Yes, Treating COVID Patients With Hydroxychloroquine Can Save Lives
By Angelo DePalma, Ph.D. | The Defender | October 11, 2023
Hospitalized COVID-19 patients treated with hydroxychloroquine (HCQ) alone, or HCQ plus the antibiotic azithromycin, had significantly lower mortality than those not receiving the drugs, according to a study released this month in New Microbes and New Infections.
Researchers in Belgium report that just 16.7% of COVID-19 patients given HCQ, with or without azithromycin, died within 28 days compared to 25.9% among those not taking HCQ — a 35% lower mortality.
After adjusting for age differences, the risk of death was still 24% lower for HCQ-treated hospitalized patients.
The survival benefit was seen across all ages and was statistically significant.
The results support the efficacy of HCQ and azithromycin in improving outcomes for hospitalized COVID-19 patients. This contrasts with earlier studies using dangerously high HCQ doses that found no benefits.
Who participated in the study?
Led by Dr. Gert Meeus, a nephrologist at AZ Groeninge Hospital, Kortrijk, Belgium, researchers collected data from March 16 to May 20, 2020 — the first few months of the pandemic.
They compared outcomes for 352 COVID-19-positive, HCQ-treated adults hospitalized at AZ Groeninge Hospital with those of 3,533 patients across Belgium who did not receive the drug.
Treated patients averaged 69.7 years versus 73.1 years for the control group. While this age difference favors the younger subjects who face less risk from the virus, this factor was more than offset by the treatment group’s higher incidence of high blood pressure, diabetes, liver and lung diseases, and weakened immunity.
Treated subjects were also more obese — a COVID-19 risk factor — with lower blood oxygen (suggesting severe illness) and higher C-reactive protein levels. C-reactive protein is a blood marker for inflammation and poor COVID-19 outcomes.
During the 28 days following initial treatment, 16.7% of patients who received HCQ, either alone or with azithromycin, died compared with 25.9% in the control group.
How was HCQ administered?
For the study, 299 patients (85%) received HCQ plus azithromycin versus 53 who took HCQ alone. Researchers only prescribed the antibiotic when they suspected bacterial pneumonia. Data for HCQ alone and HCQ plus azithromycin were combined.
Subjects received HCQ as two 400-milligram doses on day one and two 200-milligram doses on days two through five.
Patients younger than 75 years received 500 milligrams of azithromycin for five days. Older patients took 500 milligrams on day 1 and 250 milligrams per day for four days.
88% of patients received the full treatment course but 12% took the drugs for less time, at the caregiver’s discretion, due to side effects or reaching a terminal condition.
Otherwise, side effects observed in 197 patients were mild and mostly stomach issues. One patient had hallucinations and two developed a skin rash.
Thirteen patients dropped out of the study due to side effects, including 4 of 15 who developed heart muscle abnormalities — despite an earlier study reporting an association between HCQ and lower cardiovascular risk.
Nine patients dropped out because of digestive upset. One patient developed an abnormal but nonfatal post-study heart rhythm, but no treated patients experienced sudden death or irregular heartbeat during the study.
How the drugs work
HCQ and azithromycin work together to eliminate the COVID-19 virus, but the drugs may benefit patients in other ways.
Both drugs act on the immune system in ways that may suppress the COVID-19 cytokine storm responsible for much of COVID-19-related illness and death.
HCQ may also prevent blood clots in COVID-19 patients, while azithromycin may prevent additional, non-lung bacterial infections.
HCQ was approved in the U.S. in 1955 to treat malaria, but because of its anti-inflammatory effects it is also prescribed to adults to treat autoimmune diseases like lupus and rheumatoid arthritis.
Most serious side effects — including retinopathy, which causes blindness — occur after years of use, while COVID-19 treatments generally last for less than one week.
The World Health Organization lists HCQ as an “essential medicine” based on its “safety, efficacy and public health relevance.”
Study strengths and weaknesses
Meeus designed his study and interpreted his findings to include results that may not have supported the “safety and efficacy” of HCQ.
For example, all patients receiving at least one dose of HCQ were included in the treatment group regardless of whether they completed the study. One dose of HCQ was unlikely to affect their survival, but including such patients would have increased mortality numbers in the treatment group, thereby underestimating HCQ survival benefits.
Excluding very sick patients in a survival study tends to make data appear stronger because fewer deaths invariably occur among healthier subjects. Meeus and coworkers did not do this.
Meeus’ results also likely underestimated the benefits of HCQ treatment by reviewing patients only after hospitalization, when they were already quite sick. COVID-19 treatment experts stress the importance of treatment before patients reach this stage.
This retrospective study associated a current outcome (death) with an earlier effect (receiving HCQ). Retrospective studies are less capable of establishing causation than prospective studies that first look at the intervention or cause and only later for effects.
Another potential study shortcoming involves the statistics investigators chose to report HCQ’s benefits. A reduction in deaths from 25.9% to 16.7% is a 36.5% decrease, but the effect is smaller when survival, not death, is the outcome measured.
Death rates of 25.9% and 16.7% mean that 83.3% of treated and 74.1% of untreated patients survived, for an overall survival benefit under 10%.
Reporting relatively large differences between two small numbers is a common strategy for amplifying modest clinical benefits.
Meeus did not account for the many observational studies carried out by such doctors as Didier Raoult, Vladimir Zelenko, Pierre Kory, Peter McCullough and others using HCQ with azithromycin and/or zinc to treat COVID-19 beginning in 2020 — some with very large practices — all demonstrating significant benefits with early treatment.
He also did not review early treatment randomized control trials or the many other studies showing clear benefits of HCQ treatment.
Conclusion: ‘remarkable’ results
The authors described their results as “remarkable” since large HCQ studies during the first pandemic year showed no benefit.
However, where Meeus and co-workers used HCQ at standard doses, the earlier trials used a fourfold higher total dose, including an initial dose seven times higher than the maximum approved dosage.
For example the WHO “Solidarity” and U.K. “Recovery” clinical trials used HCQ dosages that were considered fatal.
According to Meeus, other studies (see here, here, and here) using more reasonable HCQ dosing failed because they did not recruit enough subjects to show a statistically significant effect.
One of these studies found a 44% reduction in death at 28 days but included too few patients to be able to claim an HCQ benefit.

Percentage of patients who died in the HCQ group (white bars) vs. the no-HCQ group (black bars) by age group. A survival benefit was seen in all age groups. While about 2.5% of untreated 31- to 44-year-olds died during the study, no treated patients in this age group died. Credit: Gert Meeus et al.
Meeus concluded:
“Our study suggests that, despite the controversy surrounding its use, treatment with hydroxychloroquine and azithromycin remains a viable option. The favorable results and reassuring safety data support the need for adequately powered confirmatory randomized controlled trials using low dose hydroxychloroquine plus azithromycin.
“Given the pandemic emergency it is reasonable to give this treatment the benefit of the doubt pending the results of these trials or the advent of better treatment options.”
Angelo DePalma, Ph.D., is a science reporter/editor for The Defender.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
CA Bill would punish Doctors over COVID ‘Misinformation,’ as other states move to protect Doctors’ rights
By David Charbonneau, Ph.D. | The Defender | February 23, 2022
Before the U.S. Supreme Court last month blocked the Biden administration’s COVID-19 vaccine mandates for large employers and allowed the mandate for healthcare workers to stand, all eyes were on the feds when it came to COVID-related policies.
But state lawmakers also have been busy drafting bills in an effort to shape COVID policies closer to home.
The California Assembly, for example, introduced over the past six months a flurry of bills designed to strengthen vaccination mandates and regulate treatment options for patients.
For example, Sen. Richard Pan (D-Sacramento) last month introduced legislation proposing COVID vaccine mandates for all K-12 students in California schools.
And this month, Assembly Member Evan Low (D-Campbell) introduced legislation (AB 2098) that, according to the Los Angeles Times, would “make it easier for the Medical Board of California to discipline doctors who promote COVID-19 misinformation by classifying it as unprofessional conduct.”
The bill defines “unprofessional conduct” as any action a physician or surgeon takes “to disseminate or promote misinformation or disinformation related to COVID-19, including false or misleading information regarding the nature and risks of the virus, its prevention and treatment; and the development, safety, and effectiveness of COVID-19 vaccines.”
Under the bill, disciplinary action could be brought against a physician for disseminating information that “resulted in an individual declining opportunities for COVID-19 treatment or prevention that was not justified by the individual’s medical history or condition.”
Additionally, doctors could be disciplined for “misinformation or disinformation” that is contradicted by contemporary scientific consensus to an extent where its dissemination constitutes gross negligence” by the physician.
Commenting on the criteria, Dr. Meryl Nass, an expert in epidemiology and vaccine injury and member of the Children’s Health Defense scientific advisory committee, said:
“I think this is clearly an attempt to legislate that the government of California or the Medical Board of California will define what is truth and what is misinformation, and medical providers will have to follow lockstep with that definition.
“This, of course, is the same thing as the Ministry of Truth in George Orwell’s “1984,” and if the California legislature actually votes for this bill, the intent of the action will be to enforce a one and only truth.
“Nowhere does this legislature define what is misinformation and disinformation. They do talk about contemporary scientific consensus but as we know in the last two years, the so-called scientific consensus — or the public health agency consensus — on masks, on vaccination, on boosters, etc. has flip-flopped all over the place. So we have adequate examples that the concept of “contemporary scientific consensus” is basically meaningless in this context.”
Contrary to typical board practice, under AB 2098, physicians could also be disciplined for public speech, including social media posts, unrelated to the actual treatment of patients.
Supporters of Low’s bill insist the legislation does not impinge on doctors’ freedom of speech.
“This isn’t a call for a policing of free speech,” Nick Sawyer, an emergency room doctor who founded a group called No License for Disinformation, told the LA Times. “This is a call for protecting the public against dangerous misinformation, which patients are parroting back to us in our emergency room departments every day.”
Nass disagreed:
“The result is removing options from doctors and patients. And the longer-term consequence is that doctors will become irrelevant if they are not needed to assess each individual’s personal risks and benefits from each type of medical care.
“The government and its partners in the healthcare industries can simply prescribe one-size-fits-all healthcare for everyone.”
Low’s bill, introduced as part of a larger effort by a group of Democratic state legislators to strengthen vaccination laws, set off a contentious debate over how far the state should go in pursuing COVID mandates.
Other COVID-related bills introduced in California include:
- Assembly Bill 1993, authored by Buffy Wicks (D-Oakland), would require employees and independent contractors to be vaccinated against COVID as a condition of employment unless they have an exemption based on a medical condition, disability or religious beliefs.
- Assembly Bill 1797, introduced by Akilah Weber (D-San Diego), allows California school officials to more easily check student vaccine records by expanding access to a statewide immunization database.
- Senate Bill 866, introduced by Sen. Scott Wiener (D-San Francisco) would let children 12 and older be vaccinated without parental consent.
Other states pursue efforts to support alternative treatments
In contrast to California, several state legislatures are moving to provide legal support for off-label prescriptions and alternative approaches supported by physicians.
In New Hampshire, legislators last month held public hearings on a bill that would allow for over-the-counter dissemination of ivermectin at pharmacies, provided certain treatment plan requirements were met.
New Hampshire HB 1022 would permit pharmacists to dispense the ivermectin by means of a standing order entered into by licensed healthcare professionals.
Sponsors of the bill argued many healthcare workers are unable to prescribe ivermectin, either because of hospital politics or outside professional pressures.
The bill has support from Dr. Paul Marik, who traveled from Virginia to testify at the public hearing.
A former professor of medicine and chief of pulmonary and critical care medicine at Eastern Virginia Medical School, Marik sued the hospital he worked for after it banned physicians from prescribing ivermectin for COVID patients.
Marik resigned late last year in protest of the ban.
During his testimony in New Hampshire, Marik described ivermectin as “cheap, exceedingly safe and exceedingly effective.”
“If ivermectin had been promoted at the beginning of this pandemic, we would not be sitting here today,” Marik said.
Kansas lawmakers last month advanced a bill supporting the prescribing of ivermectin and hydroxychloroquine. The model legislation, also introduced in Tennessee, would require pharmacists to fill prescriptions for the off-label use of ivermectin and hydroxychloroquine.
In direct contrast to the California legislation, the Kansas bill also would mandate that doctors not be subject to disciplinary action for any “recommendation, prescription, use or opinion … related to a treatment for COVID-19, including a treatment that is not recommended or regulated by the licensing board,” Kansas Department of Health and Environment or the U.S. Food and Drug Administration.
“Such actions,” the bill states, “could not be considered unprofessional conduct.”
Kansas lawmaker Sen. Mark Steffen (R-Hutchinson) supports the bill. Steffen, an anesthesiologist, said he’s under investigation by the University of Kansas Health System with which he is affiliated for prescribing ivermectin to COVID patients.
Dr. Festus Krebs III, a physician representing the Catholic Medical Association of Kansas City, also spoke in favor of the bill:
“With ivermectin and hydroxychloroquine, we now have 76 ivermectin COVID-19 controlled studies which show 66 percent overall improvement and 57 percent decreased mortality.”
Meanwhile, in Florida, legislation that would extend protection for hospitals against patient lawsuits over COVID care sits on the desk of Gov. Ron DeSantis, awaiting signature or a veto.
And in New York, the state’s comptroller — citing the investment of the state’s public pension plan in Spotify — sent a letter to the company asking it to increase its screening of “misinformation” on their platform.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
How a false hydroxychloroquine narrative was created, and more

Meryl Nass, MD
Alliance for Human Research Protection | June 28, 2020
Below, Dr. Meryl Nass reviews a long list of corrupt practices that undermine the integrity of medical science and the practice of medicine during the current medical crisis. The coronavirus crisis has been made significantly worse by stakeholders who are preventing doctors from prescribing for their patients, existing, safe and effective medicines, because the stakeholders are invested on garnering projected future profits from not-yet-developed vaccines and “countermeasures” specifically developed against COVID-19.
The stakeholders who influence and issue medical practice guidelines, include public health officials, global public health institutions, government advisory committees, and clinical trialists who design trials to provide commercially beneficial results. Editors of prestigious high impact, medical journals contribute to the corruption of medicine by publishing fraudulent studies, and reports of clinical trials that were designed to cause foreseeable deaths, The focus of Dr. Nass’ J’Accuse post are clinical trials that deliberately subjected some patients to toxic doses of Hydroxychloroquine. [Dr. Nass is a longtime member of the AHRP Board of Directors].
These collaborators engaged in an orchestrated effort to prevent physicians from utilizing an existing, off-patent, cheap and affordable drug, that thousands of clinicians attest to its therapeutic benefit.
- The problem with Hydroxychloroquine, a drug with a 70-year safety track record, is that there is no profit to be made from this cheap, off-patent drug!
*****************
It is remarkable that a series of events taking place over the past 3 months produced a unified message about hydroxychloroquine, and produced similar policies about the drug in the US, Canada, Australia, NZ and western Europe. The message is that generic, inexpensive hydroxychloroquine is dangerous and should not be used to treat a potentially fatal disease, Covid-19, for which there are no (other) reliable treatments.
- Hydroxychloroquine had been used safely for 65 years in millions of patients. And so the message was crafted that the drug is safe for its other uses, but dangerous when used for Covid-19. It doesn’t make sense, but it seems to have worked.
Were these acts carefully orchestrated? You decide.
Might these events have been planned to keep the pandemic going? To sell expensive drugs and vaccines to a captive population? Could these acts result in prolonged economic and social hardship, eventually transferring wealth from the middle class to the very rich? Are these events evidence of a conspiracy?
Here is a list of what happened, in no special order. Please help add to this list if you know of additional acts I should include. This will be a living document. I have penned this as if it is the “to do” list of items to be carried out by those who pull the strings. The items on the list have already been carried out. One wonders what else might be on their list, yet to be carried out, for this pandemic.
1. You stop doctors from using the drug in ways it is most likely to be effective (in outpatients at onset of illness). You prohibit use outside of situations you can control.
Situations that were controlled to show no benefit included 3 large, randomized, multi-center clinical trials (Recovery, Solidarity and REMAP-Covid), which are generally believed to yield the most reliable evidence. However, each of them used excessive doses that were known to be toxic; see my previous articles here and here.
2. You prevent or limit use in outpatients by controlling the supply of the drug, using different methods in different countries and states. In NY state, by order of the governor, hydroxychloroquine could only be prescribed for hospitalized patients. France has issued a series of different regulations to limit prescribers from using it. France also changed the drugs’ status from over-the-counter to a drug requiring a prescription.
3. You play up the danger of the drug, emphasizing side effects that are very rare when the drug is used correctly. You make sure everyone has heard about the man who died after consuming hydroxychloroquine in the form of fish tank cleaner.
4. You limit clinical trials to hospitalized patients, instead of testing the drug in outpatients, early in the illness, when it is predicted to be most effective.
5. You design clinical trials to give much too high a dose, ensuring the drug will cause harm in some subjects, sufficient to mask any possible beneficial effect. You make sure that dozens of trials in dozens of countries around the world use these dangerous doses.
6. You design clinical trials to collect almost no safety data, so any cause of death due to drug toxicity will be attributed to the disease instead of the drug.
7. You issue rules for use of the drug based on the results of the unethical, overdosing Recovery study.
8. You publish, in the world’s most-read medical journal, the Lancet, an observational study from a huge worldwide database that says use of chloroquine drugs caused significantly increased mortality. You make sure that all major media report on this result. Then 3 European countries announce they will not allow doctors to prescribe the drug. And Sanofi announces it will no longer supply the drug for use with Covid, and will halt its own clinical trials, based on a fabricated study.
9. Even after hundreds of people renounce this observational study due to easily identified fabrications–which, as James Todaro, MD, wrote was a “study out of thin air“–the Lancet held firm for two weeks, serving to muddy the waters about the trial, until finally 3 of its 4 coauthors (but not the journal) retracted the study. You make sure few media report that the data were fabricated and the “study” a fraud. You let people believe the original story: that hydroxychloroquine routinely kills.
10. You ensure federal agencies like FDA and CDC hew to your desired policies. For example, FDA advised use only in hospitalized patients (too late) or in clinical trials (which are limited, are difficult to enroll in, or use excessive doses). As of mid June, FDA now advises patients and doctors to only use the drug in a clinical trial!
Another example: you have FDA make unsubstantiated and false claims, such as: “Hospitalized patients were likely to have greater prospect of benefit (compared to ambulatory patients with mild illness)” and claim the chloroquine drugs have a slow onset of action. If that were really true, they would not be used for acute attacks of malaria or in critically ill patients with Covid. (Disclosure: I once dosed myself with chloroquine for an acute attack of P. vivax malaria, and it worked very fast.). Providing no other treatment advice, CDC refers clinicians to the NIH guidelines, discussed below.
11. You make sure to avoid funding/encouraging clinical trials that test drug combinations like hydroxychloroquine with zinc, with azithromycin, or with both, although there is ample clinical evidence that such combinations provide a cumulative benefit to patients.
12. You have federal and UN agencies make false, illogical claims based on models rather than human data. For example, you have the FDA state on June 15 that the dose required to treat Covid is so high it is toxic, after the Recovery and Solidarity trials have been exposed for toxic dosing. This scientific double-speak gives some legal cover to the clinical trials that overdosed their patients.
According to Denise Hinton, RN, the FDA’s Chief Scientist, or a clumsy FDA wordsmith:
”Under the assumption that in vivo cellular accumulation is similar to that from the in vitro cell-based assays, the calculated free lung concentrations that would result from the EUA suggested dosing regimens are well below the in vitro EC50/EC90 values, making the antiviral effect against SARS-CoV-2 not likely achievable with the dosing regimens recommended in the EUA. The substantial increase in dosing that would be needed to increase the likelihood of an antiviral effect would not be acceptable due to toxicity concerns.”
13. You have a WHO report claim toxic doses are needed. This of course is nonsense since
a) CDC researchers showed strong effects against SARS-1 at safely achievable concentrations,
b) the drug at normal doses is being tested in over 30 different medical conditions (see clinicaltrials.gov), and
c) reports from many different countries say that the drug is effective for Covid-19 at normal doses, while
a high dose chloroquine treatment arm was halted in Brazil and a preprint of the study was posted April 11, after finding the toxic effects were causing ventricular arrhythmias and deaths.
- Toxicity was noted after only 3 days of treatment, during which 3.6 grams of chloroquine were administered. But the Solidarity (3.2 grams of hydroxychloroquine in 3 days), Recovery (3.6 grams of hydroxychloroquine in 3 days) and REMAP-Covid trials (3.6 grams of hydroxychloroquine in 3 days) continued overdoing patients until June, despite Brazil’s evidence of deaths by overdose.
- Tellingly, JAMA editor Gordon Rubenfeld wrote about the Brazilian study, “if you are prescribing HCQ after these JAMA results, do yourself and your defense lawyer a favor. Document in your medical record that you informed the patient of the potential risks of HCQ including sudden death and its benefits (???).”
14. You create an NIH Guideline committee for Covid treatment recommendations, in which 16 members have or had financial entanglements with Gilead, maker of Remdesivir. The members were appointed by the CoChairs. Two of the three CoChairs are themselves financially entangled with Gilead. Are you surprised that their guidelines recommend specifically against the use of hydroxychloroquine and in favor of Remdesivir, and that they deem this the new “standard of care”?
15. You frighten doctors so they don’t prescribe hydroxychloroquine, if prescribing it is even allowed in their jurisdiction, because prescribing outside the “standard of care” leaves them open to malpractice lawsuits. You further tell them (through the FDA) they need to monitor a variety of lab parameters and EKG when using the drug, although this was never advised before, which makes it very difficult to use the drug in outpatients. You have the European Medicines Agency issue similar warnings.
16. You manage to control the conduct of most trials around the world by designing the WHO-managed Solidarity trials, currently conducted in 35 countries. WHO halted hydroxychloroquine clinical trials around the world, twice.
The first time, May 25, WHO claimed it was in response to the (fraudulent) Lancet study.
The second time, June 17, WHO claimed the stop was in response to the Recovery trial results.
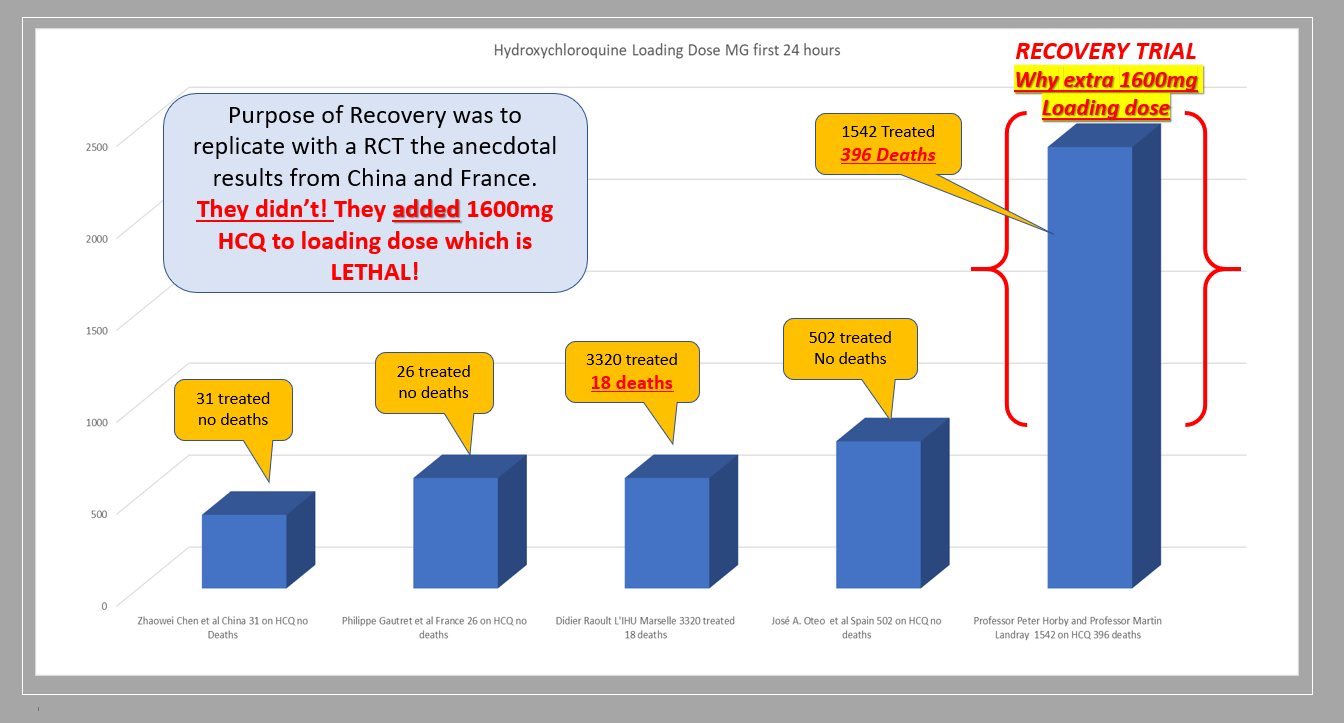
Recovery used highly toxic doses of hydroxychloroquine in over 1500 patients, of whom 396 died.
You stop the trial before the data safety monitoring board has looked at your data, a move that is unlikely to be consistent with trial protocol. WHO’s trial in over 400 hospitals overdosed patients with 2.0 g hydroxychloroquine in the first 24 hours.
WHO’s trial in over 400 hospitals was unlikely to provide useful results, as it too overdosed patients with hydroxychloroquine. The trial was halted days after the toxic doses were exposed.
17. You have the WHO pressure governments to stop doctors prescribing hydroxychloroquine.
18. You have the WHO pressure professional societies to stop doctors prescribing hydroxychloroquine.
19. You make sure that the most-consulted medical encyclopedia, UptoDate, provides bad guidance to physicians, advising them to restrict hydroxychloroquine to only patients in clinical trials, citing the above sources of information.

Anthony Fauci, MD
20. You have the head of the Coronavirus Task Force, Dr. Tony Fauci, insist the drug cannot be used in the absence of strong evidence… while he insisted exactly the opposite in the case of the MERS coronavirus outbreak several years ago, when he recommended an untested drug combination for use… which had been developed for that purpose by his agency.
And while he was bemoaning the lack of evidence, he was refusing to pay for trials to study hydroxychloroquine. And he was changing the goalposts on the Remdesivir trial, not once but twice, to make Remdesivir show just a tiny bit of benefit, but no mortality benefit. And don’t forget, Fauci was thrilled to sponsor a trial of a Covid vaccine in humans before there was any data from animal trials. So much for requiring high quality evidence before risking use of drugs and vaccines in humans!
21. You convince the public that the crisis will be long-lasting. You have the 2nd richest man in the world, and biggest funder of the WHO, Bill Gates, keep repeating to the media megaphone that we cannot go back to normal until there is a vaccine. (The Gates Foundation helped design the WHO clinical trials, and Gates is heavily invested in pharmaceuticals and vaccines.)

Bill Gates
- You have CDC (with help from FDA) prevent the purchase of coronavirus test kits from Germany, China, WHO, etc, and fail to produce a valid test kit themselves. The result was that during January and February, US cases could not be reliably identified, and for several months thereafter insufficient and unreliable test kits made it impossible to track the epidemic and stop the spread.
- You have trusted medical spokesmen lie to the public about the pandemic’s severity, so precautions weren’t taken when they might have been more effective and less long-lasting. Congress was repeatedly briefed about the pandemic in January and February, which scared several Congress members enough that they sold off large amounts of stock, risking insider trading charges. Senator Burr is one of them, currently under investigation for major stock sales on February 13.
Yet Dr. Fauci told USA Today on February 17 that Americans should worry more about the flu than about coronavirus, the danger of which was “just miniscule.” Then on February 28, Drs. Fauci and Robert Redfield (CDC Director) wrote in the New England Journal :
“… the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively.”
 You destroy the reputation of respected physicians who stand in your way. Professor Didier Raoult and his team in Marseille have used hydroxychloroquine on over 4,000 patients, reporting a mortality rate of about 0.8%. (The mortality rate of patients given hydroxychloroquine in the Recovery trial was 25.7%.) Raoult is very famous for discovering over 100 different microorganisms, and finding the long-sought cause of Whipple’s Disease. With this reputation, Raoult apparently thought he could treat patients as he saw fit, which he has done, under great duress. Raoult was featured in a New York Times Magazine article, with his photo on the cover, May 12, 2020. After describing his accomplishments, the Times very unfavorably discussed his personality, producing a detailed hit piece. He is now considered an unreliable crank in the US.
You destroy the reputation of respected physicians who stand in your way. Professor Didier Raoult and his team in Marseille have used hydroxychloroquine on over 4,000 patients, reporting a mortality rate of about 0.8%. (The mortality rate of patients given hydroxychloroquine in the Recovery trial was 25.7%.) Raoult is very famous for discovering over 100 different microorganisms, and finding the long-sought cause of Whipple’s Disease. With this reputation, Raoult apparently thought he could treat patients as he saw fit, which he has done, under great duress. Raoult was featured in a New York Times Magazine article, with his photo on the cover, May 12, 2020. After describing his accomplishments, the Times very unfavorably discussed his personality, producing a detailed hit piece. He is now considered an unreliable crank in the US.
- You have social media platforms ban content that does not agree with the desired narrative. As YouTube CEO and ex-wife of Google founder Sergey Brin, Susan Wojcicki said,
“YouTube will ban any content containing medical advice that contradicts World Health Organisation (WHO) coronavirus recommendations. Anything that would go against World Health Organisation recommendations would be a violation of our policy.”
- When your clinical trials are criticized for overdosing patients, you have Oxford-affiliated, Wellcome Trust-supported scientists at Mahidol University publish papers (a literature review with modeling and a modeling study) purporting to show that the doses used were not toxic. You develop a new method to measure hydroxychloroquine in a handful of Recovery patients who were not poisoned. However, there are 2 problems you forgot with this approach:
- The Brazilian data, including 16 deaths, extensive clinical information and documented ventricular arrhythmias, are much more valuable than theoretical models of what might be happening in the body.
- Either the drug is too toxic to use for a life-threatening disease, or even extremely high doses are safe. You can’t have it both ways.
Oxford is the institution running the Recovery trial, and invented a Covid vaccine that already has 400 million doses on order. The Wellcome Trust funded the Recovery trial.
- You change your trial’s primary outcome measures after the trials have started, in order to prevent detection of drug-induced deaths (Recovery) or to make your drug appear to have efficacy (NIAID Remdesivir trial).
- You stop manufacturers from supplying the drug. Shortly after the fraudulent Lancet paper came out, Sanofi announced it would no longer supply the drug for use with Covid, and would halt its two hydroxychloroquine clinical trials. One of the cancelled Sanofi trials was expected to test 210 outpatients early in the course of disease. The trial remains suspended at the time of writing, while the Lancet paper was retracted 13 days after publication.
- You surely don’t want a trial of hydroxychloroquine treatment early in the disease, since it might show an excellent effect.
Oklahoma AG declares medical boards can’t punish doctor for prescribing ivermectin
LifeSiteNews | February 16, 2022
OKLAHOMA CITY – Doctors in Oklahoma are well within their professional rights to prescribe ivermectin (IVM) and hydroxychloroquine (HCQ) to COVID-19 patients, state Attorney General John O’Connor affirmed, despite the drugs’ disfavored status within the federal health bureaucracy.
“The Attorney General’s office finds no legal basis for a state medical licensure board to discipline a licensed physician for exercising sound judgment and safely prescribing an FDA-approved drug – like ivermectin or hydroxychloroquine – for the off-label purpose of treating a patient with COVID-19,” O’Connor’s office concluded in a February 8 statement, declaring that “healthcare professionals should have every tool available to combat COVID-19.”
“The Attorney General’s office neither condones nor condemns a specific course of treatment for COVID-19,” the release added. “Our office maintains that proper healthcare decisions are to be made between a patient and his or her physician, and the government should not interfere with their relationship.”
Despite being misrepresented in the mainstream media as aquarium cleaner and horse dewormer, respectively, hydroxychloroquine and ivermectin are both FDA-approved medications with a range of human applications, such that both are listed on the World Health Organization’s Model List of Essential Medicines. Like many medications, ivermectin is also used for horses, but human dosages of the drug for human ailments were not controversial until IVM started gaining notice in the context of COVID-19.
While experts continue to debate the drugs’ effectiveness at treating COVID-19, promising studies as well as reports of positive results have generated significant interest in them, as has the fact that they have been used and studied for far longer than the COVID-19 vaccines, which were developed and released in record time by the Trump administration’s Operation Warp Speed initiative. Many believe the long-established drugs are safer than relatively new vaccines they believe have been rushed and politicized.
Despite the established safety of IVM and HCQ, and the evolving nature of COVID knowledge, families across the country have had to go to court to force hospitals to let them try the drugs for their loved ones, while doctors have seen their medical licenses threatened for prescribing them – a scenario the Oklahoma Attorney General’s Office indicates will not be tolerated in the Sooner State.
The University of Minnesota, Emory University School of Medicine, Northwestern Medicine, and other medical institutions are currently conducting a major at-home clinical trial to assess ivermectin’s effectiveness at treating COVID-19, as well as that of the drugs metformin and fluvoxamine or any combination of the three.
Nebraska AG Says Doctors Can Legally Prescribe Ivermectin, HCQ for COVID, Calls Out FDA, CDC, Fauci, Media for ‘Fueling Confusion and Misinformation’
By Megan Redshaw | The Defender | October 18, 2021
Few subjects have been more controversial than ivermectin and hydroxychloroquine — two long-established, inexpensive medications widely and successfully used in many parts of the world for the prevention and treatment of COVID.
By contrast, the use of both medications against COVID has been largely suppressed in the U.S, where doctors have been threatened and punished for prescribing them.
On Oct. 15, Nebraska Attorney General (AG) Doug Peterson issued a legal opinion that Nebraska healthcare providers can legally prescribe off-label medications like ivermectin and hydroxychloroquine for the treatment of COVID, so long as they obtain informed consent from the patient.
However, if they did neglect to obtain consent, deceive, prescribe excessively high doses or other misconduct, they could be subject to discipline, Peterson wrote.
The AG’s office emphasized it was not recommending any specific treatment for COVID. “That is not our role,” Peterson wrote. “Rather, we address only the off-label early treatment options discussed in this opinion and conclude that the available evidence suggests they might work for some people.”
Peterson said allowing physicians to consider early treatments will free them to evaluate additional tools that could save lives, keep patients out of the hospital and provide relief for our already strained healthcare system.
The opinion, based on an assessment of relevant scientific literature, was rendered in response to a request by Dannette Smith, CEO of the Nebraska Department of Health and Human Services.
Smith asked the AG’s office to look into whether doctors could face discipline or legal action under Nebraska’s Uniform Credential Act (UCA) — meant to protect public health, safety and welfare — if they prescribed ivermectin or hydroxychloroquine.
“After receiving your question and conducting our investigation, we have found significant controversy and suspect information about potential COVID-19 treatments,” Peterson wrote.
For example, a paper published in the Lancet — one of the most prestigious medical journals in the world — denounced hydroxychloroquine as dangerous, yet the statistics were flawed and the authors refused to provide analyzed data.
The paper was retracted, but not before countries stopped using the drug and trials were cancelled or interrupted.
“The Lancet’s own editor-in-chief admitted that the paper was a ‘fabrication,’ a ‘monumental fraud’ and a ‘shocking example of research misconduct’ in the middle of a global health emergency,” Peterson wrote in the opinion.
A recently published paper on COVID recognized that “for reasons that are yet to be clarified,” early treatment has not been emphasized despite numerous U.S. healthcare providers advocating for early treatment and “scores of treating and academic physicians” — who have published papers in well respected journals — urging early interventions.
Peterson cited numerous studies showing ivermectin and hydroxychloroquine reduced mortality by up to 75% or more when used as a preventative or prophylaxis for COVID, suggesting hundreds of thousands of lives could have been saved had the drugs been widely used in America.
“Every citizen — Democrat or Republican — should be grateful for Doug Peterson’s thoughtful and courageous counteroffensive against the efforts of Big Pharma, its captive federal regulators, and its media and social media allies to silence doctors and deny Americans life-saving treatments,” Robert F. Kennedy Jr., chairman of Children’s Health Defense, told The Defender via email.
“We finally have a leader who puts constitutional rights, peer-reviewed science and human health above industry profits. Doug Peterson is uncowed and unbowed — a genuine hero on horseback for all Americans.” Kennedy said.
Children’s Health Defense President Mary Holland agreed. “This Nebraska AG opinion lets doctors get back to being doctors — without being second-guessed by government, pharmacists and others interfering in the crucial doctor-patient relationship,” Holland said.
Although the AG’s office did not rule out the possibility that other off-label drugs might show promise — either now or in the future — as a prophylaxis or treatment against COVID, it confined its opinion to ivermectin and hydroxychloroquine for the sake of brevity.
Nebraska AG highlights science on ivermectin
In his legal opinion, Peterson concluded evidence showed ivermectin demonstrated striking effectiveness in preventing and treating COVID, and any side effects were primarily minor and transient. “Thus, the UCA does not preclude physicians from considering ivermectin for the prevention or treatment of COVID,” Peterson wrote.
In the decade leading up to the COVID pandemic, Peterson found numerous studies showing ivermectin’s antiviral activity against several RNA viruses by blocking the nuclear trafficking of viral proteins, adding to 50 years of research confirming ivermectin’s antiviral effects.
In addition, safety data for ivermectin showed side effects were “vanishingly small.” The latest statistics available through VigiAccess reported only 5,674 adverse drug reactions to ivermectin between 1992 and October 13, 2021, an “incredibly low” number given that 3.7 billion doses have been administered since the 1980s, Peterson wrote.
Peterson cited several studies showing ivermectin led to improvement of COVID outcomes when used in early treatment or as a prophylaxis, while noting many studies with negative findings about ivermectin “excluded most available evidence,” cherry picked data within studies, misreported data, made unsupported assertions of adverse reactions to ivermectin and had “conclusions that did follow from evidence.”
Peterson also found that epidemiological evidence for ivermectin’s effectiveness, derived by analyzing COVID-related data from various states, countries or regions is instructive in the context of a global pandemic.
In one instance, a group of scholars analyzed data comparing COVID rates of countries that routinely administer ivermectin as a prophylaxis and countries that did not. The research showed “countries with routine mass drug administration of prophylactic … ivermectin have a significantly lower incidence of COVID-19.”
“This ‘highly significant’ correlation manifests itself not only ‘in a worldwide context’ but also when comparing African countries that regularly administer prophylactic ‘ivermectin against parasitic infections’ and African countries that do not,” Peterson wrote. “Based on these results, the researchers surmised that these results may be connected to ivermectin’s ability to inhibit SARS-CoV-2 replication, which likely leads to lower infection rates.”
Nebraska AG calls out FDA, Fauci on hypocrisy on ivermectin
Many U.S. health agencies have now addressed the use of ivermectin for COVID. The National Institutes of Health (NIH) has adopted a neutral position, choosing not to recommend for or against the use of ivermectin — a change from its position in January 2021 where it discouraged use of the drug for treatment of COVID.
Peterson wrote:
“The reason for the change is the NIH recognized several randomized trials and retrospective cohort studies of ivermectin use in patients with COVID-19 have been published in peer-reviewed journals. And some of those studies reported positive outcomes, including shorter time to resolution of disease manifestations that were attributed to COVID-19, greater reduction in inflammatory marker levels, shorter time to viral clearance, [and] lower mortality rates in patients who received ivermectin than in patients who received comparator drugs or placebo.”
Yet, on Aug. 29, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases within the NIH, went on CNN and announced “there is no clinical evidence” that ivermectin works for the prevention or treatment of COVID. Fauci went on to reiterate that “there is no evidence whatsoever” that it works.
“This definitive claim directly contradicts the NIH’s recognition that ‘several randomized trials … published in peer-reviewed journals’ have reported data indicating that ivermectin is effective as a COVI D-19 treatment,” Peterson wrote.
In March 2021, the FDA posted a webpage, “Why You Should Not Use lvermectin to Treat or Prevent COVID-19.”
“Although the FDA’s concern was stories of some people using the animal form of ivermectin or excessive doses of the human form, the title broadly condemned any use of ivermectin in connection with COVID-19,” Peterson wrote. “Yet, there was no basis for its sweeping condemnation.”
Peterson wrote:
“Indeed, the FDA itself acknowledged on that very webpage (and continued to do so until the page changed on September 3, 2021) that the agency had not even ‘reviewed data to support use of ivermectin in COVID-19 patients to treat or to prevent COVID-19.’ But without reviewing the available data, which had long since been available and accumulating, it is unclear what basis the FDA had for denouncing ivermectin as a treatment or prophylaxis for COVID-19.
“On that same webpage, the FDA also declared that ‘[i]vermectin is not an anti-viral (a drug for treating viruses).’ It did so while another one of its webpages simultaneously cited a study in Antiviral Research that identified ivermectin as a medicine ‘previously shown to have broad-spectrum anti-viral activity.’”
“It is telling that the FDA deleted the line about ivermectin not being ‘anti-viral’ when it amended the first webpage on September 3, 2021,” Peterson noted.
Peterson said the FDA’s most controversial statement on ivermectin was made on Aug. 21, when it posted a link on Twitter to its “Why You Should Not Use lvermectin” webpage with this statement: “You are not a horse. You are not a cow. Seriously, y’all. Stop it.”
“This message is troubling not only because it makes light of a serious matter but also because it inaccurately implies that ivermectin is only for horses or cows,” Peterson wrote.
Peterson said the FDA has assailed ivermectin’s safety while ignoring the fact that physicians routinely prescribe medications for off-label use and that ivermectin is a “particularly well-tolerated medicine with an established safety record.”
Peterson added the FDA is ignoring several randomized controlled trials and at least one metaanalysis suggesting ivermectin is effective against COVID. He pointed out the Centers of Disease Control and Prevention has adopted a similar stance — unsupported by scientific evidence — and the media has fueled confusion and misinformation on the drug.
Peterson questions professional associations’ stance on ivermectin
Professional associations in the U.S. and internationally have adopted conflicting positions on ivermectin and COVID. The American Medical Association (AMA), American Pharmacists Association (APhA) and American Society of Health-System Pharmacists (ASHP) issued a statement in September strongly opposing the ordering, prescribing or dispensing of ivermectin to prevent or treat COVID outside of a clinical trial.
But their statement relied solely on the FDA’s and CDC’s suspect positions.
The AMA, APhA and ASHP also mentioned a statement by Merck — the original patent-holder — opposing the use of ivermectin for COVID because of a “concerning lack of safety data in the majority of studies.”
“But Merck, of all sources, knows that ivermectin is exceedingly safe, so the absence of safety data in recent studies should not be concerning to the company,” Peterson wrote.
Peterson called into question the objectivity of Merck in providing an opinion on ivermectin that U.S. health agencies are relying upon. “Why would ivermectin’s original patent holder go out of its way to question this medicine by creating the impression that it might not be safe?” Peterson asked. “There are at least two plausible reasons.”
Peterson explained:
“First, ivermectin is no longer under patent, so Merck does not profit from it anymore. That likely explains why Merck declined to ‘conduct clinical trials’ on ivermectin and COVID-19 when given the chance.
“Second, Merck has a significant financial interest in the medical profession rejecting ivermectin as an early treatment for COVID-19. [T]he U.S. government has agreed to pay [Merck] about $1.2 billion for 1.7 million courses of its experimental COVID-19 treatment, if it is proven to work in an ongoing large trial and authorized by U.S. regulators.”
Merck’s treatment is known as “molnupiravir,” and aims to stop COVID from progressing when given early in the course of disease. When Merck announced Oct. 1, that preliminary studies indicated molnupiravir reduced hospitalizations and deaths by half, the drug maker’s stock price immediately jumped to 12.3%.
“Thus, if low-cost ivermectin works better than, or even the same as molnupiravir, that could cost Merck billions of dollars,” Peterson wrote.
Peterson takes on science of hydroxychloroquine
Peterson said based on his review of the evidence, his office did not find clear and convincing evidence that would warrant disciplining physicians who prescribe hydroxychloroquine for the prevention or early treatment of COVID after first obtaining informed patient consent.
Peterson pointed to similar findings with hydroxychloroquine — a less toxic derivative of a medicine named chloroquine — widely used since it was approved by the FDA in 1955 for treatment of malaria.
Peterson noted that as early as 2004, a lab study revealed chloroquine was “an effective inhibitor of the replication of the severe acute respiratory syndrome coronavirus (SARS-CoV) in vitro” and should “be considered for immediate use in the prevention and treatment of SARS-CoV infections.”
In 2005, another study showed chloroquine had strong antiviral effects on SARS-CoV infection and was effective in preventing the spread of SARS-CoV in cell cultures.
Other studies showed hydroxychloroquine exhibited antiviral properties that can inhibit SARS-CoV-2 virus entry, transmission and replication, and contains anti-inflammatory properties that help regulate pro-inflammatory cytokines.
Peterson wrote, “many large observational studies suggest that hydroxychloroquine significantly reduces the risk of hospitalization and death when administered to particularly high-risk outpatients as part of early COVID-19 treatment.”
Peterson said the drug is considered to be so safe it can be prescribed for pregnant women, yet during the pandemic, the FDA raised questions about hydroxychloroquine and adverse cardiac events.
These concerns prompted one group of researchers to conduct a systematic review of the hydroxychloroquine safety literature pre-COVID. Their review indicated people taking hydroxychloroquine in appropriate doses “are at very low risk of experiencing cardiac [adverse events], particularly with short-term administration” of the drug.
Researchers noted COVID itself can cause cardiac problems, and there was no reason “to think the medication itself had changed after 70 years of widespread use,” Peterson wrote.
Peterson said one piece of key flawed data had substantially contributed to safety concerns surrounding the drug — the admittedly fraudulent Lancet study that falsely claimed hydroxychloroquine increased frequency of ventricular arrhythmias when used for treatment of COVID.
The findings were so startling that major drug trials involving hydroxychloroquine “were immediately halted” and the World Health Organization pressured countries like Indonesia that were widely using hydroxychloroquine to ban it. Some countries, including France, Italy and Belgium, stopped using it for COVID altogether.
Peterson wrote:
“The problem, however, is that the study was based on false data from a company named Surgisphere, whose founder and CEO Sapan Desai was a co-author on the published paper.
“The data were so obviously flawed that journalists and outside researchers began raising concerns within days of the paper’s publication. Even the Lancet’s editor in chief, Dr. Richard Horton, admitted that the paper was a fabrication, a monumental fraud and a shocking example of research misconduct in the middle of a global health emergency.”
Despite calls for the Lancet to provide a full expansion of what happened, the publication declined to provide details for the retraction.
As with ivermectin, the FDA and NIH adopted positions against the use of hydroxychloroquine for COVID — making assertions that were unsupported by data. The AMA, APhA and ASHP, which opposed ivermectin, also resisted hydroxychloroquine for the treatment of COVID.
By contrast, the Association of American Physicians and Surgeons, and other physician groups, support the use of both ivermectin and hydroxychloroquine as an early treatment option for COVID. Peterson cited an article co-authored by more than 50 doctors in Reviews in Cardiovascular Medicine who advocated an early treatment protocol that includes hydroxychloroquine as a key component.
Governing law allows physicians to prescribe ivermectin and hydroxychloroquine, AG says
Neb. Rev. Stat. § 38-179 generally defines unprofessional conduct as a “departure from or failure to conform to the standards of acceptable and prevailing practice of a profession or the ethics of the profession, regardless of whether a person, consumer or entity is injured, or conduct that is likely to deceive or defraud the public or is detrimental to the public interest.”
The regulation governing physicians states that unprofessional conduct includes:
“[c]onduct or practice outside the normal standard of care in the State of Nebraska which is or might be harmful or dangerous to the health of the patient or the public, not to include a single act of ordinary negligence.”
Peterson said healthcare providers do not violate the standard of care when they choose between two reasonable approaches to medicine.
“Regulations also indicate that physicians may utilize reasonable investigative or unproven therapies that reflect a reasonable approach to medicine so long as physicians obtain written informed patient consent,” Peterson wrote.
“Informed consent concerns a doctor’s duty to inform his or her patient, and it includes telling patients about the nature of the pertinent ailment or condition, the risks of the proposed treatment or procedure and the risks of any alternative methods of treatment, including the risks of failing to undergo any treatment at all.”
Peterson said this applies to prescribing medicine for purposes other than uses approved by the FDA, and that doing so falls within the standard of care repeatedly recognized by the courts.
Peterson said the U.S. Supreme Court has also affirmed that “off-label usage of medical devices” is an “accepted and necessary” practice, and the FDA has held the position for decades that “a physician may prescribe [a drug] for uses or in treatment regimens or patient populations that are not included in approved labeling.”
Peterson said the FDA has stated “healthcare providers generally may prescribe [a] drug for an unapproved use when they judge that it is medically appropriate for their patient, and nothing in the federal Food, Drug and Cosmetic Act (“FDCA”) limit[s] the manner in which a physician may use an approved drug.”
In a statement to KETV NewsWatch 7, Nebraska’s Department of Health and Human Services said:
“The Department of Health and Human Services appreciates the AG’s office delivering an opinion on this matter. The document is posted and available to medical providers as they determine appropriate course of treatment for their patients.”
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Covid Medical insanity, as described by an MD
By Matt Bettag, MD | August 6, 2021
When did the world become insane? What is the reason for it? Big Brother? Depopulation? Or people in love with control?
I don’t know and it’s driving me nuts. But I’ve decided I’m tired of complaining about it to my friends and family and I’m willing to put my name on the line. If the woke culture wants to ruin me for speaking the truth, I guess I might as well just get it over with now.
I have been a physician for 24 years, a practicing ENT for 19 years. I have never before seen the medical establishment just stop thinking. Insanity is the new rule, and common sense cannot even be discussed.
From the beginning, 15 days to “flatten the curve,” I was shocked. We had never done this before, but perhaps this virus was really bad, so I gave the government the benefit of the doubt.
Then came Fauci.
He initially said social distancing didn’t work, and masks were largely ineffective.
But by late March, he pronounced both masking and social distancing necessary. Weird… red flag.
What? So now I am alarmed.
I started researching the utility of masks. There were very good articles I found — one out of a respiratory center in Chicago, and another a good dental review. I bookmarked both of them. Less than a month later, the dental website was down, replaced by a text saying basically that their information is now irrelevant because of COVID. The Chicago article also had a disclaimer that previously wasn’t there saying people shouldn’t use their article politically. What? Don’t use a scientifically derived article to make a scientifically based decision on the utility of masks? What the hell is going on?
Next comes PCR testing. Let’s conveniently jack up the PCR Magnification cycles to 40+, resulting in a 90–97% false positive rate.
Then, let’s start testing all elective surgery, asymptomatic exposures, and hospitalized patients with this fake test to artificially increase the Covid numbers.
In addition we will reimburse hospitals greatly for any diagnosed COVID admissions and ICU visits.
Oxygen doesn’t work; go home until you get worse. Oh, and bring your family and friends with you; they’ll need testing.
Steroids were advised against early on, which made no sense, because they do decrease inflammation and in ENT have been used widely for viral illness.
Next we find a few weeks later the secret drug to treat COVID: steroids. What?
Hydroxychloroquine HCQ—suddenly not safe, even though it has been used for decades worldwide with a great safety profile, but not anymore. Mention it, and you are a lunatic.
The same went for all other proven therapeutics, such as ivermectin and vitamin D.
Vaccines? “I wouldn’t trust anything president Trump made.” That was Kamala Harris back in the fall.
Now if you don’t get vaccinated, you don’t care about other people, and you wanna watch people die.
Oh, and by the way, we should vaccinate everyone, including those who previously had COVID, pregnant women, and small children.
What about VAERS? That’s the open record report system that the CDC has made almost unnavigable. It’s slowly crept up and showed up to 12,000 deaths coincident with the vaccine. Then dropped to 6,000, only to come back up to 10,000 and now back to 12,000–Just a little glitch from our trustworthy government.
There are reports that the numbers could be ten times or more as high, and perhaps the CDC is misclassifying deaths to hide them. But let’s trust the government; they’ve been so good thus far.
Now the latest lie: “the delta variant, is surging because of the unvaccinated.”
Ignore the data from other countries that have very high vaccine rates but high spiking cases, and ignore the data from other countries that have low vaccine rates and almost no COVID.
As a matter fact, let’s not even look at Sweden, who essentially didn’t do lockdowns or masking, has a low vaccination rate, and has almost zero COVID.
I have never lived in the world like this, where open medical dialogue is completely suppressed and there is only one party line.
I thought the left was always talking about how we shouldn’t bully people, and we need to have “dialogue.” Well… let’s start.
The media and the government need to do their job and start opening dialogue to the other side. If we are crazy, it will come out.
If we are right, and the data show that to be the fact, then a large apology is warranted.
Dr. Stella Immanuel sues CNN for $100 Million after being vindicated on Hydroxychloroquine
Big League Politics | July 31, 2021
Dr. Stella Immanuel, the pro-hydroxychloroquine doctor who was derided by the fake news media for attempting to save lives near the peak of the COVID-19 pandemic, is striking back against CNN.
Immanuel has launched a $100 million lawsuit against CNN and host Anderson Cooper for what she believes were false and defamatory statements made against her character.
“In an effort to vilify, demonize and embarrass President [Donald] Trump, Cooper and CNN published a series of statements of fact about Dr. Immanuel that injured her reputation and exposed her to public hatred, contempt, ridicule, and financial injury,” the lawsuit stated. It was filed in federal court on July 27.
Immanuel said that she believes Cooper and CNN “effectively caused the deaths of hundreds of thousands whose lives would have been spared if they had been treated early with HCQ.”
Big League Politics has reported on the suppressed science showing that hydroxychloroquine can effectively treat COVID-19:
“A new study has demonstrated that treating COVID-19 with hydroxychloroquine makes patients 84 percent less likely to be hospitalized.
The study is set to be published in the International Journal of Antimicrobial Agents in December. It has determined that “low-dose hydroxychloroquine combined with zinc and azithromycin was an effective therapeutic approach against COVID-19.”
The doctors came to their conclusions after treating 141 coronavirus patients with hydroxychloroquine for five days. They compared them with a control group of 377 coronavirus patients who did not receive hydroxychloroquine as a treatment. They found that “the odds of hospitalization of treated patients was 84% less than in the untreated patients.” Only one patient from the group treated with hydroxychloroquine died while 13 people died in the other group…
The elites are suppressing hydroxychloroquine because they want the public to feel helpless against the virus. They never intend to give the public their liberties back, hoping that the public will accept a “new normal” of globalism and technocracy.“
A victory for Immanuel in court would be a powerful rebuke to the propaganda machine set up to maximize profits for Big Pharma and demonize whistleblowers who actually want to help patients.
Featured Video
Drone Strike on Egypt, War Widens /Lt Col Daniel Davis & Matt Bracken
or go to
Aletho News Archives – Video-Images
From the Archives
Israel’s threat of nukes shows us who is running U.S. foreign policy
By Martin Jay | Strategic Culture Foundation | November 27, 2025
It is a long-debated subject. Whether it is the U.S. which controls Israel or the other way around. In the 70s, under President Nixon, many analysts firmly believed, despite the JFK assassination, that it was still the U.S. who called the shots and used Israel as a useful tool in the Middle East to keep a rowdy group of Arab states in check and subservient to America’s interests. But it is in recent years where we have to see if Israel has done that effectively and meticulously in America’s interests, given that most analysts agree that Israel and the U.S. are both preparing for war with Iran.
Given that Israel’s main task was to keep the region in order to serve America’s hegemony and its energy needs, one has to ask isn’t it a failure of both U.S. foreign policy and of Israel that a war with Iran is seen as a solution to America’s failing hegemony? And doesn’t this tail wagging the dog scenario show itself in the clear light once and for all? … continue
Blog Roll
 Aletho News
Aletho News- Drone Strike on Egypt, War Widens /Lt Col Daniel Davis & Matt Bracken
- Pfizer Freezes Air Traffic Control Funds Over COVID Vaccine Contract Dispute With Poland, Romania
- Mafia buying up some of 800,000 weapons missing from Ukraine – Italian prosecutors
- NATO deploys Italian, Spanish, Turkish jets to eastern flank
- From Tehran to Riyadh: How Israel Draws the Red Lines America Can’t Cross
- Iran warns Bulgaria against hosting US warplanes, secures assurances from Cyprus on base neutrality
- Leaked: How Britain exploits US Empire
- Ukraine’s ‘turned tide’ doesn’t comport ‘with basic military reality’
- How NIH Silenced Its Critics Without Telling Them
- American journalist reveals role of Jolani regime’s Washington envoy in her 2016 kidnapping
- If Americans Knew
- Israeli Media: Israel’s Defense Chief Is Enabling Jewish Terror: 2 Articles
- Why the New York Times story on Mossad recruiting Ahmadinejad doesn’t add up
- The Facts on ICC’s Karim Khan’s Dismissal after Court’s Arrest Warrant for Netanyahu
- By 22-Point Margin, Americans Think Netanyahu Should Be Arrested on US Soil
- What an Israeli settler pogrom feels like
- As Gaza draws closer to possible ceasefire, Netanyahu draws closer to Trump – Daily Update
- Zelensky’s big idea for Trump: Ukraine is the Israel of Europe
- In Michigan’s Primary, Abdul El-Sayed Puts AIPAC on the Ballot
- Trump and Netanyahu’s Meetings: A Trail of Broken Promises
- ‘A disaster for America First’: Trump allies fear Netanyahu meeting will pull US deeper into war with Iran
- No Tricks Zone
- ECMWF Models Throwing Cold Water On Extreme Germany Heat Wave Forecast Next Week
- Greenland’s Ice Sheet Was Supposed To Be Rapidly Melting Away. It Hasn’t Been.
- Global Temperature Trend Has Cooled Over The Past 6500 Years, Scientists Have Found
- Wind Energy Means Going Back To The Middle Ages, Says German Professor Horst-Joachim Lüdecke
- New Study: A 40-Fold Increase In Earth’s Main Greenhouse Gas Contributes To Cooling The Ocean
- New Study Highlights The ‘Dominant Role’ Of Aerosol/Cloud Interactions In Shaping Climate
- Munich’s First-Ever Green Party Mayor Declares First Ever City Water Use Restrictions… Fines Up to 50,000 €!
- Experimental Lab Research: The Climate Sensitivity To A 400-Fold Increase In CO2 Is 0.1°C
- Fatal Snobbery: In France, It’s Better To Die From A Heatwave Than To Do As Americans
- New Study: NASA’s Models Wildly Underestimate The Capacity Of Clouds To Alter Solar Radiation
