This is literally ‘hot off the ‘presses’: Austrian alternative media outlet Der Status published leaked documents from the Austrian Chamber of Physicians (Ärztekammer ) that show, beyond reasonable doubt, the grand conspiracy between government, the Chamber, and its protagonists.
Without much further ado, here’s my translation; as always, emphases and bottom lines mine. The below text has been lightly edited for clarity.
Scandal! Medical Association Ordered Experts & Doctors to Recommend Vaccination
The Austrian Medical Association, under the ousted red [i.e., Social-Democratic] president Szekeres and its current president Steinhart, worked closely with the Health Ministers for years. And in doing so, it betrayed the interests of doctors. [to say nothing about patients]
Spring 2020: Collaboration with the Politicians Commences
In April 2020, Szekeres, Steinhart, and Minister Anschober [Greens, since retired] signed a ‘Memorandum of Understanding Concerning COVID-19 Vaccinations’. That is, at a time—more than half a year—before the conditional approval of these injectable products, this Memorandum dealt with, among other things, advertising campaigns by doctors for the vaccinations, the vaccination of health-care workers and their family members, vaccinations in homes and schools, and reimbursement agreements.
Yet, secretly, an additional deal was also negotiated: it was literally agreed that ‘clear blanket vaccination recommendations will be made via the National Immunisation Consortium (Nationales Impfgremium, or NlG) on the suitability of the various vaccines and their applicability, esp. for various high-risk groups’.
Explosive: the Minister of Health and the Austrian Medical Association leadership signed a contract in which they go over the head of the National Immunisation Consortium—and they did so long before the injections were even available—to determine what the National Immunisation Consortium will recommend.
[this means, in other words, that the NIG never had anything to say about the data or the underlying clinical trials; this much we already knew, but now we have the receipts: these people have failed the public, betrayed the trust of patients, and soiled themselves]
It was never about Facts or Truth
Until now, the public was not aware of any document that so clearly showed that various ‘expert panels’ and ‘commissions’ obviously only served to obligingly recommend what politicians and the medical association leadership wanted. It was never about expertise, about advice, about objective science, about health.
Long before the beginning of the mass vaccination campaign, when vaccines did not even exist (!), it was only about one thing: vaccinate, vaccinate, vaccinate! The various ‘expert committees’ and doctors served only as Komparsen [extras, in German, one may also use the term Statisten, which literally implies undue influence of the state]. And it is obvious that the medical association leadership was ‘bought’ off with the reimbursement fee agreement [I’ve omitted the screen shots of some original documents, which can be checked out, if you read German, in the original article; it suffices to say that the fees are extraordinarily high, esp. in light of the incidence of injection: 25 Euros for the first jab and 20 Euros for every successive jab; this piece of evidence is reproduced below in the same position as in the original article]. April 2020 thus was the decisive moment in the history of the Medical Association in which its leadership handed the soul of the medical profession to politicians for the equivalent of thirty pieces of silver.
The Persecution of Doctors is Decided Upon
That was not all: in an ‘Amendments to the Memorandum of Understanding on COVID-19 Vaccinations between the Austrian Chamber of Physicians and the Ministry of Health, concluded in April 2020’, dated 2 Sept. 2021, the medical association leadership ‘promised action with respect to the services rendered by the medical profession’. These, too, signed off by both parties:
The Chamber of Physicians will conduct a media campaign as well as a campaign among the medical profession to increase the willingness of the population to be vaccinated. This includes raising the vaccination issue at other medical appointments (e.g., regular health check-ups) and the promise to take stronger action against doctors who spread misinformation.
As is well known, what constituted ‘misinformation’ was left to the arbitrary whims of the leadership of the Chamber of Physicians. This disgraceful agreement formed the basis for the persecution of critical doctors, which continues to this day. The medical disciplinary law was, in fact, misused for intimidation and propaganda purposes. In doing so, the leadership of the Chamber of Physicians had turned against its paying members [membership is mandatory in Austria as the Chamber also certifies physicians, much like these boards and associations in the U.S.], which cemented into place the persecution of doctors in the style of the Inquisition.
Disciplinary Proceedings by the Medical Association Were (Are) Illegal
The behaviour of the leadership of the Chamber of Physicians’ leadership in recent years is now coming back to haunt them. For months, the medical association has been attacked, ridiculed, and had its very existence openly questioned by politicians. Having done their duty for politicians in the last three years without a peep, the Chamber is apparently no longer needed and may well be let go of. The Chamber of Physicians is sinking more and more into political insignificance. According to insiders, it is now even regarded as a political opponent, a situation that can also be seen in legacy media. After having served as a ‘doormat’ for politicians of all stripes for years, the Chamber of Physicians is now also being treated as such. Various scandals internal to the medical association reinforce this tendency. [talk about Karma, eh? Those who don’t have self-respect will have a hard time getting others’ respect… ]
In the meantime, the Regional Administrative Courts of Vienna, Lower Austria, and Vorarlberg have petitioned the Constitutional Court to repeal parts or the entire Disciplinary Law in the Physicians’ Act [Ärztegesetz, these parts of the Act permit the Chamber of Physicians to enforce standards] on grounds of their suspected unconstitutionality; it is possible that the Constitutional Court will rule even the entire Physicians’ Act unconstitutional. The Chamber of Physicians is a self-governing body. All its committees are to be selected from among its members, i.e., from medical professionals. However, the Disciplinary Commission consists of two medical assessors and a ‘judicially competent chairman’ who is appointed by the Minister of Health in agreement with the Minister of Justice, i.e., someone who must not be a trained physician and who does not come out of the Chamber of Physicians. Thus, the composition of the Disciplinary Commission is a violation of the Federal Constitution. This is the unanimous legal opinion of three state administrative courts [Verwaltungsgerichtshof] and countless jurists.
[I’ll have more to say about this particularity below, for time being: this is potentially huge—and it would be akin to completely re-writing the rules of medicine]
The Chamber of Physicians has unintentionally awakened sleeping dogs with its wave of ill-advised disciplinary hearings against critical doctors. The consequence may be that it now has to be completely re-imagined. But this could also be an opportunity for the medical profession after all the repression of doctors in recent years. For in its current form, the Chamber of Physicians is a politically superfluous enemy and, for its members, the doctors, a very expensive mandatory association whose dues are used to finance the functionaries’ luxury salaries.
Bottom Lines
From time immemorial, we’ve all known that a man’s—or woman’s—price is about, in purely monetary terms, 30 pieces of silver, to say nothing about the amorality and, yes, cowardice of most physicians everywhere.
The notion of buying off support has been well-established in the U.S. (see, e.g., here).
Here, we’re talking individual doctors who are paid handsomely for jabbing people.
Yet, this isn’t even the worst part of this.
The Three Axioms of Governance-by-Bureaucracy
You’ve gotta love them German-speakers for being so stupid to actually put these things into writing.
We now have definitive proof that the subsequent shenanigans—first and foremost the obnoxious Covid Passports — were based on the unholy trinity of questionable medical ethics (ahem), government coercion, and arbitrary definitions.
Remember that ‘fully vaccinated’ used to be two injections? Now it’s at least three, with the fourth jab ‘optional’ (haha, see above), and the Covid Passports come with expiration dates varying from 3-6 months, irrespective whether you’re ‘vaccinated’ or ‘recovered’.
Thus, we may formulate whatthe first axiom of governance-by-bureaucracy is: everything leaks.
In other words: arbitrary categories by government fiat, arrived at with the collaboration of the overwhelming majority of the medical profession.
If history is any guide, the Covid Passports are the functional equivalent of the Aryan Certificate deployed by Nazi Germany: both documents were clearly politically motivated and based on sham ‘The Science™’.
Yet, Covid is revelatory: we’ve seen the abject lack of integrity, morality, and compassion on part of the political caste, its willing executioners in legacy media, and its perpetrators among medical professionals.
Don’t ask what’s wrong with individuals. It’s the bloody ‘system’ that stands exposed.
Thus, we may formulate the second axiom of governance-by-bureaucracy: everyone has his or her price.
We’ve known this for quite some time; sure, I could cite the Nazi and Stalinist atrocities here, but I’d like to point you also to the Asch Conformity, the Milgram, and the Stanford Prison Experiments. Or the book The Wave.
And yet, despite all of this, there’s also a bright spot in all of this: contrary to the claims of postmodernist woke-fied agents-provocateurs, not everything in human society and relations is ‘socially constructed’ or about ‘power’.
A sizeable share of people everywhere has resisted the pressure to ‘get vaccinated’.
A group of doctors have resisted the pressures and temptations—remember the 30 pieces of silver—of collaboration and compliance with government tyranny.
If ‘booster’ uptake is any guide, more and more people are realising that they’ve been had.
Thus the third axiom: incentives and coercion work, until they don’t.
Our highly complex societies are, of course, more than the sum of their moving parts. Yet, given the highly integrated structures, it would be far-fetched to believe that anyone is able to control everything.
True, a lot can be dominated, but in the end, the ‘normative power of the factual’ (Georg Jellinek), in combination with individual experiences, is a powerful antidote to tyranny.
Still, this ain’t over yet, far from it.
If history is any guide, all that humans have ever been able to do is punish the perpetrators in the (vain) hope of establishing deterrence.
It has happened before, it is happening again, and it will happen again.
The next step is to see this through, re-establish the rule of law, and hold these people to account.
California legislators continue their reign of vaccine mandate terror with the proposed Assembly Bill 659, which would require children to be vaccinated for HPV before entering 8th grade. Attorney, Michael Baum, Esq., discusses his law firm’s fight to block this bill, which would stop countless crippling injuries, especially in the absence of proof of efficacy.
In the aftermath of the release of the Lockdown Files, the public is slowly coming to terms with some fairly shocking facts: that the Government was willing to lie and mislead, and to scaremonger and manipulate the media, in order to achieve its Covid policy objectives (or even just to garner a few headlines). The news is still sinking in, but a day of reckoning for those involved looks likely.
For those of us bearing the scars of long engagement in the climate and energy wars, however, none of this was a surprise. It has long been clear that the inhabitants of the Westminster village were happy to hype up fears of climate purgatory and to fib about the road to redemption – renewables – and the cost of taking it. Once the public understand the depth and extent of the deception, and the damage done to the economy and the prospects for our children, the trickery over Covid is going to look decidedly peripheral.
The latest report from the Climate Change Committee (CCC) is a case in point. On the surface it’s a roadmap to a decarbonised electricity grid, but in reality it’s merely a sales document, full of tricks, evasions and outright falsehoods that would make even the most cynical used car salesman blush.
For example, in a number of places, it says that decarbonisation of the grid will be ‘cost-effective’, but you will find next to no information on what it will cost. The game that is being played becomes a bit clearer when you read the reference to ‘carbon prices’. In normal usage, the carbon price is the estimate of the damage done by a ton of carbon dioxide, but in the CCC’s parlance it is an estimate of what it will cost to decarbonise. So, while it gives you the impression it has done a cost-benefit analysis and is going to be saving you money, in reality it is only saying that the bill to be paid will be the same as previously advised. It’s a trick.
Another trick is to assume that wind power costs will be only a quarter of what they actually are. For years, the industry has been pushing claims that they have brought about a cost-reduction revolution. The problem is that windfarms’ own financial accounts show that it isn’t true. And with new windfarms now saying they will not come on stream without further subsidies, the deception has been exposed.
I’m picking on the CCC here, simply because it is in the news today. But it’s not just the CCC. None of the bodies whom the public expect to tell the truth about the Net Zero project will do so: the Royal Academy of Engineering is silent. The Royal Society likewise. National Grid pretends the task is a cinch. The National Infrastructure Commission just repeats the Government line verbatim. Parliament asks how soon the job can be done, not whether it can be done or how much it will cost. Everywhere the tricks go unchallenged and the lies are swept under the carpet.
Such deceptions mean that we are storing up catastrophic harms for our economy, and for our children and grandchildren. Energy that was said to be as cheap as gas is actually going to cost three or four times as much. The costs of ensuring supply when the wind doesn’t blow are an order of magnitude larger.
And whether it was delivered on the back of a lie or not, you are going to have to pay for it. A huge pipeline of wind projects is in place already, each eligible for an astonishing array of hidden subsidies – the list is too long to give here. Once built, they will suck wealth from our economy and hope from our society. They will be hard, if not impossible, to close down – they have been made exempt from windfall taxes and the Government cannot simply switch them off without destroying investor confidence in the economy as a whole. If we do not reverse course soon, our children will never know the wealth we have enjoyed until now, just poverty and rationing and hardship. And all because everyone is too scared to challenge the lies. Just like Covid.
Public health experts are warning that the ‘air testing’ being carried out in East Palestine by a for-profit company hired by Norfolk Southern is “almost like smoke and mirrors.”
The ‘air testing’ recently conducted in East Palestine residents’ homes was deficient in a number of key ways and was actually carried out by a company contracted by the rail company Norfolk Southern, a new report has revealed.
East Palestine, Ohio was smothered in toxic fumes last month when the authorities intentionally burned off huge quantities of vinyl chloride following a train derailment in the village.
Residents fled the area in the immediate aftermath. However, after an evacuation order was lifted, many have returned, with some reportedly citing ‘air testing’ results which apparently determined that they could return home without danger.
But on Saturday, an explosive new report seemed to confirm what many have come to suspect: “the air testing results did not prove their homes were truly safe.”
According to a major British outlet, “the air tests were inadequate in two ways: they were not designed to detect the full range of dangerous chemicals the derailment may have unleashed, and they did not sample the air long enough to accurately capture the levels of chemicals they were testing for.”
As University of Kentucky environmental health professor Erin Haynes reportedly put it, “it’s almost like if you want to find nothing, you run in and run out.”
Making matters even worse, “CTEH, the contractor that provided them, was hired by Norfolk Southern, the operator of the freight train that derailed,” the report detailed.
As another outlet previously explained, “the Center for Toxicology and Environmental Health (CTEH) has a name that might sound like a state or federal agency, but in reality it is a private, for-profit corporation that has been present after hundreds of ecological disasters—from 9/11 to Hurricane Katrina to the Deepwater Horizon oil spill to COVID-19.”
While the relevant section has since been deleted, the company previously explained on its website how the data it’s collecting now could be weaponized against the victims of the Norfolk Southern train derailment disaster in East Palestine:
“A carrier of chemicals may be subjected to legal claims as a result of a real or imagined release,” CTEH noted, adding, “should this happen, appropriate meteorological and chemical data, recorded and saved… may be presented as powerful evidence to assist in the litigation or potentially preclude litigation.”
But despite its alarming track record and apparent desire to go after those affected by the crisis, the company remains a major force in the campaign to assuage locals’ health fears.
“It was CTEH, not the Environmental Protection Agency (EPA), that designed the testing protocol for the indoor air tests,” explains the British report, adding, “and it is CTEH, not the government, that runs the hotline residents are directed to call with concerns about odors, fumes or health problems.”
In a recently-published video, the controversial company insists that their ‘testing’ shows there’s no danger to East Palestine residents.
“All of our air monitoring and sampling data collectively do not indicate any short- or long-term risks,” a CTEH toxicologist claimed.
But CTEH’s failure to register so-called volatile organic compounds (VOCs) in its tests doesn’t necessarily mean that people’s homes are actually safe, a number of experts noted. As Haynes reportedly explained, “VOCs are not the only chemicals that could have been in the air.”
And even a week after the derailment, she said it’s likely the compounds would have dissipated already.
“To keep the focus on the air is almost smoke and mirrors,” Haynes added. “Like, ‘Hey, the air is fine!’ Of course it’s going to be fine. Now you should be looking for where those chemicals went. They did not disappear. They are still in the environment.”
You may have heard that Marburg virus is rearing its ugly head in west Africa. The subtext is Be Very Afraid.
Just in time, the NIAID (Fauci’s old fiefdom) has a vaccine ready to be tested in unfortunate Africans, after being tested on 40 unfortunate Americans. And once they convince governments or other buyers to obtain it, who gets royalties? Why NIAID of course. And its employees can collect up to $150,000/year if their name is on the patent. Sweet, since it was developed and patented on the taxpayers’ dime.
This first-in-human, Phase 1 study tested an experimental MARV vaccine candidate, known as cAd3-Marburg, which was developed at NIAID’s Vaccine Research Center (VRC). This vaccine uses a modified chimpanzee adenovirus called cAd3, which can no longer replicate or infect cells, and displays a glycoprotein found on the surface of MARV to induce immune responses against the virus. The cAd3 vaccine platform demonstrated a good safety profile in prior clinical trials when used in investigational Ebola virus and Sudan virus vaccines developed by the VRC [NIAID’s Vaccine Research Center].
So they claim the Ebola vaccine, also using the adenovirus platform, has a good safety profile—well, the death rate in the 2018-19 east African epidemic was 60%, higher than usual Ebola epidemics. The vaccine was widely used there—so did the disease kill people or the vaccine? Why were there 300 attacks on health workers, many of whom were vaccinators? I don’t think that imputing safety to the Ebola vaccine is acceptable, nor that the Ebola vaccine can be used to impute safety of the Marburg vaccine. Why did the NIAID only test the vaccine in 20 Americans if there were no serious adverse events, and it was so safe?
Plans are in place to conduct further trials of the cAd3-Marburg vaccine in Ghana, Kenya, Uganda, and the United States. If additional data supports the promising results seen in the Phase 1 trial, the cAd3-Marburg virus vaccine could someday be used in emergency responses to MARV outbreaks.
Yes, the adenovirus vector platform, which was known even before the pandemic to cause blood clots. (I have blogged on this.) And clearly proven to cause venous sinus clots around the brain with the J and J and Astra-Zeneca adenovirus vector COVID vaccines.
Marburg: CDC lists a total of 475 lab-confirmed cases during the entire 56 years since Marburg was first identified. How was it identified? It came to Europe with monkeys from Africa, affecting lab workers, of whom 7 of 31 (23%) died.
Marburg is clinically like Ebola, which has affected thousands, but still—in the US Ebola only spread from affected patients to 2 nurses and never spread further. There have been no US Marburg cases. Neither of these infections is very contagious. Using reasonable precautions you won’t get them.
My point is that the risk to us from a natural virus or bacterium is miniscule. That may not be true of a lab-developed microorganism.
It is the lab-designed bugs that are the problem. We need to stop them. Close the labs, the BSL4s, reduce the BSL3’s and get rid of basic research on “selected agents,” destroy the samples, end this form of “science” that has proven its ability to kill millions and cause worldwide economic destruction. End the field of virology and evolutionary viral genetics—which seem to be peopled by a large group of ‘scientists’ who were in cahoots to keep the lab origin covered up…or at a minimum were afraid to tell the public the truth. Keep a few medical virologists around who did not get their hands dirty. Who needs most of them? They have proven their societal value—which is NEGATIVE—over and over these last three years.
I will shed no tears if they are forced to go and do some manual labor in future. Will you?
Put tight price controls on vaccines, allow about 5% profit, and the wild west in vaccinology will disappear. End pandemic preparedness, from which the money for all the new BSL4s and the new coronaviruses in the US came.
We need to get clear on this. The naturally occurring bugs don’t cause deadly pandemics. They do kill off some weak and frail people in the developed world, and occasional a virus or bacterium will kill a young person. Those deaths are unpredictable and the bugs, often unidentified, don’t really spread beyond an occasional case or two. We have no viable path for preventing them. The so-called “spillover” infections can hardly be found.
It is the Global Biosecurity Agenda that must be stopped.
Doctor and nurse deaths from COVID-19 vaccines were always going to be the focus of cover-ups. The reason is practical: the state needs doctors and nurses to enthusiastically push COVID-19 vaccines on their patients, and it needs these same doctors and nurses to stay silent about COVID-19 vaccine injuries and deaths.
Doctors and nurses mustn’t know that their colleagues are dying suddenly from the same COVID-19 mRNA vaccines that they are pushing daily on their own patients.
31 year old NZ nurse died 4 days after booster shot
Divya Simon, 31, a rest home nurse, had her third COVID-19 booster vaccination four days before suffering a massive heart attack, according to a decision from coroner Luella Dunn released today. (click here)
“She had the booster on January 25 last year, and took the next day off work because she felt unwell. She complained of pain in the left side of her neck and shoulder.
Simon, who had two children aged 4 and 2, worked a night shift on January 28 returning home early the next morning and went to sleep at 10am. After she woke mid-afternoon she went to have a shower and told her husband she felt dizzy and had chest pains. That evening she had a cardiac arrest.
Ambulance arrived and Simon was given adrenalin, shocked and taken to Waikato Hospital. There she was intubated and taken to ICU but was not responsive and continued to deteriorate, dying the next day at 11am.
Dunn said an angiogram was unable to determine the cause of the cardiac arrest and there were no medical records to indicate why Simon would suffer a heart attack.
The pathologist who conducted her autopsy told the coroner Simon’s death was most likely related to an underlying weakness in her coronary arteries.
The pathologist found no evidence to suggest Simon’s vaccination contributed in any way to her death and the Centre for Adverse Reaction Monitoring came to the same conclusion.”
Case Closed!
That’s it. Case closed. A healthy 31 year old nurse had a massive heart attack 4 days after her COVID-19 booster shot and it was definitely not the booster shot, although the pathologist had no idea why she died.
But the pathologist is lying. And I can prove it.
New Zealand does not perform autopsies with immunohistochemical staining of tissue samples for the COVID-19 vaccine spike protein.
So when the pathologist said he “didn’t find evidence” of COVID-19 vaccine damage, that was a lie. He “didn’t find evidence” because he didn’t look for it – he did not conduct the proper staining of the pathology samples, because no one in New Zealand does.
“There is no current test (in New Zealand) that will show the Covid-19 vaccine in the heart tissue” as reported by One News New Zealand (click here)
26 year old NZ man died of myocarditis due to Pfizer COVID-19 Vaccination
Let’s look at a different case where the pathologist linked a sudden death to the Pfizer COVID-19 mRNA vaccine – the case of 26 year old NZ man Rory Nairn (click here)
Rory Nairn died of myocarditis after 1st dose of Pfizer COVID-19 vaccine.
Coroner Sue Johnson opened an inquiry into his death. After hearing evidence from pathologist Dr Noelyn Hung, Johnson said she is satisfied that the COVID-19 vaccine caused the myocarditis from which Nairn died.
Hung carried out an intensive pathological examination of the heart. She stated that the cause of the myocarditis came down to a diagnosis by exclusion.
There is no current test that will show the Covid-19 vaccine in the heart tissue, but Hung was able to exclude other causes of myocarditis. Hung also excluded all other known potential causes including certain medicines.
There was no sign of any infection or any other reason for Nairn’s death except in the myocardium (the middle muscular layer of the heart). Johnson accepted Hung’s medical opinion that the direct cause of Nairn’s death was acute myocarditis – consistent with vaccine-related myocarditis.
What this means
If there is no test available to check for COVID-19 vaccine injury to body tissues, you cannot exclude the vaccine as the cause of death. In the case of the 31 year old nurse Divya Simon, the pathologist cannot conclude “the COVID-19 vaccine didn’t do this” or “there is no evidence the COVID-19 vaccine did this”. It is not possible to come to this conclusion, because the pathologist had no way of proving this.
In the case of 26 year old Rory Nairn, COVID-19 vaccine myocarditis was declared the cause of death because every other possibility was excluded. It was the diagnosis of exclusion.
Notice the difference?
The 31 year old nurse death was a cover-up. The pathologist lied. New Zealand’s Centre for Adverse Reaction Monitoring lied. They covered-up her death. Almost certainly because she was a nurse.
My Take…
It should not surprise anyone by this point, that deaths of doctors and nurses will be treated very differently and will be covered up at all costs.
When 3 Canadian doctors died within days of each other in the same Trillium Health Hospital in Mississauga, Ontario, days after the rollout of the 4th COVID-19 vaccine (2nd booster shot), mainstream media called it a coincidence (click here) (click here)
That’s why my reporting on 132 Canadian doctor sudden deaths since the rollout of the COVID-19 vaccines has been so “controversial”.
The fiercest attacks I have faced from mainstream media so far, were about me exposing the sudden deaths of fully COVID-19 vaccinated Canadian doctors.
So whenever you see a case like this where a coroner or pathologist declares that “COVID-19 vaccine didn’t cause this death”, you will know they are lying, and you will be able to explain exactly why they are lying.
They can allow the occasional citizen’s death to be linked to the COVID-19 vaccine. But they cannot and will not allow a doctor or nurse’s death to be linked to the vaccine.
The Telegraph’s publishing of former UK Health Czar Matt Hancock’s private Whatsapp messages has been dubbed ‘The Lockdown Files.’ The messages detail multiple interactions demonstrating the U.K. Government’s willingness to abandon science and a reasoned approach to Pandemic measures, for coercion and control of the British people.
Former CDC Director, Dr. Robert Redfield, testified before The House Selection Committee on the Coronavirus Pandemic this week, letting loose on Anthony Fauci, Deborah Birx, Francis Collins, gain-of-function research and the lab origin debate detailing what he witnessed in early 2020. His testimonials are nothing short of historical.
Now that they’ve stopped telling the public to constantly cover their mouths, Japan’s government and media have moved on to telling the public to put bugs into them. And who better to advocate for people to put insects down their throats than the man who advocated most actively for people to put mRNA injections into their veins, former Vaccine Minister and current Digital Minister Taro Kono?
Taro Kono tries crickets at a venture firm exhibition, Says they are “delicious”.
Here’s a better look at the “delicious” crickets Mr Kono pulled his mask down to taste.
But since about 90% of Japanese are resistant to the idea of eating bugs, Japan’s politicians and propaganda apparatus will have to work harder at pushing crickets than they did pushing Covid jabs. Reworking some of its greatest hits from the Covid era, the media has declared “neophobia” to be the new “vaccine-hesitancy”.
Is revulsion to edible crickets due to neophobia (fear of new things)?
So are the neophobes selfishly preventing the creation of a “sustainable” society with their anti-cricket stance? Or do they have a point in sticking to foods humans have actually evolved to consume? Let’s ask the science.
In an 2018 article entitled “Novel foods: a risk profile for the house cricket”, Jannson et al. conducted a literature review to present a risk profile of house crickets as food. They found four potential concerns.
(1) high total aerobic bacterial counts; (2) survival of spore-forming bacteria following thermal processing; (3) allergenicity of insects and insect-derived products; and (4) the bioaccumulation of heavy metals (e.g. cadmium).
The aim of this study was to identify and evaluate the developmental forms of parasites colonizing edible insects in household farms and pet stores in Central Europe and to determine the potential risk of parasitic infections for humans and animals. The experimental material comprised samples of live insects (imagines) from 300 household farms and pet stores, including 75 mealworm farms, 75 house cricket farms, 75 Madagascar hissing cockroach farms and 75 migrating locust farms. Parasites were detected in 244 (81.33%) out of 300 (100%) examined insect farms. In 206 (68.67%) of the cases, the identified parasites were pathogenic for insects only; in 106 (35.33%) cases, parasites were potentially parasitic for animals; and in 91 (30.33%) cases, parasites were potentially pathogenic for humans. Edible insects are an underestimated reservoir of human and animal parasites.
Among the various parasites potentially pathogenic for humansfound in cricket samples were the following.
Isospora spp. [found in 2.67% of samples from cricket farms] are cosmopolitan protozoa of the subclass Coccidia which cause an intestinal disease known as isosporiasis. These parasites pose a threat for both humans (in particular immunosuppressed individuals) and animals. The host becomes infected by ingesting oocytes, and the infection presents mainly with gastrointestinal symptoms (watery diarrhea).
Physaloptera spp. [found in 1.33% of samples from cricket farms] form cysts in the host’s hemocoel approximately 27 days after ingestion.
Although both above-mentioned papers point to various potential issues, they admit there isn’t enough evidence yet to draw conclusions about the health effects of mass-production and mass-consumption of crickets. And I’d say we’re better off keeping it that way, no matter what names the globalist overlords call us.
On February 1st this year, the World Health Organisation released the first draft of its much heralded pandemic response treaty. The draft treaty, snappily titled the ‘Convention or Agreement on Pandemic Prevention, Preparedness and Response’, is proposed as a solution to what the WHO calls the “catastrophic failure of the international community in showing solidarity and equity” during the “coronavirus pandemic”.
A supposed lack of solidarity amongst national governments will not be the “catastrophic failure” uppermost of many readers’ minds when thinking back on Government health policy over the last three years. Despite this, the WHO’s draft treaty proposes preventing a recurrence of this alleged failure by substantially enhancing the powers of the WHO relative to those of national health authorities.
It does this despite initially affirming “the principle of sovereignty of States Parties in addressing public health matters” in its opening recital, and despite recognising the principle of state sovereignty as one of the guiding principles of the treaty in article 4. Yet notwithstanding these reassuring nods to the notion of state sovereignty, the WHO’s real attitude towards state autonomy can be gauged by a quick glance at the rest of the recitals and provisions in the agreement.
In setting out the WHO’s interpretation of the factual background to this draft agreement, many of the other recitals focus on the purported practical inability of individual sovereign states to respond adequately to the unique health challenges of the modern world. Hence other recitals note that “a pandemic situation is extraordinary in nature, requiring States Parties to prioritise effective and enhanced cooperation”; that “the international spread of disease is a global threat with serious consequences… that calls for the widest possible international cooperation”; and that “the threat of pandemics is a reality and that pandemics have catastrophic health, social, economic and political consequences”. These recitals strongly imply that state sovereignty can be of limited importance in the face of such extraordinarily grave threats.
Similarly, while recognition of state sovereignty is given as one of the guiding principles of the agreement, it is somewhat overshadowed by the raft of other guiding principles, which include abstract things like “equity”, “solidarity” and the “right to health”. Indeed, article 4 goes on to ominously assert that “previous pandemics have demonstrated that no one is safe until everyone is safe”, strongly suggesting that adherence to the principle of national sovereignty during a pandemic is not just an outdated approach to take, but a positively selfish one.
The draft agreement therefore goes on to assign considerable power to the WHO to influence and shape the responses of national health authorities to any future pandemic. The breadth of ambition of the agreement is made clear in article 5, which applies the agreement in a far-reaching way to “pandemic prevention, preparedness, response and health systems recovery at national, regional and international levels”.
Subsequent articles go on to prescribe the policies to be followed by States Parties to the agreement in each of these areas. As examples of what is intended, articles 6 and 7 set out steps to be followed to improve logistics and the workings of the global supply chain for quicker dispersal of what are euphemistically termed “pandemic-related products” (read pharmaceuticals), after which article 8 of the agreement addresses “regulatory strengthening”. Sadly, the regulatory strengthening envisaged in this agreement is not the strengthening of the accountability of national health regulators to the public, but rather the strengthening of those regulators’ accountability to the inter-governmental blob. Article 8 therefore requires signatory states to “strengthen the capacity and performance of national regulatory authorities and increase the harmonisation of regulatory requirements at the international and regional level”. In layman’s terms, more funding and powers for the regulators, yet concurrently less independent decision-making from them as well.
Subsequent articles further limit the discretion of national health authorities in responding to future WHO designated pandemics. Article 11 requires signatory states to “adopt policies and strategies… consistent with… the International Health Regulations” (themselves the target of amendment by the WHO), while article 15 stresses “the need to coordinate, collaborate and cooperate, in the spirit of international solidarity” with the various bodies active in the international healthcare space in the formulation of policies and guidelines. There are references to “establishing appropriate governance arrangements”, presumably well away from potentially meddlesome interference by elected representatives. These governance arrangements are to be complete with “mechanisms that ensure global, regional and national policy decisions are science and evidence-based”. Think blanket mask and vaccine mandates.
Signatory states will also have to take part in “multi-country or regional tabletop exercises every two years” to prepare them for the next pandemic, presumably to ensure that all health authorities remain fully briefed on the acceptable line to take in the event of any such new pandemic being declared, and to deter any of the signatory states from being tempted to go off-script as Sweden did in 2020.
Last but not least, a plethora of comfortable sinecures will be created for the international administrative class, by way of the creation of a governing body for the agreement under article 20, a consultative body for input into decision making by amorphous inter-governmental stakeholders under article 21, and a secretariat under article 24.
Conspicuously lacking in the agreement is any reference to democracy, elected legislatures, or the necessity of regulators and health authorities being accountable to national electorates. Instead, the treaty represents a brazen attempt to further move health policy away from regional or national governments and into the hands of a rarefied class of globalist administrators.
It should be stressed that the current text is only a draft, and that it may be subject to amendments following discussion between the WHO and member states. Further, even if the U.K. does sign this agreement, it will likely require ratification by Parliament under the Constitutional Reform and Governance Act 2010, and will also require implementation via domestic legislation before it will have any domestic legal effect in the U.K. Sustained pressure now on ministers and MPs might just influence any U.K. Government proposals to amend the treaty at draft stage, or alternatively such pressure might conceivably prevent the U.K. Government from signing an unacceptably worded agreement in the first place. Either way, now is the time for action to prevent the crystallisation at international level of the very policies and approaches many of us have railed against at national level for the last three years.
Adam Cross (a pseudonym) is a U.K. qualified barrister specialising in international trade law, with both public and private sector experience.
On November 19, 2020 I testified as the lead witness in the US Senate Committee on Homeland Security and Government Affairs led by Senator Ron Johnson. I used the term “academic fraud” in a series of sharp exchanges with now White House Coronavirus Coordinator Dr. Ashish Jha. I was told by colleagues that the term fraud was too strident and I should tone down my comments for the media.
Over two years later the US House of Representatives Select Subcommittee on the Coronavirus Pandemic held hearings on “Investigating the Origins of COVID-19” and has hit the tip of an iceberg of academic fraud with a trail of peer-reviewed manuscripts as evidence for the creation of the SARS-CoV-2 chimeric virus in the Wuhan Institute of Virology Biosecurity Annex Level 4 laboratory (WIV). This lab had been conducting experiments designed by UNC researcher Dr. Ralph Baric for years and publishing their progress on creation of a coronavirus that could invade human respiratory cells via the ACE2 receptor. They were also developing countermeasures including monoclonal antibodies and killed virus vaccines.
Menachery VD, Yount BL Jr, Sims AC, Debbink K, Agnihothram SS, Gralinski LE, Graham RL, Scobey T, Plante JA, Royal SR, Swanstrom J, Sheahan TP, Pickles RJ, Corti D, Randell SH, Lanzavecchia A, Marasco WA, Baric RS. SARS-like WIV1-CoV poised for human emergence. Proc Natl Acad Sci U S A. 2016 Mar 15;113(11):3048-53. doi: 10.1073/pnas.1517719113. Epub 2016 Mar 14. PMID: 26976607; PMCID: PMC4801244. Menachery, V., Yount, B., Debbink, K. et al. A SARS-like cluster of circulating bat coronaviruses shows potential for human emergence. Nat Med 21, 1508–1513 (2015). https://doi.org/10.1038/nm.3985
The House Committee found through emails that multiple researchers including Dr. Kristian Andersen and Dr. Edward Holmes messaged Dr. Anthony Fauci in January with their conclusions that SARS-CoV-2 could not have arisen from nature. These and other doctors were summoned to a teleconference with Fauci, Dr. Francis Collins, and Welcome Trust Director (now WHO Scientific Director) Jeremy Farrar and four days later the messaging from all the individuals made a 180 degree turn consistently stating the virus did not come from the WIV.
In April, 2020, an opinion paper led by Andersen and coordinated by Farrar appeared in Nature Medicine which completely ignored the work by Baric in the WIV and concluded the virus could not have come from the lab.
In September, 2021, Holmes continues the false narrative in the journal Cell this time citing Baric’s work (Menachery et al) but completely ignoring the chimeric creation in 2015 with homology to the ancestral WIV SARS-CoV-2.
These no doubt are just a few of the individuals and the manuscripts that will memorialize an academic crime that advanced a false worldwide narrative on the origins of SARS-CoV-2. Many have speculated that NIH funding was the motive to get in line with Fauci and Collins. The author list however, tells us this was a global act of fraud.
Why did so many scientists want their names on papers that intentionally misled readers away from WIV? What was the motivation for NIH NIAID UNC WIV to design SARS-CoV-2 as a lethal infection with potential to kill millions? Was this for the advancement of science or where there intentions darker? Did all of these doctors really think it could all be covered up? When I said “fraud” on the Senate record (National Archives) in 2020 I had no idea the extent would be this deep and nefarious. The work of investigative reporters has just begun.
By late 2021 it was already clear in the UK that the covid vaccines did not stop infection or transmission. And there were also already plenty of concerning safety signals. So, even though the “vaccine pass” was then required in the UK to participate in daily life, ‘vaccine hesitancy’ was on the increase.
Switching narrative to counter vaccine ‘hesitancy’
Given this increasing resistance against the vaccine programme, the official messaging was changed from “vaccines stop you getting covid” to “vaccines stop you being hospitalised and dying from covid”.
To push this new narrative the Government started pumping out ‘data’ to support the claim that almost all of those ill in hospital with covid were unvaccinated. Here is an NHS text that was sent to everybody registered with a GP in the UK in November 2021:
Vast majority of those vaccinated were not “fully vaccinated”
At the time the text was sent out, “fully vaccinated” in the UK was defined as: “at least 14 days since 3rd jab” or “between at least 14 days and less than 6 months of 2nd jab”. So, the official figure of 8 out of 10 “not fully vaccinated” might have been right but was totally misleading since almost ALL of those who were vaccinated (i.e., had at least one jab) at that time were “not fully vaccinated”.
This creates a false semantic equivalence between ‘unvaccinated’ and ‘not fully vaccinated’.
A particularly serious example was the ludicrous claim made in the BBC documentary “Unvaccinated” by Dr Mehool Patel (Consultant, University Hospital Lewisham). His statement – unchallenged in the programme – was:
“We looked at about 550 patients that were admitted in our trust between the 15th December and 15th January 2022, which in effect would mean that most if not all of them were through due to Omicron variant, and of that there were unfortunately 21 patients who had to be admitted to intensive care who were the most severe patients due to COVID. Of the 21 I’m afraid 20 of them were unvaccinated, that’s 95%.
Just one person was vaccinated. And of the 21 who were on the unit, I’m afraid unfortunately seven of them didn’t make it, all of them were unvaccinated, 100%. So that’s one figure to just illustrate the point.”
“You maintain that this claim was “either false/exaggerated or an unbelievable outlier”.
I have approached the programme makers for information about the data which were quoted by Dr Patel. I have been advised that the figures were compiled by Dr Patel himself for the purposes of research.
“Lewisham and Greenwich Hospital Trust does not record the vaccination status of patients in ICU so Dr Patel’s figures cannot independently be verified.”
Deliberately murky record keeping used to manipulate data
But the scam was based on something even more ludicrous than classifying “not fully vaccinated” as “unvaccinated”.
As a result of Freedom of Information Requests sent to some individual NHS trusts we now know that some hospitals were using the NIMS system to classify vaccine status of patients while others were using their own systems. This meant that, in many cases even if a patient had a vaccination record in NIMS, if the patient was not vaccinated in that particular hospital/Trust they were recorded as unvaccinated. Some hospitals were using a mixture of both systems (NIMS where a death was recorded and an internal system where a covid case was recorded). For those relying on NIMS, since it was not operational until June 2021, all deaths within the hospital would have had an unknown vaccination status between Jan-June 2021. The problem is that some hospitals were classifying “unknown” as “unvaccinated”.
So, deliberately murky record keeping was used to manipulate the data.
To see the implications of this, here are the data on hospital deaths (all deaths, not just covid) from the start of the vaccine programme until the end of 2021 from an undisclosed NHS trust who responded to an FOI request:
Note that every death up until 21 June 2021 was recorded as unvaccinated simply because hospitals in this Trust were using the NIMS system for classifying deaths which was not up and running until then. But, of course, an unknown number (probably most) of these 742 people were vaccinated.
There are plenty of other anomalies in the data. Note the improbable, sudden and dramatic trend changes:
A steady decline in “unvaccinated” deaths from 21 June until 13 Sept. In week ending 13 Sept only 4 out of 46 (less than 9%) were unvaccinated.
The next week (20 Sept) the unvaccinated are suddenly the majority again with 21 out of 31 deaths (68%), and this increases so quickly that just 3 weeks later (11 Oct) all 44 deaths (100%) are ‘unvaccinated’.
But then we get a sudden and rapid decline in the unvaccinated deaths. Just 2 weeks later (25 Oct) the unvaccinated are 13 out of 47 deaths (28%) and by 20 Dec none of 53 deaths (0%) were unvaccinated.
Such changes can only be the result of changes in definition of who should be classified as unvaccinated.
It is easy to see how the Government could cherry pick this kind of data to present the narrative they wanted. When the text messages were being sent out in November 2021 it is reasonable to assume that they were using the cumulative data up to, say, mid-October. Then using the data in the table up to and including 18 Oct 2021 we count:
1051 “unvaccinated” (including 17 with just a single jab)
370 “vaccinated” (with 2 jabs).
That gives 74% of all hospital deaths classified as “unvaccinated”.
But this is all an illusion. In fact, counting just the final three weeks of the data (6-20 Dec), just 18 out of the 144 deaths (12.5%) were unvaccinated.
It is also worth noting that the same NHS Trust provided the following information on “new COVID positives” in its hospitals between 19th Jan 2021 and 19th Jan 2022.
Given what we know about national vaccination take-up rates, and this Trust’s own death data, it is likely that the majority of those classified as ‘unvaccinated’ here would have been vaccinated (with the exception of those in the 0-20 age categories the vast majority of whom would not have been eligible for vaccination).
So, instead of the ‘50% of new covid cases’ being among the unvaccinated – the ‘official’ narrative pushed from this data – the true narrative should have been that the vast majority of new covid cases were vaccinated.
Why does this matter?
It matters a lot because, despite being completely bogus, these kinds of ludicrous figures were so consistently repeated that the message “vaccines stop you being hospitalised and dying from covid (even if they don’t stop infection and transmission)” was almost universally accepted. Even the strongest critics of the Government’s covid response consistently repeated this mantra:
The figures were also used as the basis for the bogus studies claiming millions of lives were saved by the vaccine.
So, yet again, we can see that statistical data was used to create an illusion of vaccine hospitalisation and mortality efficacy by the simplest of means: deliberately murky record keeping ensuring that the vaccinated get recategorized as unvaccinated when they die or are hospitalised.
Update 9 March 2023: Here is a video I made covering this article:
Postscript: A commenter below reports that the USA “was far worse”:
The 1840 Treaty of Waitangi between the British Crown and Maori chiefs was a landmark event in the history of New Zealand. Drafted in English, a Maori translation was prepared, ostensibly to ensure that Maori could have an accurate understanding of the terms. In retrospect, it is less clear that a meeting of the minds was intended:
The English and Māori texts differ.As some words in the English treaty did not translate directly into the written Māori language of the time, the Māori text is not a literal translation of the English text.It has been claimed that Henry Williams, the missionary entrusted with translating the treaty from English, was fluent in Māori and that far from being a poor translator he had in fact carefully crafted both versions to make each palatable to both parties without either noticing inherent contradictions.
“The covid vaccine is 95% effective” is a contemporary Treaty of Waitangi. The original is in the language of clinical trials. It was never translated. The public interpreted this phrase in their native language, normal English. What Pfizer said and what the public heard were quite different. The public would have been far more skeptical of these products had the clinical trial results been translated into normal English.
What we need is a proper translation and an explanation of how miscommunication happened.
The products were never expected to stop infection or transmission.
The clinical trials did not test for their ability to do so.
A clinical trial is designed to test a drug for effectiveness, which is strictly defined by one or more endpoints. An endpoint is a measurable outcome that can be assessed for each participant. With that in mind, prevention of infection was not an endpoint of the BioNTech/Pfizer injection clinical trials. And, this was known in 2020 before the products were approved for emergency use and distributed to the public starting in 2021.
In this New England Journal of Medicine research summary, Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine, under Limitations and Remaining Questions, we find that “whether the vaccine protects against asymptomatic infection and transmission to unvaccinated persons” remains unanswered by the clinical trial.
What did the clinical trial test for, if not the ability of the mRNA vaccine to stop transmission and/or infection? The trial was designed to test the ability of the injections to prevent “symptomatic Covid 19 cases” defined as one or more of a number symptoms and a positive test (see page 7 of the supplementary appendix for details).
@pfizertweeted in Jan 2021 that stopping transmission was their “highest priority”. Their product does not do that, nor did the tweet make a claim that it did so. But it was their highest priority nonetheless. That, and getting as many people injected as possible.
Failure to Prevent Infection Was Known Before the Rollout
In October 2022, a Pfizer executive testified to an EU body that Pfizer had not tested the ability of the vaccine to stop transmission. This story was shocking to some and generated accusations that Pfizer had lied about the capabilities of the shots. But this information had been available since the trial results were released early in 2021. Pfizer had already been criticized for this.
One of the more immediate questions a trial needs to answer is whether a vaccine prevents infection. If someone takes this vaccine, are they far less likely to become infected with the virus? These trials all clearly focus on eliminating symptoms of Covid-19, and not infections themselves. Asymptomatic infection is listed as a secondary objective in these trials when they should be of critical importance.
Will covid-19 vaccines save lives? Current trials aren’t designed to tell us
Peter Hotez, dean of the National School of Tropical Medicine at Baylor College of Medicine in Houston, said, “Ideally, you want an antiviral vaccine to do two things . . . first, reduce the likelihood you will get severely ill and go to the hospital, and two, prevent infection and therefore interrupt disease transmission.”
Yet the current phase III trials are not actually set up to prove either. None of the trials currently underway are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus….
Is It Even a Vaccine?
A vaccine that prevents infection is known as “neutralizing” or “sterilizing”. I am a software engineer with no training in medicine, pharmacology or clinical trials. I consider myself a good barometer of what the average untrained person would think about such things. Prior to 2021 I had thought that immunity was a necessary condition for a drug to earn the title of “vaccine”. If anyone had asked me, I would have told them that the Covid injections were a treatment, not a vaccine.
A vaccine is a biological preparation that provides active acquired immunity to a particular infectious or malignant disease. … A vaccine typically contains an agent that resembles a disease-causing microorganism and is often made from weakened or killed forms of the microbe, its toxins, or one of its surface proteins. The agent stimulates the body’s immune system to recognize the agent as a threat, destroy it, and to further recognize and destroy any of the microorganisms associated with that agent that it may encounter in the future.
Cornell Law provides the following legal definition of vaccine, sourcing 26 USC § 4132(a)(2), which is consistent with the above:
The term “vaccine” means any substance designed to be administered to a human being for the prevention of 1 or more diseases.
The definition published by the CDC prior to 2021 said much the same. But the CDC website changed the definition on or after August 2021. The older version found on the internet archive is here (emphasis added):
Immunity: Protection from an infectious disease. If you are immune to a disease, you can be exposed to it without becoming infected.
Vaccine: A product that stimulates a person’s immune system to produce immunityto a specific disease, protecting the person from that disease.
Vaccine: A preparation that is used to stimulate the body’s immune response against diseases.
The earlier pair of definitions is quite easy to understand. The latter, much more difficult. What exactly is a “preparation”? Does a vaccine stimulate the body or only prepare the body? What is or is not a vaccine according to the new definition?
While the CDC may think that they can change the meanings of words whenever they like, public memory retains the original meaning. The assumption of immunity permeates almost all non-expert level discussion of vaccines. A web search for “why are vaccines good” shows results that assume or imply immunity.
Even the CDC did not finish the job of memory-holing the old language. On the very same CDC website, under 5 Reasons It Is Important for Adults to Get Vaccinated, we read “By getting vaccinated, you can protect yourself and also avoid spreading preventable diseases to other people in your community.” And then, “Vaccines Can Prevent Serious Illness”.
The timing of the CDC’s edit suggests to me that prior to 2021, the CDC had the same understanding of vaccines as I do. I believe that they wanted a new definition because they knew that the products being developed at warp speed were not vaccines in the original sense of the word. And it was important that those products be called “vaccines” for reasons that I will explain later. This incident brings to mind a meme that I no longer have a link to. captioned: “We changed what ‘definition’ means so you can’t say that we redefined anything.”
What Does “95% Effective” Mean?
The “95% effective” message was repeated in nearly all reporting on the clinical trials. But the question, “effective at doing what?” was rarely asked. To answer this requires walking down the links of a chain of terminology from the world of clinical trials.
The first link in the chain is “risk”. Risk is the probability of a bad outcome. These are assumed to happen randomly within a group. A clinical trial must define in advance the bad outcomes that the drug intends to avoid. The next link is “endpoint”. Each distinct bad outcome is an “endpoint”. The trial compares the endpoints between a control group who did not take the drug and a test group, who did.
The purpose of a clinical trial is to determine the ability of a drug to reduce risk. A drug that reduces risk is “effective”. There are two ways of quantifying risk reduction. From the NIH glossary:
the difference in the incidence of poor outcomes between the intervention group of a study and the control group. For example, if 20 per cent of people die in the intervention group and 30 per cent in the control group, the ARR is 10 per cent (30–20 per cent).
the rate (risk) of poor outcomes in the intervention group divided by the rate of poor outcomes in the control group. For example, if the rate of poor outcomes is 20 per cent in the intervention group and 30 per cent in the control group, the relative risk is 0.67 (20 per cent divided by 30 per cent).
The difference between the ARR and RR (also known as “RRR”, to align with ARR) is in the denominator. The ARR divides by the number of participants in one of the groups. The RRR divides by the number of people with bad outcomes in the control group – a necessarily much smaller number.
The ARR is the number most relevant for a drug – such as the Pfizer injections – that was to be given to everyone. But the RRR is the preferred method of presentation for pharma when they want to exaggerate the effectiveness of a drug because it will always be a much larger number. Would you take a drug that could reduce the incidence of a rare disease by 50%? From 10 per 1 million to 5 per 1 million is an 50% RRR and an 0.0005% ARR.
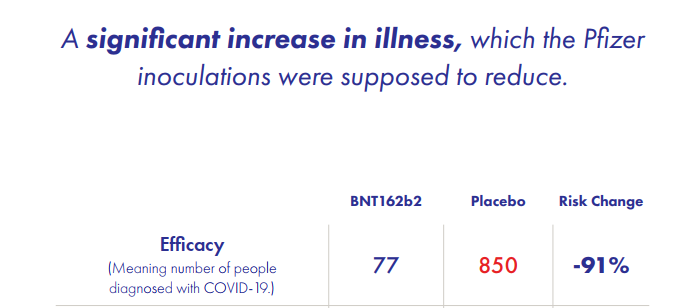
The 95% figure cited for the covid injections is the relative risk. The absolute risk reduction was 0.84%. In a slide deck from the Canadian Covid Care Alliance (CCCA), slide 11 shows how the 91% was achieved (it is 91%, not 95%, because the it refers to an earlier version of the study):
A clinical trial finding of a 1% ARR means that 99% of the people who take the drug either did not experience the condition that the drug treats, or they did experience it, but were not helped by the drug. The 1% both had the condition and were helped by the drug. Another way of saying this is the Number Needed to Treat (NNT). NNT is the reciprocal of the ARR and is the number of people who must take the drug to help one person reach the endpoint. An ARR of 1% corresponds to an NNT of 100 people.
We can now answer the question of the meaning of vaccine effectiveness. The endpoint of the trial was a severe confirmed case of covid at least 7 days after the second dose. This endpoint requires the participant in the trial to have covid symptoms and a positive covid test. “95% effective” means that 95% of the patients who had Covid symptoms and a positive test were in the control group. Five percent were in the test group.
Here’s what “95% effective” did not mean: if you take the shots, then you will have a 95% lower chance of getting covid. But that is how most people understood it because that is what the words mean in normal English.
Then the Lying Started
Once the public had their hopes raised by the false translation of the “95% effective” message, the pandemic-industrial-complex went into high gear to amplify it. They stated the incorrect message loudly, frequently, and as if it were fact. The injections would – with 100% certainty (perhaps 200%) – protect you from infection. Many of the people who said this were doctors or scientific researchers who must have understood how to interpret clinical trials.
Here are some choice quotes that did not age well:
“You’re not going to get Covid if you have these vaccinations.” Joe Biden, CNN Town Hall July 2021
“Now we know that the vaccines work well enough that the virus stops with every vaccinated person. A vaccinated person gets exposed to the virus, the virus does not infect them, the virus cannot then use that person to go anywhere else,” she added with a shrug. “It cannot use a vaccinated person as a host to go get more people. [Vaccines] will get us to the end of this.” – Rachel Maddow, March 2021
“When people are vaccinated they can feel safe that they won’t get infected, whether they’re outdoors or indoors.” – Dr. Anthony Fauci, May 2021 (outdoors: seriously?)
“Vaccination against COVID-19 prevents breakthrough infections, Stanford researchers find.” – Stanford Medicine, July 2021
The public has consistently over-estimated the infection fatality rate of Covid. Some even believed the fatality rate to be above 10%. They believed that we were in great danger. They also believed that the “95% effective” vaccine would bring the pandemic to a quick end, once everyone had taken it. Anyone who refused to do so was therefore risking not only their own life, but everybody else’s as well.
Dr Anthony Fauci estimated herd immunity would emerge when around 60% of the population had taken the vaccine … or perhaps 70, 80, no wait … 85%. Or maybe 100% (which would include large numbers who already had natural immunity). Bill Gates extended that to everyone on earth.
The narrative then turned to demonization of those who refused to submit to vaccine coercion. The selfish anti-social behavior of the anti-vaxxers with their stubborn attachment to “free dumb” that was keeping everyone locked indoors and forcing us all to wear diapers on our faces. Yale University behavioral researchers tested messaging strategies to determine whether shame, embarrassment or fear was most effective.
President Biden said that we the nation was experiencing a “pandemic of the unvaccinated”. Later, Biden ominoulsy warned the unvaccinated that he had been waiting a long time for them to get injected, but “our patience is wearing thin”. In December of 2021 the White House issued a cheery year end greeting to the vaccinated. The unvaccinated, on the other hand, were “looking at a winter of severe illness and death.” Merry Christmas.
Even South Park, which I consider a reliable source of contrarian political opinion, ran a storyline set in the year 2050 in which every single character had to be vaccinated for the 30-year pandemic to end. This episode featured one lone holdout who would not get vaccinated due to a crustacean allergy i.e. for “shellfish reasons”. This gag took aim at people who considered the vaccine to be a violation of body autonomy, and those who objected to components used in its development for religious reasons, thereby scoring a “two for one”.
Volumes can, and will, be written about the intense onslaught of propaganda aimed at getting two needles in every deltoid. I will provide one more example that represents no more than the median level of insanity; plenty of people called for the same or worse. @ClayTravis, in February 2023, tweeted the results of a Rasmussen poll from 2022:
Last January 60% of Democrats wanted to lock everyone who didn’t get the covid shot in their houses. Over 40% of Democrats wanted those who rejected the covid shot sent to quarantine camps. Over 40% also wanted anyone who criticized the covid shot fined & imprisoned. Over a quarter wanted those who didn’t get the covid shot to have their kids seized.
While there were many agendas driving the madness, the Treaty of Waitangi effect was a critical part in carrying it out. If the message had been that “everyone is going to get exposed to covid – injected or not”, then it could not have happened. The misunderstanding convinced the public that mass vaccination would stop the pandemic; and that the holdouts were prolonging it. Without this belief, none of the coercion made any sense: employment mandates, school mandates, quarantine camps, or vaccine passports. As the hysteria fades, the last remaining mandates are being dropped as the reality sinks in that the shots do not stop the spread.
Welcome to Waitangi World. I hope that you have a pleasant stay.
Robert Blumen is a software engineer and podcast host who writes occasionally about political and economic issues.
Prime Minister Benjamin Netanyahu has said that Israel felt threatened by Iran’s growing influence in the Middle East. Netanyahu expressed his Iranophobic view in a meeting with Russian President Vladimir Putin in Russia’s Black Sea resort of Sochi on Wednesday. Press TV has asked Scott Rickard, former American intelligence linguist from Tampa, Florida, and Brent Budowsky, a columnist at The Hill from Washington, to give their thoughts on the issue.
Rickard said Tel Aviv is concerned about the fact that the regime could not carry out its old project to spread sectarian divisions and pave the way for dismemberment of the countries in the Middle East region because of the Iranian-led resistance against Israeli policies, not only in the occupied territories of Palestine but also in the whole region.
“Iran is not a threat to Israel whatsoever. The threat that Israel sees is the fact that their Oded Yinon Plan is being put to a hold by Iran,” the intelligence linguist said on Thursday night.
“They (the Israelis) look at Iran as a threat only because they have no influence on their governments and Iran is autonomous and is not under the Zionist influence,” he added.
Since the victory of the Islamic Republic of Iran in 1979, Tehran has been critical of Israel’s policies in the region, whereas “no leaders [of other states] even dared to speak out against Zionism,” Rickard argued. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.



















{kind=link}
{kind=link}