normal until there is a vaccine. (The Gates Foundation helped design the WHO clinical trials, and Gates is heavily invested in pharmaceuticals and vaccines.)

Bill Gates
- You have CDC (with help from FDA) prevent the purchase of coronavirus test kits from Germany, China, WHO, etc, and fail to produce a valid test kit themselves. The result was that during January and February, US cases could not be reliably identified, and for several months thereafter insufficient and unreliable test kits made it impossible to track the epidemic and stop the spread.
- You have trusted medical spokesmen lie to the public about the pandemic’s severity, so precautions weren’t taken when they might have been more effective and less long-lasting. Congress was repeatedly briefed about the pandemic in January and February, which scared several Congress members enough that they sold off large amounts of stock, risking insider trading charges. Senator Burr is one of them, currently under investigation for major stock sales on February 13.
Yet Dr. Fauci told USA Today on February 17 that Americans should worry more about the flu than about coronavirus, the danger of which was “just miniscule.” Then on February 28, Drs. Fauci and Robert Redfield (CDC Director) wrote in the New England Journal :
“… the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively.”
 You destroy the reputation of respected physicians who stand in your way. Professor Didier Raoult and his team in Marseille have used hydroxychloroquine on over 4,000 patients, reporting a mortality rate of about 0.8%. (The mortality rate of patients given hydroxychloroquine in the Recovery trial was 25.7%.) Raoult is very famous for discovering over 100 different microorganisms, and finding the long-sought cause of Whipple’s Disease. With this reputation, Raoult apparently thought he could treat patients as he saw fit, which he has done, under great duress. Raoult was featured in a New York Times Magazine article, with his photo on the cover, May 12, 2020. After describing his accomplishments, the Times very unfavorably discussed his personality, producing a detailed hit piece. He is now considered an unreliable crank in the US.
You destroy the reputation of respected physicians who stand in your way. Professor Didier Raoult and his team in Marseille have used hydroxychloroquine on over 4,000 patients, reporting a mortality rate of about 0.8%. (The mortality rate of patients given hydroxychloroquine in the Recovery trial was 25.7%.) Raoult is very famous for discovering over 100 different microorganisms, and finding the long-sought cause of Whipple’s Disease. With this reputation, Raoult apparently thought he could treat patients as he saw fit, which he has done, under great duress. Raoult was featured in a New York Times Magazine article, with his photo on the cover, May 12, 2020. After describing his accomplishments, the Times very unfavorably discussed his personality, producing a detailed hit piece. He is now considered an unreliable crank in the US.
- You have social media platforms ban content that does not agree with the desired narrative. As YouTube CEO and ex-wife of Google founder Sergey Brin, Susan Wojcicki said,
“YouTube will ban any content containing medical advice that contradicts World Health Organisation (WHO) coronavirus recommendations. Anything that would go against World Health Organisation recommendations would be a violation of our policy.”
- When your clinical trials are criticized for overdosing patients, you have Oxford-affiliated, Wellcome Trust-supported scientists at Mahidol University publish papers (a literature review with modeling and a modeling study) purporting to show that the doses used were not toxic. You develop a new method to measure hydroxychloroquine in a handful of Recovery patients who were not poisoned. However, there are 2 problems you forgot with this approach:
- The Brazilian data, including 16 deaths, extensive clinical information and documented ventricular arrhythmias, are much more valuable than theoretical models of what might be happening in the body.
- Either the drug is too toxic to use for a life-threatening disease, or even extremely high doses are safe. You can’t have it both ways.
Oxford is the institution running the Recovery trial, and invented a Covid vaccine that already has 400 million doses on order. The Wellcome Trust funded the Recovery trial.
- You change your trial’s primary outcome measures after the trials have started, in order to prevent detection of drug-induced deaths (Recovery) or to make your drug appear to have efficacy (NIAID Remdesivir trial).
- You stop manufacturers from supplying the drug. Shortly after the fraudulent Lancet paper came out, Sanofi announced it would no longer supply the drug for use with Covid, and would halt its two hydroxychloroquine clinical trials. One of the cancelled Sanofi trials was expected to test 210 outpatients early in the course of disease. The trial remains suspended at the time of writing, while the Lancet paper was retracted 13 days after publication.
- You surely don’t want a trial of hydroxychloroquine treatment early in the disease, since it might show an excellent effect.
Featured Video
Prof. Ted Postol: Iran Already Achieved Nuclear Deterrence Against Israel
or go to
Aletho News Archives – Video-Images
From the Archives
How the occupied mentality syndrome works
Saudi Arabia on the American chessboard – Part 3
By B. J. Sabri | American Herald Tribune | June 27, 2016
Read part 2: “The occupied mentality Syndrome“
Previously I argued whether Saudi Arabia’s repeated involvements in U.S. interventions and wars stem from free national will or in response to a specific condition. For starters, in Saudi Arabia there is no national will. In Saudi Arabia, the national will is the will of the Al Saud clan. Still, when a major Arab state allies itself with a superpower that committed unspeakable crimes against humanity in almost every Arab country, then something is wrong. This fact alone should compel us to examine the U.S.-Saudi relation for one exceptional reason. As a result of the U.S.-Saudi wars, hundreds of thousands of people in Afghanistan, Iraq, Iran, Libya, Syria, Yemen, and Somalia have lost their lives. Millions became displaced in their own homelands. And millions more rendered refugees.
Attributing the Saudi policies to the bonds of “partnership” with the U.S. is frivolous. There are no bonds between these two thugs except those of business, military deals, secret plots, and wars. Proving this point, bonds such as these have no space for the American and Saudi peoples to share significant cultural or societal exchanges. If partnership is not the reason for the Saudi contribution to the U.S. strategy of empire and imperialism, then another reason must exist.
This leads to three possibilities. … continue
Blog Roll
 Aletho News
Aletho News- Hezbollah hits Israeli warship off Lebanon’s coast, sets it aflame
- Iran slams US strikes on B1 bridge, Mahshahr petrochemical plants as ‘blatant acts of state terrorism’
- In letter to UN chief, Araghchi warns of dire consequences of US-Israeli attacks on Iran’s nuclear facilities
- Why the CIA conspiracy to invade Iran with Kurdish militias failed
- Why Are Upbeat US Claims About Mission to Rescue Pilot ‘Highly Questionable’?
- Aircraft destroyed during US ‘rescue’ of downed F-15 pilot cost more than $100 million each
- Washington University removes professor who condemned US-Israeli war on Iran
- Russia Warns of Retaliation as UK Authorizes Seizure of Vessels
- Serbia thwarts plot to bomb Russia-Hungary gas pipeline – Vucic
- Al Mayadeen voices solidarity with Dr. Marandi amid death threats
- If Americans Knew
- In Iran, Israel-US take aim at “reason, research, and freedom of thought” – Daily Update
- US loses planes over Iran, Israel downgrades Lebanon war goals – Daily Update
- Israel Is Blocking Palestinians from Easter at Church Where Jesus Resurrected
- Plot to assassinate Palestinian activist follows harassment campaign promoted by Zionist groups and elected officials
- Prominent New York synagogue hosts presentation on why U.S. Jews should support the ethnic cleansing of Gaza
- Tapper vs. Piker: Is the CNN Anchor Auditioning for David Ellison?
- Shouldn’t Democrats Be Able to Condemn Genocide?
- Israel-US kill negotiators, destroy civilian structures, but Iran’s military capabilities still largely intact – Daily Update
- ‘War crime’: Global condemnation as Israeli ministers celebrate death penalty law targeting Palestinian prisoners
- 7 Ways Israel Is Turning Lebanon Into Gaza
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
