Who’s the ‘Real’ Peter Marks?
New Website Exposes Failure of Former FDA Vaccine Czar to Protect Americans From COVID Vaccine Dangers
By Michael Nevradakis, Ph.D. | The Defender | May 6, 2025
A former top U.S. Food and Drug Administration (FDA) vaccine official ignored evidence that COVID-19 vaccines caused serious injuries, and dismissed the pleas of people injured by the vaccines, all while reassuring the public the shots were safe, documents published today on TheRealPeterMarks.com website reveal.
The website hosts public statements by Peter Marks, M.D., Ph.D., recordings of his calls with vaccine-injured individuals, transcripts and previously unreleased FDA records.
Informed Consent Action Network (ICAN), React19 and Follow the Silenced — organizations that advocate for the vaccine-injured — obtained the documents through Freedom of Information Act requests and other legal work.
Dr. Danice Hertz, a retired gastroenterologist injured by the Pfizer COVID-19 vaccine, said she hopes the website reveals the side of Marks that the media ignores. Hertz said:
“We want to set the record straight about Marks. The media is misinformed about him and has falsely represented him as a hero. In my opinion, he is far from a hero. He is a dishonest, corrupt man whose allegiance has been to the vaccine manufacturers and not to the safety of the people.”
Website contradicts claims Marks makes in latest media blitz
On March 28, Marks resigned as director of the FDA’s Center for Biologics Evaluation and Research (CBER) under pressure from his new boss, U.S. Health and Human Services (HHS) Secretary Robert F. Kennedy Jr.
He has since made several appearances on mainstream media, defending his record and attacking Kennedy.
React19 co-chair Dr. Joel Wallskog, a Wisconsin orthopedic surgeon injured by the COVID-19 vaccines, accused Marks of lying during media interviews.
“He is a liar and fearful of the truth getting out,” Wallskog said. “The best defense is a good offense.”
Wallskog and Brianne Dressen, a vaccine-injury victim and co-chair of React19, said the media failed to ask the former FDA executive key questions.
Wallskog said he wants to know why Marks “refused” to give Kennedy the vaccine injury data he requested. Dressen said she wants to ask Marks “about the countless lives negatively impacted by the COVID vaccines.”
“We brought the truth front and center to Marks, and he refused to see it,” Dressen said. “His decisions not to disclose highly reported injuries had devastating impacts on the medical community’s ability to recognize and treat injuries.” As a result, she said, “countless lives” were lost and people were “permanently harmed.”
Dressen said Marks’ “real tagline is ‘profits over people.’”
In an April 13 interview on CBS’ “Face the Nation,” Marks told host Margaret Brennan, “You’re talking to the person who came up with Operation Warp Speed.”
Operation Warp Speed was the government’s public-private partnership responsible for facilitating and accelerating the development, manufacture and distribution of COVID-19 vaccines.
As the person responsible for that operation, Marks would have been privy to warning signs on the possible dangers of the new COVID-19 vaccine.
Documents on TheRealPeterMarks.com site reveal that Marks knew about adverse events following vaccinations as early as October 2020 — less than two months before the Pfizer-BioNTech and Moderna vaccines received emergency use authorization (EUA).
Dressen said she was “astonished” that Marks ignored those warning signs and instead promoted the government’s “safe and effective” narrative.
“He knew very well that there were serious problems with the COVID vaccines,” Dressen said. “What astonished me was how he can say it with such resolve.”
Marks approved COVID vaccines, boosters for kids despite knowledge of risks
The documents posted on TheRealPeterMarks.com show that Marks ignored reports and studies on COVID-19 vaccine injuries sustained by children, and that he claimed such reports were “sensationalized.”
For example:
- During a call in May 2022 with vaccine-injury victims, Marks suggested that child deaths following COVID-19 vaccination must be reported because the vaccines are under EUA. Yet during a 2021 call with FDA stakeholders, Marks said child deaths post-vaccination are “very sensationalized” and were unrelated to the vaccines.
- A Jan. 3, 2022, letter from the Siri & Glimstad law firm warned Marks about adverse events in vaccinated children. Yet that day, the FDA extended the EUA for Pfizer’s COVID-19 booster to children ages 12 to 15.
- ICAN filed a citizen petition in May 2022 urging Marks to revoke the EUA for the Pfizer and Moderna vaccines for children. But a month later, the FDA extended the EUA to children as young as 6 months — even though Marks responded to the petition that day, acknowledging adverse events in children.
- The FDA authorized a fourth dose of mRNA COVID-19 vaccines for some groups of people, including immunocompromised children ages 12 and up, four days after the Journal of Pediatrics published a study of children who developed myopericarditis following COVID-19 vaccination.
Dressen called out Marks for his handling of a prominent case of childhood vaccine injury involving Maddie de Garay, a 16-year-old who was seriously injured by the Pfizer-BioNTech vaccine in January 2021.
In June 2021, Marks accepted Pfizer’s finding that de Garay’s injuries were unrelated to the vaccine.
Marks received further updates about de Garay’s condition over the next few months, including statements by de Garay’s mother at an October 2021 meeting of the FDA’s Vaccines and Related Biological Products Advisory Committee.
But in March 2022, Marks said de Garay’s injuries were not vaccine-related and he denied her parents’ request for a meeting. “They took Pfizer’s word for it, then internally gaslit her,” Dressen said.
‘Marks was continually moving the goalpost’ on vaccine risks
Transcripts of Marks’ meetings with vaccine-injury victims showed that he repeatedly rejected safety concerns, or safety signals, related to the COVID-19 shots.
“Marks was continually moving the goalpost — it didn’t matter how we communicated the data, didn’t matter how many hoops we jumped through,” Dressen said.
For example, Marks was repeatedly informed about the prevalence of neurological injuries post-vaccination, including in emails and reports he received in February, March, April and August of 2021.
Marks claimed in a September 2021 email to Dressen that there were no safety signals for neurological injuries. He did not take action in response to several reports in late 2021 and early 2022 on the prevalence of such injuries.
“We spoon-fed their own data to them, showing exactly where the problem is, and still, Marks insisted they couldn’t see it,” Dressen said.
“We know through our work at React19 that neurological adverse events are the most common,” Wallskog said.
Other examples highlighted in the documents include:
- During a call in late 2022, Dr. Narayan Nair, then-director of CBER’s Division of Pharmacovigilance, acknowledged a safety signal for neuropathy in young women. But in the same call, Marks said this signal has “not been possible to tease out.”
- In April 2021, a peer-reviewed paper described the case of a vaccinated person who experienced small fiber neuropathy following COVID-19 vaccination. It identified a successful treatment.
- An August 2021 analysis of VAERS data showed that compared to the annual average of other vaccinations, there were 17 times more reports of serious injuries and 42 times more deaths reported after COVID-19 vaccines.
Marks also repeatedly denied the existence of safety signals for multisystem inflammatory syndrome (MIS). In an email from September 2022, Dressen told Marks that MIS occurs at a higher rate than thrombotic thrombocytopenia syndrome, which was associated with the Johnson & Johnson (Janssen) COVID-19 vaccine and led to a pause in its administration.
However, in a call three days later, Marks said there was not enough data to “make a clear association” between MIS and the COVID-19 vaccines.
‘Stone-cold’ demeanor: Marks appeared indifferent to people injured by vaccines
In several instances, Marks expressed confusion as to why the vaccine-injured were having difficulty receiving medical care for their conditions. Yet he also reportedly appeared indifferent to the victims’ plights.
Dressen and Wallskog pointed to several instances when Marks appeared to act disrespectfully toward vaccine injury victims, notably blowing off an August 2021 meeting with vaccine-injured people and doctors.
Dressen said the meeting, scheduled three weeks in advance, was held the same day the Pfizer Comirnaty COVID-19 vaccine received full FDA approval. “He was busy approving Comirnaty,” Dressen said.
Marks said in an email at the time he missed the meeting due to “urgent matters related to the ongoing pandemic.”
Marks later skipped a Nov. 2, 2021, COVID-19 vaccine injury roundtable hosted by Sen. Ron Johnson (R-Wis.), even though Johnson invited the FDA to attend. Marks did not respond to other emails from vaccine injury victims and attorneys in 2021.
According to Dressen and Wallskog, during other meetings and calls, Marks appeared unmoved by the stories recounted by the vaccine-injured. Wallskog said he acted “cold and calculated.” Dressen claimed Marks had a “stone-cold” demeanor and he was visibly performing other work while the injured shared their stories.
Related articles in The Defender
- HHS Ousts Peter Marks, Sending Vaccine Stocks Tumbling and Biopharma Lamenting Loss of ‘Ally’ at FDA
- ‘Historic’: Federal Court Says AstraZeneca Not Immune From Liability in Case Involving Woman Injured by COVID Vaccine During Clinical Trial
- Their Vaccine Injury Reports Disappeared From VAERS — So They Developed a Tool Anyone Can Use to Track Their Own Reports
- ‘Do Your Job. We Beg of You’: FDA Officials Knew of COVID Vaccine Injuries in Early 2021 But Took No Action
- White House Lacked Plan to Compensate People Injured by COVID Shots, as FDA Sped Up Approval
- ‘I Just Want My Life Back’ Says 16-Year-Old Who Developed Neurological Symptoms After Pfizer Vaccine
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
WHO Pandemic Agreement ⏤ WHO is really in charge?
By Dr Lisa Hutchinson | Health Advisory & Recovery Team | May 6, 2025
On 15 April 2025, as we approached Easter, the not so joyous news broke that member states have now reached an agreement on the WHO Pandemic Agreement or Treaty, with negotiations expected to be formalized in May (17-26) when each member state can then decide whether or not to sign the agreement. Notably, this Treaty has gone ahead without the inclusion of countries such as Argentina and also the United States. It is now well known that President Trump signed an Executive Order to pull the USA out of the agreement owing to the ‘mishandling of the Covid-19 pandemic’ and concerns of China’s ‘inappropriate political influence’. Moreover, federal health officials are also prevented from contributing to talks with WHO, due to concerns it is a harmful organization. So what does this WHO Pandemic Agreement mean for the UK and the rest of the world?
Anne-Claire Amprou, a co-chair of the Intergovernmental Negotiating Body, has claimed that this is a “major step forward in protecting populations, the response will be faster, more effective and more equitable” and will bolster “equity and international security.” She continues by noting that “nothing in the draft agreement shall be interpreted as providing WHO any authority to direct, order, alter or proscribe national laws or policies, or mandate States to take specific actions, such as ban or accept travelers, impose vaccination mandates or therapeutic or diagnostic measures or implement lockdowns.” However, many more skeptical followers of the Agreement, such as James Ruguski, indicate that this represents a Framework Convention to usher in a global pharmaceutical power grab dressed up as ‘health equity’ under the guise of ending ‘vaccine apartheid’. The fact that governments worldwide have bypassed normal safety protocols during ‘health emergencies’ sets a dangerous precedent for a totalitarian approach to a one world governance.
The latest agreement on the WHO Pandemic Agreement refers to pandemic-related health products in response to pandemic emergencies. Of note, these health products include “medicines, vaccines, diagnostics, medical devices, vector control products, personal protective equipment, decontamination products, assistive products, antidotes, cell- and gene-based therapies, and other health technologies”. The agreement continues to elaborate on the fact that a “coordinating financial Mechanism is hereby established to promote sustainable financing for the implementation of this Agreement”. In other words, this will expand the capacities around pandemic prevention and preparedness and response using the above mentioned coordinated financial mechanism to serve the implementation of this Agreement. James Roguski defines the acronym PHEIC (Public Health Emergency of International Concern) in reality as a Pharmaceutical Hospital Emergency Industrial Complex!
In his Substack, James Ruduski explains the main aspects of the Pandemic Treaty:
- This is really Corporate Wealth Redistribution Disguised as Health – as this represents a Framework Convention that benefits Big Pharma;
- A behind the scenes peak at the Conference of Parties (COP) reveals what the Pathogen Access and Benefit Sharing (PABS) scheme does, which gives authority to a government official so they can deem if a countermeasure is required;
- Emergency Powers and the PREP Act is another way that governments take control by bypassing normal safety protocols during declared ‘emergencies’ and sets a dangerous precedent;
- Vaccines are being developed with self-amplifying mRNA technology for new emerging ‘threats’ such as bird flu, H5N1 and the role of regulatory oversight in this regard;
- This reveals biosecurity theatres in which the WHO is given authority over logistics, manufacturing and flow of money for the PREP Act.
Although the World Health Assembly has reached an agreement for the WHO Pandemic Treaty which will be put forward for adoption in mid-May, the international agreements are not legally binding. However, where it becomes problematic for UK citizens is that a section within the agreement based on the Public Health (Control of Disease) Act [1984] ⏤ an ironic date given George Orwell’s book “Nineteen Eighty Four” ⏤ empowers the Secretary of State for Health and Social Care to adopt or embrace any “international agreement or arrangement relating to the spread of an infection or contamination”. While advocates of the WHO Pandemic Agreement opine that it respects national sovereignty, it is also subject to “Obligations under International Law” ⏤ an oxymoron by any standards. Disturbingly, the language of the Agreement also includes emergencies owing to climate change!
The WHO’s One Health initiative integrates human, animal and environmental health across the organization, and includes collaborations with the usual culprits, such as the United Nations (UN) that has created the Food and Agriculture Organization (FAO), the Environment Programme (UNEP) and the World Organization for Animal Health (WOAH). Censorship is also notable in this WHO Agreement document with references to the importance of “building trust and ensuring the timely sharing of information to prevent misinformation, disinformation and stigmatisation.” Most people are unaware that mandates relating to health are illegal. People should not have to comply with health mandates that are not aligned with their beliefs. Human rights educators and justice advocates have pointed out that individuals are more empowered than they realise but resilience is largely something people do not enact as they are unaware of their true legal rights.
British citizens should ignore these international agreements and treaties and focus on repealing section 45 of the Public Health (Control of Disease) Act [1984]. A recent post on platform X by Weston A. Price Foundation, London Chapter, explains how repealing section 45 of the 1984 Public Health Act will ensure we can effect how we are governed, as this can only be affected by statutes. Moreover, the 1688 Bill of Rights confirms that no treaty or government proclamation can change our laws: “That the pretended Power of Suspending of Laws or the Execution of Laws by Regall Authority without Consent of Parlyament is illegall.”
These agreements are really about taking money from wealthy nations, via the WHO, to fund and further extend the powers of Big Pharma around the world. The WHO Pandemic Agreement can enable future public health emergency provisions or pandemic-related unapproved therapies to be rolled out globally in circumstances of another health threat. The Pandemic Agreement allows an increase in the supply chain (for medicines, vaccines, and hospital protocols) that may inflict untold damage. People’s individual rights should never be usurped by government ⏤ even in a health emergency situation. The pandemic and PREP Act enabled engineered emergencies to be initiated so that the 4th Industrial Complex architects could profit from such measures. A compliant population kept in a state of perpetual fear relinquishes power too readily. We need to protect ourselves from manipulation by authorities with too much power. The deadline for member nations to reject the amendments to the International Health Regulations is rapidly approaching: July 19, 2025. But our Secretary of State, Wes Streeting, is likely to agree the terms when he attends the World Health Assembly in Geneva on 19th May, well ahead of the rejection deadline.
James Roguski summarises: 10 reasons to reject the WHO’s Pandemic Agreement
1. Lack of Public Discussion/Debate ⏤ public debate and discussion has been almost non-existent;
2. Pandemic Related Products ⏤ the proposed Pandemic Agreement is not about health, rather, it is a redistribution of wealth under the guise of ‘equity’;
3. Surveillance ⏤ within the Agreement it states that: “Parties shall take steps through international collaboration, in bilateral, regional and multilateral settings, to progressively strengthen pandemic prevention and surveillance measures and capacities, consistent with the International Health Regulations (2005)”;
4. The One Health Approach ⏤ the Agreement states: “developing, implementing and reviewing relevant national policies and strategies that reflect a One Health approach”. This is a key policy instrument for dealing with global health risks but this has far-reaching implications. The WHO Pandemic Agreement gives the WHO Director-General the ability to issue orders to all nations regarding humans, animals and plant ecosystems when a public health emergency is declared, which overrides nation sovereignty;
5. Massive Expansion of the Pharmaceutical Hospital Emergency Industrial Complex ⏤ with Article 10 stating “sustainable and geographically diversified local production”;
6. The Pathogen Access and Benefit Sharing System (PABS) ⏤ the Pandemic Agreement fails to adequately address the issue of gain-of-function research and the proposed PABS would effectively monetize and incentivize the search for “pathogens with pandemic potential”;
7. The Global Supply Chain and Logistics Network ⏤ put simply the WHO should NOT be given the authority to oversee and/or operate a Global Supply Chain and Logistics Network;
8. The Financial Coordinating Mechanism ⏤ this aims to bolster the funding of the WHO to actively control the money and supply chains;
9. The Conference of the Parties ⏤ the establishment of a new bureaucracy (the Conference of the Parties) consisting of unelected, unaccountable and largely unknown bureaucrats ⏤ is unlikely to prioritise the people’s best interests in helping to prevent, prepare for, or respond to future ‘pandemics’;
10. Relevant Stakeholders ⏤ includes private corporations but not we the people.
No informed consent or democratic debate has existed during all these negotiations.
Why this matters is that the WHO Pandemic Agreement has:
⏤ Hidden clauses and centralized control
⏤ Potential impacts on national sovereignty
⏤ Your rights during future health crises will be heavily restricted.
Ultimately public private partnerships do not work and we need transparency. The WHO Pandemic Treaty and vaccine experimentation should not be able to happen again and exiting the WHO or not complying with the Pandemic Agreement is one way to oppose this. Hopefully there is a better way to health ⏤ we need to take away power from government and global officials and we need to contact MPs to raise our objections.
Consider signing the petition linked here FINAL VOTE IMMINENT: REJECT the WHO Pandemic Treaty!
Gender-affirming care for minors under fire in sweeping US report
By Maryanne Demasi, PhD | May 4, 2025
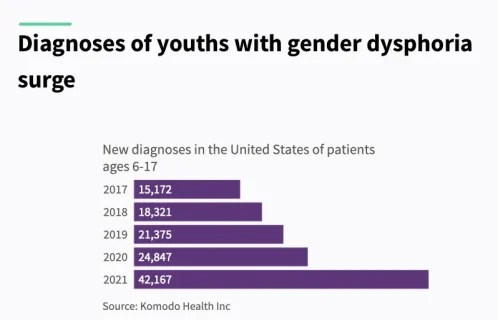
Paediatric gender dysphoria has rapidly emerged as one of the most divisive and urgent issues in medicine today. In the past decade, the number of children and adolescents identifying as transgender or nonbinary has soared.
In the US alone, diagnoses among youth aged 6 to 17 nearly tripled—from around 15,000 in 2017 to over 42,000 by 2021—signalling a seismic shift not only in culture but in clinical practice.
Children diagnosed with gender dysphoria—a condition defined by distress related to one’s biological sex or associated gender roles—are increasingly being offered powerful medical interventions.
These include puberty blockers, cross-sex hormones, and, in some cases, irreversible surgeries such as mastectomy, vaginoplasty, or phalloplasty.
An umbrella review from the US Department of Health and Human Services (HHS) states that “thousands of American children and adolescents have received these interventions,” despite a lack of solid scientific footing.
While advocates often claim the treatments are “medically necessary” and “lifesaving” the report concludes “the overall quality of evidence concerning the effects of any intervention on psychological outcomes, quality of life, regret, or long-term health, is very low.”
It also cautions that evidence of harm is sparse—not necessarily because harms are rare, but due to limited long-term data, weak tracking, and publication bias.
This 409-page report delivers a scathing review of the assumptions, ethics, and clinical practices driving gender-affirming care in the US.
An inversion of medical ethics
At the heart of the HHS critique is a reversal of medical norms.
“In many areas of medicine, treatments are first established as safe and effective in adults before being extended to paediatric populations,” the report explains. “In this case, however, the opposite occurred.”
Despite inconclusive outcomes in adults, these interventions were rolled out for children—without rigorous data, and with little regard for long-term, often irreversible consequences.
These include infertility, sexual dysfunction, impaired bone development, elevated cardiovascular risk, and psychiatric complications.
“The physical consequences are often irreversible,” the report warns.
Puberty blockers, frequently marketed as a reversible ‘pause,’ actually interrupt bone mineralisation at a critical growth stage—raising the risk of stunted skeletal growth and early-onset osteoporosis.
When followed by cross-sex hormones, as is common, the harms multiply. Known risks include metabolic disruption, blood clots, sterility, and permanent loss of sexual function.
Yet many clinics operate under a “child-led care” model, where a minor’s self-declared “embodiment goals” dictate treatment.
The report notes that some leading clinics conduct assessments “in a single session lasting two hours,” often with no robust psychological evaluation.
Consent and capacity
This raises a critical question: are children capable of consenting to life-altering medical interventions?
According to the HHS, informed consent means more than simple agreement—it requires a deep understanding of risks, alternatives, and long-term impact.
And by definition, children lack full legal and developmental capacity for medical decision-making.
“When medical interventions pose unnecessary, disproportionate risks of harm, healthcare providers should refuse to offer them even when they are preferred, requested, or demanded by patients,” the report states.
Supportive parents cannot shield clinicians from ethical responsibility. Many children who present for transition also have autism, trauma histories, depression, or anxiety—all of which can impair decision-making.
Yet clinicians frequently misread a child’s desire to transition as evidence of capacity.
The report warns that the current affirmation model “undermines the possibility of genuinely informed consent” and that the “true rate of regret is not known.”
This becomes especially urgent when the outcomes—sterility, bone loss, and sexual dysfunction—are permanent. Can a 13-year-old grasp what it means to forgo biological parenthood?
As the report suggests, the system has failed to distinguish between a young person’s wish to transition and their developmental ability to understand what that means long term.
A moral failure
The problem is not only medical—it’s moral.
The HHS accuses the medical establishment of abandoning its core duty: to protect vulnerable patients. Ideology and activism, it argues, have taken precedence over evidence and caution.
“The evidence for benefit of paediatric medical transition is very uncertain, while the evidence for harm is less uncertain,” it states.
Among the most disturbing trends highlighted in the report is the sidelining of mental health support.
Research suggests that most cases of paediatric gender dysphoria resolve without intervention. Yet clinicians continue to proceed with irreversible treatments.
“Medical professionals have no way to know which patients may continue to experience gender dysphoria and which will come to terms with their bodies,” the report explains.
The illusion of consensus
The report also takes aim at the idea that gender-affirming care enjoys universal professional backing. It reveals that many official endorsements come from small, ideologically driven committees within larger organisations.
“There is evidence that some medical and mental health associations have suppressed dissent and stifled debate about this issue among their members,” it warns.
Several whistleblowers have spoken out—often at considerable personal risk.
Jamie Reed, a former case manager at the Washington University Transgender Center, alleged that children were being rushed into medical transition without adequate psychological screening. Her testimony led to a state investigation and Senate hearing.
Clinical psychologist Erica Anderson, a transgender woman and former president of the US Professional Association for Transgender Health, has repeatedly raised concerns about the haste with which children are put on medical pathways.
Dr Eithan Haim, a surgeon in Texas, is now facing prosecution after revealing details about paediatric gender surgeries at a children’s hospital.
Rather than sparking debate, these whistleblowers have faced vilification, career damage, and in some cases legal consequences. The HHS suggests this culture of fear has stifled the scientific inquiry necessary for sound medicine.
Psychotherapy as an alternative
Instead of defaulting to hormones or surgery, the report urges a return to psychotherapy. Gender-related distress, it notes, often overlaps with broader psychological challenges that can be addressed non-invasively.
“There is no evidence that pediatric medical transition reduces the incidence of suicide, which remains, fortunately, very low,” the report finds.
Psychotherapy carries no documented harms and offers space for resolution and support. The HHS calls for greater investment in “psychotherapeutic management” as a safer and more ethical approach.
Restoring scientific integrity
Commissioned under President Trump’s Executive Order Defending Children’s Innocence by Ending Ideological Medical Interventions, the report responds to growing alarm over the medicalisation of minors.
Trump’s Executive Order directed federal agencies to evaluate practices to help “minors with gender dysphoria, rapid-onset gender dysphoria, or other identity-based confusion, or who otherwise seek chemical or surgical mutilation.”
It explicitly criticised “junk science” promoted by groups such as the World Professional Association for Transgender Health (WPATH), calling for a return to evidence-based standards and scientific discipline.
Rather than imposing new mandates, the HHS report focuses on delivering “the most accurate and current information available” to clinicians, families, and policymakers—urging caution and restraint.
“Our duty is to protect our nation’s children—not expose them to unproven and irreversible medical interventions,” said NIH Director Dr Jay Bhattacharya. “We must follow the gold standard of science, not activist agendas.”
Reform already underway
The HHS report lands amid a wave of legal reforms.
As of this year, 27 states have passed laws restricting or banning gender-affirming care for minors. These range from full bans on hormones and surgery to tighter consent requirements.
Nineteen of those laws were passed in 2023 alone, according to the Kaiser Family Foundation.

Over half of states have enacted laws/policies limiting youth access to gender affirming care
Though many face court challenges, the trend reflects mounting public concern over the medicalisation of gender-distressed youth. The HHS findings are expected to accelerate further scrutiny and legislative action.
Global shifts
The HHS review is part of a broader international movement to re-examine paediatric gender medicine.
In 2024, the UK’s Cass Review, led by paediatrician Dr Hilary Cass, delivered a landmark critique of NHS gender services. Cass concluded that the model had been adopted prematurely “based on a single Dutch study,” and lacked sufficient evidence.

Dr Hilary Cass, paediatrician
In response, the UK banned the routine use of puberty blockers and began closing the Tavistock gender clinic, replacing it with regional centres focused on holistic mental health care.
In Australia, the Queensland government took similar steps earlier this year, pausing all prescriptions of puberty blockers and cross-sex hormones for minors pending further review.
The move followed the suspension of Dr Jillian Spencer, a senior psychiatrist, from her clinical duties at Queensland Children’s Hospital after she raised concerns about the gender care protocols being used.
Her case has since become a focal point in Australia’s national debate on youth gender medicine.

Dr Jillian Spencer, paediatric psychiatrist, Queensland
A reckoning
The HHS report is more than a policy review—it is a warning.
It reveals that thousands of children—many struggling with underlying psychological issues—have been placed on a path of irreversible medicalisation without the basic safeguards expected in any other area of healthcare.
The report concludes that gender medicine has been practised backwards – treatments were introduced first, and only later did the search for evidence begin.
It calls for a course correction—one that puts evidence before ideology, and ethics above political expediency.
Whether institutions will act on its findings remains to be seen. But for families searching for answers, the report may finally provide the long-overdue clarity that has been obscured by years of activism and politics.
The Great Spillover Hoax
By Jeffrey A Tucker | Brownstone Institute | April 27, 2025
Why precisely were Anthony Fauci and his cohorts so anxious to blame SARS-CoV-2 on bats and later pangolins in wet markets? It was not just to deflect attention from the possibility that the novel virus leaked from a lab in Wuhan doing gain-of-function research. There was a larger point: to reinforce a very important narrative concerning zoonotic spillovers.
It’s a fancy phrase that speaks to a kind of granular focus that discourages nonspecialists from having an opinion. Leave it to the experts! They know!
Let’s take a closer look.
For many years, there has been an emerging orthodoxy in epidemiological circles that viruses are jumping from animals to humans at a growing rate. That’s the key assertion, the core claim, the one that is rarely challenged. It is made repeatedly and often in the literature on this subject, much like climate claims in that different literature.
The model goes as follows.
Step one: assert that spillover is increasing, due to urbanization, deforestation, globalization, industrialization, carbon-producing internal combustion, pet ownership, colonialism, icky diets, shorter skirt lengths, whatever other thing you are against, or some amorphous combination of all the above. Regardless, it is new and it is happening at a growing rate.
Step two: observe that only scientists fully understand what a grave threat this is to human life, so they have a social obligation to get out in front of this trend. That requires gain-of-function research to mix and merge pathogens in a lab to see which ones pose the most immediate threats to our existence.
Step three: in order to protect ourselves fully, we need to deploy all the newest technologies including and especially those which allow for fast production of vaccines that can be distributed in the event of the pandemics that are inevitably coming, probably just around the corner. Above all, that requires testing and perfecting mRNA shots that deliver spike protein through lipid nanoparticles so they can be printed and distributed to the population widely and quickly.
Step four: as society breathlessly awaits the great antidote to the deadly virus that comes to us via these vicious spillovers, there is no choice but to enact common-sense public-health measures like extreme restrictions on your liberty to travel, operate a business, and gather with others. The top goal is disease monitoring and containment. The top target: those who behave in ways that presume the existence of anachronisms like freedom and human rights.
Step five: these protocols must be accepted by all governments because of course we live in a globalist setting in which otherwise no pathogen can possibly be contained. No one nation can be permitted to go its own way because doing so endangers the whole. We are all in this together.
If that way of thinking strikes you as surprising, ridiculous, and scary, you have clearly not attended an academic conference on epidemiology, a trade show for pharmaceutical companies, or a planning group feeding information to the United Nations and the World Health Organization.
This is conventional wisdom in all these circles, not even slightly unusual or strange. It is the new orthodoxy, widely accepted by all experts in this realm.
The first I had heard of this entire theory was the August 2020 article in Cell written by David Morens and Anthony Fauci. Written during lockdowns that the authors helped shepherd, the article reflected the apocalyptic tone of the times. They said humanity took a bad turn 12,000 years ago, causing idyllic lives to face myriad infections. We cannot go back to a Rouseauian paradise but we can work to “rebuild the infrastructures of human existence.”
I was obviously stunned, reread the piece carefully, and wondered where the evidence for the great spillover – the crucial empirical assertion of the piece – could be found. They cite many papers in the literature but looking at them further, we find only models, assertions, claims rooted in testing bias, and many other sketchy claims.
What I found was a fog machine.
You see, everything turns on this question. If spillovers are not increasing, or if spillovers are just a normal part of the complicated relationship between humans and the microbial kingdom they inhabit alongside all living things, the entire agenda falls apart.
If spillovers are not a pressing problem, the rationale for gain-of-function evaporates, as does the need for funding, the push for the shots, and the wild schemes to lock down until the antidote arrives. It’s the crucial step, one that has mostly evaded serious public attention but which is nearly universally accepted within the domain of what is called Public Health today.
Who is challenging this? A tremendously important article just appeared in the Journal of Epidemiology and Global Health. It is: “Natural Spillover Risk and Disease Outbreaks: Is Over-Simplification Putting Public Health at Risk?” by the Brownstone-backed team at REPPARE. It’s something of a miracle that this piece got through peer review but here it is.
They present the core assumption: “Arguments supporting pandemic policy are heavily based on the premise that pandemic risk is rapidly increasing, driven in particular by passage of pathogens from animal reservoirs to establish transmission in the human population; ‘zoonotic spillover.’ Proposed drivers for increasing spillover are mostly based on environmental change attributed to anthropogenic origin, including deforestation, agricultural expansion and intensification, and changes in climate.”
And the observation: “If a genuine misattribution bias regarding spillover risk and consequent pandemic risk is arising, this can distort public health policy with potentially far-reaching consequences on health outcomes.”
Then they take it on with a careful examination of the literature generally footnoted as proof. What they find is a typical game of citation roulette: this guy cites this guy who cites this guy who cites that guy, and so on in spinning circles of authoritative-seeming apparatus but fully lacking in any real substance. They write: “We see a pattern of assertive statements of rapidly rising disease risk with anthropogenic impacts on ecology driving it. These are cited heavily, resting largely on opinion, which is a poor substitute for evidence. More concerningly, there is a consistent trend of misrepresenting cited papers.”
We’ve seen this movie many times before. What’s more, there does exist a largely ignored literature that closely examines many of the supposed causal factors that drive spillovers that reveals grave doubts about any causal connection at all. The authors then place the skeptical papers against the opinion papers usually cited and conclude that what has emerged is an evidence-free orthodoxy designed to back an industrial project.
“There are several potential reasons for this tendency to reference opinion as if it is fact. The field has been relatively small, with authorship shared across many papers. This risks the development of a mechanism for circular referencing, reviewing and reinforcement of opinion, shielding claims from sceptical inquiry or external review. The increased interest of private-sector funders in public health institutions including WHO, and its emphasis on commodities in health responses, may deepen this echo chamber, inadvertently downgrading or ignoring contrary findings while emphasizing those studies that support further funding.”
See the pattern here? Anyone who has followed sociology of “the science” over these last five years can. It’s groupthink, the acceptance of doctrine believed because all their peers believe it. In any case, the gig pays well.
Now we can better explain why it is that Fauci and the rest were so emphatic that the coronavirus of 2019 did not originate in a lab for which they had arranged the funding but instead leapt from a bat or something else from a wet market.
The wet market narrative was not only designed to cover up their scheme and avoid blame for a global pandemic of any level of severity. It was also to deploy the potentially catastrophic consequences and resulting public panic as a rationale for continuing their own biological experimentation and funding grift.
“Sadly, it appears we have a leak from a lab.”
“No worries. We’ll find some scientists and steer some grant money to prove the pathogen in question originated from zoonotic spillover, thus proving the point that we need more funding.”
“Brilliant Dr. Fauci! Do we have contacts in the media?”
“We do. We’ll get on that.”
Fauci’s Replacement at NIAID a Cheerleader for Gain-of-Function Research
By Michael Nevradakis, Ph.D. | The Defender | April 29, 2025
A virologist who supports gain-of-function research and believes COVID-19 evolved naturally is the new acting director of the National Institute of Allergy and Infectious Diseases (NIAID), the agency Dr. Anthony Fauci led for 38 years.
Jeffery Taubenberger, M.D., Ph.D., a 19-year veteran of NIAID and chief of the institute’s Viral Pathogenesis and Evolution Section, replaced Dr. Jeanne Marrazzo, who was placed on leave last month by the Trump administration.
Citing an email from Dr. Matthew Memoli, deputy director of the National Institutes of Health (NIH), Science reported that Taubenberger’s first day as acting director was April 25. Taubenberger will head an institute with a $6.56 billion budget, making it the second-largest NIH branch, overseen by the U.S. Department of Health and Human Services (HHS).
Several researchers told Science that Taubenberger has a commendable track record, highlighting his work sequencing the Spanish flu virus of 1918.
Adolfo Garcia-Sastre, Ph.D., a virologist at the Icahn School of Medicine at Mount Sinai in New York, said Taubenberger “has made many critical contributions to the field of influenza, both in pathogenesis, animal models, human data, and vaccines.”
But critics point to Taubenberger’s public support of gain-of-function research and the zoonotic theory of COVID-19’s origins, which holds that the virus crossed over naturally from animals to humans.
They also criticized his past ties to Fauci and other controversial virologists, and his prior work on COVID-19 vaccines.
Gain-of-function research, which increases the transmissibility or virulence of viruses, is often used in vaccine development. Such research was conducted at the Wuhan Institute of Virology in China, prompting fears that the virus was developed at the lab and subsequently leaked.
Concerns over the safety of gain-of-function research previously led the U.S. government to implement a moratorium on such projects between 2014 and 2017.
“Gain-of-function research, if made safe, is a tremendous tool for forecasting the evolution of pathogens,” said Karl Jablonowski, Ph.D., senior research scientist for Children’s Health Defense. “The problem is that there is no such thing as a leak-proof laboratory, just as there is no such thing as an unsinkable ship. A lab leak is not inevitable, but it is a risk — one that we witness surprisingly often.”
Rutgers University molecular biologist Richard Ebright, Ph.D., a critic of gain-of-function research, said, “Taubenberger is part of the problem at NIAID, not part of the solution.”
Ebright said Taubenberger’s track record is at odds with HHS’ “Make America Healthy Again” agenda:
“Taubenberger’s views on the need for transparency and accountability at NIAID management, on the need for re-prioritization of NIAID funding to match disease burden, on the cause and cover-up of COVID, on reckless gain-of-function research and pathogen-resurrection research, and on biosafety, biosecurity, and biorisk management all appear to be diametrically opposed to those of HHS Secretary Kennedy.
“As such, Taubenberger’s appointment as acting director of NIAID is baffling.”
In a 2014 interview with the journal EMBO Reports, Taubenberger downplayed the risks of gain-of-function research, claiming it’s what “virologists have done for a hundred years.”
In a 2013 letter to the journal mBio, Taubenberger suggested that gain-of-function research replicates natural processes. He argued that Influenza A viruses “continually undergo ‘dual use experiments’ as a matter of evolution and selection.”
According to the American Society for Microbiology, dual-use research is a type of gain-of-function research that raises “important biosafety and/or biosecurity concerns.” It requires “a higher level of review” and is “subject to strict protocols.”
Jablonowski said Taubenberger’s dismissal of concerns over the safety of gain-of-function research overlooks its inherent risks.
“The problem with the argument is actually a problem with the policy it argues — it assumes an ill-willed actor intent on ‘deliberate misuse’ as the risk. Recent history has taught us that lab leaks pose a real and serious risk, no ill-willed actor needed. … Advocates of gain-of-function research do not include a realistic assessment of pathogen escape as part of a risk-benefit balance,” Jablonowski said.
While Taubenberger has been lauded for his role in sequencing the 1918 Spanish flu virus, some scientists were critical of this work, with Ebright calling the reconstruction of the 1918 virus “reckless.”
“Taubenberger … exhumed victims of the 1918 Spanish flu from the Alaskan permafrost to sequence and reconstruct the virus,” Jablonowski said. “It is a virus that killed 50 million people in two short years, and with its resurrection, could have reinitiated a pandemic.”
Taubenberger downplayed connections between COVID, lab leak
Taubenberger has sought to downplay any connection between gain-of-function research and the origins of COVID-19, instead claiming the virus emerged naturally.
In July 2020, Taubenberger and Fauci associate Dr. David Morens co-authored an op-ed in the American Journal of Tropical Medicine and Hygiene, suggesting that COVID-19 is “a virus that emerged naturally.”
In a later email to a Science reporter, on which Taubenberger was copied, Morens described the article as a publication that “defends Peter and his Chinese colleagues” — referring to zoologist Peter Daszak, Ph.D., former president of the EcoHealth Alliance, which collaborated with Wuhan scientists on gain-of-function research.
Jablonowski said the authors of the 2020 op-ed “are unfit for office at a scientific institution — not because they got the origins of COVID-19 wrong, but because they played the game of deceiving the world. One of the villains of COVID-19 was EcoHealth Alliance, and Taubenberger’s narrative casts it as the hero.”
In their op-ed, Fauci and Morens called for the development of “broadly protective vaccines” and suggested that the role of organizations like the Coalition for Epidemic Preparedness Innovations (CEPI) “should be extended and strengthened.”
In 2021, CEPI launched its “100 Days Mission” to develop infrastructure capable of delivering a vaccine for a future pandemic within 100 days. CEPI’s supporters include the Gates Foundation, World Economic Forum and Wellcome Trust.
According to his NIAID biography, Taubenberger has overseen research aimed at developing “broadly-protective coronavirus vaccines in pre-clinical animal studies.”
“Taubenberger is wrong about the dangers of gain-of-function research and also about the ‘zoonotic theory,’” said immunologist and biochemist Jessica Rose, Ph.D. “He needs to read EcoHealth Alliance’s DEFUSE proposal.”
Project DEFUSE, a 2018 grant developed by Daszak and co-authored by U.S. and Wuhan scientists, proposed engineering high-risk coronaviruses of the same species as SARS-CoV-2.
Although the U.S. government’s Defense Advanced Research Projects Agency rejected the proposal, some scientists have likened DEFUSE to a blueprint for generating SARS-CoV-2 in the lab, noting the similarities between the proposed work and key characteristics of SARS-CoV-2 that are not found elsewhere in nature.
Last year, HHS suspended all funding for EcoHealth Alliance after finding the organization failed to properly monitor risky coronavirus experiments.
The suspension came two weeks after a U.S. House of Representatives committee investigating the COVID-19 pandemic called for a criminal investigation of Daszak and a month after the U.S. Senate launched an investigation into 15 federal agencies that were briefed about Project DEFUSE in 2018 but said nothing.
Taubenberger collaborated closely with Fauci
According to U.S. Right to Know, “Most of the NIAID employees who helped Daszak maintain funding amid the pandemic still retain positions of influence at NIAID” — including Taubenberger and Morens, formerly a key aide to Fauci who is under investigation for allegedly using his personal email address to evade Freedom of Information Act requests for communications related to the origins of COVID-19.
Ebright said that Taubenberger has maintained longstanding collaborations with such figures, noting that he co-authored 14 papers with Fauci and 66 papers with Morens.
According to U.S. Right to Know, Taubenberger also collaborated with researchers who played a key role in promoting the zoonotic theory of COVID-19’s origins — including Daszak and several co-authors of “The proximal origin of SARS-Cov-2,” a March 2020 editorial published in Nature Medicine promoting the natural origin of COVID-19 that was later used to discredit proponents of the lab-leak theory.
Earlier this month, the Trump administration launched a revamped version of the government’s official COVID-19 website, presenting evidence that COVID-19 emerged following a leak at the Wuhan Institute of Virology. The CIA, FBI, U.S. Department of Energy, U.S. Congress and other intelligence agencies have endorsed this theory.
In a 1998 interview on PBS’ “American Experience,” Taubenberger suggested that a flu pandemic was inevitable. “The odds are very great, practically a hundred percent, that another pandemic will occur,” he said.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
ICAN FIGHTS BACK: SUPPORT FOR THE INJURED, DATA FOR THE PEOPLE
The HighWire with Del Bigtree | April 18, 2025
ICAN lead counsel Aaron Siri, Esq., joins Del to unveil a groundbreaking new ICAN initiative aimed at helping COVID vaccine-injured individuals who were previously denied government compensation. He also reveals disturbing new developments from the CDC’s Vaccine Safety Datalink (VSD)—a massive database of health records from over 10 million Americans—and what it means for the long-promised vaccinated vs. unvaccinated study. Don’t miss this critical update.
EU Leaders Advocate Stronger Censorship Regulation to Counter “Disinformation” Threats
A battle to define who gets to frame reality online
By Cindy Harper | Reclaim The Net | May 2, 2025
European authorities are stepping up their campaign against what they label “disinformation,” as calls grow from within the EU’s institutional framework to expand regulatory powers over online content and digital platforms.
At the forefront is Oliver Röpke, President of the European Economic and Social Committee (EESC), who is urging tighter enforcement of the EU’s sweeping censorship mechanism, the Digital Services Act (DSA), and calling for more aggressive oversight of artificial intelligence.
Framing the issue as a direct challenge to democratic systems, Röpke claims that coordinated disinformation efforts are being waged both by foreign interests and local actors, with particularly harmful impacts on vulnerable populations. “We know that they are spreading in a coordinated manner disinformation and misinformation within our countries, the European Union, but they all work often hand-in-hand with domestic actors,” he told the European Newsroom.
He went on to argue that marginalized communities are frequent targets in these campaigns, which, he says, erode public confidence in democratic institutions. In response, the EESC has rolled out initiatives like “Citizens can defeat disinformation,” promoting what it calls grassroots resistance to online manipulation.
But the solution Röpke favors is far from bottom-up. He is calling for Big Tech companies to be bound even more tightly to EU regulation under the DSA, which he defends as a tool not of censorship but of structured debate. “I think it’s not about censoring opinions. On the contrary, it is to ensure a free debate – a free debate based on facts and on well-informed actors,” Röpke said.
He also wants to see the EU develop its own digital giants, aligned with European regulatory priorities, to compete with dominant global tech firms.
His vision includes expanding the bloc’s AI governance regime, building on the 2024 AI Act. Although that legislation introduced tiered risk-based controls for AI deployment, Röpke believes additional safeguards are needed. “We have to create a regulatory environment which is technology-open and friendly, but at the same time we have to insist on certain rules,” he stated, stressing that AI must serve ethical, not merely commercial, goals.
Meanwhile, environment ministers gathered in Warsaw to hash out strategies for combating what they see as a wave of misinformation tied to climate policy. The recent massive blackout that left large parts of Spain and Portugal without electricity gave fresh ammunition to online speculation, which officials swiftly labeled as “disinformation.”
Poland’s environment minister, Paulina Hennig-Kloska, described the flood of commentary as part of a broader pattern. “In recent months we’ve had more targeted disinformation used for political purposes, very often by our political adversaries,” she said following the meeting.
While the DSA is already in effect, Hennig-Kloska suggested it falls short. According to her, EU governments currently lack “effective measures to combat disinformation.” She confirmed that the environment ministers had agreed on the need for stronger tools and that the next stage would be engagement with the European Commission.
Underpinning much of this is the belief that foreign governments are engaged in information warfare aimed at destabilizing Europe’s climate and energy agenda.
CHD Funds Lawsuit Against CDC Over Program That Forces Pediatricians to Give COVID Vaccines to Kids on Medicaid
By Michael Nevradakis, Ph.D. | The Defender | April 28, 2025
A California pediatrician is suing the Centers for Disease Control and Prevention (CDC) over a federal program that requires doctors in her state who treat children enrolled in Medicaid to give those children all of the vaccines recommended by the CDC.
Children’s Health Defense (CHD) is supporting the lawsuit, filed April 25 in the U.S. District Court for the Central District of California, Santa Ana Division.
Dr. Samara Cardenas lost her medical practice after the CDC Vaccines for Children Program kicked her out of the program because she wouldn’t give COVID-19 vaccines to healthy kids.
California, like most states, requires pediatricians who treat Medicaid patients to be enrolled in the Vaccines for Children Program. The program, in turn, requires doctors to strictly follow the CDC’s childhood immunization schedule.
In late 2023, the Vaccines for Children Program informed Cardenas that her vaccine orders “were being scrutinized” for not including COVID-19 shots. She was later expelled from the program. As a result, she lost her Medicaid contract, forcing her to close her practice.
The Vaccines for Children Program primarily serves low-income populations by providing free vaccines to uninsured or underinsured children and children who are eligible for or enrolled in Medicaid. Medicaid compensates pediatricians for the costs associated with administering the vaccines.
In her first-of-its-kind lawsuit, Cardenas alleges the CDC’s Vaccines for Children Program violates the Fifth Amendment’s equal protection and due process provisions by subjecting children enrolled in Medicaid to different treatment standards and compelling doctors to act against their professional judgment.
The lawsuit also questions the safety and necessity of administering COVID-19 vaccines to children, the inclusion of COVID-19 shots on the CDC’s childhood immunization schedule and the impartiality of the CDC Advisory Committee on Immunization Practices (ACIP), which makes vaccine-related recommendations.
In California, 3 in 7 — or about 5 million children — are enrolled in Medicaid. Nationally, about 40% of all kids — or about 29.2 million children ages 0-17 — are covered by Medicaid.
The suit names CDC Acting Director Susan P. Monarez, as the defendant. Monarez is also President Donald Trump’s nominee to lead the agency.
Cardenas ‘followed her conscience and the science’
Attorney Rick Jaffe, who represents Cardenas, said this is “the first federal lawsuit challenging the CDC’s coercive use of the VFC [Vaccines for Children] program to enforce experimental, emergency-authorized COVID-19 vaccination as a condition of Medicaid access.”
Cardenas “followed her conscience and the science,” Jaffe said. “The VFC framework gave her no choice: vaccinate all kids or lose access.”
Kim Mack Rosenberg, CHD general counsel, said the lawsuit places policies that disproportionately affect Medicaid recipients under scrutiny, as the Vaccines for Children Program’s policy “essentially mandates these experimental shots for a population historically vulnerable to medical experimentation.”
Cardenas is not seeking compensatory damages. Instead, the lawsuit “seeks to compel the CDC to abandon its misguided and scientifically untethered policy, and stop the unnecessary mass vaccination of the nation’s poorest children.”
“We’re asking the court to say the government can’t make scientific compliance a prerequisite to serving poor patients,” Jaffe said.
Pediatrician Dr. Michelle Perro said that by requiring physicians to administer all vaccines on the childhood vaccination schedule, “medical autonomy is abolished” while “low-income children are left with fewer options and less continuity of care.”
Perro said many doctors are reluctant to oppose these policies. “The threat of speaking out is financial ruin and the potential loss of their ability to practice,” Perro said. “This is coercion and harassment.”
‘The unknowns are enough to never let these products anywhere near children’
In October 2022, ACIP, the CDC’s vaccine advisory panel, unanimously recommended adding COVID-19 vaccines for children as young as 6 months old to the CDC childhood schedule.
The complaint alleges that before making that recommendation, the CDC failed “to compile and analyze vaccine injury data.” It also alleges that ACIP is “compromised by conflicts of interest,” as many of its members “have financial or professional ties to vaccine manufacturers or related interests” — for which the CDC has granted conflict-of-interest waivers.
According to the complaint, by not presenting evidence of the vaccine’s clinical benefit, ACIP violated the Administrative Procedure Act, a federal law banning government agency actions that are “arbitrary, capricious, an abuse of discretion, or otherwise not in accordance with law.”
The lawsuit cites data from the U.S. government-run Vaccine Adverse Event Reporting System (VAERS) showing reports of “hundreds of thousands of adverse events” related to the COVID-19 vaccines, including “serious adverse events and deaths.”
As of March 28, VAERS listed 72,924 reports of adverse events in people 18 and younger, including 6,122 serious adverse events and 201 deaths.
Albert Benavides, a VAERS expert and founder of VAERSAware.com, said the true figures are higher, as many VAERS report summaries indicate the victim’s age even if the report officially lists the age as “unknown.” His analysis of reports shows that “there is more than double the amount of dead children” — 556 in total.
According to the complaint, the CDC failed to “reevaluate or rescind its blanket recommendation for COVID-19 vaccination,” and that ACIP is instead doubling down on its COVID-19 vaccine recommendations.
The complaint cites this month’s ACIP meeting, during which the committee considered revising its blanket COVID-19 vaccine recommendation and switching to risk-based recommendations.
ACIP member Dr. Denise Jamieson opposed the proposal, claiming that the “U.S. has a history of not being able to implement such variable recommendations,” which would confuse the public.
“This is not merely arrogance,” the lawsuit states. “It is government-by-committee at its most dangerous — where unelected public health advisors retain extraordinary power to shape national policy.”
Attorney Ray Flores, senior outside counsel for CHD, questioned why the CDC added COVID-19 vaccines to the childhood vaccination schedule even though they were not licensed, but only issued under emergency use authorization (EUA).
“It shocks the conscience,” Flores said. “Physicians in California must be free to exercise their best judgment, especially when it comes to administering experimental injections.”
Releasing the vaccines under EUA meant they were subject to less testing than a licensed vaccine, said Karl Jablonowski, Ph.D., senior research scientist for CHD. “The unknowns are enough to never let these products anywhere near children. There are heavy compromises made when you skip the already insufficient regulatory steps with an emergency use authorization.”
‘Can the government tell a doctor what she must inject in order to treat the poor?’
In 2022, Sweden and Denmark stopped recommending COVID-19 shots for children. In 2023, the U.K. ended its COVID-19 booster program for healthy people ages 50 and younger. That year, the World Health Organization said healthy children and teens should be considered low priority for COVID-19 vaccines.
Several recent studies have also called the practice of vaccinating healthy children for COVID-19 into question.
A December 2024 study published in the Journal of the Pediatric Infectious Diseases Society found that children under 5 who received the Pfizer COVID-19 vaccines were more likely to become infected with COVID-19 than unvaccinated children with natural immunity.
A May 2024 preprint observational study of 1.7 million U.K. children and teenagers found myopericarditis only in the group that received Pfizer’s COVID-19 vaccine and that the vaccine provided only 14 to 15 weeks of protection against infection.
Pfizer documents publicized last year showed that the company quietly studied myocarditis in children a month before its COVID-19 vaccine received an EUA for children ages 5-11.
A peer-reviewed study published earlier this month in Immunity, Inflammation and Disease, found that young adults who received a Pfizer COVID-19 vaccine exhibited spike protein production a year or more after vaccination — significantly longer than the spike protein was expected to remain in the body.
Jaffe said the lawsuit “isn’t about vaccine skepticism. It’s about professional freedom, patient-level nuance, and constitutional limits on administrative coercion.”
“Can the government tell a doctor what she must inject in order to treat the poor? That’s what this case asks. And the answer should be ‘no.’”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
The False Claims of WHO’s Pandemic Agreement
By David Bell | Brownstone Institute | April 28, 2025
One way to determine whether a suggestion is worth following is to look at the evidence presented to support it. If the evidence makes sense and smells real, then perhaps the program you are asked to sign up for is worthy of consideration.
However, if the whole scheme is sold on fallacies that a child could poke a stick through, and its chief proponents cannot possibly believe their own rhetoric, then only a fool would go much further. This is obvious – you don’t buy a used car on a salesman’s insistence that there is no other way to get from your kitchen to your bathroom.
Delegates at the coming World Health Assembly in Geneva are faced with such a choice. In this case, the car salesman is the World Health Organization (WHO), an organization still commanding considerable global respect based on a legacy of sane and solid work some decades ago.
It also benefits from a persistent misunderstanding that large international organizations would not intentionally lie (they increasingly do, as noted below). The delegates will be voting on the recently completed text of the Pandemic Agreement, part of a broad effort to extract large profits and salaries from an intrinsic human fear of rare causes of death. Fear and confusion distract human minds from rational behavior.
WHO Likes a Good Story?
The Pandemic Agreement, and the international pandemic agenda it is intended to support, are based on a series of demonstrably false claims:
- There is evidence of a rising risk of severe naturally occurring pandemics due to a rapid (exponential) increase in infectious disease outbreaks
- A massive return on financial investment is expected from diverting large resources to prepare for, prevent, or combat these
- The Covid-19 outbreak was probably of natural origin, and serves as an example of unavoidable health and financial costs we will incur again if we don’t act now.
If any of these were false, then the basis on which the WHO and its backers have argued for the Pandemic Agreement is fundamentally flawed. And all of them can be shown to be false. However, influential people and organizations want pandemics to be the main focus of public health. The WHO supports this because it is paid to.
The private sector invested heavily in vaccines, and a few countries with large vaccine and biotech industries now direct most of the WHO’s work through specified funding. The WHO is obligated to deliver what these interests direct it to.
The WHO was once independent and able to concentrate on health priorities – back when they prioritized the main drivers of sickness and premature mortality and gained the reputation they now trade from. In today’s corporatized public health, population-based approaches have lost value, and the aspirations of the World Economic Forum hold more sway than those dying before sixty.
Success in the health commodities business is about enlarging markets, not reducing the need for intervention. The WHO and its reputation are useful tools to sanitize this. Colonialism, as ever, needs to appear altruistic.
Truth Is Less Compelling Than Fiction
So, to address these fallacies. Infectious disease mortality has steadily declined over the past century despite a minor Covid blip that took us back just a decade. This blip includes the virus, but also the avoidable imposition of poverty, unemployment, reduced healthcare access, and other factors that the WHO had previously warned against, but recently actively promoted.
To get around this reality of decreasing mortality, the WHO uses a hypothetical disease (Disease X), a placeholder for something that has not happened since the Spanish flu in the pre-antibiotic era. The huge Medieval pandemics such as the Black Death were mostly bacterial in origin, as were probably most Spanish flu deaths. With antibiotics, sewers, and better food, we now live longer and don’t expect such mortality events, but the WHO uses this threat regardless.
Thus, the WHO has been reduced to misrepresenting fragile evidence (e.g. ignoring technology developments that can explain rising reports of outbreaks) and opinion pieces by sponsored panels in order to support the narrative of rapidly rising pandemic risk. Even Covid-19 is getting harder to use. If, as appears most likely, it was an inevitable result of laboratory manipulation, then it no longer even serves as an outlier. The WHO’s pandemic agenda is squarely targeted at natural outbreaks; hence the need for “Disease X”.
The WHO (and the World Bank) follow a similar approach in inflating financial Return on Investment (ROI). If you received an email promoting over 300 to 700 times return on a proposed investment, some may be impressed but sensible people would suspect something amiss. But this is what the Group of Twenty (G20) secretariat told its members in 2022 for return on investment on the WHO’s pandemic preparedness proposals.
The WHO and the World Bank provided the graphic below to the same G20 meeting to support such astronomical predictions. It is essentially subterfuge; a fantasy to mislead readers such as politicians who are too busy, and trusting, to dig deeper. As these agencies are intended to serve countries rather than fool them, this sort of behavior, which is recurrent, should call into question their very existence.
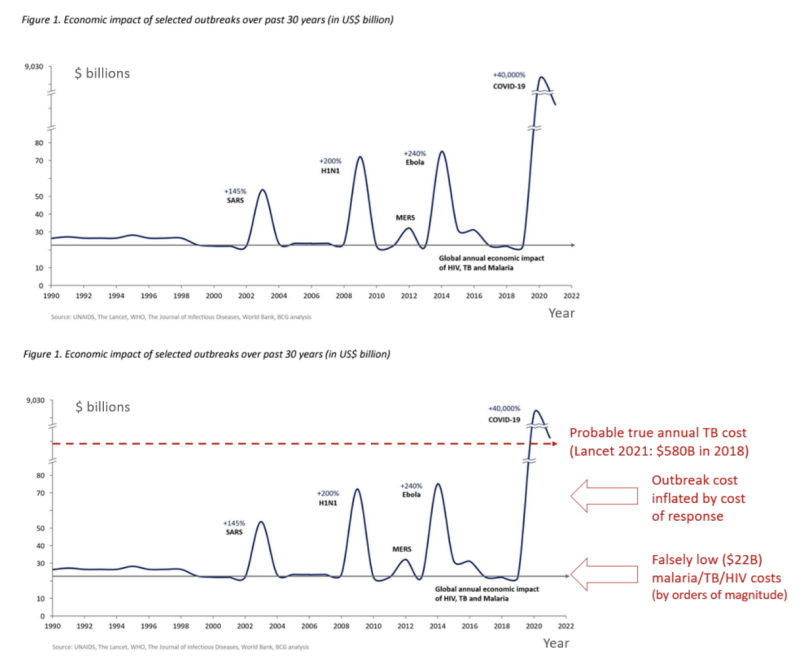
Figure 1 from Analysis of Pandemic Preparedness and Response (PPR) architecture, financing needs, gaps and mechanisms, prepared by WHO and the World Bank for the G20, March 2022. Lower chart modified by REPPARE, University of Leeds.
A virus like SARS-CoV-2 (causing Covid-19) that mostly targets the sick elderly with an overall infectious mortality rate of about 0.15% will not cost $9 trillion unless panicked or greedy people choose to close down the world’s supply lines, implement mass unemployment, and then print money for multi-trillion-dollar stimulus packages. In contrast, diseases that regularly kill more and much younger people, like tuberculosis, malaria, and HIV/AIDS, cost far more than $22 billion a year in contrast.
A 2021 Lancet article put tuberculosis losses alone at $580 billion/year in 2018. Malaria kills over 600,000 children annually, and HIV/AIDS results in similar numbers of deaths. These deaths of current and future productive workers, leaving orphaned children, cost countries. Once, they were the WHO’s main priority.
Trading on a Fading Reputation
In selling the package, the WHO seems to have abandoned any attempt at meaningful dialogue. They still justify the surveillance-lockdown-mass vaccinate model by the logic-free claim that over 14 million lives were saved by Covid vaccines in 2021 (so we all have to do that again). The WHO recorded a little over 3 million Covid-related deaths in the first (vaccine-free) year of the pandemic. For the 14 million ‘saved’ to be correct, another 17 million would somehow have been due to die in year two, despite most people having gained immunity and many of the most susceptible having already succumbed.
Such childish claims are meant to shock and confuse rather than educate. People are paid to model such numbers to create narratives, and others are paid to spin them on the WHO websites and elsewhere. An industry worth hundreds of billions of dollars depends on such messaging. Scientific integrity cannot survive in an organization paid to be a mouthpiece.
As an alternative, the WHO could advocate for investment in areas that promoted longevity in wealthy countries – sanitation, better diet and living conditions, and access to basic, good medical care.
This was once the WHO’s priority because it not only greatly reduces mortality from rare pandemic events (most Covid deaths were in people already very unwell), but it also reduces mortality from the big endemic killers such as malaria, tuberculosis, common childhood infections, and many chronic non-communicable diseases. It is, unequivocally, the main reason why mortality from major childhood infectious diseases like measles and Whooping cough plummeted long before mass vaccinations were introduced.
If we concentrated on strategies that improve general health and resilience, rather than the financial health of the pandemic industrial complex, we could then confidently decide not to wreck the lives of our children and elderly if a pandemic did arise.
Very few people would be at high risk. We could all expect to live longer and healthier lives. The WHO has elected to leave this path, instill mass and unfounded fear, and support a very different paradigm. While the Pandemic Agreement is not essential to it, it is an important part of diverting further funds to this agenda and cementing this corporatist approach into place.
The United States has done well by stepping out of this mess, but continues to push many of the same fallacies and was instrumental in sowing the mess we now reap. While a few other governments are questioning, it is hard for any politicians to stand with truth when a sponsored media stands squarely elsewhere.
Society is once more enslaving itself, at the behest of an entitled few, facilitated by international agencies that were set up specifically to guard against this. At the coming World Health Assembly, the pandemic fairytale will almost certainly prevail.
The hope is that a well-deserved erosion of trust will eventually catch up with the global health industry and too few countries will ratify this treaty for it ever to come into force. To fix the underlying problem though and derail the pandemic industry train, we will need to rethink the whole approach to cooperation in international health.
David Bell, Senior Scholar at Brownstone Institute, is a public health physician and biotech consultant in global health. David is a former medical officer and scientist at the World Health Organization (WHO), Programme Head for malaria and febrile diseases at the Foundation for Innovative New Diagnostics (FIND) in Geneva, Switzerland, and Director of Global Health Technologies at Intellectual Ventures Global Good Fund in Bellevue, WA, USA.
Klaus Schwab, Sophist

By Laurie Calhoun | The Libertarian Institute | May 1, 2025
The existence of Klaus Schwab became known to much of the thinking world during the Coronapocalypse, when so-called conspiracy theories began to flourish about the use of the novel COVID-19 virus as a pretext for reconfiguring the world. The “Great Reset” and the “New Normal” began to be spoken of fondly by bureaucrats back in 2020, shortly after the in some ways incomprehensibly influential Schwab co-authored with Thierry Malleret a short book extolling just those concepts: Covid-19: The Great Reset.
The work, or paraphrased excerpts of it, must have been spam-emailed to every government official and mainstream media journalist on the planet, because in no time pundits and their parrots in the press were gushing about the Great Reset, essentially a Brave New World to come (had none of them read Aldous Huxley’s classic work, or did they simply not understand it?). Nearly every influential person with a microphone was emitting the expression “Everything has changed,” insisting that this was because of the emergence of the novel coronavirus, not the government policies enacted in response to it. Schwab was lurking behind the scenes from the beginning, proffering gaslighting homilies and question-begging arguments camouflaged as benevolent recommendations and facts:
“The worldwide crisis triggered by the coronavirus pandemic has no parallel in modern history.”
In truth, “Everything changed” only because government officials changed everything, by closing national borders, locking down entire populations, preventing groups from assembling, and shutting down schools and all but specially designated “essential” businesses. Human beings were required to wear masks nearly everywhere they went, and those who demurred were treated as miscreants and pursued by the police. The insistence by politicians, bureaucrats and other opinion makers that “Everything has changed” was curiously reminiscent of how officials rationalized a massive and ruthless assault on Afghanistan and Iraq in the aftermath of crimes committed on September 11, 2001, by a small group of persons hailing primarily from Saudi Arabia. (Induction on two cases: when someone starts chiming, “Everything has changed!” in order to persuade you to do something or to support some initiative, you should probably turn around and walk away.)
Klaus Schwab founded and led the World Economic Forum (WEF) for more than fifty years. Many of what were revealed during the pandemic period to be the most brazen authoritarians among ostensibly democratic world leaders have connections to the organization. Canadian Prime Minister Justin Trudeau, New Zealand Prime Minister Jacinda Ardern, and French President Emmanuel Macron are notable examples of leaders who punished and even ostracized citizens for daring to defy their administration’s draconian COVID policies. Schwab recently resigned from his position, but whether that was because of age—he was born in 1938—or scandal matters little at this point, for his legacy has been secured throughout much of the world.
Key features of the Great Reset were to foist ESG (Environmental, Social and Governance investing) on people transnationally or, perhaps more accurately, meta-nationally. We have seen that elements of Schwab’s Weltanschauung have indeed made their way into not only federal government policies, with Green New Deals and carbon-limiting programs imposed in many parts of the planet, but also global corporate initiatives, as many companies now boast about their “environmental and social conscience,” using this as a marketing tool. Under the “Social Governance” guise of the ESG program, enthusiastic efforts to expand DEI (Diversity, Equity, and Inclusion) frameworks throughout the spheres of education and business have led to the appearance of “trans flags” waving alongside national flags at government buildings in what can only be characterized as a bizarre obsession with the subset of human beings, oddly in ascendance, who are said to have been born with the wrong set of genitalia.
One of the more extreme consequences of DEI has indeed been the effusive promotion of a radical trans agenda, which is arguably both homophobic and misogynistic, promoting as it does a grotesque caricature of femininity, exemplified by the skimpily clad and seemingly ditsy Dylan Mulvaney (remember the Budweiser ads?), while essentially denying the possibility of androgyny. In the name of inclusion, biological males (persons in possession of a Y chromosome) have been allowed to compete with females (persons devoid of a Y chromosome) in sports, with female competitors predictably forced to forego awards and scholarships as a result. Female athletes whose sports involve contact with competitors have been physically endangered by the admission of males into their sphere, as is evidenced by the case of volleyball player Payton McNabb and the 2024 Olympic boxing controversy, when two competitors who had previously failed a female gender test (for Y chromosome and testosterone levels) were permitted to compete. On top of all of those clear and present dangers, females in locker rooms have been faced with the prospect of seeing a penis dangling before them as they change their clothes or shower. Rather than attempt to protect females, policymakers were somehow persuaded by radical trans activists that males who decreed themselves to be female needed to be protected instead.
The incomprehensible power of the radical trans facet of the DEI agenda also brought about the enactment of laws which criminalize the “mis-pronouning” of persons who, despite having been born male, self-identify as female, or vice versa. Or neither, which necessitates, by law in some places now, that their interlocutors restrict personal pronoun usage to ‘they/them’. The latter is needless to say a no-win arrangement, for in complying with pronoun laws, one is thus obliged to commit a crime of grammar.
On the New Green Deal front, the European Union is continually devising new policies which attest to its commitments to the New Normal as envisioned by Schwab’s WEF, perhaps the most notorious slogan of which is “You’ll own nothing and be happy.” Countless memes have satirized the WEF leader for exhorting people to eat insects and stay in their “pods,” on the grounds that livestock and travel are allegedly a menace to the future of the planet. (Note: the persons who attend the ever-proliferating conferences on the environment or serve as parliament members of the EU generally fly to their meetings, sometimes in private jets.) Earnest discussion of the possibility of “15-minute cities,” where people do not need to (or are not allowed to) travel farther than fifteen minutes from their domicile has been taken up among local council members in “green-savvy” communities.
The list of rules and regulations already imposed by the European Union is seemingly endless, but to offer only two recent examples: plastic bottles sold in Europe are now required to have their caps affixed to them, and single-serving portion containers (such as are used at bed and breakfast hotels for jam, butter, honey, etc.) are in the process of being outlawed, despite having been devised as a means not only of convenience but also to prevent cross-contamination between unrelated guests. Only time will tell whether bureaucrats eventually side with public health officials or environmentalists in the latter case.
Far more important for the future of free people are the persistent censorship measures in the United Kingdom, Europe, Australia and beyond, modeled after anti-misinformation and surveillance policies aggressively enforced in many countries during the COVID period. To the shock of many thinking people, governments have taken it upon themselves to monitor the social media posts of citizens and to criminalize the expression of what are deemed unacceptable opinions, an obvious legacy of the COVID period, when persons who disagreed with the government were roundly denounced as agents of misinformation who needed to be de-platformed and silenced, lest they kill anyone with their dangerous ideas. Strikingly, reports of vaccine injury were not even false (misinformation), according to the censors themselves, but instead “malinformation,” which officials regarded as having the potential to prevent people who needed the “vaccine” from getting it.
Looking back at the surprising convergence among governments about the necessity of global lockdowns and, later, universal vaccination in the face of a virus which primarily endangered elderly and already infirm persons, it is clear that Schwab’s work served as a sort of template for how to communicate with constituents and conduct public affairs. Paternalism reigned (or, if you prefer, “maternalism” à la Nurse Ratched), as citizens were spoken to by political leaders in condescending tones as though they were toddlers who needed to be protected from themselves. This approach to governance can be summed up in a phrase: Children are to be seen, not heard.
Citizens were told that it was wrong to do their own research because only “the experts,” such as pandemic guru Anthony Fauci knew what they were doing. Despite having repeatedly lied in insisting that the virus had emerged naturally, having somehow leapt from a bat to a human being (when someone in Wuhan ate a bowl of soup?), Fauci himself, we now know, promoted and funded the gain-of-function research which culminated in the very existence—and potency—of the virus. Throughout this period of history, persons who dared to dissent from the dictates and narratives of the government were decried as enemies of humanity who needed to be controlled in order to protect other people from their nefarious tendencies. Notably, Robert F. Kennedy, Jr., author of The Real Anthony Fauci (a true tale of moral horror), who now serves as secretary of Health and Human Services (HHS) in Donald Trump’s second administration, was publicly derided and discredited as an insane conspiracy theorist throughout Joe Biden’s presidency.
The conduct of governments during the period of history from 2020 to 2023 was so confounding and preposterous that a plethora of bona fide conspiracy theories continued to emerge, reaching a peak with the release of the alleged miracle vaccine, which everyone on the planet was first encouraged (through coaxing and bribery) and then, in some cases, required to line up for, on pain of punishment for failure to comply. Some of the theories were quite creative, asserting, for example, that the shots were introducing microchips into the bodies of the recipients, or would turn them into frogs. But the term antivaxxer was affixed to anyone who declined the shot, whatever their reason, with everyone in that group assimilated and depicted as intellectually inept for defying what were claimed by officials at the time to be the dictates of common sense.
Some people, whether with formal training in science or simply endowed with critical thinking skills, understandably expressed skepticism about the new m-RNA therapy shot which they were told would eradicate the virus, while being simultaneously told that natural immunity was inadequate and that persons who already recovered from the virus would still need to undergo vaccination. Because a vaccine, by definition, exploits the subject’s own immune system, anyone with even a modicum of logical acumen must have understood that the new miracle vaccine, which depended on the immune system itself, would only work as advertised if, in fact, natural immunity was possible. This flagrant contradiction was not recognized or acknowledged as such by inept (or, in some cases, mercenarily corrupt) government officials and public health pundits, but it was the most obvious sign to people yet to be indoctrinated into the COVID cult (or not on the Big Pharma dole) that something was seriously awry.
The “Natural immunity is not possible, but this vaccine is necessary and will save you!” contradiction no doubt inspired some of the ever-mutating and proliferating theories about what was really going on. In Covid-19: The Great Reset, Schwab himself refers to antivaxxers as a dangerous impediment to getting through the crisis, and the term came swiftly to be used to denounce anyone who raised even doubts grounded in logic and science about the wisdom of submitting to an experimental treatment in cases where the person’s chances of death from the virus were quite low, as was true for all healthy young persons, and had already been demonstrated in each particular case of anyone who had recovered from previous infection.
The Pentagon required all service persons to take part in the experimental trial of the mRNA therapy, whether or not they had already recovered from infection. The more than 8,000 troops who refused the shot were discharged without pay in 2021, and the military vaccine mandate was not rescinded until 2023. Since assuming office in 2025, Pete Hegseth, Trump’s new defense secretary, has been apologizing to those persons and attempting to make amends, acknowledging that the order to take an experimental vaccine was in fact illegal and that no one was obliged to follow illegal orders. The true motives and sincerity of the new administration on this matter will be seen in how they treat the persons who suffered vaccine injury as a result of having undergone the procedure, under the erroneous belief that Joe Biden’s secretary of defense, Lloyd Austin, knew what he was doing when he ordered the entire military corps to follow his über-masked, serially vaccinated and boosted example. If the government extends its offer of compensation only to healthy troops, in an effort to woo them back into service, and ignores the persons who were disabled by the vaccine, or the individuals and families wrecked by being plunged precipitously into penury, then it will be safe to conclude that Hegseth’s apology tour is no more and no less than a measure intended to mitigate the ongoing recruitment crisis.
There seemed to be grounds for hope that the United States had managed to extricate itself from the totalitarian clutches of meta-bureaucrats such as Klaus Schwab and their “Fifty Year Plans” for humanity when Donald Trump defeated Kamala Harris (who to this day has pronouns in her profile at X) in the November 2024 presidential election. The new president immediately rescinded all DEI initiatives implemented under Biden and enacted numerous executive orders in an effort to protect women, and restore a modicum of sanity to what had become a surreal situation, by boldly asserting the biological fact that no matter how many body parts a male human being chooses to cut off or modify, every remaining cell in his body will still contain a Y chromosome. Trump also acted swiftly to criminalize the scandalous medical practice of mutilating the genitalia of minors. Both Trump and his vice president, J.D. Vance, repeatedly pronounced that free speech would always prevail in the United States as a fundamental pillar of democracy, and they vociferously denounced the censorship going on abroad.
Vestiges of the New World Order, however, can be seen in the United States, for example, the requirement that all citizens who wish to travel or enter a federal building be in possession of a Real ID. This measure, too, which begins in May 2025, having been planned long ago, in the aftermath of September 11, 2001, bears similarities to some of what was going on during the COVID period, when tracking apps and data collection at borders were nearly ubiquitous. More and more data about citizens continues to be collected by governments, and remnants of the health documentation requirements during the COVID period can be seen in the visas now needed to travel to countries where formerly a passport sufficed. Restriction of movement reached a peak during the COVID period, but the apparatus now exists and with a bit of tweaking could be used to stop anyone, anywhere, from relocating at the caprice of government officials, whoever they may be, and whatever their priorities.
The removal of students from campuses in the United States for daring to speak out against the government’s continuing support of the indiscriminate bombing of Gaza suggests that Trump, like Biden and Harris, supports free speech only so long as it does not threaten his own plans for the country or its satellite state, Israel. The libertarians who voted for Trump were needless to say thrilled when he followed through on his promise to pardon Ross Ulbricht, the founder of Silk Road who had received a double life sentence plus forty years with no possibility of parole. In choosing to vote for Trump, however, libertarians had somehow forgotten or chose to ignore the fact that Julian Assange was thrown into Belmarsh prison under Trump’s watch. (I am aware that many persons vote according to a “lesser evil” calculation, but the fact remains: the worst persecution of Assange occurred under Trump.) The fact that U.S. government drones are now acknowledged to be flying above U.S. skies (they were under Biden as well, although this was denied at the time), reveals that surveillance of residents remains a priority of the ostensibly new administration.
Antiwar activists—some of whom voted for Trump—were hopeful that he was sincere when he promised on the campaign trail not to start but to end wars. Even more welcome, albeit frankly astonishing, was Trump’s assertion on February 13, 2025, not long after having re-assumed the presidency, that he would like to cut the $800 billion Pentagon budget in half and work for the abolition of nuclear weapons. Pacific hopes were swiftly dashed less than two months later when, immediately after hosting Israel Prime Minister Benjamin Netanyahu (for the second time in 2025), Trump announced on April 7, 2025, a new, even bigger, $1 trillion defense budget, accompanied by his customary raving about how splendid the U.S. military will be, thanks to his management.
In a welcome change to citizens concerned about government overreach and the massive federal debt, the Department of Government Efficiency (DOGE), under the direction of Elon Musk, has been purging programs and canceling contracts relating to DEI and other parts of the Schwab “New Normal” agenda, including regulations intended to promote the Green New Deal and expand government power over citizens’ lives. The era of big government, however, is obviously not behind us. Along with his sudden imposition of extreme tariffs and announcement of a shocking 25% increase in defense spending, Trump’s strange fascination with the future possible annexation of Greenland, Canada, and Gaza, does not bode well for the future of free people. The idea that the leader of one country may simply “buy” another country or a part of another country (in the case of Gaza) reflects the very megalomania intrinsic to supra-national organizations such as the WEF and characters such as Klaus Schwab who attempt to impose their will on the rest of humanity.
Setting all of those substantial concerns aside, at the very least we can take solace in the fact that Klaus Schwab is no longer calling the WEF shots and penning flagrantly sophistic pamphlets replete with non sequiturs and gaslighting guidance masquerading as benevolence. Goodbye and good riddance, Herr Professor Doktor Schwab, we will not miss you. Alas, the WEF continues on (funded by not only a congeries of self-interested global corporations, but also NGOs and, by transitivity, unwitting taxpayers), and the danger it poses thus remains. Self-deluded officials named as global thought leaders will continue to comply with the WEF, as was exemplified by former New Zealand Prime Minister Jacinda Ardern, who is explicitly singled out for praise in Covid-19: The Great Reset.
Bureaucrats, for their part, will continue to conduct themselves as bureaucrats do, amassing power, devising new rules and regulations, and imposing arbitrary policies by all means necessary, as we witnessed throughout the COVID era. Peter Brabeck-Letmathe, the recently named interim chairman of the WEF, is a former CEO of Nestlé who famously claimed that people have no right to water. Unbeknownst to many of the millions of people who purchase and imbibe bottled water everyday, much of it derives from government-treated municipal water supplies filtered and then poured into plastic bottles to look as though it was sourced from natural spring wells such as Evian, Perrier, Pellegrino, Gerolsteiner, et al. It is unclear how much power Brabeck-Letmathe will exert, or for how long, but he does happen to look empirically indistinguishable from the super villains depicted in movies, so there is some chance that if he begins spouting out gaslighting prescriptions about how all human beings ought to behave, at least some among us will shudder, turn around and walk away.
European Union To Use Digital Services Act to Crack Down on Online Vaccine “Misinformation”
By Cindy Harper | Reclaim The Net | April 28, 2025
The European Union has begun wielding the controversial censorship law, the Digital Services Act (DSA), to intensify its crackdown on what it labels “misinformation” about immunization efforts. Framing the campaign as necessary for safeguarding democracy, the European Commission pointed to the European Democracy Action Plan and a reinforced Code of Conduct on Disinformation as foundational measures. According to the Commission, these initiatives, aligned with the DSA, create a “strong framework” to regulate content across major online platforms and search engines.
Citing a sharp rise in measles cases across Europe, the Commission has drawn renewed attention to immunization programs. A health spokesperson, speaking to Vaccines Today, warned, “The Commission is very concerned by the spike in reported measles cases in Europe – particularly as the number doubled in 2024 compared to 2023.” The spokesperson noted that the institution is actively cooperating with national health authorities and the European Centre for Disease Prevention and Control (ECDC) to manage the outbreaks.
The Commission argues that low vaccination rates, described as “sub-optimal” coverage, are enabling the spread of diseases like measles, which can otherwise be prevented through “safe and efficient vaccination.” Efforts are reportedly underway to support national governments in strengthening immunization programs and ensuring a steady vaccine supply across the EU while cracking down on critical online speech.
Public distrust in health authorities and vaccination campaigns is being framed as the root cause of falling immunization rates. EU officials are quick to blame what they term “misinformation” and “disinformation,” suggesting that any narrative diverging from official positions is inherently dangerous.
The Commission emphasized, “Protecting Europe from the harmful effects of disinformation, information manipulation, and interference is a high priority for the Commission,” making clear its commitment to aggressively policing speech under the guise of public health.
Meanwhile, the European External Action Service (EEAS), the EU’s diplomatic and intelligence apparatus, has ramped up its monitoring and analysis of information flows. Working hand-in-hand with member states and international organizations, it now targets so-called disinformation across an expanding array of policy areas, raising serious concerns about political overreach.
Alongside its censorship push, the Commission continues to roll out a series of public relations campaigns intended to shepherd citizens toward preferred viewpoints. Initiatives like United in Protection promote vaccination using “reliable, evidence-based information,” though what qualifies as “reliable” is determined solely by authorities. The EU has also created the European Vaccination Information Portal and collaborated with bodies such as the ECDC and European Medicines Agency (EMA) to saturate public discourse with officially approved messages.
Vaccination advocacy has been woven deeply into EU policy frameworks. Europe’s Beating Cancer Plan and the EU4Health Program are now tied to vaccine promotion, with projects like Overcoming Obstacles to Vaccination aiming to remove barriers to vaccine access, all while dismissing legitimate public hesitations as obstacles to be overcome rather than concerns to be addressed.
Featured Video
The Iran War has destroyed fertilizer markets and farmers everywhere, almost
or go to
Aletho News Archives – Video-Images
From the Archives
Truth, History and Integrity
By Gilad Atzmon | March 13, 2010
… As devastating as it may be, at a certain moment in time, a horrible chapter was given an exceptionally meta-historical status. Its ‘factuality’ was sealed by draconian laws and its reasoning was secured by social and political settings. The Holocaust became the new Western religion. Unfortunately, it is the most sinister religion known to man. It is a license to kill, to flatten, no nuke, to wipe, to rape, to loot and to ethnically cleanse. … Read full article
Blog Roll
 Aletho News
Aletho News- Iran rejects US assassination claim, says Washington trying to whitewash its own crimes against Iranians
- The Iran War has destroyed fertilizer markets and farmers everywhere, almost
- Capitulate or Die: The Gaza ‘peace process’ and Western propaganda
- FSB Blows Lid on Western Plot to Hack Russian Officials’ Phones — But Here’s the Shocker
- Do Palantir’s bosses have blood on their hands over the Starobelsk massacre?
- US Eyes Spreading its Nuclear Footprint Deeper into Europe – Report
- Kiev admitted it launched drones at NATO member – media
- Russia Raises Alarm Over Ukraine’s Surging Black Sea Terrorist Activity
- ‘Luring Russia into war’
- Russia accuses France and the UK of piracy over cargo ship seizure
- If Americans Knew
- Israeli settlers, soldiers, gov’t go all out against West Bank Palestinians – Daily Update
- A Slow-motion Execution of the West Bank Health System
- The Palestinian journalists held in Israel’s ‘cemeteries for the living’
- Super PAC Network Backing Connie Chan Received Hundreds of Thousands from AIPAC
- Israel’s Solution to the Gaza Problem Is Well Underway
- UK Bans Prominent Commentators Over Their Statements on Israel
- Israel’s killing machine deepens its invasion into Lebanon – Daily Update
- ‘To call it a ceasefire is a joke’: Israeli soldiers share rare accounts from Gaza with AP
- Israeli Espionage: How Israel and its American agents stole US uranium
- From Paul Findley to Thomas Massie: How the Israel Lobby Purges Republican Dissenters
- No Tricks Zone
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
- Germany’s AfD Party Calls Debunked Climate Scenarios “Greatest Fraud In Human History”
- Researchers Find Rapid Global Warming Phase At End Of Last Ice Age (Ca.18,000 Years Ago)
- Even The DNA Of Single-Celled Plankton Can Upend Alarmist Arctic Sea Ice Melt Claims
- Scandal: Although Climate Panic Is Canceled By IPCC, Europe’s Policymakers Continue With Their Crushing Policies
- How Once Hardcore Climate Alarmist Lucy Biggers Realized It Was All A Scam, Brainwashing
- German Expert: “No Climate Crisis” …”Warming Generally Better For Humanity”
