Top FDA official admits she refused the Covid-19 vaccine while pregnant
A senior regulator’s admission reveals uncomfortable truths about silence, ethics and trust inside the FDA
By Maryanne Demasi, PhD | May 22, 2025
One of the most powerful figures at the US Food and Drug Administration (FDA) has admitted she refused the Covid-19 mRNA vaccine while pregnant—even as her agency promoted it as “safe and effective” for all pregnant women.
Dr Sara Brenner’s explosive disclosure, made on 15 May 2025 at the MAHA Institute Round Table in Washington DC, is as revealing as it is troubling.
A preventive medicine physician, Brenner has worked at the FDA since 2019. As the FDA’s Principal Deputy Commissioner—and briefly its Acting Commissioner—Brenner was at the centre of decision-making.
Dr Sara Brenner on 15 May 2025 at the MAHA Institute
Prior to that she was Chief Medical Officer for diagnostics and was detailed to the White House to support the Biden administration’s Covid-19 response. She didn’t just participate in the pandemic response, she helped shape it from within.
“Knowing what I knew—not only about nanotechnology, about medicine, about the medical countermeasures—but also having a very strong and firm grounding in bioethics… there were many things that were not right,” she told the audience.
That someone with her seniority and access to internal data privately rejected the vaccine, while her agency promoted it to millions of pregnant women, presents a profound ethical dilemma.
Brenner’s concerns about mRNA safety
Brenner explained that her decision was driven by a lack of safety data, particularly around the biodistribution of the vaccine’s lipid nanoparticles (LNPs)—the tiny fat particles used to deliver the mRNA into cells.
“It was unknown at the time what the biodistribution patterns of those products were… That was my primary concern, and that exposure I was very concerned about,” said Brenner.
She had reason to be cautious.
As a nanomedicine expert who built an MD/PhD program in the field, Brenner had spent years researching the “biodistribution, excretion, metabolism and toxicities associated with engineered nanoparticles.”
“Materials that don’t exist in nature—there’s a lot of unknowns,” said Brenner.
She warned that unintended toxic effects—especially in vulnerable populations like pregnant women—could not be ignored.
“Regardless of the medical product or the intervention, there’s always going to be the need to evaluate both the intended outcomes… and the unintended consequences,” she cautioned.
Warnings ignored
Brenner’s concerns echoed those raised in 2021 by Canadian immunologist Dr Byram Bridle, who first exposed internal documents from Japan’s regulatory agency showing that LNPs didn’t remain at the injection site, but travelled throughout the body and accumulated in organs including the ovaries, liver, spleen and bone marrow.
At the time, Bridle’s warnings were aggressively dismissed. His reputation took a hit, and he faced institutional censure from the University of Guelph, where he was a professor, for speaking out against vaccine mandates.

Dr Byram Bridle, Canadian immunologist. Photo credit: Kenneth Armstrong
Now, Brenner’s comments confirm that these concerns were not only valid—they were quietly shared at the highest levels of the FDA.
During the event, Brenner also revealed that her worries extended to breastfeeding and potential exposure to her child after birth.
A 2022 study published in JAMA Pediatrics detected vaccine-derived mRNA in the breast milk of vaccinated mothers for at least 48 hours—the very scenario Brenner had feared.
Yet the FDA made little effort to publicly investigate or address the findings, dismissing them with the vague reassurance that there was “no evidence of harm.”
No mandate for Brenner?
It’s unclear how Brenner managed to avoid the vaccine mandate that applied to all federal employees at the time. She didn’t say. Perhaps she received a religious or medical exemption—but she left that part out.
What she did reveal was that she had concerns—deep enough not to take the vaccine during her pregnancy. Yet she said nothing publicly, while her agency told millions of other women it was safe.
For many, that silence is hard to accept and it has left many asking why she didn’t warn other women about a product with ‘zero’ clinical safety data in pregnancy.
No one but Brenner knows the full story. But the ethical contradiction is hard to ignore.
Silence inside the castle
Brenner acknowledged the immense pressure inside the FDA to stick to the official narrative.
“They don’t let you get very far out of the castle at FDA with your talking points,” she admitted nervously.
She described the period as a “dark night of the soul” for many civil servants, a time when even “very obvious things” took bravery to say.
She eventually found support through a group called Feds for Medical Freedom—federal workers advocating for informed consent, bodily autonomy, and pushing back against government overreach.
A culture change?
Today, under a new administration, Brenner says the culture inside the FDA is shifting. She praised Commissioner Dr Marty Makary and said transparency is finally becoming a priority.
“We’re moving very quickly to make it such that there will be more transparency… so that people can see and evaluate for themselves what the truths are.”
But Brenner’s remarks won’t undo what has already happened—especially to those who were vaccine injured or whose pregnancies were affected.
What her comments do offer is a rare glimpse into the internal dynamics of a government institution that issued sweeping public assurances while failing to acknowledge its own uncertainty.
“There was no acknowledgement of what was unknown. There were only statements and assertions that were really more like beliefs,” Brenner said of the FDA’s messaging during the pandemic.
That may be her most important admission.
This is more than a story about one woman’s personal decision. It is a story about institutional culture, regulatory failure, and the consequences of silence.
Those who spoke up were punished. Those who stayed silent kept their jobs and reputations. And those who were forced to comply were often left to deal with the collateral damage.
When asked whether she believed she had made the right decision in refusing the Covid-19 vaccine, Brenner replied simply, “I believe so.”
Now that she has spoken, the question remains — who else knew, and said nothing?
FERTILITY FALLOUT: MRNA VACCINES LINKED TO OVARIAN DAMAGE
The HighWire with Del Bigtree | May 15, 2025
Following last week’s spotlight on a preprint showing lower conception rates in vaccinated women, a new peer-reviewed rat study shows a 60% drop in ovarian egg reserves after mRNA vaccination. With FDA meetings looming, Del and Jefferey raise urgent questions about long-term reproductive risks, and why similar research still isn’t being done in women.
‘There Is Overwhelming Evidence to Call for a Moratorium on mRNA COVID Jabs’: New MAHA Chief Medical Advisor

By Jon Fleetwood | May 15, 2025
British cardiologist and author Dr. Aseem Malhotra, the newly appointed Chief Medical Advisor to the Make America Healthy Again (MAHA) initiative, says there is “overwhelming evidence” to ban the COVID-19 mRNA shots.
Dr. Malhotra is a former U.K. government and long-time ally of MAHA leaders like HHS Secretary Robert F. Kennedy Jr. (RFK Jr.) and NIH head Dr. Jay Bhattacharya.
He’s campaigned for taxes on sugary drinks, worked to lower the amount of Brits taking statins unnecessarily, and worked with government leaders to remove ultraprocessed foods from hospitals and schools, per The Daily Mail.
Though Malhotra is not formally employed by the federal government, he will serve as a leading voice of the movement and work closely with grassroots groups to advance its policy agenda.
In a Wednesday Twitter/X post, the British best-selling author (@DrAseemMalhotra) left no question where he stands on the COVID jab.
“It’s what you’ve been waiting for,” he wrote. “There is OVERWHELMING evidence to call for a moratorium on the mRNA covid jabs & help the vaccine injured. Let it rip.”
On the same day, MAHA Action, an organization founded by former Team Kennedy leadership, announced Malhotra’s appointment:
We are honored to announce that Dr. Aseem Malhotra has joined MAHA as our Chief Medical Advisor.
Dr. Malhotra is an NHS-trained Consultant Cardiologist and an internationally renowned authority in the prevention, diagnosis, and treatment of heart disease.
He has served as Honorary Council Member at Stanford’s Metabolic Psychiatry Clinic and Visiting Professor of Evidence-Based Medicine at the Bahiana School of Medicine. As Founding President of the Public Health Collaboration and a founding member of Action on Sugar, Dr. Malhotra has led national efforts to curb sugar intake and champion low-carb diets for type 2 diabetes.
He is the bestselling author of The Pioppi Diet, The 21 Day Immunity Plan, and A Statin-Free Life, and played a key advisory role for the UK government on the link between obesity and COVID-19. His publications have garnered an Altmetric score exceeding 10,000, one of the highest worldwide for a clinical doctor.
We are thrilled to welcome Dr. Malhotra to the MAHA team and look forward to the invaluable expertise and passion he brings to our mission of Making America Healthy Again.
Malhotra told Daily Mail, “It’s very clear to me that perhaps this is the most important issue that has galvanized MAHA and helped elect President Trump,” he said, referring to criticism of mRNA COVID injections.
“There is a pandemic of the vaccine injured. We can’t make America healthy again if we don’t address this.”
The doctor believes there are “hundreds of thousands” of vaccine injuries and wants states to pass legislation halting use of the drugs because they have shown “more harm than good and never should have been rolled out in the first place.”
CDC data show 38,541 deaths have been linked to the COVID jab since 2020, but if fewer than 1% of adverse events are reported—as a 2010 HHS-funded Harvard analysis suggests—the real number could exceed 3.8 million, compared to just 7,109 deaths that got propoxyphene pulled after nearly 30 years on the market.
Malhotra recently told Fox News that he began to doubt the safety of the COVID shot after his father died after suffering cardiac arrest.
Now leading America’s most unapologetic health freedom initiative, Malhotra is making one thing crystal clear: the COVID shot crisis isn’t over—it’s just finally being confronted.
BLOOD CLOTS IN 5 MINUTES? CELL PHONE RADIATION UNDER THE MICROSCOPE
The HighWire with Del Bigtree | May 15, 2025
Jefferey Jaxen breaks down a stunning ultrasound study showing real-time blood changes after just 5 minutes of smartphone exposure. With links to fertility issues, cancer, and hormonal disruption, the data raises urgent questions about the health impacts of EMF and why government agencies are choosing not to act.
The Deep State Goes Viral: Foreword
By Jeffrey A Tucker | Brownstone Institute | May 12, 2025
The following is Jeffrey Tucker’s Foreword introduction to Debbie Lerman’s new book, The Deep State Goes Viral: Pandemic Planning and the Covid Coup.
It was about a month into lockdowns, April 2020, and my phone rang with an unusual number. I picked up and the caller identified himself as Rajeev Venkayya, a name I knew from my writings on the 2005 pandemic scare. Now the head of a vaccine company, he once served as Special Assistant to the President for Biodefense, and claimed to be the inventor of pandemic planning.
Venkayya was a primary author of “A National Strategy for Pandemic Influenza” as issued by the George W. Bush administration in 2005. It was the first document that mapped out a nascent version of lockdowns, designed for global deployment. “A flu pandemic would have global consequences,” said Bush, “so no nation can afford to ignore this threat, and every nation has responsibilities to detect and stop its spread.”
It was always a strange document because it stood in constant contradiction to public health orthodoxies dating back decades and even a century. With it, there were two alternative paths in place in the event of a new virus: the normal path that everyone is taught in medical school (therapeutics for the sick, caution with social disturbances, calm and reason, quarantines only in extreme cases) and a biosecurity path that invoked totalitarian measures.
Those two paths existed side-by-side for a decade and a half before the lockdowns.
Now I found myself speaking with the guy who claims credit for having mapped out the biosecurity approach, which contradicted all public health wisdom and experience. His plan was finally being implemented. Not too many voices dissented, partially due to fear but also due to censorship, which was already very tight. He told me to stop objecting to the lockdowns because they have everything under control.
I asked a basic question. Let’s say we all hunker down, hide under the sofa, eschew physical meetings with family and friends, stop all gatherings of all kinds, and keep businesses and schools closed. What, I asked, happens to the virus itself? Does it jump in a hole in the ground or head to Mars for fear of another press conference by Andrew Cuomo or Anthony Fauci?
After some fallacy-filled banter about the R-naught, I could tell he was getting exasperated with me, and finally, with some hesitation, he told me the plan. There would be a vaccine. I balked and said that no vaccine can sterilize against a fast-mutating respiratory pathogen with a zoonotic reservoir. Even if such a thing did appear, it would take 10 years of trials and testing before it was safe to release to the general population. Are we going to stay locked down for a decade?
“It will come much faster,” he said. “You watch. You will be surprised.”
Hanging up, I recall dismissing him as a crank, a has-been with nothing better to do than call up poor writers and bug them.
I had entirely misread the meaning, simply because I was not prepared to understand the sheer depth and vastness of the operation now in play. All that was taking place struck me as obviously destructive and fundamentally flawed but rooted in a kind of intellectual error: a loss of understanding of virology basics.
Around the same time, the New York Times posted without fanfare a new document called PanCAP-A: Pandemic Crisis Action Plan – Adapted. It was Venkayya’s plan, only intensified, as released on March 13, 2020, three days before President Trump’s press conference announcing the lockdowns. I read through it, reposted it, but had no idea what it meant. I hoped someone could come along to explain it, interpret it, and tease out its implications, all in the interest of getting to the bottom of the who, what, and why of this fundamental attack on civilization itself.
That person did come along. She is Debbie Lerman, intrepid author of this wonderful book that so beautifully presents the best thoughts on all the questions that had eluded me. She took the document apart and discovered a fundamental truth therein. The rule-making authority for the pandemic response was not vested in public-health agencies but the National Security Council.
This was stated as plain as day in the document; I had somehow missed that. This was not public health. It was national security. The antidote under development with the label vaccine was really a military countermeasure. In other words, this was Venkayya’s plan times ten, and the idea was precisely to override all tradition and public health concerns and replace them with national security measures.
Realizing this fundamentally changes the structure of the story of the last five years. This is not a story of a world that mysteriously forgot about natural immunity and made some intellectual error in thinking that governments could shut down economies and turn them back on again, scaring a pathogen back to where it came from. What we experienced in a very real sense was quasi-martial law, a deep-state coup not only on a national but on an international level.
These are terrifying thoughts and hardly anyone is prepared to discuss them, which is why Lerman’s book is so crucial. In terms of public debate about what happened to us, we are barely at the beginning. There is now a willingness to admit that the lockdowns did more overall harm than good. Even the legacy media has started venturing out to grant permission for such thoughts. But the role of the pharmaceuticals in driving the policy and the role of the national-security state in backing this grand industrial project is still taboo.
In 21st-century journalism and advocacy designed to influence the public mind, the overwhelming concern of all writers and institutions is professional survival. That means fitting into an approved ethos or paradigm regardless of the facts. This is why Lerman’s thesis is not debated; it is hardly spoken of at all in polite society. That said, my work at Brownstone Institute has put me in close contact with many thinkers in high places. This much I can say: what Lerman has written in this book is not disputed but admitted in private.
Strange isn’t it? We saw during the Covid years how professional aspiration incentivized silence even in the face of egregious violations of human rights, including mandatory school closures that robbed children of education, followed by face-covering requirements and forced injections for the whole population. The near-silence was deafening even if anyone with a brain and a conscience knew that all of this was wrong. Not even the excuse that “We didn’t know” works anymore because we did know.
This same dynamic of social and cultural control is fully in operation now that we are through that stage and onto another one, which is precisely why Lerman’s findings have not yet made their way to polite society, to say nothing of mainstream media. Will we get there? Maybe. This book can help; at least it is now available for everyone brave enough to confront the facts. You will find herein the most well-documented and coherent presentation of answers to the core questions (what, how, why) that all of us have been asking since this hell was first visited upon us.
THE REAL PETER MARKS REVEALED
The HighWire with Del Bigtree | May 8, 2025
Del celebrates the launch of ICAN’s “Secret Recordings: The Real Peter Marks”, a comprehensive timeline featuring documents obtained through FOIA and recorded Zoom calls with Peter Marks, M.D., former Director of the FDA’s Center for Biologics Evaluation and Research. Many of the videos show victims of severe COVID-19 vaccine injuries, as well as physicians who witnessed these injuries firsthand, pleading with the FDA to take action and inform the public of the potential risks. Get a glimpse of the press conference held in Washington, D.C., and learn how to access the full timeline—including complete video recordings and a comparison of what Marks was privately acknowledging versus what he was publicly saying about the safety of these products.
Media Slam NIH for Axing ‘Safe to Sleep’ Campaign — But Evidence Shows the Program Never Reduced SIDS Deaths
By Brenda Baletti, Ph.D. | The Defender | May 8, 2025
A National Institutes of Health (NIH) program that health officials claimed reduced the number of infants who died suddenly in their sleep fell victim late last month to budget cuts, triggering an outcry from some experts and mainstream media.
The 30-year-old “Safe to Sleep” campaign was overseen by the NIH communications office at the National Institute of Child Health and Human Development. The program cut was part of the ongoing reorganization and streamlining of the NIH.
The program, which includes TV advertisements, was created to provide guidance to parents about safe sleeping practices for infants. It advises parents to place babies on their back to sleep, use a flat firm sleeping surface, keep the sleeping area clear, use a pacifier, and breastfeed, among other lifestyle interventions. That information will remain available on the website.
North Country Public Radio, Mother Jones and other mainstream media decried the program’s cancellation.
In an article published May 5, Mother Jones claimed “Safe to Sleep” was responsible for “years of progress in reducing the number of babies that succumb to Sudden Infant Death Syndrome (SIDS).”
The article smeared Children’s Health Defense (CHD) and others who suggest that the sudden and unexplained death of thousands of infants each year, often within a few days of vaccination, may in some cases be linked to vaccines rather than to sleep hygiene.
However, the plausible association between vaccines and SIDS has been reported in peer-reviewed literature for decades.
And research published in top journals has long shown that claims about the success of the “Safe to Sleep” campaign are mistaken. SIDS deaths didn’t go down after the campaign was launched in the 1990s. The deaths were simply categorized differently because of a change to the codes used by medical examiners.
A short history of SIDS in the U.S.
A SIDS diagnosis is given when an infant under age 1 dies suddenly, typically during sleep, and an investigation into the death fails to yield a cause. However, 95% of SIDS deaths occur in the first six months of life, peaking at ages 2-4 months.
Each year, the U.S. records more than five infant deaths per 1,000 live births, far exceeding the rates in other high-income countries.
After birth defects and prematurity, SIDS is the third leading cause of death among infants. Yet the medical industry claims to remain puzzled about the cause — similar to how health officials say they don’t know what causes autism.
The SIDS diagnosis didn’t exist until the late 1960s, when the category was created in response to a rise in sudden unexplained infant deaths. In 1971, the World Health Organization’s International Classification of Diseases (ICD) assigned a code to SIDS.
The ICD is the list of about 130 categories that coroners globally use to assign the cause of death when a baby dies.
In a 2021 article in the peer-reviewed journal Toxicology Reports, vaccine researcher Neil Z. Miller provides a history of the SIDS diagnosis, noting that the rise of SIDS coincided with the first mass immunization campaigns.
In the early 1960s, the number of vaccines administered to most U.S. infants took off. The federal government began appropriating money so the CDC could work with local health departments to vaccinate all children. The agency established the CDC Advisory Committee on Immunization Practices (ACIP), which makes the recommendations for vaccines to be listed on the childhood immunization schedule.
By the end of the decade, most U.S. infants were receiving the diphtheria, pertussis, and tetanus (DPT), polio and measles vaccines, and mumps and rubella vaccines also became available.
As SIDS rates rose, so did parental concern that SIDS was connected to vaccination, but authorities assured parents that unexplained death following vaccination was “merely coincidental,” Miller wrote.
He also said that before 1979, the ICD included cause-of-death classifications associated with “prophylactic vaccination” as an official cause of death. As a result, “medical examiners are compelled to misclassify and conceal vaccine-related fatalities under alternate cause-of-death classifications.”
Instead of examining the link between vaccines and SIDS, public health researchers developed a “triple-risk model” for explaining SIDS. That model says SIDS occurs when a baby has an unknown medical condition, it is going through an important period of development where the body changes quickly, and it encounters an outside stressor, such as sleeping on its stomach.
Enter the ‘back to sleep’ campaign
The American Academy of Pediatrics (AAP) in 1992 launched a national “Back to Sleep” campaign to inform parents to have children sleep on their backs rather than on their stomachs.
In 1994, the NIH’s National Institute of Child Health and Human Development institutionalized the campaign within the agency, in partnership with organizations like the AAP, and later, companies including Johnson & Johnson and Gerber — both of which have been sued for poisoning children with their products.
NIH renamed the campaign “Safe to Sleep” in 2012.
Between 1992, when the program was started, and 2001, SIDS deaths reportedly declined a whopping 55% — a number touted in every article celebrating the program, making it appear that babies sleeping on their stomachs was the cause of SIDS, not vaccines.
However, at the same time deaths from SIDS decreased, the rate of mortality from “suffocation in bed,” “suffocation other,” “unknown and unspecified causes,” and “intent unknown” all increased significantly.
What had happened was that the classification system had changed. SIDS deaths were being reclassified by medical certifiers, usually coroners, as one of the other similar categories, Miller reported.
Research published in the journal Pediatrics — the flagship journal of the AAP — concluded that deaths previously certified as SIDs were simply being certified as other non-SIDS causes, such as suffocation, that were still essentially SIDS deaths.
That change in classification accounted for more than 90% of the drop in SIDS rates.
The Pediatrics paper showed there was no decline in overall postneonatal mortality, despite the program’s — and the AAP’s — claims to the contrary.
Others verified the Pediatrics paper’s findings, and the trend continued, as reported by multiple studies in top journals. Miller reported that, for example, “From 1999 through 2015, the U.S. SIDS rate declined 35.8 % while infant deaths due to accidental suffocation increased 183.8%.”
In 2020, infant deaths from Sudden Unexpected Infant Death (SUID) — an umbrella category that accounts for both SIDS and other unknown causes began to rise even higher, according to a study published in JAMA Pediatrics.
No codes for vaccine-related sudden deaths
Dr. Paul Thomas, pediatrician and author of “Vax Facts: What to Consider Before Vaccinating at All Ages & Stages of Life,” told The Defender in an interview last year that extensive evidence links SIDS to vaccination.
Thomas said that because there are no ICD codes for vaccination, the deaths are typically recorded as something else.
“When an infant dies, no matter how soon after vaccination, coroners and pathologists do not have any codes for vaccine-related death available as options, so these deaths are generally coded as SIDS, unknown, or suffocation.”
80% of infant deaths reported VAERS between 1990-2019 happened within 7 days of vaccination
Thomas said pediatricians are not educated about the link, so even when it clearly occurs, they don’t recognize it.
“I was taught that SIDS was due to parents smoking in the room, the room being too hot, babies co-sleeping or sleeping on surfaces that were too soft, or moms smothering their babies while nursing,” he wrote, sharing insights from his new book. “While all these factors may plausibly contribute, the primary cause has been right under our noses for decades. The vaccines!”
Miller’s analysis of sudden infant deaths in the Vaccine Adverse Event Reporting System (VAERS) showed that nearly 80% of those deaths reported to the system between 1990 and 2019 happened within seven days of vaccination.
A recent peer-reviewed study found a positive statistical correlation between infant mortality rates and the number of vaccine doses received by babies — confirming findings made by the same researchers a decade ago.
The 2018 Health Affairs study reported that the bifurcation of the U.S. mortality rates from those of other wealthy countries began in the 1980s — the same time the country saw a major uptick in childhood vaccination.
A 2023 study published in the Cureus Journal of Medical Science found that the developed nations requiring the most neonatal vaccine doses tend to have the worst childhood mortality rates.
The CDC currently recommends 76 doses of 18 different vaccines for children ages 0-18.
Child mortality researchers have also noted that sudden unexplained childhood deaths in children over 1 year old are often underestimated, and many such child deaths remain unexplained due to failure to understand or investigate causes.
A recent study in JAMA Pediatrics found that hospitalized preterm infants had a 170% higher incidence of apnea within 48 hours of receiving their routine 2-month vaccinations compared to unvaccinated babies, according to the data in a new study.
Higher infant mortality has also been linked to poor maternal health or other perinatal issues, including premature birth.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
NEW STUDY LINKS COVID VACCINE TO FERTILITY DECLINE, MISCARRIAGE RISKS
By Jefferey Jaxen | May 9, 2025
If you trust the U.S. Center for Disease Control and Prevention’s (CDC) website which states there is “no Evidence That COVID-19 Vaccines Affect Fertility,” you may be missing the bigger story.
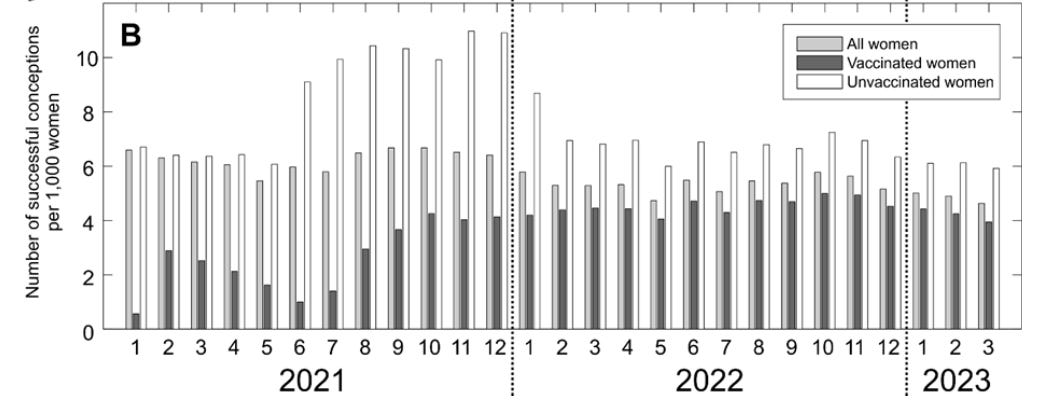
A new study using data for the number of live births for women aged 18-39 years taken from the Institute of Health Information and Statistics in the Czech Republic found from January 2021–March 2023 the following:
“During the entire study period, SCs [successful conceptions] per 1,000 women were considerably lower for women who were vaccinated, compared to those that were unvaccinated, before SC. Furthermore, SC rates for the vaccinated group were generally much lower than expected based on their proportion of the total population.”
The table below taken from the study shows that the fertility, meaning one’s ability to have a child, of unvaccinated women (clear bar) during the study period was well above vaccinated women (shaded bar) at every single time interval.
Shockingly, this is the first study to look at the relationship between COVID-19 vaccination status and rates of successful conceptions on a population level using real-world data.
Attention CDC!
This recent Czech Republic study serves to drive home previous data points.
Confidential documents obtained via FOIA from early Pfizer clinical trials showed the lipid nanoparticles, used as the mRNA delivery system in the Covid shots, bioaccumulated primarily in the female ovaries – second only to the spleen.

Meanwhile, in 2021 as the experimental Covid shot rolled out, University of Illinois researchers decided to conduct their own survey after critical masses of women noticed an alteration in their menstrual cycle. Absent any interest from U.S. health agencies and the vaccine manufactures at the time, the grassroots research did find cycle alterations were happening.

Meanwhile, the Vaccine Adverse Events Reporting System (VAERS), which has been known to capture less than 1% of actual vaccine harms, told the real story of the Covid shot.

The world is in the later innings of a fertility crisis with the US fertility rate reaching an all-time low in 2023. While fertility rates have been declining for several decades for multifactorial reasons, adding an additional layer of a Covid shot that shows evidence of further fertility reduction does little to keep society above replacement population.

Last week, news broke of a U.S. baby bonus aimed at addressing the fertility issue as ABC New reported:
“The White House has been fielding proposals aimed at persuading people to marry and have children, an effort being pushed by outside groups focused on increasing the nation’s birth rate after years of decline.
One such proposal that has been pitched to White House advisers is a $5,000 “baby bonus” to every American mother after she gives birth.”
The Trump presidency has passed the 100 day mark while RFK Jr. leads HHS with an array of dream picks at health agency point positions. Addressing and removing the root health and toxicity causes for the reduction in fertility rates is key to the future of America.
According to reports, the CDC advisory committee looks to be removing the childhood Covid shot recommendation. Will this new administration’s CDC be bold enough to publicly address the science and evidence surrounding the Covid shot’s impact on fertility?
Featured Video
The Iran War has destroyed fertilizer markets and farmers everywhere, almost
or go to
Aletho News Archives – Video-Images
From the Archives
Truth, History and Integrity
By Gilad Atzmon | March 13, 2010
… As devastating as it may be, at a certain moment in time, a horrible chapter was given an exceptionally meta-historical status. Its ‘factuality’ was sealed by draconian laws and its reasoning was secured by social and political settings. The Holocaust became the new Western religion. Unfortunately, it is the most sinister religion known to man. It is a license to kill, to flatten, no nuke, to wipe, to rape, to loot and to ethnically cleanse. … Read full article
Blog Roll
 Aletho News
Aletho News- The Iran War has destroyed fertilizer markets and farmers everywhere, almost
- Capitulate or Die: The Gaza ‘peace process’ and Western propaganda
- FSB Blows Lid on Western Plot to Hack Russian Officials’ Phones — But Here’s the Shocker
- Do Palantir’s bosses have blood on their hands over the Starobelsk massacre?
- US Eyes Spreading its Nuclear Footprint Deeper into Europe – Report
- Kiev admitted it launched drones at NATO member – media
- Russia Raises Alarm Over Ukraine’s Surging Black Sea Terrorist Activity
- ‘Luring Russia into war’
- Russia accuses France and the UK of piracy over cargo ship seizure
- Hungarian PM Magyar claims that he has obtained billions in EU funds, but what strings are attached?
- If Americans Knew
- Israeli settlers, soldiers, gov’t go all out against West Bank Palestinians – Daily Update
- A Slow-motion Execution of the West Bank Health System
- The Palestinian journalists held in Israel’s ‘cemeteries for the living’
- Super PAC Network Backing Connie Chan Received Hundreds of Thousands from AIPAC
- Israel’s Solution to the Gaza Problem Is Well Underway
- UK Bans Prominent Commentators Over Their Statements on Israel
- Israel’s killing machine deepens its invasion into Lebanon – Daily Update
- ‘To call it a ceasefire is a joke’: Israeli soldiers share rare accounts from Gaza with AP
- Israeli Espionage: How Israel and its American agents stole US uranium
- From Paul Findley to Thomas Massie: How the Israel Lobby Purges Republican Dissenters
- No Tricks Zone
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
- Germany’s AfD Party Calls Debunked Climate Scenarios “Greatest Fraud In Human History”
- Researchers Find Rapid Global Warming Phase At End Of Last Ice Age (Ca.18,000 Years Ago)
- Even The DNA Of Single-Celled Plankton Can Upend Alarmist Arctic Sea Ice Melt Claims
- Scandal: Although Climate Panic Is Canceled By IPCC, Europe’s Policymakers Continue With Their Crushing Policies
- How Once Hardcore Climate Alarmist Lucy Biggers Realized It Was All A Scam, Brainwashing
- German Expert: “No Climate Crisis” …”Warming Generally Better For Humanity”
